Summary
Abdominal aortic aneurysm (AAA) is a focal dilatation of the abdominal aorta to more than 1.5 times its normal diameter. AAAs are classified by location as either suprarenal or infrarenal aneurysms. Men of advanced age are at increased risk for their formation; smoking and hypertension are also major risk factors. AAAs are frequently asymptomatic and therefore detected incidentally. Symptomatic AAAs can manifest with lower back pain, a pulsatile abdominal mass, and a bruit on auscultation. Abdominal ultrasound is the best initial and confirmatory test to diagnose AAAs and determine their extent. Observation, close follow-up, and reduction of cardiovascular risk factors are indicated for small aneurysms, whereas pronounced (> 5.5 cm in men; > 5 cm in women) or rapidly expanding aneurysms require surgery. Surgical treatment involves open resection of the aneurysm with graft placement or, increasingly, endovascular stent placement. The prognosis is markedly worse if dissection or aneurysm rupture occurs. AAA rupture typically manifests with sudden onset of severe tearing back or abdominal pain, a painful pulsatile mass, and hypovolemic shock, and should be managed with emergent surgery. All men between 65 and 75 years of age with a history of smoking should be screened once with an ultrasound to exclude an AAA. See also thoracic aortic aneurysm for more information.
Definitions
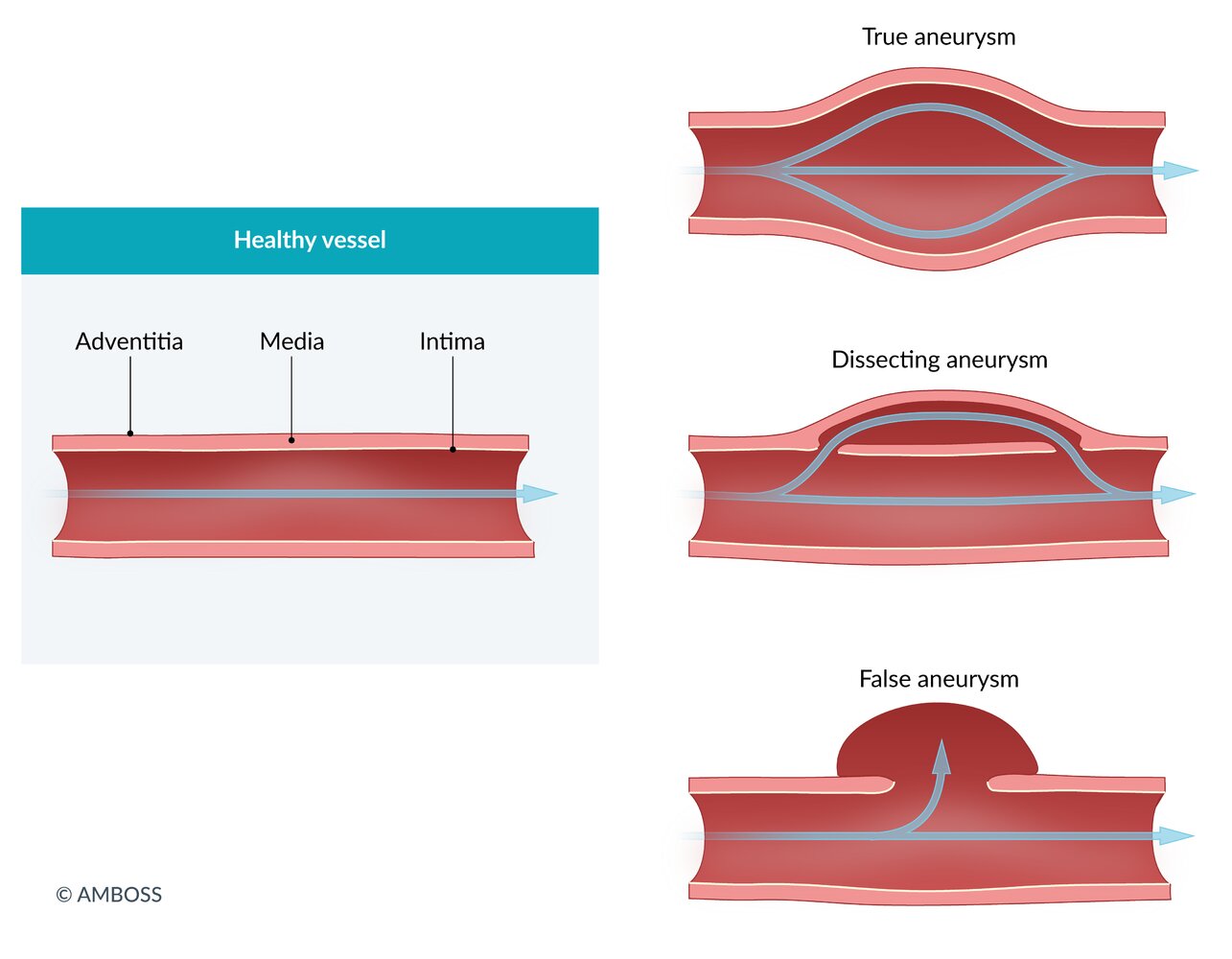
- Localized dilation of all three layers of the abdominal aortic wall (intima, media, and adventitia) to ≥ 3 cm [1]

© AMBOSS
Epidemiology
- Peak incidence: 60–70 years (rare in patients < 50 years)
- Sex: ♂ > ♀: ∼ 2:1
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Risk factors [2]
- Smoking (most important risk factor)
- Advanced age
- Atherosclerosis (ASCVD)
- Hypercholesterolemia and arterial hypertension
- Positive family history
- Male sex
- Trauma
Classification
-
Localization
-
Infrarenal: below the renal arteries
- Most common location [3]
- One-third of aneurysms extend into the iliac arteries. [1]
- Suprarenal: above the renal arteries
-
Infrarenal: below the renal arteries
-
Shape
- Saccular (spherical) [4]
- Fusiform (spindle-shaped)



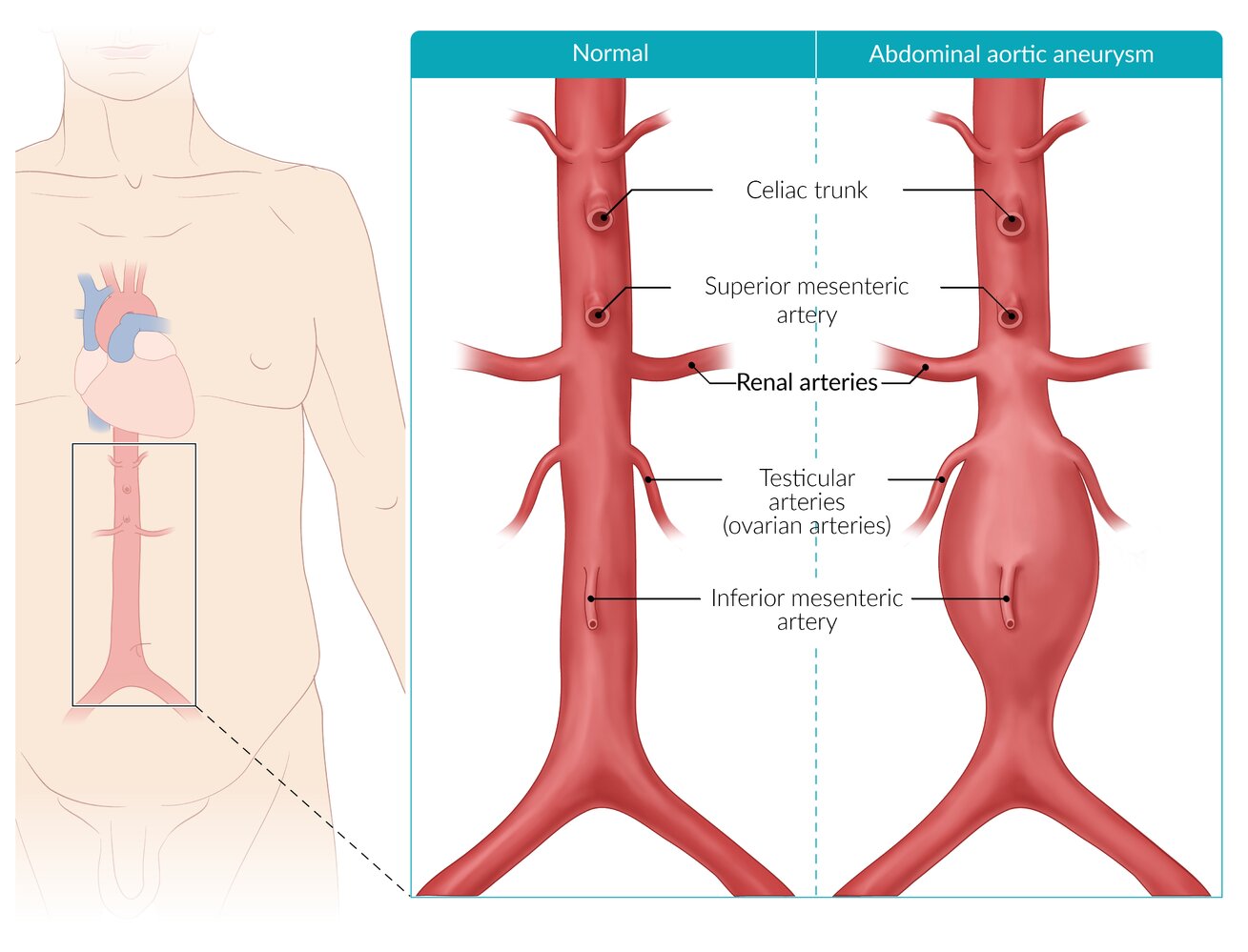
Abdominal aortic aneurysms are most commonly infrarenal (located below the renal arteries) with a fusiform (spindle) shape.
© AMBOSS
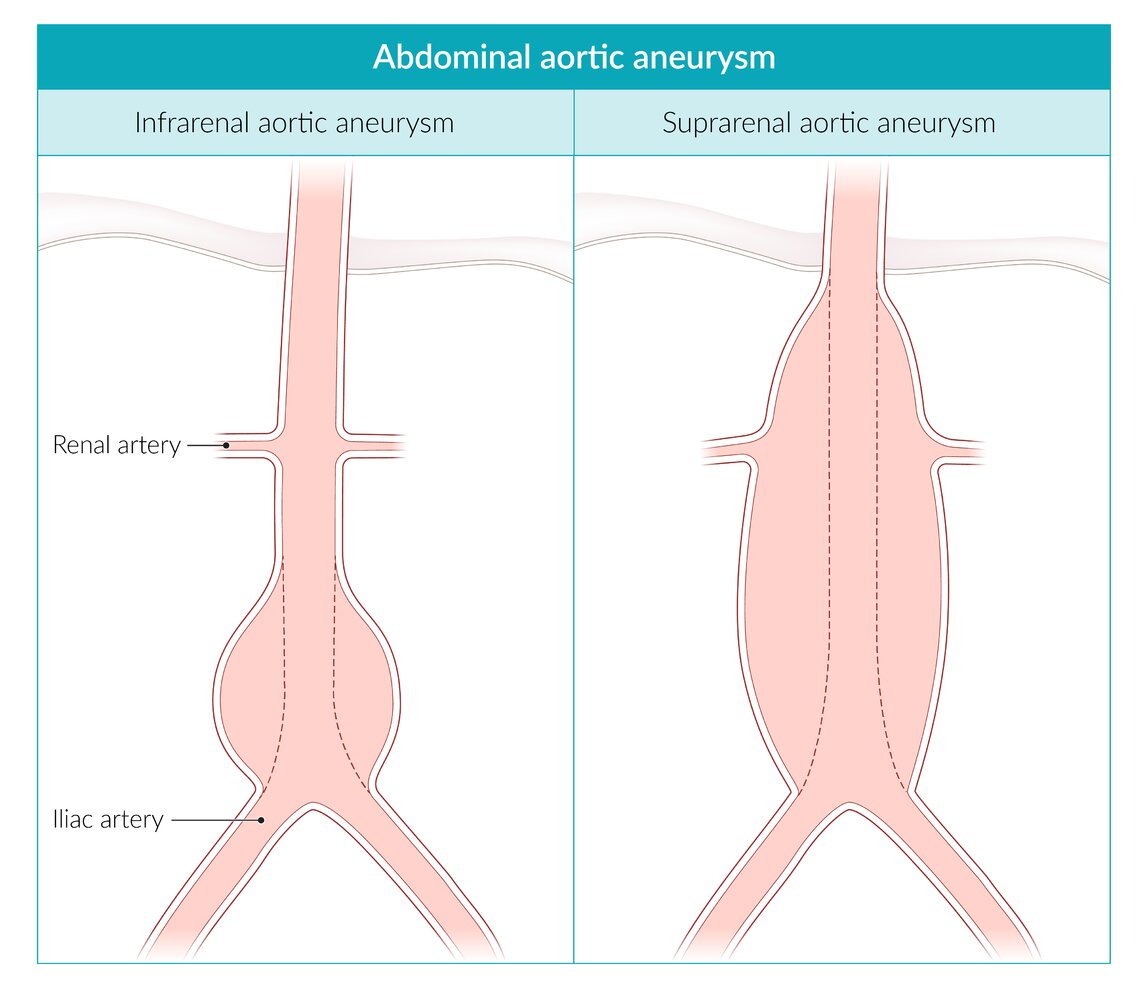
Infrarenal aortic aneurysm: located distal to the renal arteries, with a segment of normal, nondilated aorta between the aneurysm and the renal arteries
Suprarenal aortic aneurysm: extends proximal to the renal arteries (without extension into the chest)
© AMBOSS
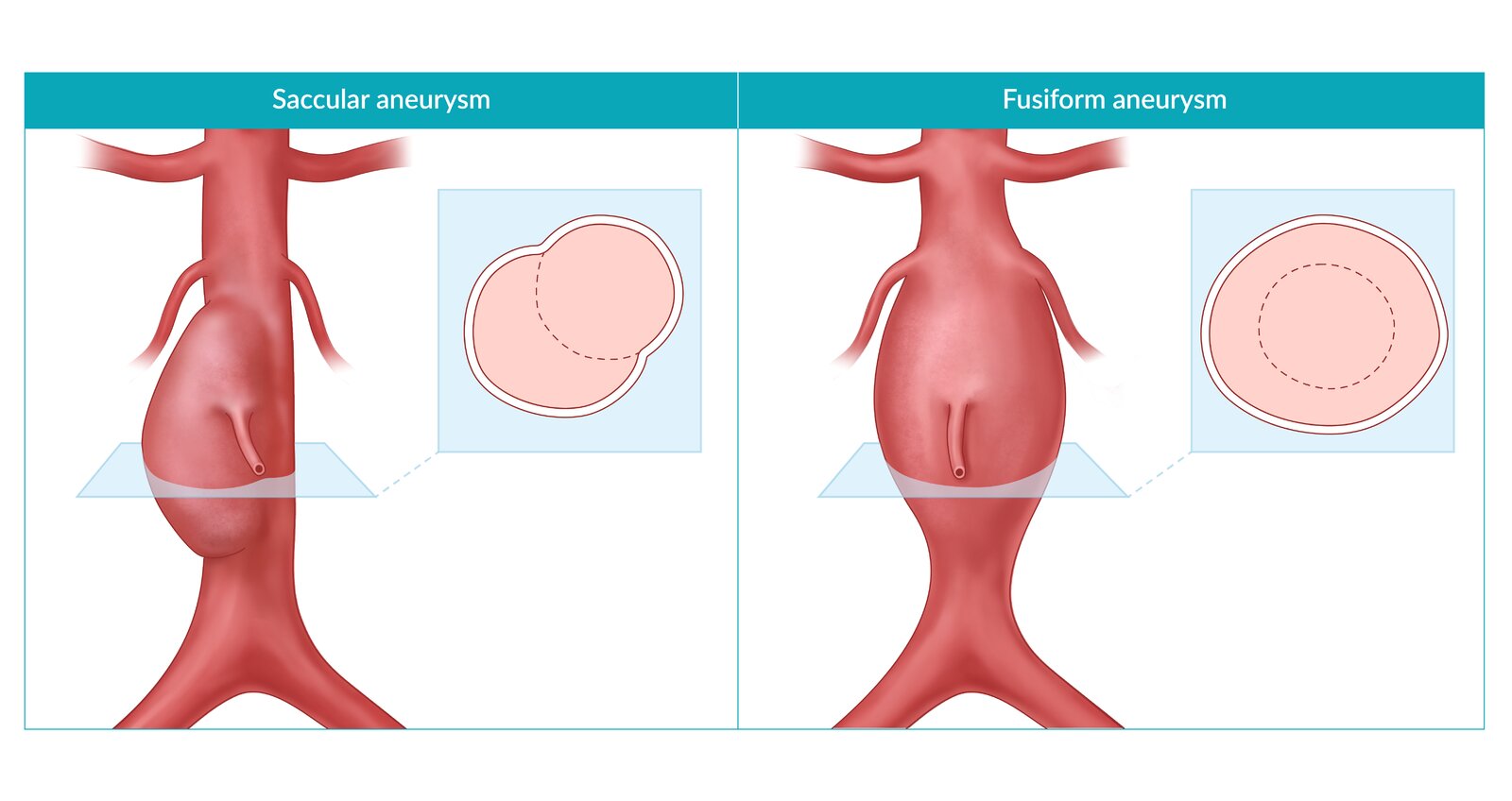
Saccular aneurysm: asymmetrical dilatation of the aortic wall (less common but with a higher risk of rupture compared to fusiform aneurysms)
Fusiform aneurysm: symmetrical dilatation of the aortic wall (most common shape)
© AMBOSS
Pathophysiology
- Inflammation and proteolytic degeneration of connective tissue proteins (e.g., collagen and elastin and/or smooth muscle cells) in high-risk patients → loss of structural integrity of the aortic wall → widening of the vessel → mechanical stress (e.g., high blood pressure) acts on weakened wall tissue → dilation and rupture may occur.
- The aneurysmatic dilatation of the vessel wall may cause disruption of the laminar blood flow and turbulence.
- Possible formation of thrombi in the aneurysm → peripheral thromboembolism

References:[5]
© AMBOSS
Our great thanks to Martin Lesiak for kindly providing this image.
Clinical features
Aortic aneurysms are usually asymptomatic or have nonspecific symptoms. They are often discovered incidentally on ultrasound or CT scan. Rupture or dissection of the aneurysm is a life-threatening condition (see “Ruptured AAA”).
- Lower back pain
- Pulsatile abdominal mass at or above the level of the umbilicus
- Bruit on auscultation
- Peripheral thrombosis and distal atheroembolic phenomena (e.g., blue toe syndrome and livedo reticularis)
- Decreased ankle brachial index


Dorsal view of the right foot showing blue/purple cyanotic discoloration of the toes
Source: “Ischemia” by Jmh649 (James Heilman, M.D.), Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Diagnosis
The diagnosis of AAA is confirmed by imaging showing aortic diameter > 3 cm. Unstable patients should be taken directly to the OR for emergency surgery if ruptured AAA is suspected (see ruptured AAA). There are no laboratory findings specific to AAA. [1]
Imaging should not delay treatment if AAA is suspected in hemodynamically unstable patients.
Imaging [6][7]
Abdominal ultrasound (formal ultrasound or POCUS)
-
Indications
-
Best initial and confirmatory test in:
- Asymptomatic patients
- Patients with abdominal pain and no known AAA or risk factors for AAA
- To determine the presence, size, and extent of an aneurysm
- Screening and surveillance
-
Best initial and confirmatory test in:
-
Formal ultrasound [8]
- Obtain longitudinal and transverse views for:
- Proximal, mid, and distal abdominal aorta
- Both proximal common iliac arteries
- Obtain AP dimension measurements of the greatest diameters of each vessel.
- See “POCUS for suspected AAA” for the point-of-care imaging technique and findings.
- Obtain longitudinal and transverse views for:
-
Supportive findings
- Dilatation of the aorta ≥ 3 cm [1]
- Thrombus may be present (hyperechoic)
- Disadvantages: Abdominal ultrasound has low sensitivity for aneurysmal leaks, branch artery involvement, and suprarenal involvement, and its findings are insufficient for procedural planning. [1][9]



If a large (≥ 5.5 cm in men, ≥ 5.0 cm in women) aneurysm is seen on ultrasound in a patient presenting with abdominal pain, refer the patient for treatment immediately.
CT angiography abdomen and pelvis for abdominal aortic aneurysm
See “Ruptured AAA” for CT findings of acute aneurysmal rupture.
-
Indications
- Imaging modality of choice in symptomatic patients and for preintervention planning
- To help confirm the diagnosis when ultrasound is not possible in asymptomatic patients
- More detailed evaluation of the location, size, and extent of the aneurysm, involvement of branch vessels, and presence of thrombus or rupture
-
Supportive findings
- Dilatation of the aorta ≥ 3 cm and, possibly, branch vessels [1]
- Reduced distribution of vasa vasorum may be seen. [10]
- Thrombus may also be present (hypodense, nonenhancing).


MR angiography abdomen and pelvis with and without IV contrast
-
Indications
- Preintervention planning when CT angiography is not possible
- To help confirm diagnosis when ultrasound and CT angiography are not possible in asymptomatic patients
- Supportive findings: similar to CT angiography
Arteriography (aortography abdomen)
-
Indications
- To help confirm diagnosis or for preintervention planning if the patient has significant contraindications to CTA and MRA
- More detailed assessment of the aortic lumen
- Supportive findings: contrast column in the lumen of the aneurysm and branch vessels [6]
- Disadvantage: may mask the actual diameter of the aneurysm (because a mural thrombus does not appear on arteriography)
An aortic aneurysm is sometimes incidentally detected on an abdominal or pelvis radiograph by the presence of a rounded soft tissue density and/or curvilinear calcification of the aneurysm wall.

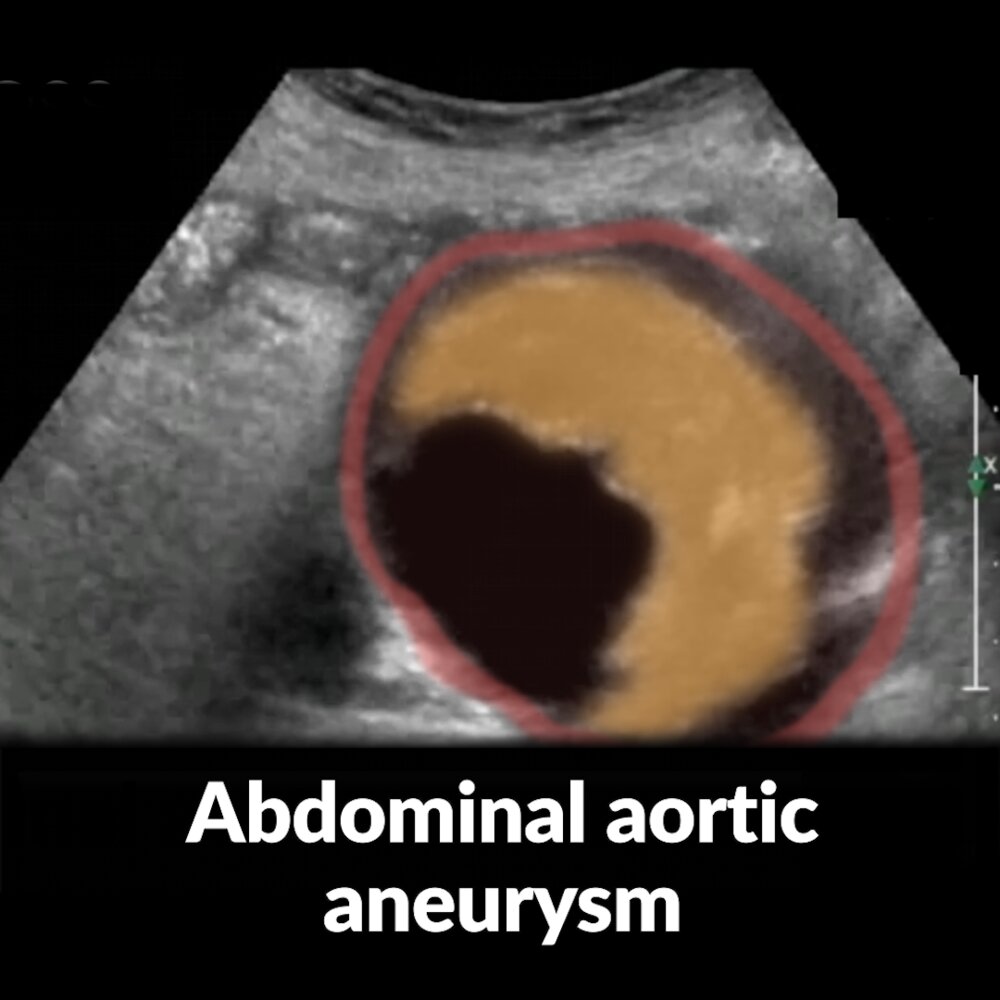
Short video of an ultrasound examination of the abdominal aorta in short axis view (a marker indicates the probe position) showing an aneurysm with a thrombus that narrows the lumen.
The abdominal aorta is seen in cross-section in the center of the image. The anechoic area in the lumen of the aorta corresponds to the expected appearance of flowing blood; the semilunar structure on the right side of the lumen is a thrombus (yellow overlay).
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
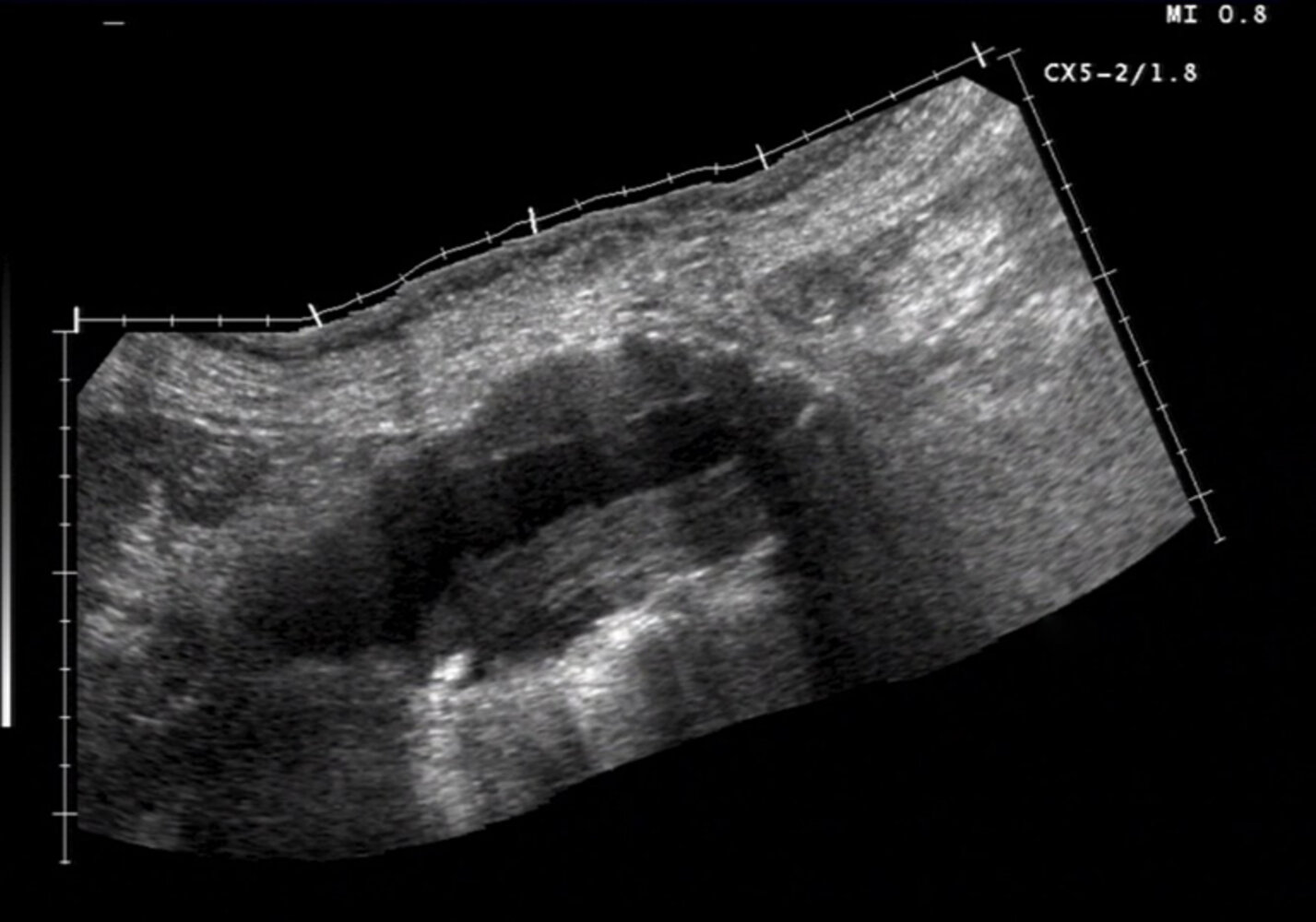
Ultrasound abdominal aorta (longitudinal plane)
A large amount of mural thrombus (yellow overlay) is visible within a fusiform aneurysm of the distal abdominal aorta (outer wall indicated by green lines). Atherosclerotic plaques (examples indicated by red overlay) are also visible.
L: lumen
Image source of original image: sonographiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg. Original title: “BAA_laengs__1__01”. Created by: Dr. J. Guntau. Modifications to original image: text removed.
© AMBOSS
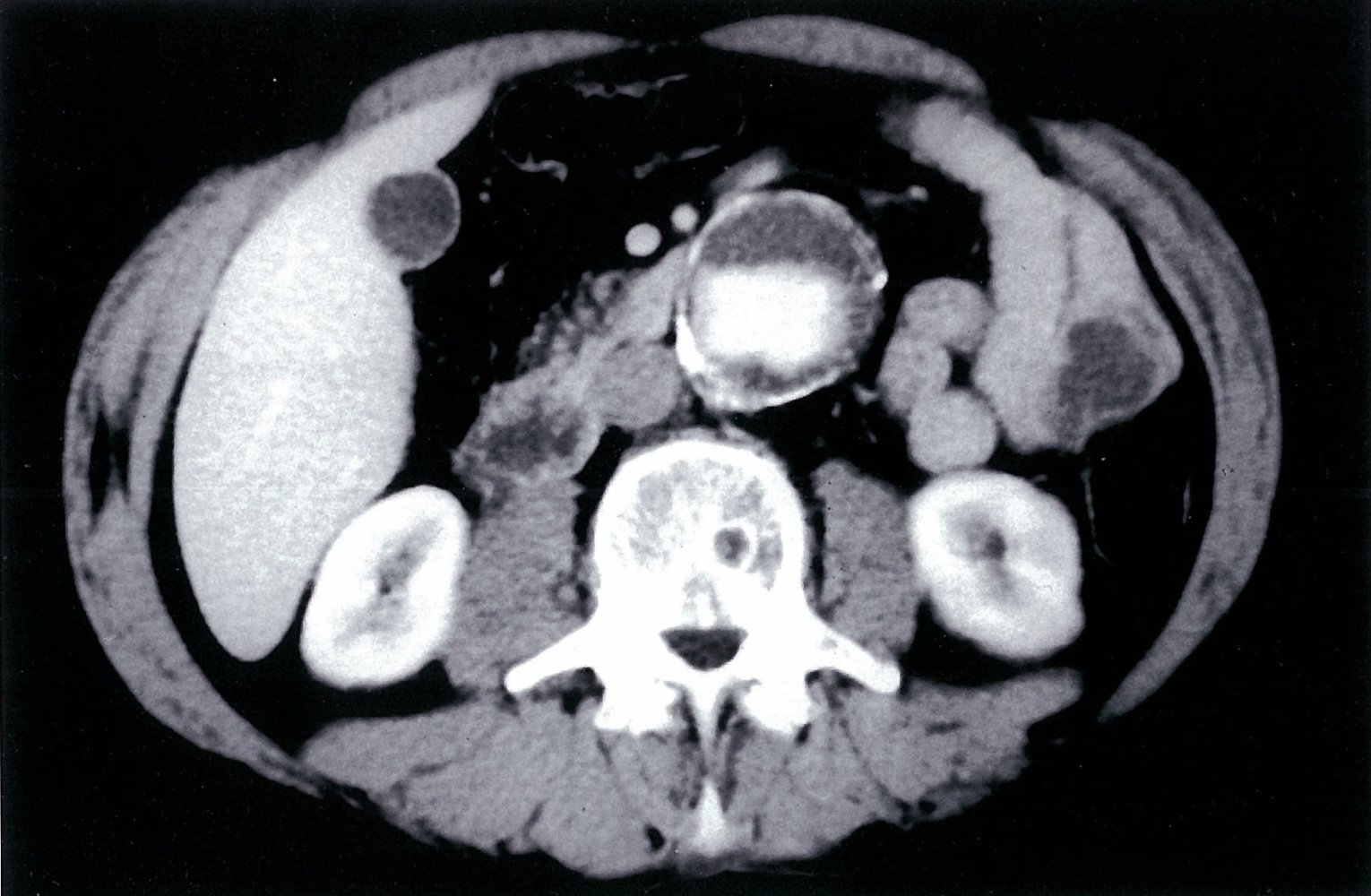
CT abdomen (with contrast; axial plane)
The atherosclerotic abdominal aorta is aneurysmal, with a central contrast-enhanced lumen (green overlay) and peripheral hypodense thrombus (red overlay).
1: liver; 2: gallbladder; 3: duodenum; 4: kidneys; 5: inferior vena cava
Source: © IMPP
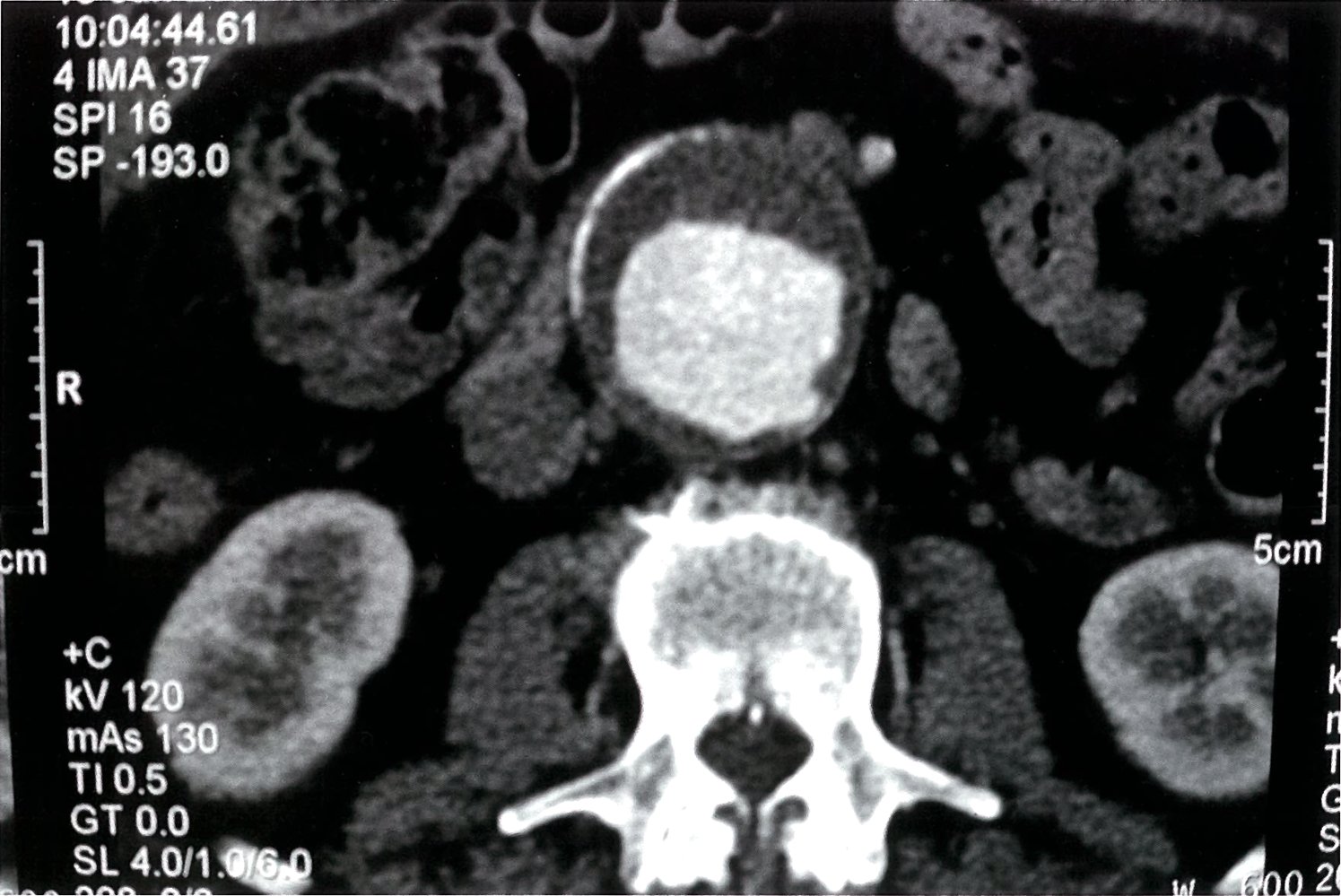
Contrast-enhanced CT scan of the abdomen (transverse section at L3; arterial phase)
Infrarenal abdominal aortic aneurysm (5 x 5.5 cm) with peripheral, hypodense thrombotic material (red overlay) and central, hyperdense contrast-enhanced blood (green overlay). A light calcification of the aortic wall is visible (red outline).
Source: © IMPP

X-ray pelvis and lower abdomen (AP view)
A thin curvilinear calcification is visible to the right and left of the L3 and L4 vertebrae (dashed lines). The convex contour of each calcification is directed laterally and located in the expected region of the abdominal aorta. Degenerative changes are visible in the lumbar spine and pelvis, and a left hip prosthesis is present (P).
An aortic aneurysm is sometimes incidentally detected on an abdominal or pelvis radiograph by the presence of a rounded soft tissue density and/or curvilinear calcification of the aneurysm wall. The American College of Radiology considers detection of abdominal aortic aneurysm an actionable finding that requires special communication with the clinician.
Arrowhead: venous phlebolith; White arrows: examples of arterial calcifications; Black arrow: example of degenerative osteophyte
Source: “RupturedAAAXray” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: Elements have been deleted.. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
| Abdominal vs. thoracic aortic aneurysm | ||
|---|---|---|
| Characteristics | Abdominal aortic aneurysm | Thoracic aortic aneurysm |
| Location |
|
|
| Epidemiology |
|
|
| Etiology |
|
|
| Clinical features |
|
|
| Diagnostics |
|
|
| Therapy |
|
|
See differential diagnoses of acute abdomen in acute abdomen.
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [1][12]
-
Patients with any symptoms: immediate vascular surgery consult
- Suspected or known rupture (regardless of patient stability) : emergency repair within 90 minutes (see “Ruptured AAA”)
-
Patients with signs or symptoms of impending rupture : urgent aneurysm repair, ideally within normal working hours, as this is associated with better outcomes
- Ensure blood product availability.
- Maintain BP strictly within normal parameters.
- Consult anesthesia.
- Optimize the treatment of and stabilize any comorbidities that could increase perioperative risk (e.g., ADHF, AKI).
- Asymptomatic patients: elective aneurysm repair or aneurysm surveillance
-
All patients: reduction of cardiovascular risk [1]
- Smoking cessation
- Appropriate medical management of other atherosclerotic risk factors (e.g., hypertension, diabetes mellitus, dyslipidemia)
Consult vascular surgery and the ICU about any patients with a symptomatic AAA.
Invasive treatment: AAA repair
- Indications
- Emergency repair: unstable patients
- Urgent repair: impending rupture or leaking AAA
-
Elective repair [13]
- Diameter: ≥ 5.5 cm in men; ≥ 5.0 cm in women
- Expansion rate: ≥ 0.5 cm/6 months
- Symptomatic aneurysm
- Saccular aneurysm
Procedures [1]
The long-term survival and complication rates of endovascular and open surgical repair are similar, and these procedures each have their advantages and disadvantages.
-
Endovascular aneurysm repair (EVAR)
- Indications: minimally invasive procedure that is preferred over open surgical repair for most aneurysms, especially in patients with a high operative risk
- Procedure: Under fluoroscopic guidance, an expandable stent graft is placed via the femoral or iliac arteries intraluminally at the site of the aneurysm.
- Disadvantage: Reintervention rates are higher for EVAR than for OSR.
-
Open surgical repair (OSR)
- Indications
- Mycotic aneurysm or infected graft
- Persistent endoleak and aneurysm sac growth following EVAR
- Anatomical contraindications for EVAR
- Procedure: A laparotomy is performed and the dilated segment of the aorta is replaced with a tube graft or Y-prosthesis (bifurcated synthetic stent graft).
- Indications
 of abdominal aortic aneurysm (AAA)")
 of abdominal aortic aneurysm (AAA)")
Preoperative assessment for elective repair [1]
- Calculation of mortality risk: used to weigh operative risk against life expectancy for patients being considered for elective AAA repair
| Elective AAA repair postoperative mortality risk score [14] | ||
|---|---|---|
| Parameter | Points | |
| Planned intervention | EVAR | 0 |
| OSR (infrarenal) | 2 | |
| OSR (suprarenal) | 4 | |
| Aneurysm size (mm) | < 65 | 0 |
| ≥ 65 | 2 | |
| Age | ≤ 75 years | 0 |
| > 75 years | 1 | |
| Sex | Male | 0 |
| Female | 1 | |
| Comorbidities | History of MI or cerebrovascular disease | 1 |
| COPD | 2 | |
| Serum creatinine (mg/dL) | < 1.5 | 0 |
| ≥ 1.5 | 2 | |
Interpretation
| ||

-
Preoperative management of comorbid conditions
- Cardiac consult in patients with cardiac diseases
- Optimize heart failure therapy.
- Consider coronary revascularization.
- 12-lead ECG in all patients
- Echocardiography in patients with worsening dyspnea or dyspnea of unknown origin
- Pulmonary function studies, including ABG, in patients with COPD, tobacco use, exertional dyspnea
- Cardiac consult in patients with cardiac diseases
- Additional considerations: Life expectancy should also be considered when planning elective repair. [15]
Perioperative care for AAA repair
- IV antibiotic prophylaxis [1]
- First-generation cephalosporin, e.g., cefazolin
- If the patient is allergic to penicillin: vancomycin
- Anticipate and treat acute blood loss anemia
- Ensure blood product availability.
- Indications for blood transfusion [1]
- Hemoglobin is ≤ 7 g/dL
- Hemoglobin is < 10 g/dL and there is ongoing blood loss
- Central venous access and arterial line monitoring during the procedure
- Consider postoperative admission to ICU:
- In patients with significant cardiac, pulmonary, or renal comorbidities
- In patients requiring mechanical ventilation
- After significant arrhythmia or hemodynamic instability during procedure
- Multimodal pain management
- E.g., morphine
- Consider epidural analgesia after OSR
- See also acute pain management.
- VTE prophylaxis
Surveillance after repair [1][7]
Postoperative surveillance following EVAR is important because it can help to detect possible endoleaks, sac growth, device migration, and device failure. Because of the risk of an anastomotic aneurysm or aneurysmal dilation in the visceral aorta or iliac arteries, regular follow-up is recommended after OSR.
-
CT angiography abdomen and pelvis with IV contrast
- After 1 month, 12 months, then annually
- After 6 months if an abnormality is seen on the 1-month scan
-
MR angiography abdomen and pelvis without and with IV contrast
- Indication: contraindications to CT angiography, avoidance of radiation
- Artifacts might be visible depending on stent material and orientation.
-
Duplex ultrasound
- Indication: may be used for annual follow-up if the 12-month scan is unremarkable
- Abdominal and pelvic CT angiography with IV contrast should still be performed every 5 years.
Conservative treatment: AAA surveillance without repair
Small (< 5.5 cm in men, < 5.0 cm in women), asymptomatic AAA can typically be observed with interval surveillance ultrasound. [13]
- To identify the expansion rate and thus decrease the risk of rupture
- Frequency depends on the size of the aneurysm.
| Follow-up frequency for AAA surveillance [13] | ||
|---|---|---|
| Maximum diameter of the abdominal aorta | Recommended follow-up interval | |
| In men | In women | |
| 3–3.9 cm |
|
|
| 4–4.9 cm | 4–4.4 cm |
|
| ≥ 5.0 cm | ≥ 4.5 cm |
|
Regular monitoring is essential because aneurysm size and expansion rate are strong predictors of the risk of rupture.
")
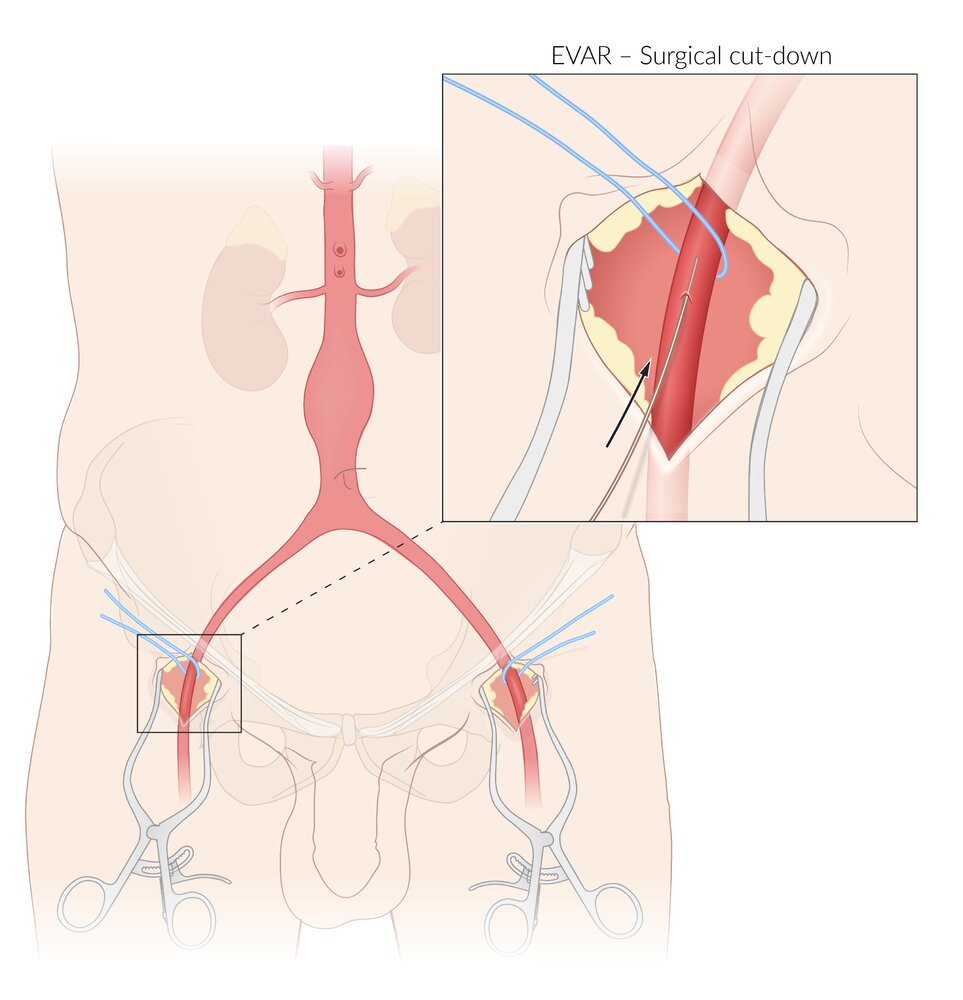
Main image: EVAR requires bilateral iliofemoral arterial access, which can be achieved either via femoral artery cutdown (shown here) or percutaneously.
Inset: enlarged view of femoral artery cutdown showing insertion of guidewire
© AMBOSS
Many configurations of EVAR stent grafts exist, but, in principle, they are composed of a supportive metal frame (stent) and an impermeable graft material. The procedure is performed under fluoroscopic guidance.
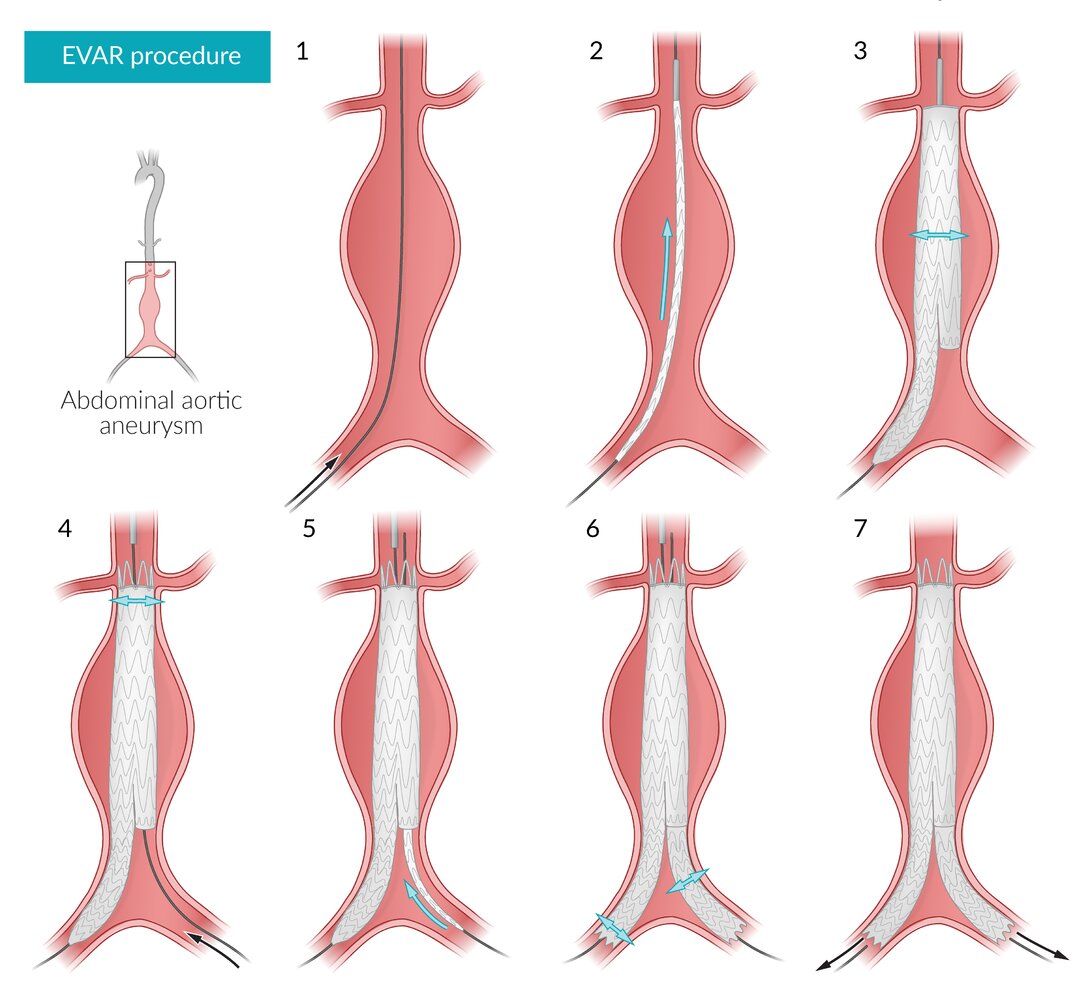
EVAR using example of a 2-component bifurcated stent graft and an infrarenal aneurysm:
1) The guidewire is inserted via the ipsilateral femoral artery into the abdominal aorta
2) Main body of the stent graft is advanced over the guidewire and positioned with the upper end of the graft material positioned immediately below the renal arteries.
3) The central part of the stent graft (with graft material) is deployed (expanded).
4) The Second guidewire is passed through the contralateral femoral artery and into the short limb of the main stent graft. The upper part of the stent (no graft material) is deployed, anchoring it to the wall of the aorta.
5) The iliac extension component of the stent graft is advanced over the contralateral guidewire until there is sufficient overlap between it and the main body.
6) The iliac extension is deployed and both iliac limbs are anchored distally.
7) The guidewires are removed.
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
AAA: abdominal aortic aneurysm
CTA: computed tomography angiography
MRA: magnetic resonance angiography
© AMBOSS
Abdominal aortic aneurysm rupture
Risk factors
- Rapidly expanding aneurysm
- Large diameter aneurysm
- Smoking, tobacco use
Clinical features
- Classic triad:
- Hypotension due to hypovolemic shock (especially in free ruptures)
- Sudden onset of severe, tearing back or abdominal pain with radiation to the flank, buttocks, legs, or groin
- Painful pulsatile mass
- Grey Turner sign and/or Cullen sign (if there is an extensive retroperitoneal hematoma)
- Nausea, vomiting
- Syncope
- Hematuria
Diagnostics [1][12][16]
The optimal diagnostic approach depends on patient stability, available resources, and clinical suspicion. Follow local protocols if available.
-
Unstable patients: : The diagnosis is clinical; refer directly for operative treatment. [1][12]
- Consider POCUS to rapidly confirm the presence of an AAA.
- Do not use POCUS to exclude a ruptured AAA if there is high clinical suspicion.
-
Stable patients (controversial) [1][12][16][17]
-
Consider imaging (in consultation with a vascular surgeon) provided it does not delay definitive management, for the following reasons:
- To evaluate for alternate etiologies if the diagnosis is uncertain [1]
- Anatomic assessment (e.g., with a thoracoabdominal CTA) to determine candidacy for EVAR and guide operative planning. [12]
- Closely monitor patients clinically during transfer outside of critical care areas for imaging.
-
Consider imaging (in consultation with a vascular surgeon) provided it does not delay definitive management, for the following reasons:
Imaging modalities
-
CTA thorax, abdomen, and pelvis
-
Study of choice if imaging can be performed without delaying operative repair [12][17]
- Higher detection rates for contained rupture and retroperitoneal bleeds than ultrasound
- Allows surgeons to determine if a patient is suitable for EVAR
- Characteristic findings
- Sign of impending rupture: high-attenuation crescent within mural thrombus [18]
- Signs of rupture: retroperitoneal hematoma, retroperitoneal stranding, indistinct aortic wall, extravasation of contrast
-
Study of choice if imaging can be performed without delaying operative repair [12][17]
-
POCUS: In an unstable patient, assume that a visible AAA on POCUS is a ruptured AAA until proven otherwise.
- Key finding: dilatation of the aorta ≥ 3 cm
- Other possible findings (depending on the location of the rupture)
- Periaortic fluid
- Free intraperitoneal fluid
- Retroperitoneal fluid
- For more detailed findings see “POCUS for suspected AAA.”
")



Additional studies
-
Laboratory findings that may be seen:
- CBC: ↓ hemoglobin, ↓ hematocrit, ↓ red blood cell count
- Metabolic acidosis in cases of shock
- ECG: may show ischemic changes secondary to acute blood loss [16]
A ruptured AAA can mimic an acute MI if blood loss impairs coronary perfusion, causing chest pain and ischemic ECG changes. Screen for an AAA in patients with cardiac chest pain and additional epigastric or back pain.
Treatment [1][12]
The main goal of treatment is operative repair by a vascular surgeon without delay.
-
Initial management (ideally within 30 minutes)
- Large-bore IV access
- Start continuous monitoring and reassess regularly as patients may deteriorate rapidly.
-
Immediate hemodynamic support
- Fluid resuscitation, or if available, blood transfusion, ideally using blood products in a 1:1:1 ratio (see “Massive transfusion”) [12][16]
- Use vasopressors and inotropes with caution. [16]
- Target: permissive hypotension (e.g., SBP 70–90 mm Hg) [1]
- Urgent vascular surgery and anesthesia consult [1]
- Pain management with IV opioids
- Definitive treatment (ideally within 90 minutes): emergency EVAR or OSR [1][12][13]
- Palliation: Consider in frail patients with multiple comorbidities. [12]
Avoid elective intubation, as it may precipitate cardiovascular collapse. [1]
Refer all patients with a suspected ruptured AAA for immediate operative evaluation.
Prognosis
- High mortality rate (∼ 81%) [2]
- Older age, loss of consciousness, and cardiac arrest prior to surgery are associated with high mortality.
Disposition [1]
- Consult vascular surgery as soon as a ruptured AAA is suspected.
- Transfer the patient to the nearest regional center with suitable facilities if a vascular surgeon is not available.
- Consider transfer to a regional center if the available in-hospital vascular surgery service manages a low number of ruptured AAAs annually and transfer can be achieved within 30 minutes. [12]
Interfacility transfer
-
Criteria
- Appropriate expertise and equipment are not available at the referring hospital.
- The patient is suitable for and willing to undergo surgical repair.
- The case has been discussed and accepted by the vascular surgery team at the receiving hospital.
- The patient is not currently in cardiac arrest.
-
Preparation prior to departure
- Establish IV access.
- Ensure BP is in the target range (i.e., SBP 70–90 mm Hg).
- Organize transfer of any imaging.
- Establish monitoring for continuous assessment of vital signs during transport.
- Conduct a telephone handover between physicians at the referring and receiving hospitals.
If patients require a transfer, it should be organized as swiftly as possible, with transfer times ideally under 30 minutes!
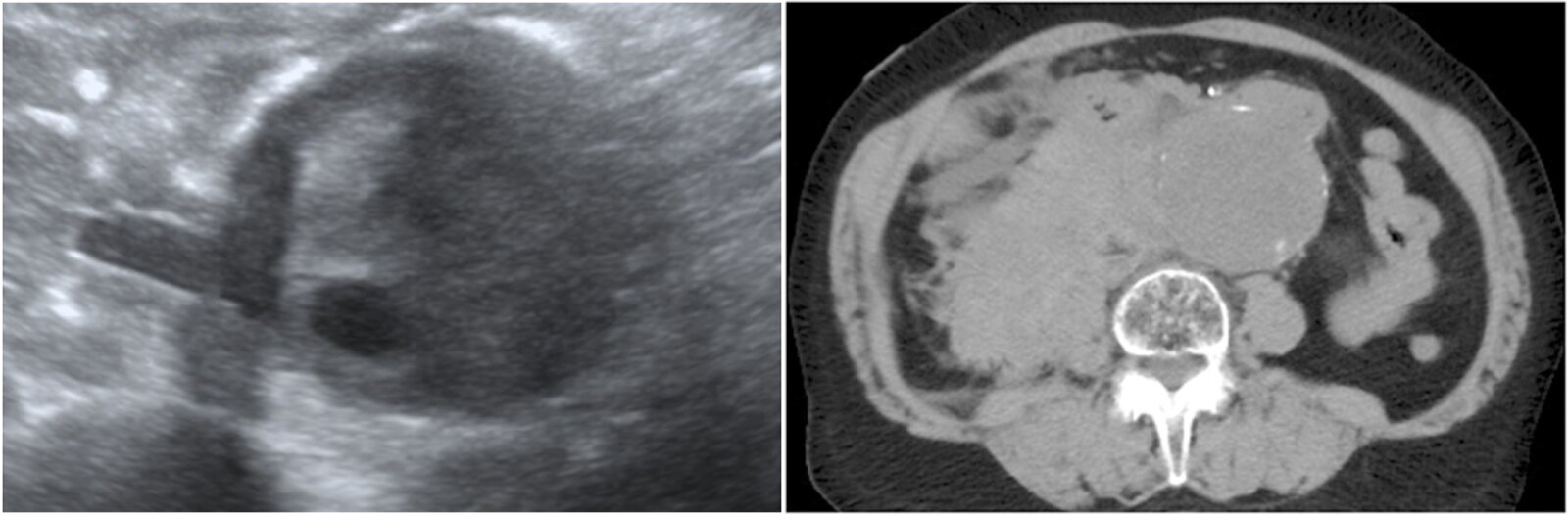
Left: ultrasound abdomen (transverse plane); right: CT abdomen (without contrast; axial plane) of a patient with a history of AAA and increasing mid abdominal pain over 24 hours
Luminal thrombus is heterogeneous on point-of-care ultrasound performed in the emergency room. An elongated hypoechoic area projecting from the right side of the aorta (red overlay) is suspicious for para-aortic hemorrhage from rupture of the aneurysm.
Intermittent calcification helps define the aortic wall on CT. The extent of a large right retroperitoneal hematoma (green overlay) is well demonstrated. The attenuation of the collection is compatible with subacute hemorrhage.
A: aneurysmal abdominal aorta
Source: “Fig 1 & 2, In: Ruptured abdominal aortic aneurysm identified on point-of-care ultrasound in the emergency department” by Diaz O, Eilbert W, BMC, licensed under CC BY 4.0. Modifications: merged Fig 1 and 2 into one & removed the asterisk and "MIP", removed the arrows. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
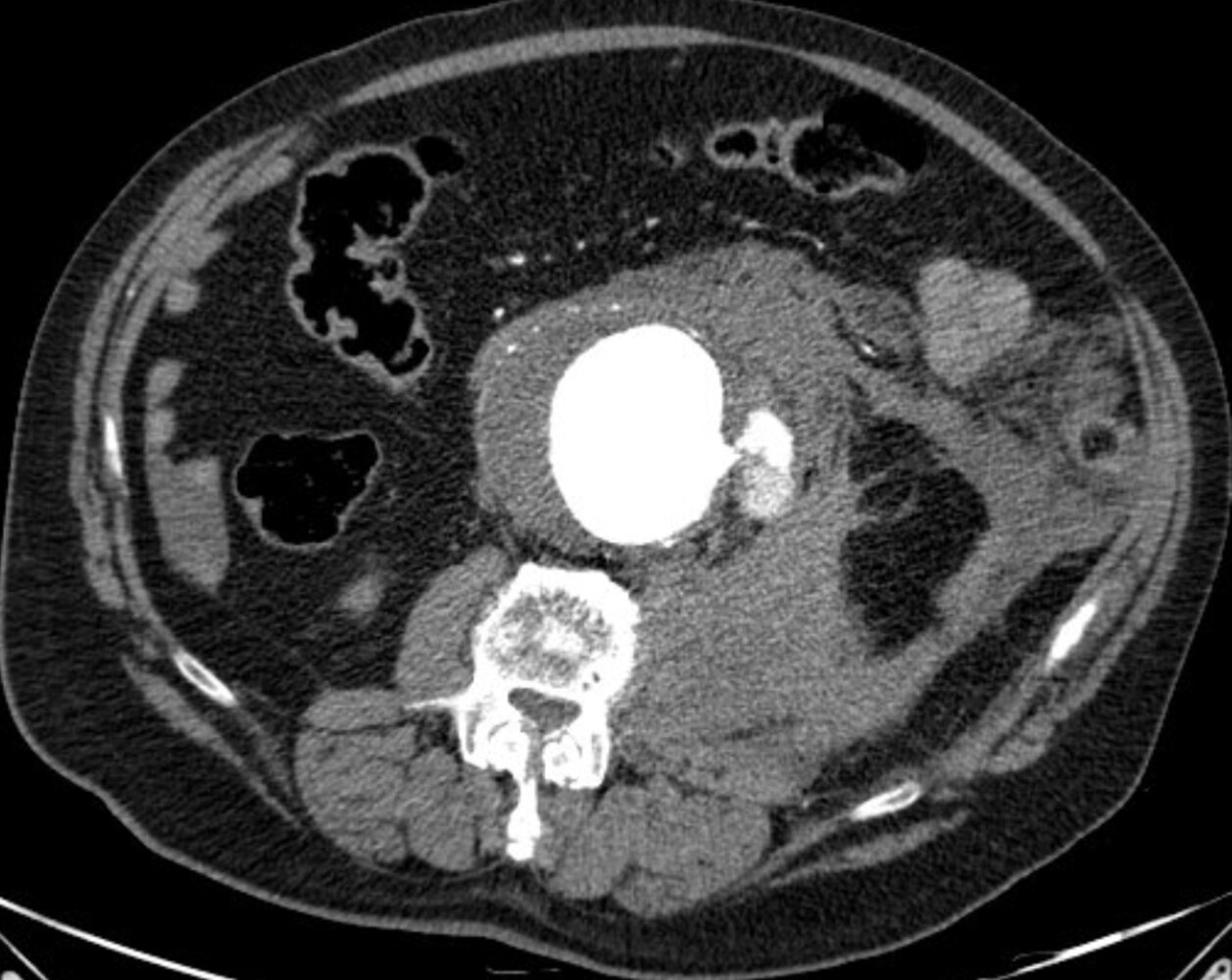
CT abdomen (with contrast; arterial phase; axial plane)
An infrarenal abdominal aortic aneurysm is measured as 8 cm in transverse diameter. Contrast extravasation (dashed outline) is seen on the left side at the site of rupture (arrowhead). A large left retroperitoneal hematoma (yellow overlay) extends inferiorly into the inguinal canal. Additional intraperitoneal fluid is seen in the pelvis and right upper quadrant (red overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
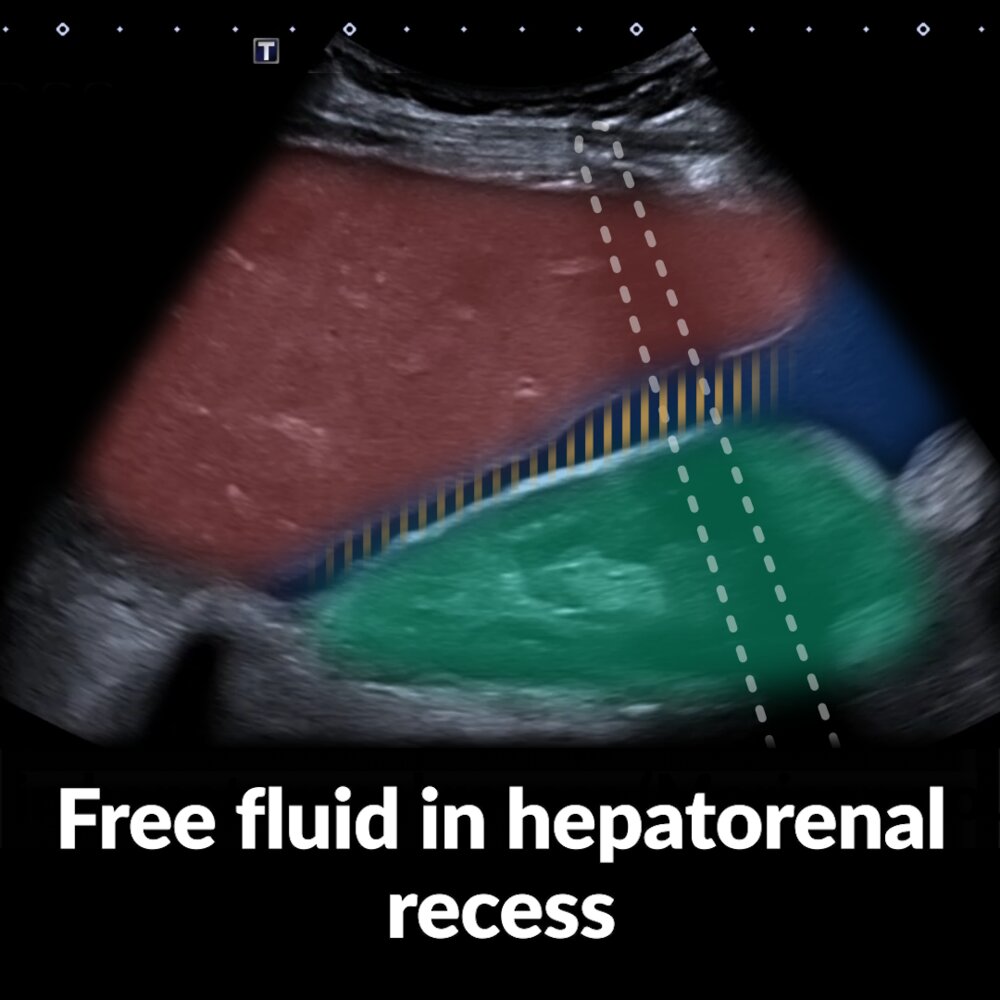
Short video of three right upper quadrant (RUQ; markers indicate the probe positions) ultrasound examinations showing free fluid in the hepatorenal recess (Morison pouch)
Case 1: The liver (red overlay) is visible near the top left of the image, the right kidney (green overlay) with its hyperechoic capsule is visible in the center and bottom right. A hypoechoic area (blue overlay) consistent with free fluid is visible within the hepatorenal recess (yellow hatching) and extending beyond the liver to the right of the image.
Case 2: The liver (red overlay) is visible near the top left of the image, the right kidney (green overlay) is visible near the bottom left. A hypoechoic area (blue overlay) consistent with free fluid is visible within the hepatorenal recess (yellow hatching) and extending beyond the liver to the right of the image.
Case 3: The liver (red overlay) is visible near the top left of the image, the right kidney (green overlay) with its hyperechoic capsule is visible near the bottom center. A hypoechoic area (blue overlay) consistent with free fluid is visible within the hepatorenal recess (yellow hatching) and extending beyond the liver to the right of the image.
Ultrasound can detect even small amounts of fluid in the hepatorenal recess.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Short video of three left upper quadrant (LUQ; markers indicate the probe positions) ultrasound examinations showing free fluid in the splenorenal recess
Case 1: The spleen (red overlay) is visible as a relatively homogeneous structure at the top left of the image, the left kidney (green overlay) with its hyperechoic capsule and more heterogeneous appearance is visible in the center and bottom right. At the beginning of the video, there is no evidence of free fluid in the splenorenal recess (yellow shading). Fanning the ultrasound beam ventrally (by tilting the transducer dorsally) reveals a homogeneous, hypoechoic area consistent with free fluid (blue overlay) medial to the spleen. At the end of case 1, we again see the classic view of the splenorenal recess, which does not show the pathology.
Case 2: The spleen (red overlay) is visible at the top left, the left kidney (green overlay) at bottom right. In the initial view there is again no evidence of free fluid in the splenorenal recess (yellow hatching). As in case 1, fanning the ultrasound beam ventrally reveals a homogeneous, hypoechoic area consistent with free fluid (blue overlay).
Case 3: The spleen (red overlay) is visible at the top of the image, the left kidney (green overlay) at the bottom. A hypoechoic area (blue overlay) consistent with free fluid extends from the splenorenal recess (yellow hatching) towards the top right of the image (anatomically inferior to the spleen).
Ultrasound can detect even small amounts of fluid in the splenorenal recess.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Complications
- Abdominal aortic aneurysm rupture
- Embolism: caused by thrombotic material from the aneurysm
- Aortic dissection
-
Postoperative complications [19]
- Ischemia of the bowel, kidneys, and spinal cord
- Anterior spinal artery occlusion
- Prosthetic graft infection
-
Aortoenteric fistula [20]
- Manifests with massive gastrointestinal hemorrhage
- Unstable patients: Urgently consult surgeons for immediate intervention.
- Stable patients: Assess with CT or endoscopy to rule out differential diagnoses and assist with surgical planning.
-
Complications following EVAR [1]
- Endoleak
- Access site complications, e.g., bleeding, hematoma, false aneurysm
- Graft limb thrombosis
We list the most important complications. The selection is not exhaustive.
Left: ultrasound abdomen (transverse plane); right: CT abdomen (without contrast; axial plane) of a patient with a history of AAA and increasing mid abdominal pain over 24 hours
Luminal thrombus is heterogeneous on point-of-care ultrasound performed in the emergency room. An elongated hypoechoic area projecting from the right side of the aorta (red overlay) is suspicious for para-aortic hemorrhage from rupture of the aneurysm.
Intermittent calcification helps define the aortic wall on CT. The extent of a large right retroperitoneal hematoma (green overlay) is well demonstrated. The attenuation of the collection is compatible with subacute hemorrhage.
A: aneurysmal abdominal aorta
Source: “Fig 1 & 2, In: Ruptured abdominal aortic aneurysm identified on point-of-care ultrasound in the emergency department” by Diaz O, Eilbert W, BMC, licensed under CC BY 4.0. Modifications: merged Fig 1 and 2 into one & removed the asterisk and "MIP", removed the arrows. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT abdomen (with contrast; arterial phase; axial plane)
An infrarenal abdominal aortic aneurysm is measured as 8 cm in transverse diameter. Contrast extravasation (dashed outline) is seen on the left side at the site of rupture (arrowhead). A large left retroperitoneal hematoma (yellow overlay) extends inferiorly into the inguinal canal. Additional intraperitoneal fluid is seen in the pelvis and right upper quadrant (red overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
Acute management checklist for abdominal aortic aneurysm
Ruptured abdominal aortic aneurysm
- Immediate vascular surgery consult for emergency surgical repair if ruptured aneurysm is suspected
- Unstable patients: Transfer to the OR immediately.
- Stable patients: Consider CTA if it can be performed rapidly and close monitoring is possible.
- NPO
- IV access with two large-bore peripheral IV lines
- Check CBC, type and screen, obtain patient consent for blood transfusion, and order pRBCs (prepare for massive transfusion protocol).
- IV fluid resuscitation with goal SBP of 70–90 mm Hg (permissive hypotension) [1][21]
- IV opioid analgesics
Symptomatic abdominal aortic aneurysm
- Urgent vascular surgery consult for surgical repair
- CT angiography abdomen and pelvis with IV contrast for preintervention planning if patient is hemodynamically stable
- Transfer to OR.
- NPO
- IV access with two large-bore peripheral IV lines
- Check CBC, type and screen, obtain patient consent for blood transfusion, and order pRBCs (prepare for massive transfusion protocol).
- Consider IV fluid resuscitation.
- IV opioid analgesics
Prevention
Primary prevention [1]
- See “Primary prevention of ASCVD” for detailed information on primary prevention.
- The following lifestyle measures are thought to reduce the risk of developing an AAA:
- Smoking cessation
- Eating nuts, fruits, and vegetables more than three times a week
- Exercising more than once a week
Screening for AAA [1][2][13]
-
Indications
- Men aged 65–75 years with a history of smoking (ever smokers) [1][2][13]
-
Consider screening:
- Individuals aged 65–75 years with a family history of AAA in a first-degree relative [1][2][13]
- Women aged 65–75 years with a history of smoking (ever smokers) [1][2][13]
- Individuals aged > 75 years with no previous screening and a history of smoking or family history of AAA [1][22]
- Individuals < 65 years with multiple risk factors for AAA or a family history of AAA [13]
- Modality: abdominal ultrasound [1][2][6]
-
Frequency
- One-time screening is recommended. [2]
- Consider rescreening after 10 years if the aortic diameter was between 2.5 cm and 3 cm at the initial assessment. [1]
AAA screening is not recommended for women who have never smoked and have no family history of AAA. [2]
Men aged 65-75 with a history of smoking should be screened with a one-time abdominal ultrasound.
External Resources
- 2019 USPSTF Recommendation Statement on Screening for Abdominal Aortic Aneurysm
- 2018 SVS Practice Guidelines on the Care of Patients with an Abdominal Aortic Aneurysm
- 2018 ACR Appropriateness Criteria Abdominal Aortic Aneurysm: Interventional Planning and Follow-Up
- 2017 ACR Appropriateness Criteria Pulsatile Abdominal Mass Suspected Abdominal Aortic Aneurysm
- 2015 AIUM Practice Guideline for Diagnostic and Screening Ultrasound Examinations of the Abdominal Aorta
References
- Graciaa DS, Mosunjac MB, Workowski KA, Kempker RR. "Asymptomatic Cardiovascular Syphilis With Aortic Regurgitation Requiring Surgical Repair in an HIV-Infected Patient". Open Forum Infect Dis. 4(4). (2017)
- Chaikof EL, Dalman RL, Eskandari MK, et al. "The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm". Journal of Vascular Surgery. 67(1). :2-77.e2. (2018)
- Reis SP et al. "ACR Appropriateness Criteria ® Pulsatile Abdominal Mass Suspected Abdominal Aortic Aneurysm". J Am Coll Radiol. 14(5). :S258-S265. (2017)
- Francois CJ et al. "ACR Appropriateness Criteria ® Abdominal Aortic Aneurysm: Interventional Planning and Follow-Up". J Am Coll Radiol. 15(5). :S2-S12. (2018)
- AIUM. "AIUM Practice Guideline for the Performance of Diagnostic and Screening Ultrasound Examinations of the Abdominal Aorta in Adults". J Ultrasound Med. 34(8). :1-6. (2015)
- Dent B, Kendall RJ, Boyle AA, Atkinson PR. "Emergency ultrasound of the abdominal aorta by UK emergency physicians: a prospective cohort study". Emerg Med J. 24(8). :547-549. (2007)
- Tanaka H, Zaima N, Sasaki T, et al. "Adventitial Vasa Vasorum Arteriosclerosis in Abdominal Aortic Aneurysm". PLoS ONE. 8(2). :e57398. (2013)
- Wanhainen A, Verzini F, Van Herzeele I, et al. "Editor's Choice - European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms.". Eur J Vasc Endovasc Surg. 57(1). :8-93. (2019)
- Isselbacher EM, Preventza O, Hamilton Black J, et al. "2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines". Circulation. 146(24). (2022)
- Eslami MH et al. "Comparison of a Vascular Study Group of New England risk prediction model with established risk prediction models of in-hospital mortality after elective abdominal aortic aneurysm repair". J Vasc Surg. 62(5). :1125-1133.e2. (2015)
- Paraskevas KI, Eckstein H-H, Schermerhorn ML. "Guideline Recommendations for the Management of Abdominal Aortic Aneurysms". Angiology. 70(8). :688-689. (2019)
- Maleux G, Koolen M, Heye S. "Complications after endovascular aneurysm repair". Semin Intervent Radiol. 26(1). :3-9. (2009)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Owens DK et al. "Screening for Abdominal Aortic Aneurysm". JAMA. 322(22). :2211. (2019)
- O'Donnell TFX, Wade JE, Liang P, et al. "Endovascular aneurysm repair in patients over 75 is associated with excellent 5-year survival, which suggests benefit from expanded screening into this cohort.". Journal of vascular surgery. 69(3). :728-737. (2019)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Thompson MM. "Infrarenal abdominal aortic aneurysms". Curr Treat Options Cardiovasc Med. 5(2). :137-146. (2003)
- Wang LJ, Prabhakar AM, Kwolek CJ. "Current status of the treatment of infrarenal abdominal aortic aneurysms". Cardiovasc Diagn Ther. 8(S1). :S191-S199. (2018)
- Moreno DH, Cacione DG, Baptista-Silva JC. "Controlled hypotension versus normotensive resuscitation strategy for people with ruptured abdominal aortic aneurysm". Cochrane Database of Systematic Reviews. (2018)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Rakita D, Newatia A, Hines JJ, Siegel DN, Friedman B. "Spectrum of CT Findings in Rupture and Impending Rupture of Abdominal Aortic Aneurysms". RadioGraphics. 27(2). :497-507. (2007)
- Schwartz SA et al. "CT Findings of Rupture, Impending Rupture, and Contained Rupture of Abdominal Aortic Aneurysms". AJR Am J Roentgenol. 188(1). :W57-W62. (2007)
- Karow T, Lang-Roth R. "Allgemeine und Spezielle Pharmakologie und Toxikologie". Dr. med. Thomas Karow (2012 und 2013). (2010). ISBN: B002UDYQB4
- Kliegman RM, Stanton BF, Geme JS, Schor NF, Behrman RE. "Nelson Textbook of pediatrics". Elsevier (2011). (2011). ISBN: 9781437707557
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Lippincott Williams & Wilkins. (2013). ISBN: 9781609133603
- Upchurch GR. "Abdominal Aortic Aneurysm". Am Fam Physician. 73(7). :1198-1204. (2006)
- Brewster DC, Cronenwett JL, Hallett JW Jr, et al. "Guidelines for the treatment of abdominal aortic aneurysms". J Vasc Surg. 37(5). :1106-1117. (2003)