Summary
Abdominal hernias are a protrusion of intraabdominal contents through a congenital or acquired defect in the abdominal wall. Abdominal hernias are broadly classified by location (anterior wall, lateral wall, groin, or pelvis) and presentation (reducible, irreducible, obstructed, or strangulated). Physiological states that increase intraabdominal pressure (e.g., ascites, pregnancy, obesity, intraabdominal tumors, chronic cough) increase the risk of developing an abdominal hernia. Clinical presentation ranges from an asymptomatic mass in reducible hernias, to pain, bowel obstruction, and systemic symptoms in strangulated hernias. Abdominal hernias are typically a clinical diagnosis made on physical examination. Imaging (e.g., ultrasound, CT scan) may be used if the examination is difficult or atypical, and before surgery. Treatment is primarily surgical repair with or without a mesh, though observation may be adequate in some patients. Emergency surgery is always required for an obstructed or strangulated (i.e., ischemic) hernia. Congenital umbilical hernias typically close spontaneously by 5 years of age and have a wide neck, and the risk of complications is low; surgical intervention is rarely necessary.
See “Inguinal hernias” and ”Femoral hernias” for more detail on these hernia types.
Classification
By anatomical location [1][2]
-
Anterior abdominal wall hernias
- Umbilical hernia: midline ventral hernia at the level of the umbilicus [3][4]
- Epigastric hernia: protrusion of intraabdominal contents through the linea alba, between the xiphoid process and the umbilicus
- Incisional hernia: protrusion of intraabdominal contents through an abdominal wall defect due to previous surgery
- Parastomal hernia: a subset of incisional hernias in which intraabdominal contents protrude through the abdominal wall defect created during stoma placement (e.g., colostomy)
-
Lateral abdominal wall hernias
-
Lumbar hernia
- Superior lumbar hernia: herniation through the superior lumbar triangle
- Inferior lumbar hernia: herniation through the inferior lumbar triangle
- Lumbar incisional hernia: herniation following surgery involving the posterolateral abdominal wall (e.g., nephrectomy, aortic aneurysm repair) [5]
- Spigelian hernia: herniation along the semilunar line; commonly adjacent to the arcuate line (i.e., below the umbilicus) [6][7]
-
Lumbar hernia
-
Groin hernias
- Inguinal hernia (direct or indirect)
- Femoral hernia
-
Pelvic hernias [8][9]
- Obturator hernia: herniation through the obturator foramen
- Perineal hernia: herniation through the pelvic floor [9]
- Sciatic hernia: herniation through the greater sciatic foramen or lesser sciatic foramen














By degree of complication [1][10]
- Reducible hernia: Hernia contents can be completely returned to the peritoneal cavity.
- Irreducible hernia (also known as incarcerated hernia): Hernia contents cannot be completely returned to the peritoneal cavity. [11]
- Obstructed hernia: a hernia in which the lumen of the intestine within the hernial sac has become completely obstructed
-
Strangulated hernia
- A hernia in which the contents of the hernial sac (e.g., omentum, bowel) have become ischemic due to a compromised vascular supply
- Richter hernia: a subset of strangulated hernias in which only the antimesenteric portion of the intestinal wall is trapped by the abdominal wall defect, causing ischemia without obstruction [12][13]
- Complex hernia: a hernia that is technically challenging to repair, requires a longer operative time, and has greater associated perioperative morbidity than a simple hernia [14]
Intermediate-sized abdominal wall defects have the highest risk of causing an incarcerated hernia. Small wall defects are less likely to allow a visceral protrusion and large wall defects are less likely to cause mechanical impingement of the contents of the hernial sac.


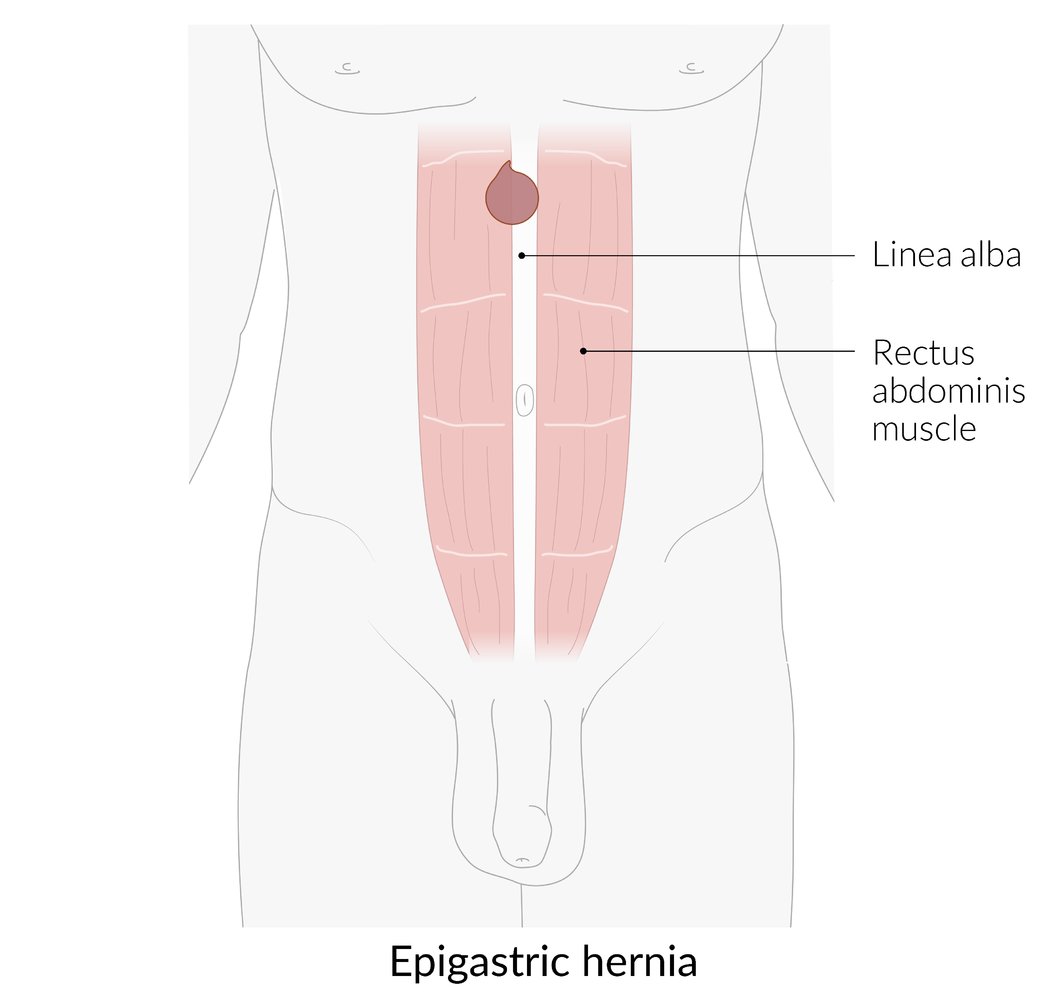
Herniation of intraabdominal contents through the linea alba, between the xiphoid process and the umbilicus.
© AMBOSS

Photograph of the abdomen of a female patient (lateral view)
The epigastric region of the abdomen is bulging ventrally.
This appearance is suggestive of an epigastric hernia.
Source: “Figure 1. in: Endoscopic-Assisted Linea Alba Reconstruction plus Mesh Augmentation for Treatment of Umbilical and/or Epigastric Hernias and Rectus Abdominis Diastasis-Early Results.” by Ferdinand Köckerling, Marinos Damianos Botsinis, Christine Rohde and Wolfgang Reinpold, Frontiersin, licensed under CC BY 4.0.

CT abdomen (with contrast; axial plane)
A midline epigastric hernia (green arrowheads) contains transverse colon (TC). A colocutaneous fistula has formed, with necrosis (N) visible near the skin surface.
RK: right kidney
Source: “Fig 2, In: Severe Mental Illness: A Contraindication to Watchful Waiting in Hernia Management?” by Milne DM, Naraynsingh V, Goolcharan S, Cureus, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen and pelvis (with contrast; axial plane) of a patient with a history of left lower quadrant colostomy
A large parastomal hernia (arrowheads and green overlay) contains portions of the stomach (S), mesentery (M), small bowel (SB), and colon (C).
K: contrast-enhanced left kidney
Source: “Fig 1, In: Gastric Parastomal Hernia: A Case Report of a Rare yet Fascinating Clinical Entity” by Waheed A, Zeller PE, Bishop PJ, Robinson SK, Tuma F, Cureus, licensed under CC BY 3.0. Modifications: removed arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
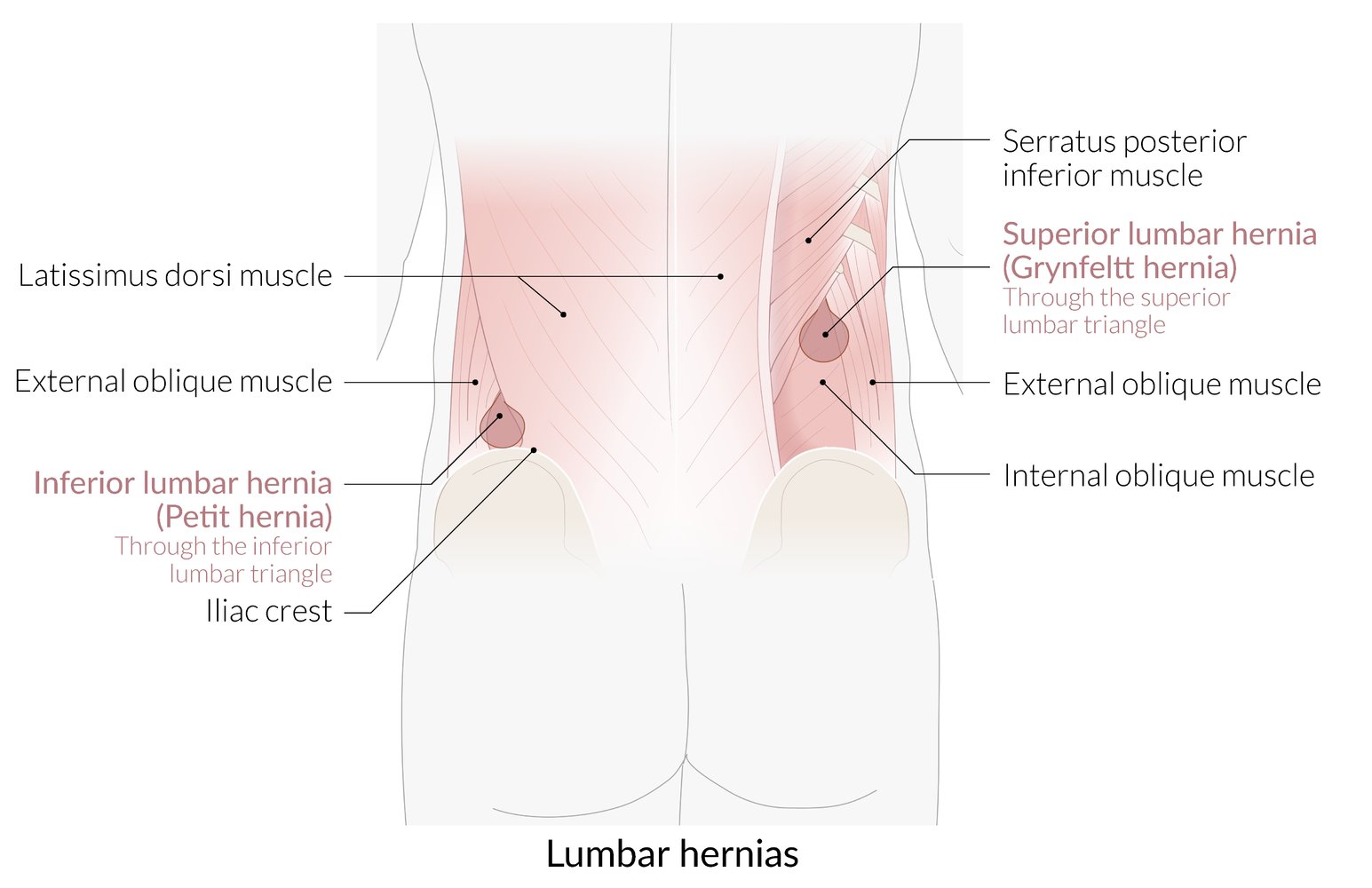
Superior lumbar hernia (Grynfeltt hernia): herniation of intraabdominal contents through the superior lumbar triangle, the boundaries of which are the 12th rib, the erector spinae muscle, and the internal oblique muscle
Inferior lumbar hernia (Petit hernia): herniation of intraabdominal contents through the inferior lumbar triangle, the boundaries of which are the iliac crest, the latissimus dorsi, and the external oblique muscle
© AMBOSS
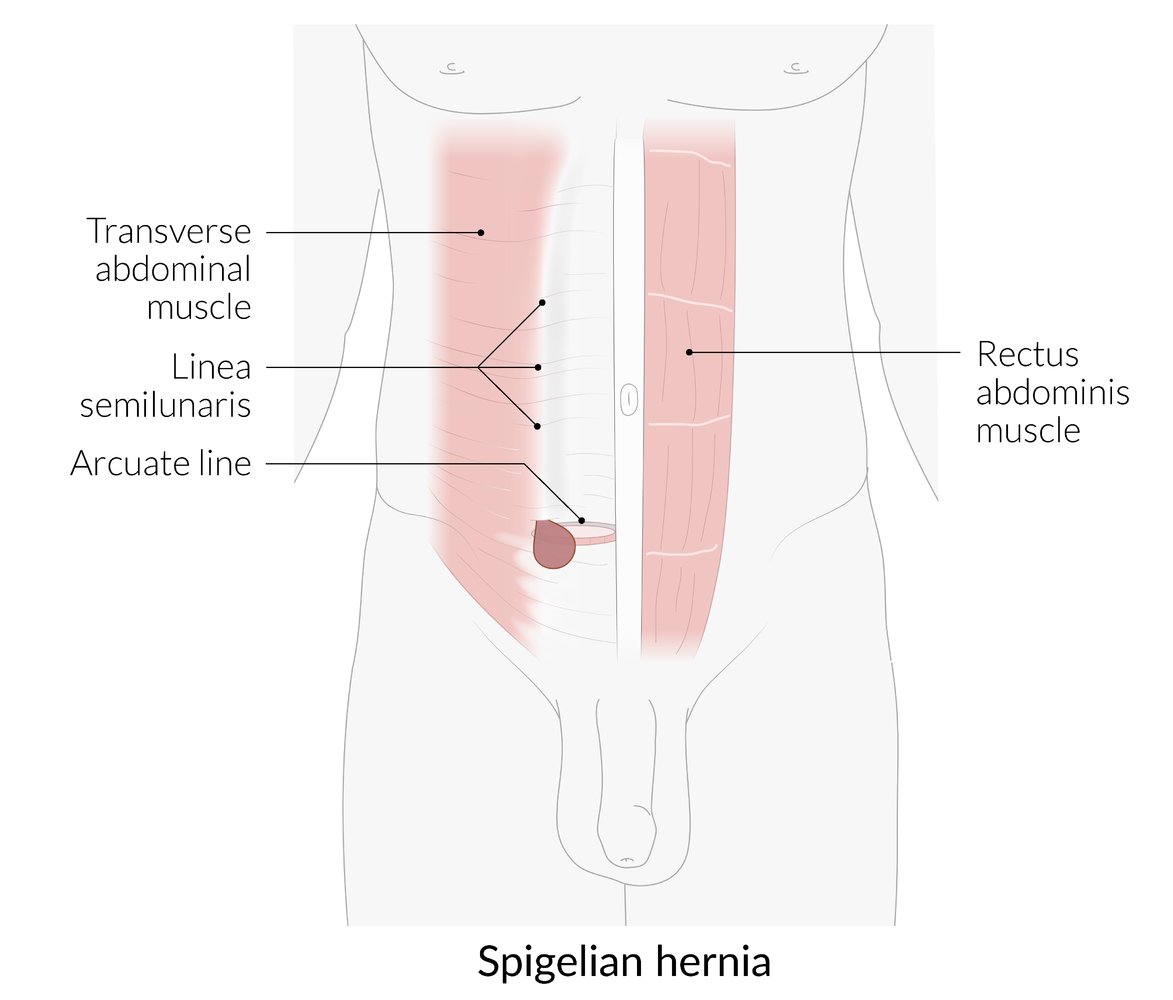
Herniation of intraabdominal contents through the semilunar line; commonly adjacent to the arcuate line (typically below the umbilicus)
The semilunar line is the lateral border of the rectus abdominis. The arcuate line is the inferior border of the posterior rectus sheath. The lack of posterior rectus sheath below the arcuate line is assumed to predispose this region to hernia formation.
© AMBOSS

Photograph of the anterior abdominal wall of a female patient
An ill-defined swelling is visible just lateral to the left rectus abdominis muscle (i.e., along the semilunar line). Examination of the mass showed a positive cough impulse.
This is the typical appearance of a Spigelian hernia, an uncommon ventral hernia.
Source: “Hernia spiegheli 01” by AfroBrazilian, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
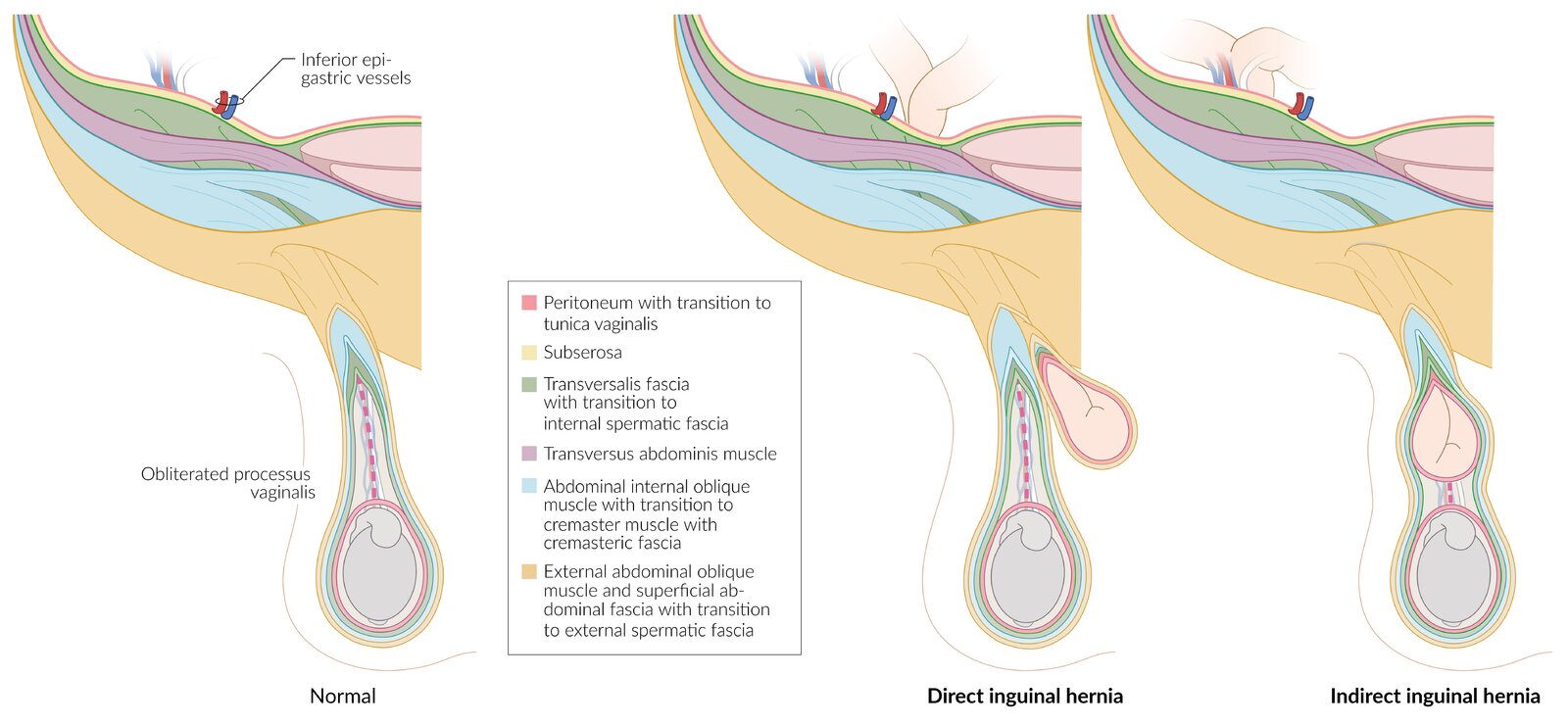
Normally, the only contents of the inguinal canal are the spermatic cord (or round ligament in females) and the ilioinguinal nerve.
Direct inguinal hernia: herniation of intraabdominal contents through the posterior wall of the inguinal canal, medial to the inferior epigastric vessels. The hernial sac lies posteromedial to and outside the spermatic cord
Indirect inguinal hernia: herniation of intraabdominal contents through the deep inguinal ring into the inguinal canal, and, in the case of large inguinal hernia, also through the superficial inguinal ring. The hernial sac lies within the spermatic cord and is therefore covered by the same tissue layers as the spermatic cord.
© AMBOSS

Pelvic and inguinal region
There is a pronounced protrusion on the right side (circled). Inguinal hernia can be confirmed with palpation and a cough test.
Source: “Hernia” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
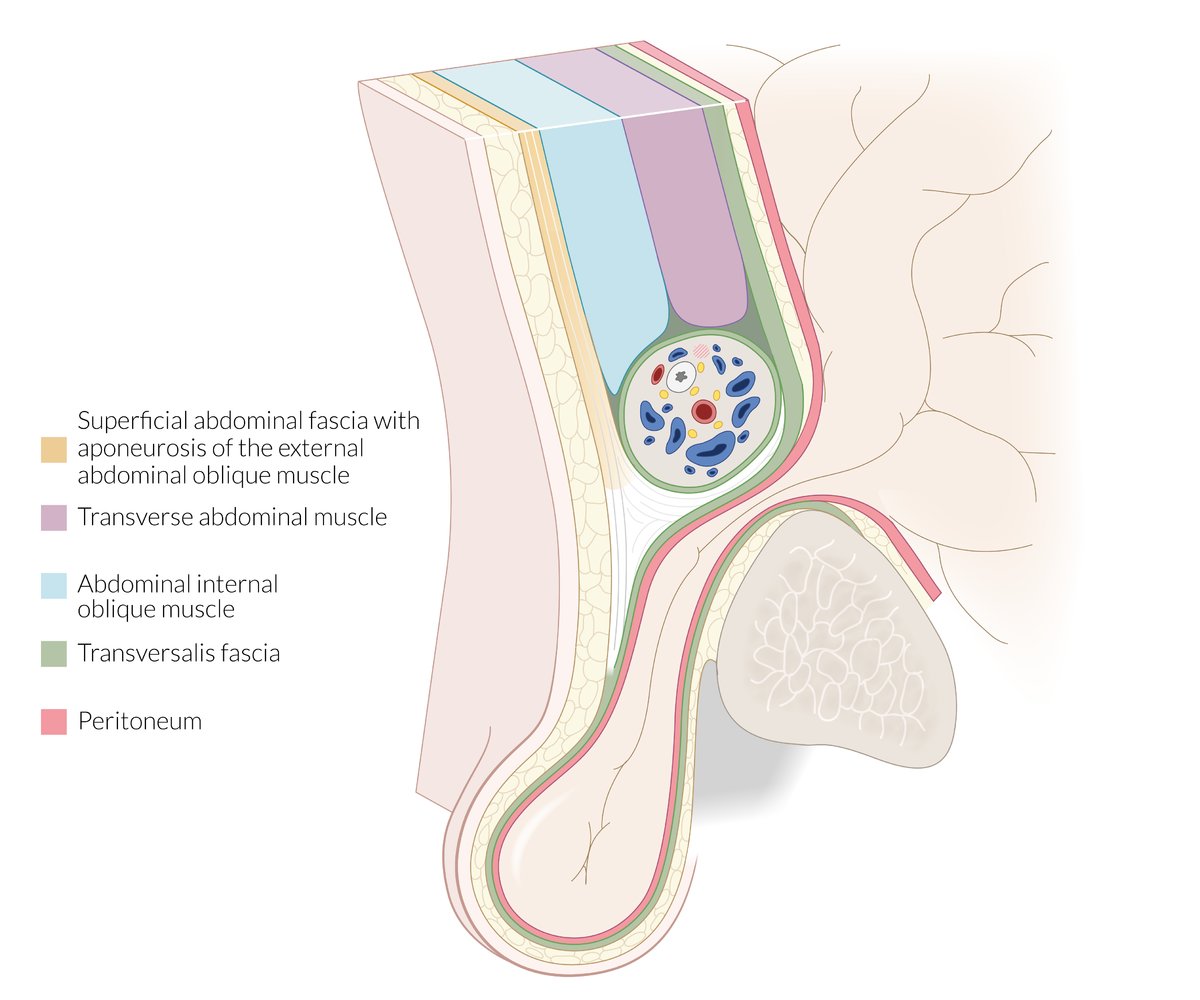
Sagittal view of the male inguinal region at the level of the superior pubic ramus, medial to the epigastric vessels
There is a protruding hernial sac (comprised of the transversalis fascia and parietal peritoneum) below the inguinal ligament but above the pubic bone, which, in the example shown, contains intestine.
© AMBOSS
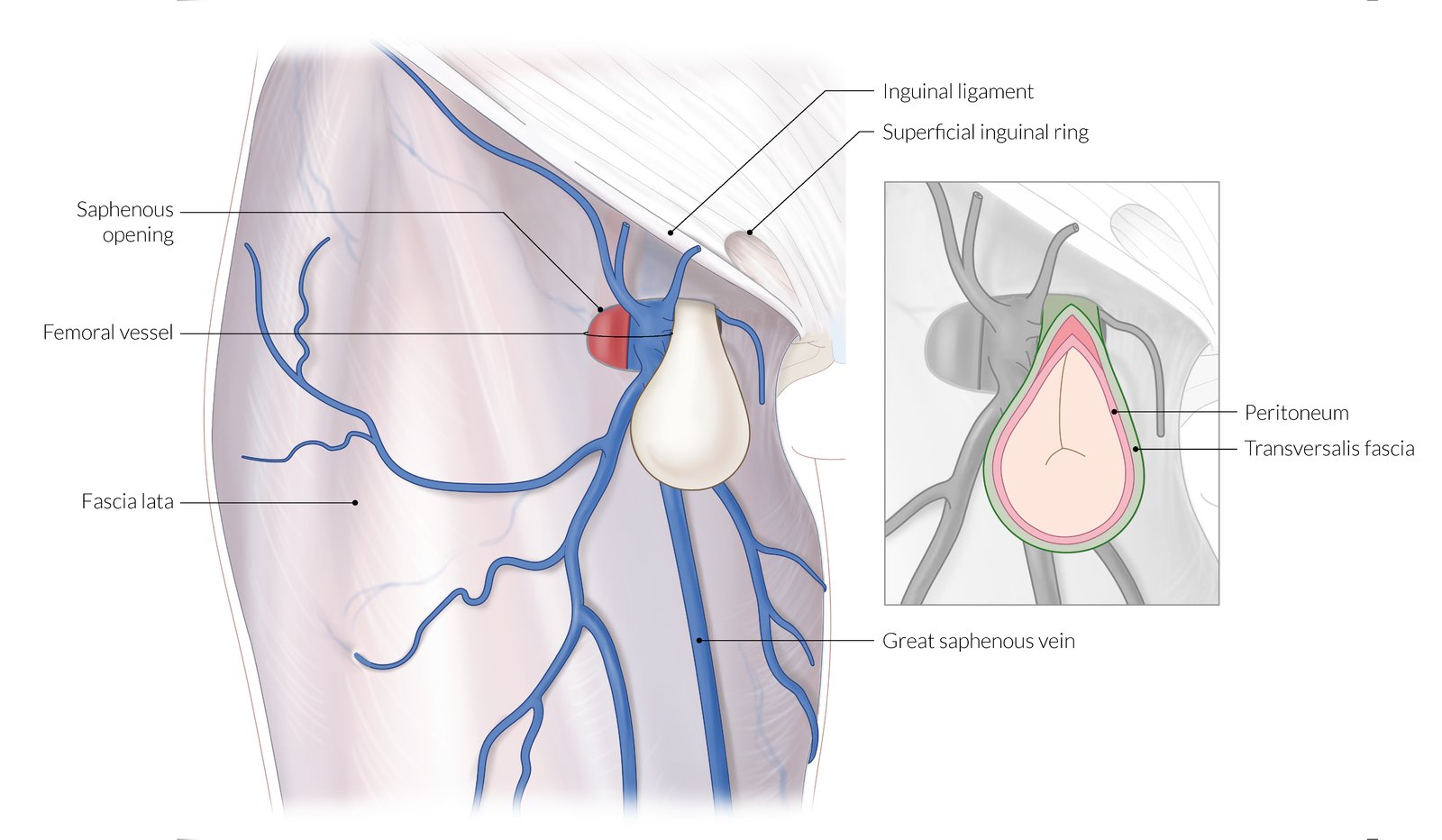
Femoral hernia passes through the vascular lacuna (internal hernial orifice), below the inguinal ligament and usually medial to the femoral vein and runs through the femoral canal until it reaches the saphenous opening (external hernial orifice; approx. 2cm caudal).
The saphenous opening typically contains loose connective and fatty tissue as well as inguinal lymph nodes.
Due to the increased width of the female pelvis, and therefore larger vascular lacuna, femoral hernia occurs predominantly in women.
© AMBOSS
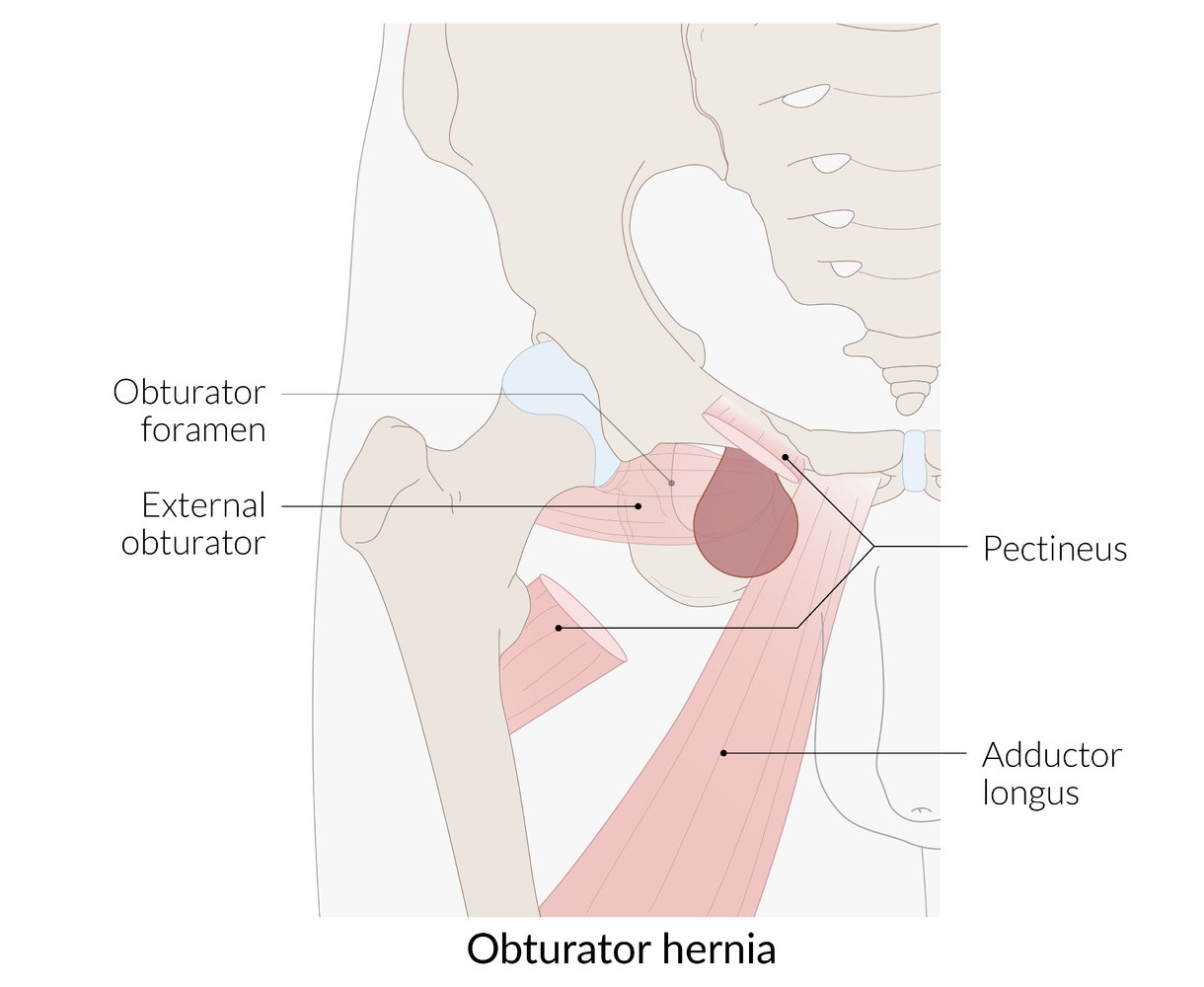
Herniation of intraabdominal contents through the obturator foramen of the pelvis.
The hernia passes superior and anterior to the external obturator muscle and lies posterior to the pectineus muscle.
© AMBOSS
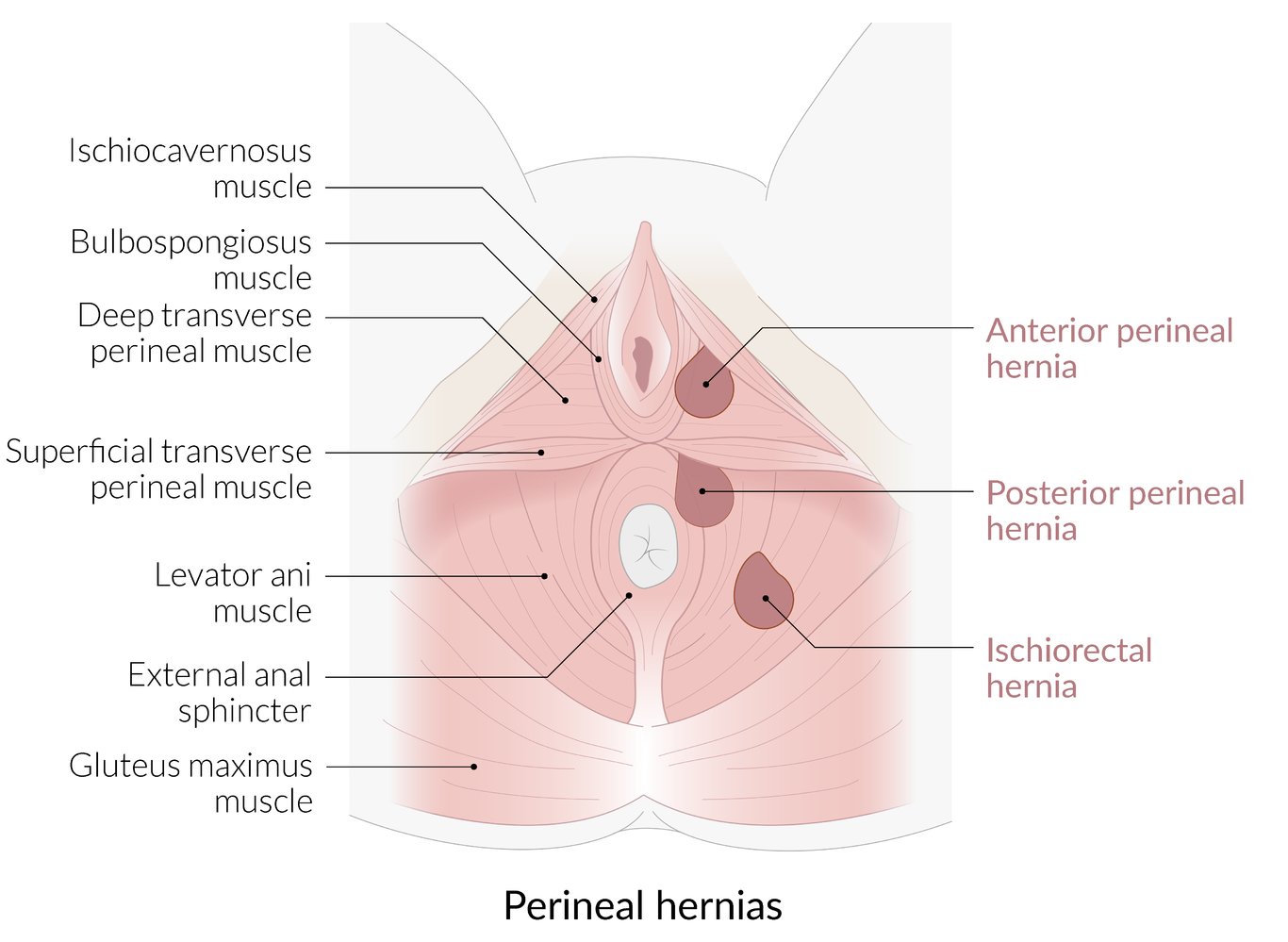
Perineal hernias involve herniation of intra-abdominal contents through a defect in the pelvic floor.
There are three types:
1. Anterior perineal hernia: herniation anterior to the superficial transverse perineal muscle
2. Posterior perineal hernia: herniation posterior to the superficial transverse perineal muscle
3. Ischiorectal hernia: herniation through the levator ani muscle
© AMBOSS
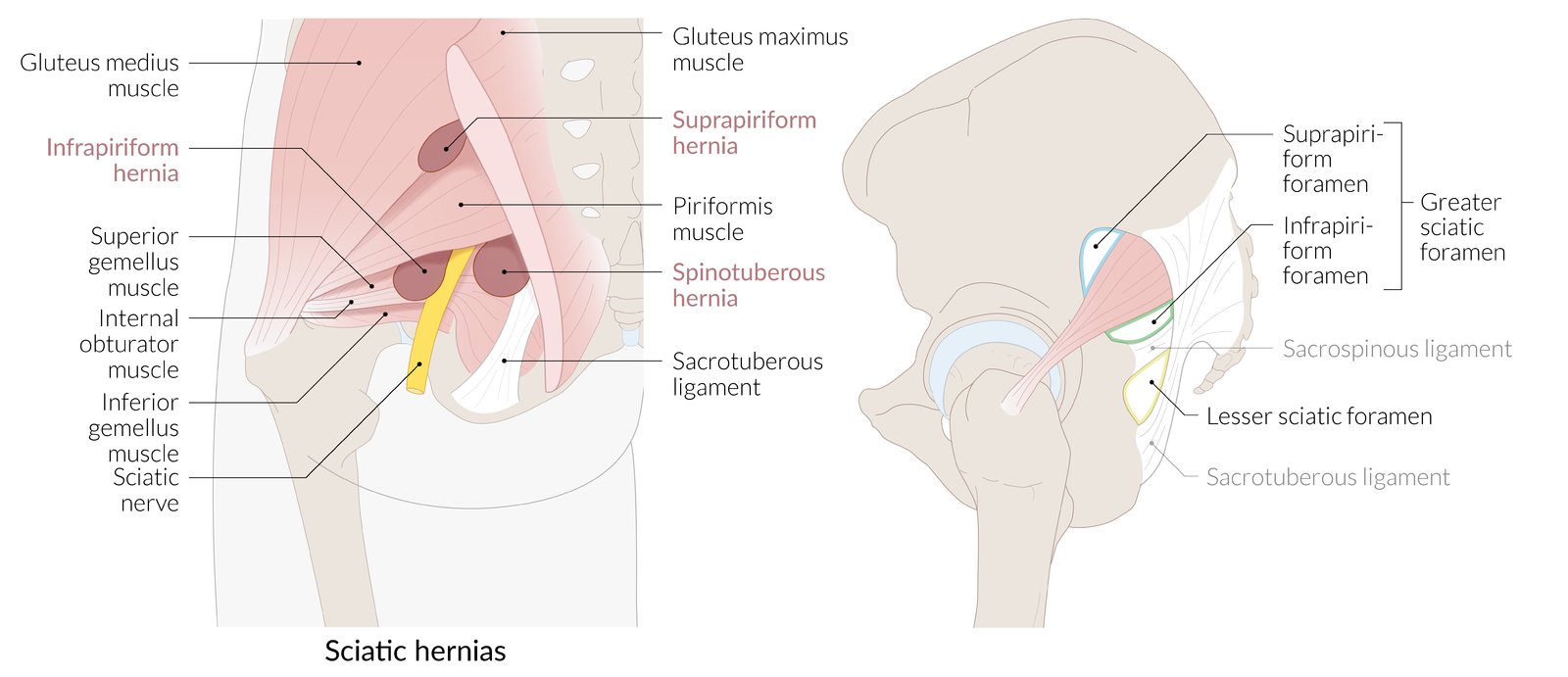
Herniation of intra-abdominal contents through the greater (more common) or lesser sciatic foramen.
Hernias through the greater sciatic foramen can be further classified into suprapiriform (more common) and infrapiriform hernias.
© AMBOSS
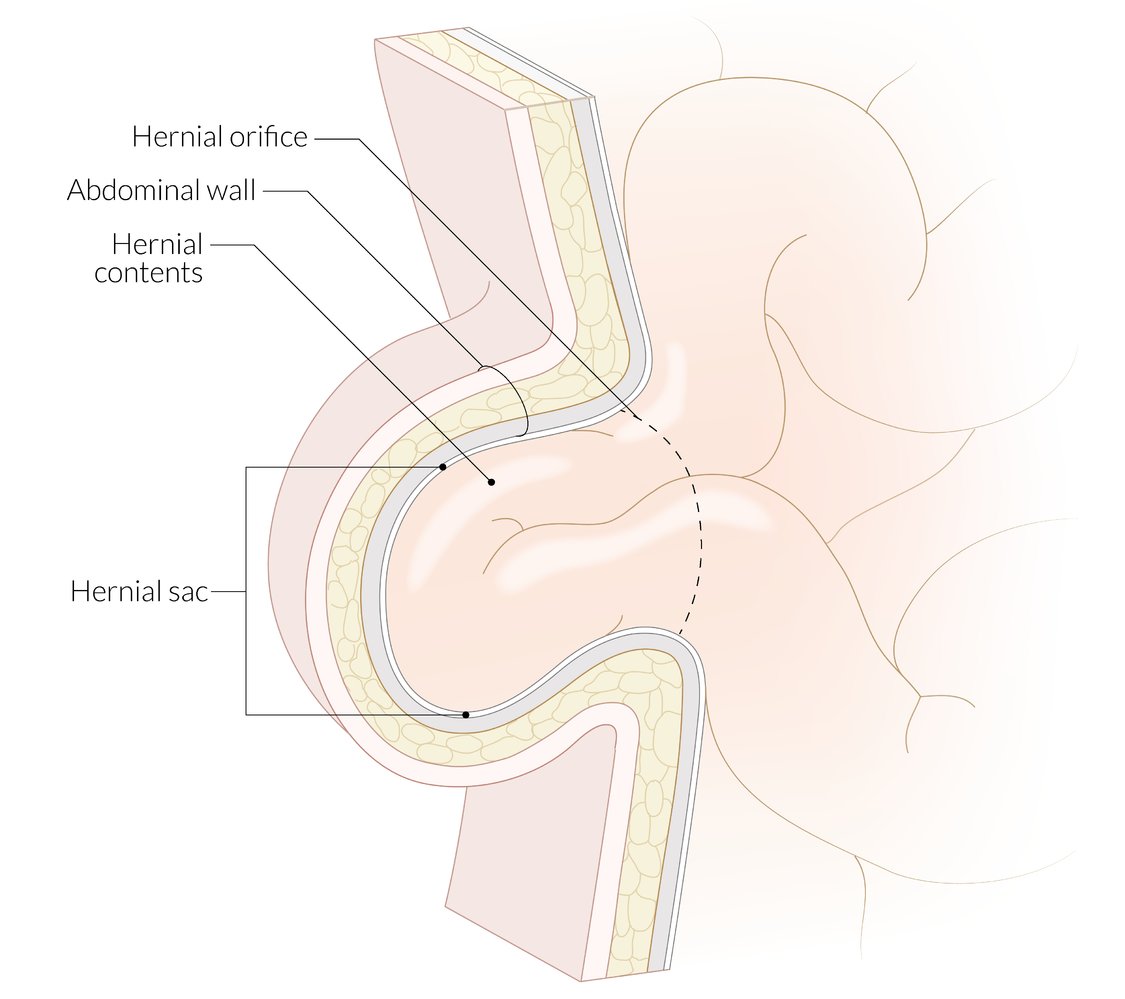
Abdominal and inguinal hernias have three components:
– Hernial sac: parietal peritoneum surrounding the hernial contents
– Hernial contents: typically the omentum and/or loops of small intestine; uncommonly, the large intestine, appendix, bladder, fallopian tubes
– Hernial coverings: layers of the abdominal wall
The hernial orifice is a hiatus (e.g., the umbilicus, deep inguinal ring, posterior wall of the inguinal canal) through which hernial contents herniate. The hernial contents are constricted at the hernial orifice; this constricted area is known as the neck of a hernia.
© AMBOSS
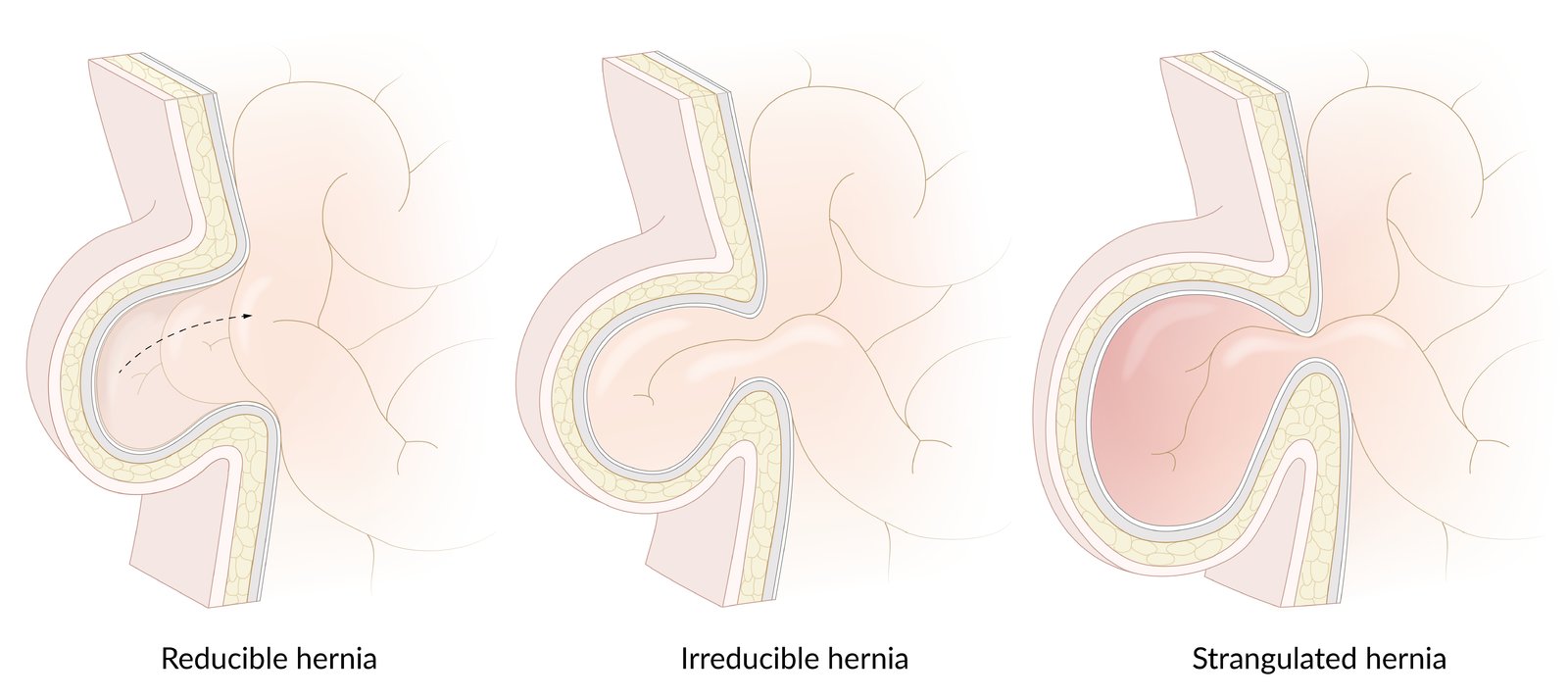
– Reducible hernia: The hernia is easily reducible.
– Irreducible hernia: The hernia is not easily reducible because its contents adhere to the hernial sac.
– Strangulated hernia: ischemia of hernial contents resulting from a tight abdominal wall defect compromising the vascular supply of the hernial contents
© AMBOSS
Clinical features
Reducible hernia [15][16][17]
-
History
- Symptomatic or asymptomatic mass or fullness
- Size decreases with recumbency
- Size increases with sitting, standing, and/or straining
-
Physical examination
- Nontender mass that returns to the peritoneal cavity with mild, externally applied pressure
- Visible or palpable cough impulse: expansion of the mass with increased abdominal pressure
- Edges of the fascial defect may be palpable.
- Bowel sounds may be present over the mass if part of the bowel is present in the hernial sac.
Irreducible (incarcerated) hernia [15][16][17]
- Chronic incarceration: nontender or minimally tender mass
- Acute incarceration: Mass may be painful.
- Neither recumbency nor external pressure significantly reduce mass size.
- Cough impulse may be present.
Obstructed hernia [15][16][17]
- Acute pain at the site of the hernia
- Symptoms of bowel obstruction
- Absent cough impulse
Strangulated hernia [15][16][17]
-
History
- Acute pain at the site of the hernia
- Symptoms of bowel obstruction (if part of the bowel is present in the hernial sac)
-
Physical examination
- Tender, nonreducible hernia
- Absent cough impulse
- Edematous, erythematous, warm overlying skin
- Systemic symptoms: fever, signs of sepsis
Intestinal strangulation can lead to gangrene, which can be fatal if not treated promptly.

Atypical manifestations [1][15][16][17]
Pelvic hernias
- Obturator hernia: pain and paresthesia in the pelvis and inner thigh, episodic intestinal obstruction
- Perineal hernia: pelvic pain, mass on rectovaginal examination
- Sciatic hernia: symptoms of bowel obstruction, mass in the gluteal or intragluteal area
Spigelian hernia (spontaneous lateral ventral hernia, hernia of semilunar line)
- Definition: protrusion of abdominal contents and/or peritoneum through a defect in the lower anterior abdomen adjacent to the semilunar line
- Epidemiology: very rare (0.1–2% of all ventral hernias) [18]
- Etiology: ↑ intraabdominal pressure (e.g., obesity, pregnancy, ascites), trauma to the abdominal wall (e.g., prior incisions), and/or degeneration of the abdominal aponeurotic layers → defect between the rectus abdominis and the semilunar line in the Spigelian aponeurosis → protrusion of abdominal contents and/or peritoneum [19]
- Risk factors: older age, disorders of collagen synthesis (e.g., Ehlers-Danlos syndrome), smoking [18][19]
-
Clinical features: variable
- Abdominal pain
- Palpable mass along the Spigelian fascia [19]
- Diagnostics: ultrasound and CT scan
- Treatment: All Spigelian hernias must be repaired surgically because of the high risk of incarceration and/or obstruction.

An ill-defined swelling with erythema of the overlying skin can be seen in the right inguinal region.
This is the typical appearance of a strangulated inguinal hernia, which should be differentiated from other causes of erythematous inguinal swellings (e.g., inguinal lymphadenitis, abscess, hematoma) with imaging.
Source: © IMPP
Diagnosis
General principles
- An abdominal hernia is usually a clinical diagnosis made on physical examination.
- Imaging may be necessary if the examination is difficult (e.g., due to tenderness, obesity, scarring) or presentation is atypical, and for surgical planning.
- Laboratory studies are indicated if strangulation or obstruction is suspected and as part of preoperative preparation.
- For patients presenting with acute abdominal pain, see also “Approach to acute abdomen.”
Imaging [4][20][21]
Indications [22]
- Unclear diagnosis, e.g., abdominal wall pain without a clinically apparent hernia
- Suspected complication, e.g., bowel obstruction or strangulation
- Obesity (BMI > 35 kg/m2)
- Recurrence of incisional hernias
- Planning for surgical repair
Modalities
-
CT abdomen
- Sensitive imaging study for suspected bowel obstruction or strangulation [10]
- Typically performed with both IV and PO contrast (unless contraindicated because of obstruction)
- Can facilitate planning for complex hernia repair [23]
-
Ultrasound
- Consider in children and for nonacute adult groin hernias.
- Allows for dynamic assessment: The patient can perform a Valsalva maneuver or reposition themselves to induce a hernia.
-
MRI abdomen
- Indications: to rule out musculoskeletal disorders and occult groin hernia [24]
- Like ultrasound, MRI allows for dynamic assessment.
- Abdominal x-ray: may be used to rapidly evaluate for bowel obstruction and perforation
Findings
- Direct visualization and quantification of the fascial defect(s)
- Presence of viscera in the hernial sac
- Strangulated hernia: signs of visceral ischemia [25]
- Obstructed hernia: radiological signs of mechanical bowel obstruction


Laboratory studies [26]
Laboratory studies may show characteristic findings if a hernia is obstructed and/or strangulated, including:
- Findings that suggest bowel ischemia, e.g.:
- ↑ Leukocytes
- ↑ Lactate
-
Laboratory findings that suggest hypovolemia, e.g.:
- Electrolyte abnormalities
- ↑ Hematocrit
CT abdomen (with contrast; axial plane)
A midline epigastric hernia (green arrowheads) contains transverse colon (TC). A colocutaneous fistula has formed, with necrosis (N) visible near the skin surface.
RK: right kidney
Source: “Fig 2, In: Severe Mental Illness: A Contraindication to Watchful Waiting in Hernia Management?” by Milne DM, Naraynsingh V, Goolcharan S, Cureus, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (with IV and oral contrast; axial plane)
An anterior abdominal wall hernia (yellow overlay) containing fat is seen lateral to the left rectus abdominis muscle.
A Spigelian hernia occurs through a defect in the linea semilunaris, a curved vertical line at the lateral margin of each rectus abdominis muscle. Spigelian hernias are usually found in the region of the arcuate line, a horizontal line that demarcates the lower extent of the posterior layer of the rectus sheath.
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Spigelian Hernia”. Created by: Wishes to remain anonymous. Licensed under Public Domain. Modifications to original image: arrow removed.
{kind=link}
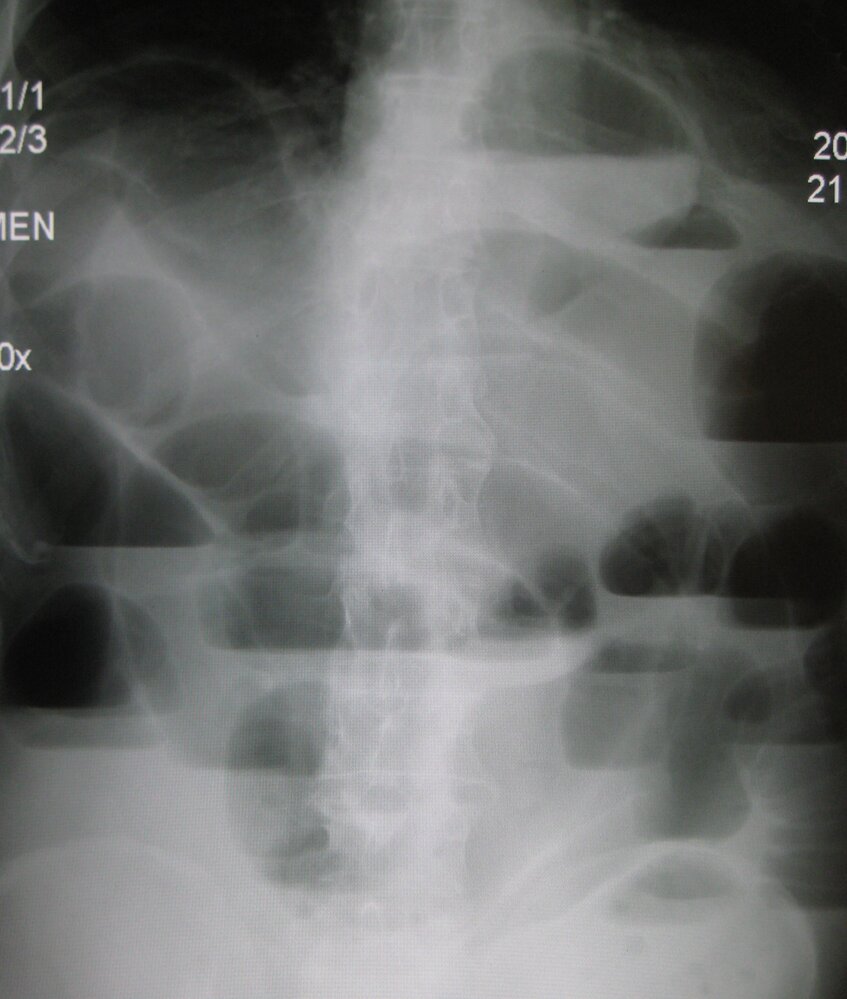
X-ray abdomen (AP view; erect)
Multiple distended bowel loops (examples indicated by white dashed outlines) are seen, many of which contain air-fluid levels (examples indicated by green overlay). A distended colon (with haustra) is not visible. The pattern of the distended loops suggests small bowel obstruction.
S: stomach
Source: “Upright X-ray demonstrating small bowel obstruction.jpg” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: - letter "R" removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
Differential diagnoses of ventral hernias
- Diastasis recti
- Abdominal wall tumor (e.g., desmoid tumor)
- Lipoma
- In newborns: omphalocele, gastroschisis

Rectus sheath hematoma
- Definition: an accumulation of blood within the rectus sheath that most commonly arises from the disruption of a branch of the inferior epigastric artery
-
Etiology [27][28]
- Blunt or penetrating trauma
- Spontaneous
-
Risk factors
- Age > 70 years
- Anticoagulation or antiplatelet therapy
- Coagulation disorders
- Pregnancy [29]
-
Clinical features [28]
- Acute onset abdominal pain
- Palpable abdominal mass
- Abdominal tenderness and/or guarding
-
Carnett sign
- The patient is in the supine position and asked to sit upright while the point of maximal abdominal tenderness is palpated
- Positive if the tenderness remains unchanged or increases during contraction of the rectus abdominis muscles
-
Fothergill sign
- The patient is asked to lie in the supine position and contract the abdominal muscles, e.g., by lifting the head or lower limbs
- Positive if the palpable abdominal mass does not cross the midline and remains palpable after contraction of the rectus abdominis muscles
- Cullen sign (periumbilical ecchymosis)
- Grey Turner sign (flank ecchymosis)
- Signs of hypovolemic shock (e.g., tachycardia, hypotension)
-
Diagnostics [27][29]
- Serial measurement of hematocrit and/or hemoglobin levels; anemia and/or leukocytosis may be present.
- CT scan (confirmatory test): hematoma confined to the abdominal wall
- Abdominal ultrasound: alternative modality to CT for children and pregnant women
-
Treatment [27]
- Compression of the hematoma
- Correction of abnormal coagulation
- IV fluid resuscitation and/or blood transfusion
-
Hemodynamically unstable patients with expanding hematoma
- Angiography with arterial embolization
- Surgical evacuation of the hematoma and ligation of the artery

Differential diagnoses of other hernias
-
Pelvic and groin hernias
- Inguinal lymphadenopathy
- Cryptorchid testes
- Lipoma
- Femoral artery aneurysm
-
Strangulated hernia
- Abscess
- Hematoma
- Lymphadenitis (strangulated groin hernias)
The differential diagnoses listed here are not exhaustive.
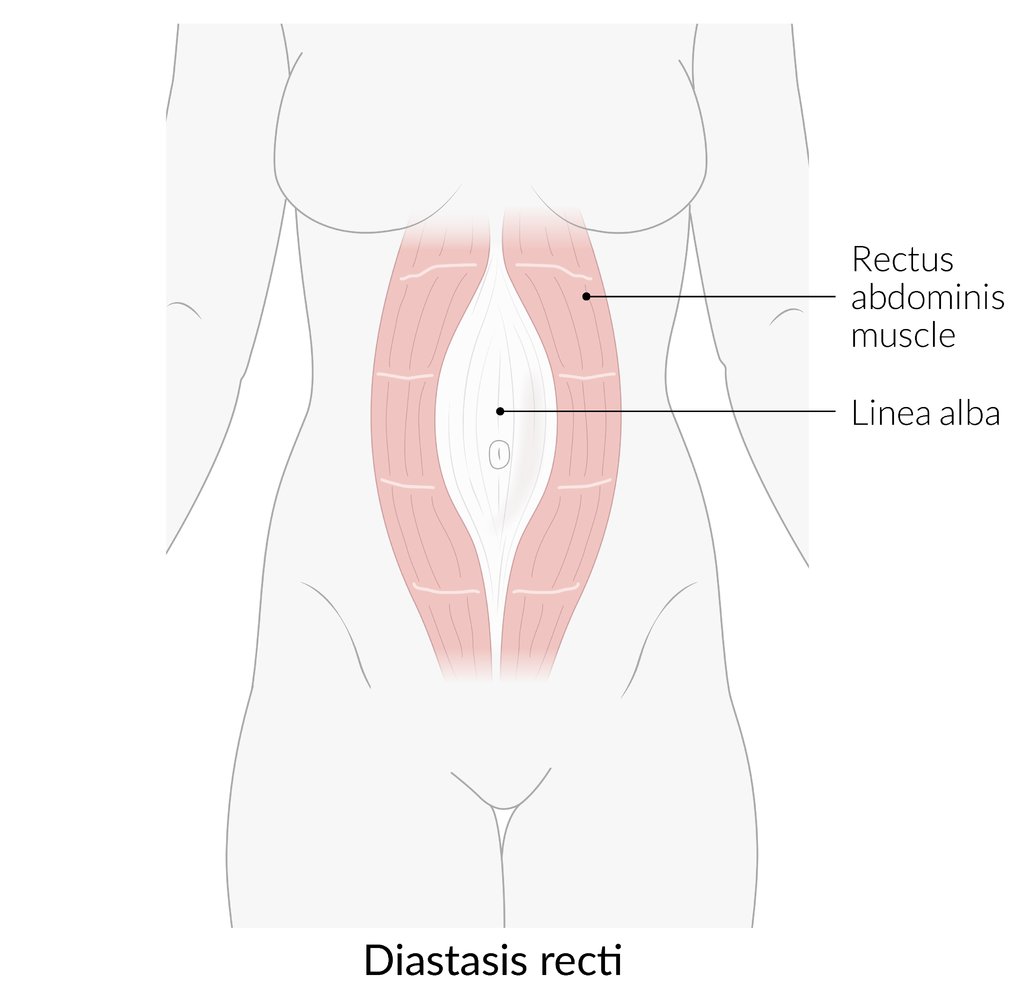
There is an abnormally large separation (>2 cm) between the two rectus abdominis muscles. This results in protrusion of intra-abdominal contents through the linea alba on straining (e.g., coughing, sitting up from a reclined posture), causing a midline bulge. The abdominal fascias (not shown here) remain intact.
© AMBOSS

CT abdomen (with contrast; axial plane) of a patient with acute left anterior abdominal pain
There is marked asymmetry in size of the right and left rectus muscles. The enlarged left rectus muscle (green overlay) is heterogeneous, with low and high attenuation components. High attenuation (hatched green overlay) represents a site of contrast-enhanced blood from acute hemorrhage.
RRM: right rectus muscle
Source: “Axial CT of rectus sheath hematoma, with active bleeding under Marcumar” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Treatment
Surgical repair is the definitive treatment for abdominal wall hernias, but management with watchful waiting may be appropriate in select patients. See also “Incisional hernia” and “Umbilical hernia” for management specific to these hernia types.
Initial management [30][31]
-
Reducible hernia or chronically irreducible hernia
- Obtain outpatient surgical consult for further management, e.g., conservative management vs. elective hernia repair.
- Provide analgesia as needed.
-
Acutely irreducible hernia without signs of obstruction or strangulation
- Obtain urgent surgical consult.
- Provide analgesia as needed.
- Consider manual hernia reduction as a temporizing measure.
- Continue to observe the patient for signs of strangulation and obstruction.
-
Strangulated or obstructed hernia
- Obtain emergency surgery consult and begin supportive care as needed.
- Keep the patient NPO; consider nasogastric tube insertion.
- Begin IV fluid resuscitation.
- Administer parenteral analgesics and antiemetics.
- Obstructed hernia without signs of strangulation: Consider manual hernia reduction. [32][33]
- Signs of strangulation: Consider IV broad-spectrum antibiotics (see “Empiric antibiotic therapy for intraabdominal infection”). [10][34]
- Obtain emergency surgery consult and begin supportive care as needed.
Treat strangulated hernias and obstructed hernias as surgical emergencies, for which operative repair is indicated within hours to prevent complications (e.g., intestinal ischemia, sepsis, and death).
Manual hernia reduction [31][32][33]
- Indications: acutely incarcerated hernias with no signs of strangulation
-
Preparation
- Obtain informed consent.
- Administer analgesia; consider the need for procedural sedation.
-
Procedure
- Ask the patient to lie in the supine position.
- Apply ice or a cold compress over the hernia.
- Apply slow, steady pressure to the hernia sac for up to 20 minutes.
-
Next steps
- Reduction successful
- Typically, patients are admitted for observation for at least 12 hours.
- Schedule early surgical repair (often performed during the same admission).
- Unsuccessful reduction or new signs of strangulation: prompt surgical intervention
- Reduction successful
- Complications: visceral rupture or perforation, peritonitis, worsened ischemia
Do not attempt to reduce a strangulated hernia! Gangrenous bowel may be forced into the abdominal cavity, which can lead to peritonitis and sepsis. [30]
Nonoperative and preoperative management
-
Watchful waiting may be considered in selected patients. [4][22][23]
- Asymptomatic patients with high perioperative risk and/or low risk of hernia complications (e.g., small umbilical hernias)
- Asymptomatic patients with modifiable risk factors that may be treated preoperatively
- If elective hernia repair is anticipated, consider starting preoperative lifestyle modifications (e.g., smoking cessation, weight loss) and optimization of chronic illnesses. [4][35]
- Hernia trusses and binders may improve patient comfort but have not been found to reduce the risk of acute hernia complications. [36]
Surgical management [1]
-
Indications
- Emergency surgery for any obstructed hernias or strangulated hernias
- Elective surgery for all symptomatic hernias and asymptomatic hernias at risk for complications
- Techniques (open or laparoscopic): include hernioplasty (i.e., with mesh) and herniorrhaphy (i.e., with sutures) [23][30][35]
-
Complications following surgery include: [23][35]
- Recurrence [35]
- Infection
- Others: e.g., seroma, wound dehiscence, enterocutaneous fistula, chronic pain
Incisional hernia
- Definition: herniation of intraabdominal contents through an abdominal wall defect due to previous abdominal surgery
- Incidence: up to 20% after abdominal surgery [37][38]
-
Risk factors [22][30][38]
- Laparotomy, especially via midline incision
- Postoperative wound infection
- Patient factors: smoking history, diabetes mellitus, obesity, immunosuppression, malnourishment, older age [35]
- Emergency abdominal surgery
- Pregnancy [1]
-
Clinical features [22][39]
- Mass or protrusion at the site of the incisional scar that increases with coughing/straining
- Edges of the hernial defect are palpable upon reduction of the hernia
- Patients may be asymptomatic or present with nonspecific symptoms such as postprandial fullness.
-
Treatment [22][39]
- Elective surgical repair (usually with mesh) is typically recommended. [30][39][40]
- Conservative management may be considered in patients at high risk for perioperative morbidity, e.g., patients with COPD. [41]
-
Complications [22][35]
- Strangulation or obstruction: Up to 20% of patients with a ventral hernia will require emergency surgery. [30]
- Recurrence after repair: ∼ 15–25% of repaired incisional hernias recur [35]
-
Parastomal hernia [1][42]
- A type of incisional hernia in which intraabdominal contents protrude through the abdominal wall defect created during stoma placement (e.g., colostomy)
- Diagnosis: usually clinical; imaging (CT or ultrasound) may be considered if the diagnosis is uncertain.
- Management
- Consult ostomy nurse to help with management.
- Asymptomatic parastomal hernias may be managed conservatively with a support garment (e.g., ostomy belt).
- Symptomatic parastomal hernias may require surgical repair.



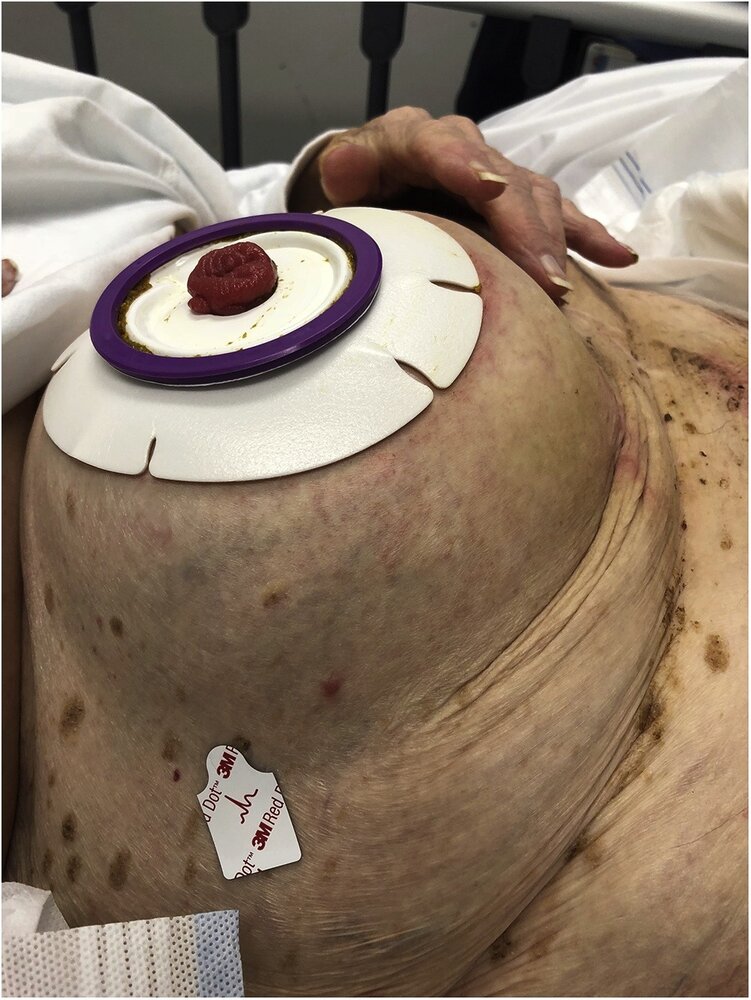
Abdominal wall of a 92-year-old woman with a long-established end ileostomy who presented with vomiting and abdominal pain
There is gross circumferential swelling around the stoma. CT showed parastomal herniation of the distal stomach.
Source: “Fig 1, In: Parastomal stomach herniation complicated by gastric outlet obstruction: A case report and literature review” by Eastment J, Burstow M, ScienceDirect, licensed under CC BY 4.0.
CT abdomen and pelvis (with contrast; axial plane) of a patient with a history of left lower quadrant colostomy
A large parastomal hernia (arrowheads and green overlay) contains portions of the stomach (S), mesentery (M), small bowel (SB), and colon (C).
K: contrast-enhanced left kidney
Source: “Fig 1, In: Gastric Parastomal Hernia: A Case Report of a Rare yet Fascinating Clinical Entity” by Waheed A, Zeller PE, Bishop PJ, Robinson SK, Tuma F, Cureus, licensed under CC BY 3.0. Modifications: removed arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

A bulging mass with an overlying midline laparotomy scar is visible in the epigastric region.
These features suggest an incisional hernia.
Source: “File:Hernia epigástrica.png” by PacoPeramo, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

A bulging mass is visible in the epigastric region, with an overlying midline laparotomy scar.
These features suggest an incisional hernia.
Source: “Fig. 1, in: Laparoscopic Incisional Hernia Repair” by Kurmann A, Beldi G, IntechOpen, licensed under CC BY 3.0.
Umbilical hernia
Umbilical hernias are defined as midline hernias at the level of the umbilicus. Ninety percent of umbilical hernias are acquired, usually as a result of increased abdominal pressure. [2][3]
| Congenital vs. acquired umbilical hernias [43] | ||
|---|---|---|
| Congenital umbilical hernia [44][45][46] | Acquired umbilical hernia [1][4] | |
| Epidemiology |
|
|
| Site of hernial defect |
|
|
| Etiology |
|
|
| Risk factors |
|
|
| Clinical features |
|
|
| Risk of developing complications (incarceration, obstruction, strangulation, or rupture) |
|
|
| Treatment |
|
|
| Differential diagnosis |
|
|
Up to 20% of patients with cirrhosis develop an umbilical hernia. [30]







Anterior abdominal wall of a newborn
There is a mass ∼2 cm in diameter protruding through the umbilical orifice.
This is the typical appearance of a congenital umbilical hernia, which characteristically increases in size on crying or coughing.
© AMBOSS

Anterior abdominal wall of an adult
There is a mass protruding directly through the umbilical orifice.
This is the typical appearance of an umbilical hernia, which is rare in adults. Paraumbilical hernias, which protrude through a fascial defect adjacent to the umbilical orifice, are more common in adults.
Source: “Nabelbruch” by Herecomesdoc, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Anterior abdominal wall of an adult
There is a protruding mass adjacent to the superior wall of the umbilical orifice. The cavity of the umbilical orifice is obliterated by the mass, resulting in a crescent-shaped umbilicus.
This is the typical appearance of a paraumbilical hernia.
Source: “Hernia umilicalis” by Milliways, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
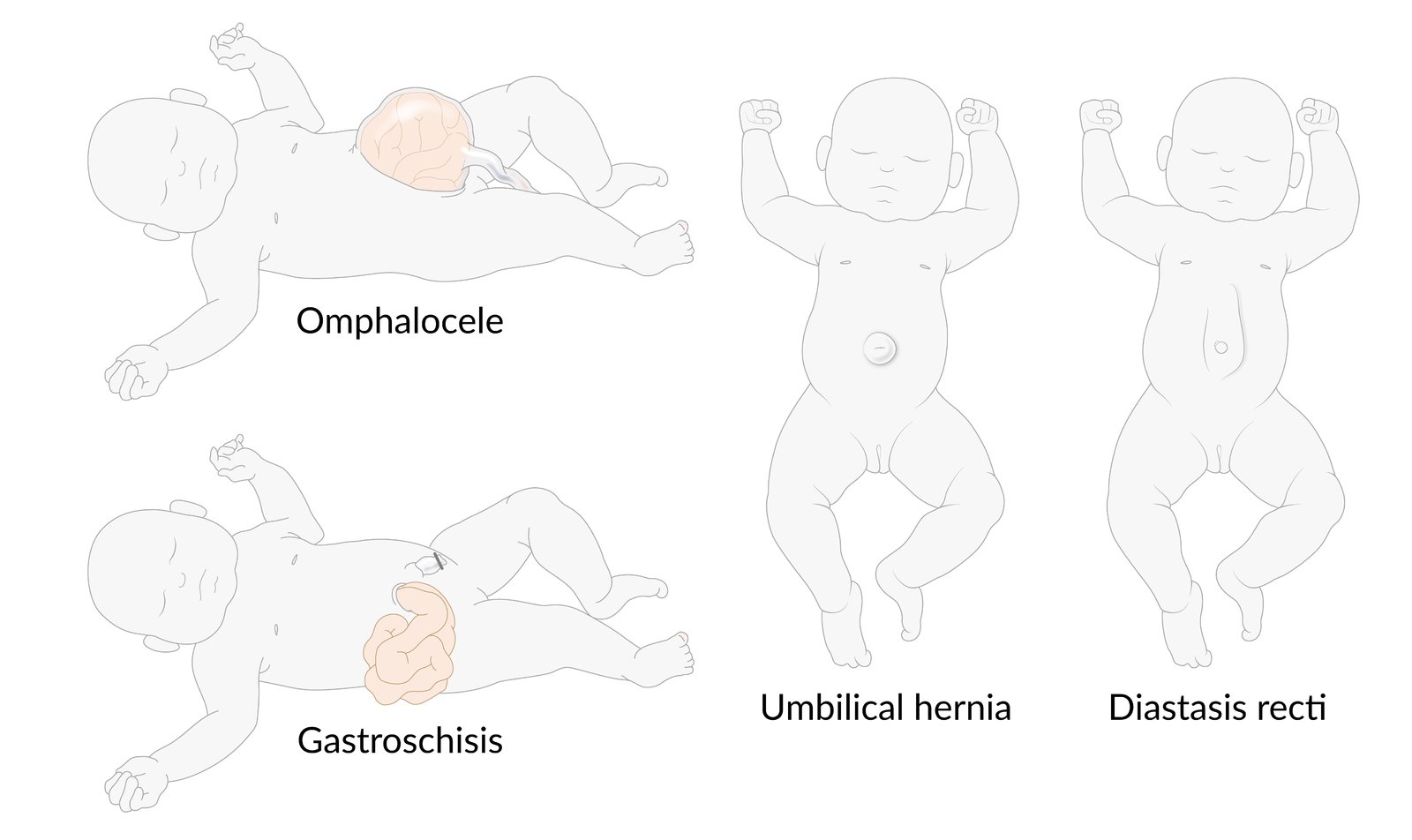
Omphalocele: herniation of intraabdominal contents through an anterior abdominal wall defect at the base of the umbilical cord caused by the failure of the midgut to return to the abdominal cavity after its physiological herniation through the umbilical ring. Accordingly, the hernial sac is formed by the amniotic membrane and peritoneum, and the umbilical cord lies at the apex of the hernia.
Gastroschisis: a developmental defect of the anterior abdominal wall in the paraumbilical region through which intraabdominal contents prolapse. As it is the anterior abdominal wall that fails to develop correctly, there is no outer peritoneal or membranous covering.
Congenital umbilical hernia: herniation of intraabdominal contents through a patent umbilical orifice, which typically closes by 2 years of age. The sac of a paraumbilical hernia is the peritoneum.
Diastasis recti: an abnormally wide separation of the right and left rectus abdominis muscles. The abdominal fascia are intact. There is therefore no herniation, but a midline bulge is visible on straining (e.g., when trying to sit up).
© AMBOSS
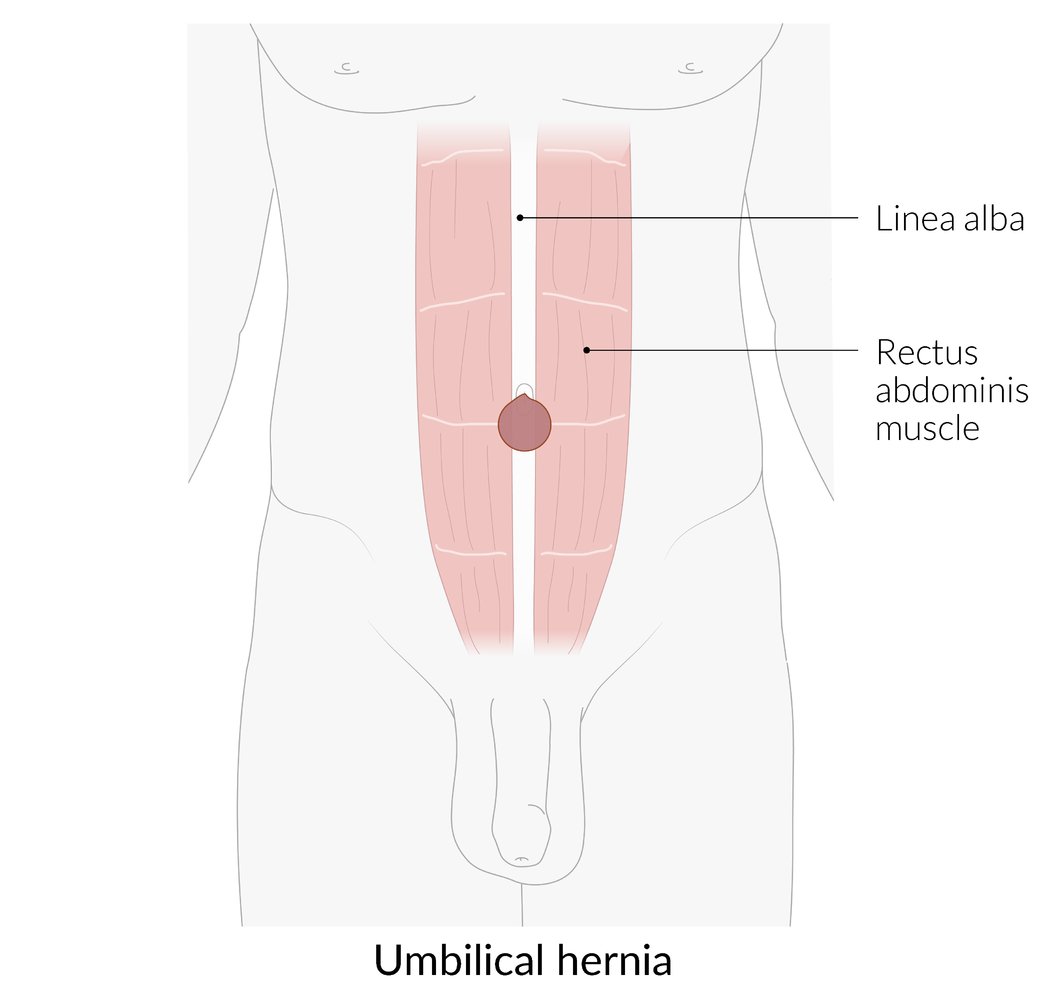
Herniation of intraabdominal contents through the umbilical orifice
A true umbilical hernia herniates through the umbilical orifice and is most common in infants (congenital umbilical hernia). Most adult umbilical hernias herniate from an abdominal wall defect adjacent to the umbilical orifice (acquired umbilical hernia).
© AMBOSS

Anterior abdominal wall of an adult
There is a protruding mass adjacent to the right lateral wall of the umbilical orifice. The right lateral wall and cavity of the umbilical orifice are obliterated by the mass, resulting in a crescent-shaped umbilicus.
This is the typical appearance of a paraumbilical hernia.
Source: “Umbilical hernia 01” by Saltanat, Wikimedia Commons, licensed under CC0 1.0.
{kind=link}
External Resources
- 2020 EHS/AHS Guidelines for Treatment of Umbilical and Epigastric Hernias
- 2019 IEHS Update of Guidelines for Laparoscopic Treatment of Ventral and Incisional Abdominal Wall Hernias
- 2018 EHS Guidelines on Prevention and Treatment of Parastomal Hernias
- 2017 WSES Guidelines for Emergency Repair of Complicated Abdominal Wall Hernias
- 2016 SAGES Guidelines for Laparoscopic Ventral Hernia Repair
References
- de Virgilio C, Frank PN, Grigorian A. "Surgery: A Case Based Clinical Review". Springer. (2015). ISBN: 9781493917259
- LeBlanc KA, Kingsnorth A, Sanders DL. "Management of Abdominal Hernias". Springer. (2018). ISBN: 9783319632506
- Reinke CE, Matthews BD. "What’s New in the Management of Incarcerated Hernia". J Gastrointest Surg. 24(1). :221-230. (2019)
- Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL. "Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice". Elsevier. (2016). ISBN: 9780323299879
- Polistina FA, Garbo G, Trevisan P, Frego M. "Twelve years of experience treating Spigelian hernia.". Surgery. 157(3). :547-50. (2015)
- Skandalakis PN, Zoras O, Skandalakis JE, Mirilas P. "Spigelian hernia: surgical anatomy, embryology, and technique of repair.". Am Surg. 72(1). :42-8. (2006)
- Yeh DD, Alam HB. "Hernia emergencies". Surg Clin North Am. 94(1). :97-130. (2014)
- Yang XF, Liu JL. "Acute incarcerated external abdominal hernia". Annals of translational medicine. 2(11). :110. (2014)
- East B, Pawlak M, de Beaux AC. "A manual reduction of hernia under analgesia/sedation (Taxis) in the acute inguinal hernia: a useful technique in COVID-19 times to reduce the need for emergency surgery-a literature review". Hernia. 24(5). :937-941. (2020)
- Ganti L. "Atlas of Emergency Medicine Procedures". Springer. (2016). ISBN: 9781493925063
- Birindelli A, Sartelli M, Di Saverio S, et al. "2017 update of the WSES guidelines for emergency repair of complicated abdominal wall hernias". World Journal of Emergency Surgery. 12(1). (2017)
- Wong PF, Gilliam AD, Kumar S, et al. "Antibiotic regimens for secondary peritonitis of gastrointestinal origin in adults". Cochrane Database of Systematic Reviews. (2005)
- Bittner R, Bain K, Bansal VK, et al. "Update of Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias (International Endohernia Society (IEHS))—Part A". Surg Endosc. 33(10). :3069-3139. (2019)
- Sanders DL, Kingsnorth AN. "The modern management of incisional hernias". BMJ. 344(e2843). (2012)
- Henriksen NA, Montgomery A, Kaufmann R, et al. "Guidelines for treatment of umbilical and epigastric hernias from the European Hernia Society and Americas Hernia Society". Br J Surg. 107(3). :171-190. (2020)
- Breuing K, Butler CE, Ferzoco S, et al. "Incisional ventral hernias: Review of the literature and recommendations regarding the grading and technique of repair". Surgery. 148(3). :544-558. (2010)
- Stabilini C, East B, Fortelny R, et al. "European Hernia Society (EHS) guidance for the management of adult patients with a hernia during the COVID-19 pandemic". Hernia. 24(5). :977-983. (2020)
- Allen M, Sevensma KE. "Rectus Sheath Hematoma". StatPearls. (2020)
- Alla VM, Karnam SM, Kaushik M, Porter J. "Spontaneous rectus sheath hematoma.". The western journal of emergency medicine. 11(1). :76-9. (2010)
- Eckhoff K, Wedel T, Both M, et al. "Spontaneous rectus sheath hematoma in pregnancy and a systematic anatomical workup of rectus sheath hematoma: a case report.". J Med Case Reports. 10(1). :292. (2016)
- Muysoms FE, Miserez M, Berrevoet F, et al. "Classification of primary and incisional abdominal wall hernias.". Hernia. 13(4). :407-14. (2009)
- Shankar DA, Itani KMF, O’Brien WJ, Sanchez VM. "Factors Associated With Long-term Outcomes of Umbilical Hernia Repair". JAMA Surgery. 152(5). :461. (2017)
- Salameh JR, Salloum EJ. "Lumbar incisional hernias: diagnostic and management dilemma.". Journal of the Society of Laparoendoscopic Surgeons. 8(4). :391-4
- Hanzalova I, Schäfer M, Demartines N, Clerc D. "Spigelian hernia: current approaches to surgical treatment—a review". Hernia. (2021)
- Webber V, Low C, Skipworth RJE, et al. "Contemporary thoughts on the management of Spigelian hernia". Hernia. 21(3). :355-361. (2017)
- Perry CP, Echeverri JD. "Hernias as a cause of chronic pelvic pain in women.". JSLS. 10(2). :212-5. (2006)
- Salameh JR. "Primary and Unusual Abdominal Wall Hernias". Surg Clin North Am. 88(1). :45-60. (2008)
- Sneiders D, Yurtkap Y, et al. "Risk Factors for Incarceration in Patients with Primary Abdominal Wall and Incisional Hernias: A Prospective Study in 4472 Patients". World J Surg. 43(8). :1906-1913. (2019)
- Judy C. Boughey, James M. Nottingham, Allan C. Walls. "Richter's Hernia in the Laparoscopic Era". Surg Laparosc Endosc Percutan Tech. 13(1). :55-58. (2003)
- Chen W, Liu L, Huang H, Jiang M, Zhang T. "A case report of spontaneous umbilical enterocutaneous fistula resulting from an incarcerated Richter’s hernia, with a brief literature review". BMC Surg. 17(1). (2017)
- Slater NJ, Montgomery A, Berrevoet F, et al. "Criteria for definition of a complex abdominal wall hernia". Hernia. 18(1). :7-17. (2013)
- Murphy KP, O’Connor OJ, Maher MM. "Adult Abdominal Hernias". American Journal of Roentgenology. 202(6). :W506-W511. (2014)
- Lassandro F, Iasiello F, Pizza NL, et al. "Abdominal hernias: Radiological features.". World journal of gastrointestinal endoscopy. 3(6). :110-7. (2011)
- Miller J, Cho J, Michael MJ, Saouaf R, Towfigh S. "Role of imaging in the diagnosis of occult hernias.". JAMA surgery. 149(10). :1077-80. (2014)
- Kanasaki S, Furukawa A, Fumoto K, et al. "Acute Mesenteric Ischemia: Multidetector CT Findings and Endovascular Management". RadioGraphics. 38(3). :945-961. (2018)
- Tanaka K, Hanyu N, Iida T, et al. "Lactate levels in the detection of preoperative bowel strangulation.". Am Surg. 78(1). :86-8. (2012)
- Schumpelick V, Fitzgibbons RJ, Conze J, et al. "Recurrent Hernia: Prevention and Treatment". Springer. (2007). ISBN: 9783540375456
- Snyder CL. "Current management of umbilical abnormalities and related anomalies". Semin Pediatr Surg. 16(1). :41-49. (2007)
- Brandt ML. "Pediatric Hernias". Surg Clin North Am. 88(1). :27-43. (2008)
- Bowling K, Hart N, Cox P, Srinivas G. "Management of paediatric hernia". BMJ. :j4484. (2017)
- Deerenberg EB, Timmermans L, Hogerzeil DP, et al. "A systematic review of the surgical treatment of large incisional hernia". Hernia. 19(1). :89-101. (2014)
- Patel SV, Paskar DD, Nelson RL, Vedula SS, Steele SR. "Closure methods for laparotomy incisions for preventing incisional hernias and other wound complications". Cochrane Database Systemat Rev. (2017)
- Dietz UA, Menzel S, Lock J, Wiegering A. "The Treatment of Incisional Hernia". Deutsches Aerzteblatt Online. (2018)
- Rogmark P, Petersson U, Bringman S, et al. "Quality of Life and Surgical Outcome 1 Year After Open and Laparoscopic Incisional Hernia Repair". Ann Surg. 263(2). :244-250. (2016)
- Kokotovic D, Sjølander H, Gögenur I, Helgstrand F. "Watchful waiting as a treatment strategy for patients with a ventral hernia appears to be safe". Hernia. 20(2). :281-287. (2016)
- Antoniou SA, Agresta F, Garcia Alamino JM, et al. "European Hernia Society guidelines on prevention and treatment of parastomal hernias". Hernia. 22(1). :183-198. (2017)