Summary
Abnormal labor and delivery occurs as a result of complications before and/or during birth. Prolonged stages of labor can lead to active-phase labor arrest, fetal malpresentation may cause mechanical obstruction of labor, abnormal rupture of membranes can increase the risk of chorioamnionitis and neonatal sepsis, and umbilical cord complications can increase the risk of birth asphyxia and stillbirth. Management of abnormal labor and delivery is typically tailored to the patient and can include induction of labor, prophylaxis for neonatal GBS infection, assisted vaginal delivery, special obstetrical maneuvers, intrauterine resuscitation, and/or emergency cesarean delivery.
See also “Normal labor and delivery,” “Preterm labor,” “Postpartum hemorrhage,” “Chorioamnionitis,” “Neonatal resuscitation,” and “Birth traumas.”
Abnormalities in fetal orientation
Fetal malpresentation and fetal malposition are associated with increased perinatal risks and may require assisted delivery or cesarean delivery to prevent maternal and fetal complications (see “Obstructed labor”).
Fetal malpresentation
- Definition: any fetal presentation or fetal lie that is not the cephalic presentation
-
Examples
-
Breech presentations
- Frank breech
- Complete breech
- Single footling breech
- Double footling breech
- Compound presentation
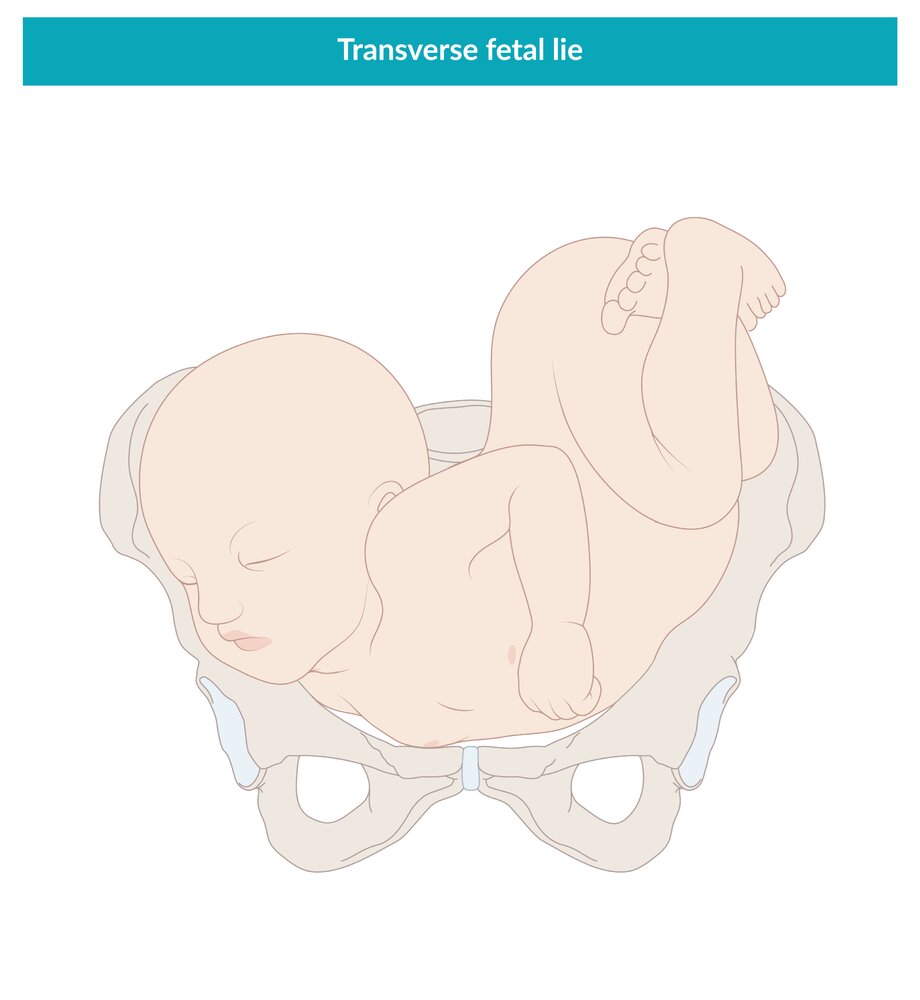
- Shoulder presentation
- Transverse lie
- Oblique lie
-
Breech presentations







Fetal malposition
- Definition: a fetal position in which the fetus is in the cephalic presentation but not oriented anteriorly
-
Examples
- Occiput posterior position
- Occiput transverse position


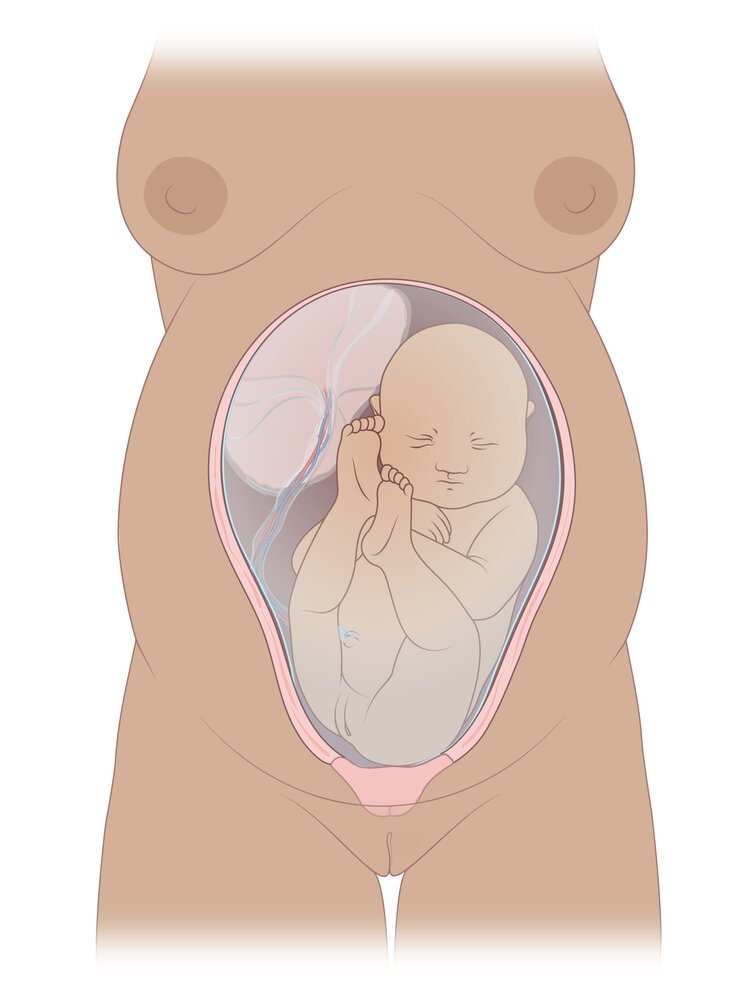
The fetus is shown in the breech presentation, in which the buttocks or feet lie closest to the cervix.
© AMBOSS
This malpresentation is characterized by flexed hips and extended knees. The buttocks of the baby are directed towards the birth canal.
© AMBOSS
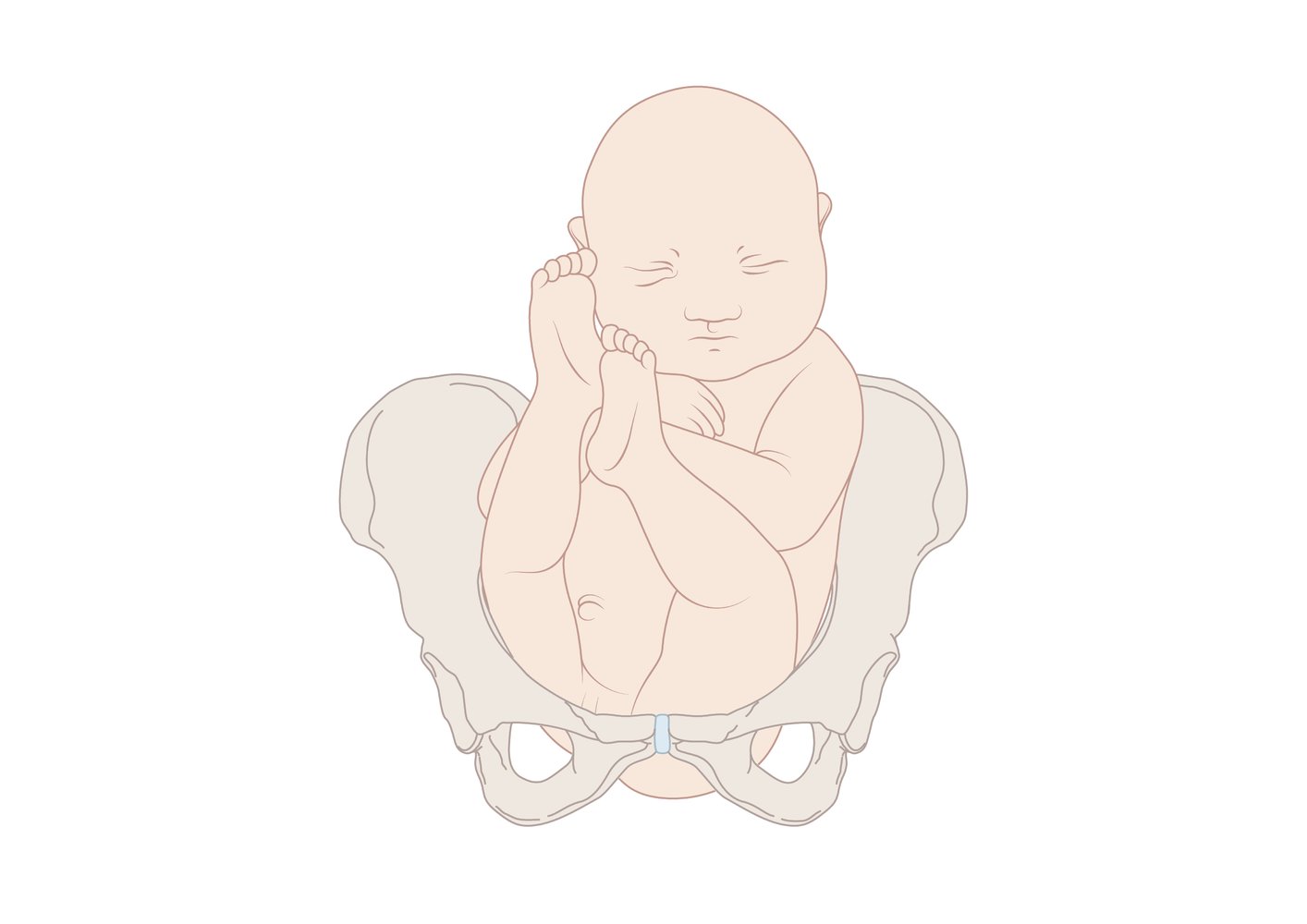
Both hips and knees are flexed with the feet close to the buttocks.
© AMBOSS

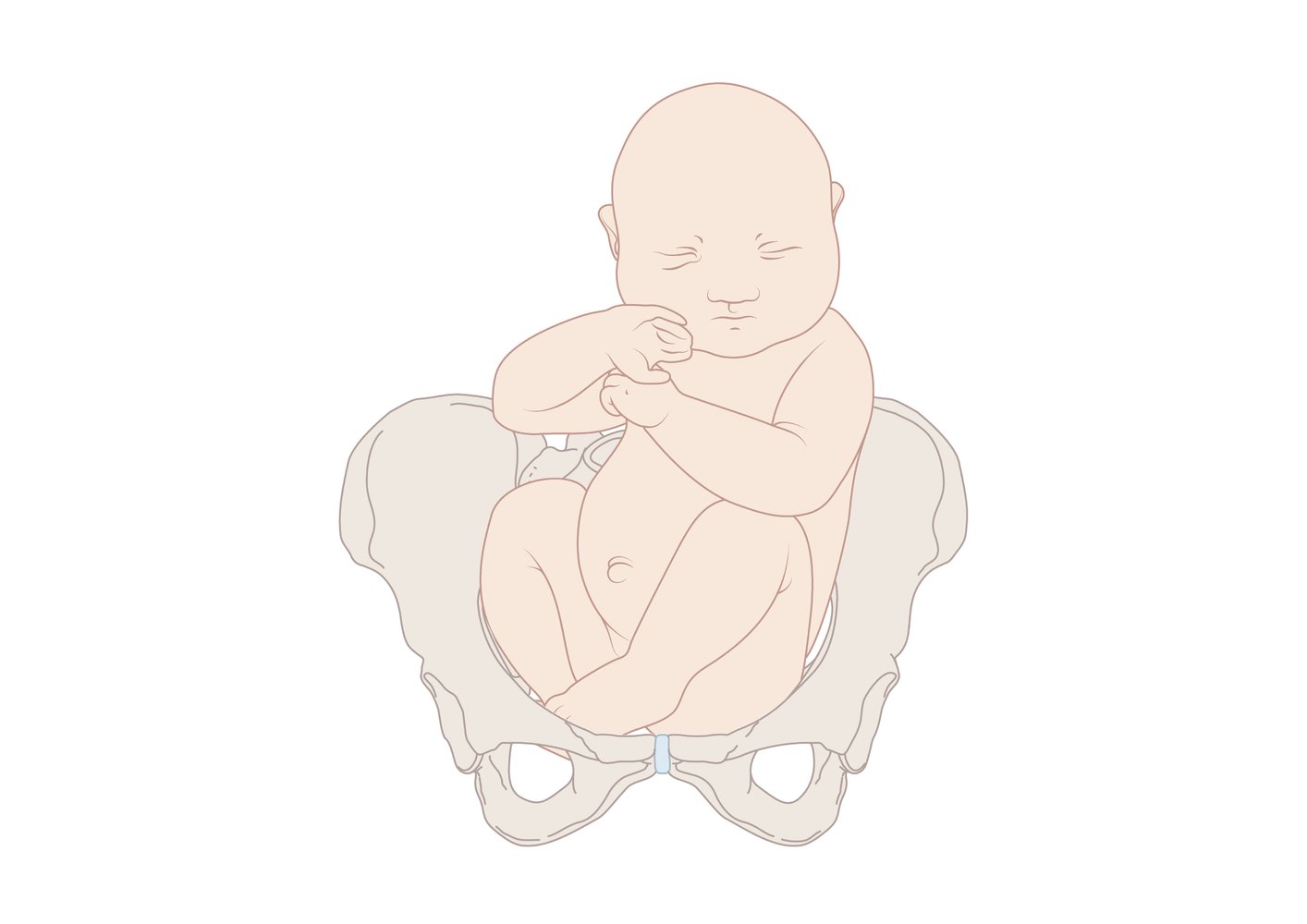
Variant of breech presentation: one foot/leg is stretched to be delivered first.
© AMBOSS

Variant of breech presentation: both feet/legs are stretched to be delivered first.
© AMBOSS
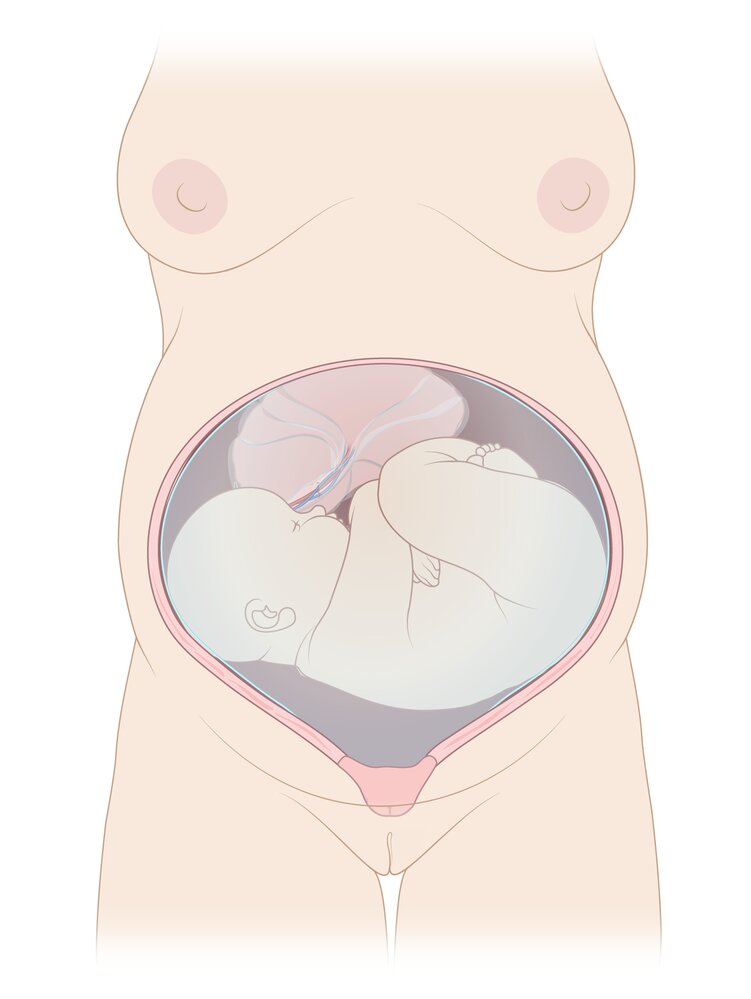
The fetus is shown in the transverse lie, a malpresentation in which the fetal long axis is perpendicular to the uterine long axis.
© AMBOSS
© AMBOSS
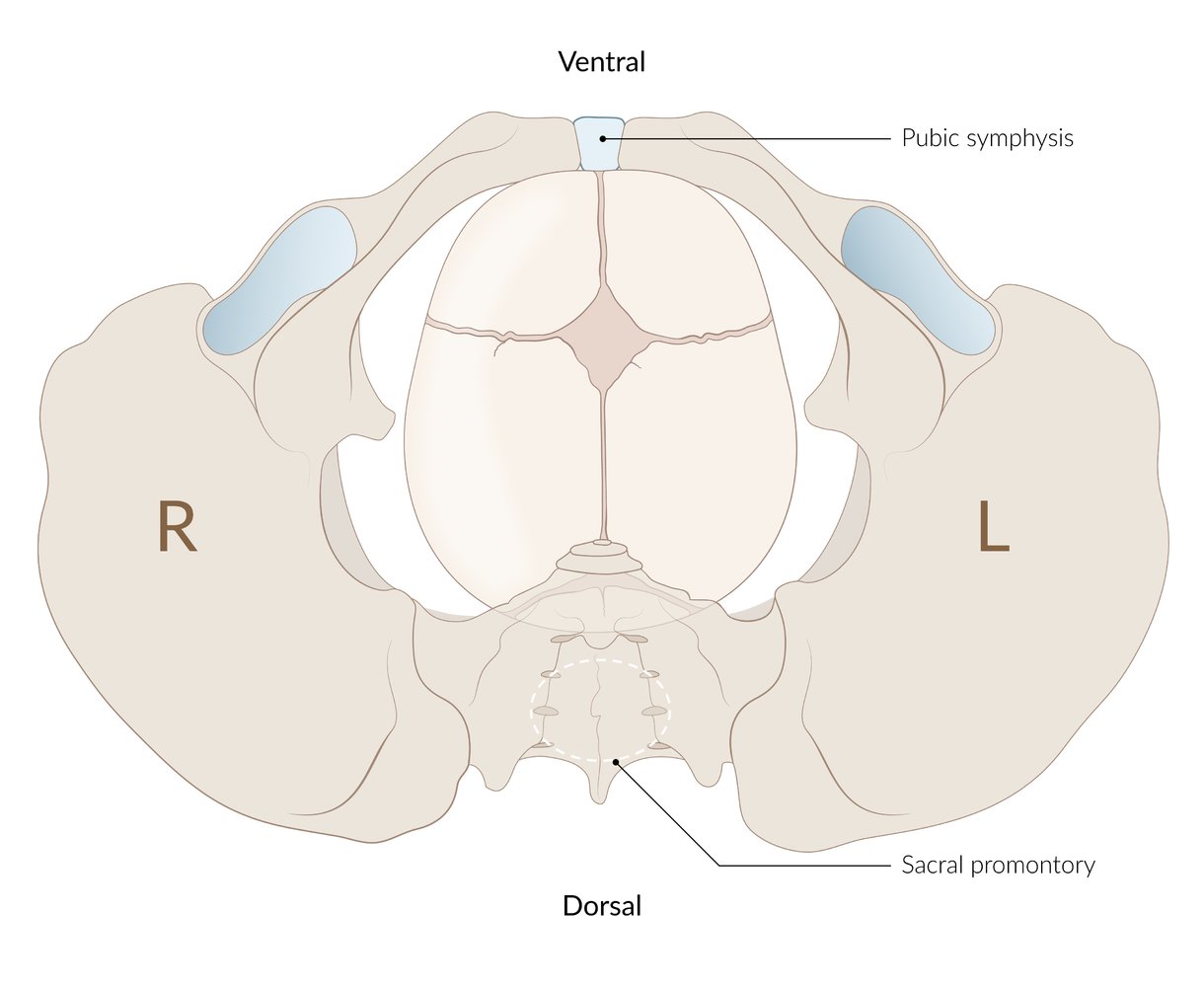
The occiput faces the promontory. From the obstetrician's perspective with the mother in the supine position, the child faces the ceiling during birth.
© AMBOSS
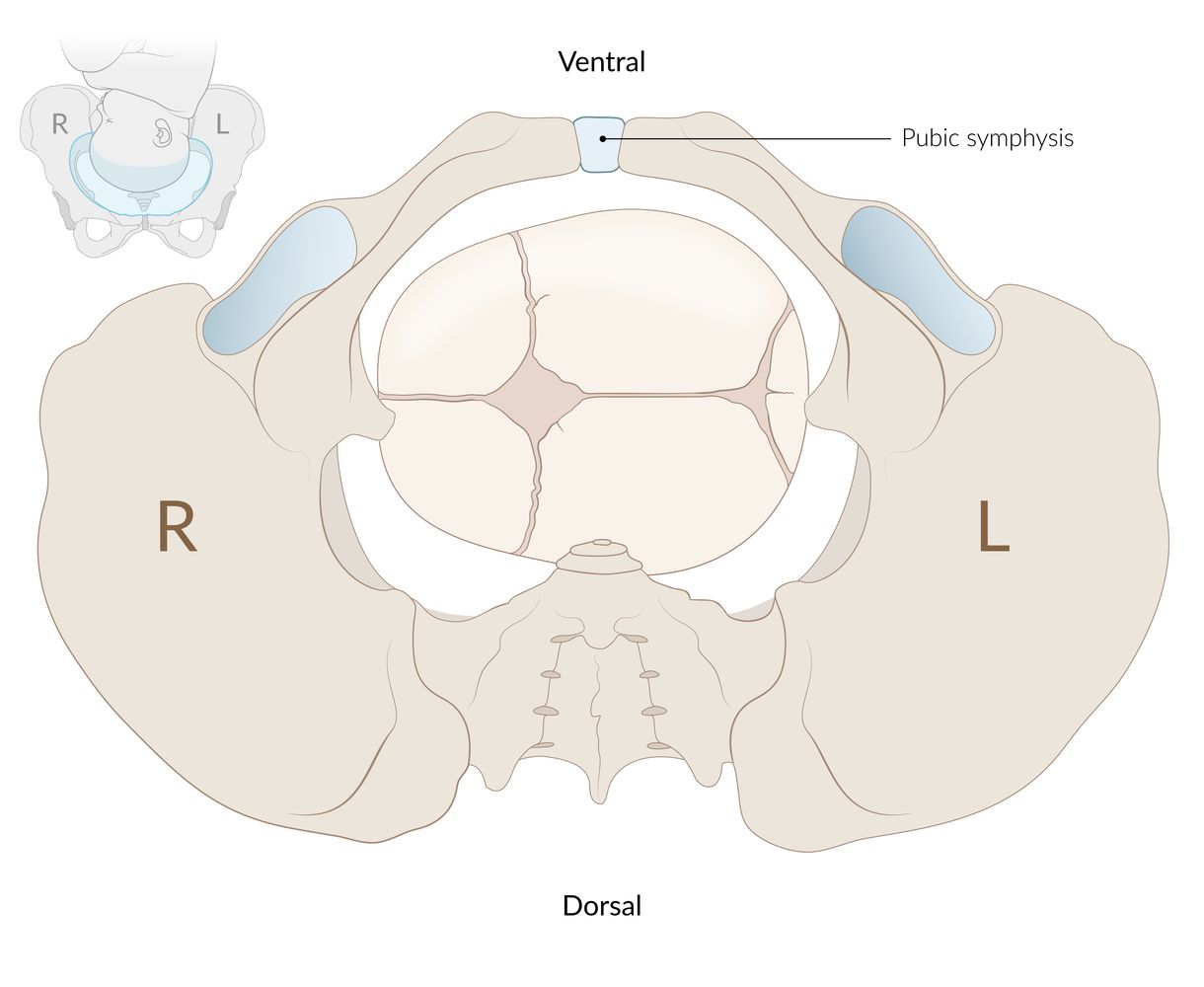
During normal vaginal births, the sagittal suture of the fetal head (arrow) lies transverse to the plane of the pelvic inlet, thus enabling passage through the plane.
© AMBOSS
Abnormal stages of labor
Definitions
- Prolonged (protracted) labor: abnormally slow progression of the labor process, typically marked by delayed cervical dilatation in the first stage or delayed descent or expulsive phase in the second stage (see "Overview of abnormal stages of labor") [1][2]
- Labor arrest: a complete halting of labor progression despite adequate augmentation of labor [1]
Risk factors for prolonged or arrested labor
-
First and second stages of labor [1]
- Induction of labor (latent phase only)
- Nulliparity
- Maternal obesity
- Advanced maternal age
-
Abnormalities of the 3 Ps of labor
- Pelvis: size and shape of the maternal pelvis (e.g., small bony pelvis)
- Passenger: size and position of the infant (e.g., fetal macrosomia or abnormal orientation)
- Power: strength and frequency of contractions (e.g., dysfunctional contractions )
- Cephalopelvic disproportion: The fetal head size is disproportionately large for the maternal pelvis.
- Second stage only
- Epidural anesthesia
- Delayed pushing [1][3]
-
Third stage of labor [4]
- Inadequate contractions
- Abnormal placental implantation
- Distortions of the uterine cavity (e.g., fibroids)
Types of abnormal labor stages
| Overview of abnormal stages of labor [1] | ||||
|---|---|---|---|---|
| Stage | Definition | Duration | ||
| Nulliparous patients | Multiparous patients | |||
| Prolonged first stage of labor | Prolonged latent phase of labor |
|
|
|
| Prolonged active phase of labor |
|
|||
| Arrested active phase |
|
|||
| Prolonged second stage of labor |
|
|
|
|
| Arrested second stage of labor |
|
|
||
| Prolonged third stage of labor [4] |
|
|||
Management of abnormal labor stages [1]
- Tailor management based on stage and whether labor is prolonged or arrested.
- Ensure adequate obstetric analgesia throughout.
- Consider nonpharmacological adjuvant supportive care.
- Continuous one-on-one support
- Hydration
- Ambulation and upright positioning
- Prepare for potential management failure (e.g., ensure staff are available for cesarean delivery).
First stage of labor
-
Prolonged first stage of labor [1]
- Start augmentation of labor, the process of stimulating uterine contractions with amniotomy and/or oxytocin infusion.
- Consider inserting an intrauterine catheter to monitor adequacy of contractions and titrate oxytocin as needed.
- Arrested active phase: : cesarean delivery [1][5]
Consider expectant management for prolonged latent stage of labor using shared decision-making. [1]
Second stage of labor
-
Prolonged stage [1][5]
- Address modifiable risk factors.
- Hypotonic uterine contractions: Start augmentation of labor or increase the rate of oxytocin infusion if already started.
- Fetal malpositioning: Consider manual rotation.
- For patients without an epidural, encourage upright positioning. [5]
- Consider delayed pushing.
- Address modifiable risk factors.
- Arrested stage: : assisted vaginal delivery or cesarean delivery [1]
Prolonged third stage of labor
- Continue active management of the third stage of labor. [4]
- If the placenta is incomplete or an accessory placenta is suspected: [6]
- Manually palpate the uterine cavity.
- Remove remaining tissue with manual extraction or suction curettage. [4]
- See "Retained placenta" for details.
Complications
-
Maternal [1]
- Infection (e.g., chorioamnionitis, endometritis) ; [4]
- Need for assisted vaginal delivery or cesarean delivery
- Postpartum hemorrhage [4]
- Perineal lacerations
-
Neonatal [1]
- Perinatal asphyxia and hypoxic-ischemic encephalopathy
- Sepsis
- Seizures
- Birth traumas
- Death
Prevention [1][5]
- Avoid admission for low-risk patients during latent labor. [5]
- Encourage continuous labor support.
- Prior to induction of labor, use cervical ripening agents if the cervix appears unfavorable.
Mechanical obstruction of labor
Definition [7]
- The arrest of vaginal delivery as a result of a mechanical obstruction
Risk factors
- Fetal macrosomia (may be physiological or pathological, e.g., due to hydrocephalus)
- Fetal malpresentation or malposition
- Uterine abnormalities, e.g., a tumor (e.g., uterine leiomyoma), deformities of the maternal pelvis, bicornuate uterus, multiparity
- Placenta previa
- Short umbilical cord
- Oligohydramnios, polyhydramnios
Clinical features [8][9]
Maternal
- Exhaustion
- Frequent uterine contractions
- Edematous vulva
- Bandl ring
Fetal
- High presenting part that is not engaged with the pelvis
- Rupture of membranes
- Significant head molding
- Caput succedaneum
- Fetal distress
Prelabor management
Patients with an increased risk for mechanical obstruction of labor should create a birth plan with their obstetrician, possibly including a scheduled cesarean delivery.
-
Breech presentation [10]
- < 37 weeks: no intervention necessary, as most fetuses spontaneously convert to a cephalic presentation as they get closer to term [11]
- ≥ 37 weeks: Consider external cephalic version.
- A planned cesarean delivery may be necessary if external cephalic version is not performed, unsuccessful, or contraindicated.
- Manually assisted vaginal delivery may be considered for low-risk pregnancies if the patient wants to avoid surgery.
-
Transverse lie
- < 37 weeks: no intervention necessary, as the majority of fetuses spontaneously convert to a cephalic or breech presentation before labor [12]
- ≥ 37 weeks: Consider external cephalic version. [13]
Primary cesarean delivery may be chosen for patients at high risk of mechanical obstruction of labor (e.g., due to congenital fetal anomalies or maternal risk factors). [14]
External cephalic version [13]
- Indication: noncephalic fetal lie (e.g., breech presentation, transverse lie) after 37 weeks' gestation
-
Contraindications [13][15]
- Indications for cesarean delivery
- Placental abruption
- Nonreassuring fetal status
- Active labor or ruptured membranes
- Oligohydramnios
- Procedure: manual adjustment of fetal position by applying pressure on the gravid abdomen to achieve a vertex presentation
Active labor management [16]
Approach
- Immediately consult obstetrics, neonatology, and anesthesia if mechanical obstruction of labor is suspected.
- Perform intrapartum transabdominal ultrasound to determine fetal presentation; , if possible.
- Initiate cardiotocography.
- Perform emergency preoperative evaluation.
- Pursue definitive fetal presentation-based management.
Transabdominal ultrasound is more accurate than digital cervical examination for determining fetal head position. [17]
Fetal presentation-based management
-
Compound presentation [16][18]
- Most patients: expectant management
- Arrested labor or umbilical cord prolapse: cesarean delivery
-
Persistent occiput posterior position [19]
- Most patients: expectant management or consider manual rotation to the occipital anterior position
- Arrested labor: cesarean delivery
- Shoulder dystocia: See “Shoulder dystocia.”
- Transverse lie: : cesarean delivery
-
Breech presentation [16][20]
- Proceed with emergency vaginal delivery if birth appears imminent.
- Allow delivery up to the umbilicus using maternal effort.
- If the legs do not deliver, flex the fetal knees and sweep the legs out.
- Allow delivery up to the scapula using maternal effort.
- If the arms do not deliver, rotate the fetus to deliver the shoulder under the pubic symphysis, then rotate the fetus to deliver the other shoulder.
- Perform the Mauriceau maneuver to deliver the head.
Complications [8][21]
Fetal
- Birth asphyxia
- Infection (intrauterine and neonatal)
- Intracranial hemorrhage
- Birth injuries
- Perinatal death
Maternal
- Vesicovaginal fistula and ureterovaginal fistula
- Uterine rupture
- Infection (e.g., postpartum sepsis)
- Postpartum hemorrhage
- Stress urinary incontinence
Shoulder dystocia
Definition [22]
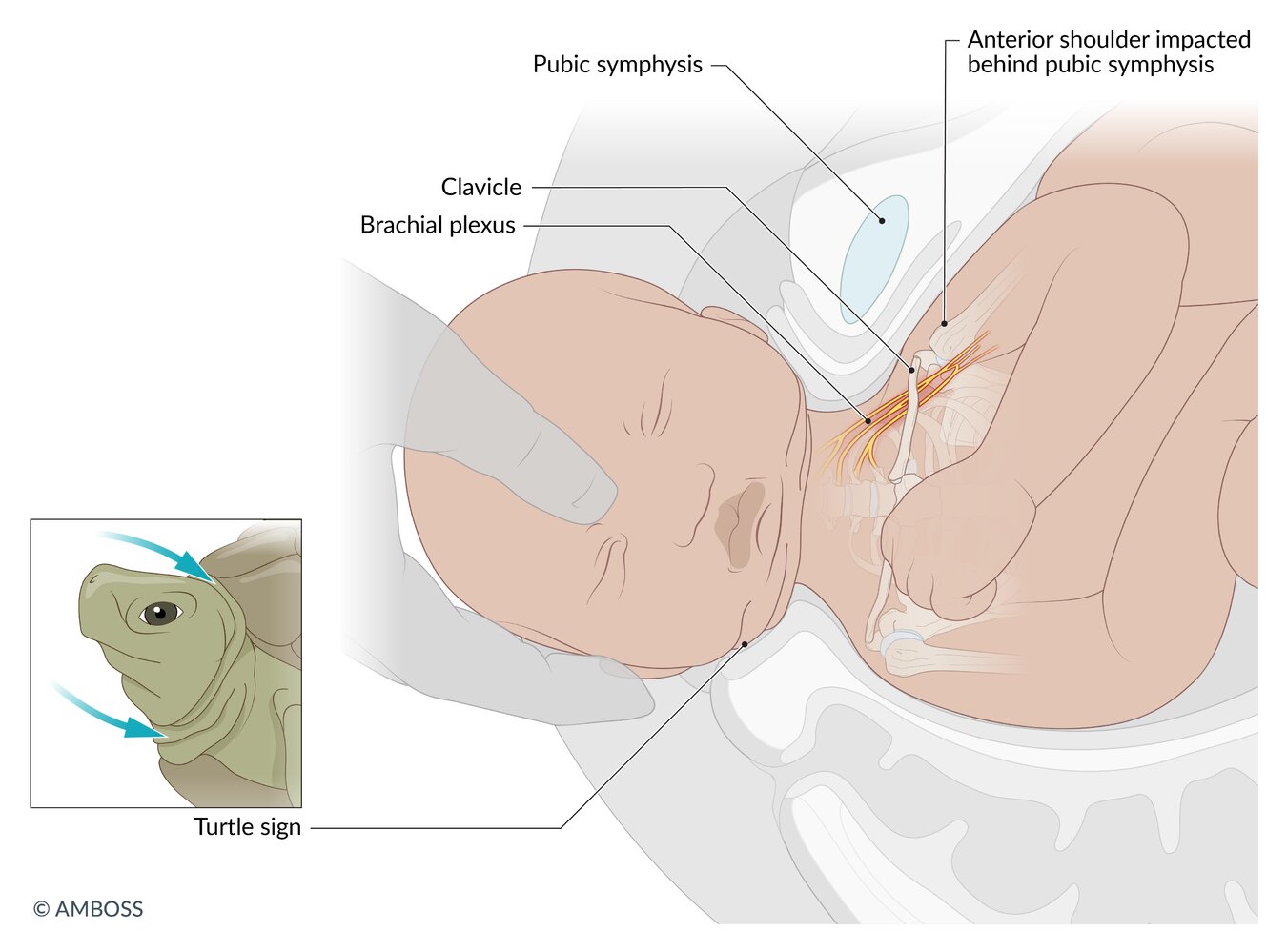
- An obstetric emergency in which the anterior shoulder of the fetus becomes impacted behind the maternal pubic symphysis during vaginal delivery, or, less commonly, the posterior shoulder becomes impacted against the sacral promontory
Epidemiology
- ∼ 0.2–3% of vaginal deliveries with vertex presentation [22]
Risk factors [22]
- History of shoulder dystocia
- Fetal macrosomia
- Maternal diabetes mellitus or gestational diabetes
- Maternal obesity
- Prolonged second stage of labor
Always be prepared for shoulder dystocia, as it can occur even in the absence of risk factors. [22]
Clinical features
- Inability to deliver either shoulder with gentle downward traction on the fetal head
- Turtle sign: retraction of the partially delivered fetal head against the perineum
- Failed restitution of the fetal head

Management
For general management of vaginal delivery, see “Manually assisted vaginal delivery.”
Approach [16][22][23]
-
Establish the presence of shoulder dystocia (clinical diagnosis).
- Declare the presence of shoulder dystocia.
- Call for obstetrics, neonatology, anesthesia, and additional nursing staff.
- Inform the mother and instruct them not to push.
- Consider insertion of a Foley catheter to decompress the bladder.
- Perform initial shoulder dystocia maneuvers, starting with the McRoberts maneuver. [23]
- Proceed to secondary shoulder dystocia maneuvers if initial maneuvers are unsuccessful.
- If the infant has still not been delivered, consider maneuvers of last resort (e.g., intentional clavicular fracture).
Shoulder dystocia maneuvers [16][20][24]
-
Initial maneuvers
-
McRoberts maneuver
- The patient should stop bearing down and lie supine with the buttocks on the edge of the bed.
- Abduct, externally rotate, and hyperflex the maternal hips (with the maternal legs pulled towards the head).
- McRoberts maneuver with suprapubic pressure (Rubin I maneuver) [22]
- Manual delivery of the posterior fetal arm
-
McRoberts maneuver
-
Secondary maneuvers
- Rubin II maneuver: Manually rotate the fetal shoulder girdle by applying pressure to the posterior part of the anterior shoulder.
- Woods corkscrew maneuver: Manually rotate the fetal shoulder girdle by applying pressure to the anterior part of the posterior shoulder.
-
Gaskin maneuver (all fours positions)
- The patient moves into hands and knees position.
- Rubin and Woods maneuvers can be repeated.
-
Maneuvers of last resort
- Intentional clavicular fracture: Fracture the clavicle by pulling the midportion of the clavicle upward or outward.
- Zavanelli maneuver: The fetal head is pushed back into the pelvis to alleviate pressure on the umbilical cord while the patient is transported to the OR for cesarean delivery.
- Symphysiotomy: surgical separation of the anterior fibers of the symphyseal ligament, only performed if all other maneuvers are unsuccessful and cesarean delivery is not available
Internal maneuvers (i.e., maneuvers requiring direct manipulation of fetal parts) may require episiotomy and can be performed together with the McRoberts maneuver. [24]
Avoid excessive downward or lateral traction on the fetal head and neck, as this can result in brachial plexus injuries. [23]

 in shoulder dystocia")

Complications [23]
- Fetal
- Brachial plexus injury (Erb palsy is more common than Klumpke palsy) [25]
- Clavicle or humerus fracture
- Perinatal asphyxia and hypoxic-ischemic encephalopathy
- Maternal
- Perineal lacerations
- Postpartum hemorrhage
© AMBOSS
© AMBOSS
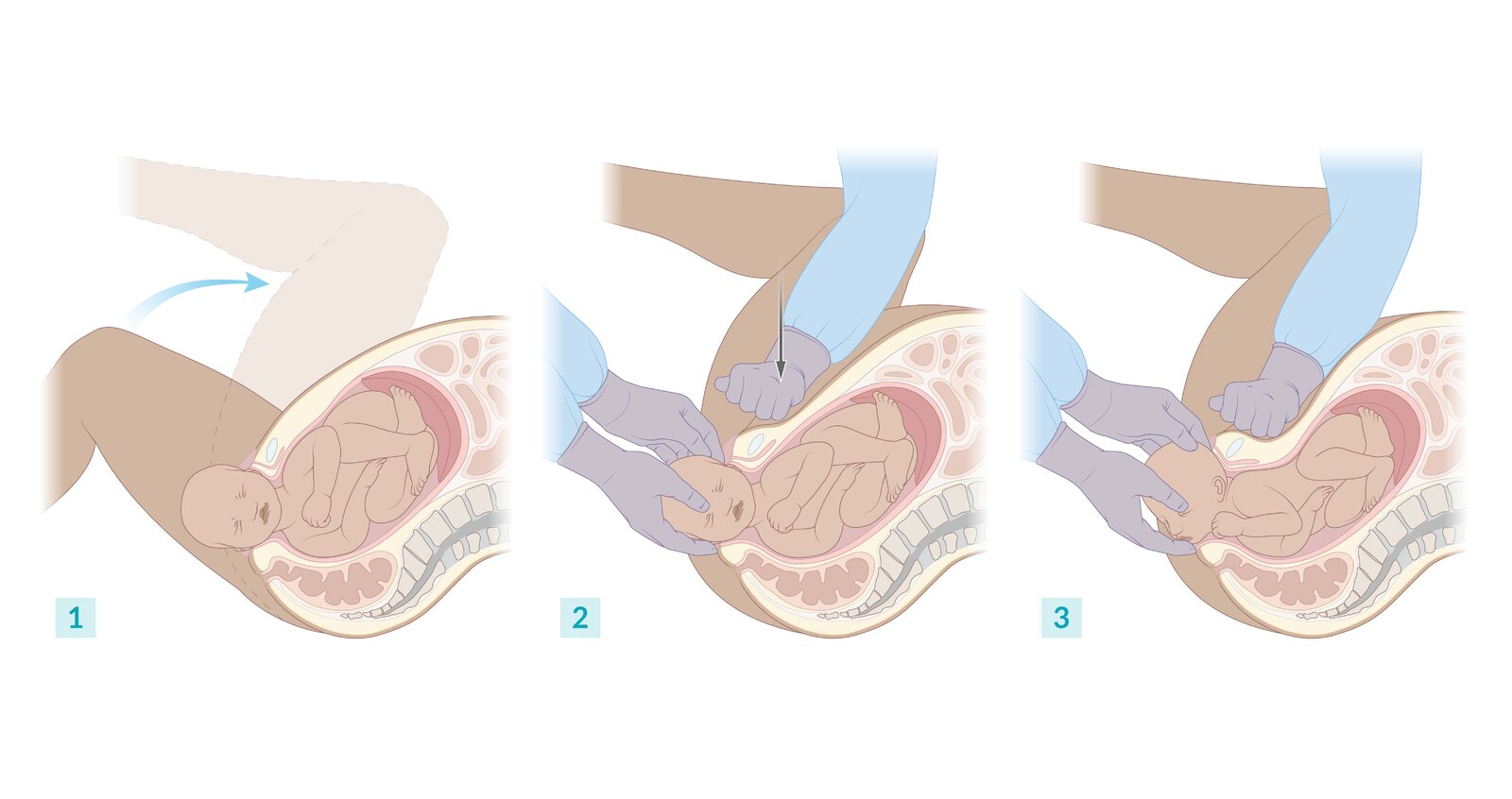
1. The fetal head is partially delivered but has retracted against the perineum (Turtle sign). Both maternal hips are abducted, externally rotated, and maximally flexed (McRoberts maneuver).
2. Suprapubic pressure is applied to the impacted anterior shoulder (Rubin I maneuver).
3. The anterior shoulder passes under the pubic symphysis, and delivery can be completed.
© AMBOSS

© AMBOSS
Abnormal rupture of membranes
Definitions [26]
- Prelabor rupture of membranes (PROM): rupture of membranes before the onset of labor at ≥ 37 weeks' gestation
- Preterm prelabor rupture of membranes (PPROM): rupture of membranes before the onset of labor and before 37 weeks' gestation
- Prolonged rupture of membranes: rupture of membranes > 18 hours before the onset of labor [27]
Epidemiology [26]
The following values pertain to patients in the US:
- PROM: ∼ 8% of pregnancies
- PPROM: ∼ 2–3% of pregnancies
Risk factors for PPROM [26][28]
Risk factors for PPROM are similar to risk factors for preterm labor, e.g.:
- History of PPROM
- Short cervical length
- Antepartum bleeding
- History of sexually transmitted infections
- Prior prenatal procedures (e.g., cervical cerclage, amniocentesis)
- Low BMI
- Low socioeconomic status
- Cigarette smoking
- Substance use disorder
Diagnostics for abnormal rupture of membranes [26]
- Clinical diagnosis: a sudden gush of pale yellow or clear fluid from the vagina
-
Sterile speculum examination
- Fluid exiting the cervix and pooling in the vaginal fornix suggests rupture of membranes.
-
Detection of amniotic fluid
- Litmus test or nitrazine test: Test strips turn blue, as amniotic fluid is alkaline.
- Positive fern test: fern pattern on glass slide
- Ultrasound: Oligohydramnios may be present.
Do not perform a digital cervical examination unless the patient is in active labor because it increases the risk of infection and has minimal diagnostic utility. [26]
Management [26][28]
Initial management
- Consult OB/GYN to determine appropriate management.
- Determine gestational age and fetal presentation, and perform a fetal status assessment.
- Establish if intrapartum prophylactic antibiotics for GBS are required.
-
Evaluate for indications for urgent delivery, e.g.:
- Fetal distress
- Intrauterine infection (e.g., chorioamnionitis)
- Placental abruption
- If necessary, initiate transfer to a hospital that can provide maternal and neonatal care.
Management by gestational age
-
≥ 37 0/7 weeks' gestation [29]
- Initiate induction of labor with manually assisted vaginal delivery.
- Consider expectant management for up to 12–24 hours for patients with reassuring maternal and fetal status and without GBS infection. [26]
-
34 0/7 to 36 6/7 weeks' gestation
- Consider expectant management or induction of labor on a case-by-case basis. [26]
- Consider steroids for induction of fetal lung maturity.
-
24 0/7 to 33 6/7 weeks' gestation
- Initiate expectant management.
- Administer steroids for induction of fetal lung maturity.
- Administer PPROM antibiotic prophylaxis.
- Consider up to 48 hours of tocolysis to inhibit uterine contractions in consultation with OB/GYN.
- Consider magnesium sulfate for fetal neuroprotection if delivery at < 32 weeks' gestation is anticipated. [30]
-
< 24 weeks' gestation
- Discuss the risks and benefits of expectant management vs. terminating the pregnancy, including predicted neonatal outcomes.
- Consider maternal-fetal medicine and neonatology consultation for patients who choose expectant management.
- Consider PPROM antibiotic prophylaxis.
- GBS prophylaxis, corticosteroids, tocolysis, and magnesium sulfate are not recommended before 24 weeks' gestation.
PPROM antibiotic prophylaxis
-
Goals
- Prolong pregnancy (reduce the risk of gestational age-dependent morbidity)
- Reduce the risk of maternal and neonatal infections
- Indication: PPROM at 20 0/7 to 33 6/7 weeks' gestation [26]
-
Treatment
- Initial 48 hours: ampicillin (off-label) PLUS erythromycin IV (off-label) [26]
- Subsequent 5 days: amoxicillin (off-label) PLUS erythromycin PO (off-label) [26]
- Alternative: A single dose of azithromycin (off-label) may replace the 7-day course of erythromycin.
Complications [26][28]
- PROM: intrauterine infection (risk increases with duration of ruptured membranes)
-
PPROM
- Fetal
- Complications of prematurity (e.g., neonatal respiratory distress, necrotizing enterocolitis)
- Umbilical cord compression
- Antepartum death
- Maternal
- Chorioamnionitis
- Placental abruption
- Fetal
Umbilical cord complications
Umbilical cord presentation [31]
- Definition: the presentation of the umbilical cord at the internal cervical os before the fetal presenting part
- Epidemiology: incidence ∼ 0.6% [31]
- Clinical features: typically absent; soft pulsatile mass may be palpable on pelvic examination
- Diagnostics: obstetric ultrasound
-
Management
- Before labor: close obstetrician follow-up with labor and delivery planning (e.g., attempted vaginal delivery, scheduled cesarean delivery)
- During labor: Prepare for umbilical cord prolapse.

Umbilical cord prolapse [16][31]
Definitions
- Overt umbilical cord prolapse: the descent of the umbilical cord into the cervical canal or vagina before the fetal presenting part after rupture of membranes
- Occult umbilical cord prolapse: the descent of the umbilical cord into the cervical canal or vagina alongside the fetal presenting part after rupture of membranes

Epidemiology
- Incidence 0.1–0.4% [16]
- Estimated perinatal mortality ∼ 10% [16]
Etiology
- Spontaneous rupture of membranes
- Iatrogenic (e.g., artificial rupture of membranes, insertion of transcervical balloon catheters)
-
Risk factors include:
-
Fetal risk factors, e.g.:
- Malpresentation (e.g., breech presentation, transverse lie)
- Prematurity
- Fetal weight < 2500 g
- Long umbilical cord
-
Maternal risk factors, e.g.:
- Grand multiparity
- Uterine abnormalities
-
Fetal risk factors, e.g.:
Diagnostics
- Pelvic examination: : visible or palpable umbilical cord
- Fetal heart rate: : prolonged fetal bradycardia or repetitive moderate to severe variable decelerations
Management
- Immediately consult obstetrics, anesthesia, and neonatology to prepare for emergency delivery.
- Initiate cardiotocography to monitor fetal heart rate and the effectiveness of interventions.
-
Relieve umbilical cord compression and maintain interventions until delivery, i.e.:
- Manually elevate the fetal presenting part.
- Position the patient in the Trendelenburg position and/or knee-chest position.
- Consider filling the bladder with 500–750 mL of saline. [32]
- Consider manual reduction of the prolapsed cord and rapid vaginal delivery if immediate cesarean delivery is not possible.
Minimize manipulation of the prolapsed cord, as this can cause vasospasm and fetal hypoxia.
Nuchal cord [16][33]
- Definition: the wrapping of the umbilical cord 360 degrees around the fetal neck
- Etiology: most often caused by fetal movement
-
Epidemiology [34]
- Single cord loop around the neck: ∼ 16% of births
- Multiple cord loops around the neck: ∼ 4% of births
-
Diagnosis
- Before labor: may be seen on ultrasound
- During labor: clinical diagnosis
-
Management
- Before labor: close obstetrician follow-up with labor and delivery planning (e.g., attempted vaginal delivery, scheduled cesarean delivery)
- During labor
- Reduce by slipping loose nuchal cords over the head at the maternal perineum.
- If unable to reduce, double clamp and cut the cord, then proceed with rapid manually assisted vaginal delivery.

Knotting of the umbilical cord
- Etiology: most often caused by fetal movement
- Epidemiology: ∼ 1% of births [35]
-
Management
- Before labor: close obstetrician follow-up with labor and delivery planning (e.g., attempted vaginal delivery, scheduled cesarean delivery) [36]
- During labor: Proceed with manually assisted vaginal delivery; avoid cord traction. [16]


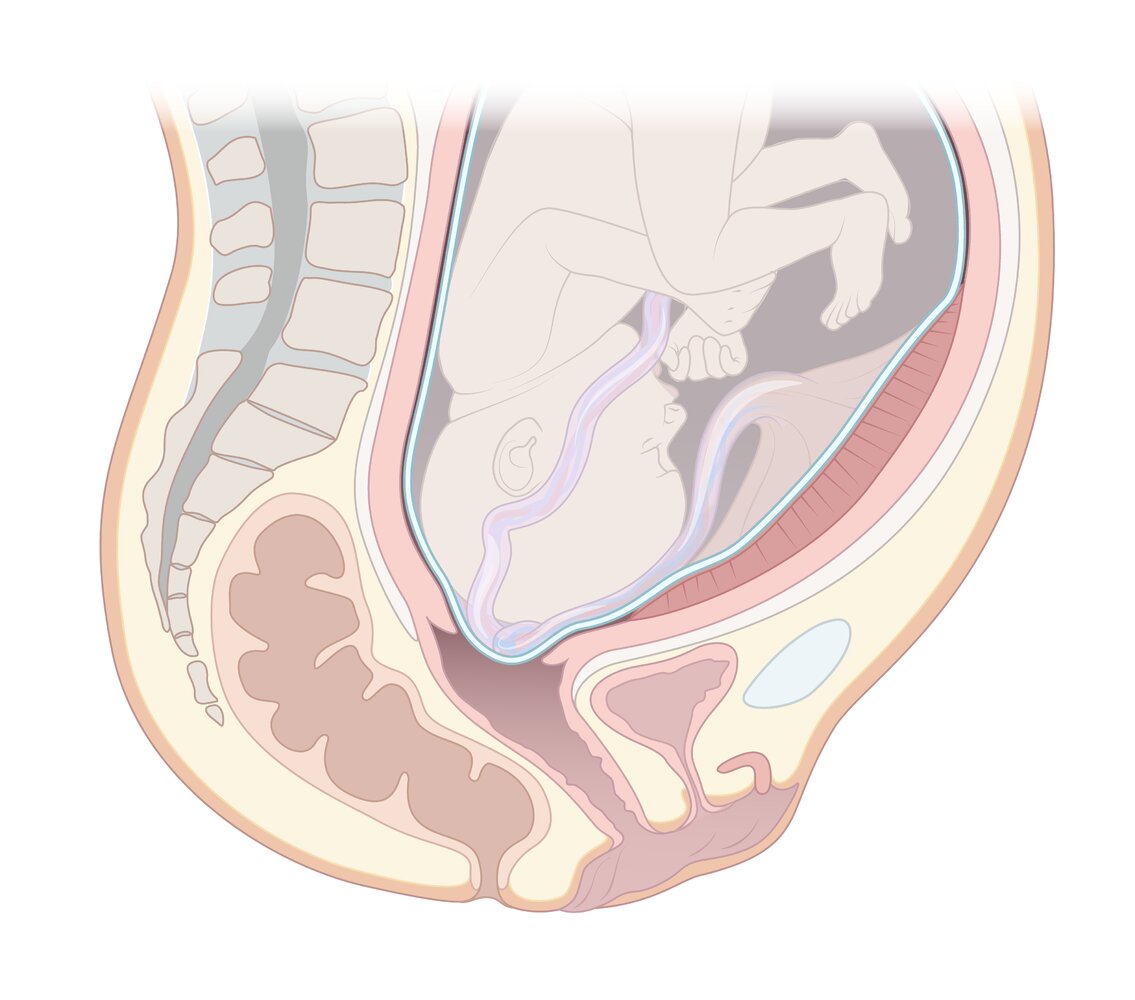
The umbilical cord lies between the fetal presenting part and the pelvic wall with the membranes intact. Cord compression and restriction of blood flow to the fetus may occur. Placing the mother in a different position (e.g., Trendelenburg) may result in spontaneous reduction of the cord into the uterus.
© AMBOSS
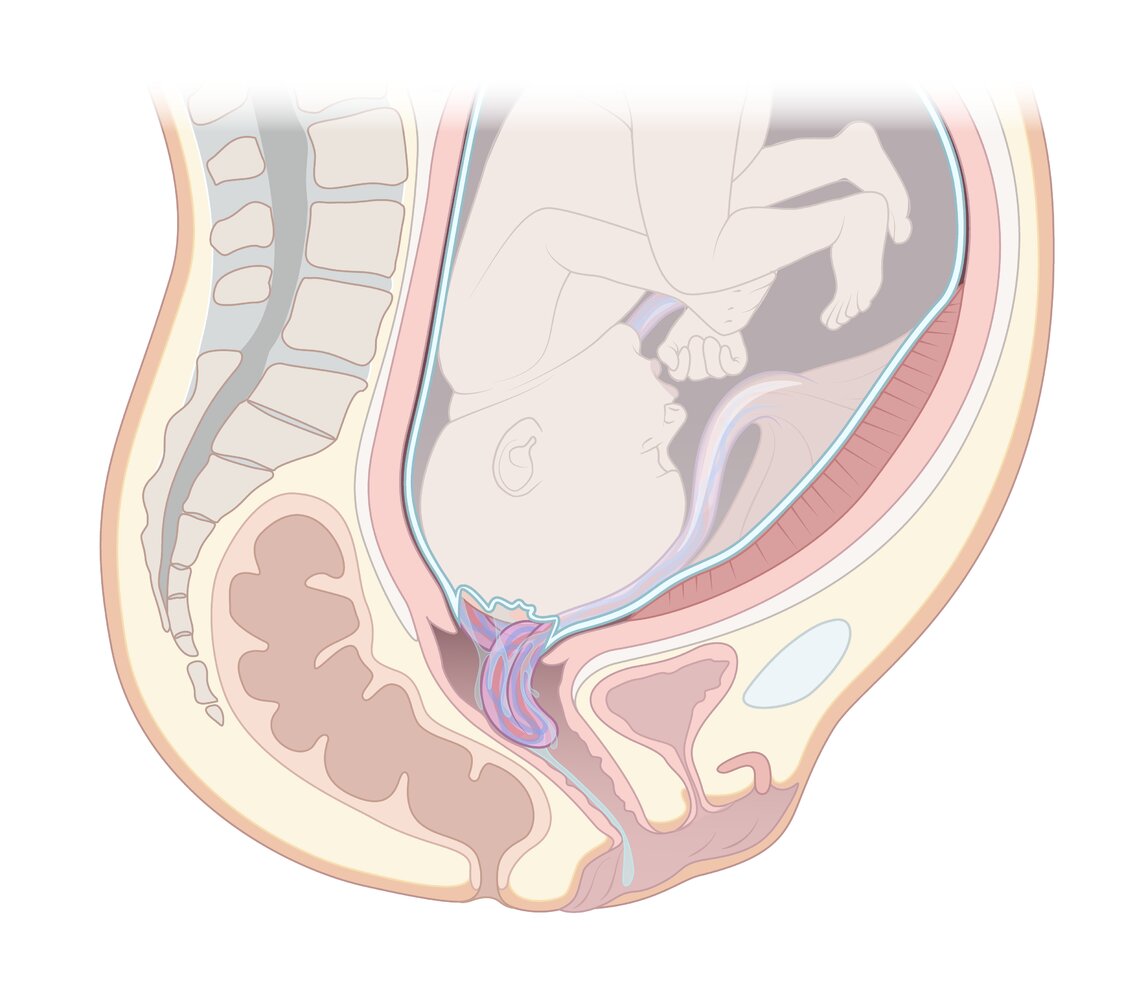
The umbilical cord lies between the presenting part of the fetus and the maternal pelvic wall. The membranes are ruptured, and the cord prolapses into the cervical canal or further. There is a high risk of cord compression and life-threatening hypoxia for the fetus. Management includes intrauterine resuscitation measures and emergency cesarean delivery.
© AMBOSS
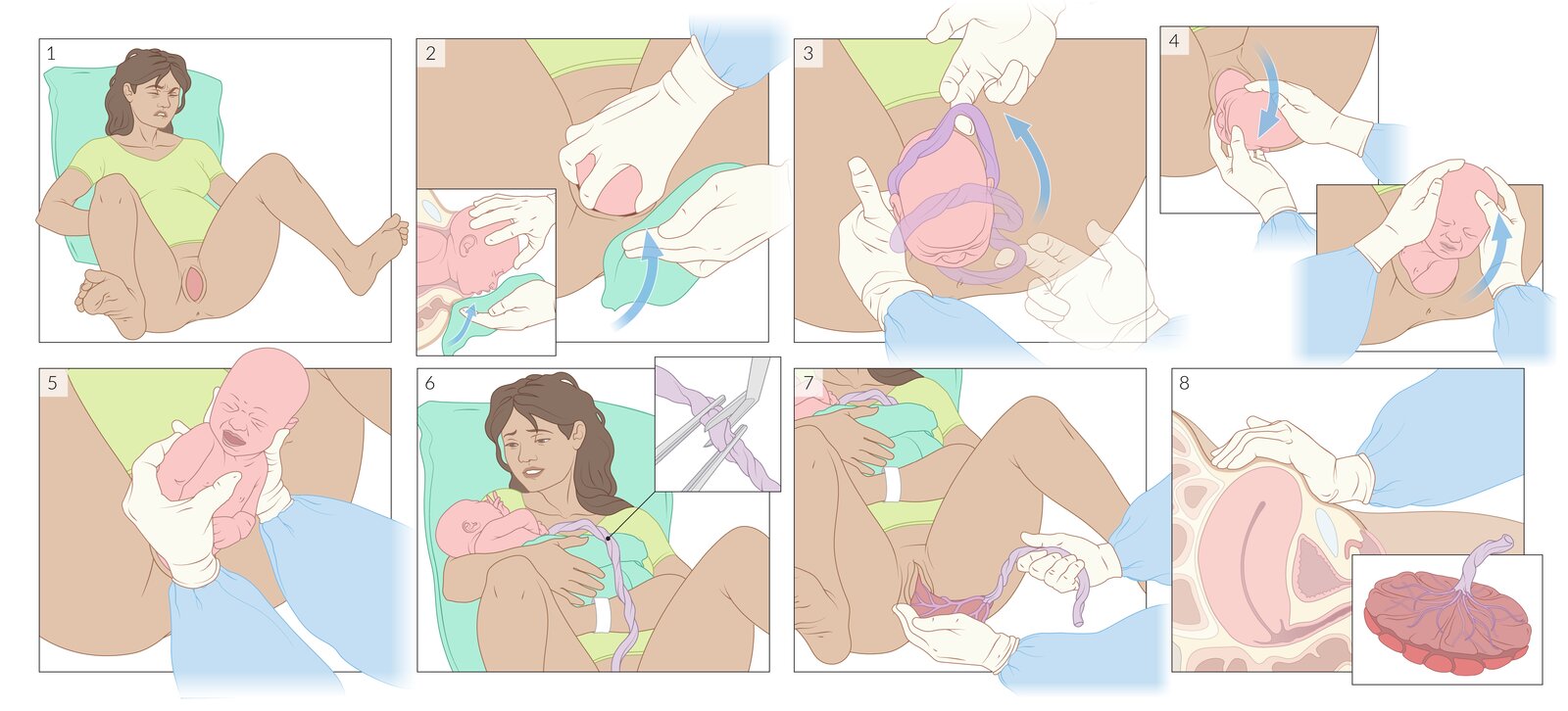
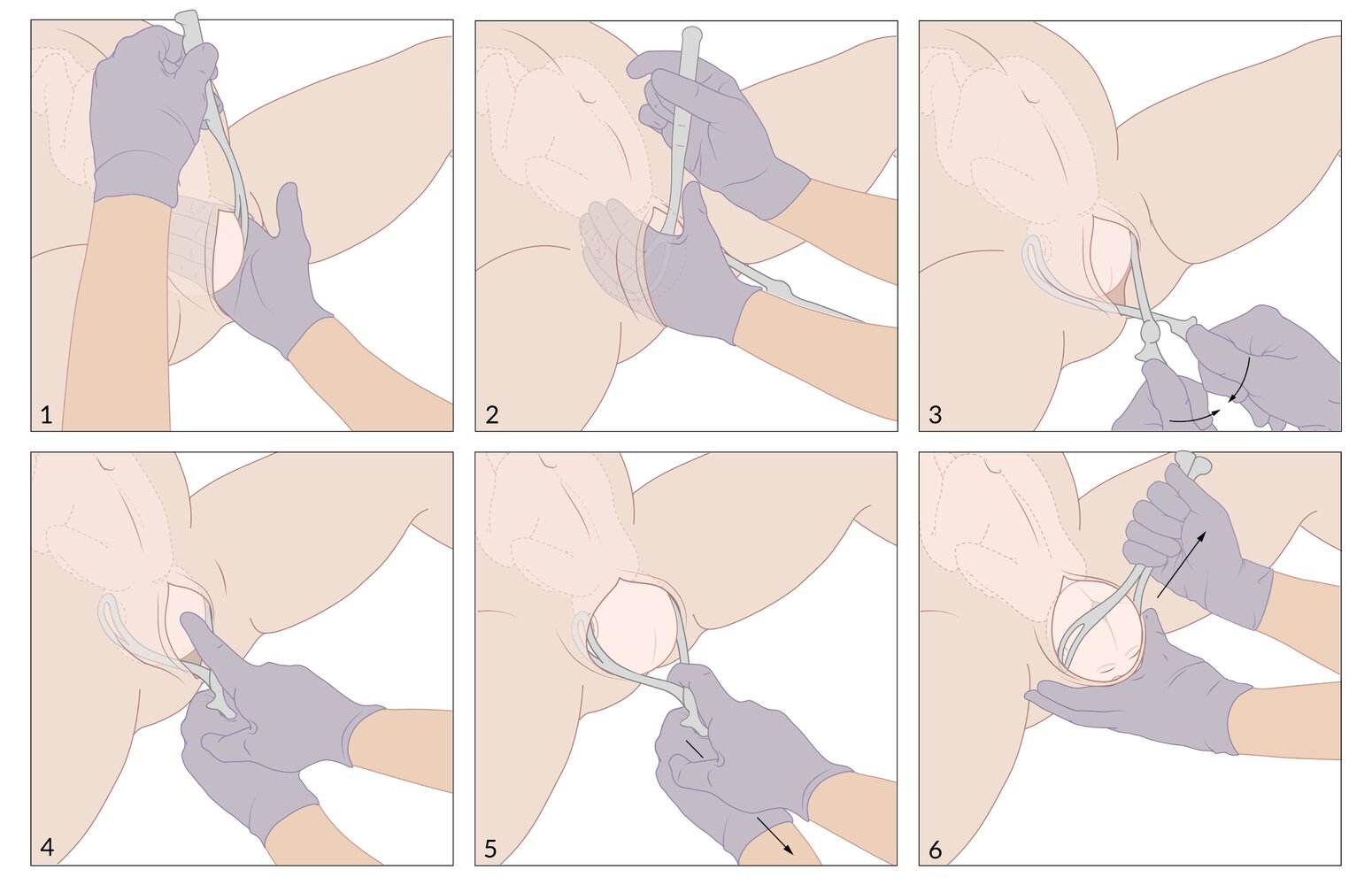
1. Once crowning occurs, the mother is helped into a comfortable position and the vulvar and perineal area are cleansed (not shown).
2. Gentle pressure on the fetal head is applied with one hand to control the rate of expulsion. The fetal chin is lifted with the other hand by applying upward pressure through the perineum.
3. If a nuchal cord is present, it is gently slipped over the fetal head.
4. Gentle downward traction is applied on the fetal head until the anterior shoulder is free, then gentle upward traction until the posterior shoulder is free.
5. The fetal body is supported with both hands and a gentle longitudinal traction is applied if necessary. The fingers should not be placed in the fetal axillae.
6. The infant is placed on the mother's abdomen and gently dried with a towel. After waiting at least 30–60 seconds, the umbilical cord is cut between two Kelly clamps placed 6–8 cm from the abdominal insertion.
7. Once signs of uterine separation have occurred, the mother is asked to bear down to expel the placenta.
8. In the immediate postpartum period, uterine tone should be assessed regularly. The placenta, membranes, and umbilical cord should be evaluated for completeness and anomalies.
© AMBOSS
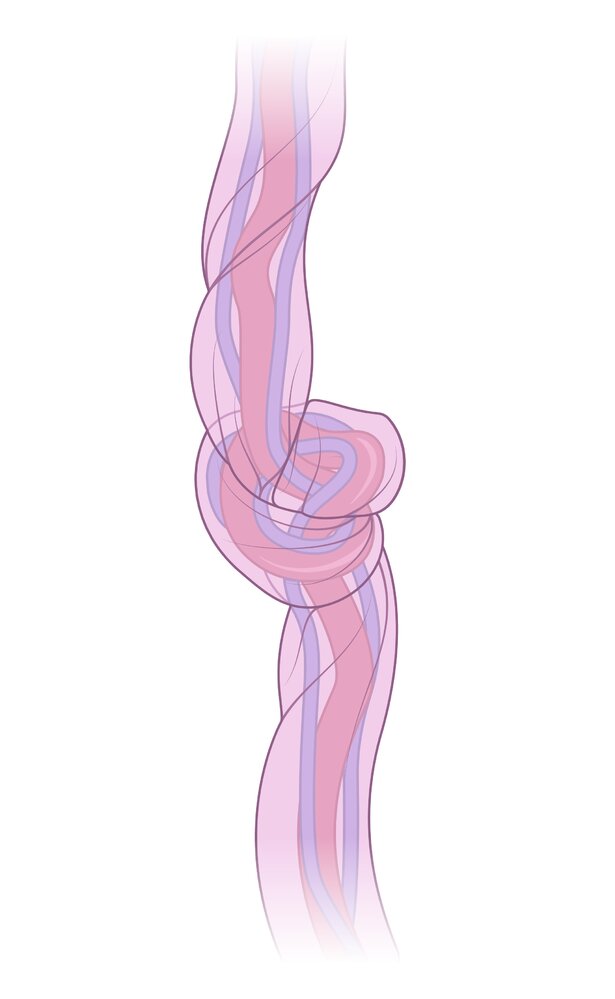
True umbilical cord knots usually arise from increased fetal movement. Tightening of the knot may result in reduced fetal perfusion with subsequent hypoxia. The diagnosis is usually only confirmed postpartum.
© AMBOSS
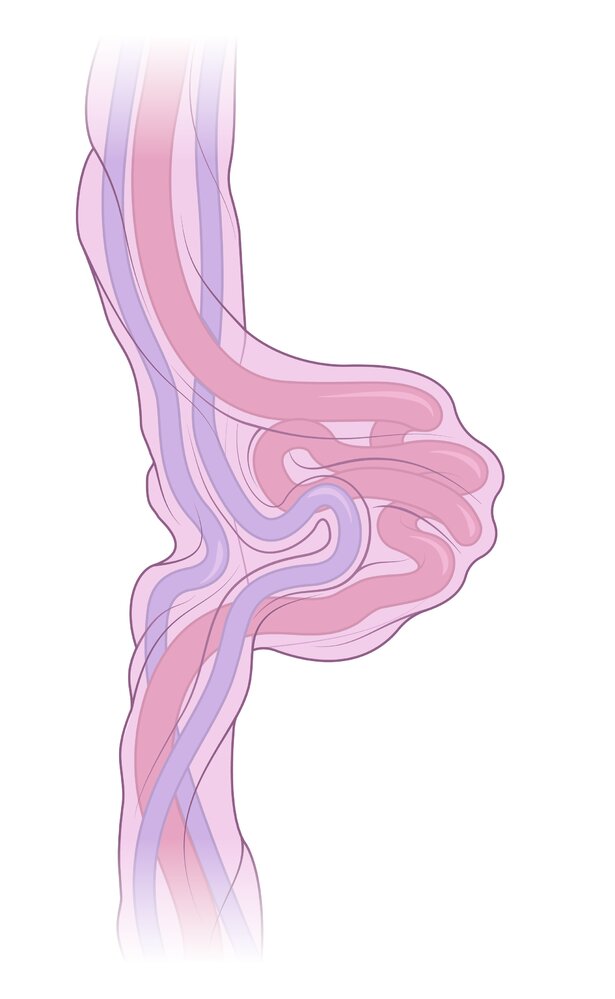
A false umbilical cord knot is a bulge or protuberance in the umbilical cord. It is caused by localized thickening of Wharton's jelly, vascular loops, or varices. There is no knotting of the umbilical cord and the finding has no clinical relevance.
© AMBOSS
Induction of labor
Indications for induction of labor
- Post-term pregnancy (≥ 42 weeks of pregnancy or gestation)
- PPROM after 34 weeks
- PROM at term
- Hypertension during pregnancy, preeclampsia, eclampsia, HELLP syndrome
- Maternal diabetes to avoid post-term pregnancy (risk of macrosomia)
- Maternal request at term
- Intrauterine fetal demise
Contraindications for induction of labor [37]
- History of uterine rupture; previous classical cesarean incision
- Complete placenta previa
- Vasa previa
- Transverse fetal lie
- Cord prolapse
- Active maternal genital herpes
- Nonreassuring fetal heart rate
Bishop score [37]
Overview
- Definition: a scoring system used to assess the cervix and the likelihood of successful induction of labor
-
Interpretation
- Bishop score ≥ 8: favorable cervix (ready for vaginal delivery)
- Bishop score ≤ 6: unfavorable cervix (not ready for vaginal delivery)
-
Alternative: simplified Bishop score [38]
- Considers only fetal station, cervical dilation, and cervical effacement
- A score of ≥ 5 indicates a favorable cervix.
Bishop score
| Bishop score [37] | ||||
|---|---|---|---|---|
| Score | ||||
| 0 points | 1 point | 2 points | 3 points | |
| Cervical position | Posterior | Midline | Anterior | |
| Cervical consistency | Firm | Moderately firm | Soft (ripe) | |
| Cervical effacement | ≤ 30% | 31–50% | 51–80% | > 80% |
| Cervical dilation | Closed | 1–2 cm | 3–4 cm | ≥ 5 cm |
| Fetal station | -3 cm | -2 cm | -1/0 cm | +1/+2 cm |
Approach
- Membrane sweeping (shortens time to onset of labor)
- If the cervix is still unfavorable: cervical ripening with prostaglandin E1 or E2 (e.g., misoprostol)
- Maternal oxytocin infusion
- Consider amniotomy (only if the cervix is partially dilated and completely effaced, and the fetal head is well applied)
- Administer under fetal heart rate monitoring.
Failure of induction [5]
- Definition: a prolonged latent phase (e.g., 12–18 hours) after induction of labor (i.e., initiation of oxytocin and rupture of membranes) [1][5][39]
-
Management
- Maternal and/or fetal distress: intrauterine resuscitation and/or immediate delivery
- Reassuring maternal and fetal signs: cesarean delivery after 18 hours of failed induction [1]
Assisted vaginal delivery
Obstetric forceps delivery [40]
- Definition: a forcep is a metal device that enables gentle rotation and/or traction of the fetal head during vaginal delivery
-
Types
- Kielland: enables rotation and traction of the fetal head
- Simpson: only enables traction of the fetal head
- Barton: used for occiput transverse position of the fetal head
- Piper: used to deliver the fetal head during breech delivery
-
Classification (See “Station” in “Mechanics of childbirth”)
- Outlet: fetal head lies on the pelvic floor
- Low: fetal head is below +2 station (not on the pelvic floor)
- Mid: fetal head is below 0 station (not at +2 station)
- High: fetal head is not engaged
-
Indications
- Prolonged second stage of labor
- Breech presentation
- Nonreassuring fetal heart rate
- To avoid/assist maternal pushing efforts (e.g., maternal fatigue or cardiopulmonary conditions)
-
Prerequisites
- Skilled clinician
- Clinically adequate pelvic dimensions (see “Mechanics of childbirth”)
- Full cervical dilation
- Engagement of the fetal head
- Knowledge of exact position and attitude of the fetal head
- Emptied maternal bladder
- No suspicion of fetal bleeding or bone mineralization disorders
-
Advantages (compared to vacuum delivery)
- Scalp injuries are less common
- Cannot undergo decompression and “pop off”
-
Complications
- Maternal: obstetric lacerations (cervix, vagina, uterus), perineal hematomas, urinary tract injury, anal sphincter injury
- Fetal: head or soft tissue trauma (e.g., scalp lacerations, injured ears), facial nerve palsy, intracranial hemorrhage, retinal hemorrhage, skull fractures, fetal death (rare)


Vacuum extractor delivery [40]
- Definition: a vacuum extractor is a metal or plastic cup, attached to the fetal head with a suction device, that enables traction of the fetal head during vaginal delivery
-
Indications
- Prolonged second stage of labor
- Nonreassuring fetal heart rate
- To avoid/assist maternal pushing efforts
-
Prerequisites
- Skilled clinician
- Clinically adequate pelvic dimensions
- Gestation ≥ 34 weeks
- Engagement of the fetal head
- Full cervical dilation
- Emptied maternal bladder
- Vertex position
- No suspicion of fetal bleeding or bone mineralization disorders
-
Advantages (compared to forceps delivery)
- Requires minimum space
- ↓ incidence of third- and fourth-degree perineal tears
- Less knowledge about exact position and attitude of the fetal head is acceptable
-
Complications
- Maternal: suction of maternal soft tissue → hematomas or lacerations
- Fetal: cephalohematoma , scalp lacerations, life-threatening head injury (e.g., intracranial hemorrhage or subgaleal hematoma)
A routine episiotomy is not recommended with assisted vaginal delivery because of the risk of poor healing and anal sphincter injury!
An advantage of assisted vaginal delivery is avoiding cesarean delivery.



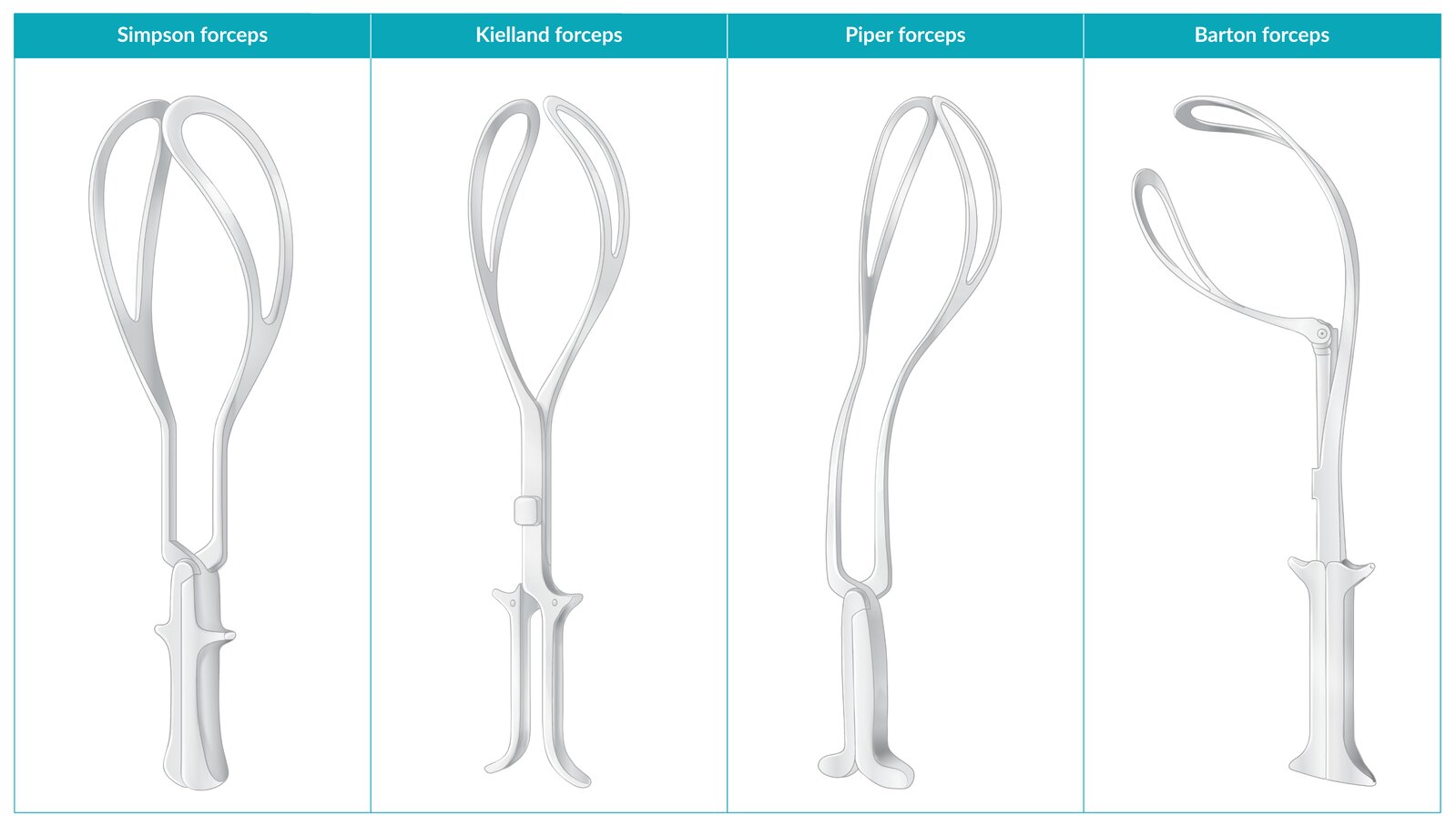
Simpson forceps: enables traction of the fetal head
Kielland forceps: enables rotation and traction of the fetal head
Piper forceps: used to deliver the fetal head during a breech delivery
Barton forceps: used for occiput transverse position of the fetal head
© AMBOSS
© AMBOSS
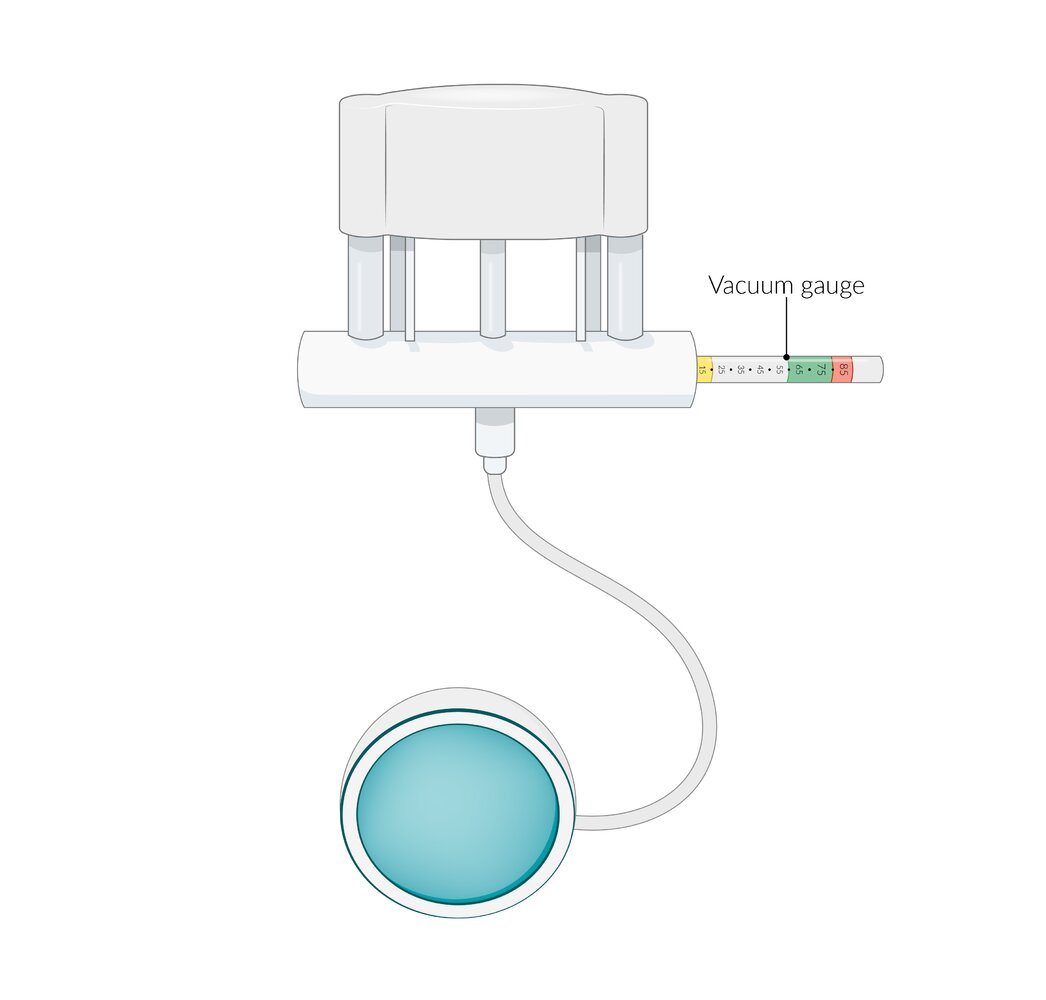
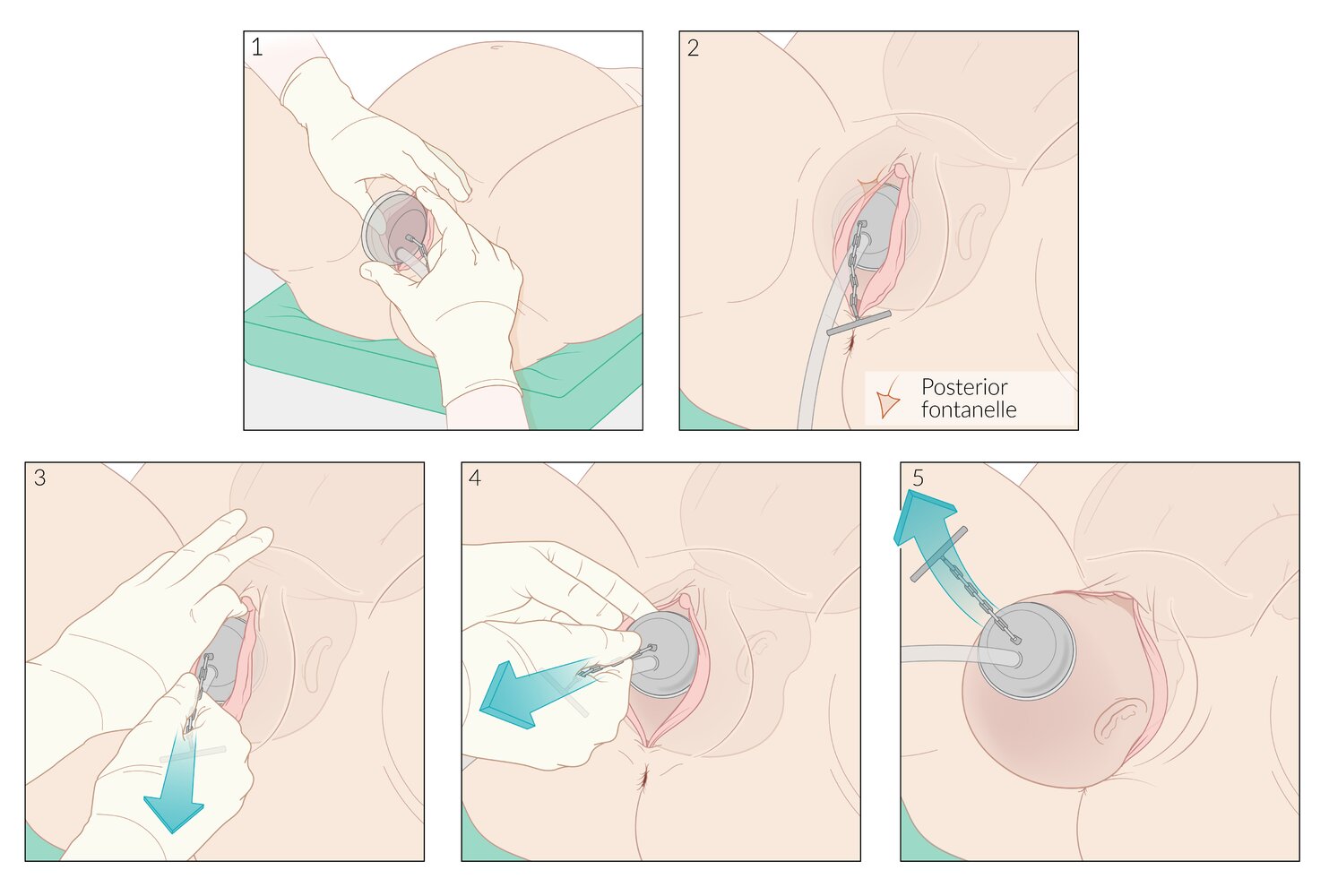
Vacuum extractor for assisted vaginal delivery:
A metal or plastic cup is inserted into the vagina and attached to the fetal head with a suction device. A centrally attached chain connects the cup to a handle that enables traction of the fetal head during delivery. The vacuum pump is operated manually. Various models are available.
© AMBOSS
© AMBOSS

Bruising and slight deformation of a newborn's scalp after vacuum extractor delivery.
Source: “Vacuum Extraction bruised scalp.JPG” by Ravedave, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Intrauterine resuscitation
Intrauterine resuscitation focuses on improving oxygen delivery to the placenta and maintaining umbilical blood flow to treat fetal distress and enable safe delivery.
- Indication: nonreassuring fetal status
-
Initial management
- Consult obstetrics immediately.
- Reposition the mother from supine to the lateral decubitus position.
- Administer a 1L IV fluid bolus. [41]
- Provide oxygen therapy if there is maternal hypoxia. [42][43]
- Discontinue uterotonic agents (e.g., oxytocin, misoprostol).
- Consider modifying maternal pushing efforts (e.g., temporary cessation, pushing with alternate contractions).
-
Obstetric management; consider the following:
- Tocolysis (e.g., for uterine tachysystole: > 5 contractions within 10 minutes)
- Amnioinfusion [44]
- Emergency cesarean delivery
Use IV fluids with caution in patients with cardiomyopathy or preeclampsia, as these patients have an increased risk of hypervolemia, which can lead to pulmonary edema. [45]
Episiotomy
- Consists of an incision of the perineum (midline or mediolateral) to enlarge the vaginal opening during delivery
- No longer routinely recommended.
- Can be considered if vaginal delivery needs to be expedited and maternal perineal tissue is thought to pose a significant obstacle, e.g.:
- Shoulder dystocia
- Inability to insert instruments required for assisted vaginal delivery
- Vaginal breech delivery
External Resources
- 2024 ACOG Clinical Practice Guideline No. 8: First and Second Stage Labor Management
- 2020 ACOG Practice Bulletin No. 217: Prelabor Rupture of Membranes
- 2020 ACOG Practice Bulletin No. 221: External Cephalic Version
- 2019 ACOG Committee Opinion No. 766: Approaches to Limit Intervention During Labor and Birth
- 2018 ACOG Committee Opinion No. 745: Mode of Term Singleton Breech Delivery
- 2017 ACOG Practice Bulletin No 178: Shoulder Dystocia
References
- Simpson KR, James DC. "Efficacy of Intrauterine Resuscitation Techniques in Improving Fetal Oxygen Status During Labor". Obstet Gynecol. 105(6). :1362-1368. (2005)
- Abati I, Micaglio M, Giugni D, et al. "Maternal Oxygen Administration during Labor: A Controversial Practice". Children. 10(8). :1420. (2023)
- Mahfouz A, Monaghan S, Zacharzewski A. "Intrauterine fetal resuscitation". Anaesth Intensive Care. 23(6). :336-340. (2022)
- Hofmeyr GJ, Lawrie TA. "Amnioinfusion for potential or suspected umbilical cord compression in labour". Cochrane Database Syst Rev. (2012)
- Garite TJ, Simpson KR. "Intrauterine Resuscitation During Labor". Clin Obstet Gynecol. 54(1). :28-39. (2011)
- Pavličev M, Romero R, Mitteroecker P. "Evolution of the human pelvis and obstructed labor: new explanations of an old obstetrical dilemma". Am J Obstet Gynecol. 222(1). :3-16. (2020)
- Neilson J, Lavender T, Quenby S, Wray S. "Obstructed labour". Br Med Bull. 67(1). :191-204. (2003)
- Ayenew AA. "Incidence, causes, and maternofetal outcomes of obstructed labor in Ethiopia: systematic review and meta-analysis". Reprod Health. 18(1). (2021)
- American College of Obstetricians and Gynecologists. "ACOG Committee Opinion No. 745: Mode of Term Singleton Breech Delivery". Obstet Gynecol. 132(2). :e60-e63. (2018)
- Carbillon L, Benbara A, Tigaizin A, et al. "Revisiting the management of term breech presentation: a proposal for overcoming some of the controversies". BMC Pregnancy Childbirth. 20(1). (2020)
- Oyinloye OI, Okoyomo AA. "Longitudinal evaluation of foetal transverse lie using ultrasonography". Afr J Reprod Health. 14(1). :129-33. (2010)
- American College of Obstetricians and Gynecologists. "External Cephalic Version: ACOG Practice Bulletin, Number 221". Obstet Gynecol. 135(5). :e203-e212. (2020)
- Boyle A, Reddy UM, Landy HJ, et al. "Primary Cesarean Delivery in the United States". Obstet Gynecol. 122(1). :33-40. (2013)
- Rosman AN, Guijt A, Vlemmix F, et al. "Contraindications for external cephalic version in breech position at term: a systematic review". Acta Obstet Gynecol Scand. 92(2). :137-142. (2012)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Haumonte JB, Blanc J, Castel P, et al. "Uncertain fetal head engagement: a prospective randomized controlled trial comparing digital exam with angle of progression". Am J Obstet Gynecol. (2022)
- Sharshiner R, Silver RM. "Management of Fetal Malpresentation". Clin Obstet Gynecol. 58(2). :246-255. (2015)
- Barth WH. "Persistent Occiput Posterior". Obstet Gynecol. 125(3). :695-709. (2015)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Van Beekhuizen HJ, Unkels R, Mmuni NS, Kaiser M. "Complications of obstructed labour: pressure necrosis of neonatal scalp and vesicovaginal fistula". The Lancet. 368(9542). :1210. (2006)
- Pagan M, Eads L, Sward L, et al. "Umbilical Cord Prolapse: A Review of the Literature". Obstet Gynecol Surv. 75(8). :510-518. (2020)
- Sayed Ahmed W, Hamdy M. "Optimal management of umbilical cord prolapse". Int J Womens Health. Volume 10. :459-465. (2018)
- Peesay M. "Nuchal cord and its implications". Matern Health Neonatol and Perinatol. 3(1). (2017)
- Hayes DJL, Warland J, Parast MM, et al. "Umbilical cord characteristics and their association with adverse pregnancy outcomes: A systematic review and meta-analysis". PLoS ONE. 15(9). :e0239630. (2020)
- Carter EB, Chu CS, Thompson Z, et al. "True knot at the time of delivery: electronic fetal monitoring characteristics and neonatal outcomes". J Perinatol. 38(12). :1620-1624. (2018)
- Gokmen Karasu AF, Kutuk MS. "Prenatal detection and obstetric management of true umbilical cord knots using color Doppler and 4D ultrasonography: a report of two cases and literature review". Case Rep Perinat Med. 8(1). (2018)
- ACOG. "First and Second Stage Labor Management". Obstet Gynecol. 143(1). :144-162. (2024)
- Bakker W, Sandberg E, Keetels S, et al. "Inconsistent definitions of prolonged labor in international literature: a scoping review". AJOG Glob Rep. 4(3). :100360. (2024)
- "ACOG Committee Opinion No. 766: Approaches to Limit Intervention During Labor and Birth". ACOG
- Hersh AR, Carroli G, Hofmeyr GJ, et al. "Third stage of labor: evidence-based practice for prevention of adverse maternal and neonatal outcomes". Am J Obstet Gynecol. 230(3). :S1046-S1060.e1. (2024)
- LeFevre NM, Krumm E, Cobb WJ. "Labor Dystocia in Nulliparous Women". Am Fam Physician. 103(2). :90-96. (2021)
- Perlman NC, Carusi DA. "Retained placenta after vaginal delivery: risk factors and management". International Journal of Women's Health. Volume 11. :527-534. (2019)
- American College of Obstetricians and Gynecologists. "Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217". Obstet Gynecol. 135(3). :e80-e97. (2020)
- Al-lawama M, AlZaatreh A, Elrajabi R, Abdelhamid S, Badran E. "Prolonged Rupture of Membranes, Neonatal Outcomes and Management Guidelines". J Clin Med Res. 11(5). :360-366. (2019)
- Medina TM, Hill DA. "Preterm premature rupture of membranes: diagnosis and management". Am Fam Physician. 73(4). :659-64. (2006)
- ACOG. "ACOG Committee Opinion No. 766: Approaches to Limit Intervention During Labor and Birth". Obstet Gynecol. 133(2). :e164-e173. (2019)
- American College of Obstetricians and Gynecologists. "Committee Opinion No 652: Magnesium Sulfate Use in Obstetrics". Obstet Gynecol. 127(1). :e52-e53. (2016)
- Dutta DC, Konar H. "Textbook of Obstetrics". Jaypee Brothers Medical Publishers. (2015). ISBN: 9789351527237
- The American College of Obstetricians and Gynecologists. "ACOG Practice Bulletin No. 107: Induction of Labor". Obstet Gynecol. 114(2). :386-397. (2009)
- Laughon SK, Zhang J, Troendle J, Sun L, Reddy UM. "Using a Simplified Bishop Score to Predict Vaginal Delivery". Obstet Gynecol. 117(4). :805-811. (2011)
- William A. Grobman, Jennifer Bailit, Yinglei Lai, Uma M. Reddy. "Defining failed induction of labor". Am J Obstet Gynecol. 218(1). :122.e1-122.e8. (2018)
- American College of Obstetricians and Gynecologists. "Practice Bulletin No 178: Shoulder Dystocia". Obstet Gynecol. 129(5). :e123-e133. (2017)
- Hill DA, Lense J, Roepcke F. "Shoulder Dystocia: Managing an Obstetric Emergency". Am Fam Physician. 102(2). :84-90. (2020)
- Lau SL, Sin WTA, Wong L, et al. "A critical evaluation of the external and internal maneuvers for resolution of shoulder dystocia". Am J Obstet Gynecol. (2023)
- Raducha JE, Cohen B, Blood T, Katarincic J. "A Review of Brachial Plexus Birth Palsy: Injury and Rehabilitation". R I Med J (2013). 100(11). :17-21. (2017)