Summary
Acid-base disorders are characterized by changes in the concentration of hydrogen ions (H+) in the body. Increased H+ concentration (acidosis) can lead to an abnormally low blood pH (acidemia) and decreased H+ concentration (alkalosis) can lead to an abnormally high blood pH (alkalemia); however, if compensation occurs, acidosis and/or alkalosis may be present without acidemia or alkalemia. Acidosis and alkalosis may be respiratory or metabolic in origin depending on the cause of the imbalance; they can also coexist as mixed acid-base disorders. Diagnosis is made based on arterial blood gas (ABG) results. In metabolic acidosis, calculation of the anion gap can also help determine the cause and reach a precise diagnosis. In metabolic alkalosis, urine chloride (Cl‑) concentration can help identify the cause. Treatment is based on the underlying cause.
Definitions
-
Acid-base processes [1]
- Acidosis: the processes by which H+ concentration is increased
- Alkalosis: the processes by which H+ concentration is decreased
-
pH scale
- A logarithmic scale that expresses the acidity or alkalinity of a solution based on the concentration of H+ (pH = -log[H+])
- Neutral pH is 7; lower values are acidic and higher values are alkaline.
-
Blood pH abnormalities
- Acidemia; : abnormally low blood pH (pH < 7.35)
- Alkalemia; : abnormally high blood pH (pH > 7.45)
Pathophysiology
-
The Henderson-Hasselbalch equation allows for the calculation of pH from HCO3- and PCO2: pH = 6.1 + log([HCO3-]/[0.03 × pCO2])
- 6.1 = pKa of carbonic acid
- 0.03 = solubility constant of PCO2
| Pathophysiology of acid-base disorders [2] | |||||
|---|---|---|---|---|---|
| Respiratory acidosis | Respiratory alkalosis | Metabolic acidosis | Metabolic alkalosis | ||
| pH |
|
|
|
|
|
| PCO2 |
|
|
|
|
|
| HCO3- |
|
|
|
|
|
| Mechanism |
|
|
|
|
|
| Compensation mechanisms in acid-base disorders |
|
|
|
|
|


This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
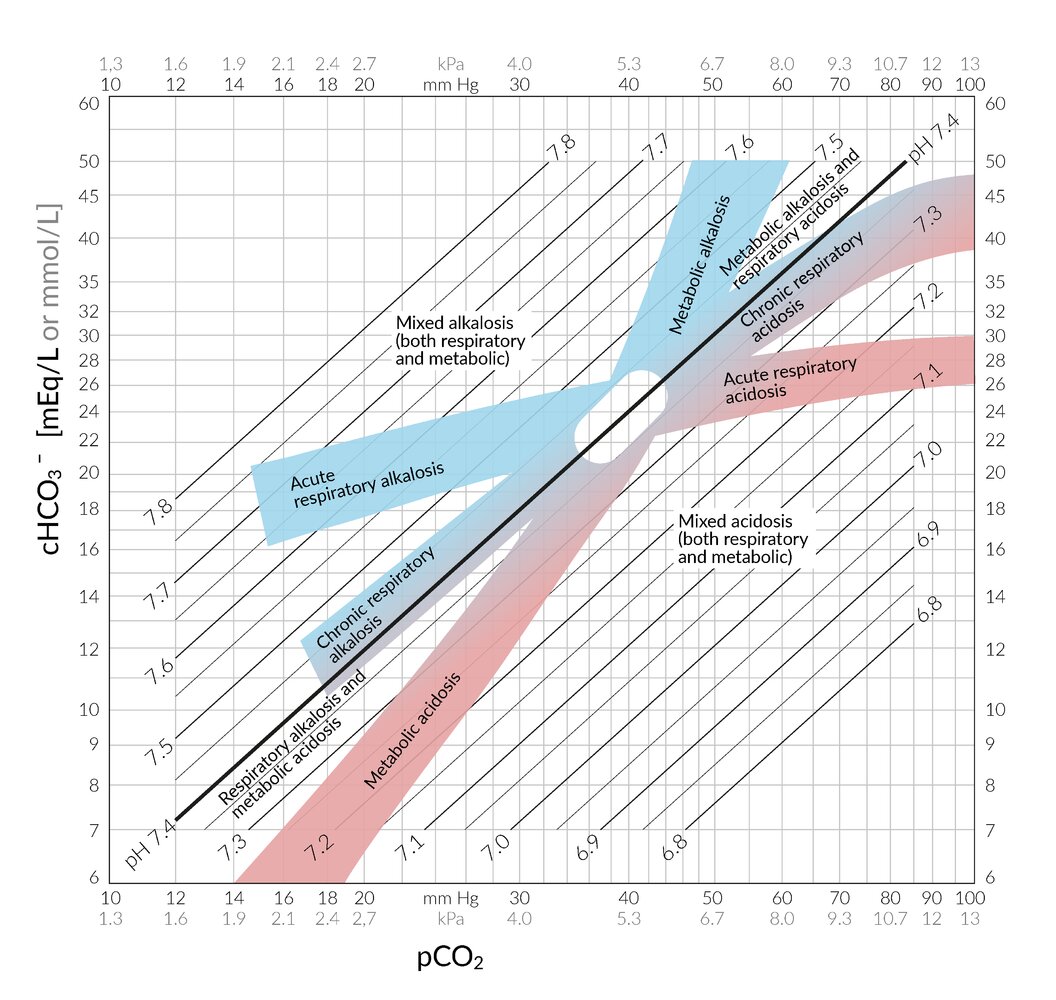
This nomogram can be used for the interpretation of an arterial blood gas analysis in the context of acid-base disorders.
PCO2 is on the x-axis and the concentration of HCO3- (cHCO3-) is on the y-axis; both are displayed logarithmically, allowing the pH to be displayed on parallel straight lines. The important areas for acid-base disorders are highlighted and labeled. The oval area in the middle around PCO2 = 40 mm Hg and cHCO3- = 24 mEq/L represents the reference range.
© AMBOSS
Diagnosis
Approach to acid-base disorders [1][3]
- Perform an initial clinical evaluation: to help identify the most likely underlying cause
- Order initial laboratory studies: ABG, BMP [4][5]
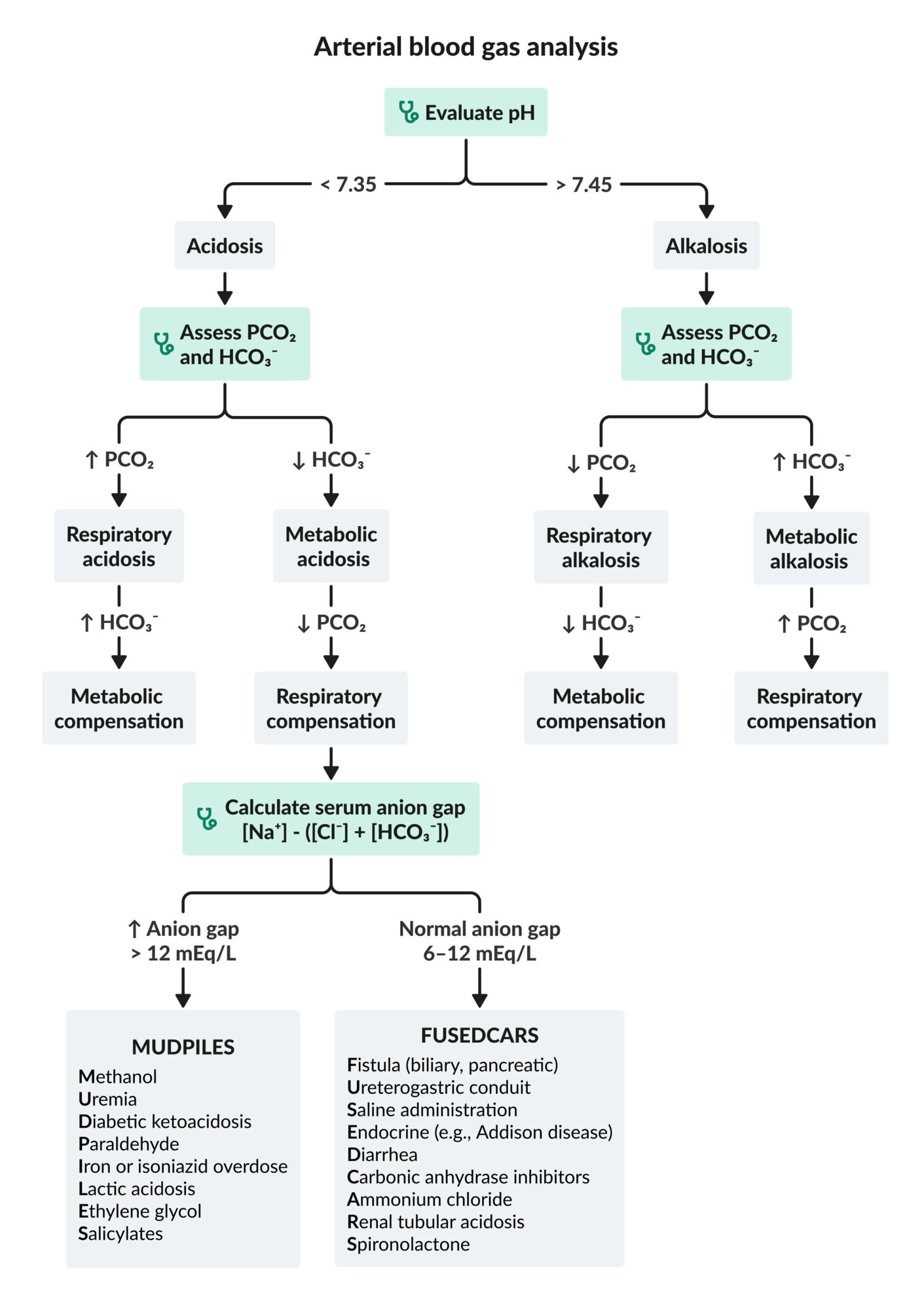
- Determine the primary acid-base disorder: i.e., using pH, PCO2, and HCO3-
-
Calculate the expected compensatory (or secondary) response.
- Mixed acid-base disorder: The expected compensatory response differs from the laboratory findings.
- No mixed acid-base disorder: The expected compensatory response aligns with the laboratory findings.
-
Perform further diagnostic workup (to determine the mechanism and the cause), e.g.:
- In metabolic acidosis: anion gap and delta gap
- In metabolic alkalosis: urinary chloride and potassium levels
Careful clinical evaluation is an important first step in the assessment of acid-base disorders, as it can provide important diagnostic clues that can help determine the underlying cause.

Initial blood gas analysis
There are different methods for the assessment of acid-base status; the following method is just one example.
Suggested approach
- Evaluate blood pH (reference range: 7.35–7.45).
- Evaluate HCO3- (reference range: 22–28 mEq/L).
- Evaluate PCO2 (reference range: 33–45 mm Hg).
Interpretation
-
pH < 7.35 (acidemia): Primary disorder is an acidosis.
- ↓ pH and ↓ HCO3-: metabolic acidosis
- ↓ pH and ↑ PCO2: respiratory acidosis
-
pH > 7.45 (alkalemia): Primary disorder is an alkalosis.
- ↑ pH and ↑ HCO3-: metabolic alkalosis
- ↑ pH and ↓ PCO2: respiratory alkalosis
Further considerations
-
Evaluate PO2.
- High: hyperoxemia
- Low: hypoxemia
- See also “Respiratory failure.”
SMORE: change in PCO2 in the Same direction as pH → Metabolic disorder; change in PCO2 in the Opposite direction to pH → REspiratory disorder
Corrections to central venous blood gas values [6][7]
Reference values for venous blood gas (VBG) are different from those for ABG; central VBG results can be corrected to approximate ABG.
- Arterial pH = venous pH + 0.03–0.05 units
- Arterial PCO2 = venous PCO2 – 5 mm Hg
Compensation (acid-base) [1][8]
- Definition: physiological changes that occur in acid-base disorders in an attempt to maintain normal body pH
-
Compensatory changes
- In metabolic disorders: rapid compensation within minutes through changes in minute ventilation (respiratory compensation)
- In respiratory disorders: typically slow compensation over several hours to days through changes in urine pH (metabolic compensation)
- See also “Compensation mechanisms in acid-base disorders.”
-
Assessment and interpretation: Calculate the expected compensation; see “Calculation of compensatory response.”
- Primary respiratory disorders
- Measured HCO3- > expected HCO3-: metabolic alkalosis in addition to respiratory disturbance
- Measured HCO3- < expected HCO3-: metabolic acidosis in addition to respiratory disturbance
- Primary metabolic disorders
- Measured PCO2 > expected PCO2: respiratory acidosis in addition to metabolic disturbance
- Measured PCO2 < expected PCO2: respiratory alkalosis addition to metabolic disturbance
- Primary respiratory disorders
| Calculation of compensatory response | |||
|---|---|---|---|
| Primary acid-base disturbance | Expected compensation [1][9] | ||
| Metabolic acidosis |
|
||
| Metabolic alkalosis |
|
||
| Respiratory acidosis | Acute |
|
|
| Chronic |
|
||
| Respiratory alkalosis | Acute |
|
|
| Chronic |
|
||
Discordance between the measured compensatory response and the expected compensatory response suggests a secondary acid-base disturbance.
In primary metabolic disorders, respiratory compensation develops quickly (within hours), whereas metabolic compensation may take 2–5 days to develop in primary respiratory disorders.
This algorithm does not account for mixed acid-base disorders.
Cl-: chloride
HCO3-: bicarbonate
Na+: sodium
PCO2: partial pressure of carbon dioxide
© AMBOSS
This nomogram can be used for the interpretation of an arterial blood gas analysis in the context of acid-base disorders.
PCO2 is on the x-axis and the concentration of HCO3- (cHCO3-) is on the y-axis; both are displayed logarithmically, allowing the pH to be displayed on parallel straight lines. The important areas for acid-base disorders are highlighted and labeled. The oval area in the middle around PCO2 = 40 mm Hg and cHCO3- = 24 mEq/L represents the reference range.
© AMBOSS
Metabolic acidosis
General principles
-
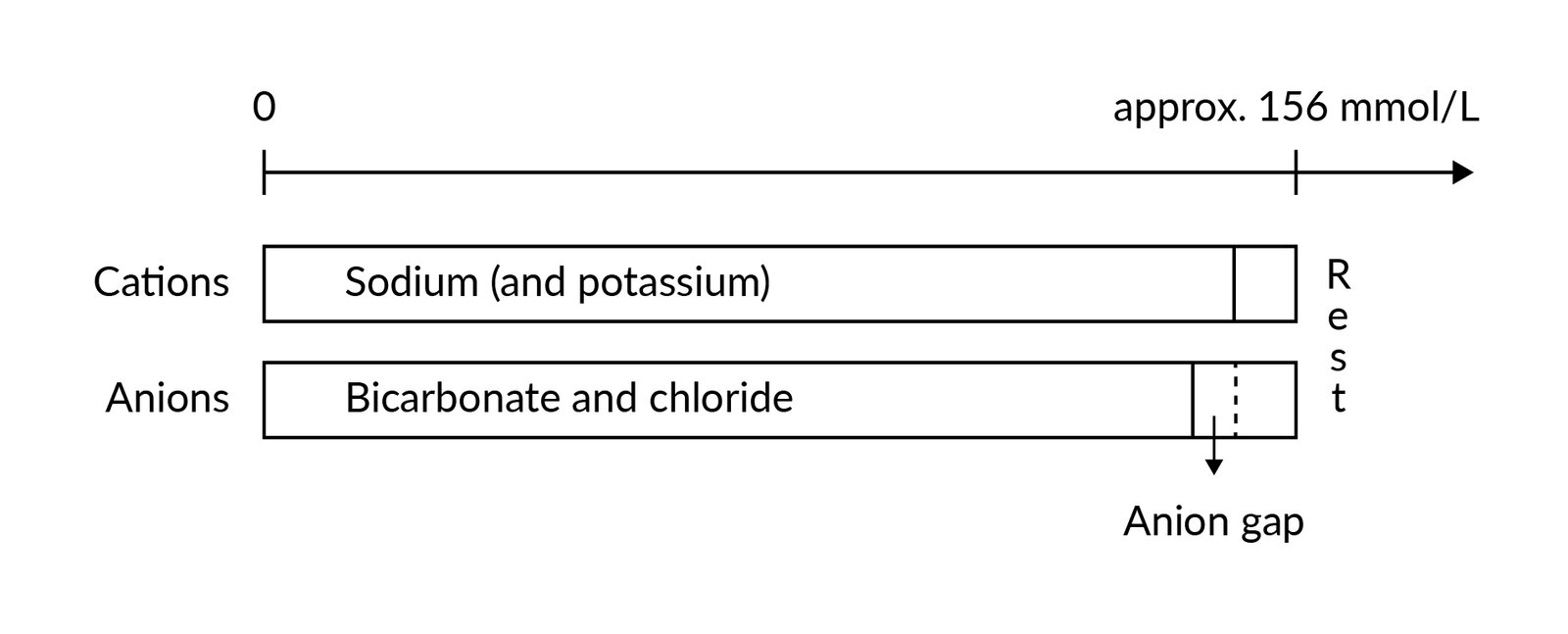
Calculation of the anion gap is the first step in the evaluation of metabolic acidosis.
- Maintenance of electrical neutrality requires that the total concentration of cations approximate that of anions.
- Anion gap: the difference between the concentration of measured cations and measured anions
- High anion gap: increased concentration of organic acids such as lactate, ketones (e.g., beta-hydroxybutyrate, acetoacetate), oxalic acid, formic acid, or glycolic acid, with no compensatory increase in Cl-.
- Normal anion gap: primary loss of HCO3- compensated with ↑ Cl-
- The measured serum sodium (Na+), not the corrected serum Na+, should be used in the formulas, even if glucose levels are high.
- Depending on the results, further evaluation and calculations may be needed (see specific subsections below).
| Metabolic acidosis formulas [1][10][11] | ||
|---|---|---|
| Anion gap | Serum anion gap |
|
| Urine anion gap |
|
|
| Osmolal gap | Serum osmolal gap |
|
| Urine osmolal gap |
|
|
| Delta gap |
|
|
| ||

High anion gap metabolic acidosis [1][11]
Review clinical features and initial studies and follow a stepwise approach to identify the underlying cause of high anion gap metabolic acidosis.
-
Exclude accumulation of endogenous organic acids.
- Exclude ketoacidosis : Consider measuring ketone levels in urine or serum (e.g., beta-hydroxybutyrate).
- Exclude lactic acidosis: Measure or review lactate levels.
- Exclude uremia: Measure or review BUN and creatinine levels.
-
Consider accumulation of exogenous organic acids (ingestion) as the cause: e.g., if the cause remains unclear, or initially if the patient is comatose
- Consider obtaining serum or urine toxicology screen.
- Calculate serum osmolal gap: If elevated (≥ 10 mOsm/kg), consider propylene glycol, ethylene glycol, diethylene glycol, methanol, and isopropanol as potential causes.
- Calculate the delta gap: to exclude concomitant acid-base disturbances
| Etiology of high anion gap metabolic acidosis | |
|---|---|
| Mechanism | Causes |
| Accumulation of endogenous organic acids |
|
| Accumulation of exogenous organic acids |
|
Causes of high anion gap acidosis (MUDPILES): Methanol toxicity, Uremia, Diabetic ketoacidosis, Paraldehyde, Isoniazid or Iron overdose, Inborn error of metabolism, Lactic acidosis, Ethylene glycol toxicity, Salicylate toxicity
Concomitant acid-base disturbances [10][11]
Calculation of the delta gap can help determine if another acid-base disturbance is present in addition to a high anion gap metabolic acidosis. Cut-off values may vary depending on the source.
- Delta gap < 1 : Hyperchloremic or normal anion gap metabolic acidosis is present in addition to high anion gap metabolic acidosis. [10]
- Delta gap 1–2 : Only high anion gap metabolic acidosis is present.
- Delta gap > 2 : A metabolic alkalosis is present in addition to high anion gap metabolic acidosis. [11]
Normal anion gap metabolic acidosis
Review clinical features and initial studies and consider further diagnostic workup to determine the underlying cause of normal anion gap metabolic acidosis.
-
Calculate the urine anion gap
- Negative urine anion gap: Acidosis is likely due to loss of bicarbonate.
- Positive urine anion gap: Acidosis is likely due to decreased renal acid excretion.
-
Consider calculating the urine osmolal gap
- Preferred over urine anion gap if the urine pH is > 6.5 or urine Na+ is < 20 mEq/L
- ↓ Urine osmolal gap (< 80–100 mOsm/kg) suggests impairment in the excretion of urinary ammonium. [13][14]
| Etiology of normal anion gap metabolic acidosis | |
|---|---|
| Mechanism | Causes |
| Loss of bicarbonate (negative urine anion gap) |
|
| Decreased renal acid excretion (positive urine anion gap) |
|
Causes of normal anion gap acidosis (FUSEDCARS): Fistula (biliary, pancreatic), Ureterogastric conduit, Saline administration, Endocrine (Addison disease, hyperparathyroidism), Diarrhea, Carbonic anhydrase inhibitors, Ammonium chloride, Renal tubular acidosis, Spironolactone
A neGUTive urine anion gap may be due to GI loss of bicarbonate.
Abnormal anion gap without metabolic acidosis [15]
-
Etiology of low anion gap
- Hypoalbuminemia → ↓ unmeasured anions → ↓ anion gap
- Paraproteinemia (e.g., in multiple myeloma), severe hypercalcemia, severe hypermagnesemia, and/or lithium toxicity → ↑ unmeasured cations → ↓ anion gap
-
Etiology of high anion gap
- Severe hyperphosphatemia → ↑ unmeasured anions → ↑ anion gap [16]
- Severe hypocalcemia and/or hypomagnesemia → ↓ unmeasured cations → ↑ anion gap
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Metabolic alkalosis
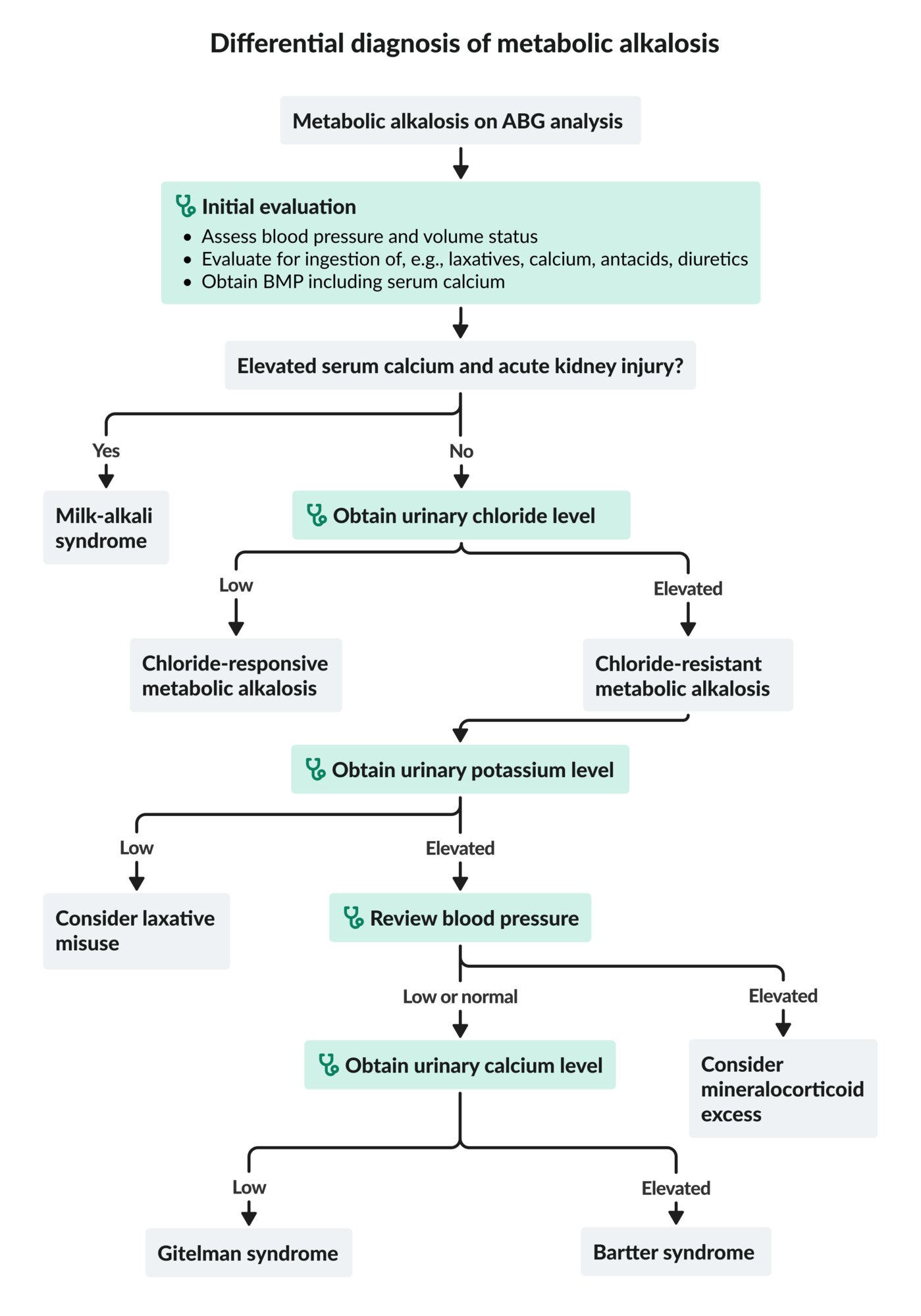
Approach to metabolic alkalosis [1]
- Assess the patient's blood pressure and volume status.
- Evaluate for ingestions (e.g., laxatives, calcium, alkali load, diuretics).
-
Obtain BMP and serum calcium, urinary chloride, and urinary potassium levels.
- Low urine chloride (< 25 mEq/L): chloride-responsive metabolic alkalosis
-
High urine chloride (> 40 mEq/L): chloride-resistant metabolic alkalosis ; check urine potassium.
- High urine potassium (> 30 mEq/L): Review blood pressure.
- Elevated blood pressure: Consider mineralocorticoid excess as a potential cause.
- Low or normal blood pressure: Consider Gitelman syndrome or Bartter syndrome as a potential cause.
- Low urine potassium (< 20 mEq/L): Consider laxative abuse as a potential cause.
- High urine potassium (> 30 mEq/L): Review blood pressure.
Elevated calcium with renal failure suggests milk-alkali syndrome.

Etiology
| Etiology of metabolic alkalosis [1][17] | |
|---|---|
| Mechanism | Causes |
| Chloride-responsive metabolic alkalosis (urine chloride < 25 mEq/L) |
|
| Chloride-resistant metabolic alkalosis (urine chloride > 40 mEq/L) |
|
ABG: arterial blood gas
BMP: basic metabolic panel
© AMBOSS
Respiratory disorders
Respiratory acidosis
- Seen in alveolar hypoventilation; see also “Respiratory insufficiency.”
- Establish the expected chronicity based on clinical presentation using the following rule:
- HCO3- increases by 1 mEq/L for every 10 mm Hg increase in PCO2 above 40 mm Hg: suggests acute respiratory acidosis
- HCO3- increases by 4–5 mEq/L for every 10 mm Hg increase in PCO2 above 40 mm Hg: suggests chronic respiratory acidosis
- Expected and measured HCO3- values may differ if additional metabolic disturbances are present; see “Compensation (acid-base).”
| Etiology of respiratory acidosis [1] | |
|---|---|
| Mechanism | Causes |
| Acute respiratory acidosis |
|
| Chronic respiratory acidosis |
|
Respiratory alkalosis
- Seen in hyperventilation; see also “Respiratory insufficiency.”
- Establish the expected chronicity based on clinical presentation using the following rule:
- HCO3- decreases by 2 mEq/L for every 10 mm Hg decrease in PCO2 below 40 mm Hg: suggests acute respiratory alkalosis
- HCO3- decreases by 4–5 mEq/L for every 10 mm Hg decrease in PCO2 below 40 mm Hg: suggests chronic respiratory alkalosis
- Expected and measured values may differ if additional metabolic disturbances are present; see “Compensation (acid-base).”
| Etiology of respiratory alkalosis [19] | |
|---|---|
| Mechanism | Causes |
| Acute respiratory alkalosis |
|
| Chronic respiratory alkalosis |
|
Gastrointestinal disorders
| Acid-base disturbances associated with GI disorders [20][21] | ||||
|---|---|---|---|---|
| GI disturbance | Acid-base disturbance | Cl- | K+ | Na+ |
| Severe diarrhea or laxative use | Metabolic acidosis | ↑ | ↓ | ↑ |
| Prolonged vomiting or nasogastric suctioning | Metabolic alkalosis | ↓ | ↓ | ↑ |
The loss of bicarbonate-rich fluid in severe diarrhea may cause non-anion gap metabolic acidosis.
Treatment
General considerations [2]
- Treatment of acid-base disorders should target the underlying cause.
- Medications (e.g., sodium bicarbonate, acetazolamide) used to correct acid-base abnormalities should be initiated in consultation with a specialist (e.g., nephrologist).
- Mechanical ventilation may be indicated in severe respiratory disorders and severe metabolic acidosis.
- Optimize ventilation in mechanically ventilated patients as needed.
- Electrolyte imbalances should be corrected: See “Disorders of potassium balance” and “Electrolyte repletion.”
Respiratory acidosis
- Severe acute respiratory acidosis: Consider noninvasive or invasive mechanical ventilation.
- See also “COPD,” “Opioid intoxication,” and “Benzodiazepine overdose.”
Respiratory alkalosis
- Acute respiratory alkalosis accompanied by increased work of breathing: Consider mechanical ventilation.
- See also “Treatment of congestive heart failure,” “Treatment of pulmonary embolism,” and “Salicylate toxicity.”
Metabolic acidosis
-
Acute severe metabolic acidosis
- Consider intravenous sodium bicarbonate and mechanical ventilation (see “High-risk indications for mechanical ventilation”)
- See also “Diabetic ketoacidosis” and “Salicylate toxicity.” [4][22]
-
Chronic metabolic acidosis
- Consider oral sodium bicarbonate
- See also “Chronic kidney disease,” and “Diarrhea.”
Metabolic alkalosis
-
Chloride-responsive metabolic alkalosis
- Start isotonic saline to increase urinary bicarbonate excretion and correct extracellular volume loss
- See “Intravenous fluid therapy” and “Treatment” in “Dehydration and hypovolemia.”
-
Chloride-resistant metabolic alkalosis
- Consider bicarbonate excess as a potential cause and administer acetazolamide.
- See also “Cushing Syndrome” and “Primary hyperaldosteronism.”
References
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Kraut JA, Madias NE. "Metabolic acidosis: pathophysiology, diagnosis and management". Nature Reviews Nephrology. 6(5). :274-285. (2010)
- Jaber S, Paugam C, Futier E, et al. "Sodium bicarbonate therapy for patients with severe metabolic acidaemia in the intensive care unit (BICAR-ICU): a multicentre, open-label, randomised controlled, phase 3 trial". Lancet. 392(10141). :31-40. (2018)
- Kasper DL, Hauser SL, Loscalzo J, et al. "Harrison's Principles of Internal Medicine Vol 1 20e". McGraw-Hill Education / Medical. (2018). ISBN: 9781259643996
- Berend K, de Vries APJ, Gans ROB. "Physiological Approach to Assessment of Acid–Base Disturbances". N Engl J Med. 371(15). :1434-1445. (2014)
- Dufour DR. "Laboratory Recognition and Testing in Acid-Base Disorders". Lab Med. 30(12). :776-781. (1999)
- Walkey AJ, Farber HW, O’Donnell C, et al. "The Accuracy of the Central Venous Blood Gas for Acid-Base Monitoring". J Intensive Care Med. 25(2). :104-110. (2009)
- Chong WH, Saha BK, Medarov BI. "Comparing Central Venous Blood Gas to Arterial Blood Gas and Determining Its Utility in Critically Ill Patients: Narrative Review". Anesth Analg. 133(2). :374-378. (2021)
- Marano M. "Evaluation of the expected ventilatory response to metabolic acidosis in chronic hemodialysis patients". Hemodial Int. 22(2). :180-183. (2017)
- Adrogué HJ, Madias NE. "Secondary Responses to Altered Acid-Base Status: The Rules of Engagement". J Am Soc Nephrol. 21(6). :920-923. (2010)
- Rastegar A. "Use of the DeltaAG/DeltaHCO3- ratio in the diagnosis of mixed acid-base disorders.". J Am Soc Nephrol. 18(9). :2429-31. (2007)
- Kraut JA, Xing SX. "Approach to the Evaluation of a Patient With an Increased Serum Osmolal Gap and High-Anion-Gap Metabolic Acidosis". Am J Kidney Dis. 58(3). :480-484. (2011)
- Tuchscherer J, Rehman H. "Metabolic acidosis in toluene sniffing". CJEM. 15(04). :249-252. (2013)
- Kim G-H, Han JS, Kim YS, et al. "Evaluation of urine acidification by urine anion gap and urine osmolal gap in chronic metabolic acidosis". Am J Kidney Dis. 27(1). :42-47. (1996)
- Halperin ML, Margolis BL, Robinson LA, et al. "The urine osmolal gap: a clue to estimate urine ammonium in "hybrid" types of metabolic acidosis.". Clin Invest Med. 11(3). :198-202. (1988)
- Lee S, Kang KP, Kang SK. "Clinical usefulness of the serum anion gap.". Electrolyte & blood pressure : E & BP. 4(1). :44-6. (2006)
- Sadjadi SA, Pi A. "Hyperphosphatemia, a Cause of High Anion Gap Metabolic Acidosis: Report of a Case and Review of the Literature". American Journal of Case Reports. 18. :463-466. (2017)
- Papadakis MA, McPhee SJ, Rabow MW. "CURRENT Medical Diagnosis and Treatment 2021". McGraw-Hill Education / Medical. (2020). ISBN: 9781260469868
- Galla JH. "Metabolic Alkalosis". J Am Soc Nephrol. 11(2). :369-375. (2000)
- Meltem AC, Figen C, Nalan MA, et al. "A hypokalemic muscular weakness after licorice ingestion: a case report". Cases Journal. 2(1). :8053. (2009)
- Gennari FJ, Weise WJ. "Acid-Base Disturbances in Gastrointestinal Disease". Clin J Am Soc Nephrol. 3(6). :1861-1868. (2008)
- Hamm LL, Nakhoul N, Hering-Smith KS. "Acid-Base Homeostasis". Clinical Journal of the American Society of Nephrology. 10(12). :2232-2242. (2015)