CME information and disclosures
To see contributor disclosures related to this article, click on this reference: [1]
Physicians can earn CME/MOC credit by using this article to address a clinical question and completing a brief evaluation about how they applied the information in their practice.
AMBOSS designates this internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and links" at the bottom of this article.
Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- Consider biliary POCUS if available.
- CBC
- BMP
- CRP
- Coagulation studies
- Liver chemistries
- Lipase
- Amylase
- Blood cultures (2 sets)
- RUQ ultrasound
- Evaluate for predictors of choledocholithiasis.
- Severity grading of acute cholecystitis
Determine the severity of acute cholecystitis once the diagnosis is confirmed to guide management.
Diagnostic criteria
Diagnostic criteria for acute cholecystitis are based on the following:
- Clinical features of acute cholecystitis (e.g., RUQ pain, Murphy sign)
- Systemic signs of inflammation (i.e., fever, leukocytosis, and/or ↑ CRP)
- Gallbladder inflammation on imaging
Fever and tachycardia are commonly absent in acute cholecystitis; maintain a high index of clinical suspicion.



Red flag features
- Severe acute cholecystitis:
- Hypotension requiring vasopressors
- Impaired consciousness
- PaO2/FiO2 ratio < 300
- Oliguria or serum creatinine > 2 mg/dL
- INR > 1.5
- Platelet count < 100,000/mm3
Management checklist
- IV access with two large-bore peripheral lines
- Immediate hemodynamic support
- Management of sepsis and septic shock
- Start empiric antibiotic therapy for acute biliary infection.
- Consult general surgery.
- Maintain NPO status.
- Initial supportive therapy for acute biliary disease (e.g., analgesia, antiemetics)
- Consider NG tube for intractable vomiting.
All patients with acute cholecystitis require inpatient management.

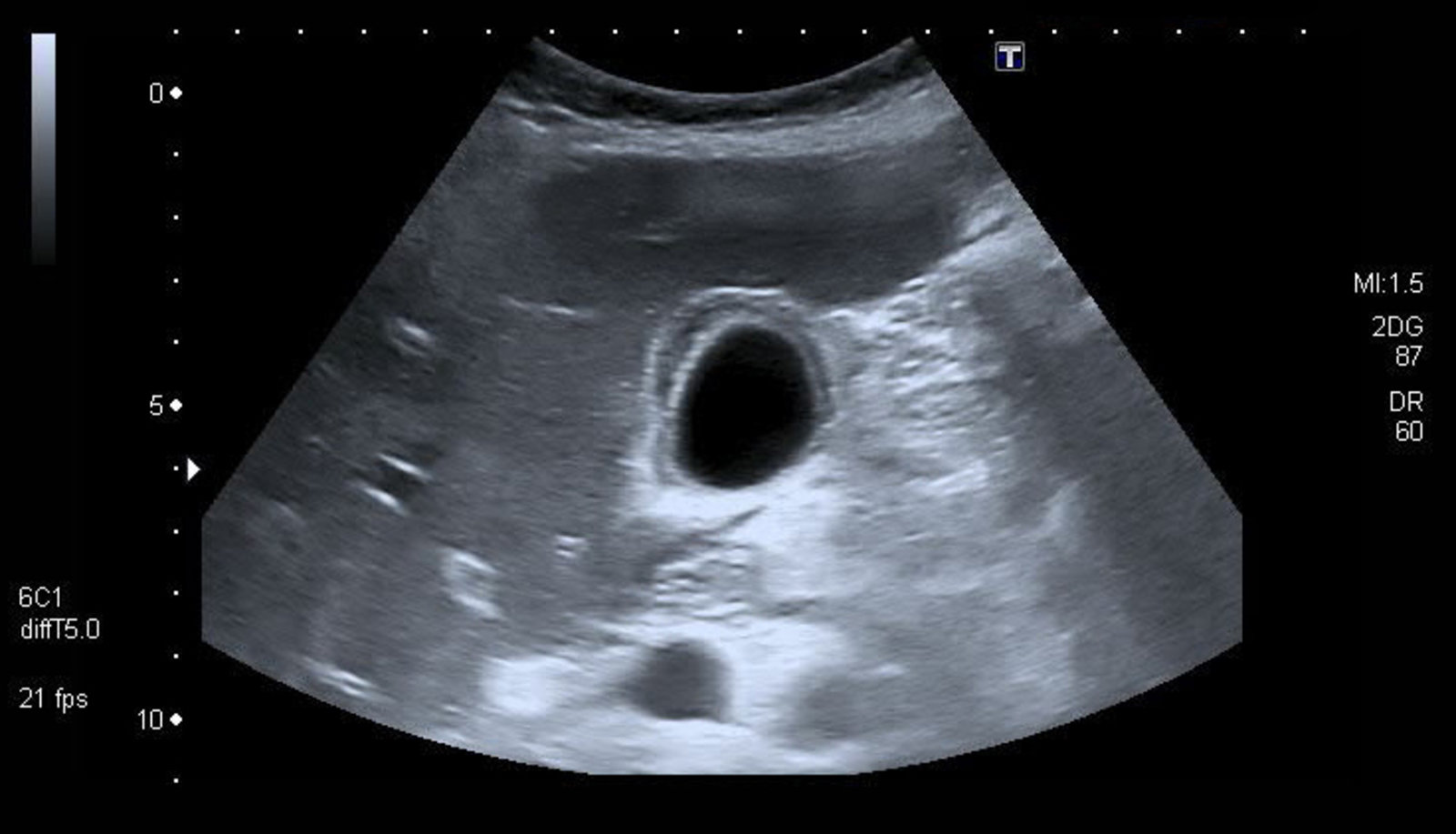
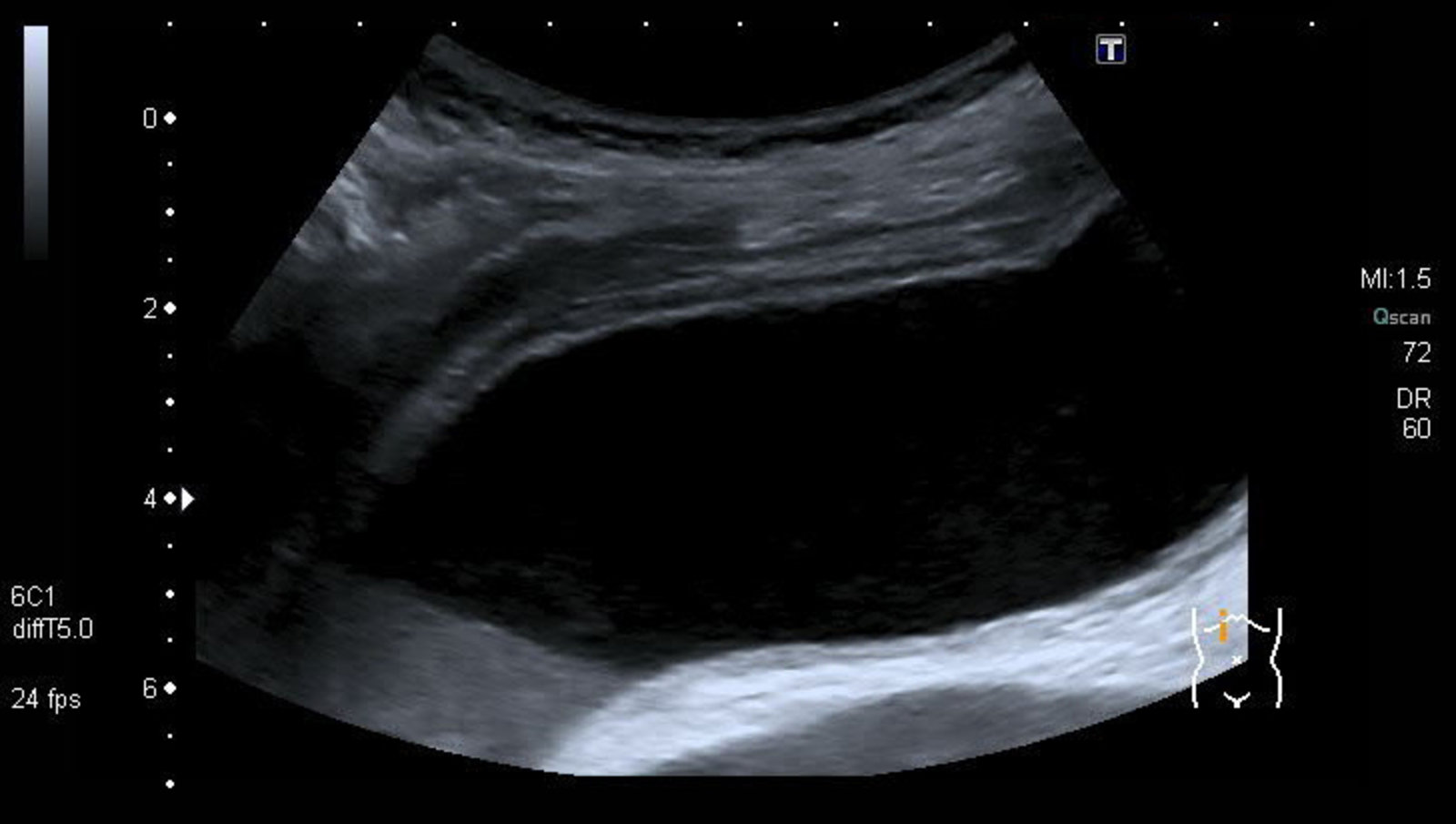
Ultrasound gallbladder (longitudinal plane)
Acoustic enhancement (green overlay) is seen distal to the gallbladder except where multiple small dependent hyperechoic calculi (yellow overlay) reflect the ultrasound beam and cast an acoustic shadow (green hatched overlay). Biliary sludge (yellow hatched overlay) is slightly hyperechoic compared to anechoic bile. The gallbladder wall is thickened (normal size: 1–2 mm) and has a layered appearance (red overlay), with central hypoechoic edema.
These findings in a patient with typical clinical features of RUQ pain strongly indicate acute calculous cholecystitis. Additional findings that would support a diagnosis of cholecystitis include an obstructing calculus, positive Murphy sign, pericholecystic fluid, gallbladder dilatation, and hyperemia of the gallbladder wall on color Doppler.
G: gallbladder; L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Ultrasound gallbladder
The gallbladder is dilated and its wall (green overlay) is thickened and striated (alternate hyperechoic and hypoechoic layers) as a result of edema. A calculus within dependent sludge in the neck produces posterior acoustic shadowing (red overlay) and has a highly reflective echogenic anterior surface (green hatched overlay).
Ultrasound findings in acute cholecystitis include wall thickening, dilatation, pericholecystic fluid, and a positive sonographic Murphy sign. The presence of multiple ultrasound findings increases diagnostic accuracy for cholecystitis.
L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Ultrasound gallbladder (transverse plane)
The gallbladder wall is thickened. Edema has produced a striated or layered appearance with hyperechoic inner and outer layers (green overlay) and a more hypoechoic middle layer (red overlay).
These features are suggestive of acute cholecystitis.
L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Summary
Acute cholecystitis refers to the acute inflammation of the gallbladder, which is typically due to cystic duct obstruction by a gallstone (acute calculous cholecystitis). Acalculous cholecystitis is less common and seen predominantly in critically ill patients. Right upper qudrant (RUQ) pain, a positive Murphy sign, and fever are the characteristic clinical features of acute cholecystitis. RUQ ultrasound is the preferred initial imaging modality, which typically shows gallbladder distension, edema, and pericholecystic fluid. Empiric antibiotic therapy and laparoscopic cholecystectomy are the mainstays of treatment. Laparoscopic cholecystectomy should be performed as soon as possible, preferably within 72 hours of admission, unless operative and anesthesia risks outweigh the benefits of urgent surgery. In high-risk patients with severe cholecystitis, a temporizing gallbladder drainage procedure (e.g., percutaneous cholecystostomy, endoscopic gallbladder stenting) should be performed and elective interval cholecystectomy scheduled after the resolution of acute symptoms. Complications of acute cholecystitis include gangrenous cholecystitis, emphysematous cholecystitis, gallbladder perforation, biliary-enteric fistula, gallstone ileus, and pyogenic liver abscess. Chronic cholecystitis may result from chronic cholelithiasis or recurrent attacks of acute cholecystitis. Chronic gallbladder inflammation increases the risk of gallbladder carcinoma.
See also “Cholelithiasis,” “Choledocholithiasis,” and “Acute cholangitis.”

© AMBOSS
Epidemiology
- Sex: ♀ > ♂
- Prevalence: most common complication of cholelithiasis
- Peak incidence: > 50 years
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Acute calculous cholecystitis: most common form [2]
- Cause: obstructing cholelithiasis
- Pathophysiology
- Cholelithiasis → passage of gallstones into the cystic duct → cystic duct obstruction → distention and inflammation of the gallbladder
- Secondary bacterial infection may also be present (E. coli, Klebsiella, Enterobacter, Enterococcus spp. most common) but is not necessary for the development of cholecystitis.
-
Acalculous cholecystitis: 5–10% of acute cholecystitis [3]
- See ”Acalculous cholecystitis” in “Subtypes and variants” section
Approximately 90% of acute cholecystitis is caused by cholelithiasis. Acalculous cholecystitis accounts for the remaining 10%. [4]
Clinical features
-
Right upper quadrant pain
- Typically more severe and prolonged (> 6 hours) than in biliary colic
- Postprandial
- Radiation to the right scapula (due to referred pain from phrenic nerve irritation)
-
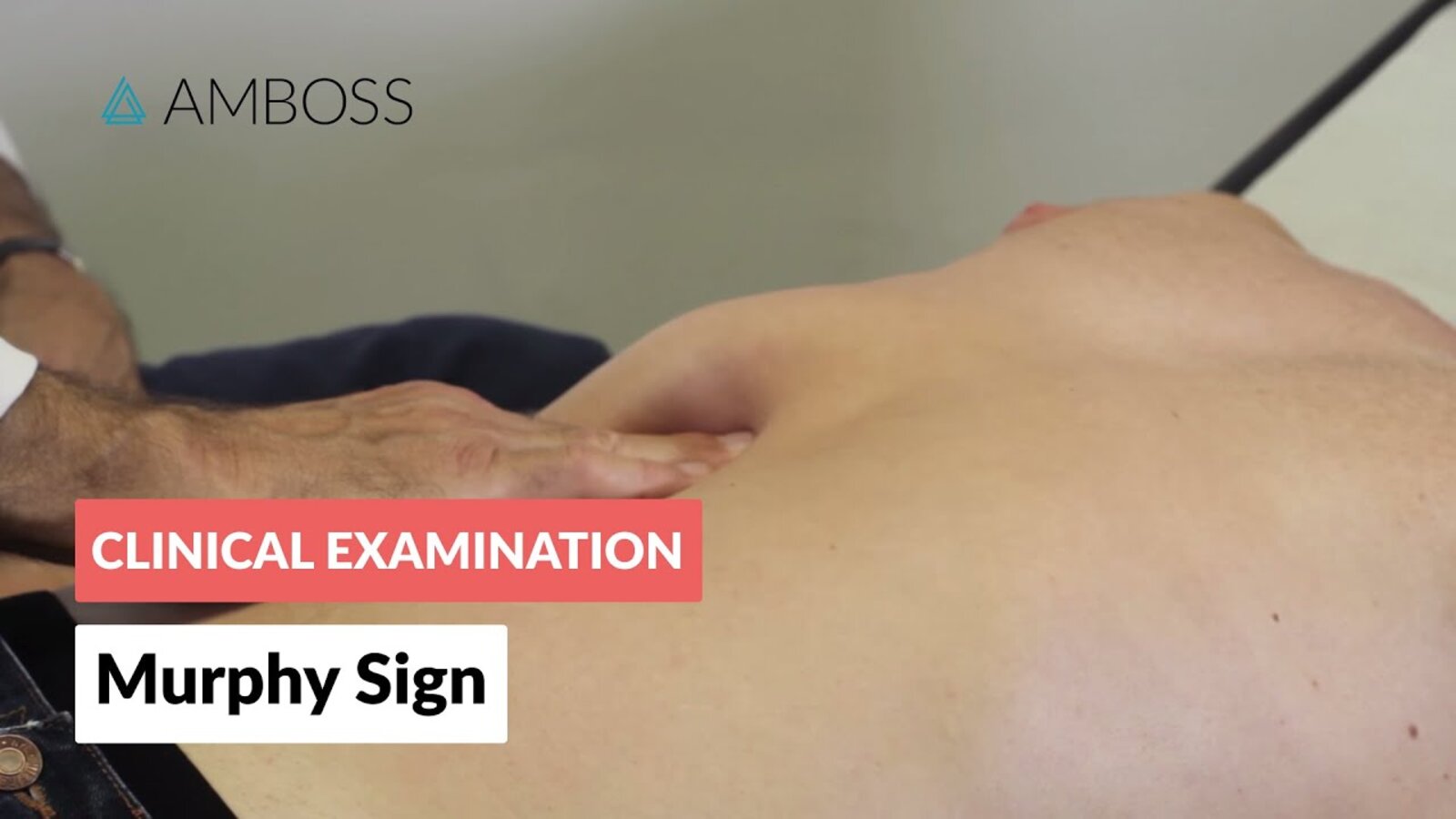
Positive Murphy sign: sudden pausing during inspiration upon deep palpation of the RUQ due to pain
- Murphy sign may be falsely negative in patients > 60 years. [5][6]
- Guarding
- Fever, malaise, anorexia
- Nausea and vomiting


Acute cholecystitis should always be suspected in a patient with a history of gallstones who presents with RUQ pain, fever, and leukocytosis
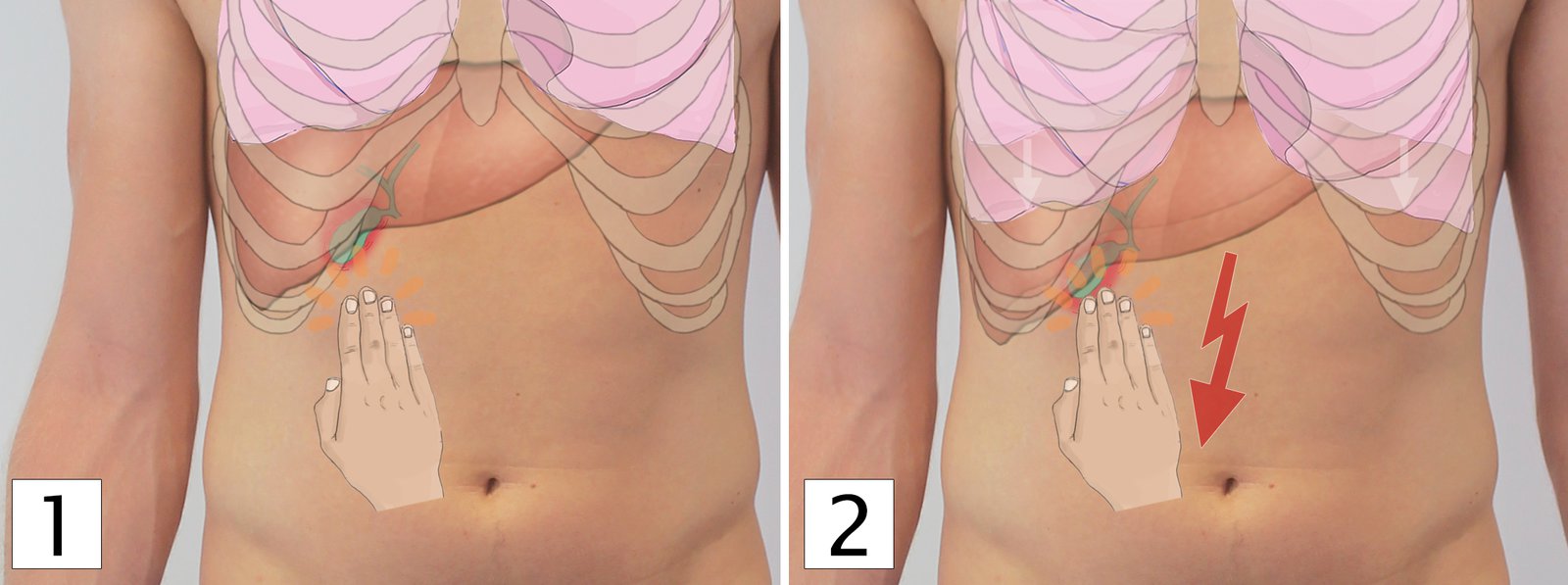
(1) The examiner positions their hands in the RUQ underneath the right costal arch, while the patient exhales.
(2) During inspiration both the liver and the gallbladder are pushed down towards the examiner's hand. If the patient experiences pain and therefore stops inspiration, the Murphy's sign is positive.
A positive Murphy's sign may indicate acute cholecystitis.
© AMBOSS
© AMBOSS
Subtypes and variants
Acute acalculous cholecystitis [3][7][8][9]
- Description: : an acute life-threatening necroinflammatory disorder of the gallbladder, usually seen in critically ill patients, that is not associated with gallstones
-
Incidence
- 5–10% of acute cholecystitis in adults [3]
- > 50% of acute cholecystitis in children [10]
- Etiology: : conditions predisposing to bile stasis and reduced perfusion of the gallbladder
-
Risk factors for acalculous cholecystitis [3][9]
- Multiorgan failure (critically ill patients)
- Severe trauma, burns
- Surgery
- Infection (e.g., CMV)
- Sepsis, septic shock
- Total parenteral nutrition
- Prolonged fasting
- Immunodeficiency
- Clinical features: similar to acute calculous cholecystitis
-
Diagnostics
- Laboratory studies and findings: similar to acute calculous cholecystitis
- Imaging [9][11]
-
Abdominal ultrasound: preferred initial imaging modality [8][11]
- Supportive findings
- Signs of gallbladder inflammation: gallbladder wall thickening (> 3–5 mm), pericholecystic fluid
- No evidence of cholelithiasis (sludge may be present)
- Supportive findings
-
HIDA scan: preferred confirmatory imaging modality if ultrasound is inconclusive [3][9][11]
- Supportive findings: similar to acute calculous cholecystitis (see HIDA scan in “Diagnostics” section)
- CT abdomen with IV contrast: an alternative to HIDA in patients with inconclusive ultrasound findings
- Supportive findings: similar to those on ultrasound
-
Abdominal ultrasound: preferred initial imaging modality [8][11]
-
Treatment [7][9]
- Initial supportive management: NPO, IV fluids, analgesics (see ''Treatment'' in ''Acute calculous cholecystitis” for details)
- IV antibiotics: see “Empiric antibiotic therapy for acute biliary infection”
- Source control
- Low surgical risk: emergency laparoscopic cholecystectomy
-
High surgical risk: percutaneous cholecystostomy
- If patients do not improve within 2–3 days, cholecystectomy should be performed.
Suspect acalculous cholecystitis in any critically ill patient with fever and RUQ tenderness.
Emphysematous cholecystitis (EC) [8][12][13]
- Description: : a rare but life-threatening form of acute cholecystitis characterized by air within the gallbladder wall that is caused by gas-forming bacteria (e.g., Clostridium spp., E.coli)
- Epidemiology: : rare; most commonly seen in older men with diabetes (esp. 50–70 years of age) [13]
-
Pathophysiology [8][13]
- Primary vascular compromise in the gallbladder (i.e., occlusion of the cystic artery) → ischemia of the gallbladder wall → necrosis → proliferation of gas-forming bacteria within the gallbladder wall or lumen
- Pathogens
- Most common: Clostridium species, Escherichia coli
- Others: Proteus vulgaris, Klebsiella aerogenes, Staphylococcus aureus, Streptococcus species, Klebsiella, Bacteroides fragilis
-
Risk factors [14]
- Hyperglycemia (e.g., diabetes mellitus)
- Immunosuppression
- Vascular disease (e.g., atherosclerosis, arterial embolism, vasculitis)
- Abdominal surgery, and trauma
-
Clinical features [13]
- Similar to acute calculous cholecystitis: fever, RUQ pain, referred pain
- Symptoms progress rapidly. [12]
- Associated with early gangrene and gallbladder perforation
-
Diagnostics
- Laboratory studies and findings: similar to those of acute calculous cholecystitis
- Imaging: The characteristic feature of EC on imaging is air within the gallbladder wall or lumen. [8][13]
- RUQ ultrasound : hyperechoic air shadows within the gallbladder wall, and within bile in the gallbladder lumen [12][13]
- Noncontrast CT abdomen : radiolucent shadows within the gallbladder wall, within bile, and within pericholecystic fluid [12]
- MRI abdomen : hypointense (signal void) areas within the gallbladder wall
- Abdominal x-ray : radiolucent rim outlining the gallbladder (pear-shaped radiolucency)
-
Treatment [13][15]
- Initial supportive management: NPO, IV fluids, analgesics (see ''Treatment'' section)
- Broad-spectrum IV antibiotics with anaerobic coverage: See Grade III community-acquired infection in “Empiric antibiotic therapy for acute biliary infection.”
- Emergency source control procedure
- Low surgical risk: emergency laparoscopic cholecystectomy
- High surgical risk: gallbladder drainage
Diagnosis
The diagnosis of acute cholecystitis is based on characteristic clinical features, systemic signs of inflammation (leukocytosis, ↑ CRP),; and evidence of gallbladder inflammation on imaging.
Fever and tachycardia are commonly absent in acute cholecystitis; maintain a high index of clinical suspicion! [16]
Approach
- Initial evaluation: laboratory studies and RUQ ultrasound (consider biliary POCUS if available)
- If ultrasound findings are inconclusive, consider abdominal CT scan, abdominal MRI, MRCP, or HIDA scan to confirm the diagnosis. [17]
- Assess for choledocholithiasis (see “Diagnosis of choledocholithiasis”).
- Once the diagnosis is confirmed, determine the severity (see “Severity grading of acute cholecystitis”).
| Diagnostic criteria for acute cholecystitis [12] | |
|---|---|
| Local signs of inflammation |
|
| Systemic signs of inflammation |
|
| Imaging findings |
|
Interpretation
| |
Laboratory studies [12][18]
-
Tests to support the clinical diagnosis
- CBC: Leukocytosis is most common, but WBC count may be normal in up to 40% of patients. [16]
- CRP: elevated
- Blood cultures: should be obtained, especially in patients with grade III acute cholecystitis (see “Severity grading of acute cholecystitis”) [19]
- Bile cultures: should be obtained in grade II-III acute cholecystitis in patients undergoing laparoscopic cholecystectomy or gallbladder drainage [19][20]
-
Tests to assess the severity of disease (see “Severity grading of acute cholecystitis”)
- Blood gas analysis: PaO2/FiO2 ratio < 300 in severely ill patients
- BMP: AKI, electrolyte derangements may be present in patients with severe disease
- PT/INR: coagulopathy in patients with severe disease
-
Tests to rule out related biliary comorbidities: should be obtained in all patients with suspected cholecystitis
-
LFTs [18][21]
- Mild elevations in AST and ALT are possible in acute cholecystitis.
- Signs of cholestasis (↑ bilirubin, ↑ ALP, ↑ GGT) are uncommon in cholecystitis; if present consider biliary obstruction (see ''Diagnosis of choledocholithiasis'' and ''Cholangitis'')
-
Lipase, amylase
- Mild elevation of amylase may be seen in acute cholecystitis [22]
- Elevation of lipase or amylase ≥ 3 times the normal is suggestive of acute biliary pancreatitis.
-
LFTs [18][21]
- Tests to rule out differential diagnoses: See “Diagnostic workup of acute abdominal pain.”
Imaging [11][12]
RUQ transabdominal ultrasound
See also “Biliary point-of-care ultrasound.”
- Indications: preferred initial imaging modality in suspected acute cholecystitis [11][12]
-
Characteristic findings [12]
-
Sonographic features of gallbladder inflammation
- Gallbladder wall thickening > 3–5 mm [8]
- Gallbladder distention (8–10 x 4 cm) [12][23]
- Gallbladder wall edema (double-wall sign): The innermost and outermost layers appear hyperechoic; edematous tissue appears as a hypoechoic layer in between.
- Sonographic Murphy sign: Tenderness upon compression of the gallbladder with the ultrasound transducer
- Pericholecystic free fluid
- Presence of gallstones and/or biliary sludge (see “Cholelithiasis” for details)
- In emphysematous cholecystitis, mural air appears as hyperechoic shadows within the gallbladder wall. [8]
-
Sonographic features of gallbladder inflammation
- Important consideration: The CBD should be assessed for choledocholithiasis (see ''Diagnosis of choledocholithiasis” for further details).



Cholescintigraphy [3][11][24]
Commonly referred to as hepatobiliary iminodiacetic acid scintigraphy or a HIDA scan.
- Indications: : preferred confirmatory test for suspected uncomplicated acute cholecystitis if ultrasound findings are inconclusive [11]
- Procedure: The radioactive tracer 99mTc-hepatic iminodiacetic acid is injected intravenously → selective uptake by hepatocytes → subsequent excretion into bile → bile with radiotracer enters the gallbladder if the cystic duct is patent → visualization of tracer within the gallbladder via a gamma camera [3]
-
Advantages
- High sensitivity (96%) and specificity (90%); considered the gold standard test to diagnose acute cholecystitis [24][25]
- Can differentiate between acute and chronic cholecystitis
-
Disadvantages
- Time-consuming
- Cannot identify complications of acute cholecystitis, if present
- Cannot be used to evaluate for potential differential diagnoses
- May not be widely available
-
Characteristic findings
- Normal: gallbladder visualized within 4 hours of administration of radioactive tracer
- Acute cholecystitis: gallbladder is not visualized within 4 hours [3]
MRI abdomen without and with IV contrast [11][23][26]
-
Indications
- Alternative to CT or HIDA scan in suspected acute cholecystitis with inconclusive ultrasound findings
- Either of the following in patients with contraindications to CT: [8][21]
- Suspected complications of cholecystitis
- Clinical diagnosis of acute cholecystitis unclear
- Suspected choledocholithiasis (MRCP) [21]
-
Characteristic findings: Similar to ultrasound findings
- Hyperintensity (T2) of the gallbladder wall and pericholecystic region, indicating inflammation
- Evidence of choledocholithiasis, if present (see ''Diagnosis of choledocholithiasis” for further details)
- Evidence of complications, such as emphysematous cholecystitis, empyema gallbladder, and gallbladder perforation (see ''Complications'' section)
CT abdomen with IV contrast [3][8]
-
Indications
- An alternative to MRI or HIDA scan in suspected acute cholecystitis with inconclusive ultrasound findings [11][26]
- Suspected emphysematous cholecystitis [12]
- Suspected complications of acute cholecystitis [8][12]
- Clinical diagnosis of acute cholecystitis unclear [3][8]
- Characteristic findings: similar to those on ultrasound and MRI


© AMBOSS
Ultrasound gallbladder (longitudinal plane)
Acoustic enhancement (green overlay) is seen distal to the gallbladder except where multiple small dependent hyperechoic calculi (yellow overlay) reflect the ultrasound beam and cast an acoustic shadow (green hatched overlay). Biliary sludge (yellow hatched overlay) is slightly hyperechoic compared to anechoic bile. The gallbladder wall is thickened (normal size: 1–2 mm) and has a layered appearance (red overlay), with central hypoechoic edema.
These findings in a patient with typical clinical features of RUQ pain strongly indicate acute calculous cholecystitis. Additional findings that would support a diagnosis of cholecystitis include an obstructing calculus, positive Murphy sign, pericholecystic fluid, gallbladder dilatation, and hyperemia of the gallbladder wall on color Doppler.
G: gallbladder; L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Ultrasound gallbladder
The gallbladder is dilated and its wall (green overlay) is thickened and striated (alternate hyperechoic and hypoechoic layers) as a result of edema. A calculus within dependent sludge in the neck produces posterior acoustic shadowing (red overlay) and has a highly reflective echogenic anterior surface (green hatched overlay).
Ultrasound findings in acute cholecystitis include wall thickening, dilatation, pericholecystic fluid, and a positive sonographic Murphy sign. The presence of multiple ultrasound findings increases diagnostic accuracy for cholecystitis.
L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Ultrasound gallbladder (transverse plane)
The gallbladder wall is thickened. Edema has produced a striated or layered appearance with hyperechoic inner and outer layers (green overlay) and a more hypoechoic middle layer (red overlay).
These features are suggestive of acute cholecystitis.
L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Ultrasound gallbladder (transverse plane)
The gallbladder wall (red overlay) is thickened, with outer and inner hyperechoic layers and a central hypoechoic layer. The edematous hypoechoic layer promotes the transmission of sound, which results in posterior acoustic enhancement (green overlay between dashed lines of ultrasound beam).
G: gallbladder lumen; L: liver
© AMBOSS
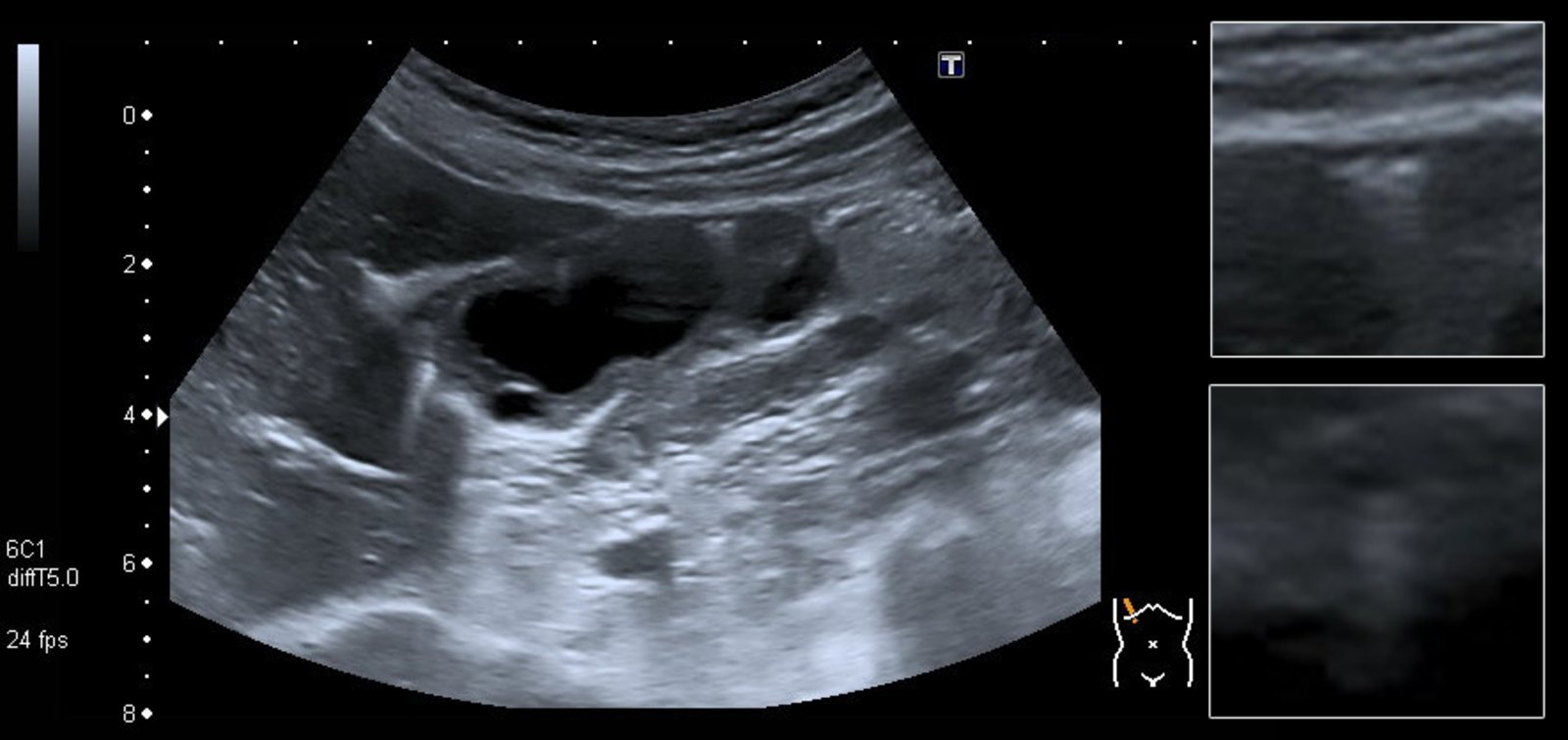
Ultrasound gallbladder (transabdominal; longitudinal plane)
The gallbladder is dilated and its wall (red overlay) is thickened. The layered appearance of the wall (hypoechoic stripe between two echogenic lines) is the result of inflammation and edema. Dependent biliary sludge (green overlay) is visible.
Many diseases cause gallbladder wall thickening. Ultrasound findings in acute acalculous cholecystitis can include mural thickening, dilatation, pericholecystic fluid, hyperemia, and a positive sonographic Murphy sign. The presence of several ultrasound criteria increases diagnostic accuracy for cholecystitis. In this case, the additional feature of gallbladder distention was helpful.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
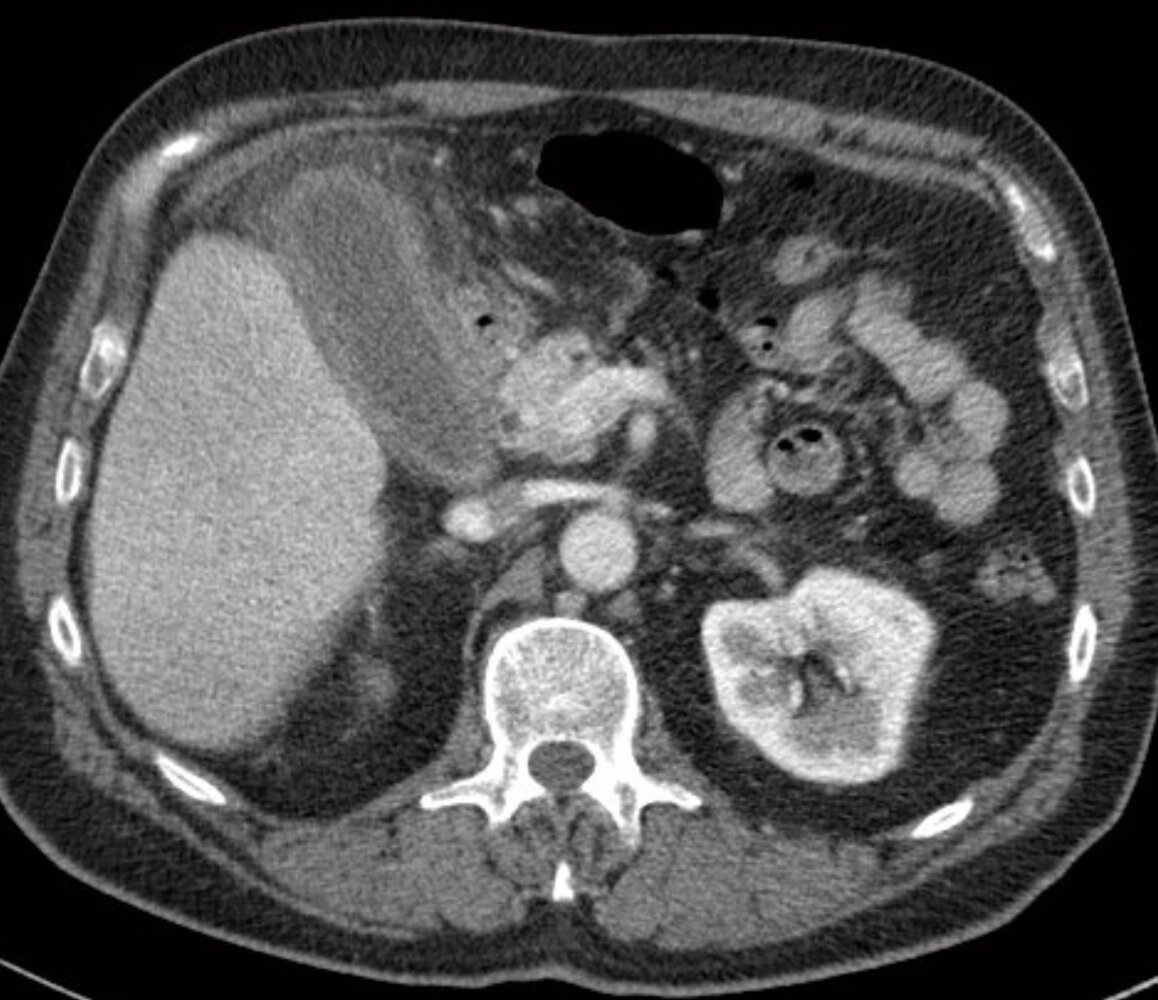
CT abdomen (with contrast; axial plane) of a patient with right upper quadrant pain and elevated WBC count
Inflammatory fatty stranding (yellow overlay) surrounds an enhanced thickened gallbladder wall, which is consistent with cholecystitis. Inflammation also involves the adjacent duodenum (blue hatched overlay) and hepatic flexure. The liver shows heterogeneous enhancement with reactive hyperemia (examples indicated by red overlay) adjacent to the gallbladder. The gallbladder is not dilated, and no calculi are seen. There is no intrahepatic or extrahepatic biliary ductal dilatation.
Additional CT findings include free peritoneal fluid (blue overlay), colonic diverticula (examples indicated by green arrowheads), small hypodense liver lesions, fat-containing umbilical (green arrow) and left inguinal (white arrow) hernias, and bilateral atelectasis or scarring (examples indicated by red overlay) in the lower lungs.
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
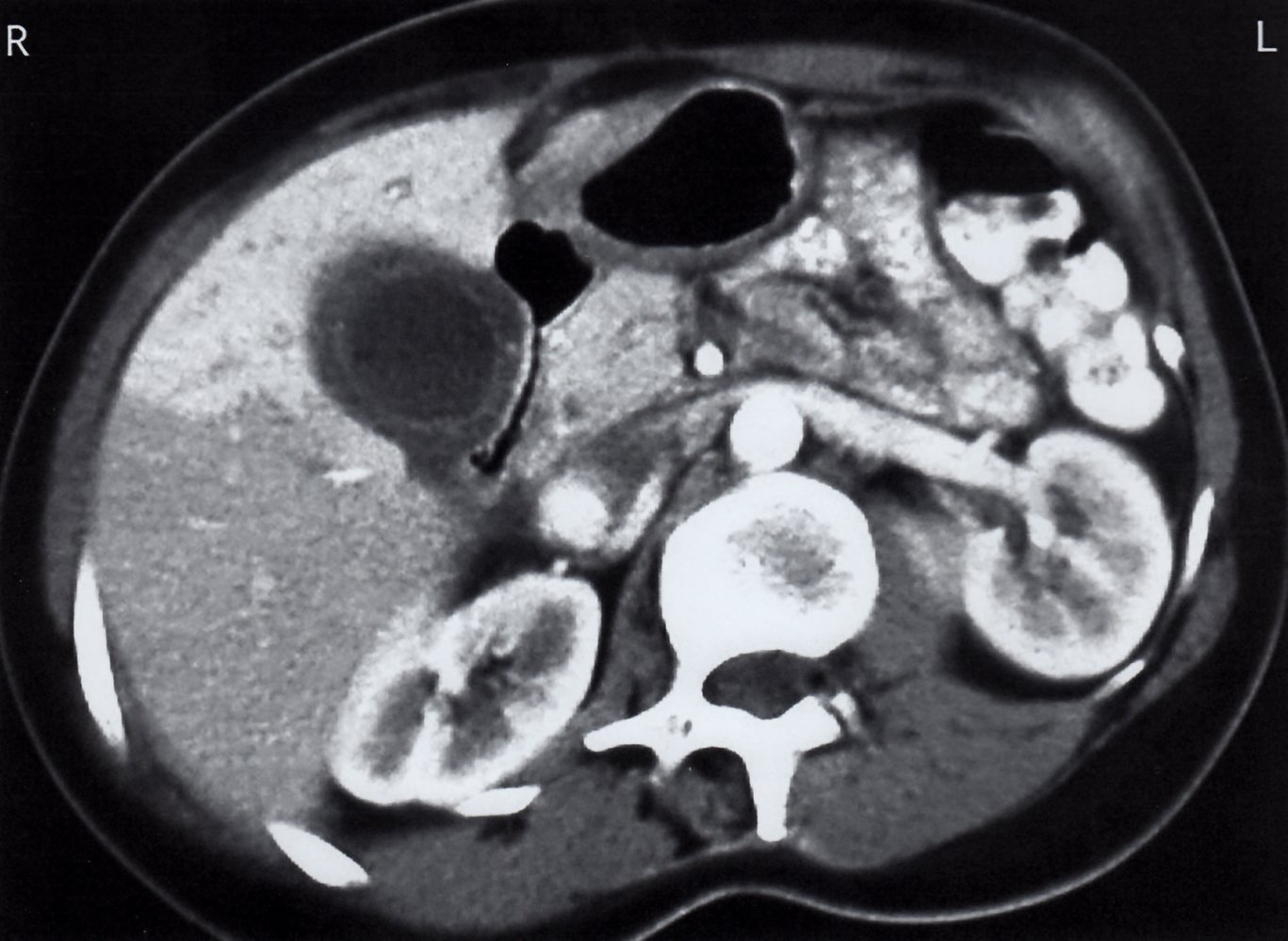
CT abdomen (with IV and oral contrast; axial plane)
The gallbladder wall is thickened (green overlay) and has a layered appearance, with hypodense edema between layers of mucosa and serosa. Hyperenhancement of the adjacent liver (red overlay) may reflect increased hepatic arterial flow in response to gallbladder inflammation.
K: kidney; S: stomach; B: small bowel
Source: © IMPP
Differential diagnoses
- See “Differential diagnosis of acute abdominal pain.”
- See “Overview of biliary disease.”
-
RUQ pain with fever
- Acute cholangitis
- Liver abscess
- Acute hepatitis
- Acute necrotizing pancreatitis
- Acalculous cholecystitis
- Chronic cholecystitis
- Bile leak (Iatrogenic)
-
RUQ pain without fever
- Biliary colic
- PUD
- Acute gastritis
- Acute pancreatitis
- Chronic pancreatitis
- Acute GERD
- Sphincter of Oddi dysfunction
- Congestive hepatopathy
- Nephrolithiasis
-
Malignancy
- HCC
- Cholangiocarcinoma
- Gallbladder cancer
- Pancreatic cancer
The differential diagnoses listed here are not exhaustive.
Severity grading
Stratify the severity of acute cholecystitis to determine the best approach to treatment. [12][27]
| Severity grading of acute cholecystitis [12] | |
|---|---|
| Grades of severity | Grading criteria |
| Grade I (Mild acute cholecystitis) |
|
| Grade II (Moderate acute cholecystitis) |
|
| Grade III (Severe acute cholecystitis) |
|
Treatment
Empiric antibiotic therapy and cholecystectomy are the mainstays of treatment for acute cholecystitis after initial supportive therapy.
Initial management [19][27][28]
- Screen patients for signs of sepsis or shock.
- Provide immediate hemodynamic support (e.g., IV fluid resuscitation) and respiratory support (e.g., oxygen therapy) if necessary.
- Start empiric antibiotic therapy for acute biliary infection.
- Provide initial supportive therapy for acute biliary disease: e.g., analgesia, antiemetics, electrolyte repletion, consider NG tube insertion.
- Maintain NPO status.
- Consult general surgery to determine:
- Surgical risk using the ASA-PS or Charlson comorbidity index (CCI).
- Definitive management and disposition based on severity grading of acute cholecystitis and risk of complications (see “Disposition”).
- Identify and treat concurrent choledocholithiasis (see “Diagnosis of choledocholithiasis”).
- Monitoring and reevaluation
- Adjust monitoring level to individual patient needs.
- If there is early deterioration, perform ABCDE assessment.
- Consider the development of complications (e.g., gallbladder perforation) or other differential diagnoses (e.g., acute cholangitis).
- Consider ICU consult.

Definitive management [27][28][29][30]
The initial procedure and duration of antibiotic therapy depend on severity grading of acute cholecystitis, patient's individual surgical risk, and presence of complications.
-
Laparoscopic cholecystectomy
- Preferred approach if expertise is available
- Perform as soon as possible, unless operative and anesthesia risks outweigh the benefits of urgent surgery.
- Conversion to open cholecystectomy may be required depending on intraoperative findings [27]
-
Gallbladder drainage procedures (e.g., percutaneous cholecystostomy) typically performed as a temporizing measure for:
- Unstable or clinically deteriorating patients: e.g., grade II–III acute cholecystitis [30][31]
- Frail patients or those at high risk of surgical complications
-
Postprocedural antibiotics
- Consider prolonging the duration of therapy (beyond the standard recommendation) in patients with:
- Signs of sepsis (e.g., persistent fever, stable or increasing leukocytosis)
- Evidence of biliary tract obstruction
- Complications (e.g., pericholecystic abscess).
- Tailor agent to bile and/or blood cultures as soon as available.
- Consider prolonging the duration of therapy (beyond the standard recommendation) in patients with:
Perform preoperative or postoperative stone extraction in patients with concurrent choledocholithiasis.
Grade I acute cholecystitis
-
Low surgical risk
- Early laparoscopic cholecystectomy
- Postoperative antibiotics not required
-
High surgical risk
- Early intervention
- Early laparoscopic cholecystectomy
- Discontinue antibiotics 24 hours after surgery.
- OR conservative approach
- Continue antibiotics until symptomatic improvement [27][28]
- Arrange interval cholecystectomy
- Early intervention
Grade II acute cholecystitis
-
Improvement with initial management
- Low surgical risk
- Early laparoscopic cholecystectomy
- Discontinue antibiotics 24 hours after surgery.
- High surgical risk :
- Continue antibiotics until symptomatic improvement.
- Arrange interval cholecystectomy
- Low surgical risk
-
Deterioration despite initial management
- Urgent gallbladder drainage followed by interval cholecystectomy
- Continue antibiotics for a total of 7 days. [32]
Grade III acute cholecystitis
-
Low surgical risk
- Early laparoscopic cholecystectomy if there is an adequate response to initial supportive care
- Continue antibiotics for 4–7 days after surgery. [33]
-
High surgical risk
-
Urgent gallbladder drainage, followed by:
- Interval cholecystectomy
- OR observation
- Continue antibiotics for a total of 7 days. [32]
-
Urgent gallbladder drainage, followed by:
Procedures
Laparoscopic cholecystectomy
- Indication: gold standard of treatment for acute calculous cholecystitis [27]
-
Timing: depends on surgical and anesthesia risks, disease severity, and symptom duration
-
Early laparoscopic cholecystectomy: performed within 10 days of symptom onset; preferably within the initial 24–72 hours [27][29]
- Indication: symptom duration of ≤ 10 days in patients with low surgical and anesthesia risk(s) [27]
- Contraindications
- High surgical or anesthesia risks
- Symptom duration > 10 days
-
Interval laparoscopic cholecystectomy (delayed lap. chole)
- Performed 45 days after resolution of symptoms [27]
- Indications
- High surgical or anesthesia risk
- Symptom duration > 10 days
-
Early laparoscopic cholecystectomy: performed within 10 days of symptom onset; preferably within the initial 24–72 hours [27][29]
Gallbladder drainage
- Indication: temporizing, minimally invasive measures in high surgical-risk patients not responding to conservative management [34]
- Contraindication: uncontrolled bleeding diathesis
-
Options
- Percutaneous cholecystostomy: image-guided placement of a catheter (cholecystostomy tube) into the gallbladder under local anesthesia through the abdominal wall to provide biliary drainage [34][35]
- Endoscopic gallbladder stenting: may be preferred over percutaneous cholecystostomy if endoscopy operator expertise is available as it is less invasive. [36][37][38]
Disposition [28]
All patients with acute cholecystitis require inpatient management.
- Grade I acute cholecystitis: healthcare facility with the ability to perform laparoscopic cholecystectomy
- Grade II acute cholecystitis: advanced healthcare facility with access to urgent gallbladder drainage and surgical expertise to handle a difficult laparoscopic cholecystectomy.
- Grade III acute cholecystitis: same as for grade II PLUS access to intensive care.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Antibiotic therapy for acute biliary infection
General principles [19]
-
Important considerations
- Obtain blood cultures prior to administering antibiotics, especially in patients with severe biliary infection.
- Obtain bile cultures at the beginning of any drainage procedure.
- Tailor antibiotic therapy to sensitivity reports as early as possible. [33]
- Switch to oral antibiotics, if feasible, once improvement is evident. [39]
-
Required coverage
- Gram-negative coverage: Escherichia coli (most common), Klebsiella spp., Enterobacter spp., Pseudomonas spp.
- Anaerobic coverage is recommended if biliary-enteric anastomosis is suspected or identified.
- Consider Enterococcus spp. coverage in grade III community-acquired and healthcare-associated infection.
-
Choice of empiric antibiotic: should be determined by the following parameters
- Community-acquired or healthcare-associated infection
- Severity of infection (see “Severity grading of acute cholecystitis” or “Severity grading of acute cholangitis” for details on grading)
- Local resistance patterns (local antibiogram)
- If a biliary-enteric anastomosis is suspected
-
Timing of antibiotic administration
- Septic shock: within one hour of presentation
- Other patients: within six hours of presentation
-
Duration of therapy
- Grade I acute cholecystitis, grade II acute cholecystitis: up to 24 hours after early lap. chole.
- Grade III acute cholecystitis and all grades of community-acquired acute cholangitis: 4–7 days after early lap. chole or until symptomatic improvement (if patient is managed conservatively).
- For patients who undergo urgent gallbladder drainage: continue antibiotics for a total of 7 days. [32]
- All grades of healthcare-associated cholangitis and cholecystitis with gram-positive bacteremia known to cause infective endocarditis : consider 14 days of treatment.
Recommended empiric regimen [19]
| Empiric antibiotic therapy for acute biliary infection | |||
|---|---|---|---|
| Class of infection | Severity of infection | Suggested single-agent empiric regimen | Suggested combination empiric regimen |
| Community-acquired biliary infection | Grade I |
|
|
| Grade II |
|
|
|
| Grade III |
|
|
|
| Healthcare-associated biliary infection (any grade) |
|
||
| Suspected multi-drug resistant organism infection |
|
||
Many ESBL-producing gram-negative organisms are resistant to fluoroquinolones.
Resistance of E. coli to ampicillin-sulbactam is becoming more common, especially in North America. Consider local resistance rates carefully before choosing an empiric antibiotic regimen.
Complications
Gangrenous cholecystitis [8][40][41]
- Definition: ischemic necrosis of the gallbladder
- Etiology: most common complication of acute cholecystitis [8]
- Clinical features: difficult to distinguish from uncomplicated acute cholecystitis
-
Imaging
- Ultrasound: features of acute cholecystitis plus echogenic membranes floating within the gallbladder lumen
- CT with IV contrast: nonenhancement of the gallbladder wall
- Treatment: emergency laparoscopic cholecystectomy and empiric antibiotic therapy for biliary infection

Gallbladder perforation [8][41][42]
- Definition: break in the continuity of the gallbladder wall, typically as a consequence of ischemic necrosis
-
Clinical features: variable; symptoms typically progress rapidly
- May be indistinguishable from uncomplicated acute cholecystitis
- Potentially accompanied by a palpable RUQ mass and/or signs of generalized peritonitis
- Imaging : focal defect in the gallbladder wall; extraluminal stone may be visualized
- Treatment: emergency laparoscopic cholecystectomy and empiric antibiotic therapy for biliary infection
Cholecystoenteric fistula
- See “Cholecystoenteric fistula” in “Fistula.”
Gallbladder empyema (suppurative cholecystitis) [8]
- Definition: distended pus-filled gallbladder
- Clinical features: similar to uncomplicated acute cholecystitis
- Imaging: gallbladder distention with hyperechoic (on ultrasound) or hyperdense (on CT abdomen with IV contrast) material within its lumen
-
Treatment [43]
- Empiric antibiotic therapy for biliary infection
- Emergency source control procedure
- Low surgical risk: laparoscopic cholecystectomy
- High surgical risk: image-guided percutaneous drainage of empyema followed by interval laparoscopic cholecystectomy
Chronic cholecystitis [4][8][44]
- Definition: chronic inflammation of the gallbladder
-
Etiology
- Chronic irritation of gallbladder mucosa by cholelithiasis
- Recurrent attacks of acute cholecystitis
- Clinical features: recurrent symptoms similar to acute cholecystitis but typically less severe and often self-limiting
-
Diagnostics
- Laboratory studies: may be normal [44]
-
Ultrasound abdomen or CT abdomen with IV contrast:
- Thickened gallbladder wall
- No evidence acute inflammatory changes (e.g., pericholecystic fluid);
- Cholelithiasis commonly present
- HIDA scan: delayed visualization of the gallbladder [45]
- All patients should also be evaluated for choledocholithiasis before treatment (see ''Imaging'' in “Choledocholithiasis”).
- Treatment: elective laparoscopic cholecystectomy [8][46]
-
Complications [8]
-
Porcelain gallbladder [8][45][47]
- Definition: calcification of the gallbladder wall due to chronic inflammation
- Imaging (x-ray or noncontrast CT abdomen): focal or diffuse hyperdensity (radiopaque appearance) of the gallbladder wall
- Clinical significance: a risk factor for gallbladder cancer [48]
- Treatment: conservative management or laparoscopic cholecystectomy based on symptoms, pattern of gallbladder calcification, and comorbidities [49][50]
- Gallbladder cancer [51]
- Cholecystoenteric fistula and gallstone ileus
-
Porcelain gallbladder [8][45][47]



Chronic gallbladder inflammation increases the risk of gallbladder carcinoma, especially when porcelain gallbladder is present.
Other [8]
- Gallstone ileus
- Pericholecystic abscess
- Subhepatic abscess
- Pyogenic liver abscess
- Hemorrhagic cholecystitis [8]
- Gallbladder cancer
We list the most important complications. The selection is not exhaustive.
Transabdominal ultrasound (right upper quadrant; longitudinal view)
The gallbladder wall is thickened (green outline). Its inner and outer walls appear hyperechoic and the intervening tissue (between the white lines) appears hypoechoic, indicating acute inflammation of the gallbladder wall. Hyperechoic areas within the gallbladder wall (blue and yellow boxes) indicate intramural gas (green overlay in magnified boxes).
Intramural air is a characteristic feature of acute emphysematous cholecystitis, which is a variant of acute cholecystitis caused by infection with gas-producing organisms.
G: gallbladder; L: liver; In: intestines
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
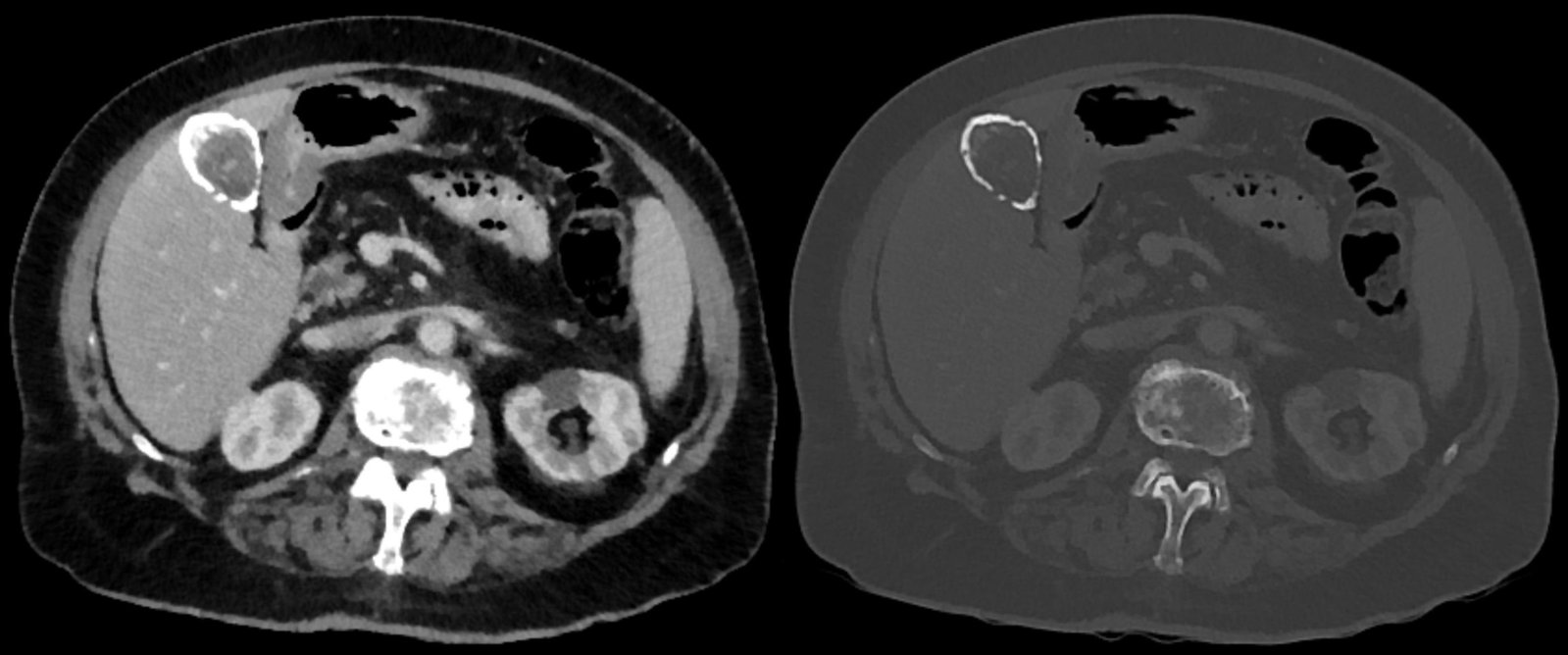
CT abdomen (with contrast; axial plane; left: soft tissue window; right: bone window)
The calcified wall of the gallbladder is seen as a hyperdense oval outline (green overlay) in the gallbladder fossa. The greater density of the gallbladder calcification compared to the intravenous contrast in several other organs is more conspicuous on the bone window than the soft tissue window.
The calcification is diagnostic of a porcelain gallbladder, a rare complication of chronic gallbladder inflammation.
L: Liver; IVC: Inferior vena cava; LK: Left kidney; RK: Right kidney; S: Spleen; Arrow: Kidney cyst
Source: “Porzellangallenblase - 88j - CT axial WT und KF - 001” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
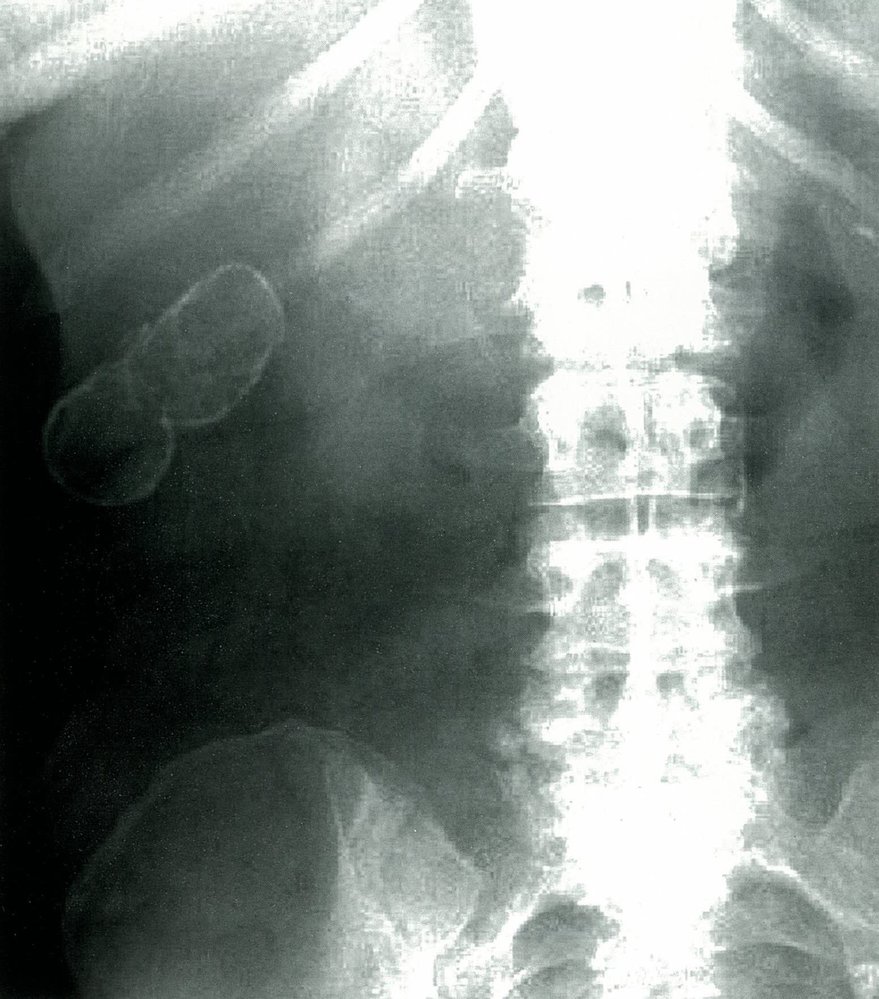
X-ray abdomen (AP view)
A well-defined oval lesion is visible in the right upper quadrant of the abdomen, encapsulated in a thin rim of radiodense material, indicating intramural calcification of the gallbladder.
This is the typical appearance of porcelain gallbladder, which is a consequence of chronic gallbladder inflammation that is usually secondary to cholelithiasis.
Source: © IMPP

Ultrasound right upper quadrant (left: portal vein and common bile duct; right: gallbladder) of a patient with elevated liver enzymes
The left image shows normal directional blood flow within the portal vein (red) and a dilated common bile duct (CBD) with a diameter of 0.94 cm. The right image shows marked posterior shadowing (indicated by dashed lines) and deep to hyperechoic areas of calcification (yellow overlay) along the anterior gallbladder wall. Additional small hyperechoic areas (indicated by arrowheads) at the posterior right aspect of the image in the region of the gallbladder also proved to be wall calcifications on CT (not shown).
A hyperechoic gallbladder wall with posterior acoustic shadowing is seen with porcelain gallbladder. The appearance should be distinguished from a gallbladder filled with calculi, which produces the wall-echo-shadow sign.
Source: “Fig. 2 and 3, in: A Case Report on Detecting Porcelain Gallbladder form Wall-Echo-Shadow Sign on Point-of-Care Ultrasound” by Fares Al-Khouja; Proma Mazumde; John Moeller, JETem, licensed under CC BY 4.0. Modifications: - image is a product of two separate images - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Special patient groups
Acute cholecystitis in pregnancy [52][53]
- Acute cholecystitis is the second most common indication for nonobstetric surgery in pregnant individuals after acute appendicitis. [52][53]
- Clinical features are largely similar to those in nonpregnant individuals; Murphy sign may be absent in pregnant individuals. [53][54]
- Additional differential diagnoses of acute cholecystitis to consider in pregnant individuals include: [55]
- HELLP syndrome (hemolysis, elevated liver enzymes, low platelets)
- Acute fatty liver of pregnancy
- Pyelonephritis
- Appendicitis
Depending on the size and position of the uterus, Murphy sign may be absent in pregnant patients with acute cholecystitis. [53]
Diagnostic evaluation and treatment of cholecystitis should not be delayed during pregnancy as the condition can have negative maternal and fetal outcomes. [52][56]
Diagnostics [53]
The diagnostic approach for cholecystitis during pregnancy is similar to that for nonpregnant individuals, with the following additional considerations.
- Preferred imaging modalities: RUQ ultrasound or MRI abdomen without contrast [17][57]
- Obtain additional diagnostics as indicated by clinical examination and imaging findings (e.g., for suspected choledocholithiasis and/or biliary obstruction).
- MRCP [53]
- ERCP [54][58]
- Intraoperative cholangiography during cholecystectomy [53]
- See “Diagnostic criteria for acute cholecystitis.”
If a diagnostic or therapeutic procedure involving ionizing radiation is deemed necessary during pregnancy, implement strategies to minimize fetal radiation exposure, such as shielding the pelvis and reducing fluoroscopy time. [53][54][57]
Management [52][53][59]
Treatment of acute cholecystitis is similar in pregnant and nonpregnant individuals, with the following considerations.
- Early laparoscopic cholecystectomy is the preferred treatment for all trimesters. [52][54][59]
- For patients at high surgical risk, consider percutaneous or endoscopic gallbladder drainage. [54][60]
- Consider corticosteroids to induce fetal lung maturity if indicated. [56]
- Assess for risk factors for venous thromboembolism and provide appropriate VTE prophylaxis. [56]
Conservative management of acute cholecystitis in pregnancy is associated with a higher risk of recurrence and complications than laparoscopic cholecystectomy. [59]
Acute cholecystitis in children [10][17][61]
Epidemiology
- Uncommon in children [17][61]
- Incidence increases with age [62]
Etiology [10][17][62][63]
-
Acalculous cholecystitis (most common) [10][62]
- Risk factors for acalculous cholecystitis are similar to those in adults.
- Additional risk factors in children include:
- Infection (e.g., Epstein-Barr virus, hepatitis A virus, Ascaris lumbricoides)
- Systemic disease (e.g., Kawasaki disease, malignancy)
- Anatomical anomalies
- Genetic conditions (e.g., cystic fibrosis, galactosemia)
-
Cholelithiasis (uncommon in children): often caused by an underlying condition, including [61][62]
- Metabolic disease (e.g., diabetes, pediatric obesity) [10][64]
- Hemolytic disease (e.g., sickle cell, hereditary spherocytosis)
- Cystic fibrosis
- Treatment of pediatric malignancies [65]
Acaclulous cholecystitis is the most common cause of acute cholecystitis in children. In contrast, cholelithiasis is the most common cause of acute cholecystitis in adults. [10][62]
Clinical features [63][64]
- Clinical features of acute cholecystitis are similar in adults and children
- Features of the underlying condition may mask features of acute cholecystitis. [10]
Consider acaclulous cholecystitis in all children with acute RUQ pain, especially those with a concurrent severe illness or recent history of trauma or surgery. [66]
Diagnosis [10][17]
- Diagnosis of calculous cholecystitis and acalculous cholecystitis is the same in children and adults.
- Identify the underlying etiology: Order additional diagnostics based on clinical suspicion.
Treatment [64][66][67]
- Urgent consult or referral to a specialist (e.g., pediatric surgery, gastroenterology, critical care) for management
- Initial management [64]
- Bowel rest
- Initial supportive therapy of acute biliary disease
- Broad spectrum IV empiric antibiotic therapy for acute biliary infection
- Further management depends on the type of cholecystitis.
- Acalculous cholecystitis: Treat the underlying condition. [64][66][67]
- Acute calculous cholecystitis: cholecystectomy [68][69]
Acalculous cholecystitis is often managed conservatively in children, while cholecystectomy is typically recommended in adults.. [66][67]
Prognosis
Acute acalculous cholecystitis may progress to chronic cholecystitis if untreated. [62][64]
External Resources
- 2024 AGA Clinical Practice Update on Pregnancy-Related Gastrointestinal and Liver Disease.
- 2024 IDSA Clinical Practice Guideline Update on Complicated Intra-abdominal Infections: Risk Assessment, Diagnostic Imaging, and Microbiological Evaluation in Adults, Children, and Pregnant People
- 2024 SAGES guidelines for the use of laparoscopy during pregnancy.
- 2019 AAST Summaries of Guidelines on Emergency General Surgery for Appendicitis, Acute Cholecystitis, Acute Diverticulitis, Acute Pancreatitis, and Small Bowel Obstruction
- 2018 Tokyo Guidelines: Diagnostic Criteria and Severity Grading of Acute Cholecystitis
- 2018 Tokyo Guidelines: Antimicrobial Therapy for Acute Cholangitis and Cholecystitis
- 2018 Tokyo Guidelines: Flowchart for the Management of Acute Cholecystitis
- 2017 WSES/SICG Guidelines: Acute Calculous Cholecystitis in Elderly Population
- 2017 American College of Gastroenterology Clinical Guideline on Liver Disease and Pregnancy
- 2016 EASL Clinical Practice Guidelines on the Prevention, Diagnosis and Treatment of Gallstones
- 2016 WSES Guidelines on Acute Calculous Cholecystitis
- CME Program Overview
- Internet Point-of-Care CME
References
- Yokoe M, Hata J, Takada T, et al. "Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos)". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :41-54. (2018)
- Schuster KM, Holena DN, Salim A, Savage S, Crandall M. "American Association for the Surgery of Trauma emergency general surgery guideline summaries 2018: acute appendicitis, acute cholecystitis, acute diverticulitis, acute pancreatitis, and small bowel obstruction.". Trauma surgery & acute care open. 4(1). :e000281. (2019)
- Gomi H, Solomkin JS, Schlossberg D, et al. "Tokyo Guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :3-16. (2018)
- Orna Nitzan, Yuri Brodsky, Hana Edelstein, et al. "Microbiologic Data in Acute Cholecystitis: Ten Years' Experience from Bile Cultures Obtained during Percutaneous Cholecystostomy". Surg Infect (Larchmt). 18(3). :345-349. (2017)
- Zimmer V, Lammert F. "Acute Bacterial Cholangitis". Visceral Medicine. 31(3). :166-172. (2015)
- Loftus TJ, Brakenridge SC, Dessaigne CG, et al. "Antibiotics May be Safely Discontinued Within One Week of Percutaneous Cholecystostomy.". World J Surg. 41(5). :1239-1245. (2017)
- "Contributor Disclosures - Acute cholecystitis. All of the relevant financial relationships listed for the following individuals have been mitigated: Jan Schlebes (medical editor, is a shareholder in Fresenius SE & Co KGaA). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy"
- Chandrasekhara V, Elmunzer BJ, Khashab M, Muthusamy M. "Clinical Gastrointestinal Endoscopy". Elsevier. (2018). ISBN: 9780323415095
- Fischer JE, Bland KI. "Mastery of Surgery". Lippincott Williams & Wilkins. 1(5). (2006). ISBN: 9780781771658
- Odze RD, Goldblum JR. "Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas". Elsevier Health Sciences. (2009). ISBN: 9781416040590
- McGee SR. "Evidence-based Physical Diagnosis". Elsevier Health Sciences. (2012). ISBN: 9781437722079
- Pisano M, Ceresoli M, Cimbanassi S, et al. "2017 WSES and SICG guidelines on acute calcolous cholecystitis in elderly population". World Journal of Emergency Surgery. 14(1). (2019)
- Balmadrid B. "Recent advances in management of acalculous cholecystitis.". F1000Research. 7. (2018)
- Smith EA, Dillman JR, Elsayes KM, Menias CO, Bude RO. "Cross-Sectional Imaging of Acute and Chronic Gallbladder Inflammatory Disease". American Journal of Roentgenology. 192(1). :188-196. (2009)
- Huffman JL, Schenker S. "Acute Acalculous Cholecystitis: A Review". Clinical Gastroenterology and Hepatology. 8(1). :15-22. (2010)
- Rothstein DH, Harmon CM. "Gallbladder disease in children". Semin Pediatr Surg. 25(4). :225-231. (2016)
- "American College of Radiology ACR Appropriateness Criteria® Right Upper Quadrant Pain". https://acsearch.acr.org/docs/69474/Narrative/. [2018-01-01]
- Safwan M, Penny SM. "Emphysematous Cholecystitis". Journal of Diagnostic Medical Sonography. 32(3). :131-137. (2016)
- Feldman M, Friedman LS, Brandt LJ. "Sleisenger and Fordtran's Gastrointestinal and Liver Disease- 2 Volume Set". Elsevier. (2020). ISBN: 9780323609623
- Chen MY, Lu C, Wang YF, Cai XJ. "Emphysematous cholecystitis in a young male without predisposing factors: A case report.". Medicine. 95(44). :e5367. (2016)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Bonomo RA, Chow AW, Edwards MS, et al. "2024 Clinical Practice Guideline Update by the Infectious Diseases Society of America on Complicated Intra-abdominal Infections: Risk Assessment, Diagnostic Imaging, and Microbiological Evaluation in Adults, Children, and Pregnant People". Clin Infect Dis. (2024)
- Ansaloni L, Pisano M, Coccolini F, et al. "2016 WSES guidelines on acute calculous cholecystitis". World J Emerg Surg. 11(1). (2016)
- Mencarini L, Vestito A, Zagari RM, Montagnani M. "The Diagnosis and Treatment of Acute Cholecystitis: A Comprehensive Narrative Review for a Practical Approach". J Clin Med. 13(9). :2695. (2024)
- Bope ET, Kellerman RD. "Conn's Current Therapy 2016". Elsevier Health Sciences. (2015). ISBN: 9780323355353
- Cameron P, Jelinek G, Kelly A-M, Murray L, Brown AFT. "Textbook of Adult Emergency Medicine E-Book". Elsevier Health Sciences. (2011). ISBN: 9780702049316
- Bates DDB, LeBedis CA, Soto JA, Gupta A. "Use of Magnetic Resonance in Pancreaticobiliary Emergencies". Magn Reson Imaging Clin N Am. 24(2). :433-448. (2016)
- Rodriguez LE, Santaliz-Ruiz LE, De La Torre-Bisot G, et al. "Clinical implications of hepatobiliary scintigraphy and ultrasound in the diagnosis of acute cholecystitis". International Journal of Surgery. 35. :196-200. (2016)
- Indar AA, Beckingham IJ. "Acute cholecystitis.". BMJ. 325(7365). :639-43. (2002)
- Hanbidge AE, Buckler PM, O’Malley ME, Wilson SR. "From the RSNA Refresher Courses". RadioGraphics. 24(4). :1117-1135. (2004)
- Okamoto K, Suzuki K, Takada T, et al. "Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis". Journal of Hepatobiliary Pancreatic Sciences. 25(1). :55-72. (2017)
- Gutt CN, Encke J, Köninger J, et al. "Acute Cholecystitis". Ann Surg. 258(3). :385-393. (2013)
- Gurusamy KS, Rossi M, Davidson BR. "Percutaneous cholecystostomy for high-risk surgical patients with acute calculous cholecystitis". Cochrane Database of Systematic Reviews. (2013)
- Viste A, Jensen D, Angelsen JH, Hoem D. "Percutaneous cholecystostomy in acute cholecystitis; a retrospective analysis of a large series of 104 patients". BMC Surg. 15(1). (2015)
- John Cameron, Andrew Cameron. "Current Surgical Therapy 13th Edition". Elsevier. (2019). ISBN: 9780323640619
- M.W. Little, J.H. Briggs, C.R. Tapping, et al. "Percutaneous cholecystostomy: The radiologist's role in treating acute cholecystitis". Clin Radiol. 68(7). :654-660. (2013)
- Widmer J, Alvarez P, Sharaiha RZ, et al. "Endoscopic Gallbladder Drainage for Acute Cholecystitis.". Clinical endoscopy. 48(5). :411-20. (2015)
- Mutignani M, Iacopini F, Perri V, et al. "Endoscopic gallbladder drainage for acute cholecystitis: technical and clinical results.". Endoscopy. 41(6). :539-46. (2009)
- Chan JHY, Teoh AYB. "Current Status of Endoscopic Gallbladder Drainage.". Clinical endoscopy. 51(2). :150-155. (2018)
- Önder A, Kapan M, Ülger BV, et al. "Gangrenous cholecystitis: mortality and risk factors.". Int Surg. 100(2). :254-60. (2015)
- Patel NB, Oto A, Thomas S. "Multidetector CT of Emergent Biliary Pathologic Conditions". RadioGraphics. 33(7). :1867-1888. (2013)
- Derici H, Kara C, Bozdag AD, et al. "Diagnosis and treatment of gallbladder perforation.". World journal of gastroenterology. 12(48). :7832-6. (2006)
- Tseng LJ, Tsai CC, Mo LR, et al. "Palliative percutaneous transhepatic gallbladder drainage of gallbladder empyema before laparoscopic cholecystectomy.". Hepatogastroenterology. 47(34). :932-6. (2000)
- Buttaro TM, Trybulski J, Sandberg-Cook J, Polgar-Bailey P. "Primary Care". Mosby. (2016). ISBN: 9780323355018
- O’Connor OJ, Maher MM. "Imaging of Cholecystitis". American Journal of Roentgenology. 196(4). :W367-W374. (2011)
- Hussain MI, Khan AF. "Outcome of laparoscopic cholecystectomy in acute and chronic cholecystitis.". Saudi Med J. 27(5). :657-60. (2006)
- Machado NO. "Porcelain Gallbladder: Decoding the malignant truth.". Sultan Qaboos University medical journal. 16(4). :e416-e421. (2016)
- Schnelldorfer T. "Porcelain Gallbladder: A Benign Process or Concern for Malignancy?". J Gastrointest Surg. 17(6). :1161-1168. (2013)
- Khan ZS. "Reassessing the Need for Prophylactic Surgery in Patients With Porcelain Gallbladder". Arch Surg. 146(10). :1143. (2011)
- Morimoto M, Matsuo T, Mori N. "Management of Porcelain Gallbladder, Its Risk Factors, and Complications: A Review". Diagnostics (Basel). 11(6). :1073. (2021)
- Espinoza JA, Bizama C, García P, et al. "The inflammatory inception of gallbladder cancer.". Biochim Biophys Acta. 1865(2). :245-54. (2016)
- Tran TT, Ahn J, Reau NS. "ACG Clinical Guideline: Liver Disease and Pregnancy". Am J Gastroenterol. 111(2). :176-194. (2016)
- Weinstein MS, Feuerwerker S, Baxter JK. "Appendicitis and Cholecystitis in Pregnancy". Clin Obstet Gynecol. 63(2). :405-415. (2020)
- Abushamma S, Early DS. "A Guide to Upper Gastrointestinal Tract, Biliary, and Pancreatic Disorders: Clinical Updates in Women's Health Care Primary and Preventive Care Review.". Obstet Gynecol. 137(6). :1152. (2021)
- GILO NB, AMINI D, LANDY HJ. "Appendicitis and Cholecystitis in Pregnancy". Obstet Gynecol. 52(4). :586-596. (2009)
- American College of Obstetricians and Gynecologists' Committee on Obstetric Practice. "ACOG Committee Opinion No. 775 Summary: Nonobstetric Surgery During Pregnancy". Obstet Gynecol. 133(4). :844-845. (2019)
- ACOG. "Committee Opinion No. 723: Guidelines for Diagnostic Imaging During Pregnancy and Lactation". Obstet Gynecol. 130(4). :e210-e216. (2017)
- Tran TT, Ahn J, Reau NS. "Corrigendum: ACG Clinical Guideline: Liver Disease and Pregnancy.". Am J Gastroenterol. 111(11). :1668. (2016)
- Kumar SS, Collings AT, Wunker C, et al. "SAGES guidelines for the use of laparoscopy during pregnancy". Surg Endosc. 38(6). :2947-2963. (2024)
- Kothari S, Afshar Y, Friedman LS, Ahn J. "AGA Clinical Practice Update on Pregnancy-Related Gastrointestinal and Liver Disease: Expert Review". Gastroenterology. (2024)
- Goldman M, Pranikoff T. "Biliary Disease in Children". Curr Gastroenterol Rep. 13(2). :193-201. (2011)
- Chandra S, Friesen C, Attard TM. "Trends in the Epidemiology of Pediatric Acute and Chronic Cholecystitis-Related Admissions in the USA: A Nationwide Emergency Department and Inpatient Sample Study". Journal Investig Med. 67(8). :1155-1159. (2019)
- Yasuda H, Takada T, Kawarada Y, et al. "Unusual cases of acute cholecystitis and cholangitis: Tokyo Guidelines". J Hepatobiliary Pancreat Surg. 14(1). :98-113. (2007)
- Goldman DA. "Gallbladder, Gallstones, and Diseases of the Gallbladder in Children". Pediatrics In Review. 41(12). :623-629. (2020)
- Dieffenbach BV, Li N, Madenci AL, et al. "Incidence of and risk factors for late cholecystectomy in survivors of childhood cancer: A report from the Childhood Cancer Survivor Study". Eur J Cancer. 133. :4-13. (2020)
- Ng JY, Gu J. "Conservative Management of Acalculous Cholecystitis in a Seven-year-old Child.". Cureus.. 10(1). :e2092. (2018)
- Poddighe D, Tresoldi M, Licari A, Marseglia GL. "Acalculous Acute Cholecystitis in Previously Healthy Children: General Overview and Analysis of Pediatric Infectious Cases". Int J Hepatol.. 2015. :459608. (2015)
- Pelizzo G, Bussani R, De Silvestri A, et al. "Laparoscopic Cholecystectomy for Symptomatic Cholecystic Disease in Children: Defining Surgical Timing". Front. Pediatr.. 8. (2020)
- Mattson A, Sinha A, Njere I, Borkar N, Sinha CK. "Laparoscopic cholecystectomy in children: A systematic review and meta-analysis". The Surgeon. 21(3). :e133-e141. (2023)
- Solomkin JS, Mazuski JE, Bradley JS, et al. "Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America". Clin Infect Dis. 50(2). :133-164. (2010)
- Lack EE. "Pathology of the Pancreas, Gallbladder, Extrahepatic Biliary Tract, and Ampullary Region ". Oxford University Press. (2003). ISBN: 0195133927
- Stinton LM, Shaffer EA. "Epidemiology of gallbladder disease: cholelithiasis and cancer". Gut Liver. 6(2). :172-187. (2012)
- Tenner S, Baillie J, Dewitt J, Vege SS. "American College of Gastroenterology guideline: management of acute pancreatitis". Am J Gastroenterol. 108(9). :1400-1415. (2013)
- Li VK, Yum JL, Yeung YP. "Optimal timing of elective laparoscopic cholecystectomy after acute cholangitis and subsequent clearance of choledocholithiasis". Am J Surg. 200(4). :483-488. (2010)
- Ahmed M. "Acute cholangitis - an update". World J Gastrointest Pathophysiol. 9(1). :1-7. (2018)
- Bouchier IA. "The formation of gallstones.". Keio J Med. 41(1). :1-5. (1992)
- Shea JA, Berlin JA, Escarce JJ, et al. "Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease.". Arch Intern Med. 154(22). :2573-81. (1994)
- Gurusamy KS, Giljaca V, Takwoingi Y, et al. "Ultrasound versus liver function tests for diagnosis of common bile duct stones.". The Cochrane database of systematic reviews. :CD011548. (2015)
- Maple JT, Ben-Menachem T, Anderson MA, et al. "The role of endoscopy in the evaluation of suspected choledocholithiasis". Gastrointest Endosc. 71(1). :1-9. (2010)
- "Choledocholithiasis". http://www.dynamed.com/topics/dmp~AN~T116085/Choledocholithiasis#Overview-and-Recommendations. [2018-12-04]
- Kimura Y, Takada T, Kawarada Y, et al. "Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines.". J Hepatobiliary Pancreat Surg. 14(1). :15-26. (2007)
- Kiriyama S, Kozaka K, Takada T, et al. "Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholangitis (with videos)". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :17-30. (2018)
- Keus F, Broeders IAMJ, van Laarhoven CJHM. "Surgical aspects of symptomatic cholecystolithiasis and acute cholecystitis". Best Practice & Research Clinical Gastroenterology. 20(6). :1031-1051. (2006)
- Crockett et al. "American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis". Gastroenterology. 154(4). :1096-1101. (2018)
- Shirley A, Rivero H, et al. "Surgical and Nonsurgical Management of Gallstones". Am Fam Physician. (2014)
- Miura F, Okamoto K, Takada T, et al. "Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :31-40. (2018)
- Tazuma S, Unno M, Igarashi Y, et al. "Evidence-based clinical practice guidelines for cholelithiasis 2016". J Gastroenterol. 52(3). :276-300. (2016)
- Mukai S, Itoi T, Baron TH, et al. "Indications and techniques of biliary drainage for acute cholangitis in updated Tokyo Guidelines 2018.". Journal of hepato-biliary-pancreatic sciences. 24(10). :537-549. (2017)
- Manes G, Paspatis G, Aabakken L, et al. "Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline". Endoscopy. 51(05). :472-491. (2019)
- Shaffer EA. "Gallbladder cancer: the basics.". Gastroenterology & hepatology. 4(10). :737-41. (2008)
- Swartz DE, Felix EL. "Elective cholecystectomy after Roux-en-Y gastric bypass: why should asymptomatic gallstones be treated differently in morbidly obese patients?". Surg Obes Relat Dis. 1(6). :555-60. (2005)
- Baron TH, Garg SK. "Routine cholecystectomy during Roux-en-Y gastric bypass with or without choledocholithiasis". Cochrane Database of Systematic Reviews. (2013)
- Gurusamy K, Samraj K, Davidson B. "Early versus delayed laparoscopic cholecystectomy for biliary colic". Cochrane Database of Systematic Reviews. (2008)
- Duncan CB, Riall TS. "Evidence-based current surgical practice: calculous gallbladder disease.". J Gastrointest Surg. 16(11). :2011-25. (2012)
- Jarnagin WR. "Blumgart's Surgery of the Liver, Biliary Tract, and Pancreas". Elsevier. (2016). ISBN: 9780323340625
- Buxbaum JL, Abbas Fehmi SM, Sultan S, et al. "ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis". Gastrointest Endosc. 89(6). :1075-1105.e15. (2019)
- "American College of Radiology ACR Appropriateness Criteria® Jaundice". https://acsearch.acr.org/docs/69497/Narrative/. [2018-01-01]
- Huang RJ, Barakat MT, Girotra M, Banerjee S. "Practice Patterns for Cholecystectomy After Endoscopic Retrograde Cholangiopancreatography for Patients With Choledocholithiasis". Gastroenterology. 153(3). :762-771.e2. (2017)
- Kiriyama S, Takada T, Strasberg SM, et al. "TG13 guidelines for diagnosis and severity grading of acute cholangitis (with videos)". Journal of Hepato-Biliary-Pancreatic Sciences. 20(1). :24-34. (2013)
- Lee JM, Boll DT. "Disease of the Gallbladder and Biliary Tree". Springer International Publishing. :49-56. (2018). ISBN: 9783319750187
- Catalano OA, Sahani DV, Forcione DG, et al. "Biliary Infections: Spectrum of Imaging Findings and Management". RadioGraphics. 29(7). :2059-2080. (2009)
- Yeh BM, Liu PS, Soto JA, Corvera CA, Hussain HK. "MR Imaging and CT of the Biliary Tract". RadioGraphics. 29(6). :1669-1688. (2009)
- Iqbal U, Khara HS, Hu Y, et al. "Emergent versus urgent ERCP in acute cholangitis: a systematic review and meta-analysis". Gastrointest Endosc. 91(4). :753-760.e4. (2020)
- Buyukasik K, Toros AB, Bektas H, Ari A, Deniz MM. "Diagnostic and therapeutic value of ERCP in acute cholangitis.". ISRN gastroenterology. 2013. :191729. (2013)
- Salerno R, Davies SEC, Mezzina N, Ardizzone S. "Comprehensive review on EUS-guided biliary drainage.". World journal of gastrointestinal endoscopy. 11(5). :354-364. (2019)
- Baars JE, Kaffes AJ, Saxena P. "EUS-guided biliary drainage: A comprehensive review of the literature.". Endoscopic ultrasound. 7(1). :4-9. (2018)
- Kashani A, Abboud G, Lo SK, Jamil LH. "Double balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography in Roux-en-Y gastric bypass anatomy: expert vs. novice experience.". Endoscopy international open. 6(7). :E885-E891. (2018)
- Ahmed M, Diggory RT. "Case-based review: bile peritonitis after T-tube removal.". Ann R Coll Surg Engl. 95(6). :383-5. (2013)
- Ha JS, Choi HJ, Moon JH, et al. "Endoscopic Extraction of Biliary Fascioliasis Diagnosed Using Intraductal Ultrasonography in a Patient with Acute Cholangitis.". Clinical endoscopy. 48(6). :579-82. (2015)
- Yılmaz S, Akıcı M, Şimşek M, et al. "Endoscopic retrograde cholangiopancreatography for biliary system parasites.". Turkish journal of surgery. 34(4). :306-310. (2018)
- Haribhakti SP, Mistry JH. "Techniques of laparoscopic cholecystectomy: Nomenclature and selection.". Journal of minimal access surgery. 11(2). :113-8. (2015)
- McNally MA, Locke GR, Zinsmeister AR, et al. "Biliary events and an increased risk of new onset irritable bowel syndrome: a population-based cohort study.". Aliment Pharmacol Ther. 28(3). :334-43. (2008)
- Yueh T-P, Chen F-Y, Lin T-E, Chuang M-T. "Diarrhea after laparoscopic cholecystectomy: Associated factors and predictors". Asian Journal of Surgery. 37(4). :171-177. (2014)
- Lee KJ. "Pharmacologic Agents for Chronic Diarrhea.". Intestinal research. 13(4). :306-12. (2015)
- Ahmad F, Saunders RN, Lloyd GM, Lloyd DM, Robertson GS. "An algorithm for the management of bile leak following laparoscopic cholecystectomy.". Ann R Coll Surg Engl. 89(1). :51-6. (2007)
- Omar M, Redwaan A. "Management of postoperative bile leak: Tertiary centers experience". Clinics in Surgery. (2017)
- Tzovaras G, Peyser P, Kow L, et al. "Minimally invasive management of bile leak after laparoscopic cholecystectomy.". HPB : the official journal of the International Hepato Pancreato Biliary Association. 3(2). :165-8. (2001)