Quick guide
Diagnostic approach
- Focused clinical evaluation
- CMP
- CBC
- Blood gas: ABG or VBG to assess for metabolic acidosis
- Urinalysis with urine sediment microscopy
- Urine sodium, urea, creatinine, and osmolality
- Calculation of excretion fractions (e.g., FENa, FEUrea)
- Bladder POCUS if concern for lower UTO
- Renal ultrasound if concern for hydronephrosis
- See “Diagnosis of AKI.”
")
Diagnostic criteria
Any of the following:
- Increase in serum creatinine by ≥ 0.3 mg/dL (≥ 26.5 μmol/L) within 48 hours
- Increase in serum creatinine to ≥ 1.5 × baseline level within 7 days
- Decrease in urine output to < 0.5 mL/kg/hour for ≥ 6 hours
Management checklist
- Prerenal: volume repletion with IV crystalloids, hemodynamic support
- Postrenal: Relieve the obstruction; consult urology as needed.
- Intrinsic: Consider IV fluids.
- Identify and treat the underlying cause.
- Hold nephrotoxic substances and nonessential medications.
- Renally dose essential medications.
- Establish or maintain euvolemia.
- Blood pressure management
- Input/output monitoring
- Correct electrolyte disturbances.
- Manage acidosis.
- Nutritional support
- VTE prophylaxis
- Consult nephrology in patients with red flag features.
- See “Management of AKI.”
Red flag features
- Indications for acute dialysis or renal biopsy
- AKI stage 3
- Inadequate response to initial treatment
- Intrinsic AKI
- History of kidney transplant
- CKD category G4 or higher
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Summary
Acute kidney injury (AKI) is a sudden loss of renal function with a subsequent rise in creatinine and blood urea nitrogen (BUN). It is most frequently caused by decreased renal perfusion (prerenal) but may also be due to direct damage to the kidneys (intrarenal or intrinsic) or inadequate urine drainage (postrenal). In AKI, the acid-base, fluid, and electrolyte balances are disturbed and the urinary excretion of substances such as drugs is impaired. AKI may be asymptomatic or manifest with oliguria or anuria and, when kidney dysfunction is severe, it may manifest with symptoms and signs of uremia; in some cases, polyuria may occur as a result of impaired tubular reabsorption. A diagnosis of AKI can be made based on an increase in serum creatinine concentration and/or decrease in urine output. Initial evaluation includes blood and urine studies, which may help identify the mechanism of kidney injury and any metabolic complications of AKI. Additional specific investigations are guided by the suspected cause. Rapid evaluation, diagnosis, and treatment are necessary to prevent irreversible loss of renal function. Management is based on the mechanism of kidney injury and the underlying causes. Treatment is primarily supportive and aims to ensure adequate kidney perfusion and prevent complications and further kidney damage.
Etiology
Prerenal acute kidney injury [1][2][3]
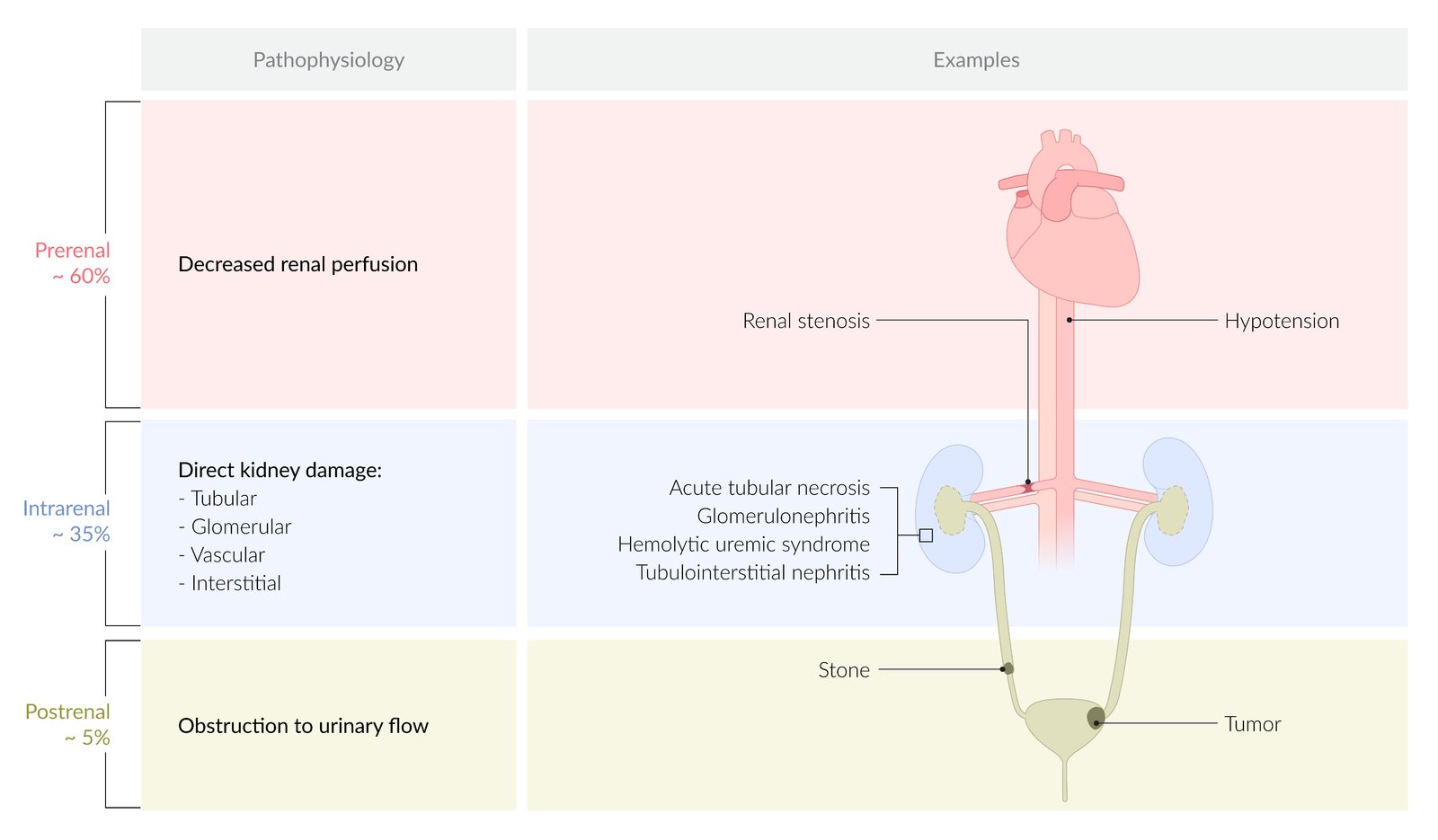
Prerenal causes include any condition that leads to decreased renal perfusion (∼ 60% of cases of AKI). [1][2][3]
- Hypovolemia: e.g., due to hemorrhage, vomiting, diarrhea, sweating, burns, diuretics, poor oral intake, dehydration, hypercalcemia
- Hypotension: e.g., due to sepsis, cardiogenic shock (decreased cardiac output), anaphylactic shock
-
Decreased circulating volume (↓ effective arterial volume)
- Cardiorenal syndrome: e.g., in congestive heart failure
- Hepatorenal syndrome: e.g., in cirrhosis, liver failure
- Abdominal compartment syndrome
- Nephrotic syndrome
- Acute pancreatitis
- Renal artery stenosis
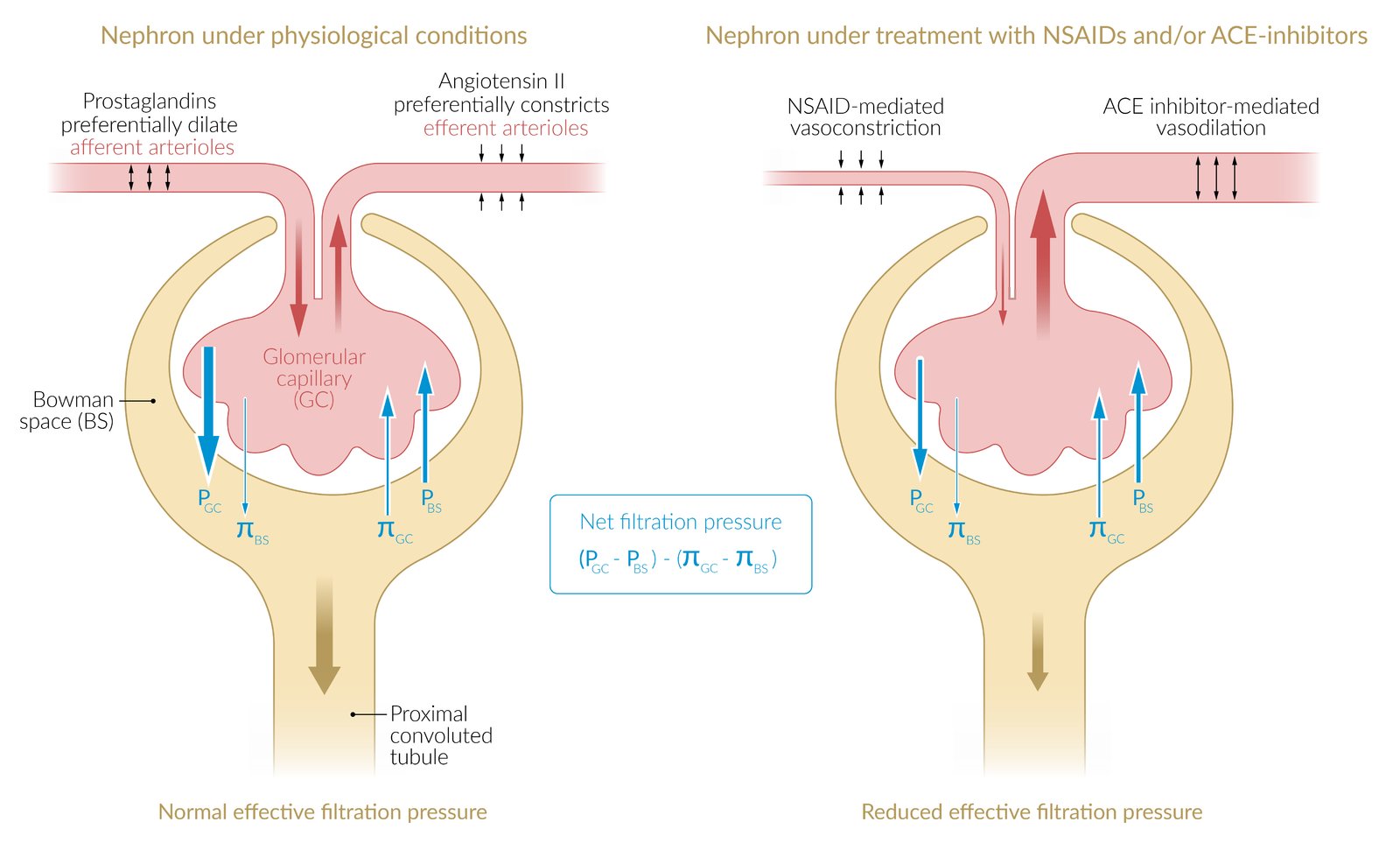
- Drugs that affect glomerular perfusion: e.g., cyclosporine, tacrolimus, NSAIDs , ACE inhibitors (ACE-Is)
Prolonged prerenal injury leads to intrinsic injury, as decreased renal perfusion causes tubular necrosis.

Intrinsic acute kidney injury
Intrinsic causes include any condition that leads to severe direct kidney damage (∼ 35% of cases of AKI). [1][2][3]
-
Acute tubular necrosis (causes ∼ 85% of intrinsic AKIs)
- Ischemia: e.g., due to prolonged hypotension
- Nephrotoxic drugs: e.g., radiographic contrast agents, aminoglycosides, cisplatin, methotrexate, ethylene glycol, amphotericin B
- Endogenous toxins: e.g., hemoglobin in intravascular hemolysis, myoglobin in rhabdomyolysis, uric acid in TLS, Bence-Jones protein light chains in multiple myeloma
-
Acute interstitial nephritis
- Medication: e.g., antibiotics , phenytoin, interferon, PPIs, NSAIDs, cyclosporine
- Infection
- Bacterial: e.g., Legionella spp., Streptococcus spp.
- Fungi: Candida, Histoplasma
- Viral: e.g., hepatitis C virus, cytomegalovirus, HIV
- Infiltrative diseases: e.g., sarcoidosis, amyloidosis
-
Vascular diseases
- Hemolytic uremic syndrome (HUS)
- Thrombotic thrombocytopenic purpura (TTP)
- Hypertensive emergency
- Vasculitis, scleroderma renal crisis
- Renal vein thromboses, renal atheroemboli, renal infarction
- Glomerulonephritis:e.g., rapidly progressive glomerulonephritis
Postrenal acute kidney injury
Postrenal causes include any condition that results in bilateral obstruction of urinary flow from the renal pelvis to the urethra (∼ 5% of cases of AKI). [1][2][3]
-
Acquired obstructions
- Benign prostatic hyperplasia (BPH)
- Iatrogenic: e.g., catheter-associated injuries
- Tumors: e.g., bladder, prostate, cervical, metastases
- Stones
- Bleeding with subsequent blood clot formation
- Neurogenic bladder: e.g., due to multiple sclerosis, spinal cord lesions, or peripheral neuropathy
- Congenital malformations: e.g., posterior urethral valves
As long as the contralateral kidney remains intact, patients with unilateral ureteral obstruction typically maintain normal serum creatinine levels.

Overview of nephrotoxic medications
| Overview | ||
|---|---|---|
| Class | Examples | |
| Antimicrobials | Antibiotics |
|
| Antivirals |
|
|
| Antifungals |
|
|
| Antimetabolites |
|
|
| Chemotherapeutic agents (e.g., platinum-based chemotherapeutic agents) |
|
|
| Antiinflammatories and immunosuppressants |
|
|
| Others |
|
|
© AMBOSS
© AMBOSS
Pathophysiology
Prerenal
- Decreased blood supply to kidneys (due to hypovolemia, hypotension, or renal vasoconstriction); → failure of renal vascular autoregulation to maintain renal perfusion → decreased GFR → activation of renin-angiotensin system → increased aldosterone release → increased reabsorption of Na+, H2O → increased urine osmolality → secretion of antidiuretic hormone → increased reabsorption of H2O and urea
- Creatinine is still secreted in the proximal tubules, so the blood BUN:creatinine ratio increases.
 inhibitors")
Intrinsic
- Damage to a vascular or tubular component of the nephron → necrosis or apoptosis of tubular cells → decreased reabsorption capacity of electrolytes (e.g., Na+), water, and/or urea; (depending on the location of injury along the tubular system) → increased Na+ and H2O in the urine → decreased urine osmolality
Postrenal
- Bilateral urinary outflow obstruction (e.g., stones, BPH, neoplasia, congenital anomalies) → increased retrograde hydrostatic pressure within renal tubules → decreased GFR and compression of the renal vasculature → acidosis, fluid overload, and increased BUN, Na+, and K+.
- A normal GFR can be maintained as long as one kidney functions normally.
Four phases of AKI
| Overview of the four phases of AKI | ||
|---|---|---|
| Phase | Characteristic features (some patients may not undergo all phases) | Duration |
| Initiating event (kidney injury) |
|
|
| Oliguric or anuric phase (maintenance phase) |
|
|
| Polyuric/diuretic phase |
|
|
| Recovery phase |
|
|
References:[2][4]
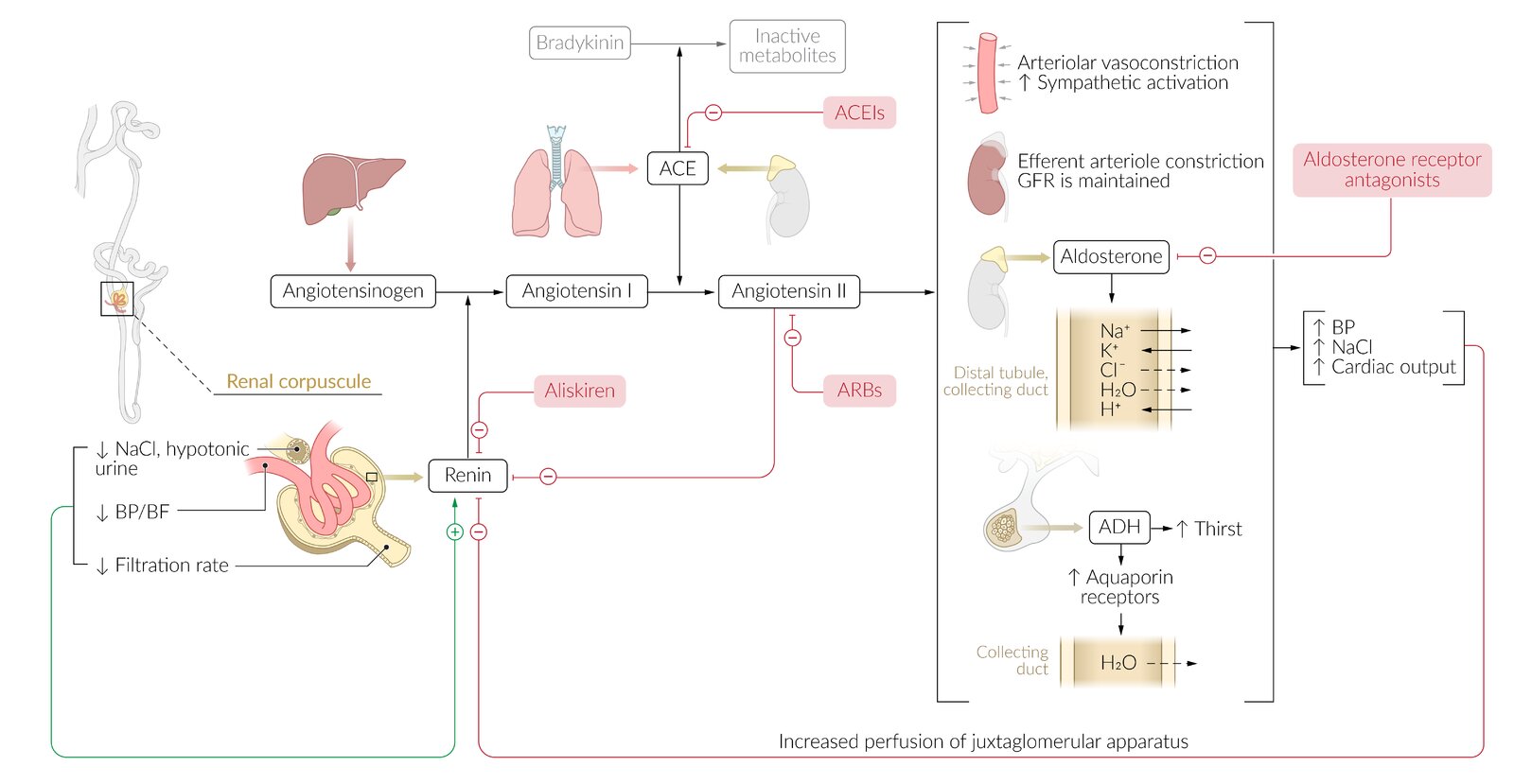
Renin is produced in response to changes in the glomerular filtration rate and solute content of the blood within the renal corpuscle. Renin catalyzes the conversion of angiotensinogen (produced by the liver) to angiotensin I, which is then converted to angiotensin II by angiotensin-converting enzyme (ACE; produced by the lungs). Angiotensin II acts to increase blood pressure by causing vasoconstriction, sodium retention, and ADH production.
The specific targets of the different RAAS inhibitors are highlighted in red.
© AMBOSS
Clinical features
- May be asymptomatic.
- Oliguria or anuria
-
Signs of volume depletion (in prerenal AKI caused by volume loss)
- Orthostatic or frank hypotension and tachycardia
- Reduced skin turgor
-
Signs of fluid overload (from Na+ and H2O retention)
- Peripheral and pulmonary edema
- Hypertension
- Heart failure
- Shortness of breath
-
Signs of uremia
- Anorexia, nausea
- Encephalopathy, asterixis
- Pericarditis
- Platelet dysfunction
-
Signs of renal obstruction (in postrenal AKI)
- Distended bladder
- Incomplete voiding
- Pain over the bladder or flanks
- Fatigue, confusion, and lethargy
- In severe cases: seizures or coma
- Affected individuals have a higher risk of secondary infection throughout all phases (most common reason for fatalities).
Subtypes and variants
Acute tubular necrosis
- Epidemiology: : causes ∼ 85% of intrinsic AKIs
-
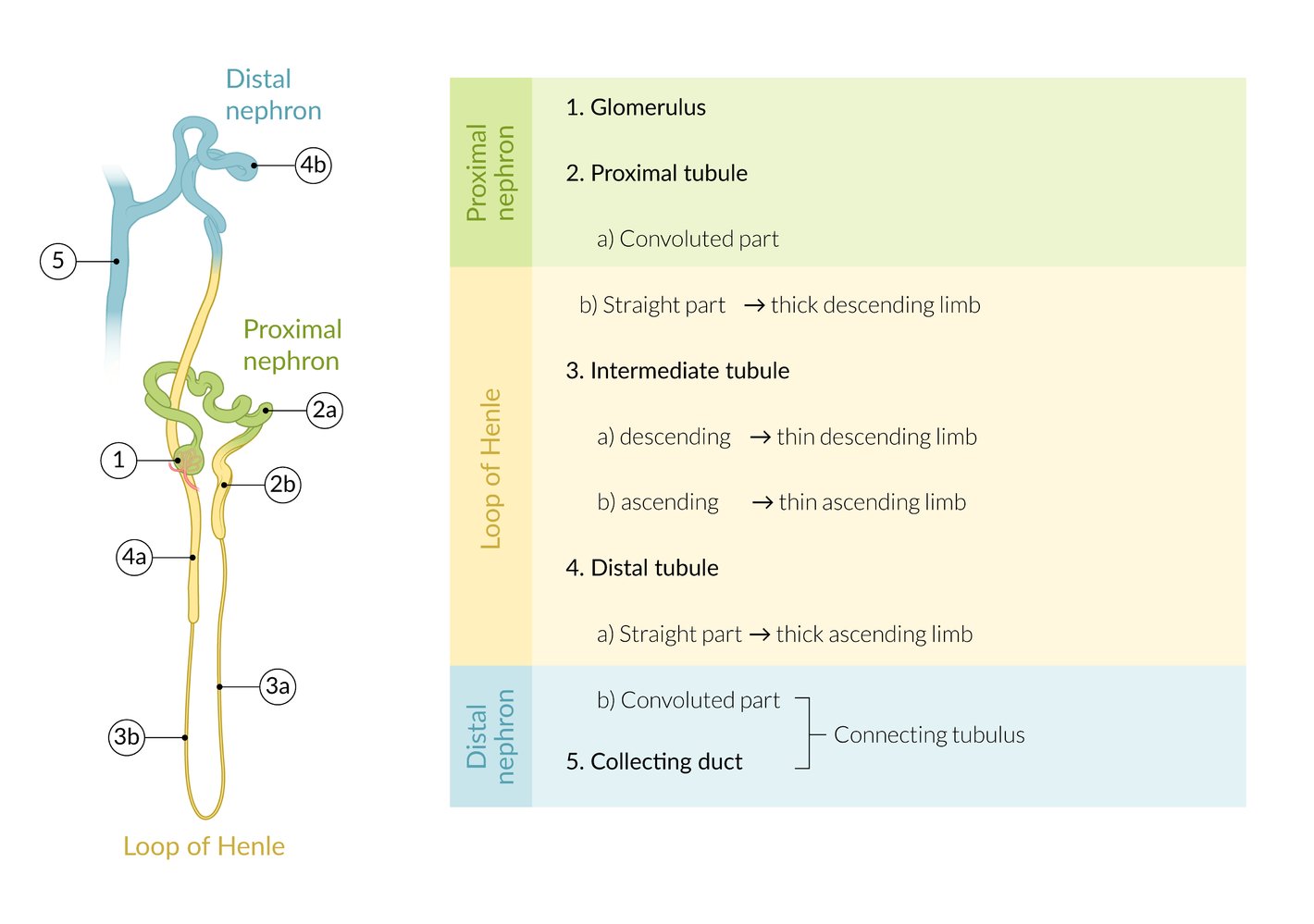
Location
- The straight segment of the proximal tubule and the straight segment of the distal tubule (i.e., the thick ascending limb) are particularly susceptible to ischemic damage.
- The convoluted segment of the proximal tubule is particularly susceptible to damage from toxins.
-
Etiology
-
Ischemic: Injury occurs secondary to decreased renal blood flow.
- Severe hypotension, especially in the context of shock: hypovolemic (e.g., hemorrhage, severe dehydration), septic, cardiogenic (e.g., heart failure), or neurogenic shock
- Thromboembolism
- Thrombotic microangiopathy
- Cholesterol embolism (atheroemboli)
-
Toxic: Injury occurs directly due to nephrotoxic substances.
- Contrast-induced nephropathy
- Medication: aminoglycosides, cisplatin, amphotericin, lead, ethylene glycol
-
Pigment nephropathy: an acute kidney injury that occurs as a result of the toxic effects of heme-containing pigments (e.g., hemoglobin, myoglobin) on proximal renal tubular cells (toxin-induced acute tubular necrosis)
- Myoglobinuria due to rhabdomyolysis (crush syndrome)
- Hemoglobinuria associated with hemolysis
- Acute uric acid nephropathy
- Other: sepsis, infections
-
Ischemic: Injury occurs secondary to decreased renal blood flow.
- Pathophysiology: necrotic proximal tubular cells fall into the tubular lumen → debris obstructs tubules → decreased GFR → sequence of pathophysiological events similar to prerenal failure (i.e., activation of RAAS; see “Pathophysiology” above)
- Clinical features: same as AKI (see “Clinical features” and four phases of AKI above)
-
Diagnostics (see “Diagnostics” below)
- Blood findings: azotemia, hyperkalemia, and metabolic acidosis
- Urinary findings
- ↑ Fractional excretion of sodium (FENa)
- Myoglobinuria, hemoglobinuria
-
Urinary sediment
- Muddy brown granular casts
- Epithelial cell casts
- Free renal tubular epithelial cells (due to denudation of the tubular basement membrane)
- Management: See “Management” below.
-
Prognosis
- After 1–3 weeks, most patients with ATN will experience tubular re-epithelialization and spontaneous full recovery is common.
- Can be lethal; if AKI is severe and not managed adequately (e.g., dialysis may be required in oliguric patients with volume overload or severe hyperkalemia)



Renal cortical necrosis
- Definition: rare cause of AKI caused by acute generalized ischemic necrosis of the renal cortex in both kidneys
- Etiology: septic shock, disseminated intravascular coagulation (DIC); , hemolytic uremic syndrome (HUS), obstetric complications; (e.g., abruptio placentae, septic abortion, postpartum hemorrhage)
- Pathophysiology: vasospasms and microvascular injury with vascular thrombosis → prolonged severe renal ischemia; → diffuse and/or patchy destruction of the renal cortex [5]
- Clinical features: flank pain, CVA tenderness and signs of AKI (see also “Clinical features” above and shock)
- Management: Dialysis can improve outcomes (see “Management” below).
- Prognosis: high mortality rates without treatment
Contrast-induced nephropathy
- Definition: AKI after IV administration of iodinated contrast medium
-
Risk factors
- Chronic kidney disease (CKD): esp. in patients with diabetes mellitus, multiple myeloma
- Congestive heart failure, arterial hypotension
- Nephrotoxic drugs: esp. NSAIDs
- Anemia
- Dehydration
- Clinical features/diagnostics: See “Clinical features” above and “Diagnostics” below.
-
Course
- Creatinine is highest 3–5 days after injury and usually falls back to the baseline level within 1 week.
- The course is typically mild because end-stage renal disease usually only occurs in patients with pre-existing CKD.
-
Prevention of contrast-induced nephropathy
- Always evaluate kidney function before administering a contrast agent.
- Use a low dose and low concentration of contrast medium.
- The patient should discontinue nephrotoxic substances before administration.
- Ensure hydration: isotonic NaCl before and after administration of contrast medium
- Acetylcysteine (no clear recommendations )
References:[2][3][6]
© AMBOSS
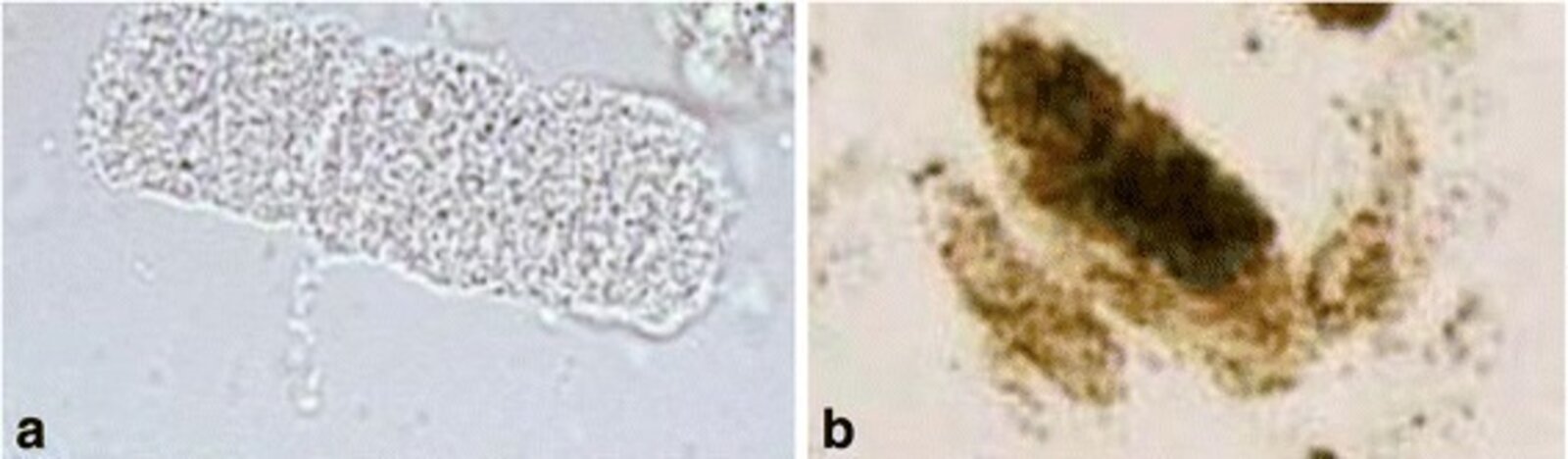
Photomicrograph of urine sediment (high magnification)
Renal tubular epithelial cell casts (a) and muddy brown casts (b) were identified in this urine sample.
Both findings indicate damage of the kidneys, likely due to acute tubular necrosis.
Source: “Practical approach to detection and management of acute kidney injury in critically ill patient” by Vahid Mohsenin, Journal of Intensive Care, licensed under CC BY 4.0. Modifications: image cropped.
Photomicrograph of a renal biopsy sample (H&E stain)
The cells of the tubules and glomeruli show clumped and highly eosinophilic cytoplasm. The nuclei of these cells are either absent or palely staining. There is debris in some tubular lumens and thrombi are visible in the capillaries on the lower right. The main outlines of the tubules and glomeruli are still intact.
Source: “Renal cortical infarction showing coagulative necrosis 40X” by Department of Pathology, Calicut Medical College, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
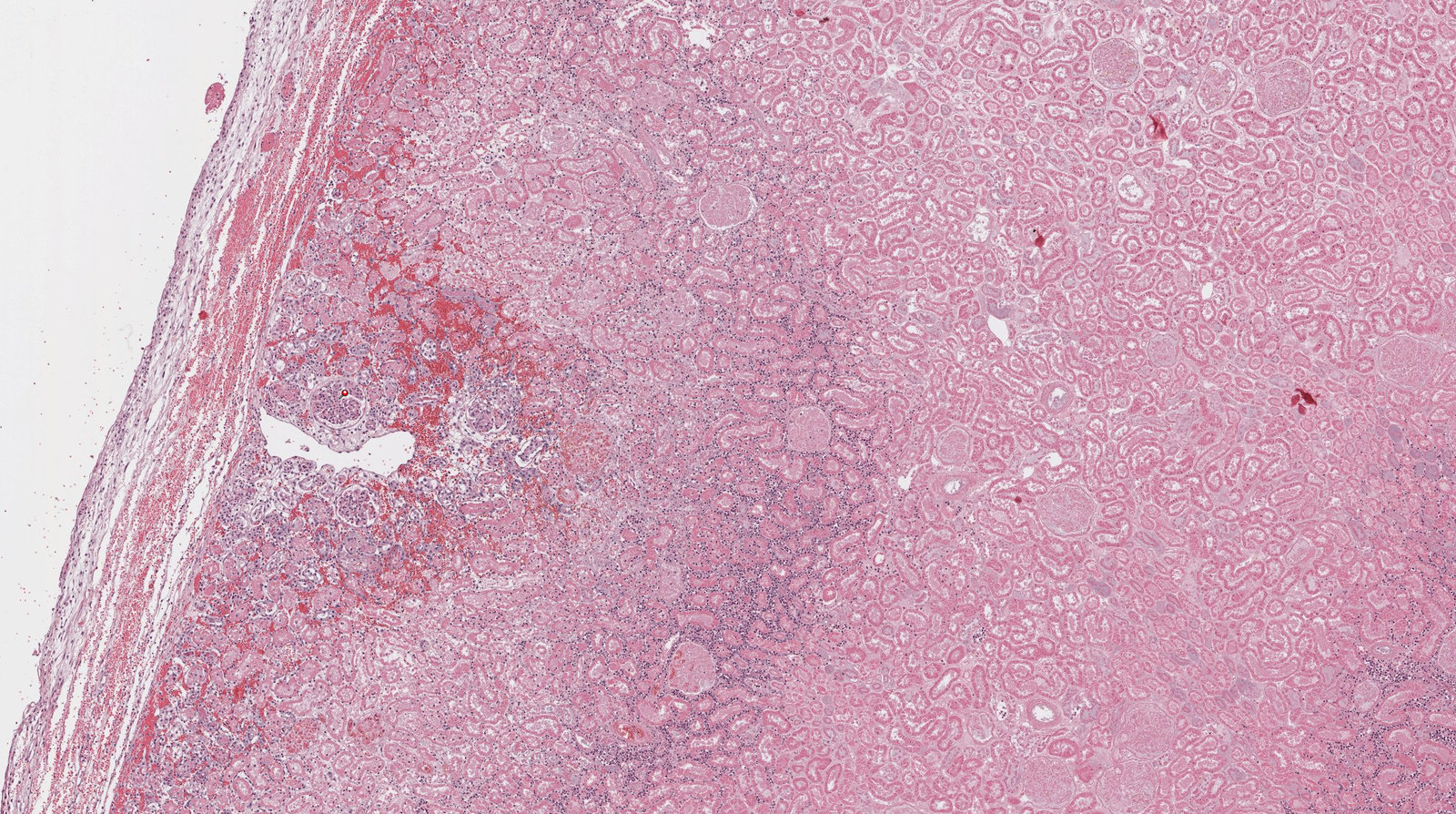
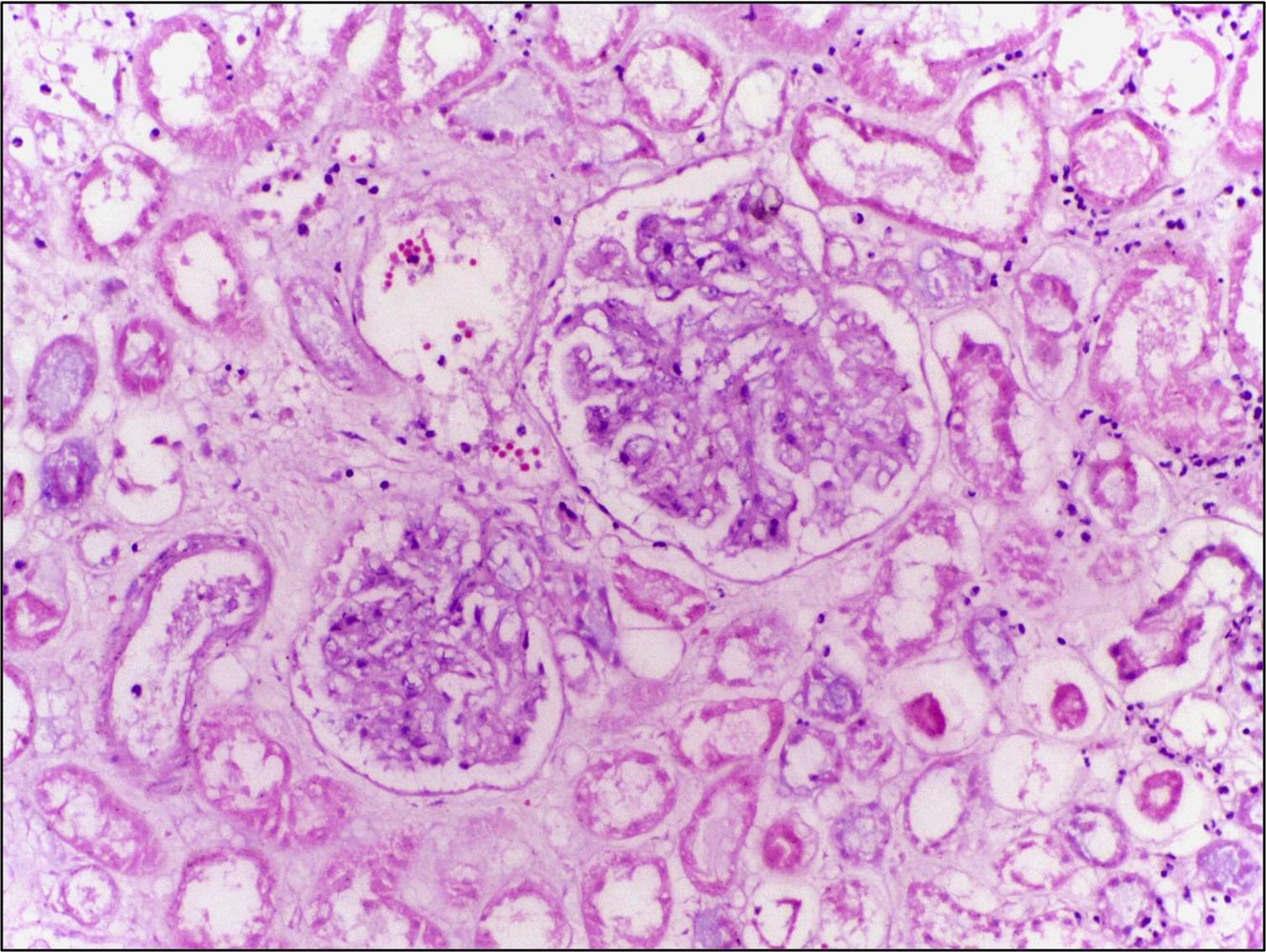
Photomicrograph of kidney tissue (H&E stain; 150x magnification)
A large area of necrosis (green overlay) is visible. Necrotic glomeruli (green arrowheads) are also visible within a highly dense area of leukocytes (white overlay). This is in contrast to the appearance of a normal glomerulus (black arrowhead).
These findings are consistent with coagulative necrosis caused by renal infarction.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Diagnosis
A diagnosis of AKI can be made based on an acute increase in serum creatinine and/or decrease in urine output in accordance with the definition of AKI.
Approach [7][8][9]
- Compare current and previous creatinine levels to determine if the process is acute.
- Check diagnostic criteria and perform staging of AKI.
- Determine the most likely mechanism of AKI (i.e., prerenal, intrinsic, or postrenal) based on:
- A comprehensive chart review, history, and physical examination
- Supportive diagnostic findings and response to initial interventions
- Consider further testing for specific underlying causes of AKI.
In the absence of previously documented creatinine levels, stable creatinine levels with findings such as chronic anemia and small hyperechoic kidneys on ultrasound suggest CKD rather than AKI.
Clinical presentation, laboratory tests, imaging, response to initial therapy, and, in some cases, histopathology are required to determine the underlying cause of AKI.
Diagnostic criteria of acute kidney injury
-
Acute kidney injury is defined as the presence of any of the following criteria: ; [7]
- Increase in serum creatinine by ≥ 0.3 mg/dL (≥ 26.5 μmol/L) within 48 hours.
- Increase in serum creatinine to ≥ 1.5 times baseline level within 7 days.
- Decrease in urine output to < 0.5 mL/kg/hour for ≥ 6 hours.
Staging of acute kidney injury
- The KDIGO stages are widely used and correlate with the risk of death, need for renal replacement therapy, and long-term outcomes (e.g., CKD).
- Other classifications include: [7]
-
RIFLE criteria: A classification system for acute kidney injury
- The acronym stands for Risk, Injury, Failure, Loss, and End-stage kidney disease.
- For the first three categories, patients are classified according to the level of kidney injury (i.e., degree of increase in serum creatinine and/or decrease in GFR and urine output) and for the last two categories, according to the duration of complete loss of kidney function.
- Acute Kidney Injury Network (AKIN) criteria
-
RIFLE criteria: A classification system for acute kidney injury
| Kidney Disease Improving Global outcomes (KDIGO) criteria for staging of AKI [7] | ||
|---|---|---|
| Stage | Serum creatinine | Urine output |
| AKI stage 1 |
|
|
| AKI stage 2 |
|
|
| AKI stage 3 |
|
|
| If serum creatinine and urine output correlate with different stages, consider staging based on the criterion that corresponds to the highest stage. [9] | ||
Initial evaluation
Laboratory studies
- Serum creatinine and BUN
- Serum electrolytes: sodium, potassium, magnesium, calcium, and phosphate
- CBC
- Blood gases: ABG or VBG
- Urinalysis with urine sediment microscopy
- Urine sodium, urea, creatinine, and osmolality
- Calculate excretion fractions: may help to differentiate prerenal AKI from intrinsic AKI [10]
- Fractional excretion of sodium (FENa)
- Fractional excretion of urea (FEUrea)
Overview of diagnostic findings
| Determination of the likely mechanism of acute kidney injury | |||
|---|---|---|---|
| Prerenal | Intrinsic | Postrenal | |
| BUN:creatinine ratio |
|
|
|
| FENa |
|
|
|
| FEUrea |
|
|
|
| Urine sodium concentration |
|
|
|
| Urine osmolality |
|
|
|
| Urine sediment |
|
|
|
Despite the common use of BUN:creatinine ratio and urinary fractional excretions (i.e., FENa, FEUrea) in clinical practice, observational data suggest that they do not reliably distinguish prerenal AKI from intrinsic AKI. [10][11]
The most likely mechanism of AKI is primarily determined based on clinical presentation and response to therapy. Evaluating patients' response to initial interventions is key to confirming the mechanism of AKI and guiding further workup and management steps.
 casts in urine sediment")


Prerenal AKI [8][9]
-
Blood study findings
- Elevated serum creatinine
- Serum BUN:creatinine ratio ≥ 20:1 [12]
-
Urine study findings
- Normal urinalysis
-
Low urinary sodium and urea excretion
- Low fractional excretion of sodium (FENa < 1%)
- Low fractional excretion of urea (FEUrea < 35%)
- High urine osmolality (> 500 mOsm/kg) and specific gravity (> 1.020) [13][14]
- Urine sediment: hyaline casts due to concentrated urine in the setting of low renal perfusion
- Clinical findings: rapid improvement in renal function following acute intervention
Patients with prerenal AKI receiving diuretic therapy may have a falsely elevated FENa. Therefore, FEUrea may be more informative in this setting. [15]
Intrinsic AKI
-
Blood study findings
- Elevated serum creatinine concentration and rapidly rising serum creatinine level
- BUN:creatinine ratio ≤ 15:1
-
Urine study findings
- High urinary sodium and urea excretion
- High urine sodium concentration (> 40 mEq/L)
- High fractional excretion of sodium (FENa > 2–3%) [8][15]
- High fractional excretion of urea (FEUrea > 50%) [15]
- Low urine osmolality (< 350 mOsm/kg)
- Urine sediment: renal tubular epithelial cells or granular, muddy brown, or pigmented casts
- High urinary sodium and urea excretion
- Biopsy: e.g., in suspected rapidly progressive glomerulonephritis
- Clinical findings: lack of response to acute intervention
A falsely low FENa may be seen in some patients with intrinsic AKI, e.g., due to glomerulonephritis, acute interstitial nephritis, rhabdomyolysis, or contrast-induced nephropathy. [15]
Postrenal AKI
-
Blood study findings
- Elevated serum creatinine concentration in bilateral obstruction
- BUN:creatinine ratio varies; usually normal (i.e., 10:1–20:1)
-
Urine study findings
- Normal urinalysis; : e.g., when due to neurogenic bladder
- Hematuria; : e.g., when due to stones, bladder cancer, clots
- Urine osmolality varies. [16]
-
Imaging (renal ultrasound or noncontrast CT scan)
- Bladder distention, high postvoid residual volume, bilateral hydronephrosis, and/or obstructing stones
- See “Imaging modalities” in “Urinary tract obstruction.”
- Clinical findings: rapid improvement in renal function following resolution of the obstruction
")
Additional evaluation
Imaging [17]
Imaging of the kidneys and urinary tract is not necessary to establish a diagnosis of AKI but may be needed to determine the etiology.
-
Ultrasound
- Obtain urgently to assess for hydronephrosis in patients with risk factors for urinary tract obstruction. [8][18]
- Consider when evaluating renal dysfunction of unclear etiology.
-
Noncontrast CT
- Obtain if ultrasound shows hydronephrosis but does not reveal the cause of the obstruction.
- Consider when clinical suspicion of obstruction remains high despite the absence of hydronephrosis on ultrasound.
- See also “Imaging modalities” in “Urinary tract obstruction.”
Obtain an urgent ultrasound to rule out hydronephrosis in patients with risk factors for urinary tract obstruction.
While ultrasound is the initial test of choice to assess for urinary tract obstruction, CT has greater sensitivity for detecting obstructions and stones. [19]

")


Renal biopsy [8][20]
- Not routinely indicated
- Consider if:
- The cause of AKI cannot be identified after a thorough initial evaluation
- Diagnostic confirmation of the cause (e.g., glomerulonephritis, myeloma nephropathy) is needed prior to initiating disease-specific therapy
Additional specific testing
Usually reserved for cases in which intrinsic AKI is initially suspected or interventions aimed at reversing presumed prerenal AKI or postrenal AKI fail to improve renal function. Studies should be guided by clinical suspicion.
| Noninvasive testing for specific underlying causes of AKI [1][20] | |||
|---|---|---|---|
| Examples | Characteristic clinical features | Diagnostic findings | |
| Nephrotoxin-induced AKI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Rapidly progressive glomerulonephritis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Others |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Photomicrograph of urine sediment (high magnification)
Renal tubular epithelial cell casts (a) and muddy brown casts (b) were identified in this urine sample.
Both findings indicate damage of the kidneys, likely due to acute tubular necrosis.
Source: “Practical approach to detection and management of acute kidney injury in critically ill patient” by Vahid Mohsenin, Journal of Intensive Care, licensed under CC BY 4.0. Modifications: image cropped.
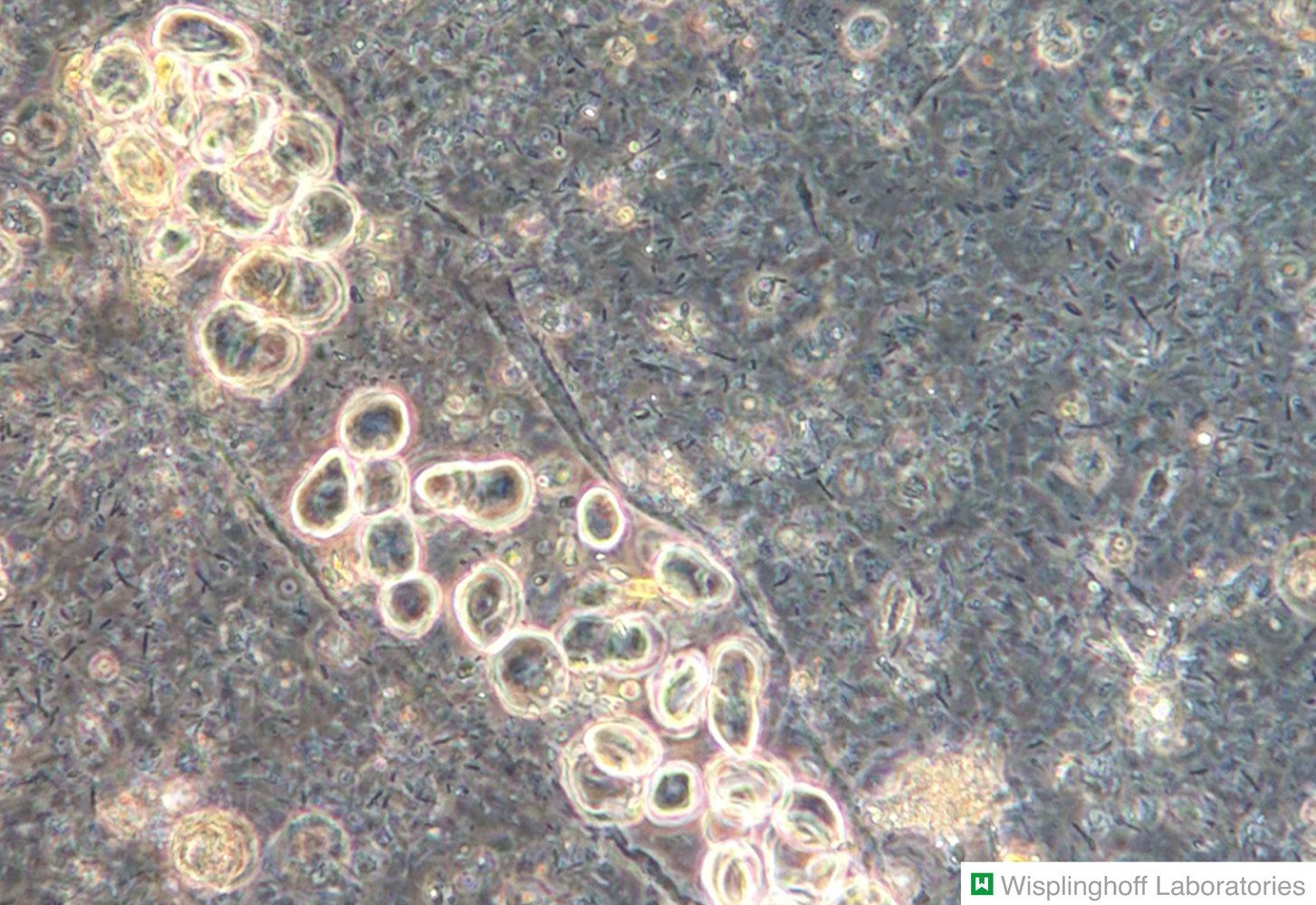
Photomicrograph of urine sediment (phase-contrast microscopy)
A tubular cast (blue overlay) is visible in the center of the image. The cast is composed of numerous RBCs, identifiable by their characteristic biconvex shape (examples outlined in yellow), in a matrix of fibrin and plasma proteins. Several epithelial cells surrounding the RBC cast are also visible.
RBC casts in urinary sediment are typically seen in glomerulonephritis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
Polarized light micrograph of lyotropic liquid crystals
These Lα liquid crystals have a characteristic Maltese cross appearance (examples indicated by green overlay) under polarized light. Fatty casts from urinary sediment have the same appearance under polarized light.
Source: “Figure 4 (a), in: Development and Characterization of Nanostructured Pharmacosomal Mesophases: An Innovative Delivery System for Bioactive Peptides” by Maryam Rezvani, Javad Hesari, Seyed Hadi Peighambardoust, Maria Manconi, Hamed Hamishehkar, Advanced Pharmaceutical Bulletin, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
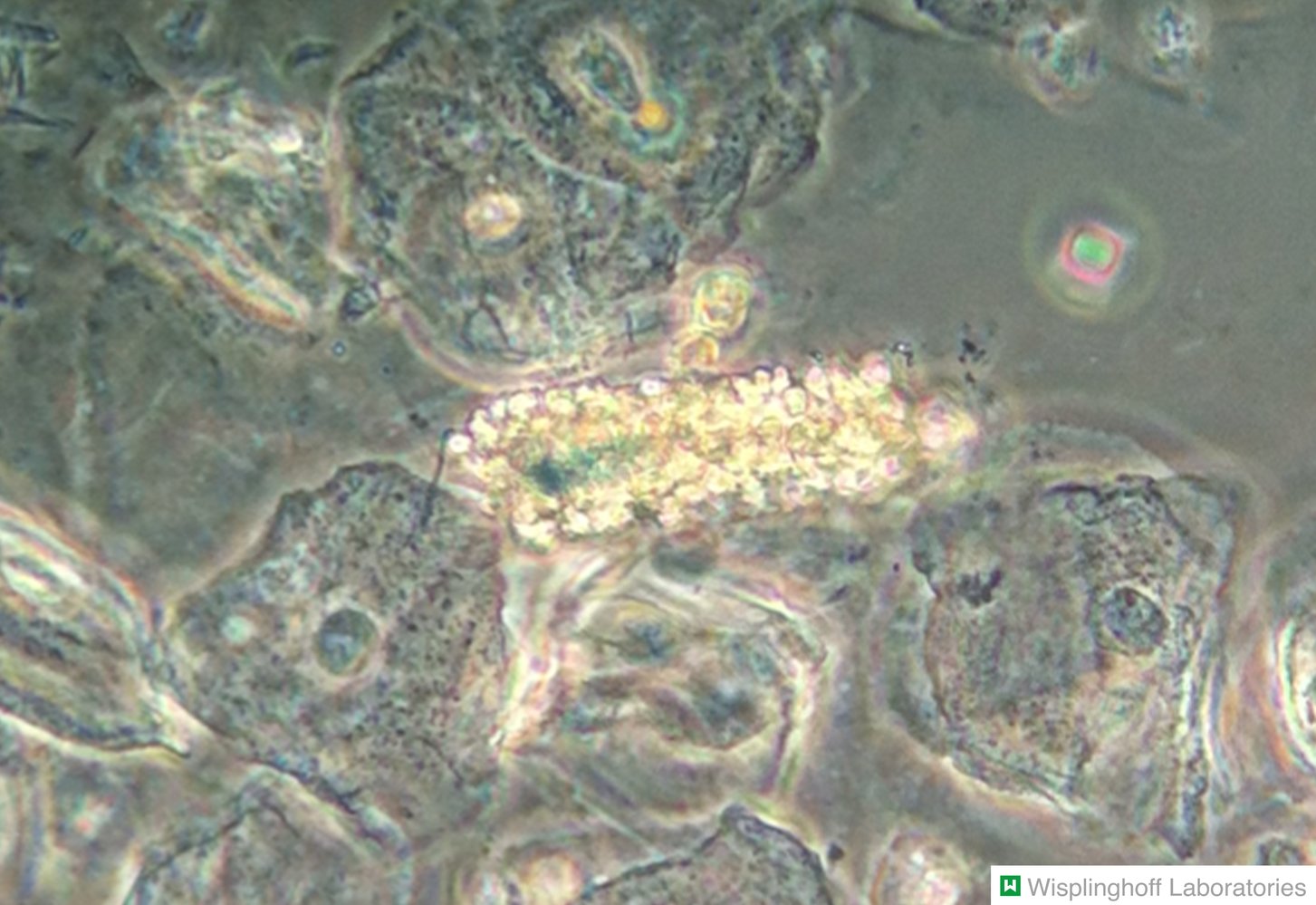
Photomicrograph of urine sediment (phase-contrast microscopy; high magnification)
White blood cell (WBC) casts (blue overlay) contain leukocytes (examples outlined in yellow) that are compressed in a matrix. Sharp margins are characteristic of WBC casts, differentiating them from randomly assembled leukocyte conglomerates.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.

Ultrasound right kidney (transverse plane)
There is marked dilatation of the collecting system (green overlay) with calyceal clubbing. Renal atrophy is seen as cortical thinning (red overlay).
These findings are consistent with grade 4 hydronephrosis (Society of Fetal Urology grading system).
Li: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Ultrasound left kidney (longitudinal plane)
The calyces (green overlay) are dilated and have lost their normal cup-shaped appearance. Flattening of papillae and blunting of fornices can be seen. Where visible, the renal cortical parenchyma is not thinned.
RP: renal parenchyma; Arrowheads: hyperechoic renal sinus
Source: “Ultrasonographic picture taken from a patient with left ureteral stone with hydronephrosis, created in Taiwan” by morning2k, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
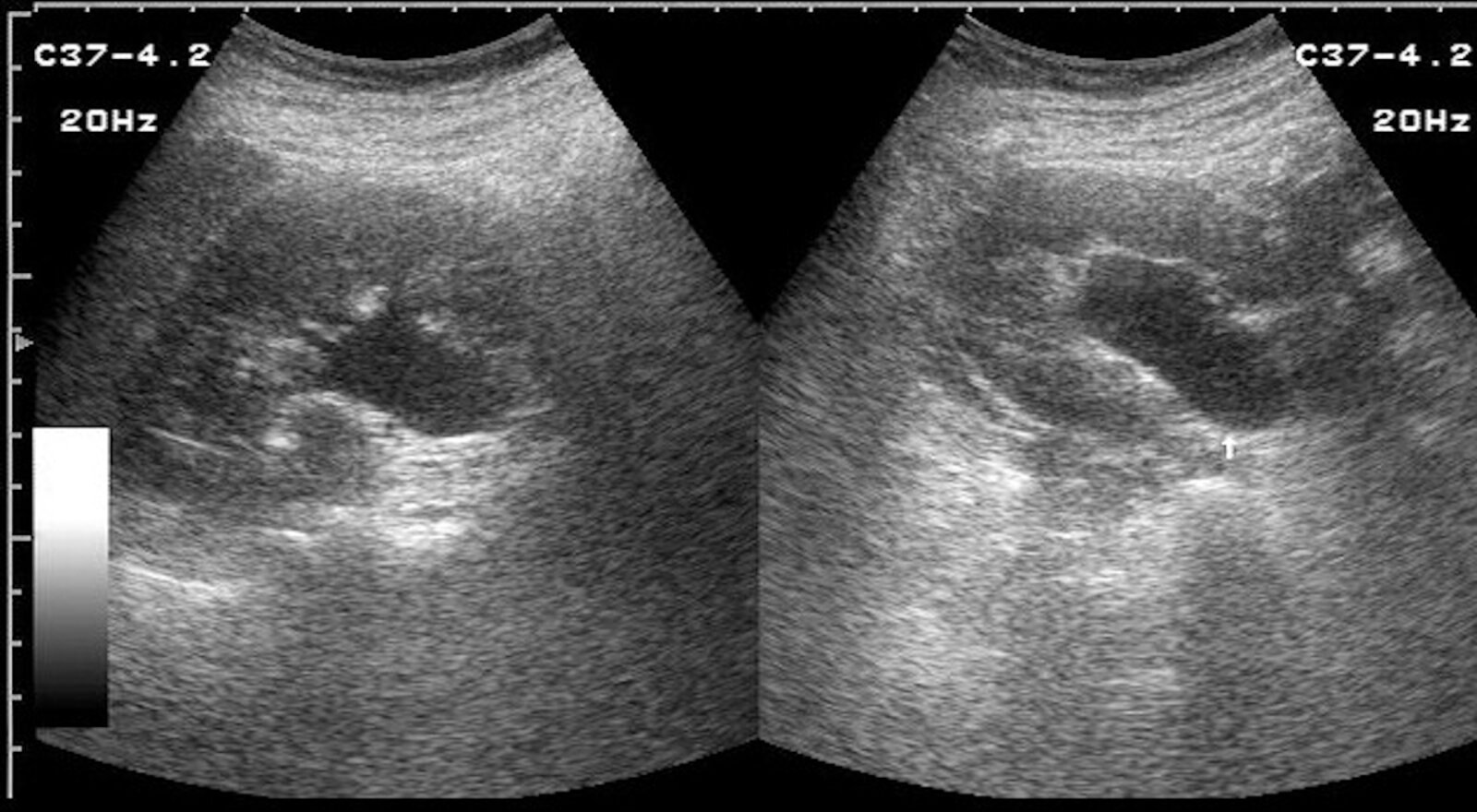
Kidney ultrasound (left: longitudinal section; right: transverse section)
The outline of the kidney is marked with a white dotted line. The renal pelvis (green overlay) is dilated.
This appearance is typical of a grade I hydronephrosis.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

CT abdomen and pelvis (without contrast; coronal plane) of a patient with a history of neurogenic bladder and recurrent urinary infections
The renal calyces, pelves, and ureters are dilated (green overlay), with normally concave (cup-shaped) renal calyces appearing convex (club-shaped; examples indicated by arrowheads). Thinning of the renal parenchyma (examples indicated by white dashed lines on the parenchymal edge) suggests that the dilatation is chronic rather than acute. Marked thickening of the bladder wall (red overlay) is likely responsible for chronic ureteral obstruction.
Source: “Figure 3: Computed tomography (coronal view) confirmed moderately severe bilateral hydronephrosis and hydroureter” by Subramanian Vaidyanathan, Fahed Selmi, Kottarathil Abraham Abraham, Peter Hughes, Gurpreet Singh & Bakul Soni, Patient Safety in Surgery Journal, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (without contrast; axial plane)
The rounded hyperdense structure (red arrow) medial to the left kidney is a ureteral calculus. Mild dilatation of the ureter (green overlay) is also visible. An additional, very small calculus (red overlay) is present in a dilated calyx.
K: kidney
Source: “Midureterstonehydro” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
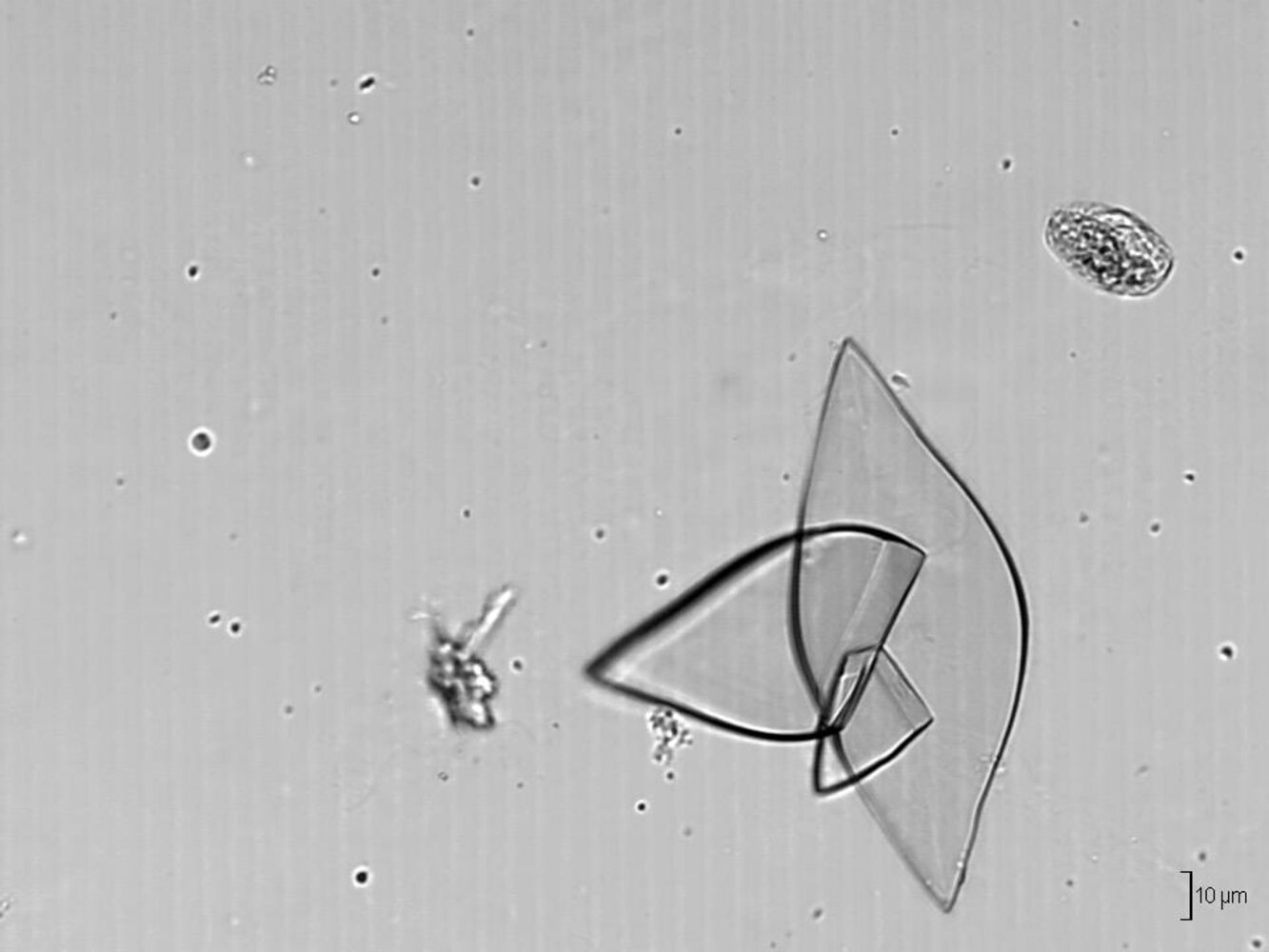
Photomicrograph of a urine sample with a pH of 5 (phase contrast microscopy; high magnification)
Multiple crystals of varying sizes and shapes can be seen (blue overlay).
Their diamond-shaped (rhomboid) form is one of the characteristic appearances of uric acid crystals, which only form in urine samples with a pH < 5.5 and are typically seen in patients with gout or in healthy individuals on a high-purine diet. Uric acid crystals may also appear barrel-shaped and needle-shaped (not seen in this image).
Source: “Uric acid crystals (urine) - Ürik asit kristalleri (idrar) - 03.png” by Doruk Salancı, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
_-_%C3%9Crik_asit_kristalleri_(idrar)_-_03.png){kind=link}
Management
Approach [7][8][9]
-
Initiate treatment for the underlying cause of AKI based on the presumed mechanism.
- Prerenal: Correct adverse hemodynamic factors and replace the depleted volume as needed.
- Postrenal: Relieve the urinary tract obstruction.
- Intrinsic: Consider a trial of IV fluids; identify and treat underlying causes that require specific interventions.
- Consider indications for acute dialysis and early nephrology consultation.
- Provide supportive care to all patients.
- Hold potentially nephrotoxic substances, ACE-Is, ARBs, NSAIDs, and nonessential medications.
- Adjust the dosing of essential renally cleared medications.
- Manage volume status and blood pressure to optimize kidney perfusion.
- Identify and manage complications (e.g., electrolyte disturbances, acidosis, fluid overload).
- Consider additional supportive care measures (e.g., nutritional support, VTE prophylaxis).
- Provide patient education and ensure adequate post-discharge follow-up.
AKI management is primarily supportive. Currently, there are no specific pharmacotherapies for AKI. [9]
Avoid coadministering RAAS inhibitors and NSAIDs in patients with reduced renal perfusion (e.g., in congestive heart failure, renal artery stenosis) because doing so can significantly decrease their GFR.
Early nephrology consult
-
Common indications [22]
- Indications for acute dialysis or renal biopsy
- AKI stage 3
- Inadequate response to initial treatment
- Intrinsic AKI
- Presence of CKD, if:
- The patient has received a renal transplant
- CKD category G4 or higher
Treatment of underlying causes [7][8][9]
| Treatment for the underlying cause of AKI | ||
|---|---|---|
| AKI subtype | Cause | Management |
| Prerenal |
|
|
|
|
|
|
|
|
|
|
|
| Intrinsic |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Postrenal |
|
|
|
|
|
The longer the underlying cause has been present, the greater the chance that AKI will progress to renal failure and/or CKD. Treat potential causes of AKI early.
Renal replacement therapy [7][9]
See also “Indications for acute dialysis.”
-
Indications; consider urgently for:
- Complications refractory to medical management
- Refractory fluid overload
- Electrolyte imbalances
- Acid-base disturbances
- Acute poisoning (e.g., by ethylene glycol); see “Approach to the poisoned patient.”
- Uremic symptoms
- Complications refractory to medical management
-
Modalities include: [7][9]
- Hemodialysis and/or hemofiltration (i.e., by CRRT or intermittent hemodialysis)
- Peritoneal dialysis [7]
Supportive care
The goal of supportive care is to avoid further renal insult and potentially aggravating factors, support adequate kidney perfusion, and ensure early identification and treatment of complications.
Medications and nephrotoxic substances [9]
-
Medication management
- Avoid nephrotoxic medications and drugs that may have a detrimental effect on glomerular perfusion.
- Discontinue metformin in patients with AKI to prevent development of metformin-associated lactic acidosis [27][28]
- Discontinue all nonessential renally cleared medications.
- For essential medications that are renally cleared, adjust dosing daily based on the patient's presumed GFR, considering the following: [9]
- Conventional eGFR formulas (e.g., Cockcroft-Gault, CKD-EPI equation, MDRD equation) are inaccurate in patients with AKI.
- GFR should be reestimated daily based on the patient's urine output and the trajectory of serum creatinine.
- The kinetic eGFR equation may provide an accurate estimation of GFR in this setting. [29][30][31]
-
Contrasted imaging
- Avoid iodinated contrast media to prevent contrast-induced nephropathy.
- The risk of CA-AKI is lower than previously thought; do not delay the use of contrast media in emergent situations to prevent CA-AKI. [27][28]
- Avoid gadolinium-based contrast agents to prevent nephrogenic systemic fibrosis.
Calculating eGFR using conventional equations does not accurately predict the true GFR in patients with AKI. Reestimate GFR daily based on the patient's urine output and the trajectory of serum creatinine.
Noncontrast imaging studies are preferred if possible. When the use of iodinated contrast is required for a critical diagnostic study or procedure (e.g., for the treatment of STEMI), the lowest clinical diagnostic dose should be used.
Volume status and blood pressure [8][9]
- Goal: optimize renal perfusion and reverse prerenal insults while avoiding fluid overload
-
Monitoring parameters
- Clinical assessment of volume status
- Fluid balance monitoring
- Hemodynamic monitoring
- Fluid responsiveness
- Management: Provide hemodynamic support and ensure continued fluid needs are met; see also “Daily fluid requirements for special patient groups.” [32]
| Hemodynamic support in patients with AKI according to presumed intravascular volume status | |
|---|---|
| Hypovolemia (and/or hypotension) |
|
| Hypervolemia |
|
| Euvolemia or indeterminate volume status |
|
Patients with AKI are at high risk of developing fluid overload, which can compromise renal function and may increase mortality. Avoid aggressive fluid resuscitation in patients who are not volume responsive.
Consider loop diuretics ONLY in patients with signs of fluid overload. Diuretics should not be used routinely to improve urine output in patients with AKI because of their lack of benefit and potential for harm. [7]
Choice of parenteral fluid [8][9][32]
- Use crystalloid solutions: Balanced IV fluid solutions, (e.g., lactated Ringer's, Plasma-Lyte A) may be preferred for most patients. [32]
- Avoid artificial colloids (e.g., hydroxyethyl starch). [8][9]
- Reserve IV albumin for select patients under specialist guidance. [33][34][35]
The use of balanced IV fluid solutions has been associated with lower mortality and better renal outcomes compared with the use of normal saline in patients with AKI.
Electrolyte and acid-base disorders
-
Goals
- To assess response to treatment and prevent complications of electrolyte disturbances
- To assess for complications of parenteral fluid therapy
- Monitoring parameters: BMP, calcium, phosphorus, magnesium, and ABG or VBG
-
Management [36]
- Obtain an urgent ECG in patients with significant potassium, calcium, and/or magnesium abnormalities.
- Address common metabolic complications of AKI.
- Follow therapeutic approach to hyperkalemia.
- Consider careful repletion regimens for hypocalcemia.
- Restrict dietary phosphate and consider oral phosphate binders for significant hyperphosphatemia.
- Acidemia: see “Indications for acute dialysis”
Obtain frequent (at least daily) laboratory studies to monitor for the presence of metabolic complications and response to treatment (e.g., improvement in creatinine levels).
Consider urgent renal replacement therapy for patients with refractory electrolyte or acid-base disturbances.
Additional considerations
-
Nutritional support [7][37]
- Ensure adequate protein and calorie intake.
- Consider dietary potassium and/or phosphate restriction for patients with hyperkalemia and/or hyperphosphatemia. [38]
-
Glucose management
- Consider insulin therapy to maintain serum glucose 110–149 mg/dL (6.1–8.3 mmol/L) in critically ill patients. [7][9]
- See also “Inpatient management of hyperglycemia.”
- Stress ulcer prophylaxis: Consider starting a PPI (e.g., pantoprazole) in critically ill patients who are at risk of GI bleeding. [39]
- VTE prophylaxis: If indicated, unfractionated heparin may be preferred over low molecular weight heparin (LMWH) or direct oral anticoagulants (DOACs) in patients with severe renal impairment.
- Uremia: Monitor for signs and symptoms; if present, consider renal replacement therapy.
The risk of GI bleeding may be increased in AKI due to uremic platelet dysfunction. [39]
Consider a nutrition consult for all patients with AKI. [37]
Follow-up care [40][41]
- Educate patients on medication management and the prevention of AKI.
- Monitor serum creatinine, eGFR, blood pressure, and weight following discharge. [40][42]
- Ensure that patients who require ongoing renal replacement therapy have access to outpatient dialysis services.
- Consider referral for outpatient nephrology follow-up in patients with significant residual renal dysfunction (i.e., eGFR < 60 mL/min).
Patients who recover from AKI are at high risk of readmission, mortality, cardiovascular events, progressive renal function deterioration, and developing de novo CKD. [40][41]
Adequate discharge planning and follow-up may help improve patient outcomes. [40][41]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Dot phrase
Prerenal AKI (inpatient management)
Assessment: This is a @AGE@-year-old @SEX@ presenting with [**acute rise in serum creatinine and/or reduction in urine output], most consistent with prerenal AKI due to [**volume depletion, decreased effective circulating volume, medications affecting renal perfusion].
Differential diagnoses: intrinsic AKI [**acute tubular necrosis, glomerulonephritis], postrenal AKI [**obstructive uropathy]
Plan
Disposition: Admit to [medical ward/ICU] for close monitoring and management based on [**evidence of volume depletion or hemodynamic instability, severe electrolyte abnormalities, signs of uremia (e.g., altered mental status, pericarditis), need for close monitoring of urine output and renal function].
Nephrology consult **[if Indications for acute dialysis or renal biopsy, stage 3 AKI, inadequate response to initial treatment, CKD in patients with a renal transplant or CKD category G4 or higher]
Stabilization and monitoring
–[**L NS or LR] for volume repletion, guided by clinical status, central venous pressure, and urine output
–Monitor MAP: Aim for ≥ 65 mm Hg.
–Goal urine output: ≥ 0.5 mL/kg/hour
–Daily labs: BMP, CBC
Cause-specific treatment
–[Volume depletion: aggressive fluid resuscitation with isotonic crystalloids]
–[Decreased effective circulating volume: Treat the underlying cause (e.g., heart failure, cirrhosis) while cautiously optimizing fluid status.]
–[Medications: Discontinue nephrotoxic agents (e.g., NSAIDs, ACEIs, ARBs) and adjust doses of renally cleared drugs.]
F/E/N
–Maintain adequate caloric intake.
–Protein restriction if severe azotemia is present
–HyperK (if emergency)
–IV Ca gluconate
–Insulin + D5
–Albuterol
–Bicarb (if acidosis)
–Loop diuretics
–K+ binders
–RRT
–Acidosis: bicarb if pH < 7.2
–HyperPhos: Phos binders if > 6 mg/dL
–HypoCa: Replace only if symptomatic or severe.
ATN (inpatient management)
Assessment: This is a @AGE@-year-old @SEX@ presenting with AKI [**elevated Cr, oliguria/anuria]. Clinical history and findings suggest ATN due to [**ischemia, sepsis, nephrotoxins [**contrast, meds, myoglobin]]. Supporting labs include [**urine muddy brown casts, renal tubular epithelial cells. FENa > 2% (if not on diuretics), urine Na > 40 mEq/L, low osmolality (< 350 mOsm/kg)] and [**serum elevated BUN/Cr with BUN:Cr ratio < 15].
Differential diagnoses: prerenal AKI (e.g., hypovolemia, hypoperfusion), postrenal AKI (e.g., obstruction), glomerular diseases (e.g., GN, vasculitis)
Plan
Disposition: Admit to [medical ward/ICU] for monitoring and management of [**persistent AKI unresponsive to fluid resuscitation, electrolyte derangements (e.g., hyperK), uremic symptoms (e.g., encephalopathy, pericarditis)]
–Strict I/Os
–Daily labs: BMP, Mg, Phos, CBC
–[Continuous telemetry if hyperkalemic].
–Stop nephrotoxins: Avoid NSAIDs, ACEis/ARBs, and contrast.
–Adjust meds for renal dosing.
–[**Ischemic ATN: Optimize perfusion with blood pressure support (IVF, vasopressors if needed)].
–Nephrology consult for worsening AKI or dialysis need [pH < 7.1 refractory to Tx; K > 6.5 or severe dysrhythmias; dialyzable toxins (e.g., methanol, lithium); refractory pulm/peripheral edema; symptomatic uremia (encephalopathy, pericarditis)]
F/E/N
–[Hypovolemic]: [**L] LR/NS bolus; reassess frequently.
–[Euvolemic/hypervolemic]: fluid restriction ± loop diuretics for volume overload
–Match fluid and electrolyte losses to prevent secondary kidney injury
HyperK
–IV Ca gluconate
–Insulin + D5
–Albuterol
–Bicarb (if acidosis)
–Loop diuretics
–K+ binders
–RRT
–Acidosis: bicarb if pH < 7.2
–HyperPhos: Phos binders if > 6 mg/dL
–HypoCa: Replace only if symptomatic or severe.
–Maintain calorie intake.
–Protein restriction in severe azotemia
Special patient groups
Neonatal acute kidney injury [43][44][45]
- Epidemiology: AKI is common in critically ill newborns (approx. 30% of NICU patients). [45]
-
Etiology [46]
- ∼85% prerenal
- ∼10% renal
- ∼5% postrenal
-
Infant risk factors
- Perinatal: prematurity, low birth weight, asphyxia, congenital heart disease
- Inflammatory: NEC, sepsis
- Iatrogenic: nephrotoxic medications, cardiac surgery, ECMO therapy
-
Diagnostics: Modifications to KDIGO staging [44]
- Baseline serum creatinine in neonates is defined as the lowest previously measured value.
- The cut-off for AKI stage 3 is a serum creatinine level ≥ 3 times baseline OR ≥ 2.5 mg/dL.
- Accurate measurement of urine output in neonates poses challenges (esp. regarding urine collection) but is still being used to diagnose and stage AKI.
- Other diagnostic biomarkers, e.g., cystatin C, are currently being investigated to improve early and accurate detection of AKI in neonates. [44]
- See “Diagnostics” section above.
-
Management
- Monitor serum creatinine and urine output in at-risk neonates.
- Treat underlying causes.
- Avoid/adjust nephrotoxic medications.
- Provide supportive management (e.g., fluid, electrolyte, and nutritional).
- Consider renal replacement therapy.
Prevention
Identify patients who are at risk of AKI and implement appropriate preventive strategies. [1][7][22]
| Prevention of acute kidney injury | |
|---|---|
| Risk factors | Preventive strategies |
| Acute illness |
|
| Nephrotoxic medication exposure |
|
| Iodinated radiocontrast agent exposure |
|
| Liver failure |
|
| Surgery |
|
| Endogenous nephrotoxins |
|
Related One-Minute Telegram
- One-Minute Telegram 51-2022-3/3: Are glucocorticoids a safe and effective treatment for IgA nephropathy?
- One-Minute Telegram 39-2021-1/3: Estimating glomerular filtration rate: Not a matter of race
- One-Minute Telegram 14-2020-3/3: GFR formulas are just estimates, but can we estimate better?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Rahman M, Shad F, Smith MC. "Acute kidney injury: a guide to diagnosis and management.". Am Fam Physician. 86(7). :631-9. (2012)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Basile DP, Anderson MD, Sutton TA. "Pathophysiology of acute kidney injury". Compr Physiol. 2(2). :1303-53. (2012)
- Prakash J, Singh VP. "Changing picture of renal cortical necrosis in acute kidney injury in developing country.". World journal of nephrology. 4(5). :480-6. (2015)
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 25th Edition". Elsevier. (2016). ISBN: 9781455750177
- "KDIGO Clinical Practice Guideline for Acute Kidney Injury". https://kdigo.org/guidelines/acute-kidney-injury/. [2012-01-01]
- Mercado MG, Smith DK, Guard EL. "Acute Kidney Injury: Diagnosis and Management.". Am Fam Physician. 100(11). :687-694. (2019)
- Moore PK, Hsu RK, Liu KD. "Management of Acute Kidney Injury: Core Curriculum 2018". American Journal of Kidney Diseases. 72(1). :136-148. (2018)
- Pahwa AK, Sperati CJ. "Urinary fractional excretion indices in the evaluation of acute kidney injury". Journal of Hospital Medicine. 11(1). :77-80. (2015)
- Manoeuvrier G, Bach-Ngohou K, Batard E, Masson D, Trewick D. "Diagnostic performance of serum blood urea nitrogen to creatinine ratio for distinguishing prerenal from intrinsic acute kidney injury in the emergency department". BMC Nephrol. 18(1). (2017)
- Schrier RW. "Blood Urea Nitrogen and Serum Creatinine". Circulation: Heart Failure. 1(1). :2-5. (2008)
- MILLER TR. "Urinary Diagnostic Indices in Acute Renal Failure". Ann Intern Med. 89(1). :47. (1978)
- Simerville JA, Maxted WC, Pahira JJ. "Urinalysis: a comprehensive review". Am Fam Physician. 71(6). :1153-62. (2005)
- Gotfried J, Wiesen J, Raina R, Nally JV. "Finding the cause of acute kidney injury: Which index of fractional excretion is better?". Cleve Clin J Med. 79(2). :121-126. (2012)
- Wilson DR, Wilson DDR. "Pathophysiology of obstructive nephropathy". Kidney Int. 18(3). :281-292. (1980)
- Remer EM, Papanicolaou N, Casalino DD, et al. "ACR Appropriateness Criteria® on Renal Failure". Am J Med. 127(11). :1041-1048.e1. (2014)
- Podoll A, Walther C, Finkel K. "Clinical utility of gray scale renal ultrasound in acute kidney injury". BMC Nephrol. 14(1). (2013)
- Ather MH, Jafri AH, Sulaiman MN. "Diagnostic accuracy of ultrasonography compared to unenhanced CT for stone and obstruction in patients with renal failure". BMC Med Imaging. 4(1). (2004)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Raina R, Krishnappa V, Blaha T, et al. "Atypical Hemolytic-Uremic Syndrome: An Update on Pathophysiology, Diagnosis, and Treatment". Therapeutic Apheresis and Dialysis. 23(1). :4-21. (2018)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- "Acute kidney injury: prevention, detection, and management". https://www.nice.org.uk/guidance/ng148. [2019-12-18]
- Davenport MS, Perazella MA, Yee J, et al. "Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation". Radiology. 294(3). :660-668. (2020)
- Howard SC, Jones DP, Pui C-H. "The Tumor Lysis Syndrome". N Engl J Med. 364(19). :1844-1854. (2011)
- "Clinical Practice Guideline Acute Kidney Injury (AKI)". https://web.archive.org/web/20211012081337/https://ukkidney.org/sites/renal.org/files/FINAL-AKI-Guideline.pdf. [2019-08-01]
- Esson ML. "Diagnosis and Treatment of Acute Tubular Necrosis". Ann Intern Med. 137(9). :744. (2002)
- Ramoutar V, Landa C, James LR. "Acute tubular necrosis (ATN) presenting with an unusually prolonged period of marked polyuria heralded by an abrupt oliguric phase". Case Reports. 2014(aug22 1). :bcr2013201030-bcr2013201030. (2014)
- Ali A, Bhan C, Malik MB, Ahmad MQ, Sami SA. "The Prevention and Management of Contrast-induced Acute Kidney Injury: A Mini-review of the Literature". Cureus. (2018)
- Ghossein C, Varga J, Fenves AZ. "Recent Developments in the Classification, Evaluation, Pathophysiology, and Management of Scleroderma Renal Crisis". Curr Rheumatol Rep. 18(1). (2015)
- "Manual on Contrast Media". https://web.archive.org/web/20260420113659/https://www.acr.org/Clinical-Resources/Clinical-Tools-and-Reference/Contrast-Manual. [2025-01-01]
- Pelletier K, Lafrance J-P, Roy L, et al. "Estimating glomerular filtration rate in patients with acute kidney injury: a prospective multicenter study of diagnostic accuracy". Nephrology Dialysis Transplantation. 35(11). :1886-1893. (2019)
- Bairy M. "Using Kinetic eGFR for Drug Dosing in AKI: Concordance between Kinetic eGFR, Cockroft-Gault Estimated Creatinine Clearance, and MDRD eGFR for Drug Dosing Categories in a Pilot Study Cohort". Nephron. 144(6). :299-303. (2020)
- Chen S. "Retooling the Creatinine Clearance Equation to Estimate Kinetic GFR when the Plasma Creatinine Is Changing Acutely". J Am Soc Nephrol. 24(6). :877-888. (2013)
- Prowle JR, Kirwan CJ, Bellomo R. "Fluid management for the prevention and attenuation of acute kidney injury". Nature Reviews Nephrology. 10(1). :37-47. (2013)
- Sola E, Guevara M, Gines P. "Current treatment strategies for hepatorenal syndrome". Clin Liver Dis (Hoboken). 2(3). :136-139. (2013)
- Salerno F, Navickis RJ, Wilkes MM. "Albumin Infusion Improves Outcomes of Patients With Spontaneous Bacterial Peritonitis: A Meta-analysis of Randomized Trials". Clinical Gastroenterology and Hepatology. 11(2). :123-130.e1. (2013)
- Duffy M, Jain S, Harrell N, Kothari N, Reddi AS. "Albumin and Furosemide Combination for Management of Edema in Nephrotic Syndrome: A Review of Clinical Studies.". Cells. 4(4). :622-30. (2015)
- Leaf DE, Christov M. "Dysregulated Mineral Metabolism in AKI". Semin Nephrol. 39(1). :41-56. (2019)
- Brown RO, Compher C. "A.S.P.E.N. Clinical Guidelines: Nutrition Support in Adult Acute and Chronic Renal Failure". Journal of Parenteral and Enteral Nutrition. 34(4). :366-377. (2010)
- Meyer D, Mohan A, Subev E, Sarav M, Sturgill D. "Acute Kidney Injury Incidence in Hospitalized Patients and Implications for Nutrition Support". Nutrition in Clinical Practice. 35(6). :987-1000. (2020)
- Ye Z, Reintam Blaser A, Lytvyn L, et al. "Gastrointestinal bleeding prophylaxis for critically ill patients: a clinical practice guideline". BMJ. :l6722. (2020)
- Vanmassenhove J, Vanholder R, Lameire N. "Points of Concern in Post Acute Kidney Injury Management". Nephron. 138(2). :92-103. (2017)
- Ostermann M, Bellomo R, Burdmann EA, et al. "Controversies in acute kidney injury: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference". Kidney Int. 98(2). :294-309. (2020)
- Starr MC, Menon S. "Neonatal acute kidney injury: a case-based approach". Pediatr Nephrol. 36(11). :3607-3619. (2021)
- Coleman C, Tambay Perez A, Selewski DT, Steflik HJ. "Neonatal Acute Kidney Injury". Front Pediatr. 10. (2022)
- Jetton JG, Boohaker LJ, Sethi SK, et al. "Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study". The Lancet Child Adolesc Health. 1(3). :184-194. (2017)
- Nada A, Bonachea EM, Askenazi DJ. "Acute kidney injury in the fetus and neonate". Semin Fetal Neonatal Med. 22(2). :90-97. (2017)