Summary
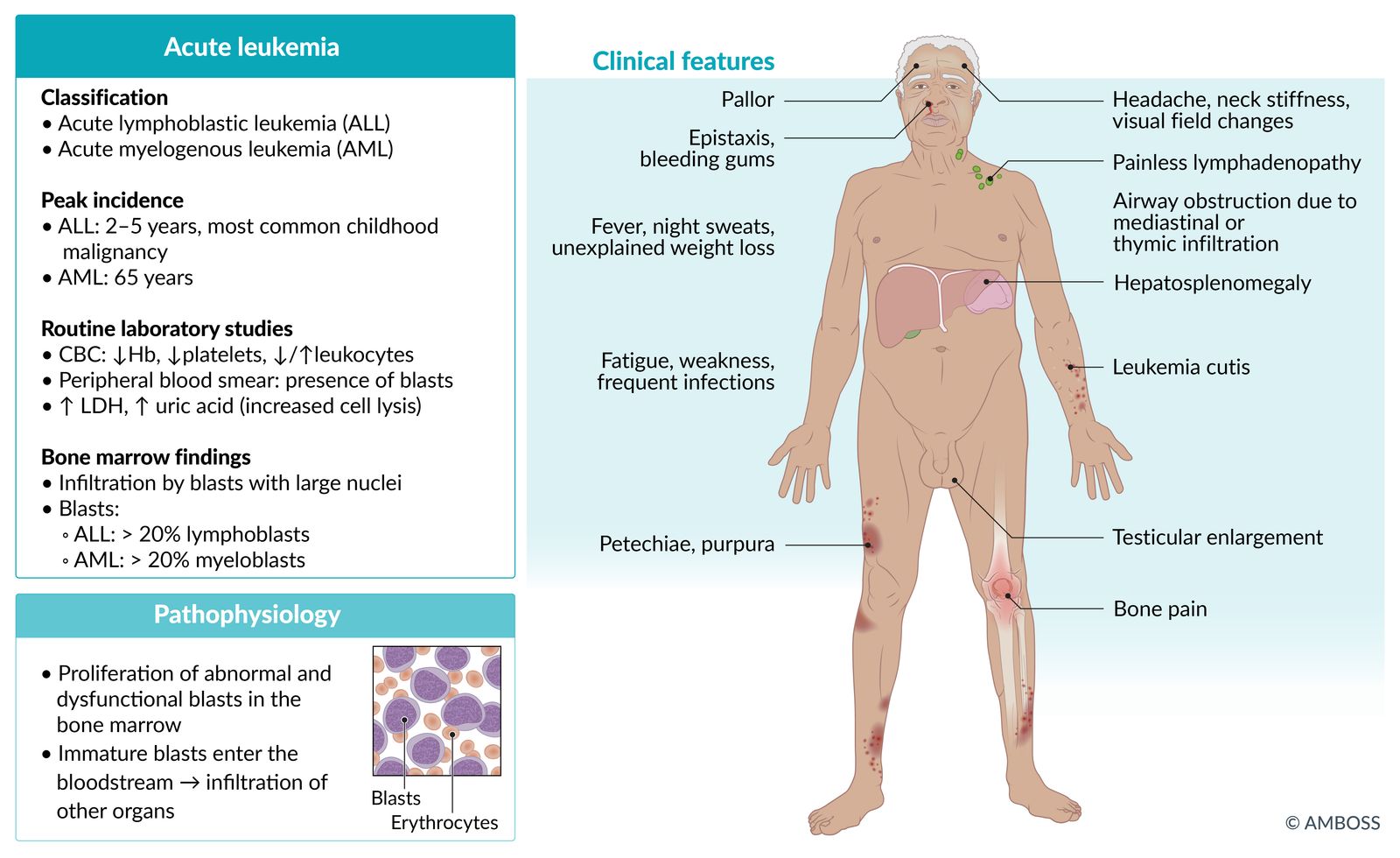
Acute leukemias are malignant neoplastic diseases that arise from either the lymphoid or myeloid cell line. Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy, whereas acute myeloid leukemia (AML) primarily affects adults. The underlying cause of acute leukemia is rarely identifiable, but risk factors include prior chemotherapy and radiation therapy, and hereditary syndromes such as Down syndrome. AML is also associated with preexisting hematologic disorders (e.g., myelodysplastic disorder, myeloproliferative disorders). Acute leukemias are characterized by the proliferation of immature, nonfunctional WBCs (blasts) in the bone marrow, which impairs normal hematopoiesis. This leads to pancytopenia, which manifests with symptoms and signs of anemia (decreased RBCs), clotting disorders (decreased platelets), and immunocompromise (decreased fully functional, mature WBCs). Patients with acute leukemia, especially those with AML, may develop extremely high WBC counts, increasing the risk of leukostasis and disseminated intravascular coagulation (DIC). Leukemic cells can also infiltrate extramedullary organs, resulting in hepatosplenomegaly, renal impairment, meningeal leukemia, and, less commonly, involvement of the skin and/or testicles. The first diagnostic steps include a complete blood count and peripheral blood smear to determine the patient's WBC count and assess for the presence of blasts. Bone marrow aspiration and biopsy are typically used to confirm the diagnosis, and subsequent cytogenetic analysis and immunophenotyping are used to identify subtypes and specific mutations. A chemotherapy regimen consisting of high-dose (induction) and low-dose (consolidation and maintenance) cycles is the mainstay of treatment. Additional measures, such as allogeneic stem cell transplantation, may be indicated in patients with poor prognostic factors (e.g., unfavorable cytogenetics) or if initial chemotherapy fails.

© AMBOSS
Epidemiology
-
Acute lymphoblastic leukemia [1]
- Peak incidence: 2–5 years
- Most common malignant disease in children
- ∼ 80% of acute leukemias during childhood are lymphoblastic.
- ♂ > ♀
-
Acute myeloid leukemia [2]
- Peak incidence: 65 years
- 80% of acute leukemias during adulthood are myelogenous.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Acute lymphoblastic leukemia (ALL)
- No identifiable cause or risk factors in most cases
- Prior bone marrow damage due to alkylating chemotherapy or ionizing radiation
- Adult T-cell leukemia/lymphoma is linked to infection with HTLV. [3][4][5]
-
Genetic or chromosomal factors
- Down syndrome: Risk of ALL is, like that of AML, 10–20 times higher in patients with Down syndrome compared to the general population. [6][7]
- Neurofibromatosis type 1
- Ataxia telangiectasia [1]
Acute myeloid leukemia (AML)
- No identifiable cause or risk factors in most cases
-
Pre-existing hematopoietic disorder (most common identifiable cause) ; [8]
- Myelodysplastic syndromes
- Aplastic anemia
- Myeloproliferative disorders (e.g., osteomyelofibrosis; , CML)
-
Environmental factors [2]
- Alkylating chemotherapy
- Ionizing radiation
- Benzene exposure
- Tobacco
-
Genetic or chromosomal factors
- Down syndrome: The risk of AML is, like that of ALL, 10–20 times higher in patients with Down syndrome compared to the general population. [7]
- Fanconi anemia



References:[9][10]
© AMBOSS
© AMBOSS
© AMBOSS
Classification
ALL [11]
-
French-American-British (FAB) historical classification of ALL
- L1 ALL with small cells (20–30%)
- L2 ALL with heterogeneous large cells (70%)
- L3 ALL with large cells, i.e., Burkitt lymphoma (1–2%)
-
The WHO Classification of Haematolymphoid Tumours (2022) organizes ALL into subtypes based on immunophenotypic, cytogenetic, and molecular factors. [11]
-
B-cell lymphoblastic leukemias/lymphomas: B-cell ALL (∼ 80–85% of ALL cases)
-
B-ALL categorized by cytogenetic or molecular genetic findings, e.g.:
- B-ALL with high hyperdiploidy
- B-ALL with BCR-ABL1
- B-ALL with ETV6-RUNX1
- B-ALL with other defined genetic abnormalities
- B-ALL not otherwise specified
-
B-ALL categorized by cytogenetic or molecular genetic findings, e.g.:
- T-lymphoblastic leukemias/lymphomas: T-cell ALL (∼ 15–20% of ALL cases),e.g., early T-precursor ALL
-
B-cell lymphoblastic leukemias/lymphomas: B-cell ALL (∼ 80–85% of ALL cases)


AML [12]
- The French-American-British (FAB) classification distinguishes between eight subtypes of AML, according to the histopathological appearance of the cells.
| FAB classification for AML | |
|---|---|
| M0-AML | Acute myeloblastic leukemia without maturation |
| M1-AML | Acute myeloblastic leukemia with minimal granulocyte maturation |
| M2-AML | Acute myeloblastic leukemia with granulocyte maturation |
| M3-AML | Acute promyelocytic leukemia (APL) |
| M4-AML | Acute myelomonocytic leukemia |
| M5-AML | Acute monocytic leukemia |
| M6-AML | Acute erythroid leukemia |
| M7-AML | Acute megakaryoblastic leukemia |
-
The WHO Classification of Haematolymphoid Tumours (2022) is based on the presence of defining genetic abnormalities or, in their absence, morphological differentiation. [12]
- AML with defining genetic abnormalities
- AML, defined by differentiation
- AML, myelodysplasia-related
- Myeloid sarcoma
- Diagnostic qualifiers for secondary myeloid neoplasms:
- Myeloid neoplasm post cytotoxic therapy
- Myeloid neoplasm associated with germline predisposition
- Myeloid proliferation associated with Down syndrome



References:[8]
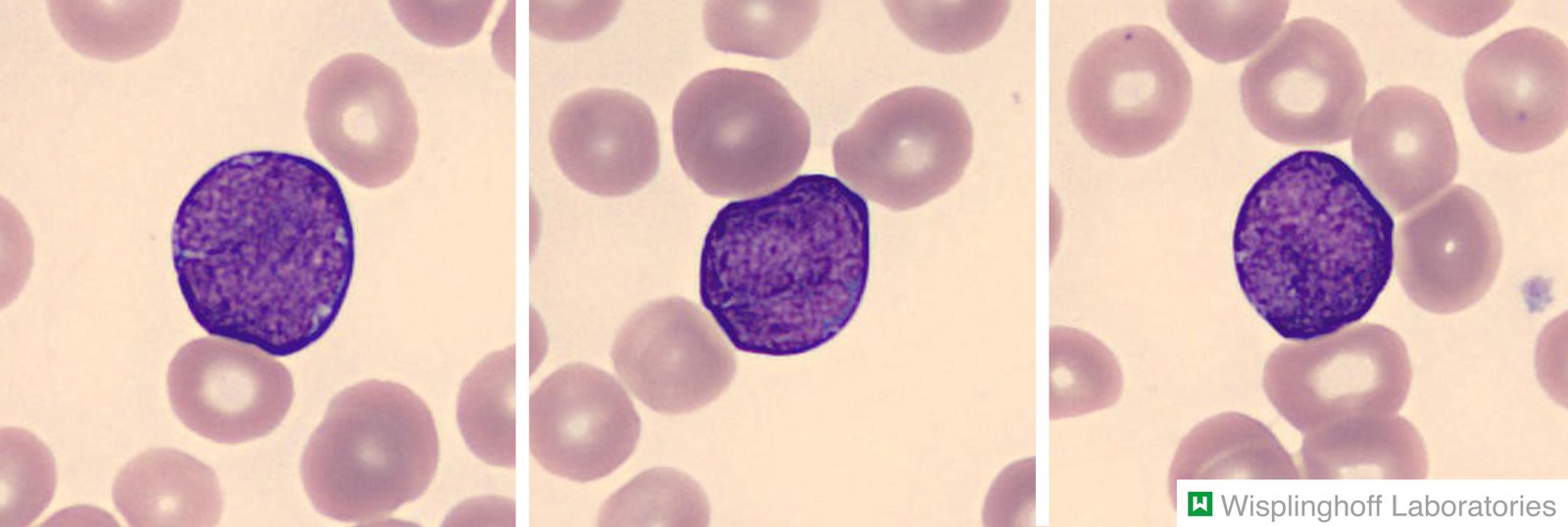
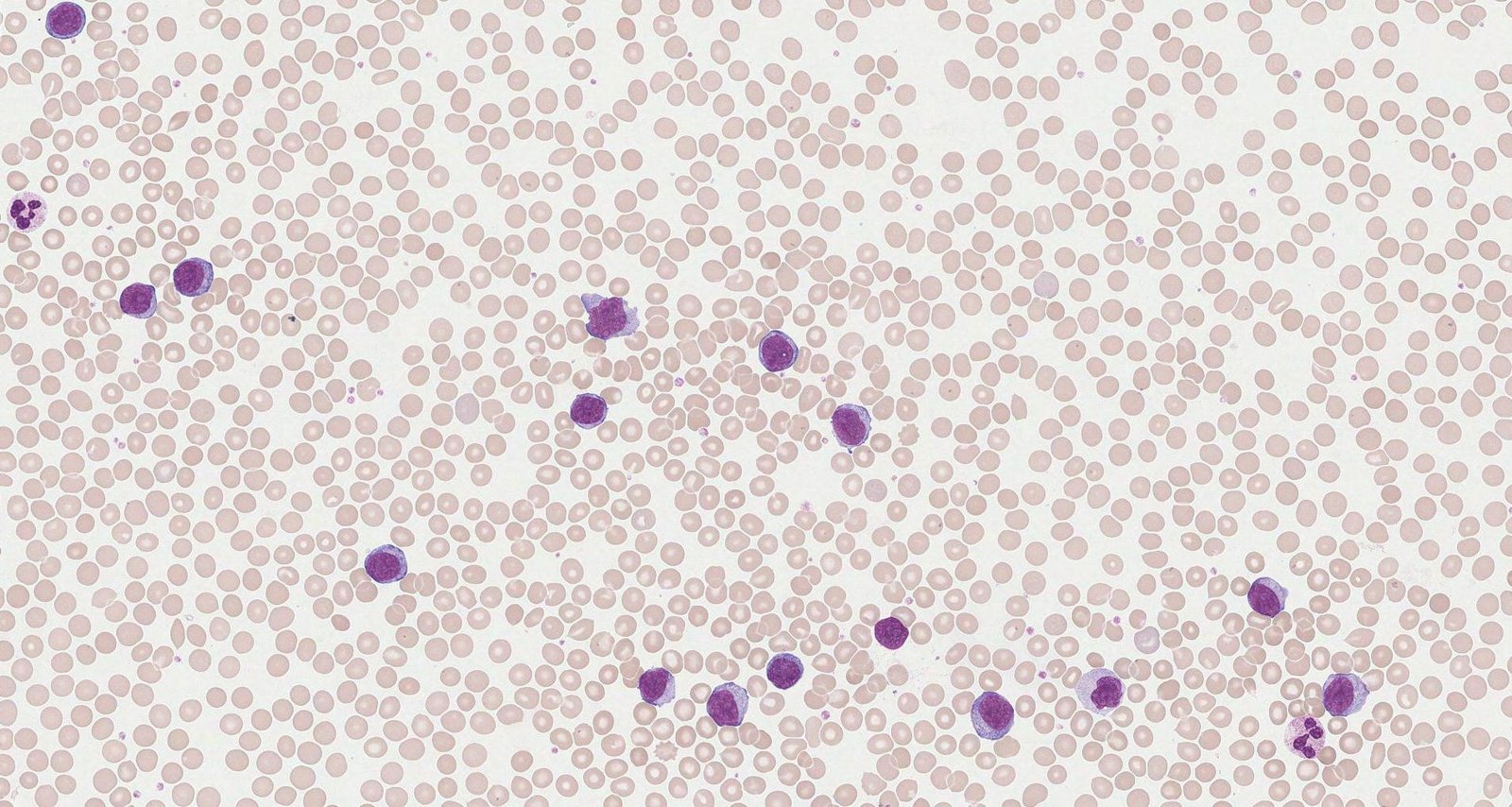
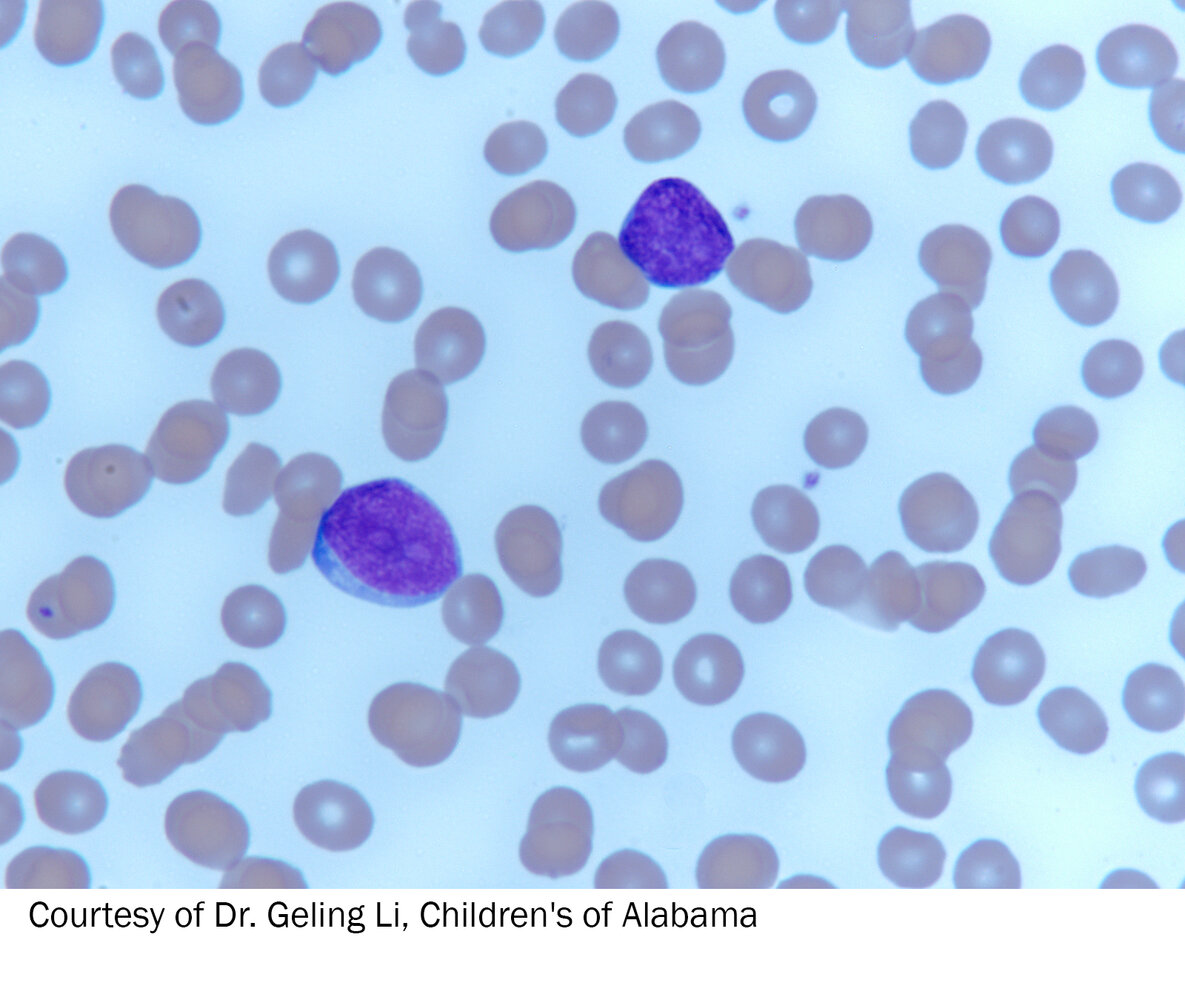
Photomicrographs of a peripheral blood smear (H&E stain; very high magnification)
The large basophilic cell in the center of each photomicrograph is a lymphoblast, identifiable by its large spherical nucleus surrounded by a thin rim of cytoplasm (high nucleocytoplasmic ratio). The nucleus of the lymphoblasts is often indented (green arrows) and shows fine loose (noncondensed) chromatin. Lymphoblasts differ from lymphocytes, which are smaller in size with smaller nuclei, condensed chromatin, and more cytoplasm.
The presence of numerous lymphoblasts in a peripheral blood smear is indicative of lymphoblastic leukemia. The diagnosis of B-cell ALL was confirmed on immunophenotyping.
Note: Basophilic remnants (Howell-Jolly bodies) are visible within the erythrocytes in the last photomicrograph, indicating (in this case) increased hematopoiesis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
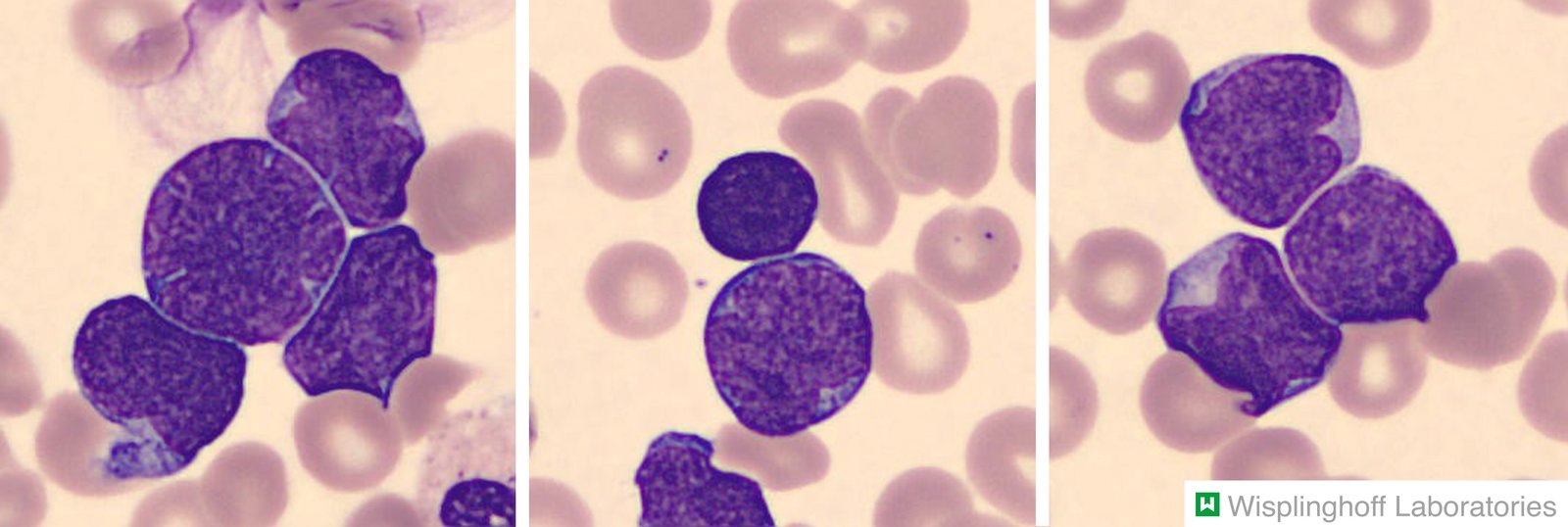
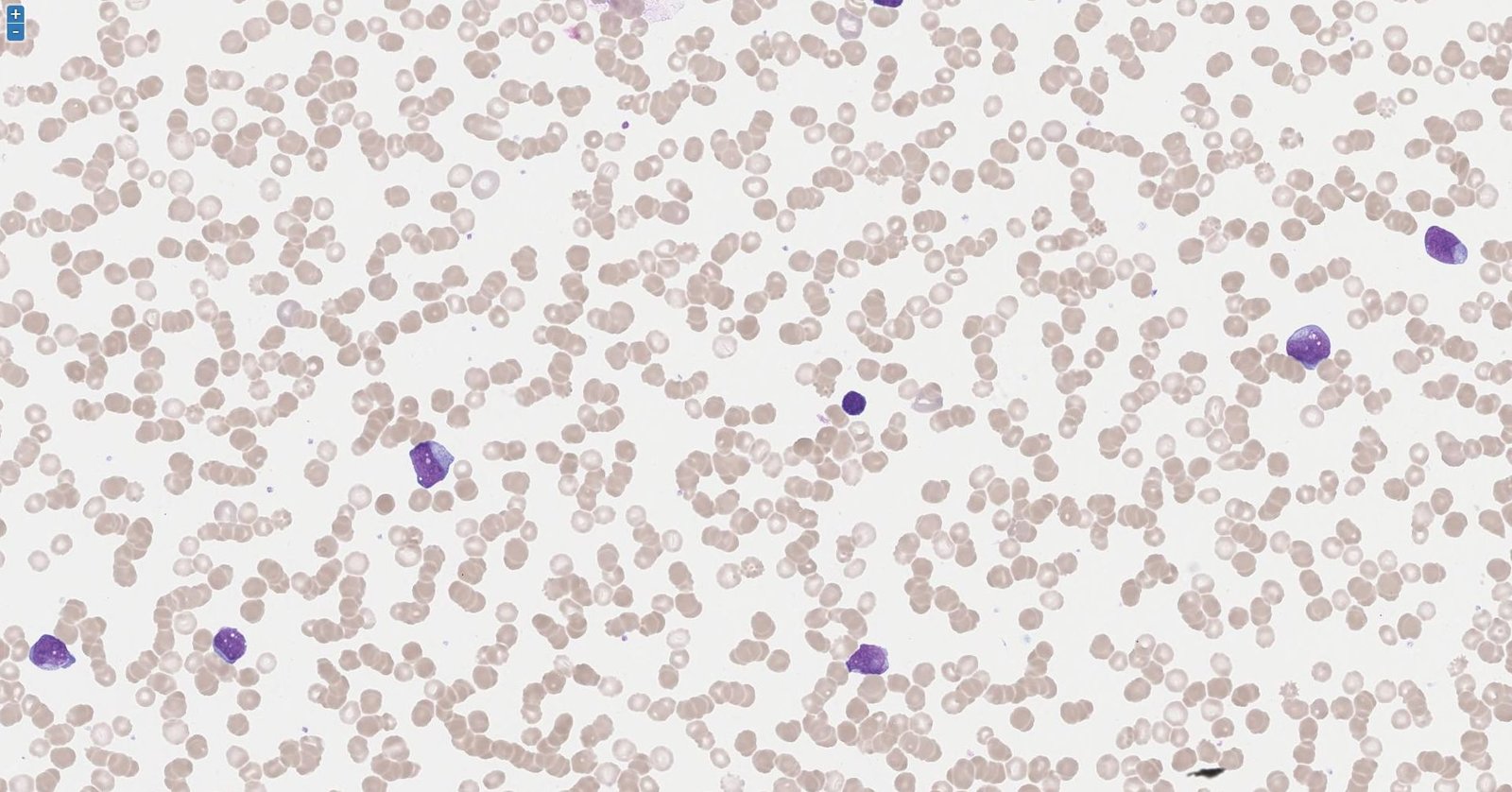
Photomicrographs of a peripheral blood smear (H&E stain; very high magnification)
The basophilic cell clusters in the center of each photomicrograph are mainly composed of lymphoblasts, identifiable by their large size, large spherical nucleus that is surrounded by a thin rim of cytoplasm (high nucleocytoplasmic ratio). The nucleus of the lymphoblasts is often indented and shows fine loose (noncondensed) chromatin. Lymphoblasts differ from lymphocytes, which are smaller in size with smaller nuclei, condensed chromatin, and more cytoplasm.
The presence of numerous lymphoblasts in a peripheral blood smear is indicative of lymphoblastic leukemia. The diagnosis of T-cell ALL was confirmed on immunophenotyping.
Note: Basophilic remnants (Howell-Jolly bodies) are visible within some of the erythrocytes, indicating (in this case) increased hematopoiesis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
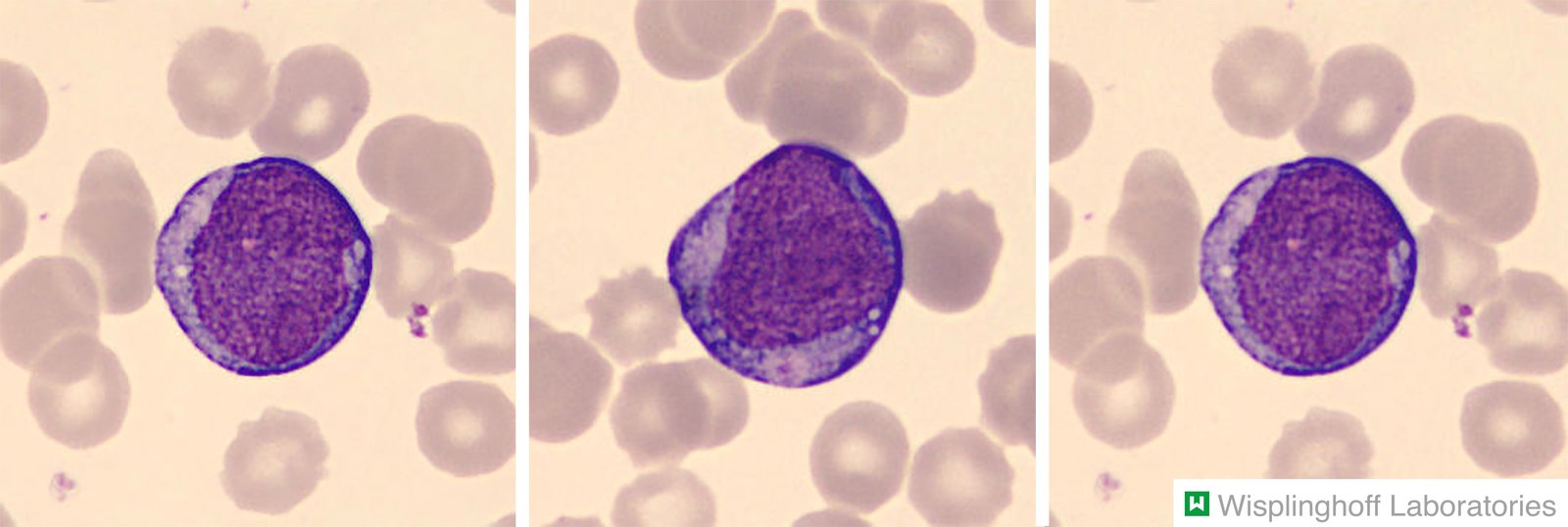
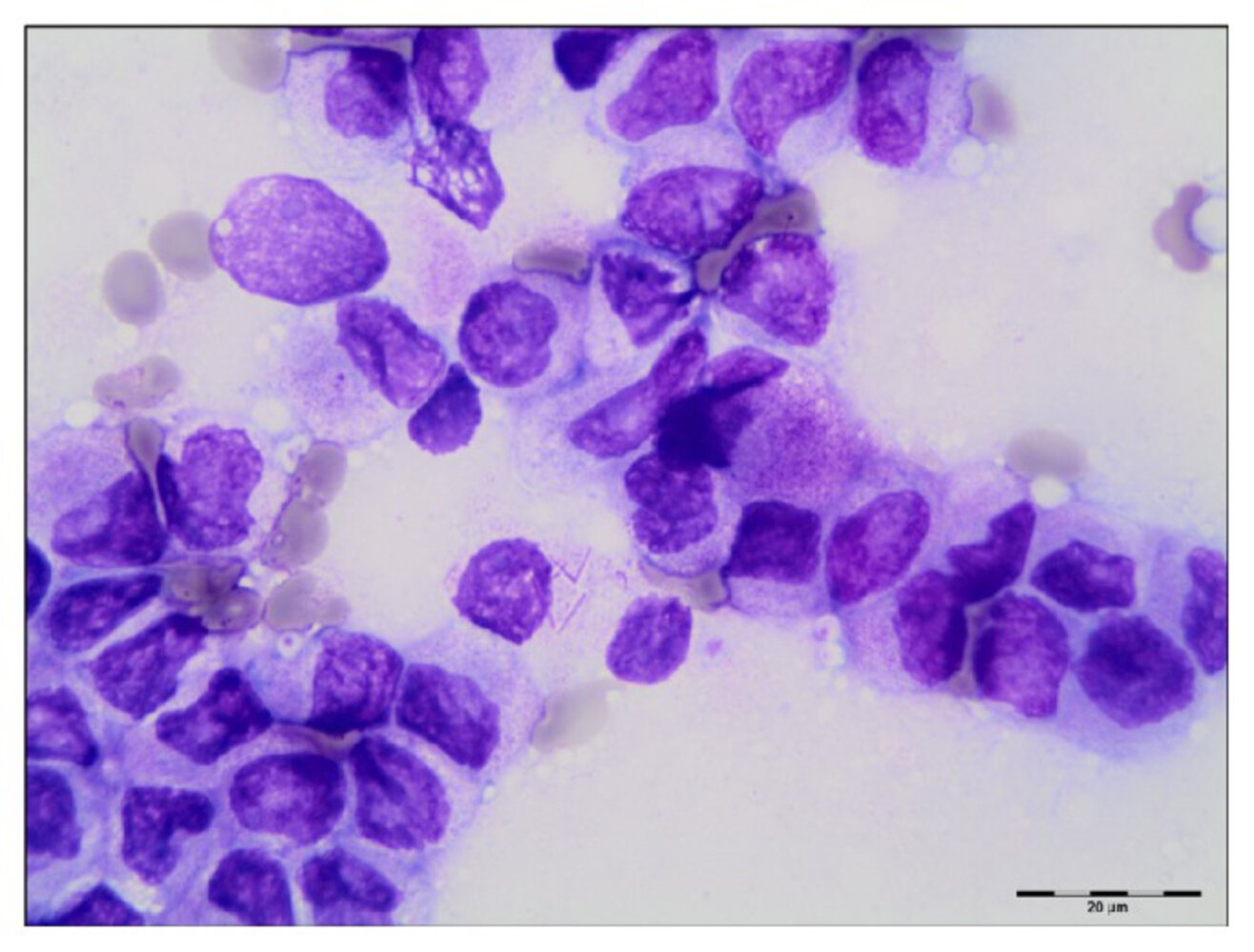
Photomicrographs of a bone marrow smear (H&E stain; very high magnification)
The large basophilic cell visible in each photomicrograph is a monocyte, identifiable by its large size, folded or lobed nucleus with fine chromatin and prominent nucleoli (green overlay), and abundant granular cytoplasm with cytoplasmic vacuoles.
Numerous monocytes on bone marrow biopsy is characteristically seen in acute monocytic leukemia. The diagnosis is confirmed on immunophenotyping.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
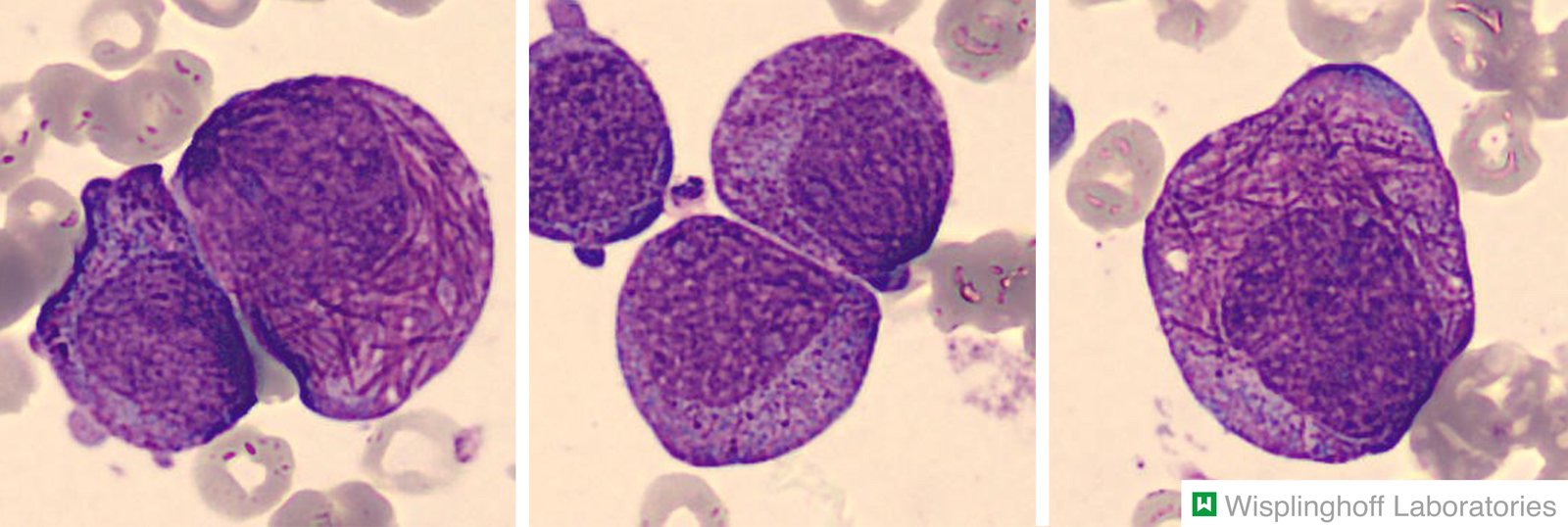
Photomicrographs of a peripheral blood smear (H&E stain; very high magnification)
The large basophilic cells are promyelocytes, identifiable by their eccentric nuclei and abundant basophilic cytoplasm containing numerous Auer rods (rod-like intracytoplasmic inclusion bodies). This type of hypergranular leukemic promyelocyte is often still referred to as a “faggot cell” for the resemblance of accumulation of Auer rods to a “bundle of sticks,” although the term is typically avoided today due to its derogatory associations.
The presence of promyelocytes containing Auer rods in a peripheral blood smear is characteristic of acute promyelocytic leukemia.
Note: Basophilic remnants (Howell-Jolly bodies) are visible within most of the erythrocytes, indicating (in this case) increased hematopoiesis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
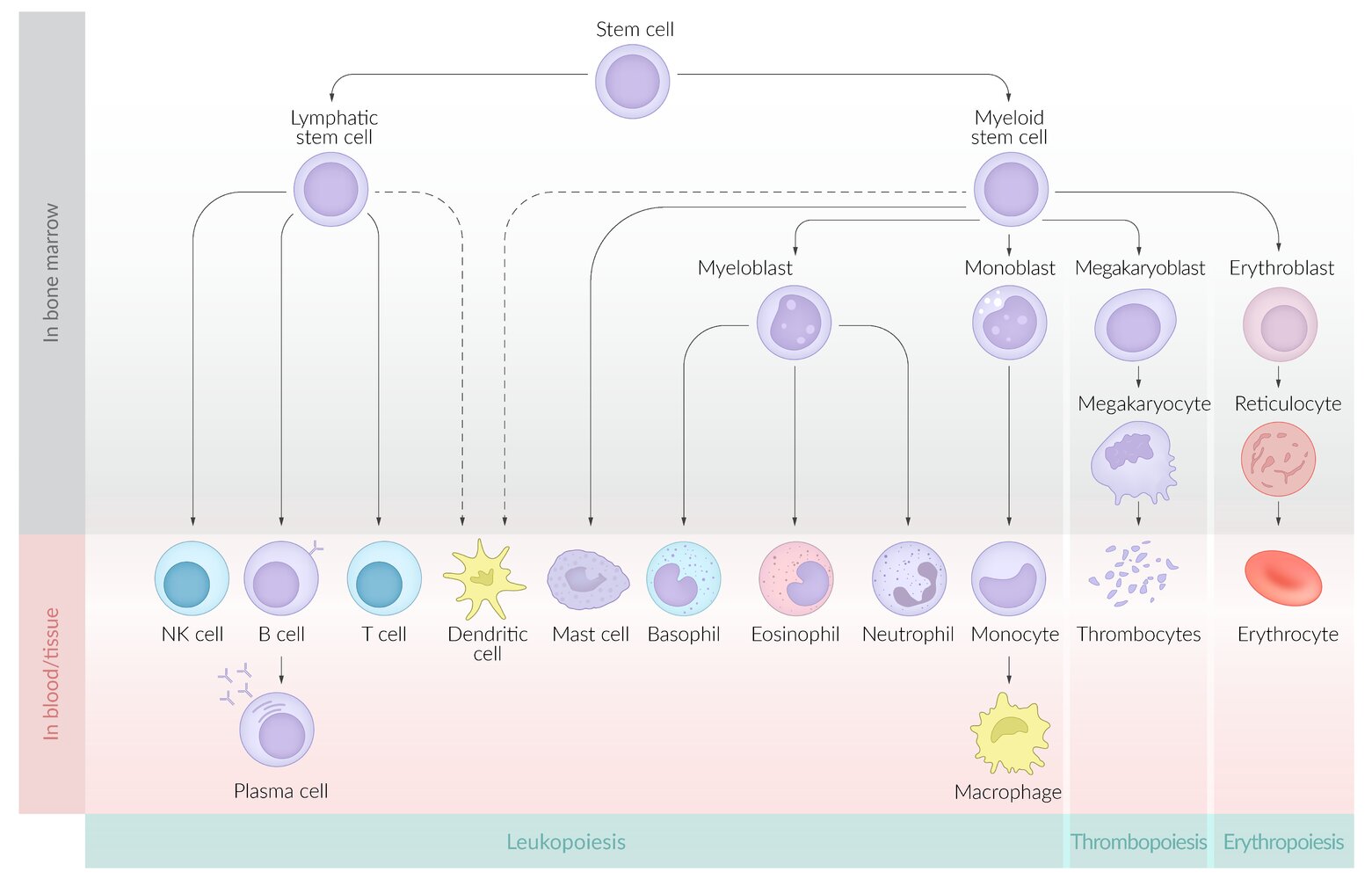
The stages of hematopoiesis, a process by which pluripotent hematopoietic stem cells in the bone marrow differentiate into two main types of precursor cells: myeloid and lymphoid.
Myeloid precursor cells differentiate into erythrocytes, leukocytes, and thrombocytes. Lymphoid precursor cells differentiate into natural killer cells (NK cells) and B and T lymphocytes. Dendritic cells, which are antigen-presenting cells, develop from both myeloid and lymphoid precursors.
© AMBOSS
Pathophysiology
- Acquired somatic mutations (chromosomal translocations and other genetic abnormalities) in early hematopoietic precursors ; → clonal proliferation of a lymphoid or myeloid stem cell line ; and arrest in cell differentiation and maturation in early stages of hematopoiesis → ; rapid proliferation of abnormal and dysfunctional blasts (with impaired apoptosis pathways) → accumulation of leukemic white blood cells in the bone marrow → disrupted normal hematopoiesis → leukopenia (↑ risk of infections), thrombocytopenia (↑ bleeding), ; and anemia
- Immature blasts enter the bloodstream → infiltration of other organs (particularly the CNS, testes, liver, and skin)
References:[8][13][14]
The stages of hematopoiesis, a process by which pluripotent hematopoietic stem cells in the bone marrow differentiate into two main types of precursor cells: myeloid and lymphoid.
Myeloid precursor cells differentiate into erythrocytes, leukocytes, and thrombocytes. Lymphoid precursor cells differentiate into natural killer cells (NK cells) and B and T lymphocytes. Dendritic cells, which are antigen-presenting cells, develop from both myeloid and lymphoid precursors.
© AMBOSS
Clinical features
Clinical features are either related to bone marrow failure, infiltration of organs by leukemic cells, or a combination of both.
| General features of acute leukemia | |
|---|---|
| |
| Clinical features of ALL | Clinical features of AML |
|
|
Fever and lymphadenopathy are rare in AML, but can be common first signs in ALL!
Fever in a patient with acute leukemia must always be treated as a sign of infection until proven otherwise!
Remember metastasis for ALL by thinking of the following: ALL metaStaSizeS to the CNS and teSteS.

References:[1][15][16][17]

Multiple erythematous papules and nodules are seen on the face and neck of this patient as a result of infiltrating malignant neoplastic cells accumulating in the dermis.
Source: “Figure 2, in: Salvage chemotherapy for the treatment of Leukemia cutis in a patient with acute monocytic leukemia” by Mehrdad Payandeh, Afshin Karami, Noorodin Karami , Soode Enayati, Mehrnoush Aeinfar, Biomedical Research and Therapy, licensed under CC BY 4.0.
© AMBOSS
Diagnosis
Approach
-
Initial evaluation
- Suspect acute leukemia in patients with suggestive clinical or laboratory features.
- Confirm the diagnosis with a morphological assessment.
- Further diagnostic studies: Immunophenotype, cytogenetics, and molecular genetic testing should be obtained in order to identify the subtype of acute leukemia.
In order to choose the best treatment strategy, the morphological assessment, immunophenotype, and genetic studies should be as comprehensive as possible.
Initial studies [18][19][20]
Routine laboratory studies
Findings on initial laboratory studies are usually nonspecific but may help to identify potentially life-threatening acute complications.
-
Complete blood count and peripheral blood smear
- Leukocytes: The white blood cell count (WBC) may be elevated, normal, or low and is not a reliable diagnostic marker.
- Platelets; : typically mild to severe thrombocytopenia
- Hemoglobin: typically anemia
- Peripheral blood smear: presence of blasts (immature WBCs)
- Liver chemistries and renal function tests: may be abnormal (e.g., secondary to disease infiltration)
-
Comprehensive metabolic panel and other metabolic studies
- Often abnormal due to increased cell lysis (see also “Tumor lysis syndrome”)
- Common findings include derangements of:
- Sodium: hyponatremia OR hypernatremia [21][22]
- Potassium; : hypokalemia OR hyperkalemia [20]
- Calcium: hypocalcemia OR hypercalcemia [20][23]
- Phosphate; : hypophosphatemia OR hyperphosphatemia [24]
- ↑ LDH
- ↑ Uric acid
- Coagulation studies: Mild coagulopathy may be present. Studies may also help to identify features of DIC.
The identification of DIC suggests APL, which is a medical emergency. Consult hematology and/or oncology immediately and transfer the patient to a critical care unit.
Confirmatory diagnostic tests [18][20][25]
Histopathological features should be assessed using bone marrow aspiration and biopsy. If unavailable, a peripheral blood smear may be sufficient.
| Histopathological features of acute leukemia | ||||
|---|---|---|---|---|
| ALL | AML | |||
| Blasts (in bone marrow or peripheral blood) [18][26] |
|
|
||
| Cell morphology [25] |
|
|
||
Cell morphology can confirm the diagnosis of acute leukemia, but in most cases, it is necessary to complete immunophenotype and genetic studies before selecting a treatment.



")


")


Specialized studies
These studies are used to further characterize the cell line involved; some characteristics may be associated with a better response to certain therapies. These studies should be ordered in consultation with a specialist.
Immunophenotype and genetic studies [19][20][25][28]
| Immunophenotype and genetic studies in acute leukemias | |||
|---|---|---|---|
| Findings in ALL | Findings in AML | ||
| Immunophenotype [28] | Immunohistochemistry |
|
|
| Flow cytometry |
|
|
|
| Genetic studies | Cytogenetics (karyotype, FISH) |
|
|
| Molecular testing (PCR, NGS) |
|
|
|
Myelogenous leukemias are myeloperoxidase positive.
Screening for extramedullary disease [18][19][31]
Consider the following studies to detect extramedullary disease based on the subtype of acute leukemia and clinical evaluation of the patient:
-
CNS infiltration (common in ALL) [20]
- Perform a lumbar puncture and obtain CSF flow cytometry.
- Consider brain and spine CT or MRI.
- Testicular infiltration (relatively common in ALL): testicular ultrasound
- Thymic infiltration (primarily in T-cell ALL): Chest x-ray or CT chest may show a mediastinal mass.
- Hepatosplenic infiltration: Abdominal CT or ultrasound may show organ enlargement.
- Other forms of extramedullary disease: Consider PET-CT and/or lymph node biopsy.
All patients with ALL should undergo screening for CNS infiltration.
Photomicrograph of bone marrow smear (H&E stain)
Multiple lymphoblasts, identifiable as large basophilic cells with abundant granular cytoplasm and a large round nucleus with clumpy chromatin and prominent nucleoli, can be seen. The presence of > 20% of lymphoblasts within a bone marrow smear is diagnostic of acute lymphoblastic leukemia. The cells surrounding the lymphoblasts are erythroid precursors, mature erythrocytes, and mature neutrophils.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
Photomicrograph of a bone marrow smear (Wright-Giemsa stain; high magnification)
Multiple myeloblasts are visible. These are identifiable as enlarged cells with abundant basophilic cytoplasm and a large curved C-shaped nucleus with fine chromatin. The presence of > 20% of myeloblasts within a bone marrow smear is diagnostic of acute myeloid leukemia.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
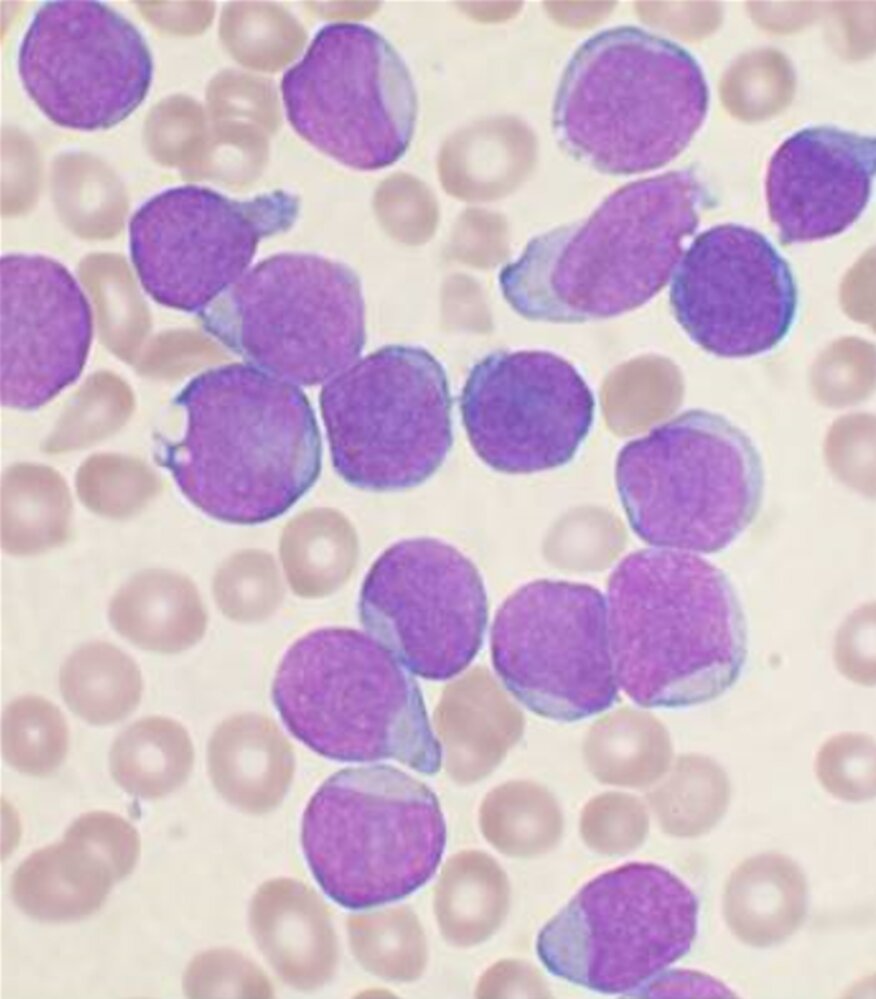
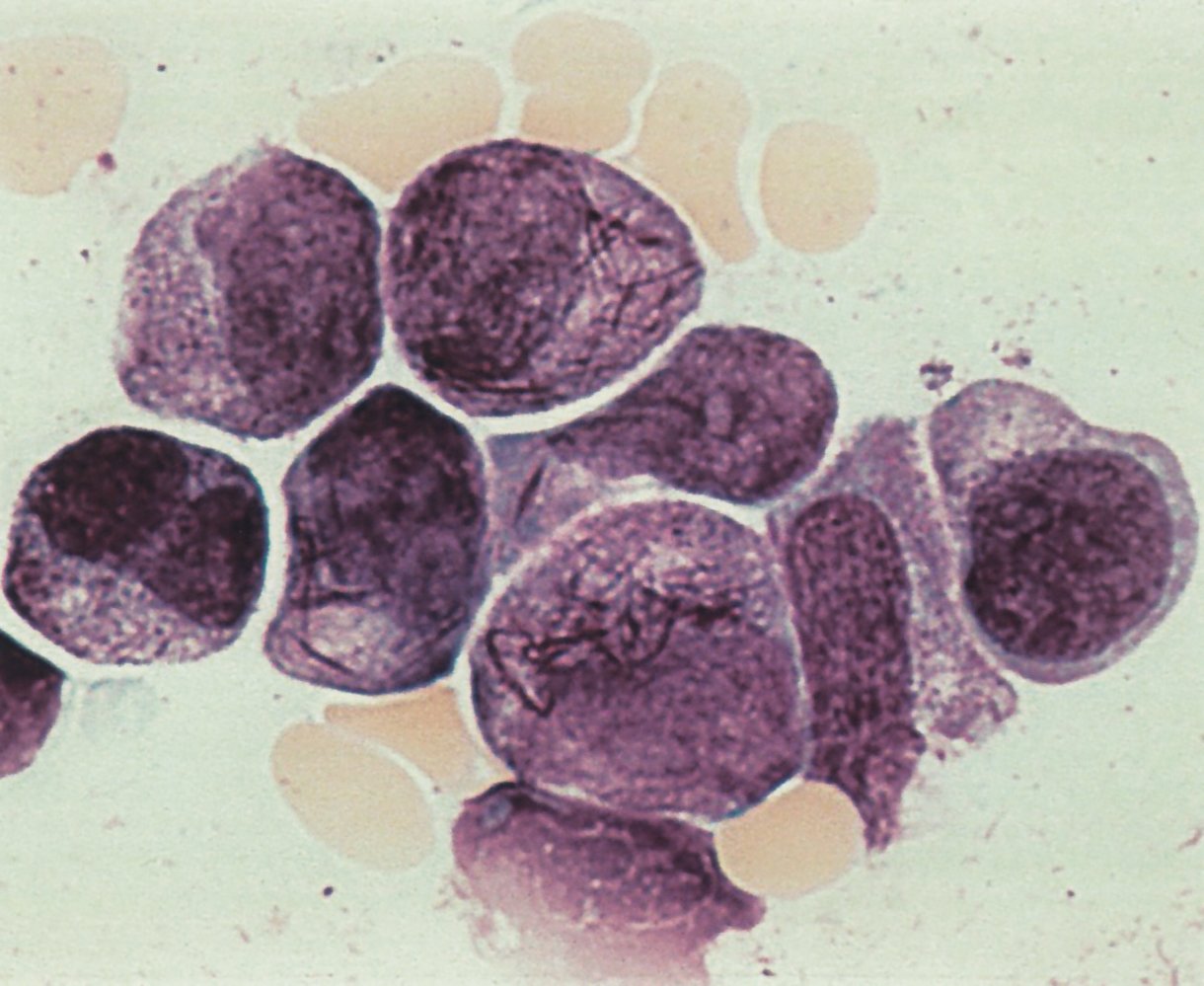
Photomicrograph of bone marrow aspirate smear (Wright staining; 1000x magnification)
Intermediate-sized blasts with dispersed chromatin, a moderate amount of cytoplasm, and indistinct nucleoli are seen alongside pale-stained erythrocytes.
These findings are consistent with precursor B-cell ALL.
Source: “Acute leukemia-ALL” by VashiDonsk, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
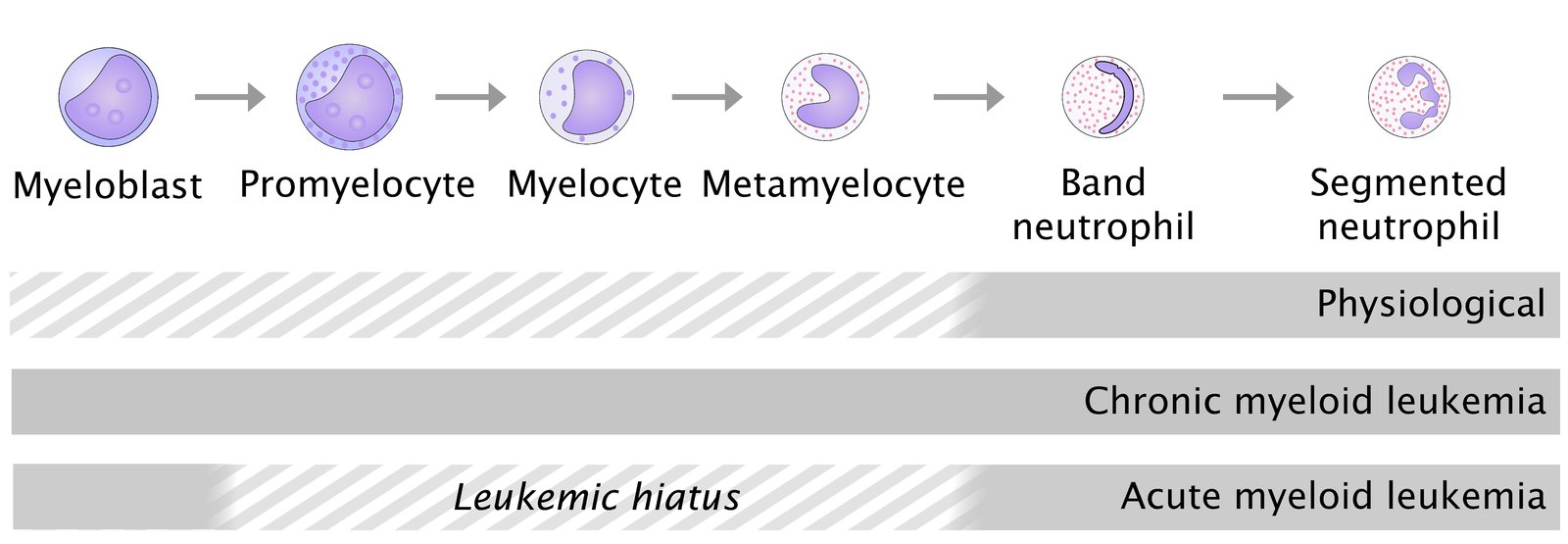
Myeloblasts differentiate within the bone marrow into mature neutrophils that then enter circulation. Physiologically, only the mature band and segmented neutrophils are visible on a normal peripheral blood smear (PBS).
In chronic myeloid leukemia (CML), myeloid precursor cells and mature neutrophils are visible on a PBS. Whereas in acute myeloid leukemia (AML), the predominant myeloid cells on a PBS are myeloblasts and mature neutrophils. The absence of the intermediate myeloid precursor cells in AML is referred to as leukemic hiatus and is useful to differentiate AML from CML.
© AMBOSS

Photomicrograph of a peripheral blood smear (Giemsa stain; high magnification)
Two red rod-like intracytoplasmic inclusions (blue overlay) are visible within the myeloblast, which is the large basophilic cell in the center of the image with an eccentric, indented nucleus and abundant cytoplasm.
These rod-like cytoplasmic inclusions are known as Auer rods, and they are typically seen in acute myeloid leukemia (e.g., acute promyelocytic leukemia) and in myelodysplastic syndromes.
Source: © IMPP
Photomicrograph of a bone marrow smear (Wright-Giemsa stain, high magnification)
Promyelocytes with azurophilic granules can be seen as well as a myeloblast containing multiple violet, rod-like intracytoplasmic inclusion bodies, known as Auer rods (examples indicated by yellow lines).
Auer rods are typically seen in certain types of acute myeloid leukemia (e.g., APL) and in myelodysplastic syndromes.
Source: “Figure 2, in: Promyelocytic Leukemia with No Retinoic Acid Receptor Alpha Abnormality but with RUNX1T1 Insertion to Chromosome 7q: A Classification and Management Dilemma” by K. Overholt, T. L. Guinipero, N. A. Heerema et al., Hindawi - Case Reports in Hematology, licensed under CC BY 3.0. Modifications: removed arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Photomicrograph of a peripheral blood smear (Pappenheim stain; high magnification)
Multiple red rod-like intracytoplasmic inclusions (Auer rods, highlighted by gray overlay) are visible within a myeloblast, the large basophilic cell (marked by arrow) with an eccentric, indented nucleus (marked by black outline) and a prominent nucleolus (green overlay).
Auer rods are typically seen in acute myeloblastic leukemia and acute promyelocytic leukemia.
Source: © IMPP
Photomicrographs of a peripheral blood smear (H&E stain; very high magnification)
The large basophilic cells are promyelocytes, identifiable by their eccentric nuclei and abundant basophilic cytoplasm containing numerous Auer rods (rod-like intracytoplasmic inclusion bodies). This type of hypergranular leukemic promyelocyte is often still referred to as a “faggot cell” for the resemblance of accumulation of Auer rods to a “bundle of sticks,” although the term is typically avoided today due to its derogatory associations.
The presence of promyelocytes containing Auer rods in a peripheral blood smear is characteristic of acute promyelocytic leukemia.
Note: Basophilic remnants (Howell-Jolly bodies) are visible within most of the erythrocytes, indicating (in this case) increased hematopoiesis.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
Photomicrograph of a peripheral blood smear of a patient with anemia and thrombocytopenia
The most numerous cells in the smear are promyelocytes, which are identifiable as large basophilic cells with a large nucleus, prominent nucleoli, and cytoplasm containing azurophilic granules that fuse to form Auer rods (red overlay).
A peripheral blood smear in which promyelocytes predominate and Auer rods are present is characteristic of acute promyelocytic leukemia.
Source: © IMPP
Photomicrographs of a bone marrow smear (H&E stain; very high magnification)
The large basophilic cell visible in each photomicrograph is a monocyte, identifiable by its large size, folded or lobed nucleus with fine chromatin and prominent nucleoli (green overlay), and abundant granular cytoplasm with cytoplasmic vacuoles.
Numerous monocytes on bone marrow biopsy is characteristically seen in acute monocytic leukemia. The diagnosis is confirmed on immunophenotyping.
Our great thanks to Dr. Wisplinghoff (Dr. Wisplinghoff's laboratory) for kindly providing this image.
© AMBOSS
Treatment
Approach [25][32][33]
The treatment of acute leukemia is decided by a hematologist-oncologist specialist depending on the specific subtype and results of molecular testing.
- Pretreatment: All patients should have prechemotherapy screening as part of preparation for cancer treatment.
-
Chemotherapy
- Systemic chemotherapy: The regimen of choice is based on individual patient and disease factors.
- Intrathecal chemotherapy (commonly used): Consider adding for patients with or at high risk of CNS infiltration (e.g., all patients with ALL).
- Targeted chemotherapy: Consider adding for leukemias with specific immunophenotype and genetic profiles, e.g., Philadelphia translocation.
- Adjunctive treatment, e.g., radiation therapy, immunotherapy, or stem cell transplantation (SCT): Consider based on individual evaluation.
- Supportive care: Provide holistic care to reduce symptoms and support patients and carers (see “Principles of cancer care”).
- Management of complications: initiate monitoring, prevention, and early aggressive treatment as needed for infection, bleeding, pancytopenia, and oncologic emergencies (see “Management of complications”).
- Relapse or refractory leukemia: Consider re-induction chemotherapy, autologous SCT, or enrollment in a clinical trial in consultation with hematologist-oncologist.
Early and aggressive chemotherapy improves the prognosis, e.g., 80–90% of patients with ALL achieve complete remission with chemotherapy. [25]
Systemic chemotherapy [32][33]
Regimens vary depending on the subtype of leukemia, the age of the patient, and immunophenotype and genetic study results.
-
Induction chemotherapy
- Average duration for an adult with ALL is 4–8 weeks
- Reinduction therapy may be required in case of relapse or failure of primary induction
- Consolidation chemotherapy: average duration for an adult with ALL is 4–8 months
- Maintenance chemotherapy: average duration for an adult with ALL is 2–3 years
| Common agents used in chemotherapy regimens for acute leukemia [18][20][25][32][33] | |
|---|---|
| ALL |
|
| AML |
|
| APL |
|
A chemotherapy regimen commonly used to treat ALL is hyper-CVAD: Cyclophosphamide, Vincristine, daunorubicin (or Adriamycin), and Dexamethasone.
If APL is suspected, start treatment early with a differentiation agent (e.g., ATRA) without waiting for immunotype or genetic confirmation. Treatment may be adjusted later depending on the results. [25]
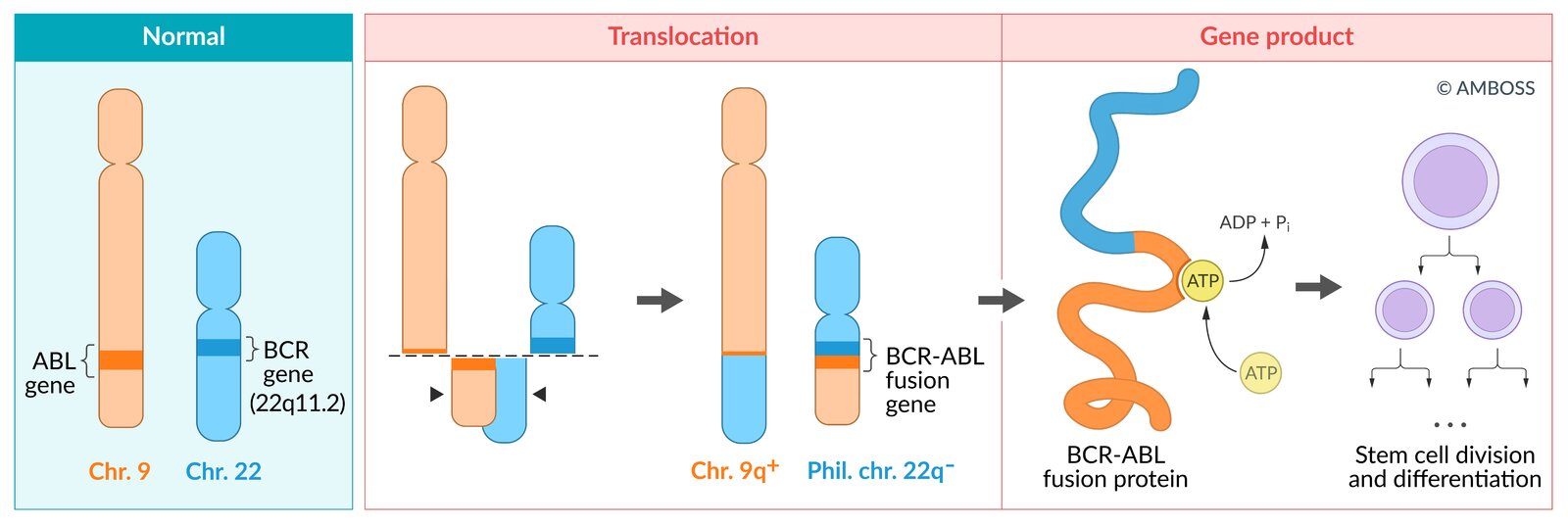
In APL, the t(15;17) translocation and subsequent formation of the PML-RARA fusion gene can inhibit myeloblast differentiation under physiological levels of retinoic acid. High doses of ATRA (a vitamin A derivative) may induce myeloblast differentiation and promote remission.
Management of CNS infiltration [32][33][34]
-
Intrathecal chemotherapy: administration of chemotherapeutic agents (e.g., triple therapy with methotrexate, cytarabine, and hydrocortisone) directly into the subarachnoid space via lumbar puncture or using an intraventricular catheter with a reservoir placed under the scalp
- Indications in ALL: Prevention of leukemic meningitis in all patients at the time of diagnosis [18][20][33]
- Indications in AML
- Treatment of patients with confirmed CNS infiltration
- Prevention in patients with high-risk APL [35]
- CNS radiotherapy: Consider directed radiation therapy alongside intrathecal chemotherapy in select patients.
Intrathecal prophylaxis should be initiated early, as prevention of CNS leukemia is usually effective. Patients with CNS infiltration are at higher risk of relapse than those without CNS infiltration.
Advanced therapies [25][31]
-
Targeted therapy: Nonstandard chemotherapy or immunotherapy is indicated if certain mutations or markers are detected.
-
Tyrosine kinase inhibitors (TKIs)
- Philadelphia chromosome-positive ALL: BCR-ABLTKIs, e.g., imatinib, ponatinib)
- FLT3-ITD AML: Consider midostaurin [36]
- Monoclonal antibodies: e.g., rituximab for CD20-positive Philadelphia chromosome-negative ALL, gemtuzumab ozogamicin for CD33-positive AML
- Chimeric antigen receptor T-cell therapy: may be used in ALL
-
Tyrosine kinase inhibitors (TKIs)
- Autologous or allogeneic stem cell transplantation: Indications include patients with poor prognostic factors (e.g., unfavorable cytogenetics) and those who do not achieve remission with chemotherapy (see “Transplantation” for more information). [25]
Management of complications [25]
-
Oncologic emergencies
-
Tumor lysis syndrome (TLS)
- Management: typically includes fluid therapy (oral or IV) and rasburicase
- Prophylaxis: Consider hydration, and urate-lowering therapy (i.e., allopurinol or rasburicase).
- Leukostasis (e.g., due to hyperleukocytosis): Consider IV fluid resuscitation and/or cytoreductive therapy.
- See “Oncologic emergencies” for details and dosages.
-
Tumor lysis syndrome (TLS)
-
Treatment-related complications
- Anticancer therapy-induced myelosuppression: anemia , thrombocytopenia , and neutropenia [37][38]
- Mucositis [39]
- See “Anticancer treatment-related complications” and “Neutropenic fever” for details and dosages.
-
Secondary hyperuricemia
- Can lead to acute gout, uric acid stones, and urate nephropathy
- Consider hydration, fluid administration, and urate-lowering therapy (e.g., allopurinol and rasburicase) as prophylaxis prior to chemotherapy.
-
Specific chemotherapy toxicity
- See “Chemotherapeutic agents.”
- Differentiation agents
- ATRA: See “Side effects” of retinoids.
- Arsenic trioxide: ECG monitoring for QTc prolongation and discontinuation of other QTc-prolonging drugs. [40]
Complications
- Tumor lysis syndrome
- Leukostasis
- See also:
- “Oncologic emergencies”
- “Complications of cancer”
- “Complications of anticancer therapy”
- “Neutropenic fever”
We list the most important complications. The selection is not exhaustive.
Prognosis
5-year survival rate following treatment
- ALL: The 5-year survival rate is generally higher compared to AML (varies from ∼ 20% in elderly patients to ∼ 80% in children and adolescents)
- AML: ∼ 30%, but it varies according to the patient's age. The survival time has increased more recently due to improvements in treatment.
Unfavorable prognostic factors
| ALL | AML | |
|---|---|---|
| Age |
|
|
| Disease features |
|
|
| Cytogenetics | ||
|
|
|
| Immunotyping |
|
|
Favorable prognostic factors
| ALL | AML |
|---|---|
|
|
To remember that translocation t(12;21) commonly manifests with pediatric B-ALL and usually has a favorable outcome, think: “Kids flip back to health!” (the number 12 is 21 flipped around).
References:[41][42][43][44][45][46]
References
- Horton TM, Steuber CP. "Overview of the presentation and diagnosis of acute lymphoblastic leukemia in children and adolescents". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-the-presentation-and-diagnosis-of-acute-lymphoblastic-leukemia-in-children-and-adolescents. [2016-10-13]
- Schiffer CA, Anastasi J. "Clinical manifestations, pathologic features, and diagnosis of acute myeloid leukemia". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-pathologic-features-and-diagnosis-of-acute-myeloid-leukemia. [2017-01-06]
- "Adult T-Cell Leukemia/Lymphoma". http://www.lymphoma.org/site/pp.asp?c=bkLTKaOQLmK8E&b=6300141. [2016-12-01]
- Marks DI, Paietta EM, Moorman AV, et al. "T-cell acute lymphoblastic leukemia in adults: clinical features, immunophenotype, cytogenetics, and outcome from the large randomized prospective trial (UKALL XII/ECOG 2993)". Blood. 114(25). :5136-5145. (2009)
- Nicot C. "Current views in HTLV-I-associated adult T-cell leukemia/lymphoma". Am J Hematol. 78(3). :232-239. (2005)
- Ostermaier KK. "Down Syndrome: Clinical Features and Diagnosis". UpToDate. UpToDate. https://www.uptodate.com/contents/down-syndrome-clinical-features-and-diagnosis. [2015-11-23]
- Goldacre MJ, Wotton CJ, Seagroatt V, Yeates D. "Cancers and immune related diseases associated with Down's syndrome: a record linkage study". Arch Dis Child. 89(11). :1014-1017. (2004)
- Seiter, K.. "Acute Myeloid Leukemia (AML)". WebMD. https://emedicine.medscape.com/article/197802-overview#showall. [2018-12-05]
- Reboursiere E, Chantepie S, Gac A-C, Reman O. "Rare but authentic Philadelphia-positive acute myeloblastic leukemia: Two case reports and a literature review of characteristics, treatment and outcome". Hematol Oncol Stem Cell Ther. 8(1). :28-33. (2015)
- Van Etten RA. "Clinical manifestations and diagnosis of chronic myeloid leukemia". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-chronic-myeloid-leukemia. [2017-04-10]
- Alaggio R, Amador C, Anagnostopoulos I, et al. "The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms". Leukemia. 36(7). :1720-1748. (2022)
- Khoury JD, Solary E, Abla O, et al. "The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms". Leukemia. 36(7). :1703-1719. (2022)
- "Acute Lymphoblastic Leukemia (ALL)". https://pedclerk.bsd.uchicago.edu/page/acute-lymphoblastic-leukemia-all-0. [2013-01-01]
- Kaplan Medical Staff. "USMLE Step 1 Lecture Notes 2017: 7-Book Set". Kaplan Publishing. (2017). ISBN: 9781506208411
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Wolters Kluwer Health. (2015). ISBN: 9781496306142
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Arber DA, Borowitz MJ, Cessna M, et al. "Initial Diagnostic Workup of Acute Leukemia: Guideline From the College of American Pathologists and the American Society of Hematology". Arch Pathol Lab Med. 141(10). :1342-1393. (2017)
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- Epameinondas Koumpis, Matilda Florentin, Eleftheria Hatzimichael, George Liamis. "Hyponatremia in Patients with Hematologic Diseases". J Clin Med. 9(11). :3721. (2020)
- Filippatos TD, Milionis HJ, Elisaf MS. "Alterations in electrolyte equilibrium in patients with acute leukemia". Eur J Haematol. 75(6). :449-460. (2005)
- Luciano RL, Brewster UC. "Kidney Involvement in Leukemia and Lymphoma". Adv Chronic Kidney Dis. 21(1). :27-35. (2014)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Goldman L, Schafer AI. "Goldman-Cecil Medicine, 2-Volume Set". Elsevier. (2019). ISBN: 9780323532662
- International Agency for Research on Cancer (IARC). "Tumors of Haematopoietic and Lymphoid Tissues". World Health Organization (WHO). (2001). ISBN: 9789283224112
- Antony AC. "Hematology: Basic Principles and Practice". Elsevier, Inc.. (2018). ISBN: 9780323357623
- Olsen RJ, Chang CC, Herrick JL, Zu Y, Ehsan A. "Acute leukemia immunohistochemistry: a systematic diagnostic approach.". Arch Pathol Lab Med. 132(3). :462-75. (2008)
- Ravandi F, Kebriaei P. "Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia". Hematol Oncol Clin North Am. 23(5). :1043-1063. (2009)
- Shao X, Chen D, Xu P, et al. "Primary Philadelphia chromosome positive acute myeloid leukemia: A case report.". Medicine. 97(44). :e12949. (2018)
- Brown PA, Wieduwilt M, Logan A, et al. "Guidelines Insights: Acute Lymphoblastic Leukemia, Version 1.2019". Journal of the National Comprehensive Cancer Network. 17(5). :414-423. (2019)
- Heuser M, Ofran Y, Boissel N, et al. "Acute myeloid leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Annals of Oncology. 31(6). :697-712. (2020)
- Hoelzer D, Bassan R, Dombret H, et al. "Acute lymphoblastic leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Annals of Oncology. 27. :v69-v82. (2016)
- Kwong Y-L, Yeung DYM, Chan JCW. "Intrathecal chemotherapy for hematologic malignancies: drugs and toxicities". Ann Hematol. 88(3). :193-201. (2008)
- Iland HJ, Seymour JF, Wei A. "Optimal approach for high-risk acute promyelocytic leukemia". Curr Opin Hematol. 21(2). :102-113. (2014)
- Gallogly MM, Lazarus HM, Cooper BW. "Midostaurin: a novel therapeutic agent for patients with FLT3-mutated acute myeloid leukemia and systemic mastocytosis". Therapeutic Advances in Hematology. 8(9). :245-261. (2017)
- Stanworth SJ, Estcourt LJ, Powter G, et al. "A No-Prophylaxis Platelet-Transfusion Strategy for Hematologic Cancers". N Engl J Med. 368(19). :1771-1780. (2013)
- Schiffer CA, Bohlke K, Delaney M, et al. "Platelet Transfusion for Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update". Journal of Clinical Oncology. 36(3). :283-299. (2018)
- Brown TJ, Gupta A. "Management of Cancer Therapy–Associated Oral Mucositis". JCO Oncol Pract. 16(3). :103-109. (2020)
- Barbey JT, Pezzullo JC, Soignet SL. "Effect of Arsenic Trioxide on QT Interval in Patients With Advanced Malignancies". Journal of Clinical Oncology. 21(19). :3609-3615. (2003)
- Horton TM, Steuber CP. "Risk group stratification and prognosis for acute lymphoblastic leukemia in children and adolescents". UpToDate. UpToDate. http://www.uptodate.com/contents/risk-group-stratification-and-prognosis-for-acute-lymphoblastic-leukemia-in-children-and-adolescents. [2017-04-07]
- Schiffer CA. "Prognosis of acute myeloid leukemia". UpToDate. UpToDate. http://www.uptodate.com/contents/prognosis-of-acute-myeloid-leukemia. [2017-02-22]
- Raynaud SD, Dastugue N, Zoccola D, et al. "Cytogenetic abnormalities associated with the t(12;21): a collaborative study of 169 children with t(12;21)-positive acute lymphoblastic leukemia". Leukemia. 13(9). :1325-1330. (1999)
- Le T, Bhushan V, Chen V, King M. "First Aid for the USMLE Step 2 CK". McGraw-Hill Education. (2015). ISBN: 9780071844574
- Zhang, Y.; Beau, M.. "Cytogenetics and molecular genetics in acute lymphoblastic leukemia". UpToDate. UpToDate. https://www.uptodate.com/contents/cytogenetics-and-molecular-genetics-in-acute-lymphoblastic-leukemia. [2018-05-18]
- "Prognostic Factors in Childhood Leukemia (ALL or AML)". https://www.cancer.org/cancer/leukemia-in-children/detection-diagnosis-staging/prognostic-factors.html. [2019-01-01]
- Becker H, Pfeifer D, Afonso JD, et al. "Two cell lines of t(8;21) acute myeloid leukemia with activating KIT exon 17 mutation: models for the 'second hit' hypothesis". Leukemia. 22(9). :1792-1794. (2008)
- Seiter, K.. "Acute Lymphoid Leukemia (ALL)". WebMD. https://emedicine.medscape.com/article/207631-overview#a3. [2018-07-17]
- Larson RA, Pui C-H. "Tumor lysis syndrome: Definition, pathogenesis, clinical manifestations, etiology and risk factors". UpToDate. UpToDate. http://www.uptodate.com/contents/tumor-lysis-syndrome-definition-pathogenesis-clinical-manifestations-etiology-and-risk-factors#H491877. [2016-09-09]
- Larson RA, Pui CH, Drews RE, et al. "Tumor Lysis Syndrome: Prevention and Treatment". UpToDate. UpToDate. https://www.uptodate.com/contents/tumor-lysis-syndrome-prevention-and-treatment. [2017-07-24]
- Le T, Bhushan V, Sochat M, et al. "First Aid for the USMLE Step 1 2019". McGraw-Hill Medical. ISBN: 9781260143683
- Larson, R.A; Pui, C.. "Tumor lysis syndrome prevention and treatment". UpToDate. UpToDate. https://www.uptodate.com/contents/tumor-lysis-syndrome-prevention-and-treatment. [2018-05-24]