Quick guide
Diagnostic approach
- ABCDE approach
- Focused clinical evaluation
- Serum lipase
- Serum amylase
- CBC
- CMP
- LDH
- CRP
- Procalcitonin
- Triglycerides
- ABG
- Ultrasound abdomen
- CECT abdomen if there is diagnostic uncertainty
Diagnostic criteria
≥ 2 of the following:
- Characteristic abdominal pain (i.e., constant, severe epigastric pain that radiates toward the back)
- Lipase or amylase ≥ 3× ULN
- Characteristic findings of acute pancreatitis on cross-sectional imaging
Management checklist
- Two large-bore IVs
- Goal-directed IV fluid therapy for acute pancreatitis
- Oxygen therapy as needed
- Electrolyte repletion as needed
- Management of ARDS as needed
- Analgesics (e.g., NSAIDs) and antiemetics as needed
- Consult GI or IR for therapeutic ERCP for patients with biliary pancreatitis.
- Consult general surgery for suspected severe or necrotizing pancreatitis.
Summary
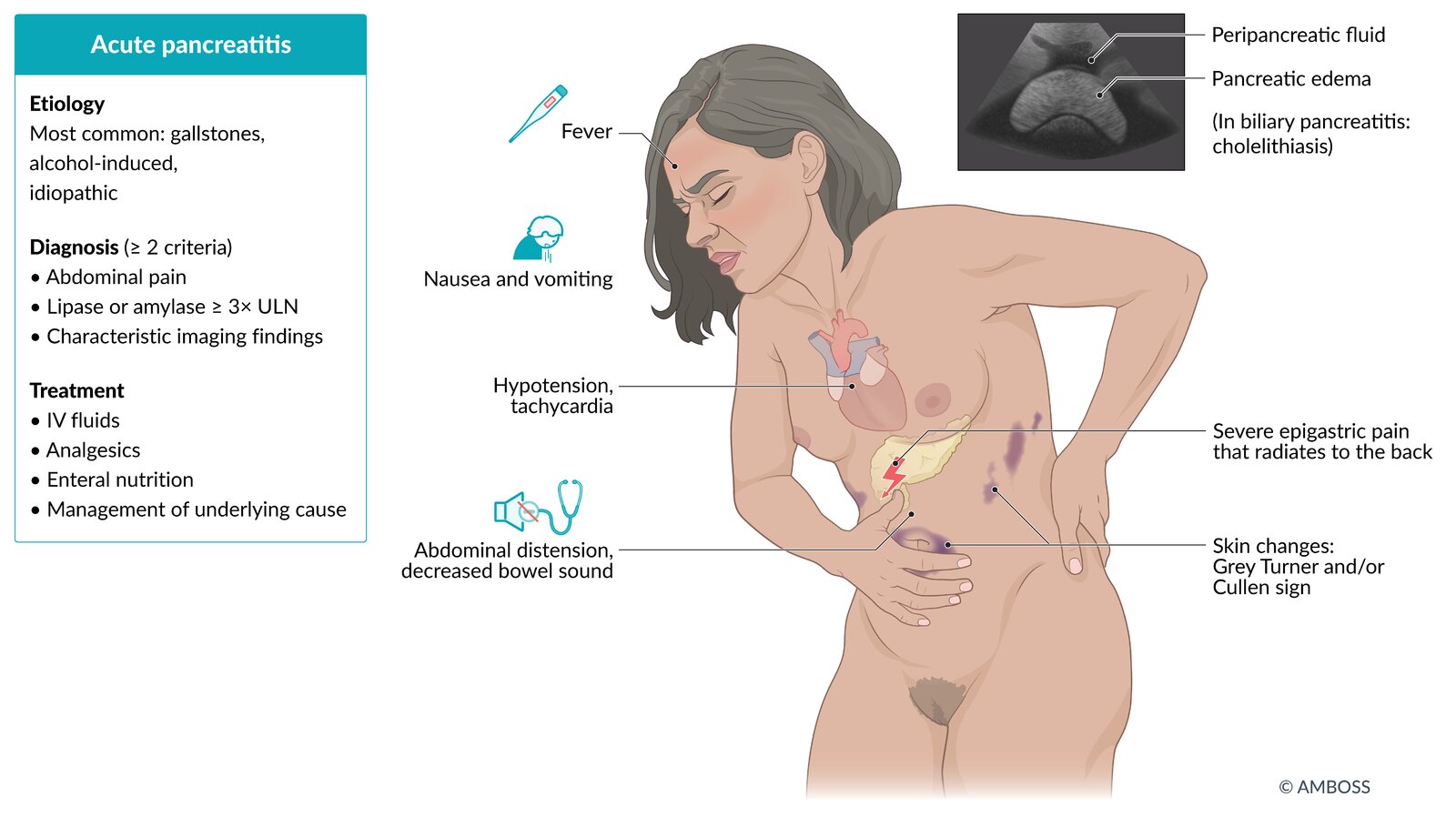
Acute pancreatitis is an inflammatory condition of the pancreas most commonly caused by gallstones or alcohol use in adults and biliary disease and medications in children. The typical manifestation includes sudden, severe epigastric pain that radiates to the back, nausea and vomiting, and epigastric tenderness on palpation. Elevation of serum lipase or amylase ≥ 3× ULN and/or characteristic findings of acute pancreatitis on cross-sectional imaging (e.g., abdominal ultrasound, contrast-enhanced CT abdomen) confirm the diagnosis. Clinical scores (e.g., Ranson criteria, APACHE II) are used to predict the severity and prognosis of pancreatitis. Initial management is primarily supportive and includes fluid resuscitation, analgesia, antiemetics, and early enteral nutrition as tolerated. The underlying cause should be identified and managed to prevent recurrence (e.g., cholecystectomy for biliary pancreatitis, long-term lipid-lowering therapy for hypertriglyceridemia-induced pancreatitis). Localized complications of pancreatitis include necrosis (necrotizing pancreatitis), which may become infected, pancreatic pseudocysts, and walled-off necrosis. Systemic complications include sepsis, ARDS, organ failure, and shock. Complications of pancreatitis are associated with significant morbidity and mortality.

© AMBOSS
Etiology
Most common causes [1]
- Biliary pancreatitis (∼ 40% of cases; mostly caused by gallstones)
- Alcohol-induced (∼ 20% of cases)
- Idiopathic (∼ 25% of cases)
Other causes [1]
- Hypertriglyceridemia-induced pancreatitis: caused by severe hypertriglyceridemia (> 1,000 mg/dL)
- Hypercalcemia
- Post-ERCP
-
Drug-induced pancreatitis
- Steroids
- Azathioprine
- Sulfonamides
- Loop and thiazide diuretics
- Estrogen
- Protease inhibitors
- NRTIs
- Anticonvulsants (e.g., valproate)
- Metronidazole
- Scorpion stings
- Viral infections (e.g., coxsackievirus B, mumps)
- Trauma (especially in children)
- Autoimmune and rheumatological disorders (e.g., Sjögren syndrome)
- Pancreas divisum
- Hereditary (e.g., mutation of PRSS1 gene, cystic fibrosis) [2]
- Cholesterol embolism
I GET SMASHED: Idiopathic, Gallstones, Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion venom, Hypercalcemia and hypertriglyceridemia, ERCP, and Drugs are causes of acute pancreatitis.


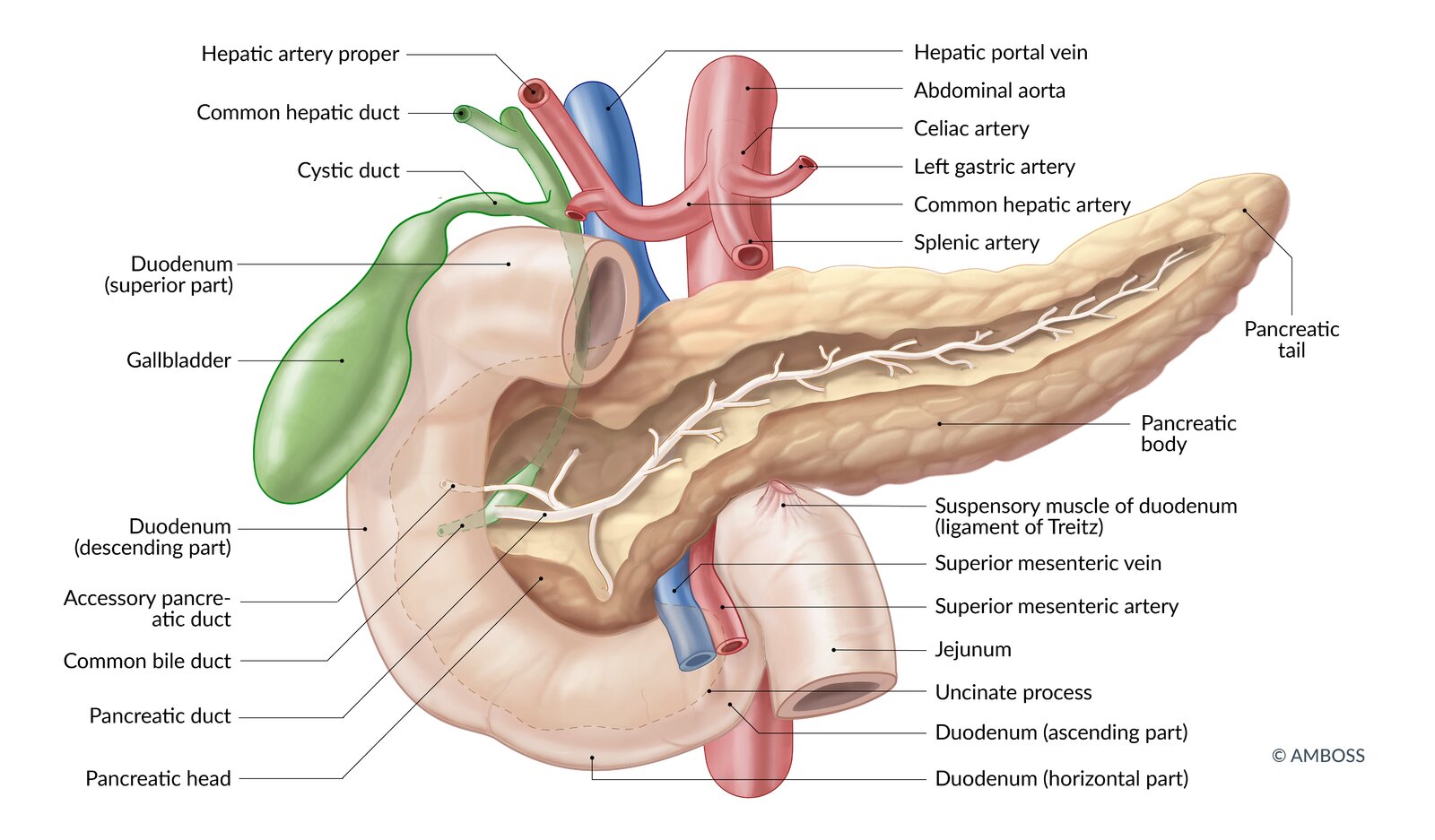
The main pancreatic duct and the common bile duct merge and enter the descending part of the duodenum at the major duodenal papilla. The accessory duct enters at the minor duodenal papilla.
Note: individual ductal anatomy may vary
© AMBOSS
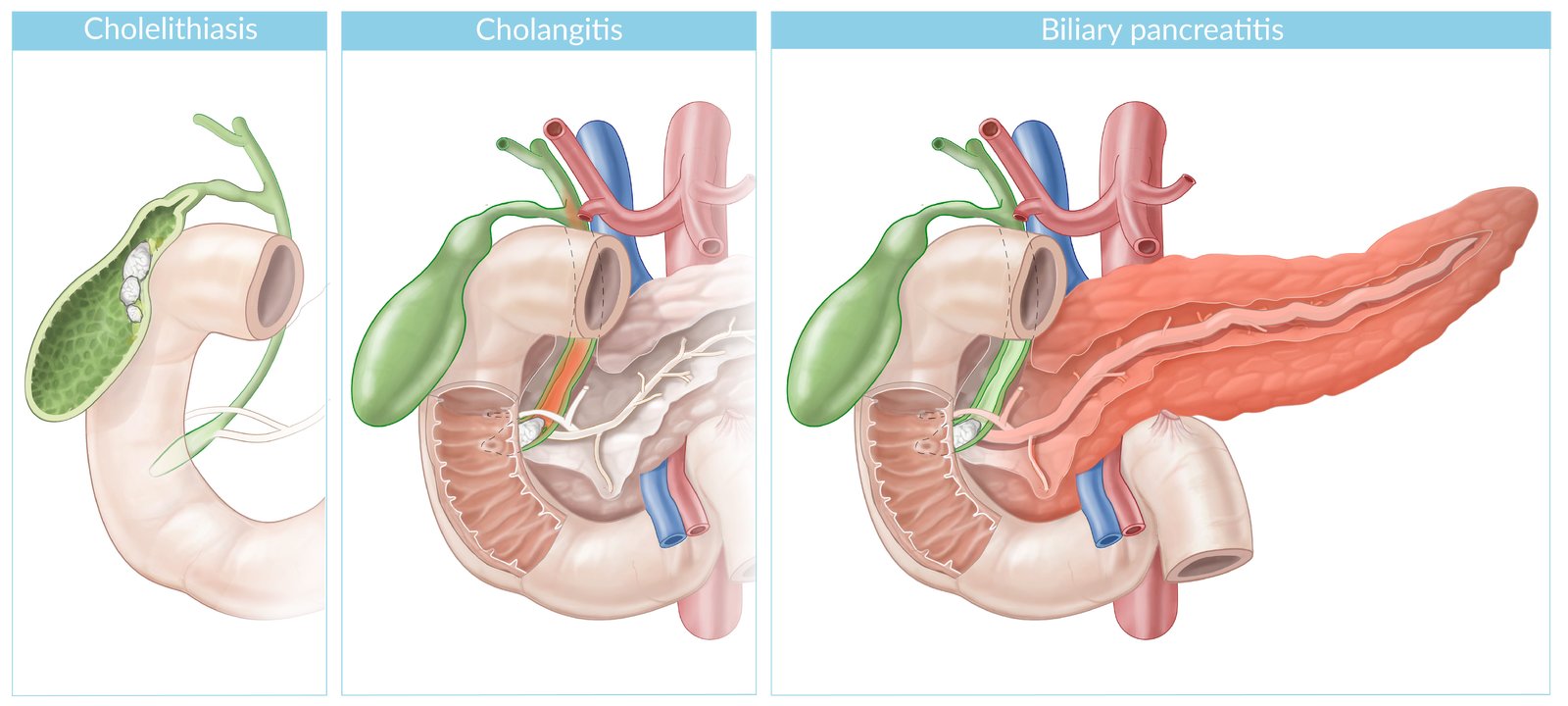
Cholelithiasis: the presence of gallstones within the gall bladder
Cholangitis: ascending biliary tract infection (orange shading) secondary to choledocholithiasis
Biliary pancreatitis: Pancreatic outflow obstruction secondary to choledocholithiasis allows for activation of pancreatic zymogens, resulting in pancreatic inflammation (orange shading).
© AMBOSS
Pathophysiology
Sequence of events
- Intrapancreatic activation of pancreatic enzymes: secondary to pancreatic ductal outflow obstruction (e.g., gallstones, cystic fibrosis) or direct injury to pancreatic acinar cells (e.g., alcohol, drugs)
- Increased proteolytic and lipolytic enzyme activity → destruction of pancreatic parenchyma
- Attraction of inflammatory cells (neutrophils, macrophages) → release of inflammatory cytokines → pancreatic inflammation (pancreatitis)
Sequelae of pancreatitis
-
Capillary leakage: release of inflammatory cytokines and vascular injury by pancreatic enzymes → vasodilation and increased vascular permeability → shift of fluid from the intravascular space into the interstitial space (third-space fluid loss) → hypotension, tachycardia, warm and flushed skin → distributive shock
- In severe cases, the third spacing of fluid from this inflammatory response can lead to hypovolemic shock.
- Pancreatic necrosis: uncorrected hypotension and third-spacing → decreased end-organ perfusion → multiorgan dysfunction (mainly renal) and pancreatic necrosis
- Hypocalcemia: lipase breaks down peripancreatic and mesenteric fat; → release of free fatty acids that bind calcium → hypocalcemia (fatty saponification) [3]

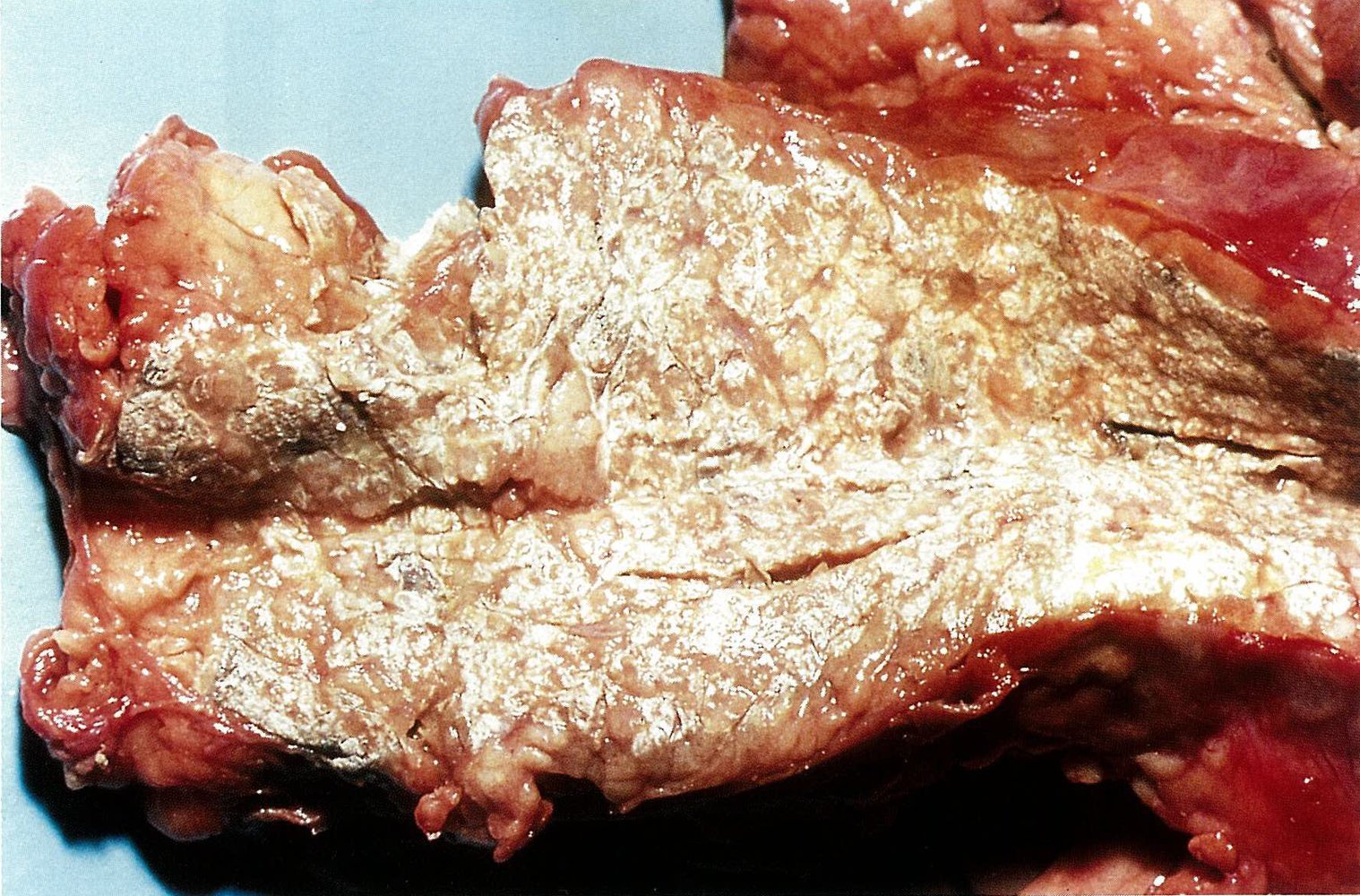
Gross pathology specimen of a pancreas dissected along the coronal plane
The pancreas appears swollen as a result of inflammation with greyish-black areas of necrosis on the left and right borders. The whitish regions throughout the specimen indicate saponification of adipose tissue due to the activation of pancreatic zymogens.
The findings are consistent with fulminant acute pancreatitis.
Source: © IMPP
Clinical features
Symptoms
-
Constant, severe epigastric pain
- Classically radiating towards the back
- Worse after meals and when supine
- Improves on leaning forwards
- Nausea, vomiting
- Fever
- If pulmonary complications are present: chest pain, dyspnea
Examination findings
-
General
- Signs of shock: tachycardia, hypotension, oliguria/anuria
- Possibly jaundice in patients with biliary pancreatitis
-
Abdominal examination
- Abdominal tenderness, distention, guarding
- Ileus with reduced bowel sounds and tympany on percussion
- Ascites
-
Skin changes (rare)
- Cullen sign: periumbilical ecchymosis and discoloration (bluish-red)
- Grey Turner sign: flank ecchymosis with discoloration
- Fox sign: ecchymosis over the inguinal ligament
- Pulmonary examination: signs of pleural effusion and/or ARDS may be present


© AMBOSS

Periumbilical ecchymosis as a result of retroperitoneal hemorrhage, commonly seen in acute pancreatitis.
Source: “Cullen's sign” by Herbert L. Fred, MD and Hendrik A. van Dijk, openstax, licensed under CC BY 2.0.
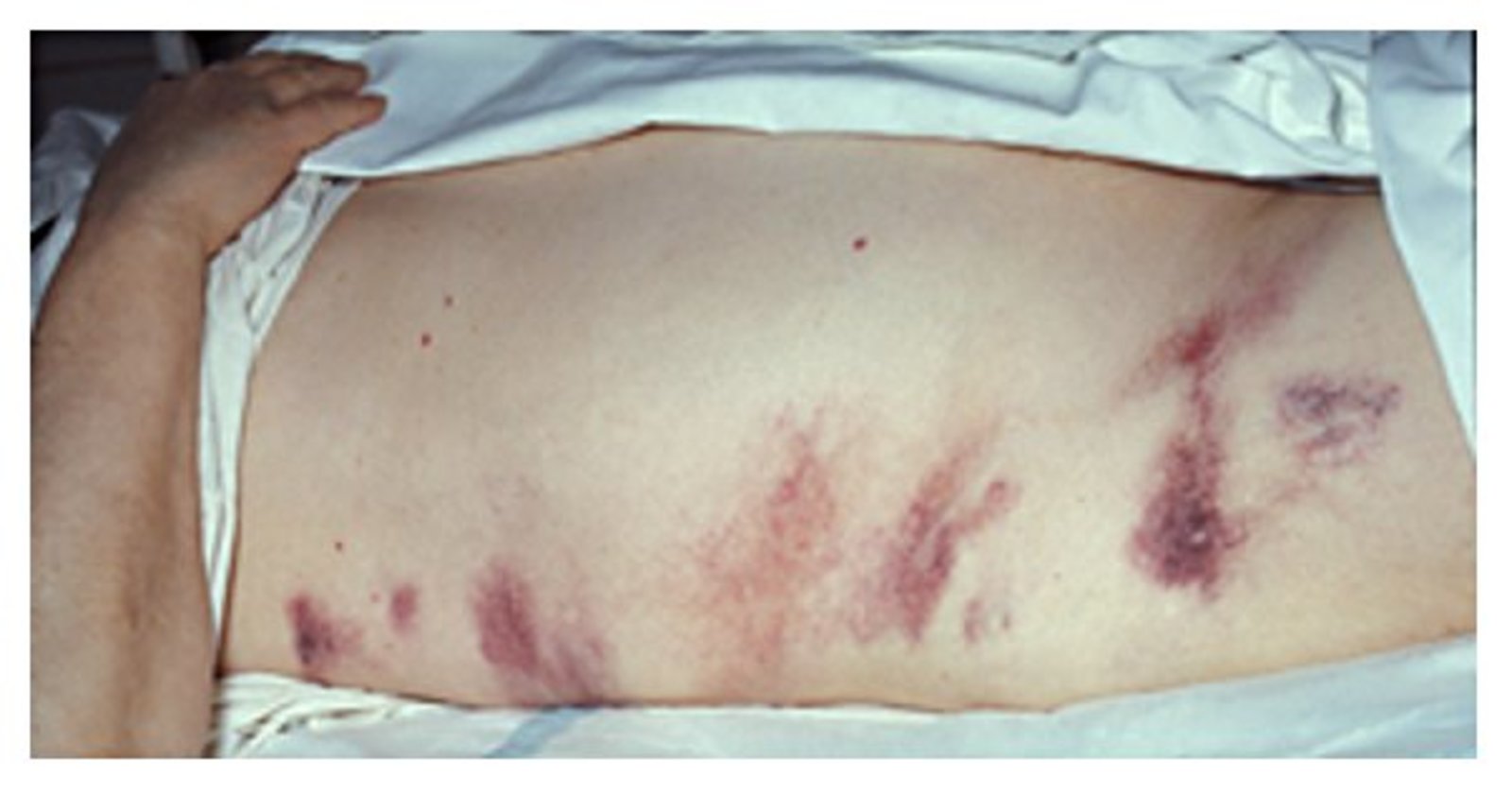
Right-sided flank ecchymosis suggestive of retroperitoneal hemorrhage, commonly seen in acute pancreatitis.
Source: “Images of Memorable Cases: Case 21: Hemorrhagic pancreatitis - Grey Turner's sign” by Herbert L. Fred, MD and Hendrik A. van Dijk, Wikimedia Commons, licensed under CC BY 2.0.
Diagnosis
Diagnostic criteria for acute pancreatitis [4][5][6]
Two of the three following criteria should be met for a diagnosis of acute pancreatitis to be made.
- Characteristic abdominal pain
- ↑ Serum pancreatic enzymes: lipase or amylase ≥ 3× ULN
- Characteristic findings of acute pancreatitis on cross-sectional imaging (e.g., abdominal ultrasound, contrast-enhanced CT abdomen)
Approach [7][8][9]
-
All patients
-
Perform laboratory studies to:
- Establish the diagnosis: serum lipase and/or amylase levels
- Determine severity: CBC, BMP, ABG, LDH, inflammatory markers, serum calcium
- Evaluate for the underlying etiology: liver chemistries, serum or plasma triglyceride levels
- Obtain ultrasound abdomen.
-
Perform laboratory studies to:
- Diagnostic uncertainty: Perform contrast-enhanced CT (CECT) abdomen.
-
Confirmed diagnosis
- Perform further diagnostics as needed to determine the etiology (e.g., MRCP for suspected biliary pancreatitis).
- Calculate severity scores of acute pancreatitis to estimate severity and prognosis.
- In patients with severe pancreatitis, consider CECT abdomen 5–7 days after the onset of symptoms to assess for necrotizing pancreatitis.
Simultaneously conduct tests to establish the diagnosis, assess severity, and rule out differential diagnoses of acute abdominal pain.
Acute pancreatitis is a medical emergency; begin fluid resuscitation as soon as it is suspected.
Laboratory studies
| Laboratory studies in acute pancreatitis | |
|---|---|
| Test | Findings and interpretation |
| Serum pancreatic enzymes [4][5][10] |
|
| CBC |
|
| BMP |
|
| Inflammatory markers [10][11] |
|
| Liver chemistries [19][20] |
|
| LDH [21] |
|
| Serum triglycerides [10][22] |
|
The degree of lipase and/or amylase elevation does not necessarily correlate with the severity of or prognosis for acute pancreatitis. [23]
Measure serum triglycerides promptly after symptom onset, as levels decrease rapidly with fasting. [24]
Determining calcium values is very important: Hypercalcemia may cause pancreatitis, which may then, in turn, cause hypocalcemia!
Imaging
Ultrasound abdomen [9][25]
- Indications: first-line imaging modality for all patients
-
Supportive findings
-
Features of acute pancreatitis (visible in 20% of cases) [9]
- Enlarged hypoechoic pancreas (pancreatic edema)
- Peripancreatic fluid and/or ascites
-
Features of biliary pancreatitis
- Cholelithiasis and/or gallbladder sludge [9]
- Dilated biliary tree
- Evidence of complications: pancreatic pseudocysts, walled-off necrosis (typically > 4 weeks from symptom onset) [15]
-
Features of acute pancreatitis (visible in 20% of cases) [9]

")
Abdominal ultrasound for suspected acute pancreatitis is primarily used to identify gallstones as features of acute pancreatitis are only visible in approximately 20% of cases. [9]
CT abdomen and pelvis with IV contrast [4][9][15]
-
Indications
- Diagnostic uncertainty (e.g., typical clinical features in a patient with moderately elevated pancreatic enzymes)
- Acute deterioration or lack of improvement within 48–72 hours of admission
- Severe pancreatitis : optimally performed > 5–7 days after symptom onset [9]
- To evaluate for underlying etiology if routine diagnostic studies are negative [7]
-
Findings
-
Features of acute pancreatitis
- Enlargement of the pancreatic parenchyma with edema
- Indistinct pancreatic margins with surrounding fat stranding
- Peripancreatic free fluid
- Evidence of complications
- Necrotizing pancreatitis: nonenhancing areas of pancreatic parenchyma
- Acute necrotic collections: ill-defined, heterogeneous appearance with varying densities
- Walled-off necrosis: an encapsulated collection of necrotic material, usually occurring > 4 weeks after the onset of necrotizing pancreatitis
- Infection: air within the pancreatic or peripancreatic tissue or fluid collections
-
Features of acute pancreatitis



CT abdomen is not routinely required to establish a diagnosis of acute pancreatitis. If performed to evaluate for necrotic pancreatitis, the optimal timing to perform a CT abdomen is at least 5–7 days after symptom onset. [9]
Suspect pancreatic tumor as the underlying cause for idiopathic acute pancreatitis in patients aged > 40 years; see “Pancreatic cancer.” [4]
X-ray chest and abdomen [9][26][27]
- Indications: not routinely indicated; may be performed as part of the initial workup of undifferentiated abdominal pain [28]
-
Supportive findings
- On abdominal x-ray
- Sentinel loop sign: dilatation of a loop of small intestine in the left upper abdomen (duodenum or jejunum) [29]
- Colon cut off sign: gaseous distention of the ascending and transverse colon that abruptly terminates at the splenic flexure. [29]
- Calcified gallstones or pancreatic stones
- On chest x-ray: pleural effusion, pulmonary edema suggesting ARDS
- On abdominal x-ray


MRI abdomen [7][9]
-
Indications
- In combination with MRCP in cases of suspected choledocholithiasis
- An alternative to CT
-
Supportive findings
- Enlarged, edematous pancreas
- Pancreatic necrosis
- Complications (e.g., walled-off necrosis, pseudocysts)
Magnetic resonance cholangiopancreatography [5][7][9]
- Indications: prior to therapeutic ERCP in suspected biliary pancreatitis
-
Findings
- Evidence of choledocholithiasis ; see “MRCP” in “Choledocholithiasis” for details
- Can also identify pancreatic ductal anomalies that may trigger acute pancreatitis
")

Endoscopic retrograde cholangiopancreatography
-
Indications
- Suspected choledocholithiasis (if MRCP or MRI are not feasible) [9]
- To evaluate for sphincter of Oddi dysfunction in patients with recurrent pancreatitis and normal or inconclusive EUS and MRCP [30]

Endoscopic ultrasound [31]
- Indication: evaluation of the underlying cause if routine initial workup fails to establish the etiology
- Findings: occult microlithiasis, pancreatic neoplasms, chronic pancreatitis, other pancreatic parenchymal, ductal, and ampullary disorders may be identified
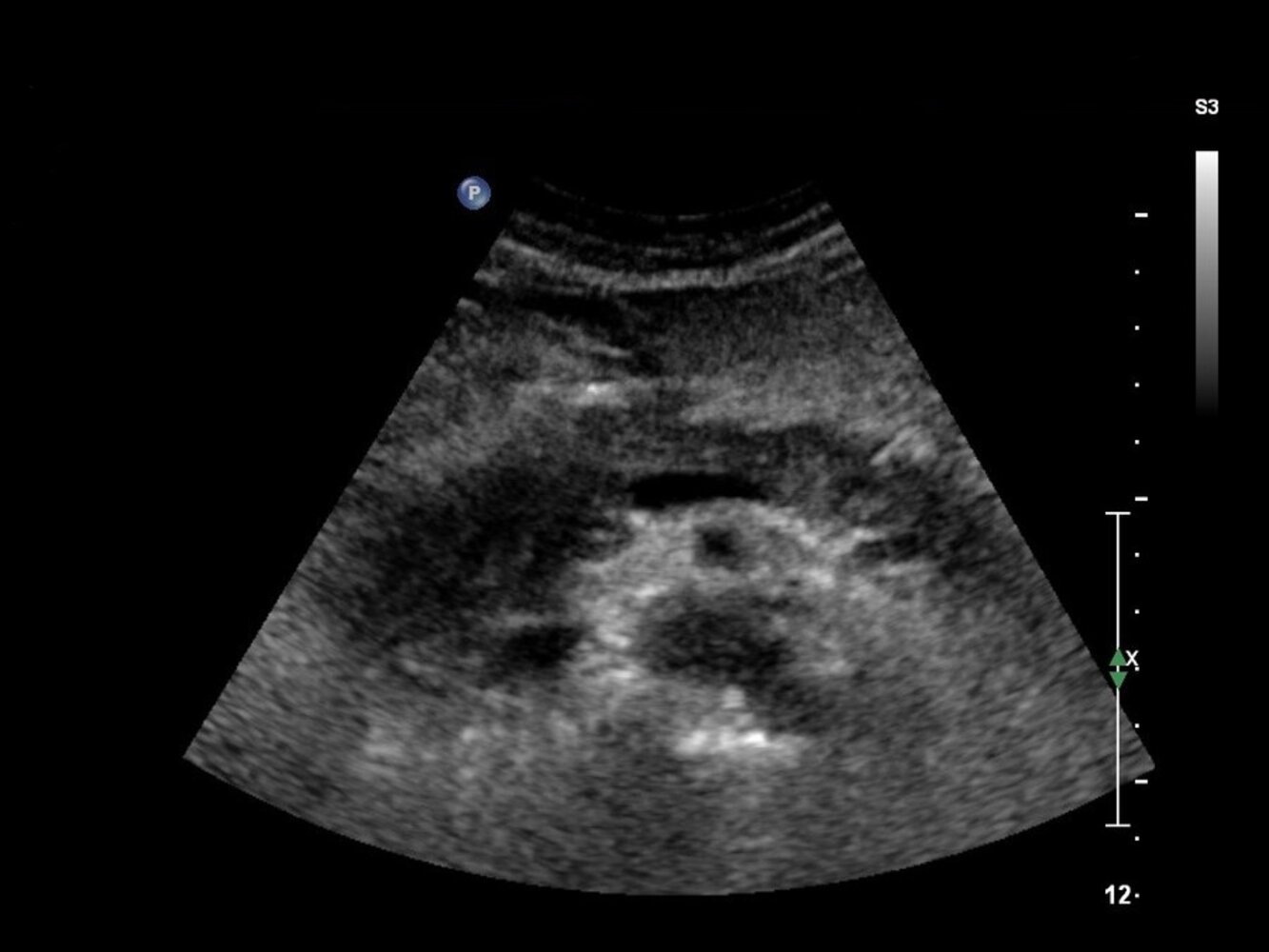
Ultrasound pancreas (transverse plane) of a patient with clinical signs of acute pancreatitis
The pancreatic head (green overlay) is enlarged and hypoechoic, with an ill-defined border.
The findings are consistent with acute pancreatitis. However, a wide spectrum of benign and malignant conditions can have a similar appearance on ultrasound.
A: aorta; dashed outline: pancreas; SMA: superior mesenteric artery; SMV: superior mesenteric vein; SV: splenic vein; V: inferior vena cava
Image source of original image: sonographiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg. Created by: Dr. J. Guntau. Modifications to original image: The text at the top and left has been removed.
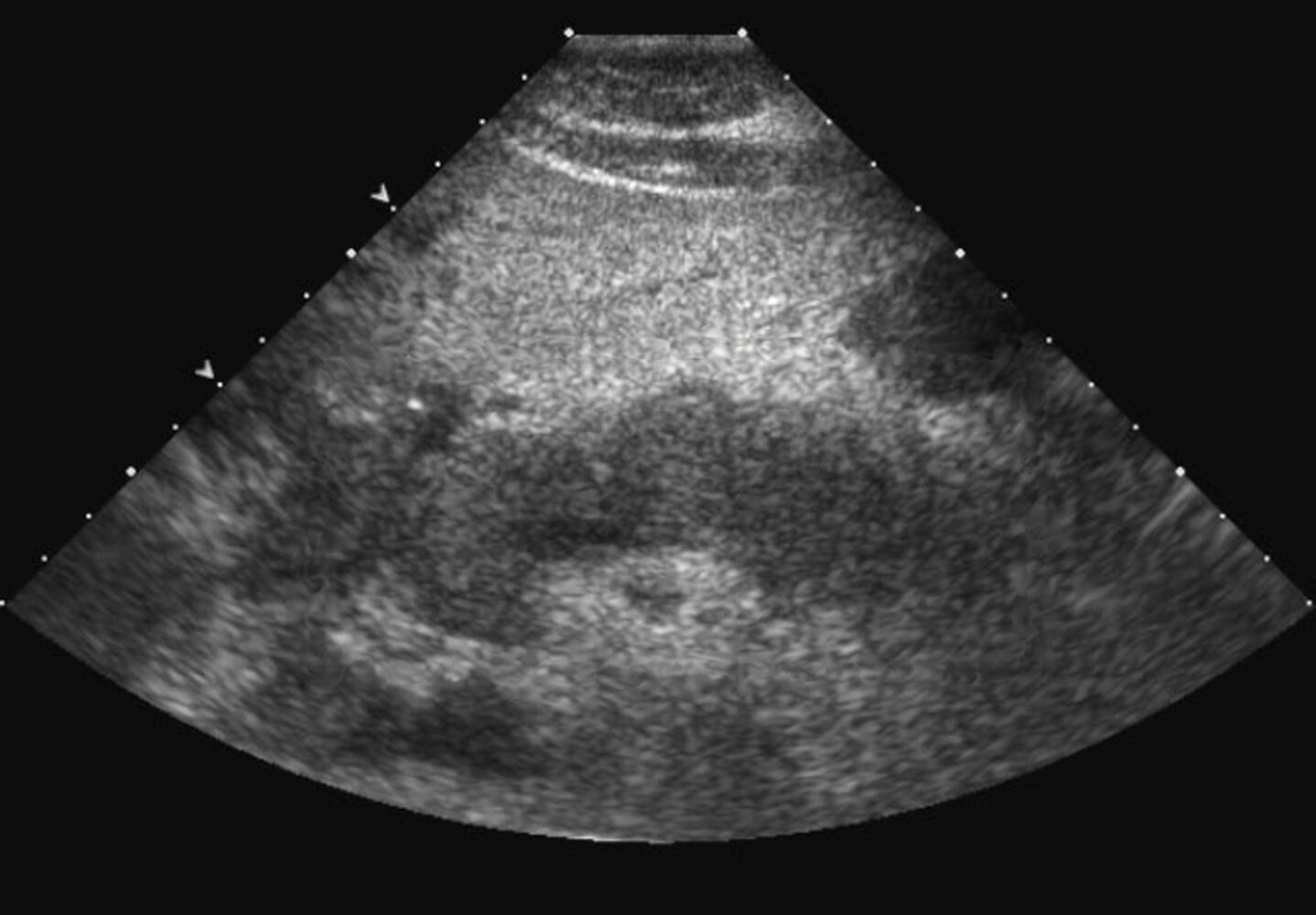
Ultrasound abdomen (transverse plane) of a patient with a history of pancreatitis
Portions of the pancreatic head (H), neck (N), and body (B) are seen. The tail is not well visualized (indicated by arrowheads). The visible pancreas is diffusely hypoechoic and lobulated.
Ultrasound is often used as a frontline tool to assess the pancreas. It is frequently used to assess for biliary dilatation and calculi in the setting of suspected pancreatitis. The pancreas may be obscured by bowel gas, particularly in the presence of an ileus, but a visible inflamed or necrotic pancreas may appear enlarged, hypoechoic, or heterogeneous. Ultrasound can be used to guide therapeutic interventions and help monitor the evolution of peripancreatic fluid collections that may accompany pancreatitis.
L: liver; S and dashed line: spine
Source: “Acute-pancreatitis-20.jpg” by Iqra Qamar, wikidoc.org, licensed under CC BY-SA 3.0. Modifications: - box and description removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
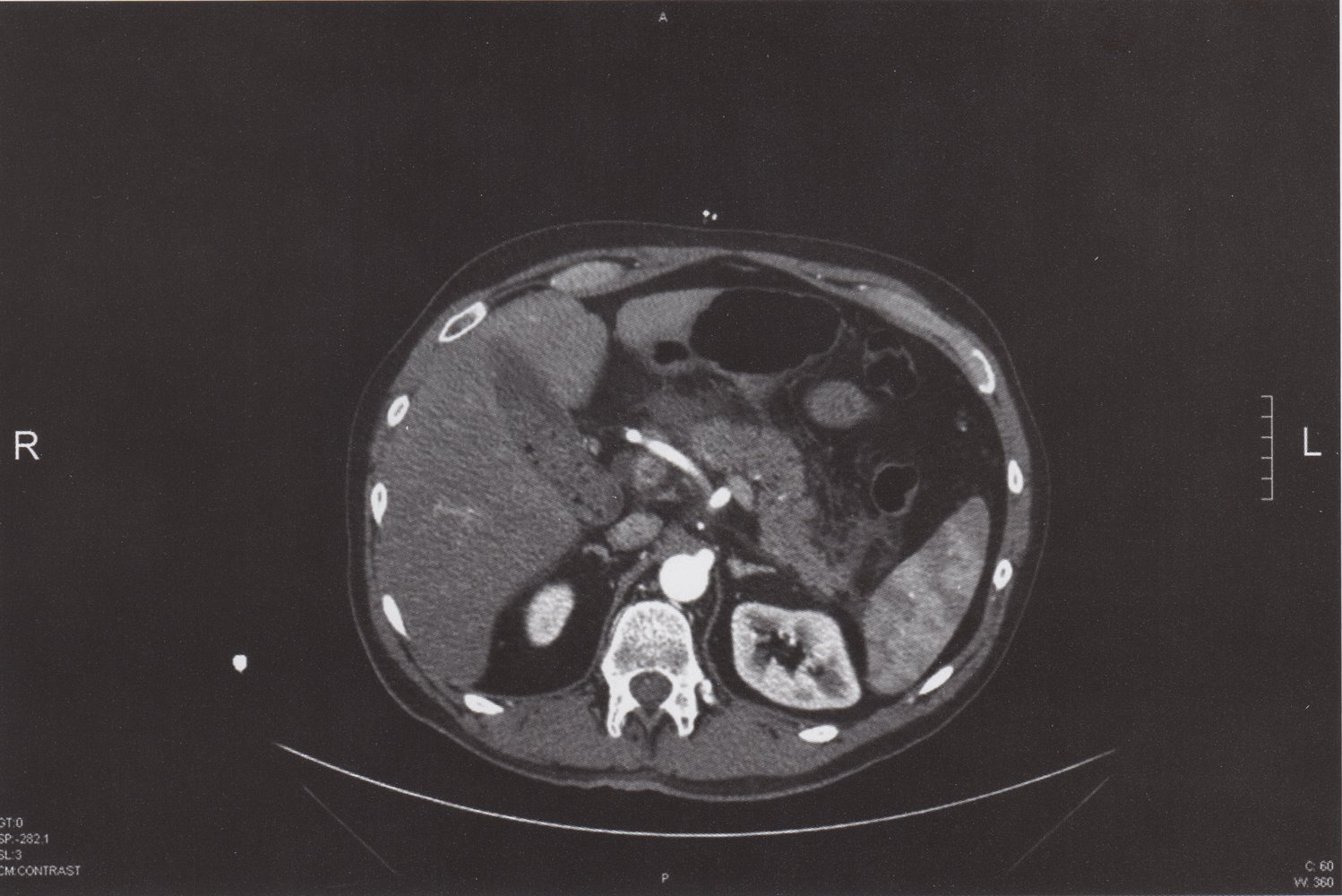
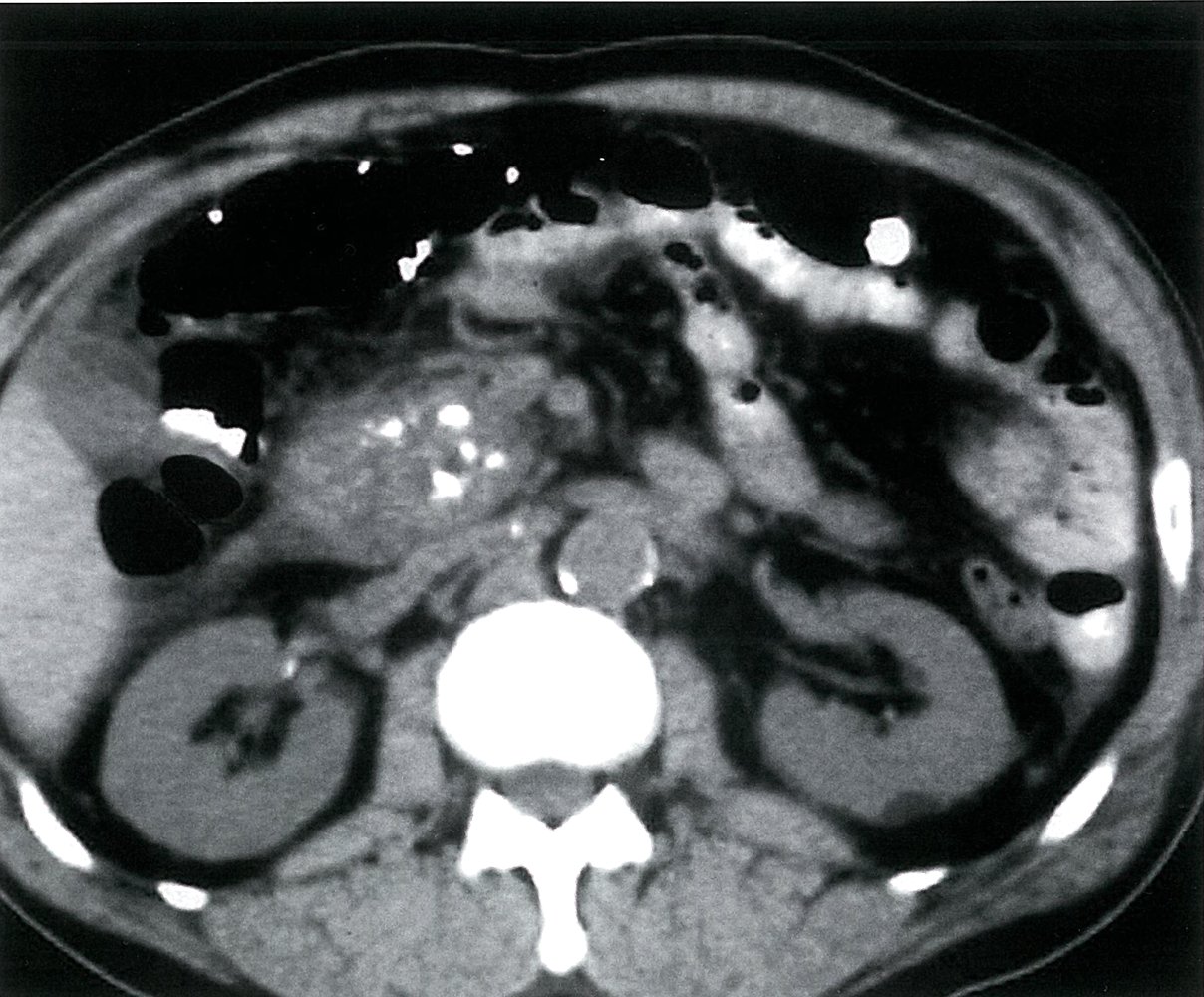
CT abdomen (with contrast; axial plane) of a patient with acute biliary pancreatitis
Fatty and fascial stranding (yellow overlay) anterior to the pancreas (P) indicates peripancreatic inflammation. The gallbladder (yellow outline) contains calculi (examples indicated by red overlay) and sludge. In addition, the common bile duct (green overlay) is slightly dilated.
The passage of a gallbladder calculus through the common bile duct can result in acute pancreatitis.
A: aorta; Vc: ascending vena cava; L: liver; Sp: spleen; Red arrow: hepatic artery; Green outline: stomach
Source: © IMPP
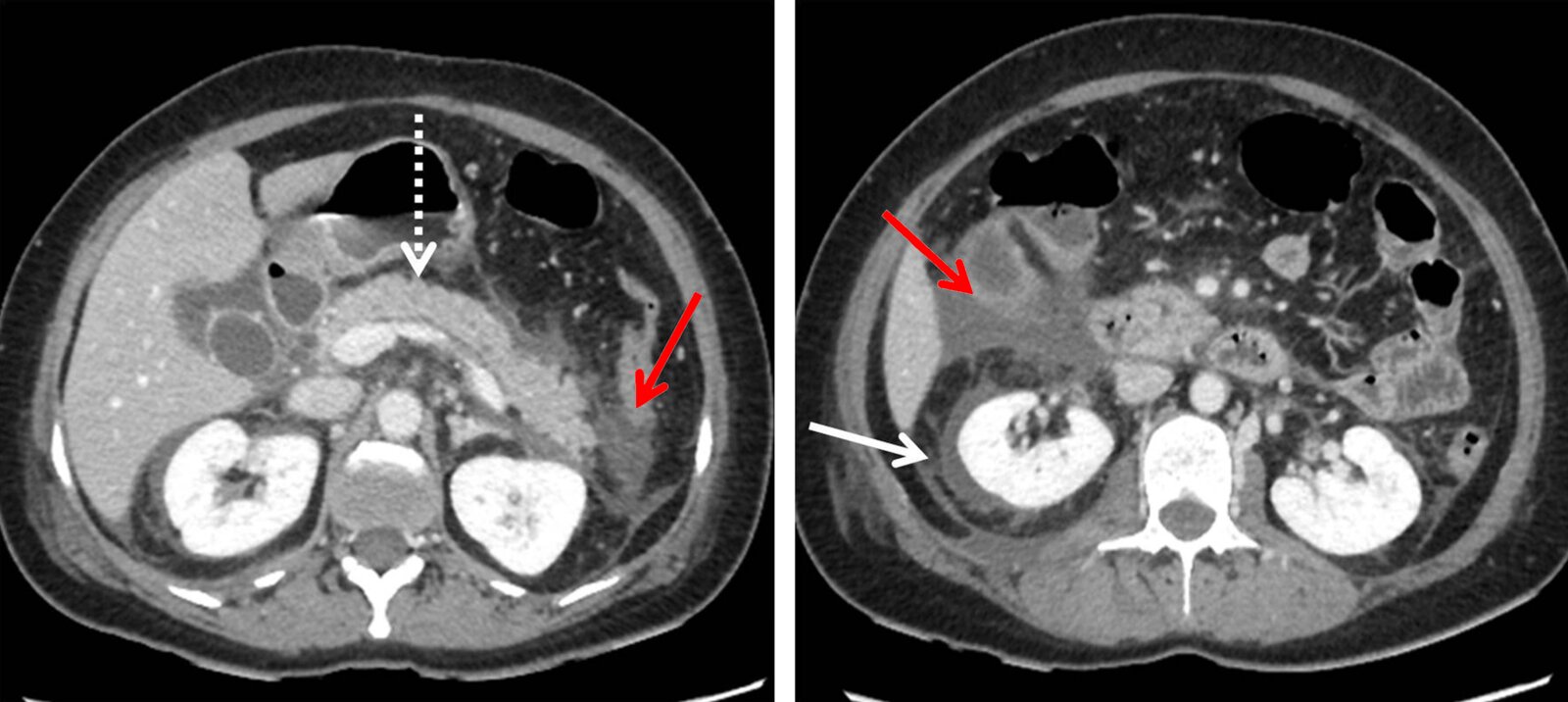
CT abdomen (with contrast; axial plane)
An unencapsulated homogeneous acute peripancreatic fluid collection (APFC) without solid components is visible. The appearance is characteristic of acute interstitial (uncomplicated) pancreatitis. Fluid and fatty stranding can be seen anterior to the pancreas as well as in the pararenal spaces (red arrows). There is also perirenal fluid (white arrow). Pancreatic tissue (dashed arrow; P) is homogeneously enhanced, without evidence of tissue necrosis.
APFCs may be single or multiple and usually develop early in acute pancreatitis. Persistence for more than 4 weeks increases the likelihood of the development of a pseudocyst.
K: kidney; L: liver
Source: “Figure 3. in: Imaging lexicon for acute pancreatitis: 2012 Atlanta Classification revisited” by Binit Sureka, Kalpana Bansal, Yashwant Patidar, Ankur Arora, Gastroenterology Report Journal, Oxford Academic, licensed under CC BY 4.0. Modifications: Deleted A and B; changed color of two arrows. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (with contrast; axial plane)
Well-demarcated nonenhancing low attenuation areas of walled-off parenchymal necrosis (green overlay) are visible throughout the pancreas. Incidentally noted very low attenuation lesions in the kidneys (K) are cysts.
L = liver
Source: “Fig. 1B, in: Open necrosectomy is feasible as a last resort in selected cases with infected pancreatic necrosis: a case series and systematic literature review” by Lucia Ilaria Sgaramella, Angela Gurrado, Alessandro Pasculli, Francesco Paolo Prete, Fausto Catena & Mario Testini, BMC World Journal of Emergency Medicine, licensed under CC BY 4.0. Modifications: Image is cropped, letter "B" is removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray abdomen (AP; supine) of an adolescent with acute hepatopancreatitis
A short segment of adynamic ileus (sentinel loop sign, white arrows) is seen in the left upper quadrant.
Identification of a sentinel loop can be helpful in localizing inflammation in the abdomen.
Source: “Fig 2, In: A Rare Cause of Acute Hepatopancreatitis in a Nepalese Teen” by Swastika Adhikari, Ashish Lal Shrestha , Sanjay Raj Thapa, Amrit Ghimire, Hindawi, licensed under CC BY 4.0. Modifications: removal of the lower arrow indicating colon cut-off sign. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
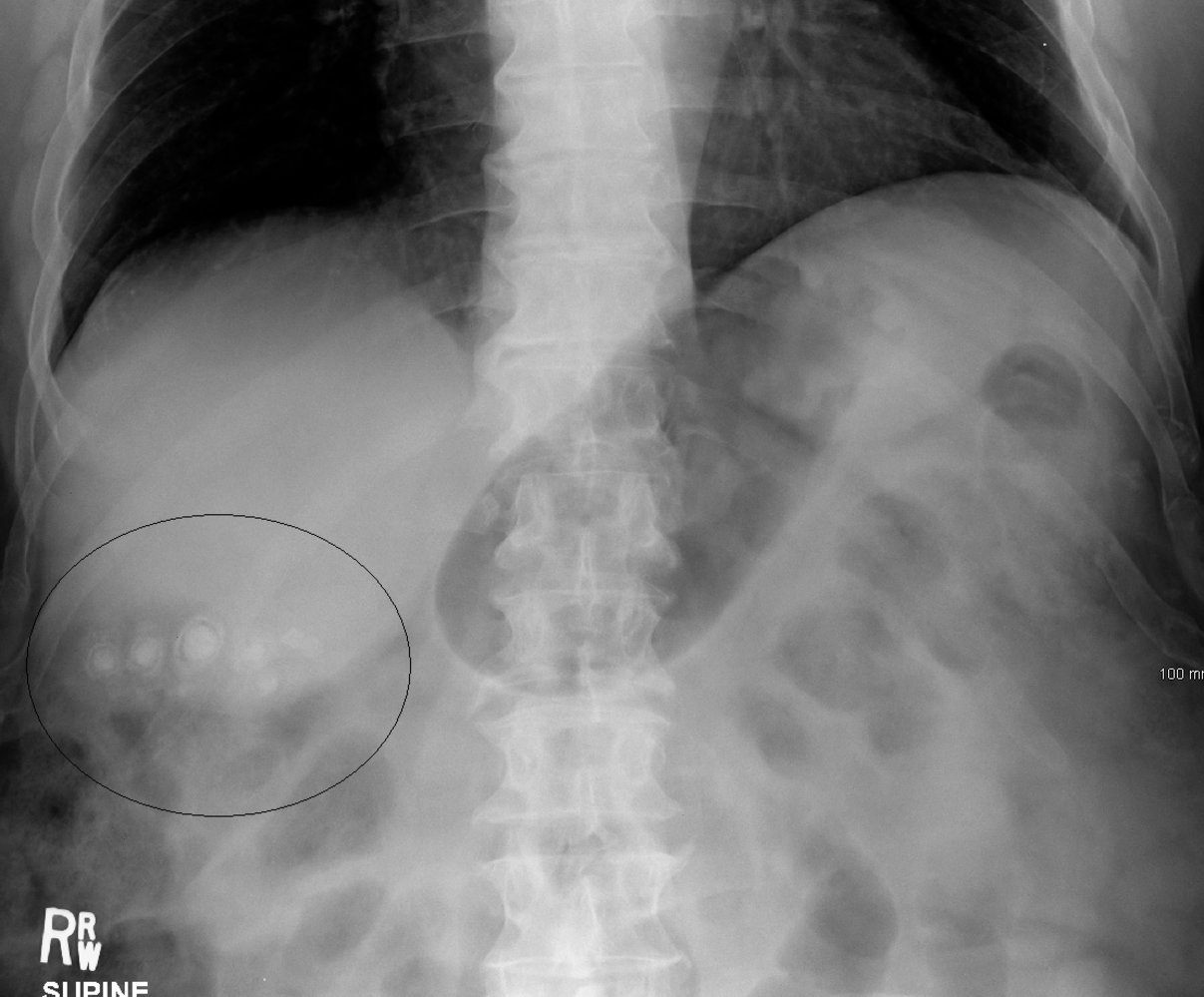
X-ray abdomen (AP view; supine position)
Multiple rounded calcified structures are visible in the right upper quadrant (black circle). Many have a laminated appearance, with a dense central calcification (green) surrounded by an inner lucent ring and outer calcified ring (white outline).
Pure cholesterol stones, the most common type of gallstone, are radiolucent on abdominal radiographs. Black pigment and mixed gallstones may contain sufficient calcium to be radiopaque.
Source: “StonesXray” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
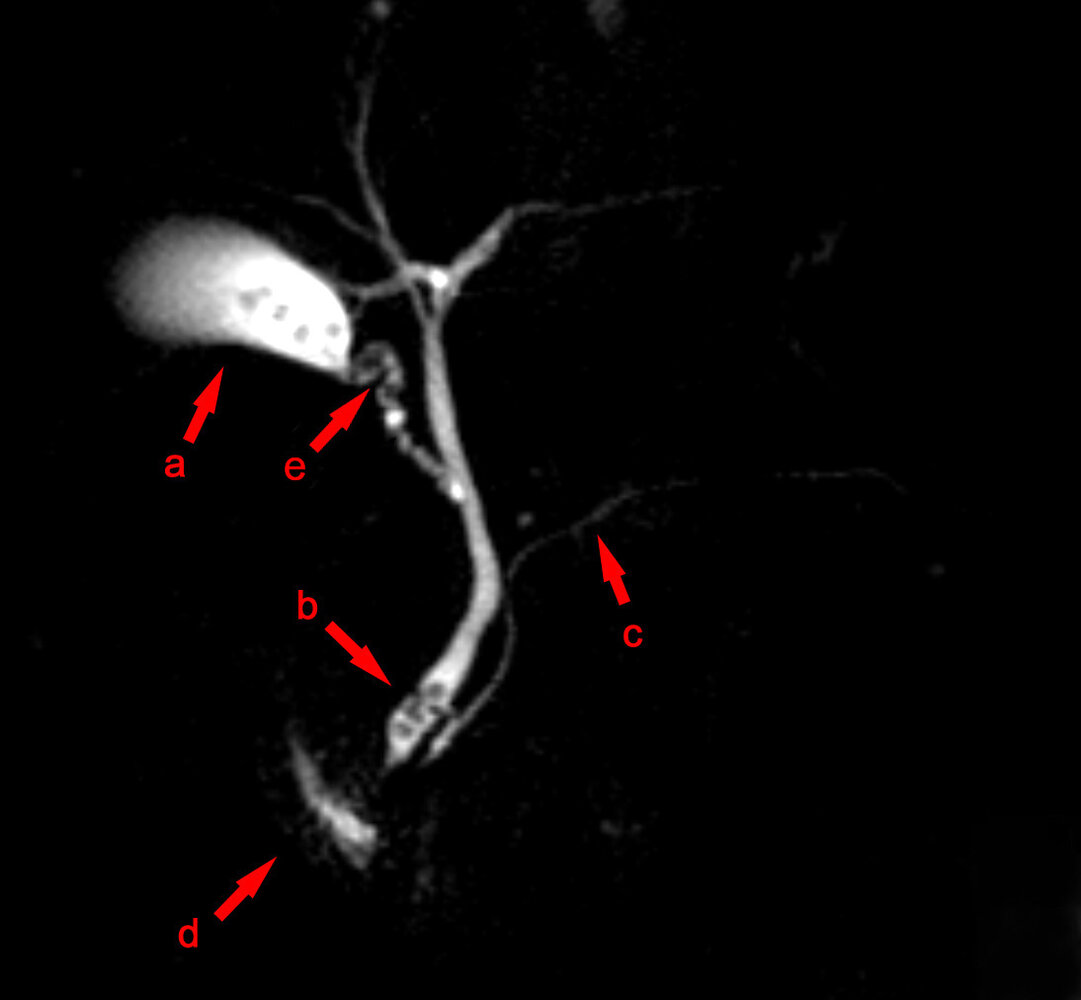
Magnetic resonance cholangiopancreatography (MRCP)
Filling defects representing calculi are visible within the gallbladder (a), cystic duct (e), and common bile duct (b).
c: pancreatic duct; d: duodenum
Source: “MRCP Choledocholithiasis” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: arrow and "e" added to mark the cystic duct.
{kind=link}
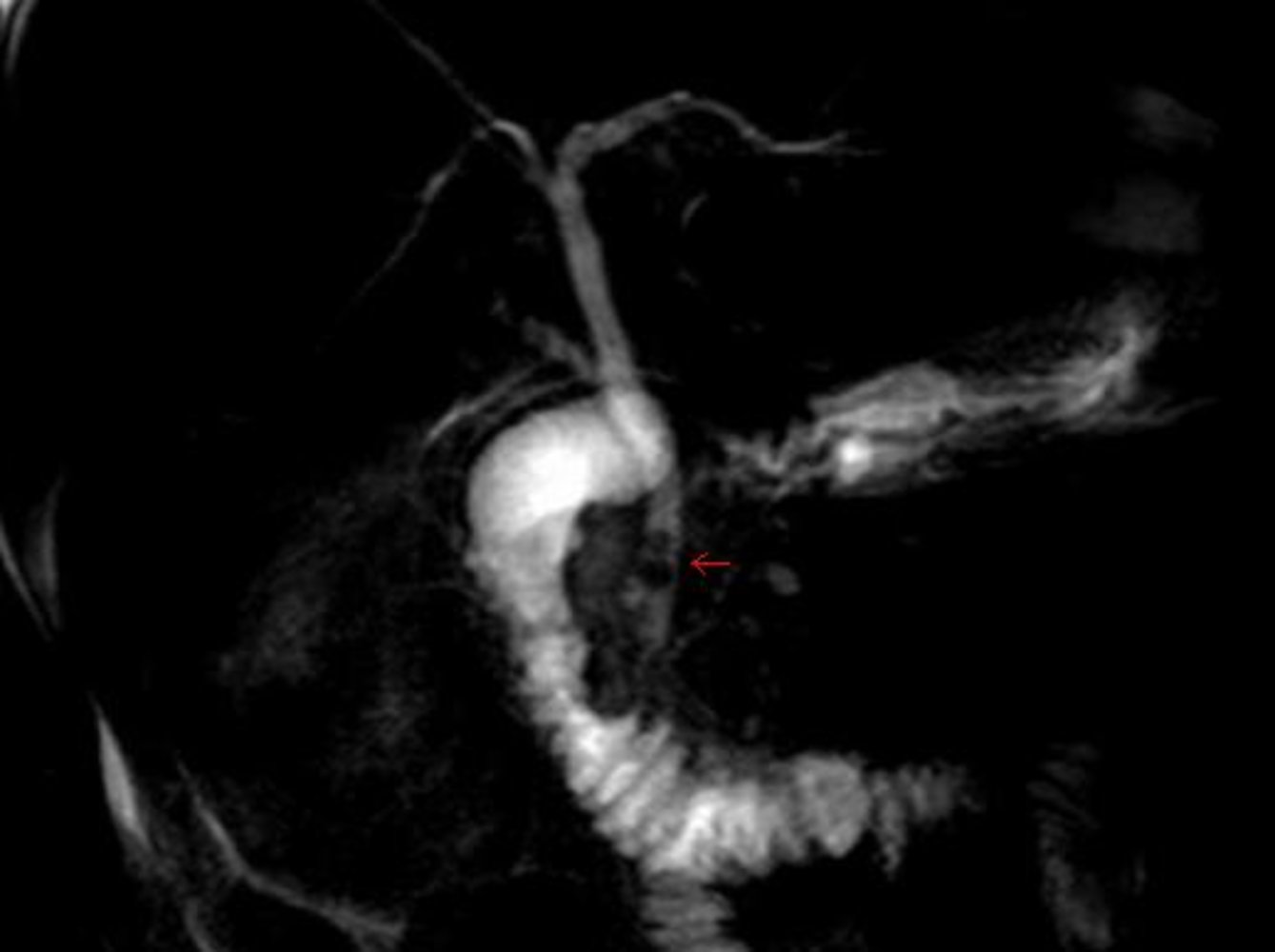
Imaging of extra- and intrahepatic bile ducts by means of magnetic resonance cholangiopancreatography (MRCP)
On the top left and right hepatic duct merge to form the common hepatic duct (CHD). The CHD can be seen as a straight, almost vertical line in this image. Towards the left-hand side of the CHD, the cystic duct leads to the gallbladder. Beneath that, two small gallstones are visible as round hypointensities within the CHD (red arrow).
Source: “CBD Stones” by Samir, Wikimedia Commons, licensed under CC BY 2.0.
{kind=link}

ERCP (positive mode; ventral view)
The tip of the endoscope (E) is located within the duodenum at the ampulla of Vater. Contrast enhancement of the hepatic biliary tract, left and right hepatic ducts, common hepatic duct (CHD), cystic duct (CD), gall bladder (G), common bile duct (CBD), and pancreatic duct (PD) can be seen. Multiple filling defects (examples indicated by green overlay) can be seen within the gall bladder and cystic duct.
These findings are diagnostic of cholelithiasis.
Source: “ERCP Roentgen” by J. Guntau, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Severity grading and prognostic scores
There are several scores used to assess the severity and prognosis of acute pancreatitis. The most commonly used and validated scores are described here.
Revised Atlanta grades of severity [6]
The revised Atlanta grades of severity classify pancreatitis as mild, moderately severe, or severe, depending on the presence of organ failure. Organ failure can be determined using the modified Marshall scoring system for organ dysfunction.
- Mild acute pancreatitis: no organ failure and no local or systemic complications
- Moderately severe acute pancreatitis: transient organ failure (< 48 hours) and/or local or systemic complications
- Severe acute pancreatitis: persistent organ failure (> 48 hours)
Patients with organ failure at presentation or within the first 24 hours of admission should be classified as having severe pancreatitis. If organ failure resolves within 48 hours, patients can be reclassified as having moderately severe acute pancreatitis. [6]

CT severity index [8][24][32]
The CT severity index for acute pancreatitis (CTSI) and modified CT severity index (MCTSI) can be used to estimate the severity, mortality, and morbidity of acute pancreatitis based on the extent of pancreatic inflammation and necrosis on a CT abdomen performed ideally > 5–7 days (or at least 72 hours) after symptom onset.
| CTSI and MCTSI | |||
|---|---|---|---|
| CTSI score [33] | MCTSI score [34] | ||
| Degree of inflammation | Normal pancreas | 0 | 0 |
| Localized or diffuse enlargement | 1 | 2 | |
| Peripancreatic inflammation | 2 | ||
| Single acute fluid collection | 3 | 4 | |
| Multiple or extensive acute fluid collections | 4 | ||
| Degree of parenchymal necrosis | None | 0 | 0 |
| < 30% | 2 | 2 | |
| ≥ 30%–50% | 4 | 4 | |
| > 50% | 6 | ||
| Presence of extrapancreatic complications | n/a | 2 | |
| Interpretation |
|
|
|
Ranson criteria [8][28]
The Ranson criteria is one of the oldest predictive models used to estimate severity and prognosis of biliary and nonbiliary pancreatitis; , but full assessment is only possible after 48 hours, and sensitivity for predicting severity and outcome can be as low as 70%.
| Ranson criteria for acute pancreatitis [23] | ||
|---|---|---|
| Parameter | Nonbiliary pancreatitis | Biliary pancreatitis |
| On admission | ||
| Age | > 55 years | > 70 years |
| WBC | > 16,000/mm3 | > 18,000/mm3 |
| Blood glucose | > 200 mg/dL | > 220 mg/dL |
| Serum LDH | > 350 U/L | > 400 U/L |
| Serum AST | > 250 U/L | > 250 U/L |
| After initial 48 hours | ||
| Hct decrease | > 10% | > 10% |
| BUN increase | > 5 mg/dL | > 2 mg/dL |
| Serum calcium | < 8 mg/dL | < 8 mg/dL |
| Arterial pO2 | < 60 mm Hg | n/a |
| Fluid sequestration | > 6 L | > 4 L |
| Serum base deficit | > 4 mmol/L | > 5 mmol/L |
Interpretation [35]
| ||
Acute physiology and chronic health evaluation II (APACHE II score) [8]
- Mainly used in the ICU setting to determine the severity of acute pancreatitis
- Scores ≥ 8 indicate severe pancreatitis with a guarded prognosis. [8][11]
Bedside index of severity of acute pancreatitis (BISAP) [11]
- Used to estimate in-hospital mortality due to pancreatitis
-
Each criterion is worth one point.
- BUN > 8.9 mmol/L
- Altered mental status
- Presence of SIRS
- Age > 60 years
- Pleural effusion on chest x-ray
- BISAP ≥ 2 indicates severe pancreatitis.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Treatment
The initial management is identical for all etiologies of acute pancreatitis and should be administered without delay. For management in pregnant individuals and children, see “Special patient groups.”
Acute stabilization [4][5][7][11]
- ABCDE survey
- Hemodynamic and respiratory support
- Maintain NPO status until potential causes of acute abdomen that require emergency surgery have been ruled out.
Goal-directed IV fluid therapy for acute pancreatitis [4][5][7][11]
Fluids and infusion rate [4][5][11]
- Crystalloids such as lactated Ringer's solution (LR) are preferred. [4]
- Hemodynamically stable patients [4]
- Moderately aggressive IV fluid therapy in the first 24–48 hours
- Normovolemic patients: LR 1.5 mL/kg/hour [4][36]
- Hypovolemic patients: LR 10 mL/kg bolus [4][36]
- Exercise caution in patients with renal or cardiovascular disease.
- Moderately aggressive IV fluid therapy in the first 24–48 hours
-
Hemodynamically unstable patients [37]
- Administer rapid fluid bolus (e.g., LR 500–1000 mL IV bolus over 10–30 minutes).
- Repeat as needed based on response.
- See also “Fluid resuscitation” for further detail.
Monitoring [8][12]
- Monitor vitals, oxygen saturation, and urine output every 1–2 hours during the initial period of IV fluid therapy.
- Obtain laboratory studies (CBC, BMP, HCT) every 6–12 hours to monitor adequacy of fluid resuscitation and tissue perfusion.
- Perform serial physical examination every 4–6 hours to assess for abdominal compartment syndrome.
Fluid therapy goals in acute pancreatitis [7]
- Heart rate < 120 bpm, MAP 65–85 mm Hg
- Urine output > 0.5–1 mL/kg/hour
- Central venous pressure 8–12 mm Hg, central venous oxygen saturation ≥ 70% [38]
- Hct 35–44%
- Reduction in BUN [4]
Intravenous fluid resuscitation in the first 12–24 hours has the greatest impact on the clinical outcome of patients with acute pancreatitis. [4]
Supportive therapy
-
Analgesics: based on the WHO analgesic ladder [39]
- NSAIDS (e.g., ketorolac , diclofenac , ibuprofen ) [40][41]
- Opioids; (e.g., hydromorphone , morphine ) [42]
- Consider patient-controlled analgesia for management of severe pain. [11][41]
- Antiemetics (e.g., ondansetron , metoclopramide )
- Electrolyte repletion
In concurrent acute kidney injury, avoid NSAIDs and use opioids with caution because of the risk of accumulation. [11]
Prophylactic antibiotics are not recommended, and should only be used in patients with evidence of infected necrosis. [4]
Consults
- Multidisciplinary care is ideal.
- Urgent gastroenterology, surgery, and/or interventional radiology for cholangitis, choledocholithiasis, or localized complications
Disposition [7][28]
- Hospital admission is usually required.
- Consider ICU admission in the following cases:
- Organ dysfunction or failure
- Ongoing SIRS or fluid resuscitation requirements
- Significant electrolyte imbalances
- Older age or high-risk comorbidities
- Severe pancreatitis on severity scores
- Refer to a specialist center if the need for surgical or interventional procedures is anticipated. [7]
Nutrition
- Early oral feeding: : low-fat, solid diet as soon as tolerated, ideally within 24 hours [4][5][43]
- Enteral tube (nasogastric or nasojejunal): preferred over parenteral nutrition if patients cannot tolerate oral intake [5][44]
- Parenteral nutrition (total or partial): only in patients who cannot tolerate enteral feeds (e.g., those with persistent paralytic ileus) [45]
Bowel rest is no longer routinely recommended. Enteral nutrition, via oral route or enteral tube, should be initiated as early as tolerated. [5]
Management of the underlying cause
Biliary pancreatitis
-
Therapeutic ERCP [5][7][38]
- Indication: biliary pancreatitis associated with cholangitis or persistent CBD obstruction
- Timing: Urgent therapeutic ERCP (within < 24 hours) is indicated if there is concurrent cholangitis.
- Procedure: sphincterotomy and stone removal; see “Treatment of choledocholithiasis”
- Complications: aggravation of pancreatitis, perforation, hemorrhage [9]
-
Cholecystectomy [5][7][46]
- Indications
- All patients with biliary pancreatitis to prevent recurrence
- Consider in patients with a recurrent episode of acute pancreatitis of unclear etiology [4]
- Timing: recommended during the initial admission for patients with mild biliary pancreatitis
- Indications
Urgent ERCP is not indicated in acute biliary pancreatitis unless acute cholangitis is present. [5]
Hypertriglyceridemia-induced pancreatitis [24]
-
Initiate measures to rapidly decrease triglyceride levels alongside fluid resuscitation and analgesia.
- Insulin therapy ; monitor blood glucose levels.
- Plasmapheresis and hemofiltration
- Evaluate for secondary causes of hypertriglyceridemia ; consider screening for familial hypertriglyceridemia if none are present.
- Long-term management
- Initiate long-term lipid-lowering therapy e.g., with fibrates, as soon as tolerated to prevent recurrences.
- Dietary and lifestyle modifications
- See “Treatment of hypertriglyceridemia in adults” for details.
Hypercalcemia-induced pancreatitis [18]
- Initial treatment: See “Treatment of hypercalcemia.”
- Definitive management: Investigate for primary hyperparathyroidism; if this is the underlying cause, perform parathyroidectomy.
Alcohol-induced pancreatitis
- Check magnesium and phosphorus levels and replete as needed. [8][47]
- Vitamin supplementation (thiamine, pyridoxine)
- See “Treatment of alcohol use disorder” for details.
- Provide counseling on alcohol use disorder before discharge. [5]
"PANCREAS": Perfusion (fluid replacement), Analgesia, Nutrition, Clinical (observation), Radiology (imaging), ERCP, Antibiotics (if indicated), Surgery (surgical intervention, if necessary)
Dot phrase
Acute pancreatitis (adult)
Assessment: This is a @AGE@-year-old @SEX@ with a [**]-day history of constant, severe epigastric pain radiating to the back, lipase [**amylase] ≥ 3x ULN, and features of acute pancreatitis on ultrasound [**CT].
Most likely diagnosis: acute pancreatitis
Severity
-Mild [**no organ failure and no local or systemic complications]
-Moderate to severe [**organ failure and/or local or systemic complications]
Differential diagnoses: peptic ulcer disease, gastritis, acute peritonitis, acute cholecystitis, acute cholangitis, biliary colic, myocardial infarction
Plan
Disposition
-ICU admission is appropriate because the patient has [**organ dysfunction or failure, ongoing SIRS or fluid resuscitation requirements, significant electrolyte imbalances, older age or high-risk comorbidities, severe pancreatitis based on severity scores].
-OR Inpatient admission is appropriate because the patient does not have severe pancreatitis, organ dysfunction or failure, SIRS or sepsis, require ongoing hemodynamic support, have significant electrolyte disturbances, high-risk comorbidities.
IV fluid therapy
-[**Normovolemic] LR 1.5 mL/kg/hour for 24–48 hours
-[**Hypovolemic] LR 10 mL/kg bolus, then 1.5 mL/kg/hour for 24–48 hours
Monitoring
-Vital signs, O2 sat, and UOP every 1–2 hours during initial fluid resuscitation
-CBC, BMP every 6–12 hours to monitor fluid resuscitation and tissue perfusion
-Abdominal exam every 4–6 hours to assess for abdominal compartment syndrome
Pain management
NSAIDs
-Ketorolac 15–30 mg IV/IM every 6 hours PRN
-OR [Diclofenac 37.5 mg IV every 6 hours PRN]
-OR [Ibuprofen 400–800 mg IV every 6–8 hours PRN]
Opioids (for NSAID contraindication or severe pain)
-Hydromorphone hydrochloride (immediate release) 2–4 mg PO every 4–6 hours PRN
-OR [Hydromorphone hydrochloride 0.2–1 mg IV every 2–3 hours PRN]
-OR [Morphine sulfate 0.1–0.2 mg/kg IV every 4 hours PRN]
-OR [Morphine sulfate 10 mg IM every 4 hours PRN]
-OR [Patient-controlled analgesia for severe pain]
Antiemetics
-[Ondansetron 4–8 mg PO/IV every 8 hours PRN]
-OR [Metoclopramide 10 mg IV/IM/PO every 4–8 hours PRN]
F/E/N
-Replete electrolytes.
-Low-fat, solid diet as soon as tolerated OR [Enteral tube feeding for patients who cannot tolerate oral intake] OR [Parenteral nutrition for patients who cannot tolerate enteral intake]
Consults: [**GI/surgery/IR] for ERCP for biliary pancreatitis with cholangitis or CBD obstruction
Special patient groups
Acute pancreatitis during pregnancy [48]
Epidemiology
- Incidence is 1:1000–1:10,000 pregnancies
- More commonly affects multiparous individuals (75%)
- The majority of cases occur in the third trimester (50%), followed by the early postpartum period (38%), and the first and second trimester (12%)
Etiology
- Most commonly gallstones, heavy alcohol use, and familial hypertriglyceridemia
- Physiologic changes during pregnancy such as altered progesterone and estrogen levels increase the risk of choledocholithiasis.
- ↑ Progesterone → ↑ pressure on the sphincter of Oddi → bile stasis
- Estrogen alters the composition of bile, making it more lithogenic.
Clinical features
Similar to clinical features of acute pancreatitis in nonpregnant individuals
Diagnostics
-
CBC
- May show physiologic alterations due to pregnancy (e.g., leukocytosis, increased serum amylase and lipase)
- If amylase and/or lipase are > 3 times greater than normal, acute pancreatitis is likely [48]
- Imaging: abdominal ultrasound or MRI are preferred (e.g., to identify choledocholithiasis or complications of acute pancreatitis such as hemorrhage, edema, or pseudocysts)
Treatment
- Identical to that for nonpregnant individuals (see “Treatment of acute pancreatitis.”)
- See “Overview of analgesics to avoid during pregnancy” for further details.
Complications
- See “Complications of acute pancreatitis.”
- Pregnancy-related complications: increased risk of preterm labor, premature birth, and/or fetal death
Acute pancreatitis in children [49][50][51]
Epidemiology
Incidence is 3–13 cases per 100,000 people per year. [51]
Etiology [51]
- Biliary pancreatitis (most common cause)
- Medications (e.g., valproic acid, mesalamine, glucocorticoids)
- Systemic disease (e.g., metabolic disorders, hemolytic uremic syndrome, Kawasaki disease)
- Underlying genetic conditions (e.g., cystic fibrosis)
- Anatomical anomalies of the pancreas (e.g., pancreas divisum, annular pancreas)
- Trauma and/or child maltreatment
- Infection (e.g., mumps, influenza, herpes viruses, hepatitis)
- Critical illness (e.g., sepsis)
- Autoimmune pancreatitis
Approximately 20% of children have > 1 underlying cause. [51]
Clinical features [51]
- Similar to clinical features of acute pancreatitis in adults
- Symptoms common in infants and young children include:
- Generalized abdominal pain
- Irritability
Diagnostics
- Similar to diagnostics for acute pancreatitis in adults [49][50]
- Use adult diagnostic criteria for acute pancreatitis.
- Serum lipase is more reliable than amylase in infants. [51]
- Abdominal ultrasound is the preferred initial imaging modality. [49]
- Studies considered by a specialist (e.g., gastroenterology) may include:
- Genetic studies [50]
- Diagnostics for cystic fibrosis
- Stool studies
Management of pediatric pancreatitis [49][50]
-
Treatment of acute pancreatitis in children is similar to adults with the following changes:
- Use pediatric parameters for fluid resuscitation (e.g., lactated Ringer's solution or normal saline). [49]
- Bolus: 10–20 mL/kg once in hemodynamically unstable patients [49]
- Maintenance rate: 1.5–2 times the typical weight-based maintenance rate for 24–48 hours [49]
-
Pain management according to the WHO analgesic ladder may include both of the following:
- Nonopioid oral analgesia in children (e.g., acetaminophen, NSAIDs)
- Opioids for acute pain
- Use pediatric parameters for fluid resuscitation (e.g., lactated Ringer's solution or normal saline). [49]
- Consult a specialist (e.g., gastroenterology, surgery) for:
- Clinical deterioration
- Suspected complications
- Consideration of invasive procedure
- Recurrent acute pancreatitis
Up to 40% of children with acute pancreatitis eventually progress to chronic pancreatitis. [51]
Differential diagnoses
-
Intestinal manifestations
- Acute peritonitis
- Appendicitis
- Acute mesenteric ischemia
- Acute cholecystitis
- Acute cholangitis
- Peptic ulcer disease
- Biliary colic
- Abdominal aortic aneurysm
-
Extraintestinal manifestations
- Myocardial infarction
- Bacterial pneumonia
- See also “Differential diagnoses of acute abdomen.”
Reference:[8]
The differential diagnoses listed here are not exhaustive.
Acute pancreatitis vs. chronic pancreatitis
| Overview of acute and chronic pancreatitis | |||
|---|---|---|---|
| Acute pancreatitis | Chronic pancreatitis | ||
| Characteristics |
|
|
|
| Etiology | Most common causes |
|
|
| Less common causes |
|
|
|
| Pathophysiology |
|
||
|
|
||
| Course |
|
|
|
| Clinical features | Main symptoms |
|
|
| Further symptoms |
|
|
|
| Diagnostics | Laboratory studies |
|
|
| Imaging |
|
|
|
| Treatment |
|
||
|
|
||
| Complications |
|
|
|
| Prognosis |
|
|
|



")
Periumbilical ecchymosis as a result of retroperitoneal hemorrhage, commonly seen in acute pancreatitis.
Source: “Cullen's sign” by Herbert L. Fred, MD and Hendrik A. van Dijk, openstax, licensed under CC BY 2.0.
Right-sided flank ecchymosis suggestive of retroperitoneal hemorrhage, commonly seen in acute pancreatitis.
Source: “Images of Memorable Cases: Case 21: Hemorrhagic pancreatitis - Grey Turner's sign” by Herbert L. Fred, MD and Hendrik A. van Dijk, Wikimedia Commons, licensed under CC BY 2.0.
CT abdomen (with contrast; axial plane) of a patient with acute biliary pancreatitis
Fatty and fascial stranding (yellow overlay) anterior to the pancreas (P) indicates peripancreatic inflammation. The gallbladder (yellow outline) contains calculi (examples indicated by red overlay) and sludge. In addition, the common bile duct (green overlay) is slightly dilated.
The passage of a gallbladder calculus through the common bile duct can result in acute pancreatitis.
A: aorta; Vc: ascending vena cava; L: liver; Sp: spleen; Red arrow: hepatic artery; Green outline: stomach
Source: © IMPP
CT abdomen (with contrast; axial plane)
Well-demarcated nonenhancing low attenuation areas of walled-off parenchymal necrosis (green overlay) are visible throughout the pancreas. Incidentally noted very low attenuation lesions in the kidneys (K) are cysts.
L = liver
Source: “Fig. 1B, in: Open necrosectomy is feasible as a last resort in selected cases with infected pancreatic necrosis: a case series and systematic literature review” by Lucia Ilaria Sgaramella, Angela Gurrado, Alessandro Pasculli, Francesco Paolo Prete, Fausto Catena & Mario Testini, BMC World Journal of Emergency Medicine, licensed under CC BY 4.0. Modifications: Image is cropped, letter "B" is removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
X-ray abdomen (AP; supine) of an adolescent with acute hepatopancreatitis
A short segment of adynamic ileus (sentinel loop sign, white arrows) is seen in the left upper quadrant.
Identification of a sentinel loop can be helpful in localizing inflammation in the abdomen.
Source: “Fig 2, In: A Rare Cause of Acute Hepatopancreatitis in a Nepalese Teen” by Swastika Adhikari, Ashish Lal Shrestha , Sanjay Raj Thapa, Amrit Ghimire, Hindawi, licensed under CC BY 4.0. Modifications: removal of the lower arrow indicating colon cut-off sign. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (with contrast; axial plane)
Multiple coarse calcifications (examples indicated by black arrowheads) in the pancreatic parenchyma are diagnostic of chronic pancreatitis. The pancreatic head also contains a hypodense structure (green overlay) that could represent a duct or small mass. A cholecystectomy clip is seen (red overlay).
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
CT abdomen (with contrast; axial plane)
An enlarged heterogeneous pancreatic head (green overlay) contains multiple calcifications, which is characteristic of chronic pancreatitis. Peripancreatic inflammatory fatty stranding (red overlay) is also seen.
Incidental findings include a small hypodense cyst (yellow overlay) in the dorsal parenchyma of the left kidney and atherosclerotic vascular calcifications (blue overlay). Intravenous contrast is seen in the liver (L), and oral contrast is seen in the bowel loops (indicated by arrows).
Source: © IMPP

Ultrasound abdomen of a patient with a history of pancreatitis
Targeted image shows a rounded, predominantly anechoic lesion (green overlay) with a few internal echoes and posterior acoustic enhancement (yellow overlay). Adjacent pancreas (P) tissue is visible.
P: pancreas
Source: © IMPP

CT abdomen (IV and oral contrast; axial section) of a patient with a history of pancreatic necrosis
A well-defined, complicated collection (solid outline) containing gas (examples indicated by arrows) is seen in the region of the pancreatic body and tail. Abdominal ascites (hatched overlay) and inflammatory fatty and fascial stranding are present in the right upper quadrant.
L: liver; G: gallbladder; CBD: common bile duct; A: abdominal aorta; K: kidney; V: vertebra
Source: © IMPP
Complications
Necrotizing pancreatitis [15]
- Definition: necrosis of pancreatic and peripancreatic tissue
- Clinical features: fever, persistent tachycardia, or insufficient symptomatic improvement over several days
- Diagnostics: nonenhancing areas of pancreatic parenchyma on CECT abdomen [9]
-
Treatment [15]
- Sterile necrotizing pancreatitis can usually be managed conservatively. [7]
- Encourage enteral nutrition if feasible.
- Provide supplemental nutritional support as needed.
Infected necrotizing pancreatitis [15]
- Definition: bacterial superinfection of necrotic pancreatic parenchyma
- Clinical features: similar to those of necrotizing pancreatitis
-
Diagnostics
- Laboratory studies: persistent or worsening leukocytosis, bacteremia, increasing inflammatory markers [15]
- CECT abdomen: gas within the pancreas and/or peripancreatic tissue or fluid collections [6]
- Fine-needle aspiration of necrotic areas: not routinely recommended [4][7][11]
-
Treatment [15]
- Supportive care: fluid therapy, analgesics, nutritional support
- Broad-spectrum empiric antibiotics with good tissue penetration (e.g., carbapenems , quinolones, third- or higher-generation cephalosporins, metronidazole) for 2–4 weeks [4][15]
- Drainage of infected material if there is clinical deterioration or persistence of symptoms despite antibiotic therapy
- Operative pancreatic debridement (necrosectomy) should ideally be performed at least 2–4 weeks after initial presentation. [4][15]
- Minimally invasive procedures (e.g., image-guided percutaneous drainage) can be performed in the first 2 weeks in seriously ill patients.
- Prognosis: high mortality rate (30%) [15]
Walled-off necrosis
-
Definition
- An encapsulated collection of sterile necrotic material, usually occurring > 4 weeks after the onset of necrotizing pancreatitis [6]
- Previously known as pancreatic abscess
- Diagnostics: CT abdomen with IV contrast showing an encapsulated heterogeneous collection containing fluid and debris [9]
- Treatment: (of symptomatic walled-off necrosis): percutaneous drainage or transmural endoscopic necrosectomy [15]
Other localized complications [53][54]
- Pancreatic pseudocyst
- Abdominal compartment syndrome
- Splenic vein thrombosis
- Pancreatic hemorrhage (blood vessel erosion with bleeding)
Systemic complications [55]
- Shock, SIRS, sepsis, DIC
- Pneumonia, respiratory failure, ARDS [55]
- Pleural effusion
- Prerenal failure due to volume depletion
- Hypocalcemia
- Paralytic ileus
- Pancreatic ascites
We list the most important complications. The selection is not exhaustive.
CT abdomen (with contrast; axial plane)
Well-demarcated nonenhancing low attenuation areas of walled-off parenchymal necrosis (green overlay) are visible throughout the pancreas. Incidentally noted very low attenuation lesions in the kidneys (K) are cysts.
L = liver
Source: “Fig. 1B, in: Open necrosectomy is feasible as a last resort in selected cases with infected pancreatic necrosis: a case series and systematic literature review” by Lucia Ilaria Sgaramella, Angela Gurrado, Alessandro Pasculli, Francesco Paolo Prete, Fausto Catena & Mario Testini, BMC World Journal of Emergency Medicine, licensed under CC BY 4.0. Modifications: Image is cropped, letter "B" is removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
CT abdomen (IV and oral contrast; axial section) of a patient with a history of pancreatic necrosis
A well-defined, complicated collection (solid outline) containing gas (examples indicated by arrows) is seen in the region of the pancreatic body and tail. Abdominal ascites (hatched overlay) and inflammatory fatty and fascial stranding are present in the right upper quadrant.
L: liver; G: gallbladder; CBD: common bile duct; A: abdominal aorta; K: kidney; V: vertebra
Source: © IMPP
Ultrasound abdomen of a patient with a history of pancreatitis
Targeted image shows a rounded, predominantly anechoic lesion (green overlay) with a few internal echoes and posterior acoustic enhancement (yellow overlay). Adjacent pancreas (P) tissue is visible.
P: pancreas
Source: © IMPP
Prognosis
-
Mortality
- In patients without organ failure: < 1%
- In patients with organ failure: ∼ 30%
- Higher mortality in patients with biliary pancreatitis than in patients with alcohol-induced pancreatitis
- Risk factors for severe disease: See “Severity scores for acute pancreatitis.” [4][56]
References:[10][57][58]
External Resources
- 2024 American College of Gastroenterology: Management of Acute Pancreatitis
- 2020 American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis
- 2019 American College of Radiology Appropriateness Criteria: Acute Pancreatitis
- 2018 American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis
References
- Nesvaderani M, Eslick GD, Vagg D, Faraj S, Cox MR. "Epidemiology, aetiology and outcomes of acute pancreatitis: A retrospective cohort study". International Journal of Surgery. 23. :68-74. (2015)
- Teich N, Rosendahl J, Tóth M, Mössner J, Sahin-Tóth M. "Mutations of human cationic trypsinogen (PRSS1) and chronic pancreatitis". Hum Mutat. 27(8). :721-730. (2006)
- Ahmed A, Azim A, Gurjar M, Baronia A. "Hypocalcemia in acute pancreatitis revisited". Indian J Crit Care Med. 20(3). :173. (2016)
- Tenner S, Vege SS, Sheth SG, et al. "American College of Gastroenterology Guidelines: Management of Acute Pancreatitis". Am J Gastroenterol. 119(3). :419-437. (2023)
- Crockett et al. "American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis". Gastroenterology. 154(4). :1096-1101. (2018)
- Banks, et al. "Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus". Gut. 62(1). :102-111. (2012)
- Working Group IAP/APA Acute Pancreatitis Guidelines. "IAP/APA evidence-based guidelines for the management of acute pancreatitis". Pancreatology. 13(4). :e1-e15. (2013)
- D Jeffrey. "Acute Pancreatitis". AAFP. (2014)
- "ACR Appropriateness Criteria: Acute Pancreatitis". https://acsearch.acr.org/docs/69468/Narrative/. [2019-11-01]
- Meher S, Mishra TS, Sasmal PK, et al. "Role of Biomarkers in Diagnosis and Prognostic Evaluation of Acute Pancreatitis". J Biomark. 2015. (2015)
- Leppäniemi A, et al. "2019 WSES guidelines for the management of severe acute pancreatitis". World Journal of Emergency Surgery. 14(1). (2019)
- Aggarwal A. "Fluid resuscitation in acute pancreatitis". World J Gastroenterol. 20(48). :18092. (2014)
- Evans RP, Mourad MM, Pall G, Fisher SG, Bramhall SR. "Pancreatitis: Preventing catastrophic haemorrhage". World J Gastroenterol. 23(30). :5460. (2017)
- Fan BG, Andrén-Sandberg A. "Acute pancreatitis". N Am J Med Sci. 2(5). :211-4. (2010)
- Baron TH, DiMaio CJ, et al. "American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis". Gastroenterology. 158(1). :67-75.e1. (2020)
- Jabłońska B, Mrowiec S. "Nutritional Support in Patients with Severe Acute Pancreatitis-Current Standards". Nutrients. 13(5). :1498. (2021)
- Martin KJ, González EA, Slatopolsky E. "Clinical Consequences and Management of Hypomagnesemia". Journal of the American Society of Nephrology. 20(11). :2291-2295. (2008)
- Diallo I, Fall CA, et al. "Primary Hyperparathyroidism and Pancreatitis: A Rare Association with Multiple Facets". Int Sch Res Notices. 2016. :1-4. (2016)
- Kwo PY, Cohen SM, Lim JK. "ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries". Am J Gastroenterol. 112(1). :18-35. (2017)
- Güngör B, Caglayan K, et al. "The Predictivity of Serum Biochemical Markers in Acute Biliary Pancreatitis". ISRN Gastroenterol. 2011. :1-5. (2011)
- Frossard JL, Hadengue A, et al. "New Serum Markers for the Detection of Severe Acute Pancreatitis in Humans". Am J Respir Crit Care Med. 164(1). :162-170. (2001)
- Mandalia A, Wamsteker E-J, et al. "Recent advances in understanding and managing acute pancreatitis". F1000Res. 7. :959. (2019)
- Dupuis CS, Baptista V, Whalen G, et al. "Diagnosis and management of acute pancreatitis and its complications". Gastrointest Interv. 2(1). :36-46. (2013)
- Garg R, Rustagi T. "Management of Hypertriglyceridemia Induced Acute Pancreatitis". BioMed Research International. 2018. :1-12. (2018)
- Tse F, Yuan Y. "Early routine endoscopic retrograde cholangiopancreatography strategy versus early conservative management strategy in acute gallstone pancreatitis". Cochrane Database Syst Rev. (2012)
- Munoz A. "Diagnosis and management of acute pancreatitis". Am Fam Physician. 62(1). :164-174. (2000)
- Koizumi M, Takada T, et al. "JPN Guidelines for the management of acute pancreatitis: diagnostic criteria for acute pancreatitis". J Hepatobiliary Pancreat Surg. 13(1). :25-32. (2006)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Schrum A. "Colon-Cut-off-Sign in the CT- Scanogram – Evidence of Pancreatitis?". J Clin Diagn Res. (2015)
- Jonathan P. Terdiman, Claudia B. Gruss, Joel J. Heidelbaugh, Shahnaz Sultan, Yngve T. Falck–Ytter. "American Gastroenterological Association Institute Guideline on the Use of Thiopurines, Methotrexate, and Anti–TNF-α Biologic Drugs for the Induction and Maintenance of Remission in Inflammatory Crohn's Disease". Gastroenterology. 145(6). :1459-1463. (2013)
- Pereira R, Eslick G, et al. "Endoscopic Ultrasound for Routine Assessment in Idiopathic Acute Pancreatitis". J Gastrointest Surg. 23(8). :1694-1700. (2019)
- de-Madaria E, Buxbaum JL, Maisonneuve P, et al. "Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis". N Engl J Med. 387(11). :989-1000. (2022)
- Levy MM, Evans LE, Rhodes A. "The Surviving Sepsis Campaign Bundle: 2018 update". Intensive Care Med. 44(6). :925-928. (2018)
- James TW, Crockett SD. "Management of acute pancreatitis in the first 72 hours". Curr Opin Gastroenterol. 34(5). :330-335. (2018)
- Pandanaboyana S, Huang W, Windsor JA, Drewes AM. "Update on pain management in acute pancreatitis". Curr Opin Gastroenterol. 38(5). :487-494. (2022)
- Nelson A, Lugo-Fagundo NS, Mahapatra S, et al. "A Systematic Review and Meta-analysis of Opioids vs Non-Opioids in Acute Pancreatitis". Am J Gastroenterol. 116(1). :S38-S39. (2021)
- Banks PA, Conwell DL, et al. "The management of acute and chronic pancreatitis". Gastroenterol Hepatol (N Y). 6(2 Suppl 3). :1-16. (2010)
- Basurto Ona et al. "Opioids for acute pancreatitis pain". Cochrane Database of Systematic Reviews. (2013)
- Pothoulakis I, Nawaz H, Paragomi P, et al. "Incidence and risk factors of oral feeding intolerance in acute pancreatitis: Results from an international, multicenter, prospective cohort study". United European Gastroenterol J. 9(1). :54-62. (2021)
- Dutta AK, Goel A, et al. "Nasogastric versus nasojejunal tube feeding for severe acute pancreatitis". Cochrane Database Syst Rev. (2020)
- Oláh A, Jr LR. "Enteral nutrition in acute pancreatitis: A review of the current evidence". World J Gastroenterol. 20(43). :16123. (2014)
- Gurusamy KS, Davidson BR. "Early versus delayed laparoscopic cholecystectomy for acute gallstone pancreatitis". Cochrane Database Syst Rev. (2013)
- Baj J, Flieger W, Teresiński G, et al. "Magnesium, Calcium, Potassium, Sodium, Phosphorus, Selenium, Zinc, and Chromium Levels in Alcohol Use Disorder: A Review". J Clin Med. 9(6). :1901. (2020)
- "Pancreatic pseudocyst". https://medlineplus.gov/ency/article/000272.htm. [2019-10-16]
- Barry K. "Chronic Pancreatitis: Diagnosis and Treatment". Am Fam Physician. 97(6). :385-393. (2018)
- Browne GW. "Pathophysiology of pulmonary complications of acute pancreatitis". World J Gastroenterol. 12(44). :7087. (2006)
- Vege SS, DiMagno MJ, Forsmark CE, Martel M, Barkun AN. "Initial Medical Treatment of Acute Pancreatitis: American Gastroenterological Association Institute Technical Review". Gastroenterology. 154(4). :1103-1139. (2018)
- Carroll JK, Herrick B, Gipson T. "Acute Pancreatitis: Diagnosis, Prognosis, and Treatment". Am Fam Physician. 75(10). :1513-1520. (2007)
- Mofidi R, Patil PV, Suttie SA, Parks RW. "Risk assessment in acute pancreatitis". Br J Surg. 96(2). :137-150. (2009)
- Bollen TL, Singh VK, et al. "Comparative Evaluation of the Modified CT Severity Index and CT Severity Index in Assessing Severity of Acute Pancreatitis". AJR Am J Roentgenol. 197(2). :386-392. (2011)
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. "Acute pancreatitis: value of CT in establishing prognosis". Radiology. 174(2). :331-336. (1990)
- Mortele KJ, Wiesner W, Intriere L, et al. "A modified CT severity index for evaluating acute pancreatitis: improved correlation with patient outcome". AJR Am J Roentgenol. 183(5). :1261-5. (2004)
- Khanna AK, Meher S, et al. "Comparison of Ranson, Glasgow, MOSS, SIRS, BISAP, APACHE-II, CTSI Scores, IL-6, CRP, and Procalcitonin in Predicting Severity, Organ Failure, Pancreatic Necrosis, and Mortality in Acute Pancreatitis". HPB Surg. 2013. :1-10. (2013)
- Benjamin O, Lappin SL. "Chronic Pancreatitis". StatPearls. (2020)
- Ducarme G, Maire F, Chatel P, Luton D, Hammel P. "Acute pancreatitis during pregnancy: a review". Journal of Perinatology. 34(2). :87-94. (2013)
- Abu‐El‐Haija M, Kumar S, Quiros JA, et al. "Management of Acute Pancreatitis in the Pediatric Population". J Pediatr Gastroenterol Nutr. 66(1). :159-176. (2018)
- Párniczky A, Abu-El-Haija M, Husain S, et al. "EPC/HPSG evidence-based guidelines for the management of pediatric pancreatitis". Pancreatology. 18(2). :146-160. (2018)
- Uc A, Husain SZ. "Pancreatitis in Children". Gastroenterology. 156(7). :1969-1978. (2019)
- Foster BR, Jensen KK, Bakis G, Shaaban AM, Coakley FV. "Revised Atlanta Classification for Acute Pancreatitis: A Pictorial Essay". RadioGraphics. 36(3). :675-687. (2016)
- Baillie J. "AGA Institute Medical Position Statement on Acute Pancreatitis". Gastroenterology. 132(5). :2019-2021. (2007)
- Mikhail N, et al. "Treatment of severe hypertriglyceridemia in nondiabetic patients with insulin". The American Journal of Emergency Medicine. 23(3). :415-417. (2005)
- Carroll MF, Schade DS. "A practical approach to hypercalcemia.". Am Fam Physician. 67(9). :1959-66. (2003)
- Rao SA, Kunte AR. "Interleukin-6: An Early Predictive Marker for Severity of Acute Pancreatitis". Indian Journal of Critical Care Medicine. 21(7). :424-428. (2017)
- Cui J, et al. "Serum lactate dehydrogenase is predictive of persistent organ failure in acute pancreatitis". J Crit Care. 41. :161-165. (2017)
- Jenssen C, et al. "Endoscopic Ultrasound in Acute Pancreatitis". Video Journal and Encyclopedia of GI Endoscopy. 1(2). :554-559. (2013)