Summary
Acute respiratory distress syndrome (ARDS) is a severe inflammatory reaction of the lungs to pulmonary damage. While sepsis is the most common cause, a variety of systemic and pulmonary factors (e.g., pneumonia, aspiration) can lead to ARDS. Affected individuals initially present with acute-onset dyspnea, tachypnea, and cyanosis. The chief finding in ARDS is hypoxemic respiratory failure with decreased arterial oxygen pressure, which can progress to hypercapnic respiratory failure. Chest x-ray typically shows diffuse bilateral infiltrates. A defining feature of ARDS is a PaO2/FiO2 ratio ≤ 300 mm Hg. Management of ARDS is focused on maintaining adequate oxygenation, which often requires intubation and lung-protective mechanical ventilation. Glucocorticoids should be considered and any treatable causes of ARDS should be addressed. Even if adequate treatment is initiated, ARDS remains an acutely life-threatening disease with a high mortality rate. Most patients improve significantly in the weeks following the initial presentation, but some cases progress to pulmonary fibrosis, which prolongs hospital stays and delays the resolution of symptoms.
Definitions
ARDS is a clinical syndrome of acute respiratory failure characterized by hypoxemia and bilateral pulmonary infiltrates that cannot be fully accounted for by heart failure or fluid overload. See the “Global definition of ARDS.” [1]
Etiology
Systemic causes
- Sepsis (most common cause), e.g., secondary to trauma, infection, or peritonitis [2]
- Trauma
- Shock
- Massive transfusion (See “TRALI” for details)
- Acute pancreatitis
- Hematopoietic stem cell transplantation
- Medication (e.g., salicylic acid, tricyclic antidepressants, bleomycin) [3]
- Recreational drug overdose (e.g., cocaine)
- Major burns [4]
Primary damage to the lungs
- Pneumonia
- Aspiration
- Inhaled toxins
- Pulmonary contusion [5]
- Inhalation injury (e.g., inhalation of hyperbaric oxygen)
- Drowning incidents [6]
- Fat embolism (e.g., through blunt trauma)
- Amniotic fluid embolism (e.g., during labor)
- Lung transplantation
Sepsis is the most common cause of ARDS. [2]
Pathophysiology
-
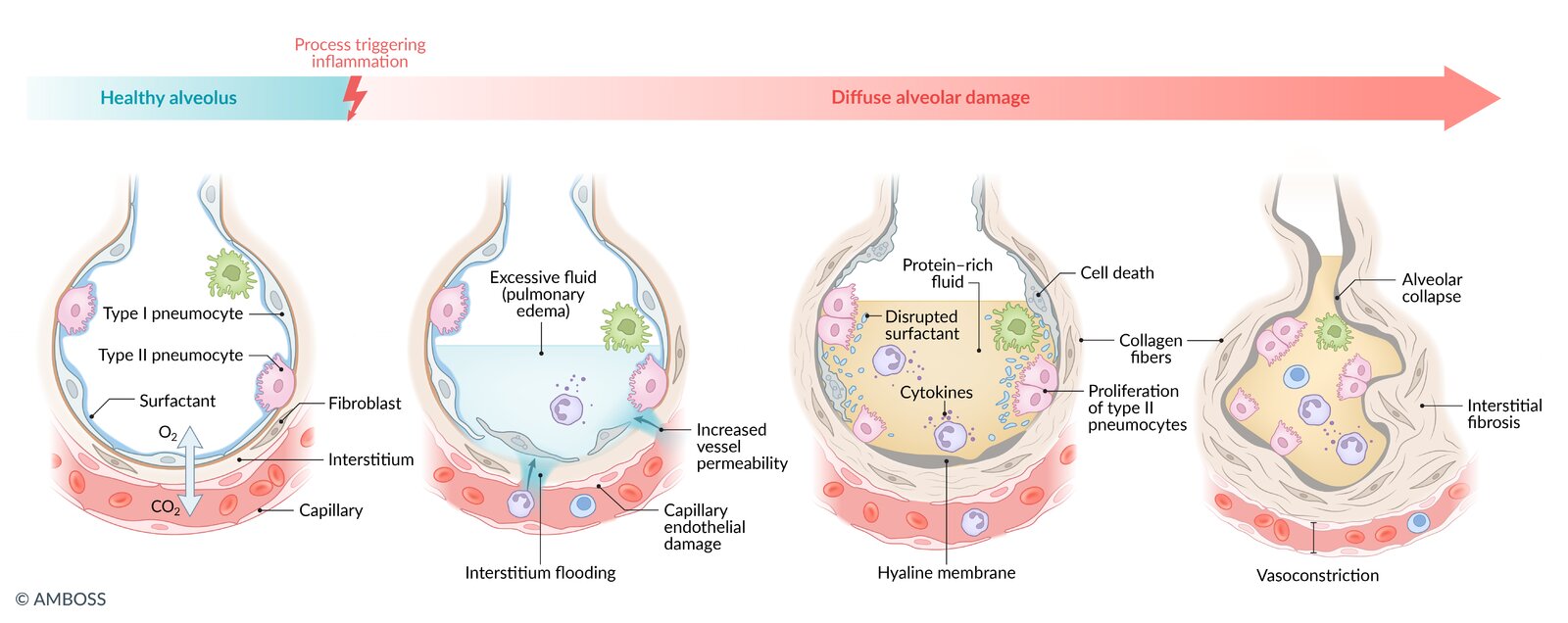
Tissue damage (pulmonary or extrapulmonary) → release of inflammatory mediators (e.g., interleukin-1) → inflammatory reaction → migration of neutrophils into alveoli → excessive release of neutrophilic mediators (e.g., cytokines, proteases, reactive oxygen species) → injury to alveolar capillaries and endothelial cells (diffuse alveolar damage, DAD) ; leading to: [7]
- Exudative phase: excess fluid in interstitium and on alveolar surface → pulmonary edema with normal pulmonary capillary wedge pressure (noncardiogenic pulmonary edema) → decreased lung compliance and respiratory distress
-
Hyaline membrane formation: exudation of neutrophils and protein-rich fluid into the alveolar space → formation of alveolar hyaline membranes → impaired gas exchange → hypoxemia
- Hypoxemia → compensation through hyperventilation → respiratory alkalosis
- Hypoxemia → chronic hypoxic pulmonary vasoconstriction → pulmonary hypertension and right-to-left pulmonary shunt (increased shunt fraction)
- Damage to type I and type II pneumocytes → decrease in surfactant → alveolar collapse → intrapulmonary shunting
- Organizing phase (late stage): proliferation of type II pneumocytes and infiltration of fibroblasts → progressive interstitial fibrosis
")

")
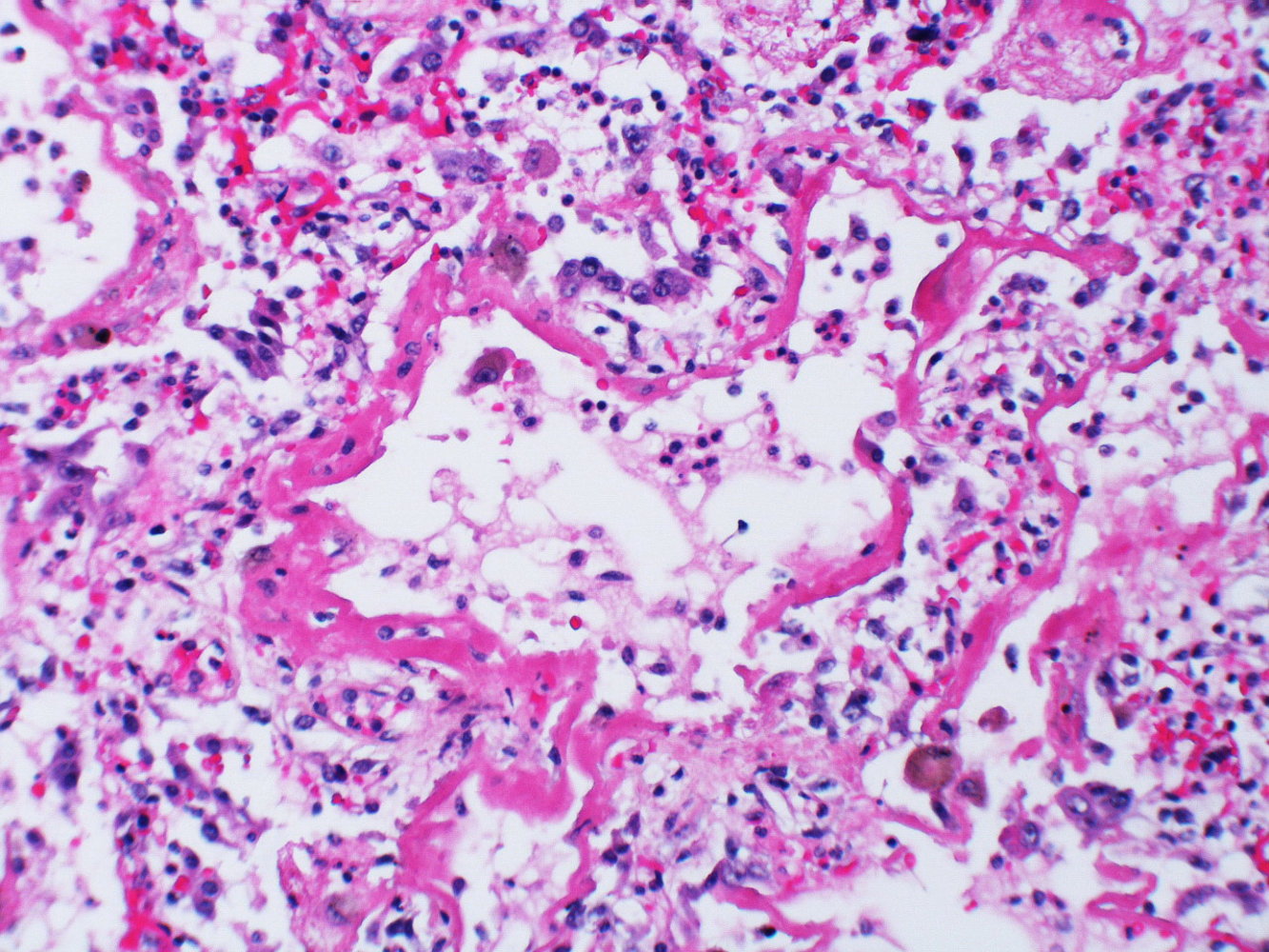
Photomicrograph of a lung biopsy specimen (H&E stain; medium power magnification)
An alveolus lined by a prominent hyaline membrane (green overlay) can be seen in the center of the image, containing numerous leukocytes (examples indicated by blue arrowheads) and erythrocytes (examples indicated by black arrowheads). The surrounding interstitium is edematous and interspersed with a dense inflammatory infiltrate (examples of inflammatory cells indicated by yellow arrowheads).
These findings are characteristic of the exudative phase of diffuse alveolar damage (DAD), which is the histopathological appearance of the acute exudative phase of acute respiratory distress syndrome (ARDS).
Source: “Diffuse alveolar damage (DAD)” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
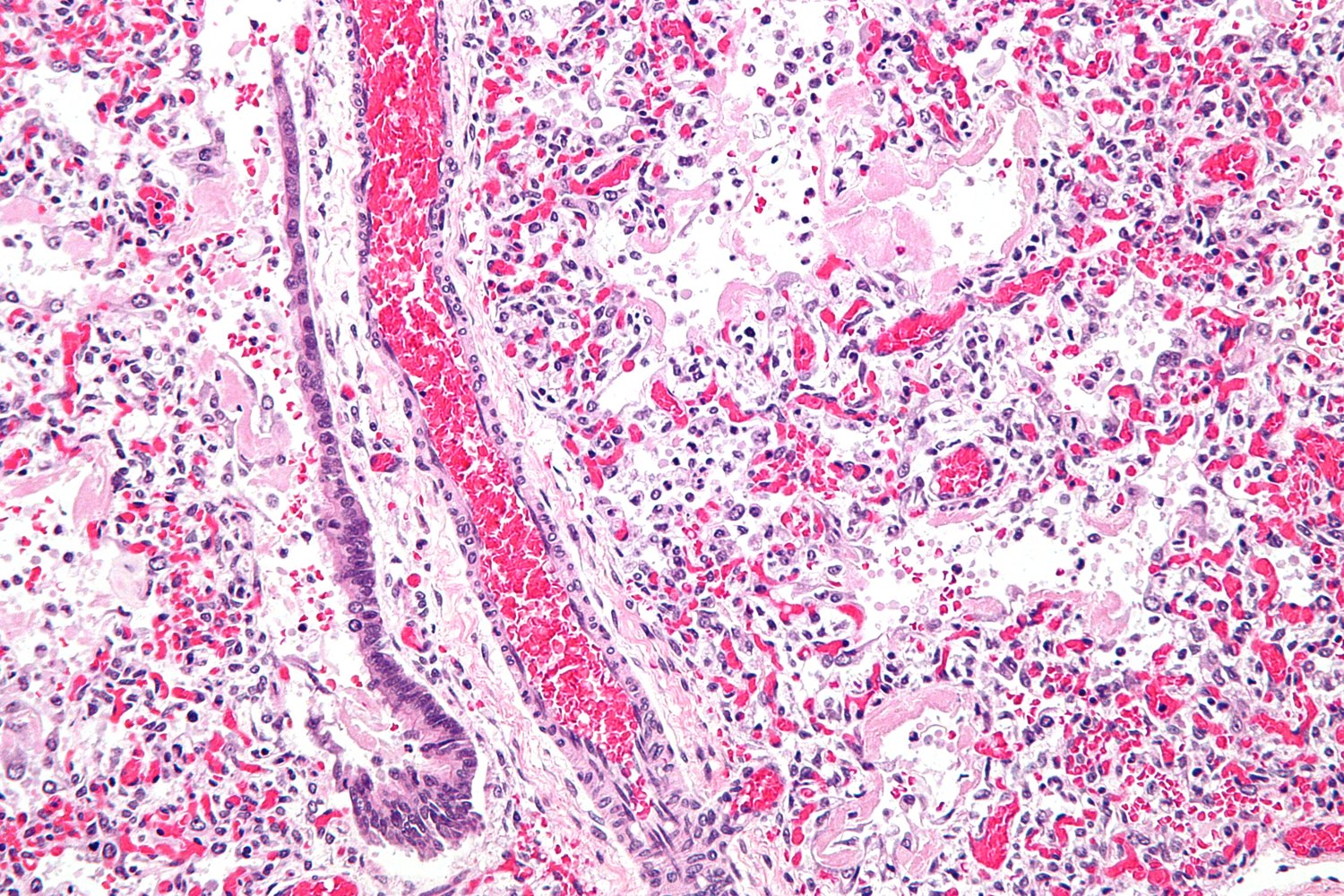
Photomicrograph of lung tissue (H&E stain; 400x magnification)
The alveolar walls are lined by eosinophilic hyaline membranes (example indicated by green overlay). The normal basophilic alveolar epithelial lining is absent. Within the interstitium, there is an extensive inflammatory infiltrate, which is visible as numerous basophilic nuclei (large basophilic nuclei: macrophages; multilobed nuclei: neutrophils). There are numerous microthrombi, visible as extracapillary aggregates of RBCs. The capillaries appear congested.
Loss of alveolar epithelium, presence of alveolar hyaline membranes, and interstitial inflammation, edema, and congestion are the typical features of the acute exudative phase of ARDS.
Source: “Hyaline membranes - intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
© AMBOSS
Clinical features
- Acute dyspnea
- Tachypnea and tachycardia
- Cyanosis
- Diffuse crackles
- Fever, cough, and chest pain may also be present.
Diagnosis
Approach [4][8]
ARDS is a diagnosis of exclusion.
- Consider ARDS in patients with acute-onset respiratory failure and a potential trigger.
- Order chest x-ray to evaluate for bilateral infiltrates.
- Perform ABG analysis and calculate the PaO2/FiO2 ratio to confirm the diagnosis and assess severity.
- Consider additional testing (e.g., CT chest, echocardiography, and BNP) to:
- Identify triggers
- Rule out differential diagnoses
- Assess for complications
Global definition of ARDS [1]
The Global definition of ARDS requires the presence of all of the following:
-
Acute-onset respiratory failure
- Within one week of a confirmed trigger (e.g., sepsis, pneumonia) and/or of worsening respiratory symptoms
- Cannot be fully accounted for by heart failure or fluid overload
-
Bilateral opacities on chest x-ray, CT, or ultrasound
- Similar appearance to pulmonary edema
- Findings cannot be fully attributed to pleural effusions, lobar or lung collapse, and/or nodules
-
Hypoxemia
- Measurements
- PaO2/FiO2≤ 300 mm Hg (preferred)
- SpO2/FiO2≤ 315 mm Hg if SpO2 is ≤ 97% (alternative if ABG is not available)
- Severity categories (intubated ARDS only)
- Mild ARDS: PaO2/FiO2201–300 mm Hg and/or SpO2/FiO2235–315 mm Hg
- Moderate ARDS: PaO2/FiO2101–200 mm Hg and/or SpO2/FiO2148–235 mm Hg
- Severe ARDS: PaO2/FiO2≤ 100 mm Hg and/or SpO2/FiO2≤ 148 mm Hg
- Measurements
-
Respiratory support required
- Intubated ARDS
- Nonintubated ARDS
- NIPPV or CPAP with ≥ 5 cm H2O PEEP [1]
- High-flow nasal cannula oxygen therapy (HFNC) with a flow of ≥ 30 L/minute
ARDS diagnostic criteria include: Abnormal x-ray, Respiratory failure < 1 week after a known or suspected trigger, Decreased PaO2/FiO2, Support required for respiration.
In resource-limited settings, ARDS may be diagnosed in patients who are not currently receiving respiratory support but meet the other three criteria. [1]
Imaging
Chest x-ray is usually sufficient for diagnosis. However, distinguishing between ARDS and CHF can be challenging. In these cases, correlation with other tests (e.g., CT chest, lung ultrasound, echocardiogram) may be useful.
Chest x-ray [9][10]
- Indications: all patients suspected of having ARDS
-
Acute findings (1–7 days)
- Often normal in the first 24 hours
- Diffuse bilateral symmetrical infiltrates
- In severe cases: bilateral attenuations that make the lung appear white on x-ray (“white lung”)
- Air bronchograms may be visible.
-
Intermediate (8–14 days) to late (> 15 days) findings
- Typical course: Acute features remain stable, then resolve.
- Fibrotic course: Reticular opacities begin to appear and may become permanent.
-
Findings supportive of ARDS rather than CHF
- Predominantly peripheral opacities
- Small or absent pleural effusions
- No cardiomegaly or septal lines








CT chest without contrast [9][10][11]
- Indications: may be used if chest x-ray findings are insufficient or to further investigate for underlying causes or complications
-
Acute findings (1–7 days)
- Symmetrical ground-glass opacities are the most important finding.
- Gravity-dependent density gradient
- The lungs may appear normal in nondependent regions.
- Dense consolidation in dependent regions
- Bronchial dilatation may be visible.
- Additional findings may include small pleural effusions, air bronchograms (see “Chest x-ray” above).
-
Intermediate (8–14 days) to late (> 15 days) findings: a phase of stability is followed either by resolution or progressive development of fibrosis
- Mixed findings may be seen.
- Potential long-term persistence of ground-glass opacities
- Cysts and bullae may develop.
")
Lung ultrasound [1][11]
- Indications: may be helpful in differentiating between cardiogenic pulmonary edema and ARDS
-
Key findings
- Bilateral B pattern
- C pattern (consolidation)
- Abnormal pleural line (thickening, irregular pattern, and/or alterations in lung sliding)

Laboratory studies [11]
-
Arterial blood gas
-
Hypoxemic respiratory failure (↓ PaO2) and, initially, respiratory alkalosis (↑ pH)
- PaO2/FiO2 ≤ 300 mm Hg
- Increased A-a gradient
- With disease progression, hypercapnic respiratory failure (↑ PaCO2; ↓ pH) may develop due to respiratory exhaustion.
-
Hypoxemic respiratory failure (↓ PaO2) and, initially, respiratory alkalosis (↑ pH)
-
Additional laboratory studies to consider
-
Underlying causes/triggers
- CBC: leukocytosis in sepsis or pneumonia
- Lipase: elevated in pancreatitis
- Blood cultures: to identify bacteremia
- Sputum gram stain and culture: to identify bacterial pneumonia
- Advanced tests: urine antigen testing, serologic tests (see “Diagnostics” in pneumonia)
- Differential diagnoses
- BNP: to evaluate for heart failure [10]
- D-dimer: to evaluate for pulmonary embolism (in patients with low to moderate pretest probability of PE)
- Troponin: to evaluate for cardiac ischemia
- Complications; see also:
- Diagnosis of AKI
- Diagnosis of sepsis
- Diagnosis of DIC
-
Underlying causes/triggers
Additional diagnostic studies [11]
- ECG: Signs of STEMI, LVH, or cardiac arrhythmias may indicate CHF.
- Echocardiography: to exclude or assess the degree of heart failure [10]
-
Bronchoscopy with bronchoalveolar lavage (BAL) [11]
- Useful for infections that are hard to diagnose, inflammatory disease (e.g., vasculitis), and cancer
- BAL samples can be tested with Giemsa/Gram staining as well as specialized cultures for intracellular bacteria, viruses, and fungi.
-
Right heart catheterization
- To exclude CHF in the absence of any risk factors
- PCWP > 18 mm Hg is considered to confirm the presence of cardiac insufficiency. [10]
-
Lung biopsy: consider in rare cases [11]
- To evaluate the stage of lung fibrosis after a prolonged ARDS course and decide whether treatment with steroids may be indicated [11]
- Indicated if other studies (e.g., BAL, blood cultures) are inconclusive
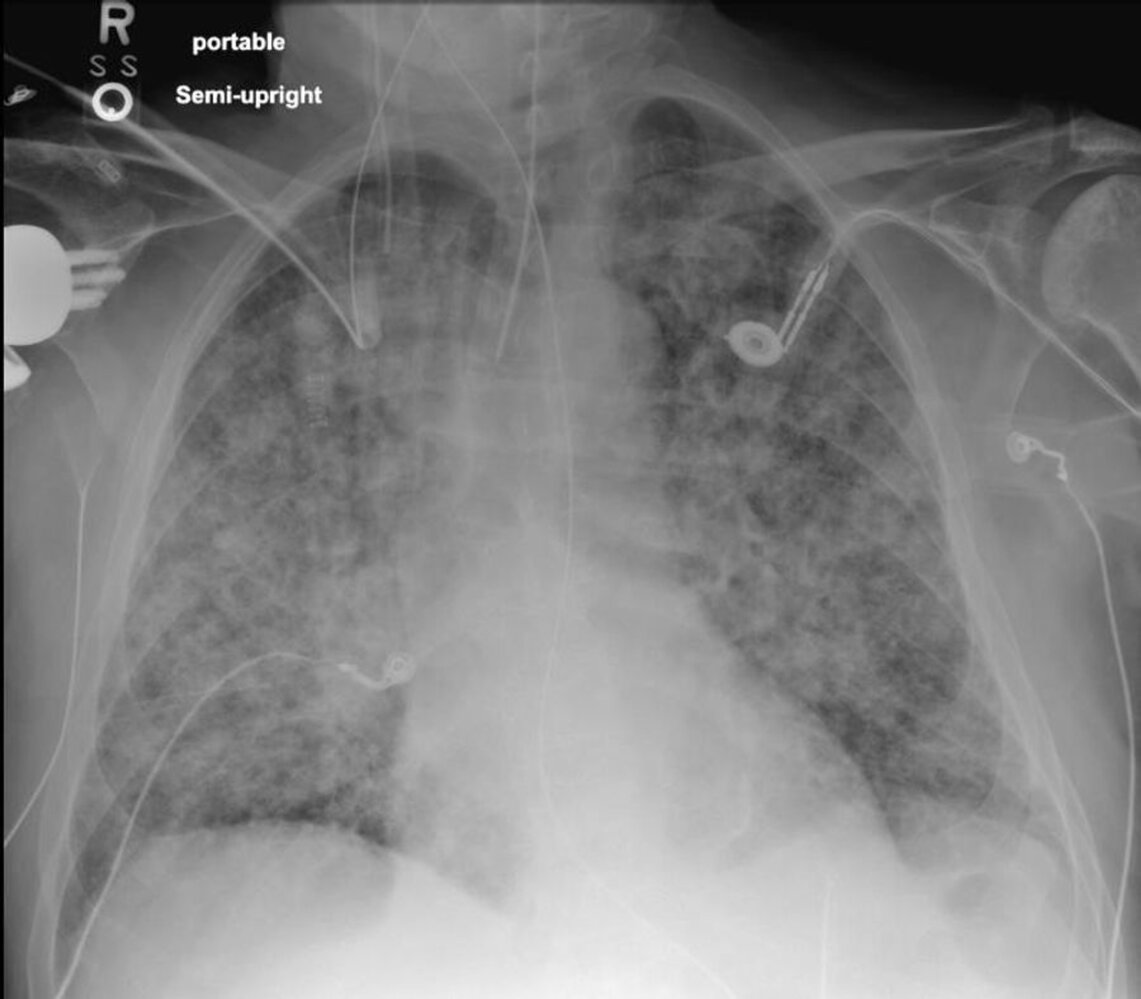
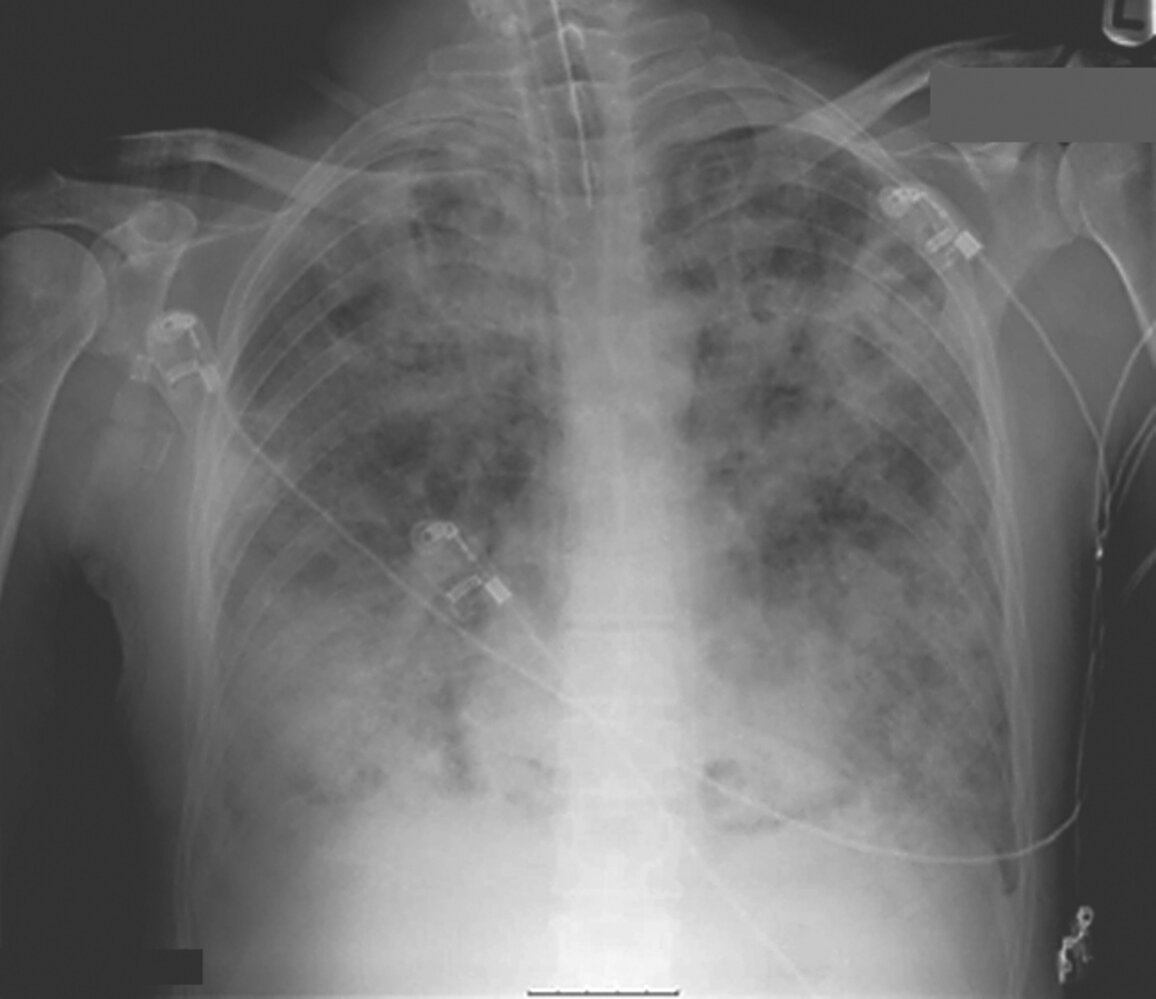
X-ray chest (AP portable view; semierect position) of a patient whose respiratory status acutely deteriorated 48 hrs after hospitalization for blastomycosis pneumonia
Poorly marginated opacities are present throughout both lungs, with relative sparing of the lung bases along the diaphragms (examples indicated by arrowheads). Features common in cardiogenic edema, such as septal thickening, perihilar and gravitational dependence, cardiac silhouette enlargement, and vascular pedicle widening) are notably lacking. Nasogastric (red overlay) and endotracheal tubes (green overlay) are present.
The radiographic appearance is consistent with noncardiogenic edema and compatible with the clinical diagnosis of ARDS.
Source: “Fig. 2, in: Blastomycosis-Induced Acute Respiratory Distress Syndrome” by Ajmal M, Aftab Khan Lodhi F, Nawaz G, et al., Cureus, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

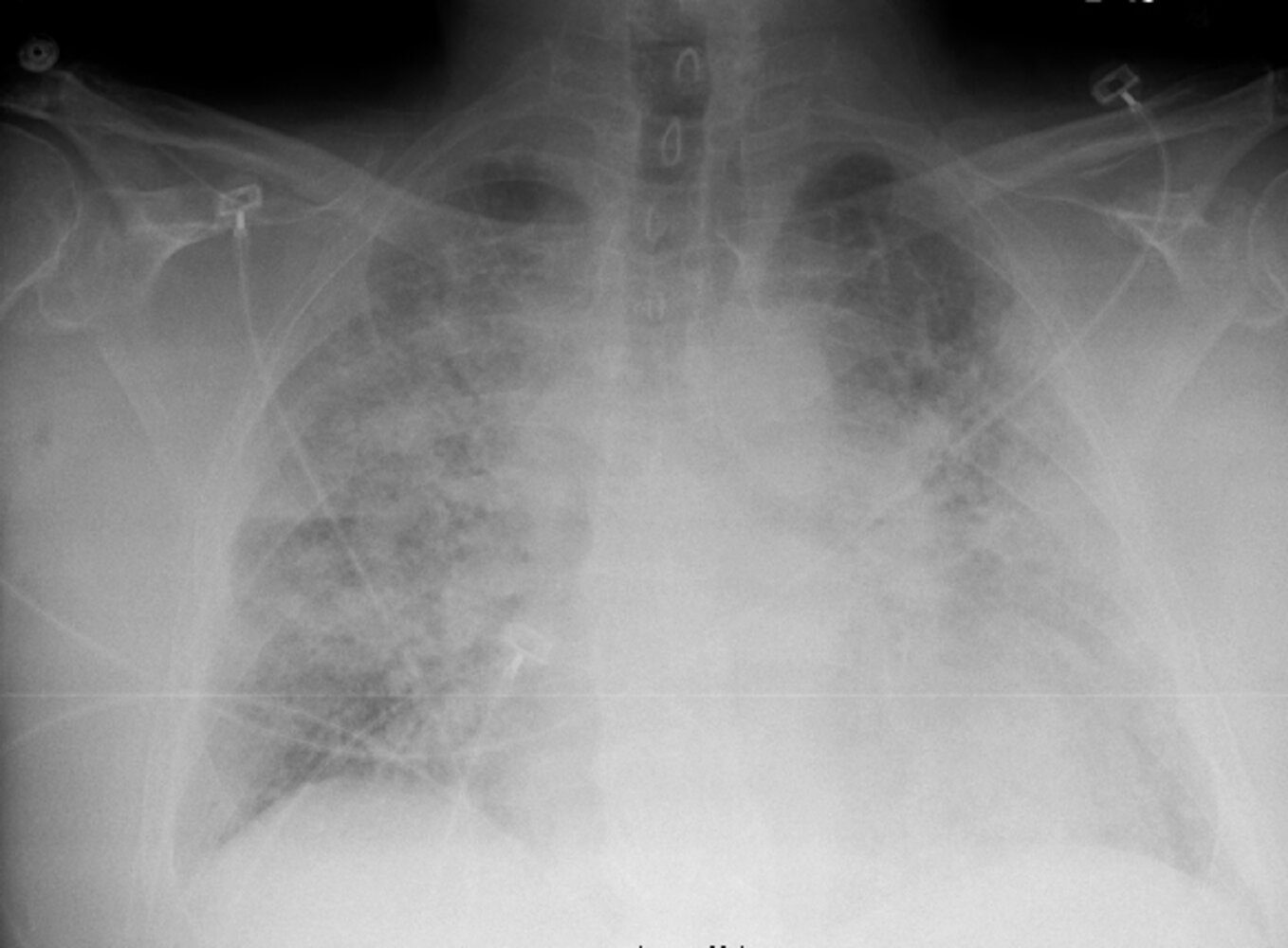
X-ray chest (AP view) of a patient with acute respiratory distress syndrome (ARDS)
Confluent and multifocal airspace opacities (examples indicated by green overlay) predominate in the lower zones of the lungs. Air bronchograms (examples indicated by red lines) are visible in some locations. There are no Kerley lines or pleural effusions. The cardiac silhouette size is normal. An endotracheal tube (arrow) is present.
ARDS and other causes of noncardiogenic edema can produce extensive airspace opacification, as can cardiogenic edema, diffuse pneumonia, diffuse alveolar hemorrhage, pneumonic-type adenocarcinoma, and pulmonary alveolar proteinosis. Radiography alone cannot establish a diagnosis of ARDS.
Source: "Chest Xray 40 yr old male acute respiratory distress syndrome as a complication of murine typhus. 13-1421-F1", Thomas W. van der Vaart et al., Centers for Disease Control and Prevention licensed under Public Domain
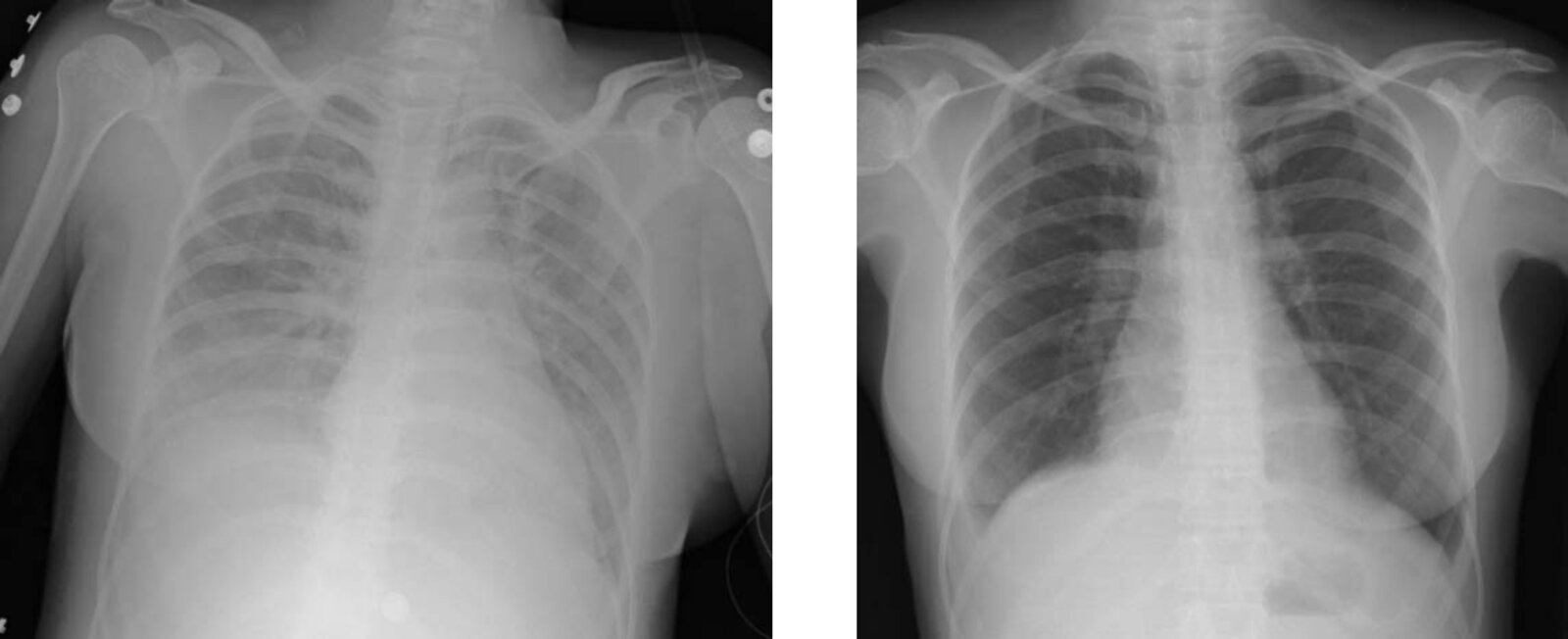
X-ray chest (AP view; left: one hour after transfusion; right: 72 hours after transfusion)
Diffuse opacification of the lungs (red overlay) correlated with clinical features of transfusion-related acute lung injury (TRALI). Improvement (right image) followed ventilator support; however, the presence of a pleural effusion (green overlay) raised the possibility of concomitant transfusion-associated circulatory overload (TACO). The costophrenic angle has been displaced (green line) from its normal position (white dashed line).
Source: “Figure 1, in: Transfusion related acute lung injury presenting with acute dyspnoea: a case report” by Altaf Gauhar Haji, Shekhar Sharma, D. K. Vijaykumar & Jerry Paul, Journal of Medical Case Reports, licensed under CC BY 2.0. Modifications: cropped image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.

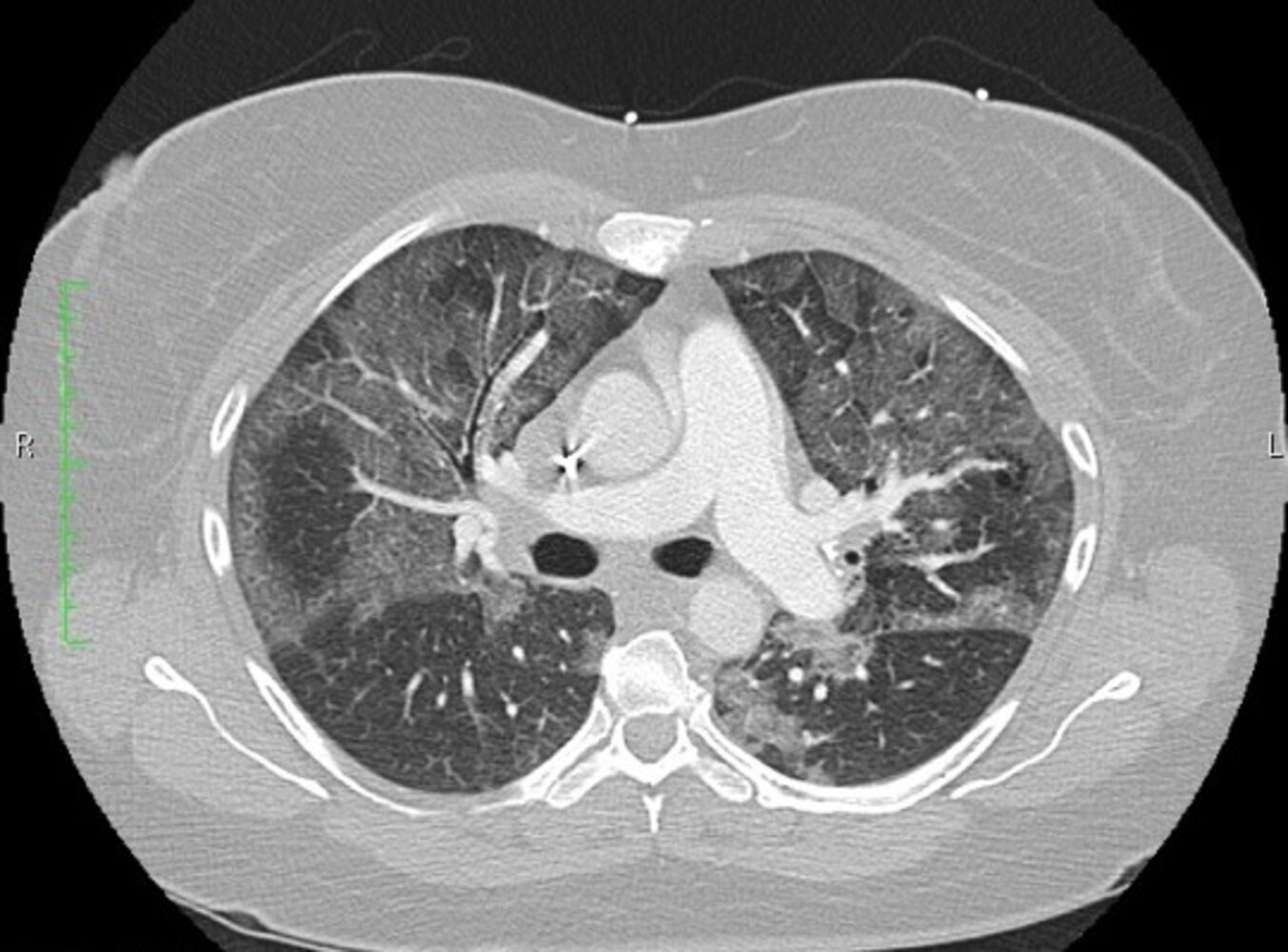
CT Thorax (axial-plane, lung window, with contrast) of a patient with dyspnea and a dry cough.
Bilateral symmetric, patchy and hazy opacification (yellow overlay) is demonstrated within the lungs. The bronchial and vascular markings are still visible in the affected areas, indicating a ground-glass type of opacification. This represents partial filling of the airspaces with substances such as fluid.
This is an example of acute respiratory distress syndrome. Symmetric bilateral ground-glass opacification is a non-specific finding and is demonstrated in a variety of other conditions such as pulmonary edema. The appearances on this study require clinical correlation to help narrow down the differential.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
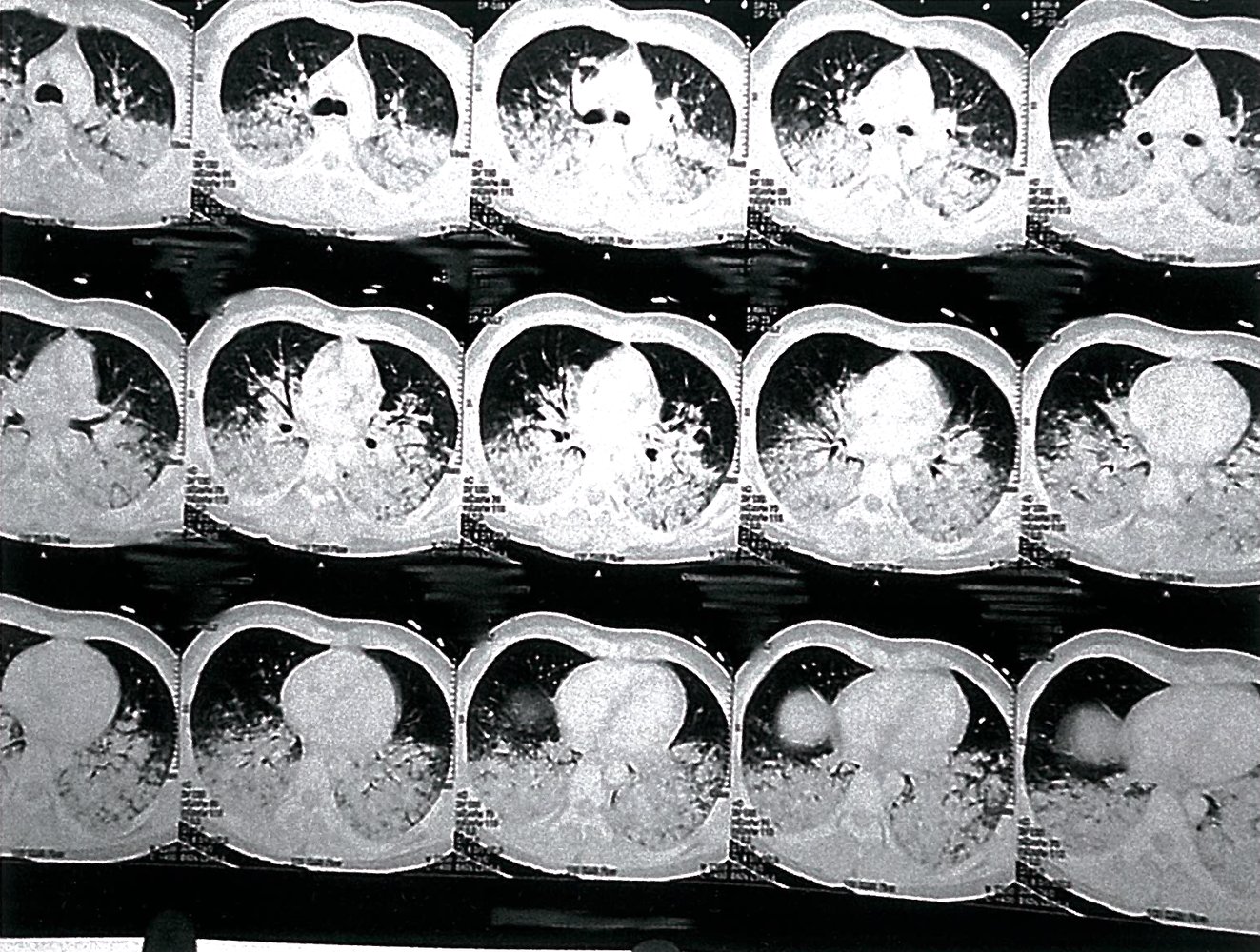
CT chest (lung window)
There are pronounced bilateral opacities visible in the posterior lung bases.
The is the characteristic supine radiological appearance of ARDS
Source: © IMPP
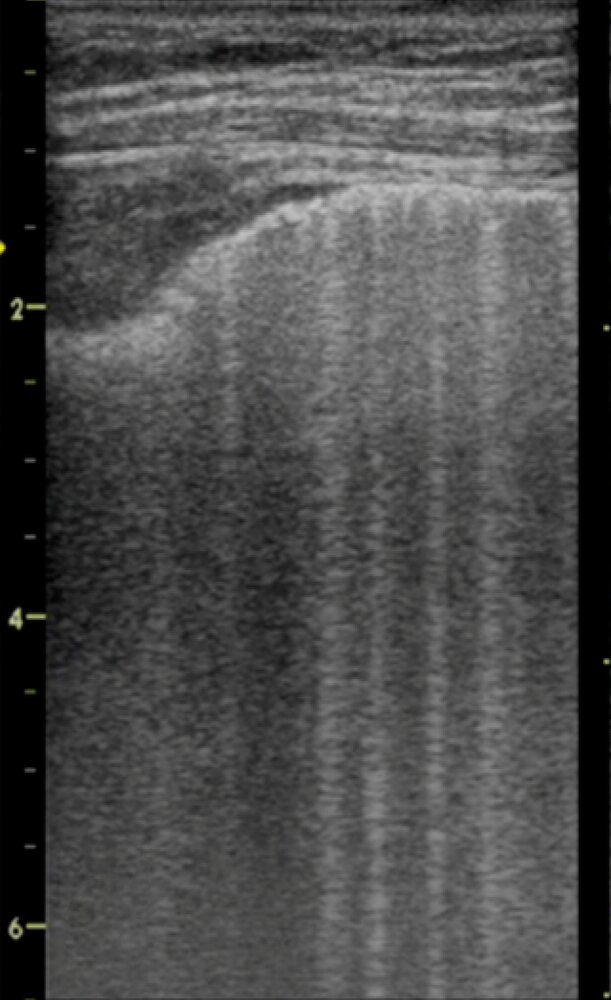
B-lines (examples indicated by green overlay) are well-defined vertical hyperechoic comet-tail artifacts that arise from the hyperechoic pleural line, move with respiration (swinging flashlight appearance), and do not fade with depth.
Fewer than three B-lines in a single field of view between two ribs is considered normal. Multiple (≥3) B-lines between two ribs are called “lung rockets” and may be seen with interlobular septal edema or fibrosis. B-lines are lost in pneumothorax. B-lines erase A-lines, which are horizontal reverberation artifacts that parallel the pleural line in the aerated lung.
Source: “Current Concepts of ARDS: A Narrative Review” by Michele Umbrello, Paolo Formenti, Luca Bolgiaghi and Davide Chiumello, International Journal of Molecular Sciences, licensed under CC BY 4.0. Modifications: image is cropped, number was removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
- Cardiogenic pulmonary edema
- Acute exacerbations of interstitial lung diseases
- Transfusion-related acute lung injury (TRALI)
- Transfusion-associated circulatory overload (TACO)
- See also differential diagnoses of dyspnea.
The differential diagnoses listed here are not exhaustive.
Management
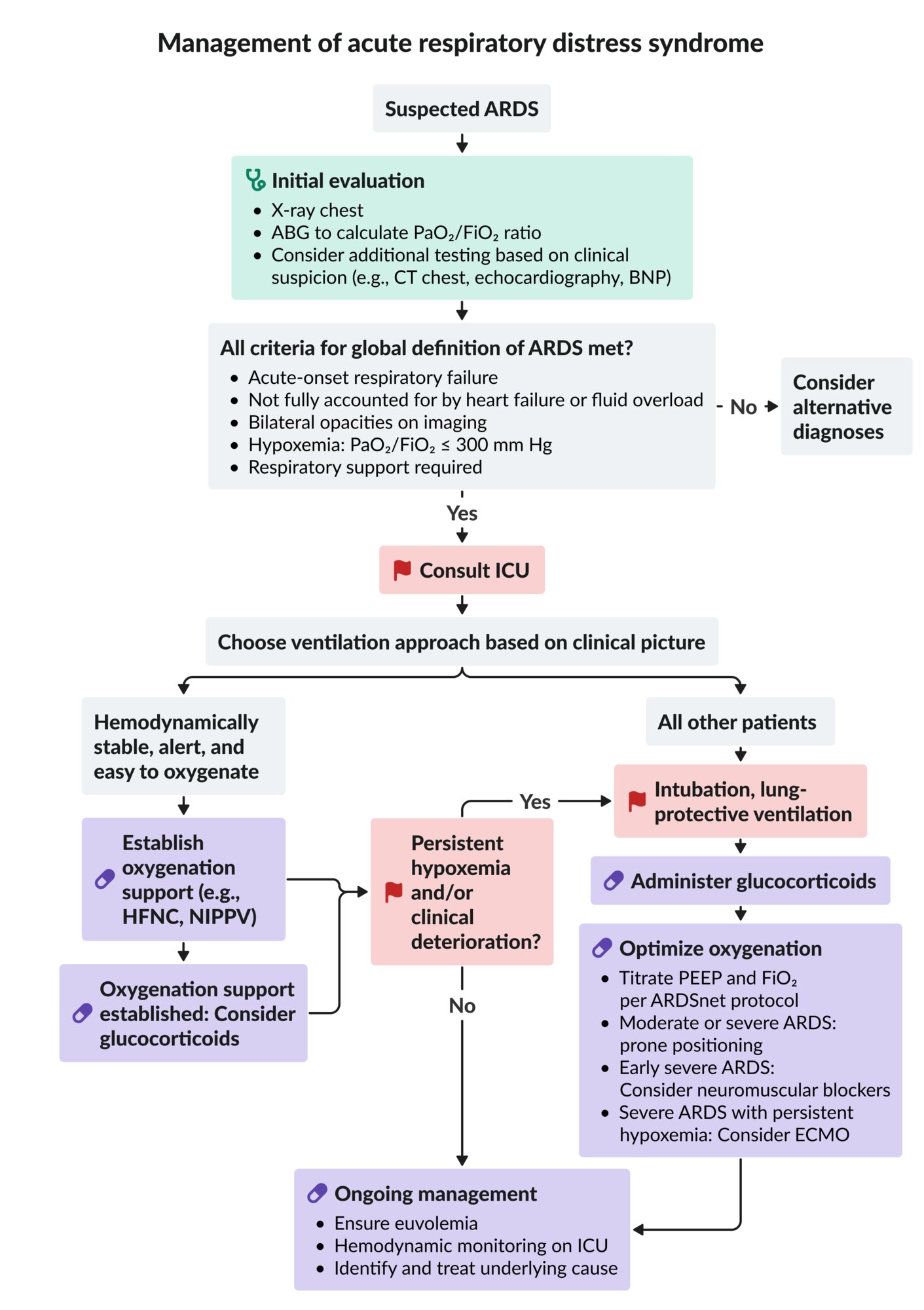
Approach [8]
- Admit all patients with ARDS to the ICU.
- Address hypoxemia.
- See “Oxygen therapy” and “Airway management” for details.
- Apply lung-protective ventilation in intubated ARDS.
- Identify and treat the underlying cause (e.g., pneumonia, pancreatitis, sepsis).
- Initiate glucocorticoids in patients with intubated ARDS and/or if the cause responds to glucocorticoids.
- Provide supportive care.
- Adjust therapy based on severity.
- Moderate or severe ARDS: Use prone positioning and consider a high PEEP strategy.
- Early severe ARDS: Consider neuromuscular blockers.
- Severe ARDS not responding to therapeutic adjustments: Consider ECMO.

ARDS is a life-threatening condition that usually requires early lung-protective ventilation (i.e., with low tidal volumes and low plateau pressures) to prevent further lung damage.
All patients with ARDS [4][8][12][13]
Oxygenation
Hypoxemia is a hallmark feature of ARDS and should be addressed immediately.
-
Noninvasive: See “Oxygen therapy.”
- Indications [14]
- May be considered for hemodynamically stable, alert patients with easy to oxygenate, mild ARDS.
- Preoxygenation prior to intubation
- Methods: maximum supplemental oxygen by HFNC, NIPPV, or nonrebreather mask
- Indications [14]
-
Invasive
- Indications: respiratory failure or rapid deterioration
- Methods: Endotracheal intubation (see “Airway management.”)
- Rapid sequence intubation
- Consider pre-oxygenation (see nonivasive methods).
Lung-protective ventilation [8][12]
All patients with intubated ARDS should be treated with lung-protective ventilation to decrease the risk of VILI. [12]
- General initial settings include:
- Low tidal volume (Vt 4–8 mL/kg) using predicted body weight: prevents alveolar distention [8]
- Low plateau pressure (PPlat ≤ 30 cm H2O): prevents barotrauma
- PEEP ≥ 5 cm H2O: allows for alveolar recruitment
- Allow for permissive hypercapnia.
-
PEEP and FiO2 can be adjusted to recruit collapsed alveoli and improve oxygenation.
- Oxygenation goal: PaO255–80 mm Hg or SpO2 88–95%
- Avoid oxygen toxicity: use lowest FiO2 possible
- See “Lung-protective ventilation strategy” in “Mechanical ventilation” for more information and specific parameter settings.
A low tidal volume and low plateau pressure are the principles of lung-protective ventilation.
Glucocorticoids in ARDS [8][15]
Glucocorticoids likely reduce mortality and the duration of mechanical ventilation in patients with ARDS.
- Optimal regimen is not established; consider:
- Dexamethasone (off-label) until extubation [15][16]
- OR methylprednisolone (off-label) [15]
- Indications
- Intubated ARDS
- A cause that responds to glucocorticoids; see also: [8]
- Treatment of pneumonia
- Management of hospitalized patients with COVID-19
- Treatment of pneumocystis pneumonia
- Precaution: may be harmful if initiated after > 2 weeks of mechanical ventilation
Supportive care
- Conservative fluid management
- Consider furosemide for volume overload.
- VTE prophylaxis
- Optimize nutrition.
- Consider stress ulcer prophylaxis.
Moderate to severe ARDS [8][14][17][18]
Prone positioning [19][20][21]
Prone positioning should be initiated promptly after stabilization.
-
Effects
- Reduces V/Q mismatch from dependent atelectasis
- Increases lung compliance
-
Indications [18]
- P/F ratio < 150 mm Hg
- Pulmonary edema
- Absolute contraindication: unstable spinal fracture
-
Relative contraindications include: [14]
- Hemodynamic instability
- Severe trauma, recent sternotomy, other unstable fractures
- ↑ ICP
- Massive hemoptysis
- Duration: typically done for at least 12–16 hours/day
-
Complications include:
- ET tube displacement or obstruction
- Abnormal vital signs: ↓ SpO2, ↓ HR, ↓ BP
- Hemoptysis
- Pressure injuries
- Other: facial edema, ocular injury , venous stasis
An unstable spinal fracture is the only absolute contraindication to prone positioning. [21]

High PEEP [8]
-
Methods
- Oxygenation-based PEEP titration
- Plateau pressure-based PEEP titration
- Titration to maximal compliance
-
Effects
- Lung recruitment maneuver: increases the surface area of lung available for gas exchange [8]
- Improves oxygenation and is thought to reduce mortality
FiO2/PEEP titration
| ARDSnet protocol for FiO2/PEEP titration [22][23][24] | |
|---|---|
| Low PEEP/FiO2 strategy: for patients with mild ARDS | |
| FiO2 (%) | PEEP (cm H2O) |
| 30 | 5 |
| 40 | 5 |
| 40 | 8 |
| 50 | 8 |
| 50 | 10 |
| 60 | 10 |
| 70 | 10 |
| 70 | 12 |
| 70 | 14 |
| 80 | 14 |
| 90 | 14 |
| 90 | 16 |
| 90 | 18 |
| 100 | 18–24 |
| High PEEP/FiO2 strategy: for patients with moderate to severe ARDS | |
| 30 | 5 |
| 30 | 8 |
| 30 | 10 |
| 30 | 12 |
| 30 | 14 |
| 40 | 14 |
| 40 | 16 |
| 50 | 16 |
| 50 | 18 |
| 50–80 | 20 |
| 80 | 22 |
| 90 | 22 |
| 100 | 22–24 |
Neuromuscular blockers [8]
- Consider within the first 48 hours for patients with a PaO2/FiO2 ratio < 150 mm Hg (i.e., early severe ARDS). [8][18]
- Optimal agent not established; cisatracurium may be considered.
- See “Muscle relaxants” for agents and dosages.
Severe ARDS with persistent hypoxemia [8][14]
The following interventions should only be considered in consultation with a specialist and if standard therapy is unsuccessful.
- Consider alternative ventilator settings (e.g., mode, parameters, or overall strategy): See “Mechanical ventilation.”
- Consider ECMO in patients with early ARDS (< 7 days) and: [18][25]
- Very severe hypoxemia (PaO2/FiO2< 80 mm Hg) or hypercapnia (pH < 7.25 and PaCO2≥ 60 mm Hg) despite optimal management (e.g., high PEEP, neuromuscular blockers, prone positioning)
- AND/OR if the plateau pressure becomes dangerously high (e.g., > 30 cm H2O)
- Use a monitoring tool (e.g., Murray score) to identify patients at risk for requiring ECMO, enabling transfer to an ECMO unit before deterioration. [25]
| Murray score for ARDS [26] | ||
|---|---|---|
| Clinical parameter | Findings | Points assigned |
| Alveolar consolidation on x-ray | None | 0 |
| 1 quadrant involved | 1 | |
| 2 quadrants involved | 2 | |
| 3 quadrants involved | 3 | |
| 4 quadrants involved | 4 | |
| P/F ratio in mm Hg | > 300 | 0 |
| 225–299 | 1 | |
| 175–224 | 2 | |
| 100–174 | 3 | |
| ≤ 100 | 4 | |
| PEEP in cm H2O | ≤ 5 | 0 |
| 6–8 | 1 | |
| 9–11 | 2 | |
| 12–14 | 3 | |
| > 15 | 4 | |
| Respiratory compliance in mL/cm H2O | > 80 | 0 |
| 60–79 | 1 | |
| 40–59 | 2 | |
| 20–39 | 3 | |
| < 19 | 4 | |
Interpretation: Add up the total points and divide the total by the number of parameters present.
| ||

ABG: arterial blood gas analysis
ARDS: acute respiratory distress syndrome
BNP: brain natriuretic peptide
ECMO: extracorporeal membrane oxygenation
FiO2: fraction of inspired oxygen
HFNC: high-flow nasal cannula oxygen therapy
NIPPV: noninvasive positive-pressure ventilation
PaO2: partial pressure of oxygen in arterial blood
© AMBOSS
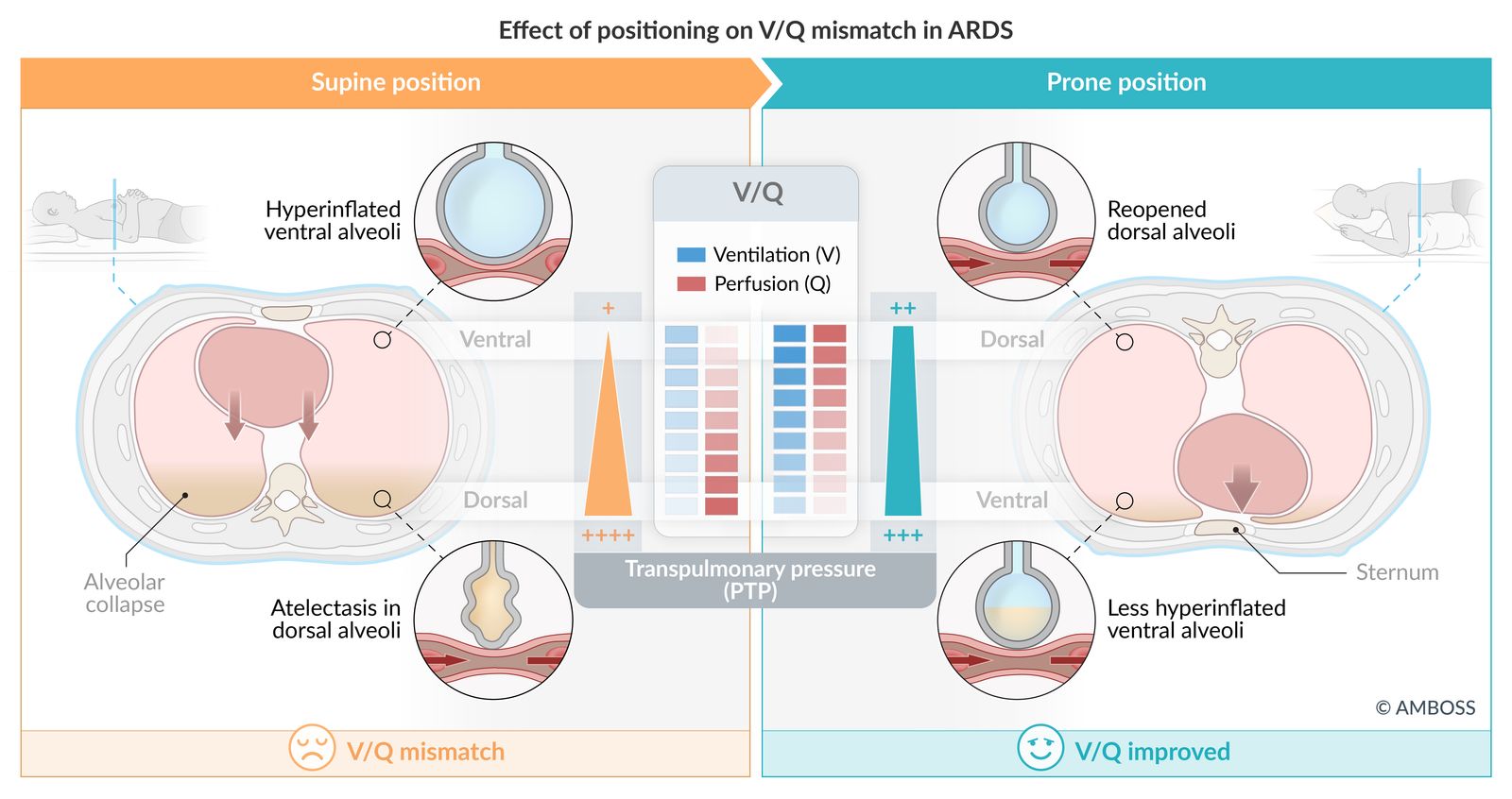
Supine position (left): In a patient lying flat, gravity causes alveolar fluid to settle in the dorsal (back) lung regions, leading to atelectasis (collapse). Simultaneously, mechanical ventilation over-distends the ventral (front) alveoli, causing hyperinflation. This creates a significant V/Q mismatch: blood flow (perfusion, Q) is highest in the collapsed dorsal areas (poor ventilation, V), while ventilation is highest in the less-perfused ventral areas.
Prone position (right): When the patient is turned onto their stomach, gravity helps drain fluid from the dorsal regions, allowing the dorsal alveoli to reopen and participate in gas exchange. This position also reduces the compression on the lungs, leading to less hyperinflation of the ventral alveoli. The result is a more even distribution of both ventilation and perfusion, which improves the V/Q match and overall oxygenation.
© AMBOSS

The centrifugal pump (P) draws deoxygenated blood from the patient's circulation and through the ECMO circuit, where the oxygenator (O) decarboxylates and oxygenates the blood before it is returned to the patient's circulation. The support system (S) controls gas exchange. The heat exchanger (W) ensures a consistent temperature of the extracorporeal circulation.
Source: "ECMO in H1N1 patient in Santa Cruz Hospital - Lisbon", Cmenesesoliveira, Wikimedia Commons licensed under Public Domain
{kind=link}
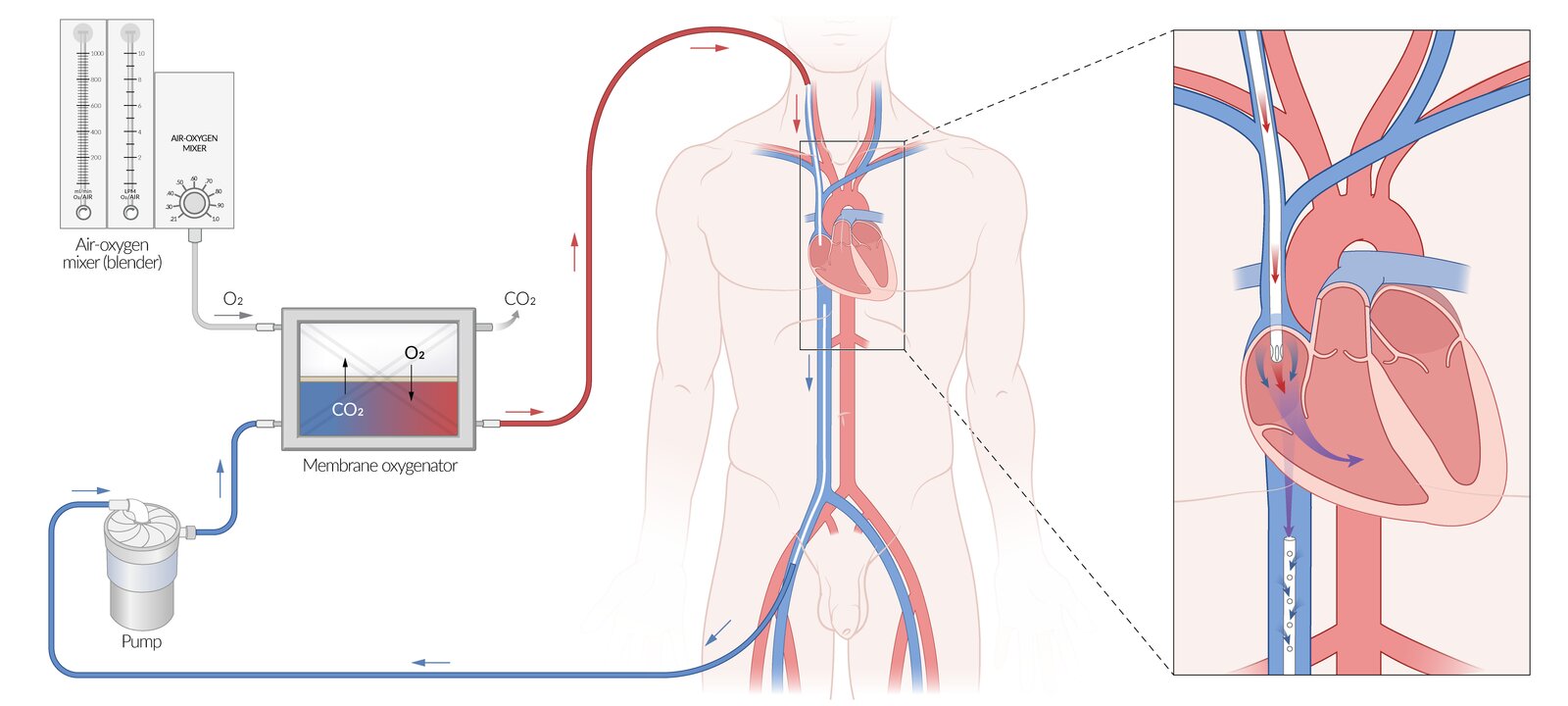
Extracorporeal membrane oxygenation (ECMO) is an advanced life support method in which a bypass system circulates the patient's blood through artificial gas exchange membranes.
This illustration shows venovenous ECMO (VV-ECMO), which supports respiratory function only and is used in patients with preserved circulatory function. VV-ECMO may be used, e.g., as a rescue treatment for patients with acute respiratory failure or as a bridge to lung transplantation.
Peripheral cannulation using the femoral vein and internal jugular vein is depicted here, but other access techniques may be used. Deoxygenated blood is removed from the inferior vena cava and returned to the right atrium after oxygenation. Circulation relies on the patient's own cardiac function.
© AMBOSS
Acute management checklist
- ABCDE survey
- Obtain a chest x-ray and ABG.
- Establish severity with the P/F ratio.
- Consult ICU and/or rapid response team.
- Optimize oxygenation.
- Provide airway management as needed.
- Lung-protective ventilation strategy
- Ensure euvolemia.
- Hemodynamic monitoring
- Glucocorticoids for patients with intubated ARDS and/or if the cause responds to glucocorticoids
- Prone positioning for moderate or severe ARDS
- Consider ECMO for very severe hypoxemia or hypercapnia.
- ICU admission
- Treat the underlying cause.
Prognosis
- Disease course
- Most patients begin to improve after the first 1–3 weeks and symptoms usually resolve fully.
- Some develop interstitial pulmonary fibrosis with prolonged ventilator dependence and restrictive lung disease.
- In patients with simultaneous multiorgan failure, the mortality rate is 30–50%. [27]
Related One-Minute Telegram
- One-Minute Telegram 20-2021-1/3: Better outcomes after implementation of critical care management protocols?
- One-Minute Telegram 1-2020-3/3: Vaping kills – but who is at risk?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- One-Minute Telegram
- 2024 ATS Guideline Update on Management of Adult Patients with ARDS
- 2023 ATS A New Global Definition of ARDS
- 2021 ELSO Guideline on Management of Adult Patients Supported with Venovenous ECMO
- 2017 ATS/ESCIM/SCCM Clinical Practice Guideline on Mechanical Ventilation in Adult Patients with ARDS
References
- Matthay MA, Arabi Y, Arroliga AC, et al. "A New Global Definition of Acute Respiratory Distress Syndrome". Am J Respir Crit Care Med. 209(1). :37-47. (2024)
- Doyle RL, Szaflarski N, Modin GW, Wiener-Kronish JP, Matthay MA. "Identification of patients with acute lung injury. Predictors of mortality". Am J Respir Crit Care Med. 152(6). (1995)
- Daphale A, Acharya S, Shukla S, Alegaonkar S. "Bleomycin Induced Acute Respiratory Distress Syndrome". Journal of Case Reports. :55-57. (2017)
- Thompson BT, et al. "Acute Respiratory Distress Syndrome". N Engl J Med. 377(6). :562-572. (2017)
- Sutyak JP, Wohltmann CD, Larson J. "Pulmonary Contusions and Critical Care Management in Thoracic Trauma". Thorac Surg Clin. 17(1). :11-23, v. (2007)
- Idris AH, Berg RA, Bierens J, et al. "Recommended guidelines for uniform reporting of data from drowning: the "Utstein style"". Circulation. 108(20). :2565-74. (2003)
- Udobi KF, Childs ED, Touijer K. "Acute Respiratory Distress Syndrome". Am Fam Physician. 67(2). :315-322. (2003)
- Qadir N, Sahetya S, Munshi L, et al. "An Update on Management of Adult Patients with Acute Respiratory Distress Syndrome: An Official American Thoracic Society Clinical Practice Guideline". Am J Respir Crit Care Med. 209(1). :24-36. (2024)
- Sheard S, et al. "Imaging of Acute Respiratory Distress Syndrome". Respir Care. 57(4). :607-612. (2012)
- Zompatori M, et al. "Overview of current lung imaging in acute respiratory distress syndrome". European Respiratory Review. 23(134). :519-530. (2014)
- Papazian L, et al. "Diagnostic workup for ARDS patients". Intensive Care Med. 42(5). :674-685. (2016)
- Stapleton RD, et al. "Causes and timing of death in patients with ARDS". Chest. 128(2). :525-32. (2005)
- Fan E, Del Sorbo L, Goligher EC, et al. "An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome". Am J Respir Crit Care Med. 195(9). :1253-1263. (2017)
- Fichtner F, Moerer O, Weber-Carstens S, et al. "Clinical Guideline for Treating Acute Respiratory Insufficiency with Invasive Ventilation and Extracorporeal Membrane Oxygenation: Evidence-Based Recommendations for Choosing Modes and Setting Parameters of Mechanical Ventilation". Respiration. 98(4). :357-372. (2019)
- Grasselli G, Calfee CS, Camporota L, et al. "ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies". Intensive Care Med. 49(7). :727-759. (2023)
- Chaudhuri D, Nei AM, Rochwerg B, et al. "2024 Focused Update: Guidelines on Use of Corticosteroids in Sepsis, Acute Respiratory Distress Syndrome, and Community-Acquired Pneumonia". Crit Care Med. 52(5). :e219-e233. (2024)
- Villar J, Ferrando C, Martínez D, et al. "Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial". Lancet Respir Med.. 8(3). :267-276. (2020)
- Rawal G, et al. "Acute respiratory distress syndrome: An update and review". Journal of Translational Internal Medicine. 6(2). :74-77. (2018)
- Papazian L, et al. "Formal guidelines: management of acute respiratory distress syndrome". Annals of Intensive Care. 9(1). (2019)
- Archambault PM, St-Onge M. "Invasive and Noninvasive Ventilation in the Emergency Department". Emerg Med Clin North Am. 30(2). :421-449. (2012)
- Guérin C, et al. "Prone Positioning in Severe Acute Respiratory Distress Syndrome". N Engl J Med. 368(23). :2159-2168. (2013)
- Rampon GL, Simpson SQ, Agrawal R. "Prone Positioning for Acute Hypoxemic Respiratory Failure and ARDS". Chest. 163(2). :332-340. (2023)
- Wright BJ. "Lung-protective Ventilation Strategies and Adjunctive Treatments for the Emergency Medicine Patient with Acute Respiratory Failure". Emerg Med Clin North Am. 32(4). :871-887. (2014)
- Mosier JM, Hypes C, Joshi R, et al. "Ventilator Strategies and Rescue Therapies for Management of Acute Respiratory Failure in the Emergency Department". Ann Emerg Med. 66(5). :529-541. (2015)
- Walkey AJ, Del Sorbo L, Hodgson CL, et al. "Higher PEEP versus Lower PEEP Strategies for Patients with Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis". Annals of the American Thoracic Society. 14(Supplement_4). :S297-S303. (2017)
- Tonna JE, Abrams D, Brodie D, et al. "Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO)". ASAIO J. 67(6). :601-610. (2021)
- Raghavendran K, Napolitano LM. "Definition of ALI/ARDS". Crit Care Clin. 27(3). :429-437. (2011)
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Wolters Kluwer Health. (2015). ISBN: 9781496306142
- Kleinman S, Kor DJ. "Transfusion-related acute lung injury (TRALI)". UpToDate. UpToDate. https://www.uptodate.com/contents/transfusion-related-acute-lung-injury-trali?source=search_result&search=transfusion%20related%20acute%20lung%20injury&selectedTitle=1~50#H2. [2015-07-09]
- Bux J. "Transfusion-related acute lung injury (TRALI): a serious adverse event of blood transfusion". Vox Sang. (2005)
- Toy P, Popovsky MA, Abraham E et al. "Transfusion-related acute lung injury: definition and review". Crit Care Med. 33(4). :721-726. (2005)
- "Acute transient leukopenia as a sign of TRALI"
- Bux J, Sachs UJH. "Pulmonary Transfusion Reactions". Transfus Med Hemother. 35(5). :337-345. (2008)
- Siegel MD. "Acute respiratory distress syndrome: Supportive care and oxygenation in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/acute-respiratory-distress-syndrome-supportive-care-and-oxygenation-in-adults?source=search_result&search=ards&selectedTitle=3~150. [2016-12-05]
- Swinamer DL, Phang PT, Jones RL, Grace M, King EG. "Effect of Routine Administration of Analgesia on Energy Expenditure in Critically III Patients". Chest. 93(1). :4-10. (1988)
- Siegel MD, Hyzy RC. "Mechanical ventilation of adults in acute respiratory distress syndrome". UpToDate. UpToDate. https://www.uptodate.com/contents/mechanical-ventilation-of-adults-in-acute-respiratory-distress-syndrome?source=search_result&search=acute%20respiratory%20distress%20syndrome&selectedTitle=4~150#H20. [2016-06-16]
- "What is ECLS?". http://www.med.umich.edu/ecmo/about/what.html. [2017-01-01]
- Bartlett R. "Extracorporeal membrane oxygenation (ECMO) in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/extracorporeal-membrane-oxygenation-ecmo-in-adults. [2016-12-16]
- "Indications for Pediatric Respiratory Extracorporeal Life Support". http://www.elso.org/Portals/0/Files/ELSO%20guidelines%20paeds%20resp_May2015.pdf. [2015-03-01]
- Siegel MD. "Acute respiratory distress syndrome: Prognosis and outcomes in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/acute-respiratory-distress-syndrome-prognosis-and-outcomes-in-adults. [2016-05-18]
- Curley GF, Laffey JG, Zhang H, Slutsky AS. "Biotrauma and Ventilator-Induced Lung Injury". Chest. 150(5). :1109-1117. (2016)
- Amato MBP, Meade MO, Slutsky AS, et al. "Driving Pressure and Survival in the Acute Respiratory Distress Syndrome". N Engl J Med. 372(8). :747-755. (2015)