Summary
Adenomyosis is a chronic disease characterized by growth of endometrial tissue within the myometrium due to nonmalignant hyperplasia of the endometrial basal layer. Adenomyosis affects individuals of reproductive age; the etiology is unknown, but it often coexists with conditions such as endometriosis and uterine fibroids. Symptoms include dysmenorrhea, abnormal uterine bleeding, chronic pelvic pain, and infertility. A globular, uniformly enlarged uterus may be detected on pelvic examination. Transvaginal ultrasound is the preferred initial test to evaluate for adenomyosis. Treatment consists of NSAIDs and hormonal contraception to relieve pain and other symptoms. For patients with refractory symptoms or who are trying to conceive, referral to a specialist for consideration of invasive treatment or medical therapy with GnRH agonists or GnRH antagonists is recommended.
Epidemiology
Peak incidence at 40–50 years
Epidemiological data refers to the US, unless otherwise specified.
Etiology
The exact etiology is unknown, although adenomyosis often occurs in patients with: [1][2]
- Endometriosis
- Uterine fibroids
- Endometrial polyps
- A history of:
- Uterine surgery (including cesarean delivery)
- Multiparity
Clinical features
-
Symptoms: present in two-thirds of patients [2]
- Abnormal uterine bleeding (AUB)
- Dysmenorrhea
- Chronic pelvic pain that is aggravated during menses
- Dyspareunia
- Infertility [1]
- Pelvic examination: soft (boggy), uniformly enlarged, globular uterus that may be tender on palpation [2][3]
Adenomyosis is asymptomatic in up to one-third of patients. [1]
Diagnosis
Adenomyosis is typically diagnosed based on clinical features and imaging studies. While histological examination of excised tissue (e.g., after hysterectomy or excision) provides a definitive diagnosis, surgery is not performed solely to confirm the diagnosis. [1][3][4]
Initial studies
Consider starting treatment for adenomyosis before confirming the diagnosis. [1][2]
Imaging
-
Transvaginal ultrasound (TVUS) [5]
- Test of choice for initial imaging of the uterus
- Findings include: [3]
- Heterogeneous myometrium
- Asymmetric myometrial thickening
- Myometrial cysts
- Subendometrial echogenic linear striations
- Obtain MRI pelvis with and without IV contrast if: [2][5][6]
- TVUS results are inconclusive
- The uterus cannot be completely visualized with TVUS
- Surgery is planned
Additional diagnostic studies
Additional studies depend on clinical features and may include:
- Diagnostics for AUB
- Diagnostics for infertility
Advanced diagnostic studies
Advanced diagnostic studies are not routinely performed but may be considered by a gynecologist.
-
Hysteroscopy [4]
- Used in diagnostic uncertainty [1]
- Findings include hypervascularization, submucosal hemorrhagic cysts, and endometrial defects. [1]
-
Histology of excised tissue [4]
- Provides a definitive diagnosis [2]
- Consider if the patient is undergoing surgical treatment for suspected adenomyosis.


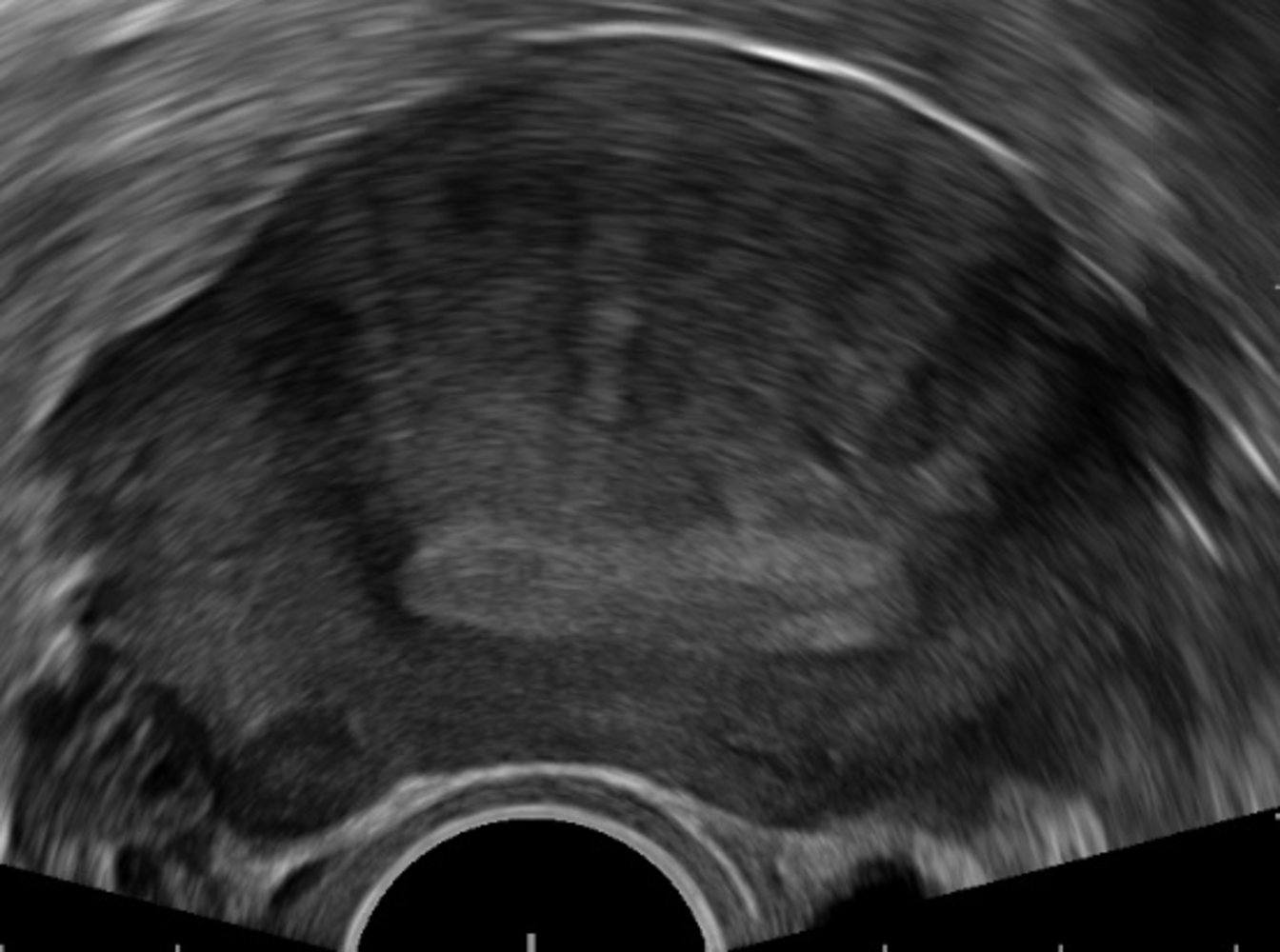
Ultrasound pelvis (transvaginal; transverse plane)
Heterogeneous asymmetric thickening of the anterior myometrium (green overlay) is accompanied by a myometrial cyst (red overlay). There is an irregular interface between the endometrium (E) and the myometrial thickening. The additional small round hypoechogenic lesion (green hatched overlay) is a leiomyoma.
P: ultrasound probe
Dashed line: uterus
Source: “Linear striations of adenomyosis” by Mikael Häggström, Wikimedia Commons, licensed under CC0 1.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
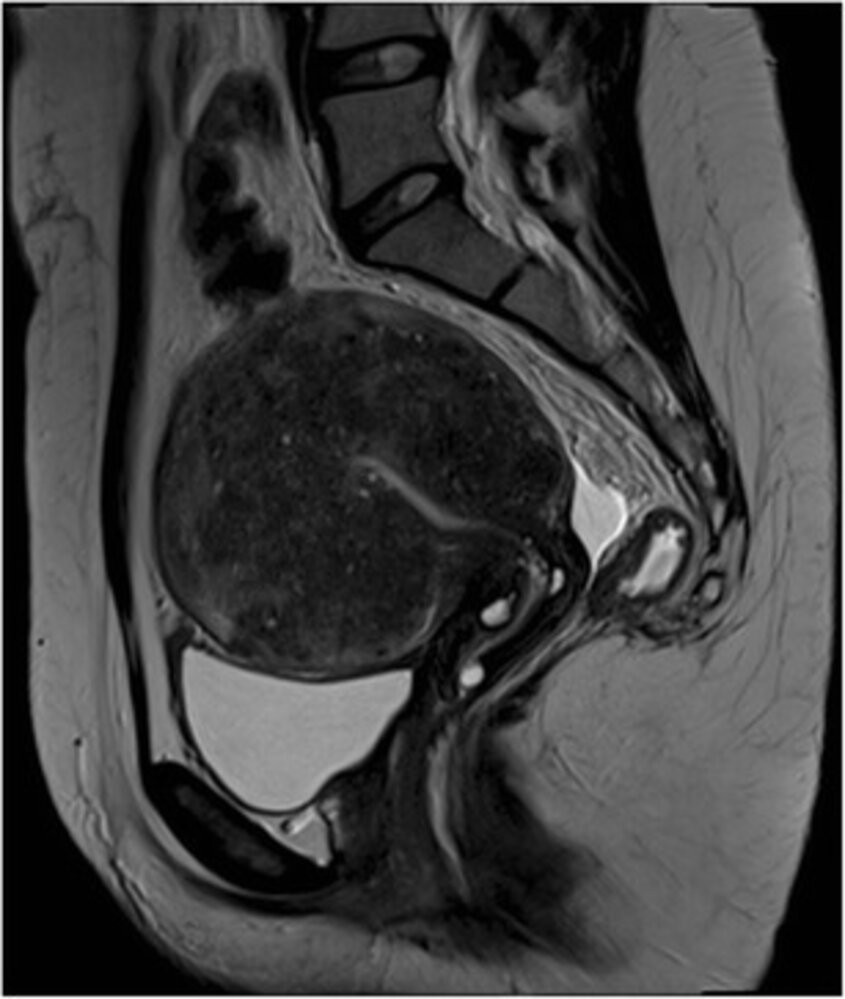
MRI pelvis (T2-weighted; sagittal plane)
Uterine enlargement accompanied by diffuse, predominantly hypointense widening of the junctional zone is seen. Multiple punctate high-intensity myometrial foci are visible within the uterine wall, demonstrating scattered foci of ectopic endometrium (examples indicated by arrowheads).
The findings are characteristic of uterine adenomyosis.
Source: “Figure 1, in: MRI for adenomyosis: a pictorial review” by L. Agostinho, R. Cruz, F. Osório et al., Springer Link - Pictorial Review, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
- Differential diagnoses of vaginal bleeding
- Causes of AUB
- Causes of pelvic pain
- Common causes of dysmenorrhea
The differential diagnoses listed here are not exhaustive.
Treatment
Treatment of adenomyosis is primarily symptom-based; see also “Treatment of abnormal uterine bleeding.”
Approach [1][2]
- Identify and treat:
- Complications of adenomyosis
- Common comorbid conditions (e.g., endometriosis)
- Start initial therapy for symptom relief. [1][2]
- Refer patients to gynecology to evaluate for advanced treatments if they:
- Are trying to conceive
- Are unable to tolerate initial therapy
- Have refractory symptoms despite initial medical therapy
Initial therapy [1][2]
- Combined oral contraceptives (off-label)
- Progestin-only contraceptive pills, e.g., high-dose norethindrone (off-label) [2]
- Progestin intrauterine device (off-label)
- NSAIDs for pain relief, e.g., ibuprofen (for dosages, see “Oral analgesia”) [2]
Advanced treatments
- Medical therapy: GnRH agonists (off-label) and GnRH antagonists (off-label) [2]
-
Invasive treatments for adenomyosis [1][2]
- Fertility-sparing procedures (e.g., adenomyomectomy, uterine wedge resection)
- Fertility-compromising procedures (e.g., endometrial ablation, uterine artery embolization, hysterectomy)
Complications
- Anemia
- Infertility
- Obstetric complications, e.g.: [2]
- Preeclampsia
- Preterm birth
- Small for gestational age
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Schrager S, Yogendran L, Marquez CM, Sadowski EA. "Adenomyosis: Diagnosis and Management". Am Fam Physician. 105(1). :33-38. (2022)
- Kho KA, Chen JS, Halvorson LM. "Diagnosis, Evaluation, and Treatment of Adenomyosis". JAMA. 326(2). :177. (2021)
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. "Practice Bulletin No. 128: Diagnosis of Abnormal Uterine Bleeding in Reproductive-aged Women (reaffirmed 2024)". Obstet Gynecol. 120(1). :197-206. (2012)
- Ferrero S, Scala C, Vellone VG, Biscaldi E, Barra F. "Transvaginal ultrasound-guided biopsy of adenomyosis". Ann Transl Med. 7(S8). :S341-S341. (2019)
- Robbins JB, Sadowski EA, Maturen KE, et al. "ACR Appropriateness Criteria® Abnormal Uterine Bleeding". J Am Coll Radiol. 17(11). :S336-S345. (2020)
- Munro MG, Critchley HOD, Fraser IS. "The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions". Int J Gynaecol Obstet. 143(3). :393-408. (2018)