CME information and disclosures
To see contributor disclosures related to this article, click on this reference: [1]
Physicians can earn CME/MOC credit by using this article to address a clinical question and completing a brief evaluation about how they applied the information in their practice.
AMBOSS designates this internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and links” at the bottom of this article.
Quick guide
Diagnostic approach
- ABCDE approach
- Targeted clinical evaluation to identify trigger and assess severity
- Imaging to rule out differential diagnoses (e.g., neck imaging, chest imaging, cardiac imaging)
Diagnostic criteria
Anaphylaxis is likely if any of the following criteria are fulfilled:
- Known allergen exposure with hypotension
- Skin and/or mucosal involvement plus cardiovascular or respiratory involvement
- Suspected allergen exposure with ≥ 2 systems involved (GI, CV, respiratory, skin)
Management checklist
- Epinephrine
- Rapid sequence intubation for airway compromise
- Supplemental O2 for hypoxia
- Bronchodilators (e.g., albuterol) as needed
- IV fluids for hypotension
- Remove the allergen.
- Consider antihistamines, e.g., diphenhydramine AND cimetadine (off-label)
- Consider corticosteroids, e.g., methylprednisolone OR prednisone
- Continuous cardiac telemetry
- Continuous pulse oximetry
- Close clinical monitoring for biphasic reaction
- Admit to ICU or medical service.
Summary
Anaphylaxis is an acute, potentially life-threatening, type 1 hypersensitivity reaction, involving the sudden IgE-mediated release of histamine mediators from mast cells and basophils in response to a trigger (e.g., food, insect stings, medication). Anaphylactoid reactions (a subtype of pseudoallergy) are IgE-independent reactions that result from direct mast-cell activation (e.g., in response to opioids); the clinical presentation and management are the same as for anaphylaxis. Typical signs and symptoms of both reactions include the acute onset of hives, angioedema, stridor, dyspnea, bronchospasm, circulatory failure (distributive shock), vomiting, and diarrhea. The diagnosis is clinical and is based on combinations of typical symptoms, plus the presence of a known or suspected trigger. Rapid recognition and treatment are key to prevent death from airway loss, respiratory failure, or cardiovascular collapse. Management consists of initial resuscitation measures that focus on administering IM epinephrine, removing triggers, securing the airway, and giving IV fluid boluses, which take precedence over adjunctive treatment like steroids and antihistamines.
Definitions
- Anaphylaxis: a severe type 1 hypersensitivity reaction that can cause life-threatening and multisystem effects due to IgE-mediated mast cell activation
-
Anaphylactoid reaction
- A reaction that is clinically similar to anaphylaxis but is mediated by direct nonimmune-mediated activation of either mast cells or the complement cascade (see “Pseudoallergy”)
- Examples include reactions to radiocontrast media and vancomycin
- Anaphylactic shock: a type of distributive shock that results from anaphylaxis
Etiology
- Trigger is idiopathic in 20% of patients [2]
- Most common triggers leading to fatal anaphylaxis [2][3][4]
- Younger patients: food allergies; (e.g., peanut, tree nuts), insect stings (e.g., bee stings)
- Older patients: drug reactions, radiocontrast media
- Hospitalized patients: food, medications (e.g., antibiotics, NSAIDs), latex
Pathophysiology
- Anaphylaxis (type I hypersensitivity reaction) or anaphylactoid reactions → degranulation of mast cells → massive histamine release → systemic vasodilation → increased capillary leakage → anaphylactic shock
- See also “Hypersensitivity classification.”
Clinical features
Onset of symptoms [3][5]
In general, the onset of symptoms is acute (within minutes to hours of exposure to a likely antigen).
| Antigen-dependent onset of anaphylaxis [3][5] | |
|---|---|
| Trigger | Median time to circulatory arrest |
| Food | 30 min |
| Insect | 15 min |
| Medication | 5 min |
Affected organ systems [3][5]
-
Skin or mucous membranes
- Flushing, erythema
- Hives, pruritus
- Swelling of the eyelids, angioedema
- Nasal congestion, sneezing
-
Respiratory
- Cough, hoarseness
- Chest tightness
- Dyspnea (due to bronchospasm or laryngeal edema), tachypnea
- Stridor, wheezing
- Hypoxia, cyanosis
-
Gastrointestinal
- Nausea, vomiting (especially in food allergies)
- Abdominal pain, diarrhea
-
Cardiovascular
-
Hypotension
- Adults: SBP < 90 mm Hg OR decrease ≥ 30% from baseline [6]
- Children: definition depends on age
- Tachycardia, weak peripheral pulses
- Signs of end-organ dysfunction
- Altered mental status, syncope
- Decreased urine output, anuria
- Skin changes (e.g., mottling)
- Low temperature
- Delayed capillary refill (e.g., > 2 seconds)
- Ischemic chest pain
-
Hypotension
Beware of atypical manifestations without skin/mucosal symptoms (10% of patients) to avoid misdiagnosis and treatment delay. [2]
Diagnostic criteria for anaphylaxis [2][5][7]
If any of the following criteria are fulfilled, anaphylaxis is likely. The onset of symptoms must be acute (minutes to hours).
- 1) Known allergen exposure with hypotension (SBP < 90 mm Hg or ≥ 30% decrease from the baseline)
- 2) Acute illness with skin and/or mucosal symptoms (e.g., hives, swollen lips, tongue, and/or uvula) AND ≥ 1 of the following:
- Cardiovascular: SBP < 90 mm Hg or ≥ 30% decrease from baseline and/or altered mental status, syncope, ischemic chest pain, incontinence, or anuria
- Respiratory: dyspnea, hypoxia, stridor, hoarseness, wheezing, cough
- 3) Suspected allergen exposure AND ≥ 2 of the following:
- Gastrointestinal: abdominal pain, nausea, vomiting, diarrhea
- Cardiovascular: systolic BP < 90 mm Hg or ≥ 30% decrease from baseline, and/or altered mental status, syncope, ischemic chest pain, incontinence, anuria
- Respiratory: dyspnea, hypoxia, stridor, hoarseness, wheezing, cough
- Skin/mucosal: hives, angioedema, pruritus, flushing
If anaphylaxis diagnostic criteria are met, empiric treatment should be given without delay.
Management
-
Stabilize the patient (ABCDE approach).
- Airway assessment and management (see “Airway management and ventilation in anaphylaxis”)
- Rapid sequence intubation (RSI) for airway compromise
- Oxygen: Provide FiO2 of 100% (e.g., high-flow O2 by nonrebreather mask).
- Aggressive IV fluid resuscitation if hypotension present (large-bore IV access; administer 1–2 L 0.9% saline IV bolus)
- Position the patient supine.
- If anaphylaxis is likely (see diagnostic criteria for anaphylaxis), start initial treatment immediately: [3][5][8]
- Remove inciting allergen
-
Administer epinephrine IM 1:1,000 (1 mg/mL) into the anterolateral thigh
- Repeat every 5–15 minutes as needed
- IM epinephrine injections always require a more concentrated solution (1:1,000)
- Epinephrine autoinjector may be used.
- See “Anaphylactic transfusion reactions” for specific considerations in patients with reactions during or up to 3 hours after transfusion of blood products.
- Once stabilized, consider adjunctive therapy with antihistamines; , corticosteroids (e.g., methylprednisolone)
- Continuous reassessment and subsequent management
The most important measures in anaphylaxis are to remove the inciting allergen and administer epinephrine as soon as possible. Delay can lead to airway compromise, respiratory failure, refractory shock, and death.
Epinephrine injections for anaphylaxis should always be given intramuscularly in a concentration of 1:1,000 (as opposed to the 1:10,000 solution used in cardiac arrest). Injecting the 1:1,000 solution into a vein can lead to cardiac arrhythmia/arrest.

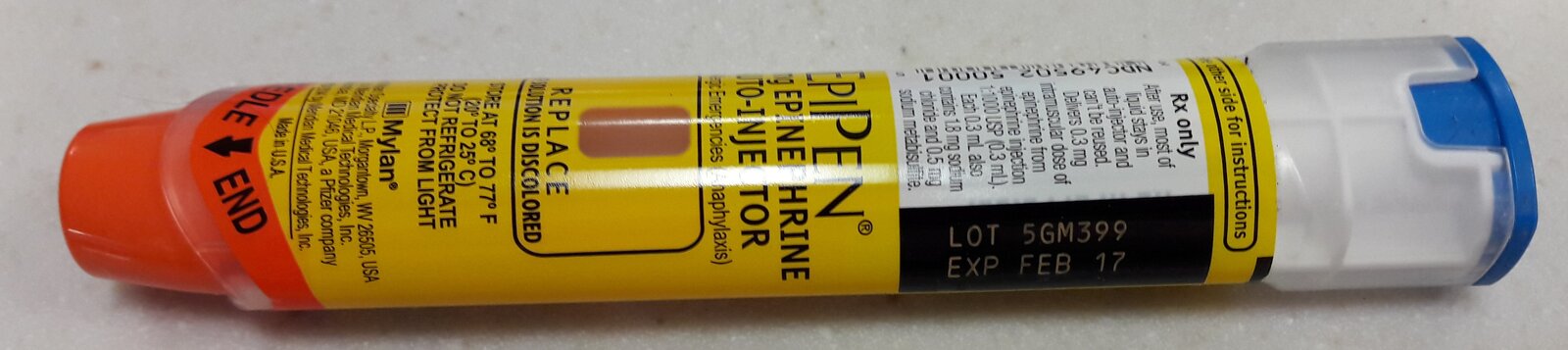
This epinephrine autoinjector (EpiPen) contains 0.3 mg of epinephrine (1:1000 dilution). It is intended for intramuscular injection into the anterolateral thigh in the case of anaphylaxis.
The autoinjector is stored in a carrier tube (not shown in this image). The blue safety release cap requires removing before application. The orange tip is then jabbed firmly into the anterolateral thigh to release the needle (until it clicks) and held in place for 3 seconds to allow the injection to complete.
Source: “Epi-Pen 2016” by Tokyogirl79, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
Diagnostics
Anaphylaxis is a clinical diagnosis (see “Diagnostic criteria for anaphylaxis”).
Laboratory studies [3][9][10]
- Not routinely indicated but can be useful to confirm anaphylaxis or screen for bradykinin-mediated angioedema.
- Serum mast-cell tryptase (MCT): if elevated, supports the diagnosis of anaphylaxis
- Normal result does not rule out anaphylaxis
- Low sensitivity in food-triggered reaction
- Complement C4 levels: can be low in hereditary angioedema (see “Laboratory findings in bradykinin-mediated angioedema”)
Imaging [3][10]
- Not routinely indicated but can be useful to rule in/out mimics.
- Screening for upper airway foreign bodies and infections (e.g., peritonsillar abscess, deep neck space infection, epiglottitis): neck x-ray, CT neck
- Evaluating for other causes of respiratory distress (e.g., pneumonia, pulmonary embolism, ARDS): CXR, CTA Chest
- Assessing cardiac function and evaluating for other causes of shock (e.g., cardiomyopathy): echocardiogram
Airway management and ventilation
See also “Airway management” and “Mechanical ventilation” for more details.
-
Lethargic patients without other overt signs of airway compromise
- Initiate basic airway maneuvers (e.g., head-tilt/chin-lift maneuver, jaw-thrust maneuver, bag-mask ventilation)
- Use basic airway adjuncts, if tolerated: nasopharyngeal airway (NPA) , oropharyngeal airway (OPA)
-
Rapid declining patients or signs of airway compromise: Maximize epinephrine therapy and prepare for early endotracheal intubation.
- Anticipate a difficult airway and difficult ventilation.
- Early anesthesia or ENT consult for awake fiberoptic intubation or surgical airway management
-
Respiratory failure or signs of complete airway obstruction: Perform rapid sequence intubation (RSI).
-
Intubation medications
- Induction agent: Ketamine preferred
- Paralytics: use with caution
- Pretreatment with inhaled racemic epinephrine can be given while preparing for intubation to improve airway edema.
- Additional considerations
- Follow a difficult airway algorithm (e.g., using adjuncts like videolaryngoscopy and/or gum-elastic bougie)
- Postintubation: sedate ideally with ketamine and follow ventilation strategy for obstructive lung disease
-
Intubation medications
-
Severe bronchospasm: Administer a bronchodilator.
- SABA: e.g., albuterol nebulizer OR albuterol MDI
- Consider a muscarinic antagonist additionally: e.g., ipratropium (off-label use)
Obtain early anesthesia or ENT consultation in patients with a rapid decline or anticipated airway compromise.
Subsequent management
Refractory anaphylaxis [3][5][8]
-
Anaphylactic shock refractory to repeated IM epinephrine and fluids
- Continuous IV epinephrine infusion 1:1,000,000 (1 mcg/mL)
- 1:1,000,000 epinephrine solutions may not commercially available and require mixing.
- Administration via central venous access recommended
- Continuous IV epinephrine infusion 1:1,000,000 (1 mcg/mL)
-
Anaphylactic shock refractory to IV epinephrine infusion
- Administer IV glucagon , especially if the patient is on a β-blocker
- Consider other vasopressors
- Ensure adequate fluid status
- Consider consulting ECMO team if above measures fail.
- Cardiac arrest: Start ACLS protocol.
Adjunctive therapy [3][5][8]
-
Antihistamines: Consider a combination of an H1-antagonist and H2-antagonist in severe cases.
- H1-antagonists: e.g., diphenhydramine
- H2-antagonists: e.g., cimetidine (off-label) [11][12][13]
-
Corticosteroids
- Methylprednisolone
- OR prednisone
Antihistamines and steroids should be administered in anaphylaxis only after the initial resuscitation measures (IM epinephrine, fluids and/or vasopressors) have been given.
A lack of response to epinephrine, antihistamines, and steroids should raise suspicion of differential diagnoses such as bradykinin-mediated angioedema, which requires its own specific treatment (see “Treatment of angioedema”).
Monitoring and disposition [3][5][8]
- Monitor in acute-care setting at least 4–8 hours
- Continuous pulse oximetry monitoring
- Continuous cardiac monitoring
- Clinical reassessment for biphasic anaphylactic reactions
- Extend monitoring if patient requires ≥ 2 doses of IM epinephrine OR IV epinephrine
- ICU admission for patients needing advanced airway, mechanical ventilation, and/or vasopressor support
- Prior to discharge:
- Alert bracelet and allergy documentation (if trigger is identified)
- Patient counseling on identification and avoidance of triggers
- Prescription and training on epinephrine autoinjector use
- Consider allergy/Immunology referral (e.g., anaphylaxis due to Hymenoptera stings)
Differential diagnoses
| Differential diagnoses of anaphylaxis [5] | |
|---|---|
| Symptom clusters | Conditions |
| Multisystem involvement |
|
| Acute upper airway obstruction/stridor |
|
| Acute respiratory distress/wheezing [5] |
|
| Loss of consciousness |
|
| Hypotension |
|
| Skin rash/flushing |
|
The differential diagnoses listed here are not exhaustive.
Complications
-
Biphasic anaphylactic reactions [4][14][15]
- Definition: recurrence of anaphylaxis symptoms despite initially successful treatment and without re-exposure to an antigen
- Frequency: occurs in 5–20% of patients with anaphylaxis
- Onset: typically 6–24 hours after treatment
- Not prevented by corticosteroids
-
Respiratory failure, cardiac arrest, death
-
Risk factors include: [2][3]
- Delayed administration of epinephrine
- Improper patient positioning
- History of peanut/tree nut allergy, previous severe/near-fatal anaphylaxis, previous biphasic reaction
- Comorbidities: asthma, cardiovascular disease, mast-cell activation disease (e.g., mastocytosis)
-
Risk factors include: [2][3]
- Drug side effects
- Complications of intubation or ventilation strategies
We list the most important complications. The selection is not exhaustive.
Prevention
Pretreatment for in-hospital triggers [16][17][18]
- Consider corticosteroid and/or antihistamine pretreatment if known triggers are crucial to clinical care and difficult to avoid: e.g., radiocontrast material (most common), chemotherapeutic agents, blood products, antivenom.
- Regimens vary by institution and indication. [18]
External Resources
References
- Campbell RL, Li JTC, Nicklas RA, Sadosty AT. "Emergency department diagnosis and treatment of anaphylaxis: a practice parameter". Ann Allergy Asthma Immunol. 113(6). :599-608. (2014)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Hariri G, Joffre J, Leblanc G, et al. "Narrative review: clinical assessment of peripheral tissue perfusion in septic shock". Annals of Intensive Care. 9(1). (2019)
- Anagnostou K, Turner PJ. "Myths, facts and controversies in the diagnosis and management of anaphylaxis". Arch Dis Child. 104(1). :83-90. (2018)
- Loprinzi Brauer, et al. "Prospective Validation of the NIAID/FAAN Criteria for Emergency Department Diagnosis of Anaphylaxis". JACI: In Practice. 4(6). (2016)
- Davenport MS, Cohan RH. "The Evidence for and Against Corticosteroid Prophylaxis in At-Risk Patients". Radiol Clin North Am. 55(2). :413-421. (2017)
- International Collaborative Study of Severe Anaphylaxis.. "Risk of anaphylaxis in a hospital population in relation to the use of various drugs: an international study.". Pharmacoepidemiol Drug Saf. 12(3). :195-202. (2003)
- O’Malley RB, Cohan RH, Ellis JH, et al. "A Survey on the Use of Premedication Prior to Iodinated and Gadolinium-Based Contrast Material Administration". Journal of the American College of Radiology. 8(5). :345-354. (2011)
- Ring J, Beyer K, Biedermann T, et al. "Guideline for acute therapy and management of anaphylaxis". Allergo Journal International. 23(3). :96-112. (2014)
- Lieberman P, Nicklas RA, Randolph C, et al. "Anaphylaxis—a practice parameter update 2015". Annals of Allergy, Asthma & Immunology. 115(5). :341-384. (2015)
- Tupper J, Visser S. "Anaphylaxis: A review and update.". Can Fam Physician. 56(10). :1009-11. (2010)
- Alqurashi W, Ellis AK. "Do Corticosteroids Prevent Biphasic Anaphylaxis?". The Journal of Allergy and Clinical Immunology: In Practice. 5(5). :1194-1205. (2017)
- Sheridan E, Curnyn D, Fellers A, McNace L. "Are H2 blockers effective for acute allergic reactions?". Evidence-Based Practice. 22(4). :32-32. (2019)
- Świeczkowski D, Zdanowski S, Merks P, et al. "The plague of unexpected drug recalls and the pandemic of falsified medications in cardiovascular medicine as a threat to patient safety and global public health: A brief review.". Cardiology journal. 29(1). :133-139. (2022)
- Fedorowicz Z, van Zuuren EJ, Hu N. "Histamine H2-receptor antagonists for urticaria". Cochrane Database of Systematic Reviews. (2012)
- Long B, Koyfman A, Gottlieb M. "Evaluation and Management of Angioedema in the Emergency Department". Western Journal of Emergency Medicine. 20(4). :587-600. (2019)
- Moellman JJ, Bernstein JA, Lindsell C, et al. "A Consensus Parameter for the Evaluation and Management of Angioedema in the Emergency Department". Academic Emergency Medicine. 21(4). :469-484. (2014)
- "Contributor Disclosures - Anaphylaxis. All of the relevant financial relationships listed for the following individuals have been mitigated: Luisa Voßbeck (medical editor, was employed by GÖK Consulting GmbH through Aug 2020); Jan Schlebes (medical editor, is a shareholder in Novo Nordisk, and was a shareholder in Fresenius SE & Co KGaA through Nov 2024). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy"
- Pollak AN, Murphy M, Stathers CL et al. "Critical Care Transport". Jones and Bartlett Publishers. (2011). ISBN: 9780763712235
- Campbell RL, Kelso JM. "Anaphylaxis: Acute diagnosis". UpToDate. UpToDate. https://www.uptodate.com/contents/anaphylaxis-acute-diagnosis. [2016-07-25]
- Campbell RL, Kelso JM. "Anaphylaxis: Emergency treatment". UpToDate. UpToDate. http://www.uptodate.com/contents/anaphylaxis-emergency-treatment. [2016-07-21]
- Kemp SF. "Pathophysiology of anaphylaxis". UpToDate. UpToDate. https://www.uptodate.com/contents/pathophysiology-of-anaphylaxis. [2017-02-23]
- Mustafa SS, Kaliner MA. "Anaphylaxis". WebMD. http://emedicine.medscape.com/article/135065. [2017-02-22]
- Lewis SR, Butler AR, Parker J, et al. "Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation: a Cochrane Systematic Review". Br J Anaesth. 119(3). :369-383. (2017)
- Apfelbaum JL, Hagberg CA, Caplan RA, et al. "Practice Guidelines for Management of the Difficult Airway". Anesthesiology. 118(2). :251-270. (2013)
- De Backer D, Fagnoul D. "Intensive Care Ultrasound: VI. Fluid Responsiveness and Shock Assessment". Annals of the American Thoracic Society. 11(1). :129-136. (2014)
- Bakker J, Nijsten MW, Jansen TC. "Clinical use of lactate monitoring in critically ill patients". Annals of Intensive Care. 3(1). :12. (2013)