Summary
Ankle fractures are the most common fractures of the lower extremity and most often result from twisting the ankle. Clinical features include ankle pain and decreased range of motion. If the patient history and physical examination are both consistent with a fracture (e.g., the patient is unable to bear weight on the affected leg), an x-ray is performed. The most important diagnostic consideration is whether the fracture is stable (e.g., isolated malleolar fractures) or unstable (e.g., bimalleolar fracture). Unstable fractures require surgery, whereas stable ones can be treated conservatively with a short leg cast.
Etiology
- Eversion or inversion injury
- Direct trauma
- Crush injury
- Axial loading (e.g., fall from a height, motor vehicle collision)
Classification
Types of ankle fractures [1]
- Lateral malleolar fracture
- Medial malleolar fracture
- Posterior malleolar fracture
- Bimalleolar fracture: fractures of the lateral and medial malleoli
- Trimalleolar fracture: fractures of the lateral, medial, and posterior malleoli
- Pilon fracture: fracture of the distal tibia involving the articular surface of the talocrural joint
- Maisonneuve fracture: fracture of the proximal fibula associated with disruption of the distal tibiofibular syndesmosis and medial malleolar injury (i.e., medial malleolar fracture, deltoid ligament rupture) [2]
- Other: Volkmann triangle refers to an avulsion fracture of the posterolateral tibial lip
")
")

")
Ankle fracture stability [3]
The ankle becomes increasingly unstable with worsening severity of injury. Generally, fractures at two or more sites are unstable.
- Usually stable: isolated lateral malleolar fracture or isolated medial malleolar fracture
- Usually unstable: posterior malleolar fracture, bimalleolar fracture, Maisonneuve fracture
- Always unstable: trimalleolar fracture, pilon fracture
Weber classification of ankle fractures [1]
The Weber classification categorizes ankle fractures according to the level of the fibular fracture in relation to the distal tibiofibular syndesmosis.
-
Weber A: lateral malleolar fracture below the syndesmosis
- Intact syndesmosis and deltoid ligament
- Possible medial malleolar fracture
- Usually stable
-
Weber B: fibular fracture at the level of the syndesmosis
- Possible syndesmotic injury and/or deltoid ligament injury
- Variable stability
-
Weber C: fibular fracture above the syndesmosis
- Ruptured syndesmosis, torn interosseous membrane
- Medial malleolus fracture and/or deltoid ligament tear
- Unstable
Maisonneuve fractures are considered Weber C fractures. [1]


X-ray ankle (left; AP view)
A transverse fracture of the medial malleolus (dashed white line) is seen along with a comminuted fracture of the distal fibula (green outlines) at the level of the ankle syndesmosis (Weber B fracture; blue overlay). The ankle mortise is disrupted, with lateral displacement of both the talus (yellow overlay) and the tibial fragment (red overlay) in relation to the tibial shaft.
Red outline: distal tibia
Source: © IMPP

X-ray ankle (left; lateral view)
A comminuted fracture of the distal fibula (green overlay) is well seen on this view, including a posterior fragment projected over the distal tibia (red outline) on the AP view. There is no fracture of the posterior aspect of the tibial plafond (posterior malleolus) as would be expected in a trimalleolar fracture. The shape of the talus (yellow overlay and dashed line) appears abnormal, consistent with its displacement on the AP view.
Red line: distal tibia
Source: © IMPP

X-ray ankle (right; AP view) after supination-external rotation injury
An oblique fracture of the distal fibula (yellow overlay and red line) is accompanied by an avulsion fracture (red lines) of the medial malleolus (green overlay). The ankle mortise has been disrupted. There is widening of the medial compartment (indicated by white arrow) and lateral displacement of the talus (indicated by a black arrow). A lateral view (not included here) showed a fracture of the posterior malleolus.
The findings indicate an unstable trimalleolar fracture that requires operative treatment. If classified based on the location of the fibular fracture (Danis-Weber classification), this would be a Weber type B injury.
Source: “Before. in: Trimalleolar Ankle Fracture Xray shown before surgery and after surgery to put in a plate and screws” by Chaim Mintz, Wikimedia Foundation, licensed under CC BY-SA 3.0. Modifications: Cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

X-ray of the right ankle, lateral view
Disruption of the dorsal distal cortical bone indicating an avulsion fracture of the dorsal tibial margin (Volkmann's triangle).
Source: © IMPP
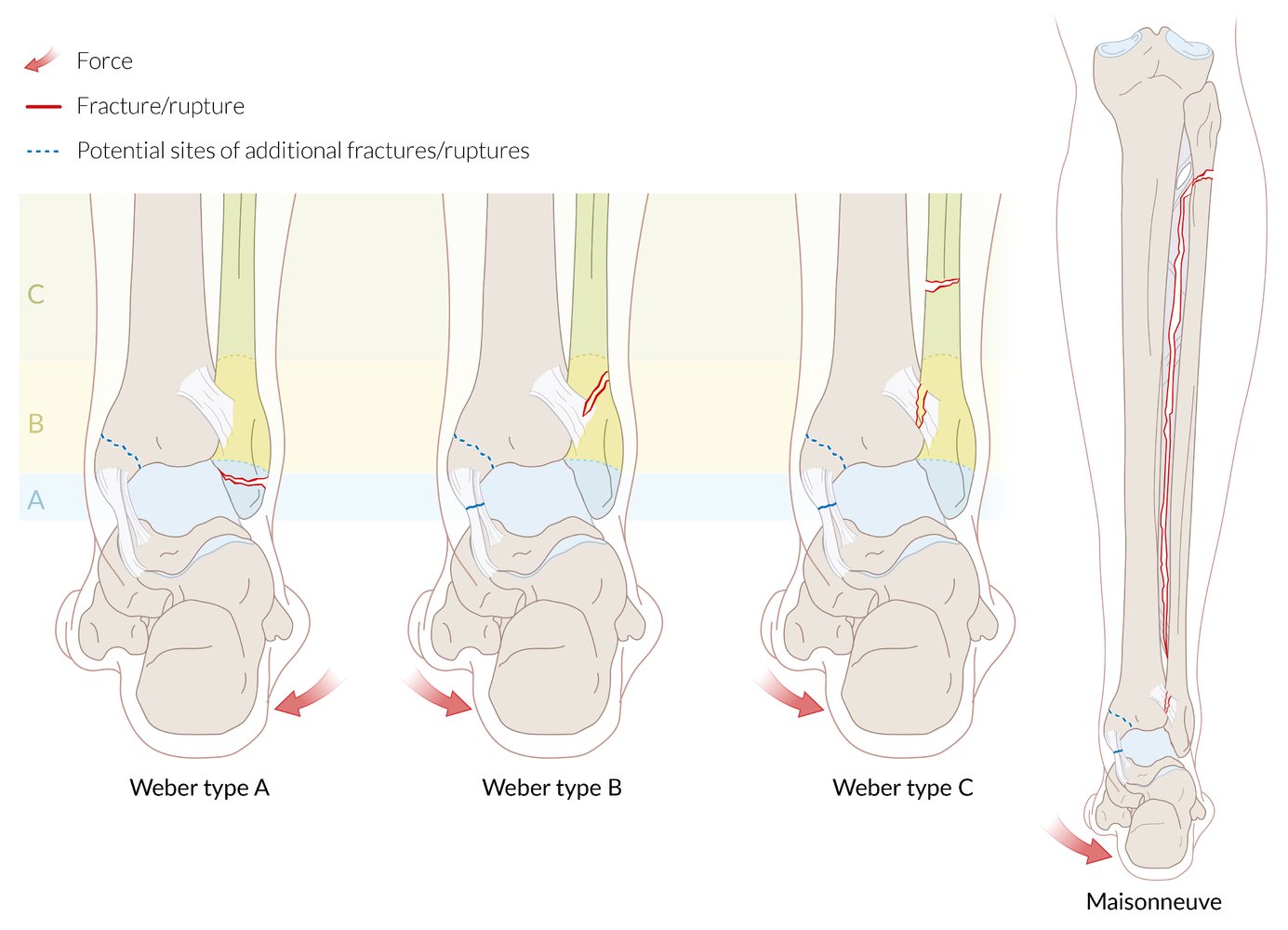
Weber A: fracture of the lateral malleolus below the syndesmosis (intact syndesmosis)
Weber B: fracture of the lateral malleolus at the level of the syndesmosis (possible syndesmotic injury)
Weber C: fracture of the lateral malleolus above the syndesmosis (ruptured syndesmosis, torn interosseous membrane)
Maisonneuve fracture: proximal subcapital Weber C fracture; rupture of the syndesmosis (definite lesions in red); medial malleolus fracture and/or deltoid ligament tear (possible lesions in blue)
© AMBOSS
Clinical features
- Local pain, swelling and hematoma
- Tenderness, especially in the area of the malleoli, the syndesmosis, and the posterior aspect of the ankle joint
- Restricted range of movement
- Skin abnormalities (lacerations, discolorations, tenting, or blistering)
- If separation of the ankle mortise elements occurs: lateral displacement of the foot
- In some cases, accompanying injury (e.g., fracture of the proximal fibula, knee, or foot)


Part of the distal tibia can be seen protruding from the wound at the medial malleolus.
Source: © IMPP
Diagnosis
Clinical evaluation [1]
Perform the following prior to imaging as abnormalities can affect urgent management (see “Approach” in “Treatment”):
-
Neurovascular exam
- Assess dorsalis pedis and posterior tibial artery pulses and distal capillary refill time.
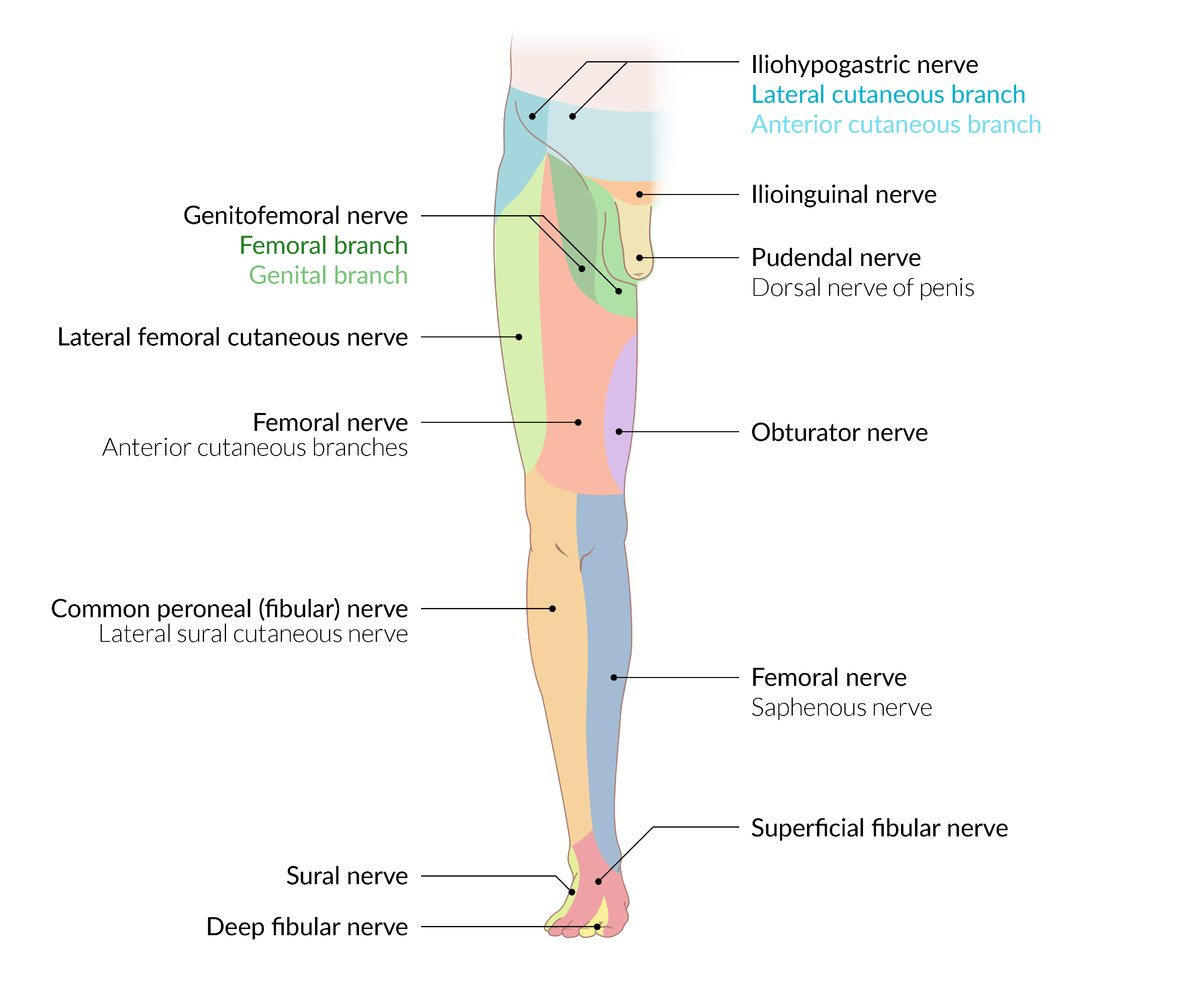
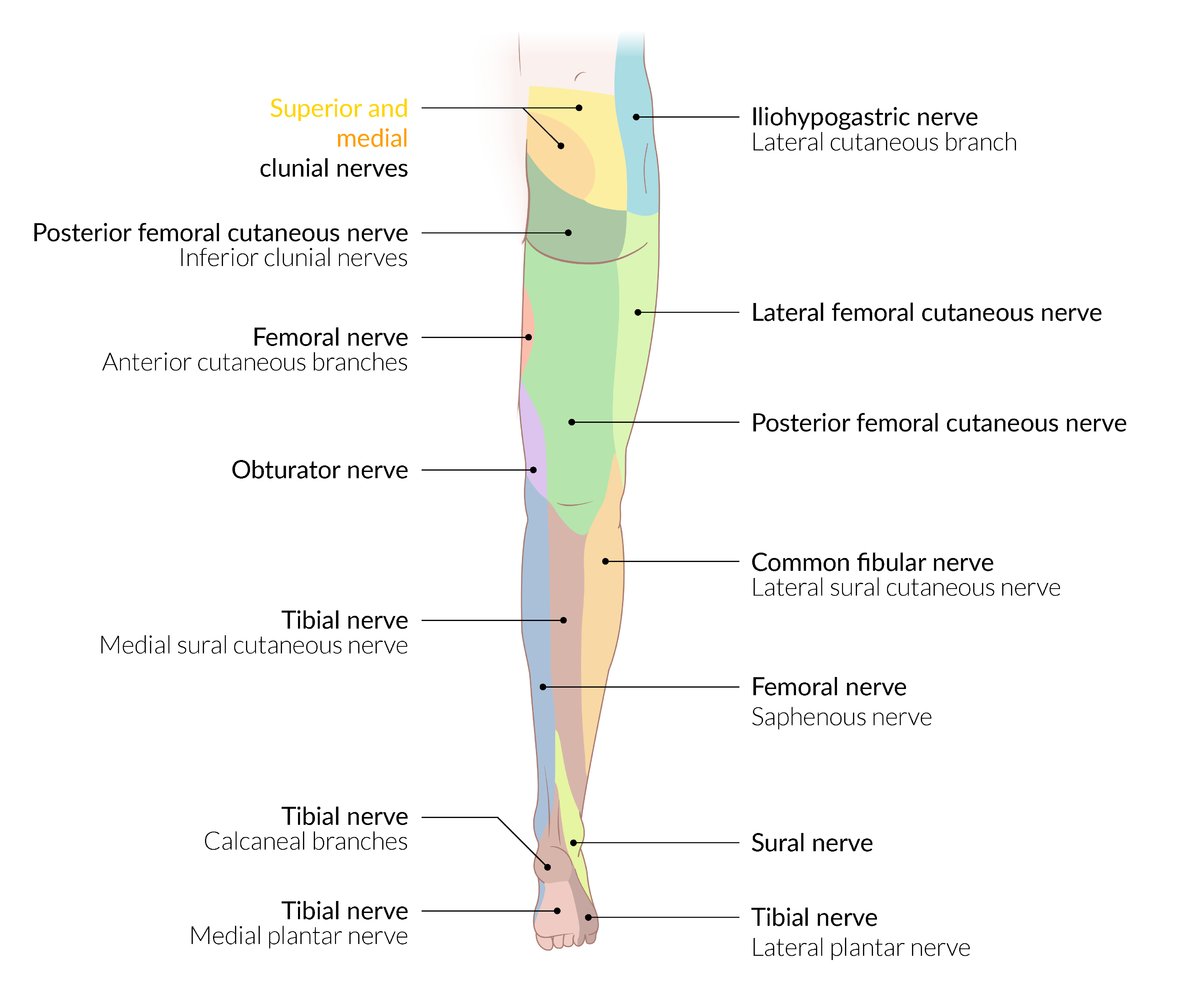
- Examine motor and sensory function of the lower leg (see “Sural nerve injury”, “Tibial nerve injury”, and “Peroneal nerve injury”).
- Skin exam: Evaluate for laceration, tearing, and tenting.
- Associated injuries: Examine the foot and knee.
Examine the entire length of the fibula in patients with ankle pain to evaluate for a Maisonneuve fracture. [1]
")
")
Ottawa ankle and foot rules [4][5]
These criteria are used to determine the need for X-rays in patients presenting to the emergency department (ED) with traumatic ankle and/or foot injuries. [4][5]
-
Ankle x-rays are indicated for pain in the malleolar region PLUS any of the following:
-
Tenderness along the posterior distal 6 cm of the:
- Lateral malleolus
- OR medial malleolus
- Inability to weight-bear both immediately post-injury AND for at least 4 steps in the ED
-
Tenderness along the posterior distal 6 cm of the:
-
Foot x-rays are indicated for pain in the midfoot region PLUS any of the following:
-
Tenderness at the:
- Base of the 5th metatarsal
- OR the navicular bone
- Inability to weight-bear both immediately post-injury AND for at least 4 steps in the ED
-
Tenderness at the:


X-ray [1]
-
3-view plain ankle x-ray: anteroposterior (AP): , lateral and mortise (oblique) views
- Evaluate for radiographic fracture signs, displacement, and dislocation.
- Compare joint spaces between the talus and medial malleolus, talus and lateral malleolus, and talus and tibial plafond.
- Evaluate the ring-like structure surrounding the talus.
- Tibia fibula x-ray: AP and lateral views to evaluate for pilon or Maisonneuve fracture



")
")
Advanced imaging [1]
- CT: may be obtained for inconclusive x-rays or preoperative planning
- MRI: may be indicated for diagnosis of associated tendon/ligament injuries
© AMBOSS
© AMBOSS
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
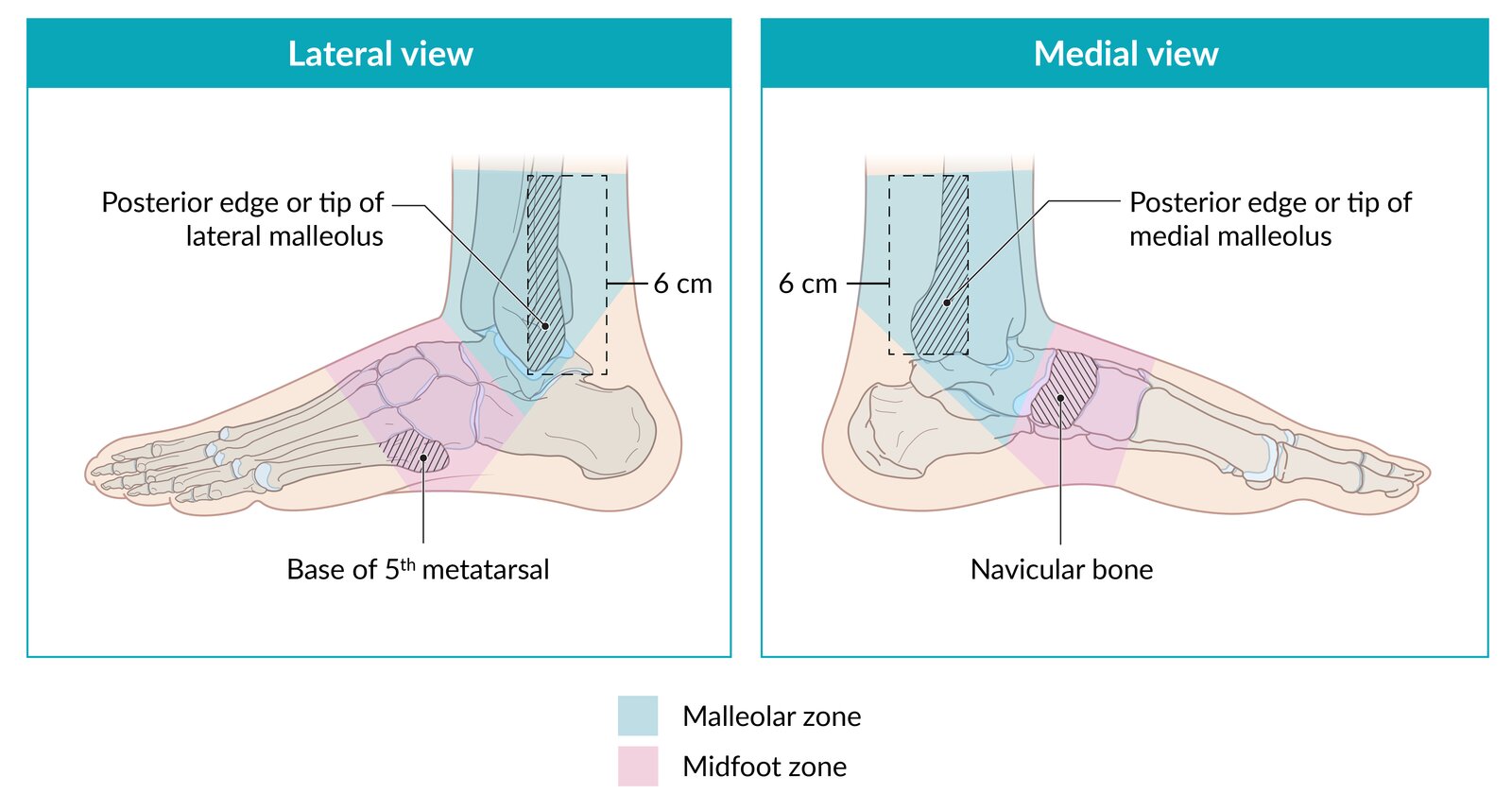
The Ottawa ankle and foot rules apply to patients presenting to the emergency department (ED) with traumatic ankle and/or foot injuries.
Ankle x-rays are indicated in the presence of pain in the malleolar zone AND one or both of the following:
- Tenderness along the posterior distal 6 cm of the lateral OR medial malleolus
- Inability to weight-bear both immediately post-injury AND for at least 4 steps in the ED
Foot x-rays are indicated in the presence of pain in the midfoot zone AND one or both of the following:
- Tenderness at the base of the 5th metatarsal OR the navicular bone
- Inability to weight-bear both immediately post-injury AND for at least 4 steps in the ED
© AMBOSS

X-ray (posteroanterior) of the right upper ankle: fibula fracture (fracture gap is marked by a green line) at the level of the syndesmosis (S). This finding indicates a Weber B fracture.
Source: © IMPP

X-ray of the right upper ankle (lateral view): a fibula fracture (the fracture gap is marked with a line) at the level of the syndesmosis (S). Diagnosis: Weber B fracture.
Source: © IMPP

X-ray of the right upper ankle (AP view): The distance between the distal tibia and the fibula is increased. Diagnosis: syndesmosis rupture and ankle mortise separation.
Source: © IMPP

X-ray right knee (AP view)
An oblique fracture (red overlay) of the proximal fibula (Fi) shows slight medial displacement of the distal fragment. Lateral subluxation of the fibula at the tibiofibular joint and widening of the distance between tibia (T) and fibula (double arrow) indicate disruption of the tibiofibular ligaments.
Fe: femur
Source: © IMPP

X-ray right knee (lateral view)
The oblique proximal fibular fracture (red overlay) shows no appreciable anterior or posterior displacement of the distal fragment.
Fe: femur; Fi: fibula; T: tibia
Source: © IMPP
Differential diagnoses
- Ankle sprain
- Foot fracture
- Stress fracture
- Tarsal tunnel syndrome
- Arthritis (e.g., osteoarthritis, gout, pseudogout, septic arthritis)
- Achilles tendon rupture
- Charcot joint
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [1]
- Immobilization and disposition: depends on fracture type and classification (See “Overview of ankle fracture management.”)
- Weight-bearing: Most ankle fractures are non-weight-bearing (NWB) except for isolated Weber A fractures which can be weight-bearing as tolerated (WBAT).
-
Urgent interventions
- Perform emergency fracture reduction if there is gross deformity with skin tenting or neurovascular compromise.
- Administer empiric IV antibiotics for open fractures without delay.
- Assess for other reasons for urgent orthopedic consultation for fractures.
Stable, isolated, nondisplaced fractures can be initially managed with immobilization and orthopedic follow-up within 48 hours.
Repeat the neurovascular exam after reduction and again after immobilization.
Overview [1]
| Overview of ankle fracture management [1] | ||||
|---|---|---|---|---|
| Fracture type | Initial immobilization | Weight-bearing status | Disposition | |
| Isolated lateral malleolus | Weber A | Walking boot | WBAT | Orthopedic follow-up within 48 hours |
| Weber B or Weber C | Posterior short-leg splint or CAM boot | NWB | Urgent orthopedics consult OR orthopedic follow-up within 48 hours | |
| Isolated medial malleolus | Posterior short-leg splint or walking boot | Orthopedic follow-up within 48 hours | ||
| Isolated posterior malleolus | Posterior short-leg splint with or without stirrup splint | |||
| Bimalleolar fracture | Urgent orthopedics consult OR orthopedic follow-up within 48 hours | |||
| Trimalleolar fracture | Urgent orthopedics consult | |||
| Pilon fracture | ||||
| Maisonneuve fracture | Posterior long-leg splint | Urgent orthopedics consult OR orthopedic follow-up within 48 hours | ||
Conservative treatment [1]
See “Conservative treatment of fractures” for further details.
- Indications: stable, closed, isolated malleollar fractures
- Definitive management: short leg cast or walking boot for 4–6 weeks
Surgical treatment [1]
-
Indications
- Unstable fractures (e.g., displaced fractures); See “Classification” for other types of unstable fractures.
- Open fractures
-
Definitive management
- Open reduction and internal fixation
- External fixation
")
")
")
")

X-ray right ankle (AP view)
Plate and screw fixation of the fibula (F) was performed, with good anatomic alignment of previous fracture fragments. A syndesmotic screw (blue overlay) connecting the fibula to the tibia (T) was placed to immobilize the syndesmotic injury during the healing process.
Surgical clips (green overlay) are seen and there is some irregularity of the skin surface (red overlay), which may be due to overlying clothing or bandaging rather than injury.
Source: © IMPP

X-ray right ankle (lateral view)
Plate and screw fixation of the fibula was performed, with good anatomic alignment of previous fracture fragments. A healing deformity (yellow overlay) of the posterior malleolus is seen. A syndesmotic screw (blue overlay) connecting the fibula to the tibia was placed to immobilize the syndesmotic injury during the healing process.
Surgical clips (green overlay) are seen and there is some irregularity of the skin surface (red overlay) likely due to overlying bandaging.
Black dashed outline: fibula; black arrowheads: vascular calcification
Source: © IMPP

X-ray ankle (left; mortise view)
Two screws traverse a previous fracture of the medial malleolus. Plate and screw fixation of the lateral malleolar fracture has also been performed. The fracture lines are no longer clearly visible.
Source: “Prä-OP 1” by Bluesharpkoenig, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

X-ray ankle (left; mortise view)
The distal fibula and medial malleolus show multiple lucent defects at sites of prior hardware (green overlay).
Source: “Post-OP 1” by Bluesharpkoenig, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Complications
- General complications of fractures
- Damage to the peroneal nerve or saphenous nerve
- Posttraumatic osteoarthritis
We list the most important complications. The selection is not exhaustive.
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Dietrich G, Prod’homme M, Müller J, Ballhausen T, Helfer L. "Conservative management of a specific subtype of Maisonneuve fractures: a report of two cases". AME Case Reports. 6. :17-17. (2022)
- Lampridis V, Gougoulias N, Sakellariou A. "Stability in ankle fractures". EFORT Open Reviews. 3(5). :294-303. (2018)
- Stiell IG. "Decision Rules for the Use of Radiography in Acute Ankle Injuries". JAMA. 269(9). :1127. (1993)
- Bachmann LM. "Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review". BMJ. 326(7386). :417-417. (2003)
- "Ankle radiograph (an approach)". https://radiopaedia.org/articles/ankle-radiograph-an-approach. [2016-01-01]