Summary
Structural anomalies of the female genital tract may be present at birth or may be acquired later in life. Common congenital anomalies of the female genital tract are anomalies of Müllerian duct fusion and an imperforate hymen. Impaired fusion of the Müllerian ducts can result in duplication of the uterus, cervix, and/or vagina, while incomplete fusion results in an intrauterine and/or intravaginal septum. Rarely, the Müllerian duct may be completely absent (Müllerian agenesis), resulting in the absence of the uterus, cervix, and vagina. Acquired structural anomalies include intrauterine adhesions and labial adhesions. Intrauterine adhesions occur following uterine curettage or as a result of pelvic inflammatory disease. Labial adhesions are the result of estrogen deficiency during childhood. Most patients with structural anomalies of the female genital tract remain asymptomatic until puberty. Intrauterine adhesions present with secondary amenorrhea, while Müllerian agenesis and imperforate hymen present with primary amenorrhea. Infertility may be the initial symptom in all structural anomalies of the genital tract. Structural anomalies of the uterus and cervix are diagnosed with imaging such as transvaginal ultrasonography. Surgical reconstruction or resection is the main treatment for both the congenital and acquired genital tract anomalies. Labial adhesions are a primarily clinical diagnosis, and are treated with topical estrogen.
Anomalies of the uterus
Anomalies of Müllerian duct fusion
- Incidence: 3–4/100 female individuals
-
Pathophysiology
- Defective fusion of the Müllerian ducts during embryonal development
- Normally functioning gonads and female karyotype → normal development of secondary sexual characteristics (e.g., breast, pubic hair development)
| Anomalies of Müllerian duct fusion [1] | ||
|---|---|---|
| Types of fusion anomalies | Relative frequency | Pathophysiology |
| Müllerian agenesis |
|
|
| Unicornuate uterus |
|
|
| Didelphic uterus |
|
|
| Bicornuate uterus |
|
|
| Septate uterus |
|
|
| DES-related abnormality |
|
|
-
Clinical features
- Asymptomatic before puberty
- Infertility and dyspareunia
- In some cases, periodic lower abdominal pain
-
Menorrhagia
- Müllerian agenesis: primary amenorrhea in a female individual with fully-developed secondary sexual characteristics
- Increased risk of the following obstetric complications:
- Cervical incompetence
- Ectopic pregnancy
- Preterm labor
- Malpresentation
- Obstructed or prolonged labor
- Retained placenta → postpartum hemorrhage
- Recurrent midtrimester abortions
- Associated with urological complications; (e.g., renal agenesis, pelvic kidney, horseshoe kidney) and skeletal malformations (e.g., cervicothoracic somite dysplasia)
-
Diagnostics
-
Screening tests
- Transvaginal or abdominal ultrasound
- Hysterosalpingography
- Confirmatory test: MRI
- Renal ultrasound should be performed in all patients to screen for renal abnormalities. [2]
-
Screening tests
-
Treatment
- Surgical treatment is usually not recommended in the following situations:
- Another treatable cause of infertility co-exists
- The woman is asymptomatic
- Metroplasty: reconstruction of the uterus
- Septoplasty: a type of metroplasty that only involves resection of the septum in a separate uterus
- Surgical treatment is usually not recommended in the following situations:
In patients with infertility and congenital uterine anomalies, it is important to rule out other causes of infertility before surgical therapy is considered.
The mere presence of a Müllerian duct anomaly does not necessitate surgical therapy.


")



Intrauterine adhesions (Asherman syndrome)
- Definition: endometrial adhesions or fibrosis
-
Etiology
- Following uterine dilation or curettage (most common cause)
- Postinflammatory (e.g., chlamydia)
- Pathophysiology: uterine dilation or curettage → endometrial basal layer damage
-
Clinical features
- Usually asymptomatic
- Abnormal uterine bleeding
- Secondary amenorrhea
- Infertility
- Recurrent pregnancy loss
- Periodic abdominal pain
-
Diagnostics [3]
- Negative progesterone withdrawal test: No bleeding after progesterone cessation suggests blockage of the outflow tract.
- Confirmatory test: hysteroscopy to directly visualize adhesions
- Hysterosalpingography: honeycomb appearance of the uterus
-
Treatment
- Hysteroscopic resection of the adhesions
- Treatment is only indicated if patients are symptomatic.
Individuals with Asherman syndrome have intrauterine Adhesions.
References:[4][5][6]
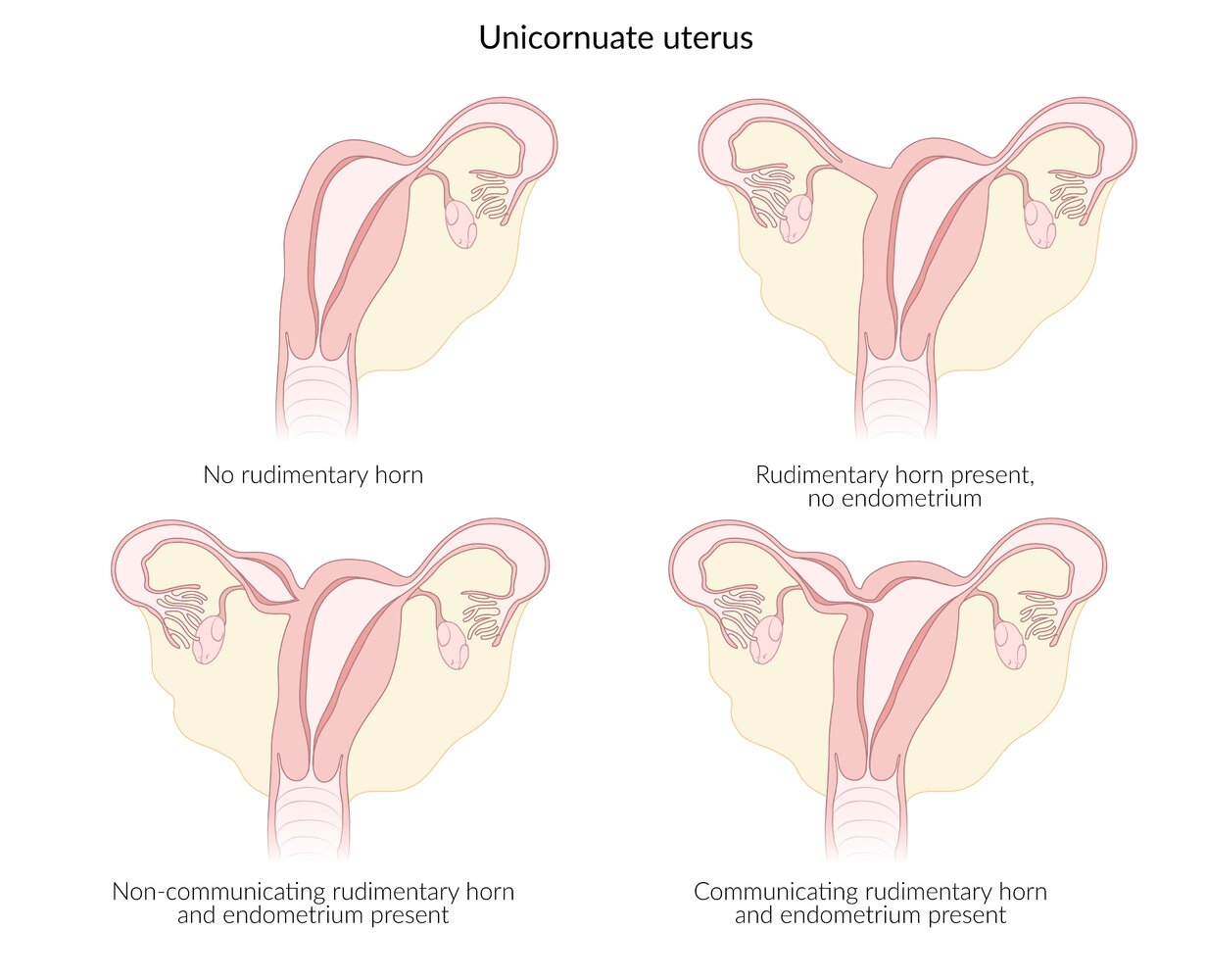
Various types of unicornuate uteri
A unicornuate uterus is caused by complete or partial anaplasia of the Mullerian duct during embryonic development. In many cases (> 70%) a second, rudimentary horn (which may feature functional endometrial tissue) is present. The rudimentary horn usually does not communicate with the fully developed horn.
© AMBOSS
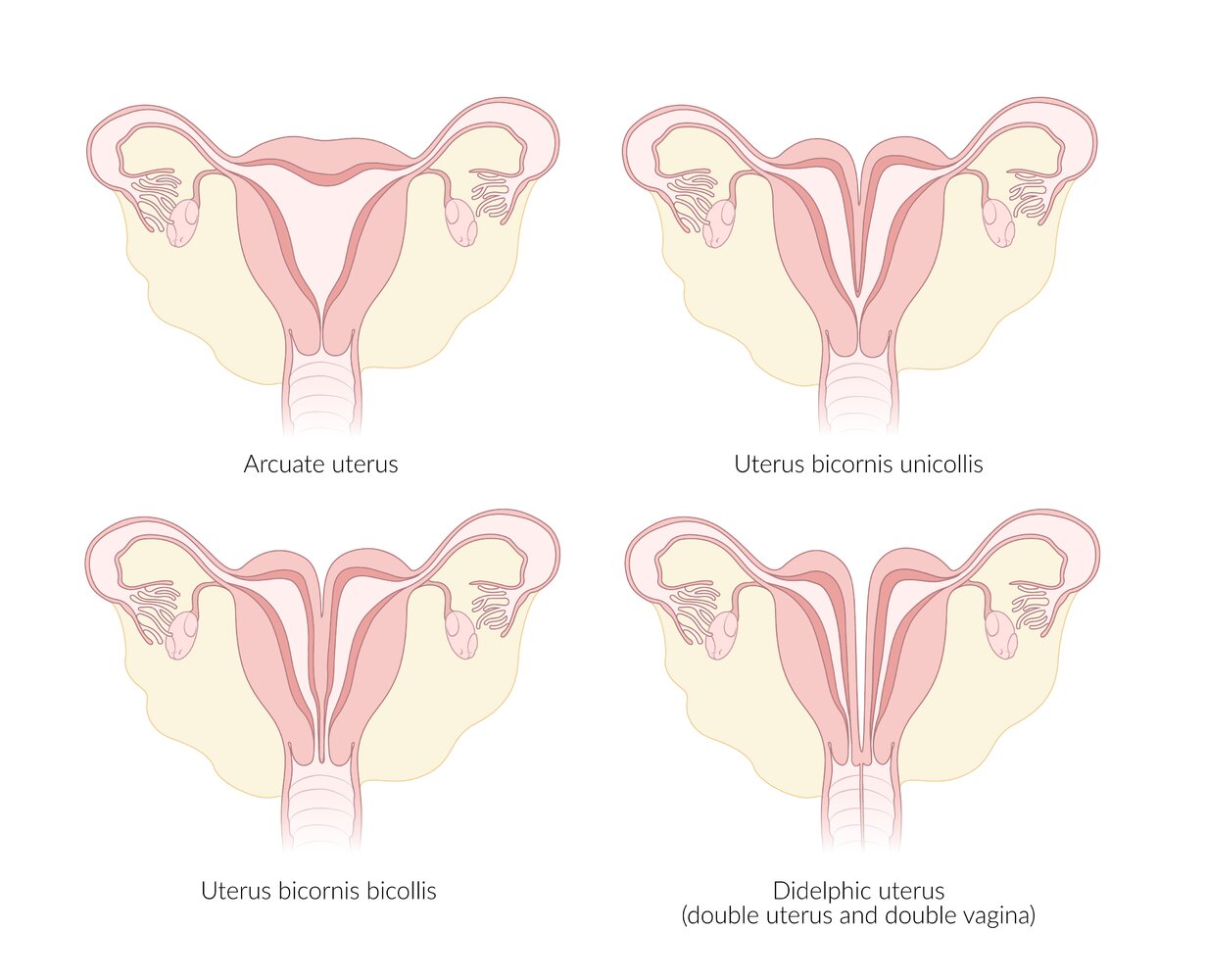
Anomalies that arise from the defective fusion of the Müllerian ducts during embryonal development
© AMBOSS

Sonograph of a bicornuate uterus (U) of a pregnant women in the first trimester
F: fetus; incomplete fusion of the uterine horns; CD: cornu dextrum/right horn; CS: cornu sinistrum/left horn
The placenta is attached to the posterior wall of the uterus.
© AMBOSS

Source: "Bicornuate Uterus.jpg", Ed Uthman, Wikipedia licensed under Public Domain
{kind=link}
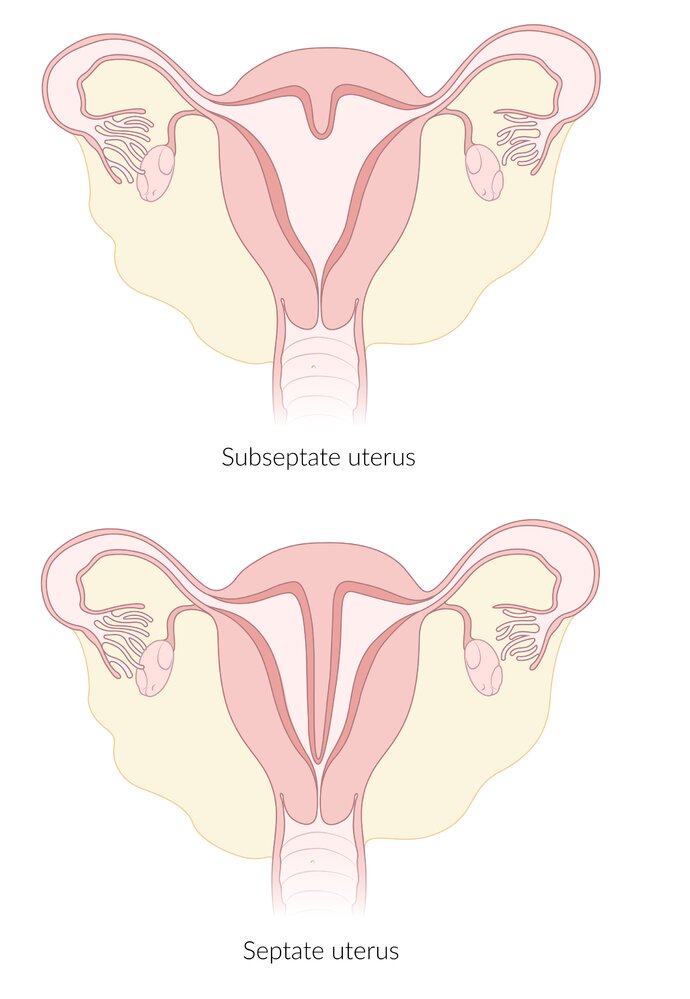
Overview of uterine deformities resulting from complete fusion of the Mullerian ducts with concomitant incomplete resorption of the uterine septum.
© AMBOSS
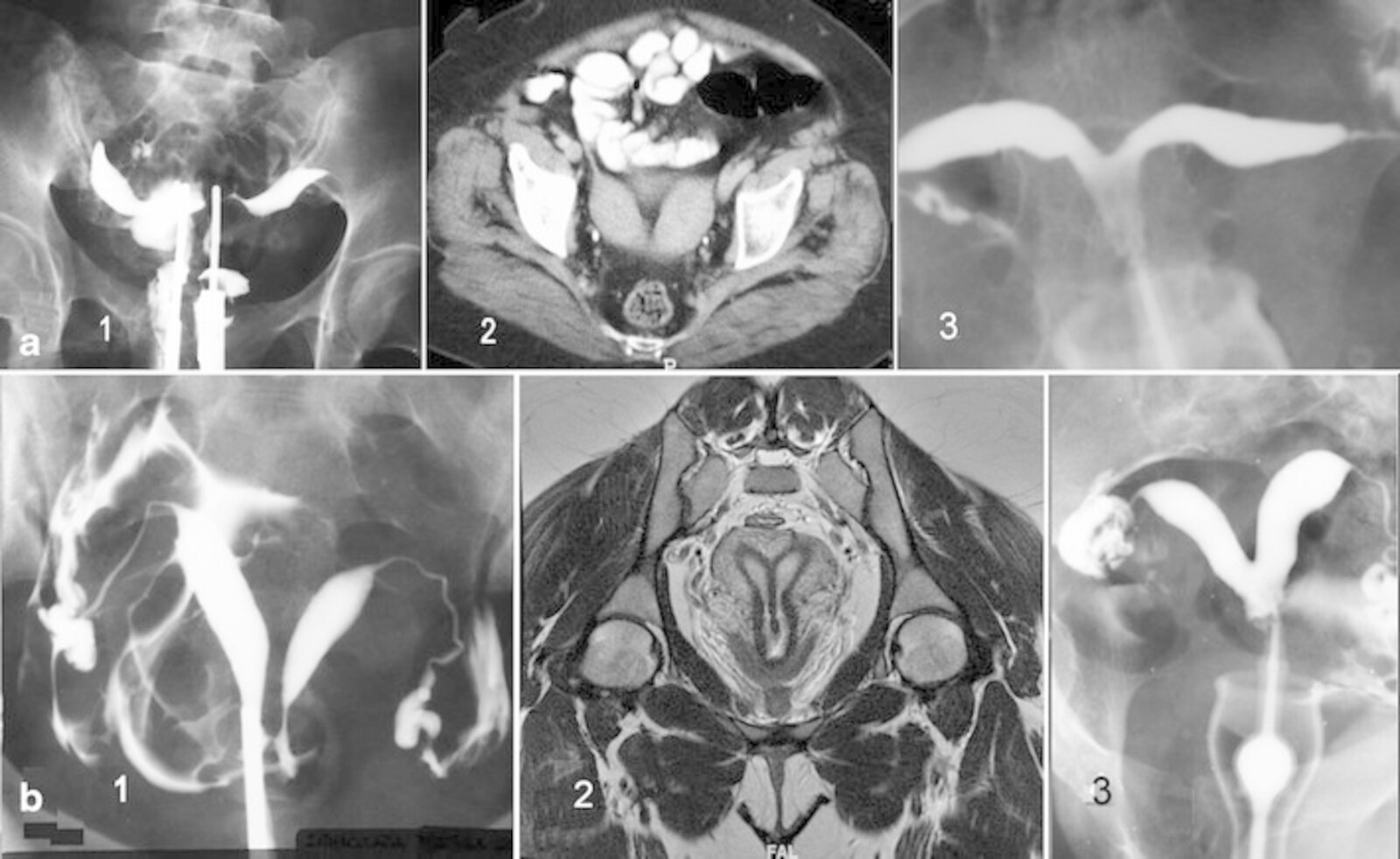
(a1) Hysterosalpingography (HSG): didelphys uterus
(a2) CT; axial plane: bicornuate uterus
(a3) HSG: bicornis-unicollis uterus
(b1) HSG: complete septate uterus and communicating septate uterus
(b2) MRI; T-2 weighted; coronal plane: septate uterus and cervix with single external os
(b3) HSG: subseptate uterus
Source: “Figure 6, in: Diagnostic imaging and cataloguing of female genital malformations” by Pedro Acién & Maribel Acién, Springer Link, licensed under CC BY 4.0.
Anomalies of the vagina
Agenesis of the upper vagina
- Definition: a condition in which the vagina is abnormally closed or absent
- Epidemiology: 1/5000 female individuals [7]
- Etiology: Müllerian agenesis
-
Pathophysiology
- Agenesis or hypoplasia of the Müllerian duct → atresia of the upper-third of the vagina
- Normally functioning gonads and female karyotype → normal development of secondary sexual characteristics (e.g., breast, pubic hair development)
- Associated anomalies
- Absent or malformed uterus and cervix (in almost all cases)
- Urological malformations (25–50% of cases): single kidney, pelvic kidney, horseshoe kidney
- Skeletal malformations (10–15% of cases)
-
Clinical features
- Asymptomatic before puberty
- Primary amenorrhea
- Infertility
- Dyspareunia
- Perineal examination: vaginal dimple and a hymenal fringe
-
Diagnostics
- Normal levels of LH, FSH, prolactin, estradiol, and testosterone
-
Ultrasound
- Absent or malformed uterus (e.g., hemiuterus, rudimentary uterus)
- Normal ovaries
- Possible associated malformations of the kidneys or urinary tract
- MRI to determine if functional endometrium is present
- Treatment: vaginoplasty
Agenesis of the lower vagina
- Etiology: abnormal development of the sinovaginal bulbs and vaginal plate
-
Clinical features
- Primary amenorrhea
- Cyclic pelvic pain
-
Diagnostics
- Vaginal dimple may be present on physical exam
- Palpable abdominal mass due to distention of the upper vagina
-
Confirmatory tests: ultrasound or MRI
- Normal ovaries, uterus, cervix, and upper vagina
- Measurement of the distance from introitus to obstruction
- Treatment: surgical pull-through procedure
Transverse vaginal septum
- Incidence: 1/70,000 female individuals
-
Pathophysiology
- Failure of recanalization of the Müllerian duct → transverse septum in the upper-third (45%), lower third (15–20%), and/or middle third (35–40%) of the vagina
- Associated with cervical hypoplasia or absence
- Cryptomenorrhea → hematocolpos
-
Clinical features
- Asymptomatic before puberty
- Primary amenorrhea
- Infertility
- Periodic lower abdominal pain
- Possibly, palpable lower abdominal mass
- Perineal examination: normal vulva and external genitalia
- Diagnostics: transvaginal ultrasonography or MRI
-
Treatment
- First-line: nonsurgical dilation over 6–12 months using graduated vaginal dilators
- Second-line: vaginoplasty
Imperforate hymen
An imperforate hymen is a congenital anomaly in which the hymen obstructs the opening to the vagina. [8]
Epidemiology
- Incidence: 1:1000–2000 individuals born with female genitalia [9][10]
Pathophysiology
Central cells of the Müllerian eminence in the urogenital sinus do not disintegrate → imperforate hymen → cryptomenorrhea at puberty (outflow tract obstruction leads to backup of menstrual blood) → hematocolpos; (accumulation of blood in the vagina) and/or hematometra (accumulation of blood in the uterus)
Clinical features [8][11]
- Neonates: a mass in the introitus (i.e., mucocolpos or hydrocolpos) may be visible due to accumulation of vaginal secretions after birth [10]
-
Pubertal individuals
- Primary amenorrhea
- Lower abdominal or pelvic pain: cyclic, acute, or constant
- Symptoms from mass effect , e.g.:
- Constipation and/or dyschezia
- Urinary retention, dysuria, and/or frequency
- Back pain [9]
-
Examination findings
- Possible palpable lower abdominal mass (due to hematometra)
- Tense, bulging, blue membrane in the vulva (due to hematocolpos)
- Tanner stages 4–5 for breast and pubic hair development [10]
Imperforate hymen may resolve spontaneously during puberty due to the effects of estrogen. [8]
Differential diagnoses [8][10]
- Other hymenal variants (e.g., microperforate, septate) [8]
- Distal vaginal atresia [8]
- Transverse vaginal septum, agenesis of the upper vagina, or cervical atresia [8]
- Urogenital sinus malformation
- Obstructed uterine horn
- Labial adhesions
Diagnosis [8][10]
- Make a preliminary clinical diagnosis based on physical examination. [8]
- Confirm diagnosis with pelvic ultrasonography.
- Transabdominal ultrasound is typically preferred over transvaginal ultrasound.
- Findings:
- Hematocolpos, hematometra
- Normal vaginal and uterine anatomy
- Diagnostic uncertainty: Perform MRI to exclude obstructive abnormalities of the internal reproductive tract (see "Differential diagnoses").
Treatment [8]
Refer all patients to gynecology.
-
Surgery: definitive treatment
- Timing: typically after onset of puberty [10][11]
- Technique: excision of the imperforate hymen (hymenectomy) and evacuation of the accumulated blood
-
Conservative management: Consider for symptom relief while awaiting definitive treatment.
- Indwelling urinary catheter for urinary retention
- Stool softeners
- Analgesia
- Menstrual suppression
Do not perform incision of an imperforate hymen with drainage of the associated hematocolpos, as there is an increased risk of complications (e.g., infection). [10][11]
Labial adhesions
- Definition: partial or complete adhesion of the labia minora
- Epidemiology: occurs in 2–5% of female individuals up to 4 years of age
-
Etiology:
- Absence of estrogen → predisposition to mild infection ; → local inflammation → raw surface epithelium of the labia minora → adhesions
- In rare cases: trauma (sexual abuse), congenital defect
-
Clinical features
- Usually asymptomatic
- If external urethral opening is obstructed: recurrent attacks of UTI, vaginitis, vestibulitis
-
Perineal examination
- A thin vertical midline fold in the perineum
- The labia, vaginal opening, and occasionally the urethral meatus are not visible.
- Diagnostics: : primarily clinical diagnosis
- Treatment: : application of topical estrogen
References
- American Fertility Society. "The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Müllerian anomalies and intrauterine adhesions". Fertil Steril. 49(6). :944-955. (1988)
- Committee on Adolescent Health Care. "ACOG Committee Opinion No. 728: Müllerian Agenesis: Diagnosis, Management, And Treatment". Obstet Gynecol. 131(1). :e35-e42. (2018)
- AAGL Elevating Gynecologic Surgery. "AAGL practice report: practice guidelines on intrauterine adhesions developed in collaboration with the European Society of Gynaecological Endoscopy (ESGE)". Gynecological surgery. 14(1). :6. (2017)
- Iverson RE Jr, DeCherney AH, Laufer MR. "Surgical management of congenital uterine anomalies". UpToDate. UpToDate. https://www.uptodate.com/contents/surgical-management-of-congenital-uterine-anomalies. [2016-04-13]
- Iverson RE Jr, DeCherney AH, Laufer MR. "Clinical manifestations and diagnosis of congenital anomalies of the uterus". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-congenital-anomalies-of-the-uterus?source=see_link. [2015-10-12]
- Cedars MI. "Intrauterine adhesions". UpToDate. UpToDate. http://www.uptodate.com/contents/intrauterine-adhesions. [2016-06-03]
- Herlin MK, Petersen MB, Brännström M. "Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome: a comprehensive update". Orphanet J Rare Dis. 15(1). (2020)
- ACOG. "Diagnosis and Management of Hymenal Variants". Obstet Gynecol. 133(6). :e372-e376. (2019)
- Lee K, Hong J, Jung H, et al. "Imperforate Hymen: A Comprehensive Systematic Review". Journal of Clinical Medicine. 8(1). :56. (2019)
- Hamouie A, Dietrich JE. "Imperforate Hymen: Clinical Pearls and Implications of Management". Clin Obstet Gynecol. 65(4). :699-707. (2022)
- ACOG. "Management of Acute Obstructive Uterovaginal Anomalies (reaffirmed 2021)". Obstet Gynecol. 133(6). :e363-e371. (2019)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Rao K. "Principles & Practice of Assisted Reproductive Technology". JP Medical Ltd. 1(1). (2013). ISBN: 9789350907368
- "Uterus". https://radiopaedia.org/articles/uterus
- Healey A. "Embryology of the Female Reproductive Tract". Springer Berlin Heidelberg. (2010). ISBN: 9783540856016