Summary
Anorectal abscesses are acute purulent collections in the perirectal area, which can progress to form fistulas. An anal fistula is a ductal connection between the epithelium-lined anorectal lumen and the perianal skin. Anorectal abscesses are most commonly caused by obstruction of the anal gland and consequent bacterial overgrowth. Less common causes include Crohn disease, gastrointestinal infections (e.g., diverticulitis), or malignancy. Clinical features of anal abscesses include anorectal pain, a palpable mass, and signs of cellulitis or systemic infection (e.g., fever). Patients with anal fistulas may present with rectal drainage or drainage from a visible site on the perianal skin. Anorectal abscesses and fistulas are clinical diagnoses. Imaging studies such as CT, MRI, or endosonography are sometimes indicated to assess occult abscesses or complex fistulas. Definitive management requires surgical intervention. Abscesses are incised and drained, followed by open wound healing, while the standard treatment for anal fistulas is fistulotomy.
Epidemiology
- Sex: ♂ > ♀ (2:1)
- Age: mean of 40 (range between 20 and 60 years)
-
Incidence
- ∼ 100,000 people per year in the US
- ∼ 50% of patients with anorectal abscess develop fistulas.
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Most common cause: flow obstruction and infection of the anal crypt glands (90% of cases)
-
Less common causes
- Chronic inflammatory bowel disease (IBD): Crohn's disease, ulcerative colitis (less commonly)
- Acute infections of the gastrointestinal tract: e.g., complicated diverticulitis, acute appendicitis
- Radiation-induced proctitis
- Iatrogenic
- Foreign body
- Malignancy: e.g., colorectal cancer
Classification
Anorectal abscesses and fistulae may be classified according to their variations in anatomical position and distribution.
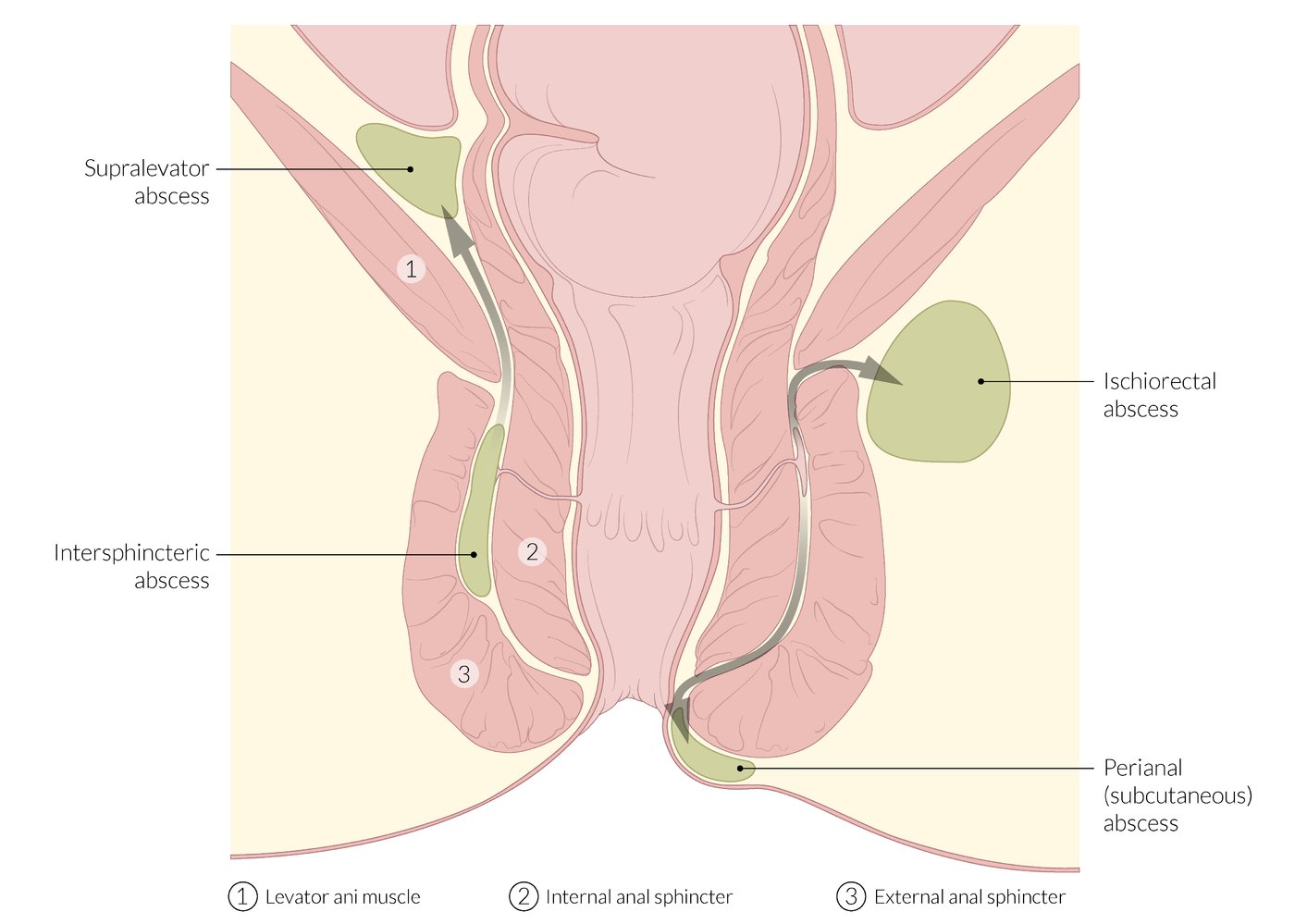
Abscesses
-
Perianal (subcutaneous): most common
- Abscess beneath the perianal skin
- Does not transverse the external sphincter
- Ischiorectal: abscess below the levator ani muscle
- Intersphincteric: abscess between the internal and external sphincters
- Supralevator (least common): abscess above the levator ani muscle

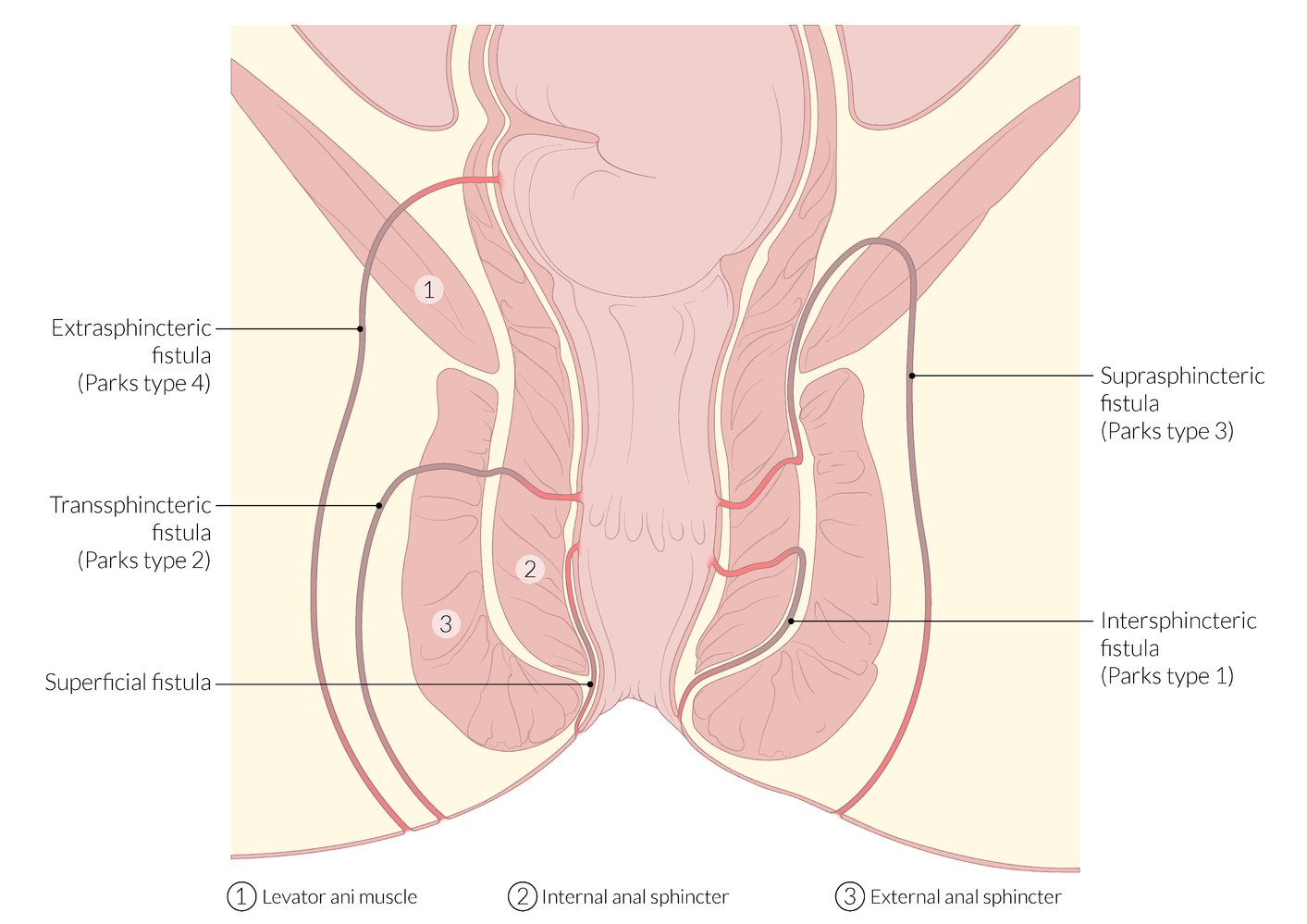
Fistulas (Park's classification)
-
Intersphincteric (Park's Type I)
- Course: along the anatomical space between the internal and external sphincter
- Opening: perianal skin (anoderm) and/or rectum
-
Transsphincteric (Park's Type II)
- Course: penetrates the external sphincter ani muscle into the ischiorectal fossa
- Opening: perianal skin (anoderm)
-
Suprasphincteric (Park's Type III)
- Course: ascends cranially within the intersphincteric space, penetrates the levator ani muscle and follows caudally towards the ischiorectal fossa
- Opening: perianal skin (anoderm)
-
Extrasphincteric (Park's Type IV)
- Course: from the internal opening of the rectal ampulla (above the dentate line) through the levator ani muscles
- Opening: perianal skin
-
Subcutaneous/subanodermal/submucosal
- Course: beneath the perianal/anal skin/rectal mucosa
- Opening: perianal skin (anoderm)/anal canal/rectum

© AMBOSS
© AMBOSS
Pathophysiology
-
Typical development
- Obstruction of anal glands by thick debris → stasis and bacterial overgrowth → abscess formation
- Abscess may extend into adjacent perirectal spaces → possible fistula formation , bacteremia and sepsis
-
Rare forms of development
- Pathophysiology and localization depend on the specific comorbidities (e.g., Crohn's disease)
- See “Less common causes” under etiology above.
Clinical features
Abscesses
| Clinical features of anorectal abscesses [1][2][3] | |||
|---|---|---|---|
| Local symptoms | Systemic symptoms (e.g., fever, chills) | Examination findings | |
| Perianal |
|
|
|
| Ischiorectal |
|
|
|
| Intersphincteric |
|
|
|
| Supralevator |
|
|
|
Anorectal pain is often exacerbated with sitting and defecation, which can lead to constipation. [1]
Deep abscesses (e.g., supralevator) may manifest with systemic symptoms (e.g., fever, signs of sepsis), but few or no localized findings on physical exam. [3]

Fistulas [1][2][3]
- Continuous or intermittent purulent drainage from the anal canal or perianal skin
- Pain during defecation [1]
- Examination may reveal a fistula tract in the perineum or anal canal.
Consider Fournier gangrene in patients with signs of extensive cellulitis and/or necrotic tissue. [1]


There is a prominent area of erythema and swelling on the left buttock and perianal region.
This is the typical appearance of an anal abscess.
Source: “Perianalabszess 01” by Dr. K.-H. Günther, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
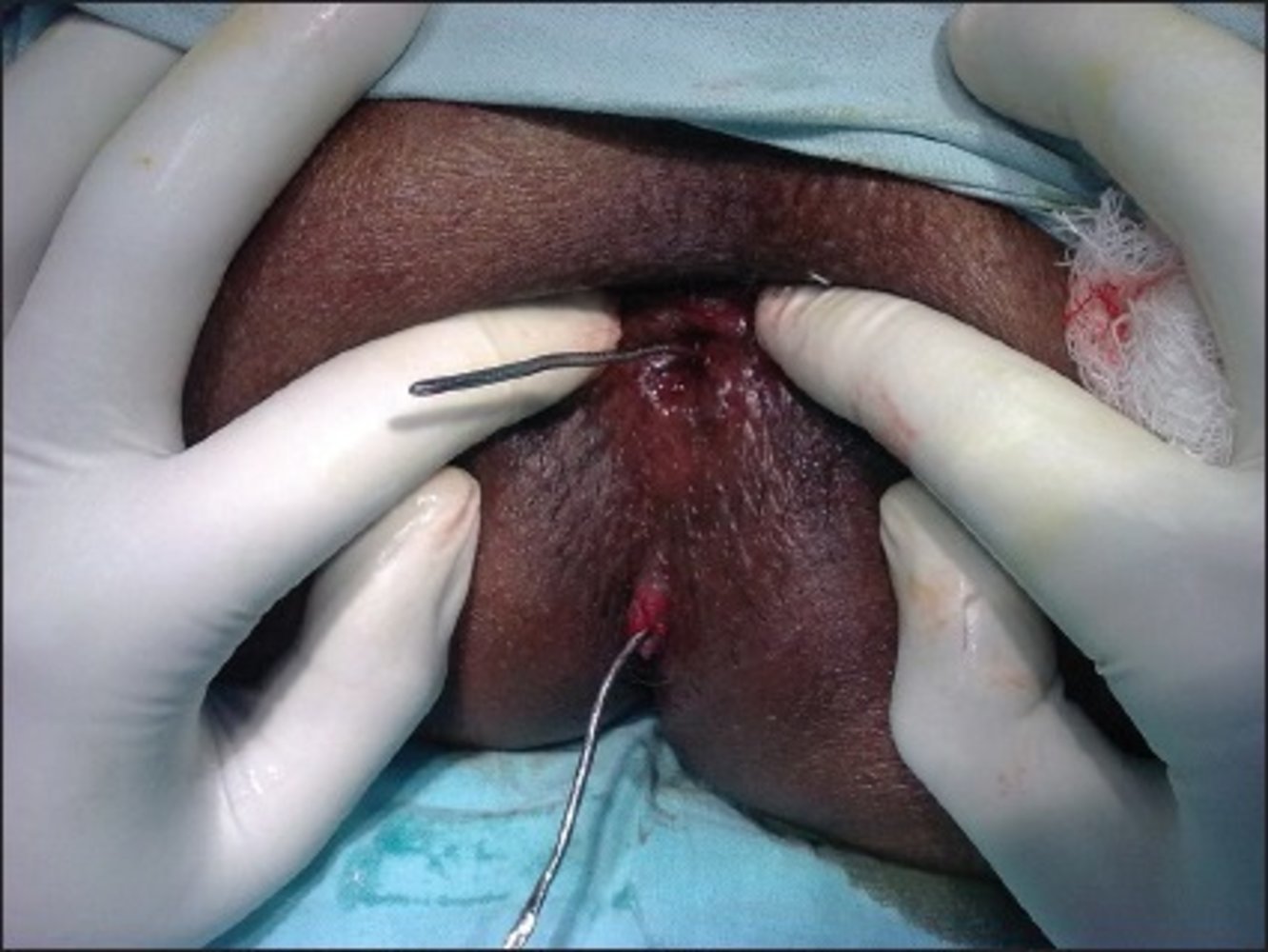
Photograph of the anal orifice of a patient: The external orifice of the anal fistula is seen at 6 O'clock.
A malleable metallic probe has been inserted through the external orifice to the internal orifice (within the anal canal) to identify the course of the fistulous tract.
Source: “Figure 2: A metallic malleable probe passed through a fistula tract” by Gouranga Dutta, Open-i library, licensed under CC BY-SA 3.0. Further notes: Pubmed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518420/
Diagnosis
Approach [2][4]
-
Anorectal abscess and fistula are clinical diagnoses (see “Clinical features”).
- Perform perianal inspection and digital rectal examination.
- Consider anoscopy or proctoscopy as needed. [2]
- Consider MRI, CT, or endosonography if the diagnosis is uncertain.
- Consider septic workup and investigations for the underlying condition (e.g., endoscopy for IBD) as needed.
Ensure adequate pain control and consider examination under sedation or general anesthesia in patients with intense pain. [4]
Avoid probing fistulas outside of operative settings to prevent creating new tracts. [1]
Imaging [2][4][5]
-
Indications
- Confirmatory testing for occult abscesses
- Recurrent or complex anal fistula
- Immunosuppression
- Known or suspected anorectal Crohn disease
-
Modalities
- MRI pelvis with and without IV contrast: preferred [4]
- CT pelvis with IV contrast: may be used in the acute setting [5]
- Anorectal endoscopic ultrasound
Additional studies [4][6]
- Septic features: Perform septic workup.
-
Workup of underlying disorders: Consider individually; not routinely required.
- Diabetes screening
- HIV screening and evaluation for other immune deficiencies
- Evaluation for Crohn disease (e.g., endoscopy)
Differential diagnoses
Other causes of anorectal pain and/or swelling include:
- Thrombosed external hemorrhoids
- Anal fissures
- Proctitis
- Pilonidal cyst
- Perianal dermatitis
- Sexually transmitted diseases (e.g., herpes simplex virus infections)
- Pelvic muscle spasms (e.g., due to proctalgia fugax or pelvic floor dysfunction)
- Malignancy: anal cancer, colorectal cancer
The differential diagnoses listed here are not exhaustive.
Treatment
Abscesses [1][2][4]
Incision and drainage [4]
Drainage is typically performed within 24 hours of presentation.
-
Bedside: can be performed by generalists using local anesthesia or procedural sedation [2][4]
- Indications
- Perianal abscess
- Superficial ischiorectal abscess
- Procedure: See “Abscess incision and drainage.”
- Indications
-
Operative: requires surgery consult and general anesthesia
- Indications [1][2][4]
- Deep abscesses
- Associated fistula
- Sepsis
- Significant comorbid risk factors (e.g., diabetes, immunosuppression)
- Procedure: operative drainage into the anorectal lumen or skin [2][4]
- Indications [1][2][4]
Uncomplicated superficial abscesses in otherwise healthy patients can be treated with incision and drainage in ambulatory settings. [1][2][4]
Consult surgery urgently for patients with signs of sepsis, extensive cellulitis, or comorbid risk-factors.
Adjunctive antibiotics [4]
- Indications: signs of cellulitis, signs of systemic infection (e.g., fever), immunosuppression [2][7]
- Regimens: See “Empiric antibiotic therapy for skin and soft tissue infections.”
In patients with MDRO risk factors, immunosuppression, and/or recurrent or non-healing abscesses, consider sampling drained pus and adjusting antibiotic therapy according to culture results. [4]
Postsurgical care [1]
- Sitz baths
- Analgesics (e.g., acetaminophen or NSAIDs)
- Stool softeners and high-fiber diet to prevent constipation
All patients require postsurgical follow-up to ensure full resolution. Evaluate for fistula tracts if the abscess recurs or fails to resolve. [6]
Fistulas [1][2][3]
- Consult colorectal surgery for operative repair.
- Multiple surgical repair options exist, including: [2][3]
- Fistulotomy (standard approach)
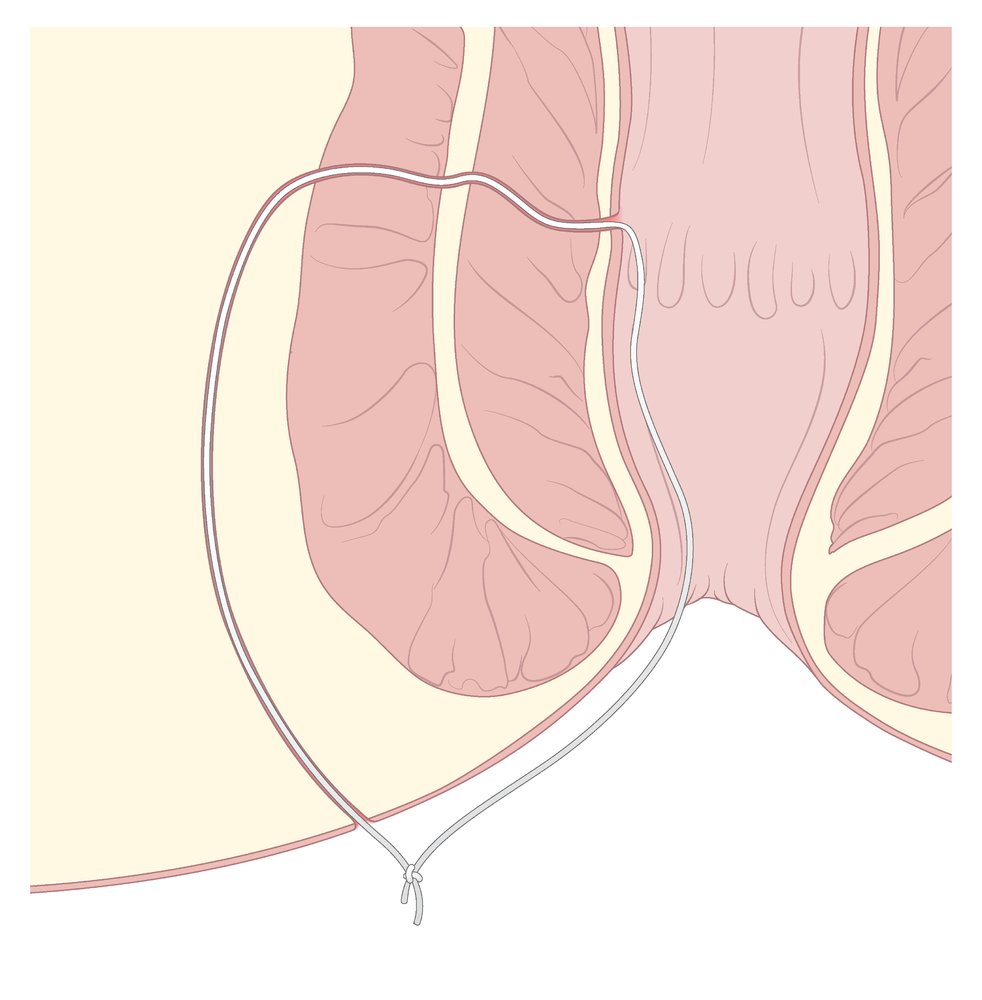
- Seton placement
- Endorectal advancement flap
- Ligation of the intersphincteric fistula tract (LIFT)
- Fistula plug insertion
- Fibrin glue injection
- For patients with Crohn disease, see also “Fistulizing Crohn disease.”


© AMBOSS
© AMBOSS
External Resources
References
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Gaertner WB, Burgess PL, Davids JS, et al. "The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula". Dis Colon Rectum. 65(8). :964-985. (2022)
- Abcarian H. "Anorectal infection: abscess-fistula". Clin Colon Rectal Surg. 24(1). :14-21. (2011)
- Tarasconi A, Perrone G, Davies J, et al. "Anorectal emergencies: WSES-AAST guidelines". World J Emerg Surg. 16(1). (2021)
- Expert Panel on Gastrointestinal Imaging, Levy AD, Liu PS, et al. "ACR Appropriateness Criteria® Anorectal Disease". J Am Coll Radiol. 18(11S). :S268-S282. (2021)
- Cohee MW, Hurff A, Gazewood JD. "Benign Anorectal Conditions: Evaluation and Management". Am Fam Physician. 101(1). :24-33. (2020)
- Mocanu V, Dang JT, Ladak F, et al. "Antibiotic use in prevention of anal fistulas following incision and drainage of anorectal abscesses: A systematic review and meta-analysis". Am J Surg. 217(5). :910-917. (2019)