Summary
Asthma is a heterogeneous disease that is characterized by chronic airway inflammation and defined by a history of respiratory symptoms (e.g., wheezing, shortness of breath, chest tightness, cough). Symptom intensity and expiratory flow characteristically vary over time. Airflow limitation may become persistent in later stages. Allergic asthma often commences in childhood and is triggered by allergens such as pollen, dust mites, and certain foods. Nonallergic asthma and adult-onset asthma (which is typically nonallergic) can develop in individuals aged > 40 years. Triggers for asthma generally include cold air, medications (e.g., aspirin), exercise, and viral infections. Clinical features of asthma include dyspnea, wheezing (often end-expiratory), and cough. Symptoms characteristically worsen at night and/or on exposure to triggers. Symptoms and airflow limitation may abate in response to asthma medications or resolve upon removal of the trigger. Diagnosis in individuals ≥ 6 years of age is supported by variable expiratory airflow on pulmonary function tests (PFTs), e.g., by confirming significant variability in FEV1 or PEF (e.g., after bronchodilator or over time). If lung function testing is not available or is normal in a patient with typical asthma symptoms, elevated fractional exhaled nitric oxide (FeNO) and/or blood eosinophil count are biomarkers that can be used to support the diagnosis. Additional tests may be performed to identify asthma triggers and comorbidities that increase the risk of acute exacerbations. Management of asthma in individuals ≥ 6 years of age is based on severity and primarily involves inhaled corticosteroids (ICS) and, often, ICS/formoterol. Systemic glucocorticoids are usually reserved for the treatment of acute asthma exacerbations but may be used in patients with severe asthma. Avoidance of asthma triggers and management of comorbidities (e.g., rhinosinusitis) are important to achieve symptomatic control and minimize the risk of exacerbations. Frequent follow-up is essential for monitoring response to therapy and for stepwise adjustment of treatment regimens.
“Asthma in children ≤ 5 years of age,” “Acute asthma exacerbations,” and “Exercise-induced bronchoconstriction” are discussed separately.
Definitions
- Asthma: a respiratory disease that is characterized by chronic airway inflammation and manifests with variable respiratory symptoms and variable expiratory airflow
- Acute asthma exacerbation: a reversible worsening of the clinical features of asthma that develops over a short period of time and can progress to life-threatening asthma
Epidemiology
-
Prevalence
- 5–10% of the US population
- More common in Black than in White individuals
- For unknown reasons, the prevalence of asthma has been increasing over the past 20 years. [1]
-
Sex: differs depending on age of onset
- ♂ > ♀ in patients < 18 years
- ♀ > ♂ in patients > 18 years
-
Age of onset
- Allergic asthma: typically in childhood
- Nonallergic asthma: typically > 40 years
References:[2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- The exact etiology of asthma remains unknown.
-
Risk factors for asthma include:
- Atopy
- Allergies
- Genetic predisposition
- Environmental and socioeconomic factors that increase exposure to asthma triggers, e.g., pollution from heating and cooking sources
| Asthma triggers | |
|---|---|
| Allergic asthma (extrinsic asthma) |
Nonallergic asthma (intrinsic asthma) |
|
|
Childhood exposure to secondhand smoke increases the risk of developing asthma.
Pathophysiology
Common underlying pathophysiology
Asthma is an inflammatory disease driven by T-helper type 2 cells (Th2-cell) that manifests in individuals with a genetic predisposition. It consists of the following three pathophysiologic processes:
- Bronchial hyperresponsiveness
-
Bronchial inflammation
- Symptoms are primarily caused by inflammation of the terminal bronchioles, which are lined with smooth muscle but lack the cartilage found in larger airways.
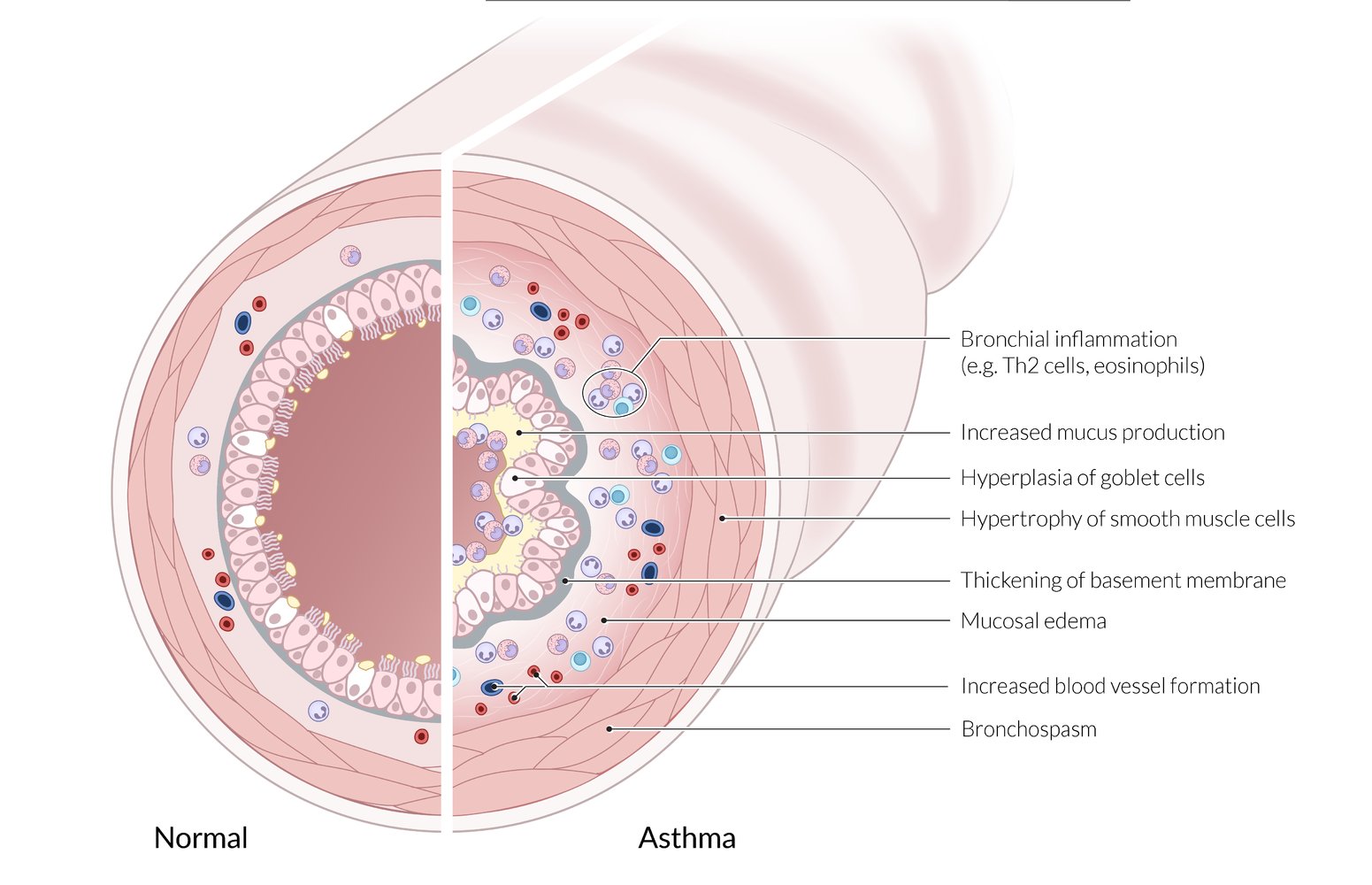
- Overexpression of Th2-cells → inhalation of antigen results in production of cytokines (IL-3, IL-4, IL-5, IL-13) → activation of eosinophils and induction of cellular response (B-cell IgE production) → bronchial submucosal edema and smooth muscle contraction → bronchioles collapse [4][5]
-
Endobronchial obstruction caused by:
-
Increased parasympathetic tone
- Reversible bronchospasm
- Increased mucus production
- Mucosal edema and leukocyte infiltration into the mucosa with hyperplasia of goblet cells
- Hypertrophy of smooth muscle cells
-
Increased parasympathetic tone
Type-specific pathophysiology
-
Allergic asthma
- IgE-mediated type 1 hypersensitivity to a specific allergen
- Characterized by mast cell degranulation and release of histamine after a prior phase of sensitization
-
Nonallergic asthma
- Irritant asthma: irritant enters lung → ↑ release of neutrophils → submucosal edema → airway obstruction
-
Aspirin-exacerbated respiratory disease is characterized by the Samter triad:
- Inhibition of COX-1 → ↓ PGE2; → ↑ leukotrienes and inflammation → submucosal edema → airway obstruction
- Chronic rhinosinusitis with nasal polyposis
- Asthma symptoms
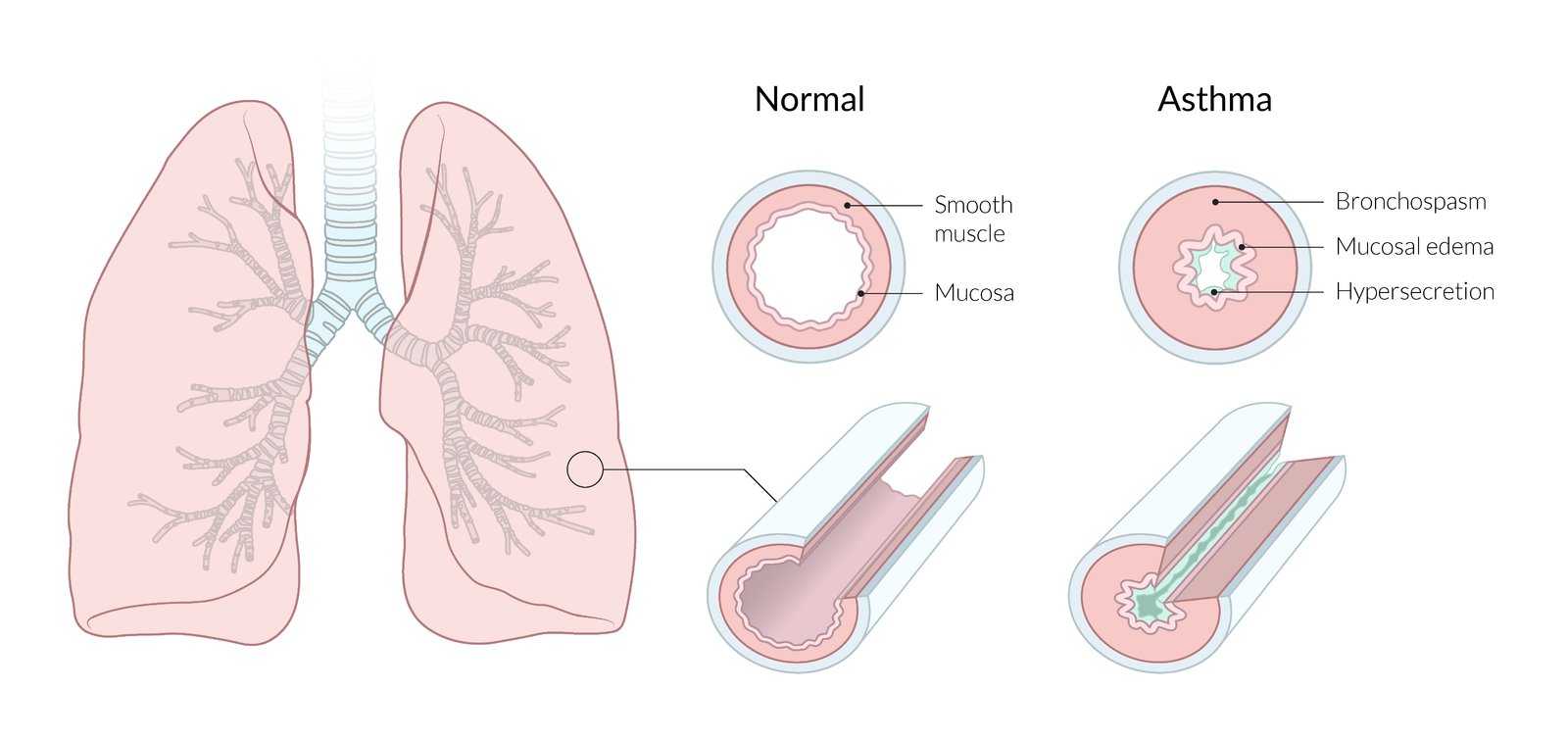
Endobronchial obstruction and the characteristic clinical presentation of asthma (i.e., dyspnea, end-expiratory wheezing, and persistent cough) are caused by bronchospasm, mucosal edema, and increased mucus production (bronchial hypersecretion).
© AMBOSS
© AMBOSS
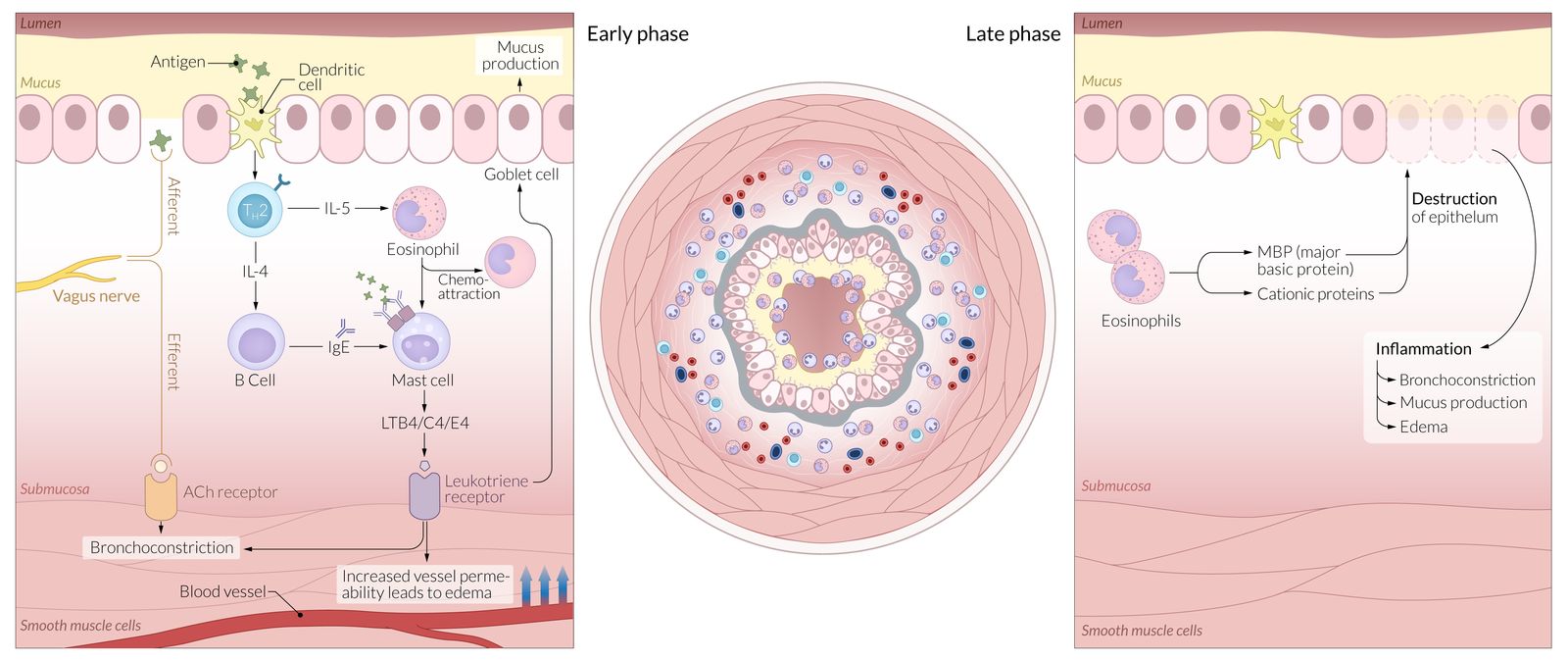
Early phase: An antigen is taken up by dendritic cells, causing the release of interleukins from T-helper cells and starting a cascade of intracellular events resulting in mast-cell chemoattraction and degranulation. Mast cells release a variety of chemokines resulting in bronchoconstriction, increased vascular permeability (edema), and mucus production.
Late phase: Prolonged activation of initial pathophysiological response (early phase) results in the cellular destruction.
© AMBOSS
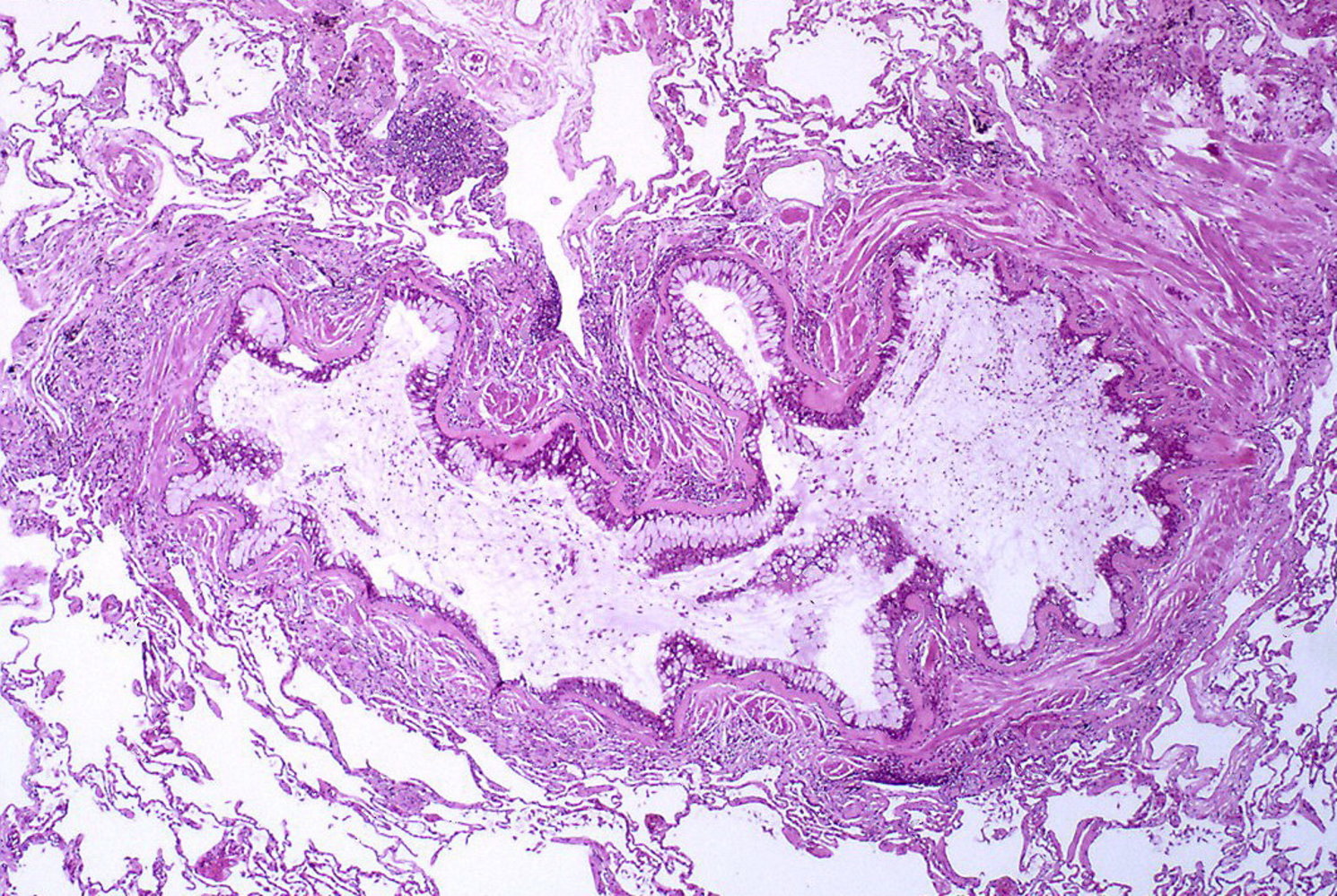
Photomicrograph of lung tissue (H&E stain; intermediate magnification)
Severe bronchial inflammation and obstruction of the lumen due to an accumulation of mucoid exudate. The epithelial basement membrane appears thickened and the number of goblet cells has increased drastically.
This is the typical appearance of bronchial asthma.
Source: “Asthma Case 103” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0.
© AMBOSS
Clinical features
-
Typical features: variable; can occur sporadically or in response to an asthma trigger
- Persistent, dry cough that worsens at night, with exercise, or on exposure to triggers/irritants (e.g., cold air, allergens, smoke)
- End-expiratory wheezes
- Dyspnea (shortness of breath)
- Chest tightness
- Prolonged expiratory phase on auscultation
- Hyperresonance to lung percussion
- Atypical features: See “Subtypes and variants.”
- Features of common comorbid conditions: : e.g., atopic conditions like allergic rhinitis or eczema
- Acute asthma exacerbations: covered in detail separately
Characteristic examination findings may not be present between asthma exacerbations, especially in children. [6]
Subtypes and variants
The following is a list of asthma phenotypes and variants.
-
Allergic asthma
- Most common phenotype
- Begins with intermittent symptoms in childhood
- Triggered by allergens
- Usually associated with atopy (e.g., eczema, rhinitis)
- Responds well to ICS-containing treatment
-
Nonallergic asthma
- Less common than allergic asthma
- Triggered by, e.g., viral upper respiratory tract infections, cold air, GERD
- Not associated with atopy
- Responds poorly to ICS-containing treatment
-
Adult-onset asthma:
- An uncommon phenotype in which symptoms first manifest in adulthood
- Typically nonallergic
- Responds poorly to ICS-containing treatment
- Cough variant asthma: a type of asthma characterized by chronic dry cough without other typical symptoms of asthma (see also “Cough”)
- Aspirin-exacerbated respiratory disease
- Asthma-COPD overlap
- Occupational asthma
- Asthma with obesity: Some individuals with obesity and asthma exhibit prominent respiratory symptoms with little eosinophilic airway inflammation.
Asthma-COPD overlap [6]
Definition [6][7][8]
Asthma-COPD overlap is the concurrent presence of features of asthma and COPD. [6][7][8]
Clinical features [6]
- Chronic presentation, most commonly with intermittent or episodic symptoms
- Common symptoms include cough, SOB, chest tightness, and wheezing.
- Symptoms may:
- Worsen after exposure to common triggers for asthma, e.g., pollen
- Improve after use of asthma medications
- May develop in patients with a known history of asthma or COPD
Individuals with asthma-COPD overlap experience more symptoms, more frequent exacerbations, and higher mortality than individuals with either asthma or COPD alone. [6]
Diagnostics [6][7]
- Take a comprehensive history, including smoking history and toxin exposure.
- All patients require spirometry and diagnostic studies for asthma and diagnostic studies for COPD, if not already performed.
- The diagnosis of asthma-COPD overlap can be made when all of the following criteria are met: [7][9][10]
- Persistent airflow limitation (FEV1/FVC < 0.7) on PFTs (suggests COPD)
- History of asthma and/or some clinical features of asthma [9]
- Episodic nature of symptoms
Do not wait for diagnostic confirmation before initiating treatment for asthma in patients with suspected asthma-COPD overlap; untreated patients are at risk of life-threatening acute asthma attacks. [6]
Asthma and COPD both cause an obstructive pattern on PFTs. A positive response to post-bronchodilator testing is more common in asthma, but reversibility of bronchoconstriction is not a reliable factor for differentiating between COPD and asthma. [8]
Management [6]
- Refer to a pulmonologist for any of the following:
- Presence of symptoms atypical of asthma or COPD
- Suspected chronic airway disease but minimal symptoms of asthma or COPD
- Uncertain diagnosis or suspicion of an alternative diagnosis
- Comorbidities causing difficulty with work-up or management
- All other patients
- Initiate asthma treatment with low-dose or medium-dose ICS, even if the diagnosis is not yet confirmed. [6]
- Add LABA and/or LAMA as needed for the treatment of COPD according to the GOLD group classification system.
- Optimize management of both underlying conditions with:
- Adjunctive therapy for asthma (e.g., reduce trigger exposure, have an asthma action plan)
- Supportive measures for COPD (e.g., smoking cessation, immunizations, pulmonary rehabilitation)
- If no improvement after 2–3 months, refer to a pulmonologist.
Patients with concurrent asthma and COPD symptoms should never be treated with a LABA or long-acting muscarinic antagonist (LAMA) alone; these must always be given in combination with an ICS. [6]
Occupational asthma
Background
-
Definition [11]
- Occupational asthma: asthma that is induced by specific workplace allergens and/or irritants
- Work-exacerbated asthma: preexisting asthma that is worsened by specific workplace allergens and/or irritants
-
Epidemiology
- The most commonly affected occupations include farmers, grain workers, and bakery workers.
- Up to 25% of adult-onset asthma is attributable to occupational asthma. [6][12]
-
Subtypes
- Sensitizer-induced (i.e., IgE-mediated, allergic): caused by exposure to high-molecular-weight (e.g., flour, animal proteins) and low-molecular-weight (e.g., diisocyanates) agents [12][13]
- Irritant-induced: caused by acute inhalation injury or repeated exposure to the irritant agent (e.g., vapors, gas, fumes)
- Reactive airways dysfunction syndrome: a type of irritant-induced occupational asthma characterized by the sudden onset of symptoms within 24 hours of exposure to a high concentration of corrosive gas, vapors, or fumes [14]
Clinical features [6]
- Asthma symptoms develop in a working environment with sensitizers and/or irritants and improve when outside of the workplace.
- Rhinitis and conjunctivitis often precede asthma symptoms. [13]
- Exacerbations after repeat exposures can be severe.
Diagnostics [6][13][15]
Refer to a specialist for diagnostic confirmation.
- Obtain a comprehensive work exposure history.
- Confirm diagnosis of asthma with PFTs.
- Perform serial peak expiratory flow (PEF) monitoring: A decrease in PEF with exposure to the offending agent supports the diagnosis.
- Obtain skin prick test or allergy-specific serum IgE testing to identify the causative agent.
Treatment [6]
- Most important: Eliminate or reduce exposure to the offending agent (e.g., use of respiratory PPE or stop the exposure through work reassignment or removal of the agent).
- Provide stepwise asthma treatment with ICS-containing therapy.
Complications
- Persistent bronchial hyperresponsiveness
Prevention
- Primary prevention: reducing or avoiding exposure by removing, replacing, or isolating the hazard
- Screening: medical surveillance programs in the workplace (e.g., regular spirometry) for early detection of occupational asthma
Diagnosis
“Diagnosis of acute asthma exacerbation” is covered separately. The following applies to individuals > 5 years of age. For younger children, see "Diagnosis of asthma in children ≤ 5 years of age".
Approach [6]
- Perform lung function tests (e.g., spirometry or PEF) before and after use of a bronchodilator.
- Consider biomarkers (e.g., blood eosinophil count, FeNO) if lung function tests are normal or not available.
- Consider additional studies to rule out differential diagnoses of asthma and/or assess for comorbidities.
- Consult an asthma specialist if there is difficulty in confirming the diagnosis.
Spirometry is the gold standard test for diagnosing asthma.
Diagnostic confirmation [6]
-
The presence of both of the following confirms the diagnosis (including in patients already receiving ICS): [6]
- Typical symptoms of asthma that vary in severity
- Excessive variability in expiratory lung function parameters (FEV1, PEF) [6]
- Expiratory airflow limitation (obstructive pattern) on PFTs further supports the diagnosis.
- Patients with typical symptoms, but non-variable lung function already receiving ICS:
- Consider diagnostic biomarkers (i.e., blood eosinophil count or FeNO) to support the diagnosis.
- Asthma diagnosis is confirmed if stepping down treatment results in increased symptoms and excessive variability in FEV1 and/or PEF.
- Review symptom control and repeat lung function tests in 2–4 weeks. [6]
- Consider tapering ICS by 25–50% or stopping other maintenance medication (if feasible). [6]
More variation or frequent instances of excessive variation in PFTs increase diagnostic certainty. [6]

Spirometry [6]
Spirometry can be paired with specialized tests in obstructive lung diseases (e.g., bronchodilator responsiveness testing or bronchial challenge tests).
- Indication: first-line test
-
Supportive findings
- Expiratory airflow limitation (e.g., post-bronchodilator FEV1 and FEV1/FVC ratio; ) below LLN
- Excessive variability in expiratory lung function, defined as ≥ 1 of the following:
-
↑ FEV1 of ≥ 12% and ≥ 200 mL (reversibility of airflow obstruction), in response to either: [16][17];
- Bronchodilator responsiveness testing
- 4 weeks of ICS-containing therapy
- Variation in FEV1 of ≥ 12% and ≥ 200 mL from one appointment to the next
-
Response during bronchial challenge testing (may be ordered if initial PFTs are inconclusive)
- ↓ FEV1 ≥ 20% from baseline with methacholine challenge test
- ↓ FEV1 ≥ 15% from baseline with hypertonic saline, hyperventilation, or inhaled mannitol
- ↓ FEV1 > 10% and > 200 mL from baseline with standardized exercise challenge
-
↑ FEV1 of ≥ 12% and ≥ 200 mL (reversibility of airflow obstruction), in response to either: [16][17];
A bronchial challenge test is sensitive but not specific for asthma. This test is most useful for ruling out asthma in patients with inconclusive spirometry results or in those with atypical symptoms and/or response to therapy. [18]


Peak flow meter (PFM) [6]
- Indication: Spirometry is normal or not available. [6]
-
Technique: Use the same meter each time. [6]
- Stand up, inhale deeply, close mouth around the PFM mouthpiece, and blow out as forcefully as possible.
- Note the level recorded on the meter.
- Repeat three times in succession.
- Record the highest reading every morning and evening.
-
Supportive findings
- Excessive variability in expiratory lung function, defined as ≥ 1 of the following:
- Daily diurnal variability of PEF of > 10% (averaged over 2 weeks)
- An increase in PEF by ≥ 20% after any of the following:
- 4 weeks of ICS-containing therapy
- Bronchodilator responsiveness testing
- ↓ PEF from baseline while symptomatic
- Excessive variability in expiratory lung function, defined as ≥ 1 of the following:
Additional studies [6]
-
Biomarkers of eosinophilic and/or allergic inflammation [6]
-
Fractional exhaled nitric oxide (FeNO): the concentration of nitric oxide in exhaled air
- May be elevated in response to airway inflammation (e.g., allergic asthma, atopy, eosinophilic bronchitis) [6][19]
- Can also be elevated in response to other inflammatory conditions (e.g., atopy, eosinophilic bronchitis)
- CBC: ↑ blood eosinophil count
-
Allergy workup: Obtain if allergens are suspected to play a significant role in exacerbations.
- Antibody testing: ↑ total IgE, ↑ allergen-specific IgE [6]
- Skin allergy tests: skin prick testing or intradermal skin testing [3]
- Clinical uses [6]
- ↑ Blood eosinophil count and/or ↑ FeNO support a diagnosis of asthma in patients with typical asthma symptoms who have normal spirometry and/or PFM.
- Normal results do not rule out asthma.
- Used to predict response to asthma medications (e.g., biologics in patients with severe asthma).
-
Fractional exhaled nitric oxide (FeNO): the concentration of nitric oxide in exhaled air
- Serum alpha-1 antitrypsin level: Obtain in individuals with adult-onset asthma or asthma that is unresponsive to treatment. [20]
- Single-breath diffusion capacity: : normal or ↑ DLCO
-
Sputum analysis (not routinely recommended)
- Curschmann spiral: a spiral mucus plug in sputum that is formed from shed bronchial epithelium
- Charcot-Leyden crystals: histopathologic finding in patients with eosinophilic inflammation and/or proliferation
- Creola bodies: aggregate of desquamated epithelial cells [21]
-
Imaging studies (e.g., HRCT)
- Not routinely recommended; useful for differential diagnosis
- Usually normal; may reveal air trapping and bronchial thickness


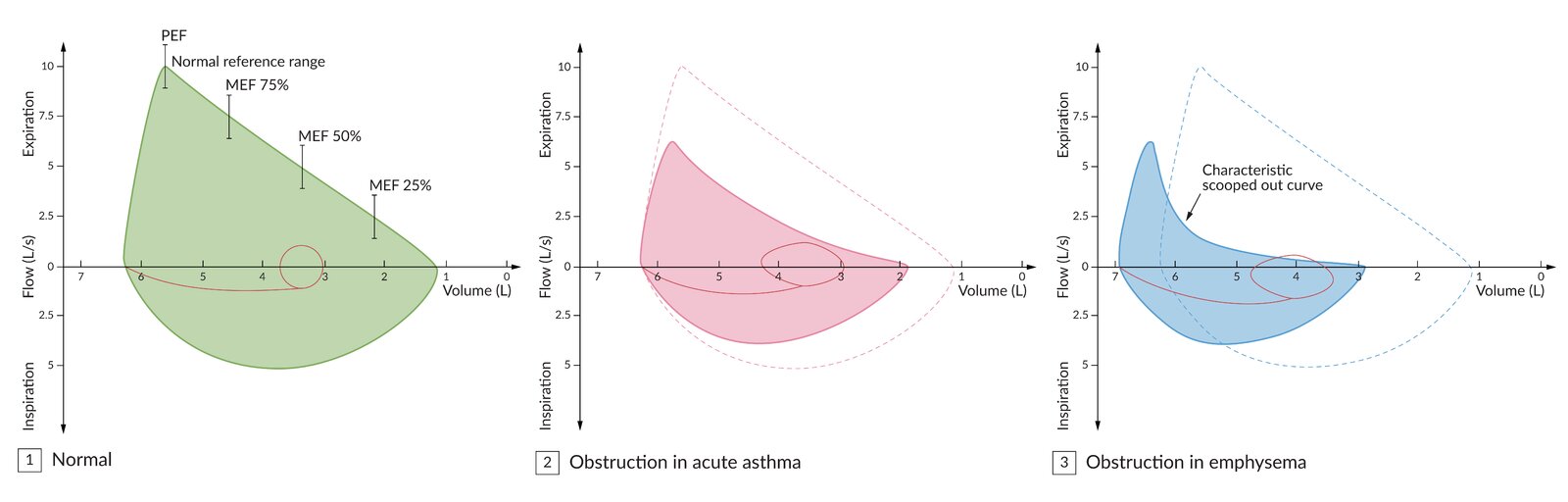
Patients with an obstructive lung disease typically have a concave flow-volume loop (middle) compared to healthy patients (left).
Emphysema typically causes a “scooped out” curve (right) due to the collapse of small airways during expiration.
© AMBOSS
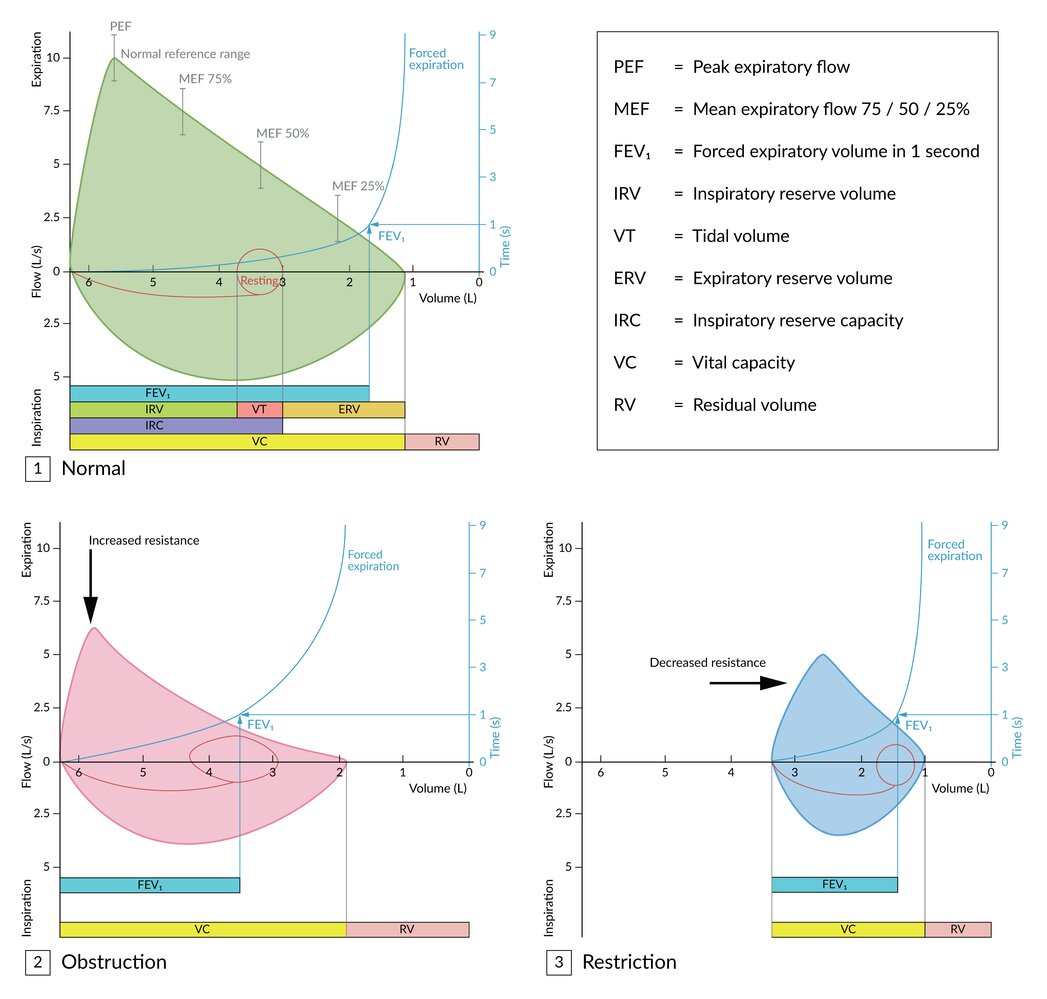
(1) The top graph is a normal flow-volume loop and a time-volume curve used to determine the FEV1.
(2) Obstructive lung diseases result in a concave flow-volume loop due to increased resistance. Absolute FEV1, as well as FEV1 relative to vital capacity (FEV1/FVC), is diminished.
(3) Restrictive lung diseases result in a narrowed flow-volume loop due to reduced vital capacity and compliance. Absolute FEV1 is diminished, but not in relation to vital capacity (FEV1/FVC).
© AMBOSS
© AMBOSS
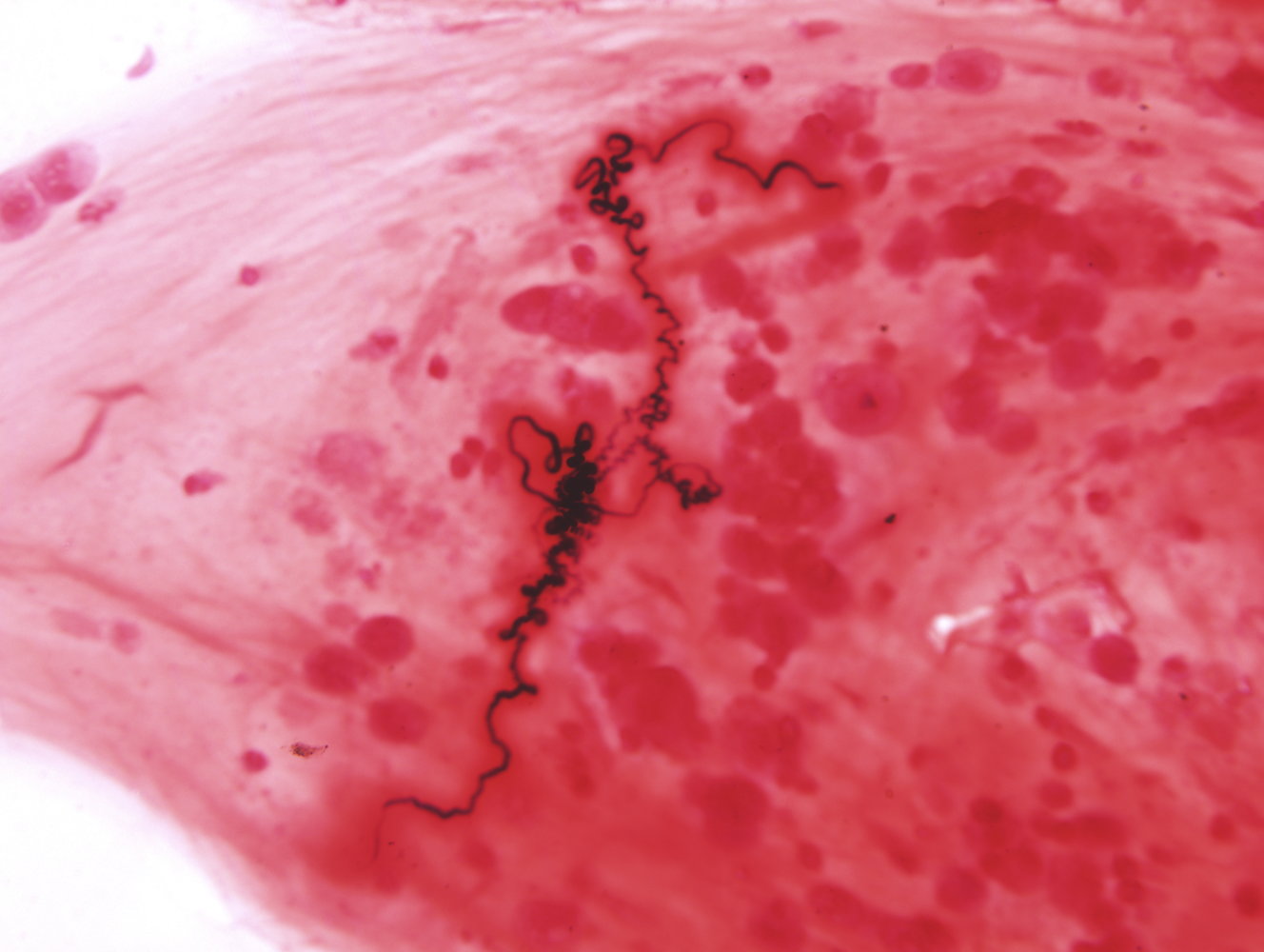
Photomicrograph of a sputum sample
Dark, spiral-shaped casts of mucus (Curschmann spirals) are visible.
Curschmann spirals are typically seen in the sputum samples of patients with bronchial asthma.
Source: “Curshman's Spiral” by Doc James, Wikimedia Commons, licensed under CC BY 4.0. Further notes: License type is not entirely clear, CC BY 4.0 is assumed to be valid. Otherwise please contact us. Thank you.
{kind=link}
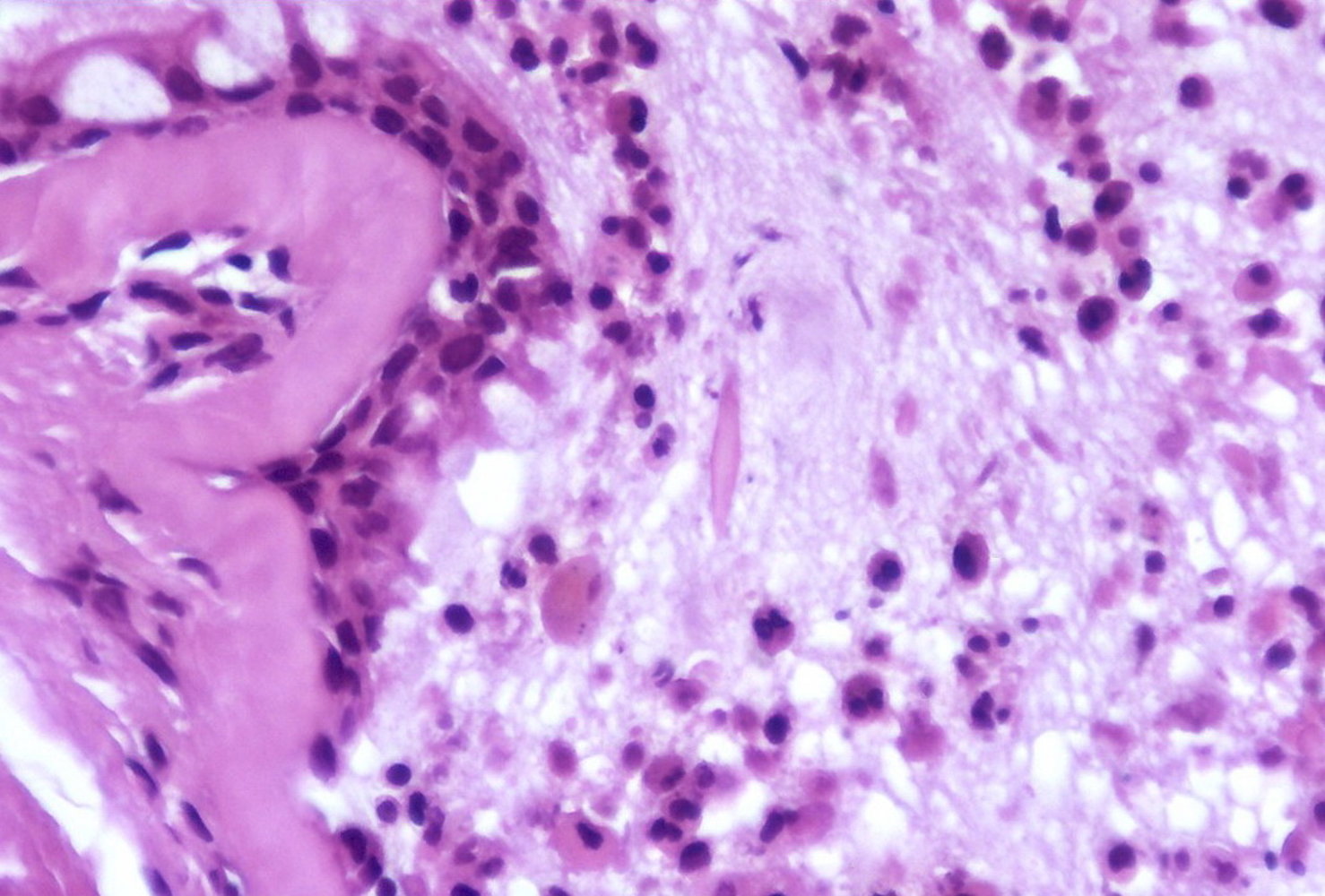
Photomicrograph of lung tissue (H&E stain)
Lumen of a bronchus filled with mucous and inflammatory exudate.
A bipyramidal hexagonal structure (yellow overlay) is visible in the center of the image.
This structure is known as a Charcot-Leyden crystal, a histopathologic finding in patients with eosinophilic inflammation and/or proliferation (e.g., asthma, parasitic infections).
Source: “Charcot-Leyden crystal - Asthma Case 103” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
Differential diagnoses
For more information on the differential diagnoses below, see “Differential diagnosis of chronic cough,” “Differential diagnosis of dyspnea,” “Differential diagnosis of acute asthma,” and “Wheezing in children.”
-
Pulmonary
- COPD or asthma-COPD overlap
- Exercise-induced bronchoconstriction
- Allergic bronchopulmonary aspergillosis
- Cystic fibrosis
- Primary ciliary dyskinesia
- Bronchiectasis
- α1-antitrypsin deficiency
- Interstitial lung disease
- Central airway obstruction
- Infection, e.g., tuberculosis, pertussis
- Reactive airway disease
-
Cardiac
- Heart failure
- Congenital heart disease
-
Upper respiratory
- Upper airway cough syndrome
- Laryngeal obstruction (e.g., inhaled foreign body)
- Vocal cord dysfunction
- Gastrointestinal: GERD
-
Other
- Adverse effect of medication, e.g., cough due to ACE inhibitors
- Hyperventilation
Consider allergic bronchopulmonary aspergillosis if respiratory symptoms worsen and/or features of bronchiectasis develop despite asthma treatment.
Comparison of asthma and COPD
| Comparison of asthma and COPD | ||
|---|---|---|
| Asthma [6] | COPD [8] | |
| Age at diagnosis |
|
|
| Etiology |
|
|
| Clinical presentation |
|
|
| Flow volume loop pattern on PFTs |
|
|
| Bronchial obstruction |
|
|
| First-line medication |
|
|
Reactive airway disease [22]
-
Description
- A nonspecific term used to describe symptoms and findings that are similar to those of asthma (e.g., wheezing, coughing, airway sensitivity)
- Underlying conditions include asthma, pneumonia, COPD, and/or bronchitis
- Most commonly used in pediatric settings when asthma is suspected, but not yet confirmed
- Clinical features: wheezing, coughing, dyspnea, and/or sputum production
Ascription of the label “Reactive airway disease” may prevent a thorough workup of the actual underlying condition and/or lead to the prescription of ineffective medication.
The differential diagnoses listed here are not exhaustive.
Patients with an obstructive lung disease typically have a concave flow-volume loop (middle) compared to healthy patients (left).
Emphysema typically causes a “scooped out” curve (right) due to the collapse of small airways during expiration.
© AMBOSS
Classification
The age cutoff used for the diagnosis of asthma in young children varies among guidelines. This section includes information for individuals > 5 years of age. For younger children, see "Initial maintenance management of asthma in children ≤ 5 years."
GINA classification for individuals ≥ 6 years of age [6]
-
Uncontrolled asthma (any of the following)
- Poor symptom control
- Exacerbations requiring oral corticosteroids ≥ 2 times per year
- Exacerbations requiring ≥ 1 hospitalization per year
-
Difficult-to-treat asthma
- Uncontrolled asthma despite the use of medium- or high-dose ICS plus either a second controller (e.g., LABA) or maintenance oral corticosteroid
- Asthma controlled only by high-dose therapy
- May result from modifiable factors
-
Severe asthma
-
Difficult-to-treat asthma with either of the following:
- Uncontrolled symptoms despite optimized high-dose ICS/LABA therapy and management of modifiable contributory factors
- Worsens when high-dose treatment is reduced
- Use of this term may guide appropriate referral, further evaluation, and eligibility for advanced treatments (e.g., biologics).
-
Difficult-to-treat asthma with either of the following:
- Mild or moderate asthma: use of these terms is discouraged; may be misinterpreted as indicating low risk [6]
American Thoracic Society/European Respiratory Society (ATS/ERS) task force severity classification for individuals ≥ 5 years of age [3][23][24]
The National Asthma Education and Prevention Program (NAEPP) guideline classifies asthma severity as intermittent or persistent in individuals who are not receiving asthma maintenance therapy. [3]
| Classification of asthma severity in individuals ≥ 5 years of age [3] | |||
|---|---|---|---|
| Severity | Impairment over the past 2–4 weeks | Lung function | Exacerbation |
| Intermittent asthma |
|
|
|
| Mild persistent asthma |
|
|
|
| Moderate persistent asthma |
|
|
|
| Severe persistent asthma |
|
|
|
In individuals who are not receiving asthma maintenance therapy, severity is classified based on impairment over the previous 4 weeks, lung function (e.g., spirometry), and number of exacerbations in the past year. [3]
Management
The following applies to individuals > 5 years of age. For younger children, see "Initial maintenance management of asthma in children ≤ 5 years."
General principles [6][25]
- Follow a step-wise approach to management.
- Manage comorbidities; reduce exposure to asthma triggers (see “Adjunctive therapy”).
-
Schedule frequent follow-ups, e.g.:
- Appointments: 1–3 months after initiating treatment, every 3–12 months thereafter
- PFTs: 3–6 months after initiating treatment, every 1–2 years once stable
- Management of acute asthma exacerbation and management of exercise-induced bronchoconstriction are discussed separately.
Long-term management of asthma involves a continuous cycle of clinical assessment and adjustment of stepwise asthma treatment.
Stepwise asthma treatment [6][25]
Prescribe asthma relievers and maintenance bronchodilators depending on the severity and previous response to treatment. See “Asthma pharmacotherapy for individuals age 12 years and older,” “Asthma pharmacotherapy for children age 6–11 years,” and "Maintenance management of asthma in children ≤ 5 years."
-
Before initiating treatment
- Document supporting evidence for asthma diagnosis, asthma severity, and risk factors for asthma.
- Provide education on proper inhaler technique.
-
Before stepping up treatment
- Consider alternative causes for new or persistent symptoms.
- Assess adherence and review proper inhaler technique.
- Identify any persistent exposures to asthma triggers.
-
Before stepping down treatment
- Consider stepping down treatment in patients with good symptom control and stable lung function for ≥ 3 months. [6]
- Optimize timing.
- Provide a written asthma action plan and instructions for how and when to restart the previous regimen if symptoms worsen.
- Schedule a follow-up visit to evaluate progress.
Indications for referral
For individuals > 5 years, refer to an asthma specialist if a patient has risk factors for asthma-related death or any of the indications listed below. For younger children, see "Management of asthma in children ≤ 5 years" for additional indications.
- Frequent exacerbations
- Treatment side effects
- Persistent or severe symptoms despite correct use of inhaler and adherence to ICS/LABA
- Need for advanced therapies, e.g., asthma biologics
Overview of asthma medications [3][6][26]
The goal of asthma pharmacotherapy is to counteract bronchoconstriction by reducing bronchial inflammation and parasympathetic tone.
-
Asthma relievers
- Medications that are effective in acute asthma exacerbation
- Examples: ICS/formoterol, SABAs, SAMAs, systemic glucocorticoids
-
Asthma maintenance therapy
- Medications that are effective in the long-term management of asthma
- Examples: ICS/formoterol, ICS, LAMA, leukotriene receptor antagonists
Patients with asthma should not be on LABAs or LAMAs without an ICS. [6]
PRN low-dose ICS/formoterol results in fewer severe exacerbations and ED visits than PRN SABA regimens regardless of baseline severity. [6]
Commonly used asthma medication
| Overview of commonly used asthma medications [3][6][26] | |||
|---|---|---|---|
| Class | Examples | Indications and uses | Mechanism |
| ICS/LABA (combination of inhaled corticosteroid and long-acting beta agonist) |
|
|
|
|
|
||
| Inhaled corticosteroids (ICS) [3][6] |
|
|
|
| Short-acting beta-2 agonists (SABA) |
|
|
|
| Long-acting beta-2 agonists (LABA) |
|
|
|
| Short-acting muscarinic antagonists (SAMA) |
|
|
|
| Long-acting muscarinic antagonists (LAMA) |
|
|
|
| Oral glucocorticoids |
|
|
|
| Leukotriene receptor antagonists (LTRAs) |
|
|
|
- See “Side effects of glucocorticoid therapy” for details.
- See “Contraindications for glucocorticoid therapy” for details.
- See “Antimuscarinic side effects” for details.
Adverse effects of LABA therapy can include arrhythmias, tachycardia, tremor, hyperglycemia, and hypokalemia.
Inhaled corticosteroids do not take full effect until they have been used for approx. 1 week.

Additional medications
These medications are typically reserved for patients under the care of a specialist.
| Overview of additional asthma drugs | ||||
|---|---|---|---|---|
| Agents | Indications and uses | Mechanism | ||
| Leukotriene pathway modifiers (e.g., zileuton) [27] |
|
|
||
| Mast cell stabilizers (chromones; e.g., cromolyn sodium) [28] |
|
|
||
| Methylxanthines (e.g., theophylline) |
|
|
||
| Biologics | Anti-IgE antibodies (omalizumab) [29] |
|
|
|
| IL-4 antibodies (i.e., dupilumab) |
|
|
||
| IL-5 antibodies (e.g., mepolizumab, reslizumab, benralizumab) [30] |
|
|
||
Theophylline is no longer routinely prescribed because of the risk of toxicity. It is used solely as an adjunctive or alternative therapy.
The following drugs are not effective during an acute asthma attack: LABAs without ICS, leukotriene pathway modifiers, theophylline, mast-cell stabilizers, and biologics.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
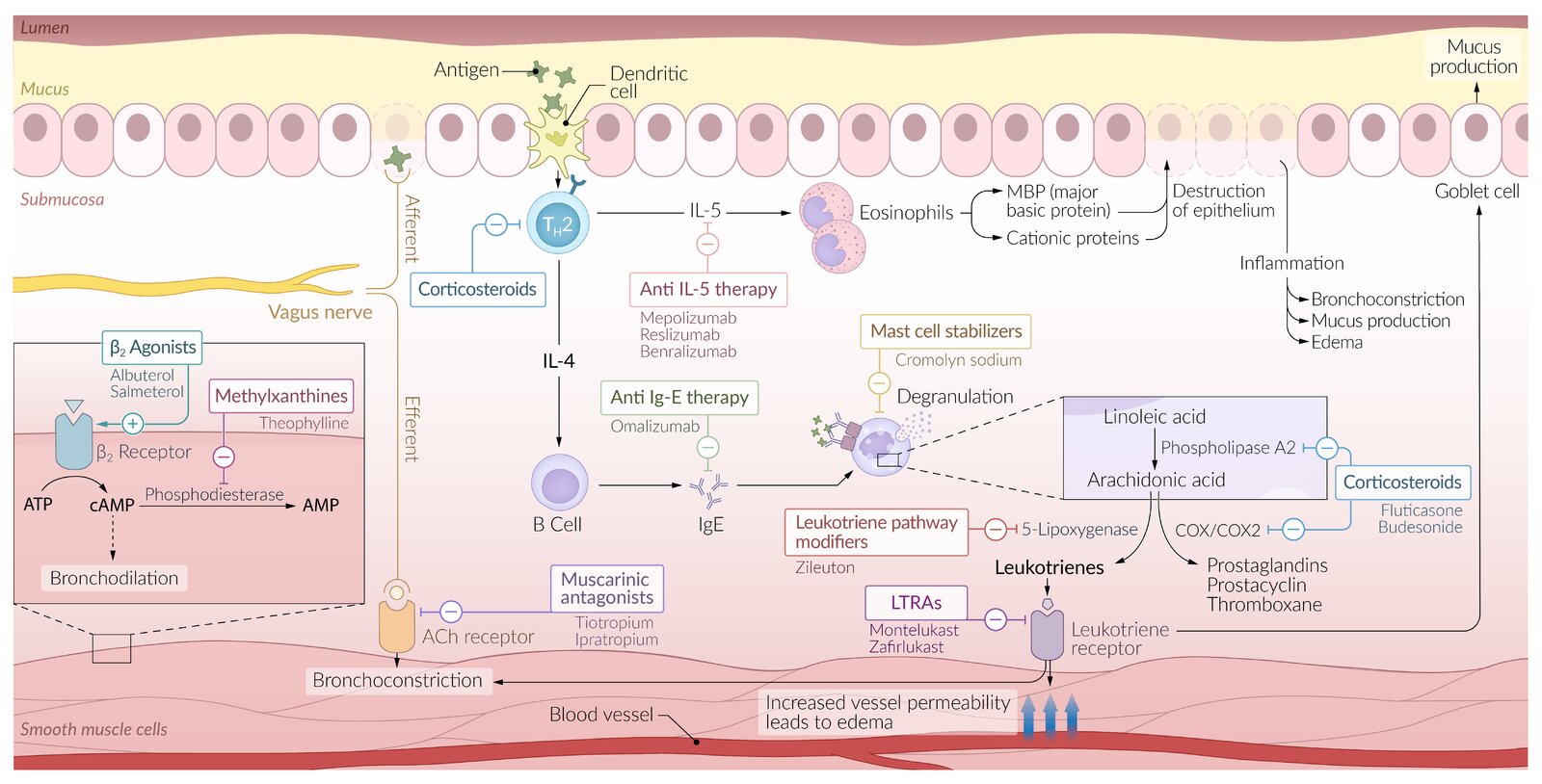
B2-agonists (e.g., salbutamol): relax bronchial smooth muscle and induce bronchodilation
Theophylline: inhibits phosphodiesterase (PDE) and the conversion of cyclic-AMP to AMP, resulting in anti-inflammatory and bronchodilatory effects
Mepolizumab (monoclonal antibody): binds to interleukin-5 and prevents binding to its receptor on eosinophils resulting in reduced eosinophil activation.
Omalizumab (monoclonal antibody): inhibits the binding of IgE and, thus, the activation of mast cells, basophils, and dendritic cells
Mast cell stabilizers (e.g., cromolyn sodium, nedocromil): block the IgE receptor on mast cells preventing degranulation and histamine release
Muscarinic antagonists (e.g., ipratropium bromide): competitively inhibit postganglionic muscarinic receptors in bronchial smooth muscle resulting in bronchodilation
Leukotriene receptor antagonists (LTRA; e.g, montelukast): counteract the pro-inflammatory effects of leukotrienes by blocking the leukotriene receptor on bronchial smooth muscle
Inhaled/oral corticosteroids (e.g., beclomethasone, prednisolone): inhibit transcription factors (e.g., NF-kB), resulting in an anti-inflammatory effect
Zileuton: inhibits 5-lipoxygenase, resulting in reduced leukotriene production
© AMBOSS
Pharmacotherapy for individuals age 12 years and older
| Preferred medications for stepwise asthma treatment for individuals ≥ 12 years of age | ||
|---|---|---|
| GINA 2025 [6] | NAEPP 2020 [26] | |
| Step 1 |
|
|
| Step 2 |
|
|
| Step 3 |
|
|
| Step 4 |
|
|
| Step 5 |
|
|
| Step 6 |
|
|
Advise patients to seek medical care if they require > 12 inhalations from their ICS/LABA inhaler in a single day. [6]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Pharmacotherapy for individuals age 6 to 11 years
Refer to guidance on stepwise asthma treatment as needed. For younger children, see "Initial maintenance management of asthma in children ≤ 5 years."
| Preferred medications for stepwise asthma treatment for individuals 6–11 years of age | ||
|---|---|---|
| GINA 2025 (6–11 years) [6] | NAEPP 2020 (5–11 years) [25] | |
| Step 1 |
|
|
| Step 2 |
|
|
| Step 3 |
|
|
| Step 4 |
|
|
| Step 5 |
|
|
| Step 6 |
|
|
Adjunctive therapy
Implementing tertiary prevention measures improves symptom control and decreases the frequency of acute asthma exacerbations. [6][26]
-
Reduce exposure to triggers or allergens.
- Indoor/outdoor allergens (e.g., dust, pollen, dust mites)
- Occupational exposure
- Medications
- Consider allergen immunotherapy in allergic asthma.
-
Manage comorbidities.
- Obesity
- Rhinosinusitis and nasal polyps
- Anxiety and depression
- PPI if GERD is suspected
-
Reduce the risk of infection-induced exacerbations.
- Early treatment of infections in infection-triggered asthma
- Immunizations (influenza, COVID-19, pneumococcal vaccines)
-
Lifestyle recommendations
- Provide information and tools for self-monitoring and self-management (e.g., written action plan, peak flow meter).
- Encourage physical activity.
- Encourage a diet rich in fruits and vegetables, e.g., Mediterranean diet, DASH diet
- Smoking cessation
- Promote strategies to reduce stress
-
Social interventions [31][32][33]
- Screen for systemic barriers to care and socioeconomic/environmental risk factors contributing to poor outcomes.
- Provide support to enhance access to care, treatment adherence, and sustainable functional improvement.
Special patient groups
-
Asthma in pregnancy
- Asthma symptoms may be worse, better, or unchanged during pregnancy.
- Same stepwise management as with other patients
- Inhalation treatments preferred
- Poorly managed asthma can increase the risk of pregnancy complications (e.g., preeclampsia, premature birth, congenital abnormalities).
- Monthly monitoring of asthma is recommended.
-
Asthma management in the perioperative patient [6]
- For elective surgery, optimize stepwise treatment of chronic asthma.
- Continue prescribed ICS-containing therapy through the perioperative period.
- Administer perioperative hydrocortisone for patients at high risk of adrenal crisis, e.g.:
- Patients on long-term high-dose ICS
- Patients on oral glucocorticoids for ≥ 2 weeks in the past 6 months [6]
- Asthma in young children: See "Asthma in children ≤ 5 years of age."
Severe perioperative bronchospasm is uncommon but may be life-threatening. [6]
Related One-Minute Telegram
- One-Minute Telegram 134-2025-2/3: Are MDIs a breath of fresh air? Not for the climate
- One-Minute Telegram 99-2024-1/3: Specialized care of newly diagnosed asthma and COPD leads to better outcomes
- One-Minute Telegram 49-2022-1/3: Improving asthma care in Black and Hispanic patients
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- "Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010". https://www.cdc.gov/nchs/data/databriefs/db94.pdf. [2012-05-01]
- "Most Recent Asthma Data". https://web.archive.org/web/20170427014512/https://www.cdc.gov/asthma/most_recent_data.htm. [2017-02-27]
- "Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma, Full Report 2007"
- "Global Strategy for Asthma Management and Prevention (2025 update)". https://ginasthma.org/2025-gina-strategy-report/. [2025-05-06]
- Taylor DR, Bateman ED, Boulet LP, et al. "A new perspective on concepts of asthma severity and control". Eur Respir J. 32(3). :545-554. (2008)
- Reddel HK, Taylor DR, Bateman ED, et al. "An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations". Am J Respir Crit Care Med. 180(1). :59-99. (2009)
- Gauvreau et al. "Effects of Interleukin-13 Blockade on Allergen-induced Airway Responses in Mild Atopic Asthma". Am J Respir Crit Care Med. 183(8). :1007-1014. (2011)
- Lloyd CM, Hessel EM. "Functions of T cells in asthma: more than just T(H)2 cells.". Nat Rev Immunol. 10(12). :838-48. (2010)
- Maselli DJ, Hardin M, Christenson SA, et al. "Clinical Approach to the Therapy of Asthma-COPD Overlap". Chest. 155(1). :168-177. (2019)
- "Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease - 2023 Report". https://web.archive.org/web/20230116094828/https://goldcopd.org/wp-content/uploads/2022/12/GOLD-2023-ver-1.1-2Dec2022_WMV.pdf. [2022-11-01]
- "Global Strategy for Asthma Management and Prevention (2022 update)". https://web.archive.org/web/20230115002305/https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf. [2022-01-01]
- Sam A, Kraft M. "Asthma-COPD Overlap". Curr Pulmonol Rep. 11(1). :1-14. (2022)
- Tarlo SM, Balmes J, Balkissoon R, et al. "Diagnosis and Management of Work-Related Asthma". Chest. 134(3). :1S-41S. (2008)
- Cormier M, Lemière C. "Occupational asthma". The International Journal of Tuberculosis and Lung Disease. 24(1). :8-21. (2020)
- Tarlo SM, Lemiere C. "Occupational Asthma". N Engl J Med. 370(7). :640-649. (2014)
- Shakeri MS, Dick FD, Ayres JG. "Which agents cause reactive airways dysfunction syndrome (RADS)? A systematic review". Occup Med. 58(3). :205-211. (2008)
- Baur X, Sigsgaard T, Aasen TB, et al. "Guidelines for the management of work-related asthma". Eur Respir J. 39(3). :529-545. (2012)
- Stanojevic S, Kaminsky DA, Miller MR, et al. "ERS/ATS technical standard on interpretive strategies for routine lung function tests". Eur Respir J. 60(1). :2101499. (2021)
- Pellegrino R, Viegi G, Brusasco V, et al. "Interpretative strategies for lung function tests.". The European respiratory journal. 26(5). :948-68. (2005)
- Coates AL, Wanger J, Cockcroft DW, et al. "ERS technical standard on bronchial challenge testing: general considerations and performance of methacholine challenge tests". Eur Respir J. 49(5). :1601526. (2017)
- Khatri SB, Iaccarino JM, Barochia A, et al. "Use of Fractional Exhaled Nitric Oxide to Guide the Treatment of Asthma: An Official American Thoracic Society Clinical Practice Guideline". Am J Respir Crit Care Med. 204(10). :e97-e109. (2021)
- Pavel Strnad, Noel G. McElvaney, David A. Lomas. "Alpha1-Antitrypsin Deficiency". N Engl J Med. 382(15). :1443-1455. (2020)
- Sakula A. "Charcot-Leyden crystals and Curschmann spirals in asthmatic sputum". Thorax. 41(7). :503-7. (1986)
- Fahy JV, O'Byrne PM. ""Reactive airways disease". A lazy term of uncertain meaning that should be abandoned.". Am J Respir Crit Care Med. 163(4). :822-3. (2001)
- Cloutier MM, Baptist AP, Blake KV, et al. "2020 Focused Updates to the Asthma Management Guidelines: A Report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group". J Allergy Clin Immunol. 146(6). :1217-1270. (2020)
- Cloutier MM, Dixon AE, Krishnan JA, et al. "Managing Asthma in Adolescents and Adults". JAMA. 324(22). :2301. (2020)
- Clark NM, KeteyianSR, Partridge M, Griffiths C. "Educational and behavioral interventions for asthma: who achieves which outcomes? A systematic review". Journal of Asthma and Allergy. :187. (2010)
- Labre MP, Herman EJ, Dumitru GG, Valenzuela KA, Cechman CL. "Public Health Interventions for Asthma". Am J Prev Med. 42(4). :403-410. (2012)
- Naar S, Ellis D, Cunningham P, et al. "Comprehensive Community-Based Intervention and Asthma Outcomes in African American Adolescents". Pediatrics. 142(4). :e20173737. (2018)
- "ZYFLO® (zileuton tablets)"
- "Intal® Nebulizer Solution (cromolyn sodium inhalation solution, USP)"
- "XOLAIR® (omalizumab) for injection, for subcutaneous use"
- "NUCALA (mepolizumab) for injection, for subcutaneous use"
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Lippincott Williams & Wilkins. (2013). ISBN: 9781609133603
- Le T, Bhushan V, Bagga HS. "First Aid for the USMLE Step 2 CK". McGraw-Hill Medical. (2009). ISBN: 9780071623544
- Saadeh CK. "Status Asthmaticus". WebMD. http://emedicine.medscape.com/article/2129484. [2017-03-03]
- Little M. "Asthma in Pregnancy". WebMD. http://emedicine.medscape.com/article/796274. [2016-06-06]
- Niimi A. "Cough and asthma". Curr Respir Med Rev. 7(1). :47-54. (2011)
- David R Stather, Thomas E Stewart. "Clinical review: mechanical ventilation in severe asthma". Crit Care. 9(6). :581-587. (2005)
- Fala L. "Nucala (Mepolizumab): First IL-5 Antagonist Monoclonal Antibody FDA Approved for Maintenance Treatment of Patients with Severe Asthma.". American health & drug benefits. 9(Spec Feature). :106-10. (2016)
- "Global Initiative for Asthma (GINA) GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION". https://ginasthma.org/wp-content/uploads/2019/04/GINA-2019-main-Pocket-Guide-wms.pdf. [2019-01-01]
- Camargo CA, Rachelefsky G, Schatz M. "Managing Asthma Exacerbations in the Emergency Department: Summary of the National Asthma Education and Prevention Program Expert Panel Report 3 Guidelines for the Management of Asthma Exacerbations". Proc Am Thorac Soc. 6(4). :357-366. (2009)
- Brenner B, Corbridge T, Kazzi A. "Intubation and Mechanical Ventilation of the Asthmatic Patient in Respiratory Failure". Proc Am Thorac Soc. 6(4). :371-379. (2009)
- Prasad Kerlin M. "Asthma". Ann Intern Med. 160(5). :ITC3-1. (2014)
- Dweik RA, Boggs PB, Erzurum SC, et al. "An Official ATS Clinical Practice Guideline: Interpretation of Exhaled Nitric Oxide Levels (FeNO) for Clinical Applications". Am J Respir Crit Care Med. 184(5). :602-615. (2011)
- Pardue Jones B, Fleming GM, Otillio JK, Asokan I, Arnold DH. "Pediatric acute asthma exacerbations: Evaluation and management from emergency department to intensive care unit". Journal of Asthma. 53(6). :607-617. (2016)
- Moriates C, Feldman L. "Nebulized bronchodilators instead of metered-dose inhalers for obstructive pulmonary symptoms". Journal of Hospital Medicine. 10(10). :691-693. (2015)
- Simonds A, Hanak A, Chatwin M, et al. "Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections". Health Technol Assess (Rockv). 14(46). :131-172. (2010)
- Dissanayake S, Suggett J. "A review of the in vitro and in vivo valved holding chamber (VHC) literature with a focus on the AeroChamber Plus Flow-Vu Anti-static VHC". Therapeutic Advances in Respiratory Disease. 12. :175346581775134. (2018)