Summary
Autoimmune hepatitis (AIH) is a rare form of chronic hepatitis that predominantly affects women. Although the etiology is unclear, it is commonly associated with other autoimmune conditions (e.g., thyroid disease, type 1 diabetes mellitus, celiac disease). The clinical presentation ranges from asymptomatic transaminitis to acute liver failure. Diagnosis is established based on the detection of autoantibodies (e.g., antinuclear antibodies, anti-smooth muscle antibodies) and the histologic findings of interface hepatitis on liver biopsy. Treatment consists of immunosuppressive medications such as prednisone and azathioprine. The prognosis is favorable with treatment; without treatment, patients may develop cirrhosis and liver failure.
Classification
- Type 1 AIH (80% of cases): characteristic autoantibodies include antinuclear antibodies (ANAs), anti-smooth muscle antibodies (ASMAs) anti-soluble liver antigen antibodies (anti-SLA)
- Type 2 AIH: characteristic autoantibodies include anti-liver-kidney microsomal-1 antibodies (anti-LKM-1), anti-liver cytosol antibodies-1 (ALC-1)
Epidemiology
- Prevalence: 0.1–2/100,000 white adults in the US, even less so in other ethnicities [1]
-
Bimodal distribution: 10–20 years and 40–60 years [2]
- Type 1 AIH: most common in adults
- Type 2 AIH: most common in children
-
Sex: ♀ > ♂
- Type 1 AIH: (∼ 4:1) [3]
- Type 2 AIH: (∼ 10:1)
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Idiopathic [4]
-
AIH is commonly associated with other autoimmune conditions
- Type 1 AIH: Hashimoto thyroiditis, Graves disease, ulcerative colitis, celiac disease, rheumatoid arthritis
- Type 2 AIH: Hashimoto thyroiditis, type 1 diabetes mellitus, vitiligo
Clinical features
AIH has an insidious onset in most patients and its presentation varies widely, ranging from asymptomatic disease to severe symptoms or even acute liver failure.
-
Nonspecific symptoms
- Fatigue
- Upper abdominal pain
- Weight loss
- Signs of acute liver failure (∼ ⅓ of patients)
- Signs of chronic liver disease

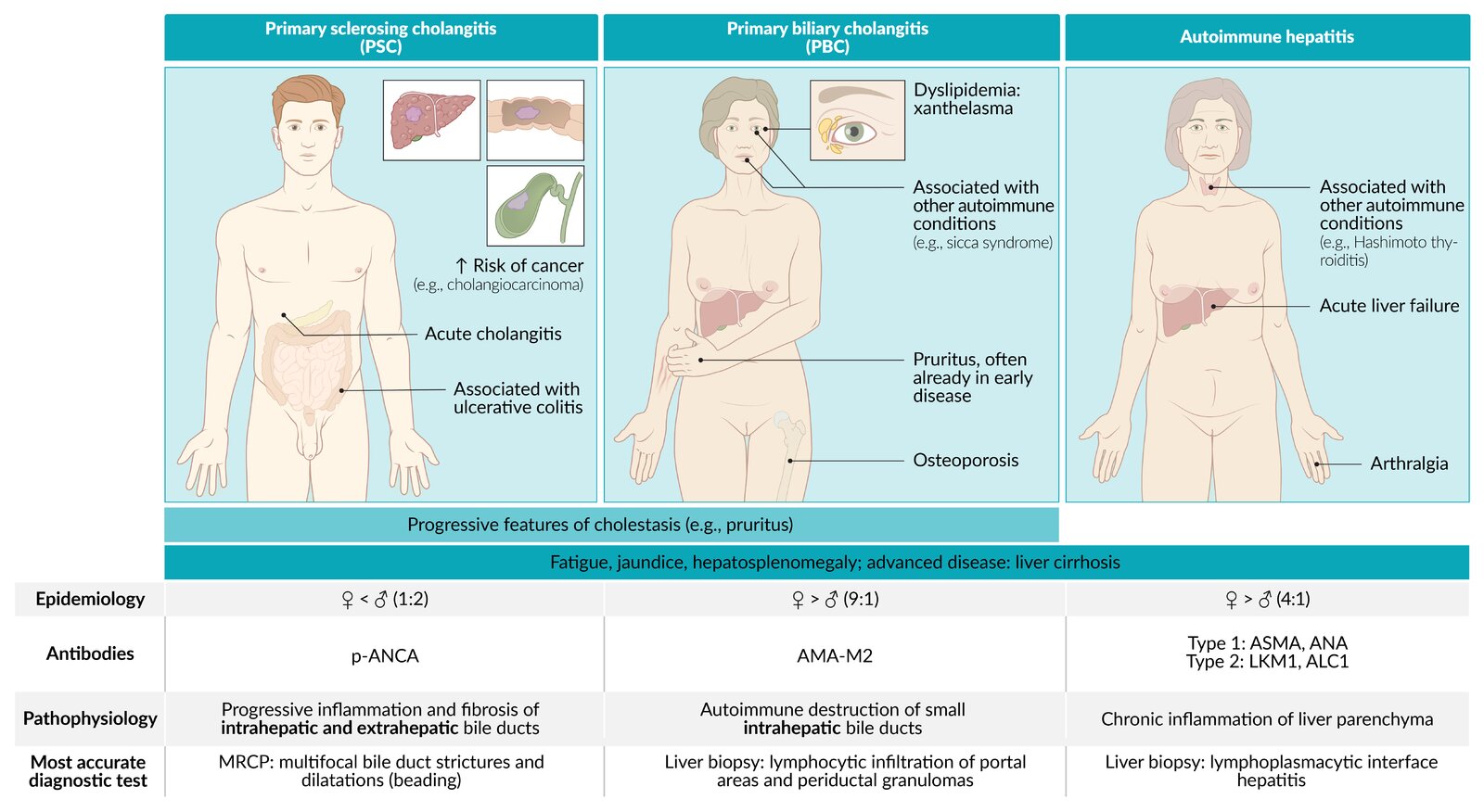
Overview illustration comparing clinical features, epidemiology, pathophysiology, and diagnostics of primary sclerosing cholangitis (PSC), primary biliary cholangitis (PBC), and autoimmune hepatitis.
© AMBOSS
Diagnosis
Approach [5]
- Consider AIH in patients with unexplained liver disease.
- Rule out other causes of hepatitis; see “Differential diagnoses.”
- Establish the diagnosis of AIH with laboratory studies and liver histology.
- Consider utilizing the Autoimmune Hepatitis Diagnosis calculator to facilitate the diagnosis. [6]
- Consult hepatology for guidance on further diagnostic testing.
The diagnosis of AIH is based on positive autoantibodies (e.g., ANA, ASMA) and histological findings of interface hepatitis on biopsy.

Initial studies [5]
Laboratory tests [7][8]
- Liver chemistries: ↑↑↑ ALT and ↑↑ AST; , ↑ GGT, normal or ↑ ALP, and ↑ bilirubin
-
Serum antibodies
- ANA, ASMA: combination is highly specific for type 1 AIH [7]
- Anti-LKM-1: typically positive in type 2 AIH
- SPEP: hypergammaglobulinemia (↑ IgG)
- CBC: normochromic anemia, thrombocytopenia, mild leukopenia
- Inflammatory markers: ↑ ESR
Liver biopsy [7]
- Perform following the detection of AIH antibodies to confirm the diagnosis.
-
Histological findings:
- Lymphoplasmacytic interface hepatitis: ongoing inflammatory process with lymphocytic infiltration, bridging or multiacinar necrosis, and fibrotic changes
- Centrilobular perivenulitis and necrosis
- Hepatocyte emperipolesis [7]
- Hepatocyte rosettes
- Bile duct changes (e.g., cholangitis, ductal injury)

Additional evaluation [5]
- Obtain further serum antibodies to clarify diagnosis if initial antibody testing is negative.
- ALC-1 (type 2 AIH), anti-SLA (type 1 AIH)
- Antimitochondrial antibody: rare in AIH; may indicate AIH-PBC overlap
- pANCA: may be present in type 1 AIH or AIH-PSC overlap
- Screen all patients for concomitant celiac disease (with anti-tTG) and thyroid disease (with TSH).
- Assess for other common comorbidities (e.g., rheumatoid arthritis, diabetes mellitus, inflammatory bowel disease) based on clinical suspicion.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
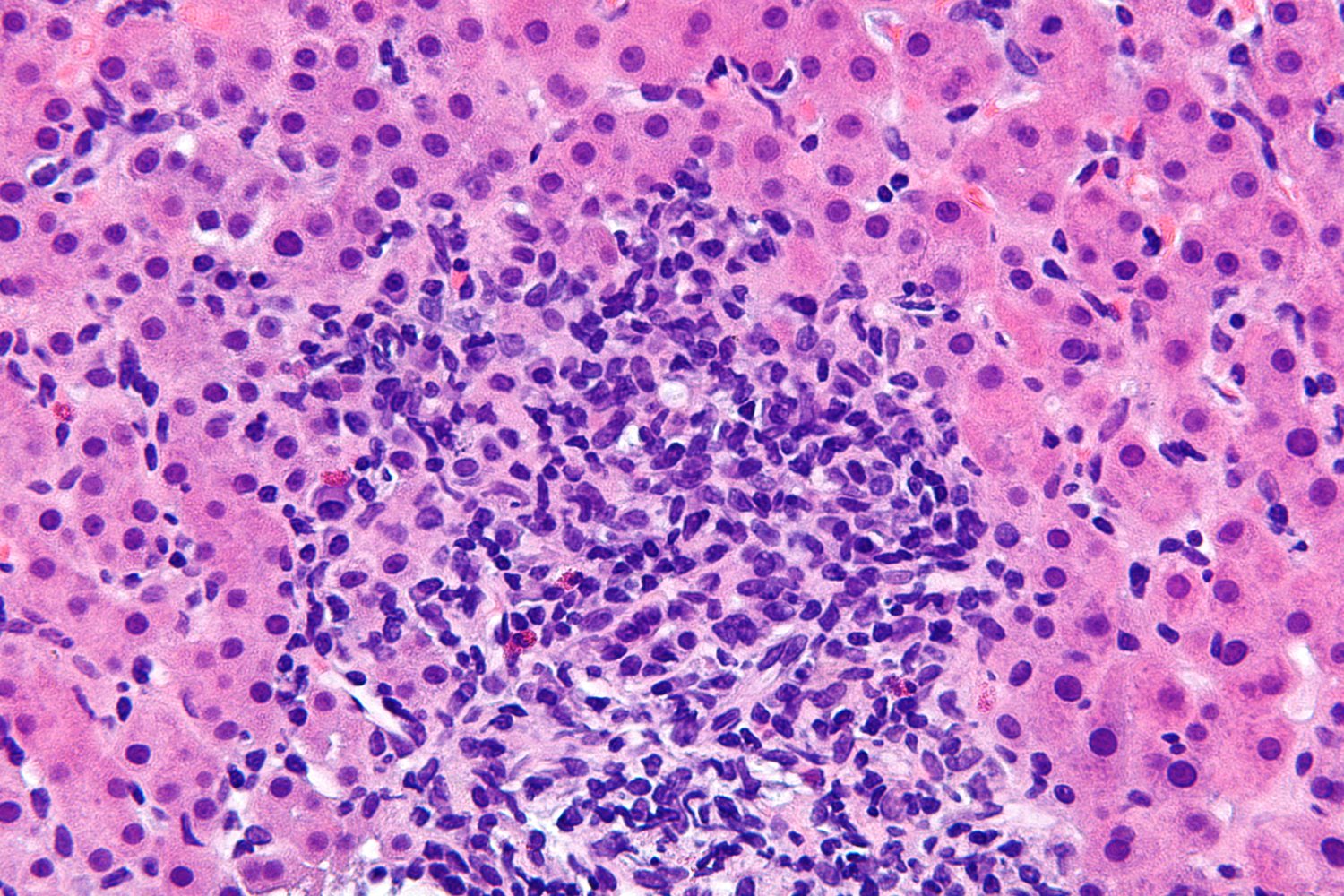
Photomicrograph of a liver biopsy specimen (H&E stain; high magnification)
A chronic inflammatory infiltrate consisting of plasma cells (examples indicated by yellow overlay), lymphocytes (multiple blue basophilic nuclei), and a few scattered eosinophilic granulocytes (examples indicated by green overlay) can be seen in the center of the image. The infiltrate is located at the interface of the portal tract and hepatic lobule, which is referred to as “interface hepatitis.”
Normal hepatocytes, identifiable as polygonal cells with prominent round nuclei and eosinophilic cytoplasm, are visible on the right and left side of the infiltrate (examples indicated by blue overlay).
Chronic interface hepatitis in combination with an abundance of plasma cells is suggestive of autoimmune hepatitis.
Source: “Autoimmune hepatitis - very high mag.jpg” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
- Viral hepatitis (e.g., hepatitis C)
- Primary sclerosing cholangitis
- Primary biliary cholangitis
- Alcohol-associated liver disease
- Metabolic dysfunction-associated steatohepatitis
- Drug-induced liver injury
- Drug-induced autoimmune-like hepatitis (DIAH)
- Hemochromatosis
- Wilson disease
The differential diagnoses listed here are not exhaustive.
Treatment
General principles [5][7]
- Initiate management of acute liver failure if necessary.
- Refer patients to a hepatologist for management.
-
Immunosuppression is the mainstay of treatment.
- Provide age-appropriate immunizations and pretreatment counseling.
- Prevent complications of glucocorticoid therapy.
- Liver transplantation is indicated in patients with decompensated liver cirrhosis.
Pharmacotherapy [5]
- Indication: active disease (i.e., elevated transaminases, elevated IgG, and/or histological disease)
-
Goals of treatment
- Reduce symptoms.
- Reverse liver inflammation and fibrosis.
- Achieve remission.
-
Induction therapy
- First line: glucocorticoids (e.g., prednisone or prednisolone) with or without azathioprine (AZA)
- Alternatives: mycophenolate, tacrolimus, infliximab, rituximab
- Maintenance: glucocorticoid discontinuation after gradual tapering; continue AZA.
-
Monitoring
- Check ALT, AST, IgG levels to assess for biochemical response and remission. [5]
- Conduct transient elastography at least 6 months after successful treatment to assess for advanced fibrosis or cirrhosis
-
Treatment withdrawal
- Consider in patients with biochemical remission for ≥ 2 years.
- Consider repeat liver biopsy to exclude active inflammation prior to withdrawal.
- Relapse is common; obtain AST, ALT, and IgG levels at regular intervals. [5]
Do not use azathioprine in patients with decompensated cirrhosis or acute severe AIH (i.e., jaundice, INR > 1.5). [5]
Prognosis
-
10-year survival rate with treatment: > 90% [9]
- Lifelong therapy is usually required.
- Increased risk of developing hepatocellular carcinoma (HCC): Follow-ups are recommended.
- Type 2 AIH is associated with more severe disease, a worse response to corticosteroids, and more frequent relapses.
- Increased risk of liver cirrhosis if left untreated
External Resources
References
- Muri Boberg K. "Prevalence and epidemiology of autoimmune hepatitis". Clin Liver Dis. 6(3). :635-647. (2002)
- Baven-Pronk MAMC, Biewenga M, van Silfhout JJ, et al. "Role of age in presentation, response to therapy and outcome of autoimmune hepatitis.". Clinical and translational gastroenterology. 9(6). :165. (2018)
- Czaja AJ, Donaldson PT. "Gender effects and synergisms with histocompatibility leukocyte antigens in type 1 autoimmune hepatitis.". Am J Gastroenterol. 97(8). :2051-7. (2002)
- Hardtke-wolenski M, Fischer K, Noyan F, et al. "Genetic predisposition and environmental danger signals initiate chronic autoimmune hepatitis driven by CD4+ T cells". Hepatology. 58(2). :718-28. (2013)
- Mack CL, Adams D, Assis DN, et al. "Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases". Hepatology. 72(2). :671-722. (2020)
- Alvarez F, Berg PA, Bianchi FB, et al. "International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis". J Hepatol. 31(5). :929-938. (1999)
- Mieli-Vergani G, Vergani D, Czaja AJ, et al. "Autoimmune hepatitis". Nat Rev Dis Primers. 4(1). (2018)
- Kwo PY, Cohen SM, Lim JK. "ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries". Am J Gastroenterol. 112(1). :18-35. (2017)
- Roberts S, Therneau T, Czaja A. "Prognosis of histological cirrhosis in type 1 autoimmune hepatitis". Gastroenterology. 110(3). :848-857. (1996)