CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by reading information in this article to address a clinical question, and then completing a brief evaluation, in which they will identify their question and report the impact of any information learned on their clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and Links" at the bottom of this article.
Summary
Avascular necrosis is a condition in which bone tissue becomes ischemic and begins to suffer pathologic decomposition, leading to joint dysfunction. Avascular necrosis (AVN) affects all age groups and is caused by direct trauma, medications, cellular insult, or mechanical compression, often in the context of predisposing conditions. Susceptible joints include the hip, knee, shoulder, wrist, and ankle. Disease type is typically characterized by location, often with eponymous names. Joint movement is decreased and pain is localized to the affected joint. Patients may be asymptomatic in early stages. X-ray is used for initial imaging, and MRI is required for definitive diagnosis. Management is typically surgical and may include total joint replacement in later stages.
For management specific to avascular necrosis of the hip, see “Osteonecrosis of the femoral head.”
Overview
Affected structures [2][3][4]
The bone tissue ischemia and necrosis characteristic of AVN most commonly affect the epiphysis of long bones.
- Hip: femoral head (most common); see also “Osteonecrosis of the femoral head.”
- Knee: medial femoral condyle
- Ankle: talar neck
- Shoulder: humeral head
- Wrist: scaphoid, lunate, capitate
Specific types of avascular necrosis
| Overview of special types of avascular necrosis | ||||
|---|---|---|---|---|
| Condition | Localization | Epidemiology | Etiology | Clinical features |
| Kienbock disease |
|
|
|
|
| Legg-Calvé-Perthes disease |
|
|
|
|
| Kohler disease |
|
|
|
|
| Freiberg disease |
|
|
|
|


X-ray right foot (dorsoplantar view)
Sclerosis (green overlay) and flattening (indicated by white line) of the articular surface of the 3rd metatarsal head are consistent with prior avascular necrosis. Osteophytes (examples indicated by red overlay) have formed on both sides of the widened joint space.
Freiberg disease (previously known as Freiberg infarction) is avascular necrosis (osteonecrosis) of a metatarsal bone. It typically develops in the second metatarsal head, but may involve any metatarsal bone.
Source: © IMPP
Etiology
- Trauma (e.g., proximal scaphoid fractures)
- Cellular toxicity (e.g., chemotherapy, radiotherapy, thermal injury, smoking, alcohol)
- Medication (e.g., corticosteroids)
- Congenital disease (e.g., sickle cell disease, Gaucher disease)
- Orthopedic conditions (e.g., slipped capital femoral epiphysis, developmental dysplasia of the hip)
- Intraosseous compression (e.g., hemorrhage, elevated bone marrow pressure)
Clinical features
- Early stage: usually asymptomatic [5]
- Advanced stage: limited movement, pain, and/or swelling in the affected joint [6][7]
Diagnosis
- Clinical evaluation: history of trauma, glucocorticoid use, or other risk factors for AVN
-
X-ray [2][6][8]
- First line to rule out acute fracture; may be nondiagnostic in early stages
- Findings include subchondral fracture, sclerosis, cystic changes, and bone collapse.
-
MRI without contrast [6][8]
- Gold standard (highly sensitive) [2]
- Findings depend on the stage and the bone affected.
Glucocorticoid use and chronic heavy drinking are the most common causes of nontraumatic avascular necrosis. [5]



X-ray right hip (AP view)
The articular surface of the femoral head is irregular (black dotted line) and the underlying bone is heterogeneous (green overlay) as a result of osteonecrosis. A zone of sclerosis (red overlay) is present along the interface with normal bone.
Source: © IMPP
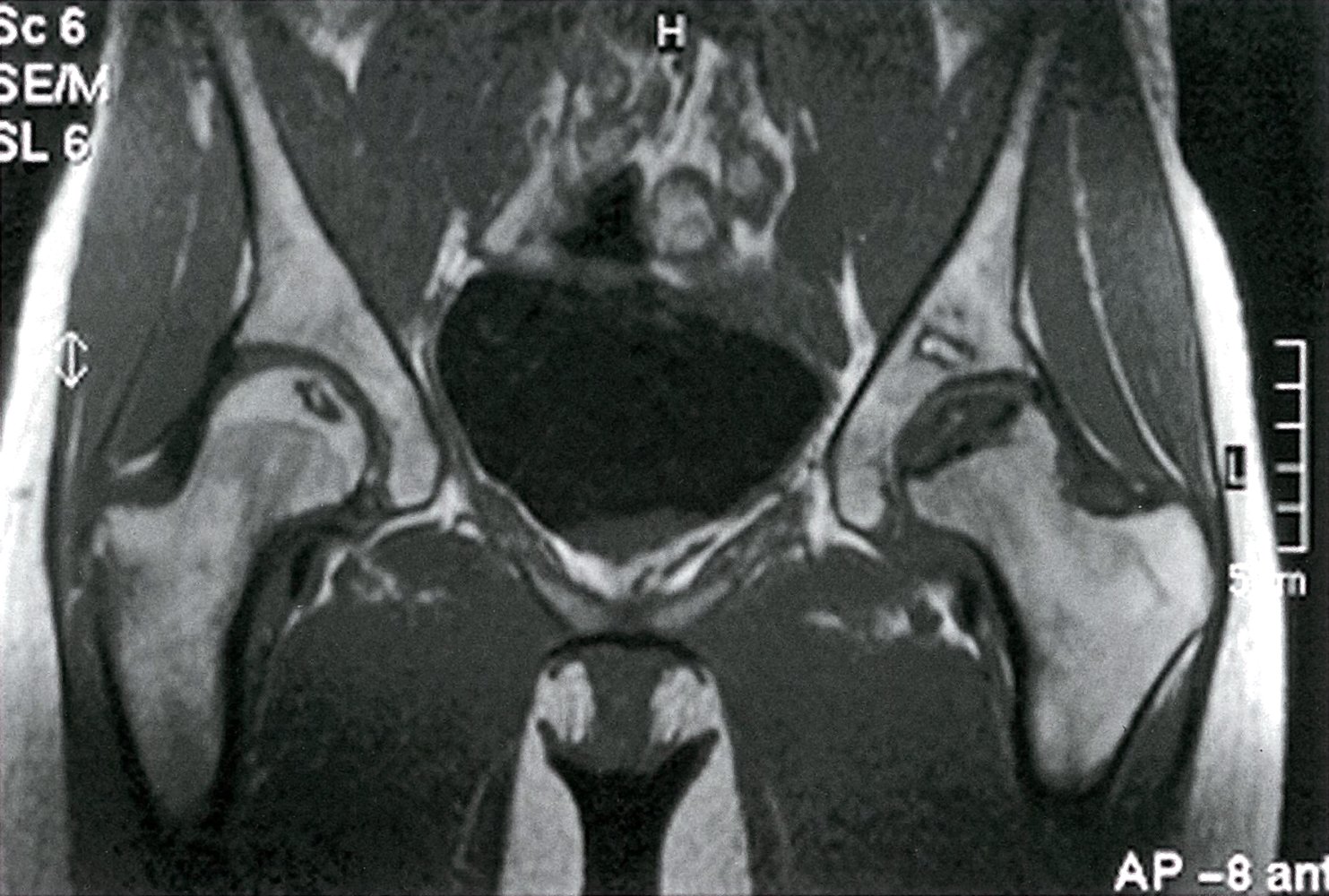
MRI hips (T1 weighted; coronal view) of a 32-year-old woman with groin pain
There is a well-defined crescent-shaped area of intermediate to low signal within the subchondral marrow of the left femoral head (green overlay). A thick peripheral band of even lower signal separates this region from the hyperintense normal bone marrow (red overlay). On the right side, there is a slightly smaller area of abnormal oval-shaped signal within the epiphysis of the right femoral head (blue overlay). The center of this region demonstrates a small area of hyperintense signal (indicated by arrow) and it also displays a very low signal periphery.
The region of intermediate to low signal within the left femoral head represents necrotic bone marrow. The thick band of very low signal surrounding this region of necrotic bone marrow represents the reactive interface between the normal and necrotic bone. On fluid-sensitive sequences, it is often demonstrated as two lines of differing signal, an inner hyperintense line and an outer hypointense line, known as the double line sign. This is pathognomonic for osteonecrosis. The smaller area of osteonecrosis in the right femoral head is in an earlier stage than the left, as it is smaller and the central region still demonstrates the expected hyperintense signal of bone marrow. Osteonecrosis of the femoral head is often bilateral unless the etiology is traumatic.
Source: © IMPP
Treatment
Treatment varies depending on location and stage of disease; refer to orthopedics for management as surgery is often required for definitive treatment. See also “Treatment of AVN of the femoral head.” [5]
-
Treatment goals [5][6]
- Preventing bone collapse, long-term disability, and chronic pain
- Preserving joint function
-
Nonoperative management: for early stages and/or symptomatic relief [5]
- Reduce weight-bearing on the joint.
- Pain management
- Risk factor reduction, e.g. smoking cessation
- Physiotherapy
-
Surgical treatment
-
Core decompression
- Operative decompression of the affected bone to restore perfusion
- May be indicated in early stages [9]
- Bone graft
- Joint replacement (e.g., hip, shoulder, knee)
-
Core decompression
Early detection and prompt treatment significantly improve prognosis. [5]
External Resources
References
- Ha AS, Chang EY, Bartolotta RJ, et al. "ACR Appropriateness Criteria® Osteonecrosis: 2022 Update". J Am Coll Radiol. 19(11). :S409-S416. (2022)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Cooper C, Steinbuch M, Stevenson R, et al. "The epidemiology of osteonecrosis: findings from the GPRD and THIN databases in the UK". Osteoporos Int. 21(4). :569-577. (2009)
- Chang C, Greenspan A, Beltran J, Gershwin ME. "Osteonecrosis". Kelley and Firestein's Textbook of Rheumatology. :1764-1787.e5. (2017)
- Afshar A, Tabrizi A. "Avascular Necrosis of the Carpal Bones Other Than Kienböck Disease". J Hand Surg. 45(2). :148-152. (2020)
- Larson E, Jones LC, Goodman SB, Koo K-H, Cui Q. "Early-stage osteonecrosis of the femoral head: where are we and where are we going in year 2018?". Int Orthop. 42(7). :1723-1728. (2018)
- Choi HR, Steinberg ME, Y. Cheng E. "Osteonecrosis of the femoral head: diagnosis and classification systems". Current Reviews in Musculoskeletal Medicine. 8(3). :210-220. (2015)
- Hua K chi, Yang X gang, Feng J tao, et al. "The efficacy and safety of core decompression for the treatment of femoral head necrosis: a systematic review and meta-analysis". J Orthop Surg. 14(1). (2019)
- "Contributor Disclosures - Avascular necrosis. None of the individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"