CME information and disclosures
To see contributor disclosures related to this article, click on this reference: [1].
Physicians can earn CME/MOC credit by using this article to address a clinical question and completing a brief evaluation about how they applied the information in their practice.
AMBOSS designates this internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and links” at the bottom of this article.
Quick guide
Diagnostic approach
- Focused clinical evaluation
- Order tests based on the suspected etiology of back pain or presence of red flags for back pain.
- Cauda equina syndrome or conus medullaris syndrome: MRI L-spine without IV contrast
- Vertebral fracture: CT spine without contrast
- Spinal epidural abscess or vertebral osteomyelitis: CBC, ESR, CRP, blood cultures, MRI with and without IV contrast
- Aortic dissection or AAA rupture: CTA chest, abdomen, and pelvis
- Spinal epidural hematoma: CBC, PT, PTT, MRI with and without IV contrast
- Malignancy: MRI with and without IV contrast
- See “Approach to imaging in back pain.”
Diagnostic testing is not routinely indicated for acute back pain.
Management checklist
- Most cases of acute, nonspecific back pain improve without intervention.
- Treat acute complications (e.g., Foley catheter placement for acute urinary retention).
- Treat the underlying cause.
- Conservative management of nonspecific back pain (e.g. NSAIDs).
- Order spinal precautions for suspected fracture.
- See “Management of traumatic back pain.”
- See “Management of compressive spinal emergencies.”
Red flag features
- Age < 18 or > 50 years
- IV drug use
- History of malignancy
- History of AAA
- Recent trauma or spine surgery
- Immunosuppression
- Medications (e.g., chronic glucocorticoids, anticoagulation)
- Abnormal vitals (e.g., fever)
- Signs of aortic pathology (e.g., aortic regurgitation)
- Signs of spinal cord compression
- Features of compressive myopathies
- Pain that is worse at night and/or does not improve with rest
Life-threatening causes
- Vertebral fractures
- Vertebral osteomyelitis
- Spinal cord compression
- Spinal epidural abscess
- Cauda equina syndrome
- Aortic dissection
- AAA rupture
- Spinal epidural hematoma
- Conus medullaris syndrome
Summary
Back pain is experienced by most adults. The majority of cases are benign, nonspecific back pain (pain that is not attributable to a specific pathology). Spinal causes of acute back pain are conditions of the spinal column or surrounding muscles and soft tissue. Spinal causes include conditions that require urgent management to prevent or minimize permanent neurological dysfunction (e.g., spinal cord compression, spinal infections) and nonurgent causes (e.g., inflammatory arthritis, bone metastases without cord compression or unstable vertebral fracture). Nonspinal causes of back pain is referred pain from a thoracic, abdominal, pelvic, retroperitoneal, or cardiovascular cause. Assessment for red flag features of back pain and a focused neurological examination is required in all patients. Initial diagnostics and management should be guided by the pretest probability of the underlying condition. Patients with new neurological findings other than isolated unilateral radiculopathy require immediate imaging, typically MRI, and urgent spinal surgery consultation. Serious and life-threatening nonspinal causes, such as myocardial infarction and aortic pathology, should be considered particularly in patients with abnormal vital signs and no neurological abnormalities. Neurologically intact patients without red flags do not require urgent imaging and typically improve with nonpharmacological treatment options (e.g., superficial application of heat, massage), symptomatic treatment with NSAIDs, and early mobilization.
Classification
By etiology [2][3]
-
Specific back pain
- Back pain attributable to a pathophysiological condition (e.g., trauma, deformity, disease, injury, or infection); see “Etiology” section for details.
- Mechanical back pain: specific back pain caused by disorders of the spine, intervertebral discs, or surrounding soft tissue [4]
- Nonspecific back pain: back pain that cannot be attributed to a specific cause after a full evaluation.
- Spinal causes: conditions of the spinal column or surrounding muscles and soft tissue
- Nonspinal causes: include thoracic, abdominal, pelvic, retroperitoneal, or cardiovascular conditions that can manifest with referred pain to the back.
By duration [2][5][6]
- Acute back pain: pain lasting ≤ 4 weeks
- Subacute back pain: pain lasting 4–12 weeks
- Chronic back pain: persistent or recurring back pain lasting > 12 weeks
By location
-
Low back pain (LBP) [2][3]
- Pain localized to the lumbar region (below the costal margin) and above the gluteal folds; may be associated with pain that radiates down the legs
-
LBP is typically further classified into three broad categories: [7]
- Nonspecific LBP (most common) [8]
- LBP associated with radiculopathy or spinal stenosis
- LBP associated with a specific spinal cause (see “Spinal causes of back pain”)
- Upper back pain: pain localized to the thoracic spine region
By severity [9]
- Uncomplicated back pain: no red flag features of back pain
- Complicated back pain: presence of red flag features of back pain
Epidemiology
- 2–3% of visits to the ED are for acute nontraumatic back pain. [10]
- In the US, low back pain affects up to 85% of individuals and, worldwide, is the leading cause of years lived with disability. [11][12][13]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Trauma can cause both spinal and nonspinal causes of back pain.
Musculoskeletal
- Intervertebral disc herniation or disc protrusion
- Spinal stenosis
- Scoliosis
- Spinal osteoarthritis (spondylosis), degenerative disc disease
- Spondylolysis, spondylolisthesis
- Vertebral fractures
- Musculoskeletal spinal injury (back strain)
- Rib fractures
Neoplastic
- Spinal metastases
- Referred pain from primary neoplastic process (e.g., renal cancer, pancreatic cancer)
- Primary spinal tumors
Infectious
- Spinal epidural abscess
- Discitis
- Vertebral osteomyelitis
- Pott disease
Vascular
- Spinal epidural hematoma
- Spinal cord infarction
Inflammatory
- Ankylosing spondylitis
- Psoriatic arthritis
- Reactive arthritis
Referred pain
- Cardiovascular: abdominal aortic aneurysm (AAA), aortic dissection, myocardial infarction, pericarditis
- Pulmonary: pneumonia, pleurisy, pulmonary embolism
- Gastrointestinal: esophageal perforation, esophageal spasm, perforated peptic ulcer, pancreatitis, cholecystitis, cholangitis
- Genitourinary: pyelonephritis, prostatitis, nephrolithiasis, hydronephrosis, renal infarction
- Other: psoas abscess, retroperitoneal hematoma
Clinical evaluation
- Assess for red flag features of back pain in all patients.
- Duration of symptoms
- Evaluate for psychosocial risk factors
- Perform a thorough neurological examination to assess for any neurological deficits.
- Sensation, power (motor strength), deep tendon reflexes, and superficial reflexes (e.g., Babinski reflex) below the level of the pain bilaterally (including relevant myotomes and dermatomes)
- Signs of radiculopathy/nerve root irritation (e.g., straight leg raise test)
- Perianal sensation and anal tone [10]


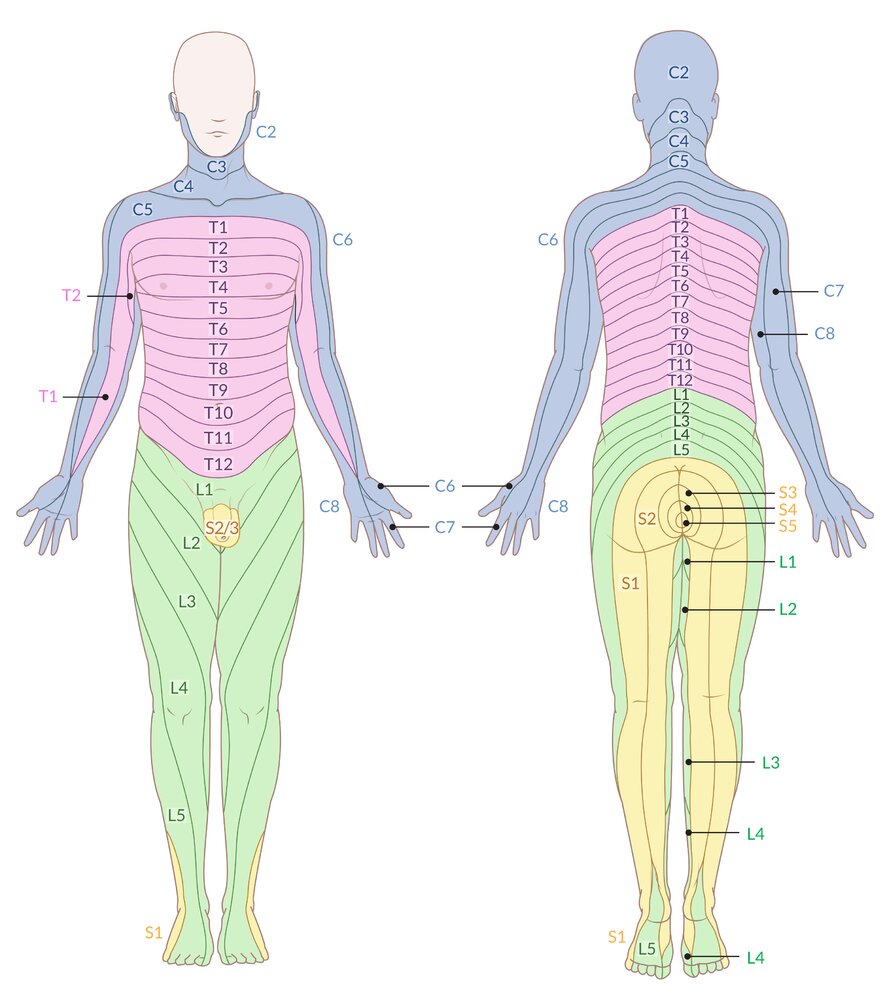
Schematic representation of the body's dermatomes (i.e., areas of skin that are innervated by a single sensory spinal root)
Note: Nearly all dermatome maps refer to publications by Head and Campbell (1900), Foerster (1933), or Keegan and Garrett (1948), which differ significantly in some areas. After careful review of the current literature, this illustration has been based on Keegan and Garrett's work, as it is most likely to be based on valid methodology and correlates with established clinical findings.
© AMBOSS
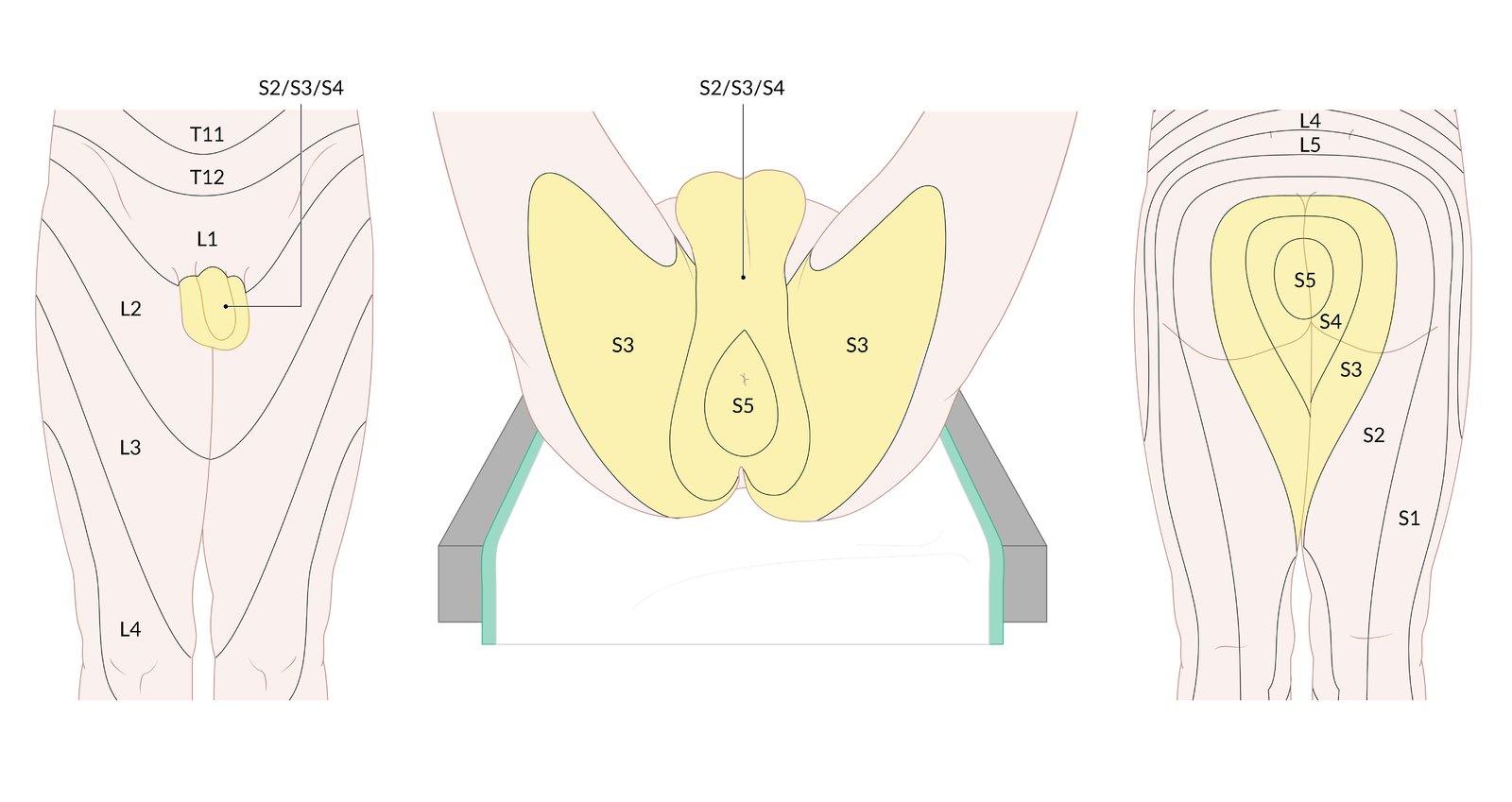
Sensory loss restricted to the perianal, perineal, and superomedial aspects of the thighs and buttocks (S2–S5 dermatome regions).
Saddle anesthesia indicates lumbar spinal injury or disease (e.g., conus medullaris syndrome, cauda equina syndrome).
© AMBOSS
Red flags for back pain
Red flag features on history or clinical examination indicate an urgent or serious underlying etiology.
| Red flags for back pain [2][8][10] | |
|---|---|
| Features | |
| Patient characteristics |
|
| Relevant medical history |
|
| Medication use |
|
| Pain characteristics |
|
| Examination findings |
|
Hypotension and bradycardia in a patient with signs of spinal cord compression are likely indicators of spinal shock. [18]
Pathological fractures, bone metastases, or referred pain (e.g., myocardial infarction, abdominal aortic aneurysm, aortic dissection) are more likely in older individuals with back pain.
Sensory loss restricted to the perianal, perineal, and superomedial aspects of the thighs and buttocks (S2–S5 dermatome regions).
Saddle anesthesia indicates lumbar spinal injury or disease (e.g., conus medullaris syndrome, cauda equina syndrome).
© AMBOSS
Initial management
- Perform focused clinical history and examination.
- Assess for red flag features of back pain and risk stratify accordingly.
- Low suspicion for serious or urgent etiology: supportive care, pain management, close follow-up and return precautions usually sufficient [8]
- High suspicion for serious or urgent etiology: targeted and expedited evaluation to identify and treat the underlying cause, e.g., [10][19]
- Concern for spinal infection: urgent MRI with and without IV contrast, empiric antibiotics, neurosurgery consult
- Concern for compressive spinal emergency: urgent MRI spine with and without IV contrast, urgent neurosurgery consult; See “Management of compressive spinal emergencies.”
- Suspected fracture: spinal precautions, XR spine; See “Management of traumatic back pain.”
- Evaluate and treat the underlying cause.
- Administer analgesics (preferably NSAIDs) after baseline neurological function and pain severity are documented. [7][10]
Most cases of acute, nonspecific back pain do not require imaging and improve without intervention. [20]
Acute spinal cord compression is a surgical emergency. Obtain immediate MRI or CT myelography, give IV glucocorticoids for malignant compression, and decompress the cord (e.g., with surgery) as soon as possible!
Diagnosis
Imaging [6][7][21][22]
- Indications for imaging may include: [6]
- Suspicion of a serious underlying etiology
- Pain that persists despite at least 4–6 weeks of conservative management.
| Approach to imaging in back pain [6][7] | |
|---|---|
| Suspected urgent spinal cause (e.g., severe or progressive neurological deficits, features of spinal infection, features of spinal malignancy, cauda equina) |
|
| Suspected inflammatory cause (e.g., ankylosing spondylitis) |
|
| Suspected vertebral fracture |
|
| Isolated radiculopathy and/or clinical features of spinal stenosis without any red flags |
|
| Suspected nonspinal causes of back pain |
|
| Nonspecific back pain |
|
In patients presenting with acute back pain without red flags or neurological deficits, imaging is not typically indicated. [7]
Laboratory studies
- Laboratory studies are not routinely required for the evaluation of acute or chronic back pain.
-
Consider obtaining laboratory studies based on the likely underlying etiology and/or the presence of red flags for back pain, e.g.:
- CBC and inflammatory markers: for suspected spinal infections, inflammatory arthritis, or malignancy
- Blood cultures: for suspected spinal infections
- Serum calcium and vitamin D levels: for suspected fragility fractures
Urgent spinal causes of acute back pain
- Urgent spinal causes of back pain include conditions that cause, or have the potential to cause, permanent neurological damage or life-threatening complications.
- Immediate management is required for patients with severe and/or progressive neurological deficits. [10]
| Overview of urgent spinal causes of back pain | |||
|---|---|---|---|
| Characteristic clinical features | Diagnostic findings | Management | |
| Compressive spinal emergencies [17][23] |
|
|
|
|
Vertebral fractures (pathological or traumatic)[24] |
|
|
|
| Spinal infections [26] |
|
|
|
| Spinal epidural hematoma causing cord compression [27] |
|
|
|
Acute urinary retention in a patient with sudden back pain and neurological deficits is strongly suggestive of cauda equina syndrome (90% sensitivity). [7]
Spinal boards should only be used for transport; remove patients from them on arrival at the hospital to reduce pain and prevent the development of pressure ulcers!










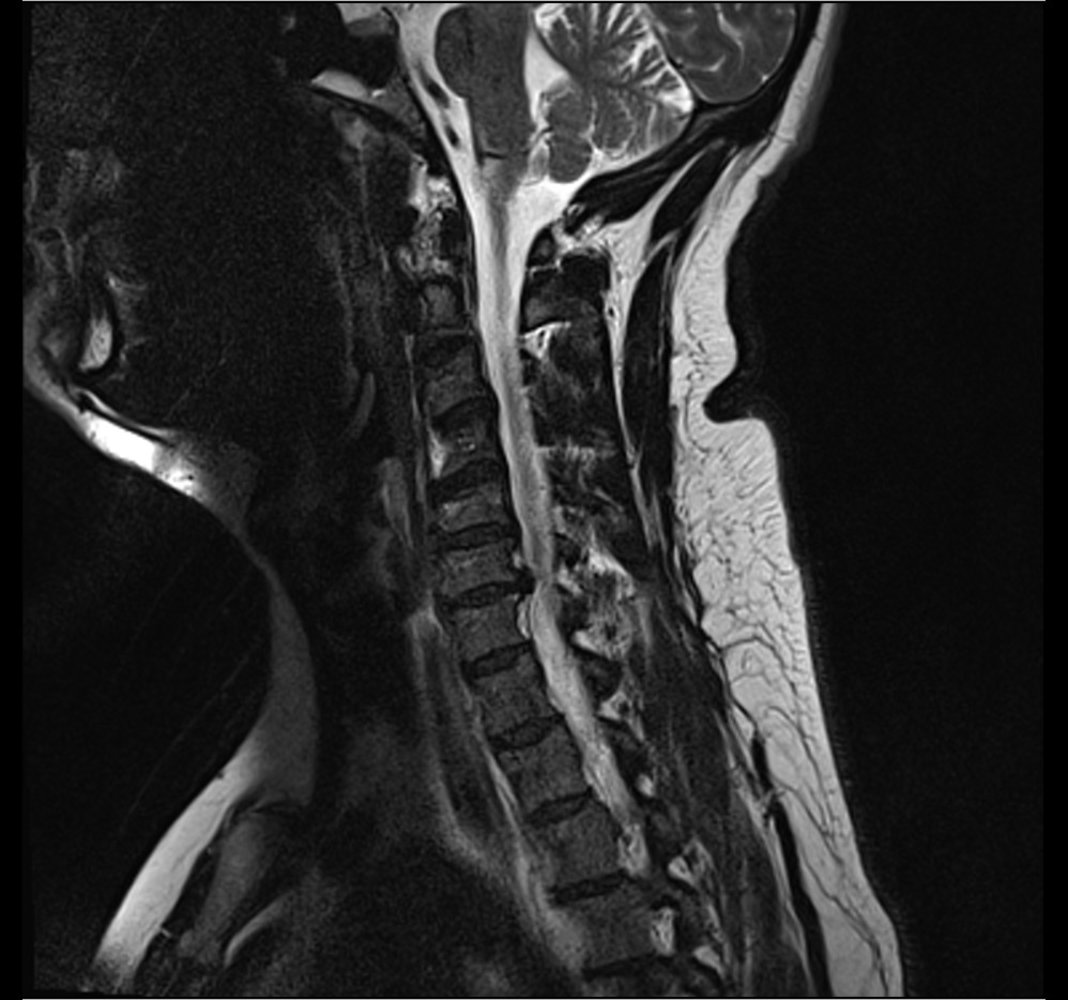
MRI cervical spine (T2-weighted; sagittal plane)
Cervical disk herniation at C6–C7 (green overlay) produces a prominent anterior extradural impression with spinal canal narrowing and cord compression.
Source: “C6-C7-disc-herniation-cevical-mri-scan” by Anthonp, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

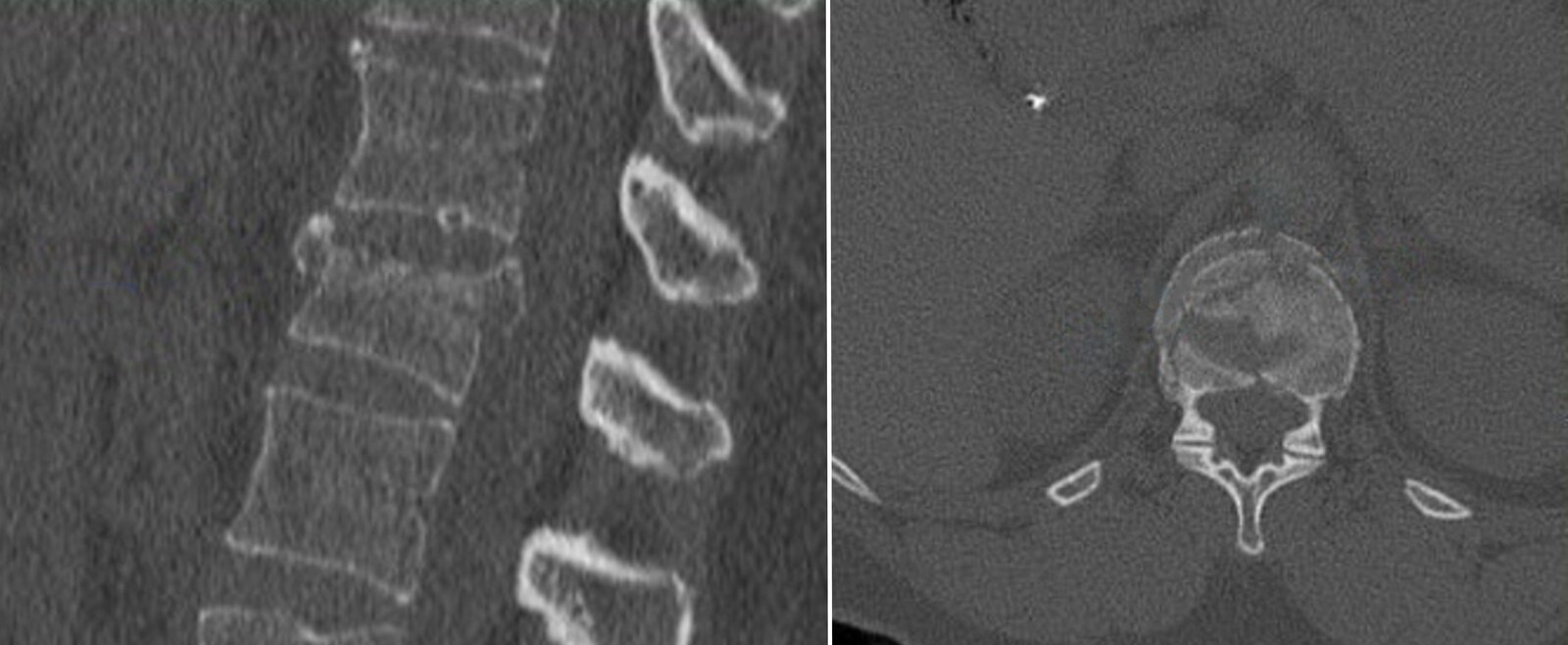
CT lumbar spine (sagittal plane)
There is a T12 burst fracture (red overlay) with retropulsion of fragments into the spinal canal and a dorsal L1 fracture with extension into the T12–L1 disc space (green overlay).
S: sacrum
Source: © IMPP
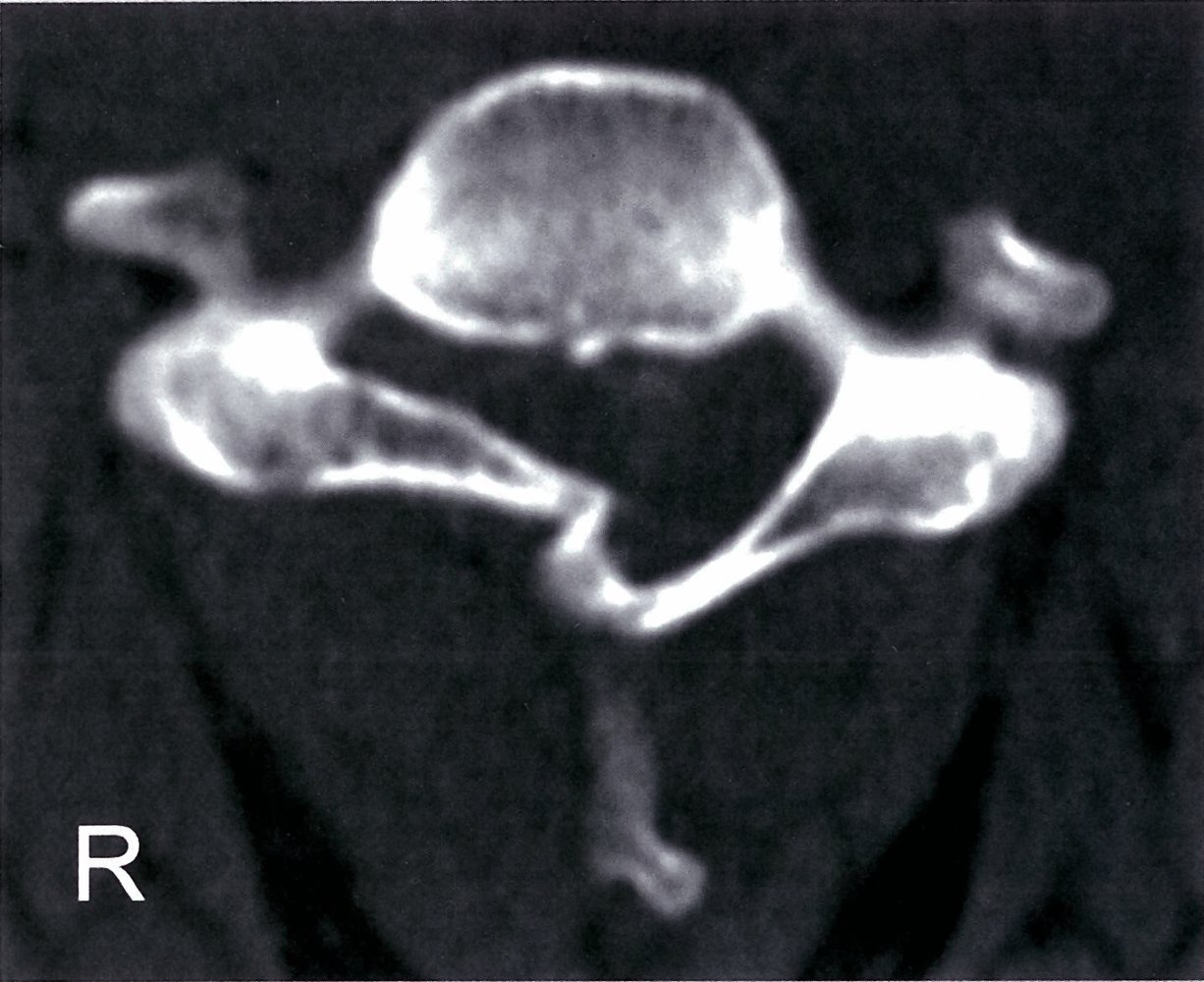
CT cervical spine (bone window; axial plane)
There is a fracture deformity of the right vertebral arch (green overlay) with depression causing narrowing of the spinal canal.
Source: © IMPP
CT thoracic spine (T12 level; left: sagittal plane; right: axial plane; bone window)
A compression fracture of the superior endplate (red overlay and lines) is accompanied by cortical disruption and retropulsion (arrow) into the spinal canal.
Burst fractures result from high-energy axial compression forces accompanied by varying degrees of flexion and/or rotation. They can be stable or unstable fractures.
Source: “Figures 1 and 2, in: A Smart Technique to Remove Ruptured Inflatable Bone Tamp From the Vertebral Body in Balloon Kyphoplasty” by Papaioannou I , Mousafeiris VK, Pantazidou G, Repantis T, Korovessis P, Cureus, licensed under CC BY 4.0. Modifications: images combined and cropped, arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

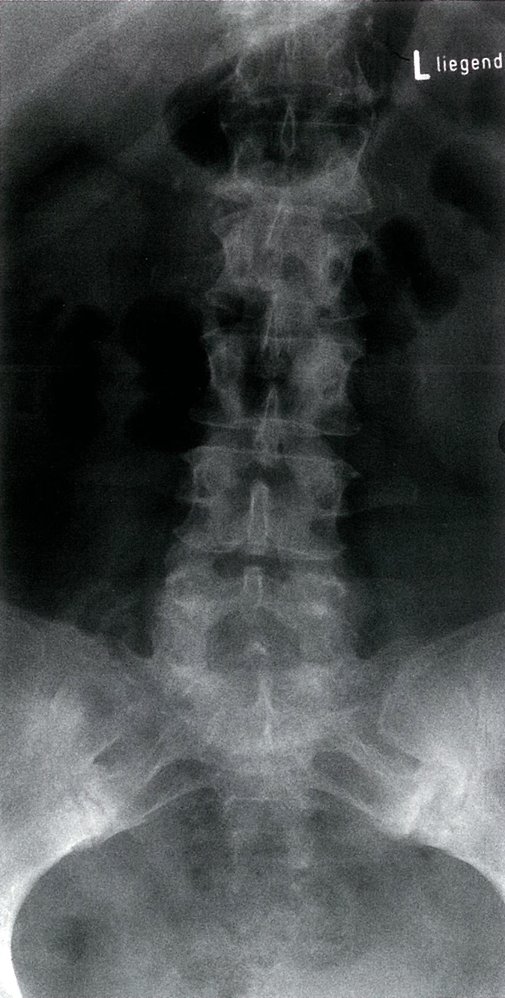
MRI lumbar spine (left: STIR image; right: T1-weighted; sagittal plane)
Compression deformities of the T8, T10, and L4 vertebrae (green overlays) are visible. The T8 and T10 fractures are hyperintense on the STIR image, indicating that they are recent. The compressed superior endplate of L4 is iso- to hypointense, indicating an old or chronic deformity. The hypointense appearance of the L2–3 intervertebral disc (green circle) on the STIR image indicates disc degeneration.
Source: © IMPP
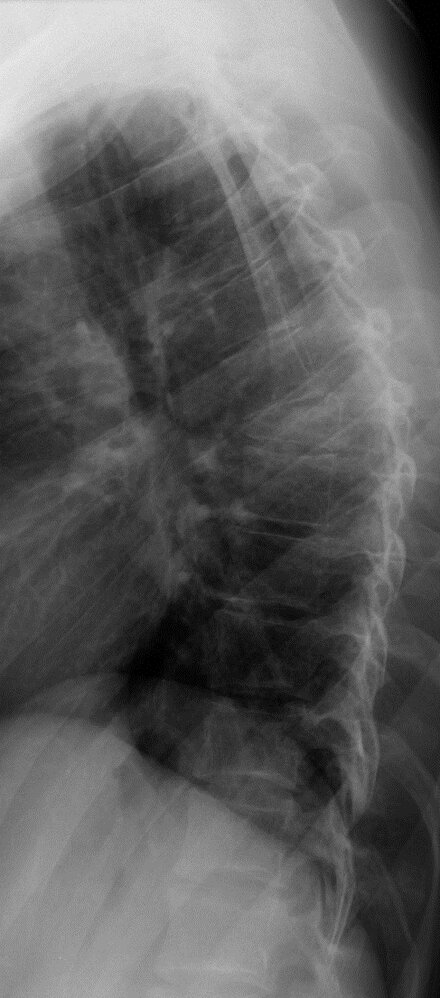
X-ray thoracic spine (lateral view) of a patient with osteoporosis
There is an insufficiency fracture of the T7 vertebral body, which is anteriorly wedged (green overlay) and accompanied by anterior subluxation (arrow) of the T6 vertebral body.
Wedge compression deformities are frequently osteoporotic, although alternatively may be pathologic (secondary to a focal bone lesion) or traumatic.
Red dashed outlines: normal vertebrae
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

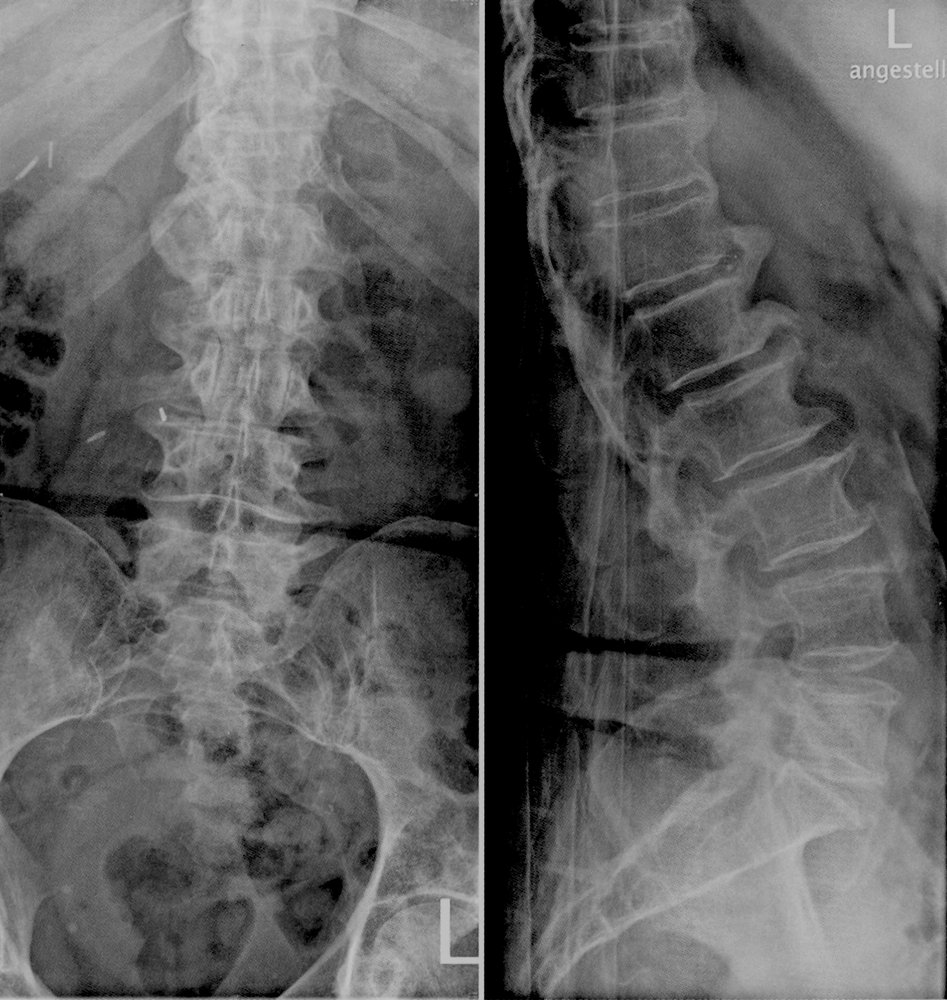
X-ray lumbar spine (lateral view)
There is a chronic compression deformity (red dimension line) of the L4 vertebral body, with displacement (red overlay) toward the spinal canal beyond the posterior vertebral lines of L3 and L5 (white dotted line). Exuberant anterior osteophyte formation is visible at L3–4 (red dotted lines).
Source: © IMPP

MRI cervical spine (T2-weighted; sagittal view)
A large, well-defined, T2-hyperintense structure in the neck, representing a fluid collection (blue overlay), is visible between the pharynx and the C1–C5 vertebrae and extends superiorly to the clivus. The C3 and C4 vertebral bodies (green overlay) demonstrate higher signal intensity than the other vertebral bodies, consistent with bone edema. The C3–4 intervertebral disc (red overlay) also demonstrates higher signal intensity than the discs at other levels. There is signal representing fluid in the epidural space at the level of C2–C4 (yellow overlay).
The differential diagnosis for a retropharyngeal fluid collection includes abscess, hematoma, and effusion. Bone marrow edema can result from, e.g., infection, osteoarthritis, and trauma. In this case, the large fluid collection near the edematous vertebrae and intervertebral disc edema raise suspicion for infection of these structures. The retropharyngeal abscess may have preceded the development of spondylodiscitis and the epidural collection, since the vertebral findings are relatively early, with no evidence of destructive changes.
Source: © IMPP

MRI cervical spine (T2-weighted; sagittal plane)
High signal intensity collections are seen in the posterior epidural space. The largest collection (blue overlay) causes anterior displacement and high-grade compression of the spinal cord from C7-T2. The appearance is consistent with epidural abscess. The differential would also include epidural hematoma.
High signal intensity consistent with osteomyelitis and discitis involves the C6 and C7 vertebral bodies (green overlay), prevertebral soft tissues (red overlay), and intervening disc space (yellow overlay).
Source: “Figure 1, in: A rare case of multiple spinal epidural abscesses and cauda equina syndrome presenting to the emergency department following acupuncture” by J. J. Chan, J. J. Oh, BMC - International Journal of Emergency Medicine, licensed under CC BY 4.0. Modifications: cropped white rim. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

MRI cervical spine (T2-weighted; sagittal plane) of a 58-year-old patient on long-term warfarin therapy presenting with acute tetraplegia
A region of heterogeneous signal lies along the posterior aspect of the spinal canal (indicated by arrows), between the dura and vertebral canal, representing a hematoma. The hematoma displaces the spinal cord anteriorly and compresses it, most prominently between the levels of C3 and C7. At the level of C7, there is an oval area of hyperintense signal within the spinal cord (arrowhead), representing myelopathic change (injury to the spinal cord).
Source: “Fig. 1, in: Anti-coagulation Drug Warfarin Contributes to Severe Adverse Outcomes in Prolonged Unsupervised Use: A Double-edged Sword” by Ordookhanian C, Kaloostian SW, Kaloostian PE, Cureus, licensed under CC BY 3.0. Modifications: Arrows have been removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Compressive spinal emergencies
The following table outlines common symptoms following compression of the spinal cord or cauda equina. Patients may also present with symptoms of incomplete spinal cord syndromes depending on the location of compression.
Spinal cord compression, conus medullaris syndrome, and cauda equina syndrome are medical emergencies that have the potential to cause permanent neurological damage. [10]
| Overview of compressive myelopathies [17] | |||
|---|---|---|---|
| Spinal cord compression | Conus medullaris syndrome | Cauda equina syndrome | |
| Etiology |
|
|
|
| Onset |
|
|
|
| Pain |
|
|
|
| Motor symptoms |
|
|
|
| Sensory symptoms |
|
|
|
| Urogenital and rectal symptoms |
|
|
|

Cauda equina syndrome typically manifests with lower motor neuron signs. Spinal cord compression and conus medullaris manifest with a combination of lower motor neuron signs (at the level of compression) and upper motor neuron signs (below the level of compression).
Management of compressive spinal emergencies
- Urgent MRI spine without contrast
- Consult neurosurgery for urgent surgical decompression.
- Document the patient's current neurological deficits and reassess frequently. [31]
- Bladder scan to evaluate postvoid residual; Insert Foley catheter for patients with urinary retention.
- Administer analgesics (preferably NSAIDs, see “Pain management”). [7][10]
- Treat the underlying cause (e.g., suspected malignant cord compression: high-dose IV dexamethasone ) [32]
- Admit the patient for frequent neurological examinations and definitive management.
Treatment of acute spinal cord compression varies based on the underlying etiology and may include decompressive surgery (e.g., for disc herniation) or IV steroids and radiation therapy (for malignant compression).
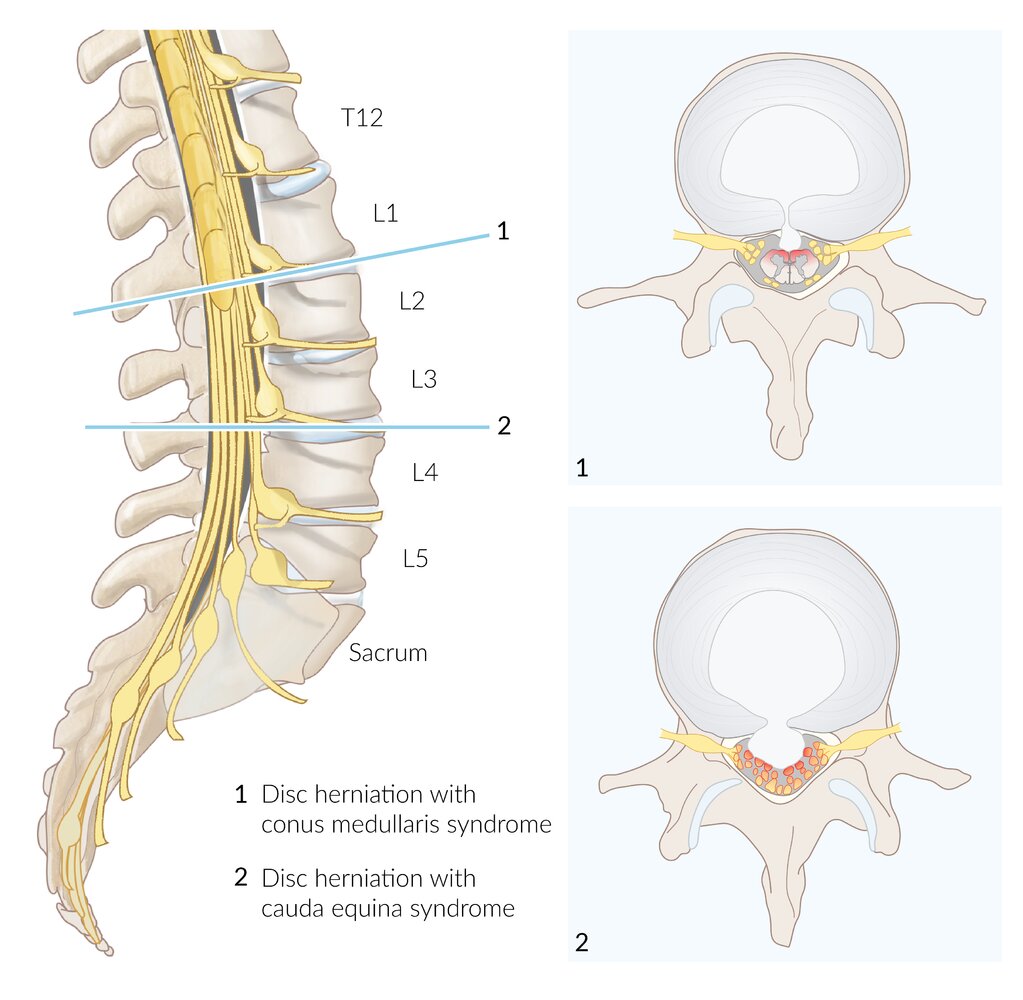
1 (conus medullaris syndrome): disc herniation at L1-L2 with pressure on the conus medullaris
2 (cauda equina syndrome): disc herniation at L3-L4 with pressure on the cauda equina
While disk herniation has been used to illustrate the process here, any pathology that compresses the conus medullaris or cauda equina can result in these syndromes.
© AMBOSS
Sensory loss restricted to the perianal, perineal, and superomedial aspects of the thighs and buttocks (S2–S5 dermatome regions).
Saddle anesthesia indicates lumbar spinal injury or disease (e.g., conus medullaris syndrome, cauda equina syndrome).
© AMBOSS
Nonurgent spinal causes
| Overview of nonurgent spinal causes of back pain [21] | |||
|---|---|---|---|
| Characteristic clinical features | Diagnostic findings | Management | |
| Back strain |
|
|
|
|
Symptomatic degenerative disc disease (without cord compression) [34][35][36] |
|
|
|
| Spinal stenosis [37][38] |
|
|
|
| Uncomplicated spinal metastases [8] |
|
|
|
|
Inflammatory back pain (e.g., ankylosing spondylitis, reactive arthritis, psoriatic arthritis) [8][41] |
|
|
|
| Spondylolisthesis [42][43] |
|
|
|
In young adults with back pain that does not improve with rest or medication and/or worsens at night, suspect inflammatory arthritis.
Patients with unilateral neurological symptoms resulting from radiculopathy typically do not require urgent spinal surgical management.

")
")
")







")



MRI lumbar spine (T2-weighted; sagittal plane)
Hypointense degenerated disks (red overlay) at L4–5 and L5–S1 are accompanied by disk space narrowing. A disk extrusion (white dashed outline) at L4–5 has migrated superiorly behind the L4 vertebral body and narrows the thecal sac (arrowhead).
Source: © IMPP

MRI lumbar spine (T1-weighted; sagittal plane)
The L4–5 disk space is narrowed. Extruded disk material (green overlay) has migrated to the level of the L5 vertebral body and is compressing the thecal sac.
Source: © IMPP

MRI lumbar spine (T2-weighted, axial plane)
Extruded disk material (green overlay) has migrated to the level of the L5 vertebral body and is compressing the thecal sac posteriorly.
V: vertebral body; SP: spinous process
Source: © IMPP

MRI lumbar spine (T2-weighted; sagittal plane)
The desiccated disk at L4–5 is hypointense and the disk space is narrowed. Extruded disk material (green overlay) has migrated to the level of the L5 vertebral body and is compressing the thecal sac.
Hatched green overlay: normal intervertebral disks
Source: © IMPP

MRI lumbar spine (T2-weighted; sagittal plane)
Advanced degenerative changes (red overlay) involve the intervertebral disks and posterior elements at multiple levels. The spinal canal (green overlay) is narrowed at L2–3 and L3–4 (indicated by arrows).
White dashed outline: spinal cord
Source: © IMPP
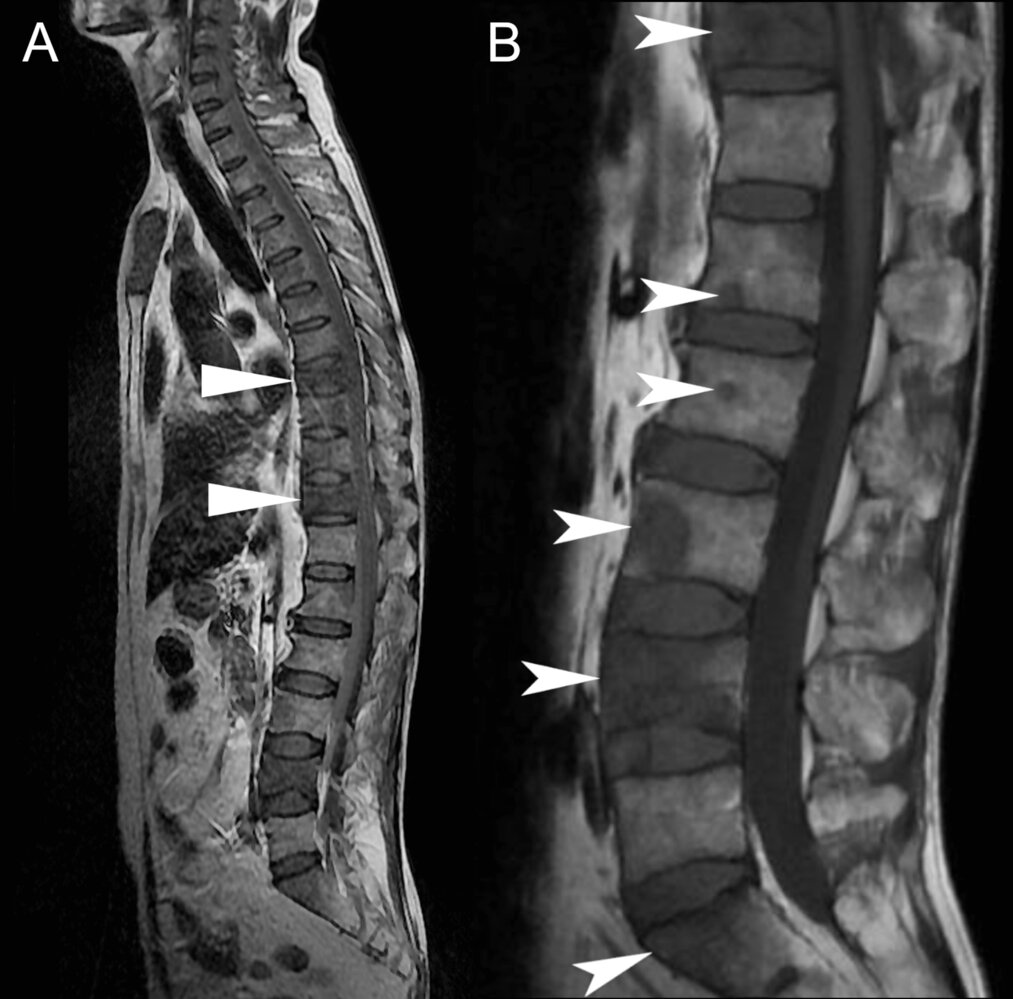
MRI spine (A: T1-weighted, scout/localizer; B: T1-weighted, sagittal view) of a 52-year-old man with low back pain.
Image A: Vertebral body height loss of T8 and T11 (triangles) with diffuse hypointense signal, representing pathological compression fractures.
Image B: Numerous hypointense lesions (arrowheads) demonstrated in the vertebral bodies of T11, L1-L4, and the sacrum.
The hypointense lesions represent osseous metastasis. In this example, the primary tumor was a lung adenocarcinoma. Bone marrow is normally bright on T1 sequences due to the presence of fat. Loss of fat signal indicates replacement of fat with other tissue. In this example, the fat is replaced with tumor cells.
Source: “Figure 1, in: Lung Cancer With Vertebral Metastases Presenting as Low Back Pain in the Chiropractic Office: A Case Report” by Chu E, Trager R J, Lee W, et al., Cureus, licensed under CC BY 4.0.
X-ray lumbar spine (AP view; supine position) of a patient with ankylosing spondylitis
Characteristic findings of sacroiliitis are visible on the sacroiliac joints, including extensive periarticular sclerosis (green overlay) and erosions (example indicated by red overlay).
Source: © IMPP

X-ray lumbar spine (lateral view)
Anterior displacement (green overlay) of L4 on L5 is visible (Meyerding grade II). In addition, there is degenerative disk disease with narrowing of the L4–L5 disk space (red overlay), as well as hypertrophic changes of the L5 vertebral body.
Source: © IMPP
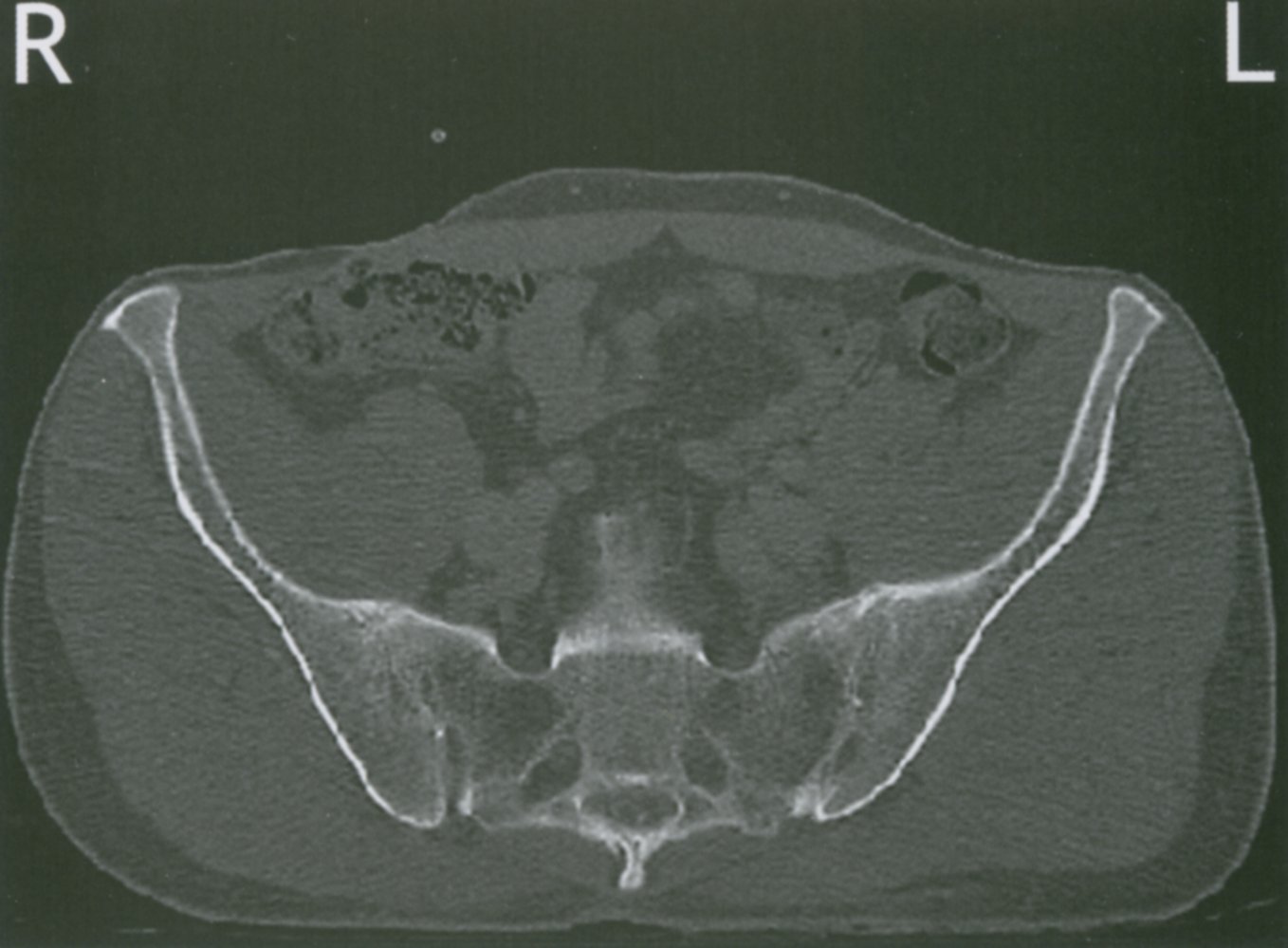
CT pelvis (axial plane; bone window)
Typical changes in ankylosing spondylitis can be seen, with multiple sites of erosion (examples indicated by green overlay) and sclerosis (examples indicated by red overlay). The courses of the sacroiliac joints (green dashed lines) are poorly visualized as a result of regions of narrowing and fusion across the joint spaces.
1: sacral foramina; 2: sacral canal
Source: © IMPP
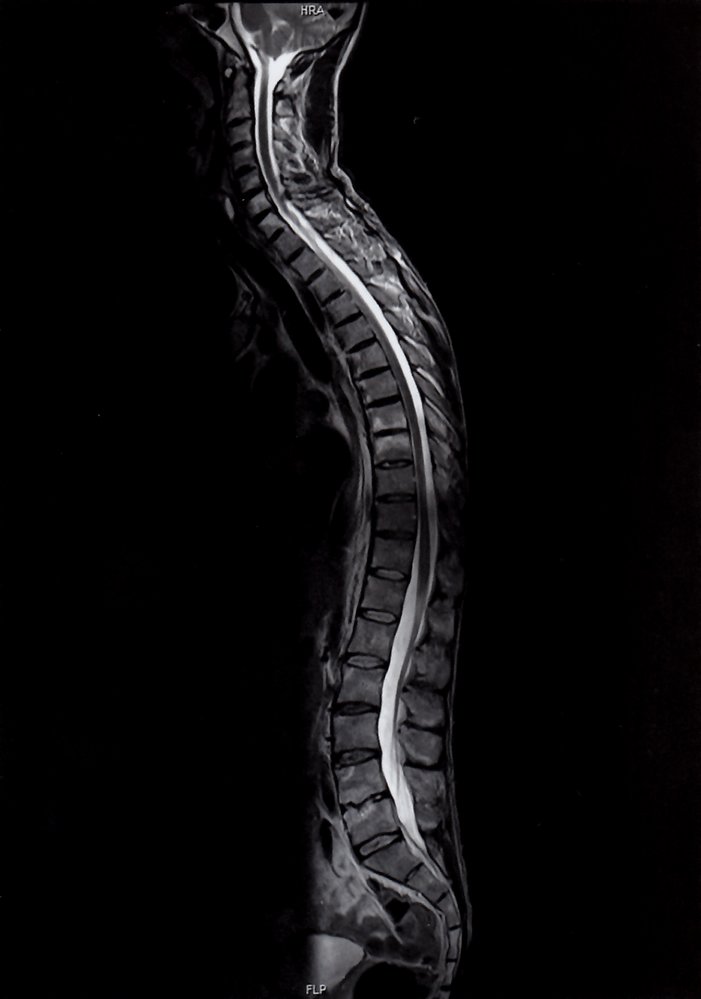
MRI spine (T2-weighted; sagittal plane)
Multiple hyperintense vertebral lesions (green overlays) correlate with sites of inflammation (spondylitis). The L4–5 disk space is narrowed and irregular (red overlay), and the anterior superior corner of L5 is fractured (red arrowhead). Syndesmophytes (examples indicated by green arrowheads) are visible at multiple levels.
Source: © IMPP
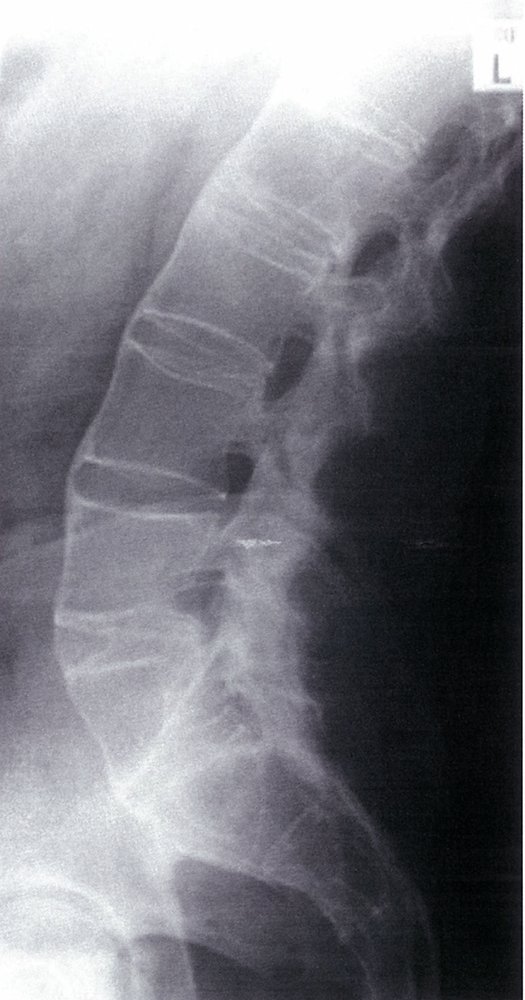
X-ray lumbar spine (lateral view)
Marginal syndesmophytes (red lines) from ossification of the annulus fibrosis bridge multiple lumbar vertebrae (known as “bamboo spine”). So-called “shiny corners” (green triangles) at the superior and inferior margins of vertebrae represent reactive sclerosis in response to inflammatory Romanus erosions. Lower lumbar facet joints are fused (green lines).
Source: © IMPP
X-ray lumbar spine (left: AP view; right: lateral view)
There are degenerative changes, with large osteophytes (examples indicated by green overlay) projecting from the anterior and lateral aspects of several vertebral endplates. Some adjacent vertebrae are fused by bridging osteophytes (examples indicated by arrows).
Source: © IMPP

X-ray lumbar spine (45° oblique view)
The normal Scottie dog sign (green overlay) has a collar (red overlay) as a result of a defect in the pars interarticularis (spondylolysis).
Source: © IMPP
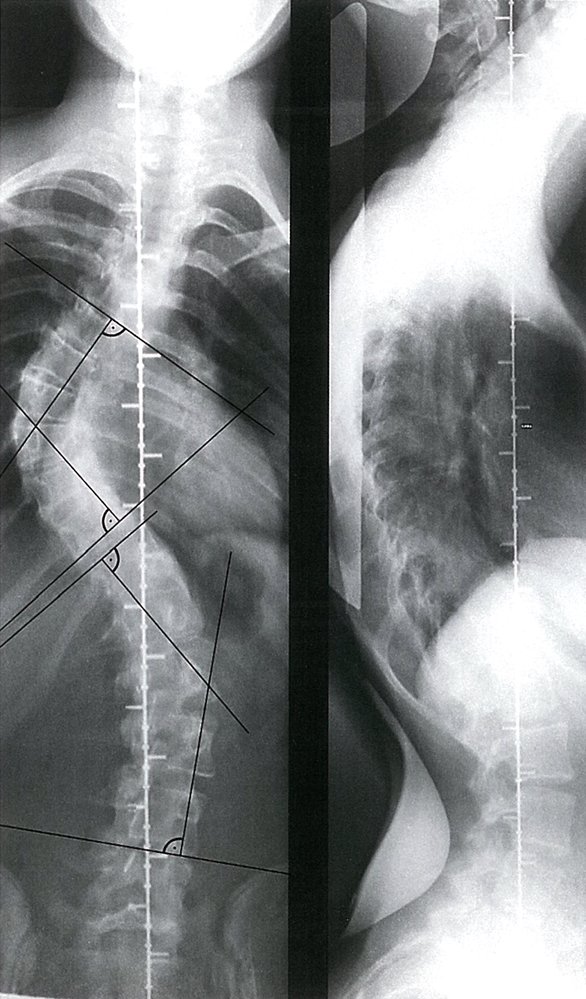
X-ray spine (left: frontal view, right: lateral view)
A severe scoliotic curvature is seen, with the Cobb angle (green overlay) of the major curve (MC) measuring 80° and the Cobb angle (red overlay) of the compensatory curve (CC) measuring 50°.
A scoliosis radiograph is generally performed PA (posteroanterior) rather than AP in order to reduce breast dose. A lateral radiograph is sometimes additionally obtained.
The Cobb angle measures the maximal angle between tangents placed along the upper endplate of the superior-end vertebra and the lower endplate of the inferior-end vertebra of the scoliotic curvature. Particularly if the tangents do not intersect, the Cobb angle is measured at the point of intersection between perpendicular lines drawn at each of the tangents. A Cobb angle in the range of 10-20° is considered to denote mild scoliosis, between 20-40° moderate scoliosis, and >40° severe scoliosis.
Source: © IMPP
Nonspinal causes (referred pain)
- Nonspinal back pain is referred pain that originates outside of the spinal cord, vertebral column, and back muscles. [7]
| Overview of nonspinal causes of back pain | |||
|---|---|---|---|
| Characteristic clinical features | Diagnostic findings | Initial management | |
| Abdominal aortic aneurysm (AAA) [45] |
|
|
|
| Aortic dissection [48][49] |
|
|
|
| Retroperitoneal hematoma [50][51][52] |
|
|
|
| Psoas abscess [56] |
|
|
|
| Pyelonephritis [60] |
|
|
|
|
Ureteric colic [61][62] |
|
|
|




")








")





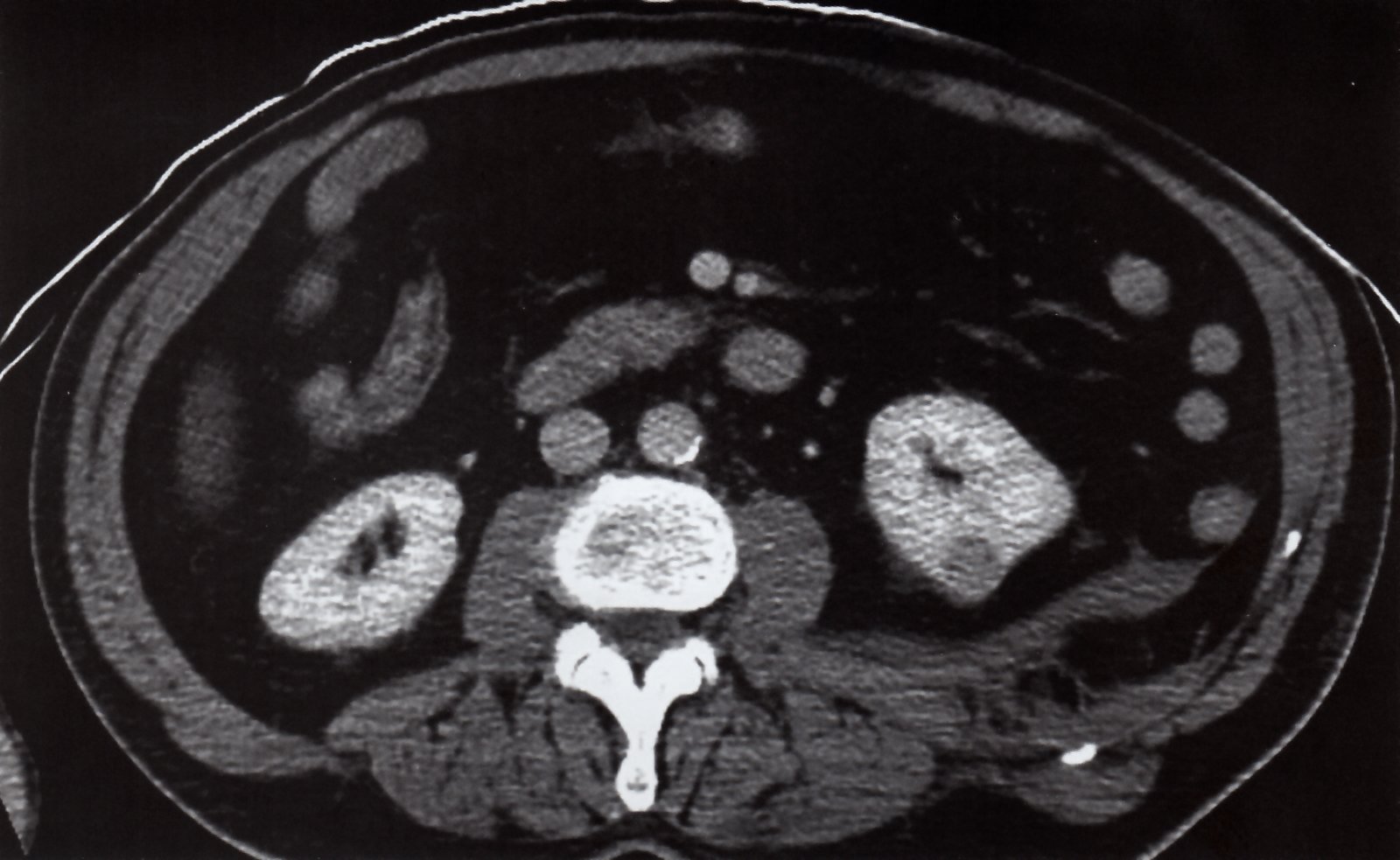
CT angiography abdominal aorta (sagittal plane) of a patient with Behcet disease
An eccentric saccular aneurysm (red overlay) of the abdominal aorta has eroded the anterior aspect of the L3 vertebral body (green overlay). The presumed physiopathological cause is repetitive mechanical pressure.
Atherosclerotic calcifications (examples indicated by arrowheads) are seen in the abdominal aorta.
Source: “Figure 2, in: Tratamento endovascular de aneurisma de aorta abdominal com erosão de vértebra lombar associada à doença de Behçet: relato de caso” by N. L. A. Rodrigues de Souza, D. E. D. Siqueira, A. A. Cantador et al., Jornal Vascular Brasileiro, licensed under CC BY 4.0. Modifications: Image cropped and enlarged. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
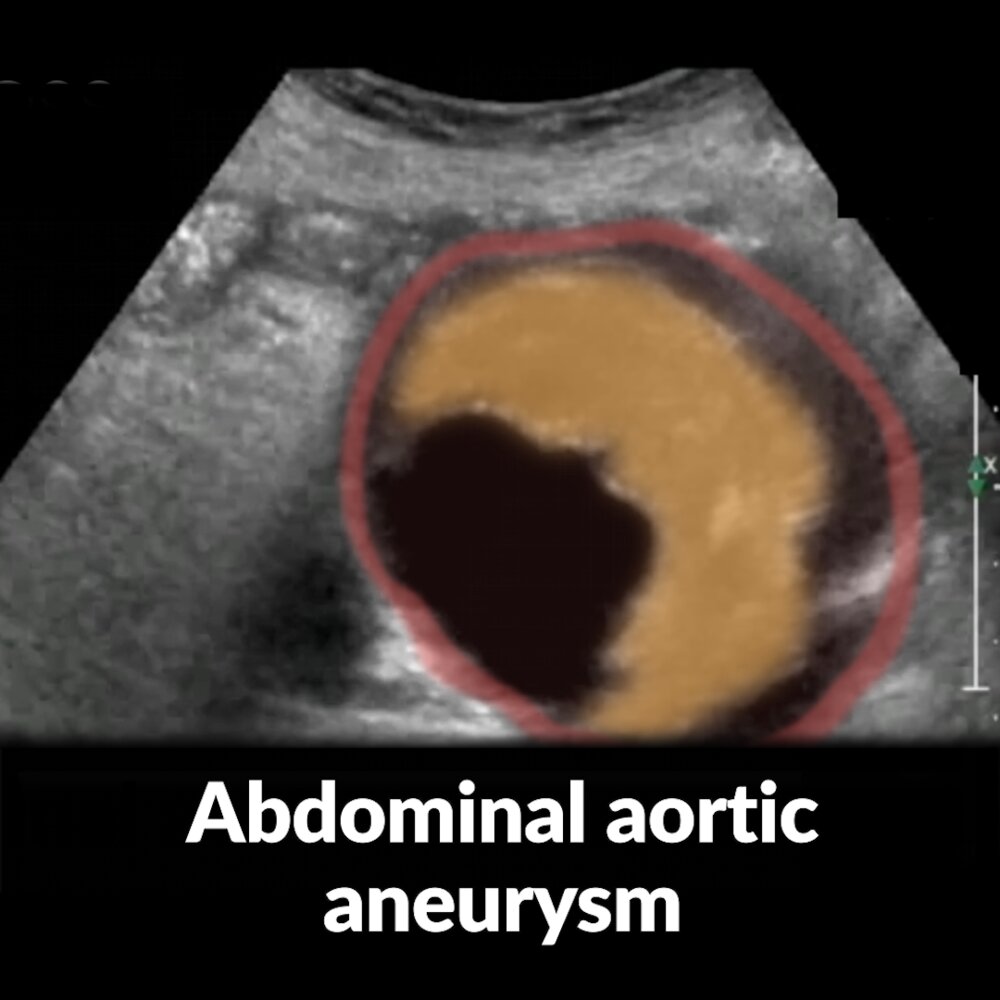
Short video of an ultrasound examination of the abdominal aorta in short axis view (a marker indicates the probe position) showing an aneurysm with a thrombus that narrows the lumen.
The abdominal aorta is seen in cross-section in the center of the image. The anechoic area in the lumen of the aorta corresponds to the expected appearance of flowing blood; the semilunar structure on the right side of the lumen is a thrombus (yellow overlay).
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
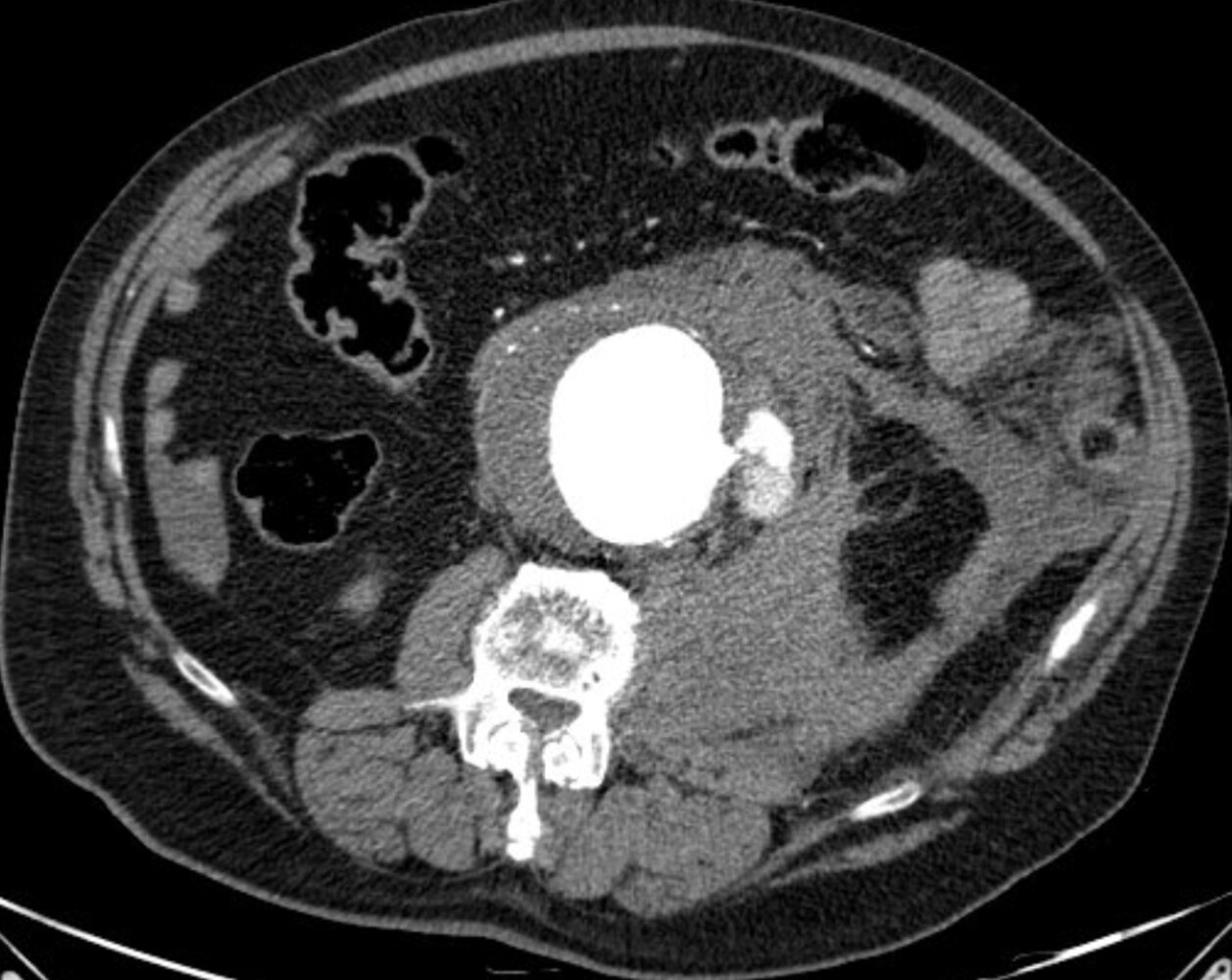
CT abdomen (with contrast; arterial phase; axial plane)
An infrarenal abdominal aortic aneurysm is measured as 8 cm in transverse diameter. Contrast extravasation (dashed outline) is seen on the left side at the site of rupture (arrowhead). A large left retroperitoneal hematoma (yellow overlay) extends inferiorly into the inguinal canal. Additional intraperitoneal fluid is seen in the pelvis and right upper quadrant (red overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.

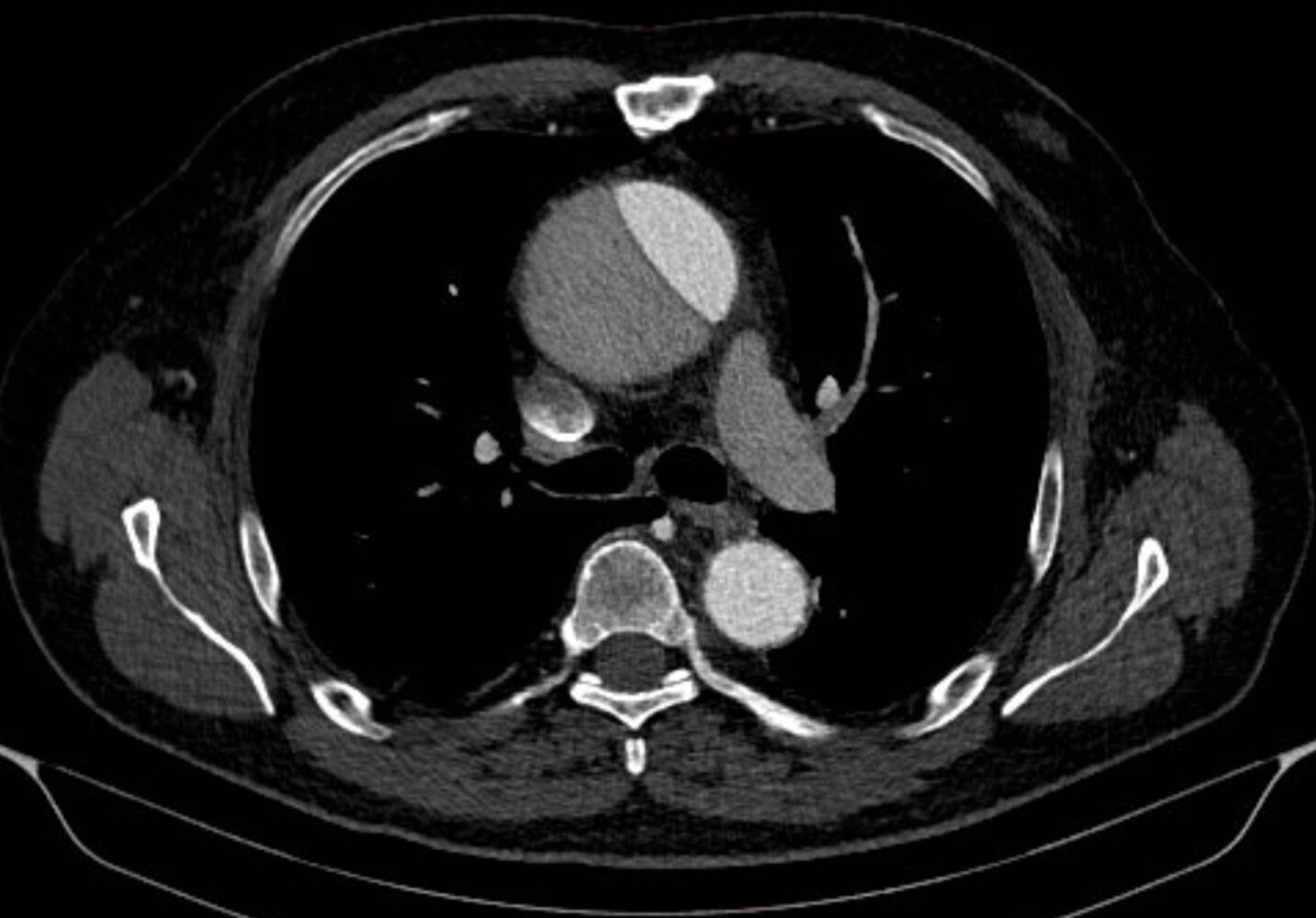
CT chest (with contrast; oblique sagittal reconstruction)
A complex Stanford type A dissection is seen, which involves the ascending aorta, arch, and descending aorta.
1: descending aorta; 2: left subclavian artery; 3: ascending aorta; red arrowheads: dissection flap
Source: “AoDiss CTRekonstr” by Dr. Lars Grenacher, Wikimedia Commons; www.grenacher.de, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT angiography (chest; ECG-gated; venous and arterial phases; axial plane) of a patient with a history of recent weakness, vertigo, and facial swelling
The ascending aorta is dilated and a Stanford type A (DeBakey type II) aortic dissection is seen. The aortic arch and descending aorta are not affected. The right and left coronary, the innominate, the left common carotid, and the subclavian arteries originate from the true lumen (green overlay; false lumen is red overlay). Facial swelling is the result of venous congestion from compression of the superior vena cava (blue overlay) by the dilated ascending aorta. Bilateral small pleural effusions are seen.
Additional findings include sternotomy wires, a prosthetic aortic valve, atherosclerotic calcifications, pancreatic calcifications, and a small hiatal hernia.
LCA: left coronary artery; RCA: right coronary artery; yellow overlay: azygos vein
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.

CT abdomen (with contrast; coronal plane) of a patient with abdominal pain after lumbar discectomy
The large collection with irregular margins in the left retroperitoneum represents hemorrhage (H; green overlay). The site of active bleeding is indicated by contrast-enhanced blood (bright green overlay) arising from the proximal left common iliac artery (CIA).
PV: portal vein; K: kidney; GB: gallbladder; A: aorta
Source: © IMPP
CT abdomen (with contrast, axial plane; soft tissue window) of a patient who fell from a height
Non-enhancing left retroperitoneal collections with fascial stranding are consistent with retroperitoneal hemorrhage (green overlay). The left kidney is anteriorly displaced.
Acute and subacute retroperitioneal hemorrhages often contain areas of high attenuation (i.e., attenuation greater than muscle). Older hemorrhages typically present as low attenuation collections.
A homogeneous, circular, and well-circumscribed lesion with a thin wall (red overlay) is visible in the posterior left kidney. The lesion measured fluid density consistent with a simple renal cyst.
Source: © IMPP
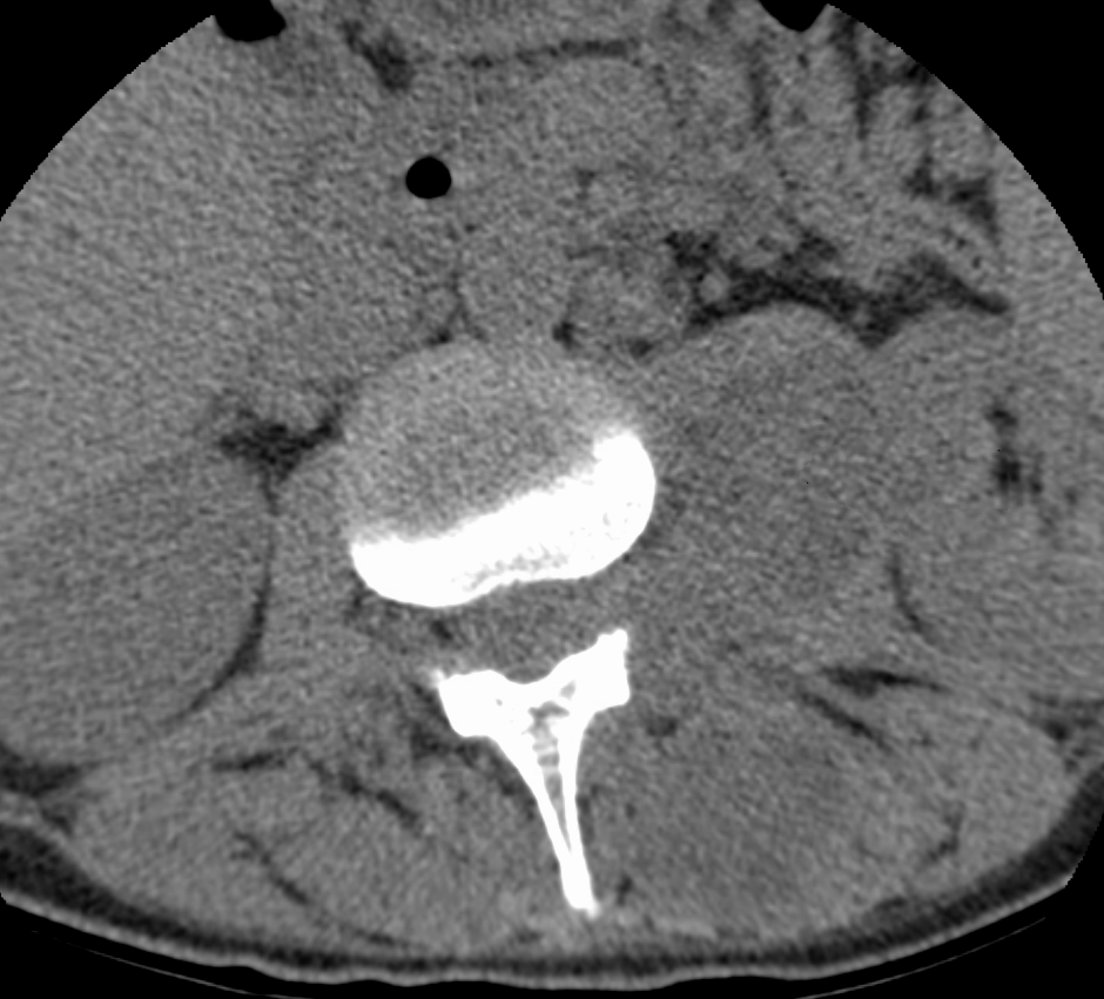
CT lumbar spine (without contrast; axial plane; soft tissue window)
The left psoas muscle is enlarged by a hypodense mass (green overlay). Involvement also extends to the level of the adjacent neural foramen and posteriorly to obliterate fat planes of the paraspinal musculature.
Findings represent a psoas abscess with paraspinal extension.
Source: “ParaspinalabscessCorMark” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. Modifications: removed arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}

CT abdomen (with oral contrast; coronal plane)
A nonobstructive hyperdense calculus (red circle) is present in the left renal pelvis. Atherosclerotic calcifications (red arrowheads) of the abdominal aorta (red overlay) are also seen. Metal streak artifacts (white arrows) between the aorta and inferior vena cava (blue overlay) are caused by an internal spinal fixator.
K and dashed lines: kidney; Li: liver, Lu: lung; PM: psoas major muscle; S: stomach with oral contrast; UB: urinary bladder
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
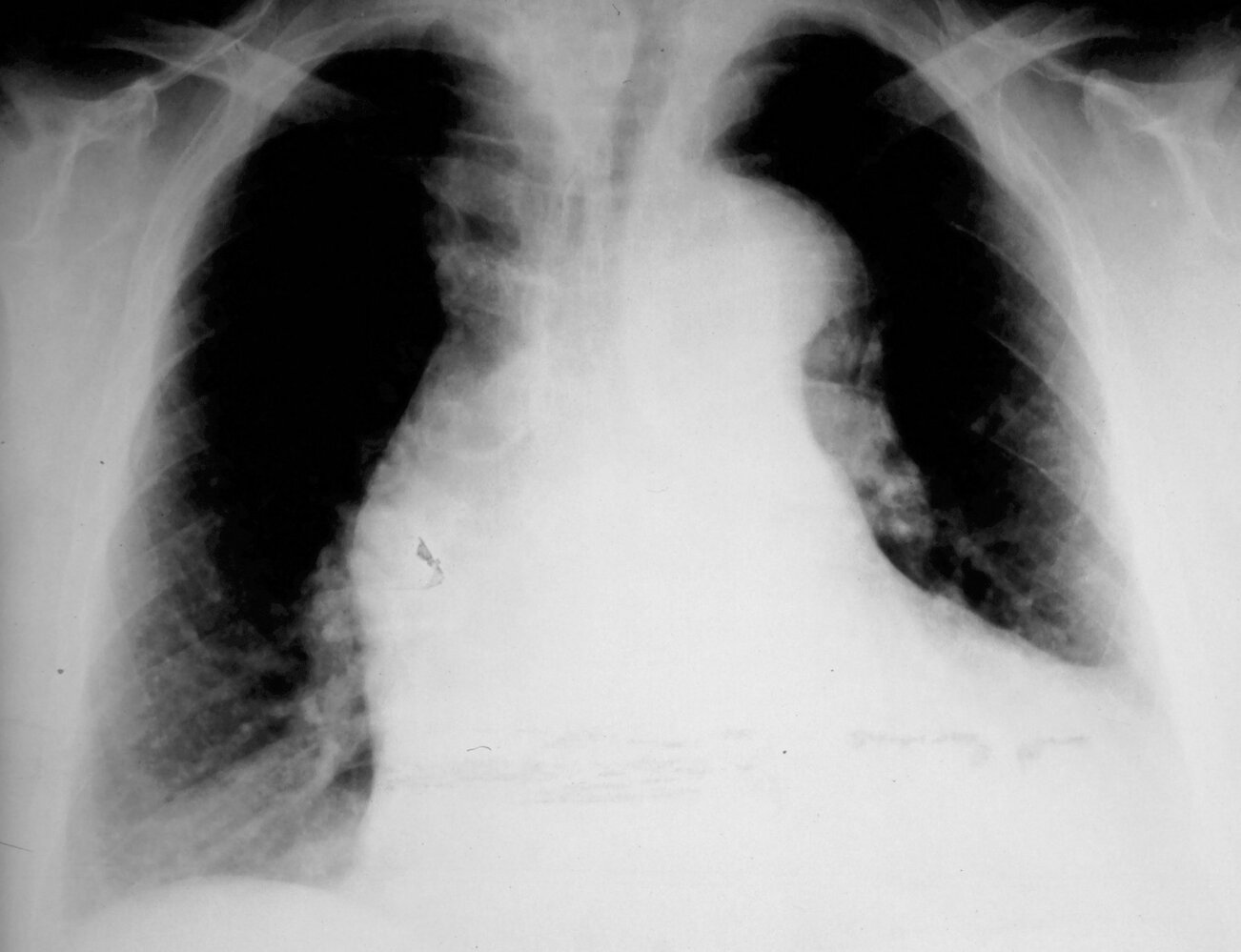
X-ray chest (PA view) of a patient with a Stanford type A dissection
Widening of the mediastinum is accompanied by a prominent aortic knob on the left side (green dashed line) and convexity in the region of the ascending aorta on the right side (red dashed line). Cardiac silhouette enlargement is also visible (black arrow line), which could indicate aortic regurgitation or pericardial effusion.
Orange dashed line: proximal descending aorta
Source: “AoDiss ChestXRay” by J. Heuser, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: delete measurements. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
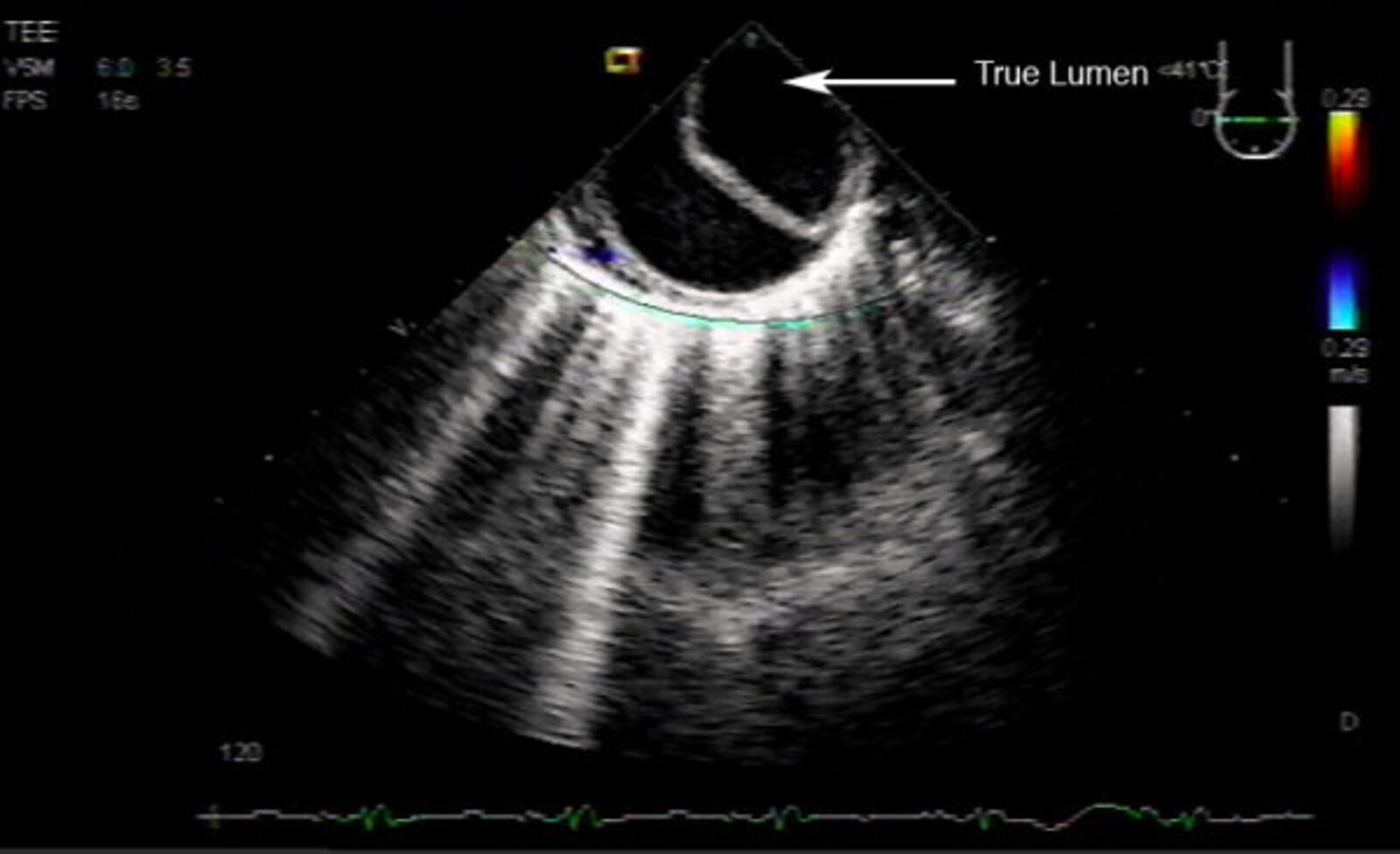
Echocardiography (transesophageal; transverse view)
The descending thoracic aorta shows a crescentic false lumen and rounded true lumen.
Source: “Figure 4 in: Transesophageal echocardiographic evaluation of an intraoperative retrograde acute aortic dissection: case report” by William C Culp Jr, Karen J Morgan-Vanderlick & Charles G Reiter, BMC Cardiovascular Ultrasound, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
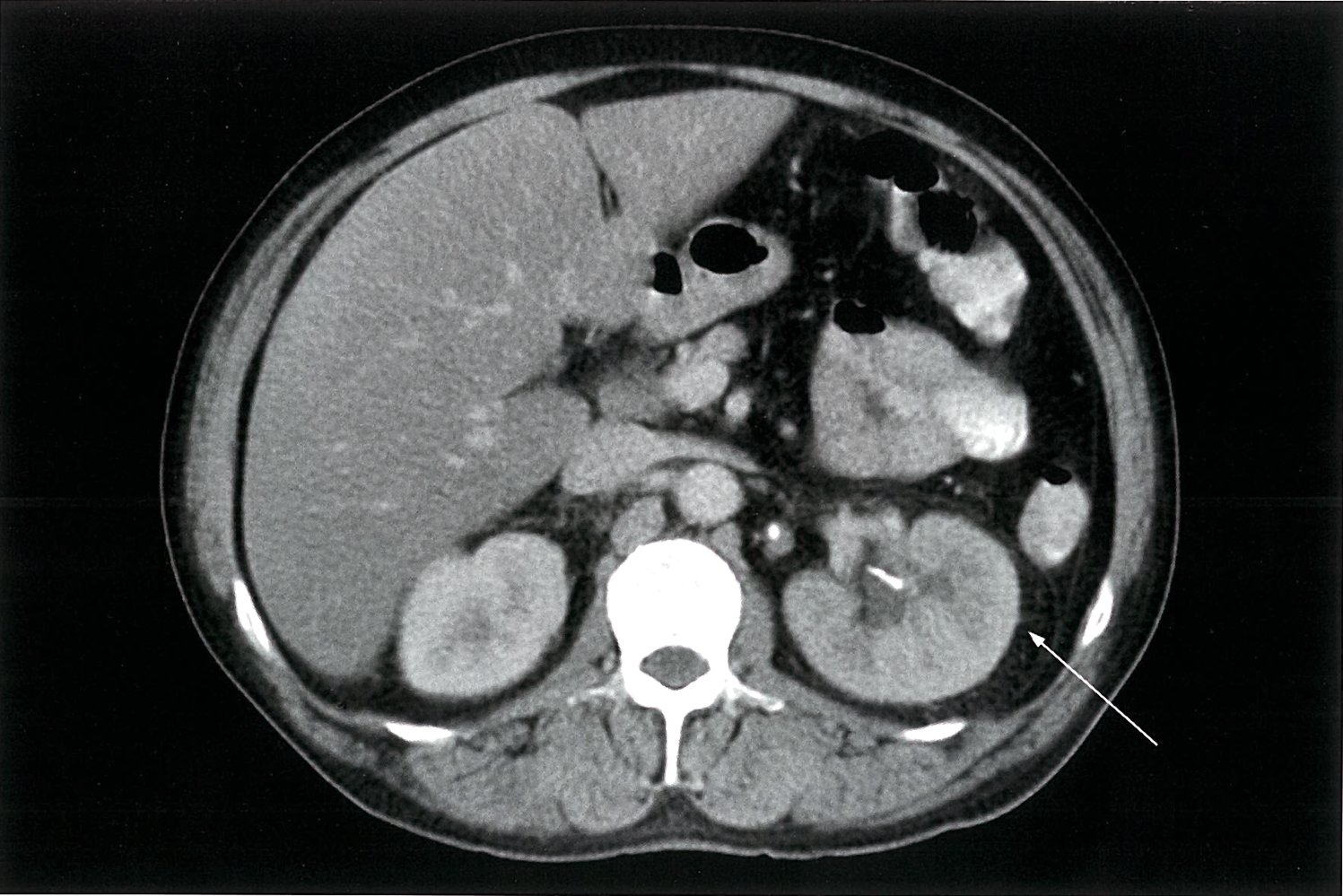
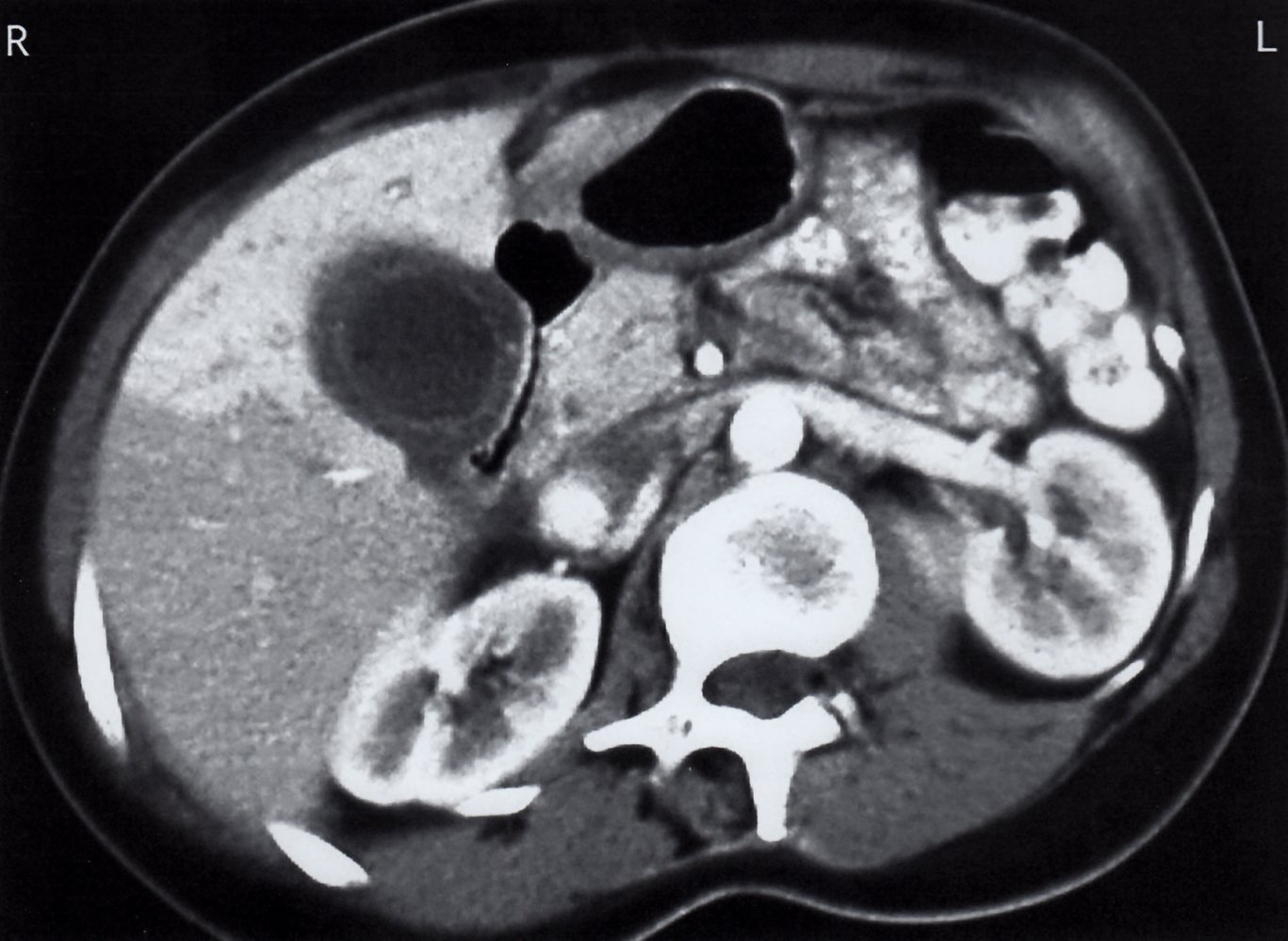
CT abdomen (with IV contrast; venous phase; axial plane) of a patient with acute pyelonephritis
The left ureter and renal pelvis are slightly dilated (red overlay) and contain hyperdense calculi (white arrowheads). The left kidney is larger than the right and the left renal parenchyma (green overlay) shows reduced contrast enhancement. There is also perinephric stranding (yellow overlay and white arrow), which is an important sign of renal inflammation or obstruction.
V: inferior vena cava; A: aorta
Source: © IMPP
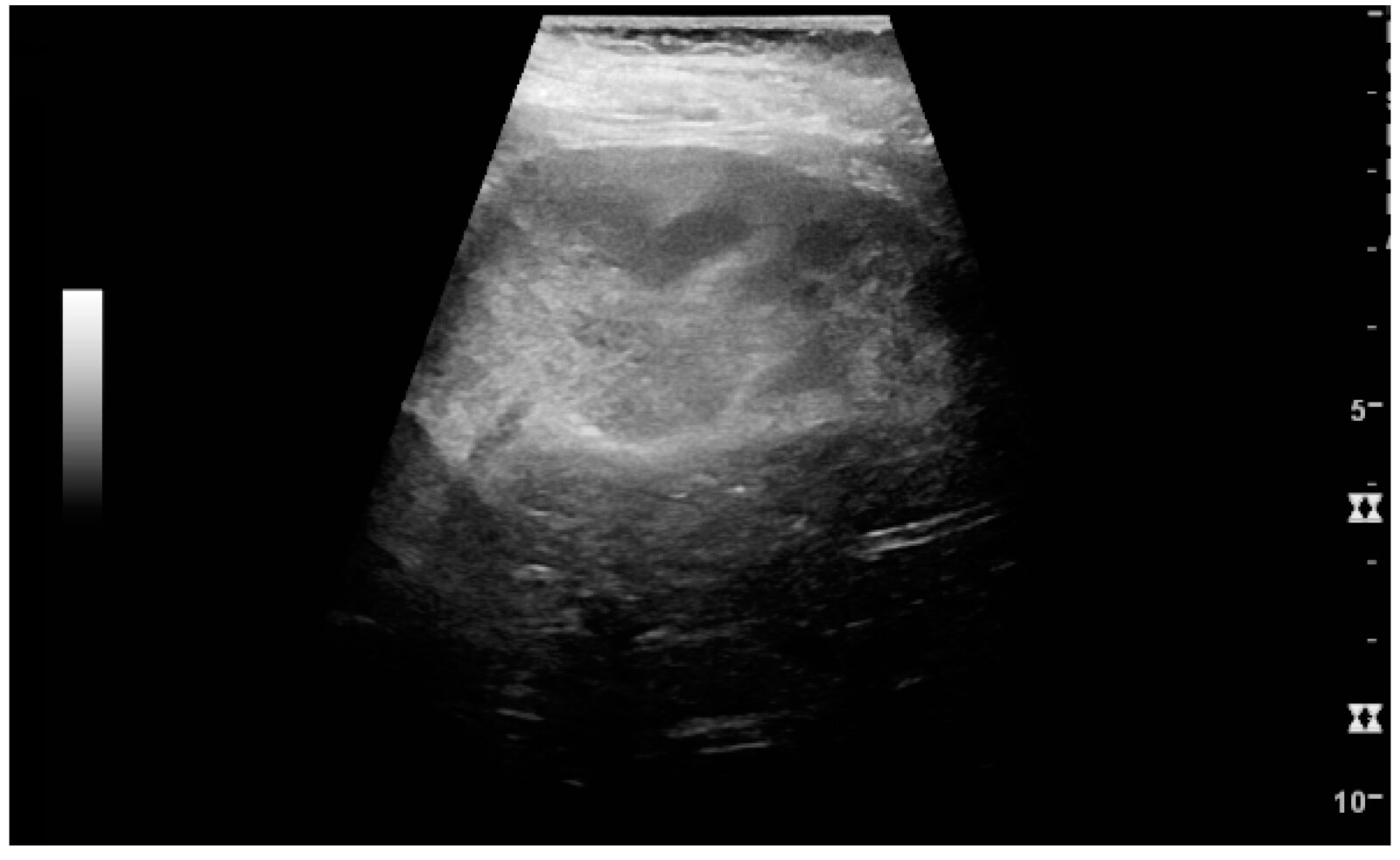
Ultrasound kidney (longitudinal plane)
The renal sinus and cortex (C) are not well differentiated from one another. Much of the central kidney is replaced by a poorly marginated area of hyperechogenicity (green overlay).
Source: “Figure 26, in: Ultrasonography of the Kidney: A Pictorial Review” by Kristoffer Lindskov Hansen, Michael Bachmann Nielsen, Caroline Ewertsen, Diagnostics, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
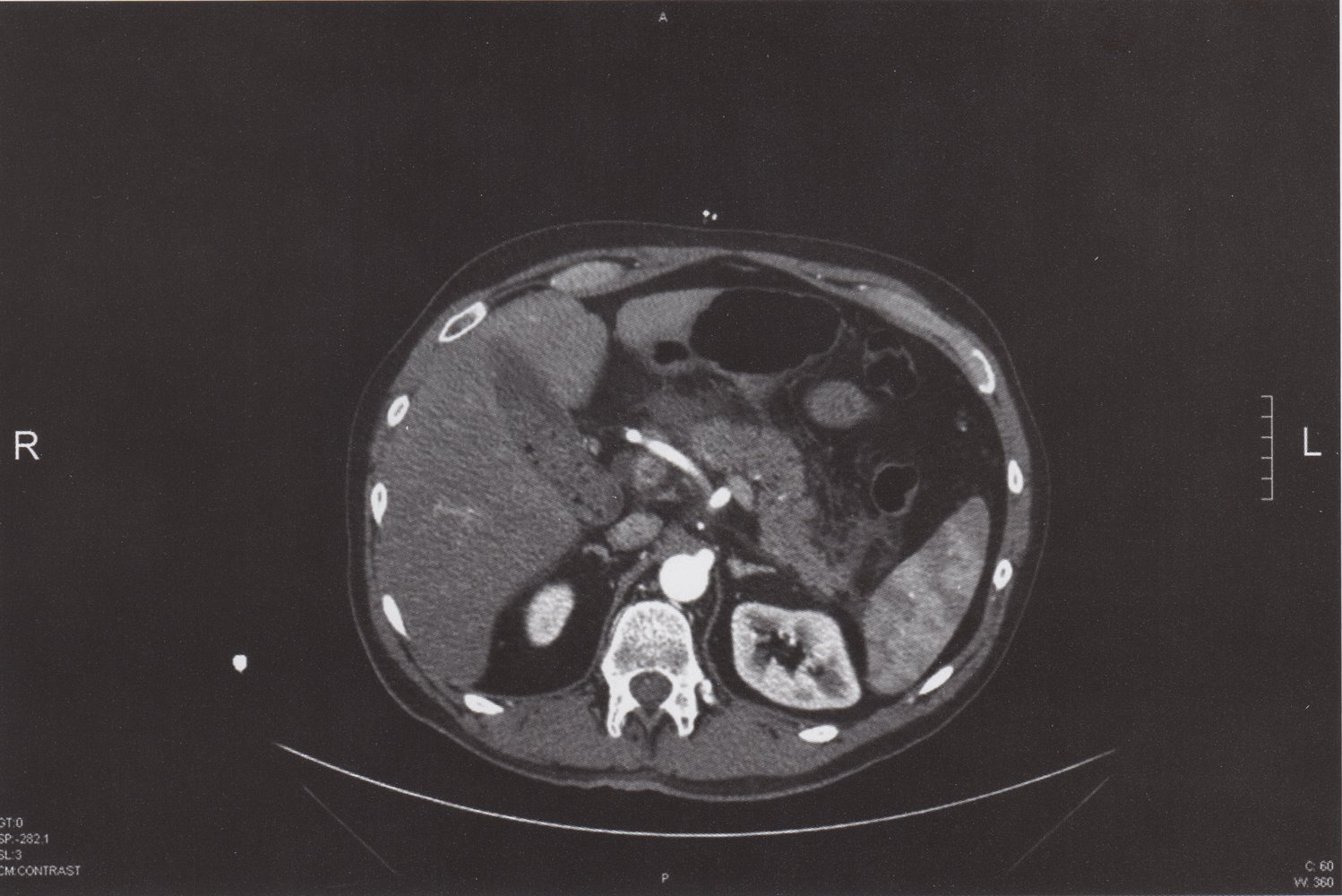
CT abdomen (with contrast; axial plane) of a patient with acute biliary pancreatitis
Fatty and fascial stranding (yellow overlay) anterior to the pancreas (P) indicates peripancreatic inflammation. The gallbladder (yellow outline) contains calculi (examples indicated by red overlay) and sludge. In addition, the common bile duct (green overlay) is slightly dilated.
The passage of a gallbladder calculus through the common bile duct can result in acute pancreatitis.
A: aorta; Vc: ascending vena cava; L: liver; Sp: spleen; Red arrow: hepatic artery; Green outline: stomach
Source: © IMPP
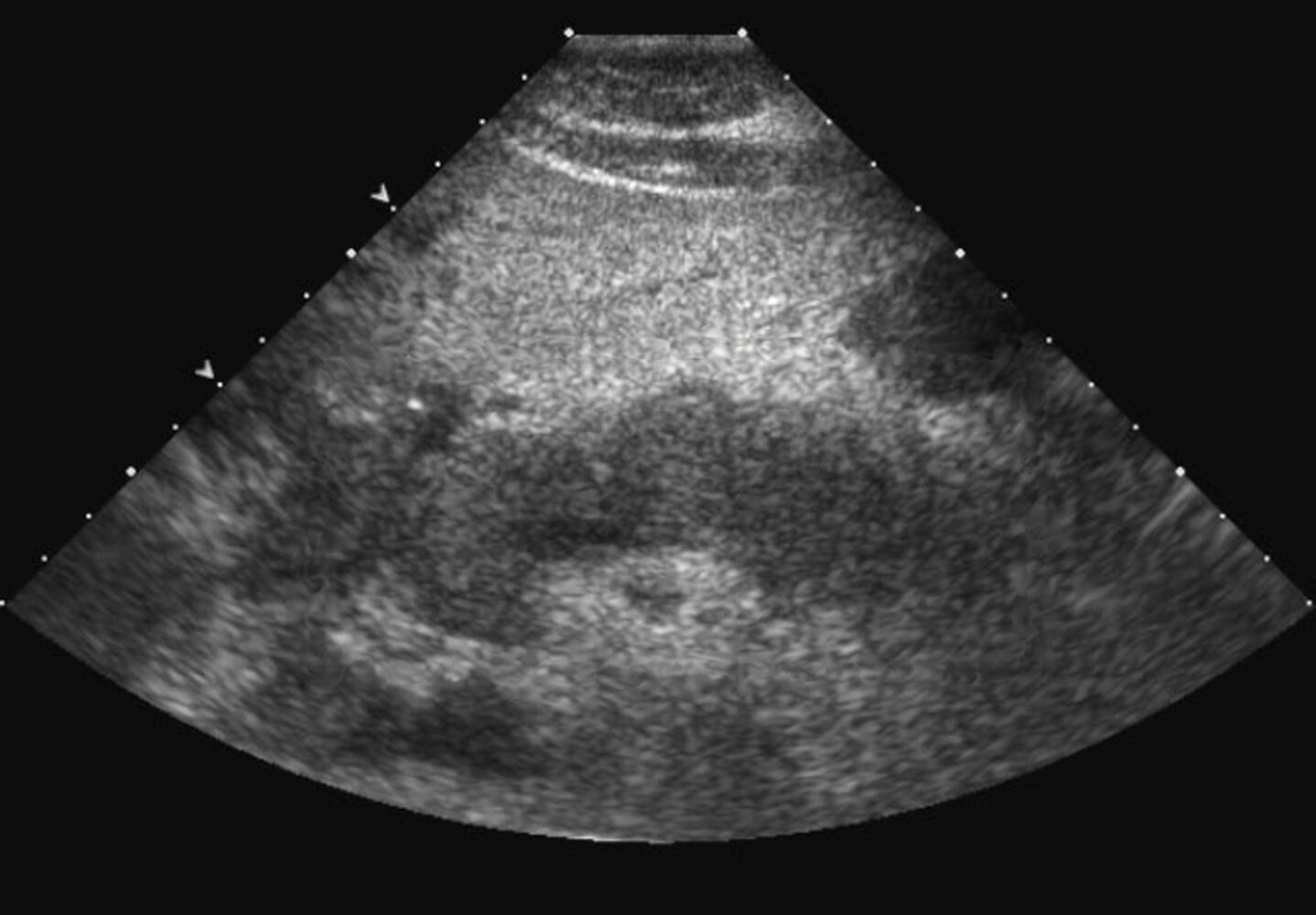
Ultrasound abdomen (transverse plane) of a patient with a history of pancreatitis
Portions of the pancreatic head (H), neck (N), and body (B) are seen. The tail is not well visualized (indicated by arrowheads). The visible pancreas is diffusely hypoechoic and lobulated.
Ultrasound is often used as a frontline tool to assess the pancreas. It is frequently used to assess for biliary dilatation and calculi in the setting of suspected pancreatitis. The pancreas may be obscured by bowel gas, particularly in the presence of an ileus, but a visible inflamed or necrotic pancreas may appear enlarged, hypoechoic, or heterogeneous. Ultrasound can be used to guide therapeutic interventions and help monitor the evolution of peripancreatic fluid collections that may accompany pancreatitis.
L: liver; S and dashed line: spine
Source: “Acute-pancreatitis-20.jpg” by Iqra Qamar, wikidoc.org, licensed under CC BY-SA 3.0. Modifications: - box and description removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

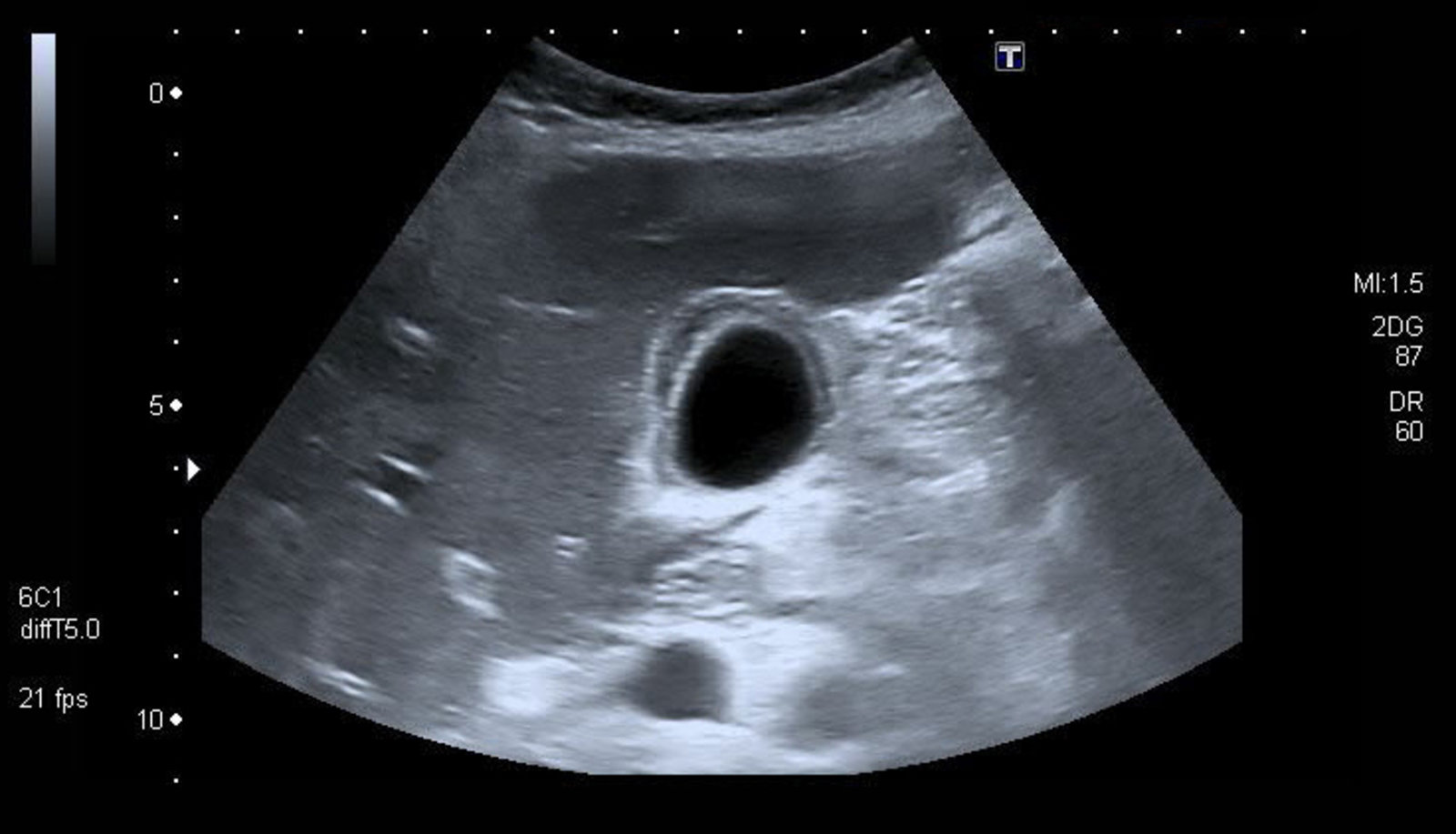
Ultrasound gallbladder
The gallbladder is dilated and its wall (green overlay) is thickened and striated (alternate hyperechoic and hypoechoic layers) as a result of edema. A calculus within dependent sludge in the neck produces posterior acoustic shadowing (red overlay) and has a highly reflective echogenic anterior surface (green hatched overlay).
Ultrasound findings in acute cholecystitis include wall thickening, dilatation, pericholecystic fluid, and a positive sonographic Murphy sign. The presence of multiple ultrasound findings increases diagnostic accuracy for cholecystitis.
L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
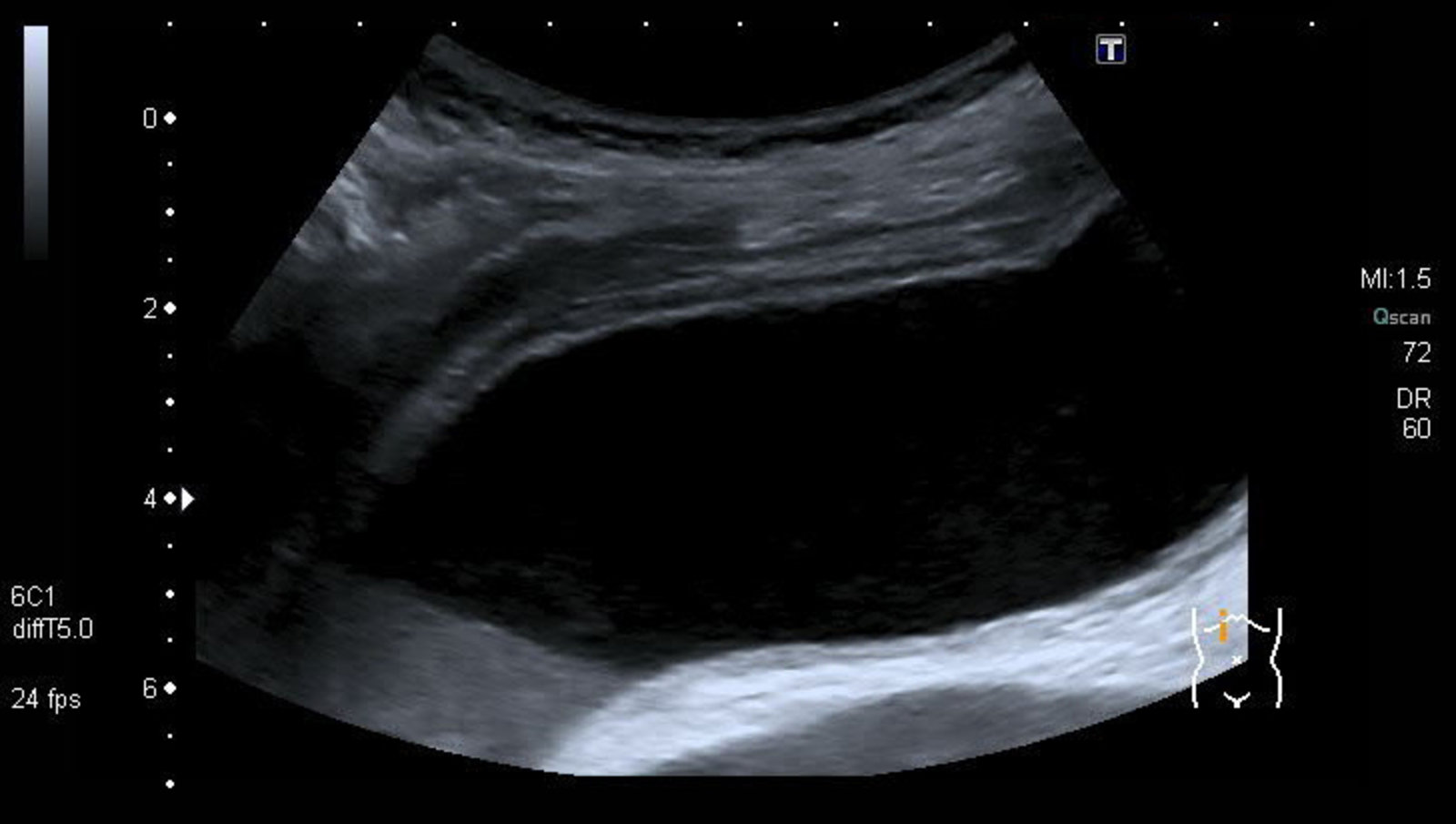
Ultrasound gallbladder (transverse plane)
The gallbladder wall is thickened. Edema has produced a striated or layered appearance with hyperechoic inner and outer layers (green overlay) and a more hypoechoic middle layer (red overlay).
These features are suggestive of acute cholecystitis.
L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Ultrasound gallbladder (transabdominal; longitudinal plane)
The gallbladder is dilated and its wall (red overlay) is thickened. The layered appearance of the wall (hypoechoic stripe between two echogenic lines) is the result of inflammation and edema. Dependent biliary sludge (green overlay) is visible.
Many diseases cause gallbladder wall thickening. Ultrasound findings in acute acalculous cholecystitis can include mural thickening, dilatation, pericholecystic fluid, hyperemia, and a positive sonographic Murphy sign. The presence of several ultrasound criteria increases diagnostic accuracy for cholecystitis. In this case, the additional feature of gallbladder distention was helpful.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
CT abdomen (with IV and oral contrast; axial plane)
The gallbladder wall is thickened (green overlay) and has a layered appearance, with hypodense edema between layers of mucosa and serosa. Hyperenhancement of the adjacent liver (red overlay) may reflect increased hepatic arterial flow in response to gallbladder inflammation.
K: kidney; S: stomach; B: small bowel
Source: © IMPP
Nonspecific back pain
Nonspecific back pain is the most common type of back pain and accounts for the majority of cases of low back pain (LBP). [7]
Definition
- Pain that cannot be attributed to an underlying disease or structural lesion after a full evaluation
Risk factors [3][64]
- Poor posture
- Sedentary lifestyle, low level of physical activity
- Heavy lifting
- Older age
- Psychological stressors (e.g., stress, anxiety, depression)
- History of lumbar surgery [6]
Clinical features [4][7][8]
- Typically LBP
- Evaluation of back pain does not reveal an underlying cause.
- No red flags for back pain [10]
- Normal neurological examination [8]
- No features suggestive of specific back pain (e.g., negative straight leg raise test)
- Usually resolves spontaneously within 6 weeks [2][65]
Imaging [3][4][6]
Imaging is not routinely recommended for the evaluation of nonspecific LBP.
-
Indications
- Progressive symptoms during conservative management
- Persistent symptoms despite 6 weeks of conservative management (if the patient is a surgical candidate)
-
Modalities
- MRI lumbar spine without IV contrast
- X-ray lumbosacral spine
- CT lumbar spine without IV contrast
Management [2][3][4][5][66][67]
- Reassure patients and provide patient education.
- Initiate conservative management alone or in combination with nonselective NSAIDs.
- For patients with risk factors for chronic back pain, consider more intensive therapy and multidisciplinary involvement.
- Reassess symptoms in 4–6 weeks or earlier if symptoms worsen during conservative management.
- Persistent symptoms despite 6 weeks of conservative management
- Consider alternative causes of back pain.
- Consider imaging for back pain if there is diagnostic uncertainty or to evaluate candidacy if surgery is being considered. [6]
- Consider referral to specialists. [2]
Patient education [2][4][5][66]
- Maintain daily activities, including work and sports; avoid bed rest. [2][10]
- Stretching, exercises, and appropriate ergonomics for LBP
- Avoid movements that aggravate pain
- Reassurance and expectation management
- Self-management of pain
Conservative management of nonspecific back pain and analgesia [2][3][4][5][66]
- Conservative management is the preferred, first-line management of nonspecific LBP.
- When analgesics are required, nonselective NSAIDs are preferred.
- In older adults, avoid skeletal muscle relaxants and use NSAIDs with caution because of the risk of adverse effects; see “Principles of pharmacotherapy for older adults.” [5]
- Glucocorticoids and back traction are not recommended for the treatment of back pain. [2][66]
Acute and subacute LBP
- Assess for risk factors for chronic back pain, which include: [2][3][7][68]
- Severe pain and functional impairment [2]
- Psychosocial and workplace factors [2][69][70]
- Previous episodes of LBP [2]
- Use of non-evidence-based management [68]
- Patients at low risk for chronic back pain: [68]
-
Initial conservative management
- Superficial heat and/or massage
- Spinal manipulation
- Acupuncture
-
Pain management
- Preferred: nonselective NSAIDs (e.g., ibuprofen , naproxen ) [2][5][71][72]
- Alternatives: Consider a short-term (< 3 weeks) nonbenzodiazepine muscle relaxant, e.g., cyclobenzaprine. [3][5]
-
Initial conservative management
- Patients with risk factors for chronic back pain: Consider more intensive initial multidisciplinary rehabilitation. [3][7]
Patients with risk factors for chronic back pain are likely to benefit from early multidisciplinary rehabilitation rather than reassurance and patient education alone. [7][68]
Chronic LBP or patients at high risk for chronic LBP
- Initial conservative management [3]
- Behavioral therapy
- Structured exercise programs
- Mobility assistive devices if needed
- Consider adjunctive therapies. [2][5][66]
-
Pain management
- Preferred: nonselective NSAIDs (e.g., ibuprofen , naproxen ) [2][5][71][72]
- Alternative: Consider short-term (< 3 months) topical capsicum. [2][66]
- Avoid routine use of:
- Adjuvant analgesics (e.g., skeletal muscle relaxants, antidepressants) [2][3][5][66][73]
- Opioids (see “Opioids for chronic noncancer pain”) [2][5][66]
Interventional therapy [2][4][74]
- Interventional therapy is rarely required for nonspecific LBP; Refer patients with refractory disabling LBP to specialists (e.g., spine surgeons) for consideration of interventional management.
- Possible benefit: radiofrequency ablation
- Limited evidence of benefit: epidural steroid injections, spinal cord stimulation, surgery (e.g., discectomy, SI joint fusion)
Regular exercise combined with patient education (e.g., on posture, safe techniques for lifting and handling, and muscle strengthening) are effective preventive measures for back pain. [75][76][77]
Traumatic back pain
Etiology
- Major trauma: e.g., motor vehicle accidents, direct high-impact injuries, fall from a height in a young, otherwise healthy individual
- Minor trauma in individuals at risk of fragility fractures: low-impact injuries, such as a minor fall or lifting heavy weights
Management of traumatic back pain
- Polytrauma patients: See “Management of trauma patients.”
- Spinal immobilization if the likelihood of unstable vertebral fracture or spinal cord compression is high
- Administer analgesics (preferably NSAIDs) after baseline neurological function and pain severity are documented (see “Pain management”).
- Obtain urgent spinal surgery or neurosurgery consult in patients with new or progressive neurological abnormalities.
- Obtain imaging. [78]
- Preferred initial imaging modality: CT thoracic and lumbar spine without IV contrast .
- Thoracolumbar injury detected on CT:
- MRI thoracic and lumbar spine without IV contrast
- Alternatively, CT myelogram to identify spinal cord compression or injury (see “Urgent spinal causes of back pain”)
- Further management depends on imaging findings
Consider imaging the entire spine, as injuries may occur at multiple levels.
Complications
- Vertebral fractures
- Intervertebral disc prolapse
- Spinal epidural hematoma
- Acute spinal cord compression (due to any of the above causes)
- Soft tissue injury

X-ray lumbar spine (lateral view)
There is marked compression of the L3 vertebral body (green overlay). Additional radiographic findings include diffuse osteopenia, multiple endplate compression deformities (examples indicated by dashed lines), and extensive atherosclerotic calcification of the abdominal aorta (A) and iliac arteries.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image. Further notes: -mirrored
External Resources
- 2023 WHO Guideline For Nonsurgical Management of Chronic Primary Low Back Pain in Adults in Primary and Community Care Settings
- 2022 New England Journal of Medicine: Nonspecific Low Back Pain
- 2021 ACR Appropriateness Criteria for Low Back Pain
- 2020 North American Spine Society Clinical Guideline: Diagnosis and Treatment of Low Back Pain
- 2020 American College of Physicians and American Academy of Family Physicians Clinical Guideline: Nonpharmacologic and Pharmacologic Management of Acute Pain From Non–Low Back, Musculoskeletal Injuries in Adults url::
- 2017 American College of Physicians Clinical Practice Guideline: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain
- 2017 New England Journal of Medicine: Acute Spinal cord Compression
- 2018 ACR Appropriateness Criteria for Suspected Spine Trauma
- 2018 American Academy of Family Physicians Article on Mechanical Low Back Pain
- 2015 Annals of Emergency Medicine: Managing Nontraumatic Acute Back Pain
- 2016 Clinical Orthopaedics and Related Research: American Spinal Injury Association(ASIA) Impairment Scale
- 2007 Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society: Diagnosis and Treatment of Low Back
References
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Edlow JA. "Managing Nontraumatic Acute Back Pain". Ann Emerg Med. 66(2). :148-153. (2015)
- "VA/DoD Clinical Practice Guideline for the Diagnosis and Treatment of Low Back Pain". https://www.healthquality.va.gov/guidelines/Pain/lbp/VADoDLBPCPGFinal508.pdf
- Chou R, Qaseem A, Snow V, et al. "Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society". Ann Intern Med. 147(7). :478. (2007)
- Chou R. "Low Back Pain". Ann Intern Med. 174(8). :ITC113-ITC128. (2021)
- "North American Spine Society: Diagnosis and Treatment of Low Back Pain (updated 1/27/2021)". https://www.spine.org/Portals/0/assets/downloads/ResearchClinicalCare/Guidelines/LowBackPain.pdf. [2020-01-01]
- Rosc-Bereza K, Arkuszewski M, Ciach-Wysocka E, Boczarska-Jedynak M. "Spinal Epidural Abscess: Common Symptoms of an Emergency Condition". Neuroradiol J. 26(4). :464-468. (2013)
- Lener S et al. "Management of spinal infection: A review of the literature". Acta Neurochir (Wien). 160(3). :487-496. (2018)
- Kollef M, Isakow W. "The Washington Manual of Critical Care". Lippincott Williams & Wilkins. (2011). ISBN: 9781451110227
- Ropper AE, Ropper AH. "Acute Spinal Cord Compression". N Engl J Med. 376(14). :1358-1369. (2017)
- Cadotte DW, Fehlings MG. "Principles of Neurological Surgery: Chapter 27 Spinal Cord Injury". Elsevier Health Sciences. (2012). ISBN: 9781437707014
- Choi S, Nah S, Jang HD, Moon JE, Han S. "Association between chronic low back pain and degree of stress: a nationwide cross-sectional study". Scientific Reports. 11(1). (2021)
- Chiarotto A, Koes BW. "Nonspecific Low Back Pain". N Engl J Med. 386(18). :1732-1740. (2022)
- "ACR Appropriateness Criteria Low Back Pain". https://acsearch.acr.org/docs/69483/Narrative/. [2021-03-01]
- Will JS, Bury DC, Miller JA. "Mechanical Low Back Pain". Am Fam Physician. 98(7). :421-428. (2018)
- Steinmetz A. "Back pain treatment: a new perspective". Ther Adv Musculoskelet Dis. 14. :1759720X2211002. (2022)
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians". Ann Intern Med. 166(7). :514. (2017)
- Ageing and Health, Guidelines Review Committee, Maternal, Newborn, Child & Adolescent Health & Ageing (MCA). "WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings". World Health Organization. (2023). ISBN: 9789240081789
- Vlaeyen JWS, Maher CG, Wiech K, et al. "Low back pain". Nat Rev Dis Primers. 4(1). (2018)
- Stevans JM, Delitto A, Khoja SS, et al. "Risk Factors Associated With Transition From Acute to Chronic Low Back Pain in US Patients Seeking Primary Care". JAMA Netw Open. 4(2). :e2037371. (2021)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Ikemoto T, Miki K, Matsubara T, Wakao N. "Psychological Treatment Strategy for Chronic Low Back Pain". Spine Surg Relat Res. 3(3). :199-206. (2019)
- Peck J, Urits I, Peoples S, et al. "A Comprehensive Review of Over the Counter Treatment for Chronic Low Back Pain". Pain Ther. 10(1). :69-80. (2020)
- Chou R, Deyo R, Friedly J, et al. "Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline". Ann Intern Med. 166(7). :480. (2017)
- Abril L, Zamora C, Cordero M, Williams AR, Friedman BW. "The Relative Efficacy of Seven Skeletal Muscle Relaxants: An Analysis of Data From Randomized Studies". J Emerg Med. 62(4). :455-461. (2022)
- "CDC Radiation and Pregnancy". https://web.archive.org/web/20240207173419/https://www.cdc.gov/nceh/radiation/emergencies/prenatalphysician.htm. [2020-06-05]
- Steffens D, Maher CG, Pereira LSM, et al. "Prevention of Low Back Pain". JAMA Intern Med. 176(2). :199. (2016)
- Daltroy LH, Iversen MD, Larson MG, et al. "A Controlled Trial of an Educational Program to Prevent Low Back Injuries". N Engl J Med. 337(5). :322-328. (1997)
- Warming S, Ebbeh⊘j NE, Wiese N, et al. "Little effect of transfer technique instruction and physical fitness training in reducing low back pain among nurses: a cluster randomised intervention study". Ergonomics. 51(10). :1530-1548. (2008)
- Chaikof EL, Dalman RL, Eskandari MK, et al. "The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm". Journal of Vascular Surgery. 67(1). :2-77.e2. (2018)
- Yildizgoren MT, Ogut H, Kayali A, Turhanoglu AD. "Abdominal Aortic Aneurysm as a Long Time Cause of Low Back Pain and Vertebral Scalloping". Pain Med. (2016)
- "Pulsatile Abdominal Mass, Suspected Abdominal Aortic Aneurysm". https://acsearch.acr.org/docs/69414/Narrative/. [2016-01-01]
- Hiratzka LF, Bakris GL, Beckman JA, et al. "2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease". Circulation. 121(13). :e266-369. (2010)
- Nienaber CA, Clough RE, Sakalihasan N, et al. "Aortic dissection". Nat Rev Dis Primers. 2(1). (2016)
- Daliakopoulos S. "Spontaneous retroperitoneal hematoma: A rare devastating clinical entity of a pleiada of less common origins". J Surg Tech Case Rep. 3(1). :8. (2011)
- Daliakopoulos SI, Bairaktaris A, Papadimitriou D, Pappas P. "Gigantic retroperitoneal hematoma as a complication of anticoagulation therapy with heparin in therapeutic doses: a case report". J Med Case Reports. 2(1). (2008)
- Frank JJ, Kamalakannan D, Kodenchery M, Savoy-Moore Rt, Rosman H. "Retroperitoneal Hematoma in Patients Undergoing Cardiac Catheterization". J Interv Cardiol. 23(6). :569-574. (2010)
- "ACR Appropriateness Criteria: Suspected Retroperitoneal Bleed". https://acsearch.acr.org/docs/3158181/Narrative/. [2021-03-01]
- Daly KP, Ho CP, Persson DL, Gay SB. "Traumatic Retroperitoneal Injuries: Review of Multidetector CT Findings". RadioGraphics. 28(6). :1571-1590. (2008)
- Bennett M. "The LANSS Pain Scale: the Leeds assessment of neuropathic symptoms and signs". Pain. 92(1). :147-157. (2001)
- Shields D, Robinson P, Crowley TP. "Iliopsoas abscess – A review and update on the literature". Int J Surg. 10(9). :466-469. (2012)
- Tomich EB, Della-Giustina D. "Bilateral psoas abscess in the emergency department". The western journal of emergency medicine. 10(4). :288-91. (2009)
- Mackenzie AR, Laing RB, Smith CC, Kaar GF, Smith FW. "Spinal epidural abscess: the importance of early diagnosis and treatment". J Neurol Neurosurg Psychiatry. 65(2). :209-12. (1998)
- Muttarak M, Peh WCG. "CT of Unusual Iliopsoas Compartment Lesions". RadioGraphics. 20(suppl_1). :S53-S66. (2000)
- Johnson JR, Russo TA. "Acute Pyelonephritis in Adults". N Engl J Med. 378(1). :48-59. (2018)
- Worcester EM, Coe FL. "Nephrolithiasis". Prim Care. 35(2). :369-391. (2008)
- Moore CL, Carpenter CR, Heilbrun ME, et al. "Imaging in Suspected Renal Colic: Systematic Review of the Literature and Multispecialty Consensus". Journal of the American College of Radiology. (2019)
- Bredemeyer M. "ACR Appropriateness Criteria for Acute Onset of Flank Pain with Suspicion of Stone Disease.". Am Fam Physician. 94(7). :575-576. (2016)
- Premkumar A, Godfrey W, Gottschalk MB, Boden SD. "Red Flags for Low Back Pain Are Not Always Really Red". J Bone Joint Surg. 100(5). :368-374. (2018)
- Ferreira ML, de Luca K, Haile LM, et al. "Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021". Lancet Rheumatol. 5(6). :e316-e329. (2023)
- Urits I, Burshtein A, Sharma M, et al. "Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment". Curr Pain Headache Rep. 23(3). (2019)
- Rao D, Scuderi G, Scuderi C, Grewal R, Sandhu SJ. "The Use of Imaging in Management of Patients with Low Back Pain". J Clin Imaging Sci. 8. :30. (2018)
- Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. "Low back pain". Lancet. 398(10294). :78-92. (2021)
- Qaseem A, McLean RM, O’Gurek D, et al. "Nonpharmacologic and Pharmacologic Management of Acute Pain From Non–Low Back, Musculoskeletal Injuries in Adults: A Clinical Guideline From the American College of Physicians and American Academy of Family Physicians". Ann Intern Med. 173(9). :739-748. (2020)
- Benzakour T, Igoumenou V, Mavrogenis AF, Benzakour A. "Current concepts for lumbar disc herniation". Int Orthop. 43(4). :841-851. (2018)
- Berry JA, Elia C, Saini HS, Miulli DE. "A Review of Lumbar Radiculopathy, Diagnosis, and Treatment". Cureus. 11(10). :e5934. (2019)
- Manfrè L, Van Goethem J. "The Disc and Degenerative Disc Disease". Springer Nature. (2020). ISBN: 9783030037154
- "North American Spine Society: Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis". https://www.spine.org/Portals/0/Assets/Downloads/ResearchClinicalCare/Guidelines/LumbarStenosis.pdf. [2011-01-01]
- Suri P, Rainville J, Kalichman L, Katz JN. "Does This Older Adult With Lower Extremity Pain Have the Clinical Syndrome of Lumbar Spinal Stenosis?". JAMA. 304(23). :2628. (2010)
- Georgy BA. "Metastatic spinal lesions: state-of-the-art treatment options and future trends". AJNR Am J Neuroradiol. 29(9). :1605-11. (2008)
- D’Oronzo S, Coleman R, Brown J, Silvestris F. "Metastatic bone disease: Pathogenesis and therapeutic options". Journal of Bone Oncology. 15. :100205. (2019)
- Weisman MH. "Inflammatory Back Pain". Rheum Dis Clin North Am. 38(3). :501-512. (2012)
- Randall RM, Silverstein M, Goodwin R. "Review of Pediatric Spondylolysis and Spondylolisthesis". Sports Med Arthrosc. 24(4). :184-187. (2016)
- Matz PG, Meagher RJ, Lamer T, et al. "Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis". The Spine Journal. 16(3). :439-448. (2016)
- Syrmou E, Tsitsopoulos PP, Marinopoulos D, et al. "Spondylolysis: a review and reappraisal". Hippokratia. 14(1). :17-21. (2010)
- "Contributor Disclosures - Acute back pain. All of the relevant financial relationships listed for the following individuals have been mitigated: Eva-Maria Elfers (medical editor, previously owned Healthy Gut, now known as intestx GmbH). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"
- Froese BB. "Lumbar Spondylolysis and Spondylolisthesis". WebMD. http://emedicine.medscape.com/article/310235. [2016-02-18]
- Gitelman A, Hishmeh S, Morelli BN, et al. "Cauda equina syndrome: a comprehensive review". Am J Orthop. 37(11). :556-62. (2008)
- Kendler DL, Bauer DC, Davison KS, et al. "Vertebral Fractures: Clinical Importance and Management". Am J Med. 129(2). :221.e1-221.e10. (2016)
- Raby N, Berman L, De Lacey G, Morley S. "Accident and Emergency Radiology". Saunders Limited. (2013). ISBN: 9780702042324
- Berbari EF, Kanj SS, et al. "2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults". Clin Infect Dis. 61(6). :e26-e46. (2015)
- Figueroa J, DeVine JG. "Spontaneous spinal epidural hematoma: literature review". J Spine Surg. 3(1). :58-63. (2017)
- Moriarty HK, O Cearbhaill R, Moriarty PD, et al. "MR imaging of spinal haematoma: a pictorial review". Br J Radiol. 92(1095). :20180532. (2019)
- Hutchins TA, Peckham M, Shah LM, et al. "ACR Appropriateness Criteria® Low Back Pain: 2021 Update". Journal of the American College of Radiology. 18(11). :S361-S379. (2021)
- Bhandutia AK, Winek NC, Tomycz ND, Altman DT. "Traumatic Conus Medullaris Syndrome". JBJS Case Connector. 6(2). :e38. (2016)
- Brouwers E, van de Meent H, Curt A, et al. "Definitions of traumatic conus medullaris and cauda equina syndrome: a systematic literature review". Spinal Cord. 55(10). :886-890. (2017)
- Roberts TT, Leonard GR, Cepela DJ. "Classifications In Brief: American Spinal Injury Association (ASIA) Impairment Scale". Clin Orthop Relat Res. 475(5). :1499-1504. (2017)
- Kumar A, Weber MH, Gokaslan Z, et al. "Metastatic Spinal Cord Compression and Steroid Treatment". Clin Spine Surg. 30(4). :156-163. (2017)
- Chou R. "Diagnostic Imaging for Low Back Pain: Advice for High-Value Health Care From the American College of Physicians". Ann Intern Med. 154(3). :181. (2011)