CME information and disclosures
To see contributor disclosures related to this article, click on this reference: [1]
Physicians can earn CME/MOC credit by using this article to address a clinical question and completing a brief evaluation about how they applied the information in their practice.
AMBOSS designates this internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see “Tips and links” at the bottom of this article.
Summary
Endometrial hyperplasia is an abnormal proliferation of the endometrium caused by increased estrogen stimulation. It manifests with abnormal uterine bleeding (AUB) or postmenopausal bleeding (PMB) and is classified as endometrial hyperplasia without atypia, which is benign; and endometrial hyperplasia with atypia (endometrial intraepithelial neoplasia; EIN), which is premalignant. Endometrial hyperplasia is a histopathologic diagnosis based on endometrial sampling and histopathology. Endometrial hyperplasia without atypia is treated with progestin therapy (i.e., levonorgestrel IUD or oral progestins). Total hysterectomy is preferred for EIN because of the high risk of concurrent endometrial cancer or progression to endometrial cancer. Progestin therapy with close surveillance may be considered for patients who desire future fertility.
Endometrial polyps are localized overgrowths of endometrial tissue and mainly affect postmenopausal individuals. Though usually asymptomatic, endometrial polyps can cause abnormal vaginal bleeding and, in premenopausal individuals, infertility. Diagnosis is typically made with transvaginal ultrasound (TVUS) and/or hysteroscopy. Treatment involves watchful waiting in asymptomatic premenopausal patients and surgical removal in symptomatic premenopausal patients, all postmenopausal patients, and patients with risk factors for malignant endometrial polyps.
Endometrial hyperplasia
- Endometrial hyperplasia is an abnormal thickening of the uterine lining caused by the proliferation of endometrium due to estrogen stimulation and insufficient progestin stimulation.
- Risk factors for endometrial hyperplasia are the same as risk factors for type I endometrial cancer. [2]
Clinical features
Abnormal vaginal bleeding is the defining symptom of endometrial hyperplasia. See:
- Clinical features of AUB (e.g., intermenstrual bleeding)
- Postmenopausal bleeding (PMB)
Diagnosis [2][3]
- The diagnostic workup for suspected endometrial hyperplasia follows the same approach as diagnostics for endometrial cancer.
- Endometrial hyperplasia is confirmed on histopathology findings of endometrial sampling; see “Indications for endometrial sampling.”
Endometrial hyperplasia is a histopathologic diagnosis. Endometrial sampling should be performed in all patients (postmenopausal or of childbearing age) with abnormal vaginal bleeding and risk factors for endometrial cancer to evaluate for EIN or endometrial cancer. [4][5][6]
Postmenopausal individuals [5]
-
Patients with PMB
- Endometrial thickness > 4 mm on TVUS suggests endometrial hyperplasia or endometrial cancer. [3][5][7][8]
- Diagnosis is confirmed on endometrial sampling and histopathology.
- See “Diagnostic workup for PMB” for a detailed approach.
-
Incidentally detected endometrial thickness > 4 mm (asymptomatic individuals)
- Routine evaluation is not required.
- Tailor further management based on risk factors for endometrial cancer.

Reproductive-aged individuals
- Endometrial thickness alone is an unreliable indicator of an endometrial pathology.
- Diagnosis is confirmed on endometrial sampling performed as part of the diagnostic workup for AUB.
Histopathology findings
| Classification of endometrial hyperplasia based on histology (WHO 2014) [9] | ||
|---|---|---|
| Endometrial hyperplasia without atypia (benign endometrial hyperplasia) | Endometrial hyperplasia with atypia (endometrial intraepithelial neoplasia; EIN) | |
| Histology |
|
|
| Risk of carcinoma |
|
|
Endometrial intraepithelial neoplasia (EIN) is a precursor for endometrial cancer. Endometrial intraepithelial carcinoma (EIC) is a distinct entity and is a precursor for papillary serous uterine cancer. [2]
")


Differential diagnoses
- Endometrial cancer [5]
- Endometrial atrophy [5]
- Other causes of AUB
- Other causes of PMB
Management [2][10]
- The choice of treatment depends on the presence of atypia and if future fertility is desired.
- In all patients, reversible causes of excess estrogen should be identified and treated.
Endometrial hyperplasia without atypia [13][14][15]
-
Progestin therapy
- Preferred management for all patients [13]
- Options
- Levonorgestrel IUD (off-label) [16]
- Continuous oral progestins, e.g., medroxyprogesterone acetate (off-label) [13][15]
- Further management: Repeat endometrial sampling to assess treatment response after 3–6 months of treatment. [13]
-
Surveillance with repeat endometrial sampling
- Indications
- Patients with contraindications to progestins
- Patient preference
- Spontaneous regression is seen in ∼ 75% of patients. [13][15]
- Advise patients to promptly follow up with their treating physician if they experience abnormal vaginal bleeding during conservative management.
- Indications
Endometrial hyperplasia with atypia (EIN) [2][10][17]
Refer patients to gynecology or gynecologic oncology for evaluation and management.
-
Total hysterectomy with or without bilateral salpingo-oophorectomy [2][10]
- Definitive management for EIN
- Indications
- All postmenopausal patients
- Premenopausal patients not desiring future pregnancy
-
Progestin therapy with surveillance [2][10][17]
- Concurrent endometrial cancer must first be ruled out, preferably with hysteroscopic-guided endometrial sampling. [10]
- Indications
- Patients who cannot undergo or decline hysterectomy
- Premenopausal patients who want to preserve fertility
- Options
- Levonorgestrel IUD and/or continuous oral progestin (e.g., megestrol acetate, medroxyprogesterone acetate)
- There is no consensus on optimal dosing and duration of treatment; consult specialists.
- Follow-up (with treating specialist)
- Endometrial sampling within 3–6 months of treatment to assess response [2][10][17]
- Consider long-term progestin therapy for patients with ongoing risk factors for endometrial cancer. [10]
- Advise patients to promptly follow up with their treating physician if they experience abnormal vaginal bleeding during conservative management.
Total hysterectomy is the definitive management for EIN. Progestin therapy is an alternative treatment option in select patients if concurrent endometrial cancer has been ruled out. [10]
Prevention [2]
- Screening for endometrial hyperplasia in asymptomatic individuals is not recommended.
- Primary prevention measures are the same for endometrial cancer; see “Prevention of endometrial cancer” for details.
Obesity is a major potentially modifiable risk factor for endometrial hyperplasia and endometrial cancer. [2][10]
Do not prescribe unopposed estrogen to a patient with an intact uterus. [18][19]
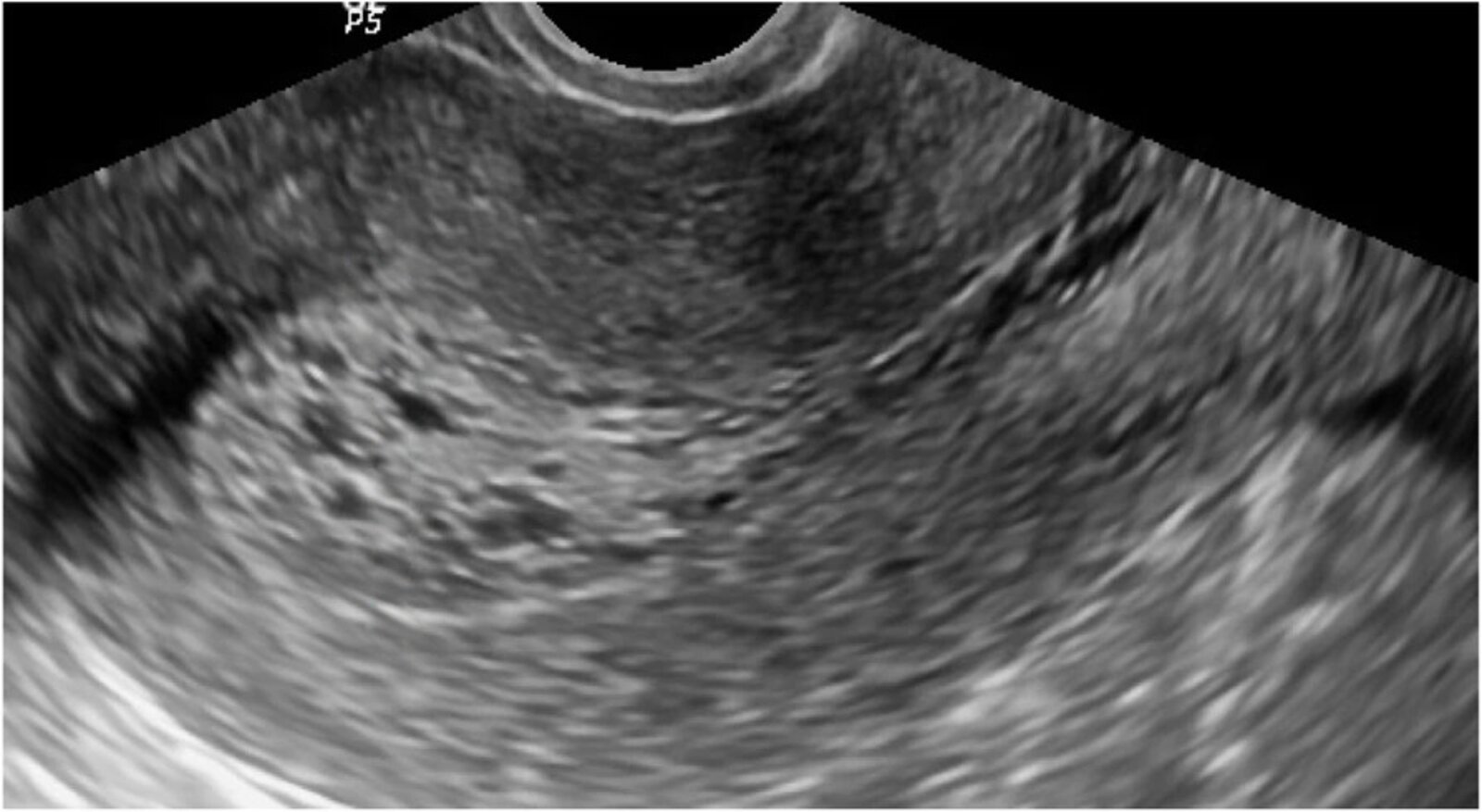
Ultrasound uterus (transvaginal; longitudinal plane)
The endometrium is diffusely thickened (16 mm) and heterogenous, with cystic changes. There is no visible irregularity at the myometrial interface to suggest invasion.
Endometrial thickness is measured on a midline longitudinal image at the thickest point and includes the echogenic basal layer (indicated by bracket). Any fluid within the endometrial cavity should be subtracted from the measurement.
Normal endometrial thickness varies throughout the menstrual cycle and in menopause. Diffuse thickening with cystic changes is a common feature of cystic endometrial hyperplasia but is not specific to that diagnosis. For example, both sessile polyps and endometrial carcinoma can produce a similar appearance. Endometrial hyperplasia may alternatively cause asymmetric thickening, which is generally considered suspicious for carcinoma. Ultrasound cannot reliably distinguish between endometrial hyperplasia and carcinoma.
Blue overlay: uterus
Source: “Figure 3, in: Role of transvaginal ultrasound in detection of endometrial changes in breast cancer patients under hormonal therapy” by Hetta WM, Samy A, Romeih M et al., Egyptian Journal of Radiology and Nuclear Medicine, licensed under CC BY 4.0. Modifications: removed green line, crosses and number. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
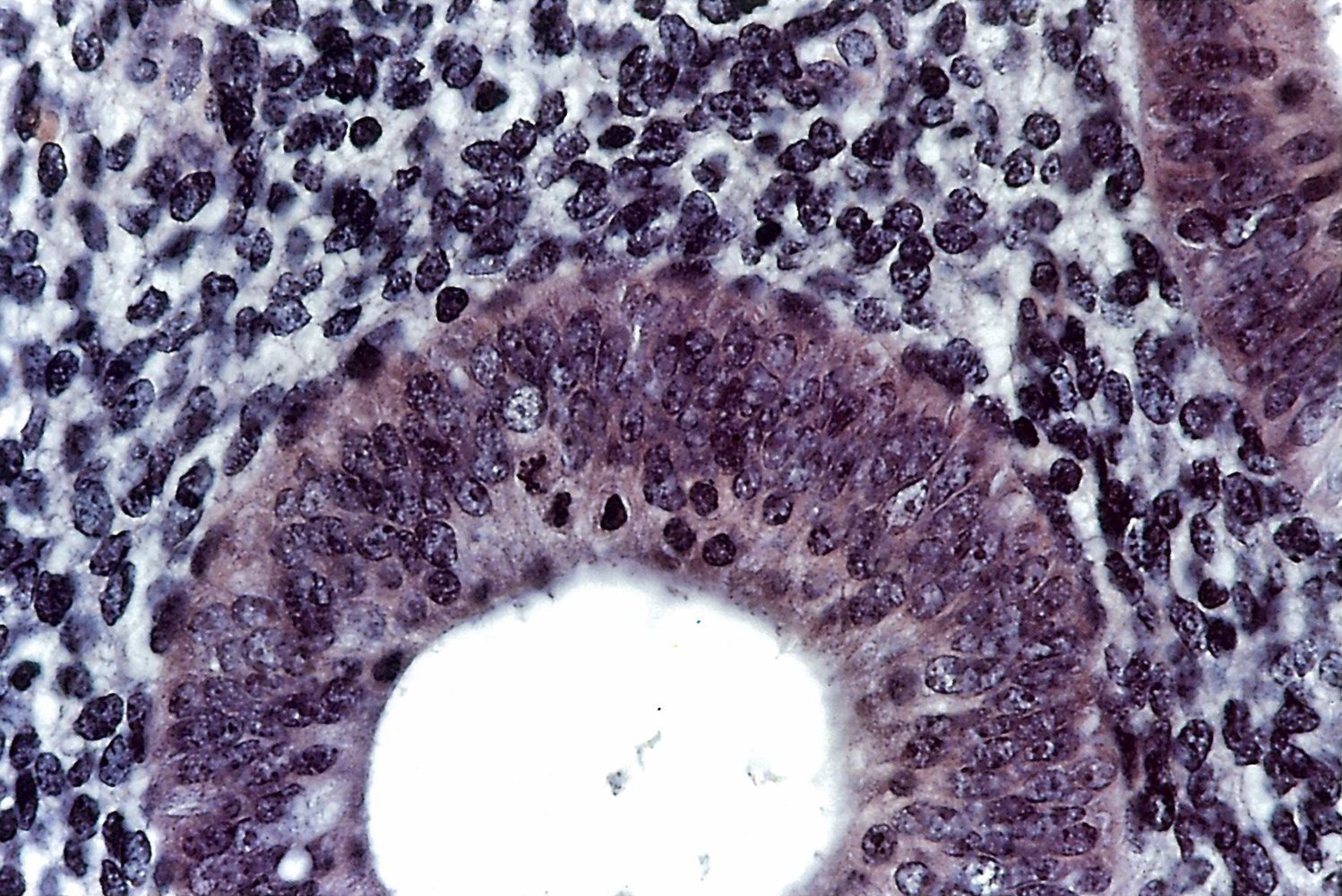
This magnified image shows columnar epithelium with no mitoses or suspected neoplastic cells (normal finding).
Source: © IMPP
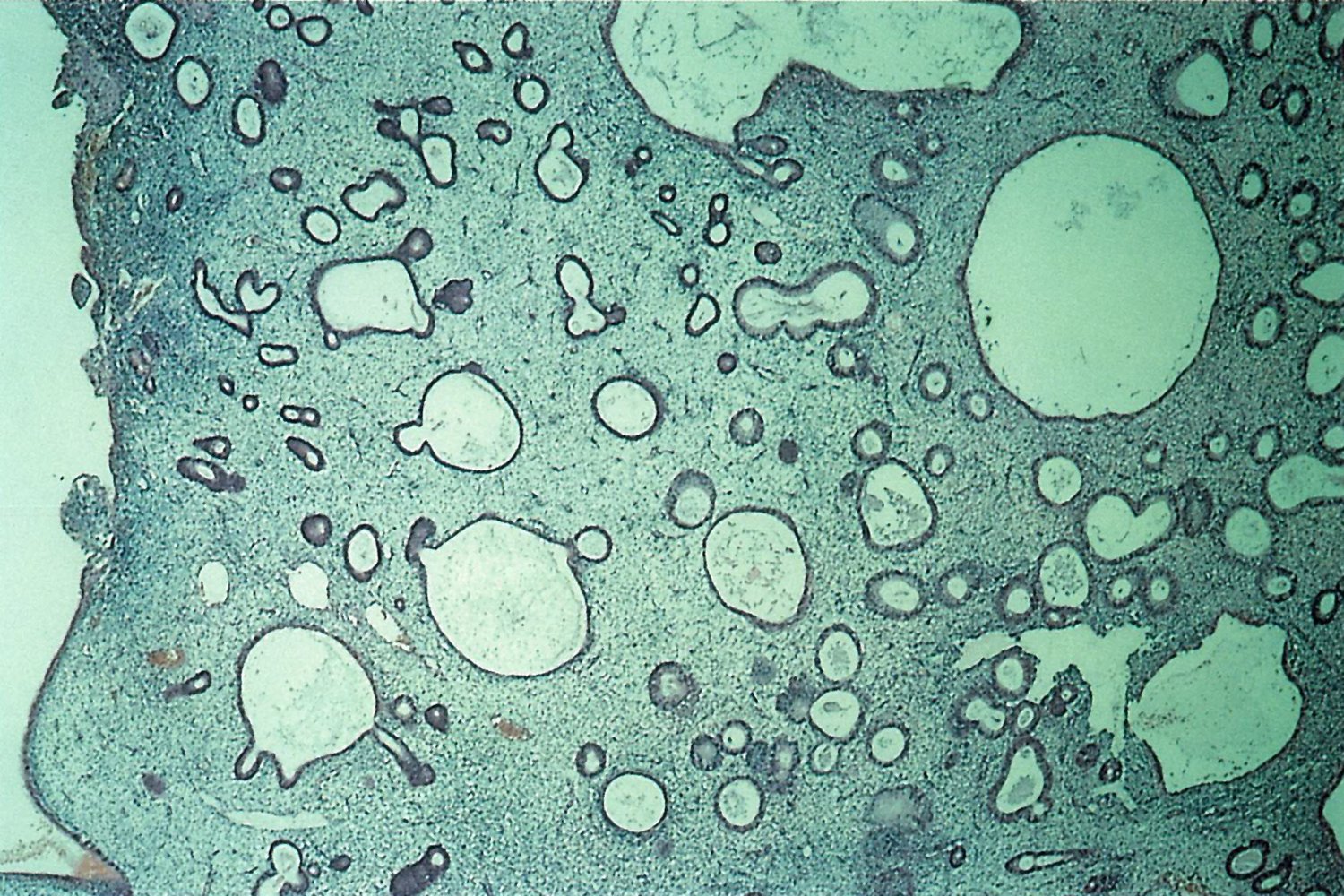
Photomicrograph of endometrium (H & E stain; low magnification)
The endometrial glands show cyst-like dilations. Some areas display glandular crowding.
These are the typical findings in simple endometrial hyperplasia (non-atypical endometrial hyperplasia).
Source: © IMPP
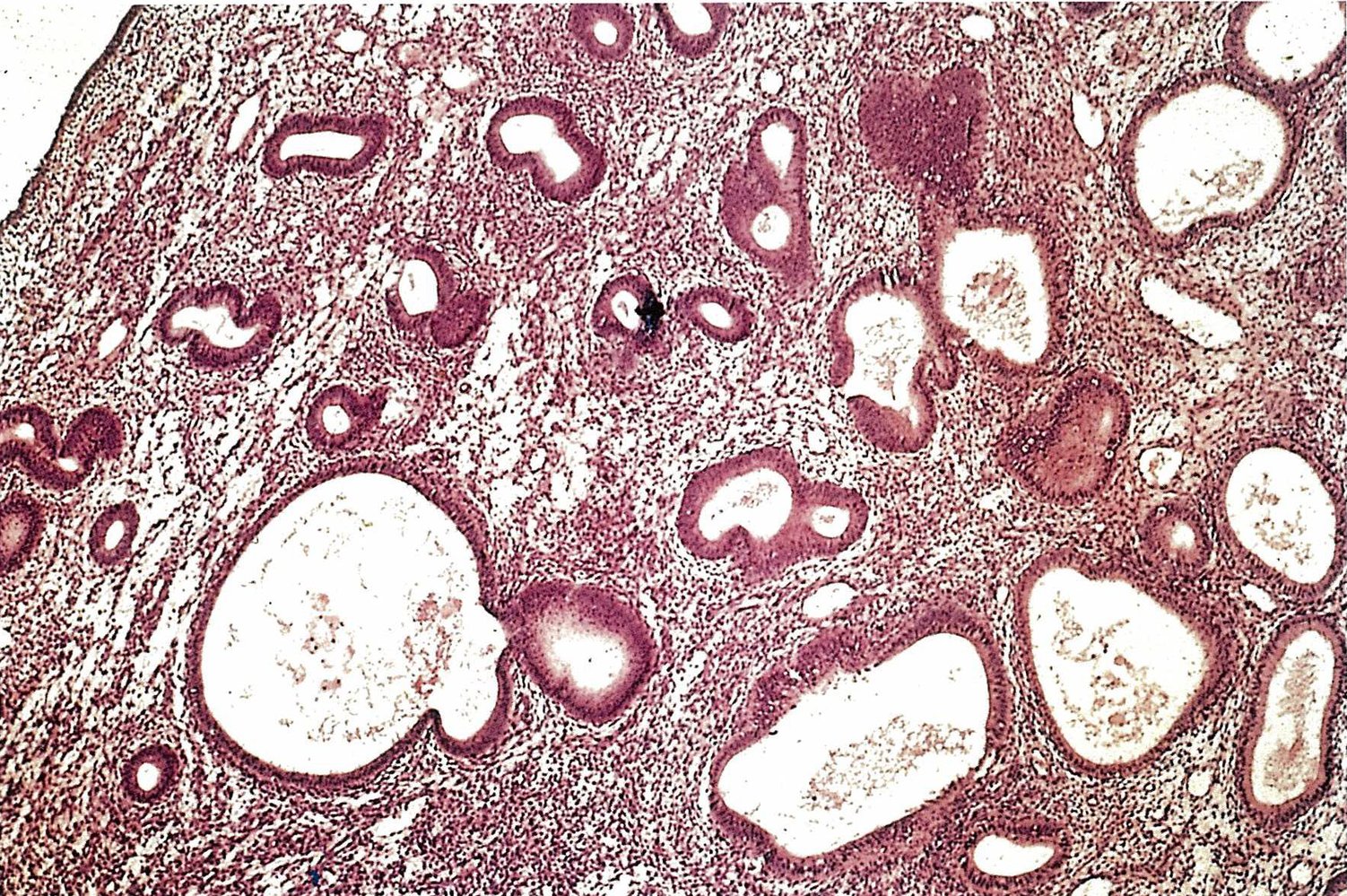
Microscopic image of the endometrium (H&E stain)
Endometrial tissue obtained via fractional curettage. The glandular cystic endometrial hyperplasia is characterized by an increase in both stromal and glandular cells. Enlarged, dilated mucosal glands (swiss cheese pattern) are located between the abundant stromal tissue.
Source: © IMPP
Endometrial polyps
Definition [20][21]
- Focal overgrowth(s) of benign endometrial tissue
- Localized within the uterine wall, extends into the uterine cavity
- Can be pedunculated or sessile, single or multiple, and up to many centimeters in size
- May contain smooth muscle cells and/or blood vessels
- Expresses both estrogen and progesterone receptors (estrogen may stimulate growth)
Etiology
The exact etiology is not clear. Risk factors for endometrial polyps include: [20][21]
- Hypertension
- Tamoxifen
- Older age
- Postmenopausal status
-
Hyperestrogenic conditions
- Obesity
- PCOS
- Estrogen-secreting ovarian sex cord-stromal tumor
- Chronic liver disease
- Late menopause
- Hormone replacement therapy [20]
Clinical features [20][22]
- Usually asymptomatic
-
Symptoms in premenopausal individuals
- Abnormal uterine bleeding (most common symptom) [21]
- Infertility [23]
- Recurrent pregnancy loss
- Symptoms in postmenopausal individuals: postmenopausal bleeding or spotting
Diagnostics [4][8]
See “Diagnostics for AUB,” “Diagnostics for infertility,” and “Diagnostics for PMB.” as needed.
-
TVUS with color Doppler ultrasound ; [8][24]
- First-line imaging for suspected endometrial polyp(s)
- Findings include: [20][25]
- Focal, homogeneous, echogenic endometrial mass with preserved endometrial-myometrial interface
- Distortion of the usual endometrial contour (interrupted mucosa sign)
- A single blood vessel supplying a polyp may be visible with color Doppler ultrasound [8]
- Additional studies for inconclusive TVUS findings [8][21]
- Hysteroscopy [4][22]
- Sonohysterography [4]
MRI pelvis with IV contrast is not a routine imaging modality to evaluate for endometrial polyps but it may be considered if there is concern for malignancy or if transvaginal access (e.g., for hysteroscopy) is not feasible. [4][8][24]
Blind endometrial biopsy may rule out differential diagnoses (e.g., endometrial hyperplasia, endometrial carcinoma) but is not recommended for the evaluation of focal lesions of the uterine cavity, such as endometrial polyps. [20][21][26]
Differential diagnoses
- Endometrial hyperplasia
- Endometrial carcinoma
- Uterine leiomyoma
- Other causes of AUB
- Other causes of PMB
Treatment [20][21]
Management is based on symptoms and risk factors for malignant endometrial polyp(s).
Observation and follow-up
- Indicated in asymptomatic premenopausal patients without indications for polypectomy
- Consider repeat imaging in 6–12 months if risk factors for type I endometrial cancer develop. [20]
- Spontaneous regression occurs in ∼ 25% of lesions; smaller lesions (≤ 1 cm) are more likely to regress. [20]
Hysteroscopic polypectomy
Referral to OB/GYN for consideration of polypectomy is indicated in the following situations.
-
Patients with risk factors for malignant endometrial polyp(s), i.e.: [20][21]
- Premenopausal patients with AUB
- Postmenopausal patients (with or without symptoms)
- Tamoxifen therapy
- Age ≥ 60 years
- Risk factors for endometrial cancer
- Premenopausal patients with infertility and/or recurrent pregnancy loss [20][21][22]
- Large polyps (e.g., ≥ 1 cm)
AUB, postmenopausal status, and tamoxifen use are the major risk factors for malignant endometrial polyps. [20]
Hysteroscopic polypectomy is indicated in symptomatic premenopausal patients, all postmenopausal patients, and patients with other risk factors for malignancy. [20][21]
Prognosis [20]
- ∼ 0.5–5% of endometrial polyps are premalignant or malignant.
- The risk increases with menopause, age ≥ 60 years, and/or tamoxifen use.
External Resources
References
- Ring KL, Mills AM, Modesitt SC. "Endometrial Hyperplasia". Obstet Gynecol. (2022)
- American College of Obstetricians and Gynecology Committee on Practice Bulletins–Gynecology and the Society of Gynecologic Oncology. "ACOG Practice Bulletin No. 149: Endometrial Cancer (reaffirmed 2021)". Obstetrics & Gynecology. 125(4). :1006-1026. (2015)
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. "Practice Bulletin No. 128: Diagnosis of Abnormal Uterine Bleeding in Reproductive-aged Women (reaffirmed 2024)". Obstet Gynecol. 120(1). :197-206. (2012)
- American College of Obstetrics and Gynecology Committee on Gynecologic Practice. "ACOG Committee Opinion No. 734: The Role of Transvaginal Ultrasonography in Evaluating the Endometrium of Women With Postmenopausal Bleeding (reaffirmed 2023)". Obstet Gynecol. 131(5). :e124-e129. (2018)
- Williams PM, Gaddey HL. "Endometrial Biopsy: Tips and Pitfalls". Am Fam Physician. 101(9). :551-556. (2020)
- Doll KM, Romano SS, Marsh EE, Robinson WR. "Estimated Performance of Transvaginal Ultrasonography for Evaluation of Postmenopausal Bleeding in a Simulated Cohort of Black and White Women in the US". JAMA Oncol. 7(8). :1158-1165. (2021)
- Robbins JB, Sadowski EA, Maturen KE, et al. "ACR Appropriateness Criteria® Abnormal Uterine Bleeding". J Am Coll Radiol. 17(11). :S336-S345. (2020)
- G. Emons, M. W. Beckmann, D. Schmidt, P. Mallmann for the Uterus commission of the Gynecological Oncology Working Group (AGO). "New WHO Classification of Endometrial Hyperplasias". Geburtshilfe Frauenheilkd. 75(2). :135-136. (2015)
- American College of Obstetricians and Gynecologists Committee on Clinical Consensus-Gynecology. "ACOG Clinical Consensus No. 5: Management of Endometrial Intraepithelial Neoplasia or Atypical Endometrial Hyperplasia". Obstet Gynecol. 142(3). :735-744. (2023)
- Matsuo K, Ramzan AA, Gualtieri MR, et al. "Prediction of concurrent endometrial carcinoma in women with endometrial hyperplasia". Gynecol Oncol. 139(2). :261-7. (2015)
- Emad Rakha, Siew Chee Wong, Irshad Soomro, et al. "Clinical outcome of atypical endometrial hyperplasia diagnosed on an endometrial biopsy: institutional experience and review of literature". The American Journal of Surgical Pathology. (2012)
- Nees LK, Heublein S, Steinmacher S, et al. "Endometrial hyperplasia as a risk factor of endometrial cancer". Arch Gynecol Obstet. 306(2). :407-421. (2022)
- Trimble CL, Method M, Leitao M, et al. "Management of Endometrial Precancers". Obstet Gynecol. 120(5). :1160-1175. (2012)
- "Green-top Guideline No. 67: Management of Endometrial Hyperplasia". https://www.rcog.org.uk/media/knmjbj5c/gtg_67_endometrial_hyperplasia.pdf. [2016-02-26]
- Mittermeier T, Farrant C, Wise MR. "Levonorgestrel-releasing intrauterine system for endometrial hyperplasia". Cochrane Database Syst Rev. 9(9). :CD012658. (2020)
- Adjei NN, Bowen MB, Wilke RN, Yates MS, Westin SN. "Uterine-Conserving Treatment Options for Atypical Endometrial Hyperplasia and Early Endometrial Cancer". Curr Oncol Rep. (2024)
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. "ACOG Practice Bulletin No. 141: Management of Menopausal Symptoms (reaffirmed 2024)". Obstet Gynecol. 123(1). :202-16. (2014)
- NAMS. "The 2022 hormone therapy position statement of The North American Menopause Society". Menopause. 29(7). :767-794. (2022)
- Bougie O, Randle E, Thurston J, et al. "Guideline No. 447: Diagnosis and Management of Endometrial Polyps". J Obstet Gynaecol Can. 46(3). :102402. (2024)
- Vitale SG, Haimovich S, Laganà AS, et al. "Endometrial polyps. An evidence-based diagnosis and management guide". Eur J Obstet Gynecol Reprod Biol. 260. :70-77. (2021)
- American College of Obstetricians and Gynecologists Committee on Gynecologic Practice and the American Association of Gynecologic Laparoscopists (AAGL) Practice Guidelines Committee. "ACOG Committee Opinion No. 800: The Use of Hysteroscopy for the Diagnosis and Treatment of Intrauterine Pathology (reaffirmed 2023)". Obstet Gynecol. 135(3). :e138-e148. (2020)
- Al Chami A, Saridogan E. "Endometrial Polyps and Subfertility". The Journal of Obstetrics and Gynecology of India. 67(1). :9-14. (2016)
- Munro MG, Critchley HOD, Broder MS, Fraser IS. "FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age". Int J Gynaecol Obstet. 113(1). :3-13. (2011)
- Kamaya A, Yu PC, Lloyd CR, et al. "Sonographic Evaluation for Endometrial Polyps". J Ultrasound Med. 35(11). :2381-2387. (2016)
- Vitale SG, Buzzaccarini G, Riemma G, et al. "Endometrial biopsy: Indications, techniques and recommendations. An evidence-based guideline for clinical practice". Journal of Gynecology Obstetrics and Human Reproduction. 52(6). :102588. (2023)
- "Contributor Disclosures - Diabetes mellitus in pregnancy. All of the relevant financial relationships listed for the following individuals have been mitigated: Jan Schlebes (medical editor, is a shareholder in Novo Nordisk, and was a shareholder in Fresenius SE & Co KGaA through Nov 2024). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy"