Summary
Benign bone lesions are a heterogeneous group of slow-growing neoplasms that arise from cartilage or bone. They appear on x-ray as localized lesions with sharp margins and without soft tissue involvement. Surgical removal or curettage may be required to manage pain and/or prevent pathological fractures.
Overview of benign bone tumors
Benign bone tumors are usually asymptomatic and do not require treatment until they become symptomatic (pain, swelling, etc). Surgery is indicated for symptomatic lesions and may involve curettage, bone grafting, or resection.
Predominantly osseous tumors
| Overview of predominantly osseous tumors | ||||
|---|---|---|---|---|
| Type | Description | Epidemiology | Location | Characteristics |
| Osteoid osteoma |
|
|
|
|
| Osteoblastoma |
|
|
|
|
| Giant-cell tumor (osteoclastoma) |
|
|
|
|
| Osteoma |
|
|
|
|
| Torus palatinus |
|
|
|
|


Tumors with cartilaginous components
| Overview of tumors with cartilaginous components | ||||
|---|---|---|---|---|
| Description | Epidemiology | Location | Characteristics | |
| (Distal) enchondroma |
|
|
|
|
| Chondroblastoma |
|
|
|
|
| Synovial chondromatosis |
|
|
|
|
| Osteochondroma (cartilaginous exostosis) |
|
|
|
|
Fibrous lesions
| Overview of fibromas | ||||
|---|---|---|---|---|
| Description | Epidemiology | Location | Characteristics | |
| Nonossifying fibroma |
|
|
|
|
| Ossifying fibroma |
|
|
|
|
| Fibrous dysplasia |
|
|
|
|
Cysts and hemangiomas
| Overview cysts and hemangiomas | ||||
|---|---|---|---|---|
| Type | Description | Epidemiology | Location | Characteristics |
| Unicameral bone cyst |
|
|
|
|
| Aneurysmal bone cyst |
|
|
|
|
| Intraosseous hemangioma |
|
|
|
|
| Langerhans cell histiocytosis |
|
|
|
|




A bony protrusion covered with normal mucosa is visible as a bump in the midline of the hard palate.
Source: “Photo taken of palatal tori.” by Dozenist, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

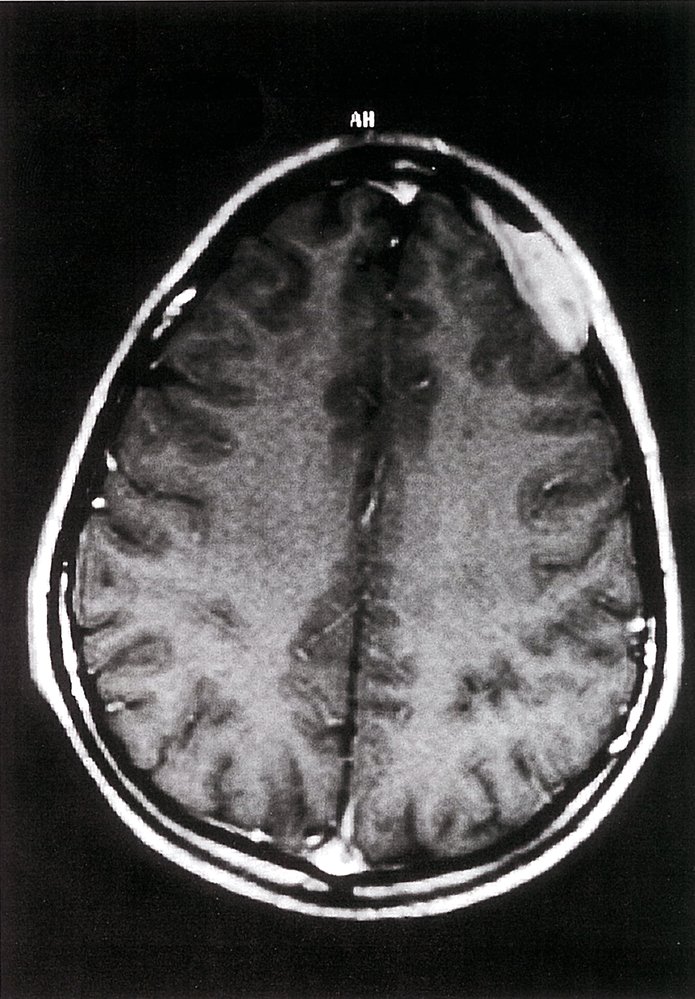
Cranial MRI (T1 weighted; axial view; with contrast)
There is an irregularly shaped, roughly ovoid, hyperintense mass (green overlay) adjacent to the inner side of the left frontotemporal skull.
This appearance is consistent with the bone lesions seen in Langerhans cell histiocytosis. Definitive diagnosis requires a biopsy with histopathological examination.
Source: © IMPP
© AMBOSS
© AMBOSS
Giant-cell tumor of bone (osteoclastoma)
- Description: benign but locally aggressive tumor composed of giant cells that arise from the bone marrow [1]
- Epidemiology: peak incidence between 20 and 40 years
-
Clinical features
- Found in the epiphysis or metaphysis of long bones (especially knee region)
- Pathological fractures
- Local pain and swelling
- Limited range of motion
-
Diagnostics
- X-ray: multicystic osteolytic lesions (soap-bubble appearance)
-
Histopathology
- Mononuclear, RANKL-expressing cells (neoplastic)
- Multinucleated giant cells (are reactive and resemble osteoclasts)
- Treatment: curettage and bone grafting or en-bloc resection to minimize recurrence rate
- Prognosis: risk of malignant degeneration increases with age; may spread to the lungs

")

X-ray left knee (AP view) of a 23-year-old patient with a giant cell tumor (osteoclastoma)
A lucent lesion in the proximal tibia (green overlay) has a bubbly appearance (examples indicated by outlines) and well-defined nonsclerotic margins. The cortex shows endosteal scalloping (examples indicated by arrowheads). The growth plate is closed and the lesion extends to the subarticular bone.
Giant cell tumor is one of several bone lesions that can have a bubbly appearance. Most giant cell tumors are eccentrically located, although large lesions may appear central. They are typically located at the ends of the long bones in the region of the closed growth plate. Some giant cell tumors contain aneurysmal bone cyst components.
Source: © IMPP
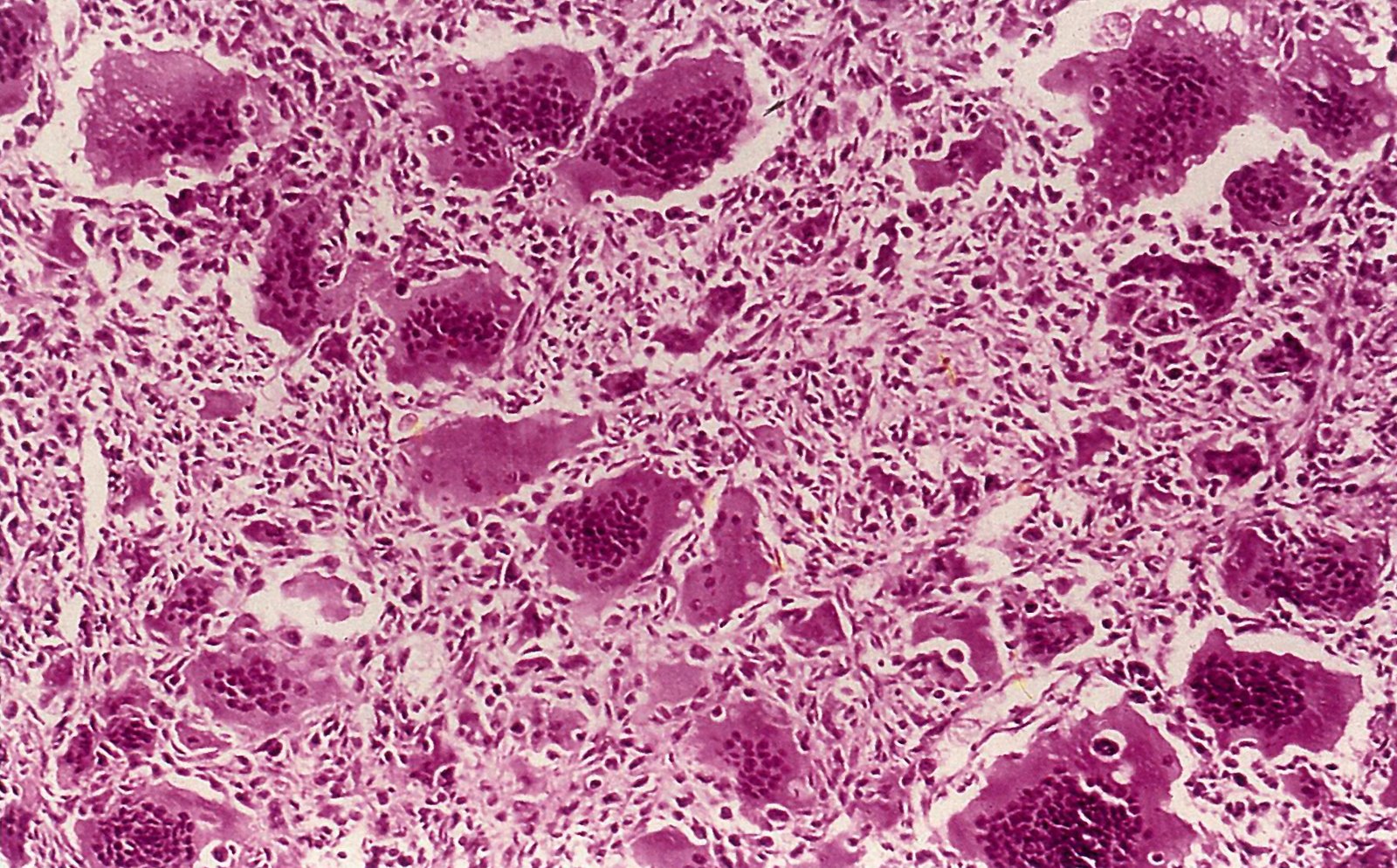
Photomicrograph of a section from a bone tumor biopsy (H&E stain)
Numerous giant cells containing multiple nuclei are visible throughout the image (examples indicated by yellow overlay). These cells are surrounded by a hypercellular stroma composed of mononuclear cells (examples indicated by black arrowheads).
These features are typical of giant-cell tumors of the bone.
Source: © IMPP
Osteochondroma (cartilaginous exostosis)
-
Description
- Bony outgrowth (exostosis) with a cartilaginous cap on the surface of long bones adjacent to growth plates
- Contains a marrow space that is continuous with the underlying bone
-
Epidemiology
- Most common primary benign bone tumor
- Peak incidence: 10–30 years [2]
- Sex: ♂ > ♀
-
Clinical features
- Typically located in metaphysis of long bones
- Usually asymptomatic, but can be painful and palpable near the ends of long bones
-
Subtypes and variants: hereditary multiple exostoses (EXT)
- Definition: autosomal dominant disorder with multiple exostoses
- Most commonly caused by autosomal dominant inheritance of a germline mutation in the EXT tumor suppressor gene.
- Malignant degeneration to chondrosarcoma may occur (∼ 5% of cases).
- Diagnostics: x-ray shows pedunculated; or sessile; lesion on the surface of the metaphysis of long bones
- Treatment: excision of tumor in symptomatic cases
- Complications: Approx. 1% transform into chondrosarcoma.





X-ray of the femur of a child (AP view)
A sessile bony outgrowth (green overlay) can be seen on the lateral metaphysis of the femur. The cartilage cap is irregular and shows arch-like calcifications.
Source: “EXOSTOSE” by Lucien Monfils, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
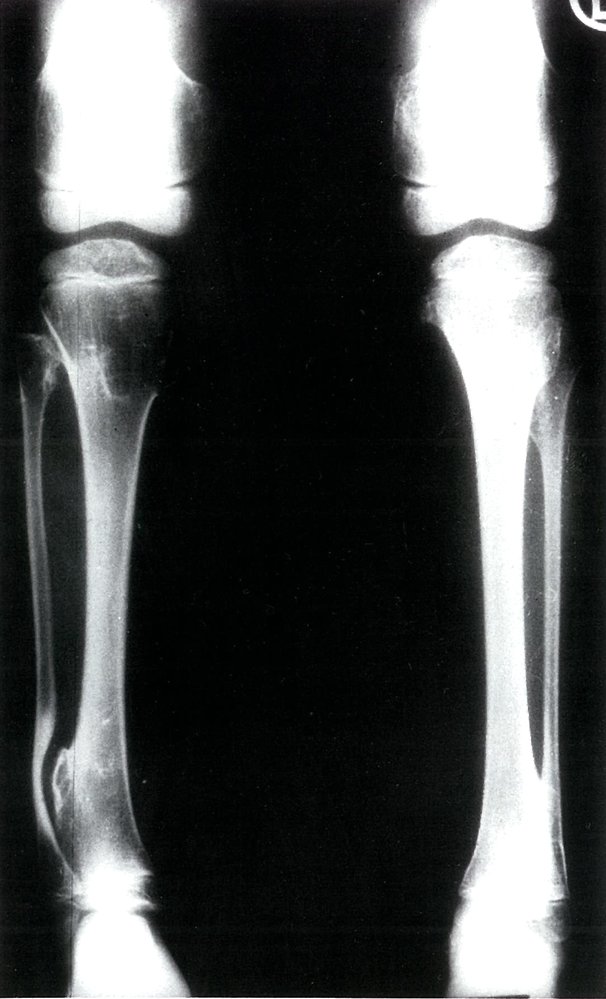
Bony exostosis on the lateral right distal tibial metaphysis and deformation of the right fibula
Source: © IMPP

Chest x-ray (PA view)
Osteochondroma of the rib.
Source: © IMPP

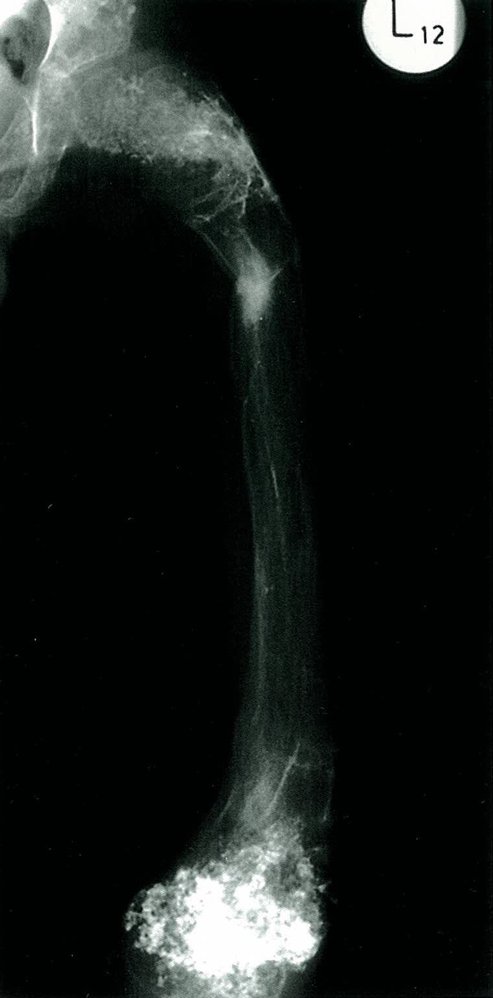
X-ray of the right upper arm
Patchy, calcified, mushroom-shaped exostosis on the surface of the humerus.
Displacement of the adjacent soft tissue (arrows) without infiltration (sharp demarcation).
Source: © IMPP
Enchondroma
- Description: benign tumor arising from hyaline cartilage
-
Epidemiology
- Most common type of hand tumor
- Peak incidence: 20–50 years (but may occur at any age)
-
Clinical features
- Usually found in medulla of the long bones of the hands and feet (most often the metacarpals of the hand and phalanges of the fingers)
- Often painless
- Widening of the bone
- Pathological (spontaneous) fractures
-
Subtypes and variants: enchondromatosis [3]
- Definition: A predominantly hereditary condition that manifests with multiple enchondromas.
- Epidemiology: peak incidence between 10 and 20 years
- Clinical features: often leads to skeletal deformities and stunted growth
- Prognosis: increased risk of malignant degeneration to chondrosarcoma
-
Treatment
- Asymptomatic tumors do not require treatment and close monitoring suffices.
- Symptomatic tumors may require surgical curettage and subsequent bone grafting to prevent pathological fractures.

")

Anteroposterior x-ray of the left hand: oval area of reduced bone density in the distal third of the fifth metacarpal bone (circled area);
Diagnosis: enchondroma of the fifth metacarpal bone
Source: © IMPP
X-ray of the left femur: lytic areas in the metaphyseal region of the femur with irregularly distributed, cloud-like calcifications, especially at the distal ends
Source: © IMPP
Chondroblastoma
- Description: benign cartilage tumor
-
Epidemiology
- Very rare
- Peak incidence: 10–20 years
-
Clinical features
- Located in epiphysis of long bones
- Joint pain (constant) and swelling
- Treatment: surgical curettage and bone grafting
Synovial chondromatosis
- Description: cartilage formation as a result of metaplasia of the synovial tissue
- Epidemiology: peak incidence between 20 and 40 years
-
Clinical features
- Most commonly located in the knees
- Pain, effusion, reduced range of motion, knee locking
- Diagnostics: x-ray shows radiographically visible (calcified) loose bodies
- Treatment: removal of loose bodies and synovial tissue
- Prognosis: extremely low risk of malignant degeneration to synovial chondrosarcoma


Lateral x-ray of the knee: radio-opaque elongated structure with calcified loose bodies in the suprapatellar recess
Source: © IMPP
Osteoid osteoma and osteoblastoma
Osteoid osteoma [4]
-
Description
- Small tumor (< 2 cm)
- Predominantly located in the cortex of long bones
-
Epidemiology
- Peak incidence: 4–25 years [5]
- Sex: ♂ > ♀
-
Clinical features
- Located in metaphysis and diaphysis of long bones (predominantly the proximal femur, tibia, and humerus) and vertebrae
- Constant, intense pain that worsens at night
- Pain is responsive to NSAIDs (e.g., ibuprofen, aspirin)
-
Diagnostics
- X-ray or CT: radiolucent core (osteoid), surrounded by perifocal sclerosis (nidus)
-
Scintigraphy: usually intense enhancement
- Double-density sign
- Intraoperative nuclear imaging using a probe to detect the tumor
- Treatment: NSAIDs or surgical removal if pain is unresponsive to medical treatment



Osteoblastoma [6]
- Description: predominantly cortical tumor larger than osteoid osteoma (> 2 cm)
-
Epidemiology
- Peak incidence: 10–20 years
- Sex: ♂ > ♀
-
Clinical features
- Typically involves the posterior elements of the vertebrae (vertebral arch)
- Severe chronic local pain (no nocturnal pain) that does not respond to NSAIDs
- Neurologic symptoms if the spinal cord is compressed
-
Diagnostics: x-ray
- Shows tumor located in the cortical bone
- Central lucent nidus with mild or absent perifocal sclerosis
-
Treatment
- Unresponsive to NSAIDs
- Surgical curettage and bone grafting preferred


X-ray right hip (AP view) of a 12-year-old boy
A small lucent nidus (hatched green overlay) in the medial proximal femur is accompanied by reactive sclerosis and cortical thickening (green overlay).
The appearance is compatible with osteoid osteoma, although other conditions (e.g., intracortical abscess, stress fracture, osteoblastoma) can mimic osteoid osteoma and must be distinguished on the basis of the clinical presentation and additional imaging.
Source: © IMPP
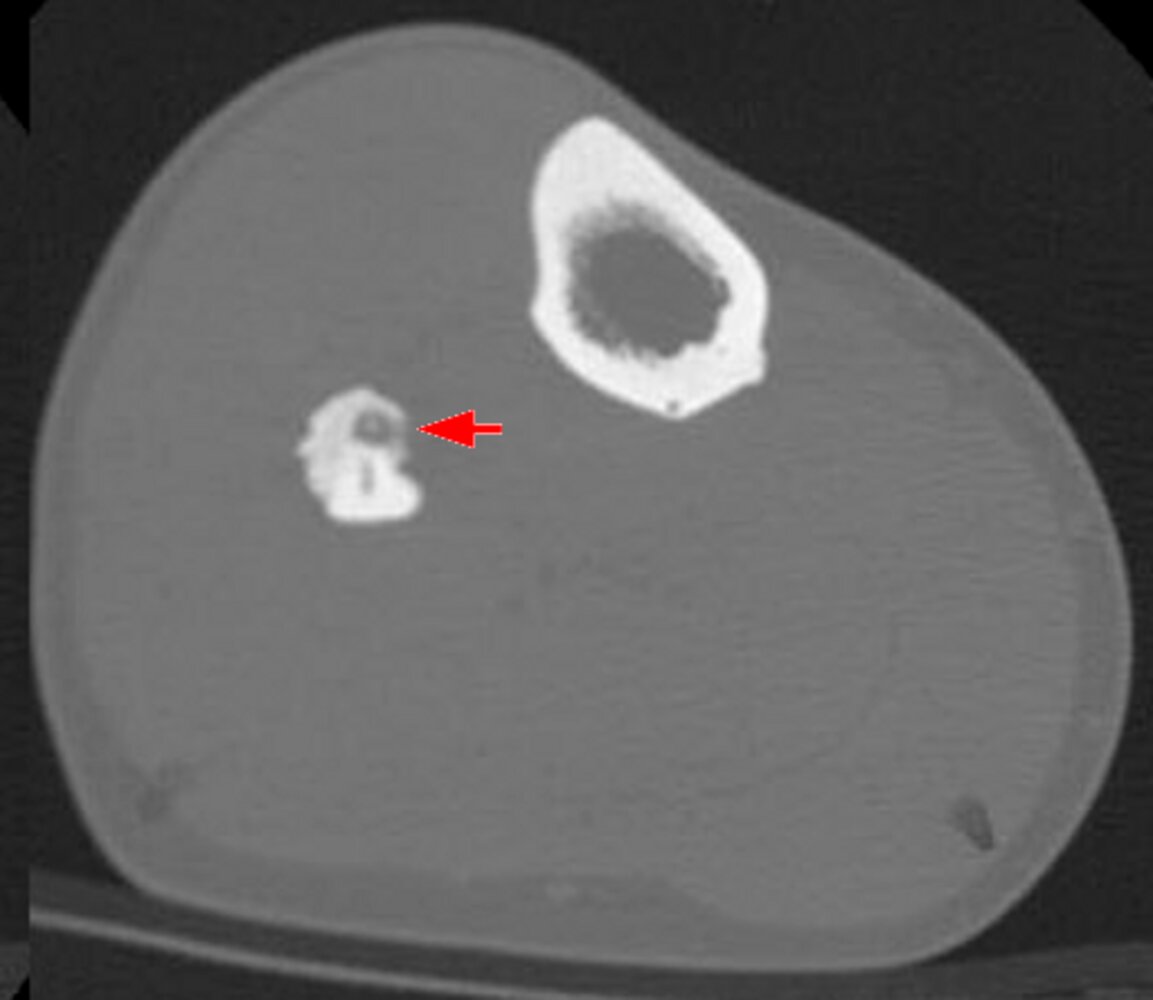
CT of the lower leg
A nidus (red arrow) is visible within the fibula. A vessel canal (green overlay) is also visible.
This appearance is typical of osteoid osteoma.
Source: “Osteoidosteom_Fibula_CT_KF” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

CT left hip (A: axial plane, B: coronal plane, C: sagittal plane; bone window)
A small, low-attenuation nidus (green arrowhead) with central high-attenuation mineralized osteoid (red arrowhead) is present in the superomedial acetabular cortex. The lesion is surrounded by reactive sclerosis (black arrowhead) and represents an acetabular osteoid osteoma (white arrows).
Source: “Figure 3, in: Hip arthroscopy for the management of osteoid osteoma of the acetabulum: a systematic review of the literature and case report” by Yousef A. Marwan, Sarantis Abatzoglou, Ali A. Esmaeel et al., BMC Musculoskeletal Disorders Journal, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
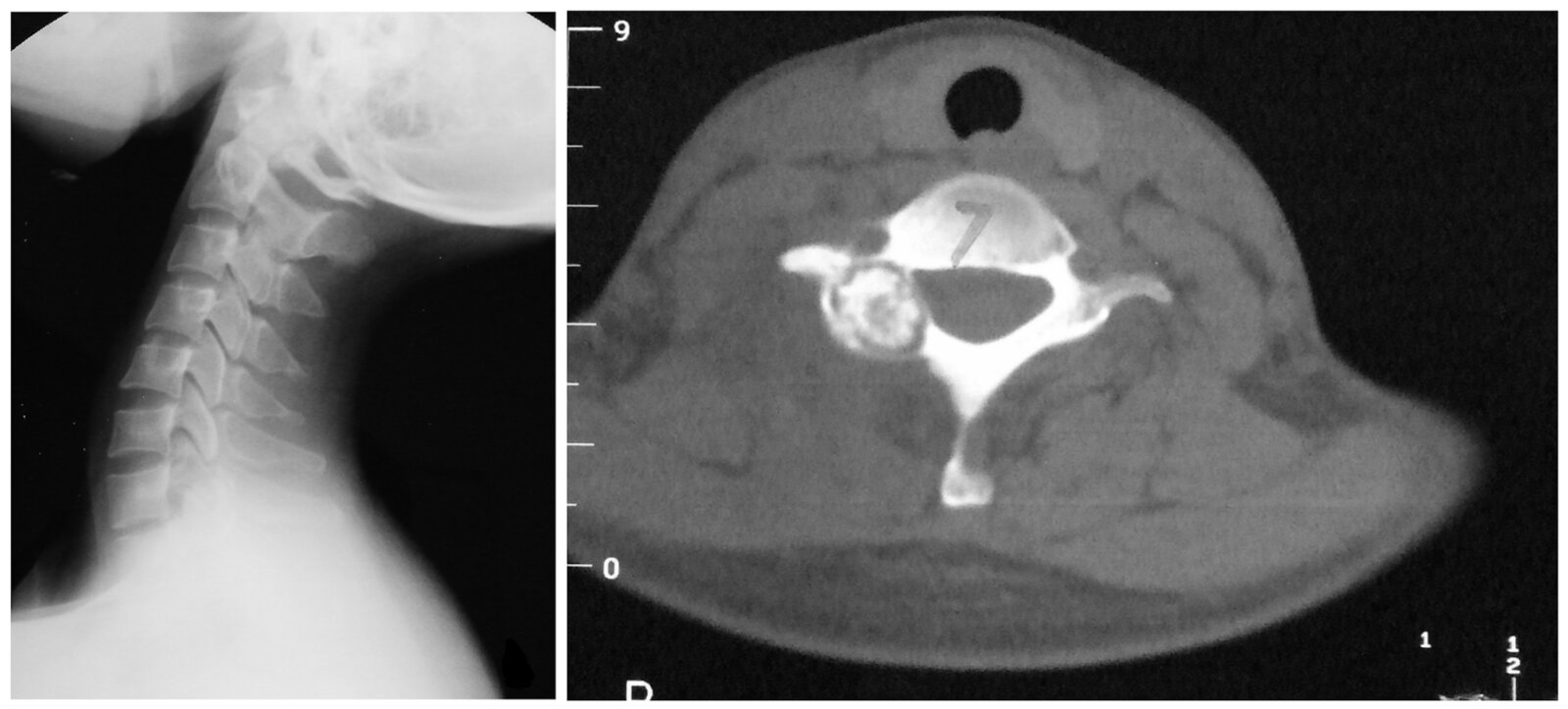
X-ray cervical spine (lateral view) and CT cervical spine (bone window; axial plane)
An expansile mixed lytic and sclerotic lesion involves the right C7 posterior elements (green overlay). The epicenter is in the region of the right lateral mass.
Source: “Clinical Features and Surgical Management of Spinal Osteoblastoma: A Retrospective Study in 18 Cases” by Zhonghai Li, Yantao Zhao, Shuxun Hou, Ningfang Mao, Shunzhi Yu, Tiesheng Hou, PLOS ONE, licensed under CC BY 4.0. Modifications: created photo collage of two pictures; one image is cropped; letter removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Osteoma
- Description: benign round bone tumor
- Epidemiology: most common in middle-aged individuals but may develop at any age
- Etiology: associated with Gardner syndrome
-
Clinical features
- Usually affects facial bones and cranial bones (most commonly affects paranasal sinuses)
- In rare cases, long bones
- Often asymptomatic
- An osteoma of the paranasal sinus may lead to obstruction of the ostium, with subsequent congestion and pressure headaches.
- Associated with Gardner syndrome: extracolonic manifestation of familial adenomatous polyposis (FAP) that includes osteomas of the skull or mandible, hypertrophy of the retinal pigment epithelium, adrenal adenomas, desmoid tumors, dental abnormalities, and cutaneous lesions
- Treatment: Surgical removal may be required if expansive tumor growth leads to symptoms.

Osteomas of the skull and mandible in conjunction with hypertrophy of the retinal pigment epithelium, adrenal adenomas, desmoid tumors, and dental abnormalities are characteristic of Gardner syndrome.
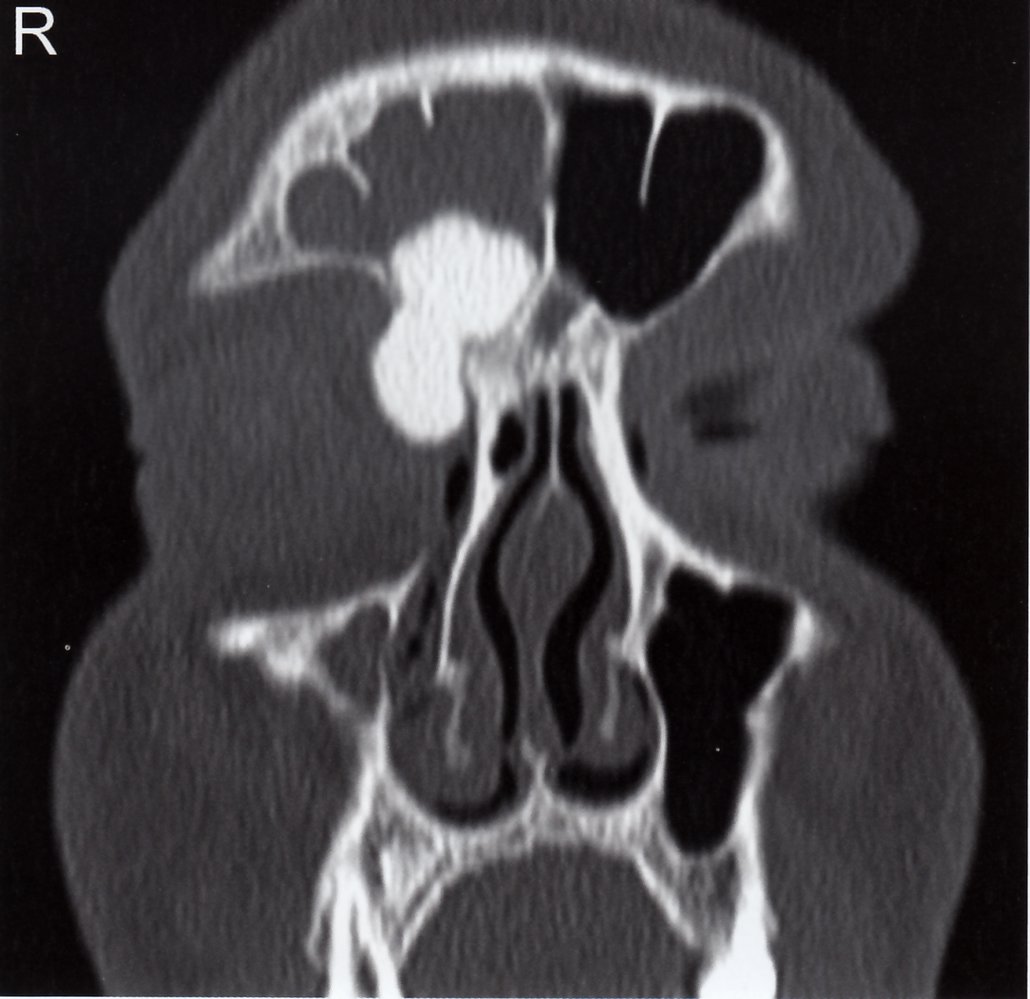
Cranial CT (coronal section, bone window)
The hyperdense, sharply demarcated lesion (green overlay) in the right frontal sinus is most likely an osteoma. There is opacification of the right frontal sinus (white area), which is likely caused by the tumor affecting secretion drainage at the ostium (white arrows) of the frontal sinus.
Source: © IMPP
Nonossifying fibroma
- Description: growth of fibrous connective tissue into areas that normally ossify; a tumor-like lesion that is considered to be a nonneoplastic disorder of bone growth, rather than a true neoplasm
- Epidemiology: peak incidence between 10 and 20 years
-
Clinical features
- Usually metaphyseal (predominantly in the distal femur and distal tibia)
- asymptomatic; usually an incidental finding [7][8]
-
Diagnostics: x-ray
- Marginal sclerosis
- Lobulated structure with translucent components
-
Treatment
- Usually self-limiting
- Bone grafting may be required for painful lesions or to prevent pathological fractures.




Posteroanterior x-ray of the right knee in an 11-year-old boy: sharply demarcated, oval translucency with marginal sclerosis in the distal femur at the transition from the metaphysis to the diaphysis (green striped area). (green shaded area = patella; Fe = femur; f = Fibula; t = Tibia; arrow = open epiphyseal plate)
Source: © IMPP

Anteroposterior x-ray of the knee; 18-year-old patient
The mediodistal femur epiphysis shows translucent areas (blue overlay) with sclerotized margins (exemplary marked with arrowheads).
The appearance is typical for a nonossifying fibroma.
Source: © IMPP

Lateral x-ray of the knee: A sharply demarcated, elongated, oval, translucent lesion with a lobulated structure and marginal sclerosis can be seen in the distal femoral diaphysis, which most likely indicates a nonossifying fibroma (1). The medial (broken line) and lateral (solid line) condyles as well as the projection of the epicondyles (2) are indicated for guidance purposes.
Source: © IMPP

Right upper ankle joint in two planes: eccentric, lobulated translucent lesion with marginal sclerosis in the metaphyseal region of the tibia
Source: © IMPP
Ossifying fibroma (osteofibrous dysplasia)
- Description: fibrous benign bone tumor
- Epidemiology: peak incidence between 1 and 5 years
-
Clinical features
- Most commonly found in tibia and fibula
- Localized swelling
- Tibial bowing
- Diagnostics: X-ray shows intracortical, osteolytic lesions with interspersed sclerosis.
-
Treatment
- If asymptomatic, monitoring is sufficient.
- If symptomatic, surgical removal is preferred.
Fibrous dysplasia
- Description: Fibrous dysplasia is a benign, developmental disorder of bone that causes normal skeletal tissue to be replaced by fibrous tissue.
-
Epidemiology
- Fibrous dysplasia accounts for approx. 5% of benign bone lesions
- Age of onset: most commonly presents during adolescence
- Sex: ♂ = ♀
- Etiology: post-zygotically acquired, somatic, gain-of-function mutation in GNAS1 gene on chromosome 20q
-
Pathophysiology
- GNAS1 codes for the α subunit of the Gs protein (Gsα).
- Mutation → constitutive activation of certain Gs-cAMP coupled pathways → inhibition of mesenchymal differentiation into osteoblasts → lack of osteocytes → skeletal lesions composed largely of mesenchymal cells → weak, imperfect bone with fibrous tissue
-
Clinical features
- Disease phenotype
- Monostotic fibrous dysplasia (∼ 70% of cases)
- Polyostotic fibrous dysplasia (∼ 25% of cases)
- Common to all disease phenotypes
- Bone pain, bone deformities, and/or pathological fractures
- Entrapment neuropathies may occur as a result of expanding bone lesions
- Age at manifestation
- Monostotic fibrous dysplasia: 20–30 years
- Polyostotic fibrous dysplasia: < 10 years
- Disease phenotype
-
Diagnostics
- Laboratory tests
- ↑ Alkaline phosphatase (occasionally)
- Normal calcium, PTH, and 1,25-dihydroxyvitamin D levels
- Imaging: x-ray
- Long bones: well-defined, lobulated lesions with a thin cortex and a radiolucent, ground-glass appearance
- Facial bones: radiodense lesions with a leonine appearance
- Pathology: bone biopsy
- Laboratory tests
-
Therapy
- Bisphosphonates
- Management of precocious puberty: See “Peripheral precocious puberty.”
-
Prognosis
- The lesions do not heal spontaneously.
- Osteosarcomas occur in < 1% of cases.
References:[9]
Syndromes associated with polyostotic fibrous dysplasia
-
McCune-Albright syndrome
- Polyostotic fibrous dysplasia
- Café au lait spots with unilateral, ragged edges
- Most commonly peripheral precocious puberty
-
Mazabraud syndrome
- Polyostotic fibrous dysplasia
- Intramuscular myxomas
-
Jaffe-Lichtenstein syndrome
- Café au lait spots
- Polyostotic fibrous dysplasia


Photograph of the torso of a 5-year-old girl
Multiple large, hyperpigmented lesions (café-au-lait spots) can be seen on the face, the left hemithorax, and the left arm. The borders of the lesions are jagged (coast-of-Maine appearance) and barely cross the midline.
Café-au-lait spots are characteristic findings in McCune-Albright syndrome.
© AMBOSS. This image was adapted from the image “Figure 1 A, in: McCune-Albright syndrome” by Dumitrescu CE, Collins MT, Orphanet Journal of Rare Diseases, licensed under CC BY 2.0.
Unicameral bone cyst
- Description: solitary, single-chambered cyst
- Epidemiology: peak incidence between 5 and 15 years
-
Clinical features
- Found in metaphysis of the long bones (predominantly the proximal humerus and proximal femur)
- Usually asymptomatic
- Pathological fractures
-
Diagnostics
- X-ray: osteolytic bone lesion with sharp margins and no sclerosis in the metaphysis of long bones
- MRI: single-chambered, fluid-filled lesion
- Treatment: monitoring or aspiration and corticosteroid injection for larger lesions
Aneurysmal bone cysts
-
Description
- Osteolytic lesions; usually septated, blood-filled cysts
- Idiopathic (primary aneurysmal bone cyst) or secondary to malignant or other benign bone diseases (secondary aneurysmal bone cyst)
- Epidemiology: peak incidence between 10 and 20 years
-
Clinical features
- Common sites are the spine and the metaphysis of the femur and tibia.
- Usually asymptomatic; local pain and swelling may occur
- Pathological fracture: often the first sign
-
Diagnostics
- X-ray: metaphyseal, osteolytic lesion with sclerotic margins
- MRI : septated, blood-filled lesions, with typical fluid-fluid levels.
- Treatment: surgical curettage and bone grafting
- Prognosis: high risk of recurrence



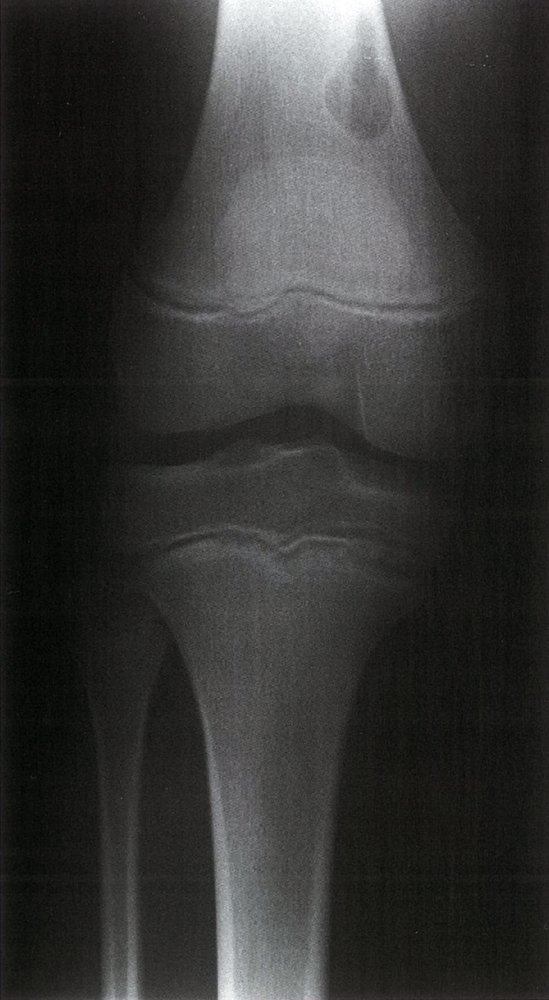
X-ray of the right knee joint (PA)
A sharply demarcated, osteolytic lesion (green area) with a thin sclerotic edge (white lines) can be seen in the lateral part of the distal femur. It is most likely an aneurysmal bone cyst, although the finding could also be unicameral bone cyst.
Source: © IMPP
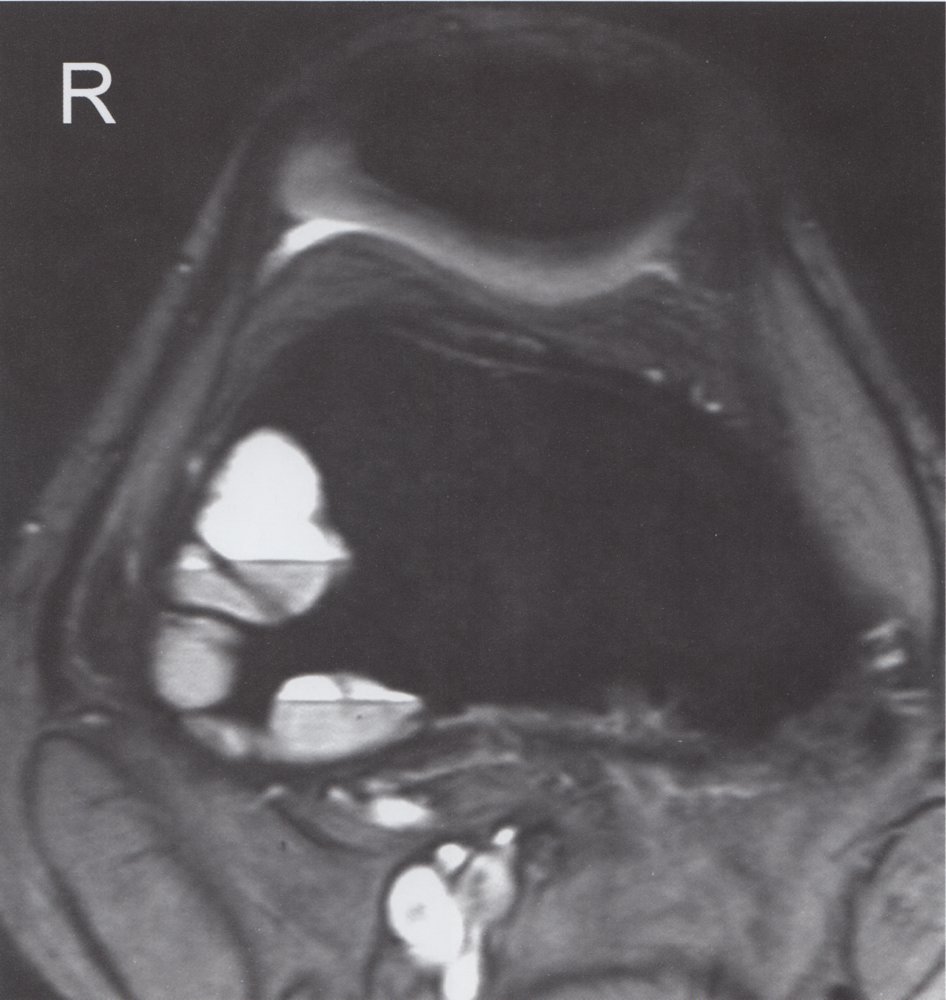
MRI of the right knee joint at the level of the femoral condyles (axial)
In the lateral part of the distal femur, there are multiple, septated, hyperintense lesions (green overlay) with a fluid-fluid level (red overlay). This is an aneurysmal bone cyst.
Source: © IMPP
Intraosseous hemangioma
- Description: vascular neoplasm [10]
-
Epidemiology
- Peak incidence: 30–50 years
- Sex: ♂ < ♀ (1:2)
-
Clinical features
- Most common benign tumor of the spine, particularly in the thoracic and lumbar vertebrae
- Usually asymptomatic; often an incidental finding
-
Diagnostics: x-ray
- Vertical streaks visible in vertebrae
- Honeycomb appearance of lesion with sharp margins
- Treatment: usually no treatment required
-
Complications
- Compression fractures
- Spinal stenosis
- Bleeding with subsequent spinal epidural hematoma


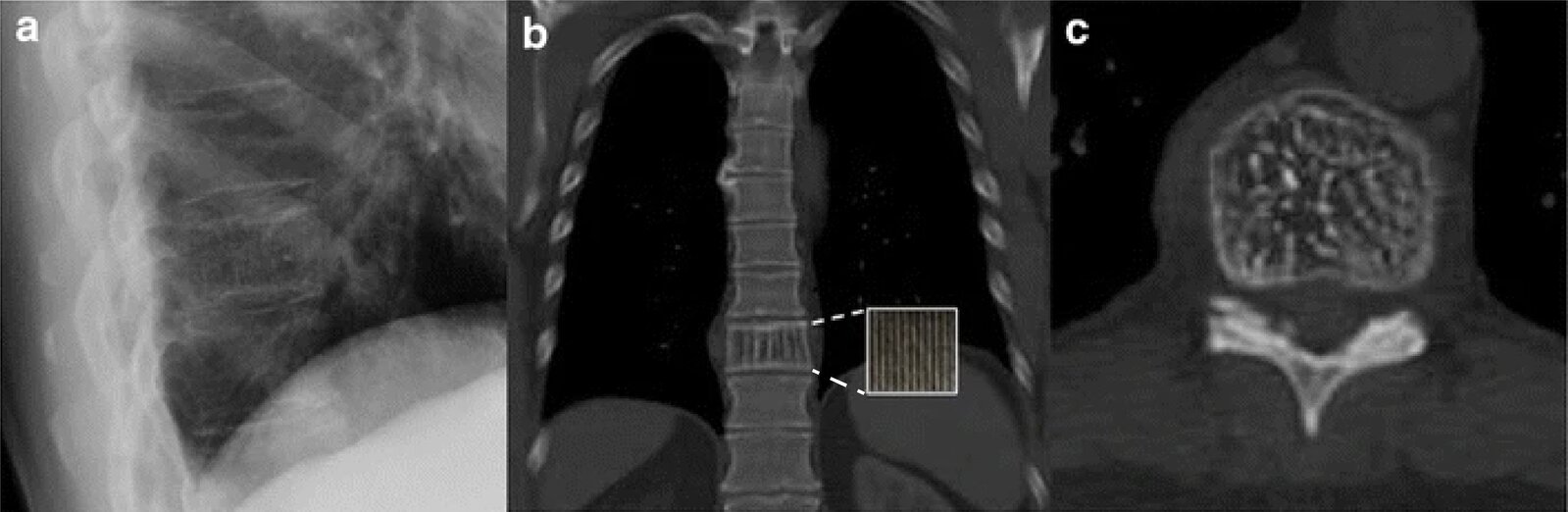
X-ray chest (A: lateral view) and CT chest (without contrast; B: coronal plane; C:axial plane)
The T10 vertebral body (green dashed outline) has a vertically striated (corduroy) appearance (examples indicated by yellow overlay) on both the lateral radiograph and the coronal CT section and a dotted (salt and pepper) appearance (examples indicated by red overlay) on the axial CT section.
Vertebral hemangiomas often have a characteristic imaging appearance. Vertical striations are the result of thickening of the bony trabeculae and produce a dotted appearance if imaged en face.
Source: “Fig 1, In: The clothes maketh the sign” by Buckley B, Chan VO, Mitchell DP et al., SpringerLink, licensed under CC BY 4.0. Modifications: Adjusted the dashed line of the zoom box. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
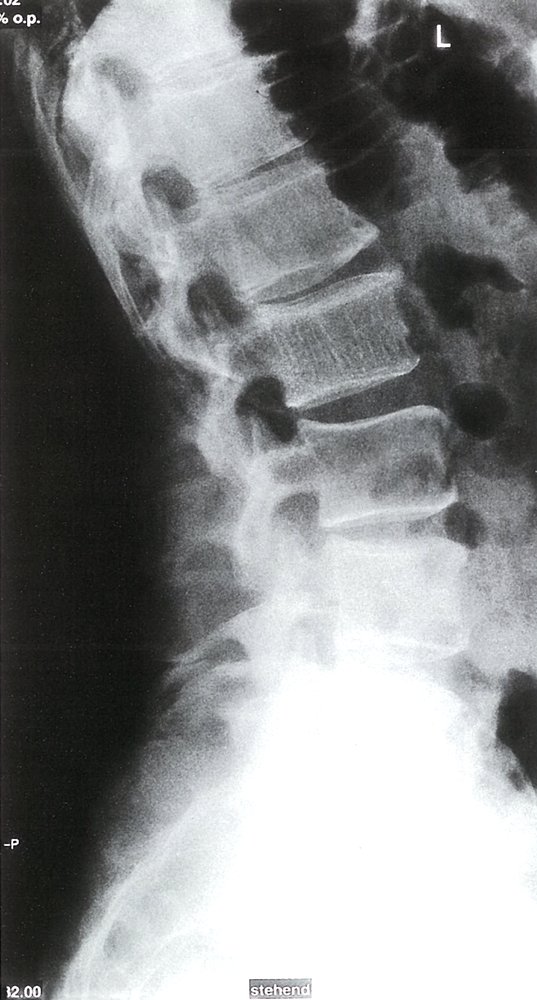
Standing X-ray of the lumbar spine: L2 shows hypertrophic sclerosis of the vertical trabeculae, which indicates an intraosseous hemangioma.
Source: © IMPP
Langerhans cell histiocytosis
- Description: : a rare disorder caused by clonal proliferation of Langerhans cells (antigen-presenting cells) [11]
- Epidemiology: : peak incidence between 5 and 10 years
-
Clinical features
-
Osseous lesions (90%): pain and/or swelling, pathological fractures
-
Localization: skull (most common site), femur, vertebra, mandible, ilium, ribs
- Can cause recurrent otitis media if the mastoid bone is involved
- Unifocal or multifocal
-
Localization: skull (most common site), femur, vertebra, mandible, ilium, ribs
- Systemic manifestations (less common)
- Skin rash: brown to purple papules and/or eczematous rash
- Hepatomegaly and/or splenomegaly
- Lymphadenopathy
- Bone marrow infiltration
- Hypopituitarism that typically manifests as central diabetes insipidus
- Exanthema
-
Osseous lesions (90%): pain and/or swelling, pathological fractures
-
Diagnostics
- Normal calcium levels
- X-ray: osteolytic lesions with or without marginal sclerosis
-
Biopsy (confirmatory test): proliferation of Langerhans cells (polygonal cells with coffee bean-shaped nuclei and eosinophilic cytoplasm) ; [12][13]
- Electron microscopy: Birbeck granules (tennis racket-shaped or rod-like structures) in the cytoplasm
- Immunohistochemistry: cells are positive for S100, CD1a, and/or CD207
-
Treatment
- Solitary bone lesions in low-risk anatomical regions
- Asymptomatic lesion: A wait-and-watch approach may be appropriate.
- Symptomatic lesion: curettage and/or excision (as a part of biopsy)
- Bone lesions in high-risk anatomical regions (e.g., lesions involving the odontoid process or regions of the skull other than the vault), multifocal bone involvement, or systemic manifestation: vinblastine and prednisone
- Solitary bone lesions in low-risk anatomical regions

")


X-ray skull (left: lateral view; right: PA view) of a child with Langerhans cell histiocytosis (LCH)
Well-defined lytic lesions without sclerotic margins are seen in the frontoparietal and high-parietal regions of the calvarium (example indicated by green overlay).
Various conditions can cause lytic skull lesions. LCH lesions are typically rounded or ovoid in shape and have nonsclerotic well-defined margins. Edges may be beveled as a result of uneven destruction of the inner and outer tables. Coalescence of enlarging lesions can produce a geographic appearance.
Source: “Fig 2, In: Infiltrating the Heart and Kidney: A Rare Pediatric Case of Multisystem Langerhans Cell Histiocytosis from Pakistan” by Mahmood S, Raza M, Nusrat K, Marsia S, Abbas A, Cureus, licensed under CC BY 3.0. Modifications: Removed white arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
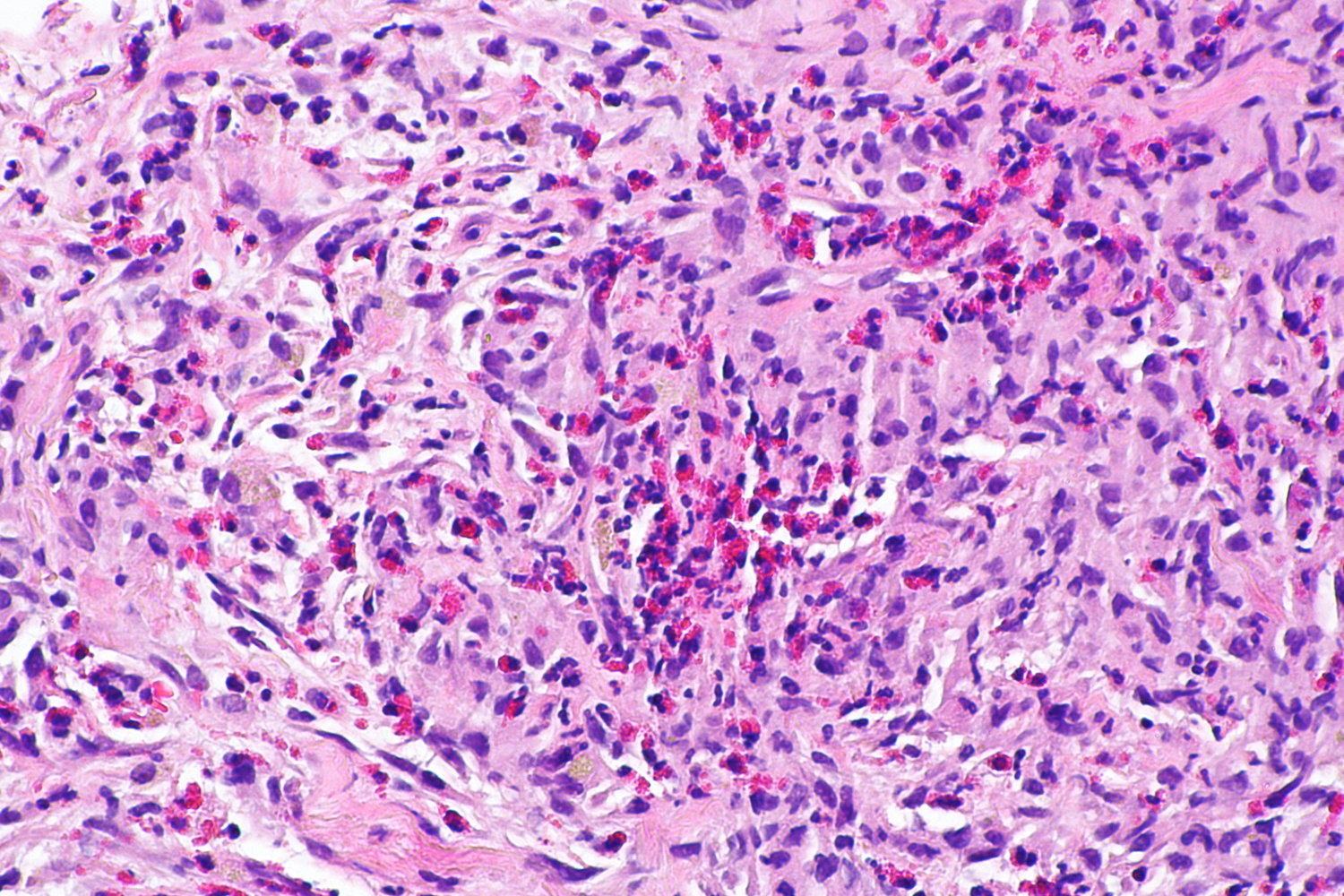
Photomicrograph of a biopsy sample from a pulmonary nodule (H&E stain; high magnification)
Numerous specialized histiocytes (Langerhans cells; examples indicated by arrowheads) are identifiable as large cells with abundant eosinophilic cytoplasm and large folded or grooved nuclei (coffee bean nuclei; zoom box). A mixed inflammatory infiltrate of eosinophils (yellow overlay), neutrophils, and lymphocytes is also visible.
The presence of Langerhans cells was confirmed by immunohistochemistry (Langerin, CD1a, and S100 positive).
Source: “Pulmonary Langerhans cell histiocytosis -- high mag” by Librepath, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Electron micrograph of a Langerhans cell
The Birbeck granules are visible as tennis-racket-shaped structures within the cytoplasm (illustration; examples indicated by green overlay).
Birbeck granules are a diagnostic marker for Langerhans cell histiocytosis.
Source: “Langerhans cell histiocytosis - Birbeck granules” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
Cranial MRI (T1 weighted; axial view; with contrast)
There is an irregularly shaped, roughly ovoid, hyperintense mass (green overlay) adjacent to the inner side of the left frontotemporal skull.
This appearance is consistent with the bone lesions seen in Langerhans cell histiocytosis. Definitive diagnosis requires a biopsy with histopathological examination.
Source: © IMPP
References
- "Osteoclastoma". https://radiopaedia.org/cases/osteoclastoma-1. [2017-02-16]
- Verdegaal SHM, Bovée JVMG, Pansuriya TC, et al. "Incidence, Predictive Factors, and Prognosis of Chondrosarcoma in Patients with Ollier Disease and Maffucci Syndrome: An International Multicenter Study of 161 Patients". Oncologist. 16(12). :1771-1779. (2011)
- ller L, Wood NH, Khammissa RA, Lemmer J, Raubenheimer EJ. "The nature of fibrous dysplasia". Head Face Med. 5. :22. (2009)
- "Primary Intraosseous Haemangioma". https://radiopaedia.org/articles/primary-intraosseous-haemangioma. [2017-09-01]
- Howlett D., Farrugia M., Ferner R., Rankin S. "Multiple lower limb non-ossifying fibromas in siblings with neurofibromatosis". Eur J Radiol. 26(3). :280-283. (1998)
- Mankin HJ, Trahan CA, Fondren G, Mankin CJ. "Non-ossifying fibroma, fibrous cortical defect and Jaffe–Campanacci syndrome: a biologic and clinical review". MUSCULOSKELETAL SURGERY. 93(1). :1-7. (2009)
- "Osteoid Osteoma". https://radiopaedia.org/articles/osteoid-osteoma. [2018-06-04]
- "Osteoid Osteoma". https://orthoinfo.aaos.org/en/diseases--conditions/osteoid-osteoma. [2019-08-01]
- Lucas DR. "Osteoblastoma". Arch Pathol Lab Med. 134(10). :1460-6. (2010)
- "Osteochondroma". https://orthoinfo.aaos.org/en/diseases--conditions/osteochondroma/. [2018-12-01]
- "Langerhans Cell Histiocytosis in Children". https://www.dynamed.com/topics/dmp~AN~T919995/Langerhans-cell-histiocytosis-in-children. [2017-09-07]
- "Langerhans Cell Histiocytosis". http://www.pathologyoutlines.com/topic/boneLCH.html. [2016-10-19]
- "Langerhans Cells". http://www.pathologyoutlines.com/topic/skinnontumorlangerhans.html. [2016-05-19]