Summary
Blunt trauma is any nonpenetrating injury caused by the impact of a blunt object against the body, resulting in damage to underlying structures. Common causes include motor vehicle collisions and falls from height. Clinical features and diagnostic studies vary based on the type and location of blunt trauma. Assessment of patients with blunt trauma follows the systematic evaluation outlined in the advanced trauma life support (ATLS) algorithm: primary survey, transfer to a trauma center (if indicated), secondary survey, and tertiary survey. Management involves treating immediately life-threatening injuries and surgical repair of traumatic injuries.
See also “Management of trauma patients” and “Penetrating trauma.”
Overview
Management of blunt trauma is based on the type and location of the injury. Recommendations in this article are consistent with the 2018 guidelines on ATLS. See also “Trauma in pregnant individuals,” “Trauma in older adults,” and “Trauma in children.” [1]
Types of blunt trauma [1][2]
- Open wounds (e.g., abrasions, lacerations)
- Contusions
- Fractures
- Crush injury
- Acceleration-deceleration injury (e.g., coup-contrecoup injury)
Blunt trauma injuries by mechanism [1][2]
The most common causes of blunt trauma injuries include motor vehicle collisions, vehicle-pedestrian collisions, falls from height, and bicycling injuries. [3]
| Blunt trauma injuries by mechanism [1][2] | |||
|---|---|---|---|
| Mechanism | Typical injuries | ||
| Motor vehicle collisions (MVC) | Frontal impact |
|
|
| Rear impact |
|
||
| Side impact |
|
||
| Rollover |
|
||
| Ejection from vehicle |
|
||
| MVC-related trauma mechanisms | Windshield-related trauma |
|
|
| Seatbelt-related trauma |
|
||
| Airbag-related trauma |
|
||
| Motor vehicle–pedestrian collision | Low-speed collision |
|
|
| High-speed collision |
|
||
| Motorcycle collisions [4] |
|
||
| Bicycle collisions [5] |
|
||
| Falls from a height [6] | Vertical impact |
|
|
| Horizontal impact |
|
||
| Ground-level falls |
|
||
| Battery |
|
||
Blunt trauma injuries by location [1]
| Blunt trauma by body region [1] | ||
|---|---|---|
|
Location |
Potential injuries | Management |
| Head |
|
|
| Neck |
|
|
| Chest |
|
|
| Abdomen and pelvis |
|
|
| Extremities |
|
|
Blunt chest trauma
Approach to blunt chest trauma [1]
Ensure the following components are included as part of the standard management of trauma patients using the ATLS algorithm:
-
Primary survey
- Identify and treat respiratory failure and shock, tension pneumothorax, massive hemothorax, and cardiac tamponade (see “Management” for details).
- Perform resuscitative thoracotomy in pulseless patients with previously documented signs of life.
- If at a nontrauma center, initiate transfer to a trauma center; high-speed MVCs, ejection from vehicle, or death of a passenger are indications for trauma team activation.
- See “Traumatic circulatory arrest” for the management of cardiac arrest due to trauma.
-
Secondary survey
- Examine the chest for paradoxical chest movement and crepitus.
- Utilize clinical decision tools while obtaining urgent diagnostics for trauma patients (see “Diagnostics”).
- Assess for indications for urgent thoracotomy.
- Begin initial management of vertebral injuries, if suspected.
Clinical features [1]
- Hemorrhagic shock and/or obstructive shock (e.g., hypotension, tachycardia)
- Respiratory distress (e.g., tachypnea, hypoxia)
- Absent or decreased breath sounds
- Jugular venous distention
- Pain (e.g., chest pain, rib pain, pleuritic chest pain)
- Chest wall deformity (e.g., flail chest)
- Subcutaneous emphysema
- Tracheal deviation
Esophageal injuries may be missed initially; suspect esophageal rupture in a patient with left-sided pneumothorax without apparent rib fracture. [1]
Diagnostics [1][7][8]
Clinical decision tools can help identify patients who do not require imaging. See “Urgent diagnostics for trauma patients” for a comprehensive approach to trauma imaging.
- Bedside assessment: CXR, eFAST, ECG
-
CT imaging in trauma
- Chest CT with IV contrast
- CTA chest if vascular injury is suspected
- Additional testing: bronchoscopy, esophagoscopy, echocardiography
NEXUS chest decision instrument for blunt chest trauma [9][10]
The NEXUS chest decision instrument for blunt chest trauma is a clinical decision tool to identify patients with a very low risk of thoracic injury who do not require thoracic imaging (e.g., CXR, chest CT).
| NEXUS chest decision instrument for blunt chest trauma [9][10] | |
|---|---|
| Criteria | Points |
| Age > 60 years | 1 |
| Rapid deceleration mechanism, e.g., fall from 20 ft or MVC > 40 mph | 1 |
| Chest pain | 1 |
| Intoxication | 1 |
| Altered mental status | 1 |
| Distracting injury | 1 |
| Chest wall tenderness | 1 |
| |

NEXUS chest CT-all decision instrument for blunt chest trauma [11]
The NEXUS chest CT-all decision instrument for blunt chest trauma is a clinical decision tool to identify patients at very low risk of thoracic injuries who do not require a chest CT.
| NEXUS chest CT-all decision instrument for blunt chest trauma [11] | |
|---|---|
| Criteria | Points |
| Abnormal CXR | 1 |
| Distracting injury | 1 |
| Chest wall, sternum, thoracic spine, or scapular tenderness | 1 |
| Rapid deceleration mechanism, e.g., fall from 20 ft or MVC > 40 mph | 1 |
| |
Management [1][2]
Bedside interventions
The following bedside interventions may be performed during the primary survey:
- Pulseless patient; with previously documented signs of life after blunt injury: resuscitative thoracotomy
- Respiratory failure: rapid sequence intubation and mechanical ventilation
- Tension pneumothorax: emergency chest decompression
- Massive hemothorax: chest tube placement
- Cardiac tamponade: pericardiocentesis followed by pericardial window; or resuscitative thoracotomy
- Esophageal injury: chest tube placement



Further management
Further management depends on the type and extent of associated injuries.
- Close monitoring of vital signs
- Definitive surgical management after stabilization, e.g., urgent thoracotomy for open pneumothorax, definitive management of vertebral injuries
- Nonsurgical management, e.g., analgesia for rib fractures
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
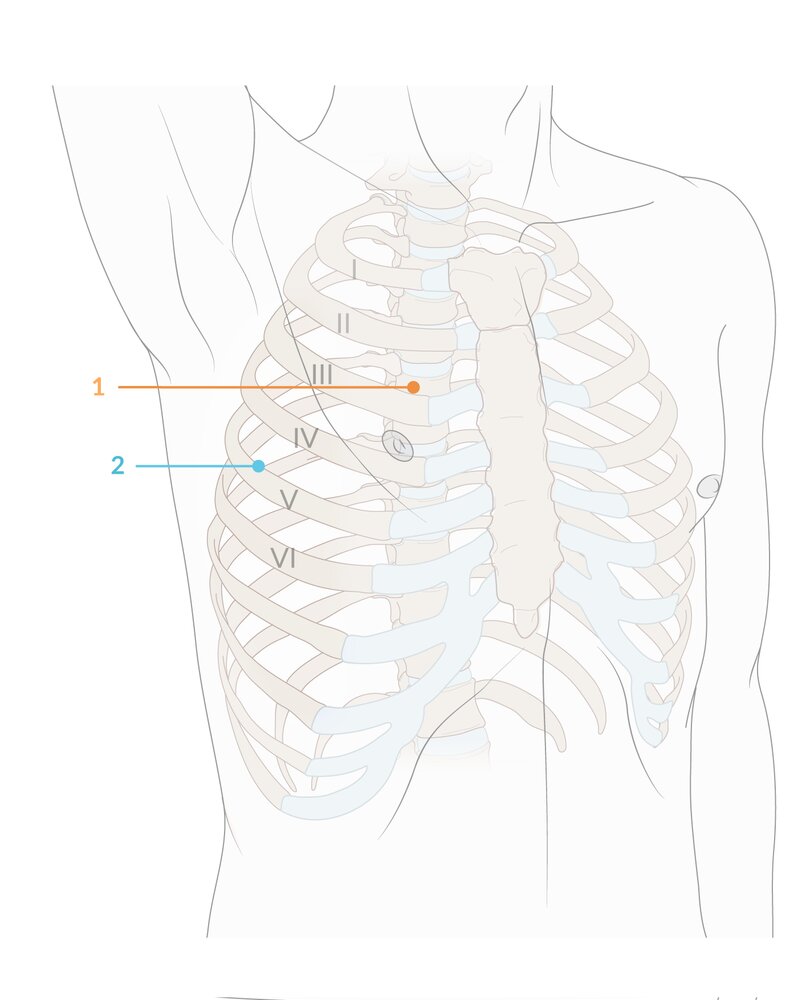
The 2nd intercostal space, located at the midclavicular line (1; orange marker), can be used in both adults and children for emergency needle thoracostomy to decompress a tension pneumothorax.
The 4th or 5th intercostal space, between the anterior and midaxillary lines (2; blue marker), is the standard site for tube thoracostomy in both adults and children and in adults may also be used for needle thoracostomy.
© AMBOSS
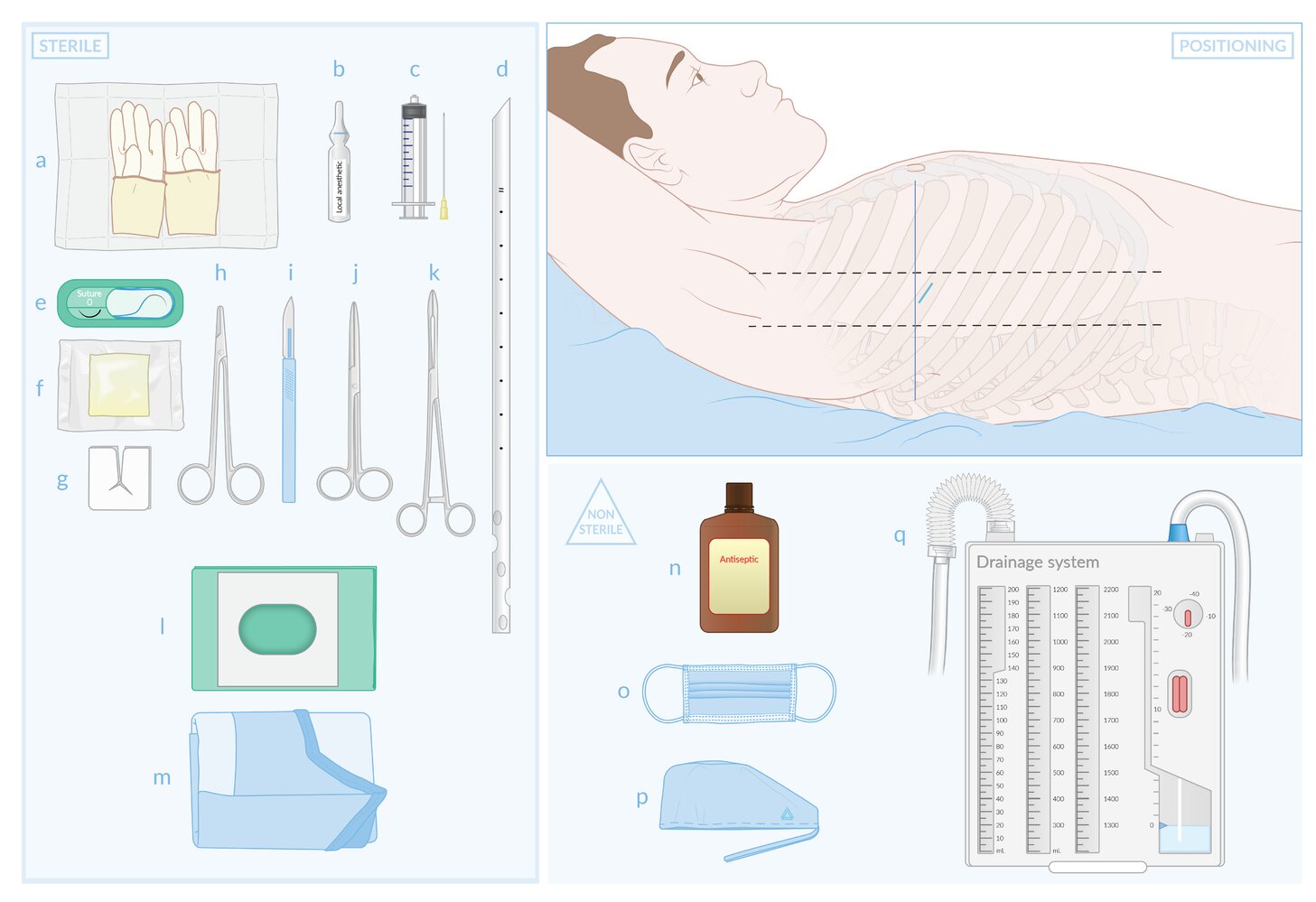
Sterile equipment (left): (a) sterile gloves; (b) local anesthetic; (c) syringe and needle for local anesthesia; (d) chest tube; (e) nonabsorbable suture; (f) petroleum-impregnated gauze; (g) split dressing; (h) needle holder; (i) scalpel; (j) blunt scissors; (k) Kelly clamp; (l) fenestrated drape; (m) surgical gown
Nonsterile equipment (bottom right): (n) antiseptic; (o) mask; (p) surgical cap; (q) drainage system
Patient positioning and insertion site (top right)
- Positioning: The patient should be supine with the head of the bed at 30–60 degrees and the ipsilateral arm raised behind the head to expose the axilla.
- Insertion site: most commonly in the 4th or 5th intercostal space (ICS), between the anterior and midaxillary lines (dotted lines). In male patients, the nipples are usually at the level of the 4th ICS (long blue line). The incision (short blue line) is made at the superior border of the rib immediately below the targeted ICS in order to avoid the neurovascular bundle located on the inferior edge of each rib.
© AMBOSS
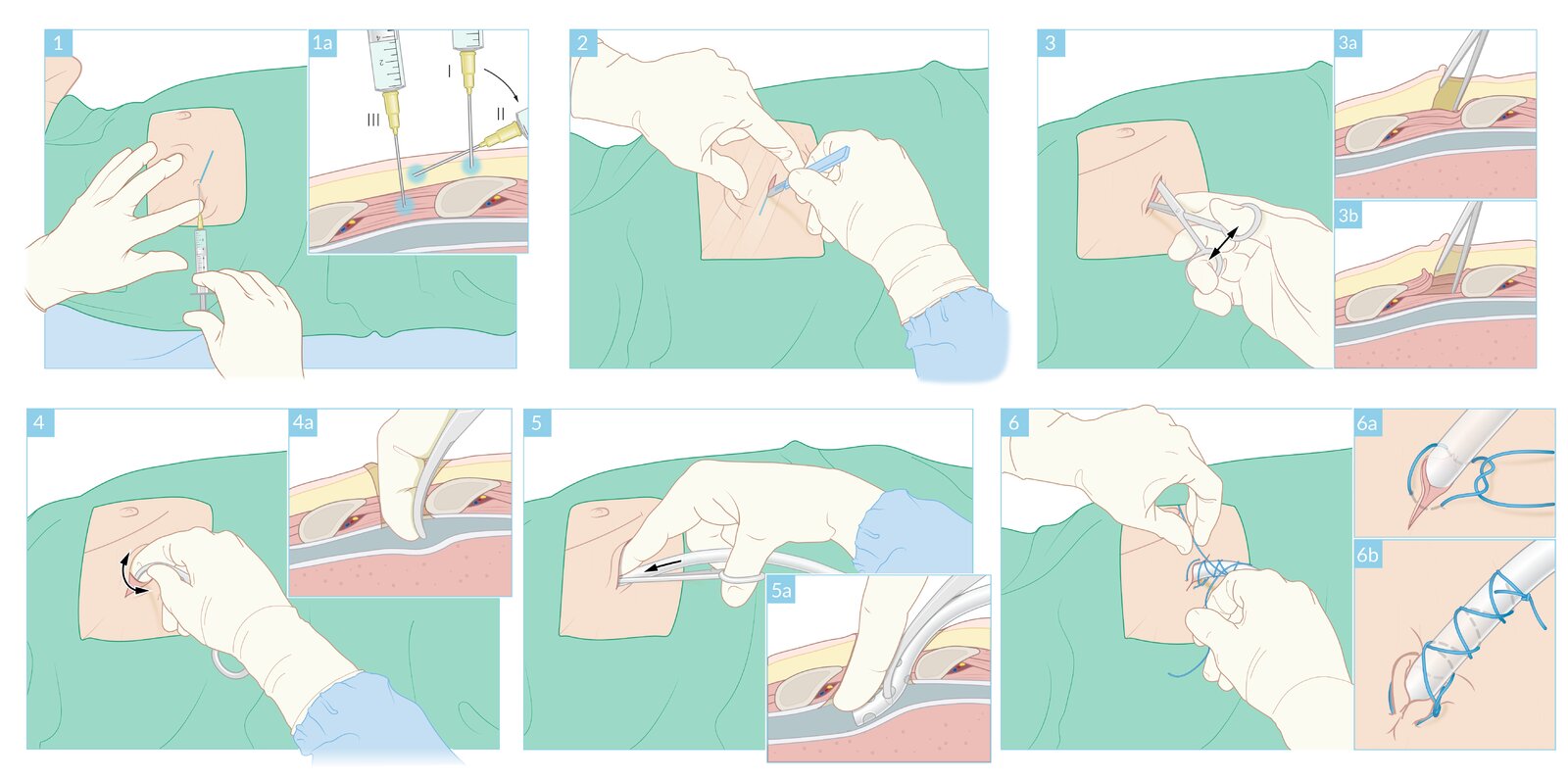
(1) The insertion site is identified.
(1a) Local anesthesia is infiltrated around the insertion site (I) and along the anticipated chest tube tract (II → III).
(2) A 3–5 cm transverse incision is made through the skin and subcutaneous tissue.
(3) The subcutaneous tissue is bluntly dissected through the intercostal muscle (3a) to the pleura along the superior border of the rib (3b).
(4) The pleura is penetrated using the closed tip of the Kelly clamp. The tip of the clamp is then opened to widen the pleural opening.
(4a) A finger is inserted into the pleural space to maintain the dissection tract before the Kelly clamp is removed.
(5) The distal end of the tube (not shown) is clamped and guided into the pleural space along the inserted finger.
(5a) The tube is directed posteriorly, medially, and superiorly until all side holes of the tube are within the pleural space. The tube is connected to a drainage system before the distal clamp is released.
(6) The tube is secured to the chest with sutures and an occlusive dressing is applied. In this example, the same suture is used for wound closure (6a) and tube fixation (6b).
© AMBOSS. See related article for detailed procedural guidance.
Chest wall injury
Rib fracture [1][12]
Etiology
- Blunt thoracic trauma (e.g., MVC, fall from height)
- Nonaccidental trauma
- Pathological fractures
Clinical features
- Pleuritic chest pain
- Respiratory distress (e.g., tachypnea, dyspnea)
- Chest wall tenderness, bruising, and/or deformity
- Crepitus
-
Flail chest
- Caused by three or more adjacent ribs fractured in two or more places
- Paradoxical chest movement: The floating rib segment moves inward during inspiration and outward during expiration.

Diagnostics [2][8][13]
- Clinical diagnosis based on physical examination findings
- Minor trauma: CXR (AP and lateral view) [14]
- Major trauma: chest CT with or without IV contrast


Treatment [2][15]
-
Isolated rib fractures: typically managed nonsurgically
- Provide pain management (e.g., acetaminophen, NSAIDs, lidocaine patches).
- Encourage deep breathing exercises (e.g., incentive spirometry).
-
Multiple rib fractures and/or flail chest
- Intubate and begin positive pressure ventilation (PPV) in patients with signs of acute respiratory distress (see “Airway management”). [16]
- Manage pneumothorax and/or hemothorax with chest tube placement.
- Provide pain management (e.g., patient-controlled analgesia, intercostal nerve block).
- Encourage deep breathing exercises (e.g., incentive spirometry).
- Flail chest: Consult thoracic surgery for surgical management.
In patients with flail chest and respiratory distress, positive pressure ventilation improves gas exchange and may provide internal stabilization while patients await surgery.
Disposition [15][17]
- Patients with ≤ 2 rib fractures with adequate pain control: may be discharged
- Patients with ≥ 3 rib fractures and/or poorly controlled pain: Admit for pain management and monitoring.
- Patients at risk for respiratory decompensation (e.g., aged > 65 years, respiratory comorbidities) with ≥ 3 rib fractures: Consider ICU admission.
Complications
- Respiratory failure
- Pneumothorax
- Hemothorax
- Atelectasis
- Pneumonia
- Pulmonary contusion
- Intraabdominal organ injury
- Nonunion



Other chest wall injuries
- Sternal fracture
- Clavicle fracture
- Vertebral fractures
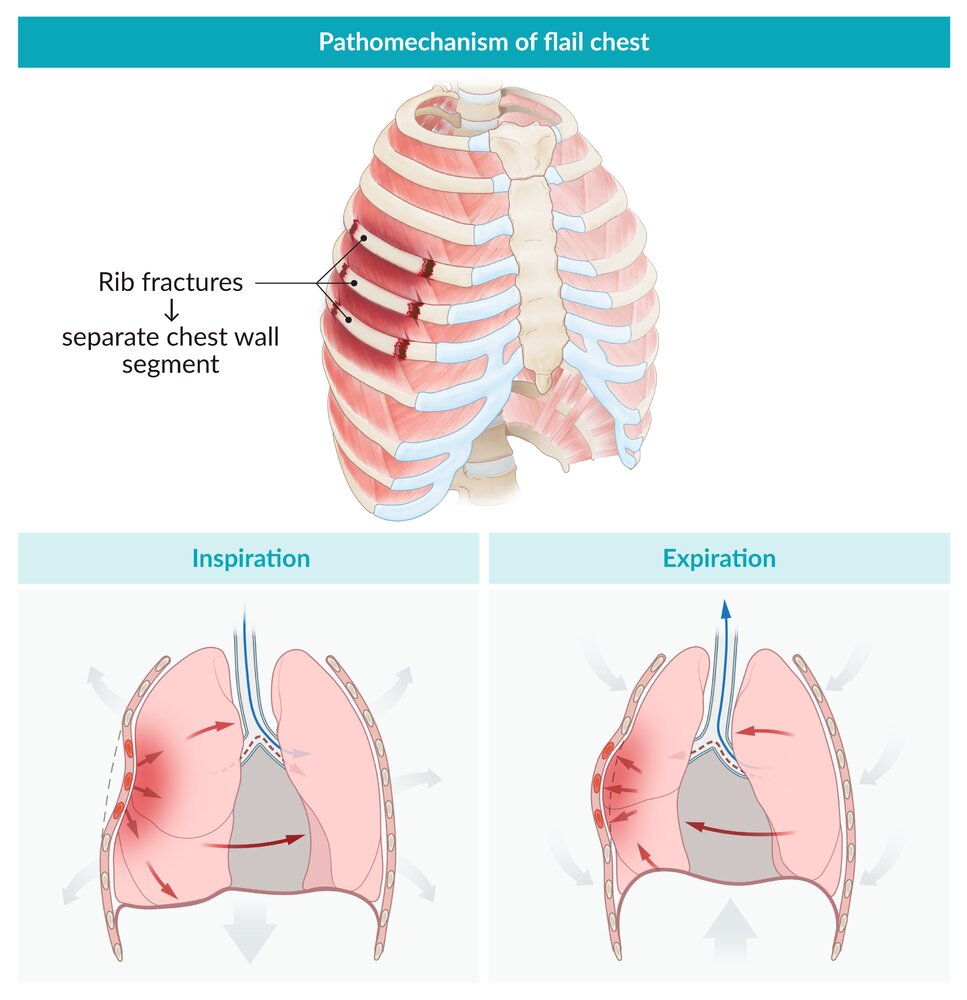
Paradoxical movement of a separate chest wall segment that moves inward during inspiration and outward during expiration. Caused by detachment of a segment of the rib cage from the chest wall due to fracture of three or more adjacent ribs in at least two places.
© AMBOSS
X-ray chest (PA view) of a patient with polytrauma from a motor vehicle collision
A displaced fracture (green overlay) of the mid-shaft of the right clavicle is accompanied by fractures of the third and fourth ribs (red overlay). Subtle buckling of the cortex of the first rib also suggests a fracture (arrowheads). A first rib fracture is a marker of severity in polytrauma, frequently associated with severe organ injury.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
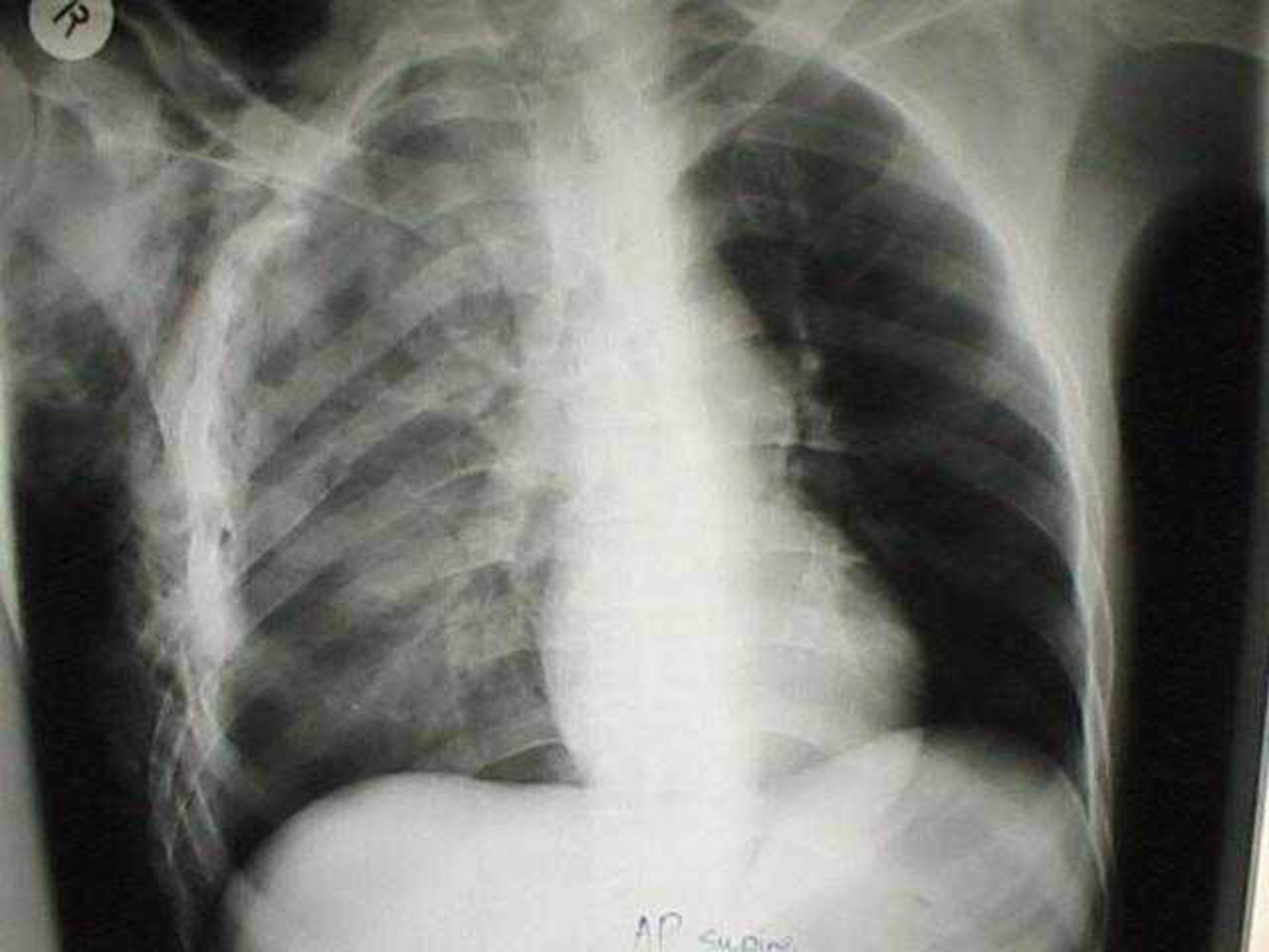
X-ray chest (AP view; supine) of patient with a history of trauma
Multiple right rib fractures (red lines) are present, some of which show marked displacement. There is extensive subcutaneous emphysema (examples indicated by arrowheads). The right lung is diffusely opaque (green overlay), likely reflective of pulmonary contusion in view of the trauma history.
White overlay: ribs
Source: “Pulmonary contusion” by Karim, Wikimedia Foundation, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

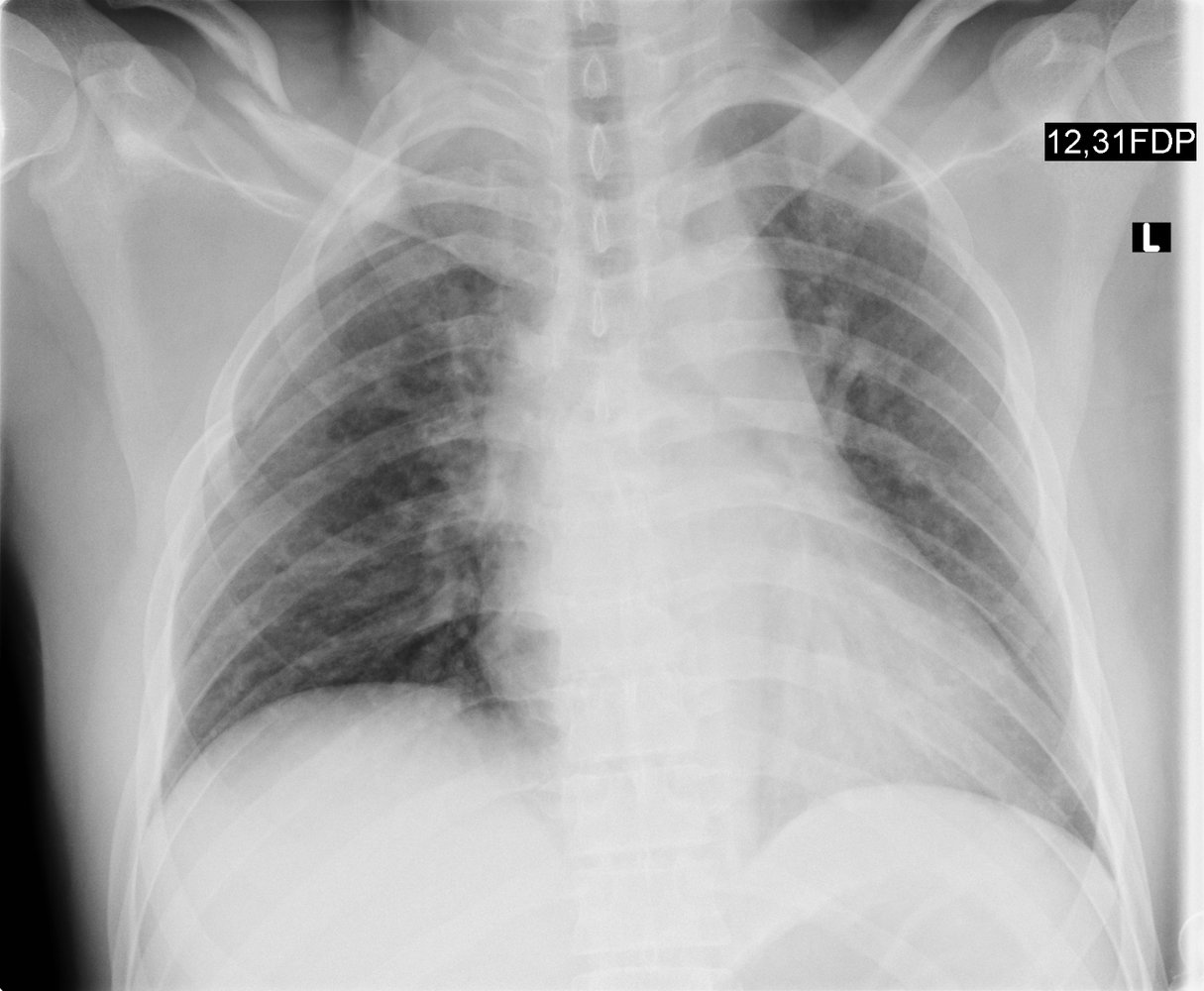
X-ray chest (PA view) of a patient with left chest trauma
Acute fractures of the posterior left 3rd through 7th ribs are accompanied by tension pneumothorax, with depression of the left hemidiaphragm (indicated by white arrow) and a rightward shift of the mediastinum (indicated by red arrow). The left lung is partially collapsed (green overlay). Pneumomediastinum, or mediastinal emphysema, is visible as vertically oriented linear lucencies in the mediastinum (examples indicated by yellow overlay). Subcutaneous emphysema in the neck and left chest wall is the result of the dissection of mediastinal air into the soft tissues (examples indicated by blue overlay). Air outlining fibers of the pectoralis muscle produces the ginkgo-leaf sign (indicated by red overlay).
Healed fractures of the right 6th, 7th, and 9th ribs are also visible, and an ECG electrode projects over the anterior aspect of the right 2nd rib.
Source: “Tpneumopneumomed” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

CT chest (with contrast; axial plane; lung window)
A displaced right rib fracture (dashed outline) is accompanied by pneumothorax (green overlay) and subcutaneous emphysema (blue overlay).
Posterior peripheral atelectasis (red overlay) is seen in both lower lobes, right greater than left.
Source: “Fig 1B, In: Occult Pneumothorax in Blunt Thoracic Trauma: Clinical Characteristics and Results of Delayed Tube Thoracostomy in a Level 1 Trauma Center” by Kim CW, Park IH, Youn Yj, Byun CS, MDPI, licensed under CC BY 4.0. Modifications: image cropped, removal of the letter B and the red arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
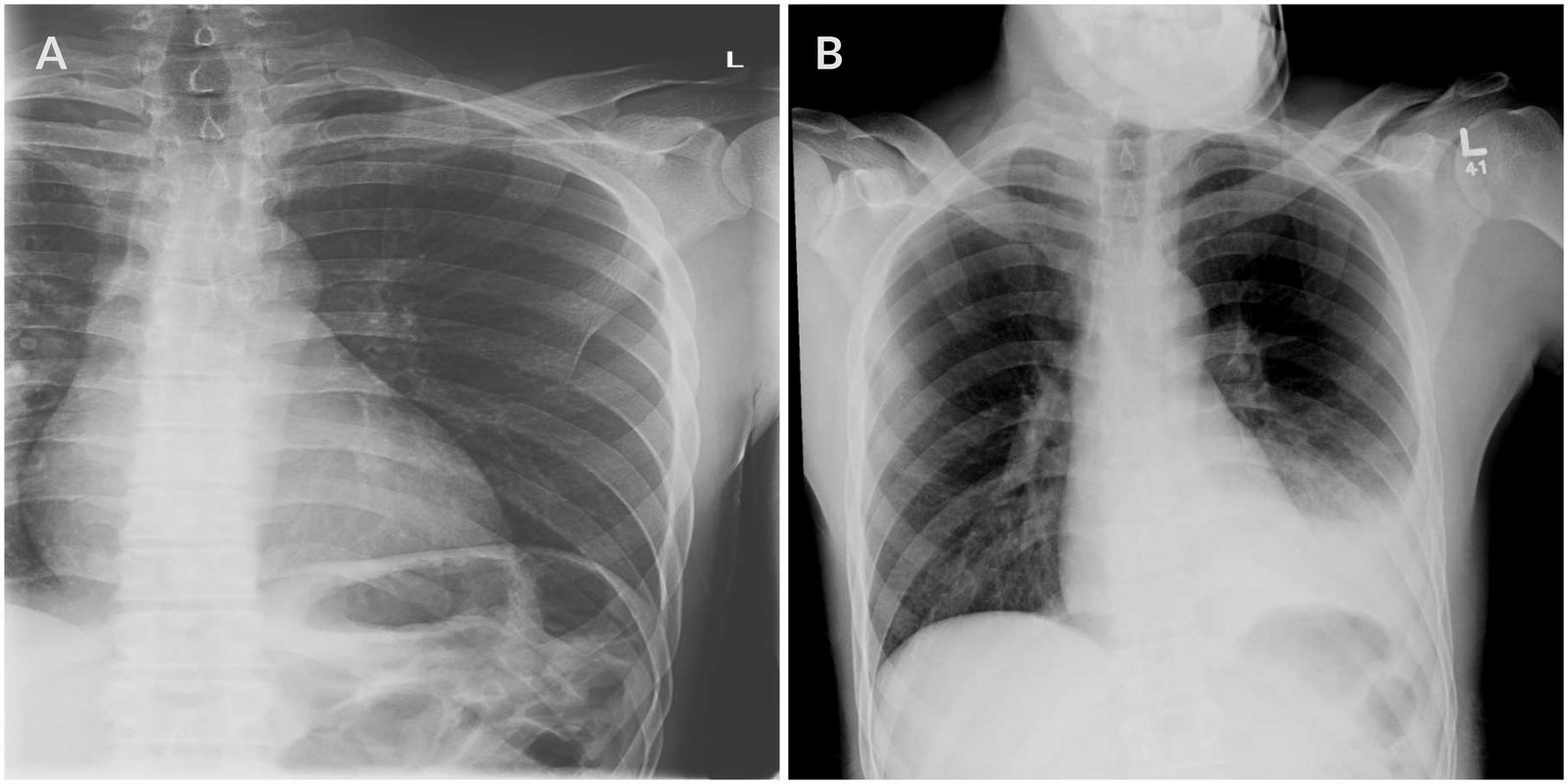
X-ray chest (A: AP view, initial presentation; B: PA view, 10 days later) of a patient with a history of fall and left-sided chest pain followed by dyspnea and orthopnea
The initial radiograph (A) shows a displaced fracture of the anterior left seventh rib (indicated by arrows).
The follow-up radiograph (B) shows obscuration of the margins of the descending thoracic aorta (dashed line) and left hemidiaphragm by extensive air space disease (green overlay) and pleural effusion; a meniscus (red line) helps confirm the presence of the effusion. In view of the trauma history, the likely causes are pulmonary contusion and hemothorax. The slightly high position of the gastric bubble (GB) also suggests the presence of left lower lobe atelectasis. The right lung and cardiac silhouette are normal.
Green circle: fracture
Source: “Fig 1 & 2, In: Massive Hemothorax Caused by a Single Intercostal Artery Bleed Ten Days after Solitary Minimally Displaced Rib Fracture” by Curfman KR, Robitsek RJ, Salzler GG et al., Hindawi, licensed under CC BY 3.0. Modifications: - merging Figure 1 and 2 into one image (consisting then of A & B) - removed arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Cardiovascular injury
Blunt cardiac injury (BCI) [1][18][19]
Cardiac injuries from blunt trauma most commonly occur after high-speed MVC and range from minor asymptomatic injury to myocardial rupture and death. [2]
Possible injuries
- Cardiac contusion: a cardiac injury secondary to blunt force thoracic trauma, which causes myocardial dysfunction with a wide range of clinical effects, including chest pain, hypotension, arrhythmias, elevated cardiac biomarkers, and cardiogenic shock
- Atrial and ventricular wall injuries
- Septal and valvular injuries
- Acute coronary syndrome, myocardial infarction
- Pericardial effusion and cardiac tamponade
- Myocardial rupture
Clinical features
- Asymptomatic
- Chest ecchymosis
- Chest pain or tenderness
- Hypotension
- Tachypnea, shortness of breath
- Tachycardia, arrhythmias
- New cardiac murmur, muffled heart sounds
- Jugular venous distention
- Dizziness, syncope
- Cardiogenic shock
- Sudden cardiac arrest
Consider BCI if tachycardia persists despite fluid resuscitation and hemorrhage has been ruled out.
Diagnostics [18][19]
See “Approach to blunt chest trauma” for initial measures.
-
ECG
- Obtain in all patients with suspected BCI.
- Potential findings include:
- Arrhythmia (e.g., sinus tachycardia, dysrhythmia)
- ST-segment abnormalities
- ECG changes in STEMI
- AV block
-
Troponin
- Obtain in all patients with suspected BCI.
- May be elevated in patients with coronary or myocardial injury
-
Echocardiography [20]
- Obtain in patients with hemodynamic instability, abnormal ECG, or elevated troponin.
- TEE may be performed if TTE is inconclusive.
- Potential findings include:
- Pericardial effusion
- Cardiac tamponade
- Myocardial rupture
- Wall motion abnormality
- Valvular injuries
- Septal injuries
-
Additional diagnostics [20]
- General imaging in trauma: e.g., eFAST, CXR, chest CT with or without IV contrast
- CT angiography: for suspected vascular injury
Management
- Initiate immediate hemodynamic support and continuous cardiac monitoring.
- Start treatment of underlying pathology (e.g., management of cardiac tamponade, management of cardiogenic shock).
- Patients with abnormal ECG or troponin levels: Monitor for delayed cardiac injuries (e.g., myocardial rupture).
- Patients with normal ECG and troponin levels: Consider discharge if there are no other injuries.
Commotio cordis [21][22]
- Definition: ventricular fibrillation and sudden cardiac death caused by a relatively mild nonpenetrating blunt force trauma to the precordial area
- Etiology: blow to the precordial area at a perpendicular angle, most commonly by a hard, spherical object (e.g., baseball, golf ball), during a brief electrically vulnerable period of T-wave upstroke
- Pathophysiology: blunt trauma leads to myocardial stretch → activation of ion channels because of mechano-electric coupling → augmentation of repolarization and premature ventricular depolarization → ventricular fibrillation [23]
-
Diagnosis is clinical and based on the following criteria:
- Blunt trauma to the chest followed by collapse
- Absence of structural myocardial injury (on imaging studies and/or autopsy)
- ECG showing ventricular fibrillation (if obtained)
-
Management
- Immediate: cardiopulmonary resuscitation
- Long-term: cardiac workup (ECG, echocardiogram, cardiac MRI, stress testing)
-
Prevention
- Avoidance of sports that involve chest wall impact (e.g., baseball, hockey, football)
- Use of chest protectors and/or safety balls may reduce risk.
- Treat any underlying cardiac disease.
- No underlying cardiac disease: no ICD necessary
Blunt thoracic aortic injury [24][25][26]
- Definition: an injury of the thoracic aorta resulting from blunt trauma; most commonly occurs distal to the left subclavian artery in the aortic isthmus
- Etiology: rapid deceleration from blunt trauma (e.g., MVC, fall from height)
-
Clinical features: Severity ranges from intimal lesions (e.g., aortic pseudocoarctation) to thoracic aortic rupture.
- Chest pain
- Upper back pain
- Dyspnea, hoarseness and/or stridor
- Dysphagia
- Chest wall instability and/or ecchymoses
- New interscapular murmur
- Thoracic aortic rupture: signs of hemorrhagic shock (e.g., tachycardia, hypotension) and tearing pain
-
Imaging [1]
-
CXR (initial imaging); potential findings include:
- Left main bronchus depression
- Tracheal deviation
- Apical pleural cap
- Left pleural effusion (hemothorax)
- Obscuration of the aortic knob
- Mediastinal widening
- Definitive imaging: based on the patient's hemodynamic status and trauma surgeon preference [1]
- CTA chest in hemodynamically stable patients
- Transesophageal echocardiography
-
CXR (initial imaging); potential findings include:
-
Management [26]
-
Initiate blood pressure and heart rate control.
- Goal: heart rate ≤ 100 bpm and systolic blood pressure ≤ 100 mm Hg
- Treatment: beta blockers (e.g., esmolol, labetalol) and vasodilator therapy (e.g., nitroprusside, nicardipine) if needed
- Definitive management
- Endovascular repair (TEVAR)
- Open surgical repair
-
Initiate blood pressure and heart rate control.
- Prognosis: very poor (∼ 80% of patients die before reaching the hospital) [26]

X-ray chest (AP view) of a patient with a recent history of a motor vehicle crash
A lobulated convexity projects along the left superior mediastinum (green overlay and arrows) in the region of the aortic knob.
The differential for the mediastinal widening includes a range of mediastinal soft tissue masses; however, traumatic mediastinal injury (particularly involving the thoracic aorta) is the primary concern in view of the trauma setting. CT angiography is the appropriate next imaging study in a hemodynamically stable patient.
Green dashed line: normal margin of the aorta
Source: © IMPP
Pulmonary injury
Pulmonary contusion [1][2][16]
- Definition: a lung injury from blunt trauma resulting in alveolar edema and hemorrhage
-
Clinical features
- Clinical features of respiratory distress (e.g., dyspnea; , tachypnea, cyanosis)
- Hypoxia
- Tachycardia
- Chest pain
- Chest ecchymosis
-
Diagnostics
-
CXR ; [2]
- Patchy alveolar infiltrates
- White-out hemithorax or diffuse opacity
- Chest CT: if CXR is inconclusive
-
CXR ; [2]
-
Management
- Provide pain management.
- Provide respiratory support (e.g., oxygen, positive pressure ventilation).
- Maintain euvolemia and avoid excessive IVF resuscitation.
- Monitor for respiratory insufficiency, e.g., with repeated ABGs.
-
Complications
- ARDS
- Pneumonia

Tracheobronchial injury [1][2]
- Definition: a tear in the tracheobronchial tree resulting from high-energy impact, decelerating forces, or a penetrating chest wall injury
-
Clinical features
- Dyspnea
- Sternal tenderness
- Subcutaneous emphysema
- Clinical features of pneumothorax
- Hamman sign
- Hoarseness
- Hemoptysis
-
Diagnostics
- CXR; : subcutaneous emphysema, pneumomediastinum, pneumothorax
- Chest CT: subcutaneous emphysema, pneumomediastinum, pneumothorax, bronchial tear, tracheal tear
- Bronchoscopy: visualization of the lesion [2]
-
Initial management [2][27]
- Prepare for difficult airway management.
- Intubate using a fiberoptic laryngoscope or bronchoscope.
- Place chest tube for concomitant pneumothorax.
- For injuries of the proximal trachea, see also “Approach to blunt neck trauma.”
- Definitive treatment: surgical repair
-
Complications [2]
- Pneumothorax with persistent air leak
- Airway obstruction
- Bronchopleural fistula
- Mediastinitis
Suspect tension pneumothorax in patients with tracheobronchial injury and midline shift or distended neck veins.


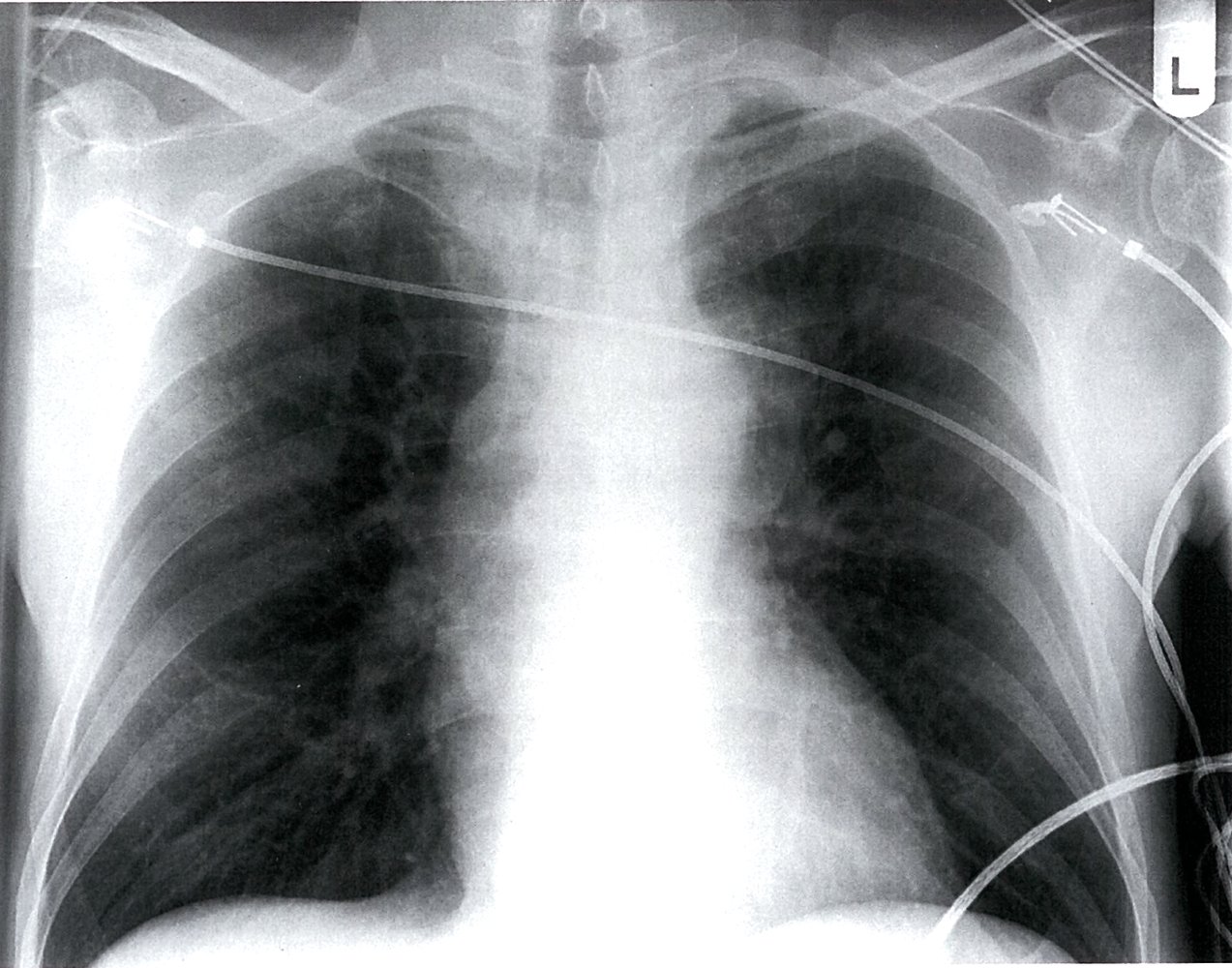
X-ray chest (AP view; supine) of patient with a history of trauma
Multiple right rib fractures (red lines) are present, some of which show marked displacement. There is extensive subcutaneous emphysema (examples indicated by arrowheads). The right lung is diffusely opaque (green overlay), likely reflective of pulmonary contusion in view of the trauma history.
White overlay: ribs
Source: “Pulmonary contusion” by Karim, Wikimedia Foundation, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
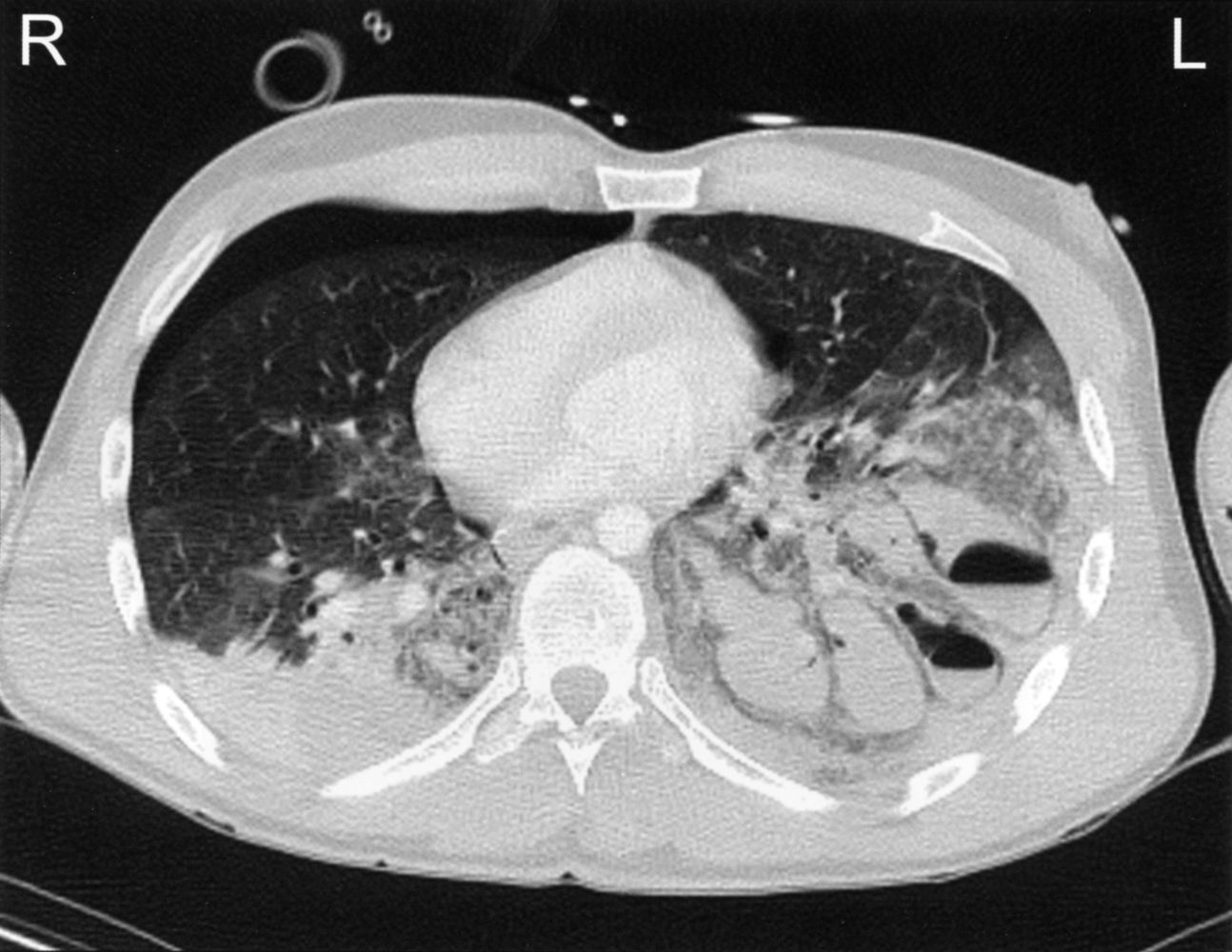
CT chest (axial plane; lung window) following trauma to the chest
Areas of ground glass and consolidation in both lungs are the result of pulmonary contusion (green overlay). Ovoid traumatic lacerations in the left lung contain opaque blood (red overlay). Two of the lacerations also contain air, producing air-fluid levels (dashed line). A pneumothorax is present anteriorly in the right hemithorax (blue overlay).
Source: © IMPP
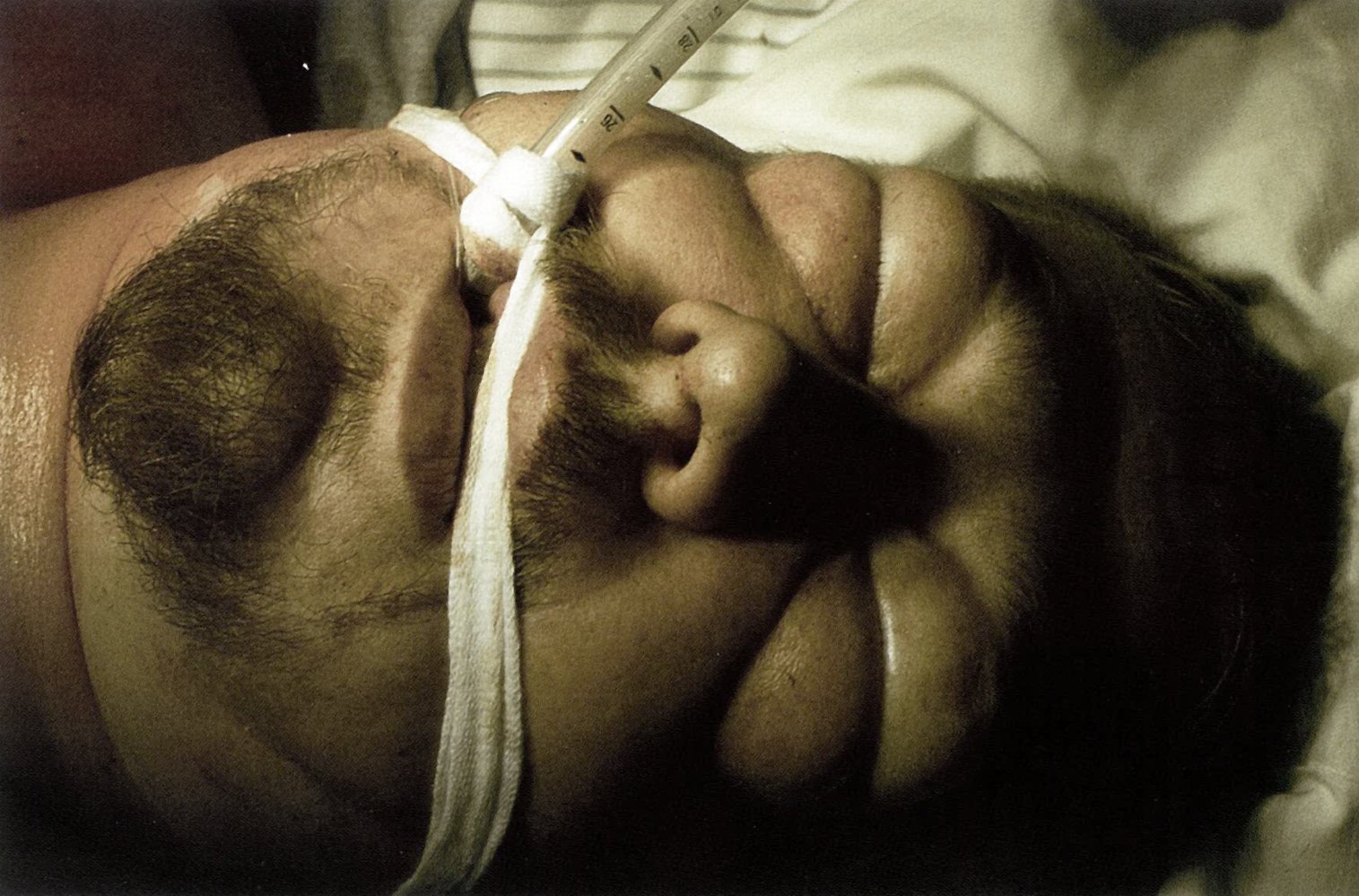
Subcutaneous emphysema of neck and face (especially the eyelids) can be seen in this patient following a traumatic bronchial rupture.
Source: © IMPP

X-ray chest (PA view)
Extensive subcutaneous emphysema is seen as linear lucencies throughout the soft tissues of the thorax, neck, and upper abdomen (examples indicated by green overlay). A small residual right pneumothorax (arrowheads) is visible and pneumomediastinum is seen along the trachea, main bronchi, and cardiac silhouette (red overlay and arrows). A chest tube (yellow overlay) is in place, with its tip in the apex of the right hemithorax.
Pneumomediastinum and pneumothorax can result from blunt or penetrating thoracic injury and various other conditions (e.g., lung disease, intestinal perforation, medical procedure). Air that escapes from the lungs, airways, or bowel can track into the mediastinal and subcutaneous soft tissues.
Source: “Fig 1, In: Massive subcutaneous emphysema after traumatic pneumothorax” by Rosat A, Gómez P, Panafrican Medical Journal, licensed under CC BY 4.0. Modifications: removal of the arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Blunt abdominopelvic trauma
Approach to blunt abdominal trauma [1][2]
Ensure the following components are included as part of the standard management of trauma patients using the ATLS algorithm:
-
All patients
- Assess for indications for trauma team activation (e.g., high-speed MVCs, ejection from vehicle, death of a passenger) and initiate transfer to a trauma center, if necessary.
- Examine abdomen, flank, back, and groin for bruising and signs of peritonitis.
- Consider portable CXR and pelvic x-ray.
- Stabilize pelvic fractures with a pelvic binder.
- Begin initial management of vertebral injuries, if suspected.
-
Hemodynamically unstable patients
- Perform FAST to quickly identify intraabdominal bleeding.
- Treat hemorrhagic shock with emergency transfusion and immediate hemodynamic support.
- Identify obvious indications for exploratory laparotomy, e.g., hypotension with a positive FAST, peritoneal signs, subdiaphragmatic air on CXR.
- Associated pelvic fracture: Coordinate interventions for pelvic hemorrhage control (e.g., angioembolization) concurrently with emergency laparotomy (see “Initial management of pelvic fractures” for details).
-
Hemodynamically stable patients
- Obtain urgent diagnostics for trauma patients as indicated, e.g., CT abdomen and pelvis with contrast.
- Identify other radiological indications for exploratory laparotomy (e.g., significant hemoperitoneum or gastrointestinal perforation).
- If there are no indications for surgery, initiate nonsurgical management with serial examinations and close monitoring of vital signs.
If there are obvious indications for immediate exploratory laparotomy (e.g., hypotension and peritoneal signs), do not delay transfer to the OR for diagnostic studies. [1][2]
Clinical features [1]
General features
- Hemorrhagic shock (e.g., hypotension, tachycardia)
- Signs of peritonitis (e.g., abdominal pain, abdominal distention, abdominal guarding)
- Decreased bowel sounds
- Abdominal bruising (e.g., seat belt sign )
The absence of abdominal pain or tenderness does not exclude intraabdominal injuries. [2]

Specific injuries
-
Splenic injury
- Left-sided abdominal pain
- Referred pain in the left shoulder (Kehr sign)
-
Liver injury
- Right-sided abdominal pain
- Referred pain in the right shoulder
-
Duodenal injury
- Nausea and vomiting
- Bilious vomiting in case of gastrointestinal obstruction
- Epigastric pain
-
Retroperitoneal injury
- Back and/or flank pain or tenderness
- Periumbilical ecchymosis (Cullen sign)
- Flank ecchymosis (Grey Turner sign)
- Renal injury: hematuria
- Pancreatic injury: upper abdominal pain, clinical features of acute pancreatitis [28]
-
Diaphragmatic injury
- Decreased breath sounds
- Bowel sounds in the thorax
- Respiratory distress
-
Vertebral injury (e.g., Chance fracture)
- Lower back pain
- Clinical features of spinal cord injury
Extensive duodenal hematoma can obstruct gastroduodenal passage and manifest with bilious vomiting.
Symptom onset in pancreatic injury may be delayed.
Suspect herniation of abdominal organs into the chest if there are bowel sounds in the thorax after abdominal or thoracic trauma.


Diagnostics [1][8][29]
See “Urgent diagnostics for trauma patients” for a comprehensive approach.
-
General imaging in trauma: CXR and pelvic x-ray
- Performed for most patients after major trauma
- May show free intraabdominal air, evidence of diaphragmatic injury, and fractures
-
Bedside intraabdominal hemorrhage assessment: FAST, eFAST, or diagnostic peritoneal lavage (DPL)
- Indicated for all hemodynamically unstable patients with blunt abdominal trauma
- Detects hemoperitoneum (collection of blood in the peritoneal cavity)
-
CT imaging in trauma
- Minimum evaluation: CT abdomen and pelvis with IV contrast
- Suspected vascular injuries: CTA abdomen and pelvis
- Suspected T-spine or L-spine injuries: See “Diagnosis of vertebral injuries.”
- Potential findings
- Hemoperitoneum
- Pneumoperitoneum
- Splenic laceration
- Liver hematoma
- Duodenal hematoma
- Pelvic fracture
- Minimally invasive surgical assessment: diagnostic laparoscopy
Pancreatic, diaphragmatic, small bowel, and mesenteric injuries may be missed on initial CT imaging. [2]



")






Management [2]
Nonoperative management [30][31][32]
Nonoperative management should take place in a center with facilities for urgent laparotomy.
- May be considered for:
- Hemodynamically stable patients with no signs of peritonitis
- Renal, splenic, pancreatic, and hepatic injuries
- Typically includes:
- Monitoring for changes in clinical status (e.g., vital signs, pain levels, serial abdominal examination)
- Serial laboratory studies (e.g., hemoglobin)
- Repeat imaging for injury progression
- Supportive care (e.g., pain management, wound care)
Operative and interventional management [33]
Hemodynamically unstable patients typically require surgical or interventional management, which may include:
- Exploratory laparotomy: e.g., for hemodynamically unstable patients with a positive FAST and/or CT scan or signs of peritonitis
- Angiographic embolization: e.g., for patients with pelvic fracture, retroperitoneal hematoma, or liver injury
- External fixation of pelvic fractures
Injury-specific management
Management depends on the type and extent of injuries and is determined in consultation with specialists (e.g., trauma surgery, interventional radiology).
-
Splenic injury [31]
- Monitoring for delayed splenic rupture
- Laparotomy and repair or splenectomy in unstable patients
-
Liver injury [32]
- Nonoperative management with observation and supportive care
- OR arteriography and hepatic embolization
- Laparotomy and repair in unstable patients
- Gastrointestinal perforation: laparotomy; see “Treatment of gastrointestinal perforation.”
- Duodenal hematoma: bowel rest, nasogastric decompression, and total parenteral nutrition [34][35]
-
Pancreatic injury [28][36]
- Nasogastric suction and total parenteral nutrition
- OR surgical debridement, repair, and percutaneous drainage
-
Pelvic fracture [37][38]
- External or internal fixation
- Hemostatic measures: angiographic embolization, preperitoneal packing
- Vertebral injuries: See "Definitive management of vertebral injuries.”

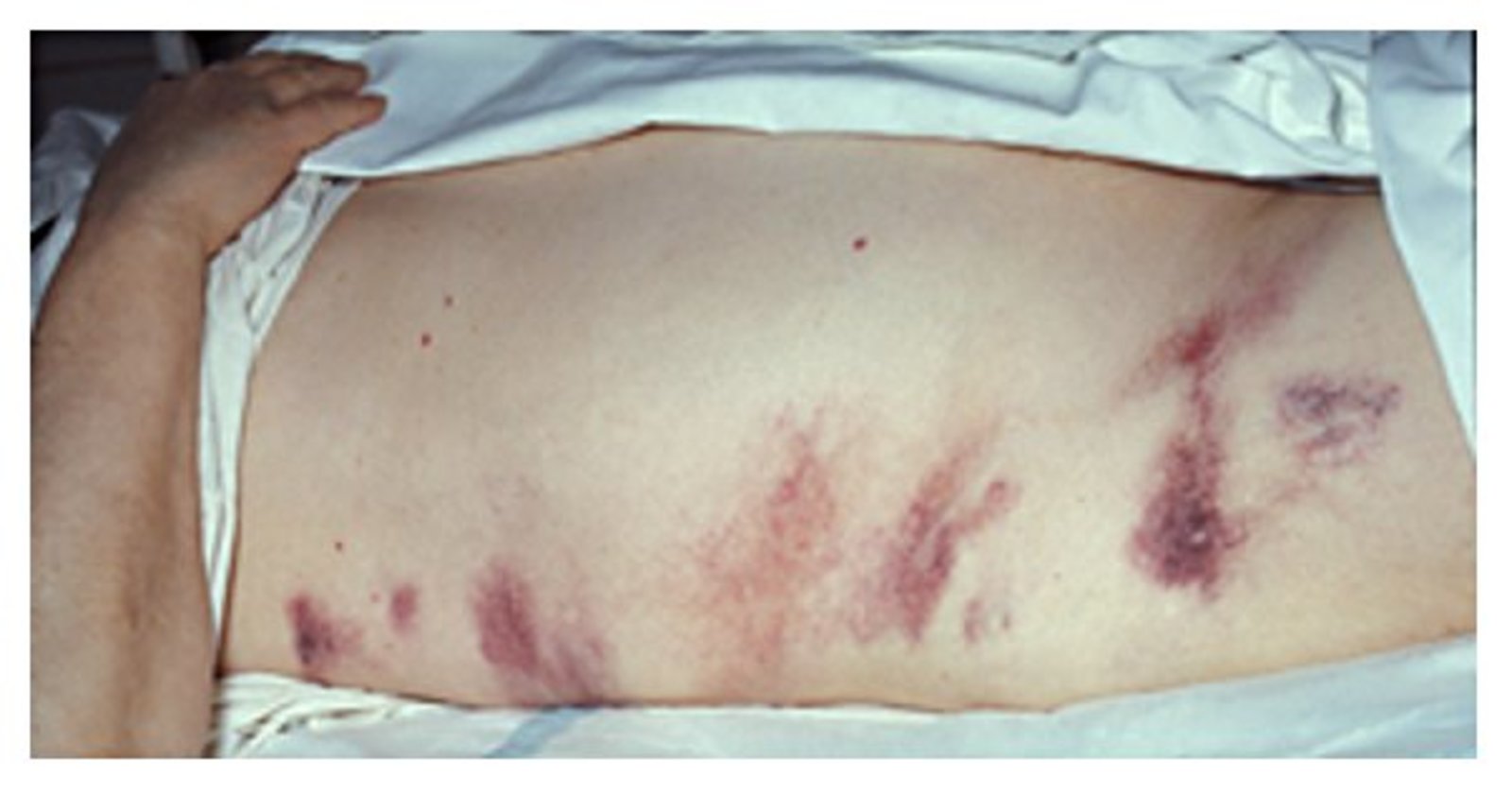
Abdomen and flank of a patient involved in a motor vehicle collision
Contusions and abrasions can be seen in the areas where the seatbelt was positioned. The presence of the seatbelt sign strongly correlates with intraabdominal and/or intraperitoneal injury. It is, however, not a sensitive sign and its absence does not rule out intraabdominal injury.
Source: “Figure 2 A, in: Seatbelts and road traffic collision injuries” by Alaa K Abbas, Ashraf F Hefny, and Fikri M Abu-Zidan, World Journal of Emergency Surgery, licensed under CC BY 2.0. Modifications: cropped image, letter removed.

Periumbilical ecchymosis as a result of retroperitoneal hemorrhage, commonly seen in acute pancreatitis.
Source: “Cullen's sign” by Herbert L. Fred, MD and Hendrik A. van Dijk, openstax, licensed under CC BY 2.0.
Right-sided flank ecchymosis suggestive of retroperitoneal hemorrhage, commonly seen in acute pancreatitis.
Source: “Images of Memorable Cases: Case 21: Hemorrhagic pancreatitis - Grey Turner's sign” by Herbert L. Fred, MD and Hendrik A. van Dijk, Wikimedia Commons, licensed under CC BY 2.0.
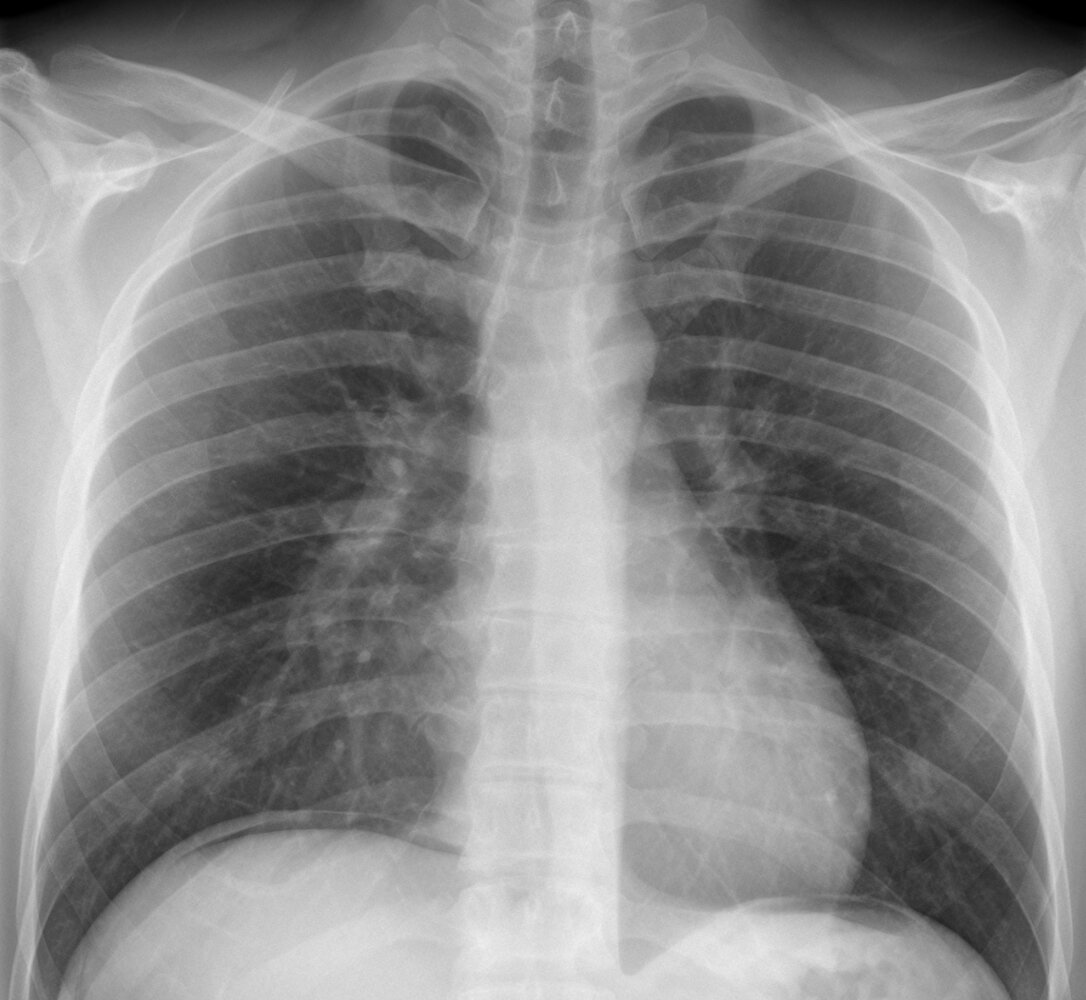
X-ray chest (PA view)
Free intraperitoneal gas (green overlay) is visible under both the right and left hemidiaphragms.
Source: “34-01-Freie Luft nach LH-OP” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
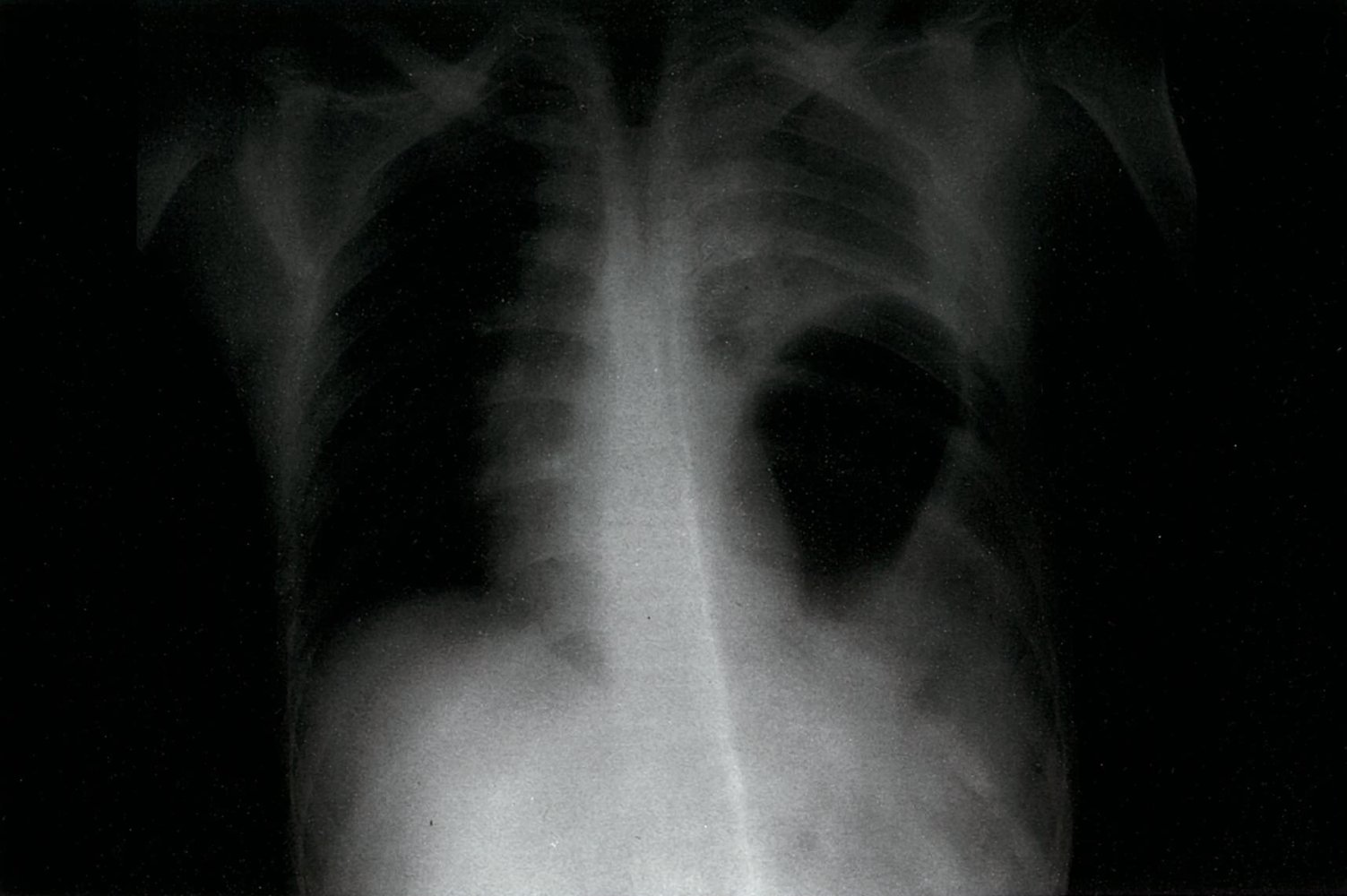
Anteroposterior chest x-ray in a 20-year-old polytrauma patient: There is marked cranial displacement of the diaphragmatic contour (white broken line) as well as the stomach (gastric bubble is indicated in green). This finding is most likely a diaphragmatic rupture with intrathoracic displacement of the abdominal organs.
Source: © IMPP

X-ray pelvis (AP view)
The right hemipelvis is displaced superiorly, compatible with disruption of the sacroiliac joint (indicated by dashed lines and double-headed arrow). Bilateral pubic ramus fractures are also present (indicated by arrowheads).
Source: “Fig 1A, In: Robot-assisted treatment of unstable pelvic fractures with a percutaneous iliac lumbar double rod fixation combined with a percutaneous pelvic anterior ring INFIX fixation” by Du W, Sun T, Ding Y et al., SpringerLink, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
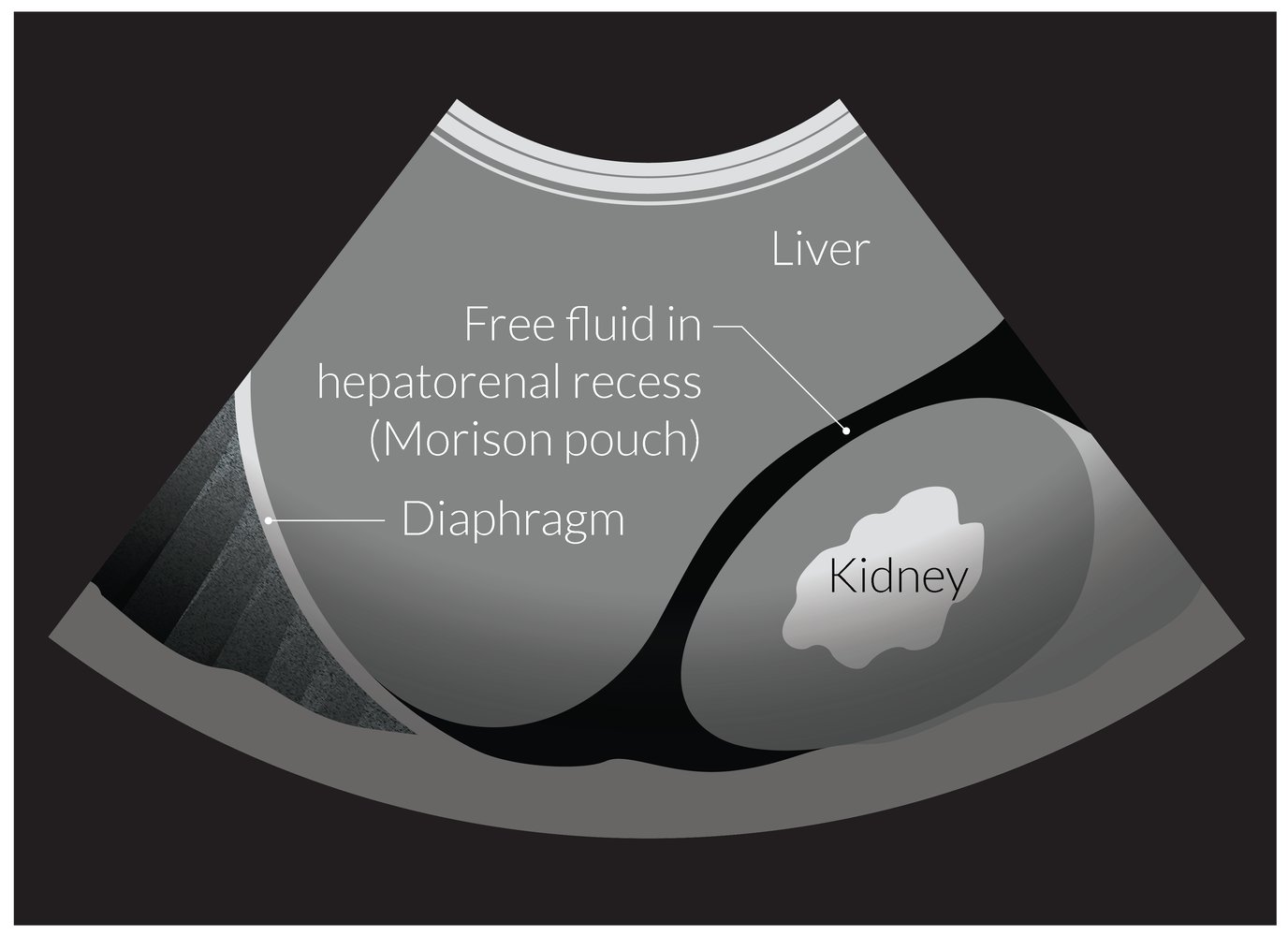
Illustration of an ultrasound showing free fluid in the hepatorenal space, which is visible as an anechoic/hypoechoic space between the liver and right kidney
Free intraperitoneal fluid (e.g., ascites, hemoperitoneum) tends to first accumulate in the hepatorenal space, as it is the lowest dependent part of the intraabdominal cavity in the supine position.
This space is evaluated as part of FAST in the workup of a patient with polytrauma or abdominal injury.
© AMBOSS

Point of care ultrasound left upper abdominal quadrant (curvilinear transducer; B-mode)
Anechoic fluid collections (arrows) are visible in the splenorenal recess.
In the setting of trauma, anechoic fluid collection in potential space is assumed to be hemorrhage until proven otherwise.
Green overlay: kidney; S: spleen
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
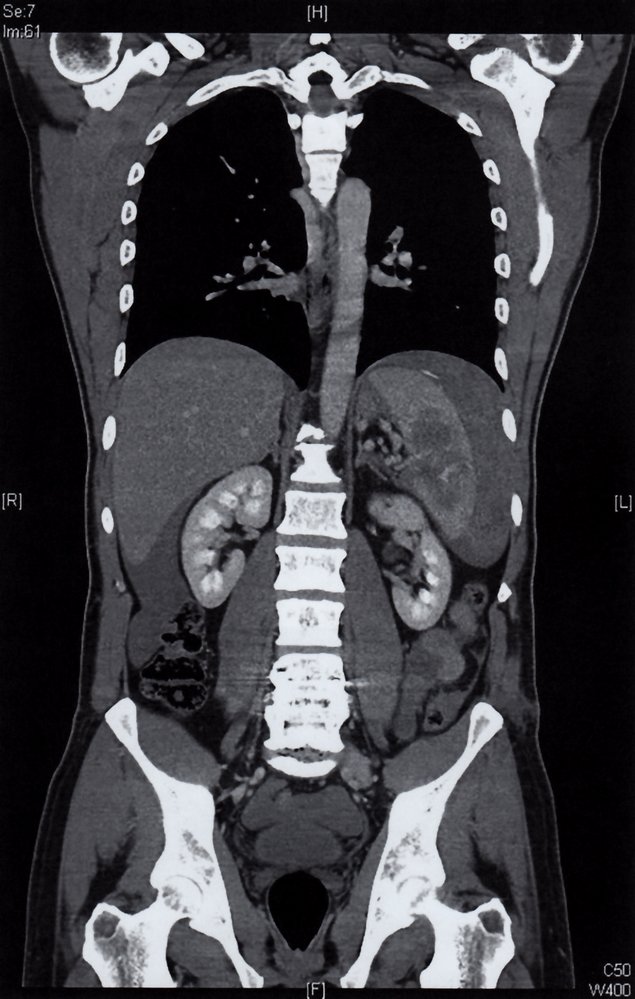
CT abdomen (with contrast; coronal plane) of a patient involved in a motorcycle crash
An irregular hypodense nonenhancing lesion within the splenic parenchyma (red overlay) is accompanied by contrast extravasation (white arrowhead), subcapsular hematoma (white dashed outline), and hemoperitoneum (green overlay).
The constellation of findings indicates a splenic laceration with hemorrhage.
Source: © IMPP

Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
CT abdomen (with contrast; axial plane; portal venous phase) of a 24 year-old patient after a high-speed front-impact crash
The spleen has an irregular contour (dashed outline) and heterogeneous enhancement. Intrasplenic low-attenuation rounded and linear areas are sites of laceration and hematoma formation. Multiple small high-density foci along the inferior aspect of the spleen indicate contrast extravasation (arrows) from active bleeding.
Hemorrhage (green overlay) into the peritoneal space extends from the spleen inferiorly along the paracolic gutter. Hemorrhagic fluid is also seen along the liver (yellow overlay) and within the right paracolic gutter and pelvis (yellow overlay).
Multiple thoracic spine fractures (examples indicated by arrowheads) are accompanied by paravertebral hematoma (red overlay).
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
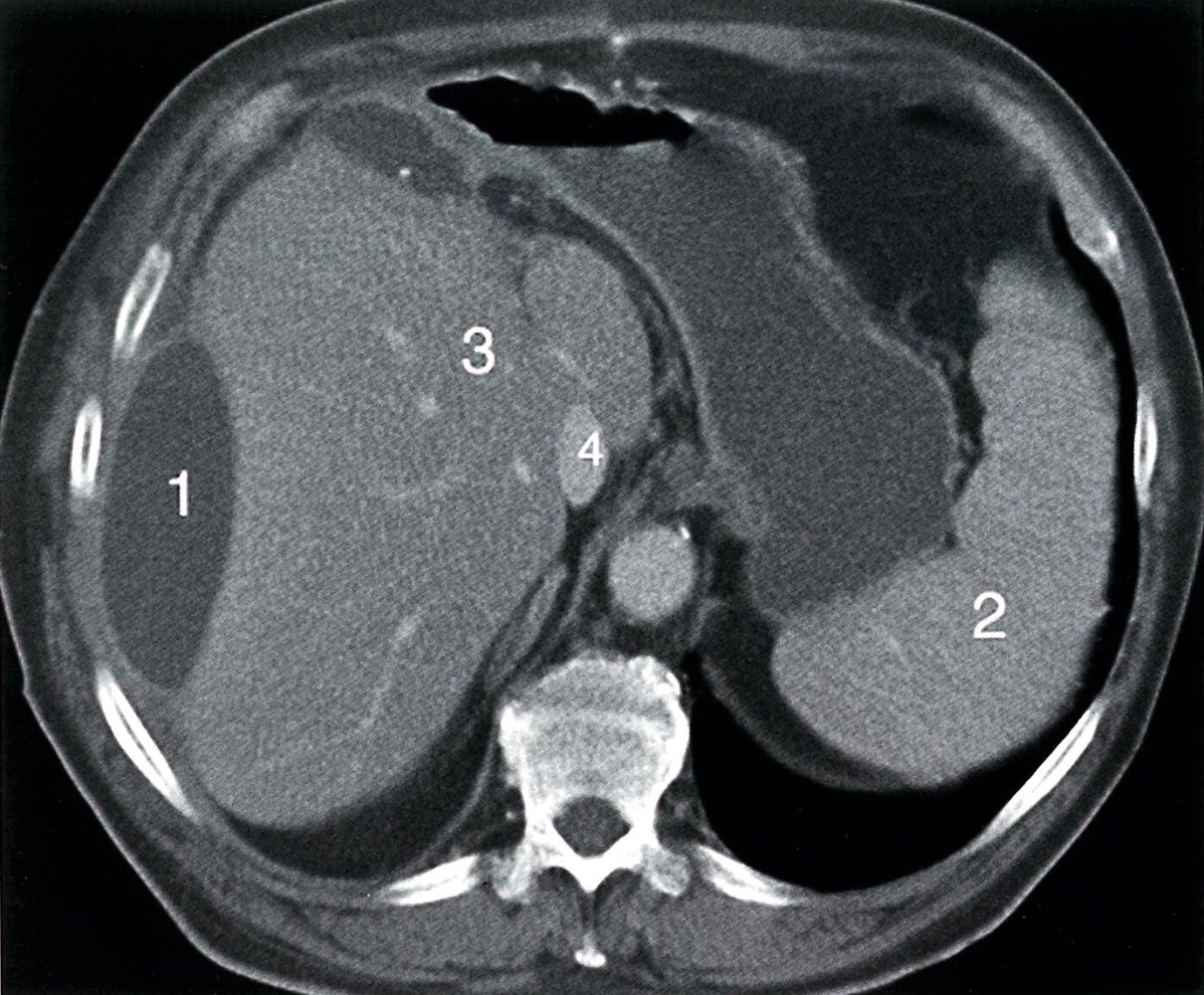
CT abdomen (with IV contrast; axial plane) of a patient involved in a motor vehicle crash
Two biconvex hypodense hematomas (1, green overlay) are seen between the hepatic capsule and parenchyma.
2: spleen; 3: liver; 4: IVC (inferior vena cava)
Source: © IMPP
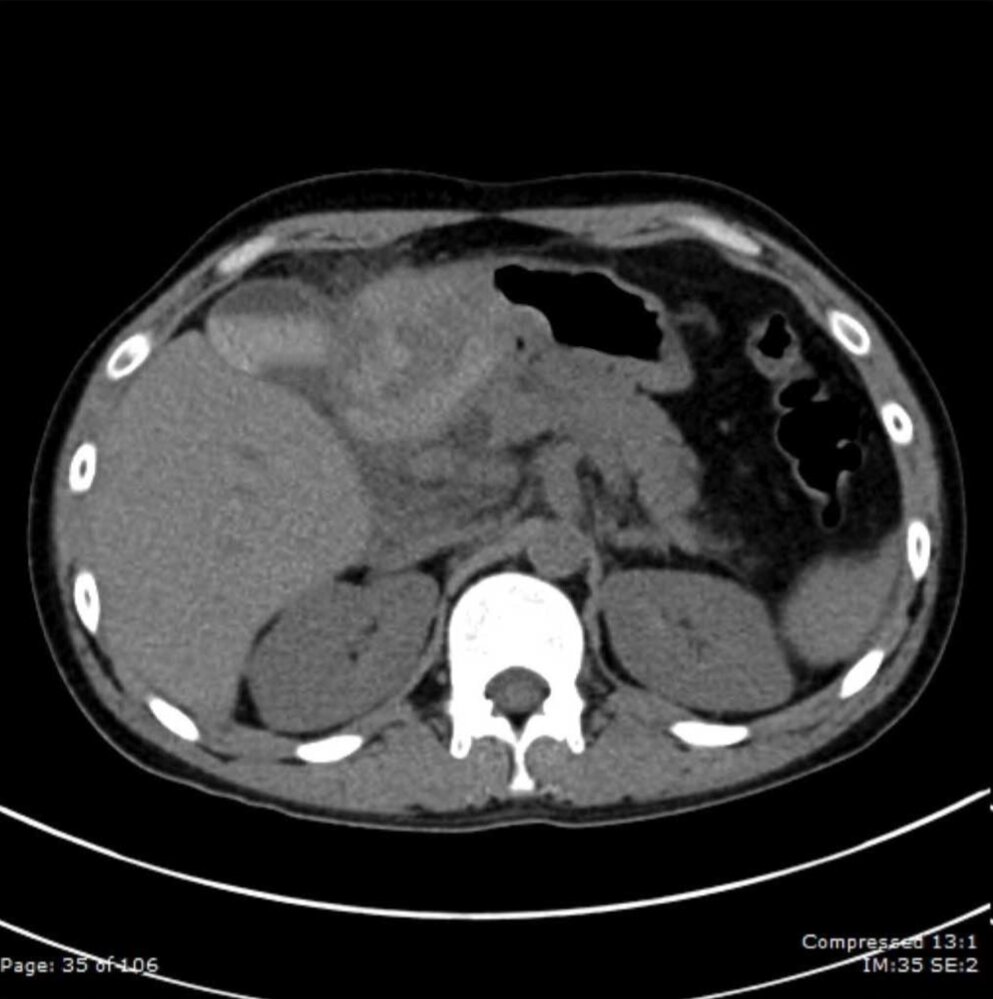
CT abdomen (without contrast; axial plane) of a patient with a duodenal hematoma
A heterogeneous mass with high attenuation areas representing hemorrhage (green overlay) is present in the right upper quadrant in the region of the proximal duodenum.
G = gall bladder, P = pancreas
Source: “Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper Intestinal Obstruction; Figure 1a” by Chalerm Eurboonyanun, Case Reports in Surgery, licensed under CC BY 4.0. Modifications: Cropped image, removed calcifications from gallbladder. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
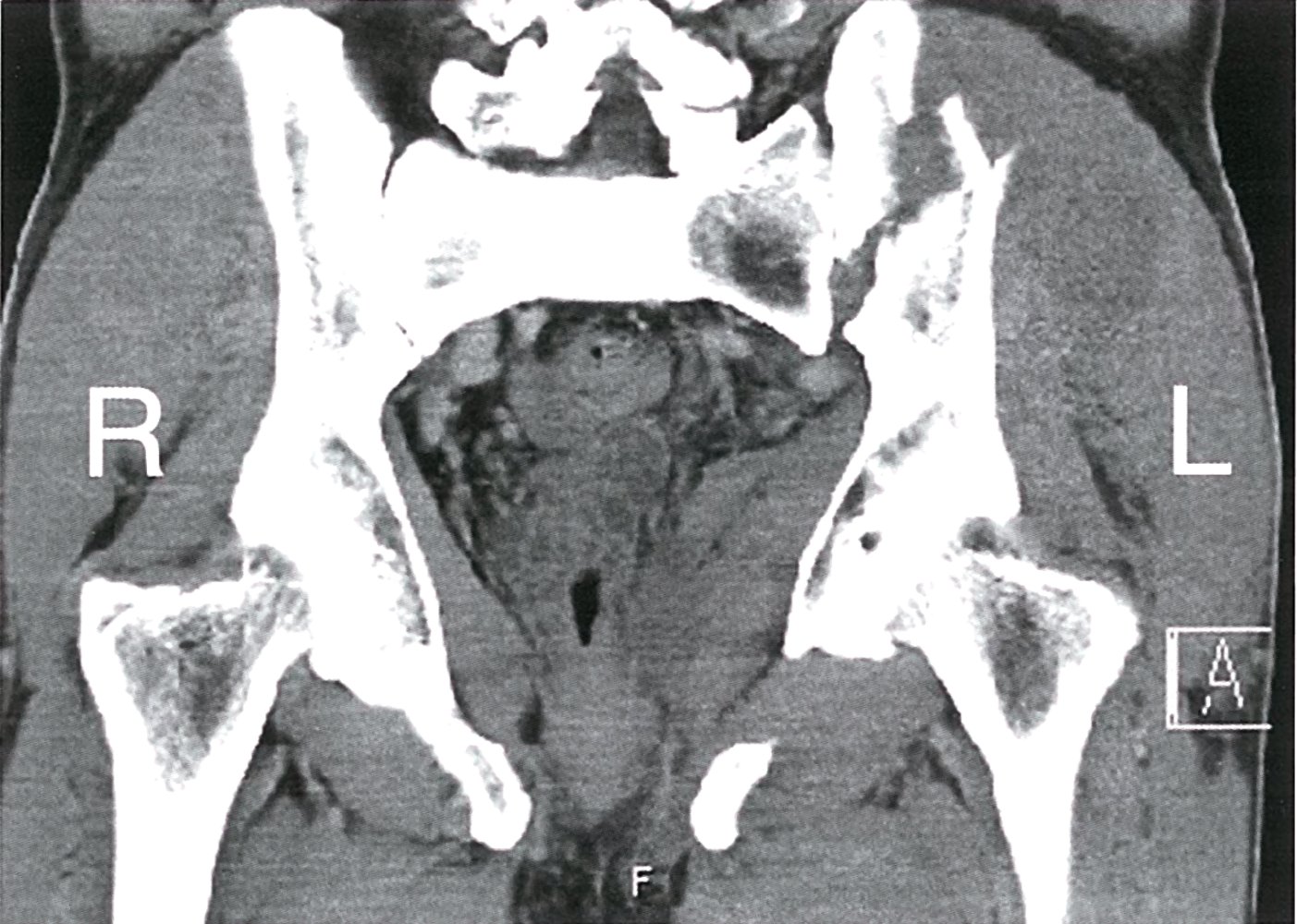
CT pelvis (soft tissue window; coronal section)
An obliquely oriented fracture, communicating with the left sacroiliac joint, is visible through the left iliac wing (green line).
Source: © IMPP
Blunt neck trauma
Approach to blunt neck trauma [1]
Ensure the following components are included as part of the standard management of trauma patients using the ATLS algorithm:
-
Primary survey
- Prepare for difficult airway management and secure the airway early (see “Treatment”).
- Apply C-spine immobilization (see “Initial management of C-spine injury”).
- Consider neurogenic shock in hypotensive patients with no evidence of hemorrhagic or obstructive shock.
- If at a nontrauma center, initiate transfer to a trauma center; airway obstruction or hypotension are indications for trauma team activation.
-
Secondary survey
- Perform neurovascular examination focusing on clinical and diagnostic features of BCVI.
- Obtain urgent diagnostics for trauma patients (see “Diagnostics”).
- Consult specialists based on injured anatomical structures (see “Surgical management”).
Associated injuries [2]
- Laryngotracheal contusions and lacerations
- Laryngeal fracture: a fracture of the thyroid cartilage and/or the cricoid cartilage
- Fractures and/dislocations of the tracheal cartilages
- Tracheal rupture: the partial or complete puncture or laceration of the trachea or the main bronchi
- Pharyngoesophageal injury
- Blunt cerebrovascular injury
- Cervical spine injuries, e.g., hangman fracture
Clinical features [1]
-
Airway or esophageal injury
- Signs of airway compromise (e.g., dyspnea)
- Hoarseness and/or stridor
- Subcutaneous emphysema (e.g., crepitus)
- Mediastinal emphysema (e.g., Hamman sign)
- Hemoptysis
- Dysphagia
- Vascular injury
- Carotid bruit
- Expanding neck hematoma
- Focal neurological deficit
-
Clinical features of strangulation [2][39]
- Asphyxiation, loss of consciousness
- Dysphagia, voice changes
- Subconjunctival hemorrhage, facial petechiae
- Bruising around the neck, strangulation marks


Diagnostics [1]
See “Urgent diagnostics for trauma patients” for a comprehensive approach.
- Bedside assessment: CXR
-
CT imaging in trauma
- Vascular injury: CTA head and neck
- C-spine injury: CT C-spine without IV contrast (See “Diagnostics for C-spine injuries” for details.)
- Laryngeal injury: CT neck with IV contrast
-
Additional testing
- Vascular injury: duplex ultrasound, angiography
- Esophageal injury: esophagoscopy, esophagography
- Laryngeal injury: direct laryngoscopy, flexible nasopharyngoscopy
Treatment [1][2]
Airway management [40]
- If there are signs of airway compromise, call for help immediately (e.g., emergent anesthesia or ENT consult).
- Perform BMV with caution.
- Prepare for difficult airway management (e.g., distorted anatomy, blood, and/or edema) by an experienced provider.
- Intubation via direct laryngoscopy or video laryngoscopy using a smaller-sized ET tube can be attempted initially.
- Awake fiberoptic intubation is preferred for distorted anatomy.
- Prepare for emergency surgical airway as a backup.
- Perform manual in-line cervical stabilization during airway management.
Cricothyroidotomy may be impossible if anatomical landmarks are invisible or deformed, e.g., due to a laryngeal fracture. Emergency tracheostomy may be required if intubation has failed. [1]
Surgical management
Consult surgical subspecialties based on clinical and diagnostic findings.
- Vascular injuries: vascular surgery
- Laryngotracheal injuries: otolaryngology
- C-spine injuries: spine surgery (See “Definitive management of C-spine injuries.”)
- Esophageal injuries: thoracic surgery

Autopsy of a 32-year-old woman; left eye
The upper eyelid is ectropionized. There are multiple petechiae of the conjunctiva.
Congestive hemorrhages are consistent with violent asphyxiation (venous outflow obstruction with preserved arterial blood supply).
Source: © IMPP

Source: “Fig 2, In: Accidental Strangulation with Cervical Nerve Root Injury Caused by the Entrapment of Clothing in a Soybean Milling Machine” by Omori K, Takeuchi I, Yanagawa Y, Hindawi, licensed under CC BY 4.0.
Cerebrovascular injury
Blunt cerebrovascular injury (BCVI) involves the carotid and/or vertebral artery and can cause a stroke as a result of thrombi formation, wall hematomas, and/or vascular occlusion.
Expanded Denver screening criteria [41][42][43]
The expanded Denver screening criteria is a tool used to identify patients at risk for BCVI and the need for advanced imaging. A positive screen is any clinical or diagnostic feature of BCVI or the combination of a high-speed mechanism and any risk factor for BCVI.
-
Clinical and diagnostic features of BCVI
- Nasal/oral/cervical arterial hemorrhage
- Carotid bruit in patients aged < 50 years
- Expanding neck hematoma
- Focal neurological deficit
- Neurological deficits inconsistent with CT head
- Ischemic stroke on CT or MRI
-
Risk factors for BCVI
- Fractures: facial (Le Fort II and Le Fort III), mandible, occipital condyle, skull (complex and basilar), upper ribs, C-spine
- TBI with GCS < 6
- Degloving injury of the scalp
- Near hanging with anoxic brain injury
- C-spine ligamentous injury or subluxation
- Combined TBI and thoracic injury
- Blunt cardiac or thoracic vascular injury
- Seat belt injury with significant pain, swelling, or change in mental status
Diagnostics [41]
- CTA head and neck
- Digital subtraction angiography
Treatment [41]
Treatment varies based on injury severity and anatomical location and may include:
- Antithrombotic therapy
- Surgical repair
- Endovascular stenting
Blunt extremity trauma
Approach to blunt extremity trauma [1]
Ensure the following components are included as part of the standard management of trauma patients using the ATLS algorithm:
-
Primary survey
- Apply direct pressure and/or a tourniquet if there is active extremity hemorrhage.
- Address life-threatening injuries (e.g., immobilize fractures associated with severe injuries).
- If at a nontrauma center, initiate transfer to a trauma center for hard signs of extremity vascular injury; traumatic amputation is an indication for trauma team activation.
-
Secondary survey
- Perform detailed neurovascular examination of the affected extremity.
- Evaluate for rhabdomyolysis and compartment syndrome.
- Provide supportive care, e.g., analgesia, tetanus prophylaxis.
- Obtain urgent diagnostics for trauma patients, including laboratory studies and x-ray and/or CTA extremity, once stable (see “Diagnostics”).
- Determine if there is a need for surgical consultation (e.g., vascular surgery, orthopedic surgery) based on injury characteristics.
Clinical features
Clinical features depend on the type and extent of associated injuries, and on any complications (e.g., compartment syndrome).
- Hemorrhagic shock (e.g., hypotension, tachycardia)
- Neurological deficit (e.g., loss of strength and/or sensation)
- Hard signs of extremity vascular injury (e.g., absent distal pulses, pulsatile hematoma)
- Clinical features of fractures (e.g., limb deformity, signs of an open fracture)
- Clinical features of compartment syndrome (e.g., pain out of proportion that worsens with passive stretching)
- Clinical features of rhabdomyolysis and crush syndrome (e.g., darkened urine, signs of shock)
Diagnostics [1][8]
See “Urgent diagnostics for trauma patients” for a comprehensive approach.
-
Vascular injury
- Arterial-brachial index (ABI) [1]
- CTA of the injured limb [44]
- Duplex ultrasound
- Bony injury: x-ray of injured limb
- Rhabdomyolysis: serial CPK, BMP
- Compartment syndrome: compartment pressure measurement
Management
-
Vascular injury
- Prioritize hemostatic control.
- Consult vascular surgery for patients with hard signs of extremity vascular injury or abnormal imaging.
-
Fracture: See “Initial fracture management.”
- Immobilize with a splint (see “Upper extremity splints” and “Lower extremity splints” for details).
- Consult orthopedic surgery and provide antibiotic prophylaxis for open fractures.
-
Dislocation
- Perform closed reduction and splint.
- Consult orthopedic surgery for neurovascular compromise.
- See “Shoulder dislocation,” “Hip dislocation,” and “Tibiofemoral joint dislocation” for details.
-
Rhabdomyolysis: See “Management of rhabdomyolysis.”
- Provide IV fluid resuscitation.
- Perform serial laboratory monitoring (e.g., CPK, BMP).
- Manage associated electrolyte derangements (e.g., hyperkalemia).
-
Compartment syndrome: See “Management of acute compartment syndrome.”
- Obtain immediate surgical consultation.
- Initiate supportive care to optimize tissue perfusion and oxygenation.
- Tendon and ligament injuries: See “Knee ligament injuries,” “Achilles tendon rupture,” and “Sports injuries” for details.
External Resources
- 2023 EAST Practice Management Guideline for Older Adults with Multiple Rib Fractures
- 2020 ACR Appropriateness Criteria: Major Blunt Trauma
- 2020 ACR Appropriateness Criteria: Blunt Chest Trauma - Suspected Cardiac Injury
- 2020 EAST Practice Management Guideline: Evaluation and Management of Blunt Cerebrovascular Injury
- 2019 ACR Appropriateness Criteria: Rib Fractures
- 2018 ACS TQP Best Practices Guidelines in Imaging
- 2015 EAST Practice Management Guideline: Evaluation and Management of Blunt Traumatic Aortic Injury
- 2012 EAST Practice Management Guideline: Screening for Blunt Cardiac Injury
References
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Chung JH, Cox CW, Mohammed TLH, et al. "ACR Appropriateness Criteria Blunt Chest Trauma". J Am Coll Radiol. 11(4). :345-351. (2014)
- Shyu JY, Khurana B, Soto JA, et al. "ACR Appropriateness Criteria® Major Blunt Trauma". J Am Coll Radiol. 17(5). :S160-S174. (2020)
- Rodriguez RM, Hendey GW, Mower W, et al. "Derivation of a Decision Instrument for Selective Chest Radiography in Blunt Trauma". J Trauma. 71(3). :549-553. (2011)
- Rodriguez RM, Anglin D, Langdorf MI, et al. "NEXUS Chest". JAMA Surg. 148(10). :940. (2013)
- Rodriguez RM, Langdorf MI, Nishijima D, et al. "Derivation and Validation of Two Decision Instruments for Selective Chest CT in Blunt Trauma: A Multicenter Prospective Observational Study (NEXUS Chest CT)". PLoS Med. 12(10). :e1001883. (2015)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Søreide K, Weiser TG, Parks RW. "Clinical update on management of pancreatic trauma". HPB (Oxford). 20(12). :1099-1108. (2018)
- "ACS TQP Best Practices Guidelines in Imaging". https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf. [2018-10-01]
- Cimbanassi S, Chiara O, Leppaniemi A, et al. "Nonoperative management of abdominal solid-organ injuries following blunt trauma in adults: Results from an International Consensus Conference". J Trauma Acute Care Surg. 84(3). :517-531. (2018)
- Stassen NA, Bhullar I, Cheng JD, et al. "Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline". J Trauma Acute Care Surg. 73(5). :S294-S300. (2012)
- Stassen NA, Bhullar I, Cheng JD, et al. "Nonoperative management of blunt hepatic injury". J Trauma Acute Care Surg. 73(5). :S288-S293. (2012)
- Johnsen NV, Betzold RD, Guillamondegui OD, et al. "Surgical Management of Solid Organ Injuries". Surg Clin North Am. 97(5). :1077-1105. (2017)
- Peterson ML, Abbas PI, Fallon SC, Naik-Mathuria BJ, Rodriguez JR. "Management of traumatic duodenal hematomas in children". J Surg Res. 199(1). :126-129. (2015)
- Ratnasekera A, Ferrada P. "Traumatic Duodenal Injury: Current Management Update". Current Surgery Reports. 8(5). (2020)
- Biffl WL, Moore EE, Croce M, et al. "Western Trauma Association Critical Decisions in Trauma: Management of pancreatic injuries". J Trauma Acute Care Surg. 75(6). :941-946. (2013)
- Tran TLN, Brasel KJ, Karmy-Jones R, et al. "Western Trauma Association Critical Decisions in Trauma: Management of pelvic fracture with hemodynamic instability — 2016 updates". J Trauma Acute Care Surg. 81(6). :1171-1174. (2016)
- Perumal R, S DCR, P SS, et al. "Management of pelvic injuries in hemodynamically unstable polytrauma patients – Challenges and current updates". J Clin Orthop Trauma. 12(1). :101-112. (2021)
- Moore EE, V. Feliciano D, Mattox KL. "Trauma, Eighth Edition". McGraw Hill Professional. (2017). ISBN: 9781260128604
- Lin MR, Kraus JF. "A review of risk factors and patterns of motorcycle injuries". Accid Anal Prev. 41(4). :710-722. (2009)
- Thompson MJ, Rivara FP. "Bicycle-related injuries.". Am Fam Physician. 63(10). :2007-14. (2001)
- Moreland B, Kakara R, Henry A. "Trends in Nonfatal Falls and Fall-Related Injuries Among Adults Aged ≥65 Years — United States, 2012–2018". MMWR Morb Mortal Wkly Rep. 69(27). :875-881. (2020)
- Clancy K, Velopulos C, Bilaniuk JW, et al. "Screening for blunt cardiac injury". J Trauma Acute Care Surg. 73(5). :S301-S306. (2012)
- Kyriazidis IP, Jakob DA, Vargas JAH, et al. "Accuracy of diagnostic tests in cardiac injury after blunt chest trauma: a systematic review and meta-analysis". World J Emerg Surg. 18(1). (2023)
- Stojanovska J, Hurwitz Koweek LM, Chung JH, et al. "ACR Appropriateness Criteria® Blunt Chest Trauma-Suspected Cardiac Injury". J Am Coll Radiol. 17(11). :S380-S390. (2020)
- Link MS, Mark Estes NA, Maron BJ. "Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 13: Commotio Cordis". Circulation. 132(22). (2015)
- Peng T, Derry LT, Yogeswaran V, Goldschlager NF. "Commotio Cordis in 2023". Sports Med. 53(8). :1527-1536. (2023)
- Spitaler P, Stühlinger M, Adukauskaite A, Bauer A, Dichtl W. "A Soccer Shot with Lengthy Consequences-Case Report & Current Literature Review of Commotio Cordis". J Clin Med. 12(6). (2023)
- Fox N, Schwartz D, Salazar JH, et al. "Evaluation and management of blunt traumatic aortic injury". J Trauma Acute Care Surg. 78(1). :136-146. (2015)
- Mouawad NJ, Paulisin J, Hofmeister S, et al. "Blunt thoracic aortic injury – concepts and management". J Cardiothorac Surg. 15(1). (2020)
- Akhmerov A, DuBose J, Azizzadeh A. "Blunt Thoracic Aortic Injury: Current Therapies, Outcomes, and Challenges". Ann Vasc Dis. 12(1). :1-5. (2019)
- Simon B, Ebert J, Bokhari F, et al. "Management of pulmonary contusion and flail chest". J Trauma Acute Care Surg. 73(5). :S351-S361. (2012)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Kim M, Moore JE. "Chest Trauma: Current Recommendations for Rib Fractures, Pneumothorax, and Other Injuries". Curr Anesthesiol Rep. 10(1). :61-68. (2020)
- Henry TS, Donnelly EF, Boiselle PM, et al. "ACR Appropriateness Criteria® Rib Fractures". J Am Coll Radiol. 16(5). :S227-S234. (2019)
- Shuaib W, Vijayasarathi A, Tiwana MH, et al. "The diagnostic utility of rib series in assessing rib fractures". Emerg Radiol. 21(2). :159-164. (2013)
- Mukherjee K, Schubl SD, Tominaga G, et al. "Non-surgical management and analgesia strategies for older adults with multiple rib fractures: A systematic review, meta-analysis, and practice management guideline from the Eastern Association for the Surgery of Trauma and the Chest Wall Injury Society". J Trauma Acute Care Surg. 94(3). :398-407. (2022)
- Brasel KJ, Moore EE, Albrecht RA, et al. "Western Trauma Association Critical Decisions in Trauma: Management of rib fractures". J Trauma Acute Care Surg. 82(1). :200-203. (2017)
- "Evaluation and Management of the Sexually Assaulted or Sexually Abused Patient, 2nd edition". https://www.acep.org/globalassets/new-pdfs/sexual-assault-e-book.pdf. [2013-01-01]
- Mayglothling J, Duane TM, Gibbs M, et al. "Emergency tracheal intubation immediately following traumatic injury". J Trauma Acute Care Surg. 73(5). :S333-S340. (2012)
- Fox N, Rajani RR, Bokhari F, et al. "Evaluation and management of penetrating lower extremity arterial trauma". J Trauma. 73(5). :S315-S320. (2012)
- Kim DY, Biffl W, Bokhari F, et al. "Evaluation and management of blunt cerebrovascular injury: A practice management guideline from the Eastern Association for the Surgery of Trauma". J Trauma Acute Care Surg. 88(6). :875-887. (2020)
- Brommeland T, Helseth E, Aarhus M, et al. "Best practice guidelines for blunt cerebrovascular injury (BCVI)". Scand J Trauma Resusc Emerg Med. 26(1). :90. (2018)
- Franz RW, Willette PA, Wood MJ, Wright ML, Hartman JF. "A Systematic Review and Meta-Analysis of Diagnostic Screening Criteria for Blunt Cerebrovascular Injuries". J Am Coll Surg. 214(3). :313-327. (2012)