Summary
Bowel obstruction refers to the interruption of the normal passage of bowel contents through the bowel, either due to a functional or mechanical obstruction. Functional bowel obstruction, or paralytic ileus, is a temporary disturbance of peristalsis in the absence of mechanical obstruction (see “Paralytic ileus”). Mechanical bowel obstruction is the interruption of normal passage through the bowel due to a structural barrier. Mechanical bowel obstruction can be classified as either a small bowel obstruction (SBO) or large bowel obstruction (LBO) according to its location, and, depending on the extent of the obstruction, as either partial or complete. Postoperative bowel adhesion is the most common cause of SBO and malignancy is the most common cause of LBO. Regardless of the cause, bowel obstruction typically manifests with nausea, vomiting, abdominal pain, abdominal distention, and constipation or obstipation. Bowel sounds are increased and high-pitched in the early phases of bowel obstruction and decreased or absent in the later stages. Bowel distention leads to third-space volume loss, resulting in dehydration and electrolyte abnormalities. The symptoms of bowel obstruction are typically less severe in partial bowel obstruction than in total bowel obstruction. A diagnosis of bowel obstruction should be confirmed on imaging (e.g., CT abdomen and pelvis). Typical findings include dilated bowel loops proximal to the obstruction, collapse of bowel loops distal to the obstruction, and multiple air-fluid levels. Laboratory tests are needed to assess severity (e.g., metabolic acidosis and elevated serum lactate suggest bowel ischemia) and identify acid-base and electrolyte imbalances. A trial of nonoperative management (NOM), which includes bowel rest and supportive care (such as IV fluids, analgesics, antiemetics, and, if needed, antibiotics) can be considered in patients with simple bowel obstruction with no evidence of complications. Surgery is indicated for complicated bowel obstruction, closed-loop bowel obstruction, or if there is no clinical improvement following NOM for simple bowel obstruction. The underlying cause of bowel obstruction should be sought for and managed appropriately.
Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- CBC
- BMP
- CRP
- Blood gas analysis
- Lactate
- Unstable: abdominal x-ray and/or POCUS
- Stable: CT abdomen and pelvis with IV contrast
Red flag features
- Pain out of proportion
- Peritoneal signs
- Clinical features of shock
- Leukocytosis
- Metabolic acidosis
- Hyperlactatemia
Management checklist
- NPO
- Two large-bore peripheral IVs
- Fluid resuscitation and electrolyte repletion
- Symptomatic management (e.g., analgesics, antiemetics)
- Consider NG tube placement.
- Consider empiric antibiotics for intra-abdominal infections.
- Consult general surgery and/or gastroenterology.

© AMBOSS
Definitions
- Bowel obstruction: the interruption of normal passage through the bowel
- Mechanical bowel obstruction: the interruption of normal passage through the bowel due to a structural barrier (e.g., a tumor, adhesions)
- Paralytic ileus (functional bowel obstruction): temporary functional impairment of peristalsis in the absence of a mechanical obstruction (see “Mechanical bowel obstruction vs. paralytic ileus”)
- According to the site of obstruction, mechanical bowel obstruction can be classified as:
- Large bowel obstruction (LBO): obstruction at the level of the cecum, colon, or rectum
- Small bowel obstruction (SBO): obstruction at the level of the duodenum, jejunum, or ileum
- Gastric outlet obstruction (GOO): obstruction at the level of the pyloric channel or duodenum
Reference:[1]
Etiology
Etiologic classification [2]
Mechanical bowel obstruction can be classified into the following etiologic categories.
| Extrinsic bowel obstruction | Intrinsic bowel obstruction | ||
|---|---|---|---|
| Intramural bowel obstruction | Intraluminal bowel obstruction | ||
| Etiology |
|
|
|
Common etiologies
The causes of bowel obstruction vary according to the site of the obstruction and the age of the patient. For children, also see "Causes associated with pediatric gastric outlet obstruction or bowel obstruction" and "Differential diagnoses of neonatal intestinal obstruction."
| Etiology of bowel obstruction [1][3][4] | ||
|---|---|---|
| SBO | LBO | |
| Most common causes |
|
|
| Other causes |
|
|
| Specific to infants and children |
|
|

")

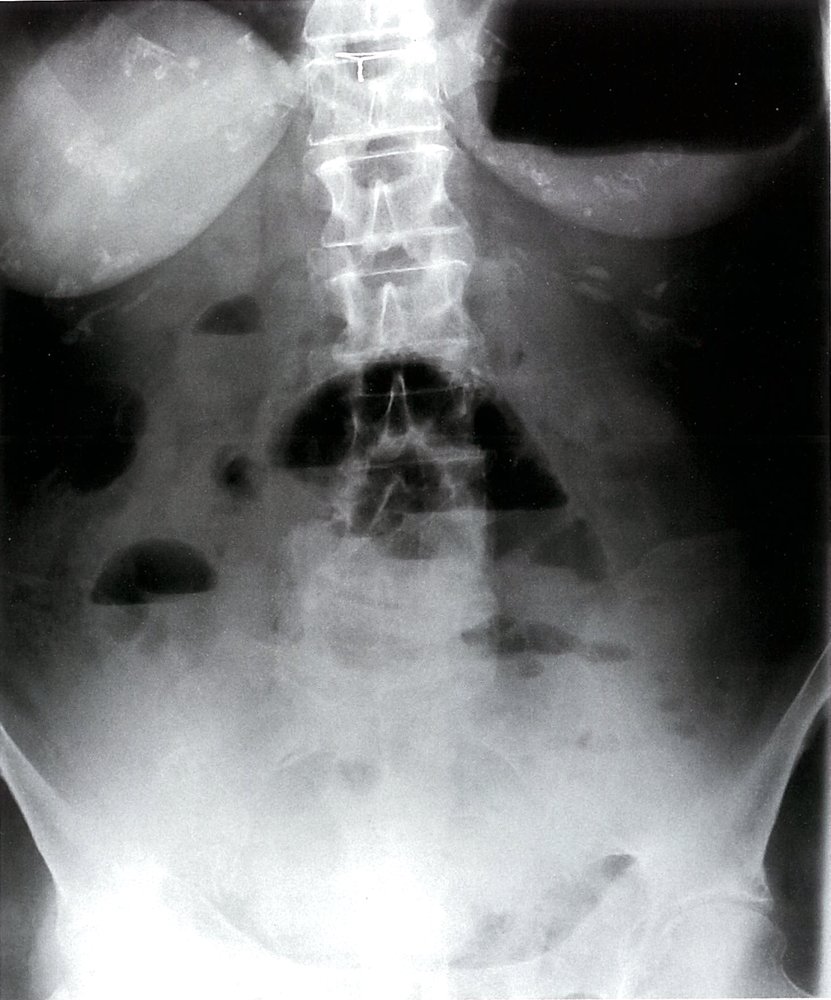
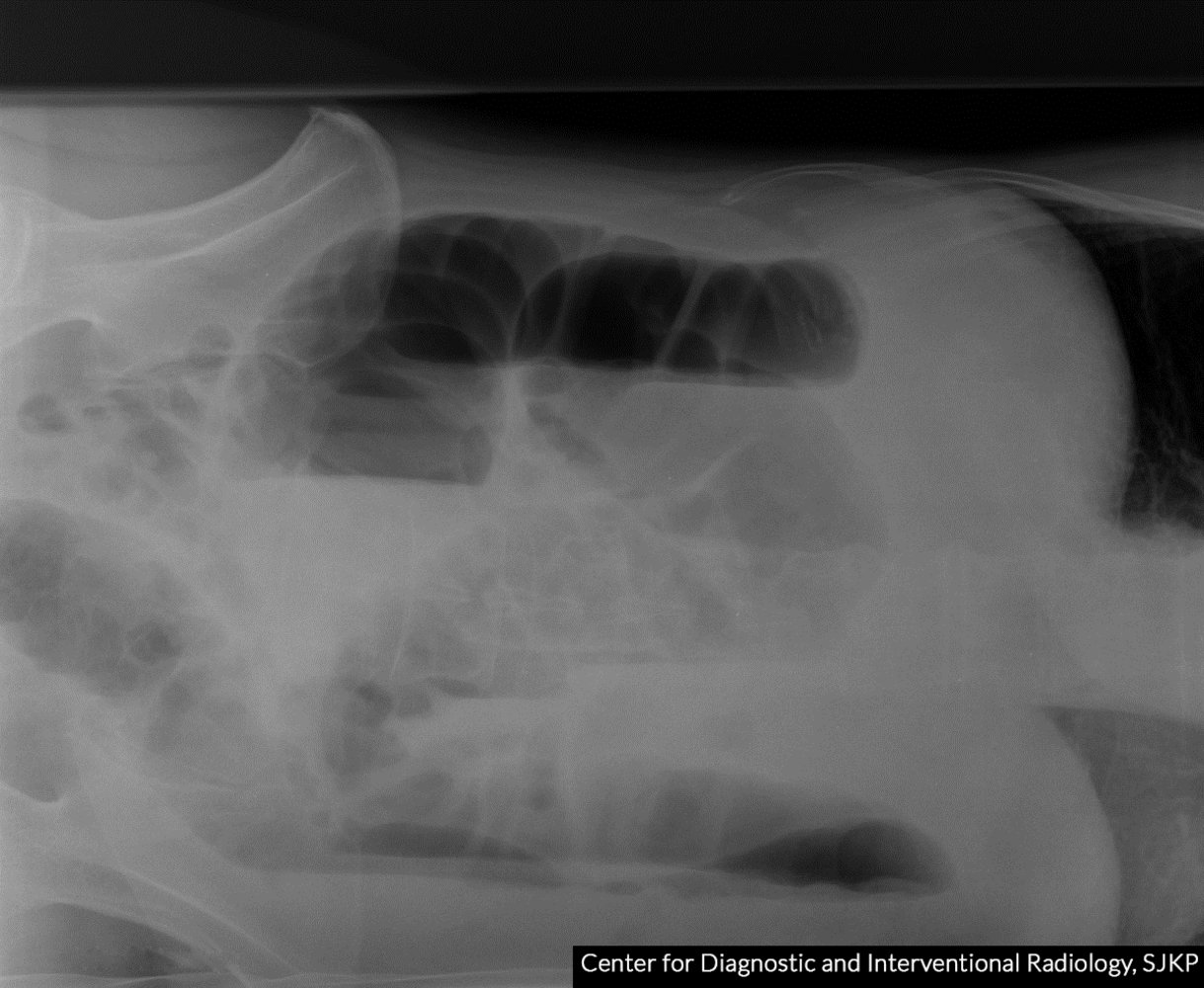
X-ray abdomen (AP view, supine) of a patient with distal small bowel obstruction
Multiple gas-filled, dilated (> 3 cm diameter) loops of bowel can be identified as small bowel loops by the presence of plicae circulares (green overlay).
This appearance on a supine abdominal radiograph may indicate ileus or distal obstruction. An erect or decubitus view is generally required to help distinguish ileus from obstruction.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
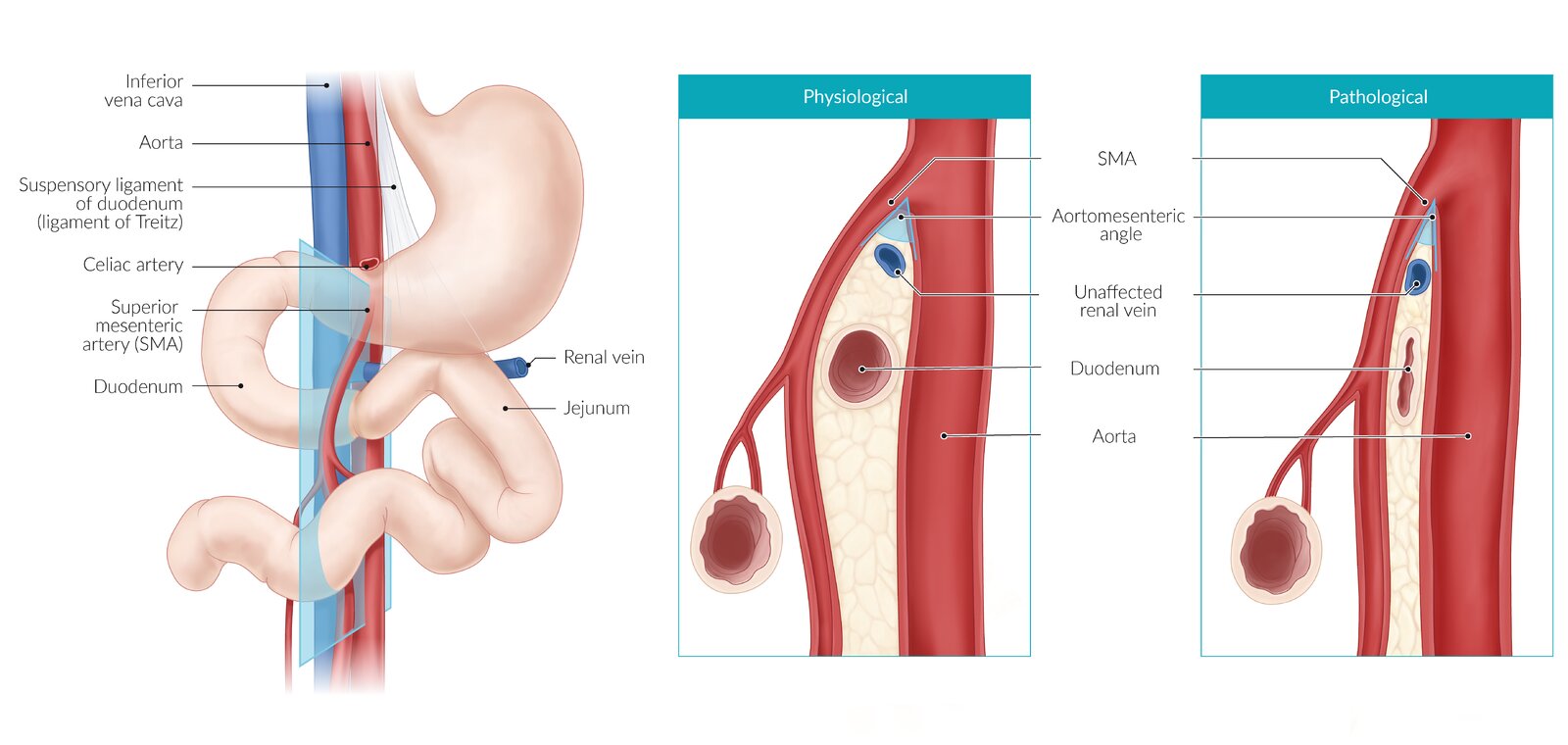
Narrowing of the angle between the superior mesenteric artery (SMA) and the aorta (aortomesenteric angle) may result in the third portion of the duodenum being compressed between the two vessels, and subsequently small bowel obstruction.
Note: This pathogenic mechanism may also cause nutcracker syndrome, in which the left renal vein (instead of the duodenum) is compressed between the SMA and the aorta.
© AMBOSS
Pathophysiology
-
Bowel obstruction → stasis of luminal contents and gas proximal to the obstruction → ↑ intraluminal pressure, which leads to the following: [1][3]
- Gaseous abdominal distention → sequestration of fluids within the distended bowel loops (third spacing) → dehydration and hypovolemia
- Vomiting → loss of fluid and Na+, K+, H+, and Cl- → hypokalemia, metabolic alkalosis, and hypovolemia
-
Compression of intestinal veins and lymphatics → bowel wall edema → compression of intestinal arterioles and capillaries → bowel ischemia, which leads to:
- ↑ Bowel wall permeability → translocation of intestinal microbes to the peritoneal cavity → sepsis
- Necrosis and perforation of the bowel wall → peritonitis
- Anaerobic metabolism and lysis of ischemic cells → accumulation of lactic acid and release of intracellular K+ → metabolic acidosis and hyperkalemia
Clinical features
Cardinal signs
The cardinal signs of mechanical bowel obstruction are abdominal pain, vomiting, constipation, abdominal distention, and decreased bowel sounds, regardless of the underlying etiology. The severity and progression of clinical features differ according to the site and severity of the obstruction.
-
Complete bowel obstruction [5]
- Total obstruction of the intestinal lumen, preventing the passage of air and fluid
- Rapid progression of clinical features
- Can be associated with obstipation (complete inability to pass stool or gas)
-
Partial bowel obstruction [6]
- Partial obstruction of the intestinal lumen, allowing a small amount of air and fluid to pass through
- Clinical features may be less severe than in complete bowel obstruction
- Can be associated with the intermittent passage of flatus and overflow diarrhea
Partial bowel obstruction causes gradually progressive symptoms that are typically milder than those caused by complete obstruction. Obstipation is only present in complete bowel obstruction.
| Clinical features associated with the site of bowel obstruction [1][3] | ||
|---|---|---|
| Clinical feature | SBO | LBO |
| Abdominal pain |
|
|
| Vomiting and/or nausea |
|
|
| Constipation or obstipation |
|
|
| Abdominal distention |
|
|
| Examination findings |
|
|
Progression
Depending on the onset and progression of clinical features, mechanical bowel obstruction can be classified as simple or complicated and acute or subacute. [6][7]
- Simple bowel obstruction: bowel obstruction with no evidence of complications (i.e., no features of bowel ischemia, bowel perforation, or red flags for complicated bowel obstruction) [1][2]
- Complicated bowel obstruction: bowel obstruction associated with strangulation, ischemic necrosis, or perforation [1][2]
-
Red flags for complicated bowel obstruction [1][2]
- Pain out of proportion
- Peritoneal signs
- Signs of systemic toxicity, e.g., SIRS
- Hemodynamic instability
- Laboratory abnormalities: e.g., significant leukocytosis, metabolic acidosis, ↑ lactate
| Clinical course of acute and subacute bowel obstruction | ||
|---|---|---|
| Acute bowel obstruction | Subacute bowel obstruction | |
| Clinical course |
|
|
| Typical causes |
|
|
Management
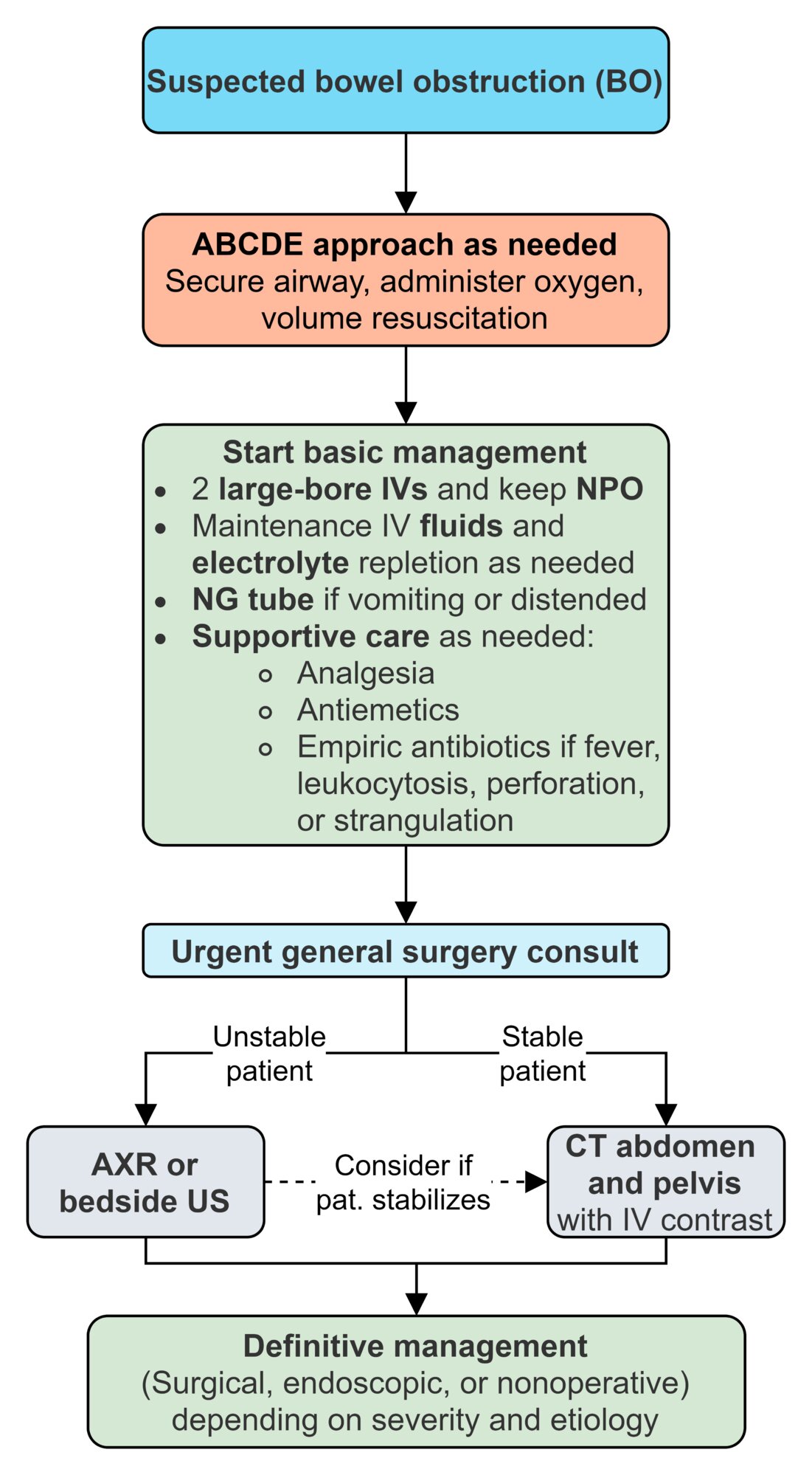
Bowel obstruction is an emergency and should be detected and managed early to minimize the risk of bowel perforation and strangulation, and the subsequent development of sepsis. The initial management of bowel obstruction is similar to that of undifferentiated acute abdomen.
- ABCDE approach: Evaluate vital signs, volume status, and the need for invasive monitoring.
- Urgent consults: general surgery, gastroenterology (also contact an intensivist as needed)
-
Initial management
- NPO status
- Obtain IV access with two large-bore peripheral IVs; simultaneously draw blood for urgent laboratory studies.
- IV fluid resuscitation
- Electrolyte repletion as needed
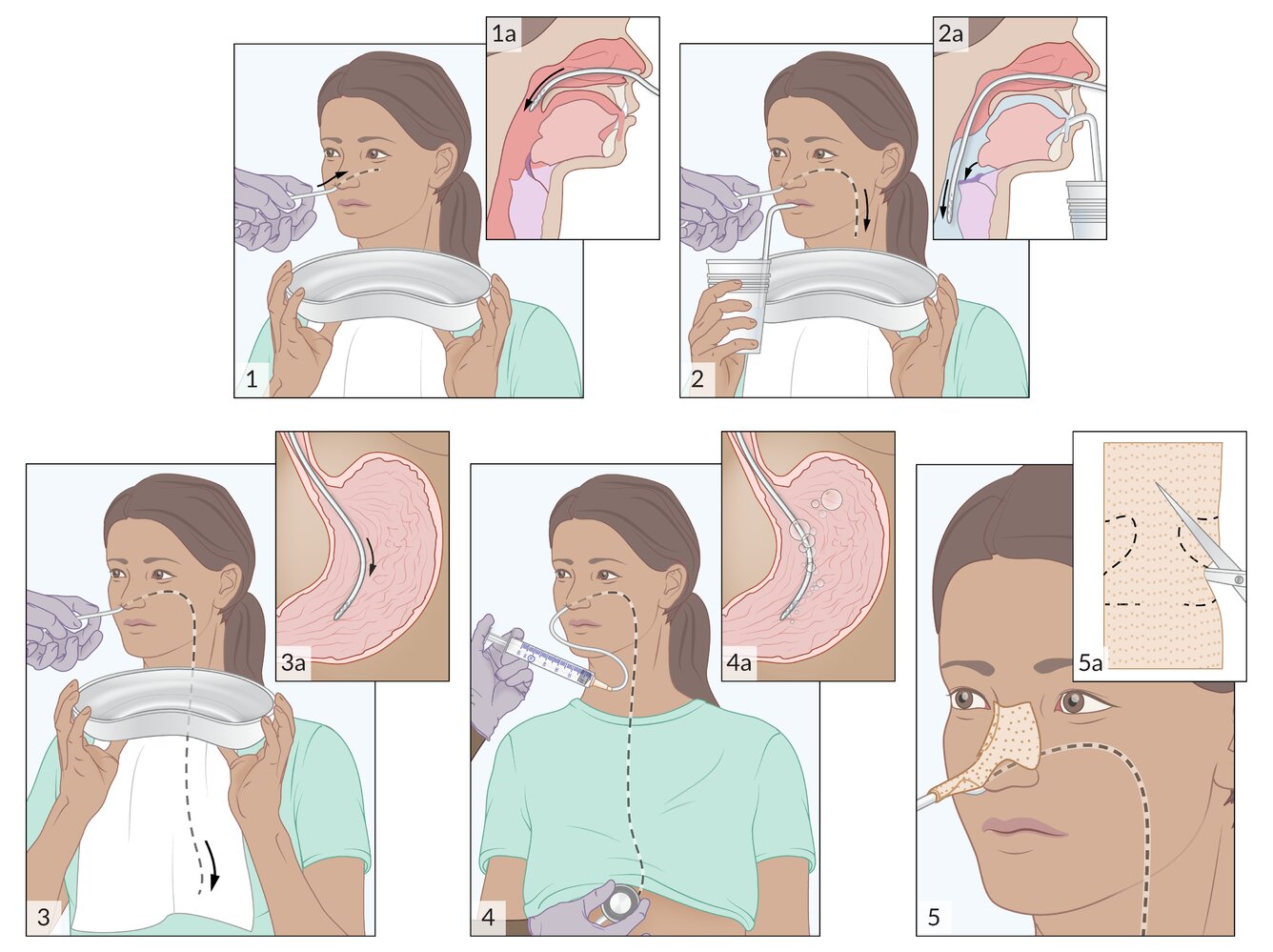
- Insert a nasogastric tube in patients with recurrent vomiting and/or significant abdominal distention.
- Supplemental oxygen as needed
-
Administer supportive care as needed.
- Parenteral analgesics
- Parenteral antiemetics
-
Empiric antibiotics for intraabdominal infections (not routinely recommended for simple bowel obstruction) [8][9]
- If fever and/or leukocytosis are present [3]
- For strangulated or perforated bowel obstruction
- As prophylaxis for operative malignant bowel obstruction [8]
- Obtain imaging: See “Diagnostics.”
- Disposition: Admit to the surgical service or transfer to the operating room (based on surgery consult). [3][6][10]
- Definitive management: See “Treatment.”
Admit patients with a bowel obstruction to a surgical service, even if conservative treatment is planned. Patients managed on a surgical service have better overall outcomes and lower health care expenditures than those managed on a medical service. [3][6][10]
References [1][3][11][12]
© AMBOSS
© AMBOSS
© AMBOSS
© AMBOSS
Diagnosis
General principles
- Imaging is required to:
- Confirm mechanical bowel obstruction
- Identify the site and assess the severity of the obstruction
- Identify complications and the underlying etiology of the obstruction
- Guide treatment planning
- Laboratory studies provide supportive evidence to help assess the severity of the obstruction.
Do not wait for imaging before initiating definitive management if there is an emergent critical finding (e.g., peritonitis). [8]
Bowel obstruction requires a swift diagnostic workup to establish if emergency surgery is required.
Imaging [3][5][13][14]
-
Initial imaging modality: depends on the type of bowel obstruction and hemodynamic stability of the patient
-
Acute bowel obstruction [3][14]
- Stable patients: CT abdomen and pelvis with IV contrast
- Unstable patients: Consider abdominal series x-ray or abdominal ultrasound first, along with urgent surgical consultation.
-
Subacute bowel obstruction
- Preferred: CT abdomen and pelvis with IV contrast
- Alternatives: MRI with and/or without IV contrast, water-soluble contrast challenge, and specialized dynamic contrast studies
-
Acute bowel obstruction [3][14]
- Findings: Radiological signs common to all imaging modalities are detailed in the table.
| Radiological signs of mechanical bowel obstruction common to all imaging modalities [2][14][15] | |
|---|---|
| Pathology | Findings |
| Dilatation of bowel loops proximal to the obstruction |
|
| Air-fluid level |
|
| Intraluminal air beyond the site of obstruction |
|
| Evidence of complications |
|
| Evidence of the underlying etiology |
|
Abdominal series x-ray
- Indication: most appropriate initial test in hemodynamically unstable patients or in resource-poor centers [3][15]
-
Findings
- Proximal bowel dilatation
- Minimal or no intraluminal air distal to the obstruction
- Stepladder sign (best seen on an upright view): multiple air-fluid levels and stacked dilated loops of small bowel
- Chest x-ray : Air under the diaphragm is an indicator of bowel perforation.
- See also “Radiological signs of mechanical bowel obstruction.”
-
Important considerations : X-rays have a number of limitations. [14]
- Variable sensitivity (50–65%) [7][8][15]
- Cannot reliably identify the site of obstruction, underlying etiology, or extent of complications
- Do not influence the management of acute bowel obstruction to the same extent as CT abdomen





")
")


To detect pneumoperitoneum on a chest x-ray, patients must be sitting upright for at least 10 minutes to allow free air to move upward and collect under the diaphragm. Patients with severe abdominal pain often require preemptive analgesia to tolerate the procedure! [17]
CT abdomen and pelvis (gold standard) [6][8][9][12][18]
-
Indications
- With IV contrast: most appropriate initial test in hemodynamically stable patients with acute bowel obstruction [7][19]
- With water-soluble oral contrast: Consider in patients with subacute bowel obstruction and no evidence of complications. [14]
- Without contrast: for patients with a contrast allergy
-
Findings
- Similar to those seen on abdominal x-ray; see “Radiological signs of mechanical bowel obstruction.”
- Transition point: sudden narrowing of the bowel lumen at the site of obstruction
-
Closed-loop bowel obstruction: a type of mechanical bowel obstruction in which the proximal and distal ends of the obstructed loop are closed
- Single site of obstruction: e.g., in volvulus or incarcerated hernia
- Multiple sites of obstruction: e.g., obstructing colorectal cancer with a competent ileocecal valve
- Progresses rapidly and is associated with an increased risk of strangulation
- Important consideration: In acute bowel obstruction, a CT scan is more accurate than an x-ray in the identification of the site of obstruction, complications, and underlying etiology, and, therefore, influences patient management to a greater extent. [14]
Closed-loop bowel obstructions are associated with an increased risk of bowel strangulation and perforation.



Abdominal ultrasound [8][10][20][21]
POCUS or formal ultrasound can be performed.
- Indication: Hemodynamically unstable patients (may be preferred over abdominal x-ray) [20][22][23]
-
Findings [20][24][25]
- Multiple fluid-filled dilated bowel loops > 2.5 cm in diameter adjacent to collapsed bowel loops (most specific finding) [23]
- Thickened bowel wall
- Prominent plicae circulares of dilated small bowel loops (sometimes referred to as the keyboard sign) [24]
- Altered peristalsis
- Increased (early finding) or decreased/absent (late finding)
- Pendular peristalsis: dysfunctional so-called “to-and-fro” peristalsis
- Intraperitoneal fluid accumulation may be present.



MRI abdomen and pelvis (with and/or without IV contrast) [14]
- Indication: hemodynamically stable patients with contraindications to radiation exposure
- Findings: similar to those identified with a CT scan; see “Radiological signs of mechanical bowel obstruction” for details.
Barium enema or water-soluble contrast enema [8][15][26]
- Indication: suspected distal LBO if CT is unavailable [8]
-
Findings [15]
- Tapering of the bowel lumen at the site of obstruction
- Complete bowel obstruction: contrast not visible beyond the obstruction
- Partial bowel obstruction: small amount of contrast visible beyond the obstruction
- Bird beak sign: in volvulus
- Apple core sign: in colonic malignancy [26]
- Tapering of the bowel lumen at the site of obstruction
Contrast enema helps differentiate complete bowel obstruction from partial bowel obstruction.
Barium enema is contraindicated if bowel perforation is suspected (water-soluble contrast enema can be used instead).


Water-soluble contrast challenge (WSCc) [8][12]
- Indication: SBO, to differentiate partial SBO from complete SBO [7][14]
- Procedure: A water-soluble contrast medium is administered orally or via an enteric tube, followed by abdominal x-ray 8 and 24 hours after ingestion. [7][12]
-
Findings [14]
- Normal WSCc: contrast reaches the colon within 24 hours of administration
- Indicates partial bowel obstruction
- The patient may be a candidate for nonoperative management.
- Intraluminal and intramural causes of bowel obstruction may be identified (see “Etiology”). [9]
- Normal WSCc: contrast reaches the colon within 24 hours of administration
-
Additional considerations
- WSCc is also used to evaluate response to nonoperative management.
- See “Nonoperative management of mechanical bowel obstruction.” [9]
Laboratory studies [6][12][13][27]
- Routine studies: CBC, BMP, serum lactate, and CRP
- Additional studies: See “Approach to acute abdomen.”
-
Supportive findings
- In patients who are dehydrated
- ↑ BUN and creatinine (prerenal acute kidney injury)
- ↑ Hematocrit (due to hemoconcentration)
-
In patients with recurrent vomiting
- Hypochloremic hypokalemic metabolic alkalosis
- Hyponatremia
-
Suggestive of complicated bowel obstruction ; [6][13][27]
- Hyperkalemia , elevated serum lactate, and metabolic acidosis: suggestive of bowel ischemia [5][7]
- Leukocytosis (> 16,000/mm3) [12]
- Elevated nonspecific inflammatory markers (↑ CRP and serum creatine kinase) [6]
- ↑ Amylase [1][5][7]
- Altered coagulation panel (e.g., elevated INR in sepsis)
- In patients who are dehydrated
Leukocytosis, metabolic acidosis, and elevated serum lactate in a patient with suspected bowel obstruction are suggestive of bowel ischemia.
© AMBOSS
X-ray abdomen (AP view, supine) of a patient with distal small bowel obstruction
Multiple gas-filled, dilated (> 3 cm diameter) loops of bowel can be identified as small bowel loops by the presence of plicae circulares (green overlay).
This appearance on a supine abdominal radiograph may indicate ileus or distal obstruction. An erect or decubitus view is generally required to help distinguish ileus from obstruction.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
X-ray abdomen (AP view; erect position)
Multiple air-fluid levels (green overlay) are visible in the mid-abdomen. The opaque appearance of the pelvis (red overlay) is due to fluid-filled loops of small bowel. There is a paucity of gas in the colon, and an air-fluid level is present in the dilated stomach (S).
Erect and decubitus radiographs can reveal air-fluid levels that are not identifiable on supine radiographs. Air-fluid levels can indicate ileus or mechanical obstruction. A lack of distal gas and air-fluid levels at different heights in the same bowel loop (differential air-fluid levels) suggest obstruction.
Source: © IMPP
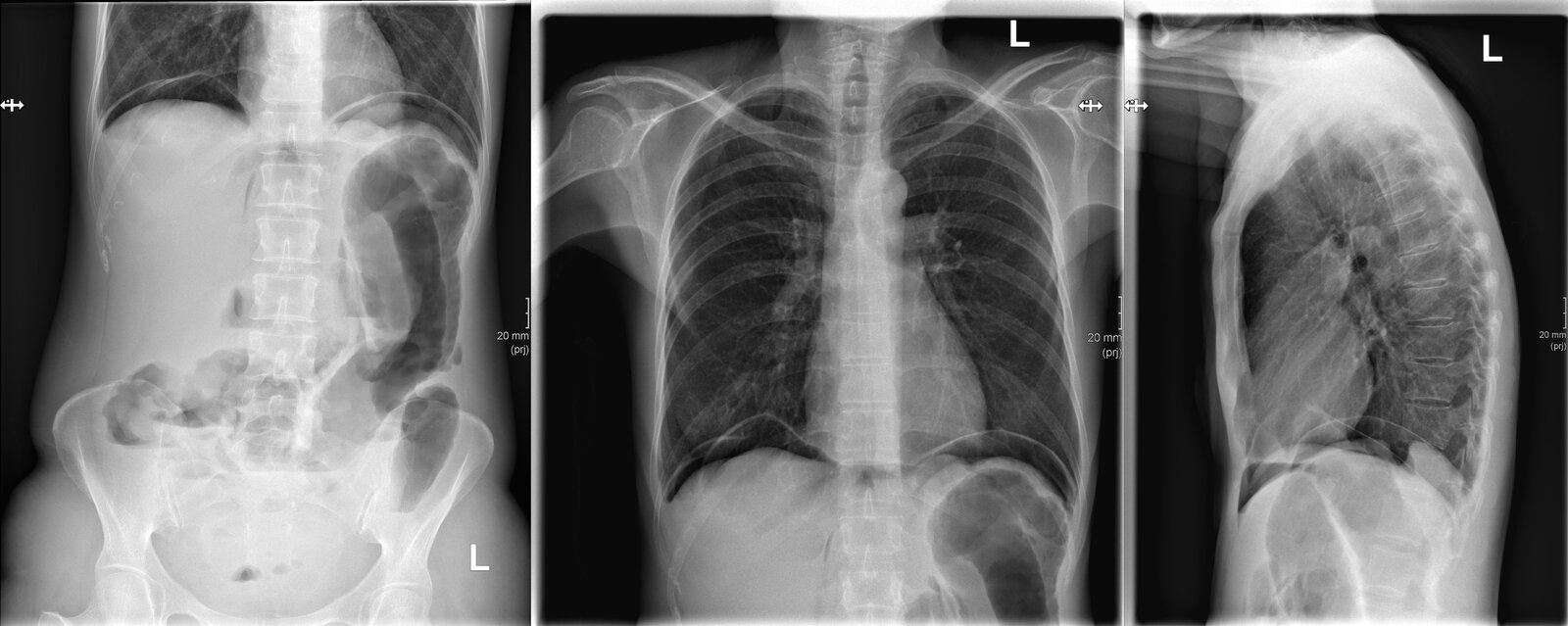
X-ray abdomen (AP erect view) and chest (PA and lateral views)
Multiple air-fluid levels are seen in the colon and small bowel (examples indicated by black lines). Some dilated segments of left colon are seen and gas is present in the peritoneal space as a result of bowel perforation. Gas is primarily located beneath the diaphragms (green overlay) because of the erect positioning of the patient. Additional gas has dissected into the retroperitoneum (examples indicated by red overlay) and is visible as linear collections parallel to the spine.
Our great thanks to Kerstin Bohse, MD (Klinikum Pfeiffersche Stiftungen), for kindly providing this case.
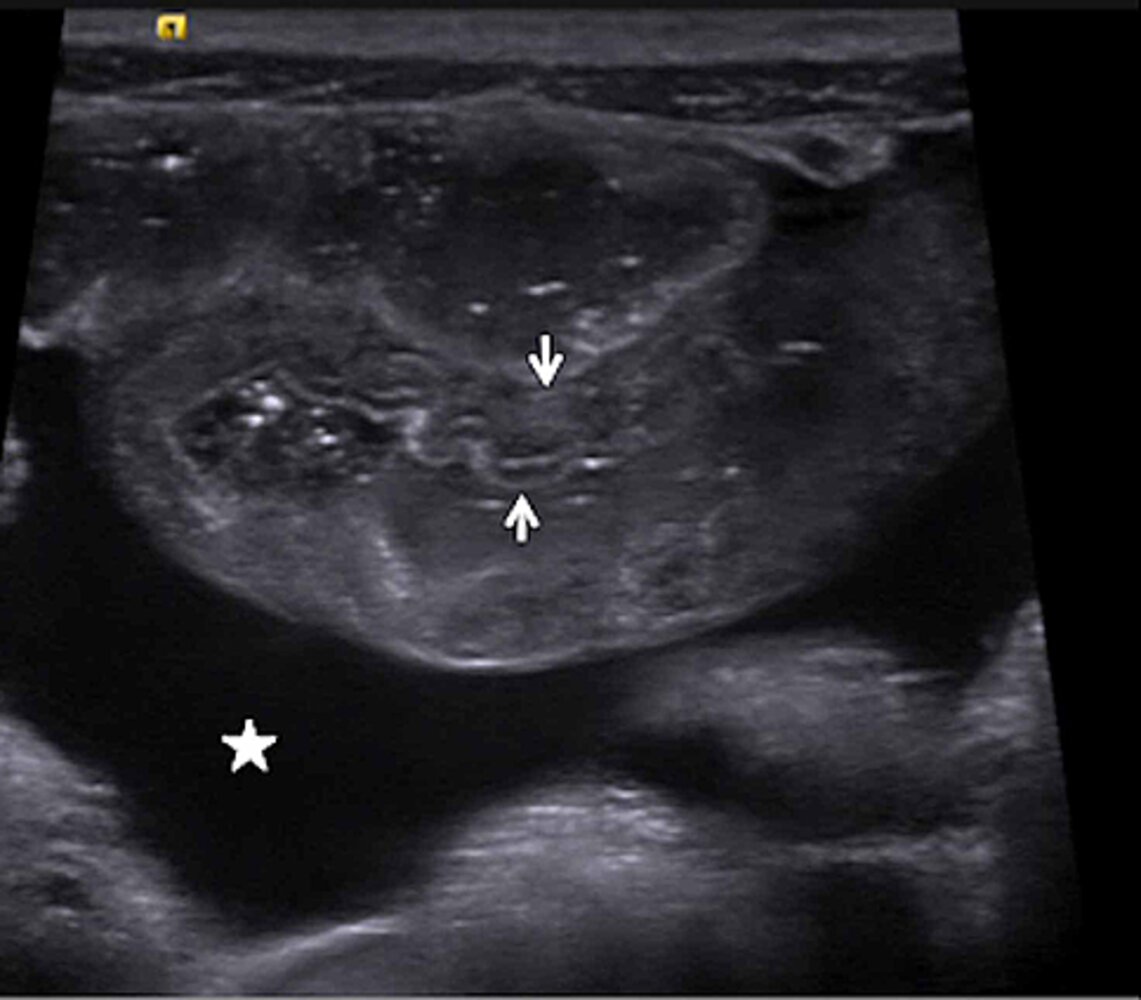
Ultrasound abdomen
A longitudinal image of a loop of small bowel shows abnormal mural thickening (arrows). Normal bowel has an average mural thickness in the range of 3–5 mm, depending on the degree of distention.
Star: ascites
Source: “Figure 1a, In: Henoch-Schönlein Purpura-Associated Hemorrhagic Shock After Secondary Norovirus Infection” by McLaughlin SK, Lawrence L, Adler J, Mehta H, Cureus, licensed under CC BY 4.0. Modifications: image cropped & letter removed.
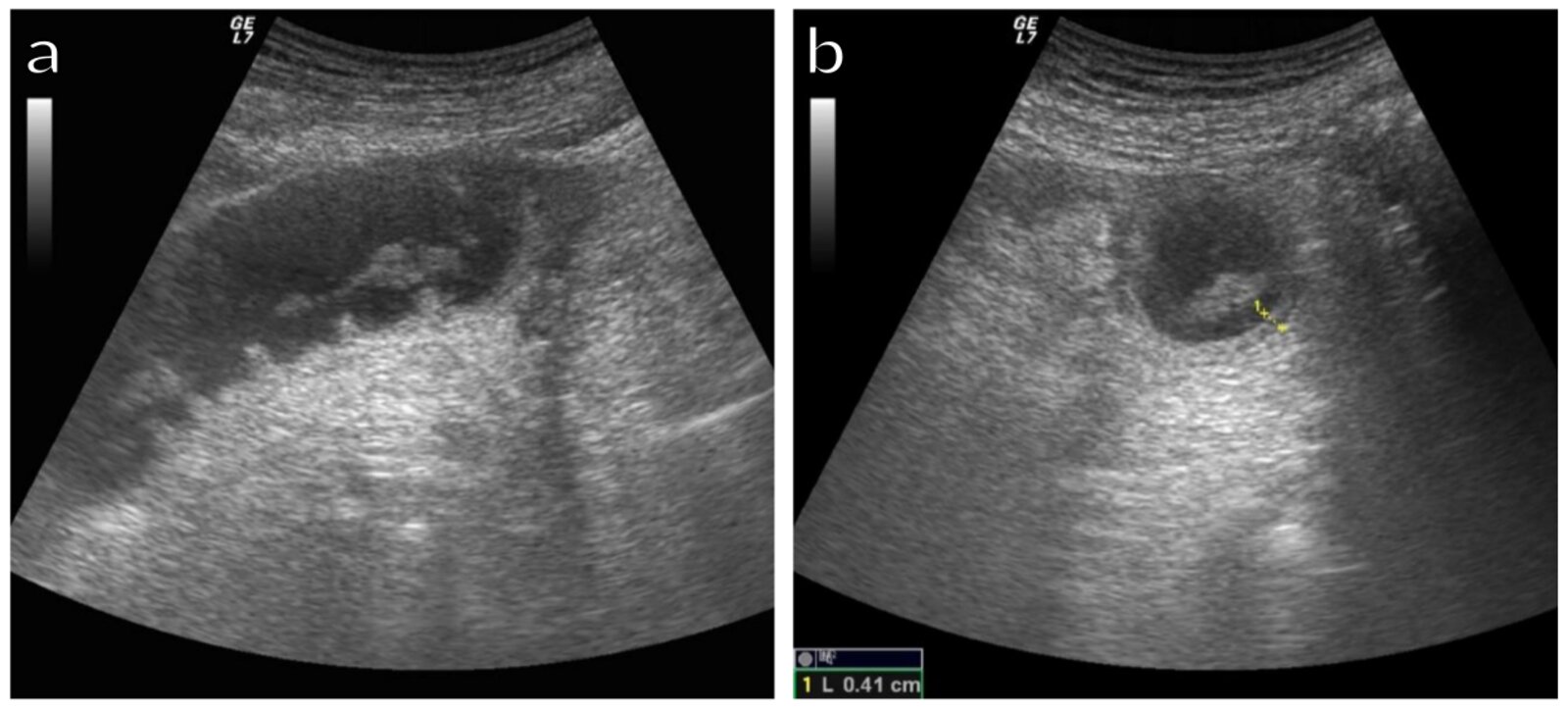
Ultrasound abdomen (a: longitudinal plane; b: axial plane)
A fluid-filled dilated small bowel loop contains floating hyperechoic material (green overlay). Hypoechoic fluid is seen adjacent to the loop (blue overlay). The bowel wall is thickened.
The presence of free fluid between dilated bowel loops, wall thickening (> 3 mm), and aperistalsis raise concern for bowel infarction.
Red overlay: valvulae conniventes
Source: “Figure 1, In: Diagnostic Accuracy of Ultrasound in the Diagnosis of Small Bowel Obstruction” by Stefania Tamburrini, Marina Lugarà, Francesco Iaselli, Pietro Paolo Saturnino, Carlo Liguori, Roberto Carbone et al., Molecular Diversity Preservation International, licensed under CC BY 4.0. Modifications: -FXV: Asterix removed; cropped; added "a" and "b". The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
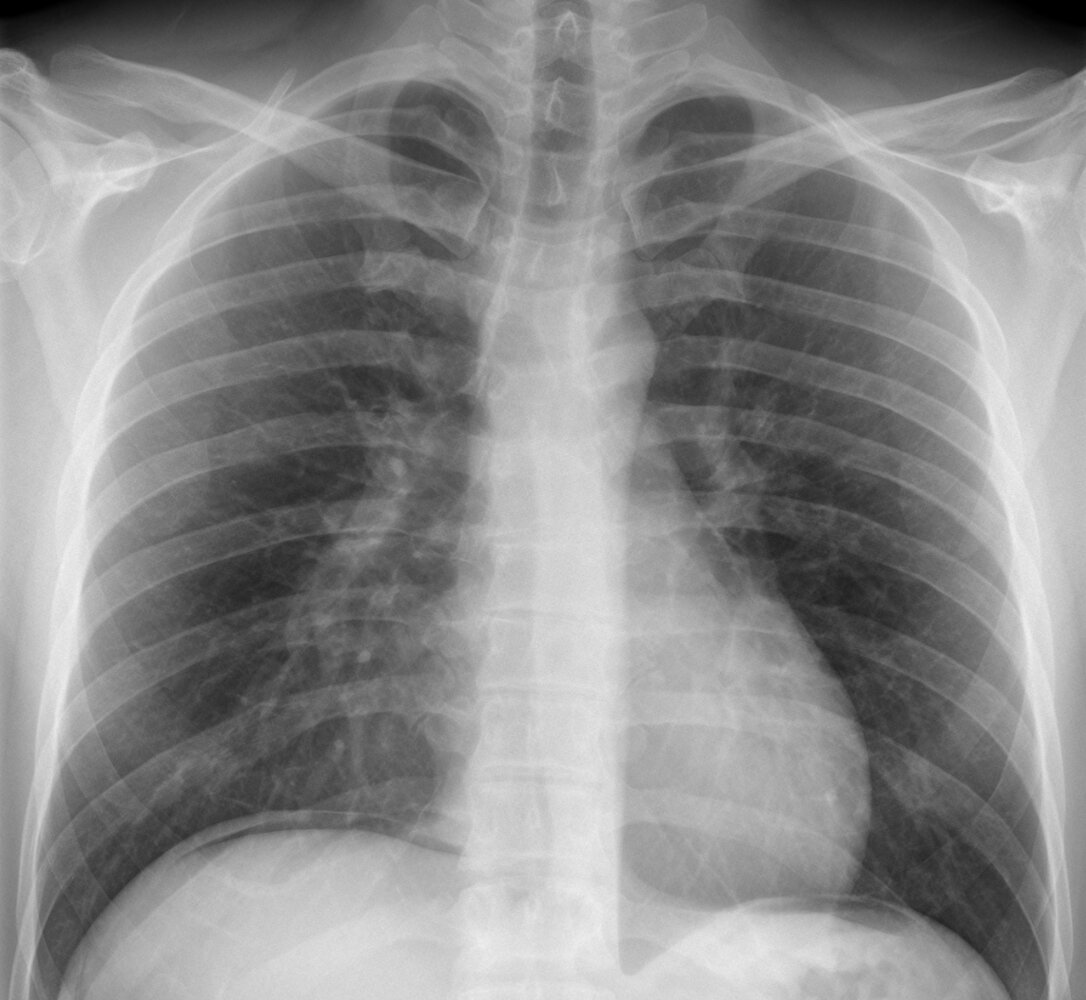
X-ray chest (PA view)
Free intraperitoneal gas (green overlay) is visible under both the right and left hemidiaphragms.
Source: “34-01-Freie Luft nach LH-OP” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

X-ray abdomen (AP view; supine position) of a patient with a history of distal colonic obstruction
The transverse colon is dilated (green outlines) and distended loops of small bowel are present in the right lower quadrant (examples indicated by red outlines). Gas is present in the descending colon (blue outline), but no gas is visible in the rectal region of the low pelvis (yellow overlay).
This radiographic appearance suggests distal mechanical obstruction or pseudo-obstruction in adynamic ileus. The acquisition of additional images (e.g., decubitus, prone) might help distinguish mechanical obstruction from pseudo-obstruction; the movement of gas would be restricted in obstruction and a transition point in the distal colon would potentially be seen.
S: stomach
Source: © IMPP

X-ray abdomen (AP view; supine position)
The ascending (green outline), transverse (red outline), and descending (yellow outline) portions of the colon are dilated. Scattered gas is seen in nondilated loops of small bowel. No gas is seen in the low pelvis in the region of the rectum (indicated by blue overlay).
The absence of rectal gas raises the possibility of distal mechanical obstruction; however, a normal posteriorly positioned rectum does not always fill with gas on a supine radiograph. Additional images (e.g., prone, decubitus) may help distinguish mechanical obstruction from pseudo-obstruction of colonic ileus.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.
X-ray abdomen (AP view; left lateral decubitus position)
Gas has migrated into the rectosigmoid, which does not appear obstructed. However, the image does not show the entire rectum, and a very distal obstruction would not be visible. The presence of differential air-fluid levels (examples indicated by green lines) within the dilated colon provides supportive evidence for a distal obstruction.
Our great thanks to Dr. Kissig (Center for Diagnostic and Interventional Radiology, Hedwigshöhe, St. Hedwig, Berlin, and St. Josefs Hospital, Potsdam) for kindly providing this image.

X-ray abdomen (AP view) of a patient with COVID-19, acute renal failure, and paralytic ileus
Gaseous distention of both small and large bowel is the result of paralytic ileus.
C: cecum; SB: small bowel; SF: splenic flexure; TC: transverse colon
Source: “Fig 2, In: Improvement of COVID-19 with renal failure and paralytic ileus by using steroids” by Kitamura A, So C, Jinta T, Wiley Online Library, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
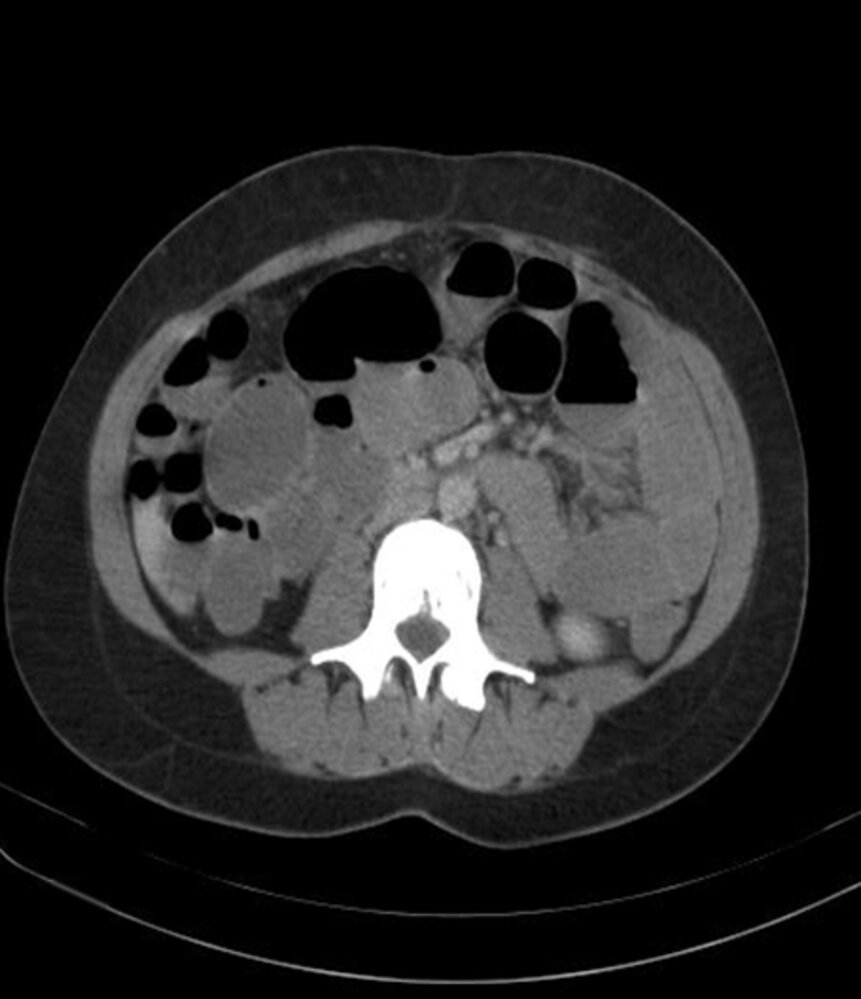
CT abdomen (IV contrast; axial plane) of a patient with small bowel obstruction
Numerous dilated loops of small bowel (examples indicated by green outline) are present in the abdomen, some of which contain fluid levels (dashed line). Small bowel dilation can be caused by mechanical obstruction or adynamic ileus.
Source: “Figure 2 B, in: A case of small bowel obstruction secondary to intestinal endometriosis” by Asiri Arachchi, Abhinav Vasudevan, Edorium Journals, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
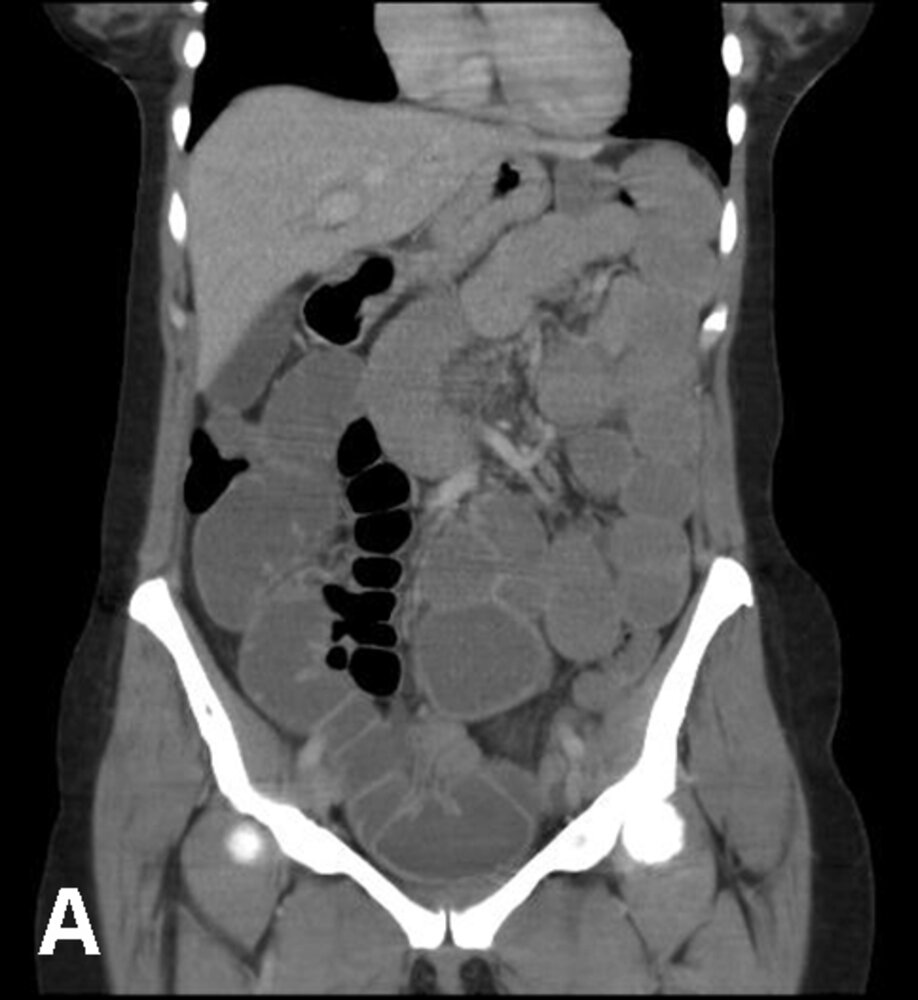
CT abdomen (IV contrast; coronal plane)
Significant dilatation of mid and distal small bowel loops can be seen (asterisks).
These findings are typical of small bowel obstruction.
Source: “Figure 2 A, in: A case of small bowel obstruction secondary to intestinal endometriosis” by Asiri Arachchi, Abhinav Vasudevan, Edorium Journals, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (with IV contrast; venous phase; axial and coronal planes) of a patient with sharp right lower quadrant pain
Multiple fluid-filled and dilated segments of small bowel (examples marked by red overlay) are seen. A site of transition (indicated by red outline) from dilated (green overlay) to decompressed small bowel is visible in the right lower quadrant. Affected bowel shows wall-thickening and intramural air (examples indicated by white outlines), which is concerning for necrosis. Interloop fluid and edema (green hatched overlay) are also seen, and free fluid is present in the pelvis (blue hatched overlay).
Surgical clips in the right upper quadrant (white arrowheads) indicate a previous cholecystectomy, and there is mild postoperative intrahepatic and extrahepatic biliary ductal dilatation (blue overlay). A small peripheral splenic defect (yellow overlay) is the site of a previous infarction.
Created by: Nándor Faluhelyi. Organization providing image: University of Pécs, Medical School. Further notes: Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this case.
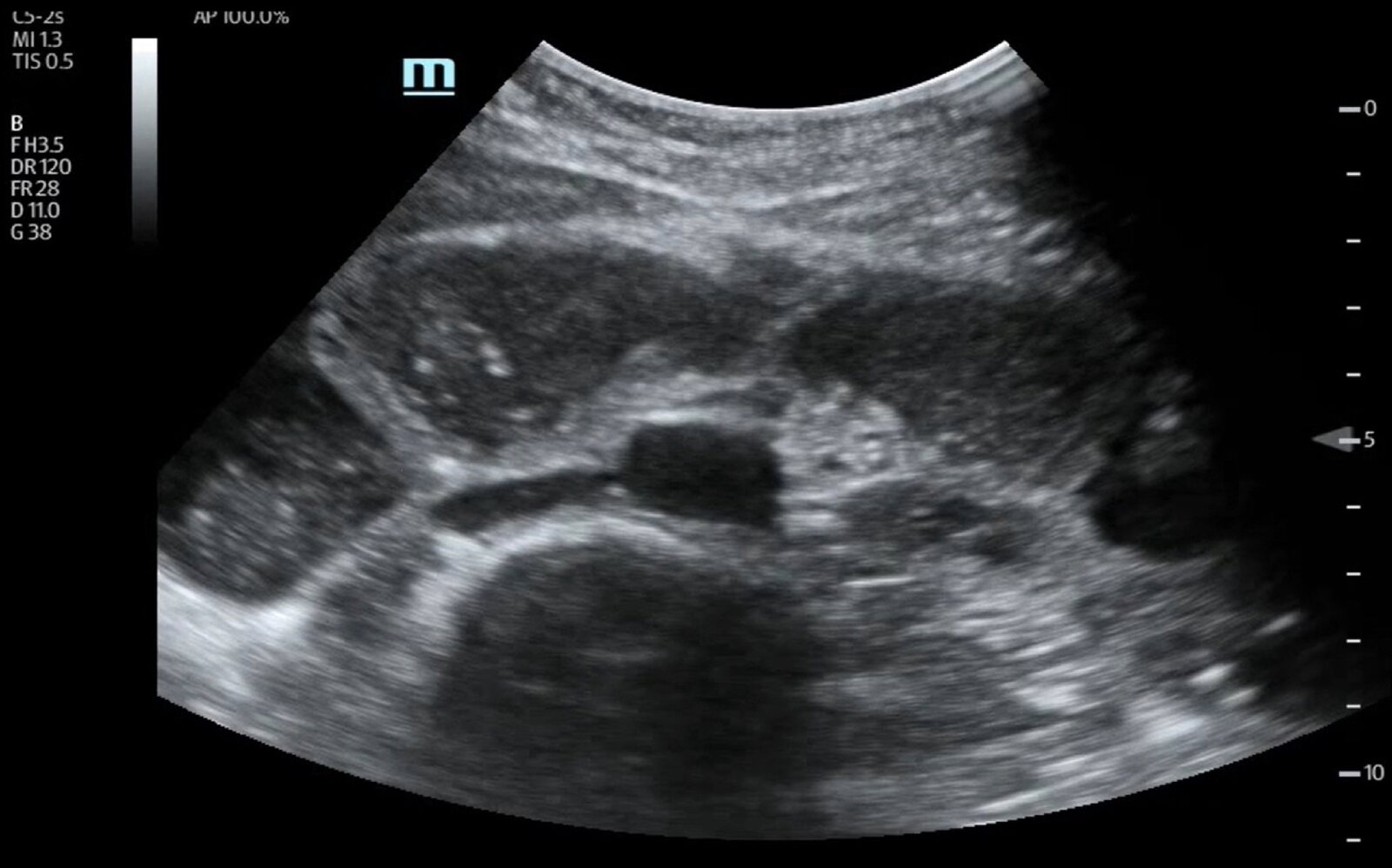
Ultrasound abdomen (transverse plane) of a patient with a one-day history of abdominal pain, vomiting, and constipation
Dilated loops of small bowel (green overlay) measuring > 3 cm in diameter are filled with echogenic material.
Ao: aorta; IVC: inferior vena cava; S and white outline: spine
Source: “Point of Care Ultrasound Illustrating Small Bowel Obstruction” by Badriah Alruwaili; Shadi Lahham, JETem, licensed under CC BY 4.0. Modifications: arrow + white line removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Ultrasound abdomen (left lower quadrant; oblique plane)
The plicae circulares (circumferential mucosal folds) can be seen as hyperechoic linear structures (green overlay) extending across the periphery of the anechoic fluid-filled loop of small bowel.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
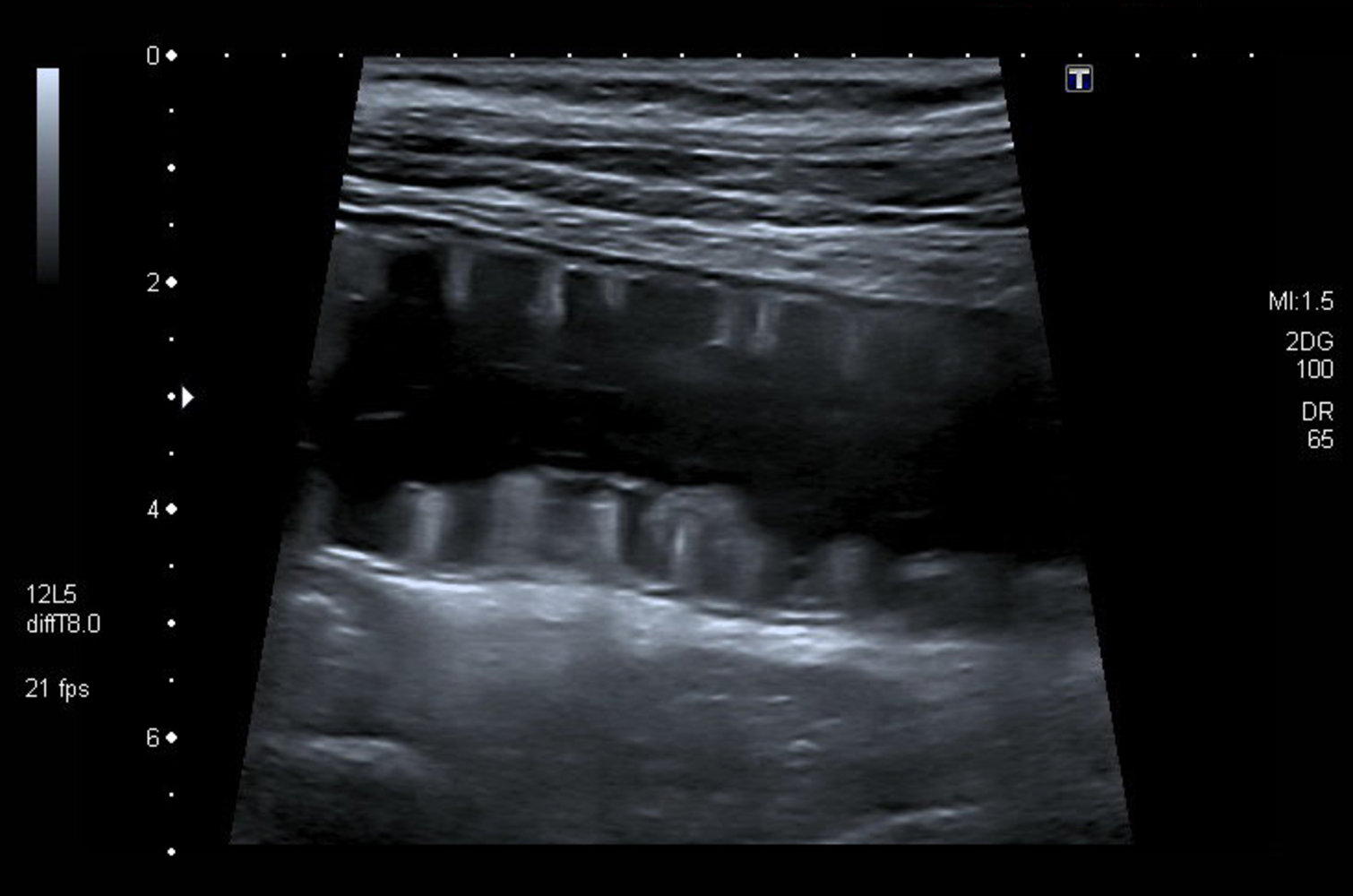
Ultrasound abdomen (small bowel loop; longitudinal plane)
The anechoic fluid-filled loop of small bowel is imaged through its center. The plicae circulares (circumferential mucosal folds) are seen as hyperechoic finger-like projections (green overlay), resembling the keys of a keyboard.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Fluoroscopy (single contrast barium enema; AP view; supine position)
As a result of axial torsion of the cecum, the barium column tapers (green overlay) until it eventually terminates at a point of complete obstruction (arrowhead). This appearance has been termed the “bird beak” sign. A featureless loop of gas-filled bowel in the left upper quadrant (white arrows) may represent the dilated cecum proximal to the point of obstruction.
Source: “Figure 2, in: Laparoscopic assisted right hemicolectomy for caecal volvulus” by Michael D Kelly, John Bunni, Anne M Pullyblank, World Journal of Emergency Surgery, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Fluoroscopy (barium enema; lateral view)
An apple core sign (also called napkin ring sign; green overlay) is seen in the distal descending colon. It is the result of annular constriction by a colorectal carcinoma.
Source: “Radiology apple core sign” by agarger, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Differential diagnoses
-
Differential diagnoses of mechanical bowel obstruction
- Paralytic ileus (see “Mechanical bowel obstruction vs. paralytic ileus”)
- Bowel perforation (secondary peritonitis)
- Mesenteric ischemia
- Inflammatory bowel disease
- Ovarian torsion
-
Differential diagnoses of SBO
- Acute appendicitis
- Acute pancreatitis
- Pelvic inflammatory disease
-
Differential diagnoses of LBO
- Diverticulitis
- Toxic megacolon
- Chronic megacolon
- Acute colonic pseudo-obstruction (Ogilvie syndrome)
- See also: “Differential diagnoses of acute abdomen.”
| Mechanical bowel obstruction vs. paralytic ileus | |||
|---|---|---|---|
| Mechanical bowel obstruction [1][3][28][29] | Paralytic ileus | ||
| Definition |
|
|
|
| Etiology |
|
|
|
| Clinical features |
|
|
|
| Findings on imaging |
|
|
|
References:[3][28][29][30]
The differential diagnoses listed here are not exhaustive.
Treatment
- See “Initial management of bowel obstruction” for first steps and supportive care.
- Definitive management: depends on the severity and etiology of the obstruction and clinical presentation of the patient
- Interventional management
- Surgery: Transfer the patient to the operating room or admit to a surgical ward depending on the urgency of surgical intervention.
- Endoscopic intervention: e.g., for the removal or fragmentation of foreign objects that are within reach of an endoscope
- Stool evacuation
- Nonoperative management: simple bowel obstruction with no evidence of complications (e.g., partial bowel obstruction or postoperative ileus)
- Identify and treat the underlying cause (see “Etiology”).
- Interventional management
Interventional management
Surgery [3][5][9][13][31]
-
Indications
- Complicated bowel obstruction (i.e., signs of ischemia, perforation, or clinical deterioration)
- Closed-loop bowel obstruction
- Suspected bowel obstruction in patients presenting with hemodynamic instability refractory to initial fluid resuscitation
- Failure of nonoperative management (i.e., no improvement after 3 days of NOM; clinical deterioration/development of complications during NOM) [9][13][32]
- Underlying etiology necessitates surgical intervention (e.g., surgery for inguinal hernia; enterolithotomy for gallstone ileus)
-
Procedure: exploratory laparotomy
- Management of the obstruction (e.g., adhesiolysis, hernia reduction, cecopexy, tumor resection)
- Resection of gangrenous bowel with restoration of intestinal transit or creation of a stoma


Endoscopic intervention [6][33][34]
Endoscopic interventions can be considered for bowel obstruction with no signs of strangulation or perforation. Rigid or flexible sigmoidoscopy, upper GI endoscopy, or colonoscopy under procedural sedation can be used for endoscopic investigation for the following indications.
- Sigmoid volvulus: Attempt endoscopic decompression, detorsion, and reduction.
- Intraluminal bowel obstruction that is within reach of an endoscope: fragmentation or removal
- Inoperable malignant bowel obstruction: Consider placement of stents and decompression tubes.
Stool evacuation [35]
- Indication: simple bowel obstruction caused by fecal impaction
-
Procedures
- The specific procedure is chosen based on the site of fecal impaction, only after bowel perforation has been definitively ruled out.
- Manual disimpaction
- Distal softening or washout with enemas or suppositories
- Proximal softening or washout with oral solutions such as polyethylene glycol or sodium phosphate
- See “Treatment of fecal impaction” for details and dosages.
- The specific procedure is chosen based on the site of fecal impaction, only after bowel perforation has been definitively ruled out.
- Important consideration: Identify and manage the underlying cause of constipation that led to fecal impaction.
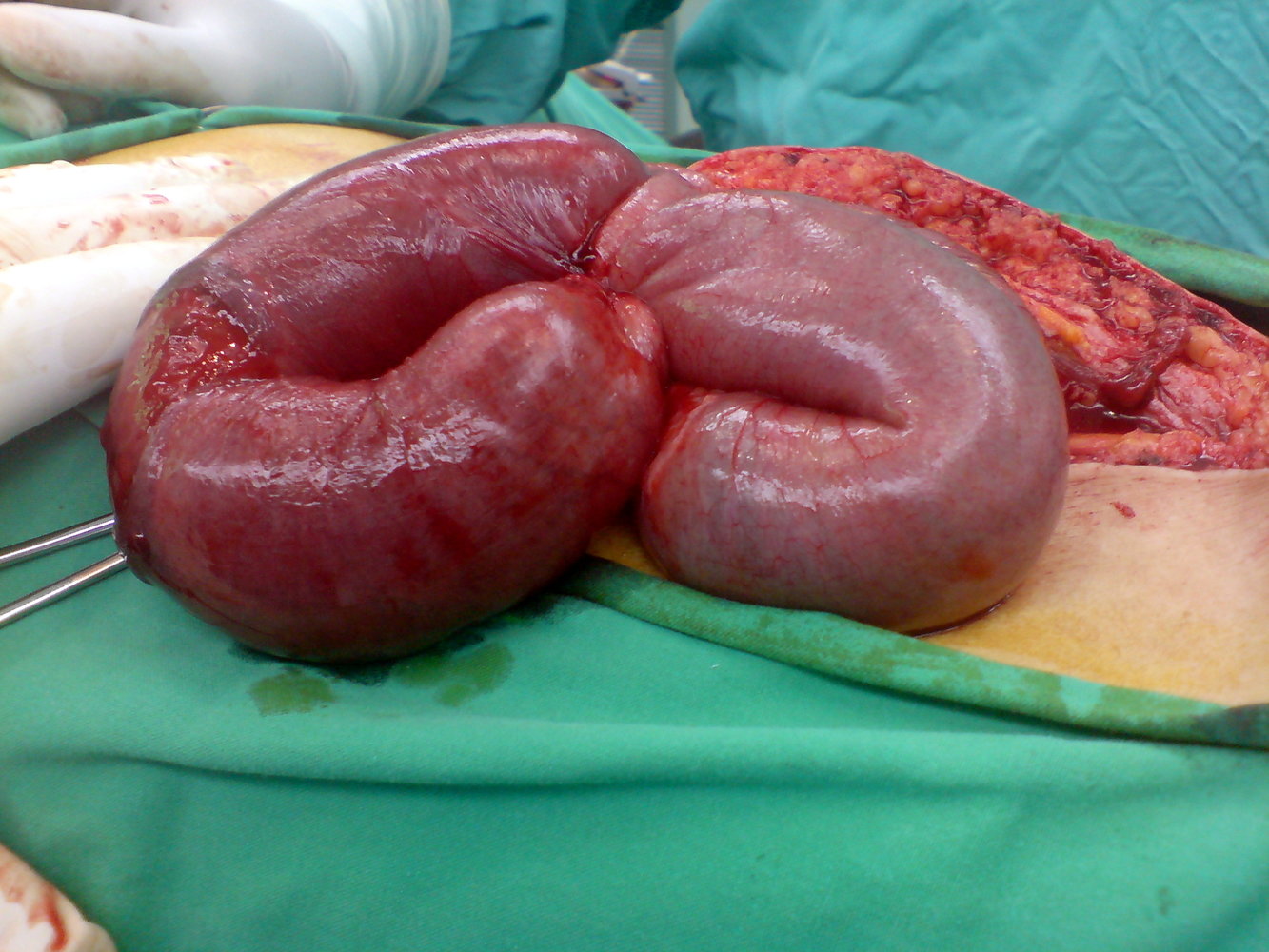
Intraoperative photograph of a patient presenting with mechanical bowel obstruction due to adhesions
The bowel loops appear edematous, distended, and congested. In the bowel loop on the left, the maroon discoloration and sloughing off of the serosal layer in patches are signs of gangrene.
This is the typical intraoperative appearance of strangulated bowel loops.
Source: “Intestinal Obstruction” by Haitham alfalah, Wikimedia Foundation, licensed under CC BY-SA 3.0.
{kind=link}

Intraoperative photograph of a patient with mechanical small bowel obstruction secondary to adhesions
Most of the visible small bowel appears hyperemic and congested. The bowel loops toward the right side of the image have a mottled red-black discoloration indicating gangrenous changes. A normal pink bowel loop is visible in the background.
Source: “Ileus2” by THWZ, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
Nonoperative management
Indications [5][6][9][13]
- Early postoperative bowel obstruction (i.e., within 6 weeks of abdominal surgery) [12]
- Partial bowel obstruction with no evidence of complications
- Consider in patients with complete SBO and no evidence of complications. [5][9][13]
Contraindications [5]
- Complicated bowel obstruction (e.g, peritoneal signs, signs of strangulation)
- Refractory metabolic acidosis
- Significant leukocytosis (> 18,000/mm3)
- Significant cecal dilation
Initial measures
- Bowel rest (NPO)
-
Supportive care
- IV fluid therapy (initial fluid resuscitation followed by maintenance fluid therapy)
- Electrolyte repletion
- Parenteral analgesics (nonopioid analgesics are preferred) [36][37]
- Parenteral antiemetics as needed
Peristalsis-inducing medications (i.e., prokinetic agents such as metoclopramide) are contraindicated in complete mechanical bowel obstruction.
Prophylactic antibiotic therapy is not routinely indicated for simple bowel obstruction that is being managed nonoperatively. [38]
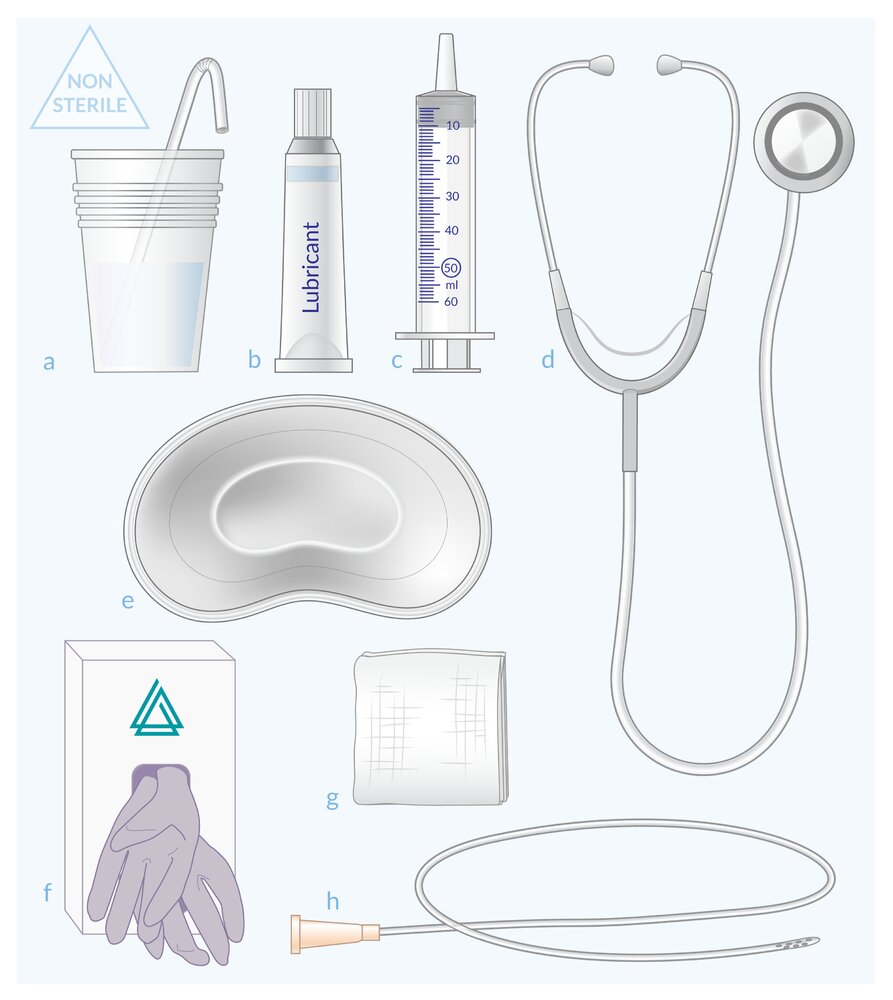
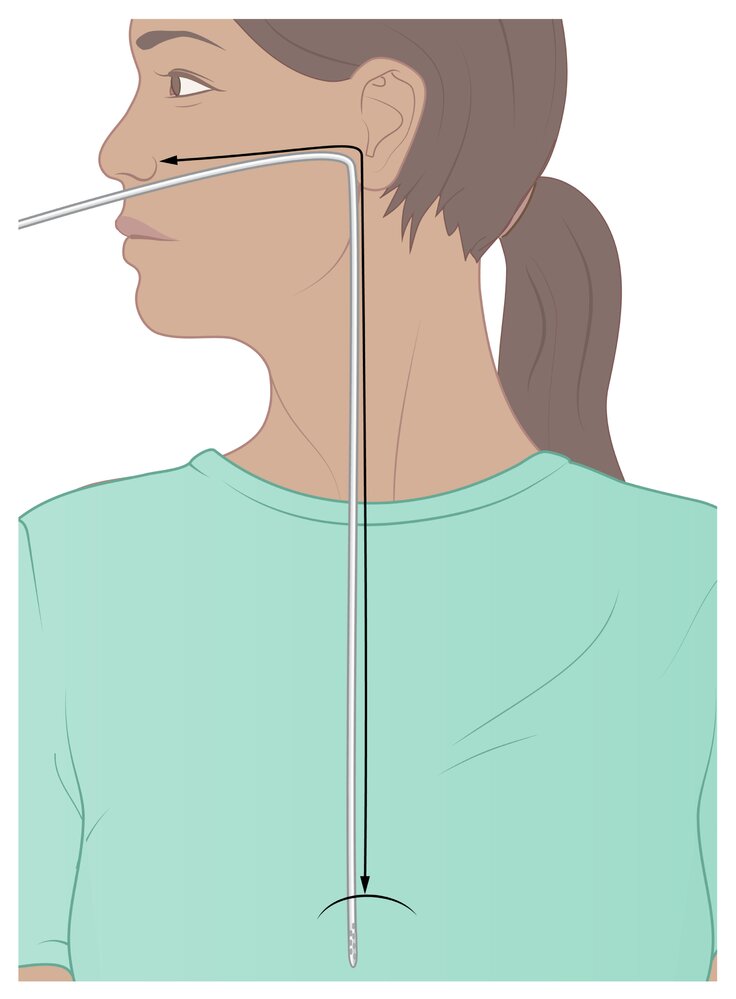
Nasogastric tube insertion (bowel decompression)
-
Indications: not routinely required but should be considered in the following situations [39][40]
- Persistent vomiting
- Significant upper GI distention
- Complete bowel obstruction
- Volvulus
- Procedure: See “Nasogastric tube placement.”



Serial monitoring
- Symptom severity
- Bowel movements
- Serial abdominal examination every 4–8 hours [12][13]
- Fluid balance (input and output chart) including nasogastric tube output [3]
Duration of nonoperative management trial [5][13][32][41]
- No longer than 72 hours
- Some authors suggest trialing NOM for a maximum of 5 days.
- Continuing nonoperative management for > 72 hours does not decrease the need for surgery but does increase surgical morbidity. [3]
Assessment of response and further management
| Assessment of response to NOM and further management | |||
|---|---|---|---|
| Response | Clinical features | Supportive evidence | Further management |
| Clinical improvement |
|
|
|
| Deterioration [13] |
|
|
|
| Lack of improvement (no evidence of complications) |
|
|
|
© AMBOSS
© AMBOSS
© AMBOSS
Complications
- Bowel ischemia
- Bowel perforation
- Peritonitis
A change in the character of pain (colicky pain becoming continuous), rebound tenderness on examination, and/or signs of sepsis in a patient with bowel obstruction indicate the onset of complications and necessitate emergency surgical intervention.
We list the most important complications. The selection is not exhaustive.
Prognosis
- Mortality rate in untreated intestinal strangulation: 100%
- High risk of recurrence , particularly with chronic or recurring etiologies
- 30-day readmission rate: 16%
- Mortality rate after delayed treatment of closed-loop obstruction: 35%
References:[5]
External Resources
References
- Griffiths S, Glancy DG. "Intestinal obstruction". Surgery. 35(3). :3
- Diamond M, Lee J, LeBedis CA. "Small Bowel Obstruction and Ischemia". Radiol Clin North Am. 57(4). :689-703. (2019)
- Jackson P, Vigiola Cruz M. "Intestinal Obstruction: Evaluation and Management". Am Fam Physician. 98(6). :362-367. (2018)
- Jaffe T, Thompson WM. "Large-Bowel Obstruction in the Adult: Classic Radiographic and CT Findings, Etiology, and Mimics". Radiology. 275(3). :651-663. (2015)
- Rami Reddy SR, Cappell MS. "A Systematic Review of the Clinical Presentation, Diagnosis, and Treatment of Small Bowel Obstruction". Curr Gastroenterol Rep. 19(6). :28. (2017)
- Hayden GE, Sprouse KL. "Bowel Obstruction and Hernia". Emerg Med Clin North Am. 29(2). :319-345. (2011)
- "American College of Radiology ACR Appropriateness Criteria® Suspected Small-Bowel Obstruction". https://acsearch.acr.org/docs/69476/Narrative/. [2013-01-01]
- Pisano M, Zorcolo L, Merli C, et al. "2017 WSES guidelines on colon and rectal cancer emergencies: obstruction and perforation". World Journal of Emergency Surgery. 13(1). :36. (2018)
- Ten Broek RPG, Krielen P, Di Saverio S, et al. "Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group". World Journal of Emergency Surgery. 13(1). :24. (2018)
- Chang KJ, Marin D, Kim DH, et al. "ACR Appropriateness Criteria® Suspected Small-Bowel Obstruction". J Am Coll Radiol. 17(5). :S305-S314. (2020)
- Mian M, Swamy N, Angtuaco T. "Imaging in Acute Intestinal Obstruction". Contemporary Diagnostic Radiology. 42(24). :1-7. (2019)
- Chuong AM, Corno L et al. "Assessment of Bowel Wall Enhancement for the Diagnosis of Intestinal Ischemia in Patients with Small Bowel Obstruction: Value of Adding Unenhanced CT to Contrast-enhanced CT.". Radiology. 280(1). :98-107. (2016)
- Long B, Robertson J, Koyfman A. "Emergency Medicine Evaluation and Management of Small Bowel Obstruction: Evidence-Based Recommendations". J Emerg Med. 56(2). :166-176. (2019)
- Eisenberg RL, Johnson NM. "Comprehensive Radiographic Pathology - E-Book". Elsevier Health Sciences. (2015). ISBN: 9780323370257
- Maung AA, Johnson DC, Piper GL, et al. "Evaluation and management of small-bowel obstruction". Journal of Trauma and Acute Care Surgery. 73(5). :S362-S369. (2012)
- Li Z, Zhang L, Liu X, Yuan F, Song B. "Diagnostic utility of CT for small bowel obstruction: Systematic review and meta-analysis.". PLoS ONE. 14(12). :e0226740. (2019)
- Bower KL, Lollar DI, Williams SL, et al. "Small Bowel Obstruction". Surg Clin North Am. 98(5). :945-971. (2018)
- Cartwright SL, Knudson MP. "Diagnostic Imaging of Acute Abdominal Pain in Adults". American Academy of Family Physicians. 91(7). :452-9. (2015)
- Pourmand A, Dimbil U, Drake A, Shokoohi H. "The Accuracy of Point-of-Care Ultrasound in Detecting Small Bowel Obstruction in Emergency Department". Emergency Medicine International. 2018. :1-5. (2018)
- Taylor MR, Lalani N. "Adult Small Bowel Obstruction". Academic Emergency Medicine. 20(6). :527-544. (2013)
- Guttman J, Stone MB, Kimberly HH, Rempell JS. "Point-of-care ultrasonography for the diagnosis of small bowel obstruction in the emergency department". CJEM. 17(2). :206-209. (2015)
- Jang TB, Schindler D, Kaji AH. "Bedside ultrasonography for the detection of small bowel obstruction in the emergency department". Emerg Med J. 28(8). :676-678. (2010)
- Beyer D, Mödder U. "Diagnostic Imaging of the Acute Abdomen". Springer Berlin Heidelberg. (1988). ISBN: 9783642718861
- Abu-Zidan F, Hefny A, Corr P. "The role of ultrasound in the management of intestinal obstruction". J Emerg Trauma Shock. 5(1). :84. (2012)
- Alzaraa A, Krzysztof K, Uwechue R, Tee M, Selvasekar C. "Apple-core lesion of the colon: a case report". Cases J. 2(1). :7275. (2009)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Landercasper J, Cogbill TH, Merry WH, et al. "Long-term Outcome After Hospitalization for Small-Bowel Obstruction". Arch Surg. 128(7). :765-771. (1993)
- Batke, Cappell. "Adynamic Ileus and Acute Colonic Pseudo-Obstruction". The Medical Clinics of North America. 92. :649–670
- Nobie BA, Talavera F. "Small-Bowel Obstruction". WebMD. http://emedicine.medscape.com/article/774140-overview. [2015-01-20]
- Macaluso C, McNamara. "Evaluation and management of acute abdominal pain in the emergency department". International Journal of General Medicine. :789. (2012)
- Gavriilidis P, de’ Angelis N, Tobias A. "To Use or Not to Use Opioid Analgesia for Acute Abdominal Pain Before Definitive Surgical Diagnosis? A Systematic Review and Network Meta-Analysis". Journal of Clinical Medicine Research. 11(2). :121-126. (2019)
- Manterola C, Vial M, Moraga J, Astudillo P. "Analgesia in patients with acute abdominal pain". Cochrane Database of Systematic Reviews. (2011)
- Konishi T, Fujiogi M, Michihata N, et al. "Comparing outcomes of nonoperative treatment for adhesive small bowel obstruction with and without antibiotics.". J Infect Chemother. 27(5). :690-695. (2021)
- Fonseca AL, Schuster KM, Maung AA, Kaplan LJ, Davis KA. "Routine nasogastric decompression in small bowel obstruction: is it really necessary?". Am Surg. 79(4). :422-8. (2013)
- Berman DJ, Ijaz H, Alkhunaizi M, et al. "Nasogastric decompression not associated with a reduction in surgery or bowel ischemia for acute small bowel obstruction". Am J Emerg Med. 35(12). :1919-1921. (2017)
- Catena F, De Simone B, Coccolini F, et al. "Bowel obstruction: a narrative review for all physicians". World Journal of Emergency Surgery. 14(1). (2019)
- Keenan JE, Turley RS, McCoy CC, et al. "Trials of nonoperative management exceeding 3 days are associated with increased morbidity in patients undergoing surgery for uncomplicated adhesive small bowel obstruction". The journal of trauma and acute care surgery. 76(6). :1367-72. (2014)
- Gero D, Gié O, Hübner M, Demartines N, Hahnloser D. "Postoperative ileus: in search of an international consensus on definition, diagnosis, and treatment". Langenbecks Arch Surg. 402(1). :149-158. (2016)
- Di Saverio S, Coccolini F, Galati M, et al. "Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2013 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group". World Journal of Emergency Surgery. 8(1). :42. (2013)
- Harrison ME, Anderson MA, Appalaneni V, et al. "The role of endoscopy in the management of patients with known and suspected colonic obstruction and pseudo-obstruction". Gastrointest Endosc. 71(4). :669-679. (2010)
- Sugawa C. "Endoscopic management of foreign bodies in the upper gastrointestinal tract: A review". World Journal of Gastrointestinal Endoscopy. 6(10). :475. (2014)
- Obokhare I. "Fecal Impaction: A Cause for Concern?". Clin Colon Rectal Surg. 25(01). :053-058. (2012)
- Franke AJ, Iqbal A, Starr JS, Nair RM, George TJ. "Management of Malignant Bowel Obstruction Associated With GI Cancers". Journal of Oncology Practice. 13(7). :426-434. (2017)