Summary
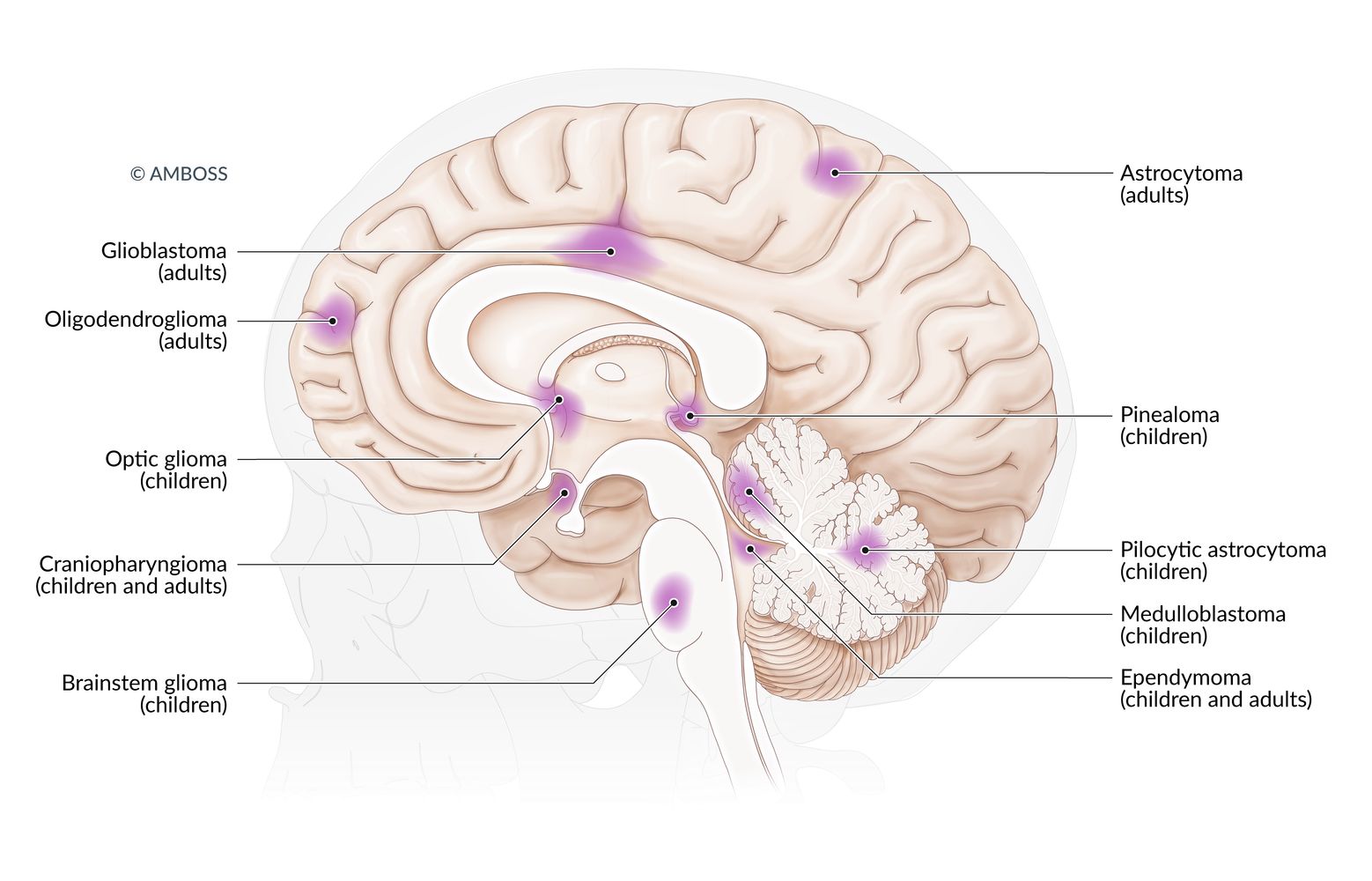
Brain tumors are masses of abnormal cells within the brain. They can be primary or metastatic, benign or malignant. Common tumors in children are pilocytic astrocytomas, medulloblastomas, ependymomas, and craniopharyngiomas. The most common brain tumors in adults are glioblastomas, meningiomas, hemangioblastomas, schwannomas, oligodendrogliomas, and pituitary adenomas. Clinical features and radiological findings vary according to the type, location, and onset of the tumor. Magnetic resonance imaging (MRI) is the primary diagnostic method. The histological grade of the tumor is an important factor in determining the prognosis. Removal of the entire tumor is a prerequisite for remission. Malignant tumors usually require additional treatment with radiotherapy and/or chemotherapy.
Meningiomas, pituitary adenomas, schwannomas, and neoplastic meningitis are discussed in separate articles.
Epidemiology
- Approx. 30% of brain tumors are primary brain tumors, while approx. 70% are metastases.
- Approx. 40% of primary brain tumors are benign.
- Sex: ♂ > ♀ (except meningiomas, which occur more frequently in women) [1]
Epidemiological data refers to the US, unless otherwise specified.
Approach
Initial evaluation [2]
Clinical assessment
- Obtain a thorough patient history and neurological examination.
- Suspect a brain tumor in patients with clinical features including:
- Headaches (especially with headache red flags)
- Other signs of elevated intracranial pressure (ICP), e.g., papilledema
- New onset seizures [3]
- Focal neurological deficits; depending on tumor location, e.g., sensory deficits
- Nonfocal neurological deficits
- Cognitive, behavioral, and personality changes
Symptom onset in patients with primary brain tumors is usually insidious, while symptom onset in patients with brain metastases is typically acute or subacute.
Diagnostic testing
- Obtain neuroimaging.
- Gadolinium-enhanced MRI head: preferred
- CT head and neck with IV contrast: if MRI is not possible
- Further testing depends on imaging findings.
- Findings suggestive of primary brain tumor: Consult neurosurgery for diagnostic confirmation, e.g., via brain biopsy or resection
- Findings suggestive of metastatic brain tumor
- Initiate diagnostics of cancer of unknown primary.
- Obtain biopsy of the brain metastasis if primary is not identified. [4]
Overview of MRI findings in brain tumors
- There is significant overlap between MRI findings in common primary brain tumors (e.g., gliomas) and brain metastases.
- Brain tumors typically appear hypointense to isointense on T1-weighted images and hyperintense to isointense on T2-weighted images.
| Overview of MRI findings in brain tumors | ||||
|---|---|---|---|---|
| MRI findings | ||||
| Tumor type | Typical location | Other findings | ||
| Pilocytic astrocytoma [5] |
|
|
||
| Anaplastic astrocytoma [6] |
|
|
||
| Glioblastoma multiforme [7] |
|
|
||
| Primary CNS lymphoma [8][9] |
|
|
||
| Meningioma [10] |
|
|
||
| Metastasis [11][12][13] |
|
|
||



")
")





Management
Principles of treatment
Management should be specialist guided; utilize a multidisciplinary approach and consult a tumor board if available.
-
Management of metastatic brain tumor
- Identify and treat primary malignancy.
- See “Brain metastases” for details on treatment options.
-
Management of primary brain tumor
- Based on both tumor and patient characteristics
- May include:
- Maximal safe surgical resection
- Radiation therapy: e.g., standard fractionated external beam radiation therapy
- Systemic therapy: e.g., chemotherapy, cancer immunotherapy
- Offer clinical trial enrollment and consider palliative care for patients with high-grade tumors (e.g., glioblastoma multiforme).
Management of complications of brain tumors [2]
See also ”Cancer-related complications” and “Cancer treatment-related complications.”
-
Venous thromboembolism (VTE) [14][15]
- Consider pharmacological VTE prophylaxis for select patients.
- Offer therapeutic anticoagulation for patients with VTE (LMWH is the preferred agent).
- Patients with brain tumors are at increased risk of intracerebral hemorrhage; use shared decision-making for anticoagulation treatment decisions.
-
Seizures [16][17]
- Primary prophylaxis is not recommended.
- Secondary prophylaxis (i.e., history of seizures): Initiate treatment of epileptic seizures. [18]
-
Vasogenic cerebral edema
- Administer glucocorticoids (e.g., dexamethasone ) for patients with signs of elevated ICP. [19][20]
- Follow local treatment protocols when available.
Certain types of metastatic brain tumor (e.g., melanoma, renal cell carcinoma) are more likely to hemorrhage, but are not an absolute contraindication to therapeutic anticoagulation. [16]
Taper and discontinue perioperative prophylactic medications within 7–10 days of surgery, unless otherwise indicated. [2]
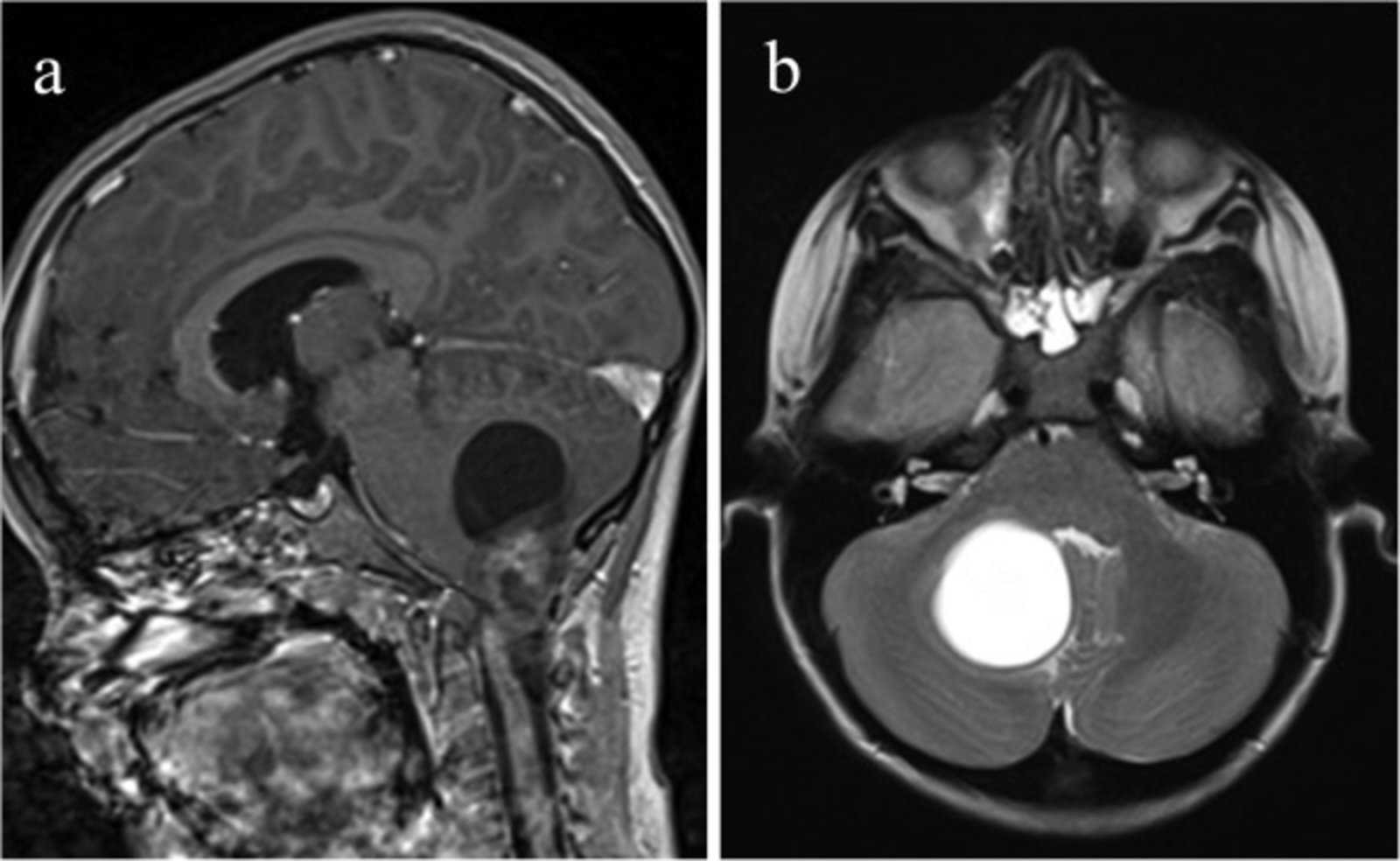
MRI head (a: T1-weighted; with contrast; sagittal plane; b: T2-weighted; axial plane) of a child
A large lesion in the right cerebellar hemisphere displaces the vermis to the left of midline. It has a large cystic component (T1 hypointense and T2 hyperintense; red overlay) and a heterogeneously enhancing solid nodular component (green overlay).
Cerebellar pilocytic astrocytoma frequently manifests as a large cystic lesion with an enhancing mural nodule.
Source: “Figure 1, in: The Journal of Headache and Pain” by Irene Toldo, Debora De Carlo, Rodica Mardari et al., The Journal of Headache and Pain, licensed under CC BY 2.0. Modifications: - Labels have been removed from original image (asterix and two arrows). - letters edited. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
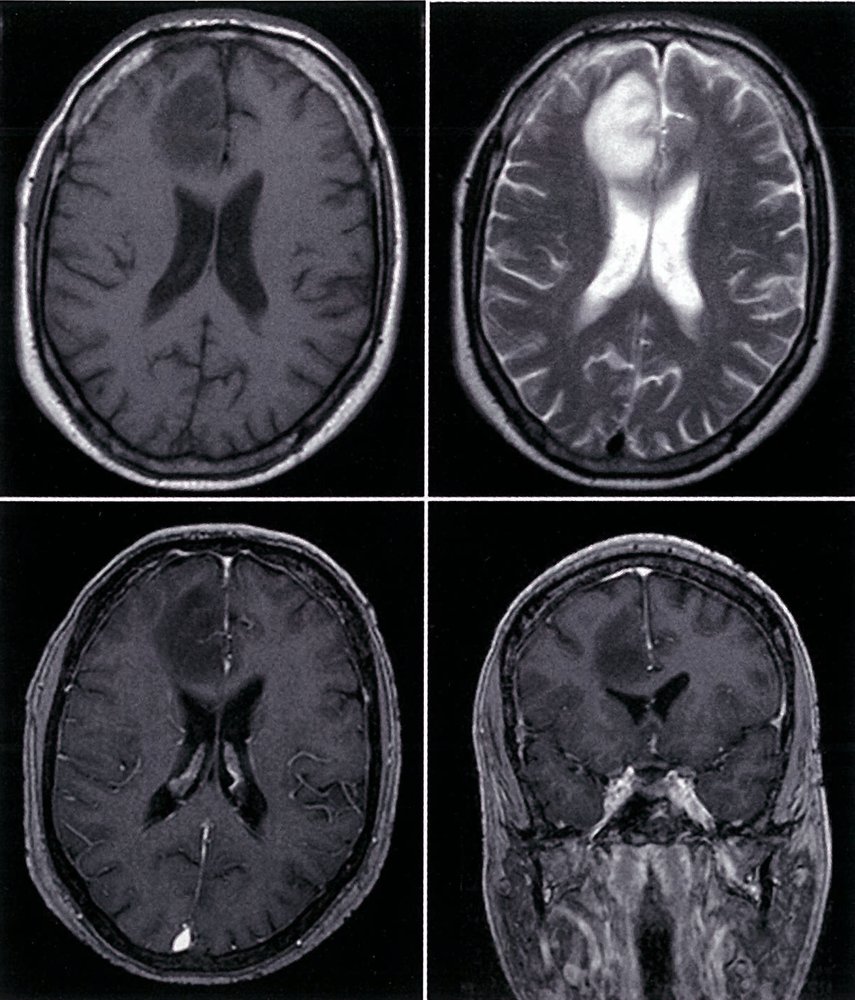
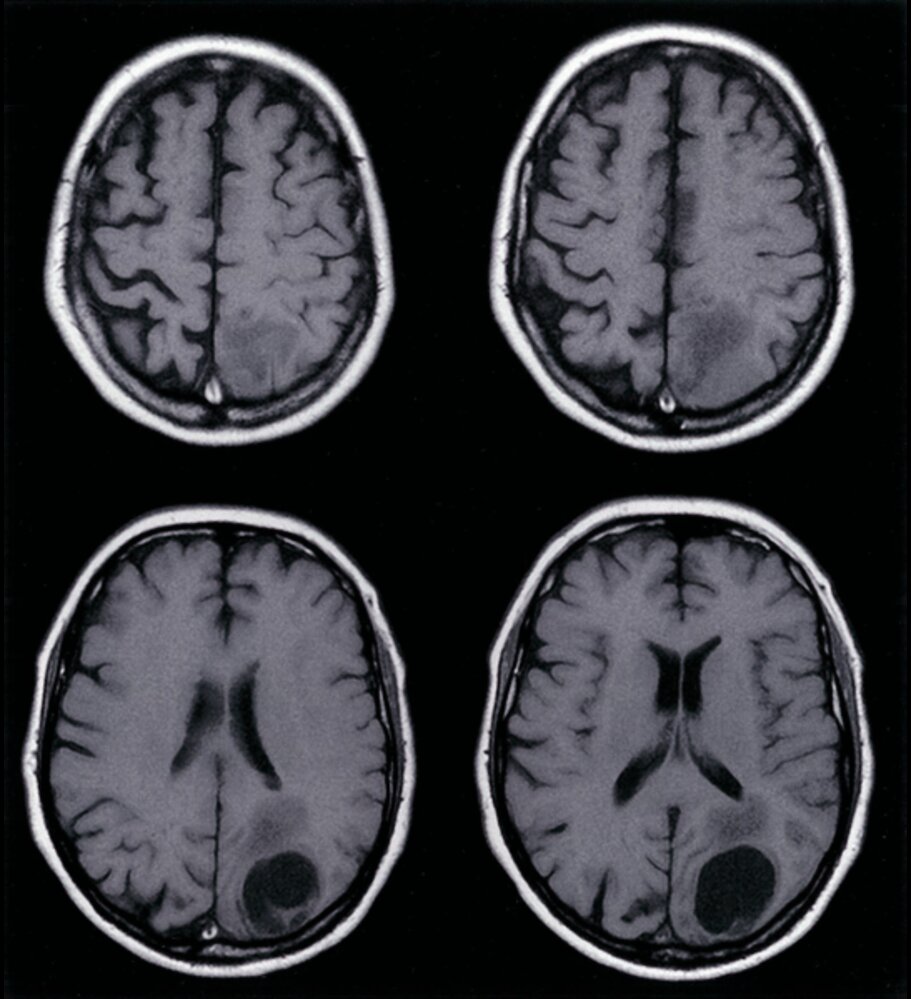
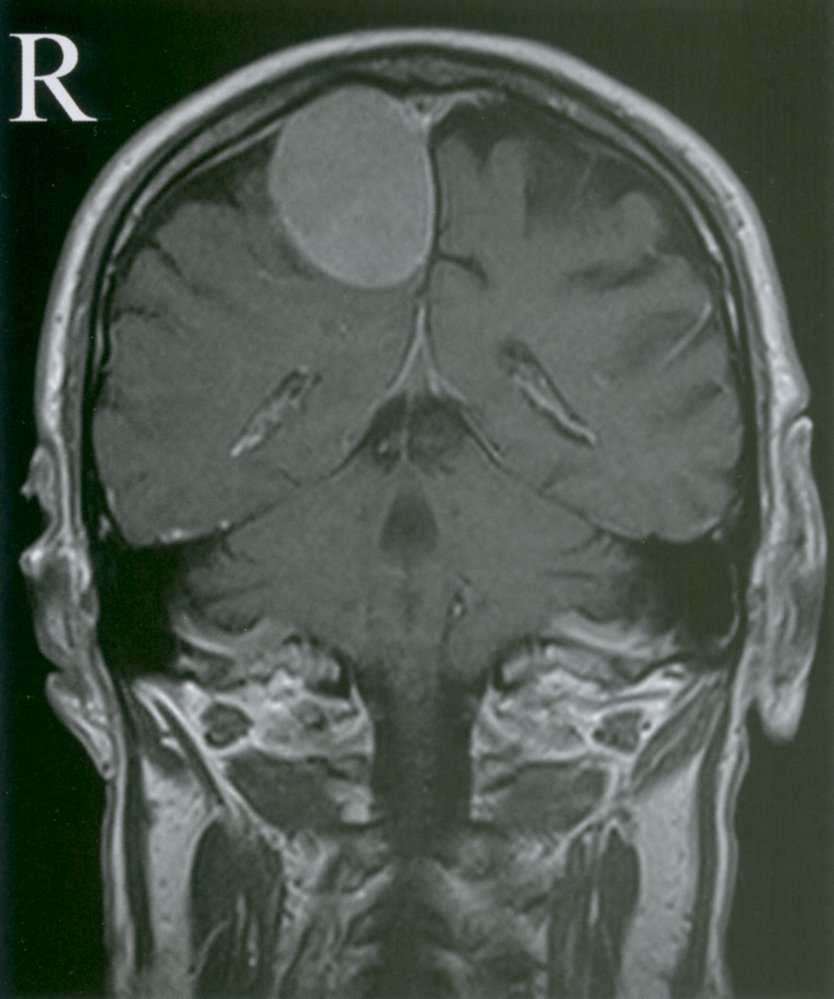
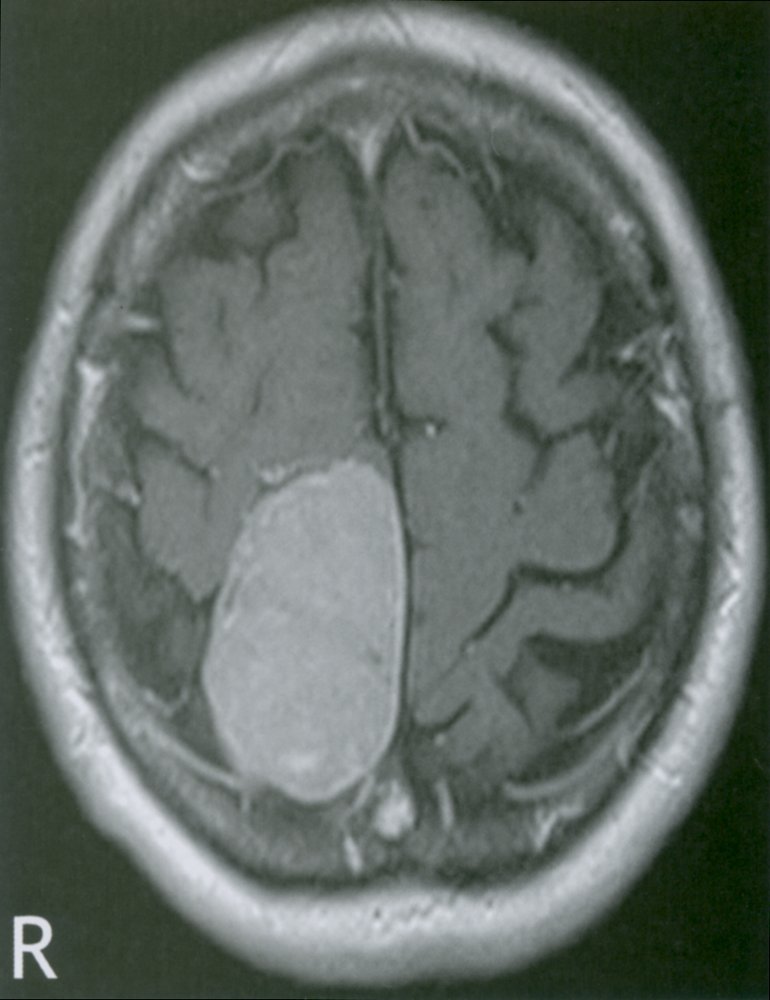
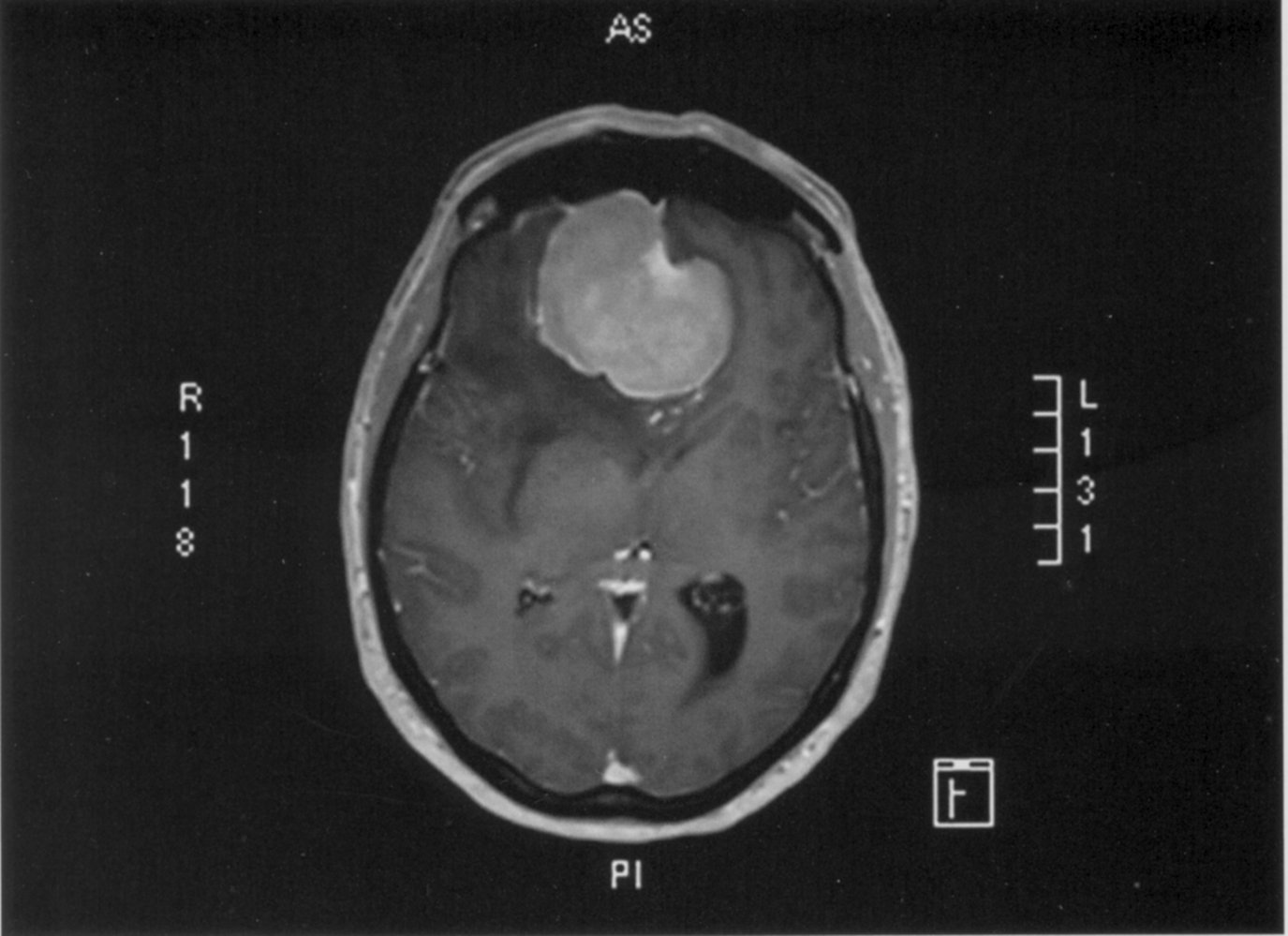
MRI head (top left: T1-weighted, axial plane; top right: T2-weighted, axial plane; bottom left: T1-weighted, with contrast, axial plane; bottom right: T1-weighted, with contrast, coronal plane)
There is a large, well-defined mass in the right frontal lobe (green overlay), which demonstrates hypointense signal on the T1-weighted images and hyperintense signal on T2-weighting with no significant surrounding edema. No significant enhancement is demonstrated on the post-contrast sequences.
Source: © IMPP
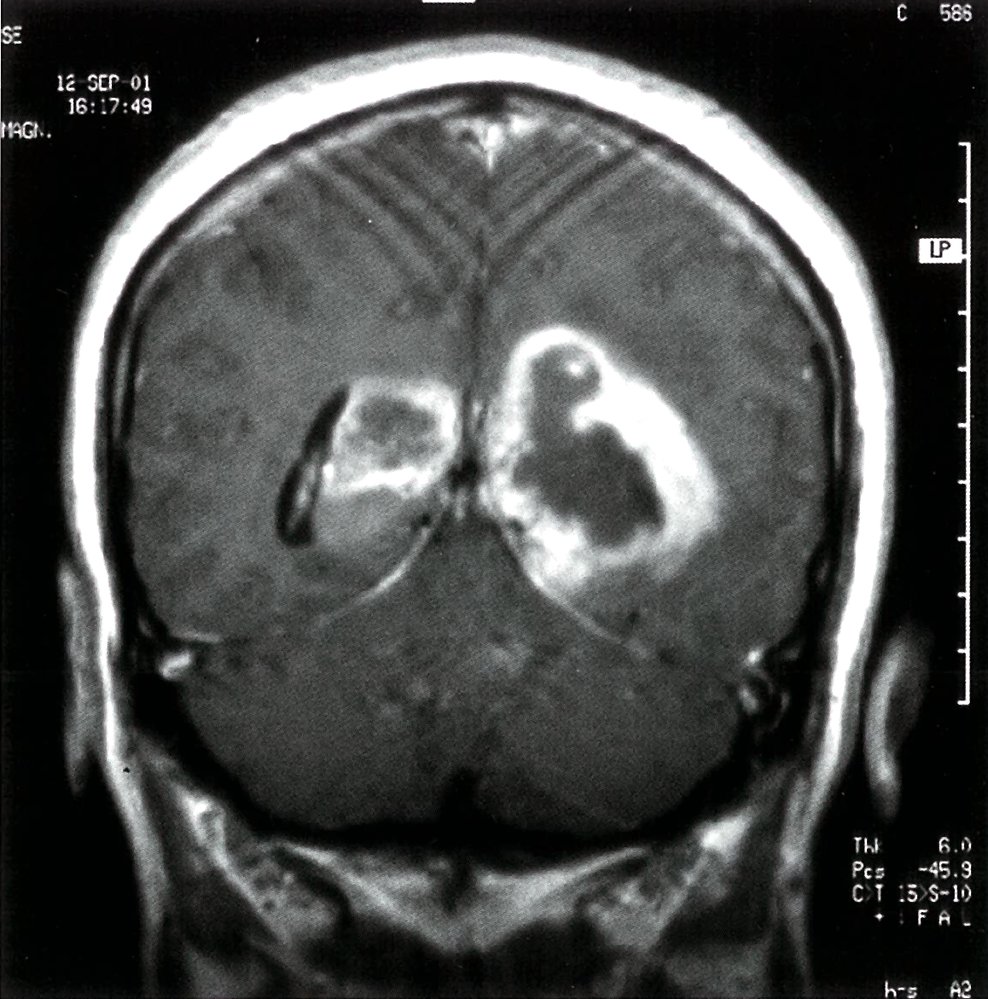
T1-weighted contrast-enhanced MRI, frontal view: bihemisphere garland-like contrast enhancement. There is peripheral contrast agent enhancement (blue overlay) with central necrosis (green overlay). The third ventricle (arrowhead) is centrally located. The tumor is displacing the posterior horn of the lateral ventricle (red overlay). Diagnosis: bilateral glioblastoma (butterfly glioma).
Source: © IMPP
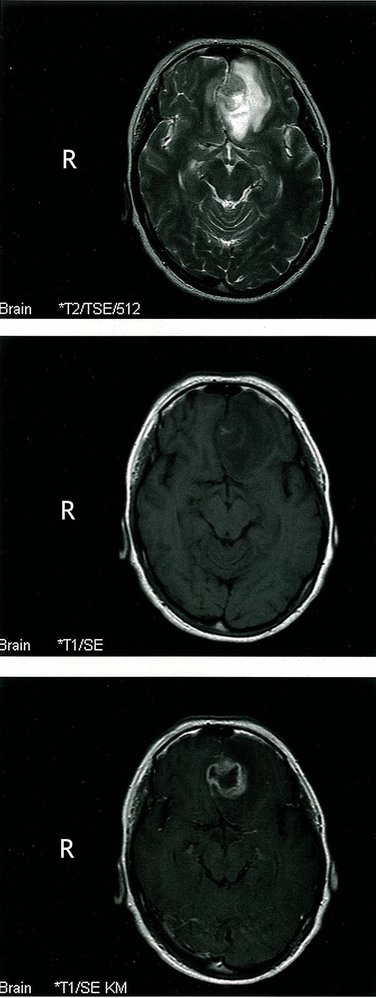
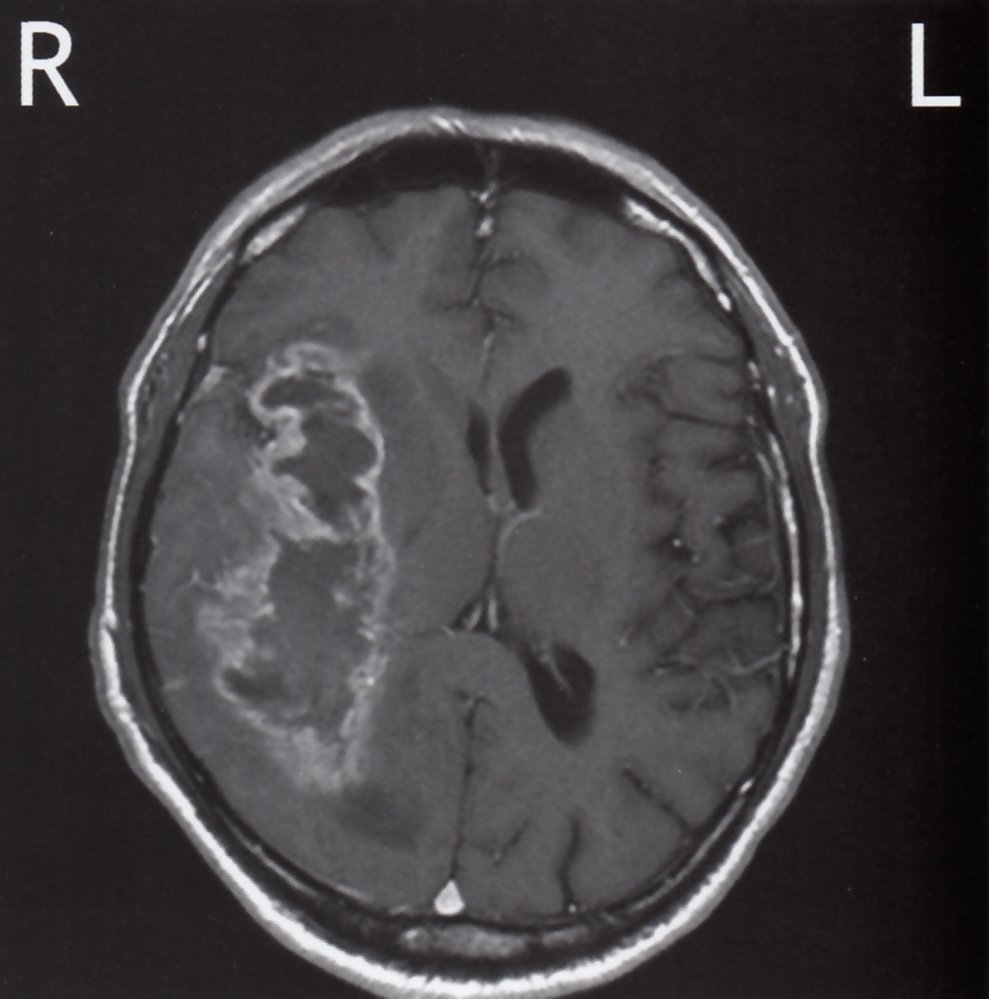
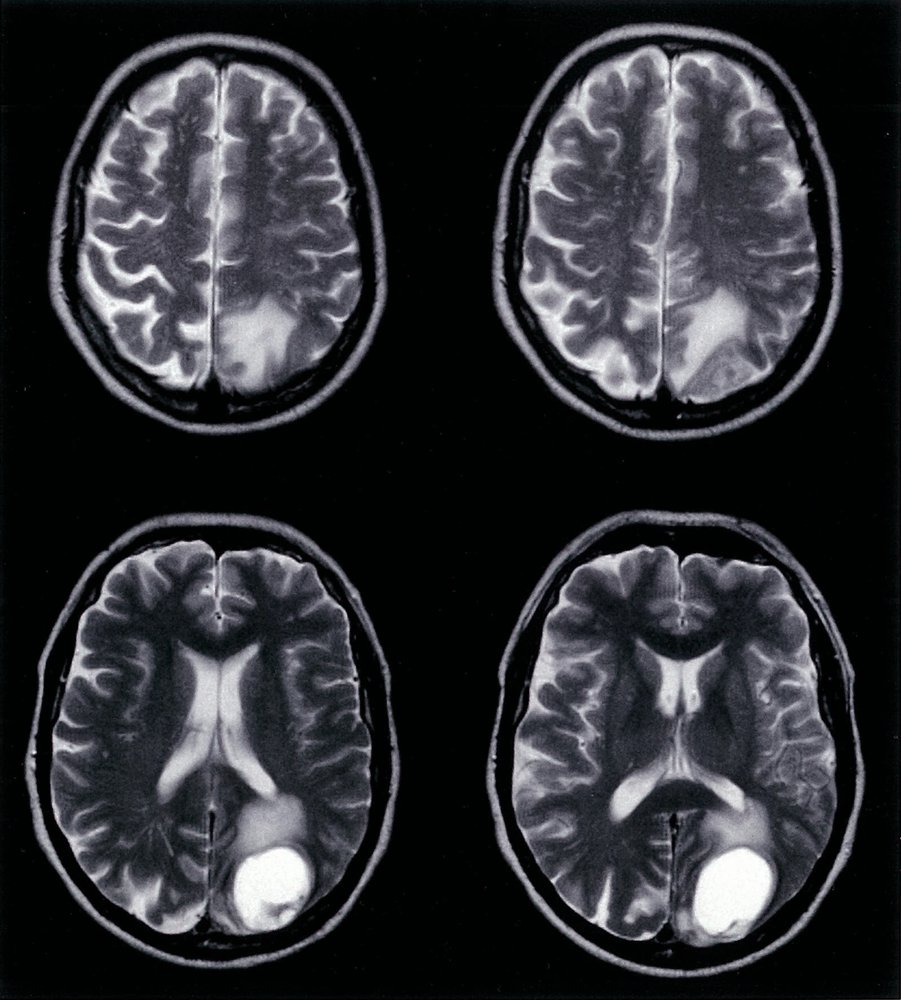
MRI head (top: T2-weighted; middle: T1-weighted without contrast; bottom: T1-weighted with contrast; axial plane)
A heterogeneous lesion in the left frontal lobe distorts the interhemispheric fissure (indicated by white arrowhead). On the T1-weighted sequences, the lesion is predominantly hypointense (green overlay) with garland-like enhancement (yellow overlay). Associated edema is hyperintense on the T2-weighted sequence (red overlay).
Source: © IMPP
MRI brain (T1-weighted; with contrast; axial plane) of a 69-year-old patient with personality changes and left-sided hemiparesis.
In the white matter of the right hemisphere, there is a large, poorly circumscribed space-occupying lesion, which is hypointense centrally (green overlay) with strong peripheral contrast enhancement (red overlay). The lesion is surrounded by edema (white overlay), suggesting rapid growth and displacement of surrounding structures. The mass effect has also caused a slight midline shift to the contralateral side (white dashed line), and compression of the right lateral ventricle (white arrowheads indicate anterior horn compression).
These radiographic features are typical of a glioblastoma.
Source: © IMPP
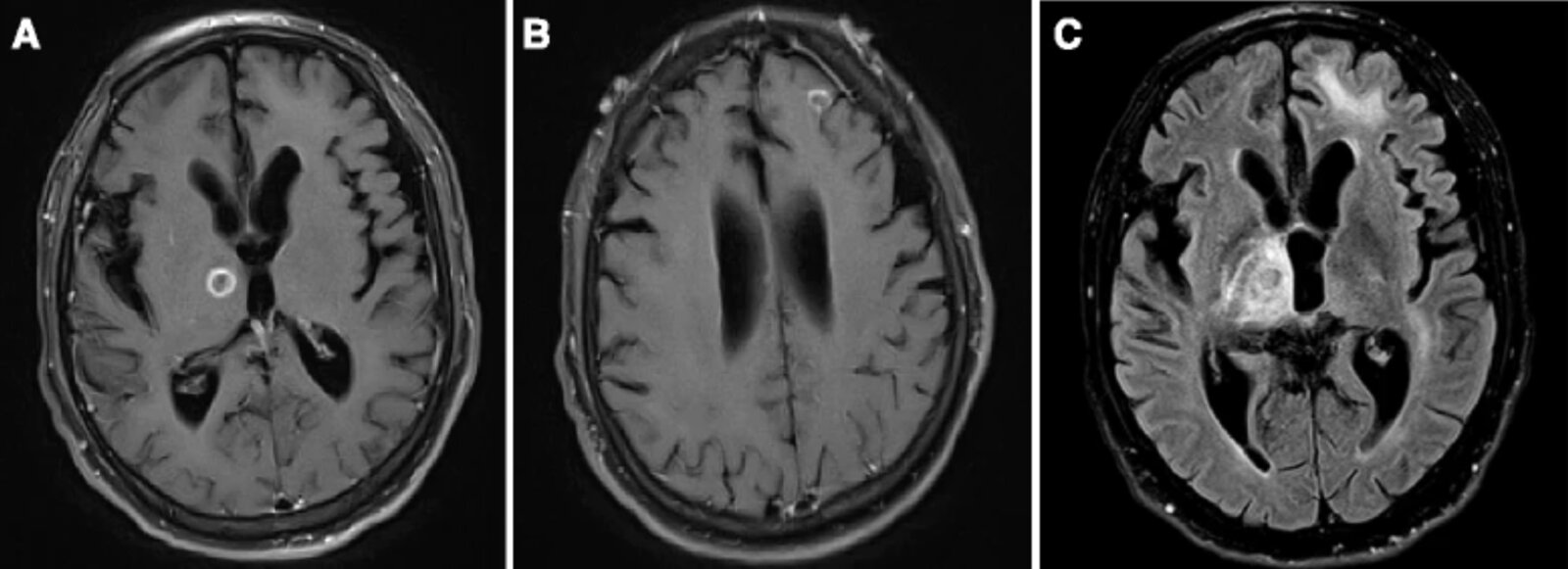
MRI head (A and B: T1-weighted, with contrast; C: FLAIR; axial plane) of a patient with HIV-associated primary CNS lymphoma
Ring-enhancing lesions in the right thalamus (A) and left frontal lobe (B) have central, low-signal intensity (hatched green overlay), suggesting necrosis. Hyperintense edema (green overlay) surrounds both lesions on the FLAIR sequence. Prominent sulci and ventricles reflect mild, generalized cerebral volume loss.
Toxoplasmosis and primary CNS lymphoma in patients with HIV/AIDS can have similar appearances, and further workup is needed if MRI cannot distinguish between them.
Source: “Fig. 1, in: An unusual and challenging case of HIV-associated primary CNS Lymphoma with Hodgkin-like morphology and HIV encephalitis” by Isaac E. Lloyd, Parker W. Clement, Karen L. Salzman, Randy L. Jensen, Mohamed E. Salama & Cheryl A. Palmer, Diagnostic Pathology, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
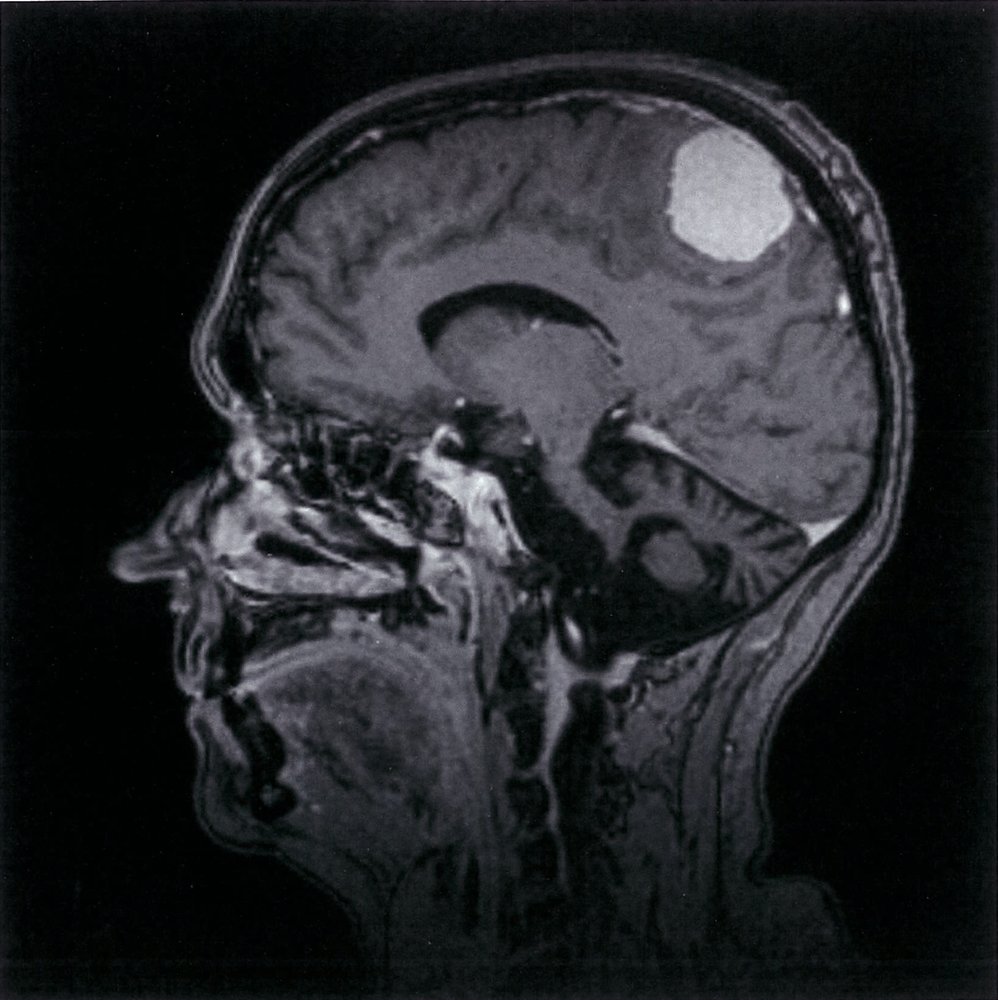
MRI head (T1-weighted; with contrast; sagittal plane)
There is a well-circumscribed homogeneous mass (green overlay) along the cerebral convexity. It demonstrates intense, homogeneous enhancement, equivalent to that of adjacent dura mater. Displacement without invasion of the surrounding white matter supports an extra-axial location.
This is a case of meningioma, a dural-based tumor. The dura is represented in this image by the thin, discontinuously enhancing line covering the inner surface of the skull (indicated by arrowhead).
Source: © IMPP
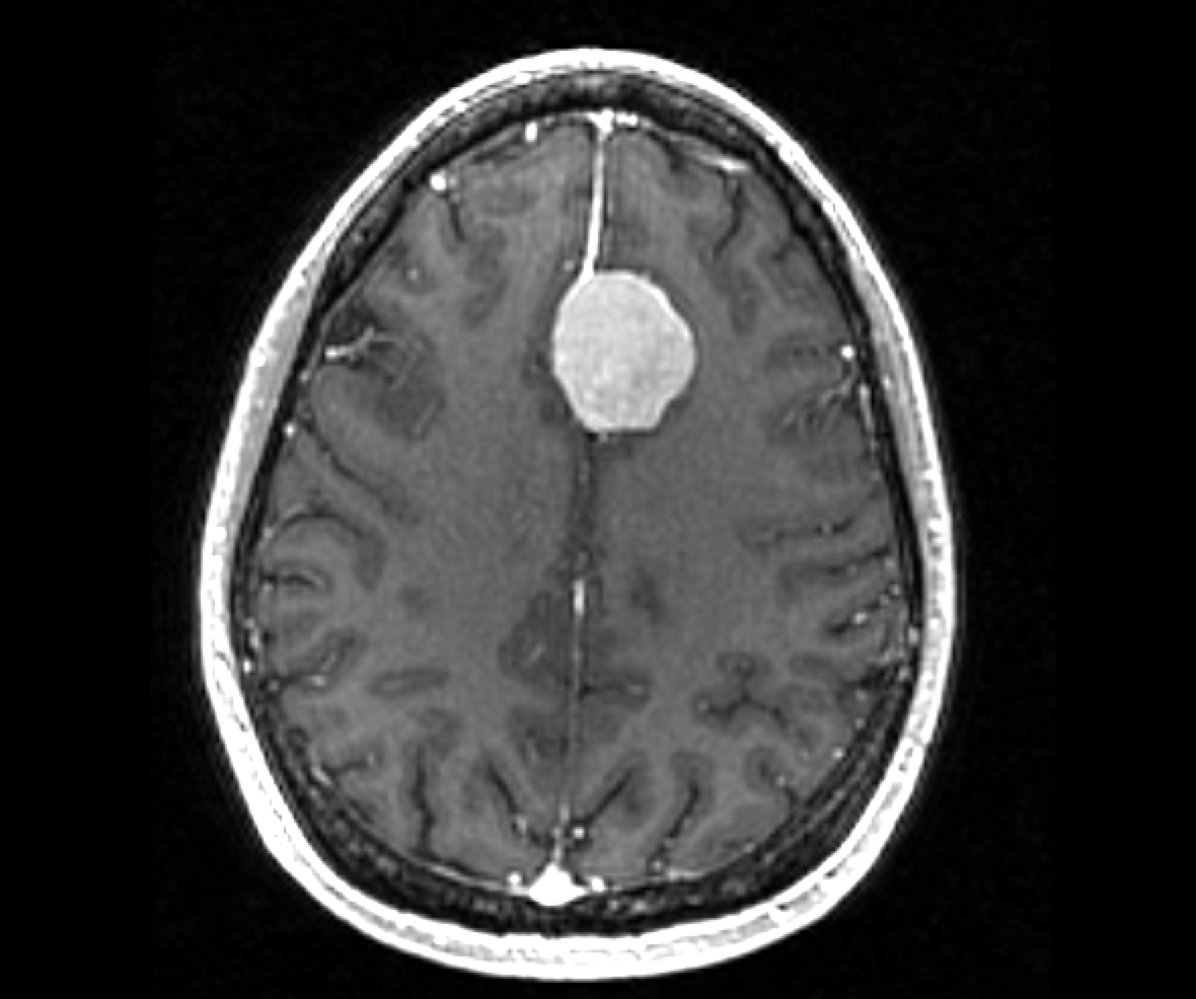
Cranial MRI, axial view (T1-weighted; with contrast)
Round, sharply delimited, homogeneously enhancing, hyperintense lesion (snowball appearance) in the interhemispheric region of the frontal lobe (green overlay).
The lesion displaces brain tissue. The dura is connected to the meninges of the frontal bone (dural tail sign) by a thick, hyperintense strand. A thin rim separates the lesion from surrounding brain parenchyma (CSF cleft sign).
These are characteristic radiologic features of a meningioma.
Source: “MeningiomaMRISegmentation” by Rkikinis, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: cropped image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
MRI head (T1-weighted; without contrast; axial plane) of a patient with lung carcinoma
A solitary, well-circumscribed, predominantly hypointense mass (hatched overlay) in the left occipital lobe is accompanied by perifocal edema (green overlay).
The lesion is consistent with a cerebral metastasis.
Source: © IMPP
MRI head (T2-weighted; without contrast; axial plane) of a patient with lung carcinoma
A solitary, well-circumscribed, predominantly hyperintense mass (hatched overlay) in the left occipital lobe is accompanied by perifocal edema (green overlay).
The lesion is consistent with a cerebral metastasis.
Source: © IMPP
Primary brain tumors
Classification
Primary brain tumors arise within the CNS and are classified based on the growth characteristics and cell type from which the tumor arises.
By the spreading potential
| Types of brain tumors by growth characteristics | ||
|---|---|---|
| Low-grade brain tumors | High-grade brain tumors | |
| WHO grade | I–II | III–IV |
| Borders | Well-defined | Poorly-defined |
| Spreading potential | Low | High |
| Recurrence | Rare | Frequent |
By the cell type
- Gliomas (e.g., astrocytomas and oligodendrogliomas)
- Choroid plexus tumors (e.g., choroid plexus papilloma, choroid plexus carcinoma)
- Neuronal and mixed neuronal-glial tumors (e.g., paraganglioma, central neurocytoma)
- Meningiomas (see “Classification of meningiomas”)
- Embryonal neuroectodermal tumors (e.g., medulloblastoma: , CNS neuroblastoma)
- Pituitary tumors: a group of tumors that arise from the pituitary gland (e.g., pituitary adenoma, craniopharyngioma)
- Pineal tumors
- Tumors of the cranial and paraspinal nerves (e.g., schwannoma: , neuroma, neurofibroma)
- Mesenchymal nonmeningeothelial tumors (e.g., hemangiomas, hemangioblastoma, lipoma, hamartoma)
- Germ cell tumors (e.g., teratoma)
- Primary central nervous system lymphoma (PCNSL)
Metastasis
- Primary CNS tumors do not metastasize to organs outside the CNS.
-
Drop metastases (intradural extramedullary spinal metastases ) and leptomeningeal metastases may occur. [21]
- Typically manifest as nodules along the spine and cauda equina that can cause back pain with neurologic symptoms (e.g., limb weakness)
- Can be detected by lumbar puncture
Astrocytoma
Overview
Astrocytomas are neuroepithelial tumors (gliomas) that arise from astrocytes, which are a specific type of glial cell.
| Classification of astrocytomas | |||||
|---|---|---|---|---|---|
| Grade | Type | Description | Epidemiology | Location | Prognosis |
| I | Pilocytic astrocytoma |
|
|
|
|
| II | Diffuse astrocytoma |
|
|
|
|
| III | Anaplastic astrocytoma [22][23] |
|
|
|
|
| IV | Glioblastoma multiforme (GBM) [24][25][26] |
|
|
|
|





Pilocytic astrocytoma [27][28][29][30]
- Description: slow-growing, circumscribed, non-invasive tumor
-
Epidemiology
- Most commonly affects children and young adults (< 20 years)
- The most common primary brain tumor of childhood
- Associated conditions: neurofibromatosis type I
-
Typical location
- Cerebellum (most common)
- Cerebral hemispheres (supratentorial)
-
Clinical features
- Insidious onset and slow progression of symptoms
- Vomiting
- Ataxia
- Failure to thrive
-
Diagnostics
-
MRI findings
- Well-demarcated cystic lesion
- Bright contrast-enhancing solid nodule in the wall of the cyst
-
Histopathology
- Microcysts
- Bipolar cells; hair-like projections
- Eosinophilic fibers with corkscrew appearance (Rosenthal fibers)
-
MRI findings
- Treatment: Surgical resection
-
Prognosis
- Favorable prognosis: high rates of long-term survival
- Curable with complete resection of the tumor
- Median survival: > 10 years
Optic glioma [31]
-
Description
- Low-grade, slow-growing tumor that arises from the glial cells of the optic pathway
- Typically a grade I pilocytic astrocytoma
- Epidemiology: most frequently in children (< 10 years)
- Associated conditions: neurofibromatosis type I
-
Clinical features
- Insidious onset and slow progression of symptoms
- Proptosis
- Strabismus
- Asymmetric nystagmus
- Impaired vision (in case of chiasmal involvement)
-
Diagnostics
- Fundoscopy findings: retinal pallor, papilledema
- MRI findings: thickening of the optic nerve or optic chiasm; suprasellar mass
-
Treatment
- No treatment in asymptomatic patients with no signs of tumor growth
- Surgical resection
-
Radiotherapy
- Unresectable tumors, e.g., chiasmal or optic tract lesions in optic glioma
- Adjuvant to surgery
-
Prognosis
- Favorable; high rates of long-term survival
- Many patients have long-term visual impairment.
Diffuse astrocytoma
- Description: slow-growing, infiltrative tumor that arises from glial cells in the CNS and has the potential to progress to higher-grade tumors
- Epidemiology: peak age 20–40 years
- Location: cerebral hemispheres
-
Clinical features
- Insidious onset and slow progression of symptoms
- Initially manifest with nonspecific features such as headaches, seizures
- Focal symptoms may develop (e.g, progressive paralysis, aphasia)
-
Diagnostics
- CT: hypodense lesion with no contrast enhancement
-
MRI
- T1 hypointense or isointense
- T2 hyperintense
-
Treatment
- Complete surgical resection is often not possible. resection until definable margins can be attempted
- Percutaneous radiotherapy for very diffuse, unresectable tumors
- Prognosis: incurable; median survival: 2–12 years
Anaplastic astrocytoma [22][23]
- Description: A high-grade infiltrative tumor with variable rates of growth that arises from glial cells in the CNS
- Epidemiology: peak age 30–50 years of age
-
Clinical features
- Headache
- Seizures
- Focal neurologic deficits
- Altered mental status
-
Diagnostics
-
MRI
- Inhomogenous lesion with perifocal edema
- No necrosis (in contrast to glioblastoma)
- CT
- Hypodense lesion with variable contrast enhancement
- Positive mass effect
-
MRI
-
Treatment
- Tumor debulking through surgery. However, complete surgical resection is not possible.
- Percutaneous radiotherapy/chemotherapy
- Prognosis: incurable; median survival between 18 months and 10 years
Glioblastoma multiforme
- Description: : a highly malignant tumor derived from glial cells (e.g., astrocytes)
-
Epidemiology [32][33][34]
- Most common malignant brain tumor
- Accounts for approx. 16% of all CNS neoplasms
- ♂ > ♀ (1.6:1)
- Peak incidence: 64 years of age
- Primary glioblastoma (∼ 90%): more frequent in elderly patients (6th decade of life)
- Secondary glioblastoma (∼ 10%): affects primarily younger patients (4th decade of life)
-
Etiology
- Environmental factors: ionizing radiation
- Genetic or chromosomal factors [33]
- Primary glioblastoma: arises de novo
- EGFR overexpression
- PTEN gene mutations [35]
- Loss of chromosome 10q
- Secondary glioblastoma: arises from a preexisting low-grade tumor (e.g., diffuse astrocytoma, anaplastic astrocytoma)
- Isocitrate dehydrogenase 1 (IDH1) mutations
- p53 gene mutations
- Loss of chromosome 19q
- Primary glioblastoma: arises de novo
- Associated conditions: rare occurrence of glioblastoma in patients with certain genetic syndromes (e.g., type I and II neurofibromatosis, tuberous sclerosis, Li Fraumeni syndrome, Turcot syndrome)
-
Classification: The 2016 WHO classification groups glioblastomas mainly on the basis of IDH mutation status. [36]
- IDH-wildtype glioblastoma (∼ 90%): usually corresponds with the clinically defined primary glioblastoma
- IDH-mutant glioblastoma (∼ 10%): usually corresponds with the clinically defined secondary glioblastoma
-
Clinical features
- General clinical features of brain tumors (e.g., signs of ↑ ICP, seizures, focal neurologic symptoms)
- Short disease course with death within weeks (Rapid tumor growth)
- Apoplectic glioma: mimics intracranial hemorrhage and manifests with signs of ↑ ICP
-
Typical location
- Primary glioblastoma
- White matter of the cerebral hemispheres (supratentorial)
- Possibly bilateral, crossing the corpus callosum: butterfly glioma
- Secondary glioblastoma: frontal lobe
- Primary glioblastoma
-
Diagnostics
- Characteristic features on MRI and CT
- Irregularly shaped, inhomogeneous mass
- Perifocal vasogenic edema
- Mass effect: midline shift, ventricular distortion
- Possibly hemorrhage
-
MRI (gadolinium-enhanced)
- Garland-like, enhanced margins with a hypointense necrotic core
- T1 hypointense
- T2 hyperintense
- May also have multifocal enhancements
- Contrast-enhanced CT: irregular, heterogeneous enhancement of the margins and hypointense center
- Evaluation of IDH mutation status (via immunohistochemistry or genome sequencing)
-
Biopsy
-
Dense, pleomorphic anaplastic cells that form pseudopalisades due to central necrosis or hemorrhage
- A histopathologic finding characterized by elongated nuclei stacked in rows that often radiate away from a central area of necrosis
- Classically associated with glioblastoma multiforme
- Microvascular proliferation
- GFAP positive
-
Dense, pleomorphic anaplastic cells that form pseudopalisades due to central necrosis or hemorrhage
- Characteristic features on MRI and CT
-
Treatment
- Surgical resection
- Palliative radiochemotherapy with temozolomide
- Adjuvant chemotherapy with temozolomide
- Glucocorticoids
- After recurrence
- Reresection, temozolomide, and/or radiation (if tolerated)
- The use of other chemotherapeutic agents (carboplatin, etoposide, irinotecan, nitrosoureas) can be tried as single agents or in regimens.
- Bevacizumab
-
Tumor-treating fields (TTFields) [37]
- Noninvasive treatment modality based on the transcutaneous delivery of alternating intermediate-frequency and low-intensity electric fields to disrupt tumor cell division and inhibit tumor growth
- The electric field interferes with cancer cells in a number of ways, including the alteration of cell membrane polarization and inhibition of microtubule polymerization.
- Can be given in combination with adjuvant chemotherapy (e.g., temozolomide)
-
Prognosis [33]
- Median survival: 15 months
- Positive prognostic factors: IDH-mutant glioblastoma, lower patient age, higher Karnofsky performance score, accessible tumor location for surgery
- Negative prognostic factors: large tumor size (> 5–6 cm), midline-crossing tumors
")

Glial fibrillary acidic protein (GFAP) is an important diagnostic marker for astrocytomas; it is almost always positive in glioblastoma multiforme!
Brainstem glioma [38]
- Description: a tumor arising from the glial cells in the brainstem that may be low-grade (I-II) or high-grade (III-IV)
- Epidemiology: peak age 3–10 years
-
Clinical features
- Vomiting
- Cranial nerve deficits
- Ataxia
- Hydrocephalus
- Upper motor neuron signs
-
Diagnostics: MRI
- No contrast enhancement
- T2 hyperintense lesion
-
Treatment
- Radiation and/or chemotherapy
- Surgical resection is often impossible
-
Prognosis
- Poor, especially in diffuse pontine gliomas
- Median survival: ∼ 10 months
MRI head (a: T1-weighted; with contrast; sagittal plane; b: T2-weighted; axial plane) of a child
A large lesion in the right cerebellar hemisphere displaces the vermis to the left of midline. It has a large cystic component (T1 hypointense and T2 hyperintense; red overlay) and a heterogeneously enhancing solid nodular component (green overlay).
Cerebellar pilocytic astrocytoma frequently manifests as a large cystic lesion with an enhancing mural nodule.
Source: “Figure 1, in: The Journal of Headache and Pain” by Irene Toldo, Debora De Carlo, Rodica Mardari et al., The Journal of Headache and Pain, licensed under CC BY 2.0. Modifications: - Labels have been removed from original image (asterix and two arrows). - letters edited. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
MRI head (top: T2-weighted; middle: T1-weighted without contrast; bottom: T1-weighted with contrast; axial plane)
A heterogeneous lesion in the left frontal lobe distorts the interhemispheric fissure (indicated by white arrowhead). On the T1-weighted sequences, the lesion is predominantly hypointense (green overlay) with garland-like enhancement (yellow overlay). Associated edema is hyperintense on the T2-weighted sequence (red overlay).
Source: © IMPP
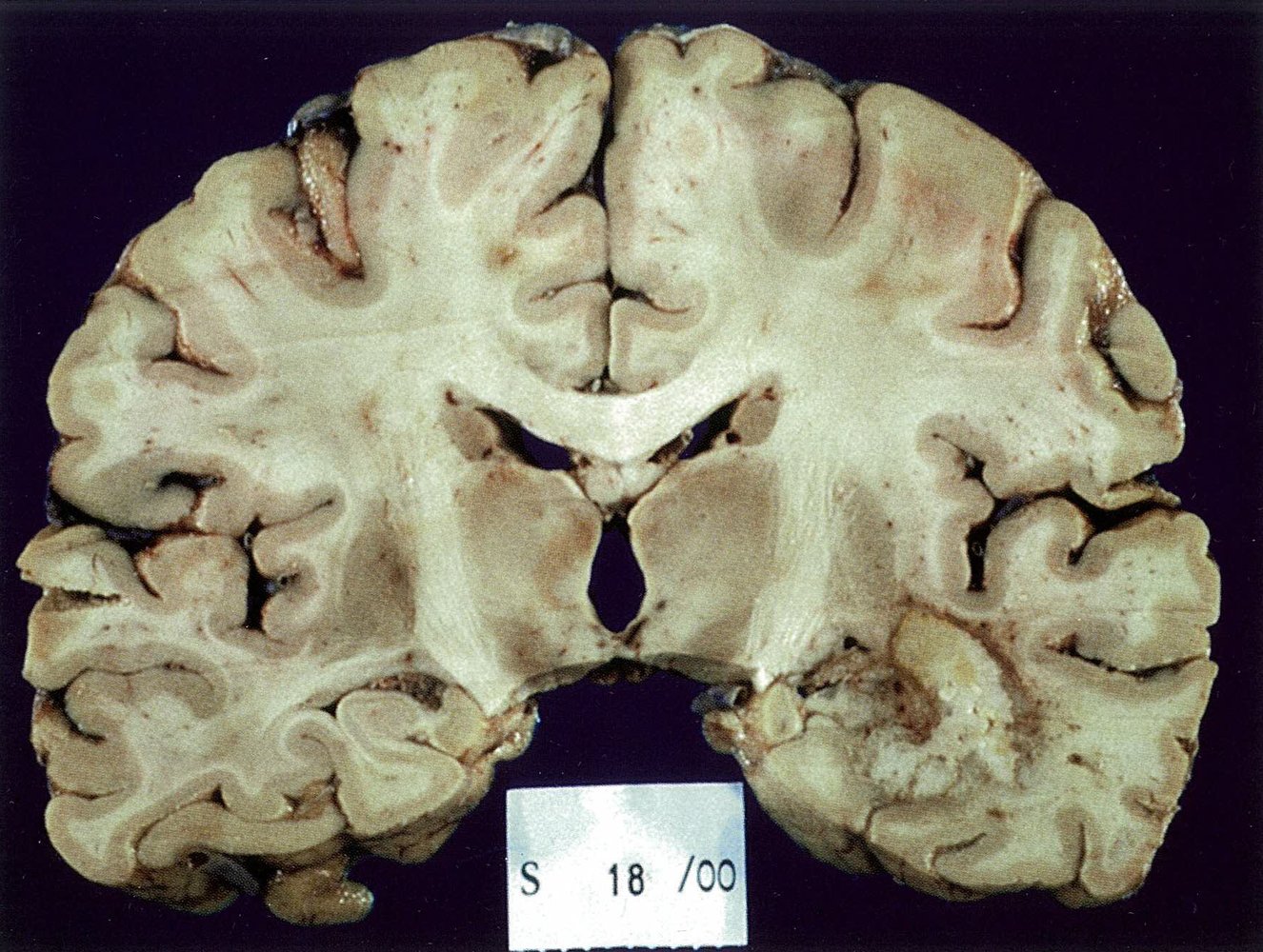
Frontal section of a macroscopic brain preparation: There is a tumorous lesion with a macroscopic typical "colorful cut surface" in the temporal lobe. The yellow areas are necrosis and the marked white areas are cell dense regions. The surrounding red marked areas most likely correspond to the margin of a vessel or hemorrhage. The findings correspond to a glioblastoma.
Source: © IMPP
T1-weighted contrast-enhanced MRI, frontal view: bihemisphere garland-like contrast enhancement. There is peripheral contrast agent enhancement (blue overlay) with central necrosis (green overlay). The third ventricle (arrowhead) is centrally located. The tumor is displacing the posterior horn of the lateral ventricle (red overlay). Diagnosis: bilateral glioblastoma (butterfly glioma).
Source: © IMPP
Upper row: axial native CCT scan. Lower row: axial CCT with contrast medium. Finding: grade II (diffuse) astrocytoma in the frontal lobe
Source: © IMPP
MRI head (top left: T1-weighted, axial plane; top right: T2-weighted, axial plane; bottom left: T1-weighted, with contrast, axial plane; bottom right: T1-weighted, with contrast, coronal plane)
There is a large, well-defined mass in the right frontal lobe (green overlay), which demonstrates hypointense signal on the T1-weighted images and hyperintense signal on T2-weighting with no significant surrounding edema. No significant enhancement is demonstrated on the post-contrast sequences.
Source: © IMPP
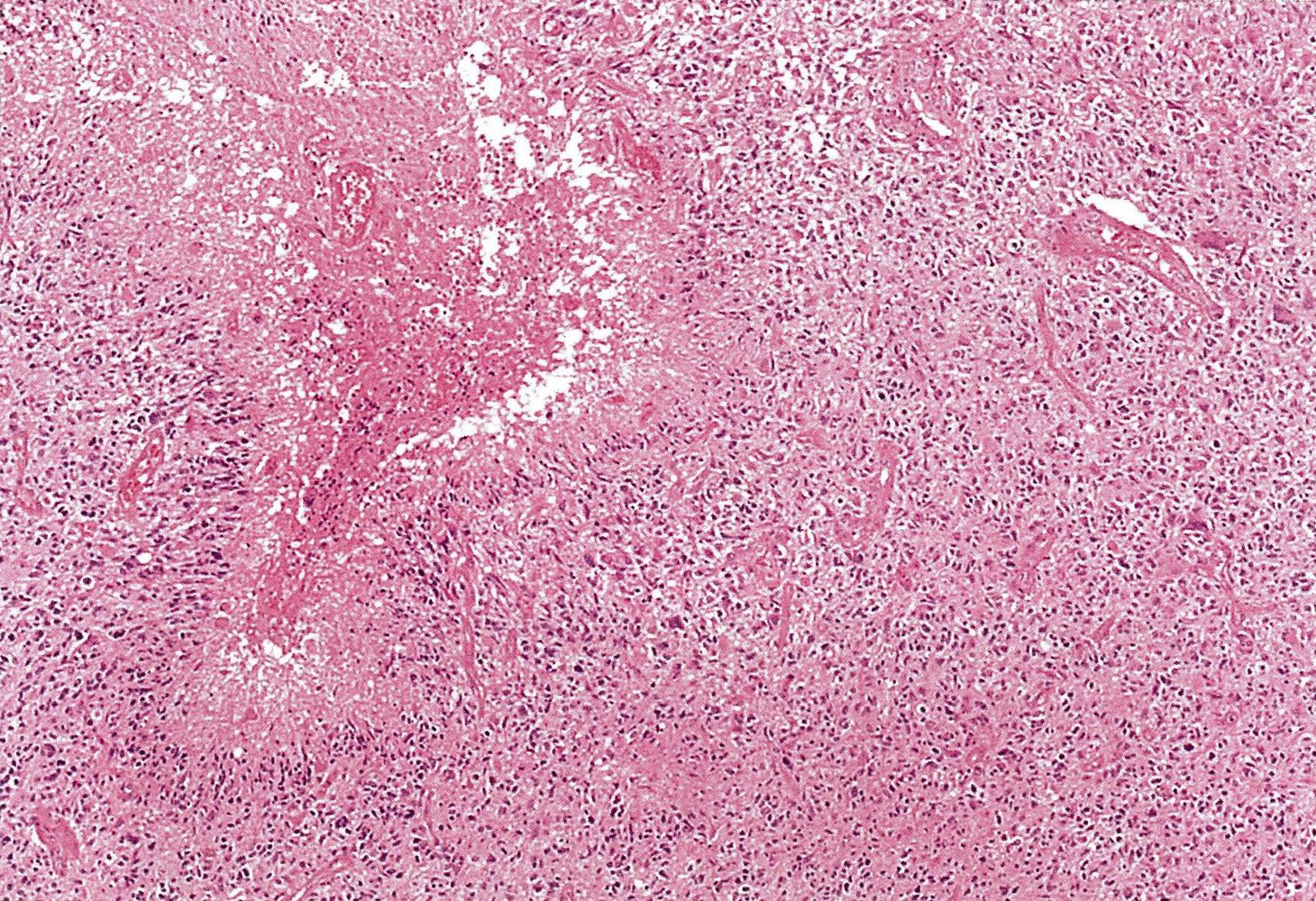
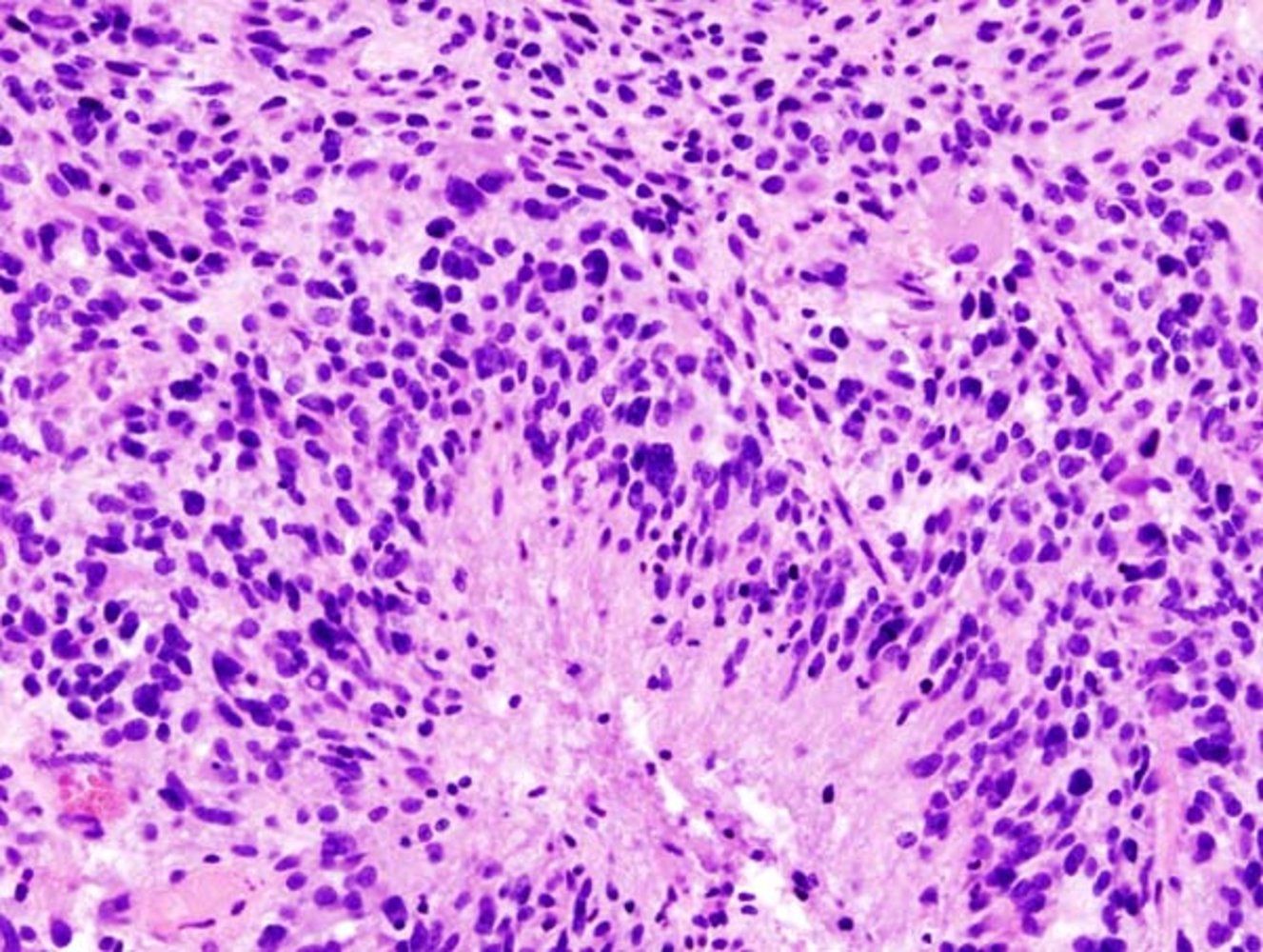
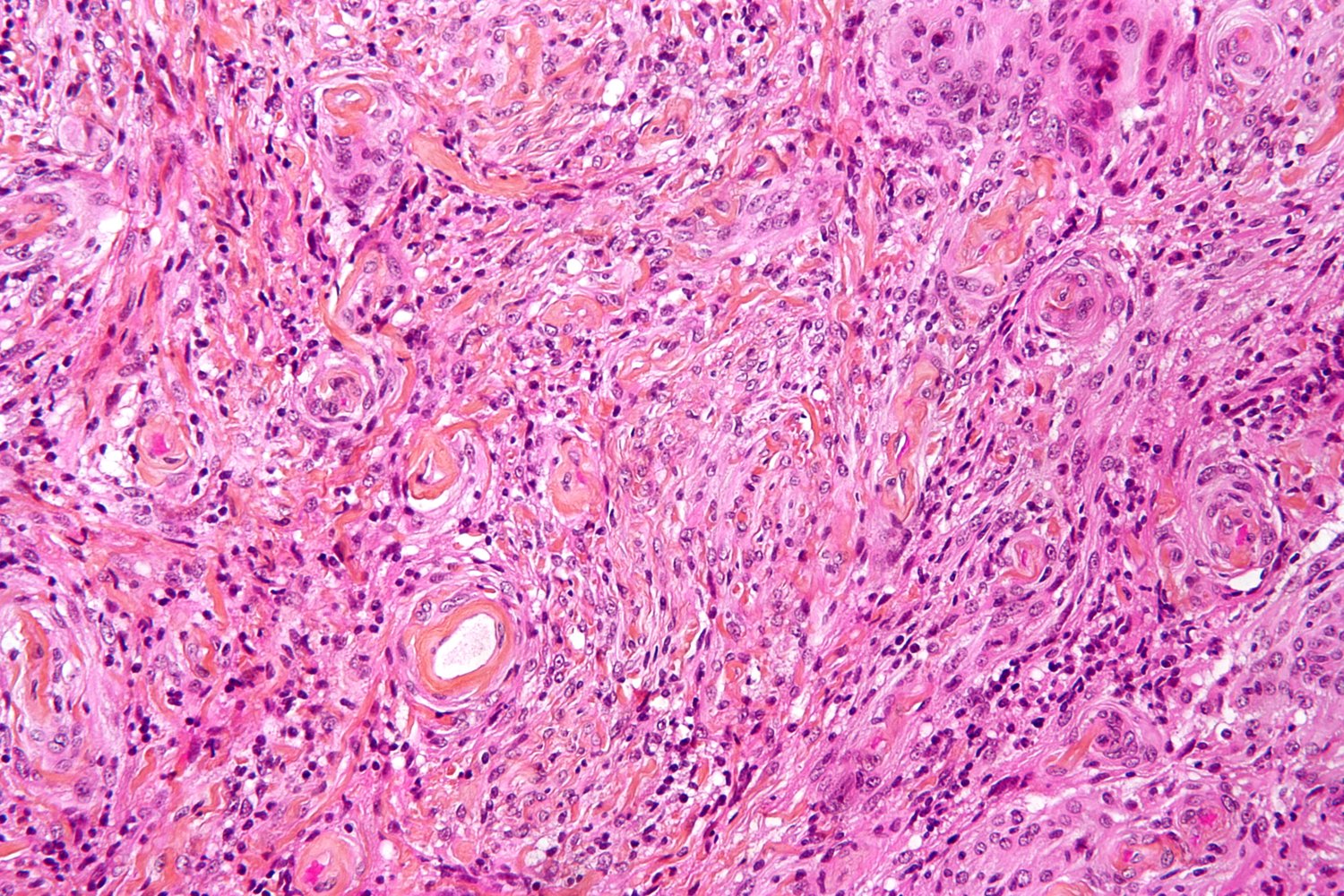
Photomicrograph of the brain (H&E stain)
Diffuse infiltration of the central nervous tissue by astrocytic tumor tissue can be seen. Palisade-like deposits of tumor cells with hyperchromatic, polymorphic nuclei surround the anuclear necrotic lesions. There are numerous mitotic figures. There is an abundance of capillary bundles with a hyperplastic endothelium. The tissue shows extensive, regressive changes.
Diagnosis: glioblastoma (WHO grade IV)
Source: © IMPP
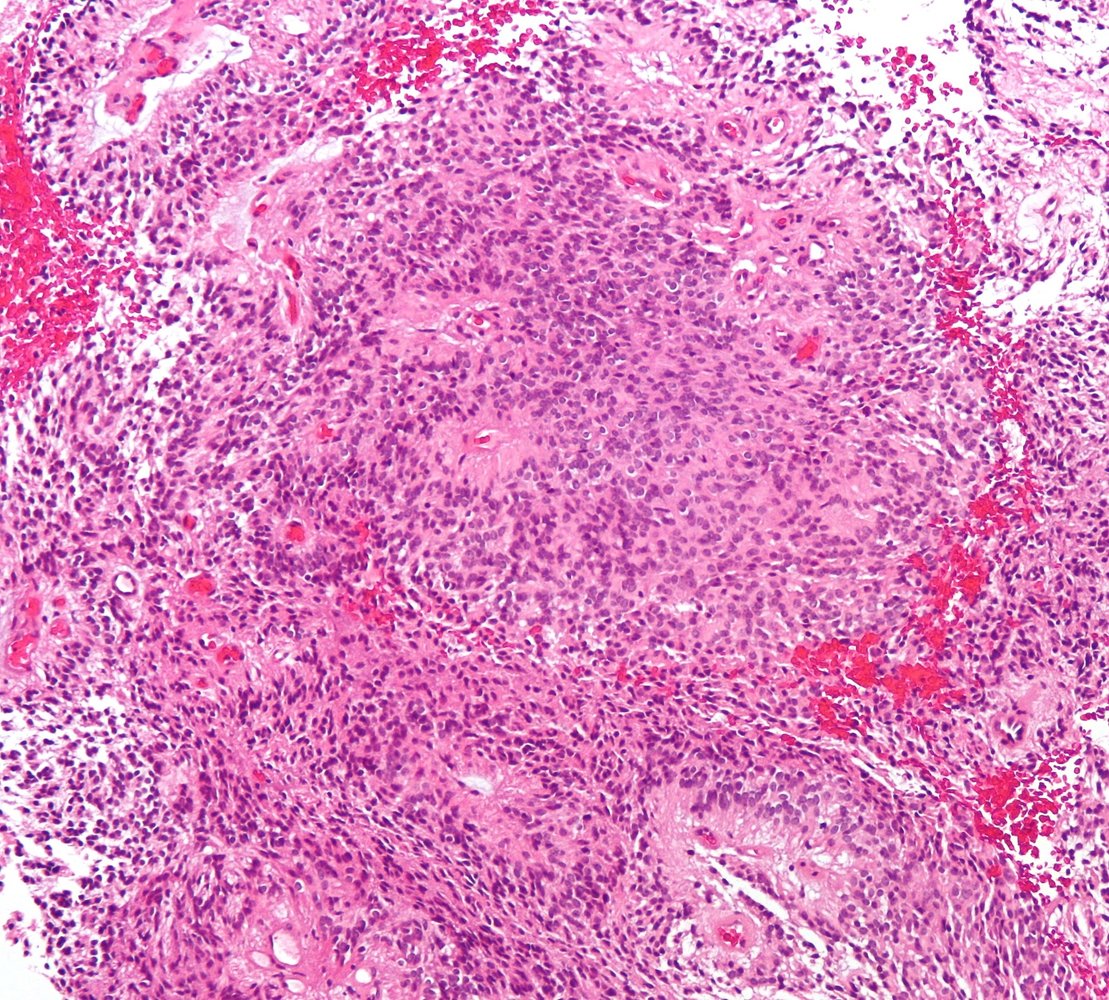
Photomicrograph of cerebellar tissue (H&E stain)
There are numerous bipolar cells, composed of a central basophilic nucleus with eosinophilic pilocytic processes (examples indicated in green) arising from either end. The pilocytic processes are arranged in bundles, which resemble matted hair. The bright red-pink bodies are intracytoplasmic inclusions (examples indicated by black arrowheads) in astrocytes and indicate intense gliosis (Rosenthal fibers).
These are the characteristic features of pilocytic astrocytoma.
Source: “PilocyticAstrocytoma 20x HE” by Marvin 101, Wikipedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
© AMBOSS
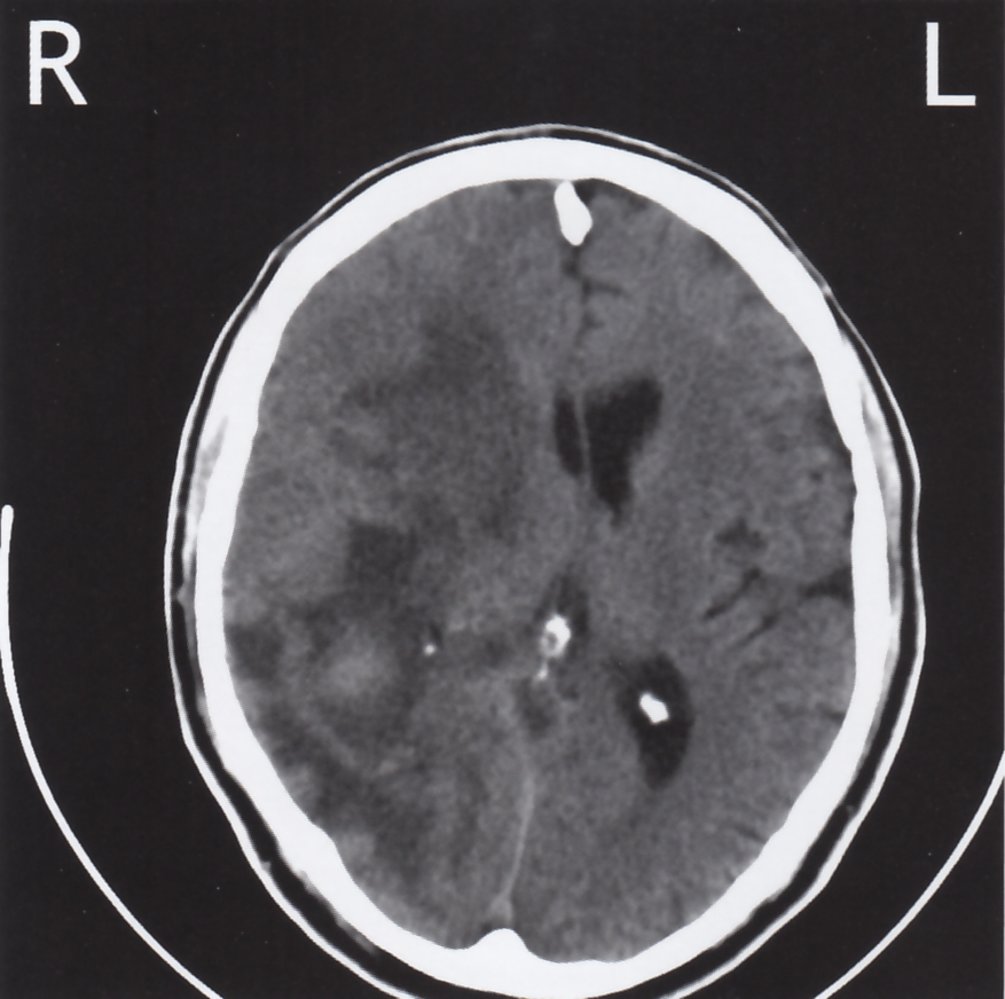
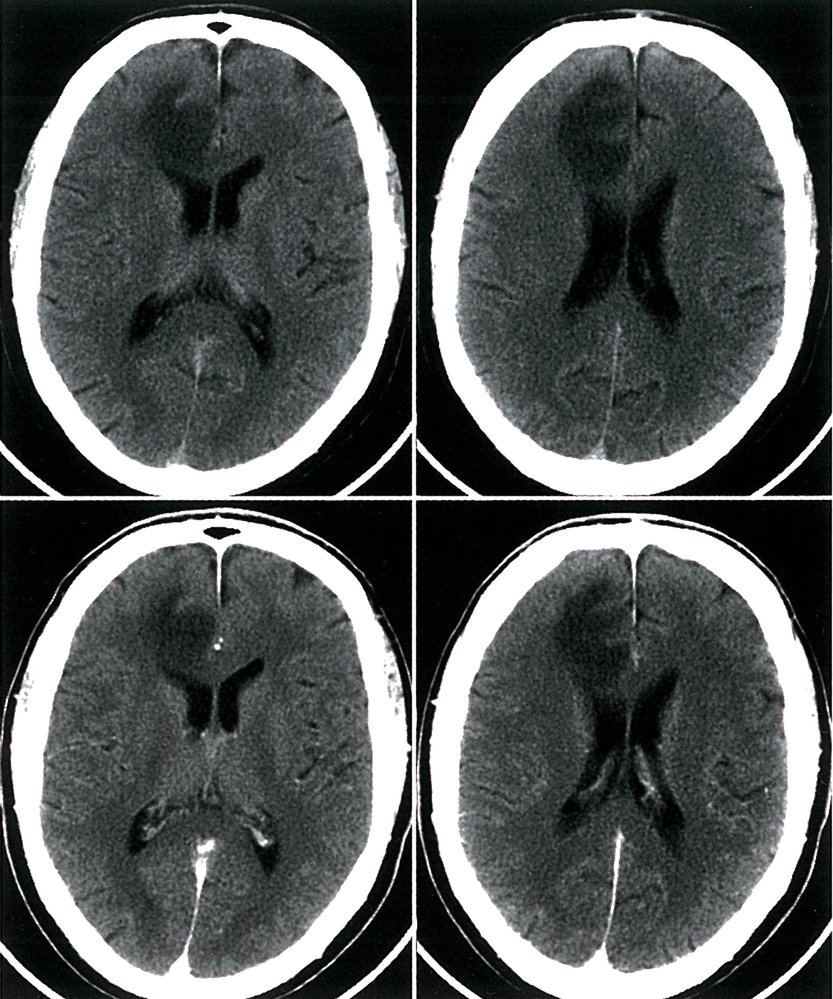
CT head (without contrast; axial plane) of a 69-year old man with a history of personality changes and left-sided hemiparesis from glioblastoma
The right cerebral hemisphere is diffusely abnormal, with intermixed hypodense (green overlay), isodense, and hyperdense (red overlay) areas. There is mass effect with sulcal effacement and midline shift to the left (dashed line). The frontal and occipital horns (arrowheads) of the right lateral ventricle are effaced.
Yellow overlay: choroid plexus calcification
Blue overlay: falx cerebri calcification
Source: © IMPP
MRI brain (T1-weighted; with contrast; axial plane) of a 69-year-old patient with personality changes and left-sided hemiparesis.
In the white matter of the right hemisphere, there is a large, poorly circumscribed space-occupying lesion, which is hypointense centrally (green overlay) with strong peripheral contrast enhancement (red overlay). The lesion is surrounded by edema (white overlay), suggesting rapid growth and displacement of surrounding structures. The mass effect has also caused a slight midline shift to the contralateral side (white dashed line), and compression of the right lateral ventricle (white arrowheads indicate anterior horn compression).
These radiographic features are typical of a glioblastoma.
Source: © IMPP
Photomicrograph of a cerebral tissue specimen (H&E stain; high magnification)
A high number and density of highly pleomorphic cells with hyperchromatic and irregular nuclei are visible (examples indicated by arrowheads. These cells are aggregated around the periphery of the necrotic zone (green overlay), forming a nuclear pseudopalisading architecture.
These are the characteristic features of glioblastoma multiforme.
Source: “Histopathological image of cerebral glioblastoma. Hematoxylin & esoin stain.” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
.jpg){kind=link}
Oligodendroglioma
- Description: : a tumor that arises from oligodendrocytes
-
Epidemiology
- Median age: 40–50 years
- Relatively rare: ∼ 10% of primary CNS tumors
- Clinical features: : the most common location is the cerebral hemisphere (typically the frontal lobe) → seizures, focal neurological deficits, personality changes
-
Diagnostics
-
Imaging: intra-parenchymal tumor with calcifications [39]
- CT: hypodense lesion
-
MRI
- T1: hypointense or mixed lesions
- T2: hyperintense lesions
-
Biopsy [40]
- Cells with a clear cytoplasm and round nucleus (fried egg cells)
- Chicken-wire pattern of capillary anastomoses
- Molecular testing: assessment of 1p/19q codeletion [41]
-
Imaging: intra-parenchymal tumor with calcifications [39]
-
Treatment
- Resection
- Adjuvant radiotherapy and chemotherapy
- Common chemotherapeutic regimens [42]
- Procarbazine PLUS lomustine PLUS vincristine
- Temozolomide monotherapy
-
Prognosis
- Recurrence rate ∼ 100%
- 5-year survival rate 50–60%


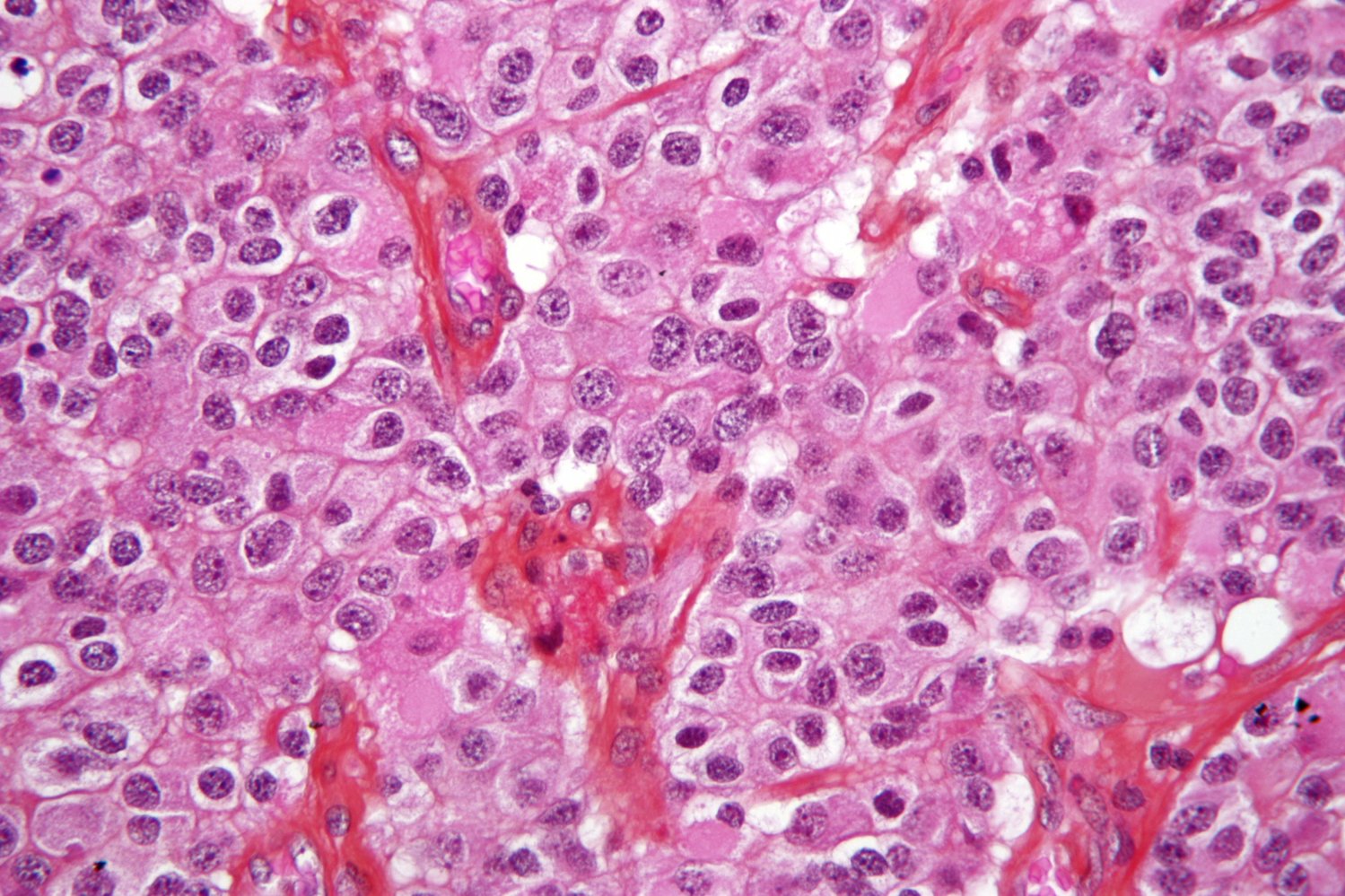
Photomicrograph of brain tissue (H&E stain; very high magnification)
Monomorphic cells with enlarged, round/oval nuclei surrounded by a clear halo of unstained cytoplasm, which is an artifact of processing, are visible (green overlay). Thin blood vessels with an interlacing pattern are also visible (yellow overlay).
These are the typical features of oligodendroglioma.
Source: “Oligodendroglioma1 high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Cranial CT scan (axial view)
A large hypodense lesion (green overlay) with multiple intralesional hyperdense calcifications (yellow overlay) is visible in the temporal lobe.
Source: “Oligodendroglioma 001” by RadsWiki, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Ependymoma
- Description: a tumor that arises from ependymal cells of the ventricular system
- Epidemiology: peak incidence in children and young adults
- Associated conditions: neurofibromatosis type II
- Clinical features: the 4th ventricle is the most common location in children → noncommunicating hydrocephalus → features of increased intracranial pressure (e.g., papilledema, headache)
-
Diagnostics
- Imaging: intra-parenchymal tumor with calcifications and cystic components due to necrosis and/or hemorrhage
-
Biopsy
- Perivascular pseudorosettes
- Rod-shaped bodies (blepharoplasts) near the nucleus
-
Treatment
- Resection
- Adjuvant radiotherapy
-
Prognosis
- Depends on the WHO grade, but usually poor
- Overall 5-year survival rate: 65–90% [43][44]



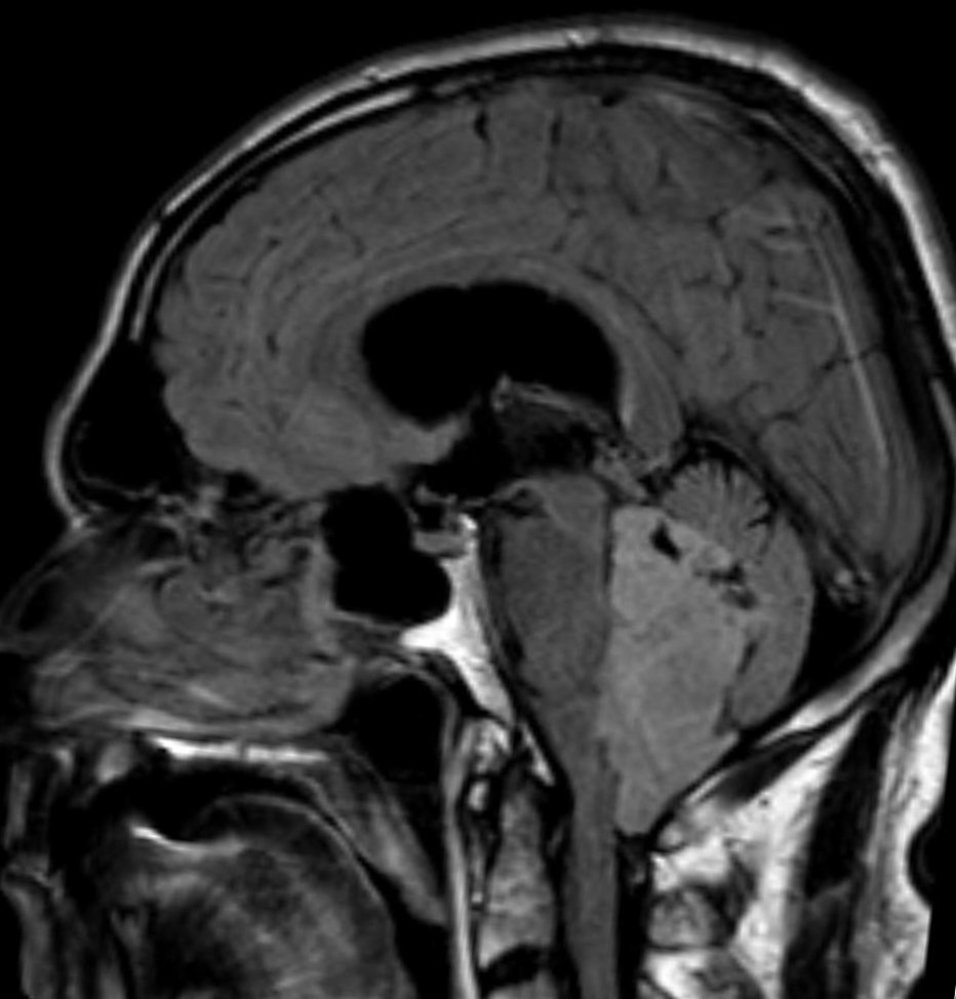
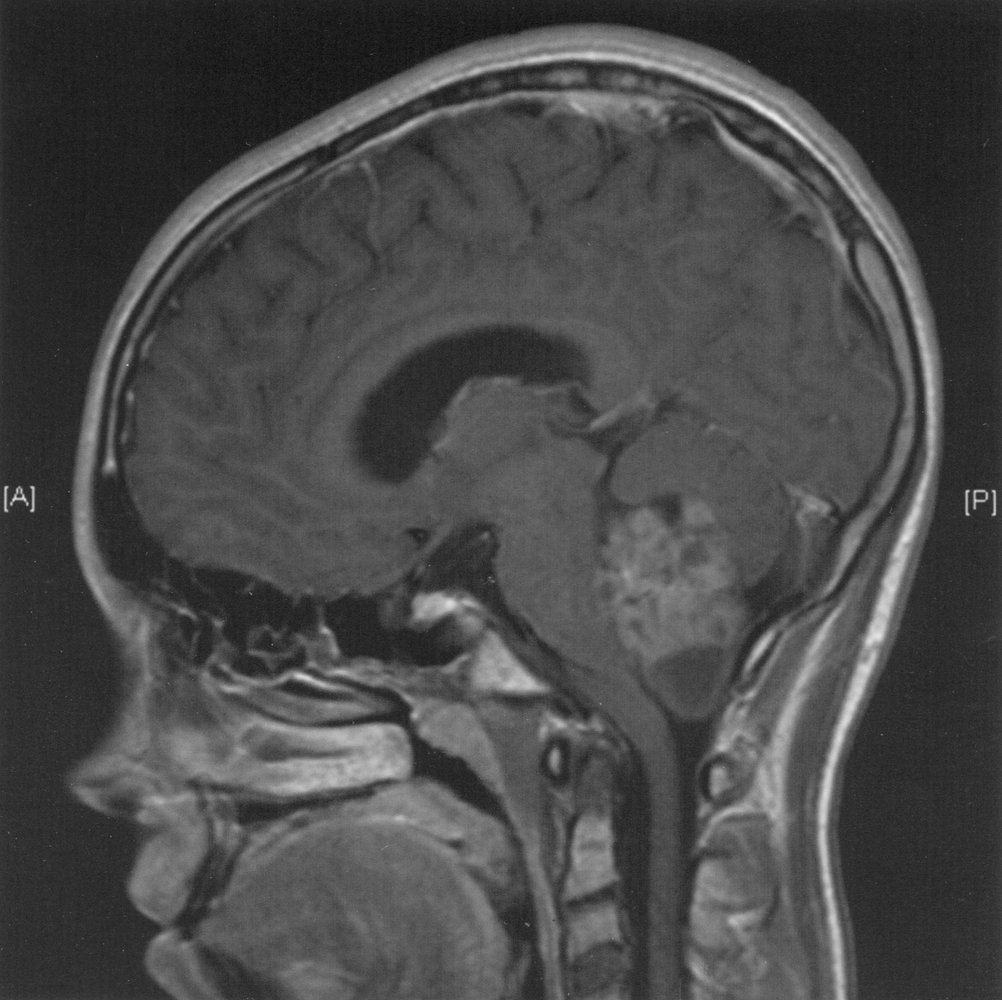
MRI brain (FLAIR; sagittal view)
A well-defined heterogeneous hyperintense lesion is visible within the expanded 4th ventricle (green overlay). At the superior aspect of the lesion, multiple dark foci are present (arrowheads), representing cysts. They appear dark in this image as the fluid signal is removed on FLAIR sequences. This lesion has obstructed circulation of the cerebrospinal fluid, resulting in ventriculomegaly (indicated by dashed line).
Ependymomas commonly arise within the fourth ventricle. They are usually hyperintense on T2 weighted/FLAIR images and can demonstrate cystic change, such as in this case, as well as hemorrhage.
Source: “Ependymom sag FLAIR” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
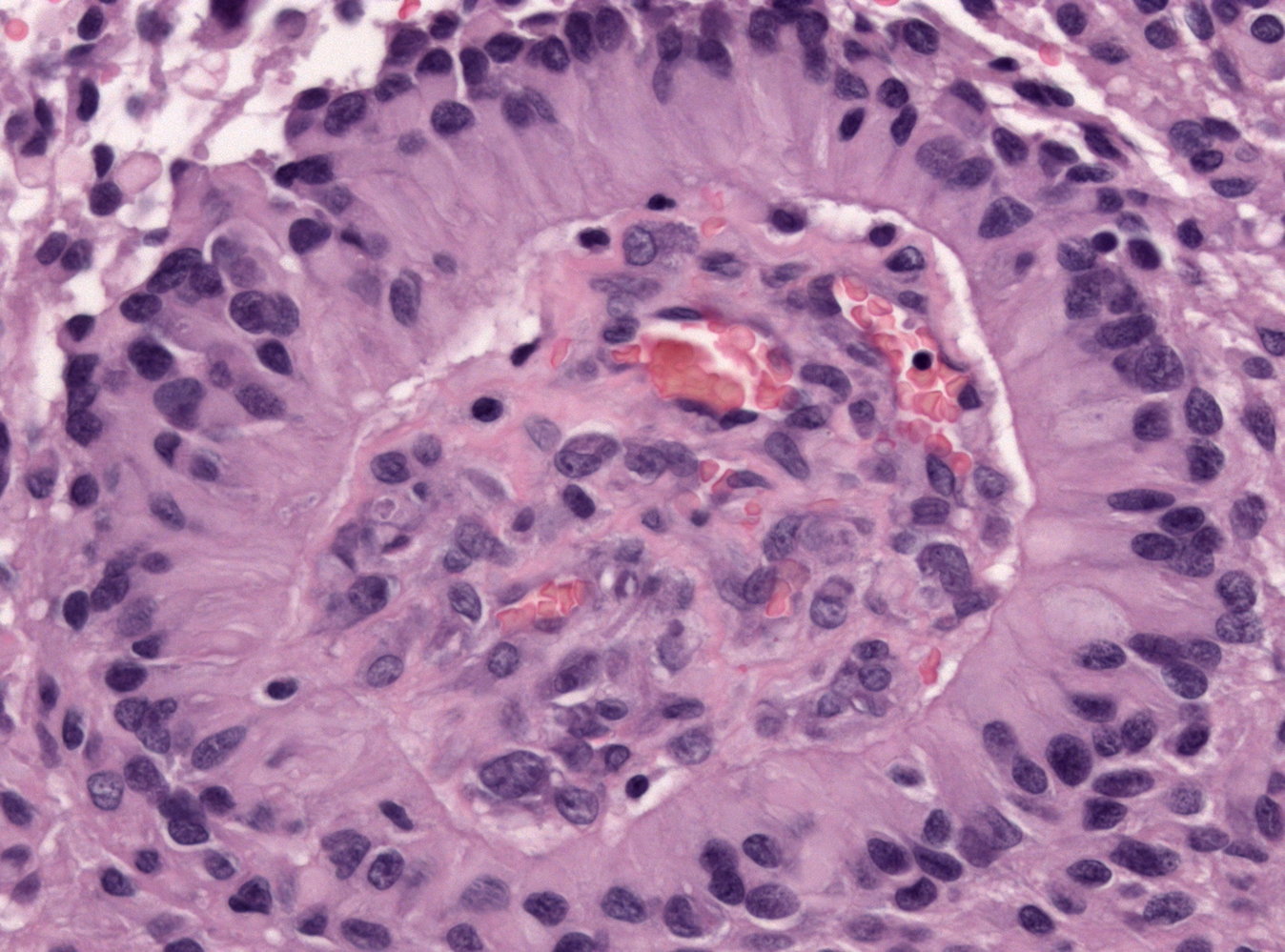
Photomicrograph of brain tissue (H&E stain)
Tumor cells (cylindrical epithelium) are arranged in a radial manner around several vessels. This pattern is called a perivascular pseudorosette.
Perivascular pseudorosettes are a hallmark of ependymoma.
Source: “Ependymoma pseudorosette” by Jensflorian, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Photomicrograph of a brain tumor tissue specimen (H&E stain; low magnification)
There is an abnormally high number of cells with round nuclei and abundant eosinophilic cytoplasm. Some cells are arranged in a spoke-and-wheel pattern, surrounding an empty central space. Such patterns are called ependymal rosettes (example indicated by green overlay). Other cells are arranged concentrically around blood vessels, producing a similar appearance (perivascular pseudorosettes; example indicated yellow overlay).
These are typical histopathological features of ependymoma.
Source: “Ependymoma low intermed mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Medulloblastoma
- Description: a highly malignant tumor derived from primitive, neuroectodermal tissue [45]
-
Epidemiology
- Peak incidence: 1st decade
- Most common malignant pediatric brain tumor (20–25% of all cases)
- Associated conditions: Turcot syndrome
-
Clinical features [46]
- The most common location is the cerebellum → cerebellar defects (e.g., broad-based gait)
- Most tumors arise within the cerebellar vermis (midline) → truncal ataxia
- Invasion or compression of the 4th ventricle → noncommunicating hydrocephalus → features of raised intracranial pressure (e.g., papilledema, vomiting, headache)
- Drop metastases to the spinal cord are common → paraplegia
-
Diagnostics [47]
-
Imaging: intraparenchymal contrast-enhancing mass [48]
- CT scan: isodense or hyperdense mass
-
MRI
- T1: hypointense mass
- T2: isointense mass
- Biopsy: anaplastic small round blue cells; that surround a central neuropil (Homer-Wright rosettes) [49]
-
Imaging: intraparenchymal contrast-enhancing mass [48]
-
Treatment [50]
- Resection
-
Adjuvant therapy
- Children ≥ 3 years: chemotherapy and craniospinal radiotherapy
- Children < 3 years: chemotherapy
- Common chemotherapeutic agents: vincristine, cisplatin, cyclophosphamide, lomustine [50]
-
Prognosis
- 5-year survival rate: 60–80% [51][52]
- Poor prognostic factors [53]
- Inadequate resection
- Presence of drop metastases
- ERBB2 mutation






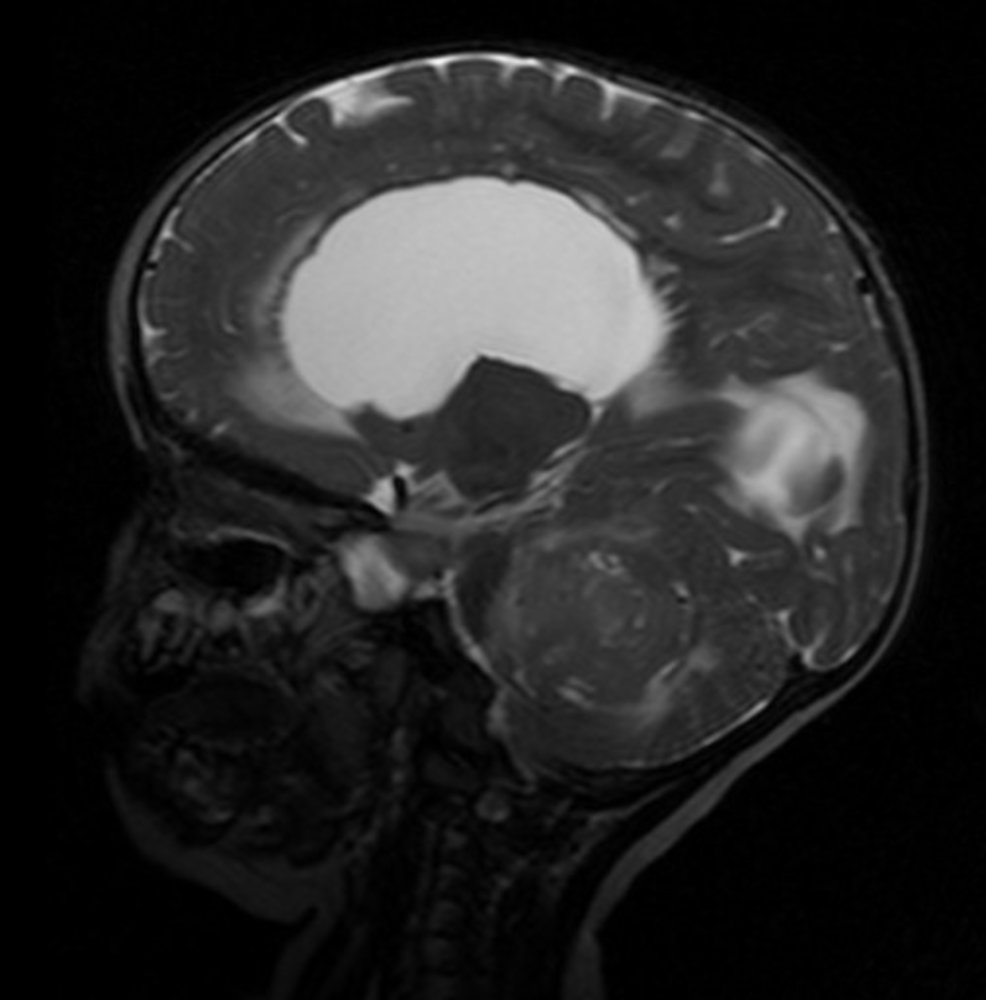
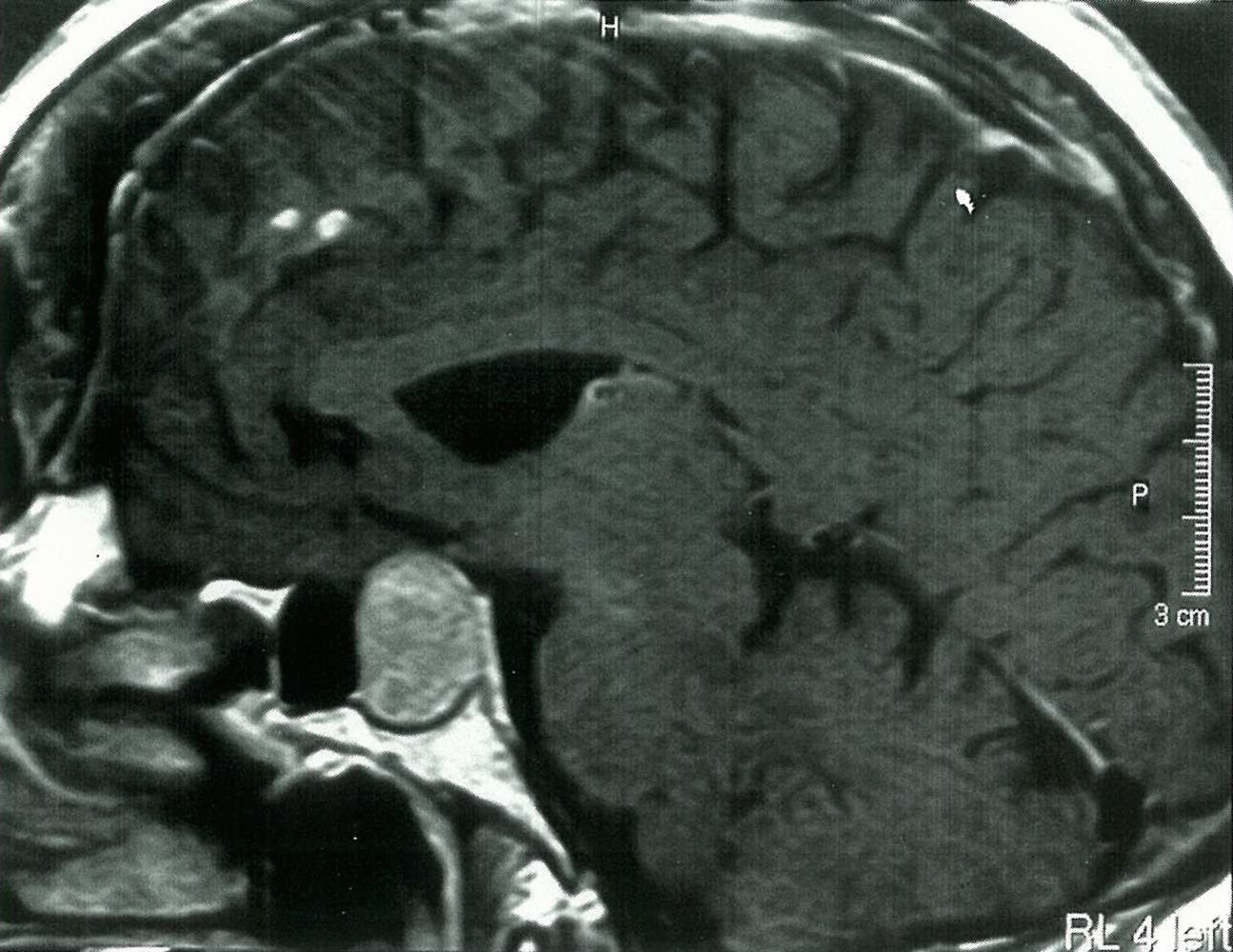
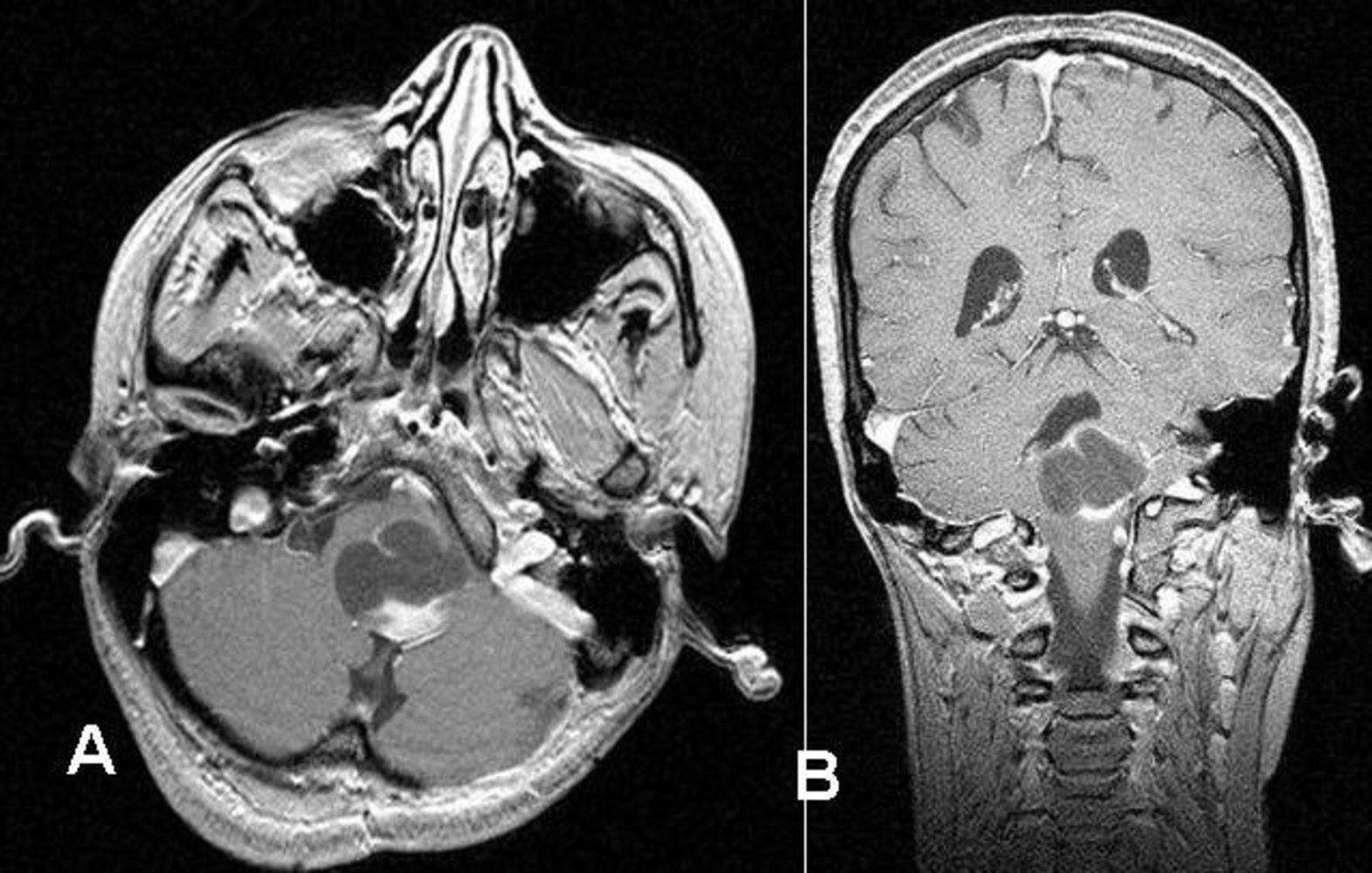
T2-weighed cranial MRI of a 6-year-old child presenting with features of increased intracranial pressure (midsagittal section with contrast)
There is a large hypointense mass occupying the third (upper yellow overlay) and fourth (lower yellow overlay) ventricles that is causing obstructive hydrocephalus (pink overlay).
The pink overlay also highlights the leakage of CSF into the periventricular space (transependymal edema) and into the occipital lobe due to the increased intraventricular pressure.
This appearance of a fourth ventricular mass in a child is characteristic of medulloblastoma.
Source: “Medulloblastom - MRT - T2 sagittal - 012” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Cranial MRI (T1-weighted, with contrast)
There is a mass in the posterior cranial fossa. It features solid parts (green overlay) and cystic parts (red overlay).
Location and appearance are typical of a medulloblastoma.
(D: diencephalon; P: pons; C: cerebellum; yellow outline: cerebellar tentorium)
Source: © IMPP
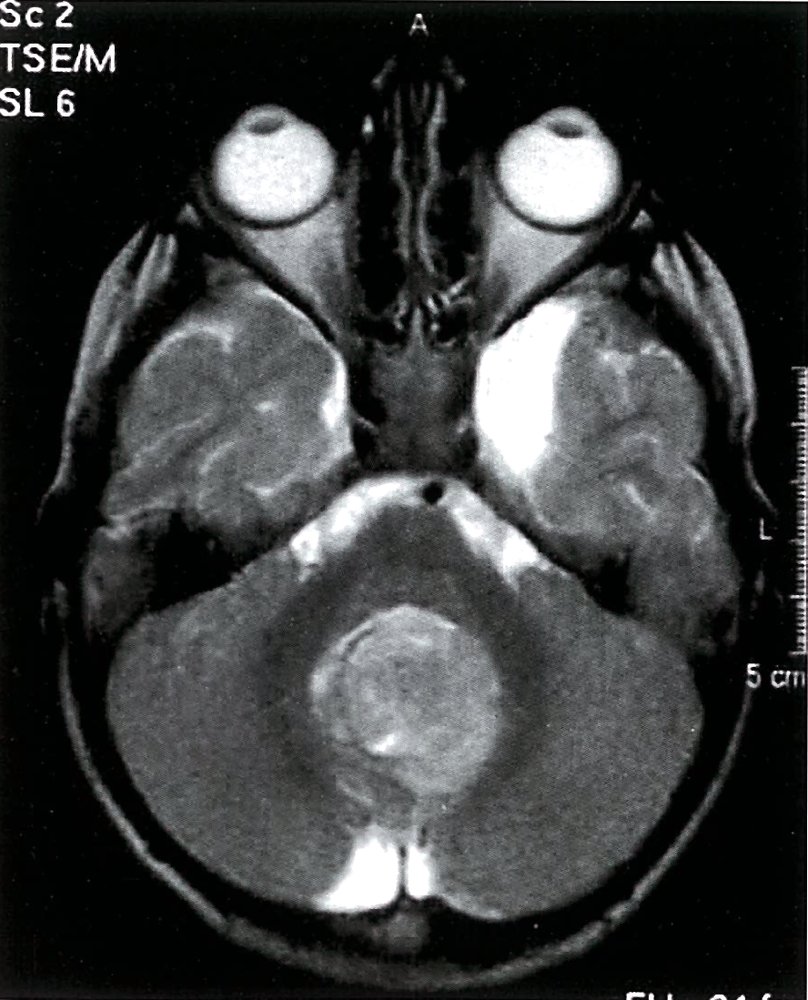
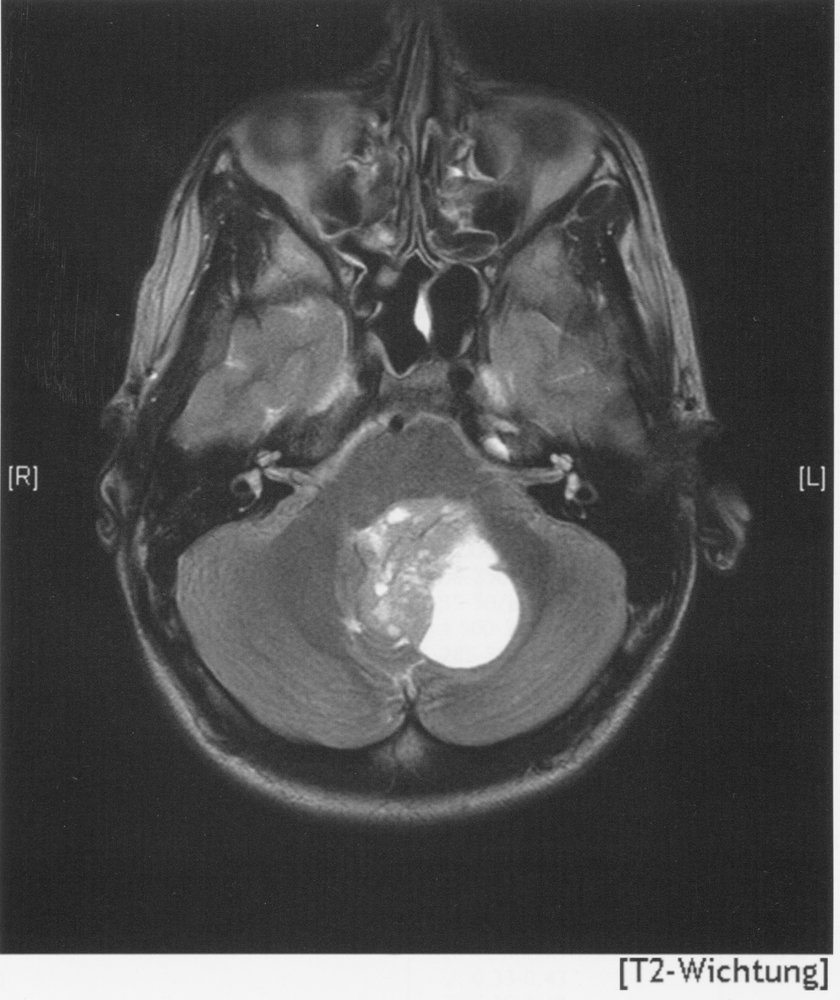
MRI Head (T2-weighted; axial view) of a 7-year-old boy
There is a lobulated heterogeneous posterior fossa mass (green overlay) present in the midline of the cerebellum at the level of the fourth ventricle. The fourth ventricle is obscured by the mass and is, therefore, not well seen in this image.
This is a medulloblastoma, the most common malignant pediatric tumor of the central nervous system. Medulloblastomas most commonly involve the cerebellar vermis, the structure that connects the two cerebellar hemispheres. In the pediatric population, other tumors that commonly occur in similar locations include brainstem glioma, ependymoma, choroid plexus papilloma, atypical teratoid/rhabdoid tumor, and astrocytoma. All of these should be considered in this case, although a brainstem glioma would rather be located predominantly within the brainstem rather than the vermis and is, therefore, less likely.
Arrowhead: basilar artery; C: cerebellum
Source: © IMPP
Head MRI (T2 weighted image)
Medulloblastoma within the posterior cranial fossa (green border in overlay). The lesion contains cystic areas, particularly on the left side (green overlay).
Source: © IMPP
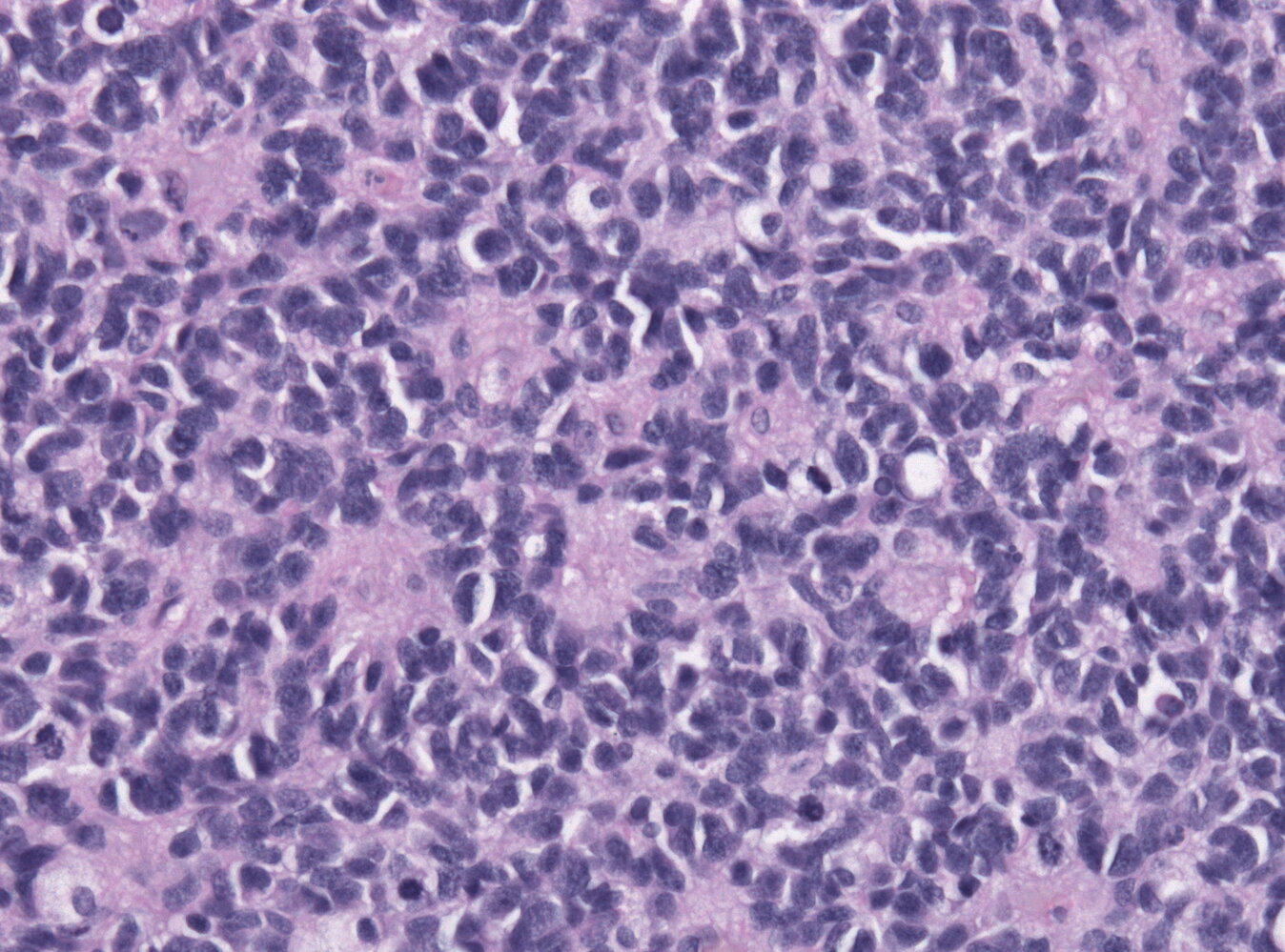
Photomicrograph of cerebellar vermis tissue (H&E stain)
Numerous small, blue, round cells with scant cytoplasm can be seen throughout the specimen (examples indicated by green overlay). Their nuclei vary in size and structure (nuclear pleomorphism) and many cells feature distinctly hyperchromatic nuclei.
The majority of the cells are arranged in concentric clusters around lighter central areas consisting of neuropil (examples indicated by yellow overlay). These clusters are referred to as Homer Wright rosettes.
These histopathological features, particularly the Homer Wright rosettes, are characteristic of a medulloblastoma.
Source: “Medulloblastoma with rosettes” by Jensflorian, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
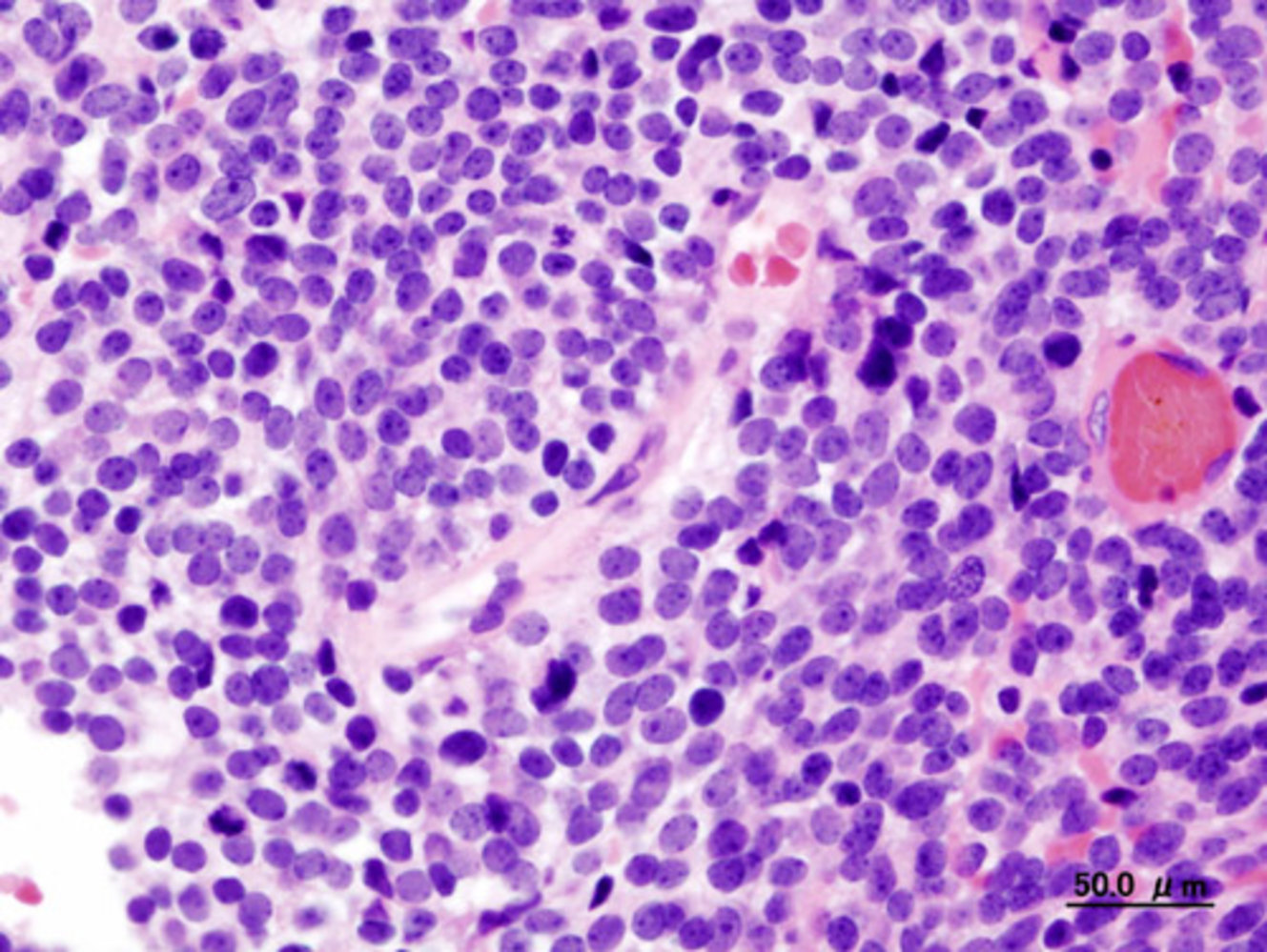
Photomicrograph of cerebellar vermis tissue (H&E stain)
Densely packed, small, blue anaplastic cells are present throughout the specimen. The cells have pleomorphic and hyperchromatic nuclei.
On the right, a vessel (its lumen mostly obstructed by eosinophilic material) can be seen.
These are typical histopathological findings of medulloblastoma.
Source: “Histopathologic image of medulloblastoma in cerebellar vermis in an adult patient. H & E stain.” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0.
_in_adult.JPG){kind=link}
Craniopharyngioma
- Description: a benign dysontogenetic tumor arising from a remnant of the Rathke pouch (ectodermal derivative)
-
Epidemiology
- Bimodal distribution: 5–14 years; second peak at 50–75 years
- Most common childhood supratentorial tumor
-
Clinical features: The tumor arises in the suprasellar region and can extend into the intrasellar region. [54]
-
Compression of the pituitary gland due to intrasellar extension → hypopituitarism
- Hypogonadotropic hypogonadism
- Failure to thrive
- Central diabetes insipidus
- Compression of the ventromedial hypothalamic nucleus → hyperphagia and obesity
- Compression of the infundibular stalk → disconnection hyperprolactinemia
- Compression of the optic chiasm → bitemporal hemianopsia
- Compression of interventricular foramina and/or aqueduct → obstructive hydrocephalus
-
Compression of the pituitary gland due to intrasellar extension → hypopituitarism
-
Diagnostics [55]
- Imaging: suprasellar calcified cyst with a lobulated contour
- Biopsy: cholesterol crystals found in a motor oil-like fluid on gross examination
- Consider obtaining diagnostics for hypopituitarism.
-
Histological variants
-
Adamantinomatous (common)
- Reticular epithelial cells
- Frequently associated with calcifications
- Cysts and keratin nodules
-
Papillary
- Metaplastic squamous cells
- Calcifications and cysts are rare.
- No keratin nodules
-
Adamantinomatous (common)
-
Differential diagnoses
- Pituitary adenoma
- Rathke cleft cyst
-
Treatment
- Resection
- Adjuvant radiotherapy
- Treatment of hypopituitarism
- Prognosis: generally good, with a 10-year survival rate of ∼ 90%; however, the recurrence rate is high [56][57][58]




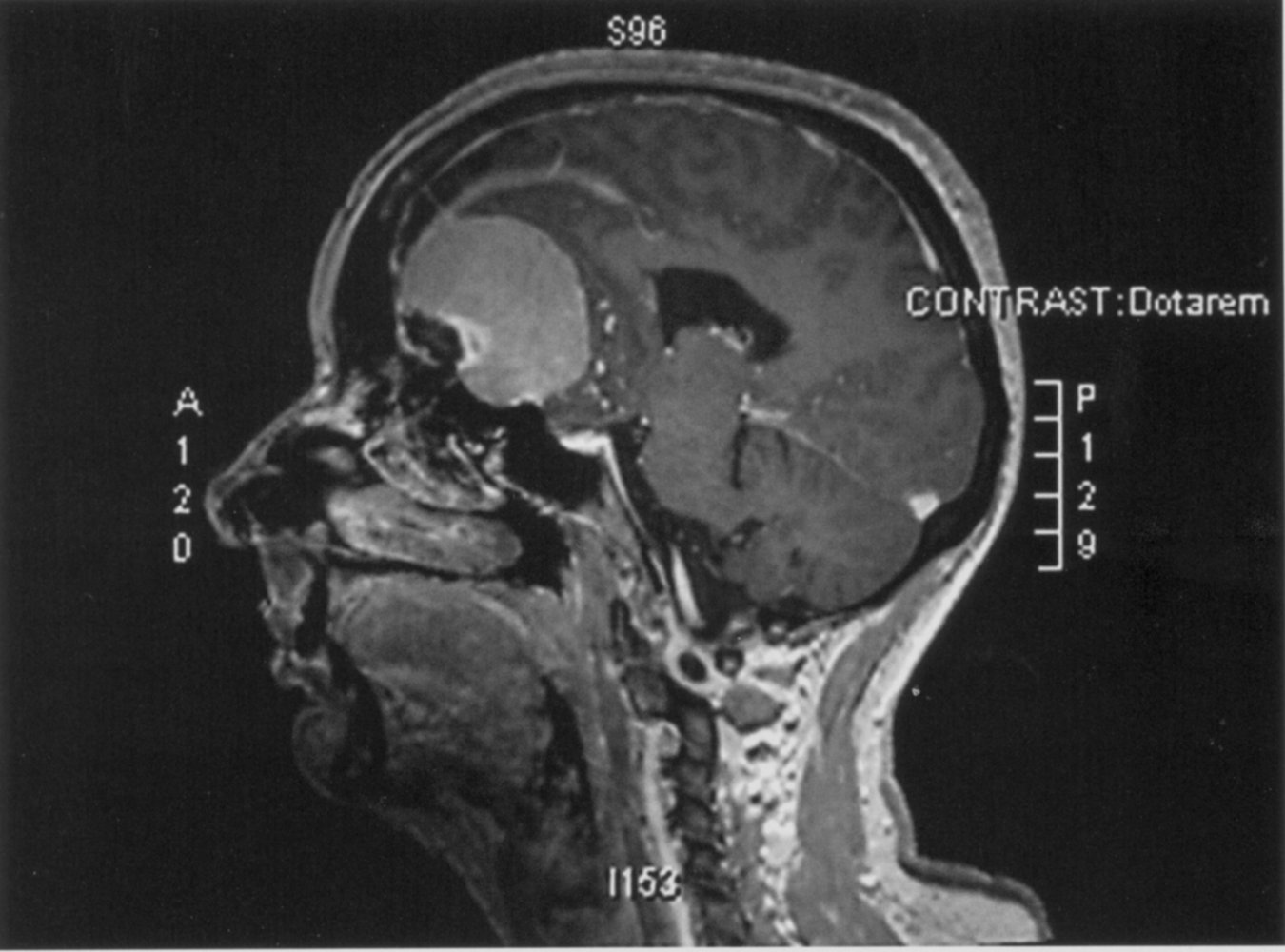
MRI of the brain (T1-weighted; sagittal view; with contrast)
A hyperintense, ovoid, sharply demarcated lesion (green overlay) is visible within the sella turcica and partially extends into the sphenoidal sinus.
The location and appearance of the lesion suggest a craniopharyngioma or a pituitary adenoma.
Source: © IMPP
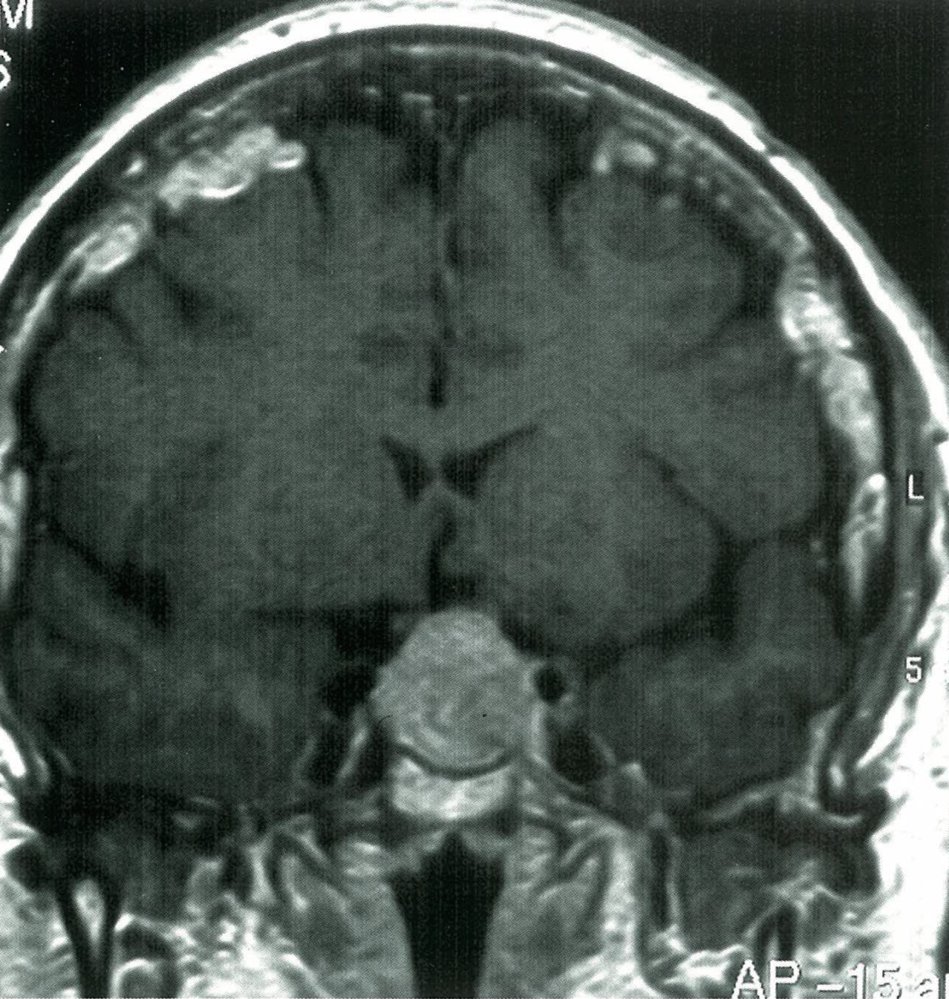
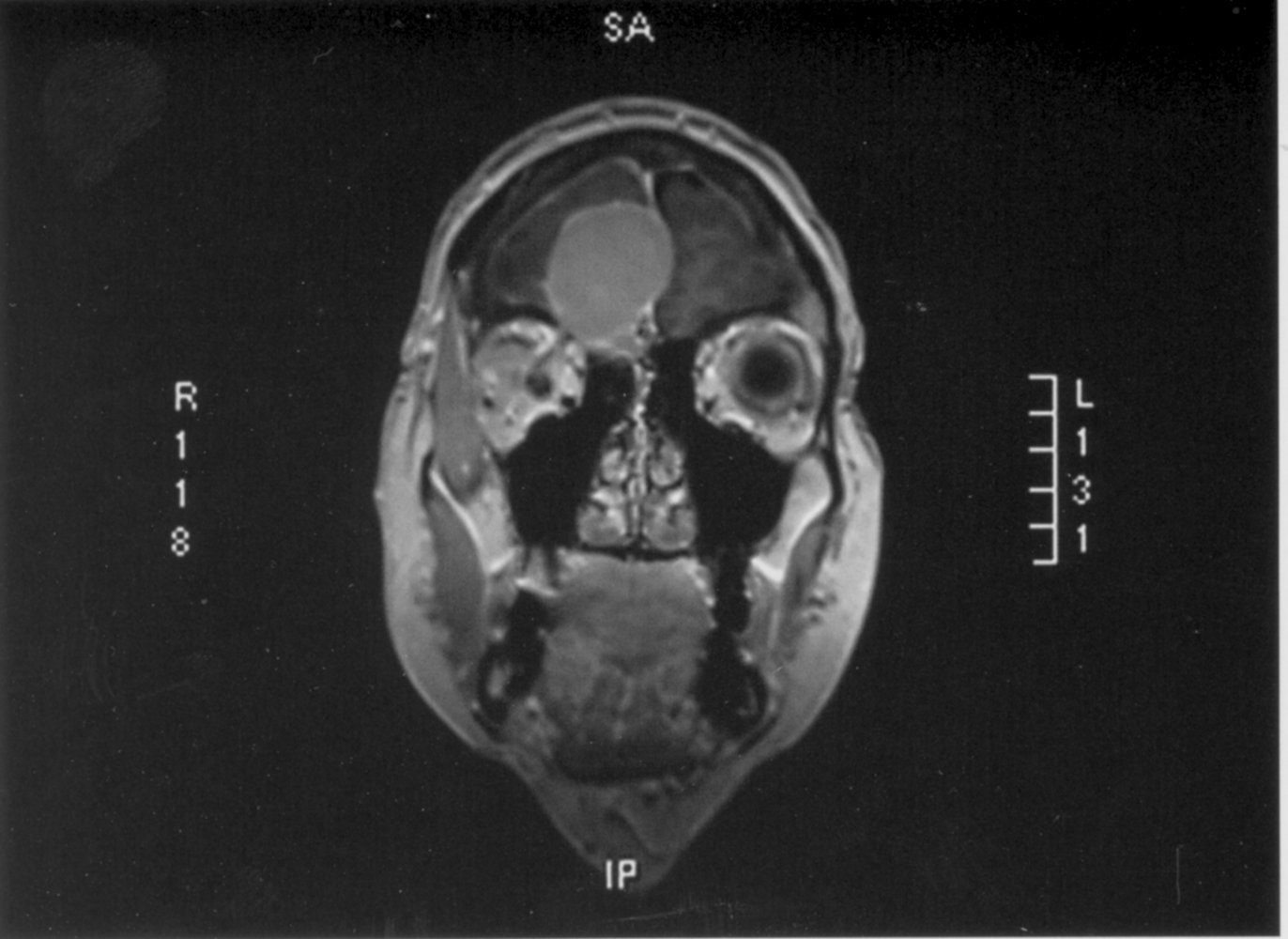
Cranial MRI after i.v. contrast administration of a patient with increasing headache and mid bitemporal hemianopia (T1-weighted, coronal view, early venous phase).
A hyperintense, rounded, clearly defined tumor in the area of the sella turcica.
It rests on the corpus sphenoidalis, has contact with both cavernous sinuses and compresses the optic chiasm.
The pituitary gland is not recognizable.
The patients' presenting symptoms alongside the radiographical appearance suggest a differential diagnosis of craniopharyngioma or pituitary adenoma.
Source: © IMPP
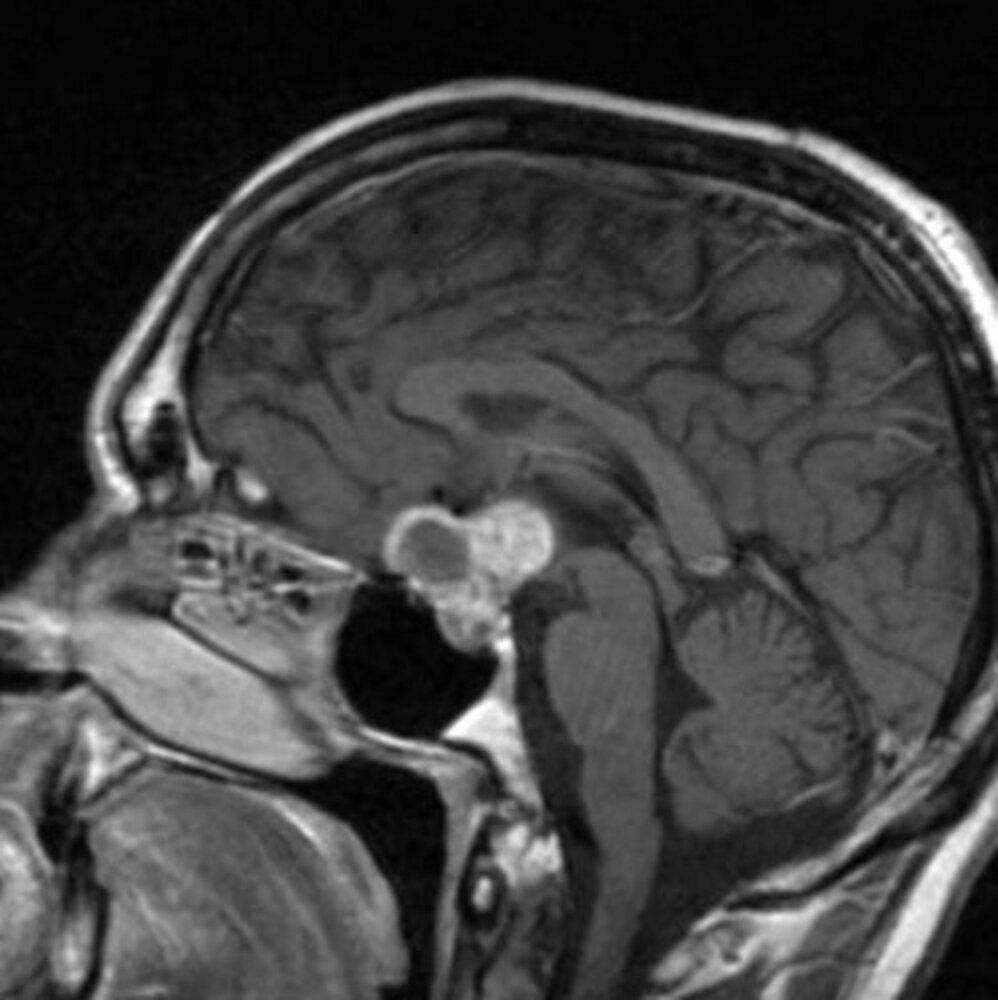
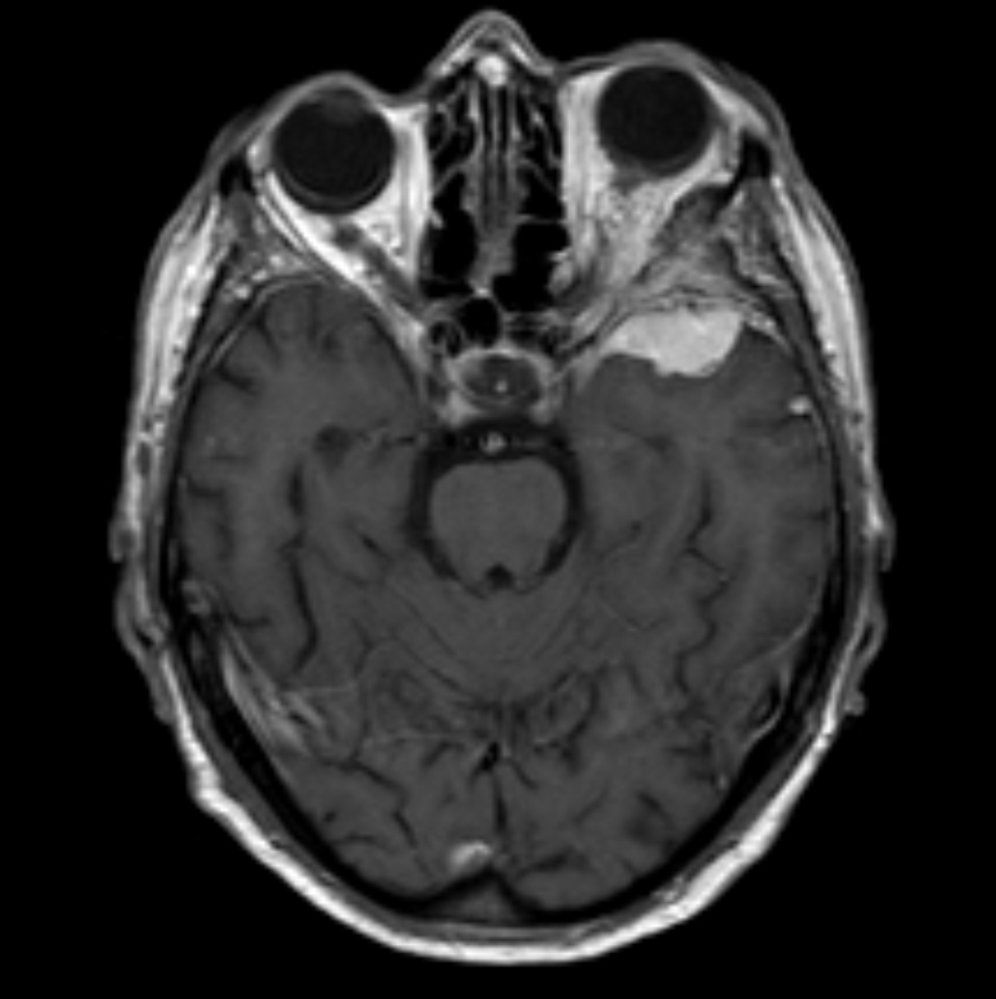
MRI head (T1 weighted; with contrast; sagittal plane) of a patient with acute visual loss in the right eye
There is an intrasellar and suprasellar mass (green overlay) with both cystic and solid portions. The solid portions show strong contrast enhancement.
Source: “Craniopharyngioma-t1sagkm-005” by Hellerhoff, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
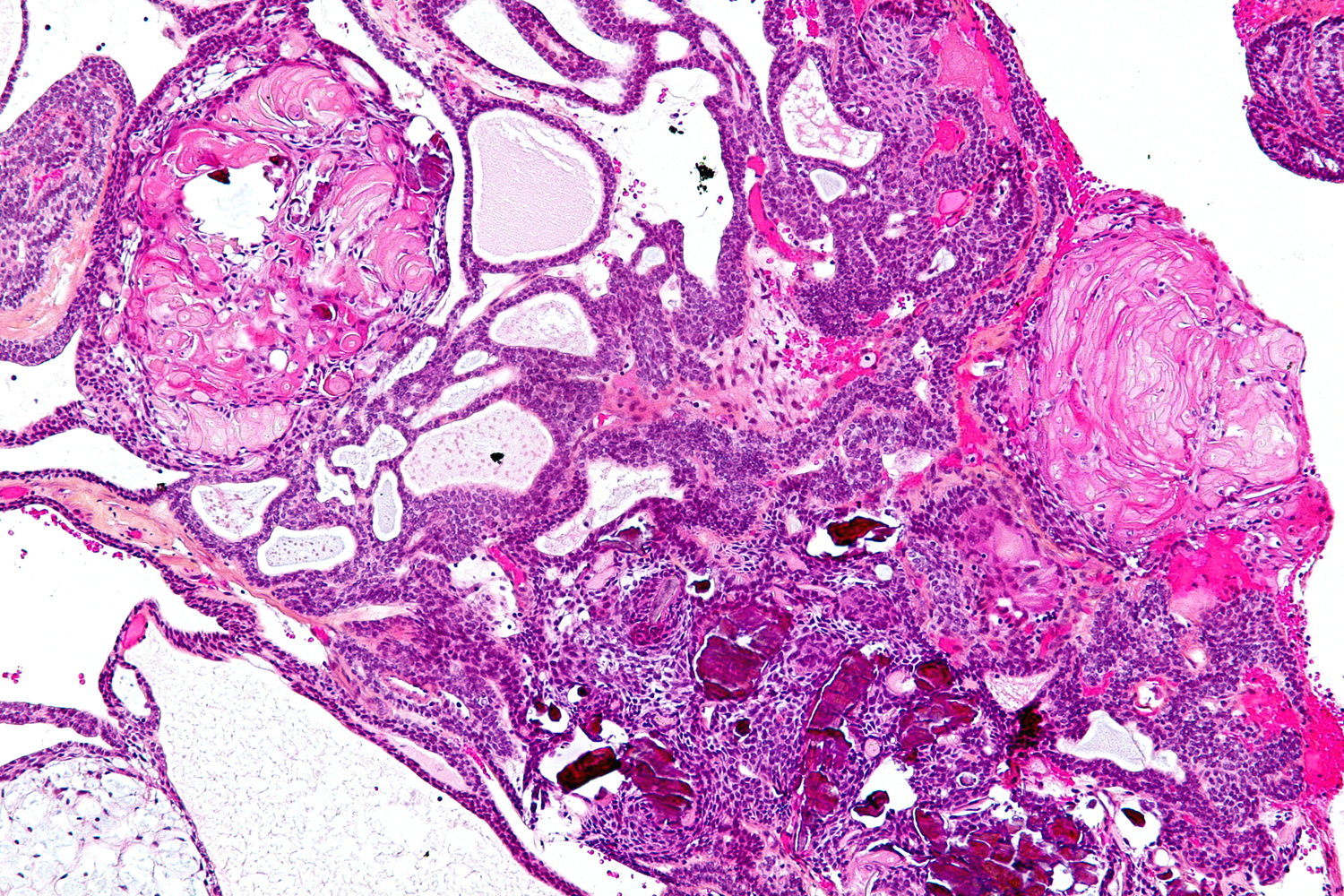
Photomicrograph of a brain tissue sample (HPS stain; intermediate magnification)
Trabeculae and nests of squamous epithelium (examples indicated by yellow overlay) with palisading cells (examples indicated by blue hatched overlay) are visible.
Additionally, there are multiple cysts (examples indicated by yellow hatched overlay), nodules of anuclear ghost cells (examples indicated by blue overlay) containing wet keratin, and calcifications (examples indicated by blue outline) .
This is the typical histological appearance of an adamantinomatous craniopharyngioma.
Source: “Adamantinomatous craniopharyngioma - intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Pineal gland tumor
- Description: a tumor that forms in or near the pineal gland and includes pineocytomas, pineoblastomas, and pineal germinomas
-
Epidemiology
- ♂ > ♀
- < 1% of all CNS tumors in adults
-
Clinical features
-
Compression of dorsal midbrain leads to:
- Compression of tectum → vertical gaze palsy (Parinaud syndrome)
- Compression of cerebral aqueduct → noncommunicating hydrocephalus
- Compression of hypothalamic inhibiting pathways → increased hCG secretion → precocious puberty
-
Compression of dorsal midbrain leads to:
- Diagnostics: MRI of the brain and biopsy
-
Histology
- Approx. 70% are germinomas (similar appearance to testicular seminoma)
- Large vacuolated cells with round nuclei (fried egg cells)
- Lymphoid stroma
-
Treatment
- Resection
- Adjuvant radiochemotherapy
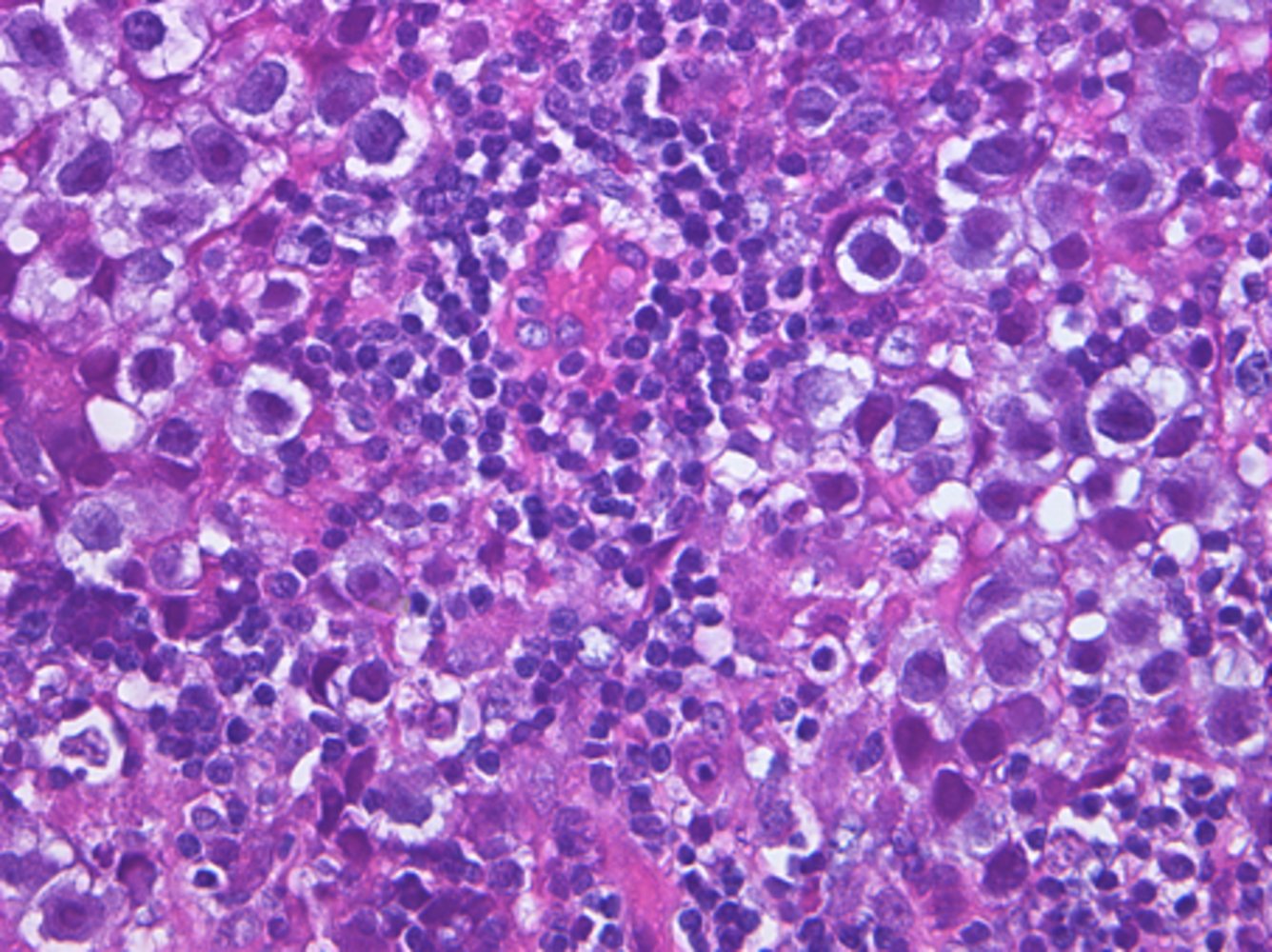
Photomicrograph of a pineal tumor biopsy sample (H&E stain; high magnification)
Large tumor cells with abundant pale cytoplasm and pleomorphic nuclei can be seen (examples marked by green overlay). Additionally, the tumor tissue contains numerous intermixed lymphocytes (comparatively small cells with round dark nuclei).
These histopathological findings are consistent with a pineal germinoma, which was confirmed by immunohistochemistry; ovarian dysgerminomas and testicular seminomas have a very similar appearance.
Source: “Figure 2A. in: Synchronized multiple regression of diagnostic radiation-induced rather than spontaneous: disseminated primary intracranial germinoma in a woman: a case report” by Yuichiro Yoneoka, Itaru Tsumanuma, Shinya Jinguji, Manabu Natsumeda & Yukihiko Fujii, Journal of Medical Case Reports, BioMed Central, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Hemangioblastoma
- Description: : a benign, highly vascularized neoplasm
-
Epidemiology
- Rare
- Peak incidence: 20–50 years
- Associated conditions: von Hippel-Lindau disease
-
Clinical features
- The cerebellum is the most common location → cerebellar defects
- Compression of the 4th ventricle → non-communicating hydrocephalus → features of raised ICP (e.g., papilledema, headache)
- Erythropoietin production by tumor cells → secondary polycythemia
-
Diagnostics
-
MRI; : sharply demarcated intra-parenchymal cystic mass with a non-enhancing wall and an enhancing mural nodule in ∼ 60% of cases [59][60]
- T2: hyperintense mass
- T1: hypointense or isointense mass
- Biopsy: thin-walled capillary vessels, densely packed together with scarce parenchyma
-
MRI; : sharply demarcated intra-parenchymal cystic mass with a non-enhancing wall and an enhancing mural nodule in ∼ 60% of cases [59][60]
-
Treatment
- Resection
- Antiangiogenic therapy (e.g., bevacizumab)
- Prognosis: Recurrence risk is < 20% in sporadic cases. [61]


")

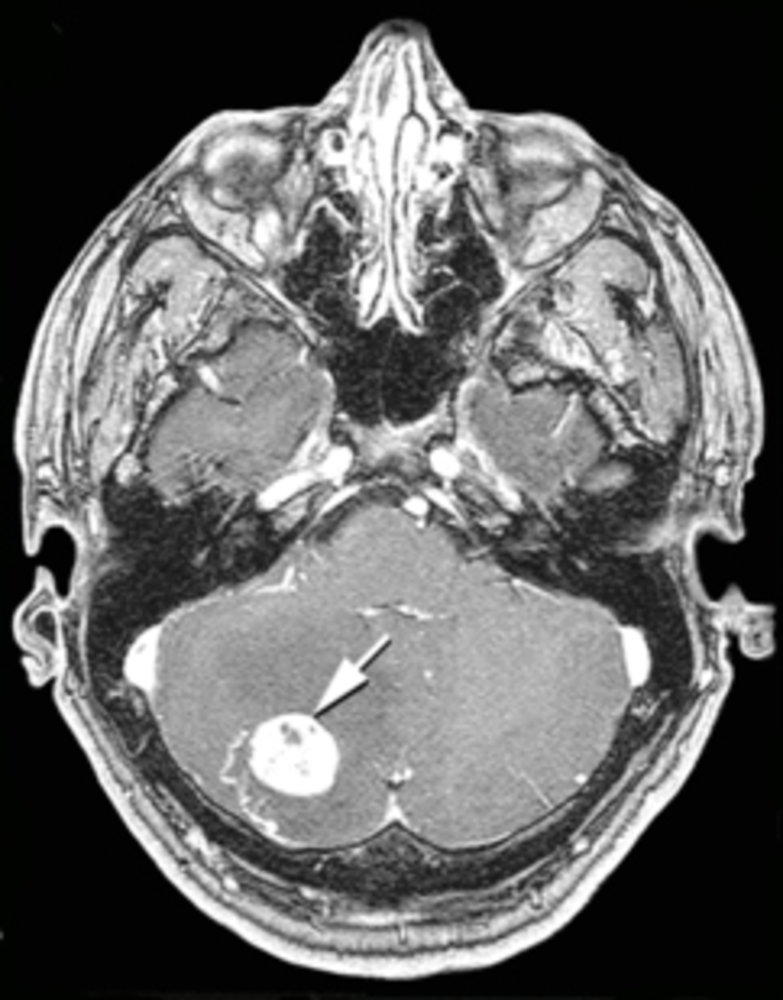
MRI head (with contrast; axial view)
A brightly enhancing, sharply delimited nodular mass (white arrow) with nonenhancing, cystic areas is visible within the right cerebellar hemisphere.
These findings are consistent with cerebellar hemangioblastoma.
Source: “Figure 1, in: von Hippel-Lindau Disease-Associated Hemangioblastomas Are Derived from Embryologic Multipotent Cells” by Deric M Park, Zhengping Zhuang, Ling Chen et al., Plos Medicine, licensed under CC BY 2.5.
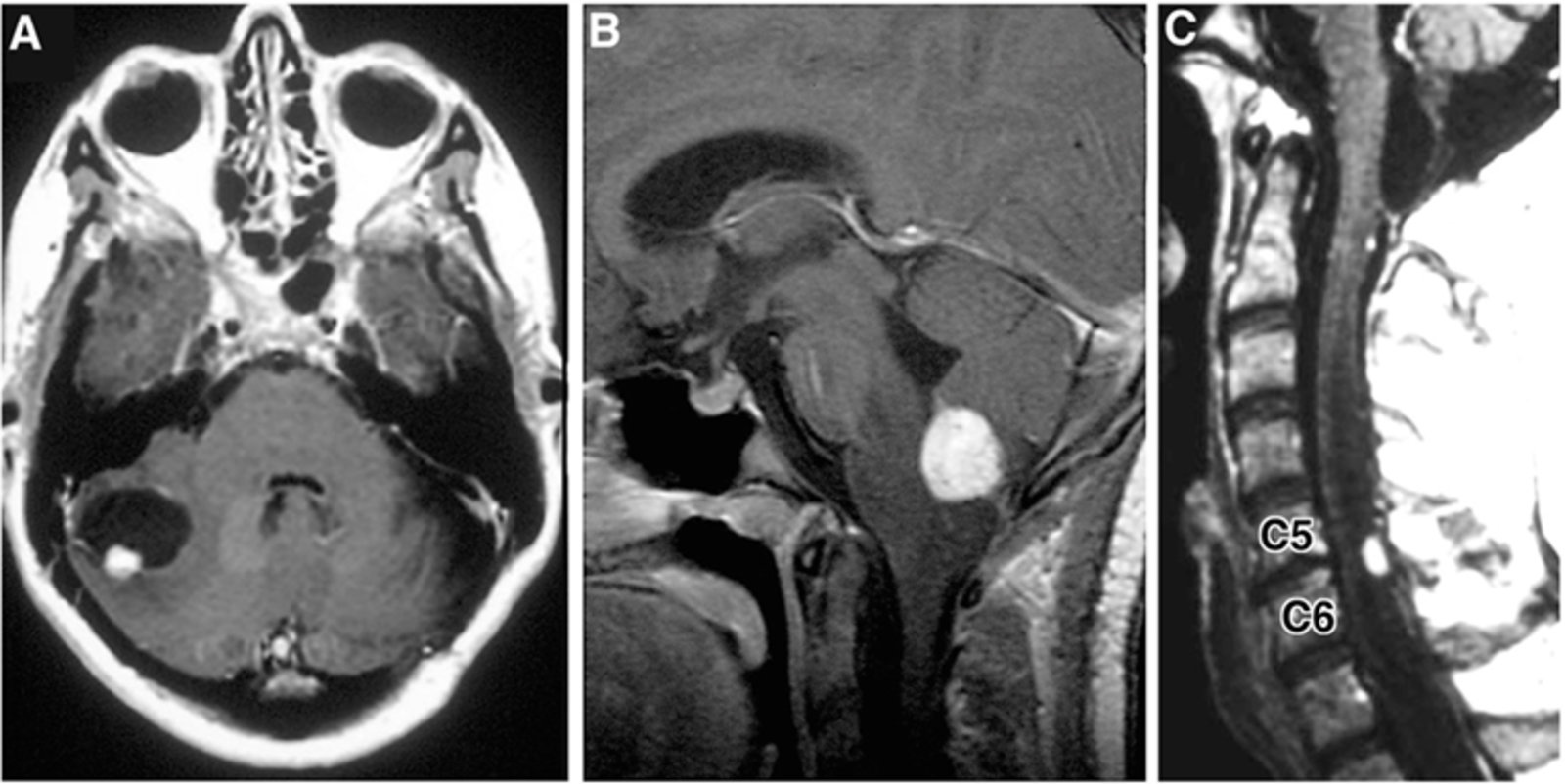
MRI images (contrast-enhanced; T1-weighted) of a patient with Von-Hippel-Lindau syndrome.
Image A (brain; axial view) shows a tumor within the lateral aspect of the right cerebellum. It consists of an enhancing solid component (red overlay) and a larger, hypointense part representing a cystic component (blue overlay).
Image B (brain; sagittal view) shows a contrast-enhancing tumor (green overlay) between medulla oblongata and cerebellum, within the region of the foramen of Magendie/median aperture.
Image C (spine MRI; sagittal view) shows a hyperintense tumor (yellow overlay) within the dorsal/posterior spinal canal at the level of vertebra C5-C6.
Von-Hippel-Lindau syndrome is a hereditary disorder characterised by the development of tumors in multiple parts of the body. This includes hemangioblastomas of the central nervous system, such as in this example. Hemangioblastomas are highly vascular tumours, resulting in the intense enhancement demonstrated on these post contrast images. Peritumoural cysts are common in these tumors, and result from plasma ultrainfiltrate passing through the permeable tumor blood vessels.
Source: “Figure 3. in: Personalized Medicine for Nervous System Manifestations of von Hippel–Lindau Disease” by Victoria Schunemann, Kristin Huntoon, Russell R. Lonser, Frontiers in Surgery Journal, Neurosurgery, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
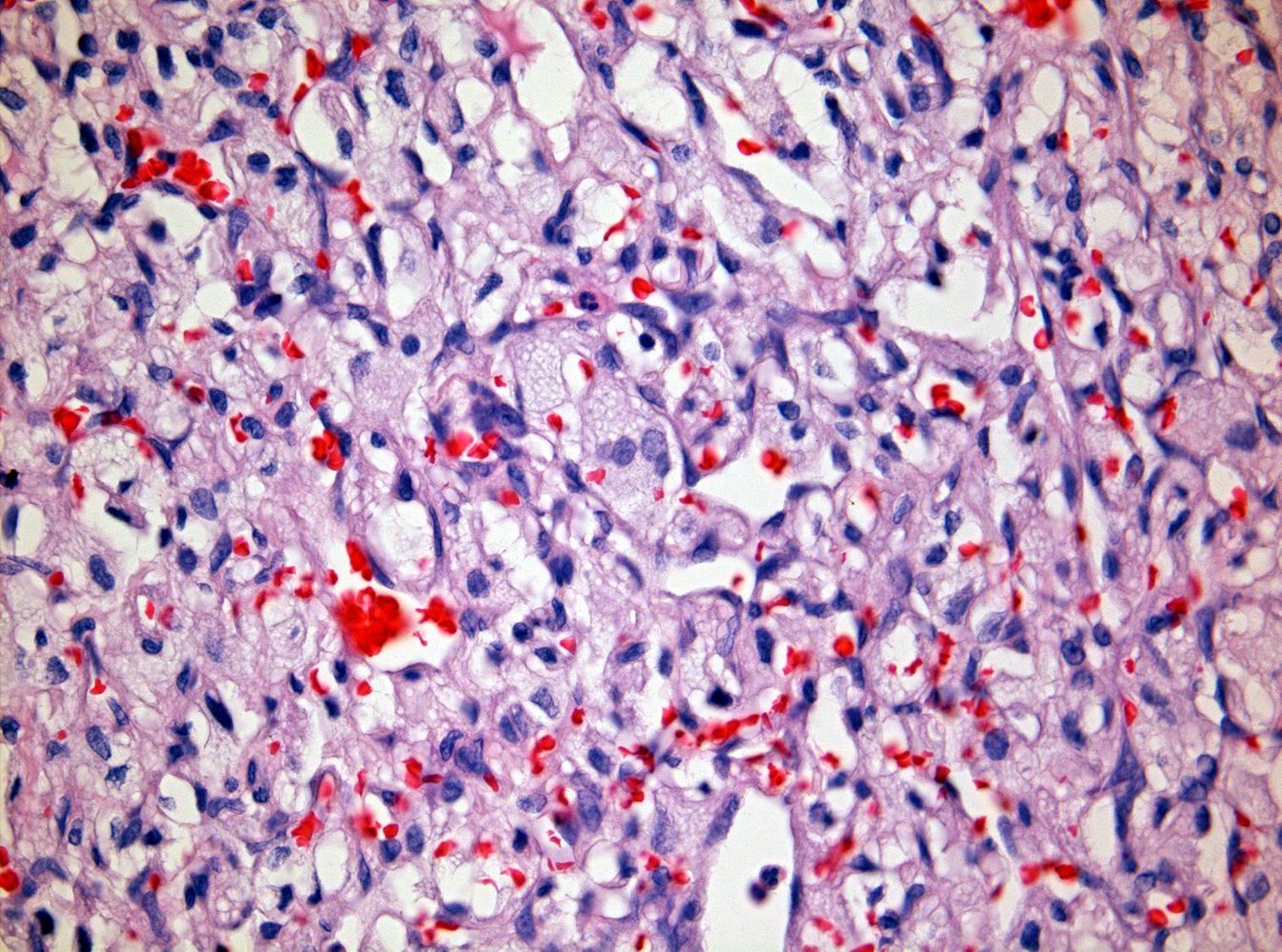
Photomicrograph of a cerebellar tissue specimen (HPS stain; high magnification)
Numerous polygonal neoplastic stromal cells with lipid-laden vacuoles (examples indicated by arrowheads) can be seen, resulting in the typical clear-cell appearance. Additionally, there is an abundance of small, thin-walled blood vessels, many of which are densely packed together (examples indicated by blue overlay).
Source: “Cerebellar hemangioblastoma high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
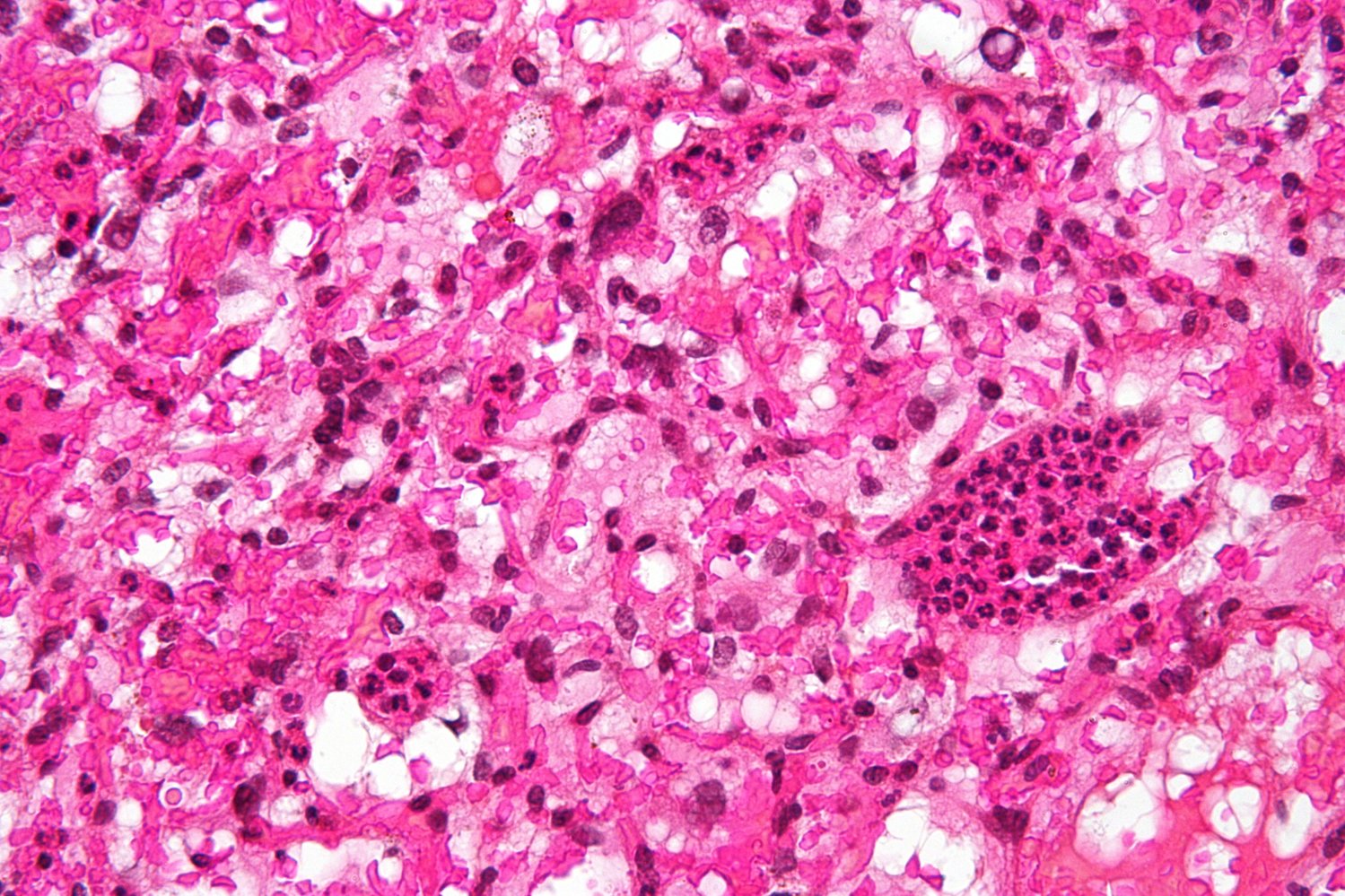
Photomicrograph of a biopsy from a cerebellar mass (H&E stain; high magnification)
Numerous thin-walled small blood vessels (examples indicated by yellow overlay) containing red stained erythrocytes are visible throughout the tumor.
Surrounding the blood vessels large stromal cells (examples indicated by blue overlay) with pale intracytoplasmic lipid inclusions (so-called "foamy" cytoplasm) can be seen.
This appearance is indicative of hemangioblastoma. The diagnosis was confirmed by immunohistochemistry.
Source: “Hemangioblastoma Histology HE” by Marvin 101, Wikimedia Commons, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
{kind=link}
Primary CNS lymphoma (PCNSL)
Definition [9][62]
PCNSL is a rare form of extranodal non-Hodgkin lymphoma that affects the CNS (e.g., brain, eyes, spinal cord, CSF).
Epidemiology [9]
- ∼ 4% of CNS neoplasms [9]
- Highest incidence: adults aged 70–79 years [9]
- Commonly associated with immunosuppression (e.g., poorly controlled HIV/AIDS) and/or EBV infection
Clinical features [9]
- Focal neurological deficits
- Nonspecific cognitive or behavioral changes
- Signs of increased ICP, e.g., headache
- Seizures (less common)
Diagnostics [9][63]
Initial evaluation
-
Neuroimaging
-
Gadolinium-enhanced MRI brain
- Obtain for all patients.
- Supportive findings include periventricular lesions with homogeneous enhancement.
- Gadolinium-enhanced MRI spine: Obtain if there are symptoms of spinal cord lesions.
-
Gadolinium-enhanced MRI brain
-
Histopathology or cytopathology: necessary for diagnostic confirmation
- Preferred: stereotactic brain biopsy
- Alternatives
- Lumbar puncture: CSF cytology or flow cytometry
- Vitrectomy: vitreous fluid cytology or flow cytometry
When present, lymphoma cells in CSF or vitreous fluid may be sufficient to establish a diagnosis of PCNSL. [9]
Additional evaluation [63]
-
Pretreatment evaluation
- Clinical evaluation
- Thorough physical examination including lymph nodes and testicles
- Cognitive assessment to establish baseline cognitive function
-
Laboratory studies
- CMP: Ensure hepatic and renal function are adequate for undergoing treatment.
- LDH: Elevated LDH is a poor prognostic factor.
- HIV testing
- Clinical evaluation
-
Staging
- Obtain NHL staging, including:
- Lumbar puncture with CSF assessment
- Whole-body imaging
- Bone marrow biopsy
- Refer for ophthalmology evaluation (including a slit-lamp examination).
- Assess for secondary malignancies.
- Obtain NHL staging, including:
Treatment [9][62]
- Optimal treatment regimens are an area of ongoing investigation.
- Most regimens include rituximab, high-dose methotrexate, and an alkylating agent.
- Surgical resection is usually not indicated.
- Low-dose whole brain radiotherapy can be used as part of consolidation therapy or palliative therapy.
- Monitor for complications of brain tumors.
Glucocorticoids can decrease diagnostic yield in lymphoma. Except in situations of life-threatening increased ICP, avoid glucocorticoid use until diagnostic tissue and fluid samples have been obtained. [9]
Prognosis [9]
- Variable
- Typically better than other primary CNS tumors but less favorable than non-CNS lymphomas
MRI head (A and B: T1-weighted, with contrast; C: FLAIR; axial plane) of a patient with HIV-associated primary CNS lymphoma
Ring-enhancing lesions in the right thalamus (A) and left frontal lobe (B) have central, low-signal intensity (hatched green overlay), suggesting necrosis. Hyperintense edema (green overlay) surrounds both lesions on the FLAIR sequence. Prominent sulci and ventricles reflect mild, generalized cerebral volume loss.
Toxoplasmosis and primary CNS lymphoma in patients with HIV/AIDS can have similar appearances, and further workup is needed if MRI cannot distinguish between them.
Source: “Fig. 1, in: An unusual and challenging case of HIV-associated primary CNS Lymphoma with Hodgkin-like morphology and HIV encephalitis” by Isaac E. Lloyd, Parker W. Clement, Karen L. Salzman, Randy L. Jensen, Mohamed E. Salama & Cheryl A. Palmer, Diagnostic Pathology, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Primary brain tumors according to age
Pediatric primary brain tumors [64][65][66]
-
Most pediatric brain tumors are primary.
- Most common type of benign pediatric primary brain tumor: pilocytic astrocytoma
- Most common malignant pediatric primary brain tumor: medulloblastoma
- Brain tumors are the second most common cause of pediatric cancer; after leukemia, accounting for approx. 20% of all cases of pediatric cancer and the primary cause of pediatric cancer deaths in the US.
| Overview of pediatric primary brain tumors [47][66][67] | |||
|---|---|---|---|
| Tumor | Precursor | Typical location [45] | Typical histology [49][68] |
| Supratentorial | |||
| Craniopharyngioma [55] |
|
|
|
| Infratentorial | |||
| Pinealoma |
|
|
|
| Pilocytic astrocytoma |
|
|
|
| Medulloblastoma |
|
|
|
| Ependymoma [69] |
|
|
|
In children, most primary brain tumors arise infratentorial, craniopharyngiomas being an important exception.



Adult primary brain tumors [2]
-
Primary brain tumors are less common than brain metastases in adults.
- Most common benign primary brain tumor in adults: meningioma
- Most common malignant primary brain tumor in adults: glioblastoma multiforme
- Primary brain tumors account for 1–2% of cancer cases in adults.
| Overview of adult primary brain tumors [47][67] | |||
|---|---|---|---|
| Tumor | Precursor | Typical locations [45] | Typical histology [49] |
| Glioblastoma multiforme (WHO grade IV astrocytoma) [70] |
|
|
|
| Meningioma [71] |
|
|
|
| Hemangioblastoma [72] |
|
|
|
| Schwannoma [73] |
|
|
|
| Oligodendroglioma [41] |
|
|
|
| Pituitary adenoma [74] |
|
|
|
In adults, most primary brain tumors arise supratentorially, hemangioblastomas and schwannomas being important exceptions.












")



")
© AMBOSS
MRI of the brain (T1-weighted; sagittal view; with contrast)
A hyperintense, ovoid, sharply demarcated lesion (green overlay) is visible within the sella turcica and partially extends into the sphenoidal sinus.
The location and appearance of the lesion suggest a craniopharyngioma or a pituitary adenoma.
Source: © IMPP
Photomicrograph of a brain tissue sample (HPS stain; intermediate magnification)
Trabeculae and nests of squamous epithelium (examples indicated by yellow overlay) with palisading cells (examples indicated by blue hatched overlay) are visible.
Additionally, there are multiple cysts (examples indicated by yellow hatched overlay), nodules of anuclear ghost cells (examples indicated by blue overlay) containing wet keratin, and calcifications (examples indicated by blue outline) .
This is the typical histological appearance of an adamantinomatous craniopharyngioma.
Source: “Adamantinomatous craniopharyngioma - intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Photomicrograph of a pineal tumor biopsy sample (H&E stain; high magnification)
Large tumor cells with abundant pale cytoplasm and pleomorphic nuclei can be seen (examples marked by green overlay). Additionally, the tumor tissue contains numerous intermixed lymphocytes (comparatively small cells with round dark nuclei).
These histopathological findings are consistent with a pineal germinoma, which was confirmed by immunohistochemistry; ovarian dysgerminomas and testicular seminomas have a very similar appearance.
Source: “Figure 2A. in: Synchronized multiple regression of diagnostic radiation-induced rather than spontaneous: disseminated primary intracranial germinoma in a woman: a case report” by Yuichiro Yoneoka, Itaru Tsumanuma, Shinya Jinguji, Manabu Natsumeda & Yukihiko Fujii, Journal of Medical Case Reports, BioMed Central, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
MRI head (a: T1-weighted; with contrast; sagittal plane; b: T2-weighted; axial plane) of a child
A large lesion in the right cerebellar hemisphere displaces the vermis to the left of midline. It has a large cystic component (T1 hypointense and T2 hyperintense; red overlay) and a heterogeneously enhancing solid nodular component (green overlay).
Cerebellar pilocytic astrocytoma frequently manifests as a large cystic lesion with an enhancing mural nodule.
Source: “Figure 1, in: The Journal of Headache and Pain” by Irene Toldo, Debora De Carlo, Rodica Mardari et al., The Journal of Headache and Pain, licensed under CC BY 2.0. Modifications: - Labels have been removed from original image (asterix and two arrows). - letters edited. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
MRI head (T1-weighted; with contrast; A: axial view; B: coronal view) of a 19-year-old patient
There is a large mass within the midline of the posterior fossa predominantly located within the pons but also extending towards and indenting the cerebellar peduncles and cerebellar hemispheres. Most of the lesion does not enhance and is cystic, demonstrated by the hypointense signal (green overlay). There is peripheral enhancement, demonstrated by the hyperintense signal, with a particularly prominent region of enhancement shown posteriorly on the axial image (red overlay), representing a mural nodule.
This mass is a pilocytic astrocytoma. The mass is in an atypical region, considering the patient's age, as these tumors usually arise in the posterior fossa in children and in the supratentorial area in adults. Other tumors that occur in a similar location in the posterior fossa would be medulloblastoma, hemangioblastoma, and ependymoma.
Source: “Figure 4. in: Stereotaxic gamma knife surgery in treatment of critically located pilocytic astrocytoma: preliminary result” by Raef FA Hafez, World Journal of Surgical Oncology, BioMed Central, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Photomicrograph of cerebellar tissue (H&E stain)
There are numerous bipolar cells, composed of a central basophilic nucleus with eosinophilic pilocytic processes (examples indicated in green) arising from either end. The pilocytic processes are arranged in bundles, which resemble matted hair. The bright red-pink bodies are intracytoplasmic inclusions (examples indicated by black arrowheads) in astrocytes and indicate intense gliosis (Rosenthal fibers).
These are the characteristic features of pilocytic astrocytoma.
Source: “PilocyticAstrocytoma 20x HE” by Marvin 101, Wikipedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Photomicrograph of a tissue section of a brain mass (H&E stain; high magnification)
There is an abundance of eosinophilic, fusiform inclusions (Rosenthal fibers; examples indicated by blue overlay).
Rosenthal fibers are intracellular inclusions within astrocyte cytoplasmic processes. They represent a nonspecific degenerative changes that are often found in CNS tumors (in this case in pilocytic astrocytoma).
Source: “Rosenthal HE 40x.jpg” by Marvin 101, Wikimedia commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
MRI Head (T2-weighted; axial view) of a 7-year-old boy
There is a lobulated heterogeneous posterior fossa mass (green overlay) present in the midline of the cerebellum at the level of the fourth ventricle. The fourth ventricle is obscured by the mass and is, therefore, not well seen in this image.
This is a medulloblastoma, the most common malignant pediatric tumor of the central nervous system. Medulloblastomas most commonly involve the cerebellar vermis, the structure that connects the two cerebellar hemispheres. In the pediatric population, other tumors that commonly occur in similar locations include brainstem glioma, ependymoma, choroid plexus papilloma, atypical teratoid/rhabdoid tumor, and astrocytoma. All of these should be considered in this case, although a brainstem glioma would rather be located predominantly within the brainstem rather than the vermis and is, therefore, less likely.
Arrowhead: basilar artery; C: cerebellum
Source: © IMPP
Head MRI (T2 weighted image)
Medulloblastoma within the posterior cranial fossa (green border in overlay). The lesion contains cystic areas, particularly on the left side (green overlay).
Source: © IMPP
Cranial MRI (T1-weighted, with contrast)
There is a mass in the posterior cranial fossa. It features solid parts (green overlay) and cystic parts (red overlay).
Location and appearance are typical of a medulloblastoma.
(D: diencephalon; P: pons; C: cerebellum; yellow outline: cerebellar tentorium)
Source: © IMPP
Photomicrograph of cerebellar vermis tissue (H&E stain)
Densely packed, small, blue anaplastic cells are present throughout the specimen. The cells have pleomorphic and hyperchromatic nuclei.
On the right, a vessel (its lumen mostly obstructed by eosinophilic material) can be seen.
These are typical histopathological findings of medulloblastoma.
Source: “Histopathologic image of medulloblastoma in cerebellar vermis in an adult patient. H & E stain.” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0.
Photomicrograph of cerebellar vermis tissue (H&E stain)
Numerous small, blue, round cells with scant cytoplasm can be seen throughout the specimen (examples indicated by green overlay). Their nuclei vary in size and structure (nuclear pleomorphism) and many cells feature distinctly hyperchromatic nuclei.
The majority of the cells are arranged in concentric clusters around lighter central areas consisting of neuropil (examples indicated by yellow overlay). These clusters are referred to as Homer Wright rosettes.
These histopathological features, particularly the Homer Wright rosettes, are characteristic of a medulloblastoma.
Source: “Medulloblastoma with rosettes” by Jensflorian, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
MRI brain (FLAIR; sagittal view)
A well-defined heterogeneous hyperintense lesion is visible within the expanded 4th ventricle (green overlay). At the superior aspect of the lesion, multiple dark foci are present (arrowheads), representing cysts. They appear dark in this image as the fluid signal is removed on FLAIR sequences. This lesion has obstructed circulation of the cerebrospinal fluid, resulting in ventriculomegaly (indicated by dashed line).
Ependymomas commonly arise within the fourth ventricle. They are usually hyperintense on T2 weighted/FLAIR images and can demonstrate cystic change, such as in this case, as well as hemorrhage.
Source: “Ependymom sag FLAIR” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Photomicrograph of brain tissue (H&E stain)
Tumor cells (cylindrical epithelium) are arranged in a radial manner around several vessels. This pattern is called a perivascular pseudorosette.
Perivascular pseudorosettes are a hallmark of ependymoma.
Source: “Ependymoma pseudorosette” by Jensflorian, Wikimedia Commons, licensed under CC BY 3.0.
Photomicrograph of a brain tumor tissue specimen (H&E stain; low magnification)
There is an abnormally high number of cells with round nuclei and abundant eosinophilic cytoplasm. Some cells are arranged in a spoke-and-wheel pattern, surrounding an empty central space. Such patterns are called ependymal rosettes (example indicated by green overlay). Other cells are arranged concentrically around blood vessels, producing a similar appearance (perivascular pseudorosettes; example indicated yellow overlay).
These are typical histopathological features of ependymoma.
Source: “Ependymoma low intermed mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
MRI brain (T1-weighted; with contrast; axial plane) of a 69-year-old patient with personality changes and left-sided hemiparesis.
In the white matter of the right hemisphere, there is a large, poorly circumscribed space-occupying lesion, which is hypointense centrally (green overlay) with strong peripheral contrast enhancement (red overlay). The lesion is surrounded by edema (white overlay), suggesting rapid growth and displacement of surrounding structures. The mass effect has also caused a slight midline shift to the contralateral side (white dashed line), and compression of the right lateral ventricle (white arrowheads indicate anterior horn compression).
These radiographic features are typical of a glioblastoma.
Source: © IMPP
CT head (without contrast; axial plane) of a 69-year old man with a history of personality changes and left-sided hemiparesis from glioblastoma
The right cerebral hemisphere is diffusely abnormal, with intermixed hypodense (green overlay), isodense, and hyperdense (red overlay) areas. There is mass effect with sulcal effacement and midline shift to the left (dashed line). The frontal and occipital horns (arrowheads) of the right lateral ventricle are effaced.
Yellow overlay: choroid plexus calcification
Blue overlay: falx cerebri calcification
Source: © IMPP
MRI head (top: T2-weighted; middle: T1-weighted without contrast; bottom: T1-weighted with contrast; axial plane)
A heterogeneous lesion in the left frontal lobe distorts the interhemispheric fissure (indicated by white arrowhead). On the T1-weighted sequences, the lesion is predominantly hypointense (green overlay) with garland-like enhancement (yellow overlay). Associated edema is hyperintense on the T2-weighted sequence (red overlay).
Source: © IMPP
Frontal section of a macroscopic brain preparation: There is a tumorous lesion with a macroscopic typical "colorful cut surface" in the temporal lobe. The yellow areas are necrosis and the marked white areas are cell dense regions. The surrounding red marked areas most likely correspond to the margin of a vessel or hemorrhage. The findings correspond to a glioblastoma.
Source: © IMPP
T1-weighted contrast-enhanced MRI, frontal view: bihemisphere garland-like contrast enhancement. There is peripheral contrast agent enhancement (blue overlay) with central necrosis (green overlay). The third ventricle (arrowhead) is centrally located. The tumor is displacing the posterior horn of the lateral ventricle (red overlay). Diagnosis: bilateral glioblastoma (butterfly glioma).
Source: © IMPP
Photomicrograph of a cerebral tissue specimen (H&E stain; high magnification)
A high number and density of highly pleomorphic cells with hyperchromatic and irregular nuclei are visible (examples indicated by arrowheads. These cells are aggregated around the periphery of the necrotic zone (green overlay), forming a nuclear pseudopalisading architecture.
These are the characteristic features of glioblastoma multiforme.
Source: “Histopathological image of cerebral glioblastoma. Hematoxylin & esoin stain.” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Photomicrograph of the brain (H&E stain)
Diffuse infiltration of the central nervous tissue by astrocytic tumor tissue can be seen. Palisade-like deposits of tumor cells with hyperchromatic, polymorphic nuclei surround the anuclear necrotic lesions. There are numerous mitotic figures. There is an abundance of capillary bundles with a hyperplastic endothelium. The tissue shows extensive, regressive changes.
Diagnosis: glioblastoma (WHO grade IV)
Source: © IMPP
CT head (with contrast; axial plane)
A rounded circumscribed extraaxial mass (blue overlay) located in the midline low anterior cranial fossa shows homogenous contrast enhancement.
Source: © IMPP
MRI head (T1-weighted; with contrast; sagittal plane)
There is a well-circumscribed homogeneous mass (green overlay) along the cerebral convexity. It demonstrates intense, homogeneous enhancement, equivalent to that of adjacent dura mater. Displacement without invasion of the surrounding white matter supports an extra-axial location.
This is a case of meningioma, a dural-based tumor. The dura is represented in this image by the thin, discontinuously enhancing line covering the inner surface of the skull (indicated by arrowhead).
Source: © IMPP
MRI brain (T1-weighted, with contrast, sagittal plane) of a 68-year-old with reduced strength and increasing discomfort in his left leg.
There is a well-defined intracranial mass overlying and appearing adherent to the inner surface of the cranium in the parasagittal region. It enhances intensely and homogeneously. This mass compresses the surrounding brain parenchyma without invading it.
Meningiomas arising from the sagittal midline normally arise from the falx cerebri, the dural fold separating the two cerebral hemispheres, and are given the subtype of parasagittal meningioma.
Source: © IMPP
MRI Head (T1 weighted; with contrast; coronal plane)
There is a well-circumscribed, homogeneously enhancing rounded mass (green overlay) continuous with the falx cerebri and dura of the right parietal bone. It does not invade the surrounding brain tissue or bone.
This is a case of meningioma. This is the most common diagnosis for a dural-based mass with smooth margins and homogeneous contrast enhancement. Other important differentials include lymphoma and metastasis, both of which would more likely (but not always) be less uniform in shape and enhanceheterogeneously.
Source: © IMPP
MRI Head (T1 weighted; with contrast; axial plane)
There is a well-circumscribed, homogeneously enhancing rounded mass (green overlay) continuous with the falx cerebri. It does not invade the surrounding brain tissue.
Source: © IMPP
Cranial MRI, axial view (T1-weighted; with contrast)
Round, sharply delimited, homogeneously enhancing, hyperintense lesion (snowball appearance) in the interhemispheric region of the frontal lobe (green overlay).
The lesion displaces brain tissue. The dura is connected to the meninges of the frontal bone (dural tail sign) by a thick, hyperintense strand. A thin rim separates the lesion from surrounding brain parenchyma (CSF cleft sign).
These are characteristic radiologic features of a meningioma.
Source: “MeningiomaMRISegmentation” by Rkikinis, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: cropped image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
MRI head (T1-weighted; with contrast; sagittal plane) of a 58-year-old patient with parosmia.
There is a large, well-defined mass with homogeneous contrast enhancement in the olfactory groove (green overlay.
This is an example of an olfactory groove meningioma.
Source: © IMPP
MRI Head (T1-weighted; with contrast; coronal plane) of a 58-year-old patient with parosmia.
A well-defined and homogeneously enhancing lesion is demonstrated in the olfactory groove (green overlay). It is continuous with the falx cerebri and dura of the olfactory grove.
This is an example of an olfactory grove meningioma. The differential diagnosis includes other dural-based lesions such as dural metastasis or a solitary fibrous tumor of the dura. Homogenous enhancement is a feature that is more in keeping with a meningioma rather than these two differentials.
Source: © IMPP
MRI Head (T1-weighted; with contrast; axial plane) of a 58-year-old patient with parosmia.
A well-defined and homogeneously enhancing lesion is demonstrated in the olfactory groove (green overlay). It is continuous with the dura. The cerebral parenchyma on the right side of the lesion demonstrates poorly defined hypointense signal due to edema.
This is an example of an olfactory grove meningioma. Large meningiomas can cause compression of the surrounding cerebral parenchyma resulting in edema, as demonstrated in this example.
Source: © IMPP
MRI brain (T1-weighted, with contrast, axial plane)
There is a well-defined intracranial mass (green overlay) overlying the left sphenoid bone demonstrating intense homogeneous enhancement. There is thickening and enhancement of the surrounding dura, and the lesion is also continuous with the dura, known as the dural tail sign (blue overlay). The bone underlying the meningioma is enlarged compared to the contralateral side and demonstrates heterogeneous signal (red overlay), representing hyperostosis. The enlargement of this bone has resulted in mild anterior displacement of the left eye (proptosis; asterisk).
The intense homogeneous enhancement, dural tail sign, and hyperostosis are common features of meningiomas.
Source: “Keilbeinmeningeom MRT T1KMax” by Hellerhoff, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}
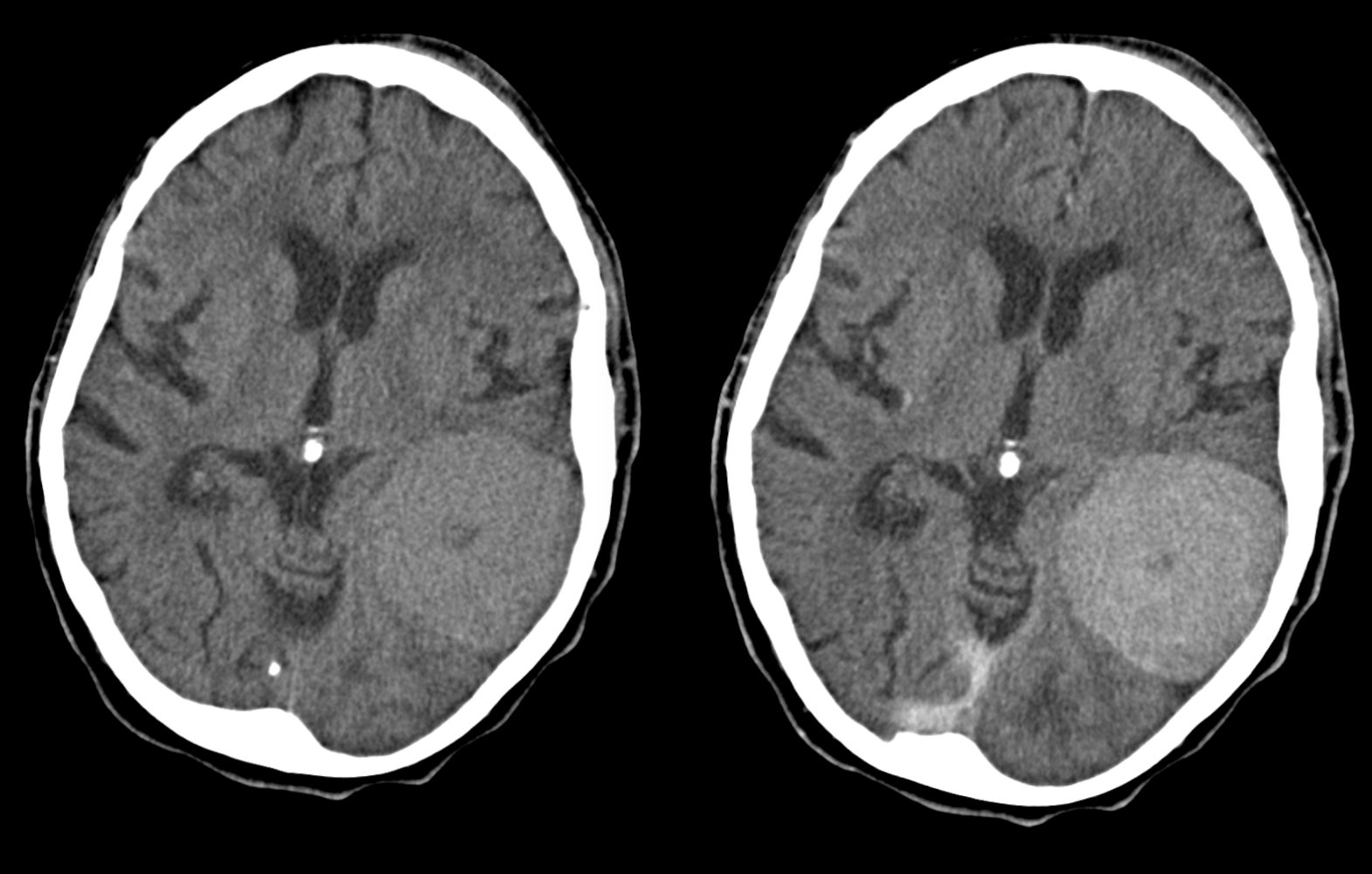
CT, axial view, plain (left) and with IV contrast (right)
Large, sharply demarcated, hyperdense lesion with a central hypodense area located in the left parietal region. Homogenous uptake of contrast medium apart from the hypodense central region. Discrete perifocal edema, which indicates compression of the surrounding tissue.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
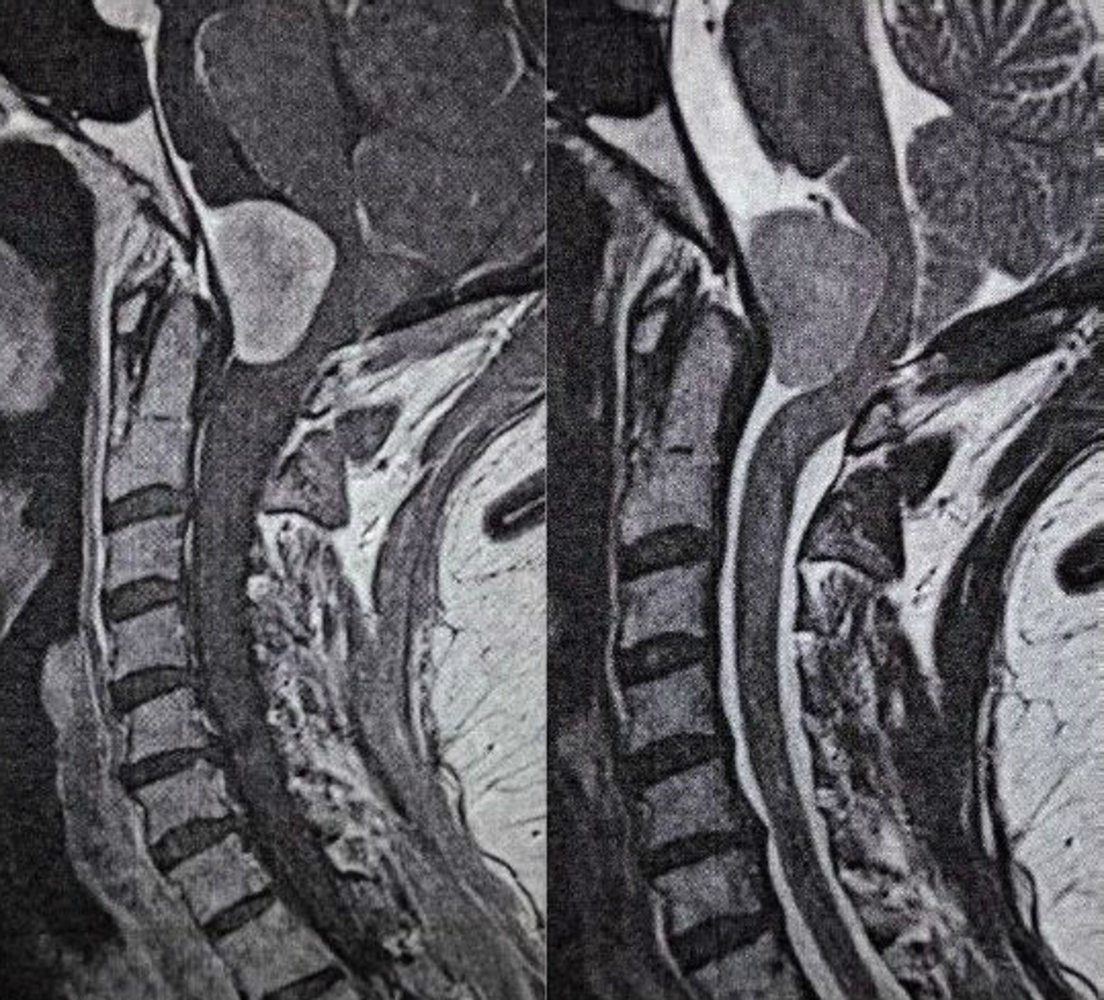
MRI of the neck and base of the skull (left: T1-weighted, with contrast, sagittal plane; right: T2-weighted, sagittal plane)
There is a well-defined mass in the anterior aspect of the foramen magnum, which enhances on the T1-weighted post-contrast image (red overlay) and appears hyperintense to gray matter on the T2-weighted image (green overlay). The mass is continuous with the adjacent thickened and enhancing dura (arrowhead). This is known as the “dural tail sign.”
The dural tail sign suggests lesion originates from the dura mater. The sign is most commonly seen in meningiomas but may also be seen in other malignancies originating in the dura mater, such as lymphoma and metastasis.
Source: “Figure 1, in: Insidious Presentation of a Foramen Magnum Meningioma – A Case Report” by Panagiotis Zogopoulos, Elyns Group, licensed under CC BY 3.0. Modifications: image has been cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Photomicrograph of tissue biopsied from a brain tumor (HPS stain)
Several eosinophilic cells are visible, arranged in whorls (purple overlay) and sheets. A mass of disorganized cells is visible in the top right corner (yellow overlay). The nuclei of these cells show features of malignancy (i.e., large size or high N:C ratio, nuclear pleomorphism, prominent nucleoli, and mitotic figures). The intervening stroma contains numerous blood vessels (green overlay).
Hypercellularity, whorled or sheet-like architecture, and hypervascularity are typical features of a meningioma. Psammoma bodies (not seen here) are another characteristic feature of meningioma and would appear as basophilic whorls.
Source: “Meningioma intermed mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
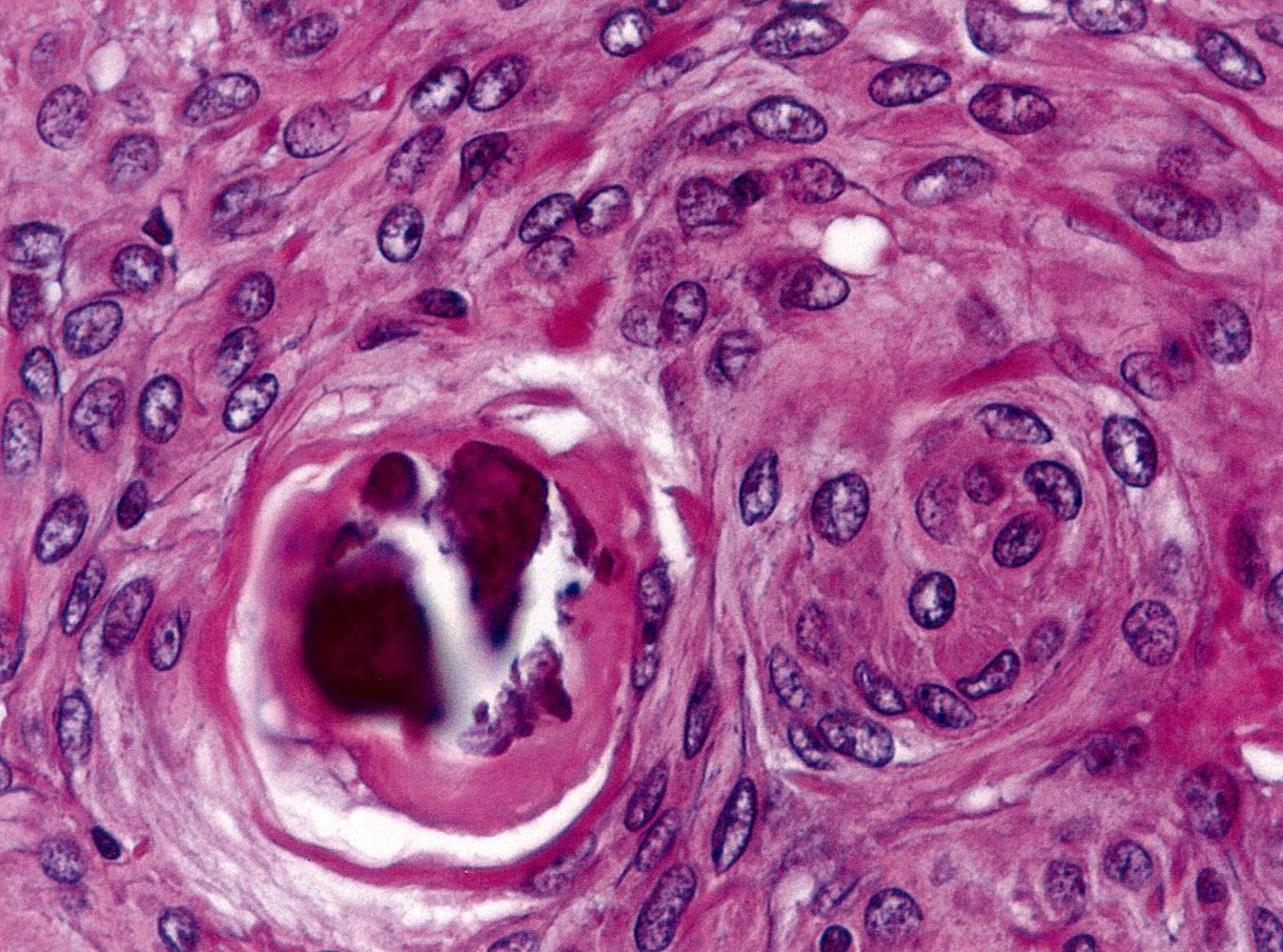
Photomicrograph of tissue biopsied from a brain tumor (H&E stain)
Several eosinophilic spindle-shaped cells with large nuclei containing prominent nucleoli are visible. The cells are arranged in a whorl-like pattern.
- Meningocytic whorl: the whorl on the right, which is composed of layers or lamellae of cells, resembling the layers of an onion
- Psammoma body: the whorl on the left, which has an acellular basophilic core surrounded by acellular lamellae. Psammoma bodies represent dystrophic calcification in areas of apoptotic tumor cells.
Psammoma bodies and spindle-shaped cells arranged in onion-skin whorls are pathognomonic features of meningioma.
Source: © IMPP
MRI head (with contrast; axial view)
A brightly enhancing, sharply delimited nodular mass (white arrow) with nonenhancing, cystic areas is visible within the right cerebellar hemisphere.
These findings are consistent with cerebellar hemangioblastoma.
Source: “Figure 1, in: von Hippel-Lindau Disease-Associated Hemangioblastomas Are Derived from Embryologic Multipotent Cells” by Deric M Park, Zhengping Zhuang, Ling Chen et al., Plos Medicine, licensed under CC BY 2.5.
Photomicrograph of a cerebellar tissue specimen (HPS stain; high magnification)
Numerous polygonal neoplastic stromal cells with lipid-laden vacuoles (examples indicated by arrowheads) can be seen, resulting in the typical clear-cell appearance. Additionally, there is an abundance of small, thin-walled blood vessels, many of which are densely packed together (examples indicated by blue overlay).
Source: “Cerebellar hemangioblastoma high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Photomicrograph of a biopsy from a cerebellar mass (H&E stain; high magnification)
Numerous thin-walled small blood vessels (examples indicated by yellow overlay) containing red stained erythrocytes are visible throughout the tumor.
Surrounding the blood vessels large stromal cells (examples indicated by blue overlay) with pale intracytoplasmic lipid inclusions (so-called "foamy" cytoplasm) can be seen.
This appearance is indicative of hemangioblastoma. The diagnosis was confirmed by immunohistochemistry.
Source: “Hemangioblastoma Histology HE” by Marvin 101, Wikimedia Commons, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
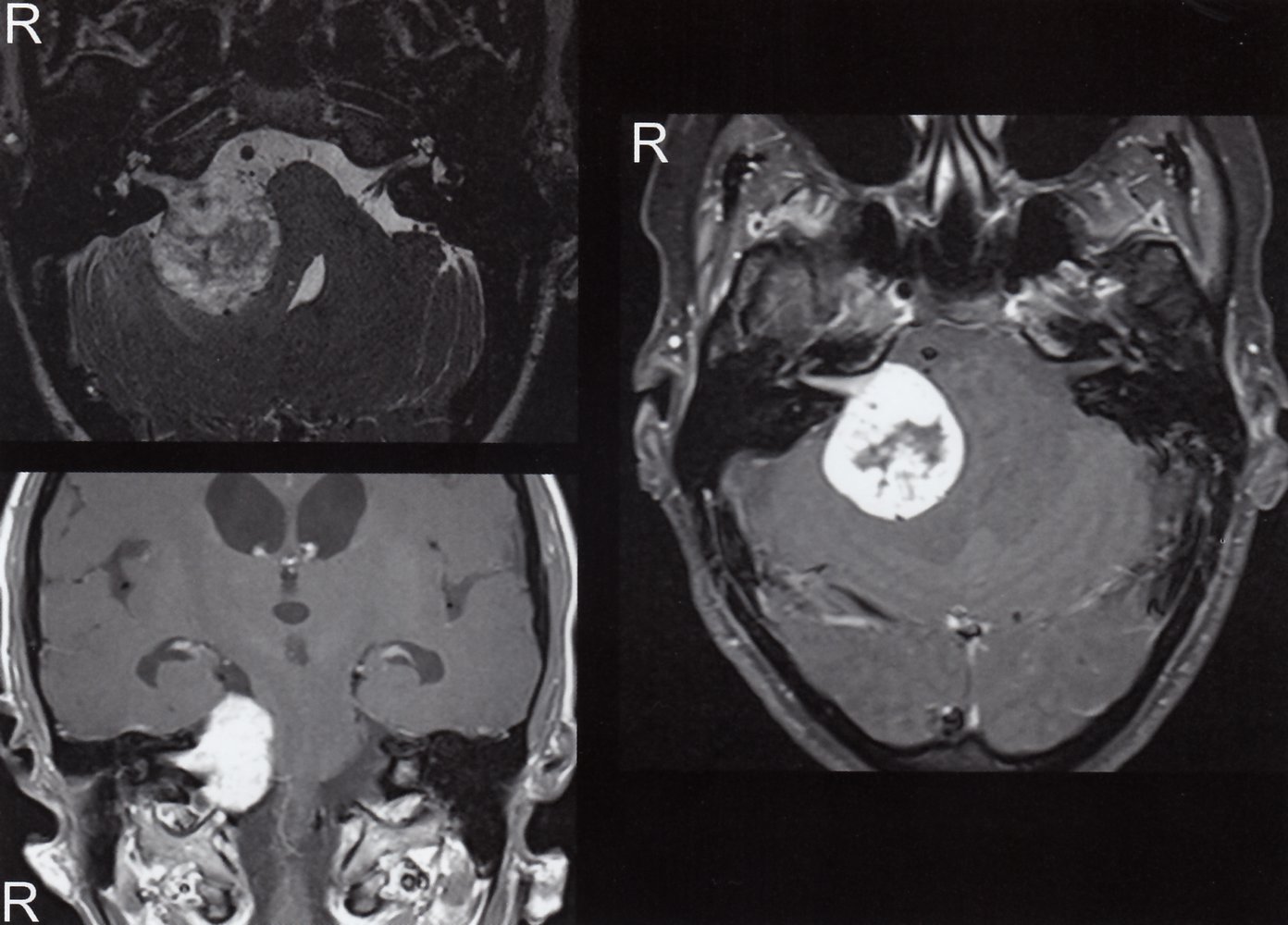
Cranial MRI
Upper left: T2-weighted image (axial view)
Lower left and right: T1-weighted images after application of contrast agent (axial and coronal views)
A tumor is visible on the right side between the brainstem and the cerebellum (green overlay), extending into the porus acousticus (arrow). There is strong contrast enhancement within the lesion and it has a hypointense center (red overlay), suggesting necrosis.
Source: © IMPP
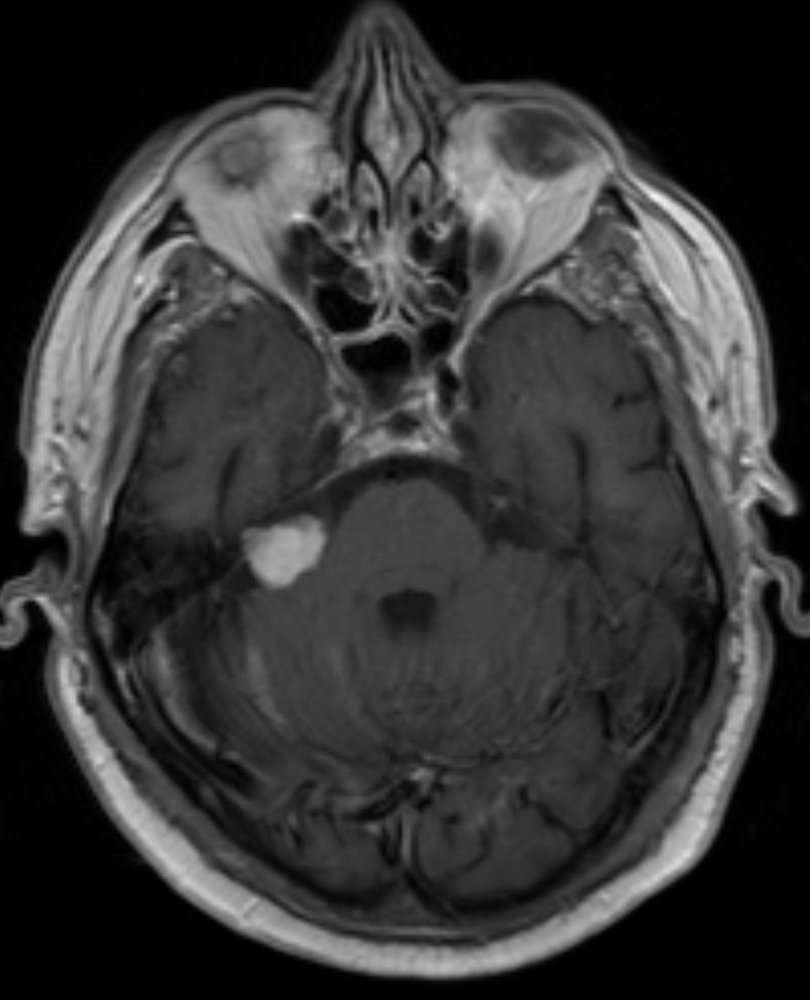
Cranial MRI (T1-weighted; with contrast; axial view)
An intensely contrast-enhancing, homogeneous mass (green overlay) is visible in the right cerebellopontine angle.
This is the typical appearance of an acoustic neuroma.
Source: “Akustikus-Schwannon_rechts_MRT_T1KM_axial_002” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
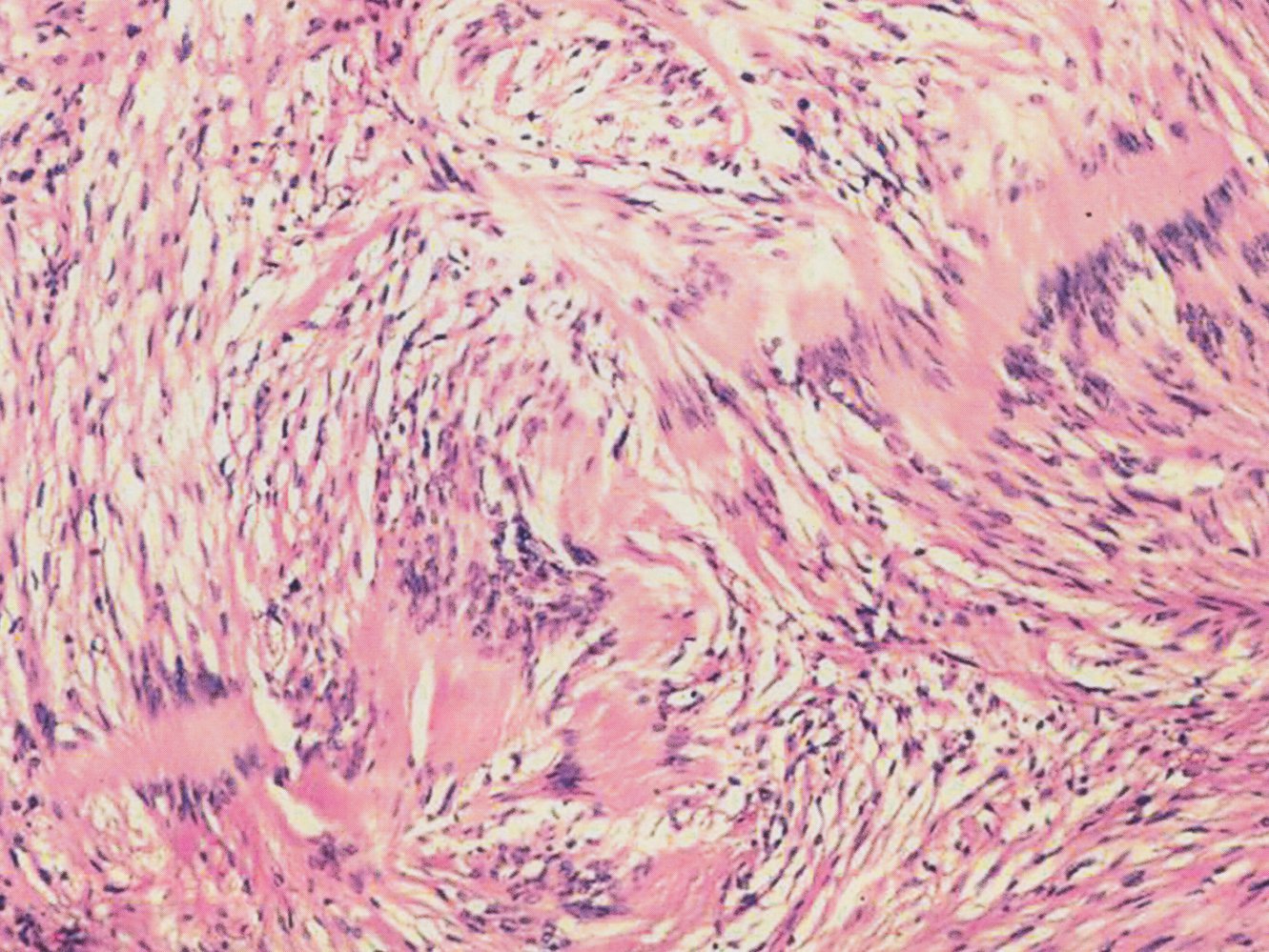
Photomicrograph of a tumor arising from the vestibular portion of cranial nerve VIII (H&E stain; medium magnification)
A characteristic finding of neuromas is the simultaneous occurrence of areas with densely packed nuclei (palisade pattern; A) and scattered or anuclear areas (B). There is also a large number of vacuolated cells (C).
Source: © IMPP
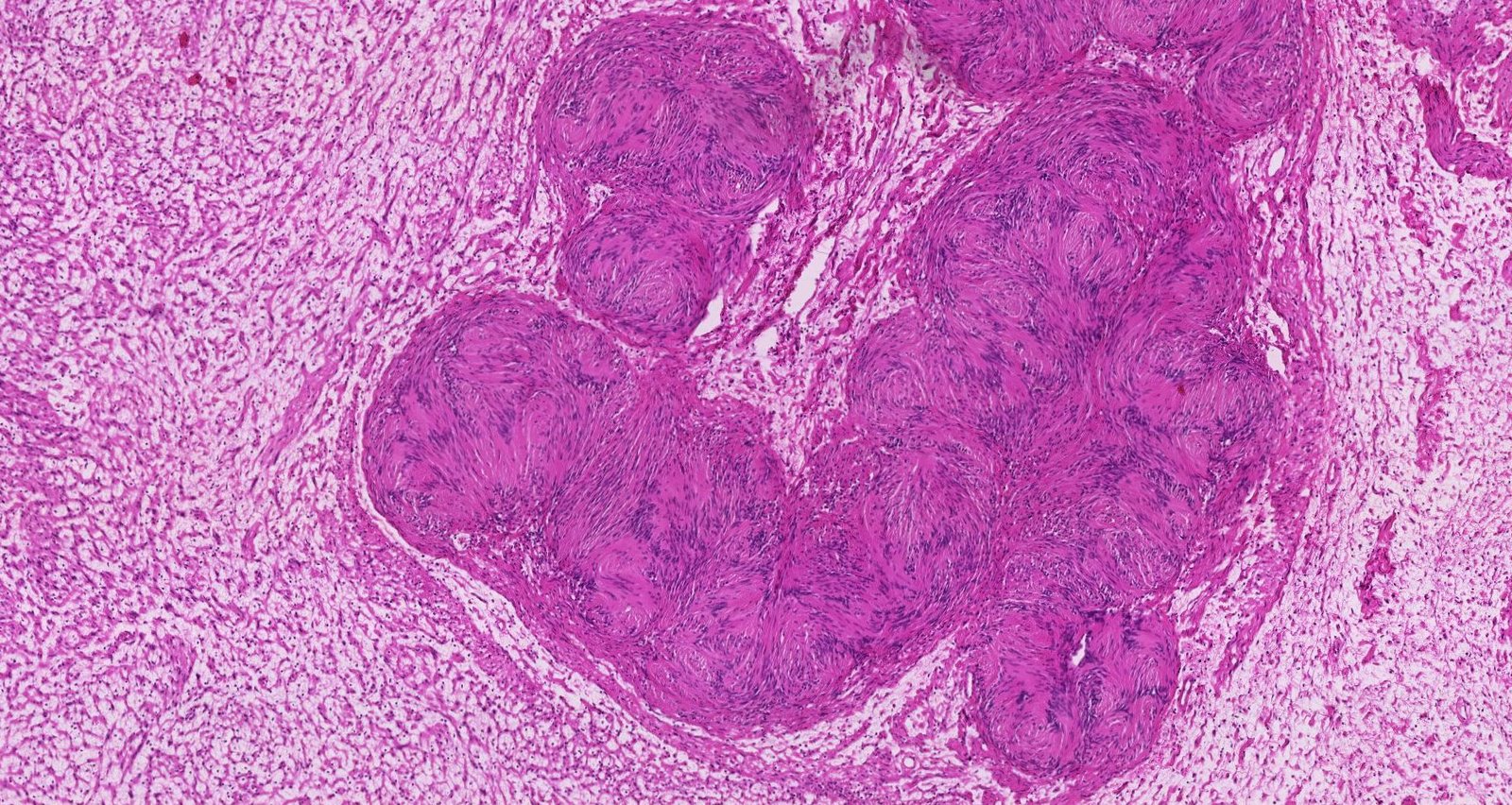
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
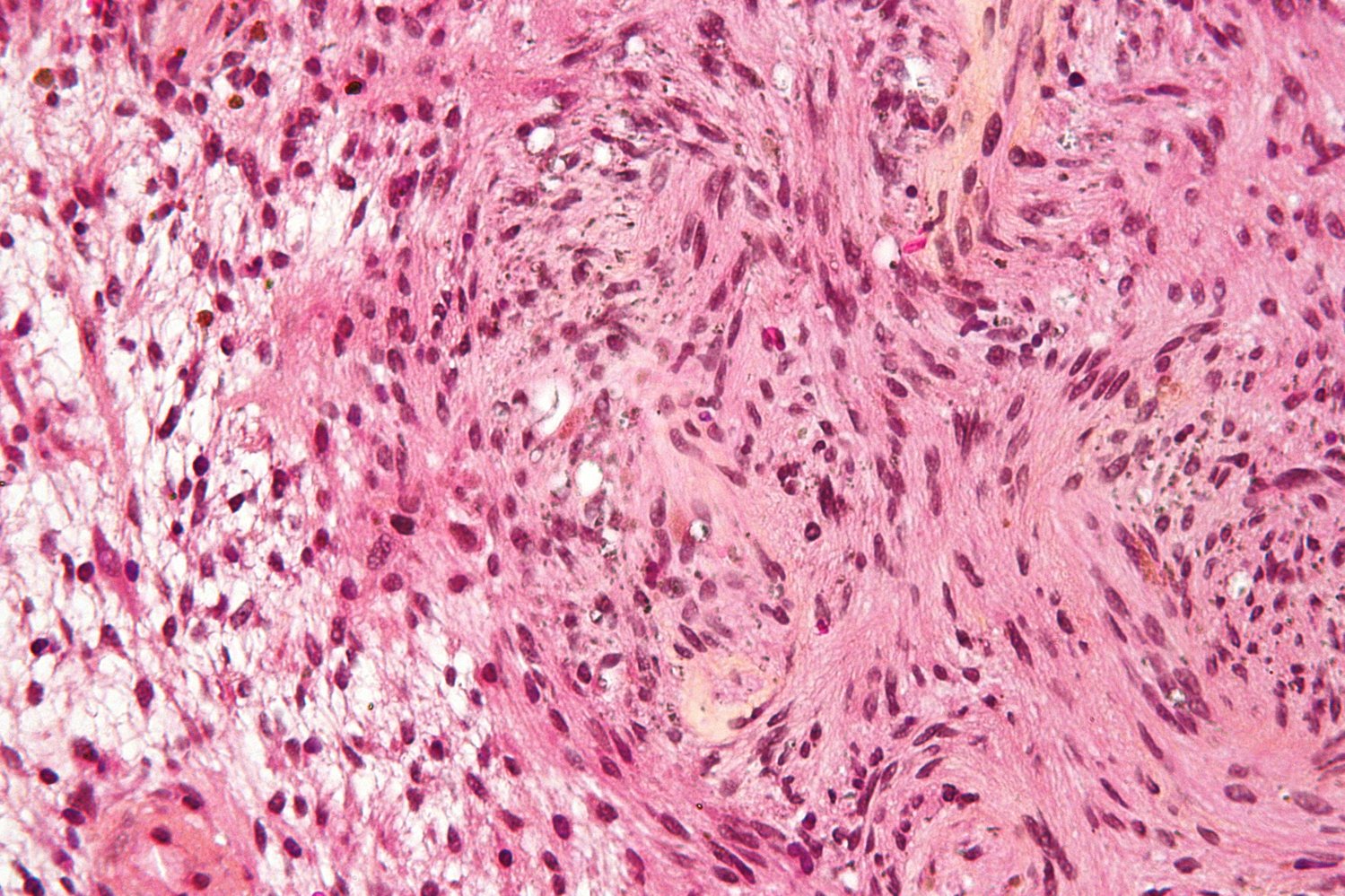
Photomicrograph of a biopsy from a peripheral nerve tumor (H&E stain)
Antoni A area (A): area of high cellularity with Verocay bodies. The Verocay bodies consist of rows of pallisading nuclei (green overlay) interspersed with anuclear eosinophilic areas (red overlay).
Antoni B area (B): paucicellular area with unstained myxoid stroma
This is the typical histological appearance of a schwannoma, a benign tumor of the nerve sheath.
Source: “Schwannoma - Antoni A and B - very high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Cranial CT scan (axial view)
A large hypodense lesion (green overlay) with multiple intralesional hyperdense calcifications (yellow overlay) is visible in the temporal lobe.
Source: “Oligodendroglioma 001” by RadsWiki, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Photomicrograph of brain tissue (H&E stain; very high magnification)
Monomorphic cells with enlarged, round/oval nuclei surrounded by a clear halo of unstained cytoplasm, which is an artifact of processing, are visible (green overlay). Thin blood vessels with an interlacing pattern are also visible (yellow overlay).
These are the typical features of oligodendroglioma.
Source: “Oligodendroglioma1 high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
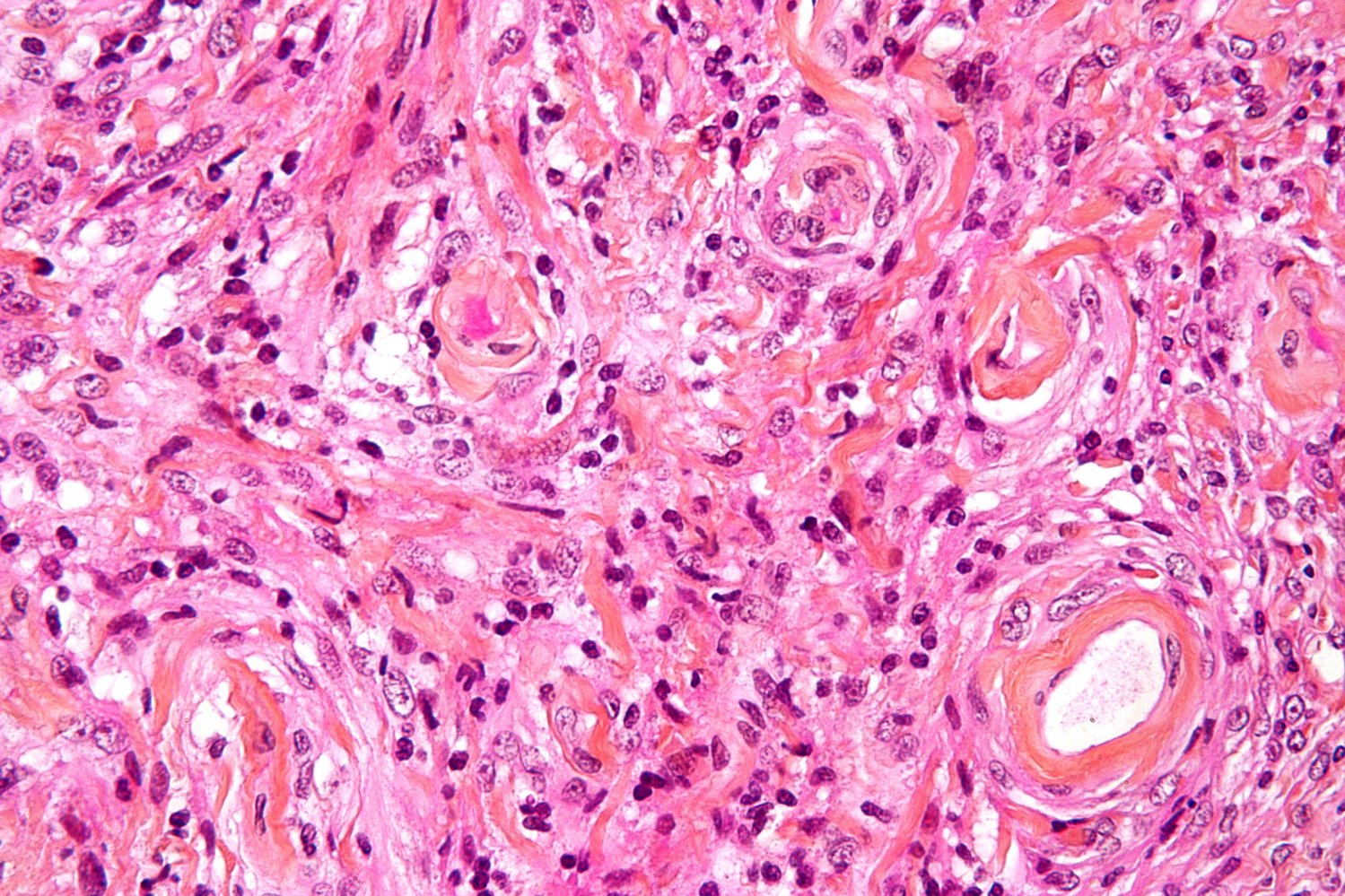
Photomicrograph of tissue biopsied from a brain tumor (HPS stain; 400x)
Several eosinophilic cells are visible, arranged in whorls (yellow overlay) and sheets. The nuclei of these cells show features of malignancy (i.e., large size or high N:C ratio, nuclear pleomorphism, prominent nucleoli, and mitotic figures). The intervening stroma contains numerous blood vessels (green overlay).
Hypercellularity, whorled or sheet-like architecture, and hypervascularity are typical features of a meningioma. Psammoma bodies (not seen here) are another characteristic feature of meningioma and would appear as basophilic whorls.
Source: “Meningioma high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Brain metastases
Definition
Brain metastases are secondary brain tumors due to metastasis of primary malignancies of other organs.
Epidemiology
- Most common cause of brain tumors in adults [11]
- Rare in children < 14 years of age [75]
Etiology [76]
- Lung cancer (most common) [76]
- Breast cancer
- Pancreatic cancer
- Malignant melanoma
- Renal cell carcinoma
- Colorectal carcinoma
- Testicular cancer [77]
Clinical features
- Onset: acute or subacute due to rapid tumor growth
- Seizures
- Focal neurological deficits
- Cognitive deficits
- Headaches
Diagnostics [2]
-
Gadolinium-enhanced MRI
- Well-circumscribed tumors at the junction of gray and white matter and/or watershed areas of the arterial system [78]
- Small metastases: homogeneous enhancement
- Large metastases: ring enhancement due to central necrosis
-
Further evaluation
- If the primary tumor is unknown: Obtain “Diagnostics of cancer of unknown primary.”
- If no primary tumor is identified: Obtain biopsy of the brain metastasis. [4]

Treatment [4][79]
Management of brain metastases is based on the primary tumor type, extent of metastases, and the patient's performance status.
-
Anticancer therapies: typically involves a combination of systemic and local therapy
- Systemic therapy: chemotherapy, cancer immunotherapy, and/or targeted agents
- Local therapy: radiosurgery, radiation therapy, and/or surgical resection
- Limited brain metastases: surgical resection or stereotactic radiosurgery (e.g., Gamma Knife, CyberKnife, proton beam)
- Extensive brain metastases: stereotactic radiosurgery and/or whole-brain radiotherapy (WBRT)
- Tumors causing mass effect: Consider surgical resection.
-
Supportive care
- Glucocorticoids; (e.g., dexamethasone) as needed to reduce tumor edema and ICP [80]
- Palliative care for patients with a high primary tumor burden and a poor functional status (based on Karnofsky performance status)
Prognosis [81]
- Varies widely based on primary tumor and patient factors
- The brain metastases prognostic index estimates survival in patients with brain metastases.
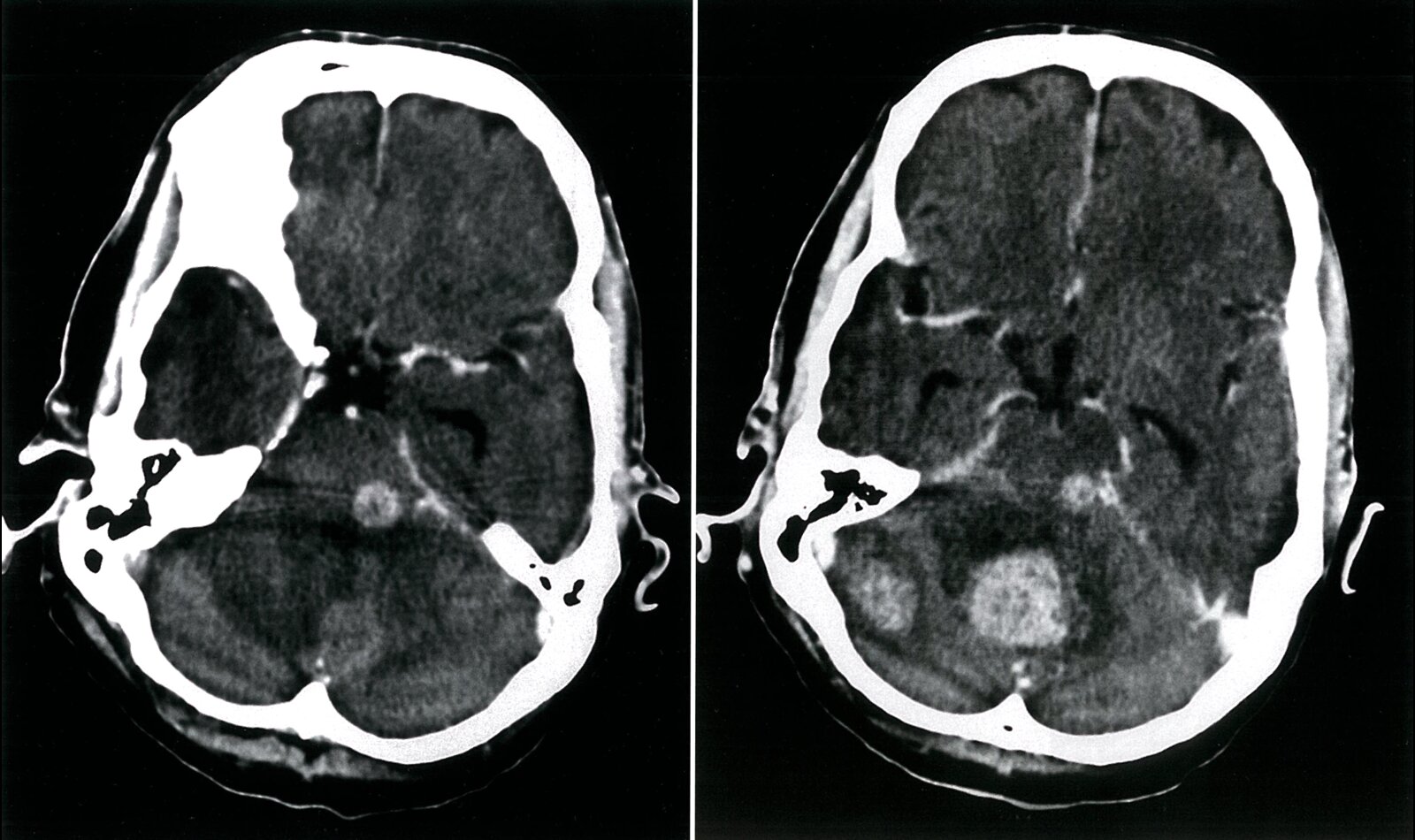
CT head (with contrast; axial plane) of a patient with a history of lung cancer presenting with weight loss, gradual reduction in consciousness, and deficits in swallowing, speech, coordination, and gait
Cerebellar (green overlay) and brainstem (red overlay) lesions that show intense contrast enhancement are suspicious for metastases.
P: petrous bone; S: sphenoid bone; T with arrows: tentorium cerebellum
Source: © IMPP
MRI head (T1-weighted; without contrast; axial plane) of a patient with lung carcinoma
A solitary, well-circumscribed, predominantly hypointense mass (hatched overlay) in the left occipital lobe is accompanied by perifocal edema (green overlay).
The lesion is consistent with a cerebral metastasis.
Source: © IMPP
MRI head (T2-weighted; without contrast; axial plane) of a patient with lung carcinoma
A solitary, well-circumscribed, predominantly hyperintense mass (hatched overlay) in the left occipital lobe is accompanied by perifocal edema (green overlay).
The lesion is consistent with a cerebral metastasis.
Source: © IMPP
Acute management checklist
- Consult neurosurgery and oncology.
- Start VTE prophylaxis. [82]
- Manage increased intracranial pressure (ICP), if present.
- Urgent neurosurgery and anesthesiology consult
- Assess and secure the airway.
- Consider therapeutic hyperventilation.
- Consider dexamethasone in patients with cerebral edema.
- Consider mannitol
- Admission to ICU and ICP monitoring
- Serial neurologic examination
- Admission to neurology or oncology service
External Resources
References
- Marinoff AE, Ma C, Guo D, et al. "Rethinking childhood ependymoma: a retrospective, multi-center analysis reveals poor long-term overall survival.". J Neurooncol. 135(1). :201-211. (2017)
- "Survival Rates for Selected Adult Brain and Spinal Cord Tumors". https://www.cancer.org/cancer/brain-spinal-cord-tumors-adults/detection-diagnosis-staging/survival-rates.html. [2020-05-05]
- Fix JD. "Neuroanatomy". Lippincott Williams & Wilkins. (2008). ISBN: 0781772451
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- Provenzale JM, Nelson RC. "Duke Radiology Case Review: Imaging, Differential Diagnosis, and Discussion". Lippincott Williams & Wilkins. (1998). ISBN: 0397516134
- Colafati GS, Voicu IP, Carducci C, et al. "MRI features as a helpful tool to predict the molecular subgroups of medulloblastoma: state of the art.". Therapeutic advances in neurological disorders. 11. :1756286418775375. (2018)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Northcott PA, Robinson GW, Kratz CP, et al. "Medulloblastoma". Nat Rev Dis Primers. 5(1). (2019)
- Packer RJ, Vezina G. "Management of and Prognosis With Medulloblastoma". Arch Neurol. 65(11). :1419. (2008)
- Editors: Donald W Kufe, MD, Raphael E Pollock, et al. "Holland-Frei Cancer Medicine". BC Decker. (2003). ISBN: 1550092138
- Packer RJ, Cogen P, Vezina G, Rorke LB. "Medulloblastoma: Clinical and biologic aspects". Neuro Oncol. 1(3). :232-250. (1999)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Siegel DA, Richardson LC, Henley SJ, et al. "Pediatric cancer mortality and survival in the United States, 2001‐2016". Cancer. 126(19). :4379-4389. (2020)
- Cohen AR. "Brain Tumors in Children". N Engl J Med. 386(20). :1922-1931. (2022)
- Pestana C. "Dr. Pestana's Surgery Notes: Top 180 Vignettes for the Surgical Wards". Kaplan. (2015). ISBN: 9781625231123
- Pfister S, Hartmann C, Korshunov A. "Histology and Molecular Pathology of Pediatric Brain Tumors". J Child Neurol. 24(11). :1375-1386. (2009)
- Evans JJ, Kenning TJ. "Craniopharyngiomas: Comprehensive Diagnosis, Treatment and Outcome". Academic Press. (2015). ISBN: 9780124167230
- "Childhood Ependymoma Treatment (PDQ®): Health Professional Version". https://www.ncbi.nlm.nih.gov/books/NBK65935/#CDR0000062843__1. [2016-08-12]
- Perkins A, Liu G. "Primary Brain Tumors in Adults: Diagnosis and Treatment.". Am Fam Physician. 93(3). :211-7. (2016)
- Stoyanov GS, Dzhenkov D, Ghenev P, et al. "Cell biology of glioblastoma multiforme: from basic science to diagnosis and treatment". Med Oncol. 35(3). (2018)
- Mawrin C, Chung C, Preusser M. "Biology and clinical management challenges in meningioma.". ASCO Educational Book. :e106-15. (2015)
- Rachinger J, Buslei R, Prell J, Strauss C. "Solid haemangioblastomas of the CNS: a review of 17 consecutive cases". Neurosurg Rev. 32(1). :37-48. (2008)
- Goldbrunner R, Weller M, Regis J, et al. "EANO guideline on the diagnosis and treatment of vestibular schwannoma.". Neuro Oncol. 22(1). :31-45. (2020)
- Wesseling P, van den Bent M, Perry A. "Oligodendroglioma: pathology, molecular mechanisms and markers.". Acta Neuropathol. 129(6). :809-27. (2015)
- Kronenberg H, Williams RH. "Williams Textbook of Endocrinology". Saunders Elsevier. (2008). ISBN: 1416029117
- Mosarla RC, et al. "Anticoagulation Strategies in Patients With Cancer". J Am Coll Cardiol. 73(11). :1336-1349. (2019)
- Buerki RA, Horbinski CM, Kruser T, et al. "An overview of meningiomas". Future Oncology. 14(21). :2161-2177. (2018)
- Baker KB, Moran CJ, Wippold FJ, et al. "MR Imaging of Spinal Hemangioblastoma". American Journal of Roentgenology. 174(2). :377-382. (2000)
- She D, Yang X, Xing Z, Cao D. "Differentiating Hemangioblastomas from Brain Metastases Using Diffusion-Weighted Imaging and Dynamic Susceptibility Contrast-Enhanced Perfusion-Weighted MR Imaging". American Journal of Neuroradiology. 37(10). :1844-1850. (2016)
- Li AY, Post AF, Dai JB, Choudhri TF. "Spontaneous Arrest of Sporadic Spinal Hemangioblastoma Growth after Postoperative Nodular Recurrence: Case Report". Cureus. (2018)
- Koeller KK, Rushing EJ. "Oligodendroglioma and Its Variants: Radiologic-Pathologic Correlation". RadioGraphics. 25(6). :1669-1688. (2005)
- Gupta M, Djalilvand A, Brat DJ. "Clarifying the diffuse gliomas: an update on the morphologic features and markers that discriminate oligodendroglioma from astrocytoma". Am J Clin Pathol. 124(5). :755-768. (2005)
- Mohile NA, Messersmith H, Gatson NT, et al. "Therapy for Diffuse Astrocytic and Oligodendroglial Tumors in Adults: ASCO-SNO Guideline". J Clin Oncol. 40(4). :403-426. (2022)
- Kronenberg H. "Williams Textbook of Endocrinology". Elsevier Health Sciences. (2007). ISBN: 9781437721812
- Dekkers OM, Biermasz NR, Smit JWA, et al. "Quality of life in treated adult craniopharyngioma patients". European Journal of Endocrinology. 154(3). :483-489. (2006)
- "Craniopharyngioma". https://rarediseases.org/rare-diseases/craniopharyngioma/
- Müller HL. "Craniopharyngioma". Endocr Rev. 35(3). :513-543. (2014)
- Campos S, Davey P, Hird A, et al. "Brain metastasis from an unknown primary, or primary brain tumour? A diagnostic dilemma.". Curr Oncol. 16(1). :62-6. (2009)
- Lamba N, Groves A, Torre M, Yeo KK, Iorgulescu JB. "The epidemiology of primary and metastatic brain tumors in infancy through childhood". J Neurooncol. 156(2). :419-429. (2022)
- Nayak L, Lee EQ, Wen PY. "Epidemiology of Brain Metastases". Curr Oncol Rep. 14(1). :48-54. (2011)
- Fink K, Fink J. "Imaging of brain metastases". Surg Neurol Int. 4(5). :209. (2013)
- Hwang T-L, Close TP, Grego JM, Brannon WL, Gonzales F. "Predilection of brain metastasis in gray and white matter junction and vascular border zones". Cancer. 77(8). :1551-1555. (1996)
- Vogelbaum MA, Brown PD, Messersmith H, et al. "Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline". J Clin Oncol. 40(5). :492-516. (2022)
- Gondi V, Bauman G, Bradfield L, et al. "Radiation Therapy for Brain Metastases: An ASTRO Clinical Practice Guideline". Pract Radiat Oncol. 12(4). :265-282. (2022)
- Ryken TC, McDermott M, Robinson PD, et al. "The role of steroids in the management of brain metastases: a systematic review and evidence-based clinical practice guideline". J Neurooncol. 96(1). :103-114. (2009)
- Sperduto PW, Mesko S, Li J, et al. "Survival in Patients With Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient". J Clin Oncol. 38(32). :3773-3784. (2020)
- Grommes C, DeAngelis LM. "Primary CNS Lymphoma". J Clin Oncol. 35(21). :2410-2418. (2017)
- Grommes C, Rubenstein JL, DeAngelis LM, Ferreri AJM, Batchelor TT. "Comprehensive approach to diagnosis and treatment of newly diagnosed primary CNS lymphoma". Neuro Oncol. 21(3). :296-305. (2018)
- Abrey LE, Batchelor TT, Ferreri AJM, et al. "Report of an International Workshop to Standardize Baseline Evaluation and Response Criteria for Primary CNS Lymphoma". J Clin Oncol. 23(22). :5034-5043. (2005)
- Butowski NA. "Epidemiology and Diagnosis of Brain Tumors". Continuum (Minneap Minn). 21. :301-313. (2015)
- Gaudino S, Martucci M, Russo R, et al. "MR imaging of brain pilocytic astrocytoma: beyond the stereotype of benign astrocytoma". Childs Nerv Syst. 33(1). :35-54. (2016)
- Grimm SA, Chamberlain MC. "Anaplastic astrocytoma". CNS Oncol. 5(3). :145-157. (2016)
- Nelson SJ, Cha S. "Imaging Glioblastoma Multiforme". Cancer J. 9(2). :134-145. (2003)
- Haldorsen IS, Espeland A, Larsson E-M. "Central Nervous System Lymphoma: Characteristic Findings on Traditional and Advanced Imaging". AJNR Am J Neuroradiol. 32(6). :984-992. (2010)
- Watts J, Box G, Galvin A, et al. "Magnetic resonance imaging of meningiomas: a pictorial review.". Insights Imaging. 5(1). :113-22. (2014)
- Suh JH, Kotecha R, Chao ST, et al. "Current approaches to the management of brain metastases". Nat Rev Clin Oncol. 17(5). :279-299. (2020)
- Pope WB. "Brain metastases: neuroimaging". Handb Clin Neurol. :89-112. (2018)
- Key NS, Khorana AA, Kuderer NM, et al. "Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update". J Clin Oncol. 38(5). :496-520. (2020)
- Diaz M, Jo J. "Venous Thrombotic Events and Anticoagulation in Brain Tumor Patients". Curr Oncol Rep. 24(4). :493-500. (2022)
- Schiff D, Lee EQ, Nayak L, et al. "Medical management of brain tumors and the sequelae of treatment". Neuro Oncol. 17(4). :488-504. (2014)
- Englot DJ, Chang EF, Vecht CJ. "Epilepsy and brain tumors". Handb Clin Neurol. :267-285. (2016)
- Chen DY, Chen CC, Crawford JR, Wang SG. "Tumor-related epilepsy: epidemiology, pathogenesis and management". J Neurooncol. 139(1). :13-21. (2018)
- Pruitt AA. "Medical Management of Patients With Brain Tumors". Curr Treat Options Neurol. 21. :314-331. (2015)
- Ryan R, Booth S, Price S. "Corticosteroid-use in primary and secondary brain tumour patients: a review". J Neurooncol. 106(3). :449-459. (2011)
- Smoll NR, Hamilton B. "Incidence and relative survival of anaplastic astrocytomas". Neuro Oncol. 16(10). :1400-1407. (2014)
- "Anaplastic Astrocytoma". https://radiopaedia.org/articles/anaplastic-astrocytoma. [2018-04-01]
- "Glioblastoma". https://radiopaedia.org/articles/glioblastoma. [2017-01-01]
- Nizamutdinov D, Stock EM, Dandashi JA, et al. "Prognostication of survival outcomes in patients diagnosed with glioblastoma". World Neurosurg. 109. :e67-e74. (2018)
- Westphal M, Maire CL, Lamszus K. "EGFR as a Target for Glioblastoma Treatment: An Unfulfilled Promise". CNS Drugs. 31(9). :723-735. (2017)
- "Low grade infiltrative astrocytoma". https://radiopaedia.org/articles/low-grade-infiltrative-astrocytoma. [2017-01-01]
- "Astrocytoma". http://www.mdguidelines.com/astrocytoma. [2017-01-01]
- Collins VP, Jones DTW, Giannini C. "Pilocytic astrocytoma: pathology, molecular mechanisms and markers". Acta Neuropathol. 129(6). :775-788. (2015)
- "Pilocytic Astrocytoma". https://radiopaedia.org/articles/pilocytic-astrocytoma. [2018-01-01]
- "Optic Nerve Glioma". http://eyewiki.aao.org/Optic_Nerve_Glioma. [2016-09-27]
- Thakkar JP, Dolecek TA, Horbinski C, et al. "Epidemiologic and Molecular Prognostic Review of Glioblastoma". Cancer Epidemiol Biomarkers Prev.. 23(10). :1985-1996. (2014)
- Davis M. "Glioblastoma: Overview of Disease and Treatment". Clin J Oncol Nurs. 20(5). :S2-S8. (2016)
- Ohgaki H, Kleihues P. "The Definition of Primary and Secondary Glioblastoma". Clinical Cancer Research. 19(4). :764-772. (2012)
- Benitez JA, Ma J, D’Antonio M, et al. "PTEN regulates glioblastoma oncogenesis through chromatin-associated complexes of DAXX and histone H3.3". Nature Communications. 8(1). (2017)
- Louis DN, Perry A, Reifenberger G, et al. "The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary". Acta Neuropathol. 131(6). :803-820. (2016)
- Rominiyi O, Vanderlinden A, Clenton SJ, et al. "Tumour treating fields therapy for glioblastoma: current advances and future directions". Br J Cancer. 124(4). :697-709. (2020)
- Hu J, Western S, Kesari S. "Brainstem glioma in adults". Front Oncol. 6. (2016)
- Choi PP, Shapera S. "Drop metastases". CMAJ. 175(5). :475. (2006)
- Michaud D, Schiff D, Batchelor T. "Incidence of primary brain tumors". UpToDate. UpToDate. https://www.uptodate.com/contents/incidence-of-primary-brain-tumors?source=search_result&search=brain%20tumors&selectedTitle=2~150. [2017-09-12]
- "Overview of Brain Tumors in Children". http://www.merckmanuals.com/professional/pediatrics/pediatric-cancers/overview-of-brain-tumors-in-children. [2015-08-01]
- "Astrocytomas". http://www.merckmanuals.com/professional/pediatrics/pediatric-cancers/astrocytomas. [2015-08-01]
- "Medulloblastoma". http://www.merckmanuals.com/professional/pediatrics/pediatric-cancers/medulloblastoma. [2015-08-01]
- Wong ET, Wu JK. "Clinical presentation and diagnosis of brain tumors". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-presentation-and-diagnosis-of-brain-tumors?source=search_result&search=brain%20tumor&selectedTitle=1~150#H4. [2016-02-16]
- Lay CL, Sun-Edelstein C. "Brain tumor headache". UpToDate. UpToDate. https://www.uptodate.com/contents/brain-tumor-headache?source=see_link#H4462344. [2015-11-30]
- "Brain Tumor - Systematic Approach". http://www.radiologyassistant.nl/en/p47f86aa182b3a/brain-tumor-systematic-approach.html#i47f86b18db49d. [2008-07-02]
- George AE, Russel EJ, Kricheff II. "White matter buckling: CT sign of extraaxial intracranial mass". AJR Am J Roentgenol. 135(5). :1031-1036. (1980)