Summary
Breast cancer is the second most common malignancy in women (after nonmelanoma skin cancer). In the US, the lifetime risk of a woman developing breast cancer is approximately 13%. The most important risk factors are increased exposure to estrogen, advanced age, and genetic predisposition (e.g., BRCA mutations). The majority of tumors are adenocarcinomas. The two most common types of breast cancer are invasive ductal carcinoma and the often less aggressive invasive lobular carcinoma. Breast cancer is usually asymptomatic and incidentally detected on routine screening. Symptoms of breast cancer are variable; these include a palpable breast mass, nipple inversion, blood-tinged nipple discharge, and features of regional or distant metastasis. Breast cancer is diagnosed based on biopsy results of lesions detected on clinical evaluation and/or breast imaging. Breast cancer treatment is multidisciplinary, involving surgery, radiation therapy, and systemic therapy (chemotherapy, endocrine therapy, targeted therapy), alone or in combination. The most important prognostic factors are cancer stage, tumor receptor status, and aneuploidy. Individuals at a high risk of developing breast cancer (e.g., positive BRCA mutation status) should be offered breast cancer risk-reducing interventions.
Lobular carcinoma in situ, previously classified as a premalignant lesion, is now considered a benign condition and is detailed in a separate article.
Epidemiology
Breast cancer is the second most common malignant disease in women. [1]
-
Incidence
- In 2020, an estimated 276,480 new cases of invasive breast cancer were diagnosed. [1]
- ♀ >> ♂ : The female-to-male incidence ratio in the US is 125.8 to 1. [2]
-
Peak incidence
- Postmenopausal
- Incidence increases with age. [3]
- 50% of breast cancers are diagnosed in women ≥ 65 years of age. [4]
- Mortality: second leading cause of cancer death in women in the US [1]
One in 8 women in the US (∼ 13%) will develop invasive breast cancer during their lifetime.
")
")
Epidemiological data refers to the US, unless otherwise specified.
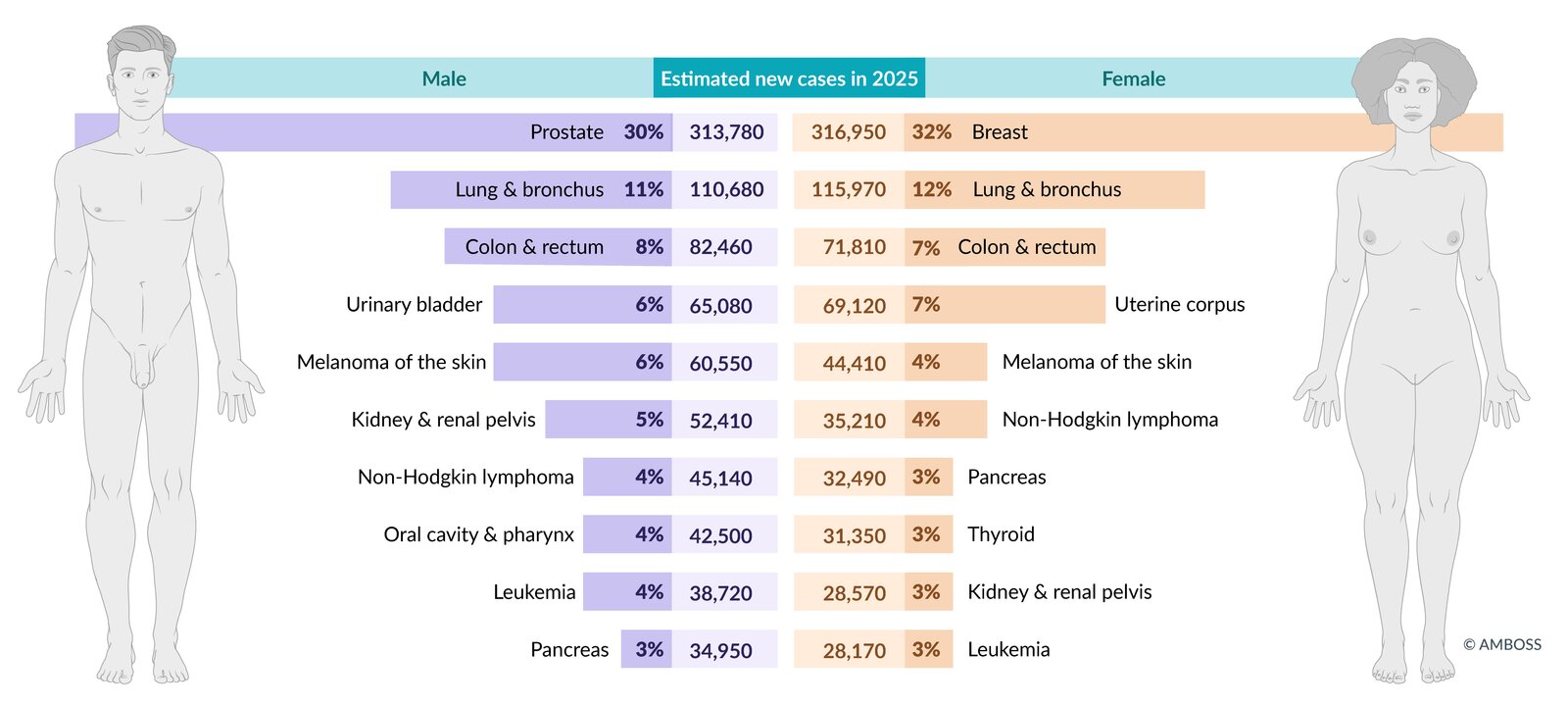
Estimated incidence of the most common cancers in the US in total figures and as a percentage of total cancer incidence (excluding non-melanoma skin cancers and in-situ carcinoma, except urinary bladder). Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
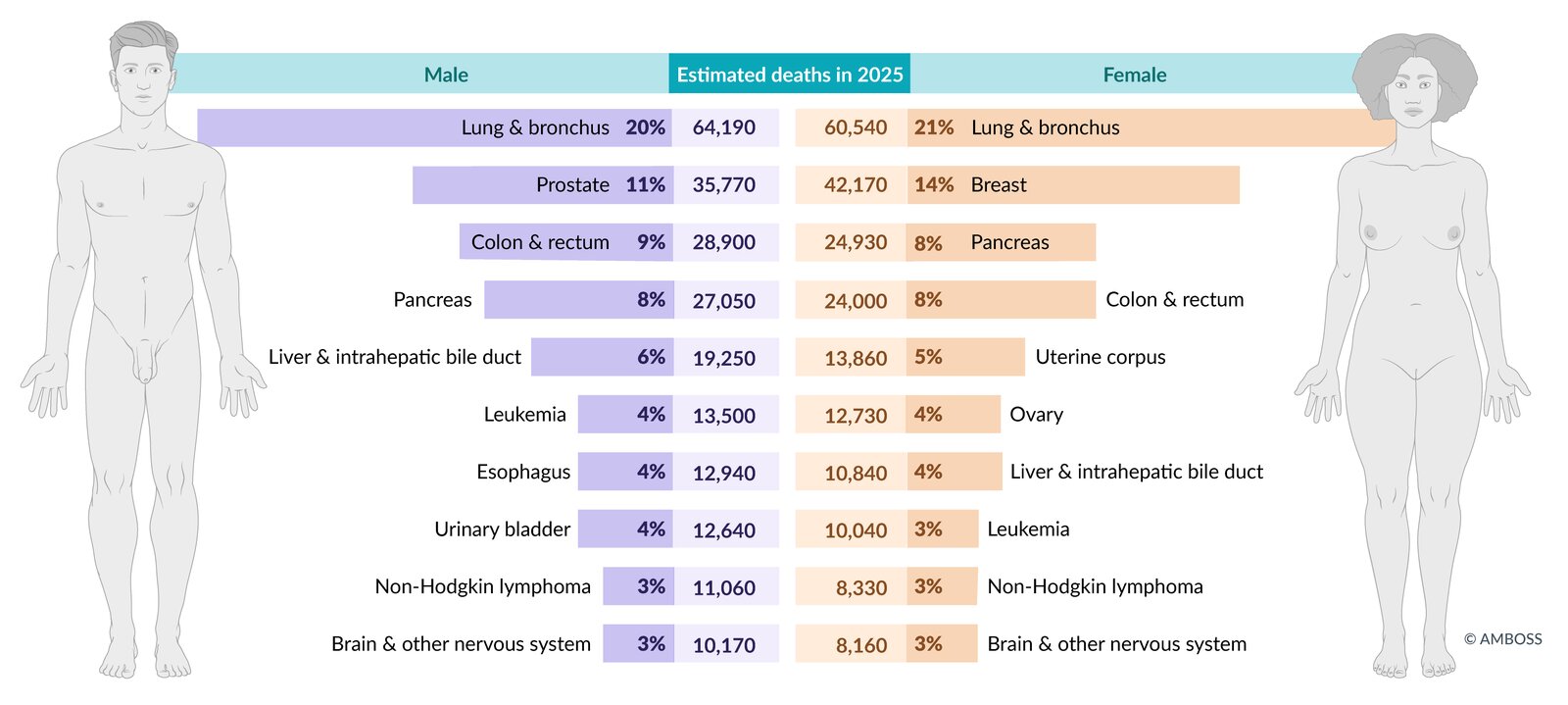
Estimated mortality from the most common cancers in the US in total figures and as a percentage of total cancer mortality. Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
Etiology
Predisposing factors
Hormonal risk factors
-
Increased exposure to endogenous estrogen
- First viable pregnancy after 35 years of age
- Nulliparity and/or absence of breastfeeding [5]
- Early menarche and/or late menopause
- Obesity; in postmenopausal women (lipocytes convert androstenedione to estrone)
-
Exogenous estrogen intake
- Hormone replacement therapy after menopause [6]
- Hormonal contraception [7]
The use of combined oral contraceptives or progesterone-only is associated with a slightly increased risk of breast cancer. However, hormonal contraceptive use is associated with a reduced risk of ovarian and endometrial cancer, which may decrease the overall risk of cancer. See “Noncontraceptive benefits of hormonal contraception.” [8][9]
Individual risk factors
- Sex: female
- Age: advanced age (most commonly in women ≥ 65 years) [4]
-
Ethnicity
- Individuals of European descent are at highest risk.
- African Americans are at increased risk for triple-negative breast cancer.
-
Lifestyle
- Low-fiber and high-fat diet
- Smoking
- Alcohol consumption
-
Positive medical history
- Breast cancer in the contralateral breast
- Breast conditions with cellular atypia (e.g., fibrocystic change, fibroadenoma)
- Endometrial cancer , ovarian, or colorectal cancer
- Radiation therapy during childhood [10]
Hereditary risk factors
- Positive family history (e.g., in first-degree relatives)
Mutations
-
Tumor suppressor genes
-
BRCA1 and BRCA2: BRCA are tumor suppressor genes that code for a DNA repair protein.
- Autosomal-dominant mutation
- Associated with an increased risk for breast cancer and ovarian cancer
- 5–10% of breast cancer cases are hereditary; BRCA mutations account for most of these. [11]
- BRCA-positive women develop breast cancer earlier than women without the mutation.
- An estimated 55–60% of women with BRCA1-positive status will develop invasive breast cancer before 70 years of age; the number is 45% in BRCA2-positive women. [12]
- Men with breast cancer are often positive for BRCA2.
- PTEN, RB1, CDH1
-
BRCA1 and BRCA2: BRCA are tumor suppressor genes that code for a DNA repair protein.
- Oncogenes: (e.g., RAS)
-
Mutations responsible for receptor overexpression
- Estrogen/progesterone receptors
- ERBB2 (HER2/neu)
Genetic conditions
-
Li-Fraumeni syndrome: autosomal dominant mutation of the p53 tumor suppressor gene
- Pathophysiology
- One abnormal copy of the TP53 gene is inherited.
- If the second allele is somatically mutated or deleted (loss of heterozygosity), it results in unregulated cell proliferation and cancer.
-
Clinical features: multiple malignancies at an early age
- Breast cancer
- Osteosarcoma
- Leukemia, lymphoma
- Brain tumors
- Adrenocortical carcinoma
- Pathophysiology
- Peutz-Jeghers syndrome
- Klinefelter syndrome
For the characteristics of Li-Fraumeni syndrome, think BLAST53: Breast cancer/Brain tumors, Leukemia/Lymphoma, Adrenocortical carcinoma, Sarcoma, and Tp53.
Types of breast cancer
Noninvasive carcinomas
Ductal carcinoma in situ (DCIS)
-
Characteristics
- No penetration of the basement membrane
- Preceded by ductal atypia
- Frequently appears as a pattern of grouped microcalcifications on mammography
- Higher risk of subsequent ipsilateral invasive carcinoma
Comedocarcinoma
- Characteristics: subtype of DCIS characterized by central necrosis
Noninvasive carcinomas are characterized by the absence of stromal invasion.
Invasive carcinomas
Invasive ductal carcinoma (IDC)
-
Characteristics
- Most common type of invasive breast cancer (∼ 80%) [13]
- Aggressive formation of metastases
-
Localization
- Unilateral
- Mostly unifocal
Medullary breast cancer [14]
-
Characteristics
- Rare subtype of invasive ductal carcinoma
- Most common tumor associated with the BRCA1 mutation
- Well-circumscribed soft tumor with smooth borders (may appear benign)
- Usually triple-negative
- Lymphadenopathy
- Differential diagnosis: fibroadenoma
Invasive lobular carcinoma (ILC) [13]
-
Characteristics
- ∼ 10% of all invasive breast carcinomas
- Less aggressive than ductal carcinoma
-
Localization
- Bilateral in ∼ 20% of cases
- Frequently multifocal
Less common subtypes [13]
- Mucinous carcinoma (< 5%; more common in older women)
- Mixed carcinoma (ductal/lobular)
- Tubular carcinoma
-
Papillary carcinoma of the breast
- A rare type of invasive ductal carcinoma with a peak incidence between the ages of 60 and 70
- More common among non-white women
- The tumor has a very low frequency of lymph node metastasis.
- Nearly 90% of the tumors express estrogen receptors.
- Micropapillary carcinoma
Clinical features
Breast cancer is frequently asymptomatic and often detected on routine screening. Symptoms typically manifest at more advanced stages of the disease.
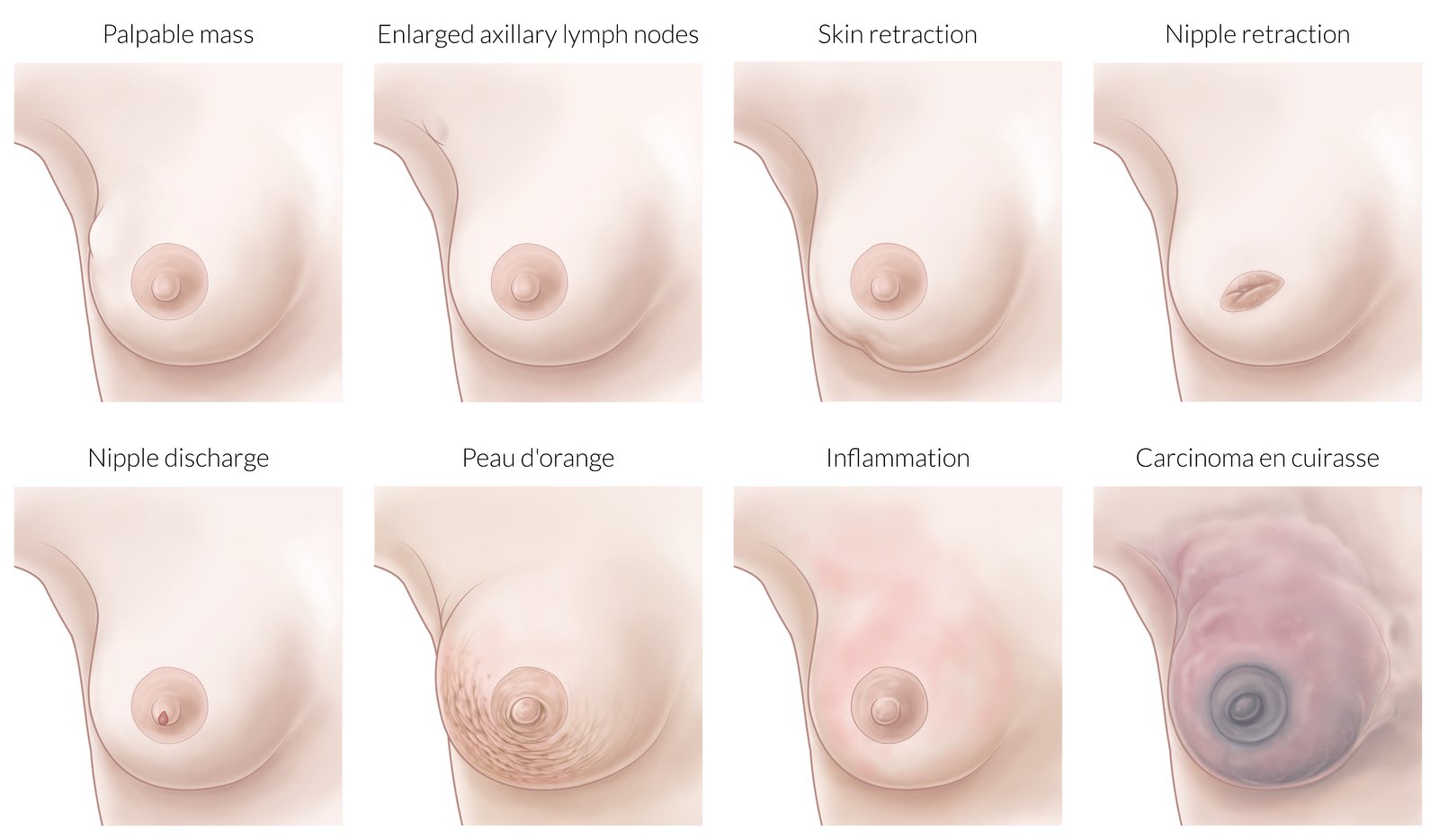
Breast changes
-
Palpable breast mass with the following characteristics:
- Typically single, nontender, and firm
- Poorly defined margins
- Most commonly located in the upper outer quadrant (∼ 55%)
- Breast asymmetry
-
Skin changes
- Retractions or dimpling (due to fixation to the pectoral muscles, deep fascia, Cooper ligaments, and/or overlying skin)
- Peau d'orange
- Nipple inversion
- Blood-tinged nipple discharge


To make skin retractions more visible, it can be helpful to stretch the skin or gently elevate the patient's arm.
Regional lymphadenopathy
- Nontender, firm, enlarged lymph nodes (> 1 cm in size), that may be fixed or matted
- The axillary nodes are most commonly involved.
- The supraclavicular, infraclavicular, and parasternal lymph nodes may also be involved.


Features of distant metastasis
Distant metastases of breast cancer can produce a number of heterogeneous symptoms.
-
Bone metastasis
- Bone pain
- Pathologic fractures
- Spinal compression
-
Liver metastasis
- Abdominal pain, distention
- Nausea
- Jaundice
-
Lung metastasis
- Cough
- Hemoptysis
- Dyspnea
- Chest pain
-
Brain metastasis
- Headaches
- Seizures
- Cognitive deficits, focal neurological deficits
More than 90% of breast cancers are diagnosed in early (nonmetastatic) stages. [15]

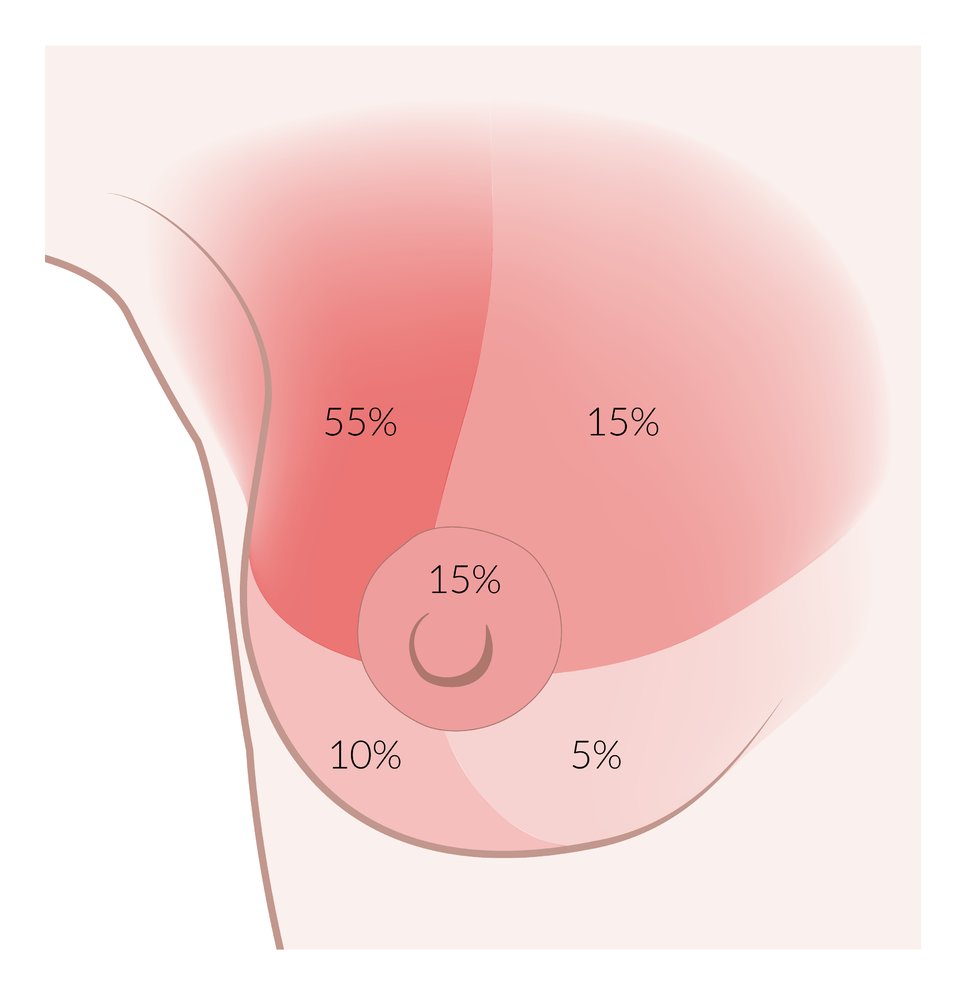
∼ 55%: upper outer quadrant
∼ 10–15%: upper inner quadrant
∼ 10–15%: nipple
∼ 10–15%: lower outer quadrant
∼ 5%: lower inner quadrant
© AMBOSS
© AMBOSS
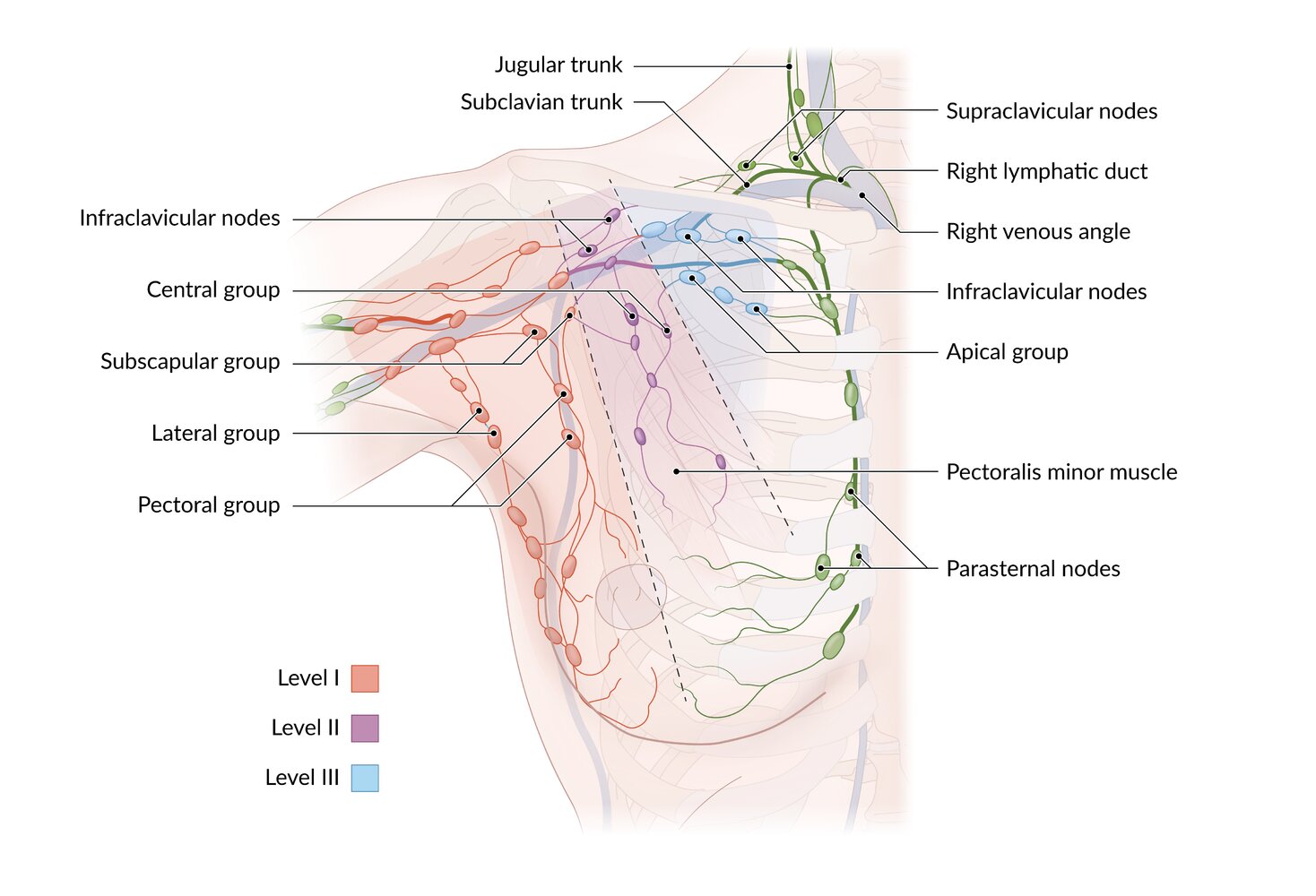
Lymphatics of the breast drain into three groups:
1. Axillary group, further divided into three levels
– Level I: lateral to the lateral border of the pectoralis minor
– Level II: behind the pectoralis minor
– Level III: medial to the medial border of the pectoralis minor
2. Parasternal (internal thoracic) group
3. Posterior intercostal group (not shown here)
Efferent lymphatics travel to the supraclavicular nodes and terminate in the thoracic duct (on the left; not shown here) or the right lymphatic duct.
© AMBOSS
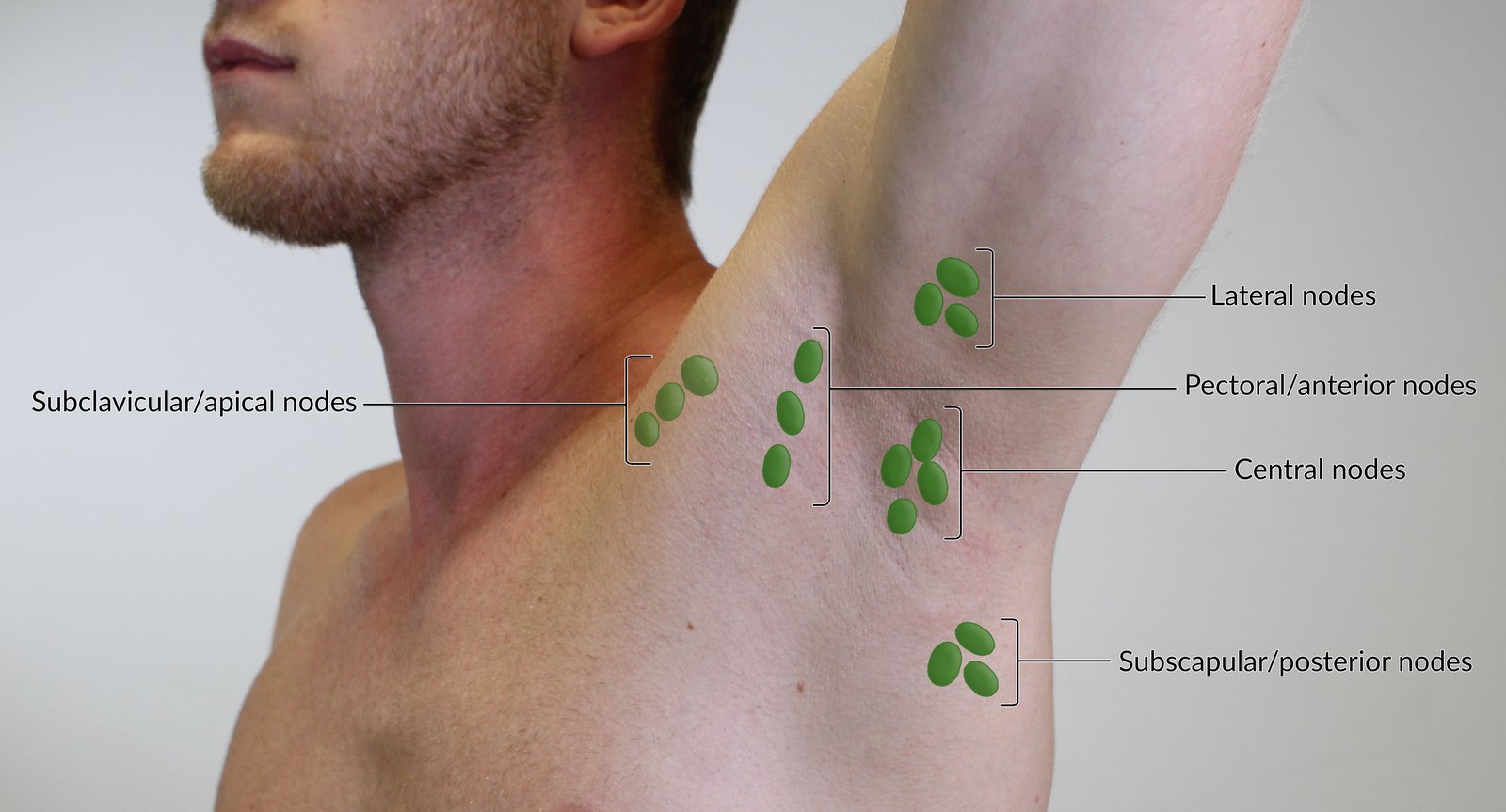
The lateral nodes drain most of the arm and shoulder and are palpable near the proximal humerus. The pectoral or anterior nodes drain the thoracic wall and parts of the thorax and are palpable in the anterior axillary line. The subscapular or posterior nodes drain the posterior thoracic wall and parts of the arm and are palpable in the posterior axillary line.
All these lymph nodes drain into the central nodes, which are palpable at the base of the axilla. Before entering the venous system, lymph from the central nodes passes through the subclavicular or apical nodes before entering the venous system. Therefore, these nodes should also be palpated in the examination.
For educational purposes, the lymph nodes are depicted enlarged.
© AMBOSS
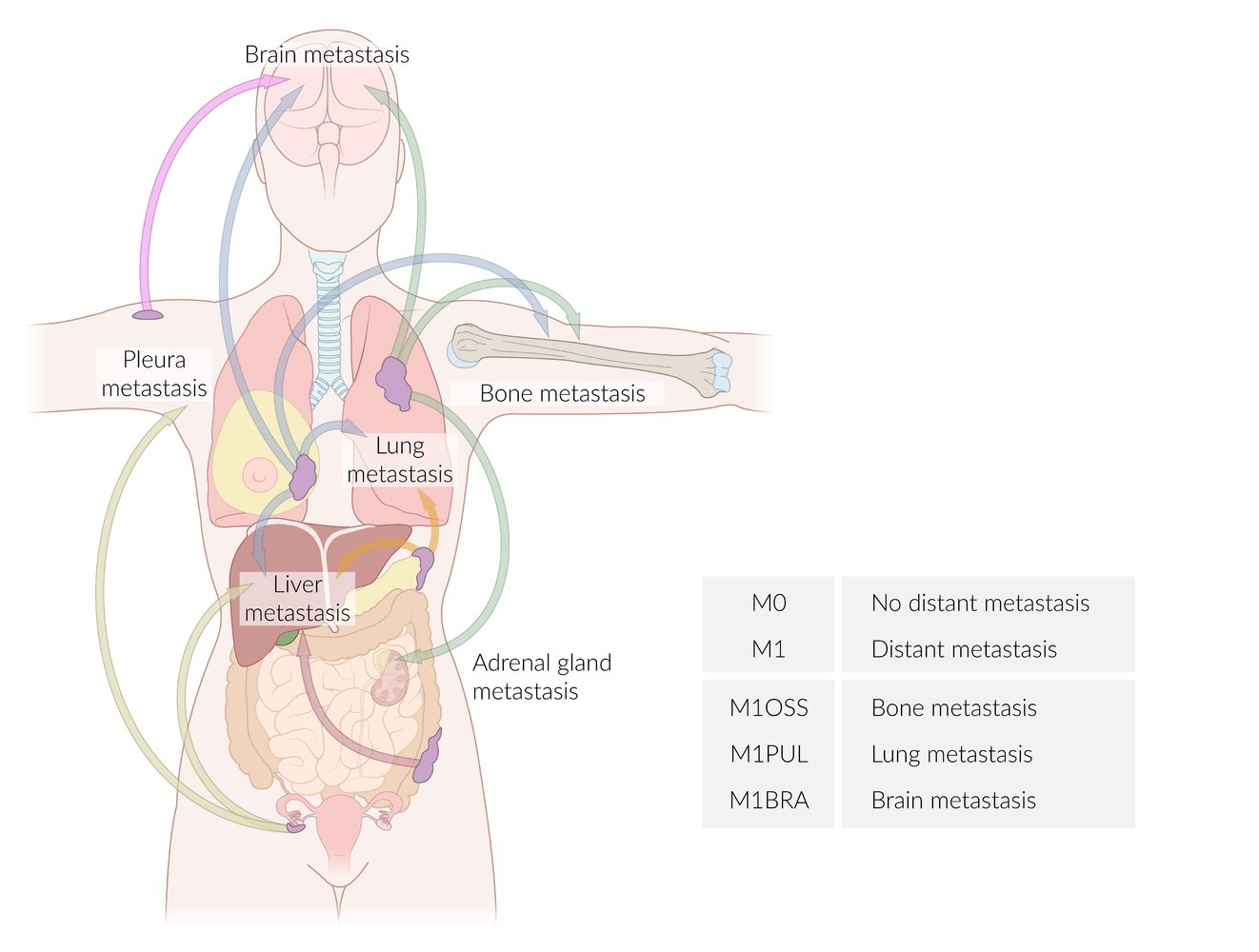
Arrows have been color-coded according to the site of the primary tumor:
Pink: skin cancer
Blue: breast cancer
Green: lung cancer
Orange: pancreatic cancer
Red: colon cancer
Lime: ovarian cancer
The table provides examples of suffixes used to specify the affected organs according to the TNM classification.
© AMBOSS
Subtypes and variants
Paget disease of the breast [16]
- Definition: a rare type of breast cancer; that affects the lactiferous ducts and the skin of the nipple and areola
-
Pathogenesis
- Not fully understood
- The following hypotheses have been postulated: [17]
- Migratory/epidermotropic theory: neoplastic ductal epithelial cells from an underlying DCIS or IDC; move through the lactiferous ducts and invade the surrounding epidermis of the nipple.
- In situ malignant transformation of existing cells into Paget cells, meaning that the condition is a carcinoma in situ, without preexisting DCIS/IDC.
-
Clinical features
- Erythematous, scaly, or vesicular rash affecting the nipple and areola
- Pruritus; burning sensation
- Nipple retraction
- Ulceration that causes blood-tinged nipple discharge
-
Diagnostics
- Punch/wedge or surface biopsy of nipple tissue: Paget cells confirm disease.
- Imaging to look for underlying DCIS/IDC (see “Diagnostics” below)
- Differential diagnosis: mamillary eczema
-
Treatment
- Breast-conserving surgery with subsequent adjuvant whole-breast radiation (see “Treatment” below)
- Mastectomy

Inflammatory breast cancer (IBC) [18]
- Definition: a rare form of advanced, aggressive invasive carcinoma characterized by dermal lymphatic invasion of tumor cells
-
Clinical features
-
Peau d'orange
- Erythematous, warm, and edematous skin plaques with prominent hair follicles that resemble orange peel
- Caused by obstruction of the lymphatic channels due to tumor growth
- Tenderness, burning sensation
- Blood-tinged nipple discharge
- Signs of metastatic disease (e.g., axillary lymphadenopathy) [19]
- Can present with or without a palpable mass
-
Peau d'orange
-
Diagnostics: The diagnostic process involves a comprehensive clinical examination, followed by imaging studies (mammography and ultrasound) and a biopsy to confirm the diagnosis. [20]
-
Diagnostic criteria: (all must be met)
- Rapid onset of breast erythema, edema, warmth, and peau d'orange, with or without palpable mass on breast examination
- Erythema involving at least one-third of the breast
- Symptoms have been present for < 6 months
- Core needle biopsy confirming the presence of invasive carcinoma
-
Imaging
- Bilateral mammogram and ultrasound of the breast and regional lymph nodes: skin thickening, tumor mass, increased breast density
- Optional MRI
-
Biopsy
- Core needle biopsy: recommended in all patients for diagnostic confirmation
- Full-thickness skin biopsy: recommended in all patients to assess for dermal involvement
- Further testing
- Hormone receptor status evaluation
- Optional PET/CT
-
Diagnostic criteria: (all must be met)
-
Differential diagnosis
- Mastitis
- Paget disease of the breast
- Breast abscess
- Erysipelas of the breast
- Treatment: modified radical mastectomy with neoadjuvant and adjuvant systemic therapy and adjuvant radiation therapy
- Prognosis: 5-year survival rate is ∼ 40%.



Inflammatory breast cancer is always classified as T4 because it involves the skin.
ALND (not SLNB) should be performed in patients with inflammatory breast cancer. [21][22]
Occult breast cancer [23]
- Definition: a rare type of cancer ; characterized by clinically recognizable metastases originating from an undetectable primary breast tissue carcinoma
- Clinical features: axillary adenopathy (most common)
-
Diagnostics
- Biopsy of the lymph node
- Breast ultrasound
- Mammography
- Breast MRI (only if ultrasound and mammography are inconclusive)
-
Treatment [24]
- ALND
- Mastectomy
- Chemotherapy and radiation
- For further information, see “Treatment” below.

An erythematous, scaling rash with irregular borders and erosion of the nipple is visible on the left breast of a female patient. The pathology extends beyond the areola region.
These findings are typical of Paget's disease of the breast, a rare type of ductal carcinoma that is often accompanied by nipple discharge. Age-appropriate imaging and biopsy are required for diagnosis.
Source: “Figure 1a, in: Paget’s disease of the breast: clinical, imaging and pathologic findings: a review of 16 patients” by M. Muttarak, B. Siriya, P. Kongmebhol et al., Biomedical Imaging and Intervention Journal, licensed under CC BY-SA 3.0. Further notes: Original publication available at: https://web.archive.org/web/20120905132437/http://www.biij.org/2011/2/e16/e16.pdf

The right breast is swollen and shows diffuse erythema that extends over most of its surface. Conspicuous hair follicles produce the typical orange peel appearance (peau d'orange). The nipple is also markedly retracted.
Edematous swelling, orange peel appearance, and nipple retraction are all caused by blockage of lymphatic channels. The swelling and erythema distinguish inflammatory breast cancer from locally advanced breast cancer.
Source: “Figure 1. in: What is inflammatory breast cancer? Revisiting the case definition.” by Paul H. Levine, Ladan Zolfaghari, Heather Young, Muhannad Hafi, Timothy Cannon, Chitra Ganesan, Carmela Veneroso, Rachel Brem and Mark Sherman, MDPI, licensed under CC BY 3.0.

An edematous lump with marked erythema is visible on the left breast of this 60-year-old male patient. The central area, as well as the upper and lower outer quadrants of the breast, are primarily affected. Some scarring can be seen in the lower outer quadrant.
These features are concerning for inflammatory breast cancer. The diagnosis should be confirmed on biopsy and histopathological examination.
Source: © IMPP
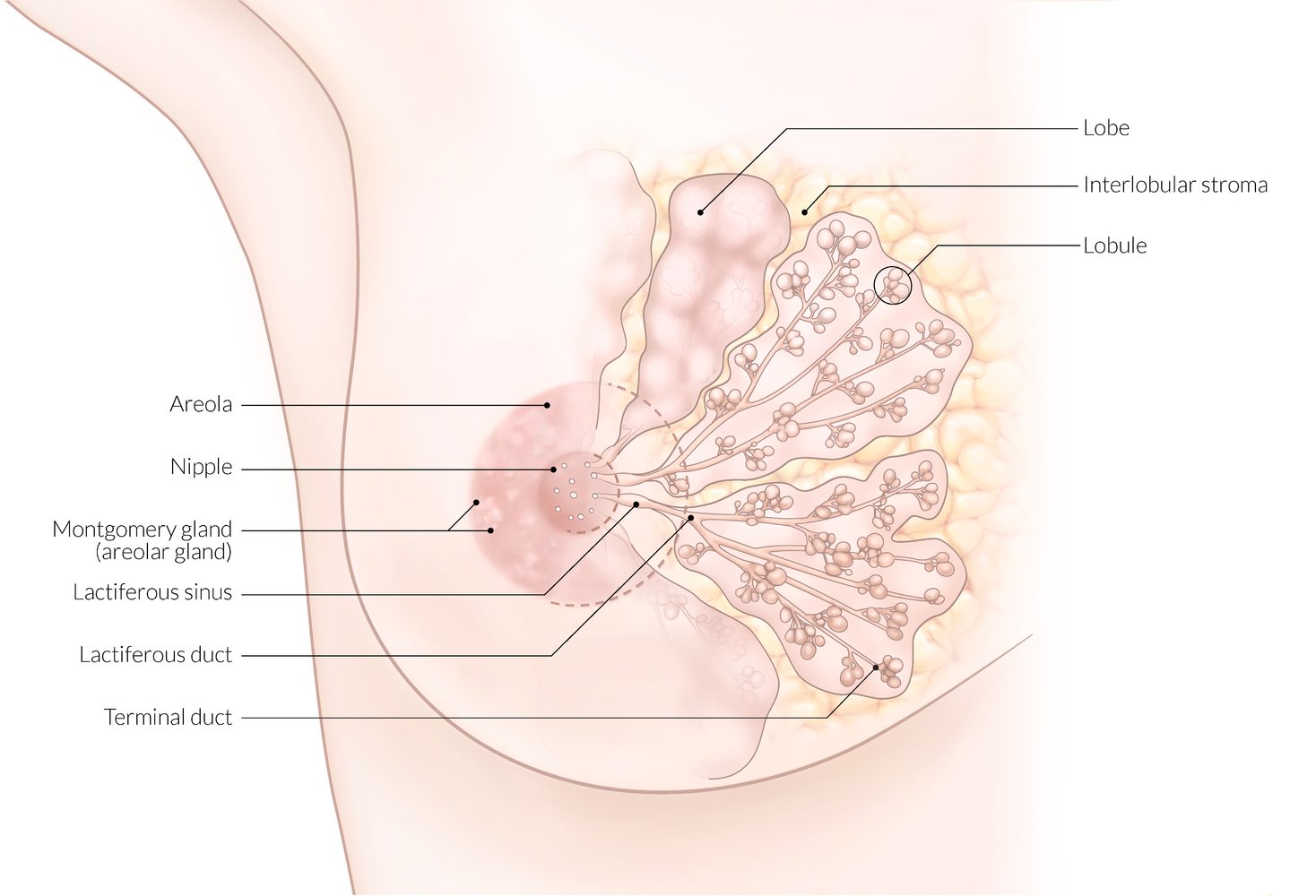
The breast parenchyma is made up of 10–20 lobes with interlobar stroma in between.
Each lobe is made up of multiple lobules, which are drained by a single lactiferous duct that opens onto the surface of the nipple.
The lactiferous sinus is the terminal dilation of the lactiferous duct.
© AMBOSS
Diagnosis
Breast cancer is diagnosed based on biopsy results of lesions detected on clinical evaluation and/or breast imaging. The diagnostic approach depends on clinical presentation but typically includes all of the following, in sequence (see “Palpable breast mass,” “Nipple discharge,” “Mastalgia,” and “Breast cancer screening” for specific algorithms). [25]
Clinical evaluation
-
Comprehensive patient history, including:
- Relevant family history
- Assessment of risk factors for breast cancer
- Review of systems
- Bilateral examination of the breasts and regional lymph nodes (axillary, supraclavicular)
Breast imaging
The choice of initial imaging modality is based on patient age, symptoms, and risk factors for breast cancer.
- Indications
- Clinical findings concerning for breast cancer
- Breast cancer screening
- Options
- Mammography
- Breast MRI
- Breast ultrasound
- Findings
- See “Benign vs. malignant lesion on breast ultrasound.”
- See “Benign vs. malignant lesion on mammography.”
Breast imaging results are typically reported using the standardized American College of Radiology Breast Imaging Reporting and Data System (BI-RADS).
Confirmatory biopsy
- Indications: all lesions with clinical and/or imaging features concerning for malignancy
- Options (see “Breast biopsy” for details)
- Image-guided core needle biopsy (preferred)
- Excisional biopsy
- Punch biopsy
- Fine needle aspiration biopsy
- Findings: See “Pathology” for histopathologic types of breast cancer.
Staging and receptor testing
General principles [15][26]
Refer all patients with newly diagnosed invasive breast cancer and DCIS to specialists for staging. Staging is used to guide management and estimate prognosis and is summarized as follows:
-
All patients
- Preoperative TNM staging (clinical staging)
- Receptor testing and tumor grading (on breast cancer biopsy samples) [27]
- Selected patients: multigene panel testing
- Postoperative patients: histopathology assessment of tumor extent (i.e., T and N stages) on tissue excised during surgery (pathologic staging)
Serum tumor marker testing (e.g., CEA, CA 15-3, and CA 27-29) is not recommended for disease monitoring. [28][29]
The workup of newly diagnosed breast cancer should ideally involve a multidisciplinary cancer care team. [30][31]
Receptor testing [30][31]
All invasive breast cancer biopsy samples should be tested for expression of the following receptors to guide optimal treatment. DCIS biopsy samples should also be tested for hormone receptors. [32]
-
Hormone receptors, i.e.: [32]
- Estrogen receptors (ER)
- Progesterone receptors (PR)
-
Human epidermal growth factor receptor 2 (ERBB2; formerly HER2/neu): [33]
- An epidermal growth factor receptor with intracellular tyrosine kinase activity
- Promotes cell growth and differentiation and inhibits apoptosis
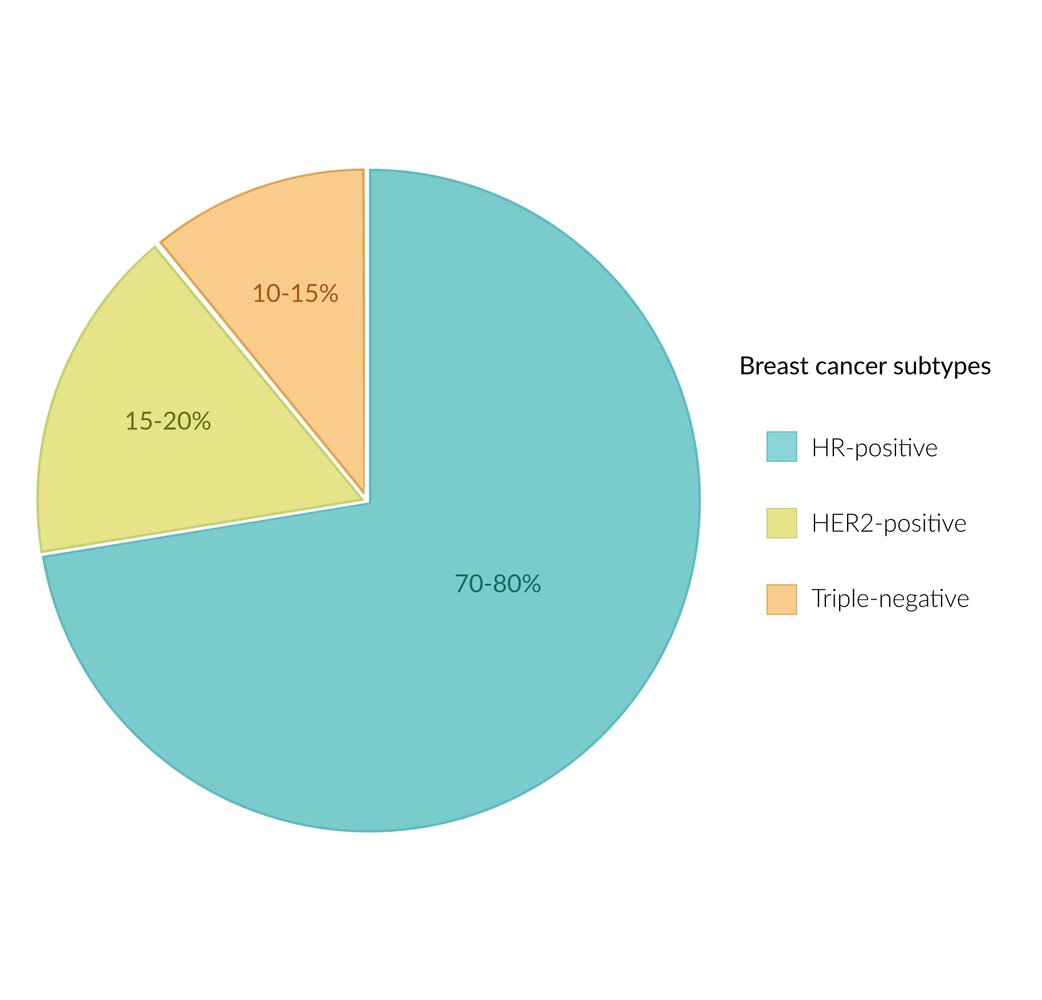
| Classification of breast cancer by receptor status [15] | ||||
|---|---|---|---|---|
| Description | Percentage of breast cancers | Considerations for systemic therapy | Additional considerations | |
| Hormone receptor-positive breast cancer (HR+) |
|
|
|
|
| ERBB2-positive breast cancer (ERBB2+) |
|
|
|
|
| Triple-negative breast cancer |
|
|
|
|

Clinical staging [37]
Evaluation of locoregional extent
- Indication: all patients (if not already performed during initial evaluation)
-
Modalities
- Bilateral breast imaging: bilateral diagnostic mammography, usually combined with breast ultrasound [37][38]
-
Axillary lymph node status ; [22]
- Palpable lymph nodes: Image-guided FNA or CNB is indicated to confirm nodal metastasis.
-
Nonpalpable lymph nodes
- SLNB is usually indicated. [22]
- Consider axillary ultrasound (not routinely recommended).
- See “Axillary staging in breast cancer” for details.
Evaluation for distant metastasis [37][39][40]
-
Indications
- Clinical features suggestive of metastasis
- Consider in asymptomatic individuals with late-stage (stage II B, stage III) disease at presentation.
- Laboratory studies: e.g., CBC, CMP, liver chemistries, ALP
-
Imaging [41]
- Suspected bone metastasis : bone scan, sodium fluoride PET/CT, or FDG-PET/CT [42]
- Suspected lung metastasis : CT chest
- Suspected liver metastasis : CT or MRI abdomen and pelvis [43]
- Suspected brain metastasis : MRI brain
- Consider FDG-PET/CT from the base of the skull to mid-thigh as an adjunctive modality to any of the above as needed.
Patients with early-stage disease and no clinical features suggestive of metastasis do not require imaging to assess for distant metastasis. [37][44]



© AMBOSS
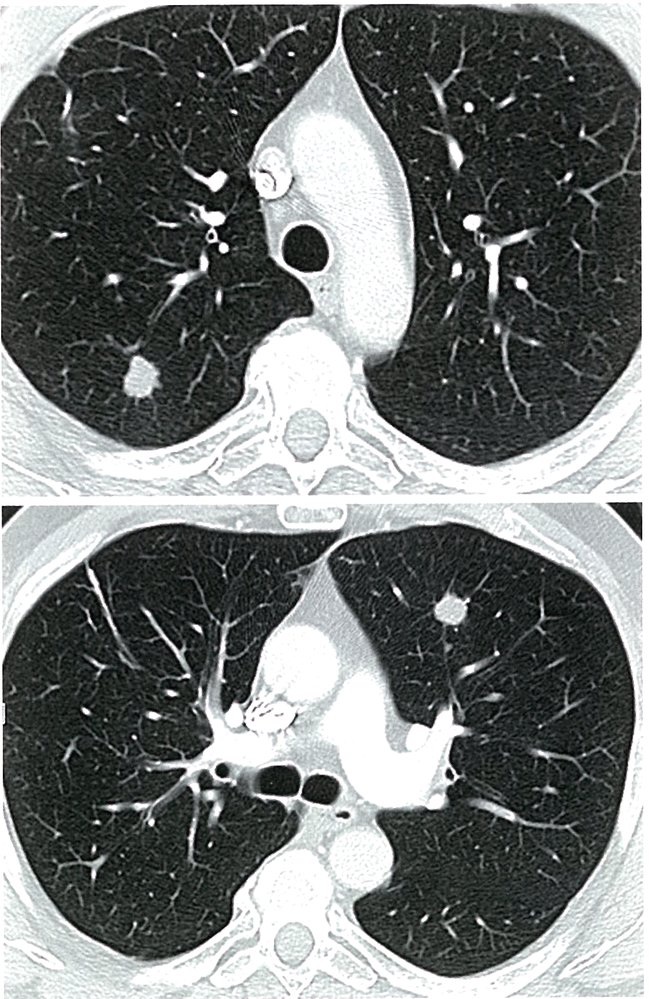
CT scan of the lung (transverse section)
Two smoothly marginated, noncalcified lesions are visible (left, ventral, right, dorsal). These lesions are lung metastases in breast cancer.
Source: © IMPP
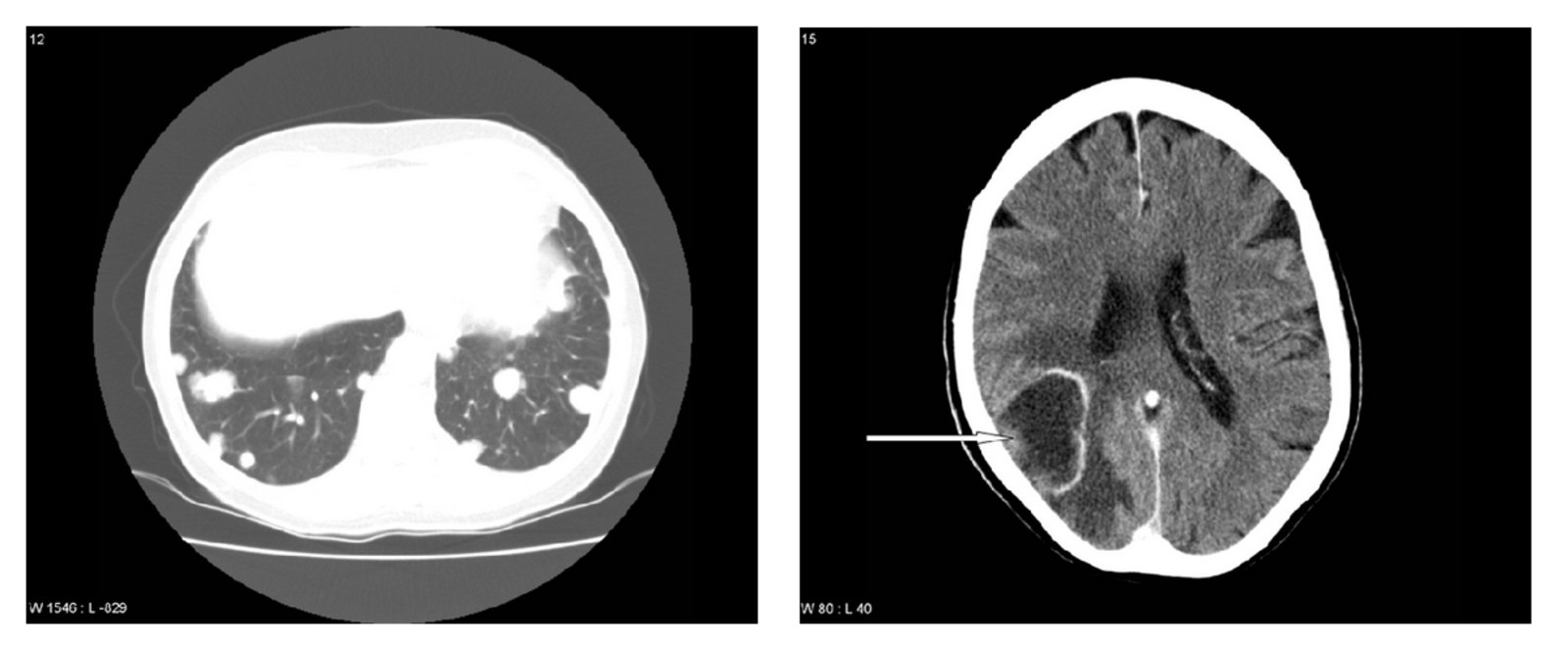
Left: CT chest (axial section)
Multiple high-density nodules are present bilaterally.
This appearance suggests lung metastases.
Right: CT head (axial section)
A large hypodense lesion is present in the right parietal lobe with a hyperdense rim and surrounding edema.
This appearance suggests partially necrotic brain metastases.
Source: “Figure 2. in: A Case of Brain Metastases from Breast Cancer Treated with Whole-Brain Radiotherapy and Eribulin Mesylate” by Carsten Nieder, Gro Aandahl and Astrid Dalhaug, Case Reports in Oncological Medicine Journal, Hindawi Corporations, licensed under CC BY 3.0.
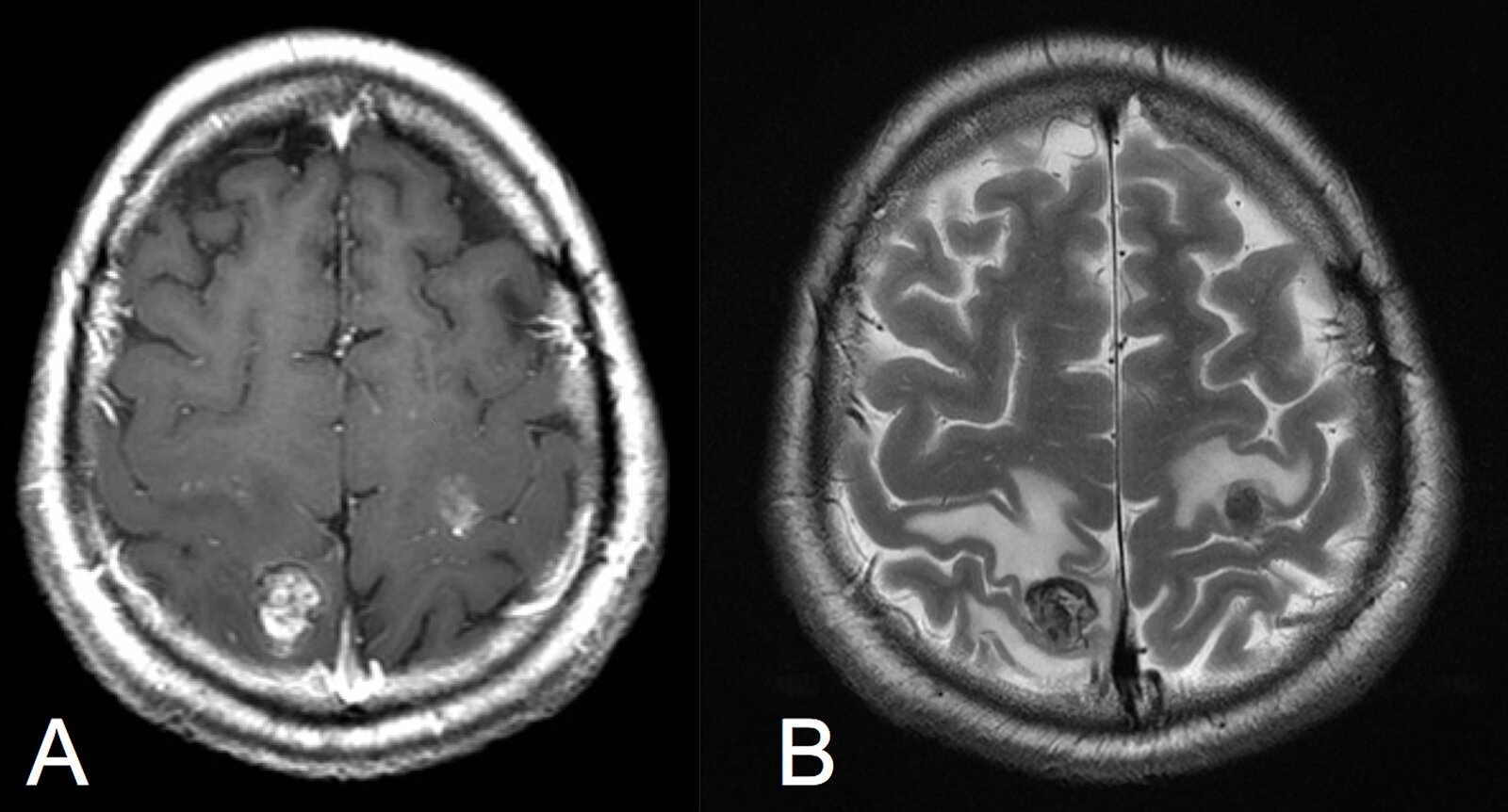
MRI brain (axial plane; A: T1-weighted, with contrast; B: T2-weighted, without contrast)
Two metastatic lesions are visible, one in the right high parietal lobe and one in the left high frontal lobe in the central region. Both metastases show perifocal edema, strong contrast enhancement, and reduced signal intensity in the T2 sequence, indicating hemorrhage.
Source: “Fig. 1, in: Primary Cardiac High-grade Myxofibrosarcoma Presenting with Multiple Brain Metastases: A Case Report” by Badaloni F, Pozzati E, Marucci G, Fiaschi P, Fioravanti A, Cureus, licensed under CC BY 3.0. Modifications: -arrows removed.
TNM classification
| TNM classification of breast cancer | |||
|---|---|---|---|
| Stage | Primary tumor | ||
| Tis |
|
||
| T1 |
|
||
| T2 |
|
||
| T3 |
|
||
| T4 |
|
||
| Lymph node involvement (clinical) | |||
| N1 |
|
||
| N2 |
|
||
| N3 |
|
||
| Distant metastases | |||
| M |
|
||
Pathology
Noninvasive carcinomas
DCIS
- Enlarged ducts lined with atypical epithelium
- Neoplastic cells within ductal lumen
- Intact basal membrane
- Microcalcifications

Comedocarcinoma
- Cells with high-grade nuclei
- Extensive central caseous necrosis
- Dystrophic calcifications

Invasive carcinomas
Invasive ductal
-
Findings
- Disorganized, small, duct-like glandular cells with stromal invasion (desmoplastic stroma)
- Fibrosis of surrounding tissue
- Microcalcifications
-
Subtypes
- Tubular
- Well-differentiated tubular structures without myoepithelium
- Stromal invasion (radial pattern)
-
Mucinous
- Well circumscribed tumor
- Copious extracellular mucus
- Tubular

 1/3")
 2/3")
 3/3")
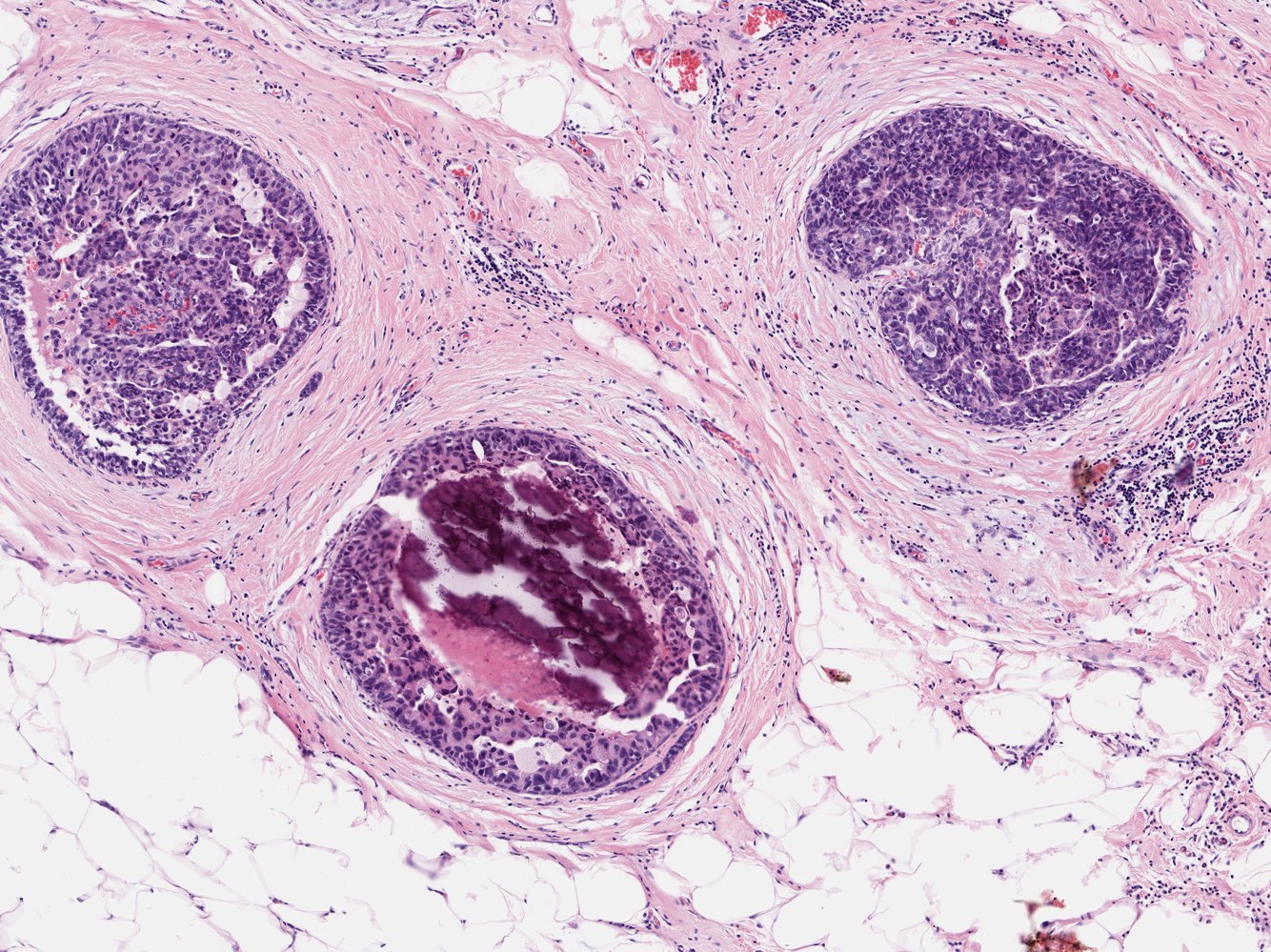
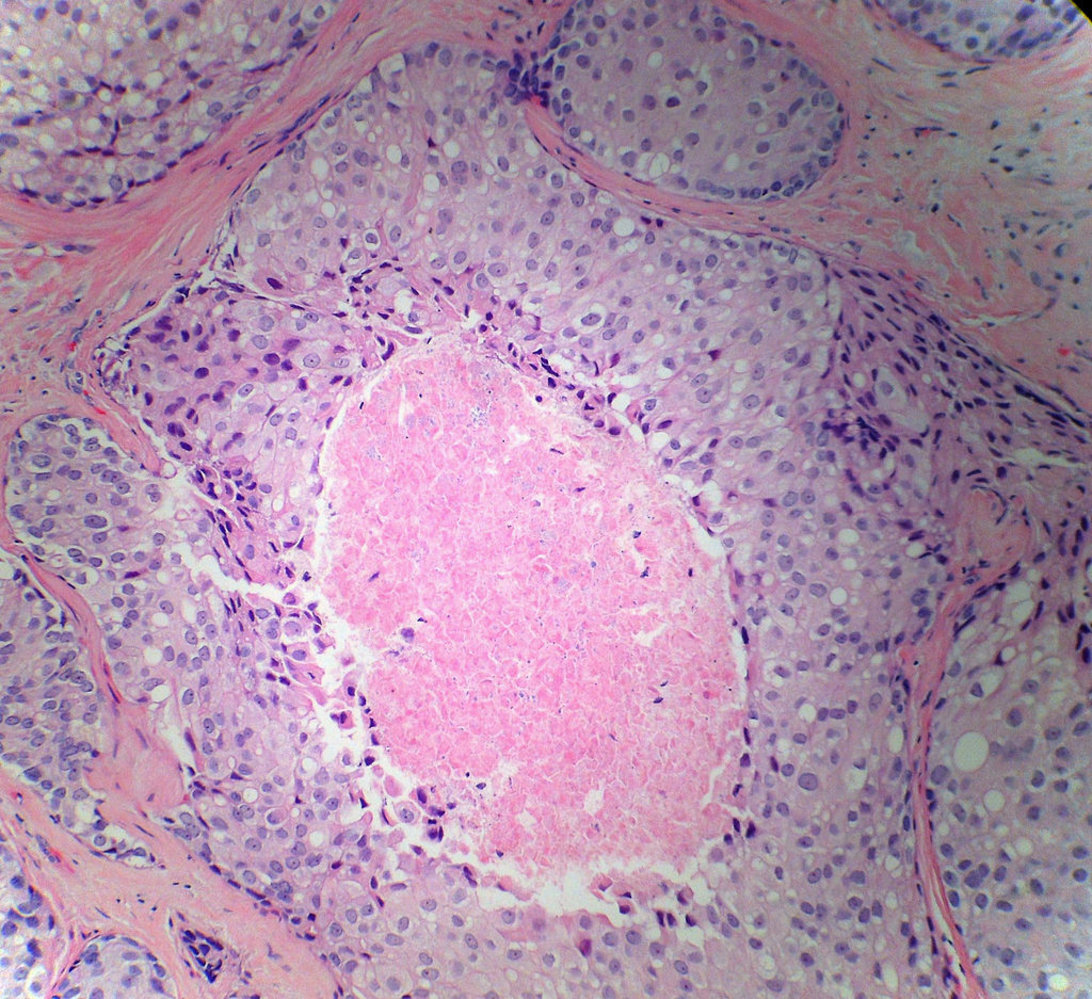
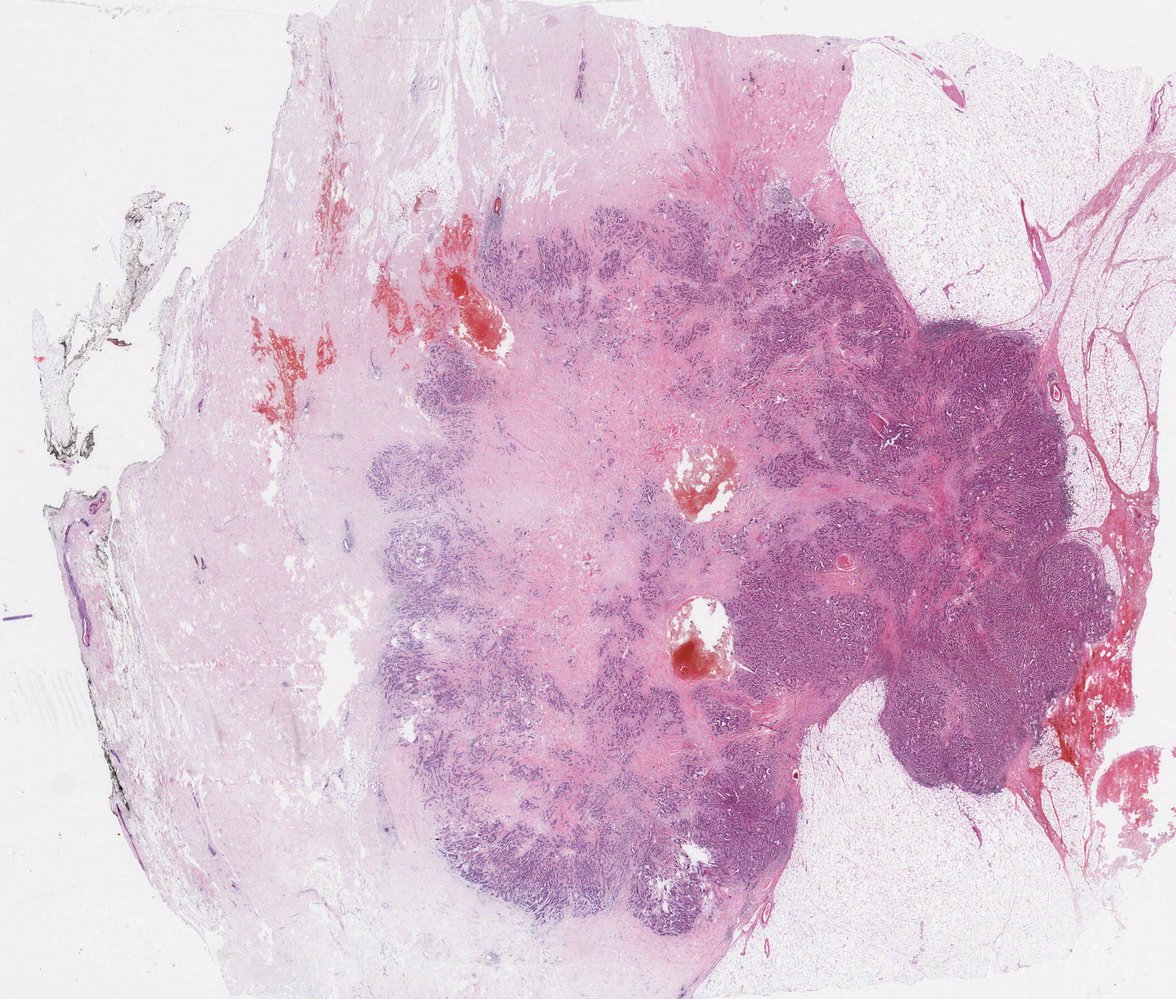
Medullary carcinoma
- Well circumscribed, rapidly growing tumor (can mimic fibroadenoma)
- Large, poorly differentiated cells with syncytial growth involving lymphocytic and plasma cell infiltration
Invasive lobular
- Malignant cells in lobules
- Monomorphic cells in a single file pattern due to a decrease in E-cadherin expression
- Absence of new duct formation
- Often without desmoplastic response
In INvasive Lobular carcinoma, neoplastic cells arranged IN Lines.

Subtypes and variants
Inflammatory carcinoma
- Dermal lymphatic invasion and angioinvasion
- Rapid growth
- No mass formation
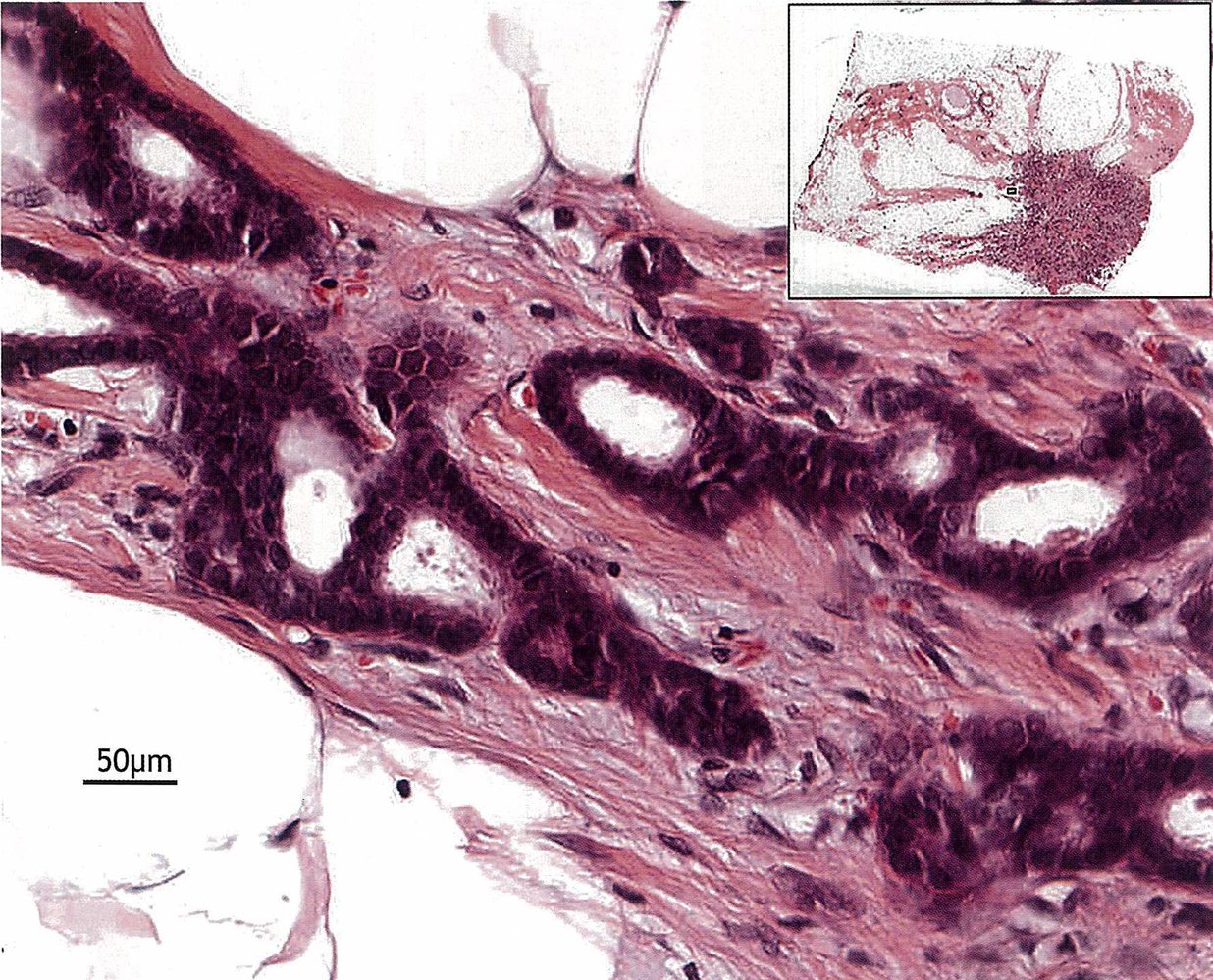
Paget disease of the breast
- Paget cells (large, round cells with clear halo and prominent nuclei) form an intraepithelial adenocarcinoma.
- Extend up the lactiferous ducts and into the skin of the nipple
Photomicrograph of a breast tissue biopsy specimen (H&E stain; high magnification)
Intraductal tumor cells (green overlay) with a hyperchromatic nucleus are visible. Calcifications (red overlay) are visible in the lower duct.
These are characteristic histological features of ductal carcinoma in situ.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Photomicrograph of comedocarcinoma (H&E stain)
There is central accumulation of cell debris (green overlay; necrosis), which is surrounded by pleomorphic cells. Mitotic figures (examples indicated by black arrowheads) can be found within the parenchyma. There are also coarse collagen bundles (red overlays) and widened septae, which indicate periductal fibrosis, an indirect sign of inflammation (no abundant leukocytes present).
This appearance is characteristic of comedocarcinoma.
Source: “Breast DCIS Comedonecrosis MP PA” by Sarahkayb, Wikimedia commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
Photomicrograph of a surgical sample of breast tissue (H&E stain, low magnification)
An area of sclerosis (light purple) is visible in the center of the invasive ductal carcinoma (dark purple).
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
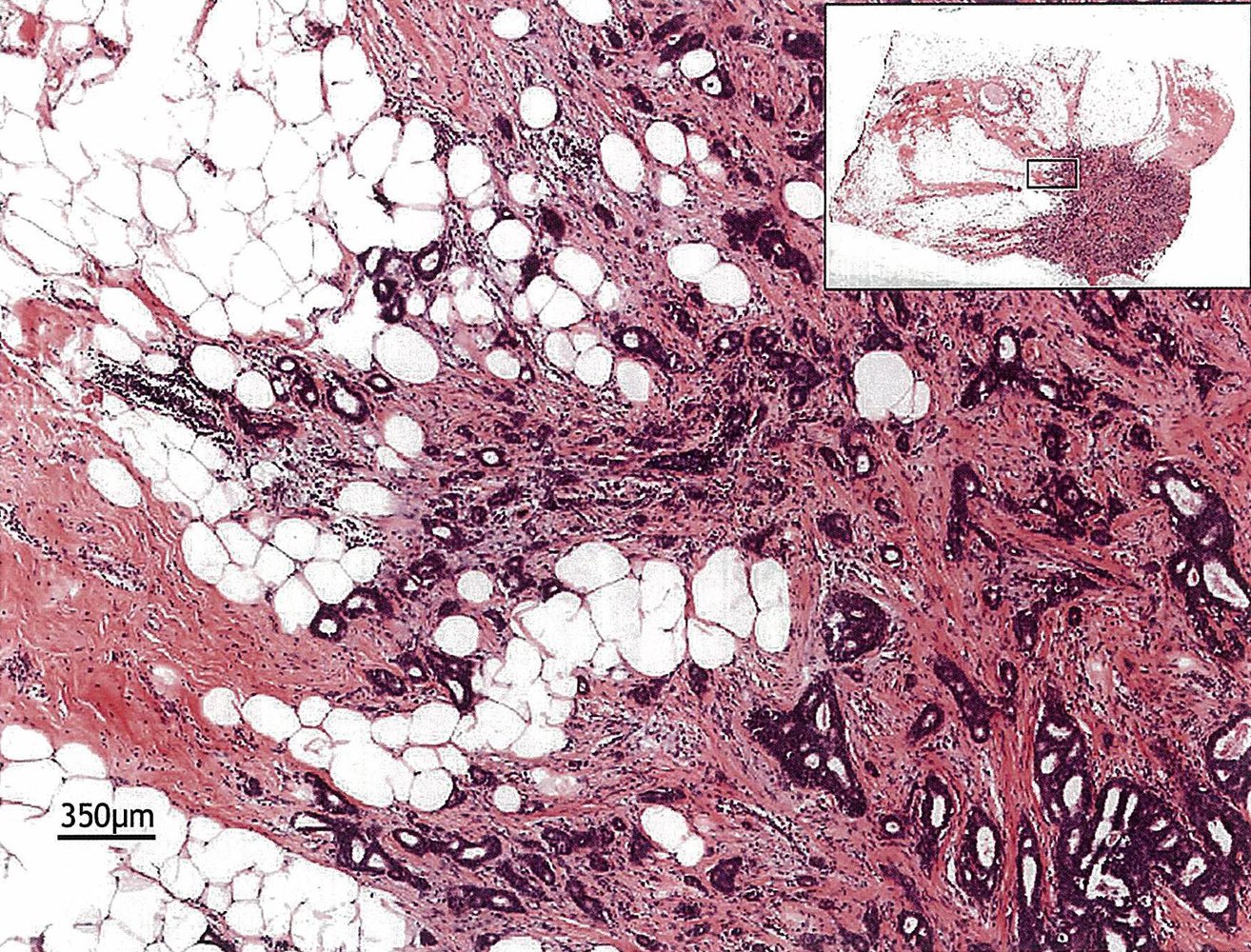
Photomicrograph of biopsy specimen (H&E stain; high magnification) from a mobile breast lump in 64-year-old female patient
Main image: At high magnification, the tubular formations of the carcinoma can be seen in detail, showing hyperchromatic nuclei and an increased nuclear:cytoplasmic ratio (i.e., shifted in favor of the nuclei). These changes cause the marked dark blue/basophilic appearance of the tumor tissue in the overview magnification.
Top right inset: very low magnification overview indicating the location of the main image on the specimen
Source: © IMPP
Photomicrograph of biopsy specimen (H&E stain; medium magnification) from a mobile breast lump in 64-year-old female patient
Main image: At intermediate magnification, the morphology of the carcinoma (dark blue/basophilic staining) invading the adipose breast tissue (white) becomes clearer. The disorganized tubular formations of the carcinoma (examples indicated by green overlay) have highly variable lumen diameters and are irregularly spaced in the surrounding collagenous connective tissue (pink/eosinophilic staining; also known as “desmoplastic stroma”).
Top right inset: very low magnification overview indicating the location of the main image on the specimen
Source: © IMPP
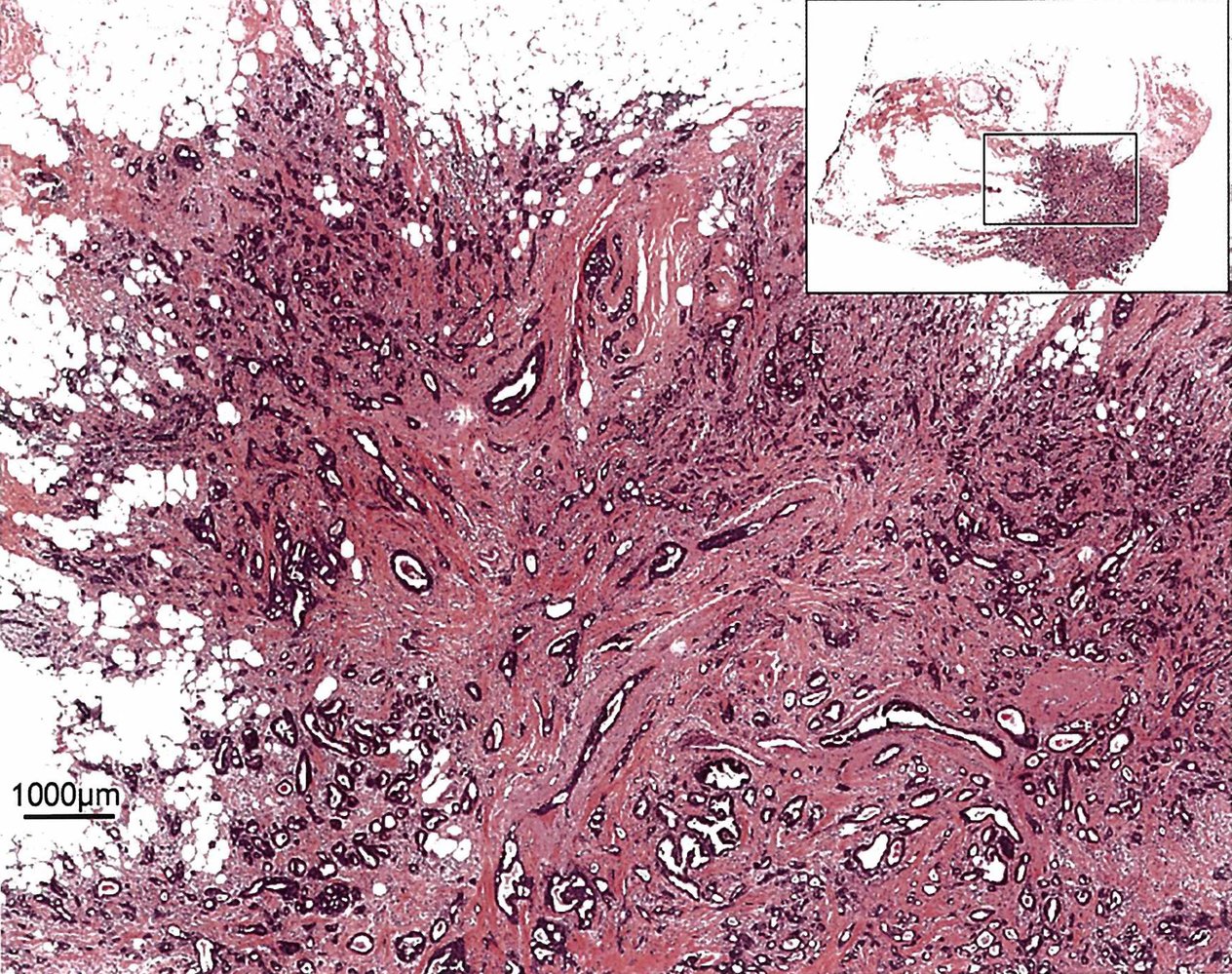
Photomicrograph of biopsy specimen (H&E stain; low magnification) from a mobile breast lump in 64-year-old female patient
Main image: At low magnification, a dense irregular mass (purple/pink) with poorly circumscribed borders can be seen infiltrating the mature adipose tissue of the breast (white). The mass is composed of disorganized tubular formations of the carcinoma (dark blue/basophilic staining) and surrounding collagenous connective tissue (pink/eosinophilic staining; also known as “desmoplastic stroma”).
Top right inset: very low magnification overview indicating the location of the main image on the specimen
Source: © IMPP
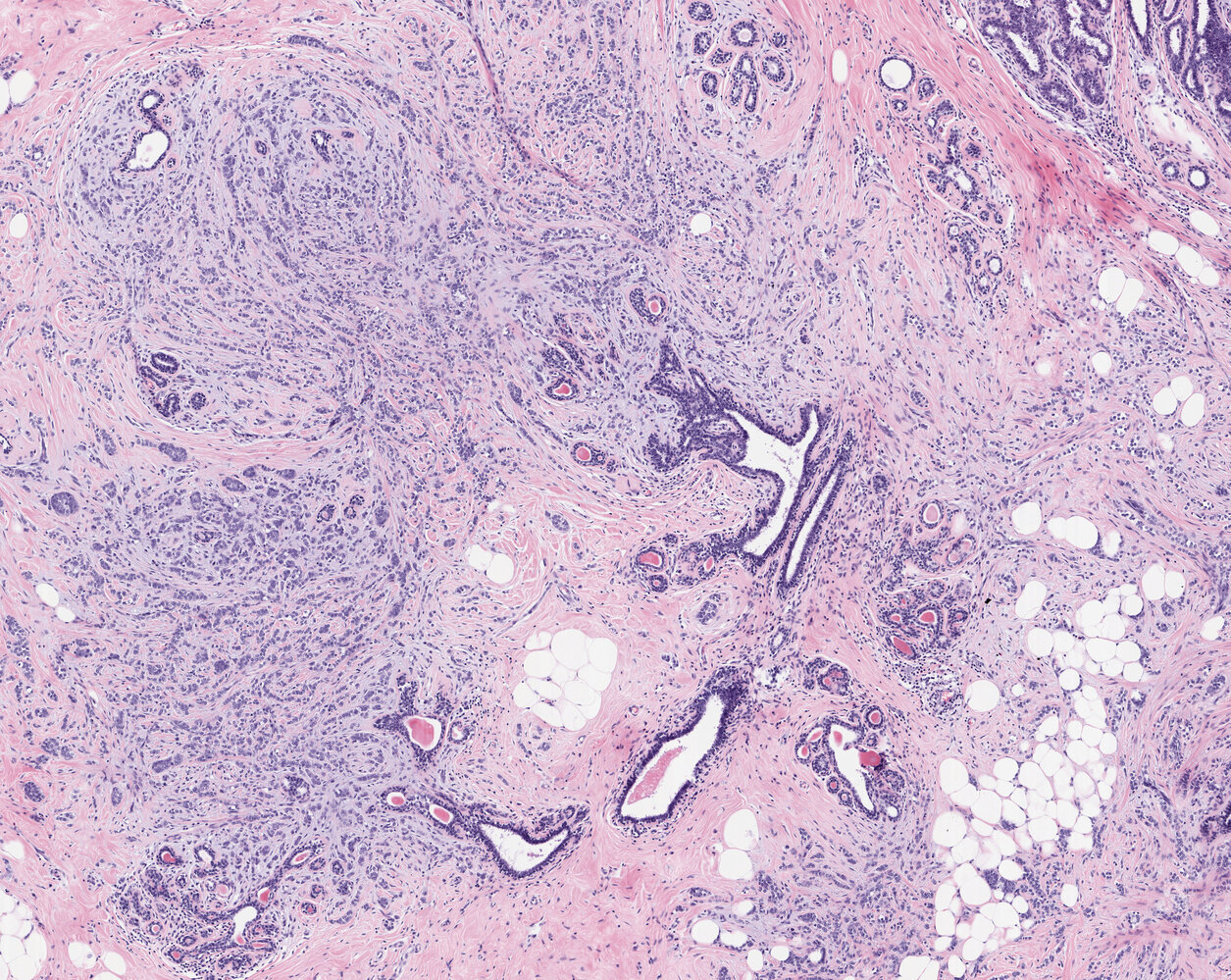
Photomicrograph of a breast tumor tissue specimen (H&E stain; 40x magnification)
Infiltrating malignant cells can be seen as single cells, narrow chords (examples indicated by green overlay), and characteristic single-file formations (examples indicated by blue overlay). The tumor cells are seen growing between distorted ductuli (D) and lobuli (L), surrounded by conspicuously pale connective tissue. There is no tubule formation of the tumor (as is commonly seen in other types of adenocarcinomas of the breast).
This is the typical appearance of invasive lobular carcinoma of the breast.
Click on the microscope icon (at the top) to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Treatment
Overview [15][37]
Breast cancer treatment is multidisciplinary, involving surgery, radiation therapy, and systemic therapy (chemotherapy, endocrine therapy, targeted therapy), alone or in combination. The choice of treatment regimen is based on the tumor stage, grade, receptor status, and patient preference.
Ductal carcinoma in situ (DCIS)
- Breast-conserving surgery (BCS) and adjuvant radiation; or mastectomy
- SLNB at the time of surgery as needed
- Adjuvant endocrine therapy for HR+ breast cancer
Nonmetastatic invasive breast cancer (M0)
- Surgical resection of tumor (BCS and adjuvant radiation; or mastectomy)
- Appropriate axillary staging and management
- Neoadjuvant and/or adjuvant systemic therapy based on tumor receptor status
- Adjuvant radiation as needed
Metastatic breast cancer (M1)
- Systemic therapy tailored to the subtype of breast cancer and menopause status [45]
- Palliative surgery and/or radiation therapy as needed for symptom management
Patients aged ≤ 35 years or those who are premenopausal and known carriers of the BRCA mutation require a risk assessment, counseling, and consideration for risk-reducing interventions for breast cancer. [37]
Supraclavicular and/or internal mammary nodal disease are managed with systemic therapy and radiation therapy. [46]
Reproductive care considerations for premenopausal patients
- Systemic therapy for breast cancer impacts fertility; refer patients who wish to have children to a fertility specialist to consider options for fertility preservation. [37]
-
Contraception
- All premenopausal patients with breast cancer should receive contraception counseling at diagnosis and follow-up visits. [47]
-
In patients with current or past history of breast cancer: [47][48][49]
- Hormonal contraceptives are contraindicated.
- Nonhormonal contraception (e.g., copper IUD) is preferred.
Several breast cancer treatment modalities are teratogenic. Advise patients to use contraception during treatment. [37]
Surgical resection of tumor and breast reconstruction
- Techniques to remove the primary tumor include BCS and mastectomy. [15]
- Axillary staging and management are typically performed at the time of surgery.
- Breast reconstruction surgery may also be performed at the time of tumor resection or at a later date. [50]
Breast-conserving surgery (BCS) [15][37][51]
BCS is the removal of breast cancer with clear surgical margins and preservation of most of the breast tissue (i.e., a wide local excision of breast cancer). [30][51]
-
Indications
- Nonmetastatic breast cancer
- DCIS
-
Contraindications
- Absolute
- Unlikely to achieve negative surgical margins and acceptable cosmesis with BCS
- Multicentric tumors
- Extensive microcalcifications on imaging
- Inflammatory breast cancer
- Early pregnancy
- Relative
- Large tumor-to-breast volume ratio
- Relative contraindications to adjuvant radiation therapy (e.g., history of chest radiation, certain collagen vascular diseases)
- Absolute
Resection of the nipple-areolar complex is not a contraindication for BCS, and it may be performed even in individuals with subareolar tumors. [52]
Mastectomy [37][53]
Mastectomy is the removal of the entire breast tissue and, depending on the specific procedure, possibly other structures, such as lymph nodes and the pectoralis muscles.
-
Indications
-
Treatment of breast cancer in patients with, e.g.:
- Contraindications to BCS
- Preference for mastectomy
- Recurrence following BCS and radiotherapy
- Breast cancer prophylaxis in high-risk patients (see “Risk-reducing interventions for breast cancer”)
-
Treatment of breast cancer in patients with, e.g.:
| Types of mastectomy [54] | |
|---|---|
| Description | |
| Total mastectomy |
|
| Skin-sparing mastectomy |
|
| Nipple-sparing mastectomy |
|
| Radical mastectomy |
|
| Modified radical mastectomy |
|
| Double mastectomy |
|
Breast reconstruction [50][57]
- Breast reconstruction surgery may be performed at the time of tumor resection (immediate reconstruction) or at a later date (delayed reconstruction).
- Reconstructive procedures include:
- After lumpectomy: breast lift and/or breast reduction surgery to shape the breast using remaining breast tissue
- After mastectomy
- Implant-based breast reconstruction: Removed breast tissue is replaced with a prosthetic device.
- Autologous breast reconstruction: Removed breast tissue is replaced with tissue from the patient.
- Use shared decision-making to discuss reconstructive options.
- Potential benefits of breast reconstruction surgery after mastectomy compared with mastectomy alone include improved: [58]
- Psychosocial and sexual well-being
- Body image
- Risks of reconstructive options should always be reviewed with patients; see “Complications of breast implants.”
- Potential benefits of breast reconstruction surgery after mastectomy compared with mastectomy alone include improved: [58]
Breast implants [50][57]
- Breast implants are prosthetic devices that consist of a silicone shell filled with silicone gel or saline.
- Implants are not expected to last a lifetime, but there is no formal guidance on the timing of implant removal. [57][59]
- Patients with breast implants should continue to receive breast cancer screening based on their risk for cancer.
Silicone-filled implants
- Compared to saline-filled implants, silicone-filled implants:
- Feel more similar to natural breast tissue
- Have a lower rate of capsular contracture
- Regular screening for implant rupture is recommended. [57][60]
- Ruptures of silicone-filled implants are often silent (i.e., no noticeable changes on examination).
- Screening is recommended 5–6 years after implant placement, then every 2–3 years. [57][60]
- Screening modalities include breast MRI and ultrasound.
Asymptomatic individuals who have silicone-filled breast implants should be regularly screened for silent implant rupture. [57][60]
While most silicone-filled implant ruptures are asymptomatic, silicone from a ruptured implant can leak into surrounding breast tissue and cause pain, breast lumps, or changes in breast shape. [57][59]
Saline-filled implants
- Implant rupture is easily identifiable (implant deflation).
- In an implant leak or rupture, saline is absorbed by the body.
Individuals who have saline-filled breast implants do not need to undergo screening for silent rupture. [57]
Complications of breast implants [57]
Some complications may necessitate the removal of the breast implant; refer to plastic surgery as needed for complete evaluation and appropriate management.
-
Acute complications
- Pain
- Seroma or hematoma
- Delayed wound healing
- Breast implant infection
-
Chronic complications
- Capsular contracture causing pain and/or breast distortion
- Implant rupture or leak
- Implant-associated malignancy (rare): a malignancy arising in the pericapsular scar tissue adjacent to breast implants and distinct from breast cancer [61]
- Breast implant-associated squamous cell carcinoma
- Breast implant-associated anaplastic large cell lymphoma
- Other lymphomas
- Breast implant illness
Breast implants are medical devices; reporting associated complications to the FDA is encouraged.
Although complications associated with breast implants are uncommon, preprocedural counseling should include information on alternative options for breast reconstruction (e.g., autologous tissue reconstruction) and details on the risks and follow-up care for breast implants, including the possible need for implant removal. [57][61]
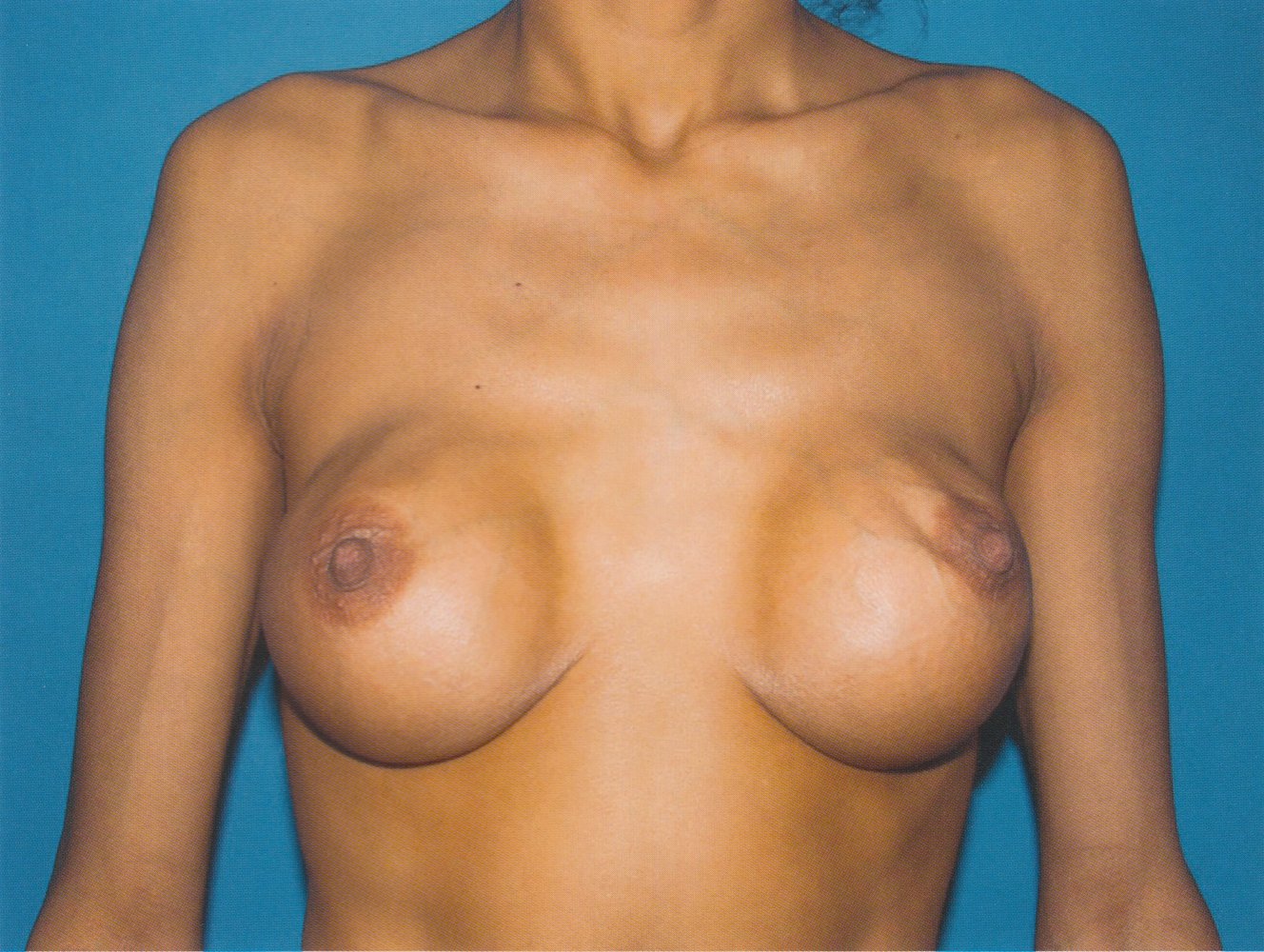
The breasts and nipple-areolar complexes are distorted and asymmetrical, which is consistent with capsular contracture.
On physical examination, capsular contracture typically feels firm or hard on palpation.
Source: © IMPP
Management of axillary lymph nodes
Overview [22][37][46]
Axillary staging and management should only be performed if results will affect management.
| Axillary staging in breast cancer [22][37][46] | |
|---|---|
| Modality | Indications |
| Sentinel lymph node biopsy (SLNB) [21] |
|
| Axillary lymph node dissection (ALND) [62] |
|
| Observation [46] |
|
Management of axillary lymph nodes in early-stage breast cancer (T1/T2) [22][37][46]
No palpable lymph nodes on examination
- Complete neoadjuvant chemotherapy if planned. [22]
- Perform SLNB.
- ≥ 3 positive sentinel lymph nodes on biopsy: ALND and axillary radiation are recommended.
- No or ≤ 2 positive sentinel lymph nodes: Consider axillary radiation as needed.
Palpable axillary lymph nodes
- Confirm lymph node involvement on image-guided FNA or CNB.
-
Biopsy-confirmed lymph node involvement:
- Consider neoadjuvant chemotherapy to downstage the axilla.
- Palpable lymph nodes after neoadjuvant chemotherapy: Perform ALND followed by axillary radiation therapy.
- No palpable lymph nodes after neoadjuvant chemotherapy: SLNB may be appropriate.
- Patients not receiving neoadjuvant chemotherapy: Perform ALND.
- Consider neoadjuvant chemotherapy to downstage the axilla.
ALND is associated with significant complications, including lymphedema, and has largely been replaced by SLNB in the management of early-stage breast cancer. [37]
SLNB is not recommended before the completion of neoadjuvant chemotherapy. [22][46]
Radiation therapy
-
Indications
-
Adjuvant radiation therapy is indicated for:
- DCIS and early-stage breast cancer in patients with nodal involvement disease or patients who have undergone BCS
- Locally advanced breast cancer
- Palliative radiation therapy: as needed for individuals with metastatic breast cancer
-
Adjuvant radiation therapy is indicated for:
-
Sites of radiation administration : [15][22][64]
- Partial or whole breast
- Locoregional lymph nodes
- Chest wall
Radiation therapy is contraindicated during pregnancy. [65]
Radiation therapy is performed after the completion of chemotherapy in patients requiring both of these modalities as adjuvant treatment. [37]
Systemic therapy
- Systemic therapy can be given as neoadjuvant and/or adjuvant therapy in combination with other treatment modalities. [15][30][66]
- The choice of therapy is based on tumor characteristics.
- HR+ tumors: endocrine therapy with or without chemotherapy
- ERBB2+ tumors: targeted immunotherapy and chemotherapy
- Triple-negative breast cancer: chemotherapy
Patients with ERBB2+/HR+ tumors should receive both endocrine therapy and targeted immunotherapy. [31]
Chemotherapy [15][30][31]
-
Indications
- Triple-negative breast cancer with tumor size ≥ 0.5 cm
- ERBB2+ breast cancer (adjunct to targeted therapy)
- HR+/ERBB2- breast cancer (adjunct to endocrine therapy in selected patients)
- Positive lymph nodes
- Tumor size > 2 cm
-
Agents
- Typically include anthracyclines (e.g., adriamycin, doxorubicin) and/or taxanes (e.g., docetaxel, paclitaxel)
- Example regimens: [15]
- Adriamycin/cyclophosphamide
- Docetaxel/cyclophosphamide
- Cyclophosphamide/methotrexate/5-FU
PARP inhibitors (e.g., olaparib, talazoparib) disrupt cellular DNA damage repair and can be used to treat ERBB2- or triple-negative metastatic or high-risk breast cancer in patients with BRCA mutations. [15][67]
Genomic testing can help guide decisions on whether to include chemotherapy as part of treatment. [15][30][68]
Endocrine therapy [15][30]
-
Indications
- HR+ tumors
- Chemoprevention in patients at high risk of breast cancer
- Goal: suppression of hormone-induced tumor growth to decrease the risk of breast cancer or its recurrence
-
First-line agents: anti-estrogen therapy; generally administered for 5–10 years [15]
-
Premenopausal patients with HR+ breast cancer
- Tamoxifen
- OR GnRH agonists (e.g., leuprolide acetate, goserelin) to induce ovarian suppression; PLUS either tamoxifen or an aromatase inhibitor
-
Postmenopausal patients with HR+ breast cancer
- Tamoxifen
- OR aromatase inhibitors (e.g., anastrozole, exemestane, letrozole)
- Chemoprevention for high-risk patients: See “Risk-reducing interventions for breast cancer.”
-
Premenopausal patients with HR+ breast cancer
The first-line management for metastatic HR+/ERBB2- breast cancer is typically endocrine therapy in combination with CDK4/6 inhibitors (e.g., abemaciclib, palbociclib), which arrest the cell cycle. [15][45]
ERBB2-targeted therapy [15][30]
ERBB2-targeted therapy includes ERBB2 antibodies (e.g., trastuzumab, pertuzumab) and tyrosine kinase inhibitors (e.g., lapatinib, neratinib).
- Indication: all ERBB2+ tumors
-
First-line agent: trastuzumab
- A humanized monoclonal antibody against the ERBB2 tyrosine kinase receptor; used in the treatment of ERBB2+ breast and gastric cancer [69][70]
- Mechanism of action: targets c-erbB2 tyrosine kinase receptor → ↓ of ERBB2-initiated cellular signaling and ↑ antibody-dependent cytotoxicity → ↓ tumor growth
- Adverse effects: cardiotoxicity (e.g., dilated cardiomyopathy with systolic CHF) [71]
- Other agents: pertuzumab, ado-trastuzumab emtansine, neratinib, lapatinib
Trastuzumab causes dilated cardiomyopathy: Trust HER2 enlarge your heart.
Echocardiography should be performed before, during, and after treatment with trastuzumab. [72]
Follow-up
Surveillance for recurrence should be individualized ; consult the treating oncology team. Counsel all patients on signs of local and regional recurrence. [73]
- Comprehensive history and physical examination
- Every 3–6 months for 3 years
- Every 6–12 months for an additional 2 years
- Annually thereafter
-
Breast imaging
- Prior bilateral mastectomy: routine breast imaging not recommended
- Prior unilateral mastectomy: annual mammography of the intact breast
- Prior lumpectomy: annual mammography of both breasts
- Consider supplemental surveillance (e.g., with breast MRI) only in high-risk individuals.
Assess for recurrence, complications of treatment, and body image concerns at every follow-up visit.
Complications
Cancer-associated complications
- Malignant pleural effusion: affects 7–11% of all individuals with breast cancer [74]
- Paraneoplastic syndromes
- Recurrence occurs in ∼ 40% of all cases. [75]
Recurrence typically occurs in the first five years after completion of treatment.
Treatment-associated complications
Long thoracic nerve damage
- Intraoperative complication during radical mastectomy
- Causes winged scapula, which may lead to muscle disorders and shoulder, neck, and upper back pain
Secondary lymphedema of the arm [76]
-
Etiology
- Surgical intervention and/or radiation in the axillary region
-
The frequency of lymphedema varies depending on the treatment modality.
- Lumpectomy alone: 3%
- Total mastectomy PLUS axillary radiation: ∼ 15%
- ALND PLUS axillary radiation: 21–51%
-
Risk factors
- Location of the tumor in the upper outer quadrant
- ALND
- Radiation after ALND
-
Clinical features
- Immobility of the limb, swelling, feeling of tightness
- ↑ Risk of infection
- ↓ Wound healing
- Cosmetic disfigurement
-
Diagnostics: clinical diagnosis
- Review of medical and surgical history
- Skin inspection and palpation; assessment of tissue consistency and skin mobility
- Measurement of volume and girth
-
Treatment
- Hyperbaric oxygen therapy
- Low-level laser therapy
- Microsurgical lymphatic-venous anastomoses
- Complete decongestive therapy
- Manual lymph drainage
- Compression
- Complications: angiosarcoma of the breast (see below)
Secondary malignancies
-
Angiosarcoma of the breast
- Rare malignancy that is sometimes referred to as lymphangiosarcoma or hemangiosarcoma, depending on whether it arises from lymphatic or capillary endothelial cells
- Results from chronic lymphedema in patients who have undergone lymphadenectomy and/or radiation therapy
- Manifests with multiple blue/purple, macular, and papular lesions in the area of the breast, chest wall, and/or upper extremity
- Endometrial cancer: risk increased by tamoxifen therapy

We list the most important complications. The selection is not exhaustive.

Right breast of a 56-year-old female patient after receiving radiotherapy for ductal carcinoma in situ
A purple macule measuring approximately 7 × 5 cm and resembling a hematoma is visible on the previously irradiated lower right quadrant of the right breast. Parts of the macule appear darker and indurated.
This type of cutaneous lesion combined with the patient's medical history suggest an angiosarcoma of the breast, which can occur secondary to radiation therapy. Since this is a rare condition, the clinical features seen here are easily mistaken for benign angiomas, small hematomas, or atypical telangiectasia. Histopathological investigation is needed to confirm the diagnosis.
Source: “Fig 1, In: A case report on radiation-induced angiosarcoma of breast post skin-sparing mastectomy and reconstruction with transverse rectus abdominal muscle” by Aljarrah A, Nos C, Clough KB, Lefrere-Belda MA, Lecuru F, ecancermedicalscience, licensed under CC BY 3.0.
Special patient groups
Breast cancer in pregnancy
Breast cancer occurs in about 1 in 3000 pregnant women. [77]
Management [65][78]
- The risks and benefits of treatment options for the mother and fetus should be considered and discussed with the patient.
- If breast cancer is diagnosed in the first trimester, discuss the option of terminating the pregnancy.
-
Diagnosis, staging, and management options are similar to those for breast cancer in nonpregnant individuals, with some modifications for fetal safety such as:
- Use of ultrasound or noncontrast MRI for staging instead of x-ray or CT
- Mastectomy may be preferred over BCS.
- ALND may be preferred over SLNB.
- There is a paucity of data on the safety of systemic therapy for the fetus.
- Chemotherapy is contraindicated in the first trimester but may be considered in the second and third trimesters. [79]
- Endocrine therapy and ERBB2-targeted therapy are contraindicated during pregnancy. [80]
Radiation therapy, endocrine therapy, and ERBB2-targeted therapy are contraindicated during pregnancy. [65]
Breastfeeding is not recommended if patients are receiving ERBB2-targeted therapy or endocrine therapy. [81]
Male breast cancer [82][83]
Male breast cancer is rare (∼ 1% of all breast cancers) and typically manifests as a painless retroareolar mass with or without skin or nipple changes. Invasive HR+/ERBB2- breast cancer is the most common subtype in men.
Risk factors
- BRCA mutation (most important risk factor)
- Radiation exposure
- Elevated estrogen (e.g., Klinefelter syndrome, chronic liver disease, obesity)
Diagnostics
- Imaging for a breast mass
- Age < 25 years: breast ultrasound
- Age ≥ 25 years: mammography
- Diagnostic confirmation: CNB
- Staging and receptor testing: same as for female breast cancer
- Consider genetic counseling and genetic testing for all male individuals with breast cancer.
Treatment
The treatment approach is similar to that for women with breast cancer.
- Nonmetastatic breast cancer: mastectomy with SLNB or ALND followed by adjuvant therapy as indicated
-
Metastatic breast cancer
-
HR+/ERBB2- breast cancer
- First-line: endocrine therapy
- CDK inhibitors or mTOR inhibitors may also be considered in combination with endocrine therapy.
- Chemotherapy
-
HR+/ERBB2- breast cancer
In patients with HR+ male breast cancer, endocrine therapy with tamoxifen is preferred. For all patients with ERBB2+ breast cancer, ERBB2-targeted therapy is indicated. [82]
Male breast cancer is typically diagnosed at an advanced stage and is associated with a poorer prognosis than breast cancer in women. [84]
Follow-up [84]
- Regular clinical examination to assess for recurrence or metastasis
- Imaging
- Patients who have undergone BCS: annual ipsilateral mammogram (if feasible)
- Patients with a genetic predisposition for breast cancer: Consider an annual contralateral mammogram.
Screening [84][85]
- Routine screening is not recommended.
- Individuals with known BRCA mutations
- Annual screening for breast cancer with clinical breast examination starting at 35 years of age [85]
- In patients with gynecomastia, consider screening with annual bilateral mammogram starting at age 50 years or 10 years before the earliest onset of breast cancer in the family, whichever is earlier. [85]
Prognosis
Prognostic factors [86]
Stage at diagnosis
The most important prognostic factor is the breast cancer stage at time of diagnosis. Earlier stages have a significantly better prognosis than late stages.
-
Tumor size
- Large tumors have a less favorable prognosis because they are associated with higher rates of recurrence.
- Positive correlation between tumor size and number of involved lymph nodes
- Lymphatic spread: Axillary lymph node status is the one of most important prognostic factors.
- Distant metastasis: Distant metastasis limited to bone has a more favorable prognosis than visceral or brain metastasis. [15]
- Histological tumor grade: High-grade tumors are associated with aggressive progression.
-
Receptor status
- HR- breast cancer has a poorer prognosis than HR+ breast cancer.
- ERBB2+ tumors show aggressive growth and metastasize quickly compared to ERBB2- tumors.
- Triple-negative disease is associated with a poor prognosis.
HR+/ERBB2- breast cancer has the best prognosis.
ERBB2+ cancers demonstrate more aggressive tumor growth and higher recurrence rates and are, therefore, associated with a poor prognosis. However, since the development of targeted therapy with trastuzumab, the prognosis for patients with ERBB2+ cancers has improved.
Other prognostic factors
- Advanced age
- Aneuploidy
- Interval between initial diagnosis and development of metastatic recurrence [15]
- Patient performance status
- Black race
In the US, breast cancer in Black individuals is associated with a poorer prognosis than in White individuals because of a higher incidence of triple-negative and HR- breast cancer and disparities in access to appropriate and timely health care. [86]
Survival [87]
| Survival of breast cancer patients [87] | |||
|---|---|---|---|
| SEER stage | AJCC/UICC | Description | 5-year survival rate |
| Localized |
|
|
|
| Regional |
|
|
|
| Distant |
|
|
|
Screening
Approach
The following recommendations are for screening asymptomatic individuals. The diagnostic approach to patients with breast symptoms (e.g., palpable breast mass, nipple discharge) is detailed in separate articles. [88][89][90]
- Consider risk assessment for breast cancer in all women by the age of 25 years. [90][91][92]
- Initiate age- and risk-appropriate breast cancer screening.
- Benign features on breast imaging (i.e., BI-RADS 1–2): Continue routine age- and risk-appropriate screening. [25]
- Inconclusive features or features concerning for malignancy detected on initial imaging:
- Further imaging may be needed (e.g., diagnostic mammography after screening mammography). [93]
- All lesions suspicious for malignancy (e.g., BI-RADS 4–5) should be biopsied; image-guided core needle biopsy is preferred. [25]
- Biopsy-proven breast cancer: See “Diagnostics” for further workup.
Risk assessment [90][91][92]
There is a lack of standardized recommendations for breast cancer risk assessment; consider the following approach.
- Assess all women for risk factors for breast cancer by the age of 25 years.
- Consider further risk assessment in individuals with risk factors for breast cancer using a validated tool.
- Tailor screening recommendations to the lifetime risk of breast cancer. [94]
- Average risk: < 15% lifetime risk of breast cancer
- Intermediate risk: 15–20% lifetime risk of breast cancer
- High risk: ≥ 20% lifetime risk of breast cancer
Refer individuals with a high risk of breast cancer to specialists (e.g., oncologist, genetic counselor) for individualized screening recommendations and consideration of risk-reducing interventions for breast cancer. [92]
There is no standard approach to screening individuals at intermediate risk for breast cancer. Tailor screening frequency and modality to individual risk factors. [94]
Individuals at average risk [88][89][90][94]
These individuals do not have a high-risk condition for breast cancer but may have other risk factors for breast cancer.
Screening modalities
- Recommended: screening mammography
-
Not routinely recommended
- Supplemental MRI: may be considered in women with dense breasts and a normal screening mammogram [88][91][95]
- Clinical breast examination (CBE): generally not recommended for individuals at average risk of breast cancer [88][89][90]
Mammography is considered safe during pregnancy because it uses only a small amount of focused radiation on the breast tissue. The use of a lead shield effectively minimizes fetal radiation exposure.
Lactation is not a contraindication for screening mammography. Recommend breastfeeding or pumping immediately before performing mammography to minimize the effect of lactation on findings. [93]
Screening recommendations
Recommendations vary; use shared-decision making.
| Breast cancer screening for individuals at average risk | |||
|---|---|---|---|
| USPSTF (2024) [88] | ACS (2015) [89] | ACOG (2017; reaffirmed in 2021) [90] | |
| Screening recommendations |
|
|
|
| Discontinuation of screening |
|
|
|
For women with a family history of breast cancer, it is generally recommended to start breast cancer screening 10 years before the age of the earliest diagnosis in the family; but not before the age of 30 years. [94]
Routine breast self-examination is not recommended for individuals at average risk of breast cancer, but these individuals should be counseled on breast self-awareness and advised to alert their physician if they notice any breast changes. [89][90]

Individuals at high risk [96][97]
Individuals at high risk have any high-risk condition for breast cancer or a lifetime risk for breast cancer ≥ 20%; based on risk assessment tools such as the BRCAPRO or Gail model. [91][98][99]
High-risk conditions for breast cancer [89][91][96][98]
- Genetic predisposition, e.g.:
- Known BRCA mutation
- First-degree relative with a BRCA mutation and never tested for BRCA mutation
- Personal or family history of hereditary cancer syndromes (e.g., Li-Fraumeni syndrome, Cowden syndrome)
- History of chest radiation at a young age [100]
- Previous invasive breast cancer or high-risk lesion on biopsy
In individuals with a personal or family history of BRCA-related cancers, consider familial risk assessment tools (e.g., BRCAPRO or the Ontario family history assessment tool) to identify a genetic predisposition for breast cancer, and refer these individuals for genetic counseling. [30][55][99]
Screening recommendations [55][91]
Age to start screening, screening frequency, and screening modalities should be tailored to patient risk factors; ; consult a breast specialist.
| Breast cancer screening for individuals at high risk [55][91] | |
|---|---|
| Genetic predisposition to breast cancer |
|
| Lifetime risk for breast cancer ≥ 20% | |
| History of chest radiation at a young age [91][100] |
|
| Previous invasive breast cancer or high-risk lesion on biopsy [73][91] |
|
Transgender individuals [101]
As data for this population remains sparse, recommendations vary and are mostly based on expert consensus. [101]
Transgender women
- Average risk for breast cancer
- ≥ 5 years of gender-affirming hormone therapy (GAHT): Consider screening with mammography every 1–2 years, starting at 40 years of age.
- < 5 years of or no GAHT: Screening is not recommended.
-
High-risk condition for breast cancer
- ≥ 5 years of GAHT: Consider annual mammography starting from 25–30 years of age.
- < 5 years of or no GAHT: Consider screening mammography based on individual risk factors.
Transgender men
- Prior bilateral mastectomy
- The ACR does not recommend screening for breast cancer in this group of individuals. [101]
- Other societies suggest breast cancer screening be continued with an annual physical examination, breast ultrasound, or breast MRI. [102]
- Prior breast reduction surgery or no surgery: Management is the same as for cisgender women, based on risk for breast cancer. [88]
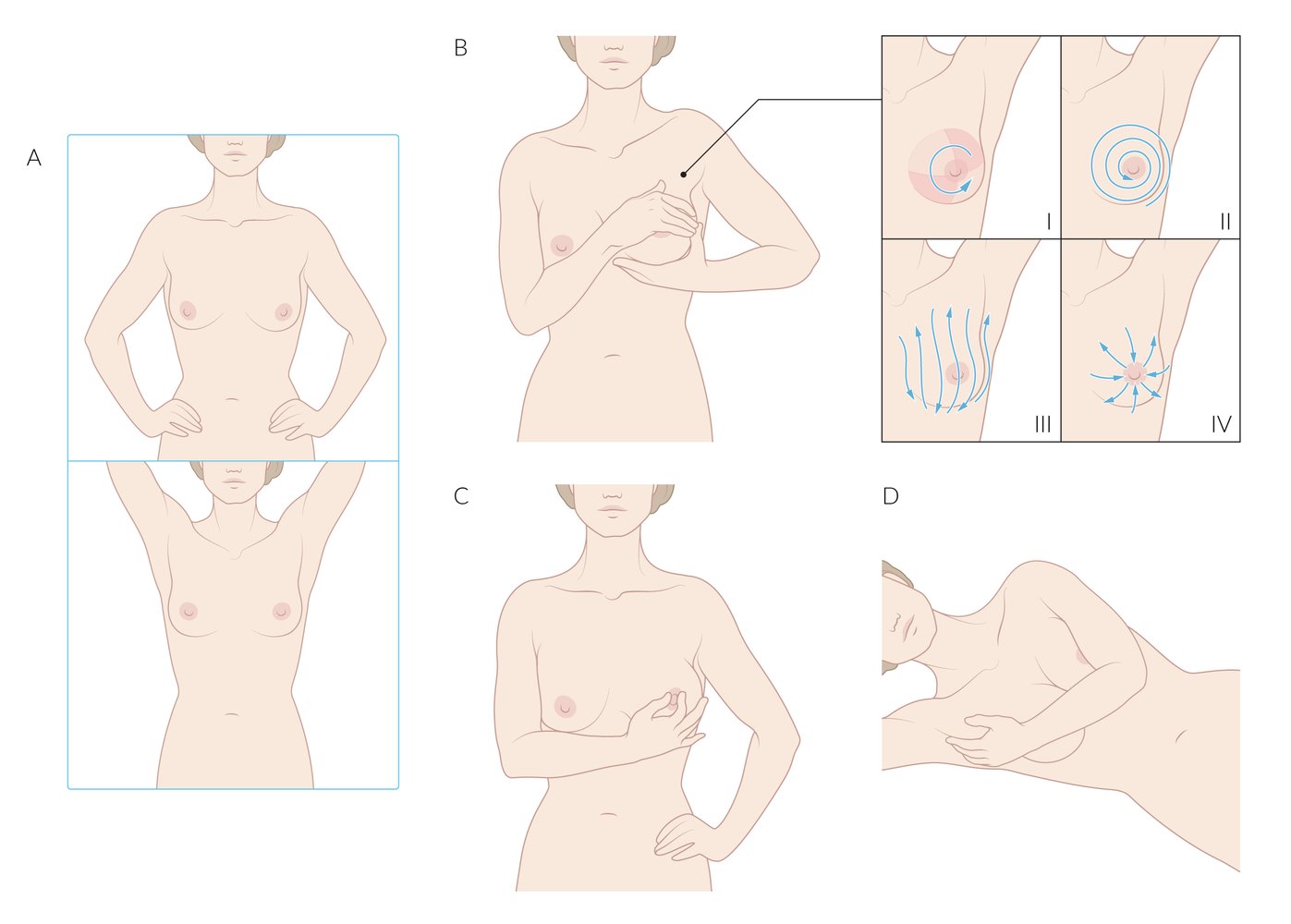
Breast self-examination (BSE) is a screening method for breast abnormalities (primarily signs of breast cancer) that involves the following technique:
A) Inspection: Look at the breasts directly in a mirror, with the arms at the sides, then raised above the head. Inspect the shape of each breast and look for changes in skin texture (e.g., dimpling, puckering, orange peel texture).
B) Palpation of the breast tissue using one of the four patterns depicted to cover all breast tissue
C) Palpation of the nipple: Squeeze the nipple gently and inspect for discharge (milky or bloody).
D) Palpation of axillary breast tissue: While standing or lying down, palpate the axillary tail of the breast, which extends into the axilla.
Note: The efficacy of routine BSE is still the subject of ongoing debate and, as such, is no longer recommended. Various studies have shown that it does not help reduce deaths from breast cancer but does lead to higher rates of biopsies of benign masses (unnecessary surgical biopsies). However, these studies have been criticized for employing inadequate BSE techniques and thereby introducing bias. In addition, many women continue to regard BSE as an important part of their health maintenance.
© AMBOSS
Risk-reducing interventions for breast cancer
Breast cancer risk-reducing interventions for individuals at high risk of breast cancer (e.g., known BRCA mutations) include surgery and chemoprevention.
-
Prophylactic surgery [55][99]
- Bilateral prophylactic mastectomy [103]
- Bilateral salpingo-oophorectomy [99]
-
Chemoprevention: usually prescribed for 5 years [104][105][106]
- Premenopausal women ≥ 35 years of age at high risk: tamoxifen [99][104]
-
Postmenopausal women at high risk
- Selective estrogen receptor modulators: tamoxifen or raloxifene [104]
- Aromatase inhibitors: anastrozole or exemestane [105]
Raloxifene and aromatase inhibitors should not be used for breast cancer risk reduction in premenopausal women. [105][106]
Related One-Minute Telegram
- One-Minute Telegram 126-2025-2/3: Navigating the path to cancer screening
- One-Minute Telegram 114-2025-2/3: Less frequent breast cancer screening does not correlate with higher breast cancer stage at diagnosis
- One-Minute Telegram 104-2024-3/3: Get the mammo? Breast cancer screening preferences among women in their 40s
- One-Minute Telegram 98-2024-1/3: USPSTF update: start breast cancer screening at 40 years of age
- One-Minute Telegram 47-2022-3/3: How many cases of breast cancer are overdiagnosed through screening?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Subscribe to the One-Minute Telegram
- 2024 USPSTF Recommendations on Screening for Breast Cancer
- 2023 ACR Appropriateness Criteria on Breast Implant Evaluation
- 2021 ACR Appropriateness Criteria on Transgender Breast Cancer Screening
- 2019 USPTF Recommendations on Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer
References
- "How Common Is Breast Cancer?". https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html
- Ly D, Forman D, Ferlay J, Brinton LA, Cook MB. "An international comparison of male and female breast cancer incidence rates". International Journal of Cancer. 132(8). :1918-1926. (2012)
- Anders CK, Johnson R, Litton J, Phillips M, Bleyer A. "Breast cancer before age 40 years". Semin Oncol. 36(3). :237-249. (2009)
- Pedro Exman, Harold J. Burstein. "How Old is Too Old? Breast Cancer Treatment in Octogenarians". Annals of Surgical Oncology. (2018)
- Britt K, Short R.. "The plight of nuns: hazards of nulliparity". The Lancet. (2012)
- Christopher I. Li, Kathleen E. Malone, Peggy L. Porter, et al. "Relationship between Menopausal Hormone Therapy and Risk of Ductal, Lobular, and Ductal-Lobular Breast Carcinomas". Cancer Epidemiology, Biomarkers & Prevention. (2008)
- White ND. "Hormonal Contraception and Breast Cancer Risk". American Journal of Lifestyle Medicine. 12(3). :224-226. (2018)
- ACOG. "Hormonal Contraception and Risk of Breast Cancer". ACOG
- Fitzpatrick D, Pirie K, Reeves G, Green J, Beral V. "Combined and progestagen-only hormonal contraceptives and breast cancer risk: A UK nested case–control study and meta-analysis". PLoS Med. 20(3). :e1004188. (2023)
- "How does radiation therapy affect the risk of second cancers?". https://www.cancer.org/treatment/treatments-and-side-effects/physical-side-effects/second-cancers-in-adults/radiation-therapy.html. [2014-12-11]
- "Breast Cancer: Risk Factors and Prevention". https://www.cancer.net/cancer-types/breast-cancer/risk-factors-and-prevention. [2018-10-01]
- "BRCA: The Breast Cancer Gene". https://www.nationalbreastcancer.org/what-is-brca
- Waks AG, Winer EP. "Breast Cancer Treatment". JAMA. 321(3). :288. (2019)
- "Paget Disease of the Breast". https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/types-of-breast-cancer/paget-disease-of-the-nipple.html. [2019-09-20]
- Karakas C. "Paget′s disease of the breast". J Carcinog. 10(1). :31. (2011)
- "Inflammatory Breast Cancer". https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/types-of-breast-cancer/inflammatory-breast-cancer.html. [2019-09-20]
- Wingo PA, Jamison PM, Young JL, Gargiullo P.. "Population-based statistics for women diagnosed with inflammatory breast cancer (United States).". Cancer Causes & Control. (2004)
- Dawood S, Merajver SD, Viens P, et al. "International expert panel on inflammatory breast cancer: consensus statement for standardized diagnosis and treatment". Annals of Oncology. 22(3). :515-523. (2011)
- "Performance and Practice Guidelines for Sentinel Lymph Node Biopsy in Breast Cancer Patients". https://www.breastsurgeons.org/docs/statements/Performance-and-Practice-Guidelines-for-Sentinel-Lymph-Node-Biopsy-in-Breast-Cancer-Patients.pdf. [2014-11-25]
- Brackstone M, Baldassarre FG, Perera FE, et al. "Management of the Axilla in Early-Stage Breast Cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline". J Clin Oncol. :JCO.21.00934. (2021)
- Ofri A, Moore K. "Occult breast cancer: Where are we at?". The Breast. 54. :211-215. (2020)
- Losa F, Soler G, Casado A, et al. "SEOM clinical guideline on unknown primary cancer (2017)". Clin Transl Oncol. 20(1). :89-96. (2017)
- Pleasant V. "Management of breast complaints and high-risk lesions". Best Practice & Research Clinical Obstetrics & Gynaecology. 83. :46-59. (2022)
- Gradishar WJ, Moran MS, Abraham J, et al. "Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology". Journal of the National Comprehensive Cancer Network. 20(6). :691-722. (2022)
- Al Sukhun S, Temin S, Barrios CH, et al. "Systemic Treatment of Patients With Metastatic Breast Cancer: ASCO Resource–Stratified Guideline". JCO Glob Oncol. (2024)
- "Consensus Guideline on the Management of the Axilla in Patients With Invasive/In-Situ Breast Cancer". https://www.breastsurgeons.org/docs/statements/Consensus-Guideline-on-the-Management-of-the-Axilla.pdf?v2. [2019-09-24]
- Lambertini M, Massarotti C, Havas J, et al. "Contraceptive Use in Premenopausal Women With Early Breast Cancer". JAMA Network Open. 5(9). :e2233137. (2022)
- Nguyen AT, Curtis KM, Tepper NK, et al. "U.S. Medical Eligibility Criteria for Contraceptive Use, 2024". MMWR Recomm Rep. 73(4). :1-126. (2024)
- Curtis KM, Jatlaoui TC, Tepper NK, et al. "U.S. Selected Practice Recommendations for Contraceptive Use, 2016". MMWR Morb Mortal Wkly Rep. 65(4). :1-66. (2016)
- Penz E, Watt KN, Hergott CA, Rahman NM, Psallidas I. "Management of malignant pleural effusion: challenges and solutions". Cancer Management and Research. Volume 9. :229-241. (2017)
- Gerber B, Freund M, Reimer T. "Recurrent Breast Cancer". Deutsches Aerzteblatt Online. (2010)
- Lawenda BD, Mondry TE, Johnstone PAS. "Lymphedema: A primer on the identification and management of a chronic condition in oncologic treatment". CA Cancer J Clin. 59(1). :8-24. (2009)
- Giaquinto AN, Sung H, Miller KD, et al. "Breast Cancer Statistics, 2022". CA Cancer J Clin. 72(6). :524-541. (2022)
- "Cancer Stat Facts: Female Breast Cancer Subtypes". https://seer.cancer.gov/statfacts/html/breast-subtypes.html. [2022-01-01]
- Keyser EA, Staat BC, Fausett MB, Shields AD. "Pregnancy-associated breast cancer.". Reviews in obstetrics & gynecology. 5(2). :94-9. (2012)
- Case AS. "Pregnancy-associated Breast Cancer". Clin Obstet Gynecol. 59(4). :779-788. (2016)
- Shachar SS, Gallagher K, McGuire K, et al. "Multidisciplinary Management of Breast Cancer During Pregnancy". Oncologist. 22(3). :324-334. (2017)
- Loibl S, Schmidt A, Gentilini O, et al. "Breast Cancer Diagnosed During Pregnancy". JAMA Oncology. 1(8). :1145. (2015)
- Gougis P, Grandal B, Jochum F, et al. "Treatments During Pregnancy Targeting ERBB2 and Outcomes of Pregnant Individuals and Newborns". JAMA network open. 6(10). :e2339934. (2023)
- Johnson HM, Mitchell KB, Young M, et al. "ABM Clinical Protocol #34: Breast Cancer and Breastfeeding". Breastfeeding Medicine. 15(7). :429-434. (2020)
- Hassett MJ, Somerfield MR, Baker ER, et al. "Management of Male Breast Cancer: ASCO Guideline". J Clin Oncol. 38(16). :1849-1863. (2020)
- Khan NAJ, Tirona M. "An updated review of epidemiology, risk factors, and management of male breast cancer.". Med Oncol. 38(4). :39. (2021)
- Giordano SH. "Breast Cancer in Men". N Engl J Med. 378(24). :2311-2320. (2018)
- Daly MB, Pal T, Berry MP, et al. "Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology". J Natl Compr Canc Netw. 19(1). :77-102. (2021)
- "Invasive Breast Cancer (IDC/ILC)". https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/types-of-breast-cancer/invasive-breast-cancer.html. [2019-09-20]
- "Carcinoma subtypes: Carcinoma with medullary features (CMF)". http://www.pathologyoutlines.com/topic/breastmalignantmedullary.htmlhttp://www.pathologyoutlines.com. [2019-01-25]
- Hortobagyi GN, Edge SB, Giuliano A. "New and Important Changes in the TNM Staging System for Breast Cancer". American Society of Clinical Oncology Educational Book. :457-467. (2018)
- Rakha EA, Reis-Filho JS, Baehner F, et al. "Breast cancer prognostic classification in the molecular era: the role of histological grade". Breast Cancer Res. 12(4). (2010)
- Harris L, Fritsche H, Mennel R, et al. "American Society of Clinical Oncology 2007 Update of Recommendations for the Use of Tumor Markers in Breast Cancer". J Clin Oncol. 25(33). :5287-5312. (2007)
- Khatcheressian JL, Hurley P, Bantug E, et al. "Breast Cancer Follow-Up and Management After Primary Treatment: ASCO Clinical Practice Guideline Update". J Clin Oncol. 31(7). :961-965. (2013)
- Trayes KP, Cokenakes SEH. "Breast Cancer Treatment". Am Fam Physician. 104(2). :171-178. (2021)
- Ruddy KJ, Ganz PA. "Treatment of Nonmetastatic Breast Cancer". JAMA. 321(17). :1716. (2019)
- Allison KH, Hammond MEH, Dowsett M, et al. "Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update". J Clin Oncol. 38(12). :1346-1366. (2020)
- Wolff AC, Somerfield MR, Dowsett M, et al. "Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: ASCO–College of American Pathologists Guideline Update". J Clin Oncol. 41(22). :3867-3872. (2023)
- Li Y, Yang D, Yin X, et al. "Clinicopathological Characteristics and Breast Cancer–Specific Survival of Patients With Single Hormone Receptor–Positive Breast Cancer". JAMA Netw Open. 3(1). :e1918160. (2020)
- Dempsey N, Sandoval A, Mahtani R. "Metastatic HER2-Positive Breast Cancer: Is There an Optimal Sequence of Therapy?". Curr Treat Options Oncol. 24(9). :1120-1137. (2023)
- Shimelis H, LaDuca H, Hu C, et al. "Triple-Negative Breast Cancer Risk Genes Identified by Multigene Hereditary Cancer Panel Testing". J Natl Cancer Inst. 110(8). :855-862. (2018)
- Davis C. Teichgraeber, Mary S. Guirguis, Gary J. Whitman. "Breast Cancer Staging: Updates in the <i>AJCC Cancer Staging Manual</i>, 8th Edition, and Current Challenges for Radiologists, From the <i>AJR</i> Special Series on Cancer Staging". American Journal of Roentgenology. 217(2). :278-290. (2021)
- "ACR Appropriateness Criteria® Imaging of Invasive Breast Cancer". https://web.archive.org/web/20240614133529/https://acsearch.acr.org/docs/3186697/Narrative/. [2023-01-01]
- Ali B, Mubarik F, Zahid N, Sattar AK. "Clinicopathologic Features Predictive of Distant Metastasis in Patients Diagnosed With Invasive Breast Cancer". JCO Global Oncology. :1346-1351. (2020)
- Pesapane F, Downey K, Rotili A, Cassano E, Koh DM. "Imaging diagnosis of metastatic breast cancer". Insights Imaging. 11(1). (2020)
- Roberts CC, Daffner RH, Weissman BN, et al. "ACR Appropriateness Criteria® on Metastatic Bone Disease". J Am Coll Radiol. 7(6). :400-409. (2010)
- Kaur H, Hindman NM, Al-Refaie WB, et al. "ACR Appropriateness Criteria® Suspected Liver Metastases". J Am Coll Radiol. 14(5). :S314-S325. (2017)
- Schnipper LE, Smith TJ, Raghavan D, et al. "American Society of Clinical Oncology Identifies Five Key Opportunities to Improve Care and Reduce Costs: The Top Five List for Oncology". J Clin Oncol. 30(14). :1715-1724. (2012)
- Lee GK, Sheckter CC. "Breast Reconstruction Following Breast Cancer Treatment 2018". JAMA. 320(12). :1277. (2018)
- "Performance and Practice Guidelines for Breast-Conserving Surgery/Partial Mastectomy". https://www.breastsurgeons.org/docs/statements/Performance-and-Practice-Guidelines-for-Breast-Conserving-Surgery-Partial-Mastectomy.pdf. [2015-02-22]
- Expert Panel on Radiation Oncology–Breast, Park C, Sethi R, et al. "Conservative Surgery and Radiation for Stage I and II Breast Cancer". J Am Coll Radiol. (2015)
- "Performance and Practice Guidelines for Mastectomy". https://www.breastsurgeons.org/docs/statements/Performance-and-Practice-Guidelines-for-Mastectomy.pdf. [2014-11-25]
- Jones C, Lancaster R. "Evolution of Operative Technique for Mastectomy". Surg Clin North Am. 98(4). :835-844. (2018)
- American College of Obstetricians-Gynecologists. "Practice Bulletin No 182: Hereditary Breast and Ovarian Cancer Syndrome". Obstetrics & Gynecology. 130(3). :e110-e126. (2017)
- Lim DW, Metcalfe KA, Narod SA. "Bilateral Mastectomy in Women With Unilateral Breast Cancer". JAMA Surg. 156(6). :569. (2021)
- Schrager S, Lyon SM, Poore SO. "Breast Implants: Common Questions and Answers". Am Fam Physician. 104(5). :500-508. (2021)
- Roy N, Downes MH, Ibelli T, et al. "The psychological impacts of post-mastectomy breast reconstruction: a systematic review". Annals of Breast Surgery. 8. :19-19. (2024)
- Hillard C, Fowler JD, Barta R, Cunningham B. "Silicone breast implant rupture: a review". Gland Surg. 6(2). :163-168. (2017)
- Chetlen A, Niell BL, Brown A, et al. "ACR Appropriateness Criteria® Breast Implant Evaluation: 2023 Update". J Am Coll Radiol. 20(11). :S329-S350. (2023)
- Glasberg SB, Sommers CA, McClure GT. "Breast Implant-associated Squamous Cell Carcinoma: Initial Review and Early Recommendations". Plast Reconstr Surg Glob Open.. 11(6). :e5072. (2023)
- Nicholson WK, Silverstein M, et al. "Screening for Breast Cancer". JAMA. (2024)
- Oeffinger KC, Fontham ET, Etzioni R, et al. "Breast Cancer Screening for Women at Average Risk: 2015 Guideline Update From the American Cancer Society". The Journal of the American Medical Association. (2015)
- "Practice bulletin no. 179: Breast cancer screening". https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2017/07/breast-cancer-risk-assessment-and-screening-in-average-risk-women. [2017-07-01]
- Monticciolo DL, Newell MS, Moy L, Lee CS, Destounis SV. "Breast Cancer Screening for Women at Higher-Than-Average Risk: Updated Recommendations From the ACR". J Am Coll Radiol. 20(9). :902-914. (2023)
- Michaels E, Worthington RO, Rusiecki J. "Breast Cancer". Med Clin North Am. 107(2). :271-284. (2023)
- "Practice Parameter for the Performance of Screening and Diagnostic Mammography". https://www.acr.org/-/media/ACR/Files/Practice-Parameters/Screen-Diag-Mammo.pdf. [2023-01-01]
- "ACR Appropriateness Criteria® Female Breast Cancer Screening". https://web.archive.org/web/20240520104012/https://acsearch.acr.org/docs/70910/Narrative/. [2023-01-01]
- Expert Panel on Breast Imaging, Weinstein SP, Slanetz PJ, et al. "ACR Appropriateness Criteria® Supplemental Breast Cancer Screening Based on Breast Density". J Am Coll Radiol. 18(11S). :S456-S473. (2021)
- Monticciolo DL, Newell MS, Moy L, et al. "Breast Cancer Screening in Women at Higher-Than-Average Risk: Recommendations From the ACR". J Am Coll Radiol. 15(3). :408-414. (2018)
- Lambert M. "ACOG Guidelines for Managing Hereditary Breast and Ovarian Cancer Syndrome". Am Fam Physician. 80(12). :1505-1507. (2009)
- Khan M, Chollet A. "Breast Cancer Screening: Common Questions and Answers.". Am Fam Physician. 103(1). :33-41. (2021)
- Owens DK, et al. "Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer". JAMA. 322(7). :652. (2019)
- Gao Y, Perez CA, Chhor C, Heller SL. "Breast Cancer Screening in Survivors of Childhood Cancer". RadioGraphics. 43(4). (2023)
- Runowicz CD, Leach CR, Henry NL, et al. "American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline". CA Cancer J Clin. 66(1). :43-73. (2015)
- "ACR Appropriateness Criteria® Transgender Breast Cancer Screening". https://acsearch.acr.org/docs/3155692/Narrative/. [2021-01-01]
- Sterling J, Garcia MM. "Cancer screening in the transgender population: a review of current guidelines, best practices, and a proposed care model". Transl Androl Urol. 9(6). :2771-2785. (2020)
- "Performance and Practice Guidelines for Axillary Lymph Node Dissection in Breast Cancer Patients". https://www.breastsurgeons.org/docs/statements/Performance-and-Practice-Guidelines-for-Axillary-Lymph-Node-Dissection-in-Breast-Cancer-Patients.pdf. [2014-11-25]
- Shah C, Al-Hilli Z, Vicini F. "Advances in Breast Cancer Radiotherapy: Implications for Current and Future Practice". JCO Oncology Practice. 17(12). :697-706. (2021)
- Recht A, Comen EA, Fine RE, et al. "Postmastectomy Radiotherapy: An American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Focused Guideline Update". J Clin Oncol. 34(36). :4431-4442. (2016)
- Carbine NE, Lostumbo L, Wallace J, Ko H. "Risk-reducing mastectomy for the prevention of primary breast cancer". Cochrane Database Syst Rev. 2019(1). (2018)
- Visvanathan K, Hurley P, Bantug E, et al. "Use of Pharmacologic Interventions for Breast Cancer Risk Reduction: American Society of Clinical Oncology Clinical Practice Guideline". Journal of Clinical Oncology. 31(23). :2942-2962. (2013)
- Visvanathan K, Fabian CJ, Bantug E, et al. "Use of Endocrine Therapy for Breast Cancer Risk Reduction: ASCO Clinical Practice Guideline Update". J Clin Oncol. 37(33). :3152-3165. (2019)
- Owens DK, Davidson KW, et al. "Medication Use to Reduce Risk of Breast Cancer". JAMA. 322(9). :857. (2019)
- Denduluri N, Somerfield MR, Chavez-MacGregor M, et al. "Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer: ASCO Guideline Update". J Clin Oncol. 39(6). :685-693. (2021)
- Nadine M. Tung, Dana Zakalik, Mark R. Somerfield. "Adjuvant PARP Inhibitors in Patients With High-Risk Early-Stage HER2-Negative Breast Cancer and Germline BRCA Mutations: ASCO Hereditary Breast Cancer Guideline Rapid Recommendation Update". Journal of Clinical Oncology. 39(26). :2959-2961. (2021)
- Henry NL, Somerfield MR, Abramson VG, et al. "Role of Patient and Disease Factors in Adjuvant Systemic Therapy Decision Making for Early-Stage, Operable Breast Cancer: Update of the ASCO Endorsement of the Cancer Care Ontario Guideline". J Clin Oncol. 37(22). :1965-1977. (2019)
- Hudis CA. "Trastuzumab — Mechanism of Action and Use in Clinical Practice". N Engl J Med. 357(1). :39-51. (2007)
- Lordick F, Carneiro F, Cascinu S, et al. "Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up". Ann Oncol. 33(10). :1005-1020. (2022)
- Dempsey N, Rosenthal A, Dabas N, et al. "Trastuzumab-induced cardiotoxicity: a review of clinical risk factors, pharmacologic prevention, and cardiotoxicity of other HER2-directed therapies". Breast Cancer Res Treat. 188(1). :21-36. (2021)
- Dobson R, Ghosh AK, Ky B, et al. "BSE and BCOS Guideline for Transthoracic Echocardiographic Assessment of Adult Cancer Patients Receiving Anthracyclines and/or Trastuzumab". JACC CardioOncol. 3(1). :1-16. (2021)
- "Cancer Facts & Figures 2017". https://onlinelibrary.wiley.com/doi/full/10.3322/caac.21387. [2017-01-05]
- Stevens KN, Vachon CM, Couch FJ.. "Genetic susceptibility to triple-negative breast cancer.". Cancer Research. (2013)
- Ganesh N. Sharma, Rahul Dave, Jyotsana Sanadya, Piush Sharma, and K. K Sharma. "VARIOUS TYPES AND MANAGEMENT OF BREAST CANCER: AN OVERVIEW". Journal of Advanced Pharmaceutical Technology & Research. (2010)
- Hannah Y Wen, MD, PhD and Edi Brogi, MD, PhD. "Lobular Carcinoma in Situ". Surgical Pathology Clinics. (2019)
- Harris EE, Schultz D, Bertsch H, et al. "Ten-year outcome after combined modality therapy for inflammatory breast cancer.". International Journal of Radiation Oncology, Biology, Physics. (2003)
- Huang SF, Chang RF, Chen DR, Moon WK.. "Characterization of spiculation on ultrasound lesions.". IEEE Transactions on Medical Imaging. (2004)
- Łukasiewicz E, Ziemiecka A, Jakubowski W, et al. "Fine-needle versus core-needle biopsy – which one to choose in preoperative assessment of focal lesions in the breasts? Literature review". J Ultrason. (2017)
- "Biopsy". https://www.cancerquest.org/patients/detection-and-diagnosis/biopsy
- Adam M.Brufsky. "Long-term management of patients with hormone receptor-positive metastatic breast cancer: Concepts for sequential and combination endocrine-based therapies". Cancer Treatment Reviews. (2017)
- Franco Lumachi, Davide A Santeufemia, and Stefano MM Basso. "Current medical treatment of estrogen receptor-positive breast cancer". World Journal of Biological Chemistry. (2015)
- Beth N. Peshkin, MS, CGC, et al. "BRCA1/2 mutations and triple negative breast cancers.". Breast Disease. (2010)
- Ariel Toomey; Jacqueline K. Le.. "Abscess, Breast". StatPearls. (2019)
- "Intraductal papilloma of breast". https://radiopaedia.org/articles/intraductal-papilloma-of-breast. [2019-03-12]
- Julie Margenthaler. "Technique of axillary lymph node dissection". UpToDate. UpToDate. https://www.uptodate.com/contents/technique-of-axillary-lymph-node-dissection. [2019-02-13]
- Robertson JF, Blamey RW.. "The use of gonadotrophin-releasing hormone (GnRH) agonists in early and advanced breast cancer in pre- and perimenopausal women.". European Journal of Cancer. (2003)
- Irene E. G. van Hellemond, MD, Sandra M. E. Geurts, et al. "Current Status of Extended Adjuvant Endocrine Therapy in Early Stage Breast Cancer". Current Treatment Options in Oncology. (2018)
- Ammar Taha Abdullah Abdulaziz, MD, Xiao Qing Yu, et al. "Paraneoplastic cerebellar degeneration associated with cerebellar hypermetabolism". Medicine. (2018)
- Elizabeth A. Brett, Matthias M. Aitzetmüller, Matthias A. Sauter, et al. "Breast cancer recurrence after reconstruction: know thine enemy". Oncotarget. (2018)
- Philippe Rouanet, Pascal Roger, Emilie Rousseau, et al. "HER2 overexpression a major risk factor for recurrence in pT1a-bN0M0 breast cancer: results from a French regional cohort". Cancer Medicine. (2014)
- "Statistics on breast cancer survival rates by stage". https://www.medicalnewstoday.com/articles/316867.php#5-year-survival-rates. [2019-08-19]
- Fisher B, Anderson S, Bryant J, et al. "Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer.". The New England Journal of Medicine. (2002)
- "What is the role of tamoxifen and raloxifene for the reduction of breast cancer risk?". https://www.medscape.com/answers/1947145-155372/what-is-the-role-of-tamoxifen-and-raloxifene-for-the-reduction-of-breast-cancer-risk. [2019-05-21]
- "Raloxifene". https://www.drugbank.ca/drugs/DB00481. [2019-09-17]
- Hitisha K., Patel Teeru Bihani. "Selective estrogen receptor modulators (SERMs) and selective estrogen receptor degraders (SERDs) in cancer treatment". Pharmacology & Therapeutics. (2018)
- American College of Obstetricians-Gynecologists. "Practice bulletin no. 122: Breast cancer screening". Obstetrics & Gynecology. (2011)
- Siu AL; U.S. Preventive Services Task Force. "Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement.". Annals of Internal Medicine. (2016)
- Michael S Sabel, MD, Laura C Collins, MD. "Atypia and lobular carcinoma in situ: High-risk lesions of the breast". UpToDate. UpToDate. https://www.uptodate.com/contents/atypia-and-lobular-carcinoma-in-situ-high-risk-lesions-of-the-breast. [2017-11-29]