Summary
Bronchiectasis is an irreversible and abnormal dilation in the bronchial tree caused by cycles of bronchial inflammation leading to mucous plugging and progressive airway destruction. Bronchiectasis is classified according to etiology as either cystic fibrosis (CF) bronchiectasis or non-CF bronchiectasis (e.g., secondary to severe or protracted pneumonia, immunodeficiency, or COPD). The characteristic clinical feature is a chronic cough with copious mucopurulent sputum. Other symptoms may include dyspnea, rhinosinusitis, and hemoptysis. Physical examination reveals crackles and rhonchi on auscultation, often accompanied by wheezing. High-resolution computed tomography confirms the diagnosis and usually shows thickened bronchial walls, with so-called “signet-ring” and “tram track” signs. Patients can periodically experience an acute worsening of symptoms, referred to as an acute exacerbation of bronchiectasis, which commonly requires antibiotic treatment. The goal of long-term management of bronchiectasis is to control symptoms and prevent exacerbations, and includes pulmonary physiotherapy and pharmacological therapy. Massive hemoptysis is a rare complication of bronchiectasis and requires surgery or pulmonary artery embolization.
Definitions
- Bronchiectasis: an irreversible and abnormal dilation of the bronchial tree that produces chronic respiratory symptoms (e.g., chronic productive cough)
- Acute exacerbation of bronchiectasis: a deterioration in the symptoms of bronchiectasis that requires a change in the regular treatment (e.g., adding antibiotics, increasing airway clearance techniques) [1]
Etiology
Bronchiectasis requires the combination of two important processes taking place in the bronchi: either local infection or inflammation along with either inadequate clearance of secretions, airway obstruction, or impaired host defenses. These processes result in the permanent dilation of airways.
- Pulmonary infections (i.e., bacterial, viral, fungal), especially severe or chronic infections
-
Disorders of secretion clearance or mucous plugging
- Cystic fibrosis (CF) [2]
- Primary ciliary dyskinesia (PCD)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Smoking: associated with poor ciliary motility
-
Bronchial narrowing or other forms of obstruction
- COPD
- Aspiration
- Tumors
- α1-antitrypsin deficiency
- Other congenital and acquired conditions (e.g., congenital bronchiectasis, tracheomalacia, bronchogenic cyst)
- Immunodeficiency (e.g., common variable immunodeficiency, hypogammaglobulinemia, HIV)
- Chronic inflammatory diseases (e.g., rheumatoid arthritis, Sjogren syndrome, Crohn disease)
Primary prevention of bronchiectasis includes antibiotic control of bronchial and pulmonary infections in predisposed individuals.


References:[2][3][4]
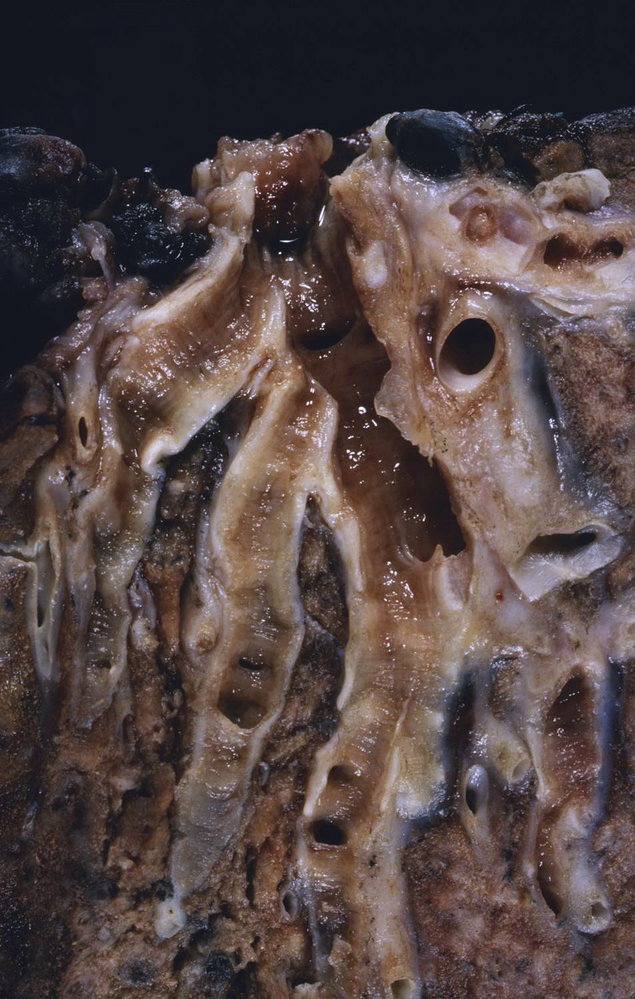
Photograph of a section of a lung specimen
The bronchi have been opened along their longitudinal axis. The bronchi in the center of the image (green overlay) appear broadened, reflecting an enlarged diameter (bronchiectasis), and show a brownish-red mucosal discoloration, indicating chronic inflammation. Note the more narrow difference and gray color of mucosa in the normal bronchi seen in the left periphery of the image (red overlay).
Source: “Bronchiectasis” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.

Photograph of a longitudinally sectioned right lung (sagittal view)
Markedly distended peripheral bronchi, especially in the lower lobe.
This is the typical gross appearance of bronchiectasis.
Source: “Bronchiectasis” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0.
Clinical features
- Chronic productive cough (lasting months to years) with copious mucopurulent sputum ;
-
Auscultation
- Crackles and rhonchi
- Wheezing (due to obstruction from secretions, airway collapsibility, or a concomitant condition)
- Bronchophony
- Rhinosinusitis
- Dyspnea
- Hemoptysis: usually mild or self-limiting, but severe hemorrhage that requires embolization may occur
- Nonspecific symptoms (i.e., fatigue, weight loss, pallor due to anemia)
- Clubbing of nails (uncommon)
-
Exacerbations of bronchiectasis
- Recurrent bouts of pneumonia and acute bacterial infection of sections of dilated bronchi
- Frequently due to Pseudomonas aeruginosa [5]
- Features
- Increased production of mucous above baseline
- Low-grade fever
Bronchiectasis should be suspected in patients with a chronic cough that produces large amounts of sputum.
References: [4][6]
Diagnosis
Approach [7]
- Confirm the diagnosis with imaging studies in patients with features suggestive of bronchiectasis.
- Poor control or frequent exacerbations in patients with chronic pulmonary disease (e.g., COPD, asthma)
- Chronic cough or recurrent pulmonary infections in patients with immunosuppression or conditions associated with bronchiectasis
- Productive cough lasting > 8 weeks in otherwise healthy patients
- Identify the underlying etiology.
- Routine laboratory studies, sputum culture and smear, and pulmonary function tests
- Clinical suspicion for a specific etiology: Obtain additional studies based on individual evaluation.
In patients with suspected bronchiectasis, diagnosis is confirmed using imaging studies, preferably a HRCT scan. Additional diagnostic studies are useful to identify the underlying cause and possibly provide specific treatment.
Imaging [7][8][9]
-
Imaging modalities
- X-ray chest: best initial test (may not show mild disease)
- High-resolution computed tomography; (HRCT) chest: confirmatory test
-
Findings
-
Bronchial dilation ; [7][8]
- Cylindrical or tubular (most common) : parallel tram track sign and signet ring sign
- Varicose
- Saccular or cystic (most severe form)
- Thickened bronchial walls; , mucus plugging, honeycombing (suggests late-stage bronchiectasis)
- Specific findings suggestive of the underlying etiology
- Focal distribution : localized disease (e.g., tumors, foreign bodies, strictures)
- Diffuse distribution: fibrosing diffuse lung diseases
- Lower lung predominance (e.g., recurrent aspiration, pulmonary fibrosis, α1-antitrypsin deficiency)
- Upper or middle lung predominance (e.g., CF, sarcoidosis, ABPA, tuberculosis)
- Perihilar lymphadenopathies (e.g., sarcoidosis, tuberculosis)
- Situs inversus (seen in primary ciliary dyskinesia)
-
Bronchial dilation ; [7][8]



Identification of the underlying etiology
Studies to determine the underlying etiology of bronchiectasis are usually requested by a specialist. In many cases, it is not possible to reach a specific diagnosis and the disease may be classified as idiopathic. [10]
Initial workup [7][11]
Perform at the time of diagnosis to obtain baseline references. Sputum culture and smear, as well as spirometry, are also used for monitoring.
-
Laboratory studies [7][11]
-
CBC: Findings are variable and depend on the underlying etiology.
- ↓ Hb
- Variable leukocyte levels
- ↑ Thrombocytes
- Consider ABG (e.g., in patients with ↓ SaO2 on room air): may show hypercapnia
- Quantitative measurement of serum immunoglobulins and electrophoresis (IgA, IgG, IgM, and IgG subclasses): to exclude immunodeficiencies [11]
- Aspergillus fumigatus IgG and IgE: to exclude ABPA
- Serum AAT level: to evaluate for AAT deficiency [12]
-
CBC: Findings are variable and depend on the underlying etiology.
-
Sputum culture and smear: culture induced sputum or bronchoalveolar lavage for all of the following pathogens to detect infection or colonization [7][13]
- Bacterial cultures: e.g., H. influenzae or P. aeruginosa
- Fungal cultures: Candida spp. or Aspergillus spp.
- Mycobacterial culture (with AFB smear microscopy): tuberculosis or nontuberculous mycobacteria
-
Spirometry: not needed to establish a diagnosis but useful to monitor disease progression [7][14]
- Mixed obstructive/restrictive pattern
- Restrictive pattern (i.e., ↓ FEV1 and FVC with normal or ↑ FEV1/FVC ratio)
- Obstructive pattern (i.e., ↓ FEV1/FVC ratio)
Additional diagnostics [7][11]
These studies may be considered depending on clinical suspicion if the initial workup was not diagnostic.
-
Laboratory studies
- Specific antibodies (e.g., rheumatoid factor, ANAs, anti-CCP antibodies, ANCAs): suspected connective tissue or autoimmune diseases
- Sweat chloride test and/or genetic testing for CFTR mutations: suspected CF
- HIV testing , serum α1-antitrypsin levels , nasal nitric oxide testing for primary ciliary dyskinesia
-
Further studies
-
Bronchoscopy
- Indicated to visualize tumors, foreign bodies, or other lesions (most useful in patients with localized disease)
- May also be used in combination with bronchoalveolar lavage (BAL) to obtain specimens for staining and culture
- Upper GI studies (e.g., upper endoscopy, barium swallow, esophageal manometry): consider for suspected gastroesophageal reflux disease or recurrent pulmonary aspiration
- Colonoscopy with biopsies: if associated inflammatory bowel disease is suspected (e.g., GI bleeding)
-
Bronchoscopy
If the initial workup does not identify the underlying cause, perform further studies guided by the patient's clinical features and consider referral to a specialist.
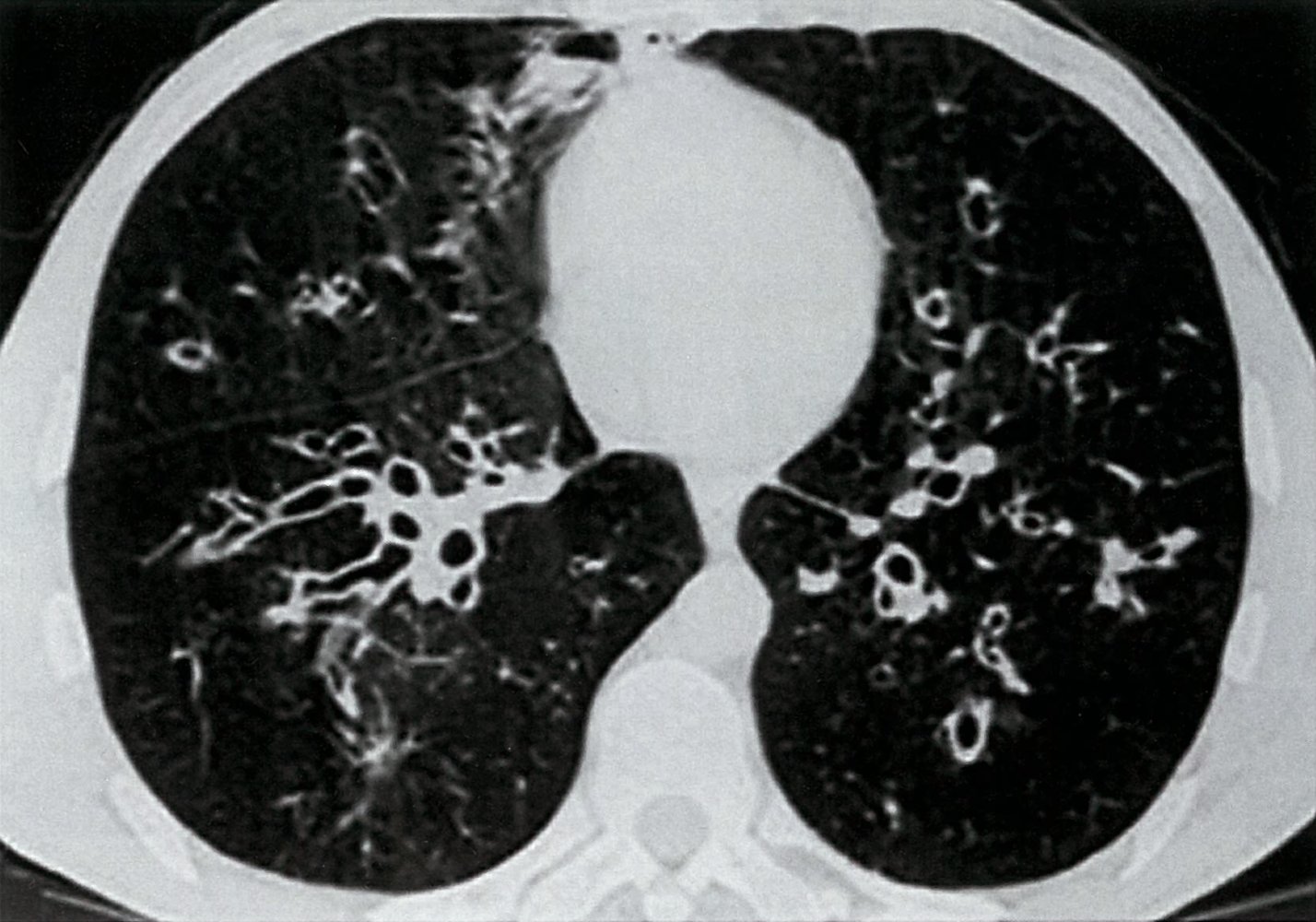
CT chest (axial section)
Numerous bilateral dilated bronchi (bronchiectasis) show wall thickening and an increased bronchoarterial ratio. Several bronchi imaged in cross-section have a diameter greater than the accompanying pulmonary artery diameter (1; signet ring sign), while others imaged in long axis have parallel walls (2; tram track sign).
Source: © IMPP

X-ray chest (PA view; right lung) and CT (coronal plane; lung window; right lung) of a patient with bronchiectasis
The right lung is diffusely abnormal. Numerous parallel lines (tram track sign; examples indicated by arrows and green lines) representing thickened bronchial walls demarcate lucent air within dilated bronchi. Some thick-walled bronchi are alternatively imaged in cross-section and are visible as circles with lucent centers (examples indicated by red overlay).
Source: “Chest imaging using signs, symbols, and naturalistic images: a practical guide for radiologists and non-radiologists” by Alessandra Chiarenza, Luca Esposto Ultimo, Daniele Falsaperla, Mario Travali, Pietro Valerio Foti, Sebastiano Emanuele Torrisi, Matteo Schisano, Letizia Antonella Mauro, Gianluca Sambataro, Antonio Basile, Carlo Vancheri & Stefano Palmucci, Insights Imaging, licensed under CC BY 4.0. Modifications: image cropped, letter removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
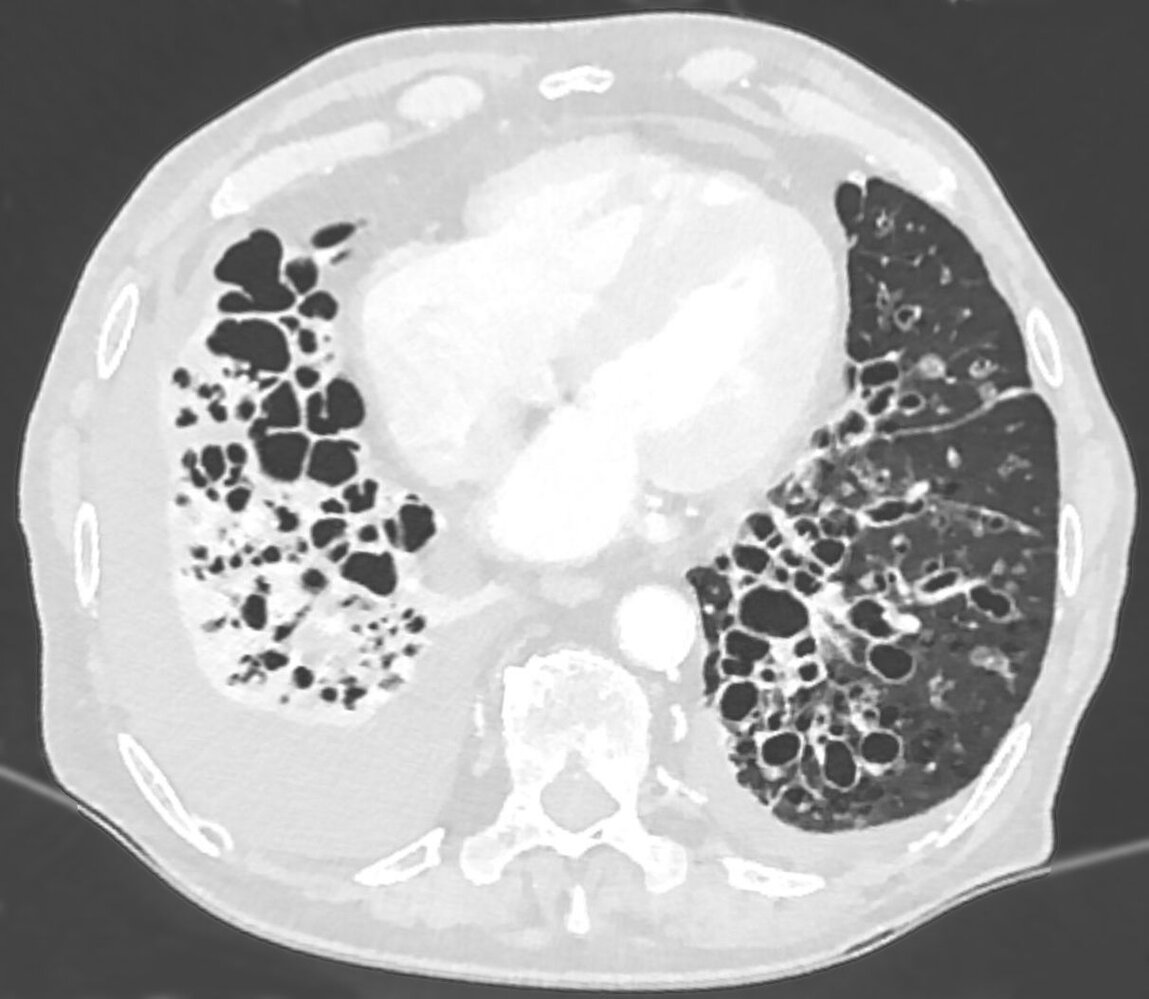
CT chest (axial plane; lung window)
Multiple dilated bronchi in the lower lobes and lingula are accompanied by inflammatory wall thickening. Many bronchi are larger than the adjacent pulmonary arteries (signet ring sign; examples indicated by red arrowheads), in contrast to the normal appearance of approximately equal size. Additional abnormalities include right lower lobe consolidation with volume loss and bilateral pleural effusions.
The severe form of bronchiectasis seen here is termed cystic bronchiectasis.
Source: “Massive Bronchiektasen - CT LF axial 001.jpg” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Management
This section focuses on the management of non-CF bronchiectasis. See “Cystic fibrosis” for specific recommendations regarding that condition.
Management of acute exacerbations
Approach [7][11][15]
- Provide supportive treatment and oxygen therapy as needed.
- Optimize mucoactive agents (see “Pharmacotherapy for airway clearance in bronchiectasis”).
- Optimize airway clearance techniques.
- Obtain a new sputum culture and start empiric antibiotic therapy, based on the most recent sputum culture.
- Tailor antibiotics to the most recent sputum culture once available and preferably complete 14 days of therapy.
Monitoring and disposition [7][11]
- Outpatient treatment: for hemodynamically stable patients with mild to moderate symptoms
- Consider inpatient treatment in the following cases:
- Clinical deterioration or no clinical improvement following completion of an oral antibiotic regimen (e.g., lasting 10–14 days)
- Sepsis or severe pneumonia (see “Pneumonia treatment” and “Acute management checklist for sepsis” for more information)
- Hemoptysis ≥ 10 mL in 24 hours and clinical deterioration
- New isolation of P. aeruginosa
| Common empiric antibiotic regimens for bronchiectasis exacerbations [7][11] | ||
|---|---|---|
| Outpatient treatment [7][15] |
|
|
| Inpatient treatment [7][15] |
|
|
Acute exacerbations are defined as acute deterioration or worsening local symptoms and/or additional systemic symptoms such as fever or malaise. Exacerbations are associated with increased inflammation and progressive damage to the lungs. [11]
Long-term management
Management goals are to stop or delay disease progression, reduce exacerbation frequency (goal ≤ 2 per year), achieve symptom control, and improve the patient's quality of life.
Approach [7][11]
-
General measures
- Educate the patient regarding prognosis and the use of long-term medications.
- Promote lifestyle changes like regular exercise and smoking cessation.
- Educate the patient on airway clearance techniques. [7][11][16]
- Bronchopulmonary hygiene and chest physiotherapy: e.g., cupping and clapping, postural drainage, directed cough, hydration
- Pulmonary rehabilitation: may improve exercise capacity and respiratory symptoms [10]
- Administer vaccinations (i.e., seasonal influenza vaccine, pneumococcal vaccine).
- Consider treatment with mucoactive agents, bronchodilators, or corticosteroids if airway clearance is difficult.
- Provide specific treatment for the underlying cause if identified.
-
Follow-up: Perform follow-ups every 6–12 months to identify disease progression.
- Bacterial and fungal sputum culture: every 6–12 months
- Spirometry: every 12 months
-
Disease progression
- Consider long-term antibiotic therapy for bronchiectasis with ≥ 3 exacerbations per year.
- Repeat diagnostic studies to assess disease progression.
- Screen for complications.
- ECG
- Consider echocardiogram.
- Consider CT chest with contrast.
-
Advanced disease
- Ensure respiratory support as needed.
- Long-term oxygen therapy for chronic respiratory failure (indications are the same as for COPD)
- Consider oxygen with humidification for patients with respiratory failure with hypercapnia.
- Invasive procedures: not routinely indicated
- Ensure respiratory support as needed.
Perform a careful reassessment of patients who are progressively deteriorating (i.e., patients with increased frequency and/or severity of exacerbations, frequent hospital admissions, worsening symptoms, rapid decline in lung function). Identify the cause of bronchiectasis if still unknown, and exclude any comorbidities or exacerbating conditions such as new pathogen colonization.
For patients with bronchiectasis and chronic productive cough or difficulty expectorating, consider referral to a trained respiratory physiotherapist for airway clearance techniques. [16]
Pharmacotherapy for airway clearance in bronchiectasis
Mucoactive agents
Consider in patients with difficulty expectorating or persistent symptoms despite adequate airway clearance techniques; continue use based on clinical benefits. There is a paucity of evidence for the benefit of mucoactive agents in bronchiectasis. [7][17]
-
Nebulized mucoactive agents: Trial for at least 3 months. [11]
- Hypertonic saline (3–7% NaCl) [7][18][19]
- Mannitol [20]
- Oral mucolytics: Trial for at least 6 months, e.g., N-acetylcysteine .
Bronchodilators
Consider on a case-by-case basis. Evidence to support the use of bronchodilators in bronchiectasis is limited. [7][11]
- Short-term bronchodilators (e.g., SABA): in patients with airway reactivity and bronchospasm or prior to inhaled mucoactive treatment [16]
- Long-term bronchodilators (e.g., LABA, LAMA): may be used in patients with severe dyspnea
- Regular use of bronchodilators (e.g., for asthma or COPD): Continue as usual.
Corticosteroids
Corticosteroids are not routinely recommended because of the limited benefit and side effects of corticosteroid therapy. [7][21]
- Inhaled corticosteroids: Continue if already indicated for asthma or COPD.
- Systemic corticosteroids: indicated in patients with ABPA [10]
For patients receiving multiple inhaled treatments and chest physiotherapy, consider the following order of treatment to avoid bronchospasm: bronchodilators, mucoactive agents, respiratory physiotherapy, inhaled antibiotics. [11]
Avoid treatment with recombinant human DNase (e.g., dornase alfa), as it can increase the frequency of exacerbations in patients with non-CF bronchiectasis. [7][22]
Long-term antibiotic therapy [7][11][15]
The goal is to suppress bacterial growth and to reduce symptoms and exacerbations as a measure of secondary prevention in patients with ≥ 3 exacerbations per year. Antibiotic therapy should be administered for at least 3 months and may be extended based on clinical response and tolerability.
Before starting treatment, obtain new sputum cultures with antibiotic sensitivity testing and consult an infectious diseases specialist.
| Long-term antibiotic therapy for bronchiectasis | ||
|---|---|---|
| No colonization with P. aeruginosa |
|
|
| Colonization with P. aeruginosa [7][11] |
|
|
| Isolation of other pathogens |
|
|
Chronic macrolide use can increase the growth of macrolide-resistant mycobacterial strains. It is recommended to rule out active nontuberculous mycobacterial infection with a negative culture before starting treatment.
Long-term macrolides can lead to QT-prolongation and fatal arrhythmias. Before starting treatment, perform an ECG and review whether any medications the patient is taking are known to alter the QT interval. [7][10]
Invasive procedures [7]
- Surgical resection of bronchiectatic lung or lobectomy: indicated in pulmonary hemorrhage, inviable bronchus, and poor control of symptoms despite optimal medical therapy in unilateral bronchiectasis with well-localized disease
- Pulmonary artery embolization: indicated in pulmonary hemorrhage
- Lung transplantation: Consider for severe disease or rapid disease progression.
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
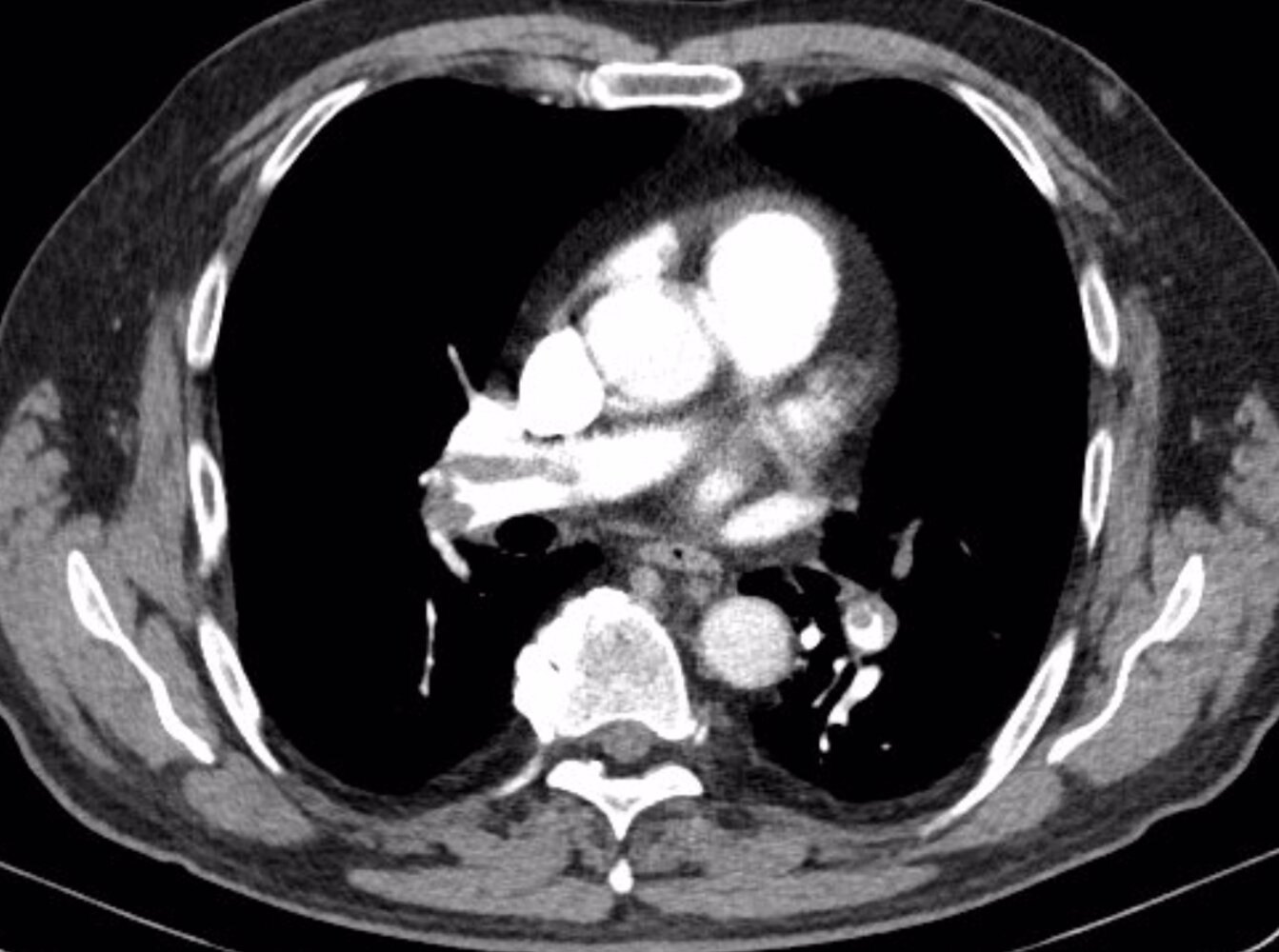
CT chest (with contrast; axial plane, lung window; axial plane, mediastinal window; coronal plane, mediastinal window) of a patient with shortness of breath, post-circulatory collapse, elevated D-dimer (5,086 ug/L; normal < 5), and normal C-reactive protein (CRP; < 3.0 mg/L)
Multiple intraluminal filling defects in the right and left pulmonary arteries and their lobar, segmental, and subsegmental branches represent pulmonary emboli of different age. The acute emboli are seen as central filling defects, whereas the older emboli are eccentric and show irregular thickening of the arterial wall.
Right ventricular and atrial enlargement, septal flattening, and contrast reflux into the hepatic veins are evidence of right ventricular strain. The causes of ground glass opacification in the left upper lobe and misty mesentery with nodes in the upper abdomen are not readily evident. Incidental findings include a hypodense cyst within a small, irregular left kidney and slight deformity of the right sixth rib from a previous fracture.
Our great thanks to Nándor Faluhelyi (University of Pécs, Medical School) for kindly providing this image.
Complications
- Recurrent bronchopulmonary infections → chronic obstructive pulmonary disease → respiratory failure and cor pulmonale
- Pulmonary hemorrhage (massive hemoptysis)
- Lung abscess
References: [6]
We list the most important complications. The selection is not exhaustive.
External Resources
References
- Magis-Escurra C, Reijers MH. "Bronchiectasis". BMJ clinical evidence. 2015. (2015)
- Gao Y, Guan W, Liu S, et al. "Aetiology of bronchiectasis in adults: A systematic literature review". Respirology. 21(8). :1376-1383. (2016)
- Chang AB, Bush A, Grimwood K. "Bronchiectasis in children: diagnosis and treatment". The Lancet. 392(10150). :866-879. (2018)
- Gao Y, Guan W, Zhu Y, Chen R, Zhang G. "Antibiotic-resistant Pseudomonas aeruginosa infection in patients with bronchiectasis: prevalence, risk factors and prognostic implications". International Journal of Chronic Obstructive Pulmonary Disease. Volume 13. :237-246. (2018)
- Kasper DL, Fauci AS, Hauser S, et al. "Harrisons Principles of Internal Medicine ". McGraw-Hill Medical Publishing Division. 19. (2016). ISBN: 9780071802154
- T Hill A, L Sullivan A, D Chalmers J, et al. "British Thoracic Society Guideline for bronchiectasis in adults". Thorax. 74(Suppl 1). :1-69. (2018)
- Neves PC, Guerra M, Ponce P, Miranda J, Vouga L. "Non-cystic fibrosis bronchiectasis". Interact Cardiovasc Thorac Surg. 13(6). :619-625. (2011)
- Milliron B, Henry TS, Veeraraghavan S, Little BP. "Bronchiectasis: Mechanisms and Imaging Clues of Associated Common and Uncommon Diseases". Radiographics. 35(4). :1011-1030. (2015)
- McShane PJ, Naureckas ET, Tino G, Strek ME. "Non–Cystic Fibrosis Bronchiectasis". Am J Respir Crit Care Med. 188(6). :647-656. (2013)
- Polverino E, Goeminne PC, McDonnell MJ, et al. "European Respiratory Society guidelines for the management of adult bronchiectasis". Eur Respir J. 50(3). :1700629. (2017)
- Pavel Strnad, Noel G. McElvaney, David A. Lomas. "Alpha1-Antitrypsin Deficiency". N Engl J Med. 382(15). :1443-1455. (2020)
- Máiz L, Nieto R, Cantón R, Gómez G. de la Pedrosa E, Martinez-García M. "Fungi in Bronchiectasis: A Concise Review". International Journal of Molecular Sciences. 19(1). :142. (2018)
- Maguire G. "Bronchiectasis - a guide for primary care". Aust Fam Physician. 41(11). :842-50. (2012)
- Hill AT, Haworth CS, Aliberti S, et al. "Pulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical research". European Respiratory Journal. 49(6). :1700051. (2017)
- Pasteur MC, Bilton D, Hill AT. "British Thoracic Society guideline for non-CFbronchiectasis". Thorax. 65(Suppl 1). :i1-i58. (2010)
- Hill AT, Barker AF, Bolser DC, et al. "Treating Cough Due to Non-CF and CF Bronchiectasis With Nonpharmacological Airway Clearance". Chest. 153(4). :986-993. (2018)
- Tarrant BJ, Le Maitre C, Romero L, et al. "Mucoactive agents for chronic, non-cystic fibrosis lung disease: A systematic review and meta-analysis". Respirology. 22(6). :1084-1092. (2017)
- Kellett F, Robert NM. "Nebulised 7% hypertonic saline improves lung function and quality of life in bronchiectasis". Respir Med. 105(12). :1831-1835. (2011)
- Nicolson CHH, Stirling RG, Borg BM, et al. "The long term effect of inhaled hypertonic saline 6% in non-cystic fibrosis bronchiectasis". Respir Med. 106(5). :661-667. (2012)
- Bilton D, Tino G, Barker AF, et al. "Inhaled mannitol for non-cystic fibrosis bronchiectasis: a randomised, controlled trial". Thorax. 69(12). :1073-1079. (2014)
- Chalmers JD, Restrepo MI. "Bronchiectasis Management". Chest. 152(6). :1097-1099. (2017)
- O’Donnell AE, Barker AF, Ilowite JS, Fick RB. "Treatment of Idiopathic Bronchiectasis With Aerosolized Recombinant Human DNase I". Chest. 113(5). :1329-1334. (1998)
- Wong C, Jayaram L, Karalus N, et al. "Azithromycin for prevention of exacerbations in non-cystic fibrosis bronchiectasis (EMBRACE): a randomised, double-blind, placebo-controlled trial". The Lancet. 380(9842). :660-667. (2012)
- Altenburg J, de Graaff CS, Stienstra Y, et al. "Effect of Azithromycin Maintenance Treatment on Infectious Exacerbations Among Patients With Non–Cystic Fibrosis Bronchiectasis". JAMA. 309(12). :1251. (2013)
- Daley CL, Iaccarino JM, Lange C, et al. "Treatment of Nontuberculous Mycobacterial Pulmonary Disease: An Official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline". Clin. Infect. Dis. 71(4). :e1-e36. (2020)