Summary
Burns can be caused by heat, chemicals, electricity, friction, and radiation. Injury severity is determined by the depth and extent of the burn. Burn depth is classified as first degree (superficial), second degree (superficial partial thickness or deep partial thickness), third degree (full thickness), or fourth degree (deep injury). Burn extent is classified by the percentage of the body surface area involved, known as the total body surface area (TBSA), typically using the rule of nines or the Lund-Browder chart. Major burns often cause extensive tissue necrosis and severe systemic inflammatory reactions. Early treatment for major burns includes airway management, supplemental oxygen, and large volumes of IV fluid; IV fluid resuscitation is initiated using a protocol but guided by clinical response, e.g., urine output and blood pressure. Inhalation injuries and acute compartment syndrome can complicate burn management, e.g., escharotomy may be required. Serial arterial blood gas, electrolyte, CBC, and creatinine studies are essential in the management of major burns; frequent assessment of peripheral perfusion is required in circumferential limb burns. All burns are initially managed with pain management, topical ointments, and nonadherent dressings, and major burns often require further management such as debridement of necrotic tissue followed by interventions such as skin grafting or flap reconstruction. Burn wounds are susceptible to infection, which increases mortality rates. Shock, sepsis, and respiratory failure are among the most common causes of death after a burn injury.
Etiology
Thermal burns [1]
- Most common type of burn
- Flame burns: fire
- Contact burns: hot surfaces
- Scalding: hot liquids or steam
Nonthermal burns [2]
-
Chemical burns
- Acids such as sulfuric acid (e.g., in lead acid batteries), nitric acid (e.g., explosives and polymer industry), hydrofluoric acid (e.g., in cleaning products for electronics), phenol, and acetic acid
- Alkalis such as anhydrous ammonia (e.g., in fertilizers), calcium oxide (e.g., in cement), sodium hydroxide, and potassium hydroxide
- Miscellaneous: white phosphorus (e.g., in fireworks), metals (e.g., sodium, potassium, lithium), bleaching agents (e.g., hydrogen peroxide, hypochlorite), vesicants (e.g., mustard gas), hydrocarbons (e.g., gasoline, diesel fuel)
-
Electrical burns
- Low-voltage sources: electrical cords, outlets in households
- High-voltage sources: power lines, lightning
-
Radiation burns
- Electromagnetic waves
- UV radiation (e.g., from sunlight, phototherapy)
- X-rays, gamma rays (e.g., from radiotherapy, radiodiagnostic procedures, nuclear accidents)
- Infrared waves (e.g., from warming lamps), microwaves
- High-energy particles (e.g., from radiotherapy, nuclear accidents): alpha particles, beta particles, high-energy neutrons
- Electromagnetic waves
- Friction burns: skin injury caused by abrasion against a hard surface (esp. at high speeds) and the heat generated by the resulting friction (e.g., from skidding across the street due to a motorcycle accident)
Although most burn injuries are unintentional, intentional injury must always be suspected in vulnerable populations, such as children and older adults.
Classification
Burn severity [3]
- Burn severity is primarily based on the depth of burn and extent of burn.
- Additional factors that determine severity include:
- Burn location, e.g., face, hands, across joints
- Concurrent injuries
- Patient age
- Comorbid diseases or conditions
- Small burns can have severe consequences; consult a burn specialist for second- to fourth-degree burns.
Depth of burn [4]
Burn depth is determined by the skin layers involved.
| Overview of burn depth | ||||||
|---|---|---|---|---|---|---|
| Degree of burns | Affected tissue layers | Clinical features | Prognosis | |||
| Pain | Wound blanching on pressure | Appearance | ||||
| 1st-degree burn (superficial burn) |
|
|
|
|
|
|
| 2nd-degree burn (partial thickness burn) | 2a (superficial partial thickness burn) |
|
|
|
|
|
| 2b (deep partial thickness burn) |
|
|
|
|
|
|
| 3rd-degree burn (full thickness burn) |
|
|
|
|
|
|
| 4th-degree burn (deeper injury burn) |
|
|
|
|||
In deep partial-thickness burns, pain may be absent due to damage to sensory nerve endings.
Reassess burn depth periodically, as it can increase after initiating resuscitation.

")
")
")
")

")


")
")
Extent of burn [3]
The percentage of total body surface area (TBSA) injured is used to quantify the extent of burn injury relative to the entire skin surface.
First-degree burns are not included when calculating TBSA.
Rule of nines
- A clinical tool used to rapidly assess the TBSA affected by burns in adults
- The adult body is divided into regions, each comprising ∼ 9% of the body surface area: head/neck, two regions on the anterior trunk, two regions on the posterior trunk, each arm, and two regions on each leg. The genital/perineal region accounts for 1%.
-
The rule of nines does not accurately account for proportions in children.
- Children's heads are up to 20% proportionally larger than adults.
- Children's legs are up to 13% proportionally smaller than adults.
Lund-Browder chart
- A standardized table used to estimate TBSA affected by burns by age group
- Most accurate method for assessing burn extent
| Body surface area estimation with Lund-Browder chart | |||
|---|---|---|---|
| Region | Adult | Child | Infant |
| Head | 7% | 9–17% | 19% |
| Trunk | 26% (13% anterior, 13% posterior) | ||
| Arms and hands | 19% (9.5% each side) | ||
| Thighs | 19% (9.5% each side) | 13–18% (6.5–9% each side) | 11% |
| Lower legs and feet | 21% (10.5% each side) | 17–20% (8.5–10% each side) | 17% |
| Genital | 1% | ||
Palmar method
- A method of calculating TBSA using the patient's palm, which is equivalent to ∼ 1% of their body surface area
- Least accurate method


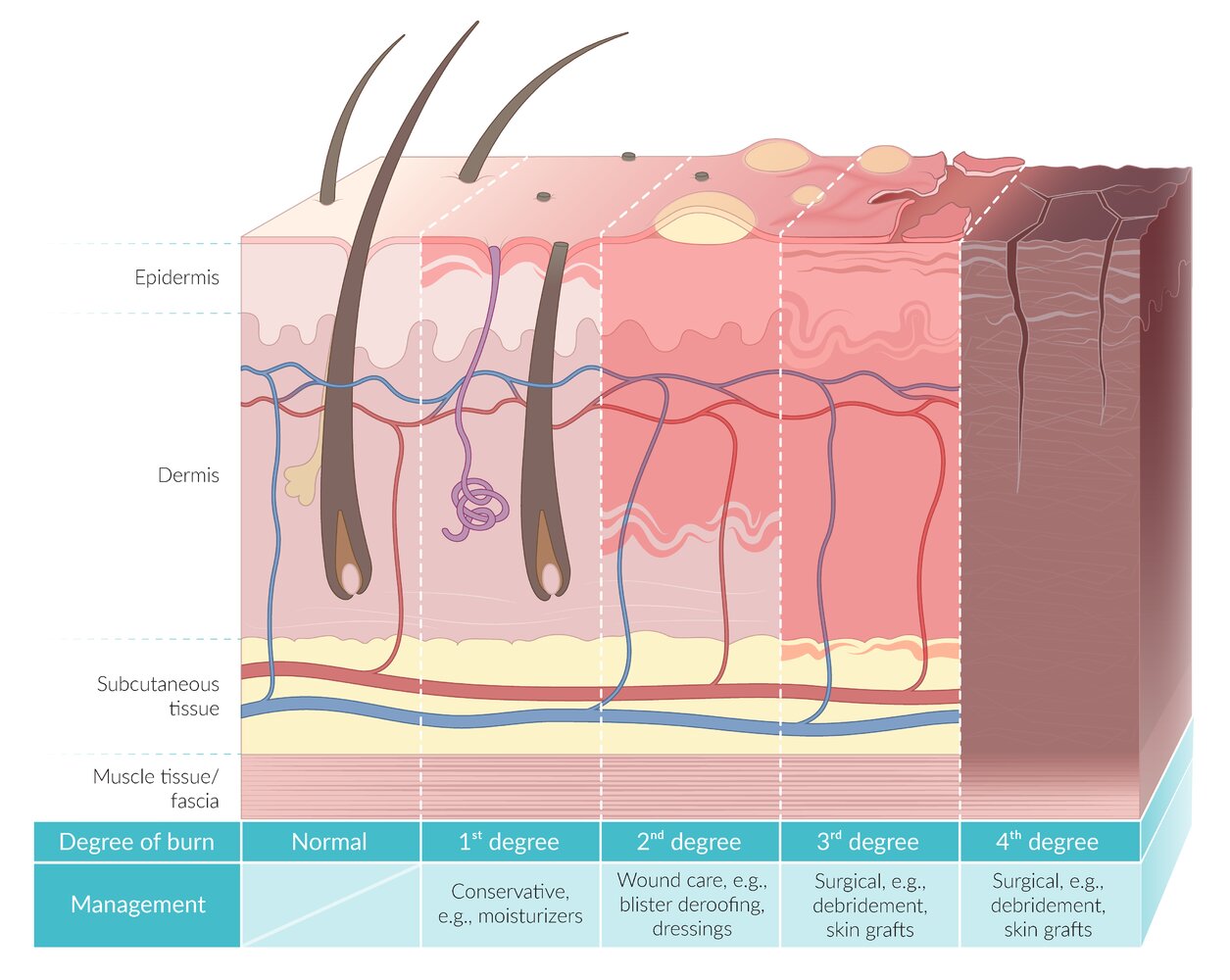
Burns are classified according to the depth of the burn.
1st-degree burns (superficial burns) only affect superficial layers of the epidermis. The skin is erythematous, dry, and may be swollen, but there is no blistering.
2nd-degree burns (partial-thickness burns) also affect the upper (2a; superficial partial-thickness burn) or lower (2b; deep partial-thickness burn) layers of the dermis. The skin blisters (vesicles and bullae) and deep partial-thickness burns may appear mottled with red/white patches.
3rd-degree burns (full-thickness burns) also affect subcutaneous tissue. The skin is black, white, or gray and appears dry and leathery.
4th-degree burns (deeper injury burns) also affect deeper structures, e.g., muscles, fat, fascia, and bones.
© AMBOSS

Upper body of a patient with moderate sunburn
Patches of erythema are visible across the areas of skin that were most exposed to the sun. The absence of blisters distinguishes this presentation from a second-degree burn (partial-thickness burn).
Sunburn most commonly manifests as a first-degree burn, but higher-degree burns are possible with prolonged sun exposure.
Source: "A moderate sunburn sustained over the course of four hours spent in the sun.", QuinnHK, Wikimedia Commons licensed under Public Domain
{kind=link}

A singular blister on an erythematous base is visible on the back of the hand.
The presence of a blister within the area of erythema differentiates this from a first-degree burn. No deeper tissue injury suggestive of a higher-degree burn is evident, confirming a second-degree burn.
Source: “Scalded skin with thin-walled blister. Second degree burn after 2 days.” by Themidget17, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Source: “Scaldburn” by Snickerdo, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Back and gluteal region
A large burned area with many vesicles and multiple large, fragile bullae (partially ruptured or deroofed) is visible.
The presence of blistering differentiates this from a first-degree burn. Wound bases appear to extend into deeper layers of the dermis than would be expected with a superficial partial-thickness burn (especially where blisters have been deroofed). There is no obvious tissue necrosis or eschar formation, differentiating this from higher-degree burns.
Source: “Verbrennung 2grad02” by Dr. Andreas Settje, Wikimedia Foundation, licensed under CC BY 3.0.
{kind=link}
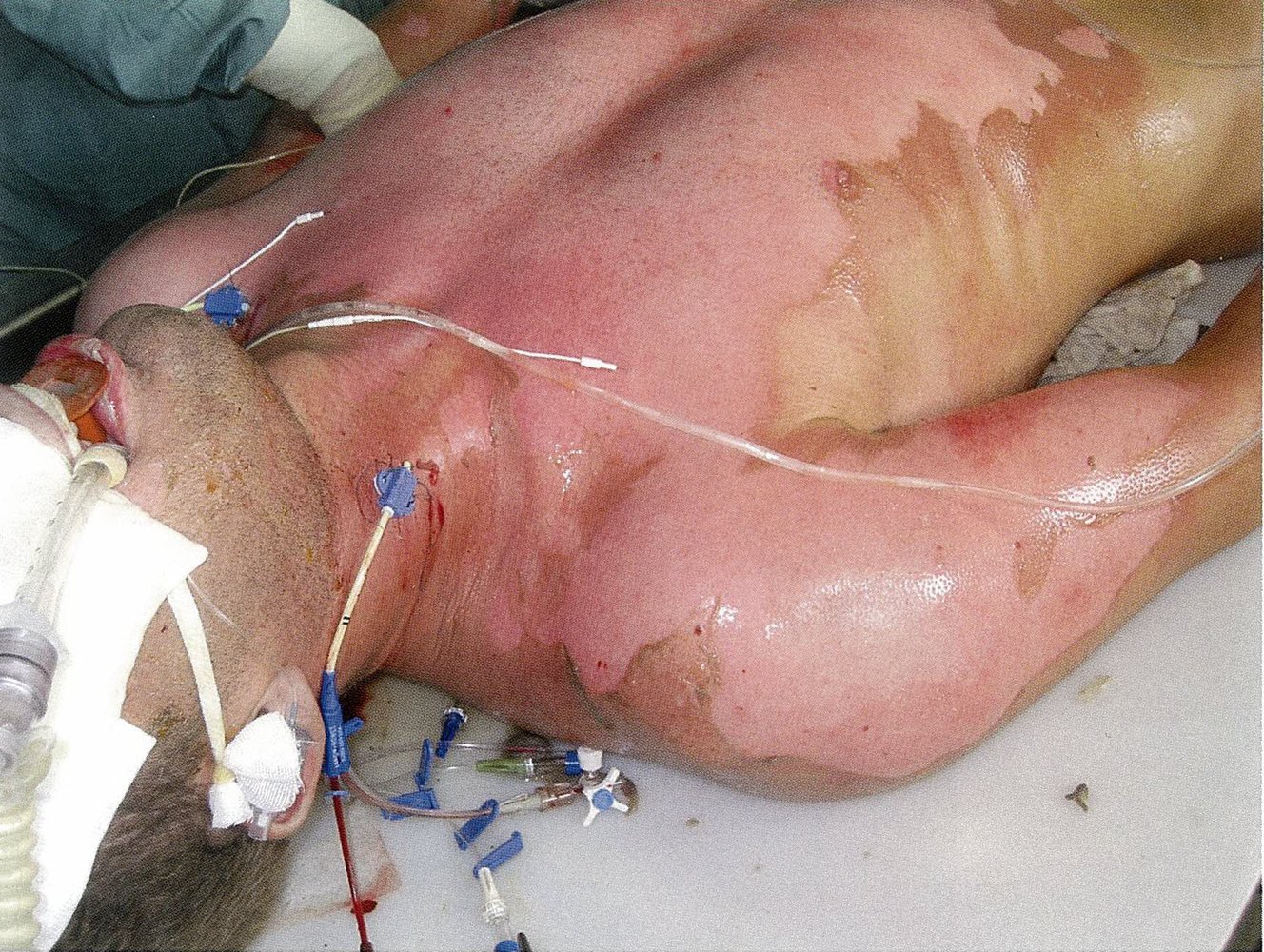
Photograph of the upper body and head of a 35-year-old male intubated patient. The injuries resulted from a suicide attempt using a high-voltage power line.
Extensive burns extend across the chest, shoulders, and upper arms. The damaged epidermis has been debrided and no blistering remains. Most of the burn area appears to be superficial partial-thickness burns (2a), though small areas of deeper red mottling (e.g., on the medial side of the right upper arm) may indicate deep partial-thickness burns (2b).
In electrical injury, the extent of visible skin damage may not correlate with the extent of deeper tissue damage, and further diagnostic studies are often necessary.
Source: © IMPP

Photograph of the left leg of a 35-year-old male intubated patient. The injuries resulted from a suicide attempt using a high-voltage power line.
An extensive burn injury extends across the calf, heel, and plantar surface of the foot. The area has been debrided and no blistering remains. The mottled red and white coloration likely indicates a mix of superficial (2a) and deep (2b) partial-thickness burns, but areas of full-thickness burn (third-degree burn) in the white-colored regions cannot be identified from this photo.
In electrical injury, the extent of visible skin damage may not correlate with the extent of deeper tissue damage, and further diagnostic studies are often necessary.
Source: © IMPP

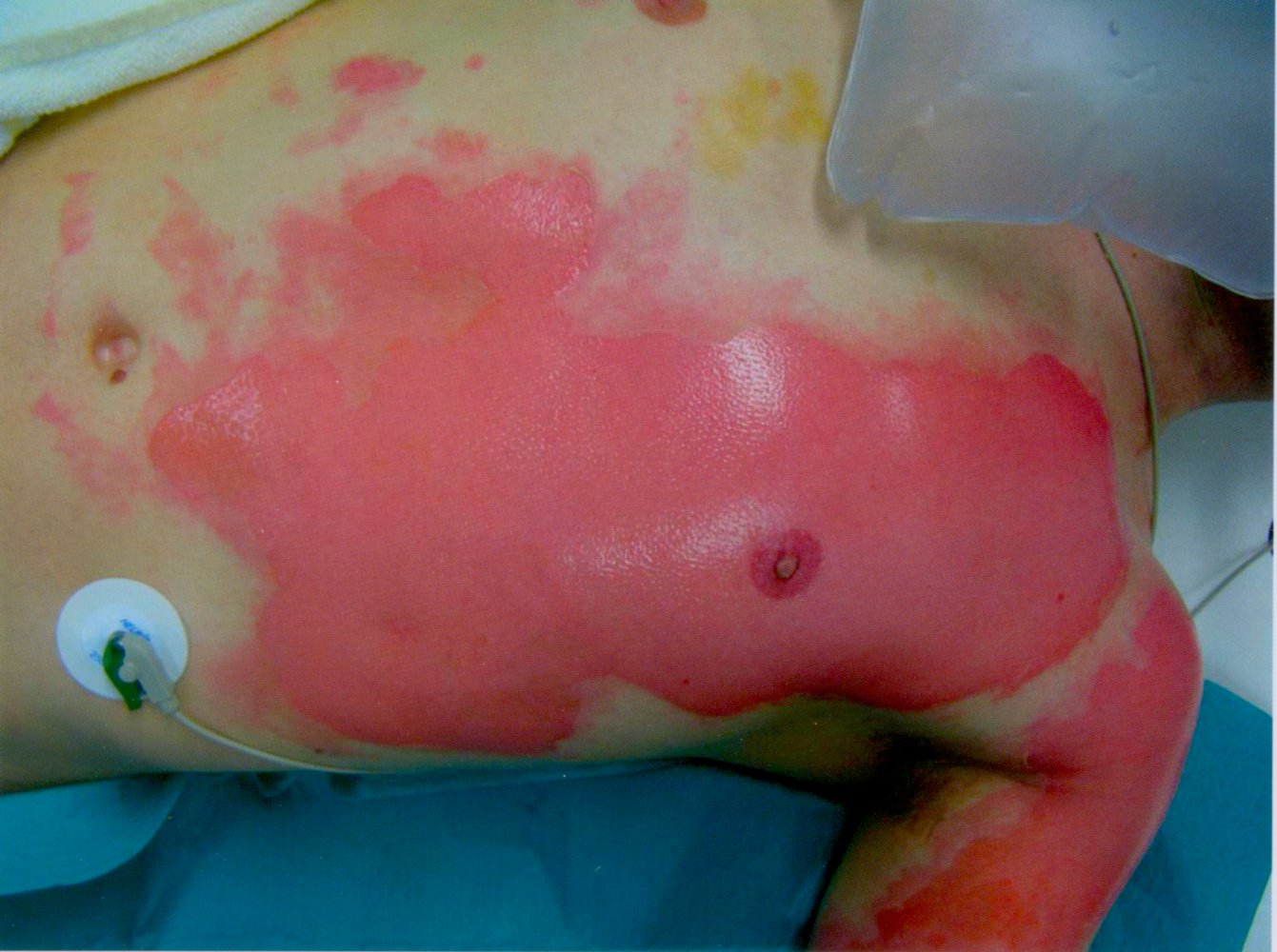
Photograph of the left side of the chest
There is a large burn extending across the central chest and left arm. Multiple large bullae have ruptured or been deroofed.
Blistering differentiates this from a first-degree burn.
Source: © IMPP
Photograph of the chest and upper-left arm
There is a large burn extending from the central chest to the left arm. This image shows the appearance after the blisters have been deroofed, exposing the moist erythematous wound base.
Blistering differentiates this from a first-degree burn.
Source: © IMPP

Photograph of the chest and right shoulder
The skin appears dry, leathery, and black, indicating tissue necrosis (eschar). There is no visible blistering.
These features are characteristic of a third-degree burn, which affects all the layers of the skin (i.e., the epidermis, dermis, and subcutaneous tissue).
Source: “Verbrennung 3gradig01.jpg” by Dr. Andreas Settje, Wikimedia Foundation, licensed under CC BY-SA 3.0.
{kind=link}

Photograph of the left hand
There are deep burn injuries visible across all digits, with charred black tissue and exposed bone and tendon. Second-degree burns are present on the palmar skin, indicated by erythema, vesicles, and blistering.
Source: “"Ожог кисть": (2nd- to 4th-degree hand burns with tissue charring)” by goga312, Wikimedia Foundation, licensed under CC BY-SA 3.0.
{kind=link}
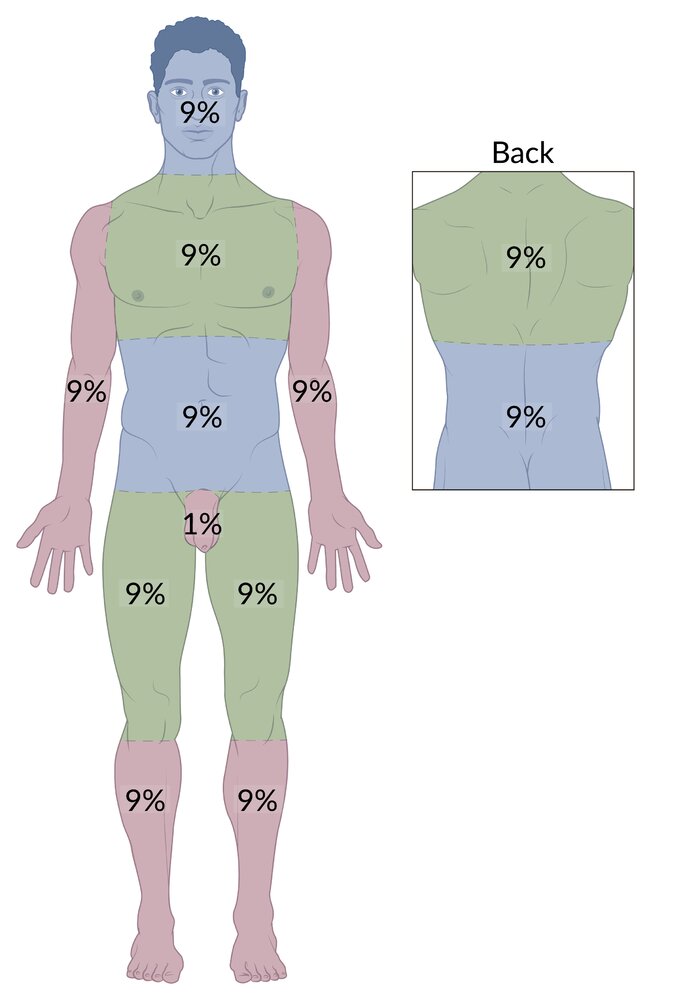
The entire body surface of an adult can be divided into 11 regions, each comprising approximately 9% of the total body surface area. The external genitalia accounts for the remaining 1%. The rule of nines is used to quickly estimate the total body surface area affected by burns in adults.
© AMBOSS
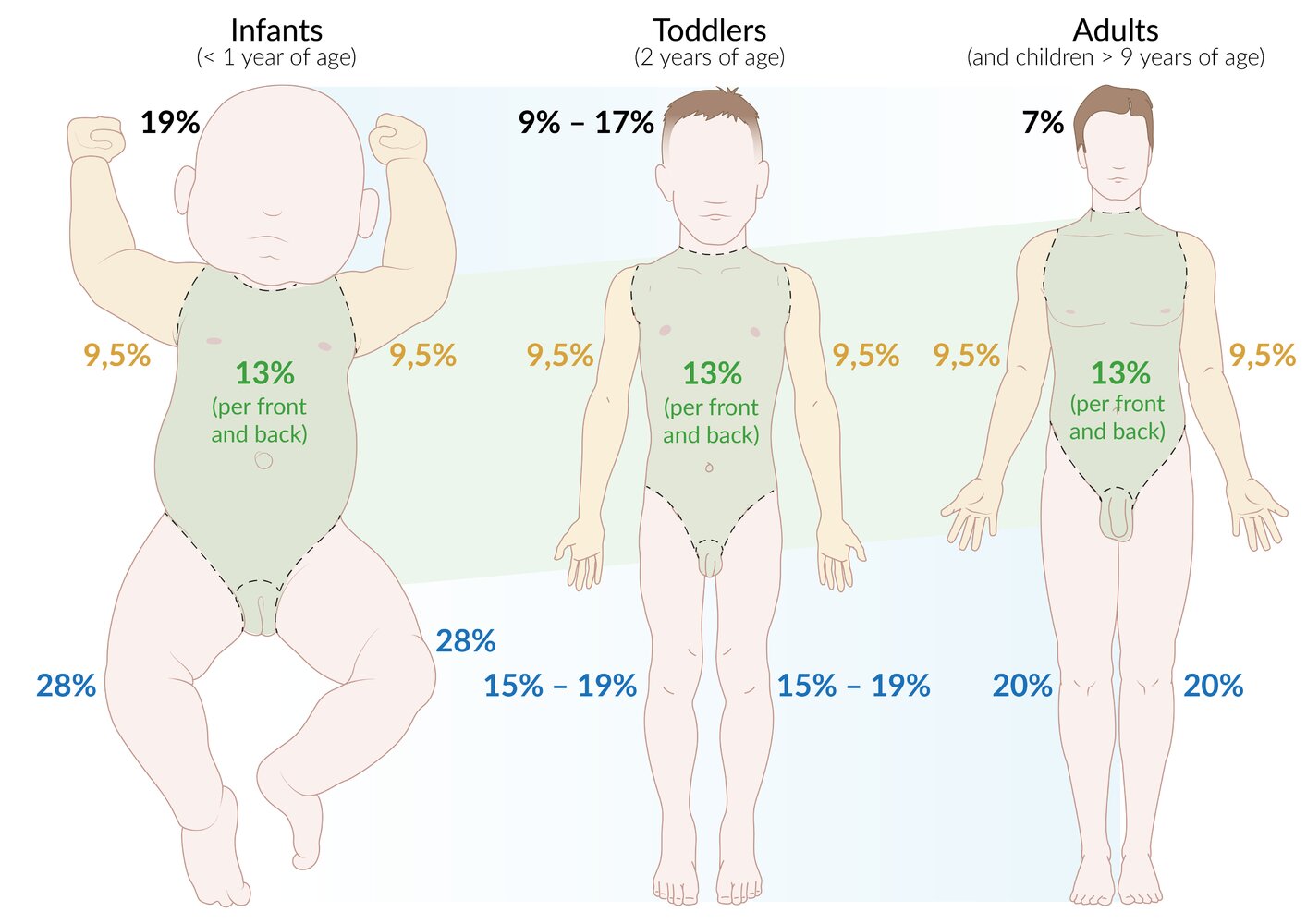
Representation of development from infant to toddler to adulthood (according to Wallace rule of nines). The regions of the body that occupy the same percentage of the total body surface area throughout development are indicated in green, whereas regions of the body in which the relative proportion of the total body surface area varies with age are depicted in blue.
© AMBOSS
Pathophysiology
Thermal burns
Local effects
- Local changes at the burn site (Jackson model of the burn wound) [1]
- Zone of coagulation: a central zone of irreversible, coagulative necrosis
- Zone of stasis: surrounds the central zone of coagulation and is comprised of damaged but viable tissue with decreased perfusion
- Zone of hyperemia: surrounds the zone of stasis and is characterized by inflammation and increased blood flow
- Bacterial colonization of the burn site
- Almost all burn wounds are colonized by bacteria.
- Common pathogens that infect burn wounds include MRSA, Pseudomonas, Klebsiella, Acinetobacter, and Candida.
-
Eschars: a skin lesion characterized by dried, necrotic skin tissue
- Can cause constrictive effects
- Circumferential eschars (burns that fully encircle the chest, neck, abdomen, and/or an extremity) → loss of skin elasticity → impaired blood flow and/or compartment syndrome (caused by an accumulation of fluids) → acute ischemia distal to the eschar
- Significant eschar on chest or neck → restriction of chest excursion → asphyxia
Inadequate resuscitation and/or wound care may result in irreversible damage to the zone of stasis and increased burn depth.
Systemic effects [5]
Burns involving > 30% of the body surface area and third- or fourth-degree burns are likely to have systemic effects.
-
Release of cytokines and other inflammatory mediators → systemic inflammatory response syndrome
- Increased vascular permeability → extravasation of protein and fluid from the intravascular compartment into interstitial tissue → generalized edema, acute respiratory distress syndrome, and hypovolemic shock with paralytic ileus
- Disseminated intravascular coagulation (DIC)
- Evaporative fluid loss → hypothermia, dehydration
- Hemolysis, muscle damage → hemoglobinuria and/or myoglobinuria → acute tubular necrosis
- Immunosuppression
Nonthermal burns [6]
-
Chemical burns [7]
- Acid exposure → coagulative necrosis → limited depth of tissue damage
- Alkali exposure → cell membrane fatty acid saponification and protein complex formation → liquefactive necrosis → deeper penetration of the agent → increased risk of systemic poisoning
-
Electrical burns [8]
- Electrical current enters the body (entry point) → tissue resistance converts electrical energy to heat → direct heat damage → current exits the body (exit point)
- Low-voltage electricity (< 1000 V): entry and exit points are typically close together → burns at the site of contact
- High-voltage electricity (≥ 1000 V): entry and exit sites are far away from each other → extensive deep-tissue and/or organ damage despite little or no apparent skin injury → high risk of rhabdomyolysis, compartment syndrome, and vascular thrombosis
- See also “Electrical and lightning injuries.”
- Electrical current enters the body (entry point) → tissue resistance converts electrical energy to heat → direct heat damage → current exits the body (exit point)
-
Radiation burns [9]
- UV waves, x-ray waves, gamma waves, alpha particles, beta particles → DNA damage (directly or indirectly via free radical formation) → cell apoptosis
- See also “Radiation injury.”
Alkali burns cause significantly more tissue damage and have a higher risk of systemic toxicity than acid burns. Local tissue damage from alkalis can continue for up to 2–3 days after exposure.
Initial management
For treatment of minor burns, see “Local burn wound care.”
Approach to burns
- Initiate a primary survey (ABCDE survey), including burn-specific considerations.
- Perform a secondary survey, including the following:
- Determination of burn severity
- Urgent specialist consultation and/or disposition as indicated
- Evaluation for signs of acute compartment syndrome
- Provide supportive care for burn injuries.
- Obtain further diagnostics based on burn severity.
- Determine the disposition of patients with burn injuries.
- Begin definitive treatment.
Primary survey
The primary survey should follow the ATLS and Advanced Burn Life Support algorithms. Obtain specialist consultation concurrently with management if indicated (e.g., activate the trauma team for trauma patients, consult obstetrics for pregnant patients).
- Don PPE.
- Stop the burning process, e.g., remove clothes and/or caustic substances (see “Special mechanisms”).
- Airway: Consider immediate advanced airway management if indications for early intubation in burns are present.
- Breathing: Administer 100% oxygen for suspected carbon monoxide poisoning (CO poisoning) or inhalation injury.
- Circulation: Begin fluid resuscitation in burns.
- Initiate acute pain management.
Be prepared for a difficult airway as a result of direct thermal injury and/or upper airway edema from IV fluid resuscitation.
Treat pain due to major burns with small, frequent doses of IV opioids; avoid subcutaneous and intramuscular opioid administration because drug absorption is unpredictable. [3][12]
Secondary survey
- Place a urinary catheter and monitor urine output.
- Determine burn severity based on the depth of burn and extent of burn.
- Consider urgent specialist consultation and disposition as indicated (see “Urgent disposition”).
-
Examine limbs for signs of acute compartment syndrome.
- Elevate injured limbs to reduce edema formation and the risk of developing acute compartment syndrome.
- Assess perfusion with pulse oximetry, capillary refill time, and a handheld Doppler device.
- Treat acute compartment syndrome with immediate escharotomy and/or fasciotomy.
Indications for early intubation in burns [3][10]
- Signs of airway obstruction
- Signs of impending respiratory failure
- Facial and/or oropharyngeal burns
- Difficulty swallowing
- > 40% TBSA burns
- Significant and/or progressive edema
- Reduced level of consciousness and/or impaired airway protective reflexes
- Limited advanced airway management during transport to a burn center
Special mechanisms [3]
Additional early management steps may be required depending on the cause of the burn injury.
-
Chemical burns
- Immediately irrigate most burn wounds with large volumes of water.
- Exceptions to immediate irrigation with water include:
- Cement (dry lime): Wipe off powder before irrigation.
- Phenols: Wipe off the phenol solution, then preferentially irrigate with PEG; use water if PEG is not available.
- Elemental metals (e.g., elemental lithium, sodium, magnesium): Remove fragments with forceps then cover the area with mineral oil.
-
Electrical and lightning injuries
- Begin continuous cardiac monitoring to assess for cardiac arrhythmias.
- Obtain diagnostics for rhabdomyolysis.
- If urine appears red, begin management of rhabdomyolysis without waiting for laboratory confirmation.
- Blast injuries: Assess for primary blast injuries, e.g., blast lung injury, blast-induced abdominal injury.
Certain burn patterns (e.g., scald burns) should raise concern for nonaccidental injury.
Urgent consults
-
Activate the trauma team for any of the following: [10]
- > 15% TBSA burns in adults
- > 10% TBSA burns in children
- Signs of airway involvement
- Contact a burn center to discuss transfer if any criteria for transfer to a burn center are met.
Diagnosis
Diagnostic testing is based on burn severity. Patients with minor burns may not require any testing. Patients with major burns require testing, but care and/or transfer should not be delayed. [3]
Bedside diagnostics
- Pulse oximetry or pulse CO-oximetry: to monitor for progressive hypoxemia, CO poisoning
- Bronchoscopy: direct evaluation for possible airway injury, e.g., mucosal edema, inhaled soot
-
Imaging studies
- CXR: to evaluate endotracheal tube position and assess for associated trauma
- Additional radiographs: depend on concomitant injuries, e.g., fractures
- ECG: to assess for arrhythmias in electrical injuries
Laboratory studies [3][10]
-
Initial studies (all patients with major burns)
- BMP: to monitor for hyperkalemia and hyponatremia in the acute phase, hypernatremia in the postacute phase, and acute renal failure
- CBC
- POC glucose
- Pregnancy test
- Urinalysis: to distinguish myoglobinuria from hematuria
-
Specialized studies (based on the mechanism and severity of injury)
- ABG: to establish baseline pulmonary status and to monitor for hypoxemia, and metabolic and respiratory acidosis
- Lactate: trends used to guide resuscitation
- Preoperative studies: coagulation studies, type and screen
- Wound and blood cultures: if there is concern for infection
A single normal ABG does not rule out inhalation injury; remain vigilant for the development of symptoms for 24 hours. [10]
Management
Follow the initial management of burns for all patients. For suspected nonaccidental injury, see also “Approach to suspected child maltreatment.”
Overview
- Management should be guided by a specialist based on burn severity and secondary injuries.
- To avoid delaying treatment, some interventions should be initiated concurrently with specialist consultation, including:
- Fluid resuscitation in burns
- Local burn wound care
- Supportive care for burn injuries
- Consult a burn center immediately to discuss transfer if any criteria for transfer to a burn center are met.
Definitive management
Definitive management should be guided by a specialist and may include:
- Early debridement of necrotic tissue [13]
- Wet-to-dry dressings for infected wounds or wounds with devitalized tissue
- Free skin grafts (i.e., split-thickness or full thickness skin graft)
- Burn reconstruction, e.g., flap reconstruction with free or pedicled flaps [14]
Fluid resuscitation in burns
Major burns (e.g., > 20% TBSA) result in increased capillary permeability, causing significant intravascular hypovolemia requiring IV fluid resuscitation. [3][15][16]
Approach
- Establish IV access: two large peripheral IVs, central line, or intraosseous access.
- Use lactated Ringer's solution to avoid hyperchloremic metabolic acidosis. [3]
- Give half the calculated 24-hour fluid volume in the first 8 hours and the remainder over the next 16 hours.
-
Place a Foley catheter and titrate IV fluid therapy to urine output and clinical response. [3]
- Adults and children > 30 kg (> 66 lb): goal urine output ≥ 0.5 mL/kg/hour
- Children ≤ 30 kg (≤ 66 lb): goal urine output ≥ 1 mL/kg/hour
- Consider colloids (e.g., albumin, plasma) in close consultation with a burn specialist. [15]
Titrate fluid resuscitation to clinical response to minimize edema formation. [3]
American Burn Association recommended protocol [3][15]
This protocol is recommended over the Parkland formula to reduce the risks of overresuscitation, e.g., perfusion-threatening; edema, pleural effusion.
-
Flame, chemical, or scald injury: first 24-hour total volume
- Adults and children ≥ 14 years of age: 2 mL x % of TBSA affected by 2nd- and 3rd-degree burns x weight in kg
- Children < 13 years of age: 3 mL x % of TBSA affected by 2nd- and 3rd-degree burns x weight in kg
- Children ≤ 30 kg (≤ 66 lb) and infants: Add D5LR maintenance fluid requirement to the resuscitation volume.
-
Electrical injury: first 24-hour total volume
- 4 mL x % of TBSA affected by 2nd- and 3rd-degree burns x weight in kg
- Children ≤ 30 kg (≤ 66 lb) and infants: Add D5LR maintenance fluid requirement to the resuscitation volume.
Parkland formula
- A traditional fluid resuscitation protocol for patients with burn injuries
- Risk of overresuscitation, which can lead to complications
- First 24-hour total volume: 4 mL x % of TBSA affected by 2nd- and 3rd-degree burns x weight in kg
Local burn wound care
Minor burns [3][13]
- Provide acute pain management (typically acetaminophen or NSAIDs).
- Irrigate the wound to cool the area and remove debris.
- Clean the wound with soap or diluted chlorhexidine gluconate.
- Treat first-degree burns with topical moisturizers (e.g., aloe vera-based gels) for symptom relief. [13][17]
- Consider applying a topical antibiotic, e.g., bacitracin.
- Consider a nonadherent wound dressing if the skin is broken.
Major burns [3][13]
Consult a burn specialist as soon as possible.
- Administer acute pain management: typically small, frequent doses of IV opioids.
- Consider immediate escharotomy or fasciotomy if limb perfusion is compromised. [3][10]
- Irrigate the wound to cool the area and remove debris.
- Clean the wound with soap or diluted chlorhexidine gluconate.
- Debride devitalized skin and blisters > 2 cm using sterile gauze or scissors.
- Apply a topical antibiotic.
- Silver sulfadiazine is commonly used for full-thickness burns.
- Bacitracin is commonly used for partial-thickness burns.
-
Apply a wound dressing.
- Dressing choice depends on burn depth, location, and infection risk.
- Types of dressing: occlusive dressing, hydrocolloid dressing, biosynthetic dressing
Treat hypoxemia and hypovolemia before giving narcotics or sedatives to avoid masking features of these life-threatening conditions. [10]
Supportive care for burn injuries
-
Hypothermia prevention
- Increase the ambient temperature in the treatment room.
- Monitor core body temperature.
- Use fluid warmers for IV fluid therapy if core body temperature is low.
-
Nutritional support
- Consult nutrition early to manage postburn hypermetabolism.
- Enteral nutrition is preferred over parenteral nutrition.
- Anxiety management: See “Benzodiazepines for the treatment of agitation.”
-
Antibiotic prophylaxis [18]
- Not recommended for acute burns
- If sepsis is suspected, include coverage for MRSA (e.g., vancomycin) and Pseudomonas (e.g., cefepime).
- Stress ulcer prophylaxis: , e.g., proton pump inhibitors or H2 antagonists [3]
- Tetanus prophylaxis for all patients
- Physical therapy when tolerated
Escharotomy
- Definition: incisions made through constricting eschars to improve perfusion and/or ventilation
-
Indications: symptoms caused by constricting circumferential burns on the neck, chest, abdomen, and/or limbs
- Limbs: signs of acute compartment syndrome
- Chest: increased airway pressures, decreased tidal volumes, decreased preload, decreased cardiac output
- Abdomen: clinical features of abdominal compartment syndrome
-
Technique [19]
- Don PPE and create a sterile field.
- Partial-thickness burns: Administer local anesthesia and/or sedation.
- Make incisions on both the medial and lateral aspects of the extremity, trunk, and/or chest.
- Only incise through the depth of the skin, until underlying subcutaneous fat is exposed.
- Incisions should extend 1 cm above and below the constricting lesion.
- Limb escharotomy
- Avoid incising over neurovascular structures.
- Verify that peripheral perfusion has improved after escharotomy is complete.
- Thoracic escharotomy
- Incise from the clavicles to the costal margin along the anterior axillary line, bilaterally.
- Make a transverse incision along the subcostal line to join both vertical incisions.
- Verify that ventilation and/or cardiac output have improved after escharotomy is complete.
Fasciotomy is indicated if signs of acute compartment syndrome persist after escharotomy. [20]
Disposition
- Minor burns: outpatient follow-up at a burn clinic [6]
- Consider hospital admission for patients with any of the following: [6]
- Large, deep burn wounds
- Comorbidities
- Concurrent trauma injuries
- Inability to care for wounds in an outpatient setting
-
Criteria for transfer to a burn center [3][10]
- > 10% TBSA partial-thickness burns
- Burns on the face, hands, feet, genitalia, or over major joints
- Third-degree burns (full thickness)
- Electrical and chemical burns
- Inhalation injury
- Comorbidities requiring complex management, e.g., diabetes, renal failure
- Concurrent injuries, e.g., fractures
- All children (if pediatric expertise is not immediately available)
- Psychosocial support or rehabilitation required
Complications
-
Shock, sepsis, and respiratory failure
- Most common causes of death from burns.
- Common causative organisms of sepsis include Staphylococcus aureus (including MRSA), Enterococcus (including VRE), and Pseudomonas.
-
Circumferential burns may lead to:
- Compartment syndrome
- Acute limb ischemia (e.g., weak/absent pulse, paresthesia, pallor in the affected limb)
- Abdominal compartment syndrome
- Increased intraabdominal pressure (e.g., jugular venous distension, hypotension, tachycardia)
- Curling ulcers
- Keloid formation, contractures
- Marjolin ulcer
- Complications of chemical burns
- Cataracts or vision loss (if the burn involves the eyes)
- Esophageal strictures (if the burn involves the esophagus)
- Systemic poisoning
- Complications of electrical burns: arrhythmias
We list the most important complications. The selection is not exhaustive.
Inhalation injury
Definition [3]
Inhalation injuries are defined as damage to the respiratory tract caused by inhalation of superheated gas or steam, toxic byproducts of fire, or other primary irritants.
Etiology
- Smoke
- Superheated gases or steam
- Particulate matter, e.g., soot
- Irritants and asphyxiants, which can lead to poisoning (e.g., CO poisoning, ammonia intoxication, cyanide poisoning, chlorine poisoning)
Pathophysiology [3]
- Supraglottic injuries: mainly due to thermal damage, which leads to epithelial sloughing, hypersecretion, and airway obstruction from swelling and secretions
- Subglottic injuries: due to chemical irritation, which leads to epithelial damage, hypersecretion, impaired ciliary function, and potential airway obstruction
Clinical features [3]
- Signs of airway obstruction (primarily caused by upper airway edema)
- Bronchospasm
- Signs of pulmonary edema
Red flags for inhalation injury [21]
- Burn injury occurred in a confined space
- Facial burns, singed eyebrows and/or nose hair
- Evidence of soot on the face or in the airway, e.g., carbonaceous sputum
- Stridor, dysphonia
- Extensive TBSA
Management of inhalation injury [3][10][21]
Initial management
- Begin oxygen therapy based on the clinical scenario, e.g., high-flow humidified oxygen through a nonrebreather mask for suspected CO poisoning.
- Monitor end-tidal CO2 (EtCO2) and pulse oximetry.
- Obtain a chest x-ray to evaluate for pulmonary edema, associated trauma, and ARDS.
- Consider advanced airway management (e.g., early intubation) for signs of airway obstruction or respiratory failure.
Ongoing management
- Further diagnostics
- Perform flexible fiberoptic laryngoscopy to assess for laryngeal edema and help guide airway management.
- Consider flexible fiberoptic bronchoscopy; to assess for airway damage, e.g., mucosal erythema, edema, blistering, ulceration, and/or soot deposition.
- Obtain ABG and serum lactate levels to quantify lung injury severity and as a surrogate marker for cyanide poisoning.
- Measure carboxyhemoglobin levels; see “CO poisoning.”
- Conduct pulmonary function tests to rule out airway obstruction.
- Use lung protective ventilation strategies in intubated patients to prevent further pulmonary injury.
- Initiate specific management based on the cause and severity of the injury.
- Management of CO poisoning
- Management of asphyxiant and irritant exposure
- See “Management” in “Cyanide poisoning.”
- Management of ARDS
Complications
- Airway obstruction due to laryngeal edema
- Tracheobronchitis
- Pneumonitis
- ARDS
- Arsenic poisoning
- Carbon monoxide poisoning
- Cyanide poisoning
A normal ABG and/or CXR at presentation does not exclude an inhalation injury; injuries can manifest after 24–48 hours. [3]
Always assess for CO poisoning in patients with major burns, even if pulse oximetry is normal.


Fiberoptic bronchoscopy image of trachea on day of injury (at level of carina)
There is mucosal erythema, edema, and soot deposition.
These findings are characteristic of the early stages of inhalation injury (damage to the respiratory tract that occurs due to the inhalation of hot smoke and/or noxious gases).
Source: “Fig. 1, in: Diagnosis and management of inhalation injury: an updated review” by Walker PF, Buehner MF, Wood LA et al., BMC Critical Care, licensed under CC BY 4.0. Modifications: image cropped.
Postburn hypermetabolism
- Definition: a metabolic phenomenon that can occur in patients with moderate to severe burn injuries characterized by an initial hypometabolic phase followed by a hypermetabolic state
-
Pathophysiology: an increase in catecholamines, cortisol, and inflammatory cytokines → severe metabolic alterations
- Elevated resting energy expenditures
- Insulin resistance
- ↑ Gluconeogenesis
- ↑ Lipolysis
- Protein catabolism
-
Clinical features
- Hypometabolic phase (ebb phase)
- Onset within 48 hours of the burn injury
- Decreased cardiac output, oxygen consumption, and metabolic rate
- Hypermetabolic phase (flow phase)
- Onset 5–7 days after the injury
- Can persist for up to ∼ 3 years
- Hyperdynamic circulation: ↑ blood pressure, ↑ heart rate
- Muscle wasting, protein loss
- Significant weight loss
- Hyperglycemia
- Increased body temperature
- Multiorgan dysfunction
- Hypometabolic phase (ebb phase)
-
Management
- Early excision and grafting
- Analgesia
- Nutritional support
- Anabolic steroids
- Glycemic control with insulin
- Beta blockers (e.g., propranolol) to decrease resting metabolism
References:[22][23]
References
- Hettiaratchy S, Dziewulski P. "Pathophysiology and types of burns". BMJ. 328(7453). :1427-1429. (2004)
- Friedstat J, Brown DA, Levi B. "Chemical, Electrical, and Radiation Injuries". Clin Plast Surg. 44(3). :657-669. (2017)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- R. Palao, I. Monge, M. Ruiz, J.P. Barret. "Chemical burns: Pathophysiology and treatment". Burns. 36(3). :295-304. (2010)
- Gentges J, Schieche C. "Electrical injuries in the emergency department: an evidence-based review". Emerg Med Pract. 20(11). :1-20. (2018)
- Julie L. Ryan. "Ionizing Radiation: The Good, the Bad, and the Ugly". Journal of Investigative Dermatology. 132(3). :985-993. (2012)
- "Advanced Burn Life Support Course". https://ameriburn.org/wp-content/uploads/2019/08/2018-abls-providermanual.pdf. [2018-01-01]
- American College of Surgeons and the Committee on Trauma. "ATLS Advanced Trauma Life Support". American College of Surgeons. (2018). ISBN: 9780996826235
- Greenhalgh DG. "Management of Burns". N Engl J Med. 380(24). :2349-2359. (2019)
- Brunicardi F, Andersen D, Billiar T, et al. "Schwartz's Principles of Surgery". McGraw-Hill Education. (2014). ISBN: 9780071800921
- Lloyd EC, Rodgers BC, Michener M, Williams MS. "Outpatient burns: prevention and care". Am Fam Physician. 85(1). :25-32. (2012)
- Walker PF, Buehner MF, Wood LA, et al. "Diagnosis and management of inhalation injury: an updated review". Crit Care. 19(1). (2015)
- Jeschke MG. "Postburn Hypermetabolism: : past, present and future". Journal of Burn Care & Research. 37(2). :86-96. (2016)
- Williams FN, Herndon DN, Jeschke MG. "The Hypermetabolic Response to Burn Injury and Interventions to Modify this Response". Clin Plast Surg. 36(4). :583-596. (2009)
- Hettiaratchy S, Papini R. "Initial management of a major burn: II—assessment and resuscitation". BMJ. 329(7457). :101-103. (2004)
- Vercruysse GA, Alam HB, Martin MJ, et al. "Western Trauma Association critical decisions in trauma: Preferred triage and initial management of the burned patient". J Trauma Acute Care Surg. 87(5). :1239-1243. (2019)
- Romanowski KS, Carson J, Pape K, et al. "American Burn Association Guidelines on the Management of Acute Pain in the Adult Burn Patient: A Review of the Literature, a Compilation of Expert Opinion and Next Steps". J Burn Care Res. 41(6). :1152-1164. (2020)
- Cartotto R, Johnson LS, Savetamal A, et al. "American Burn Association Clinical Practice Guidelines on Burn Shock Resuscitation". J Burn Care Res. (2023)
- Cartotto R, Greenhalgh DG, Cancio C. "Burn State of the Science: Fluid Resuscitation". Journal of Burn Care & Research. 38(3). :e596-e604. (2017)
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Teunissen CE, Petzold A, Bennett JL, et al. "A consensus protocol for the standardization of cerebrospinal fluid collection and biobanking". Neurology. 73(22). :1914-1922. (2009)
- Marc G. Jeschke, Margriet E. van Baar, Mashkoor A. Choudhry, et al. "Burn injury". Nature Reviews Disease Primers. 6(1). (2020)