Summary
Cardiomyopathies are diseases of the muscle tissue of the heart. Types of cardiomyopathies include dilated (most common), hypertrophic, restrictive, and arrhythmogenic right ventricular cardiomyopathy.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) primarily affects the right ventricle and is characterized by fibrofatty replacement of myocardium, which causes myocardial thinning and subsequent ventricular dilation. Although the hallmark finding is arrhythmia, symptoms are highly variable. Because management depends greatly on individual factors, such as the extent of the disease, there is no single best course of treatment. All patients should avoid strenuous exercise.
Arrhythmia-induced cardiomyopathy is a very rare type of cardiomyopathy. It is caused by long-standing arrhythmia and typically affects the left ventricle. Features include palpitations, syncope, and signs of arrhythmia on ECG. Progression to left heart failure is possible in severe cases. Treatment involves antiarrhythmics such as beta blockers for rhythmic control.
“Dilated cardiomyopathy”, “Hypertrophic cardiomyopathy,” “Restrictive cardiomyopathy,” and “Peripartum cardiomyopathy” are described in their respective articles in more detail.
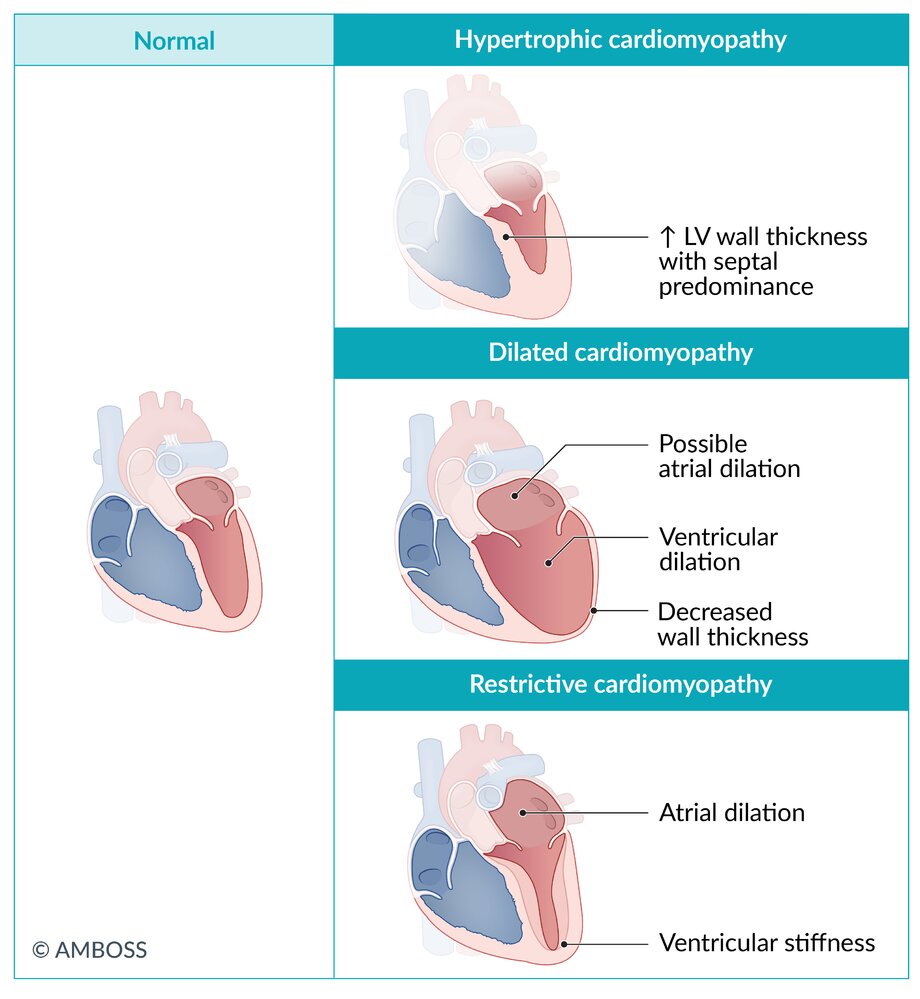
Overview of major types of cardiomyopathy
| Differential diagnosis of major cardiomyopathies | ||||
|---|---|---|---|---|
| Types | Dilated cardiomyopathy | Hypertrophic cardiomyopathy | Restrictive cardiomyopathy | |
| Etiology |
|
|
|
|
| Pathophysiology |
|
|
|
|
| Distinctive clinical features |
|
|
|
|
| Echocardiography | LV cavity size |
|
|
|
| EF |
|
|
|
|
| Wall thickness |
|
|
|
|
| Additional findings |
|
|
|
|
| Other characteristics |
|
|
|
|






© AMBOSS

Autopsy specimen of a heart
The opened left atrium and ventricle can be seen. There is substantial endocardial fibroelastosis, which manifests as increased whiteness of the endocardium (star).
Source: “Fig 2A, In: Barth syndrome” by Clarke SL, Bowron A, Gonzalez IL et al., BMC Orphanet Journal of Rare Diseases, licensed under CC BY 2.0. Modifications: image cropped & removal of the letter A.
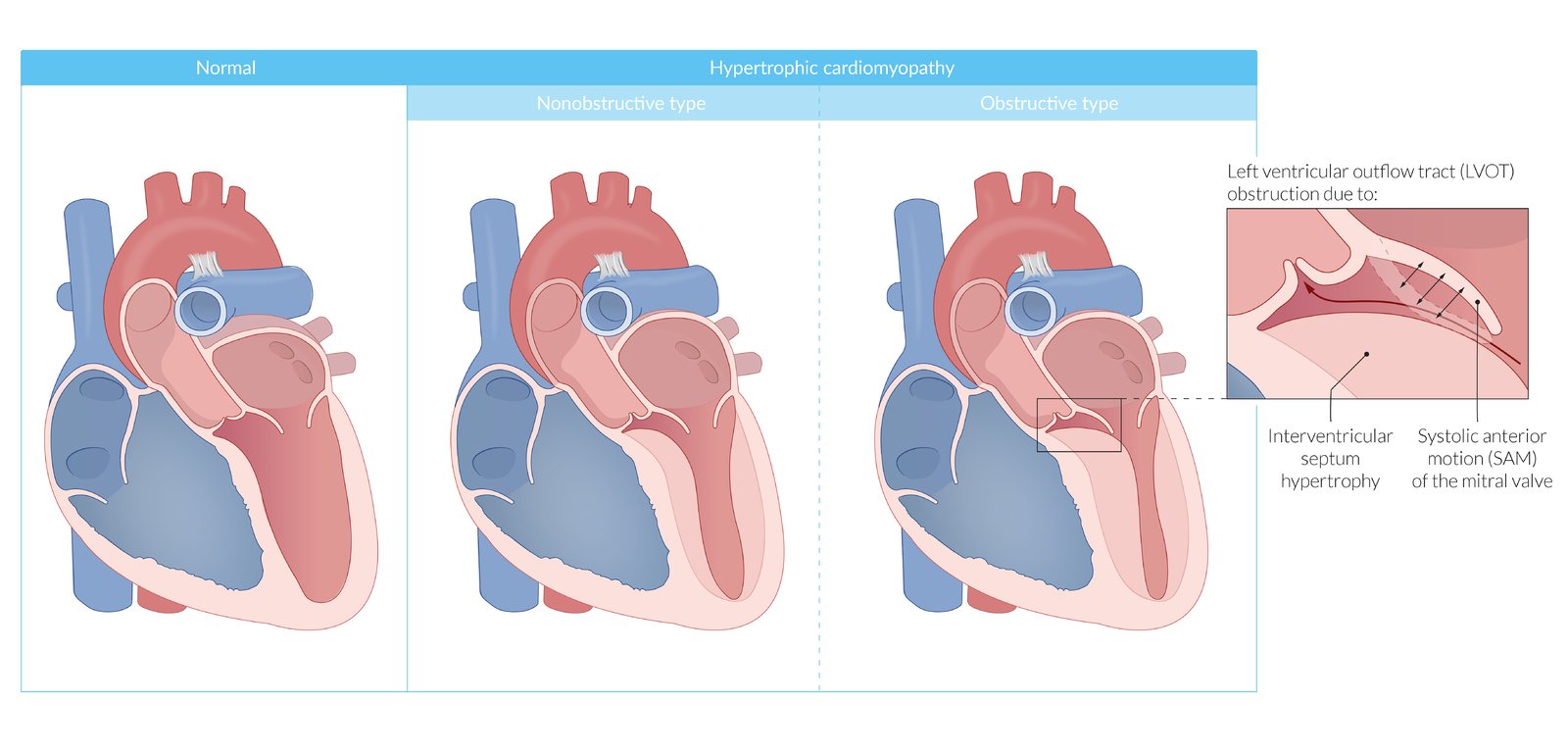
Hypertrophy of the myocardium results in reduced diastolic compliance and filling of the left ventricle (sometimes also of the right ventricle). Hypertrophic cardiomyopathy can occur with or without left ventricular outflow tract obstruction. Hypertrophic obstructive cardiomyopathy (HOCM) occurs when hypertrophy of the interventricular septum and systolic anterior movement (SAM) of the mitral valve leaflet results in the left ventricular outflow tract (LVOT) obstruction.
© AMBOSS
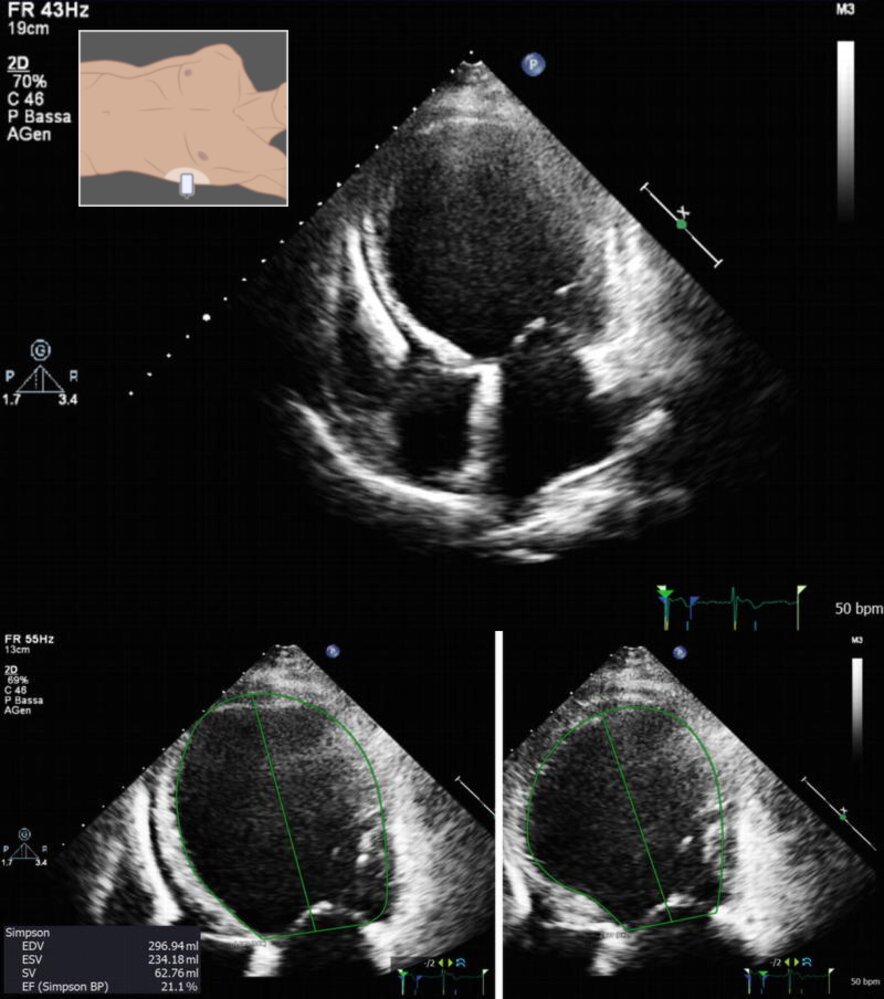
Transthoracic echocardiogram (upper image: apical four-chamber view; lower left image: end-diastolic apical four-chamber view; lower right image: end-systolic apical four-chamber view)
Upper image: Compared to normal findings (green dashed outline), the left ventricular cavity size (red overlay) is significantly increased (green arrows); ventricular wall thickness is normal. The left atrium is also dilated. An implantable cardioverter defibrillator (ICD) lead is visible in the right ventricle.
Lower images (calculations using biplane Simpson method): Both end-diastolic volume (EDV; left image) and end-systolic volume (ESV; right image) are markedly increased, and the ejection fraction (EF) is markedly below normal at 21% (normal value is ∼ 55%).
This combination of findings is typical of dilated cardiomyopathy.
LV: left ventricle; MV: mitral valve; LA: left atrium; RA: right atrium; TV: tricuspid valve; RV: right ventricle
Source: “Fig. 7.2, and 7.3, in: Role of Cardiac Imaging: Echocardiography” by Pinamonti B, Abate E, De Luca A, Finocchiaro G, Korcova R, Dilated Cardiomyopathy, licensed under CC BY 4.0. Modifications: - two images were combined - added illustration. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
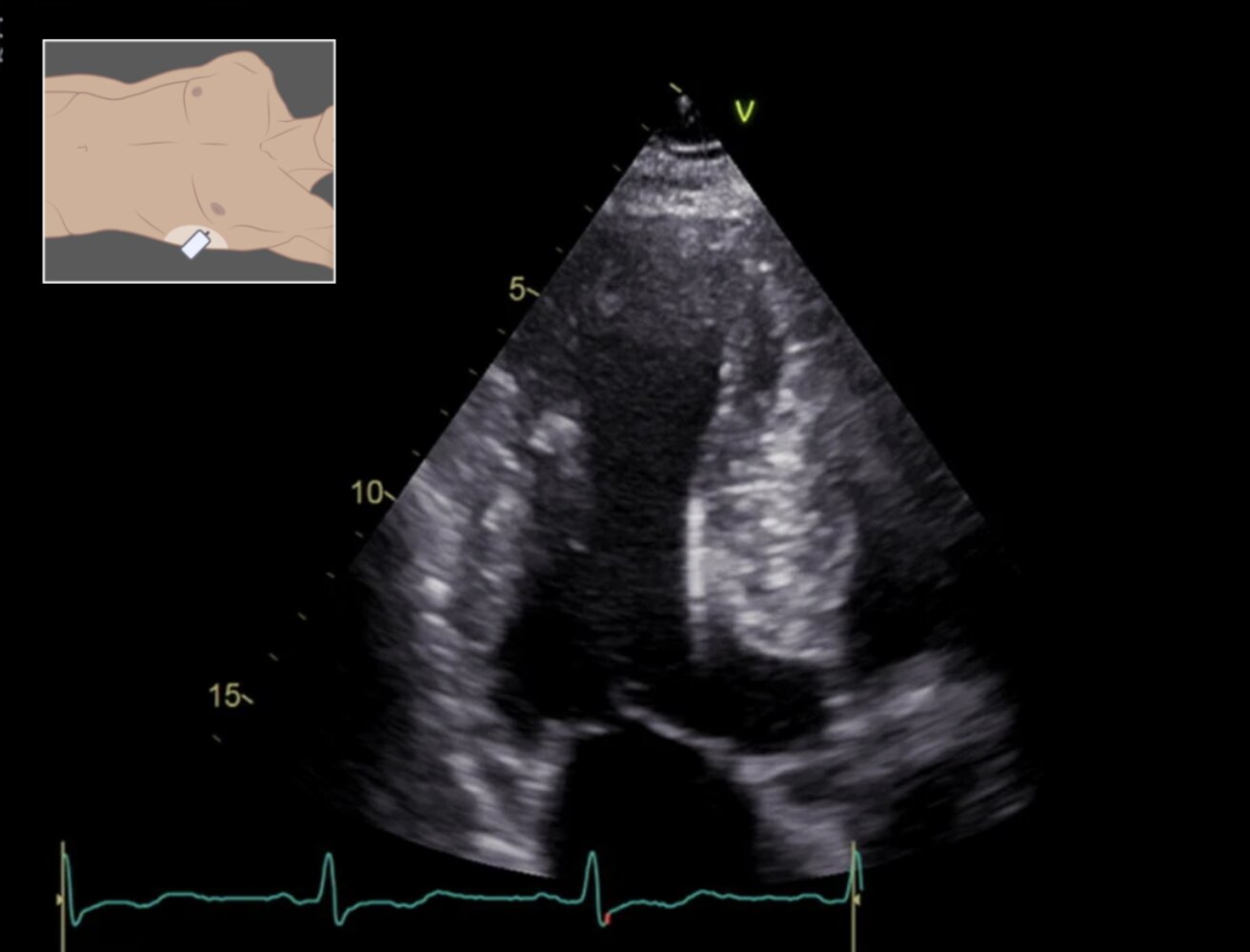
Transthoracic echocardiogram (apical three-chamber view)
The walls of the left ventricle are asymmetrically hypertrophied. Compared to normal findings (green dashed outline), the interventricular septum (red overlay) is markedly thickened (green arrows). The lateral wall is also thickened, but not to the same extent as the interventricular septum.
These findings are suggestive of hypertrophic cardiomyopathy. To assess for left ventricular outflow tract (LVOT) obstruction, the LVOT pressure gradient during systole should be measured.
LW: lateral wall; LV: left ventricle; IVS: interventricular septum; MV: mitral valve; AV: aortic valve; LA: left atrium
Source: “Fig. 1, in: The role of echocardiography for diagnosis and prognostic stratification in hypertrophic cardiomyopathy” by Mandeş L, Roşca M, Ciupercă D, Popescu BA, Journal of Echocardiography, licensed under CC BY 4.0. Modifications: - cropped image - removed letter - added illustration. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
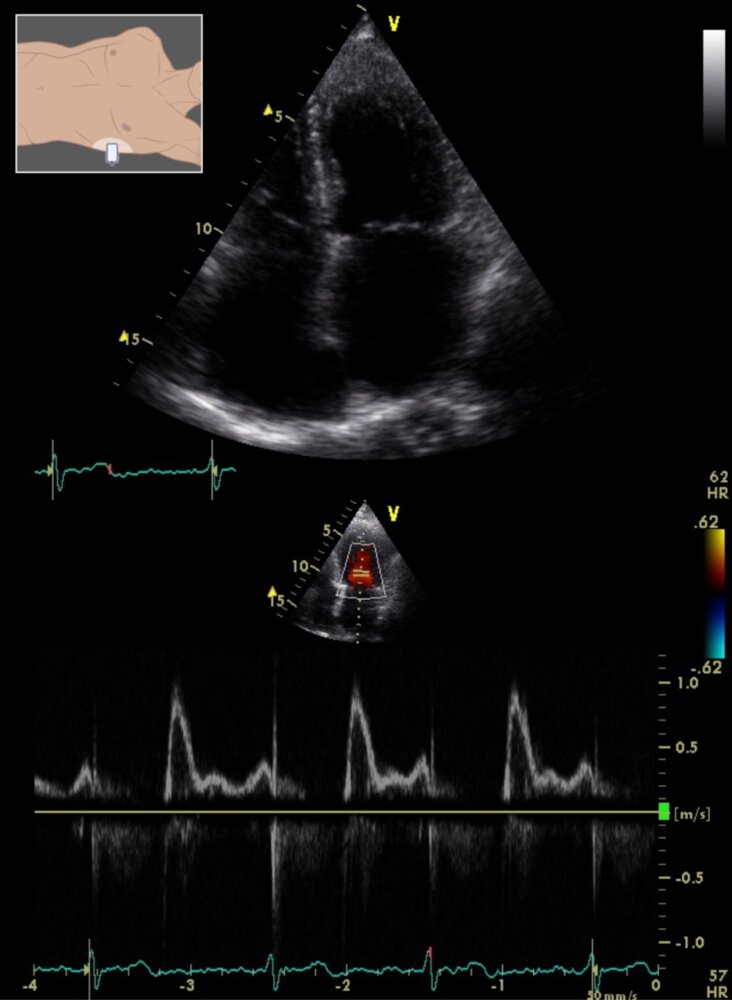
Transthoracic echocardiogram (upper image: apical four-chamber view in systole; lower image: apical four-chamber view, pulse wave Doppler of left ventricular inflow)
Upper image: Compared to normal findings (green dashed outlines), both atria (red overlay) are significantly enlarged (green arrows). Left ventricular volume and wall thickness are normal, and left ventricular ejection fraction is also normal (62%; not shown on image).
Lower image: The E/A ratio is > 1.5 (the velocity of the E wave of early diastolic left ventricular filling is ∼ 1 m/s and that of the A wave of late diastolic left ventricular filling is ∼ 0.4 m/s, resulting in a ratio of ∼ 2.5), indicating a restrictive diastolic filling pattern and severe diastolic dysfunction.
The combination of normal ventricular volume, wall thickness, and ejection fraction with atrial enlargement and diastolic dysfunction is consistent with restrictive cardiomyopathy. An important differential is constrictive pericarditis.
RV: right ventricle; LV: left ventricle; TV: tricuspid valve; MV: mitral valve; RA: right atrium; LA: left atrium; E: E wave; A: A wave
Source: “Fig. 1(b) and 1(c), in: Restrictive Cardiomyopathies: The Importance of Noninvasive Cardiac Imaging Modalities in Diagnosis and Treatment—A Systematic Review” by Rammos A, Meladinis V, Vovas G, Patsouras D, Hindawi, licensed under CC BY 4.0. Modifications: - two images combined - added illustration. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Arrhythmogenic right ventricular cardiomyopathy (ARVC)
Epidemiology
- Most common in young adults (mean age at diagnosis: ∼ 30 years) [2]
- Prevalence: 1:1,000–2,000 [3]
Etiology
- Mutations of various genes (e.g., JUP gene)
- Autosomal recessive or autosomal dominant inheritance [3][4]
Pathophysiology
- Right ventricular myocardial cell death (due to myocyte apoptosis, inflammation, and fatty/fibrotic tissue replacement) → thinning of the right ventricular wall → dilation of the ventricle → ventricular arrhythmia and dysfunction [2]
- The left ventricle can also be affected, but consequences are usually less severe.

Clinical features
- Highly variable
- Many patients remain asymptomatic.
- Angina pectoris
- Dyspnea
- Peripheral edema, ascites, hepatic and splenic congestion
- Palpitations, syncope, possibly sudden cardiac death (particularly during or after exercise)
Diagnostics [2][3][5]
Approach
ARVC is diagnosed based on the AHA criteria which include the following features:
- Dysfunction and structural abnormalities of RV (can be revealed by echocardiography, MRI, or RV angiography)
- Histological characteristics (require myocardial biopsy)
- Abnormal repolarization (diagnosed with ECG)
- Depolarization/conduction abnormalities (diagnosed with ECG)
- Arrhythmias (diagnosed with ECG)
- Family history (confirmation of ARVC in a relative either by criteria, pathological examination in surgery or autopsy, or by genetic testing)
Findings
-
ECG
-
Repolarization disturbances in the right precordial leads (V1-3)
- Possibly epsilon wave (at the end of a widened QRS complex)
- Highly specific for ARVC but only occurs in ∼ ⅓ of patients
- Increased QRS duration
- Ventricular tachycardia
- Ventricular extrasystoles
-
Repolarization disturbances in the right precordial leads (V1-3)
-
Echocardiography and cardiac MRI
- RV enlargement
- RV wall motion abnormalities
- ↓ RV EF
- Localized RV aneurysms
- Endomyocardial biopsy: fibrofatty replacement of myocardial tissue
- Genetic testing: Multiple genetic abnormalities that can cause ARVC have been identified (e.g., plakoglobin (JUP), desmoplakin (DSP), plakophilin-2 (PKP2), desmoglein-2 (DSG2), desmocollin (DSC2)). [4]
, including torsades de pointes")
Management [5]
- Avoid intense physical exertion.
-
Antiarrhythmic treatment
- Pharmacologic: beta blockers (e.g., sotalol), amiodarone, calcium channel blockers
- Invasive
- AICD implantation (in high-risk patients, e.g., patients with left ventricular involvement)
- Radiofrequency ablation (only as ancillary treatment)
- Heart transplant (in severe cases that are refractory to all other treatments)
- Screening and genetic counseling for first-degree relatives [6]
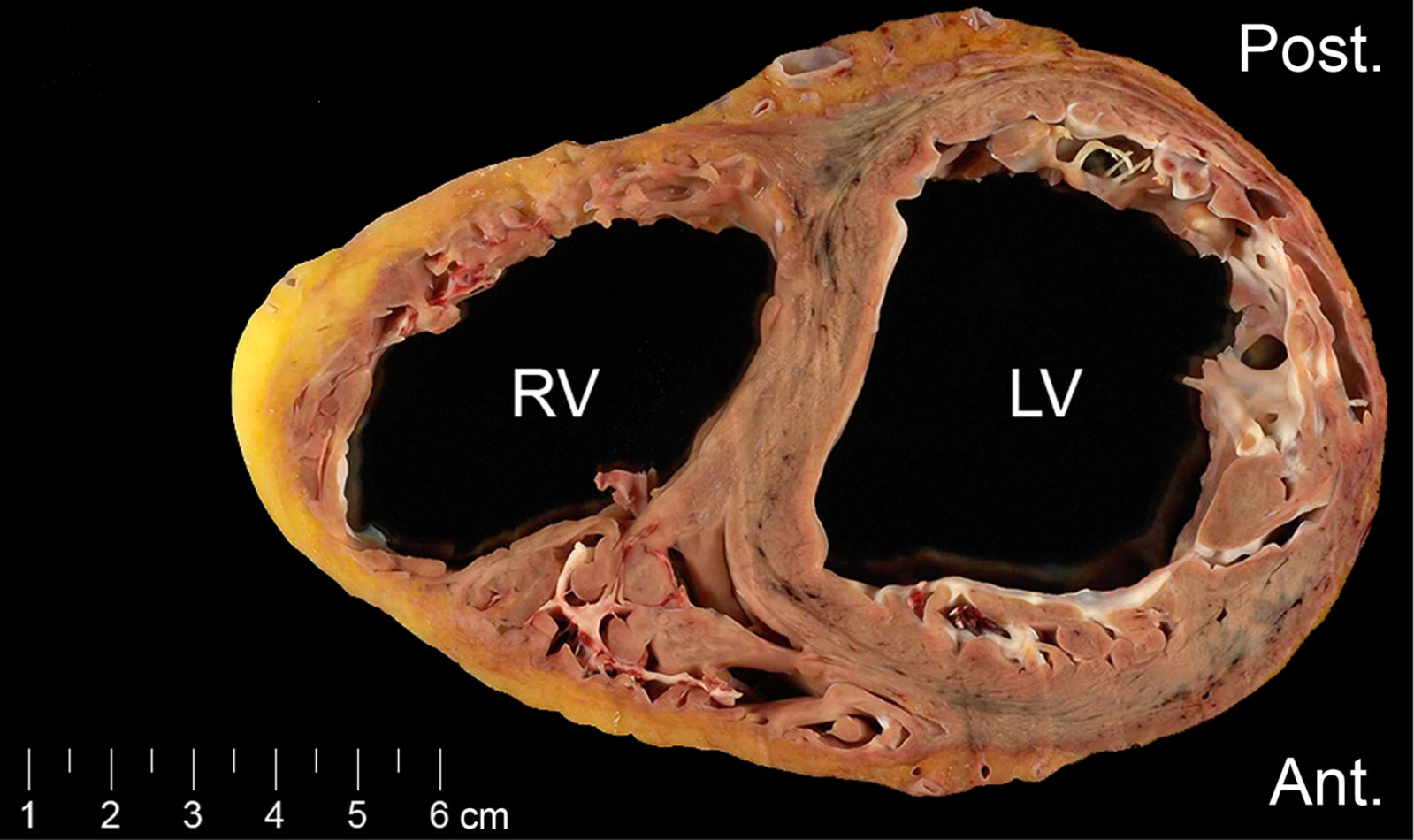
Heart (transverse section)
The myocardium of the right ventricular wall is largely replaced by fibrotic and adipose tissue (green overlay). The left ventricle is less severely affected. As a result of myocardial thinning, both ventricles are significantly dilated.
These findings are consistent with arrhythmogenic right ventricular cardiomyopathy (ARVC). Despite its name, biventricular involvement in ARVC is common.
Source: “Figure 1A. in: High Resolution Systematic Digital Histological Quantification of Cardiac Fibrosis and Adipose Tissue in Phospholamban p.Arg14del Mutation Associated Cardiomyopathy” by Johannes M. I. H. Gho et al., PLOS ONE Journal, licensed under CC BY 4.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
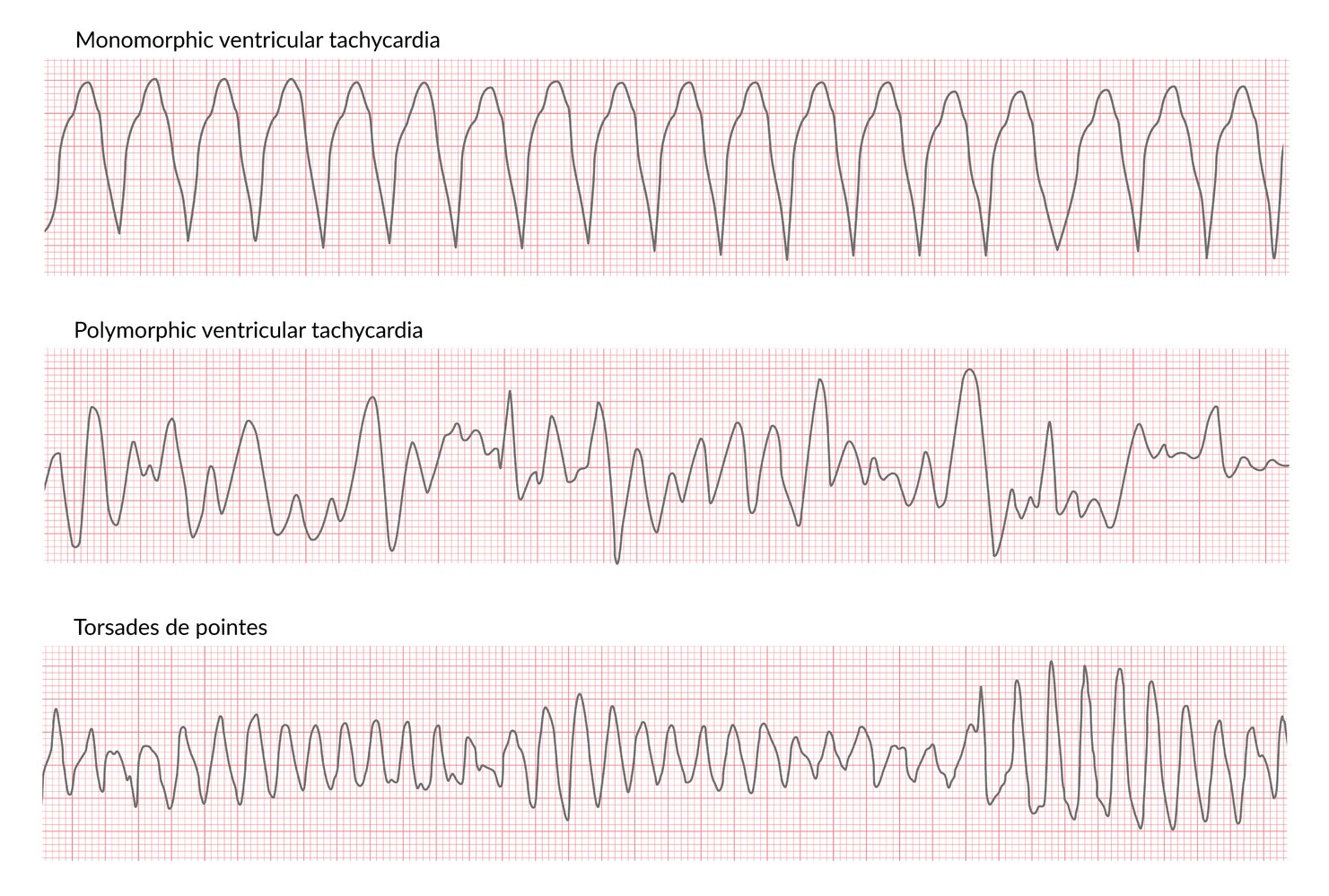
Monomorphic VT: QRS morphology is similar throughout, indicating a single arrhythmogenic focus.
Polymorphic VT: QRS morphology varies, indicating multiple arrhythmogenic foci.
Torsades de pointes is a subtype of polymorphic VT occurring in patients with QT prolongation, in which the QRS complexes appear to twist around the isoelectric line.
© AMBOSS
Unclassified cardiomyopathies
Left ventricular noncompaction [7]
- Definition: rare inherited cardiomyopathy which is associated with structural abnormalities of the left ventricular myocardium (prominent trabeculations and deep intertrabecular recesses)
-
Clinical findings
- Signs of heart failure and arrhythmia (e.g., dyspnea, edema, chest pain, palpitations, syncope)
- Thromboembolisms
- Diagnostics: echocardiography and/or cardiac MRI: LV wall thickening, prominent trabecular meshwork, detection of abnormal flow (within the deep intertrabecular recesses)
-
Treatment: no causal treatment available
- Avoid intense physical exertion
- Symptomatic treatment of complications (e.g., heart failure)
- Prevention of thromboembolism
- AICD
- Heart transplant
- Family and genetic counseling
Arrhythmia-induced cardiomyopathy [8][9]
- Definition: recurring or persistent atrial or ventricular arrhythmias causing structural cardiac changes and left ventricular dysfunction (potentially reversible)
-
Etiology
- Supraventricular tachyarrhythmias (i.e., tachycardia, atrial fibrillation, atrial flutter, supraventricular reentry tachycardia)
- Ventricular tachyarrhythmia (less commonly than supraventricular tachyarrhythmias)
- Atrial or ventricular ectopy (with or without tachycardia)
-
Clinical features
- Signs of underlying arrhythmia (e.g., palpitations, syncope)
- Signs of left heart failure (e.g., dyspnea, chest pain, pulmonary edema)
-
Diagnostics
- ECG: tachyarrhythmia, ectopic foci
- Cardiac monitoring (e.g., Holter monitor)
- Echocardiography and/or cardiac MRI: to evaluate cardiac structure and function (e.g., LVEF measurement)
- To exclude other causes (e.g., coronary heart disease via coronary angiography)
-
Treatment
- Beta blockers: management of CHF, rate control in tachyarrhythmias
- Antiarrhythmics (e.g., amiodarone): rhythm control in tachyarrhythmias
- Catheter ablation: rhythm control in tachyarrhythmias, ectopic foci
References
- William J McKenna, MD. "Arrhythmogenic right ventricular cardiomyopathy: Anatomy, histology, and clinical manifestations". UpToDate. UpToDate. https://www.uptodate.com/contents/arrhythmogenic-right-ventricular-cardiomyopathy-anatomy-histology-and-clinical-manifestations. [2019-06-06]
- William J McKenna, MD. "Arrhythmogenic right ventricular cardiomyopathy: Pathogenesis and genetics". UpToDate. UpToDate. https://www.uptodate.com/contents/arrhythmogenic-right-ventricular-cardiomyopathy-pathogenesis-and-genetics. [2019-06-06]
- "Arrhythmogenic Right Ventricular Dysplasia (ARVD)". https://emedicine.medscape.com/article/163856-overview#a4. [2014-09-14]
- William J McKenna, MD. "Arrhythmogenic right ventricular cardiomyopathy: Treatment and prognosis". UpToDate. UpToDate. https://www.uptodate.com/contents/arrhythmogenic-right-ventricular-cardiomyopathy-treatment-and-prognosis. [2019-06-06]
- Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. "2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary". Circulation. 138(13). :e210–e271. (2018)
- Arman Arghami, Joseph A. Dearani, Sameh M. Said, Patrick W. O’Leary, and Hartzell V. Schaff. "Hypertrophic cardiomyopathy in children". Annals of Cardiothoracic Surgery. (2017)
- Connolly HM, Attenhofer-Jost CH. "Isolated left ventricular noncompaction". UpToDate. UpToDate. https://www.uptodate.com/contents/isolated-left-ventricular-noncompaction. [2016-09-12]
- Tracy CM. "Arrhythmia-induced cardiomyopathy". UpToDate. UpToDate. https://www.uptodate.com/contents/arrhythmia-induced-cardiomyopathy. [2016-07-06]
- Gopinathannair R, Etheridge SP, Marchlinski FE, et al. "Arrhythmia-Induced Cardiomyopathies Mechanisms, Recognition, and Management". J Am Coll Cardiol. 66(15). :1714-1728. (2015)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Agabegi SS, Agabegi ED. "Step-Up To Medicine". Wolters Kluwer Health. (2015). ISBN: 9781496306142
- Le T, Bhushan V, Chen V, King M. "First Aid for the USMLE Step 2 CK". McGraw-Hill Education. (2015). ISBN: 9780071844574
- Le T, Bhushan V, Bagga HS. "First Aid for the USMLE Step 2 CK". McGraw-Hill Medical. (2009). ISBN: 9780071623544
- Fischer C. "Master the Boards USMLE Step 2 CK". Kaplan Publishing. (2015). ISBN: 9781506207285
- Elliott PM, Anastasakis A, Borger MA et al. "2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC) ". Eur Heart J. 35(39). :2733-2779. (2014)
- Maron MS. "Patient education: Hypertrophic cardiomyopathy (Beyond the Basics)". UpToDate. UpToDate. http://www.uptodate.com/contents/hypertrophic-cardiomyopathy-beyond-the-basics. [2015-11-18]
- Gersh BJ, Maron BJ, Bonow RO et al. "2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy : A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines ". J Thorac Cardiovasc Surg. 142(6). :e153-203. (2011)
- "Hypertrophic Cardiomyopathy". http://www.heart.org/HEARTORG/Conditions/More/Cardiomyopathy/Hypertrophic-Cardiomyopathy_UCM_444317_Article.jsp#.WKreI7bhC8p. [2016-07-06]
- Cisneros S, Duarte R, Fernandez-perez GC, et al. "Left ventricular apical diseases". Insights Imaging. 2(4). :471-482. (2011)
- Le T, Bhushan V, Sochat M, Chavda Y, Zureick A. "First Aid for the USMLE Step 1 2018". McGraw-Hill Medical. (2017). ISBN: 1260116123
- Van Diepen S, Katz JN, Albert NM, et al. "Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association". Circulation. 136(16). (2017)
- Nishimura RA, Seggewiss H, Schaff HV. "Hypertrophic Obstructive Cardiomyopathy". Circ Res. 121(7). :771-783. (2017)
- Maron MS, Hauser TH, Dubrow E, et al. "Right Ventricular Involvement in Hypertrophic Cardiomyopathy". Am J Cardiol. 100(8). :1293-1298. (2007)
- Christian Prinz, Dr. med., Martin Farr, et al. "The Diagnosis and Treatment of Hypertrophic Cardiomyopathy". Deutsches Ärzteblatt. (2011)
- Martin S. Maron, MD; Ethan J. Rowin, MD; Barry J. Maron, MD. "How to Image Hypertrophic Cardiomyopathy". Circulation: Cardiovascular Imaging. (2017)
- Dr. Irena Peovska Mitevksa. "Focus on echocardiography in hypertrophic cardiomyopathy - fourth in series". ESC Council for Cardiology Practice. (2015)
- Veselka J, Anavekar NS, Charron P. "Hypertrophic obstructive cardiomyopathy". Lancet. 389(10075). :1253-1267. (2017)
- "Diagnosis of Hypertrophic Cardiomyopathy: What Every Cardiologist Needs to Know". https://www.acc.org/latest-in-cardiology/articles/2020/02/25/06/34/diagnosis-of-hypertrophic-cardiomyopathy. [2020-02-27]
- Lee PT, Dweck MR, Prasher S, et al. "Left Ventricular Wall Thickness and the Presence of Asymmetric Hypertrophy in Healthy Young Army Recruits". Circulation: Cardiovascular Imaging. 6(2). :262-267. (2013)
- Afonso LC, Bernal J, Bax JJ, Abraham TP. "Echocardiography in Hypertrophic Cardiomyopathy". J Am Coll Cardiol Img. 1(6). :787-800. (2008)
- Maron BJ. "Clinical Course and Management of Hypertrophic Cardiomyopathy". N Engl J Med. 379(7). :655-668. (2018)
- Ammirati E, Contri R, Coppini R, et al. "Pharmacological treatment of hypertrophic cardiomyopathy: current practice and novel perspectives". European Journal of Heart Failure. 18(9). :1106-1118. (2016)
- Sherrid MV, Barac I, McKenna WJ, et al. "Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy". J Am Coll Cardiol. 45(8). :1251-1258. (2005)
- Houston BA, Stevens GR. "Hypertrophic cardiomyopathy: a review.". Clin Med Insights Cardiol. 8(Suppl 1). :53-65. (2014)