CME information and disclosures
To see contributor disclosures related to this article, hover over this reference: [1]
Physicians may earn CME/MOC credit by reading information in this article to address a clinical question, and then completing a brief evaluation, in which they will identify their question and report the impact of any information learned on their clinical practice.
AMBOSS designates this Internet point-of-care activity for a maximum of 0.5 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For answers to questions about AMBOSS CME, including how to redeem CME/MOC credit, see "Tips and Links" at the bottom of this article.
Summary
Critically ill patients are typically cared for in intensive care units (ICUs), which are designated hospital units dedicated to managing patients who require a higher level of care than that available on a general medical ward or step down unit, staffed by highly trained clinicians. After initial resuscitation and stabilization, management of ICU patients typically involves ongoing hemodynamic monitoring (often via invasive devices such as an arterial line) and respiratory monitoring (including interpretation of ventilator alarms for mechanically ventilated patients), supportive care of the critically ill patient (including nutrition and metabolic support, analgesia, and sedation), and the prevention of common complications (e.g., VTEs, pressure ulcers, nosocomial infections, delirium). Predictive scoring systems (e.g., the SOFA score, APACHE II score) may be useful for the prognostication of ICU patients. Given the critical nature of ICU care, teamwork and communication, and end-of-life care are essential. Typical reasons for admission to an ICU include the need for organ support (e.g., for patients with brain injury, acute coronary syndrome, COPD exacerbation, sepsis, GI bleeding) and/or close, continuous monitoring (e.g., postoperatively or while receiving a high-risk medication).
Definitions
- Critical illness: a state of poor health with vital organ dysfunction and/or imminent death [2]
- Critical care: provision of medical care to critically ill patients by supporting vital organ function [2]
-
Intensive care units
- Units that provide the highest level of care available in a hospital
- Can be open or closed
- Can be general medical or surgical, or specialized units (e.g., neurological, cardiac)
- Indicated for patients who require close or continuous monitoring:
- While receiving (or in imminent need of) organ support: e.g., mechanical ventilation, vasopressors, extracorporeal therapies
- During treatment for severe illness, often with continuous IV infusions (see “Common conditions treated in the ICU”)
- Immediately post-surgery or post-procedure
- Units that provide the highest level of care available in a hospital
- Intermediate care units: units that provide a higher level of care than a general ward but a lower level of care than an ICU
There are no established general criteria for ICU admission. The decision to admit a patient typically relies on the clinical judgment of the physician and the availability of beds and resources.
Resuscitation and stabilization
The first step in caring for critically ill patients is resuscitation and stabilization. See also “ABCDE approach” for more detail.
Hemodynamic support
- Establish a route of access for parenteral fluid therapy and medications.
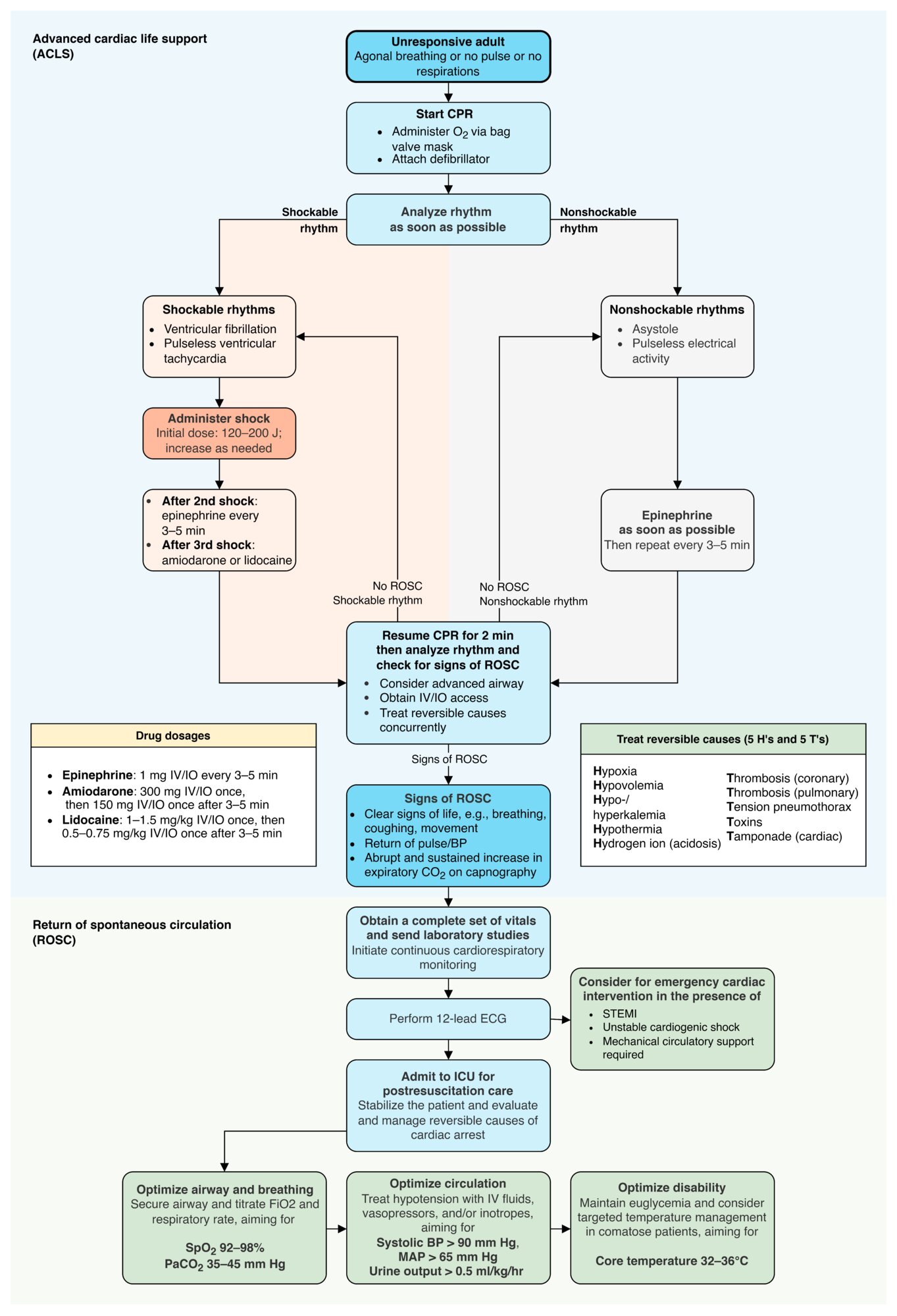
- Provide advanced cardiac life support if cardiac arrest is present.
- Evaluate and treat for any clinical features of shock.
- Provide immediate hemodynamic support for undifferentiated shock.
- Perform appropriate diagnostics in shock.
- Consider mechanical circulatory support in patients with refractory cardiogenic shock.
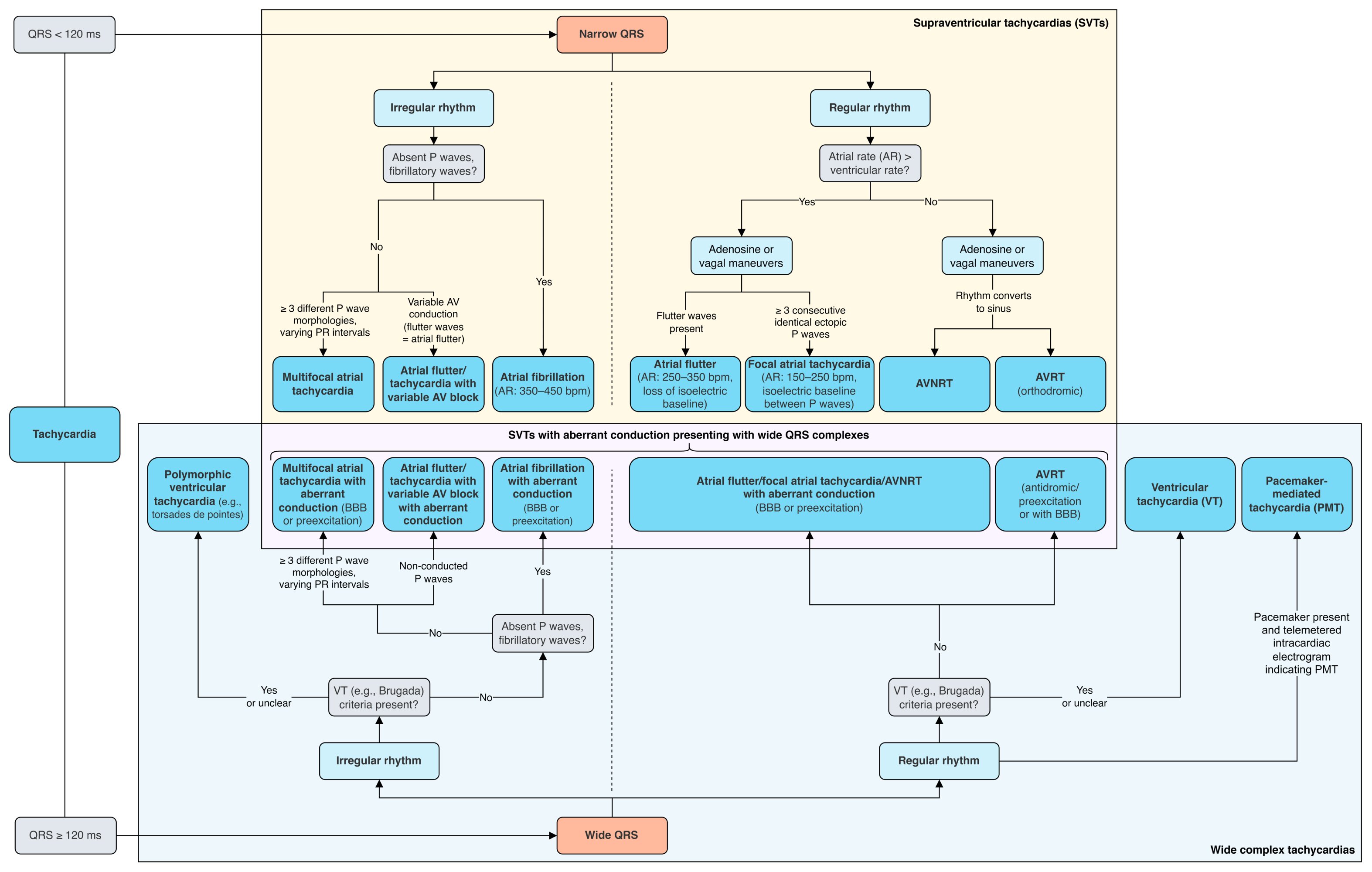
- Evaluate and treat any arrhythmias.
- Management of tachycardia
- Management of bradycardia
")


Respiratory support
See also “Management of respiratory failure.”
- Identify airway obstruction and perform basic airway maneuvers.
- Start oxygen therapy (if applicable) via one of the following:
- Basic oxygen delivery systems
- High-flow nasal cannula
- Noninvasive positive-pressure ventilation
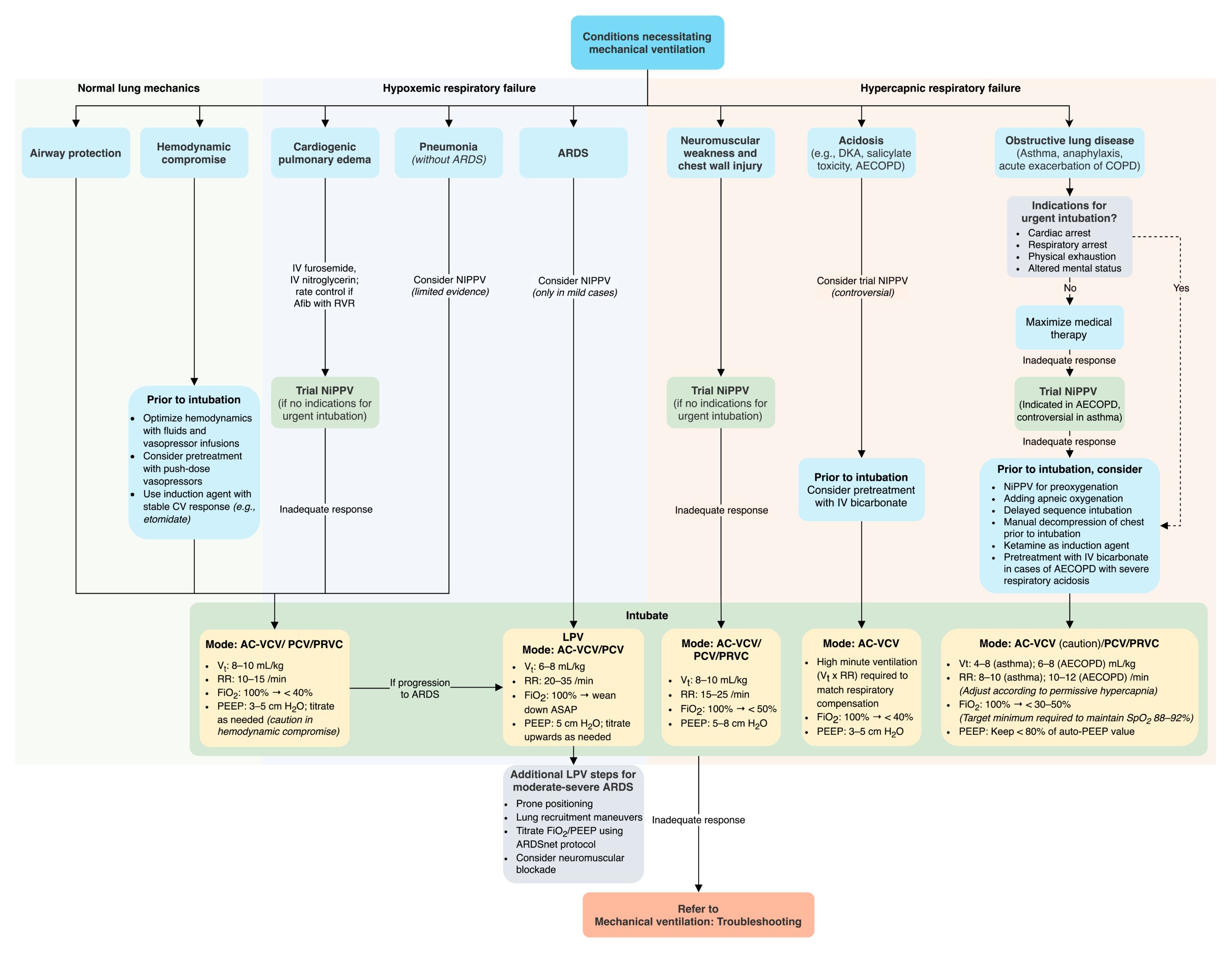
- If indications for invasive mechanical ventilation are present:
- Prepare for and perform endotracheal intubation.
- Start invasive mechanical ventilation.
- Select the appropriate ventilator settings and ventilator strategies.
- Start sedation (see “Adjunctive care of the ventilated patient”).
- Anticipate and manage complications of intubation.

Extracorporeal membrane oxygenation (ECMO)
- Consider use in patients who require advanced respiratory and/or circulatory support
- VA-ECMO: provides respiratory and circulatory support
- VV-ECMO: provides respiratory support only
")


© AMBOSS
© AMBOSS
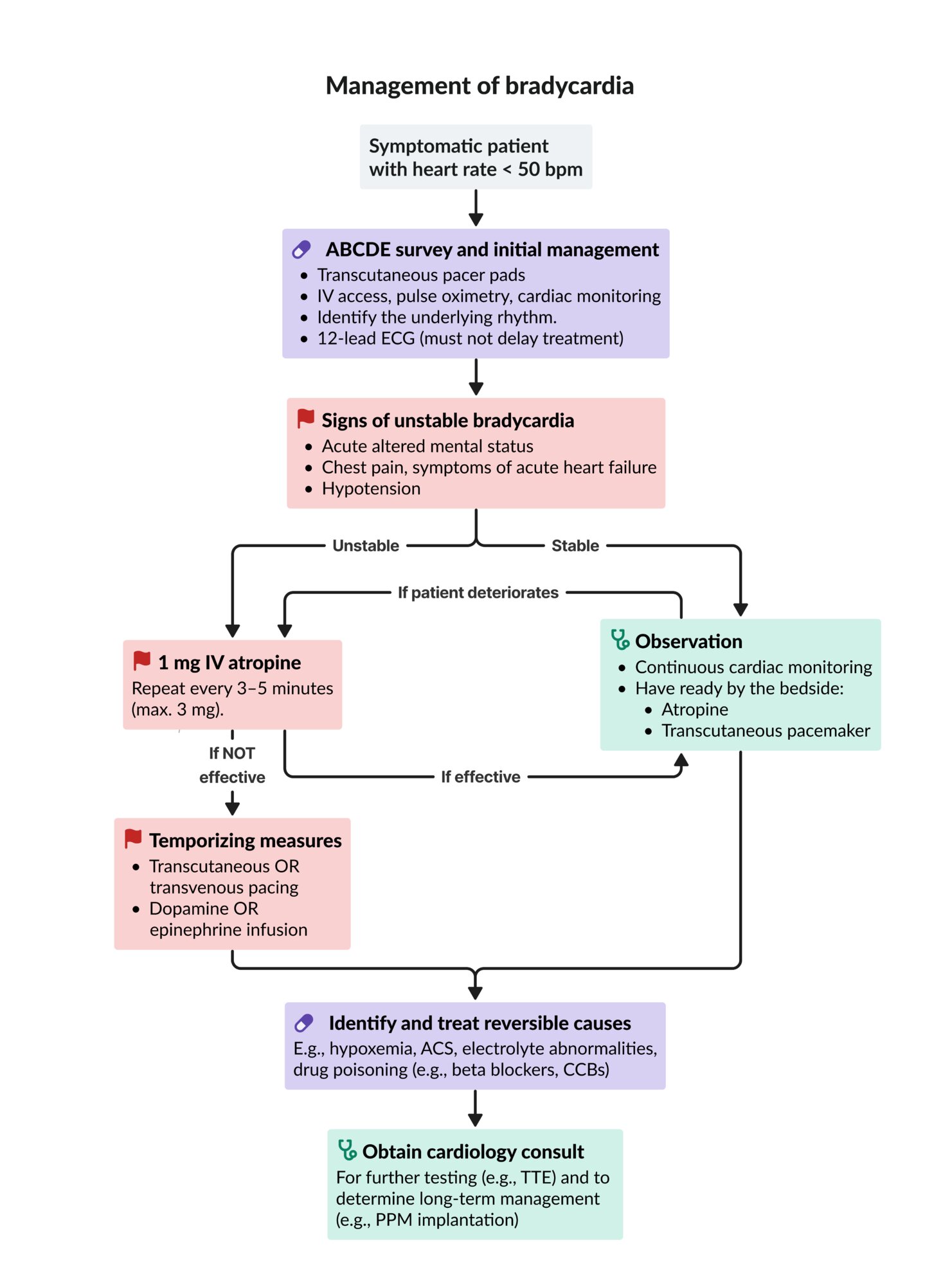
ACS: acute coronary syndrome
CCBs: calcium channel blockers
ECG: electrocardiogram
IV: intravenous
PPM: permanent pacemaker
TTE: transthoracic echocardiography
© AMBOSS
© AMBOSS

The centrifugal pump (P) draws deoxygenated blood from the patient's circulation and through the ECMO circuit, where the oxygenator (O) decarboxylates and oxygenates the blood before it is returned to the patient's circulation. The support system (S) controls gas exchange. The heat exchanger (W) ensures a consistent temperature of the extracorporeal circulation.
Source: "ECMO in H1N1 patient in Santa Cruz Hospital - Lisbon", Cmenesesoliveira, Wikimedia Commons licensed under Public Domain
{kind=link}
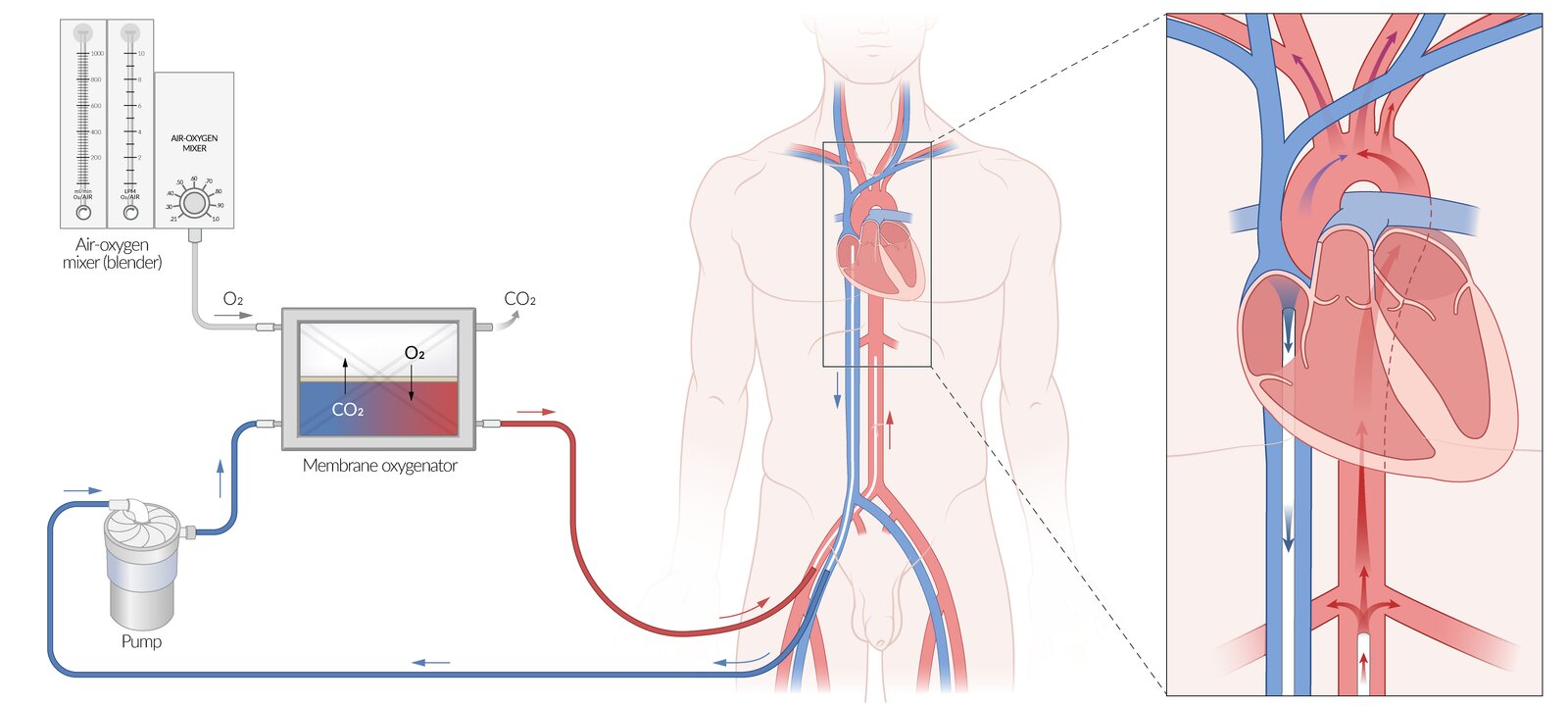
Illustration of peripheral cannulation using the femoral vein and femoral artery; other access techniques may be used
Deoxygenated blood is removed from the right atrium and returned to the descending aorta after oxygenation in a retrograde direction. If the heart is not beating and there is no residual cardiac output, this retrograde flow will reach as far back as the closed aortic valve, and the extracorporeal membrane oxygenation (ECMO) system will provide all of the patient's circulation. If there is remaining physiological output from the left ventricle, the two flows meet and create a “mixing cloud” of poorly oxygenated blood from the native circulation and well-oxygenated blood from the ECMO circuit.
The mixing cloud depicted here is in the aortic arch (where red and blue arrows meet). It may, however, be located anywhere between the aortic valve and the ECMO cannula tip and shift depending on changes in left ventricular output and ECMO blood flow. The location of the mixing cloud influences the oxygen content of the blood reaching the various aortic branches. In this example, while the renal arteries receive well-oxygenated blood from the ECMO circuit (red arrows), the carotid and subclavian arteries receive more poorly oxygenated blood from the mixing cloud (purple arrows).
© AMBOSS
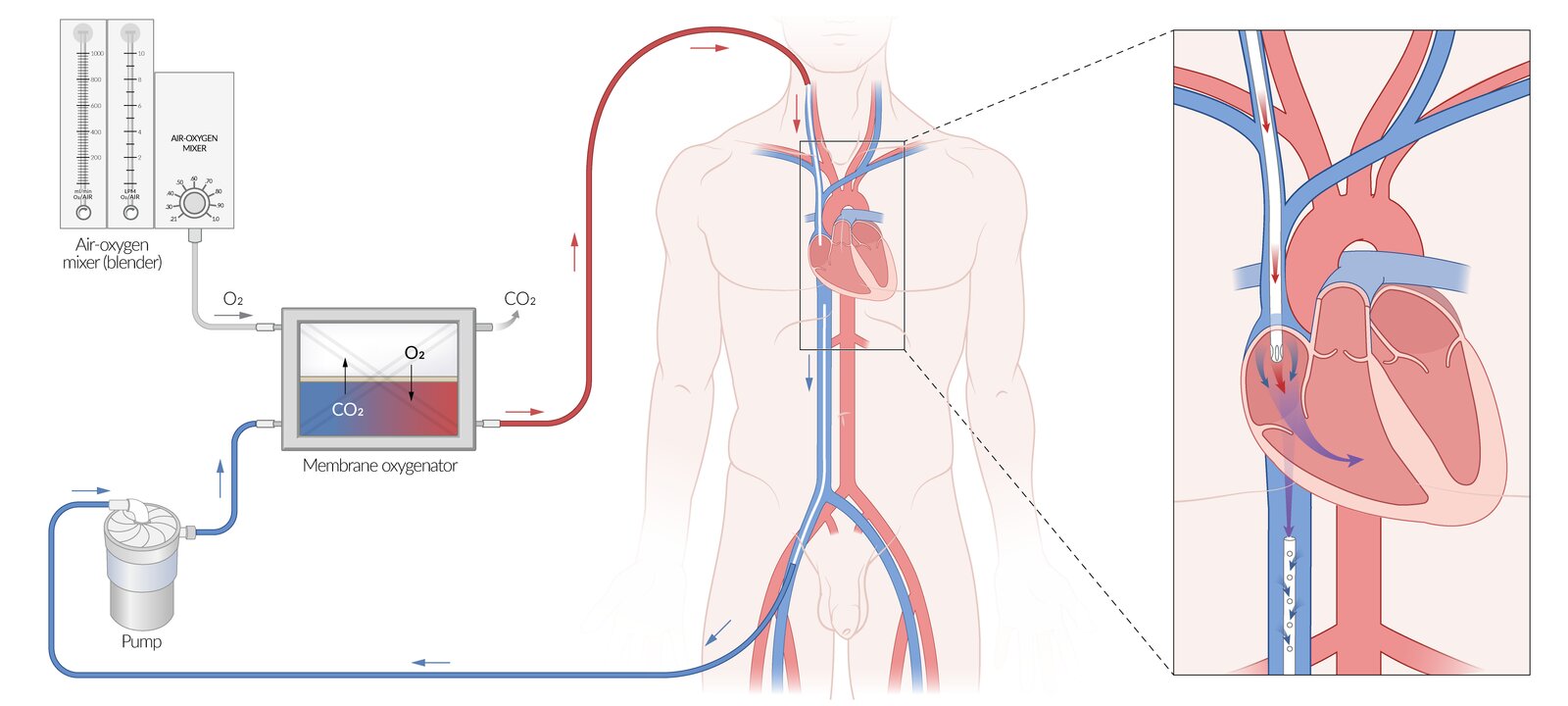
Extracorporeal membrane oxygenation (ECMO) is an advanced life support method in which a bypass system circulates the patient's blood through artificial gas exchange membranes.
This illustration shows venovenous ECMO (VV-ECMO), which supports respiratory function only and is used in patients with preserved circulatory function. VV-ECMO may be used, e.g., as a rescue treatment for patients with acute respiratory failure or as a bridge to lung transplantation.
Peripheral cannulation using the femoral vein and internal jugular vein is depicted here, but other access techniques may be used. Deoxygenated blood is removed from the inferior vena cava and returned to the right atrium after oxygenation. Circulation relies on the patient's own cardiac function.
© AMBOSS
Monitoring parameters
All critically ill patients require close monitoring of hemodynamic and respiratory status.
Hemodynamic monitoring
- Follow relevant monitoring parameters for parenteral fluid therapy.
- Follow relevant monitoring parameters for patients with shock.
Invasive devices
- Arterial line: used to accurately measure blood pressure
- Central venous catheter : used to measure central venous pressure
-
Pulmonary artery catheterization
- Not routinely recommended for hemodynamic monitoring
- Consider for specific cases, including: [3][4]
- Refractory shock: especially in patients with ARDS or right ventricular dysfunction
- Undifferentiated shock: especially if there is uncertainty about the fluid status of patients at very high risk of pulmonary edema
Routine pulmonary artery catheterization for hemodynamic monitoring has not been shown to improve outcomes in critically ill patients with shock and, therefore, should only be used in specific cases. [3][4]
")

Respiratory monitoring
- Conduct appropriate monitoring of mechanically ventilated patients.
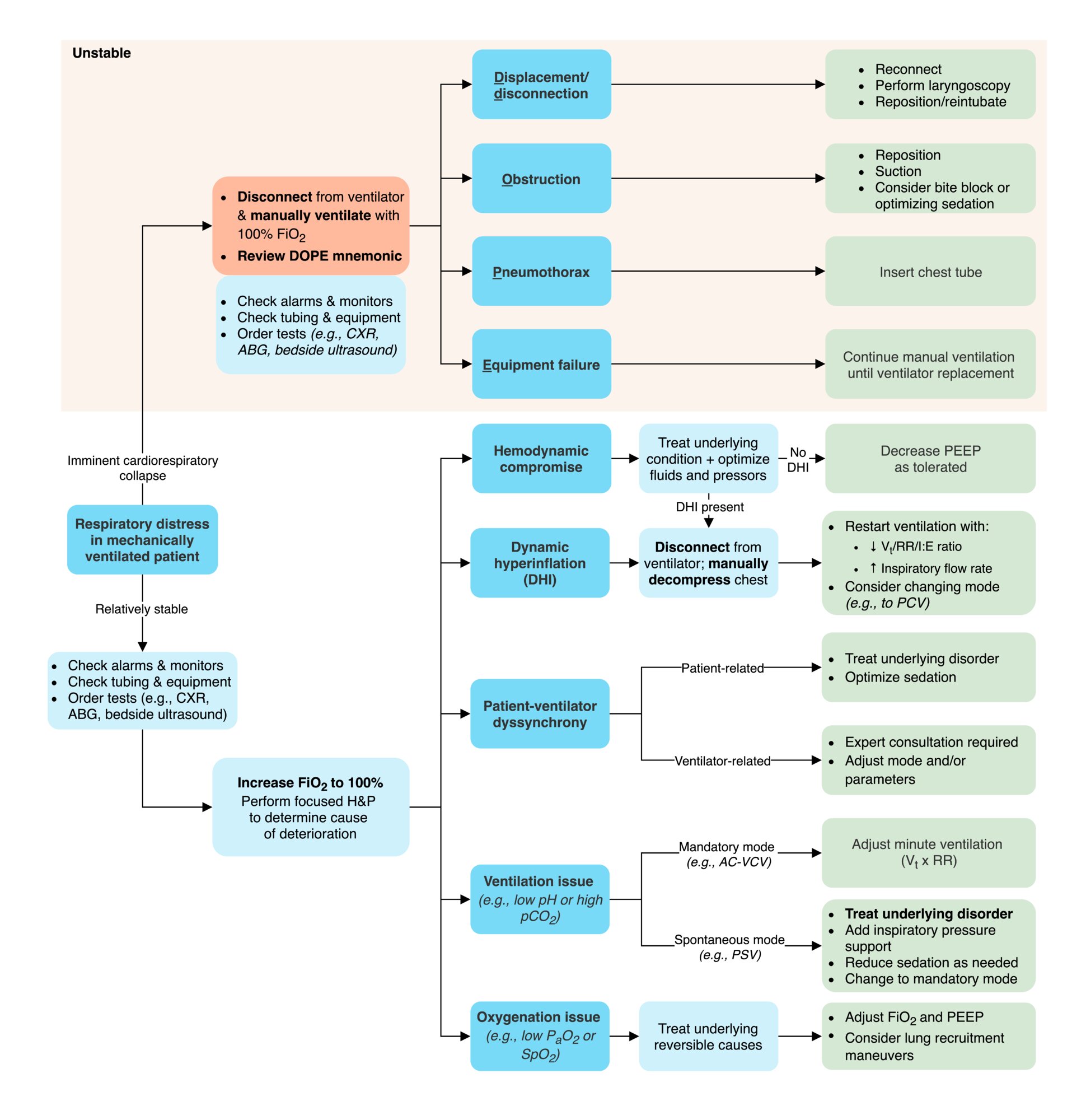
- For patients who are deteriorating (or in respiratory distress), simultaneously: [5]
- Conduct initial maneuvers ; see also “Troubleshooting of mechanical ventilation.”
- Try to identify the underlying cause: See “Interpretation of ventilator alarms.”
Consider using the DOTTS mnemonic to remember the interventions in a mechanically ventilated patient who is deteriorating: Disconnect, Oxygenate, assess the Tube position and function, Tweak ventilator settings, and perform a chest Sonogram (e.g., to identify pneumothorax). [5]



Triple lumen central line in situ
The catheter was advanced via the right internal jugular vein into the vena cava and fixed to the skin with stitches tied to each perforation lateral to the suture wings. The CVC site is protected with a transparent dressing. All three lumens have colored plug connectors to identify the different lumen sizes. The lumens can be closed with clamps. The white lumen is connected to a delivery line and the clamp is open. The brown and blue lumens were sealed with Luer-lock obturator caps. Their clamps are closed.
Source: "Triple-Lumen", Jsonp, Wikimedia Commons licensed under Public Domain
{kind=link}
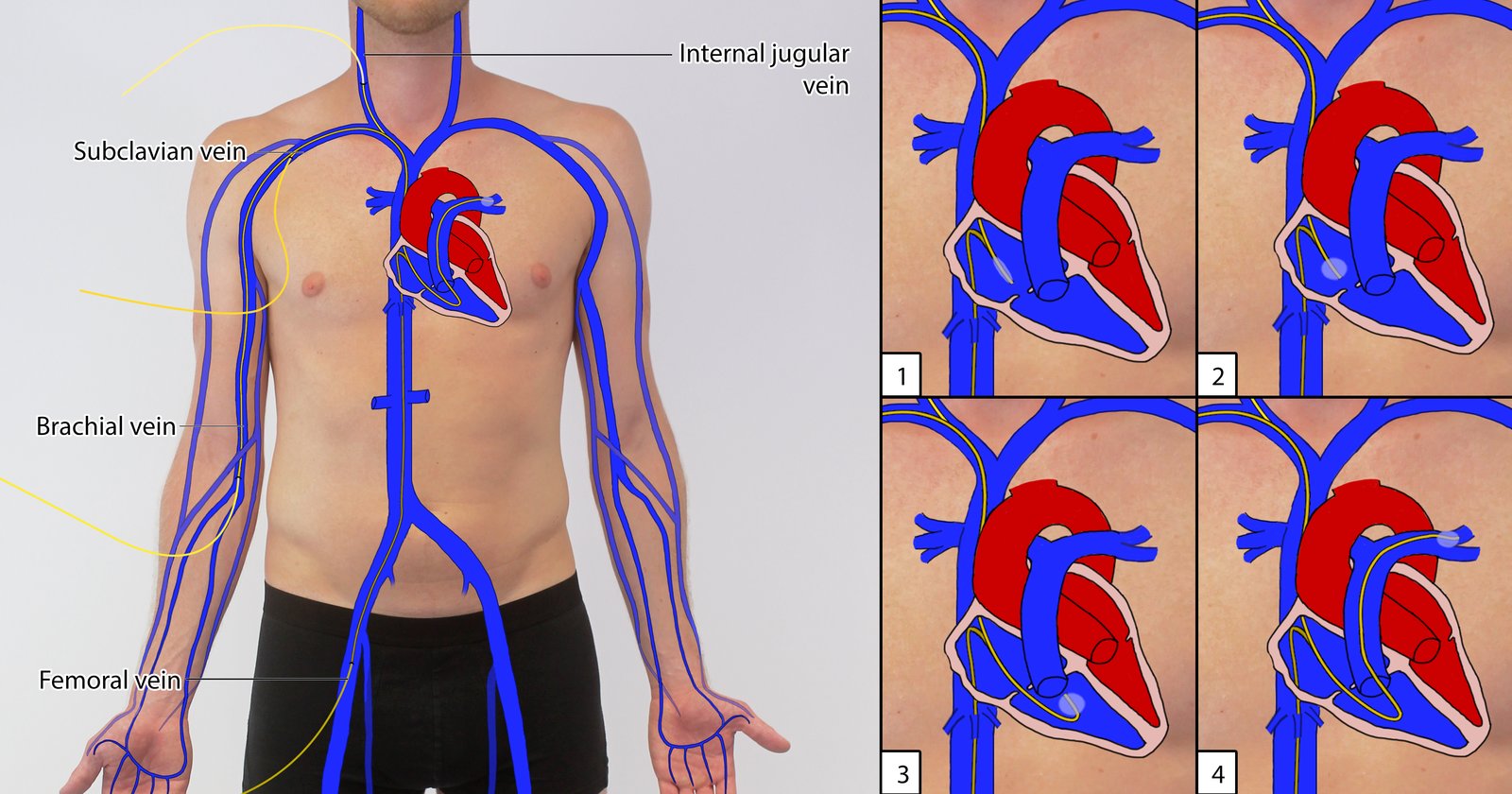
Suitable IV access is achieved with Seldinger's technique (most common sites shown in the image). A balloon-tipped, multi-lumen catheter (Swan-Ganz catheter) is introduced into the body and moved to the right atrium (1). Next, the balloon is inflated (2). The catheter is now pushed forward along the blood flow through the right ventricle (3) to a pulmonary artery, which it blocks (4).
© AMBOSS
© AMBOSS
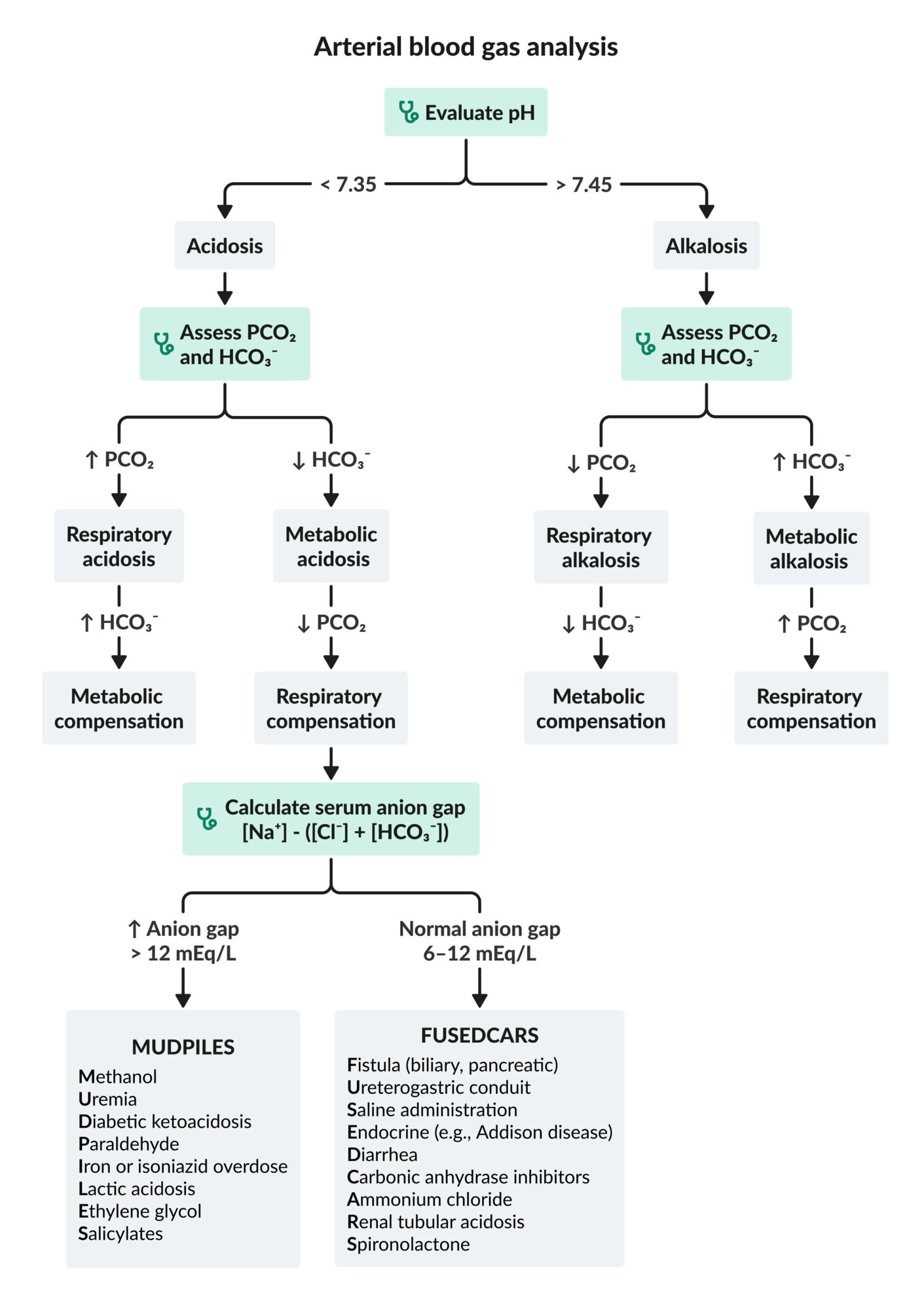
This algorithm does not account for mixed acid-base disorders.
Cl-: chloride
HCO3-: bicarbonate
Na+: sodium
PCO2: partial pressure of carbon dioxide
© AMBOSS
Supportive care
Management should be individualized for each patient, but there are some common features of supportive care in critically ill patients.
Critically ill patients need FAST HUGS DAILy: every day, evaluate their Feeding and fluids, Analgesia, Sedation, Thromboembolic prevention, Head of the bed elevation, Ulcer prophylaxis, Glucose control, Skin pressure ulcer prophylaxis, Deescalation of drugs, Assessment of delirium, Indwelling catheters, Last bowel movement. [6]
Nutrition and metabolic support of critically ill patients [6][7][8]
-
Specialized nutrition support (when oral intake is not possible)
- Start within 24–48 hours of ICU admission.
- Can be enteral nutrition (preferred) or parenteral nutrition
-
IV fluid therapy
- Adjust strategies for parenteral fluid therapy based on the patient's needs.
- Monitor and evaluate parenteral fluid therapy daily.
-
Metabolic support
- Glycemic control:
- Provide inpatient management of hyperglycemia. [9]
- Treat hypoglycemia, if present.
- Provide electrolyte repletion.
- Consider the need for stress-dose steroids to prevent acute adrenal insufficiency (i.e., critical illness-related corticosteroid insufficiency).
- Glycemic control:
Enteral nutrition is associated with fewer metabolic complications and bloodstream infections and better patient outcomes compared to parenteral nutrition. [6]
Pain management in critically ill patients [10]
-
Evaluate pain using validated scales such as:
- Behavioral pain scale
- Critical care pain observation tool
-
Individualize the acute pain management approach.
- Timing: e.g., continuous infusions or interval dosing [11][12]
- Pain type: e.g., nociceptive pain, neuropathic pain.
- Contraindications and adverse effects
Sedation [8][10]
- Choose an appropriate agent: For agents and dosages, see “Adjunctive care of the ventilated patient.”
-
Monitor sedation levels. [8]
- Use the Richmond Agitation-Sedation Scale (RASS).
- Light sedation is generally recommended instead of deeper sedation . [10]
- For mechanically ventilated patients: See “Adjunctive care of ventilated patients”
-
Reevaluate sedation indications: Consider regular breaks from sedation. [8]
- Spontaneous awakening trials
- Spontaneous breathing trials
Prevention of complications [6][7][8]
Prevention of complications is paramount to minimizing harm and improving outcomes.
| Prevention of complications in ICU patients | |
|---|---|
| Complication | Prevention strategy |
| VTE prophylaxis |
|
| Stress ulcer prophylaxis |
|
| Decubitus ulcer prophylaxis |
|
| Nosocomial infections |
|
| Delirium |
|
| Medication adverse effects |
|
| ICU-acquired weakness |
|
Prevent delirium in critically ill patients using the ABCDEF bundle: Assessment of pain, Both spontaneous awakening trials and spontaneous breathing trials, Choice of analgesia and sedation, Delirium screening, Early mobilization, Family engagement. [8]
The use of lorazepam or diazepam for sedation may cause iatrogenic propylene glycol poisoning, as both drugs are dissolved in propylene glycol. Midazolam is an alternative benzodiazepine that does not use propylene glycol as a solvent. [15]
Predictive scoring systems
Scoring systems can give a general sense of prognosis but they should not be the sole factor used to determine the level of care required or if a patient should be moved to a lower level of care.
Sequential organ failure assessment score (SOFA score) [16][17]
- Used in critical care settings as a tool to identify organ failure and predict mortality
- The score should be calculated 24 hours after ICU admission and then every 48 hours.
- Commonly used to assess mortality risk in patients with sepsis
| SOFA score [16][18] | |||||
|---|---|---|---|---|---|
| System | 0 points | 1 point | 2 points | 3 points | 4 points |
| Respiration PaO2:FiO2 ratio (mm Hg) |
|
|
|
|
|
| Coagulation Platelets (x 1000/mm3) |
|
|
|
|
|
| Liver Bilirubin (mg/dL) |
|
|
|
|
|
| Cardiovascular |
|
|
|
|
|
| Central nervous system Glasgow coma scale score |
|
|
|
|
|
| Renal function Creatinine (mg/dL) |
|
|
|
|
|
Interpretation
| |||||
 Score")
Acute physiology and chronic health evaluation II (APACHE II score)
The APACHE II score should be calculated within the first 24 hours of ICU admission. [19][20]
-
Components
- Physiological score
- Age score
- Chronic health score
- Result: an estimate of the patient's in-hospital mortality risk
-
Potential limitations
- Generalizability
- Accuracy
Additional scoring systems for specific conditions
Commonly used scoring systems for specific conditions include:
- Pneumonia: PSI/PORT score (estimates mortality risk)
- Pancreatitis: Ranson criteria (estimates mortality risk)
- Cirrhosis: MELD score, Child-Pugh score (estimate mortality risk)
- Upper GI bleeding: Glasgow-Blatchford bleeding score (estimates risk of requiring intervention)
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
End-of-life considerations
End-of-life considerations should be addressed for all patients upon admission to the ICU. Essential tasks include establishing a decision-maker, confirming advance directives, and considering the need for a palliative care consult.
-
Decision-making
- Evaluate the decision-making capacity and legal competence of the patient.
- Identify an appropriate surrogate decision-maker, if necessary.
- Confirm advance directives regarding all end-of-life care for the patient.
-
Palliative care
- Provide appropriate palliative pain control.
- Other management as necessary, e.g.:
- Palliative pharmacotherapy for dyspnea
- Management of delirium in palliative care
- Palliative anxiolysis
-
Death and dying
- Follow recommendations for the management of imminently dying patients.
- Follow the process for pronouncing death or brain death (if relevant).
-
Document patient death (adhere to institutional protocols).
- Determine whether the situation falls under reportable types of death.
- Confirm plans for an autopsy.
Addressing family and friends after death should be prioritized.
Teamwork and communication
An essential part of ICU care is ensuring appropriate communication with the following people. See also “Key principles of communication and counseling.”
-
Patients and family:
- Update the patient's family regularly (by phone if the family are not at the bedside).
- Communicate in an empathic, patient-centered way.
- Elicit the patient's and family's needs and wants.
- See also “Breaking bad news.”
- Nonphysician team members: See “Communicating with nonphysician team members.”
-
Other physicians
- Update consultants and other team physicians regularly throughout the day.
- If a patient begins to deteriorate, do not hesitate to request help immediately.
- Ensure you provide a focused and constructive signout.
Common conditions treated in the ICU
| Common ICU conditions by system | |
|---|---|
| System | Management |
| Neurological |
|
| Cardiovascular |
|
| Pulmonary |
|
| Infectious disease |
|
| Gastrointestinal |
|
| Renal |
|
| Endocrine |
|
| Hematologic |
|
| Oncologic |
|
Management checklists
This section provides checklists for managing the major aspects of patient care over the course of an ICU admission. The following checklists may serve as general guidance but may not be applicable to all patients and/or settings; follow institutional protocols.
Admission checklist
- Review electronic medical records for the following (before admission if possible):
- Medical history and current medication list
- Emergency department course
- Microbiology
- Previous advance directives
- Immediately upon admission:
- Note current vital signs.
- Resuscitate and stabilize the patient as necessary.
- Place any urgent orders.
- Perform a focused history and examination. If the patient has the capacity:
- Confirm home medications.
- Address end-of-life considerations (see “End-of-life considerations” in “General principles of ICU care”).
- Ask for permission to update a family member and obtain relevant contact information.
- Place admission orders.
- Perform thorough medication reconciliation.
- Use standard admission order sets.
- Include any laboratory studies and/or imaging to be performed overnight or the next morning.
- Write an admission note and make sure to document the following:
- General prognostic score (e.g., APACHE II, SOFA score)
- Scores relevant to the patient's reason for admission (e.g., PSI for pneumonia)
- Wishes regarding advance directives (and complete any relevant forms)
- Update family members if appropriate.
- Update signout template (see “Signout checklist”).
Daily care checklist
- Obtain signout from the overnight resident.
- Review the following:
- New recommendations from consultants
- Overnight events and orders placed
- Vital signs
- Intake-output monitoring over the past 24 hours
- Laboratory studies and microbiology
- Imaging
- Telemetry (if applicable)
- Assess the patient at the bedside.
- Check monitors and note current vital signs and ventilator settings.
- Perform a focused examination, including an assessment of:
- Neurological status (e.g., RASS score, pupils, reflexes)
- Volume status
- Check all current lines, tubes, and catheters.
- Check the rate of all current IV infusions.
- Coordinate with respiratory therapy and nurses to perform a spontaneous breathing trial or spontaneous awakening trial if appropriate.
- Check and place orders for supportive care of the critically ill patient.
- Update the patient's family (by phone if not present at the bedside).
- Update signout template.
Signout checklist
Due to the complexity of ICU patients, a signout template with the following information for each patient is usually maintained and updated daily by each physician. A verbal signout should also be performed, highlighting the most relevant information. It is often helpful to sign out while walking around the unit to briefly check on each patient. The signout should include:
- Overall status: i.e., unstable, deteriorating, stable, or up for transfer
- Reason for admission
- Active issues (e.g., complications) and to-do list
- Current neurological and mental status
- Lines, tubes, and catheters
- Anticipated and potential complications along with contingency plans
- Code status and advance directives
- Contact information for the patient's family
Transfer/discharge checklist
Patients are usually transferred to the general medical floor before being discharged, but some patients may be discharged directly from the ICU or cardiac intensive care unit.
- Begin planning for transfer or discharge.
- Begin ventilator weaning when the patient meets the criteria.
- Deescalate medications (e.g., pressors, sedatives) and IV fluids as appropriate.
- Convert medications from IV to PO form.
- Advance the patient's diet.
- Perform medication reconciliation.
- Write a transfer note (this should be similar to a discharge summary).
- Provide a verbal signout to the accepting service.
- Update the patient's family as appropriate.
Related One-Minute Telegram
- One-Minute Telegram 145-2026-3/3: Less restraint for ventilated ICU patients does not improve outcomes
- One-Minute Telegram 69-2023-1/3: The jury is still out on the best treatment approach to early sepsis
- One-Minute Telegram 54-2022-3/3: Should we rethink resuscitation in septic shock?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Vincent J-L. "Give your patient a fast hug (at least) once a day*". Crit Care Med. 33(6). :1225-1229. (2005)
- Nair AS, Naik VM, Rayani BK. "FAST HUGS BID: Modified Mnemonic for Surgical Patient.". Indian J Crit Care Med. 21(10). :713-714. (2017)
- Marra A, Ely EW, Pandharipande PP, Patel MB. "The ABCDEF Bundle in Critical Care". Crit Care Clin. 33(2). :225-243. (2017)
- Farrokhi F, Smiley D, Umpierrez GE. "Glycemic control in non-diabetic critically ill patients". Best Pract Res Clin Endocrinol Metab. 25(5). :813-824. (2011)
- Devlin JW, Skrobik Y, Gélinas C, et al. "Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU". Crit Care Med. 46(9). :e825-e873. (2018)
- Erstad BL, Puntillo K, Gilbert HC, et al. "Pain Management Principles in the Critically Ill". Chest. 135(4). :1075-1086. (2009)
- Reardon DP, Anger KE, Szumita PM. "Pathophysiology, assessment, and management of pain in critically ill adults". Am J Health Syst Pharm. 72(18). :1531-1543. (2015)
- Consortium for Spinal Cord Medicine.. "Early acute management in adults with spinal cord injury: A clinical practice guideline for health-care professionals.". J Spinal Cord Med. 31(4). :403-79. (2008)
- Bansal C, Scott R, Stewart D, Cockerell CJ. "Decubitus ulcers: A review of the literature". Int J Dermatol. 44(10). :805-810. (2005)
- Devlin JW, Mallow-Corbett S, Riker RR. "Adverse drug events associated with the use of analgesics, sedatives, and antipsychotics in the intensive care unit". Crit Care Med. 38. :S231-S243. (2010)
- Singer M, Deutschman CS, Seymour CW, et al. "The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)". JAMA. 315(8). :801-810. (2016)
- Rhodes A, Evans LE, Alhazzani W, et al. "Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016". Intensive Care Med. 43(3). :304-377. (2017)
- Marik PE, Taeb AM. "SIRS, qSOFA and new sepsis definition". J Thorac Dis. 9(4). :943-945. (2017)
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. "APACHE II: a severity of disease classification system.". Crit Care Med. 13(10). :818-29. (1985)
- Vincent J-L, Moreno R. "Clinical review: Scoring systems in the critically ill". Crit Care. 14(2). :207. (2010)
- Cecconi M, De Backer D, Antonelli M, et al. "Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine". Intensive Care Med. 40(12). :1795-1815. (2014)
- Hunt SA, Abraham WT, et al. "2009 Focused Update Incorporated Into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults". Circulation. 119(14). (2009)
- Przybylo JA, Wittels K, Wilcox SR. "Respiratory Distress in a Patient with a Tracheostomy". J Emerg Med. 56(1). :97-101. (2019)
- "Towards definitions of critical illness and critical care using concept analysis". http://dx.doi.org/10.1101/2022.01.09.22268917. [2022-01-10]
- "Contributor Disclosures - Care of the critically ill patient. All of the relevant financial relationships listed for the following individuals have been mitigated: Alexandra Willis (copyeditor, was previously employed by OPEN Health Communications). None of the other individuals in control of the content for this article reported relevant financial relationships with ineligible companies. For details, please review our full conflict of interest (COI) policy:"