Summary
Celiac disease, also referred to as celiac sprue or nontropical sprue, is a common condition characterized by a maladaptive immune response to gluten, a protein found in many grains (e.g., wheat). The disease often occurs in patients with other autoimmune illnesses, as both are associated with HLA variants (human leukocyte antigens, which encode immunoregulatory proteins) that cause pathologically increased immune responses. The underlying pathophysiology is believed to be a combination of gluten intolerance, which triggers an autoimmune reaction, and production of autoantibodies that target tissue transglutaminase, specifically within the proximal small intestine. Typical findings include changes in bowel habits and symptoms associated with malabsorption (e.g., fatigue, weight loss, vitamin deficiencies). Diagnostic tests include the detection of various antibodies. To confirm the diagnosis, an endoscopic biopsy from the small intestine is needed. Histopathological findings often include villous atrophy and crypt hyperplasia. A definitive diagnosis is necessary, as therapy involves a lifelong commitment to a gluten-free diet. If patients comply with this diet, the prognosis is generally very good and the increased risk of celiac-associated malignancies (e.g., intestinal lymphoma) is mitigated.
Definitions
- Definition: autoimmune disorder characterized by an intestinal hypersensitivity to gluten, a grain protein [1]
- Synonyms: celiac sprue; gluten-sensitive enteropathy
Epidemiology
- Sex: ♀ > ♂
-
Age of onset
- The disease can occur at any age.
- Peak incidence is bimodal:
- At 8–12 months (or 2–3 months following the first exposure to gluten through diet containing wheat)
- Third to fourth decade of life
- Prevalence: in the US ∼ 1:150 [2]
- Race: more common in individuals of northern European descent
Epidemiological data refers to the US, unless otherwise specified.
Etiology
-
Genetic predisposition with association to HLA antigens [3]
- HLA-DQ2 in 90–95% of patients
- HLA-DQ8 in 5–10% of patients
- Consuming gliadin from grains such as wheat, rye, and barley leads to an autoimmune reaction within the small intestinal wall.
- Commonly associated with autoimmune diseases (see “Clinical features” below)
Pathophysiology
Symptoms manifest when a genetically predisposed individual develops an immunological response to gliadin, an alcohol-soluble fraction of gluten.
- Consumption of food containing gluten → tissue transglutaminase is released ; → modifies gliadin from gluten proteins → pathogenic T cells react to and are activated by modified gliadin → mediate chronic intestinal inflammation → epithelial damage resulting in villous atrophy, crypt hyperplasia, and loss of brush border → impaired resorption of nutrients in the small intestine (especially in the distal duodenum and proximal jejunum) → malabsorption symptoms

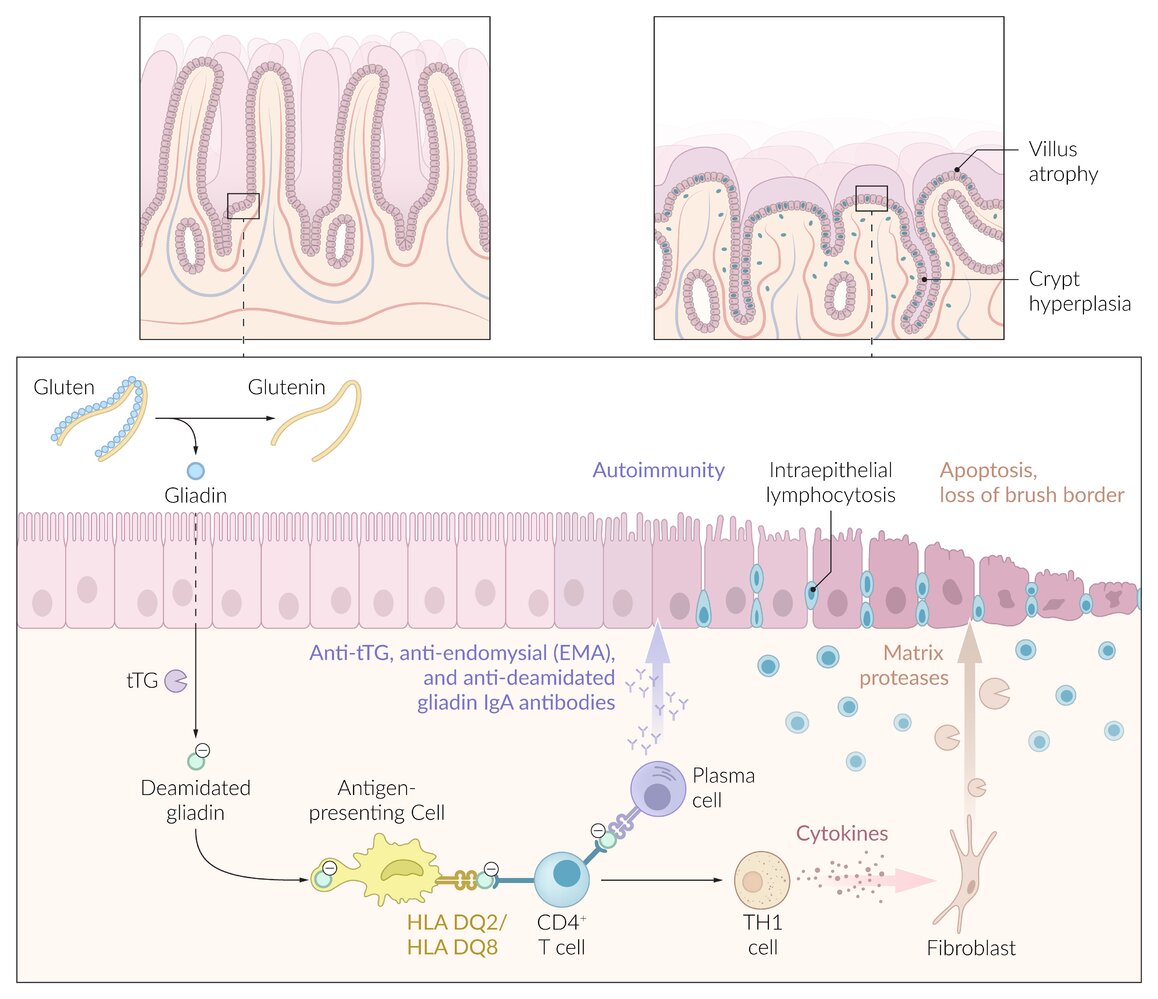
The ingestion of gliadin, a component of gluten, leads to an immune response in the intestinal epithelium in individuals with celiac disease. Gliadin is deamidated by tissue transglutaminase (tTG) and then ingested by antigen-presenting cells (APC), which activate T cells via MHC II receptors. The activated T cell then activates plasma cells to release anti-tTG, anti-endomysial, and anti-deamidated gliadin antibodies (which all function as diagnostic markers of celiac disease). T cells also differentiate into TH1 cells, which activate cytoplasmic fibroblasts to release matrix proteases. This leads to the destruction of the intestinal architecture with villus atrophy, crypt hyperplasia, and the loss of the brush border.
© AMBOSS
Clinical features
Gastrointestinal symptoms
- Chronic or recurring diarrhea
- Steatorrhea
- Flatulence, abdominal bloating, and pain
- Nausea/vomiting
- Lack of appetite
- Constipation (rarely)
Extraintestinal symptoms and associations
- Malabsorption symptoms: fatigue, weight loss, vitamin deficiency, iron deficiency anemia, osteoporosis, hypocalcemia
- In children: failure to thrive, growth failure, delayed puberty, secondary hyperparathyroidism
- Dermatologic associations: dermatitis herpetiformis
- Neuropsychiatric symptoms: peripheral neuropathies (numbness, burning and tingling of the hands and feet) , headache, ataxia, depression, irritability [4]
- Gynecological associations: reduced fertility or infertility
- Endocrine associations: autoimmune thyroid disease, type 1 diabetes mellitus
- Associated chromosomal syndromes: Turner syndrome, Down syndrome
-
Other associated conditions
- Autoimmune hepatitis
- Irritable bowel syndrome
- Inflammatory bowel disease
- Rheumatoid arthritis
- Sarcoidosis
- Selective IgA deficiency
- Atrophic glossitis
In both children and adults, mild or asymptomatic cases are more common than the classic presentation of the disease.
Diagnosis
General principles [5][6][7]
- Celiac disease is an underdiagnosed condition that requires a high index of suspicion.
-
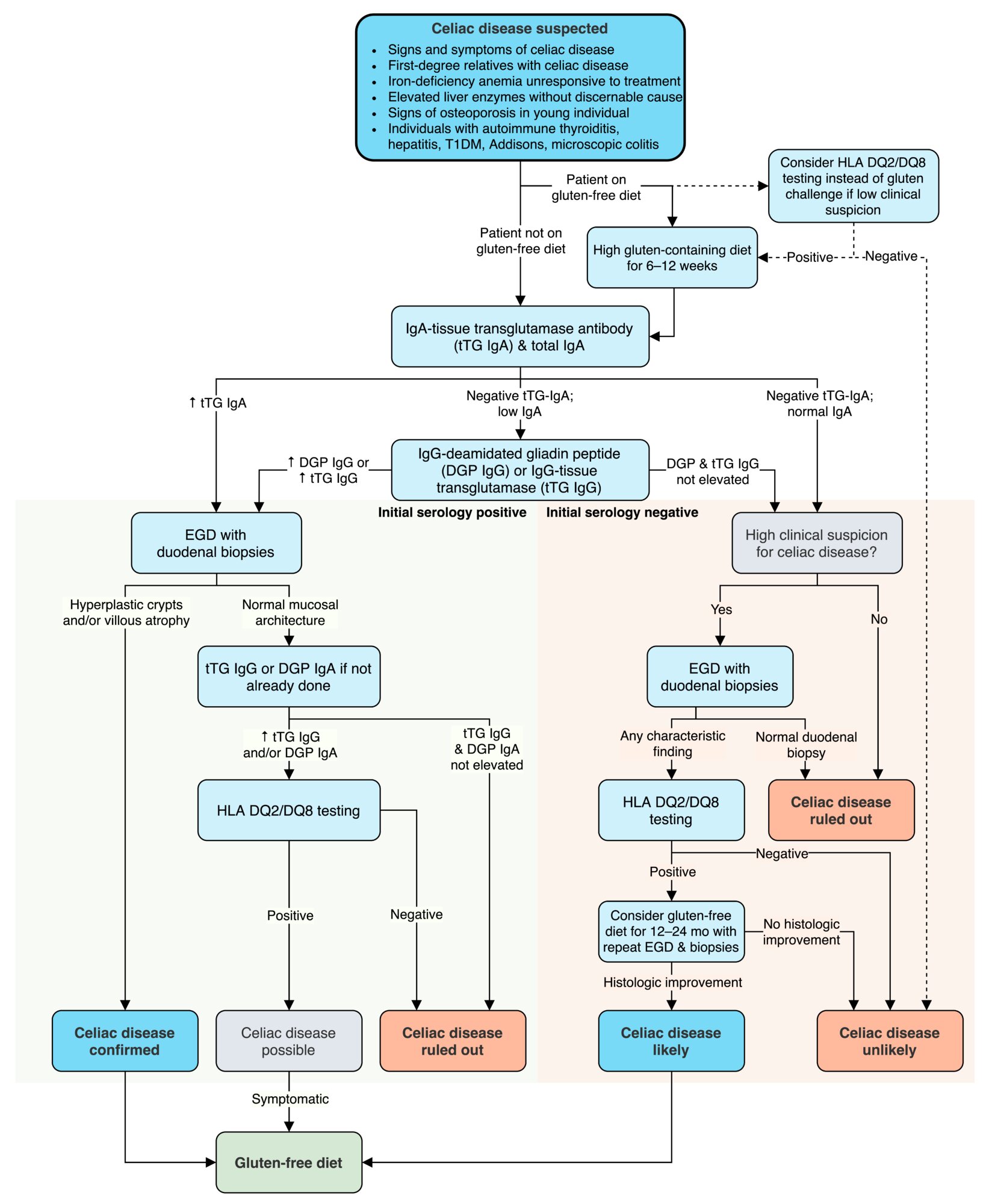
Diagnosis is based on serology (initial testing) and EGD with duodenal biopsy (confirmation).
- A gluten-free diet can cause negative test results.
- HLA-based testing and/or a gluten challenge are options for patients not consuming gluten.
- Common indications for testing include:
- Symptoms of malabsorption (e.g., steatorrhea)
- First-degree relatives with celiac disease [6]
- Iron deficiency anemia unresponsive to treatment [6]
- Elevated liver enzymes with no discernable cause
- Type 1 diabetes mellitus
- Signs of osteoporosis (e.g., repeated, unexplained fractures)
- Workup of other autoimmune disorders (e.g., thyroiditis, hepatitis)

Laboratory studies [5][7]
Routine studies
-
IgA tissue transglutaminase antibody (tTG IgA): initial test, crucial part of celiac disease serology
- Widely available test with high specificity (≥ 96%) [5]
- Risk of false negatives (e.g., in IgA deficiency, gluten-free diet)
-
Total IgA
- Indicated for all patients because of the high prevalence of IgA deficiency in patients with celiac disease (approx. 2–3%) [3]
- If patients have low IgA, perform further IgG-based testing.
Additional studies
-
Deamidated gliadin peptide
-
IgG-based testing: indicated in IgA deficiency or discordant biopsy and serology
- IgG-tissue transglutaminase (tTG IgG)
- IgG deamidated gliadin peptide (DGP IgG)
- IgA-based testing: IgA deamidated gliadin peptide (DGP IgA)
-
IgG-based testing: indicated in IgA deficiency or discordant biopsy and serology
-
HLA testing: second-line testing after unclear initial evaluation
- Assesses for haplotypes HLA-DQ2 and HLA-DQ8
- Indications include:
- Uncertain diagnosis (e.g., disparity between serology and histopathology)
- Gluten-free diet prior to diagnosis
- Patients with Down syndrome [3]
- Anti-endomysial antibody (EMA): Potential second-line confirmatory test (high-specificity) [7]
Endoscopy [5][7]
-
EGD with small intestine biopsy (confirmatory test) [8]
- Indications: positive serology or high clinical suspicion despite negative serology
- At least five duodenal biopsies should be taken (with ≥ 1 from the duodenal bulb). [5][9]
-
Histological findings: typically ranked by severity according to the Marsh classification ; [10]
- Intraepithelial lymphocytic infiltration
- Crypt hyperplasia
- Villous atrophy
- Video capsule endoscopy: if EGD is declined or as follow-up if symptoms persist despite treatment [11]
False-negative serology and histopathology results are possible if patients are already adhering to a gluten-free diet.





")
Diagnosis without endoscopy [5][7]
- Adults: diagnosis without biopsy not recommended.
- Children: consider diagnosis without biopsy in case of high titers of tTG-IgA and positive EMA (controversial) [12][13]
Further evaluation
-
Gluten challenge: may be indicated if patients are already adhering to a gluten-free diet [5]
- Systematic reintroduction of gluten into a patient's diet prior to (repeated) serologic and endoscopic testing
- 3 g gluten per day for up to eight weeks OR until the patient develops characteristic symptoms
-
Nutrient deficiency screening (individualize): indicated in confirmed celiac disease [14][15]
- Ferritin, iron (see “Diagnosis of iron deficiency anemia”)
- Zinc, calcium
- Vitamin B12 and B6, folate
- Fat-soluble vitamins, especially vitamin D
- Associated autoimmune disorders: Consider further testing if there are symptoms for thyroiditis, autoimmune hepatitis, and/or diabetes.
-
Tests for malabsorption: not routinely indicated (low sensitivity and specificity)
- D-xylose absorption test: low urine d-xylose levels (The passive absorption of d-xylose in the proximal small intestine is impaired by the mucosal defect and bacterial overgrowth.)
- Fat malabsorption: quantitative stool fat assays or qualitatively via fat stains (e.g., Sudan III stain)
- See “Diagnostics” in “Malabsorption” for further information.
Follow-up
- Repeat laboratory studies after 3–6 months and 12 months, then annually [5][7]
- tTG-IgA or DGP antibodies
- Nutrient levels if the patient had a deficiency at the time of diagnosis [8]
- Endoscopy: only if symptoms persist or return in patients adhering to a gluten-free diet [5][6][8]
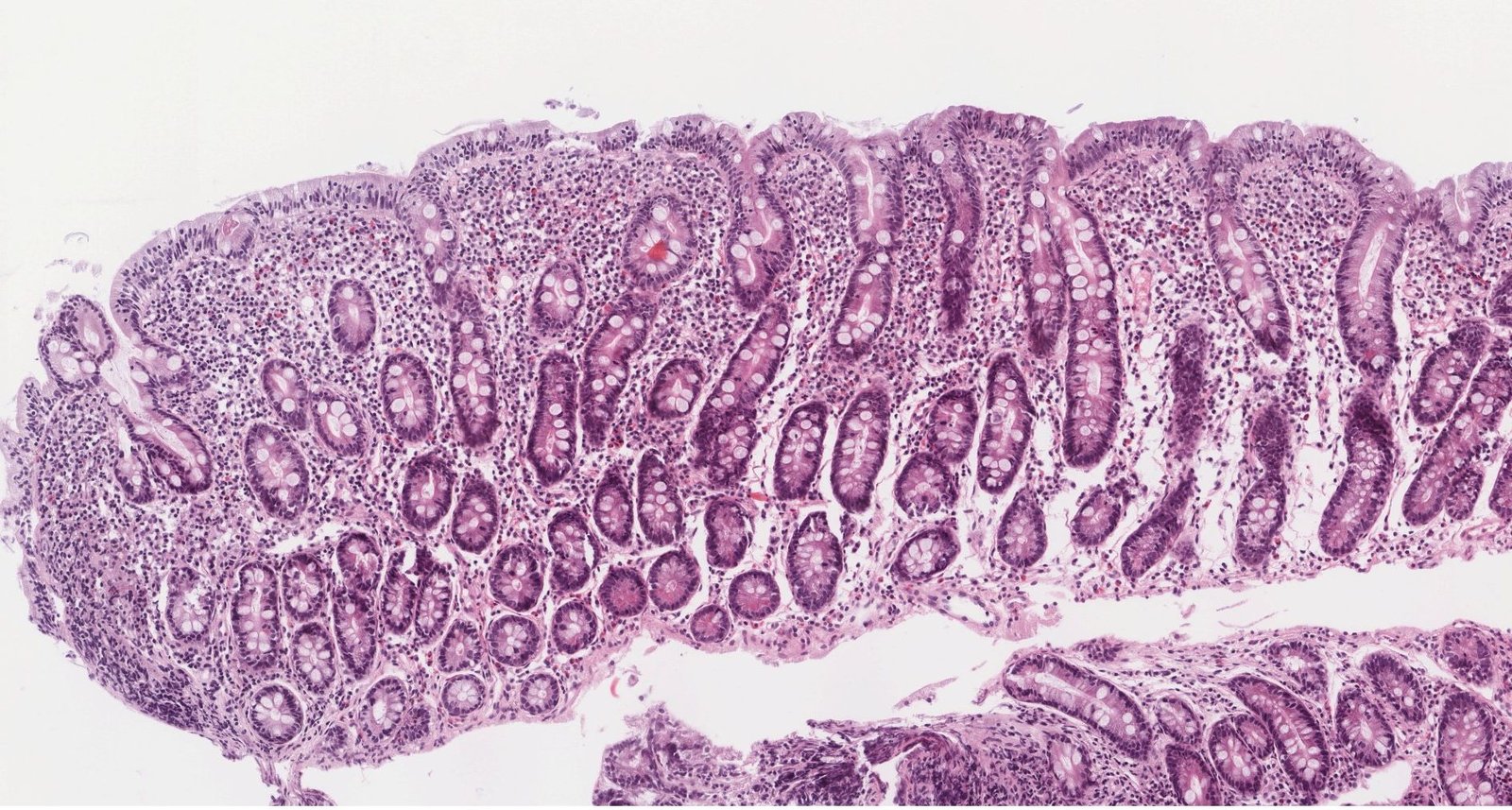
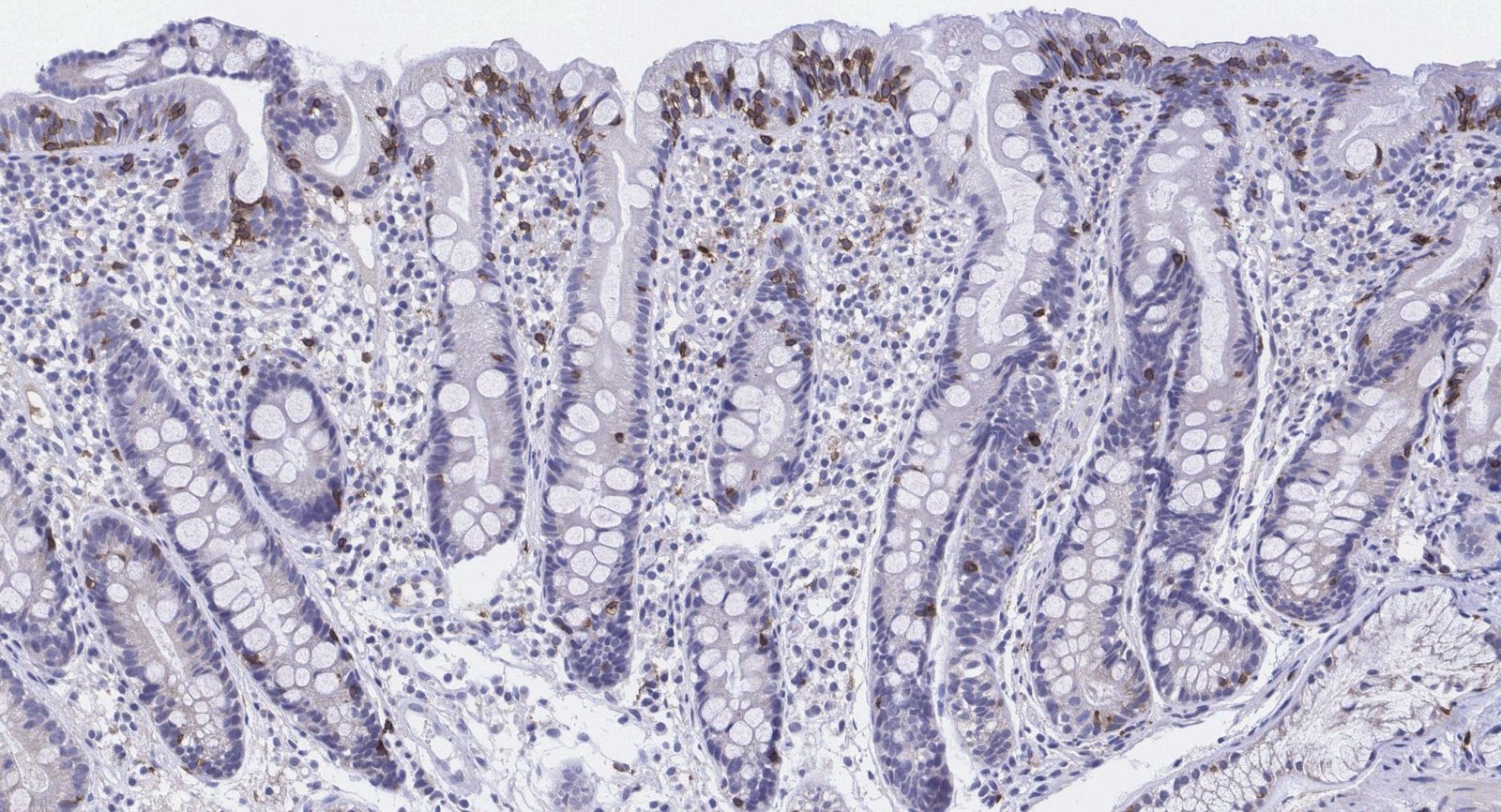
Photomicrograph of a biopsy specimen of duodenal tissue (H&E stain; low magnification)
Intraepithelial lymphocytosis (examples indicated by arrowheads), villous atrophy (dashed outline showing the approximate height of a normal villus), and crypt hyperplasia (example indicated by green overlay) are visible.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
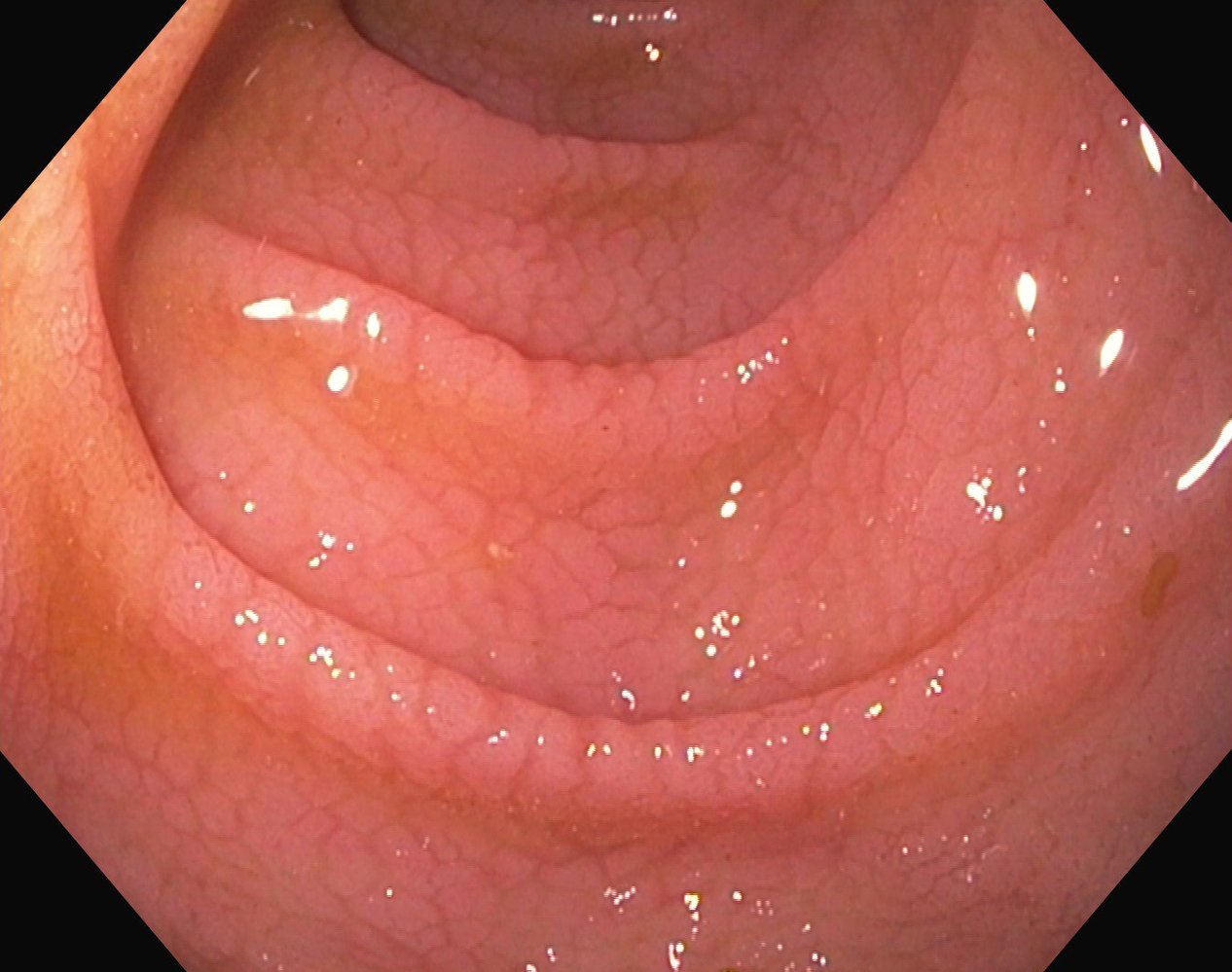
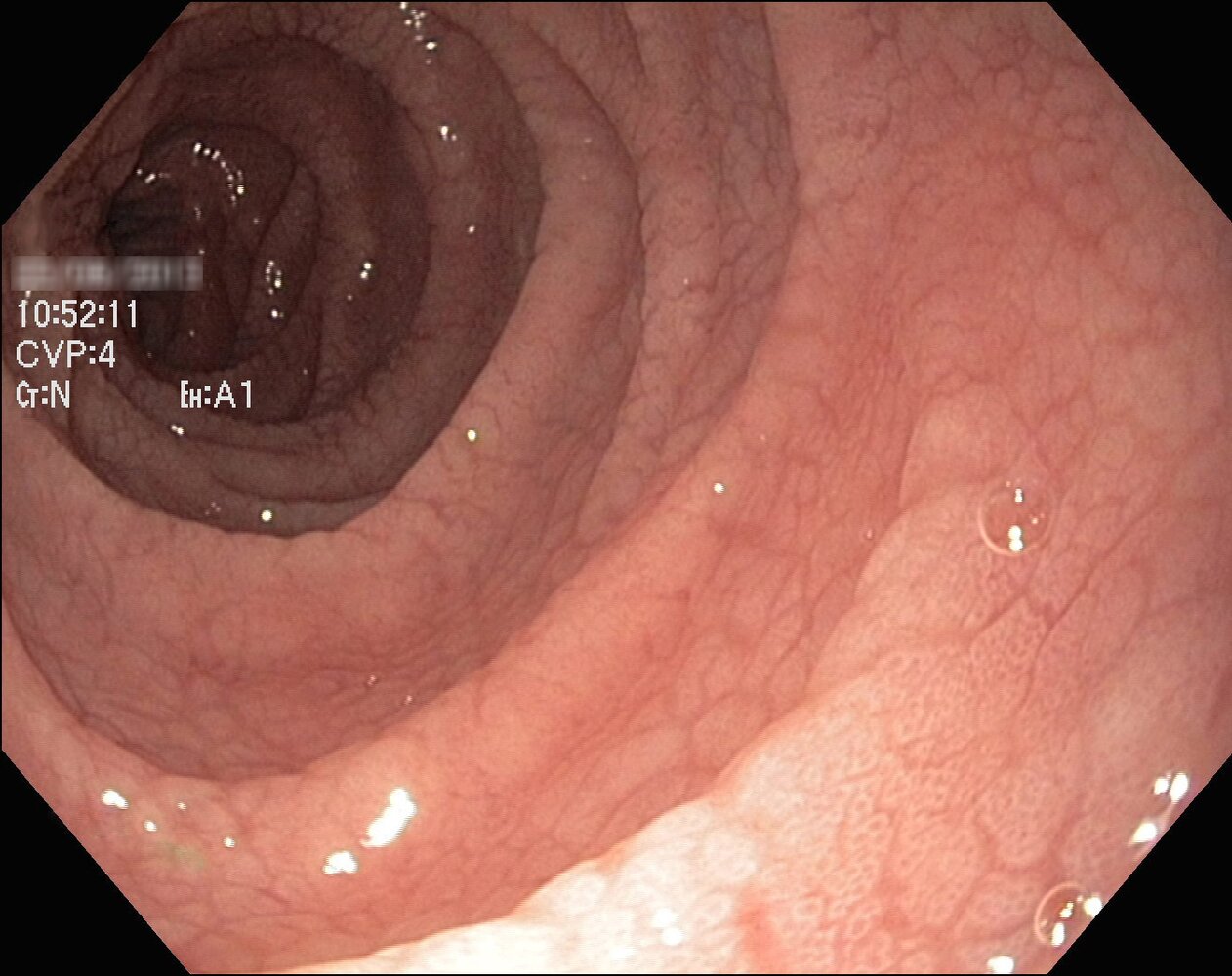
Endoscopic view of the duodenum
The plicae circulares appear normal but there is villous atrophy. The mucosa is smooth with hyperplastic crypts, and small notches form a mosaic pattern.
These findings are characteristic of celiac disease.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
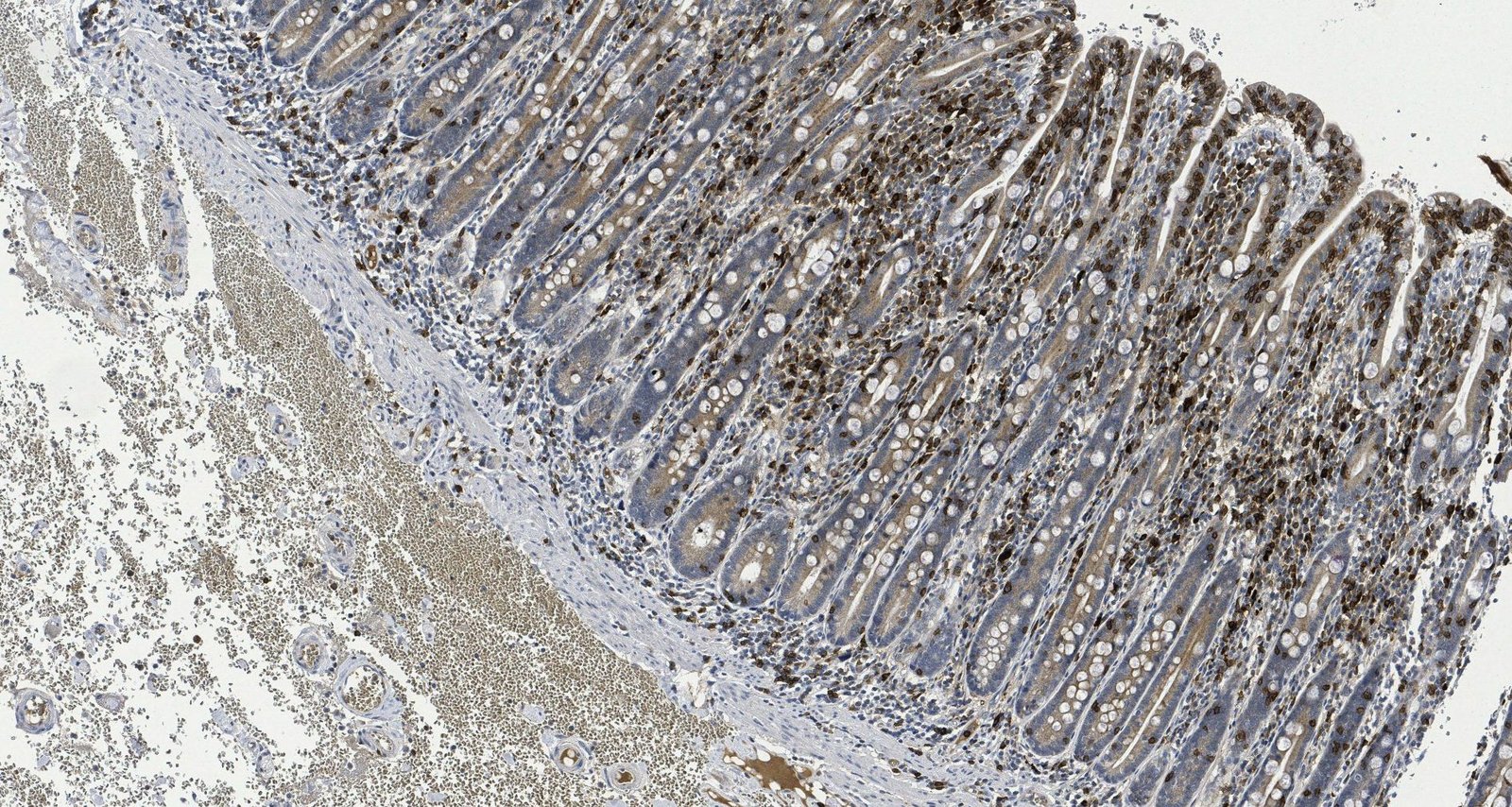
Endoscopic view of the duodenum
The surface of the duodenum is smooth, with small notches forming a mosaic pattern. Villous atrophy and hyperplastic crypts (examples indicated by green overlay) are visible.
These findings are characteristic of celiac disease.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
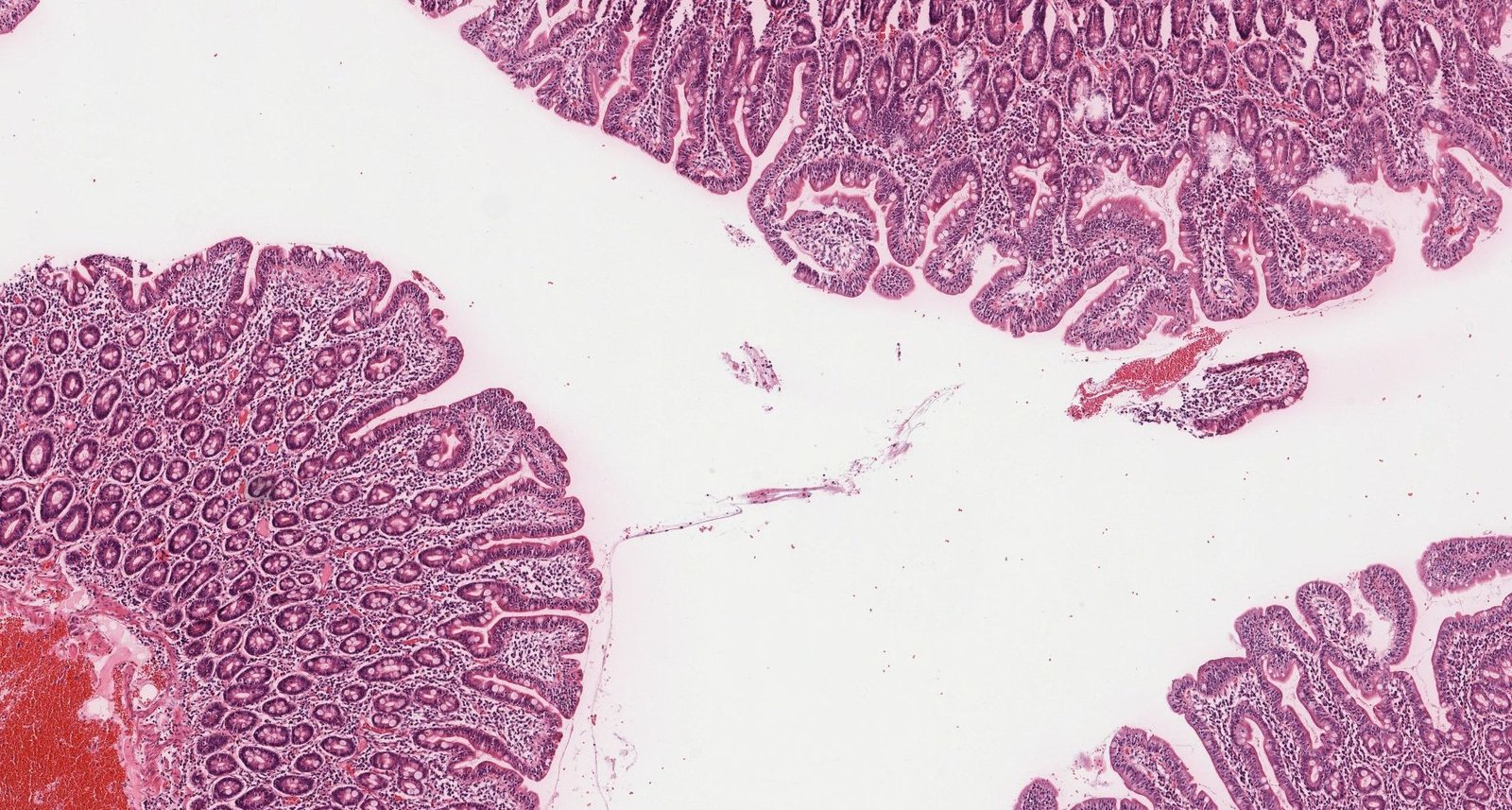
Photomicrograph of surgical resection specimen of duodenal tissue (H&E stain; low magnification), showing villous atrophy, crypt hyperplasia, and intraepithelial lymphocytosis.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Differential diagnoses
- Tropical sprue
- Whipple disease
- Other wheat-related diseases, e.g., nonceliac gluten sensitivity
The differential diagnoses listed here are not exhaustive.
Treatment
Diet [5][16]
-
Strict, lifelong gluten-free diet
- Abstain from products containing wheat, rye, barley, or spelt.
- Symptoms usually improve quickly [16]
- Recommended foods: rice, corn, potatoes, soybeans, millet
- Patients with secondary lactase deficiency: Avoid milk products.
Other
- Iron and vitamin supplementation, if there are deficiencies (e.g., iron deficiency anemia) [15]
- Consider osteoporosis screening in adult patients [8]
- Refer patients to a dietitian and advise joining support groups. [5][8]
Managing celiac disease mainly consists of maintaining a lifelong gluten-free diet.
Complications
- See “Clinical features” in “Malabsorption.”
- Secondary lactase deficiency
-
Moderately increased risk of malignancies
-
Enteropathy-associated T-cell lymphoma (EATL)
- Origin: intraepithelial T cells
- Localization: often proximal jejunum
- Clinical presentation: initially often asymptomatic, but B symptoms and gastrointestinal symptoms may be present
- Adenocarcinoma of the small bowel
- Esophageal cancer [17]
-
Enteropathy-associated T-cell lymphoma (EATL)
-
Refractory celiac disease (RCD): persistence and worsening of celiac symptoms despite strict adherence to gluten-free diet for 12 months
- The condition manifests with one of three possible courses
- Only partial improvement despite gluten-free diet
- Initial improvement followed by relapse despite maintaining gluten-free diet
- Nonresponsive celiac disease (no response to gluten-free diet)
- May lead to ulcerative jejunitis
- In severe cases, total parenteral nutrition and treatment with steroids or immunosuppressants may be necessary.
- The condition manifests with one of three possible courses
We list the most important complications. The selection is not exhaustive.
Prevention
- There is no proven measure to prevent celiac disease.
- With infants, introducing small amounts of wheat (into the supplementary diet) between 4–6 months of age does not increase the risk of developing celiac disease
External Resources
- 2022 ACG Guidelines Update: Diagnosis and Management of Celiac Disease
- 2018 AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease
- 2017 US Preventive Services Task Force recommendations (Screening for Celiac Disease)
- 2017 AGA Clinical Practice Guidelines for the Use of Video Capsule Endoscopy
- 2005 Pediatrics (NASPGHAN) Guidelines for the Management of Celiac Disease in children
- 2020 ESPGHAN Guidelines for Diagnosing Coeliac Disease
References
- Alaedini A, Green PH.. "Autoantibodies in celiac disease. Autoimmunity". Autoimmunity. 41(1). :19-26. (2008)
- Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA, Everhart JE. "The Prevalence of Celiac Disease in the United States". Am J Gastroenterol. 107(10). :1538-1544. (2012)
- Rubio-tapia A, Hill ID, Kelly CP, Calderwood AH, Murray JA. "ACG clinical guidelines: diagnosis and management of celiac disease". The American Journal of Gastroenterology. 108(5). :656-76. (2013)
- Chin RL, Sander HW, Brannagan TH, et al. "Celiac neuropathy". Neurology. 60(10). :1581-5. (2003)
- Rubio-Tapia A, Hill ID, Semrad C, Kelly CP, Lebwohl B. "American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease". Am J Gastroenterol. 118(1). :59-76. (2022)
- Leonard MM, Sapone A, Catassi C, Fasano A. "Celiac Disease and Nonceliac Gluten Sensitivity: A Review". JAMA. 318(7). :647-656. (2017)
- Husby S, Murray JA, Katzka DA. "AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease-Changing Utility of Serology and Histologic Measures: Expert Review". Gastroenterology. 156(4). :885-889. (2019)
- Oxentenko AS, Rubio-Tapia A. "Celiac Disease". Mayo Clinic proceedings. 94(12). :2556-2571. (2019)
- Hopper AD, Cross SS, Sanders DS. "Patchy villous atrophy in adult patients with suspected gluten-sensitive enteropathy: is a multiple duodenal biopsy strategy appropriate?". Endoscopy. 40(3). :219-24. (2008)
- Schiepatti A, Sanders DS, Zuffada M, et al. "Overview in the clinical management of patients with seronegative villous atrophy". Eur J Gastroenterol Hepatol. 31(4). :409-417. (2019)
- Enns RA, Hookey L, Armstrong D, et al. "Clinical Practice Guidelines for the Use of Video Capsule Endoscopy". Gastroenterology. 152(3). :497-514. (2017)
- Hill ID, Dirks MH, Liptak GS, et al. "Guideline for the Diagnosis and Treatment of Celiac Disease in Children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition". J Pediatr Gastroenterol Nutr. 40(1). :1-19. (2005)
- Husby S, Koletzko S, Korponay-Szabó I, et al. "European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020". J Pediatr Gastroenterol Nutr. 70(1). :141-156. (2020)
- Wierdsma NJ, van Bokhorst-de van der Schueren MA, Berkenpas M, Mulder CJ, van Bodegraven AA. "Vitamin and mineral deficiencies are highly prevalent in newly diagnosed celiac disease patients". Nutrients. 5(10). :3975-92. (2013)
- Kreutz JM, Adriaanse MPM, van der Ploeg EMC, Vreugdenhil ACE. "Narrative Review: Nutrient Deficiencies in Adults and Children with Treated and Untreated Celiac Disease". Nutrients. 12(2). (2020)
- Murray JA, Watson T, Clearman B, Mitros F. "Effect of a gluten-free diet on gastrointestinal symptoms in celiac disease". Am J Clin Nutr. 79(4). :669-73. (2004)
- Han Y, Chen W, Li P, Ye J. "Association Between Coeliac Disease and Risk of Any Malignancy and Gastrointestinal Malignancy". Medicine. 94(38). :e1612. (2015)
- Hill ID, Fasano A, Guandalini S, et al. "NASPGHAN Clinical Report on the Diagnosis and Treatment of Gluten-related Disorders". J Pediatr Gastroenterol Nutr. 63(1). :156-65. (2016)