Summary
Cerebral palsy (CP) is a heterogenous group of disorders affecting the muscle tone and the development of movement and posture. CP results from a non-progressive damage to the brain in utero or during infantile development up to the age of 3 years. Depending on the affected brain area, spastic, ataxic, or dyskinetic cerebral palsy develops. While, in many cases, there is no identifiable cause, risk factors for cerebral palsy are prematurity, perinatal complications such as chorioamnionitis, birth trauma with intracerebral hemorrhage, or postnatal infections such as meningitis. The diagnosis of CP is usually not made until features become apparent as children fail to meet certain milestones during the postneonatal period (e.g., inability to roll over or sit independently). Physical indicators of spastic cerebral palsy include spastic paresis of multiple limbs and joint contractures, scissors gait, and persistence of primitive reflexes. Patients with non-spastic cerebral palsy present with dysarthria and abnormal involuntary movements (choreoathetoid, dystonic, or ataxic) that worsen with stress. Seizure disorders and intellectual disability are associated with all types. Diagnosis is mainly based on the clinical picture but cranial ultrasound or MRI can help identify the causative lesion (e.g., hemorrhage, brain malformation). Since there is no cure, management follows a multidisciplinary approach with a focus on treating contractures (e.g., bracing, antispasmodics, physical therapy, surgery) and ensuring social participation (e.g., speech therapy, social support). Depending on the severity and type of cerebral palsy, patients may be slightly restricted or severely disabled and unable to walk.
Epidemiology
- Most common motor disability in children
- Approx. 2/1000 live births [1]
References:[2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Idiopathic (most cases)
-
Risk factors [1]
- Preterm birth and low birth weight (most important risk factors)
- TORCH infection
- Perinatal asphyxia
- Intracranial hemorrhage
- Periventricular leukomalacia
- Structural abnormality of the brain
- Neonatal seizures
- Kernicterus
- Postnatal infection (e.g., meningitis, encephalitis)
- Thyroid disorder in pregnancy
Studies have shown that antenatal administration of magnesium sulfate in birthing parents at risk of premature delivery (e.g., likely to enter preterm labor within 24 hours) has neuroprotective effects on the fetus and is associated with reduced incidence of cerebral palsy. [3][4][5]
References:[6]
Classification
- Spastic cerebral palsy: spastic paresis of one or more limbs (75% of cases)
-
Non-spastic cerebral palsy :
- Dyskinetic: abnormal involuntary movements (choreoathetoid, dystonic)
- Ataxic: intention tremor, lack of balance and coordination

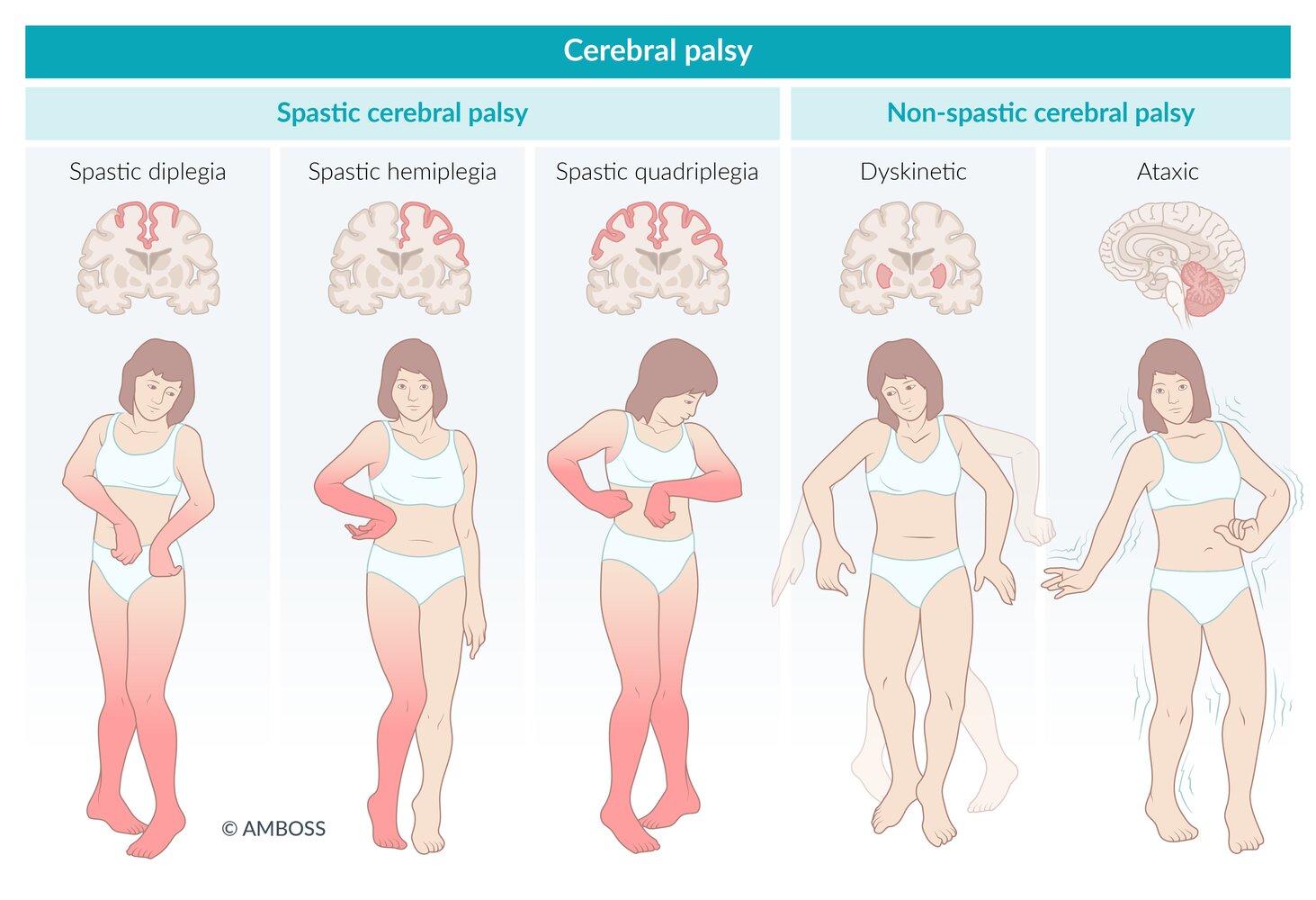
Based on the localization of the brain damage, a distinction can be made between pyramidal and extrapyramidal cerebral palsy.
Pyramidal cerebral palsy is characterized by spastic paralysis of one or more extremities. Depending on the pattern of damage, it can manifest as spastic diplegia, spastic hemiplegia, or spastic tetraplegia.
Extrapyramidal cerebral palsy results in variable movement disorders of the extremities, e.g., dyskinesia (athetosis, dystonia) or ataxia.
© AMBOSS
Clinical features
Patients may present with mixed types of cerebral palsy (e.g., combination of spastic and athetoid CP).
-
All types ; Spastic type
- ↑ Muscle tone in one or more limbs
- ↑ DTRs
- Persistence of primitive reflexes (e.g., positive Babinski sign)
- Toe walking or equinus deformity
- Scissor gait (due to spastic paraplegia of the hip adductors)
- Muscle weakness and/or atrophy
- Hip dislocation
- Scoliosis
- Hearing or vision impairment
- Intellectual disability (50%)
- Seizure disorder (35%–50%)
- Upper motor neuron signs (e.g., spasticity, hyperreflexia, clonus)
- Behavioral difficulties
- Developmental delay, particularly motor function (e.g., rolling over from back to belly, sitting independently, crawling).
- Attention deficit hyperactivity disorder
-
Non-spastic type
- Abnormal involuntary movements that worsen with stress and stop during sleep
- Chorea
- Athetosis
- Dystonia
- Ataxia
- Dysarthria and dysphagia
- Abnormal involuntary movements that worsen with stress and stop during sleep
Definite hand preference before 1 year of age suggests one-sided muscle weakness and is a red flag for hemiplegia.
Based on the localization of the brain damage, a distinction can be made between pyramidal and extrapyramidal cerebral palsy.
Pyramidal cerebral palsy is characterized by spastic paralysis of one or more extremities. Depending on the pattern of damage, it can manifest as spastic diplegia, spastic hemiplegia, or spastic tetraplegia.
Extrapyramidal cerebral palsy results in variable movement disorders of the extremities, e.g., dyskinesia (athetosis, dystonia) or ataxia.
© AMBOSS
Diagnosis
Diagnosis is mainly based on clinical findings. A comprehensive assessment of vision, hearing, and developmental milestones should be conducted. [1]
- Cranial ultrasonography (early neonatal period): e.g., intracerebral hemorrhage: and/or hypoxic-ischemic injury, structural abnormalities
- MRI (in older infants): to detect causative lesion (e.g., periventricular leukomalacia, congenital malformation, intracranial hemorrhage)
- EEG: patients with suspected seizures
Differential diagnoses
- Hypothyroid myopathy
- Mitochondrial myopathy
- Progressive muscular dystrophies
- Myelomeningocele
- Traumatic peripheral nerve lesions
- Genetic syndromes
The differential diagnoses listed here are not exhaustive.
Treatment
There is no curative therapy for cerebral palsy. Management is dependent on the severity and nature of symptoms. A multidisciplinary approach is employed in management to improve function and quality of life.
-
Nonpharmacological management
- Physical therapy: prevents muscle contractures
- Occupational therapy: motor skill development
- Speech therapy: communication skills and dysphagia
- Orthotic devices (e.g., braces, splints, and casts) and assistive devices (e.g., wheelchairs, walkers)
- Educational support for intellectual disability
- Nutritional support for dysphagia
- Social and psychological support
-
Pharmacological management
- Antispasmodics; (e.g., botulinum toxin, baclofen, dantrolene, benzodiazepines)
- Anticonvulsants
- Anticholinergics for rigidity and sialorrhea
-
Surgery
- Orthopedic surgery to treat scoliosis and relieve contractures
- Selective dorsal rhizotomy to relieve spasticity and pain





Source: "Walker. frame.jpg", High Plains Drifter, Wikimedia Commons licensed under Public Domain
{kind=link}

Source: “Modern Rollator.jpg” by Hansimglueck70, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Source: "Standard rollstuhl.jpg", Bestrossi, Wikimedia Commons licensed under Public Domain
{kind=link}

Source: “Electric-powered wheelchair Belize” by Memasa, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
References
- Patel DR, Neelakantan M, Pandher K, Merrick J. "Cerebral palsy in children: a clinical overview". Translational Pediatrics. 9(S1). :S125-S135. (2020)
- "Cerebral Palsy (CP) - Data & Statistics for Cerebral Palsy". https://web.archive.org/web/20170719183748/https://www.cdc.gov/ncbddd/cp/index.html. [2016-05-02]
- Kathleen F. Brookfield, Abigail Vinson. "Magnesium sulfate use for fetal neuroprotection". Current Opinion in Obstetrics & Gynecology. 31(2). :110-115. (2019)
- The American College of Obstetricians and Gynecologists. "Committee Opinion No. 455: Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection". Obstetrics & Gynecology. 115(3). :669-671. (2010)
- Amy L. Turitz, Gloria T. Too, Cynthia Gyamfi-Bannerman. "Proximity of magnesium exposure to delivery and neonatal outcomes". American Journal of Obstetrics and Gynecology. 215(4). :508.e1-508.e6. (2016)
- Abdel-Hamid HZ. "Cerebral Palsy". WebMD. http://emedicine.medscape.com/article/1179555. [2016-08-12]