Summary
Cervical cancer is the third most common cancer of the female genital tract in the US. Persistent infection with any high-risk HPV genotype is the most common cause of cervical cancer. HPV immunization, counseling on safe sex practices, and screening for cervical cancer are the most effective prevention measures. All asymptomatic individuals with a cervix between the ages of 21–65 years of age are at increased risk of cervical cancer and should be screened at regular intervals (the age to initiate screening is a point of debate; the American Cancer Society recommends initiating screening at 25 years of age). Screening modalities include primary HPV testing, cytology-alone screening, and HPV/Pap cotesting. Endocervical sampling and p16 immunohistochemistry may be considered in select situations. Management of abnormalities detected on screening has shifted away from a result-based approach to an individualized risk-based approach. There are some exceptions to the risk-based approach (e.g., abnormalities detected in individuals < 25 years of age, certain cytology results). Management options include expedited treatment (e.g., with conization, LEEP, laser cone biopsy), diagnostic excision (i.e., colposcopic biopsy), and surveillance. Individuals with high-grade precursor lesions remain at high risk of developing invasive cervical cancer even after treatment and should be followed up for recurrence for at least 25 years after management.
Invasive cervical cancer is detailed in a separate article.
Cervical cancer precursors
- Precancerous lesions of the cervix are noninvasive dysplastic lesions that can progress to invasive cervical cancer. [1][2]
- They are typically asymptomatic and detected on cervical cancer screening.
- Precursor for squamous cell carcinoma of the cervix: squamous intraepithelial neoplasia (SIL) or cervical intraepithelial neoplasia (CIN)
- Precursor for adenocarcinoma of the cervix: endocervical adenocarcinoma in situ (AIS)
Pathology
Overview of terminology [1][2]
Two-tiered terminology (Bethesda system)
A unified system of reporting histological and cytological samples of all squamous intraepithelial lesions (SIL) of the anogenital tract.
-
High-grade squamous intraepithelial lesion (HSIL)
- Lesions with moderate to severe epithelial dysplasia that are most likely associated with persistent HPV infection
- HSIL lesions can progress to invasive cervical cancer (precancerous lesion).
-
Low-grade squamous intraepithelial lesion (LSIL)
- Lesions with mild epithelial dysplasia that are typically associated with transient HPV infections
- Correlates with CIN1
Three-tiered terminology
- Cervical intraepithelial neoplasia; (CIN) is characterized by epithelial dysplasia that begins at the basal layer of the squamocolumnar junction and extends outward.
- Based on the degree of dysplasia, lesions are classified as CIN1 (mild), CIN2 (moderate), or CIN3 (severe).
Current standard
The current standard for reporting cervical histopathology and cytopathology to ensure optimal management is a combination of the two-tier and three-tier system (i.e., the two-tiered nomenclature with an additional qualifier using the intraepithelial neoplasia nomenclature).
- LSIL correlates with CIN1.
- HSIL correlates with CIN3 and p16 positive CIN2.
- HSIL should be specified as HSIL (CIN2), HSIL (CIN3), or HSIL unspecified.
Cervical cytology findings [1]
| Grading of cytological abnormalities | Bethesda system for reporting cervical cytology [1][3][4] | |
|---|---|---|
| Characteristic features | ||
| Low-grade cervical cytology [5] | Negative for intraepithelial lesion or malignancy (NILM) |
|
| Atypical squamous cells of undetermined significance (ASC-US) |
|
|
| Cytological LSIL |
|
|
| High-grade cervical cytology | Cytological HSIL |
|
| Atypical squamous cells likely to contain HSIL cells (ASC-H) |
|
|
| Atypical glandular cells (AGCs) |
|
|
Endometrial cells are typically a benign cytology finding but can suggest endometrial neoplasia in women ≥ 45 years of age. [3][5]
")



")
")
Cervical histology findings [1][2]
| Reporting cervical biopsy [1][2] | |||
|---|---|---|---|
| Two-tiered system | Three-tiered system | Severity of cellular proliferation | |
| Low-grade cervical histology | Histological LSIL [5] | CIN1 |
|
| High-grade cervical histology [5] | Histological HSIL | p-16 positive CIN2 |
|
| CIN3 |
|
||
| Endocervical adenocarcinoma in situ (AIS) |
|
||
| Invasive cervical cancer |
|
||
Koilocytes are epithelial cells with perinuclear halos that are pathognomonic of HPV infection and may be present from early HPV infection. [1][2]
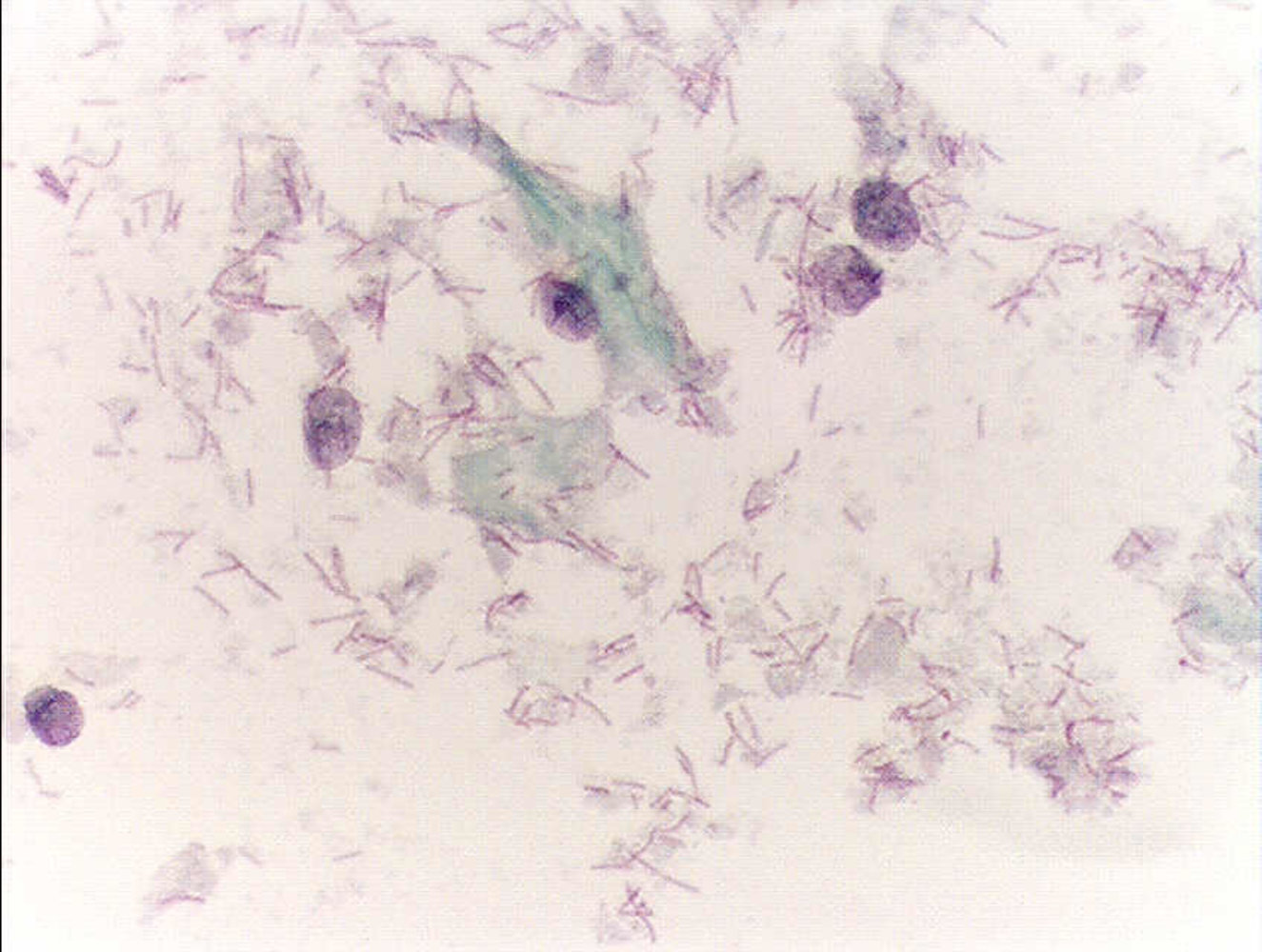
Photomicrograph of cervical cells from a Papanicolaou test of a premenopausal woman (Papanicolaou stain; high magnification)
Normal squamous epithelial cells are present. The cells with blue (cyanophilic) cytoplasm on the left of the image are intermediate cells (marked by blue dotted line). The cell with the red (eosinophilic) cytoplasm on the right of the image is a superficial cell (marked by yellow dotted line). Neutrophils can also be seen (small cells with a segmented nucleus).
These findings are consistent with a normal Papanicolaou test.
Circled in black: rod-shaped bacteria
Source: “Pap test normal” by Alex_brollo, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Photomicrograph of a pap smear in a patient with clinical signs of vaginitis (Papanicolaou stain; high magnification)
A reddish-stained (eosinophilic) superficial squamous cell can be seen (black arrow). Peripherally, multiple blue (cyanophilic) intermediate squamous cells can be distinguished (black outlines). In the upper right part of the image, the flagellate stage of Trichomonas vaginalis can be seen (blue overlay). The typical granulocytic inflammatory response cannot be seen in this image. However, the nuclei of the squamous cells show signs of degeneration (examples indicated by arrowheads), and some cells have perinuclear halos (yellow overlay). Both are signs of inflammation, indicating trichomoniasis.
The diagnosis of trichomoniasis should be confirmed with wet-mount microscopy.
Source: “Trichomonas pap test” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Photomicrograph of a pap smear (Papanicolaou stain, very high magnification)
Normal intermediate squamous cells (black outline) with light blue cytoplasm and physiological nuclei can be seen. Some scattered neutrophils (exemplary indicated by blue dashed line) are present as well.
In the center a tight cluster of relatively small cells (yellow outline) is present. These cells have scant cytoplasm, which can be vacuolated (exemplary indicated by red outline line). Their nuclei (exemplary indicated by yellow dashed line) are equal or slightly smaller than the intermediate cell nucleus (exemplary indicated by black dashed line), and show dense chromatin.
This is the typical appearance of normal endometrial cells.
Source: “Endometrial cells on Pap - 2a -- very high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Photomicrograph of a pap smear showing squamous cells of the cervix (Papanicolaou stain, very high magnification)
A cluster of squamous epithelial cells with dense, mostly eosinophilic to orangeophilic cytoplasm is seen in the center. The borders of the individual cells are not clearly definable. The nuclei are enlarged (yellow overlay) approximately twofold to threefold the size of a regular intermediate cell nucleus (white arrowhead). Therefore, these squamous cells present an enlarged nuclear-to-cytoplasmic ratio. Features of a HPV infection (e.g., koilocytes) are not present in this case.
These findings are consistent with atypical squamous cells of undetermined significance (ASC-US).
Source: “Atypical squamous cell of undetermined significance - 1 -- very high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
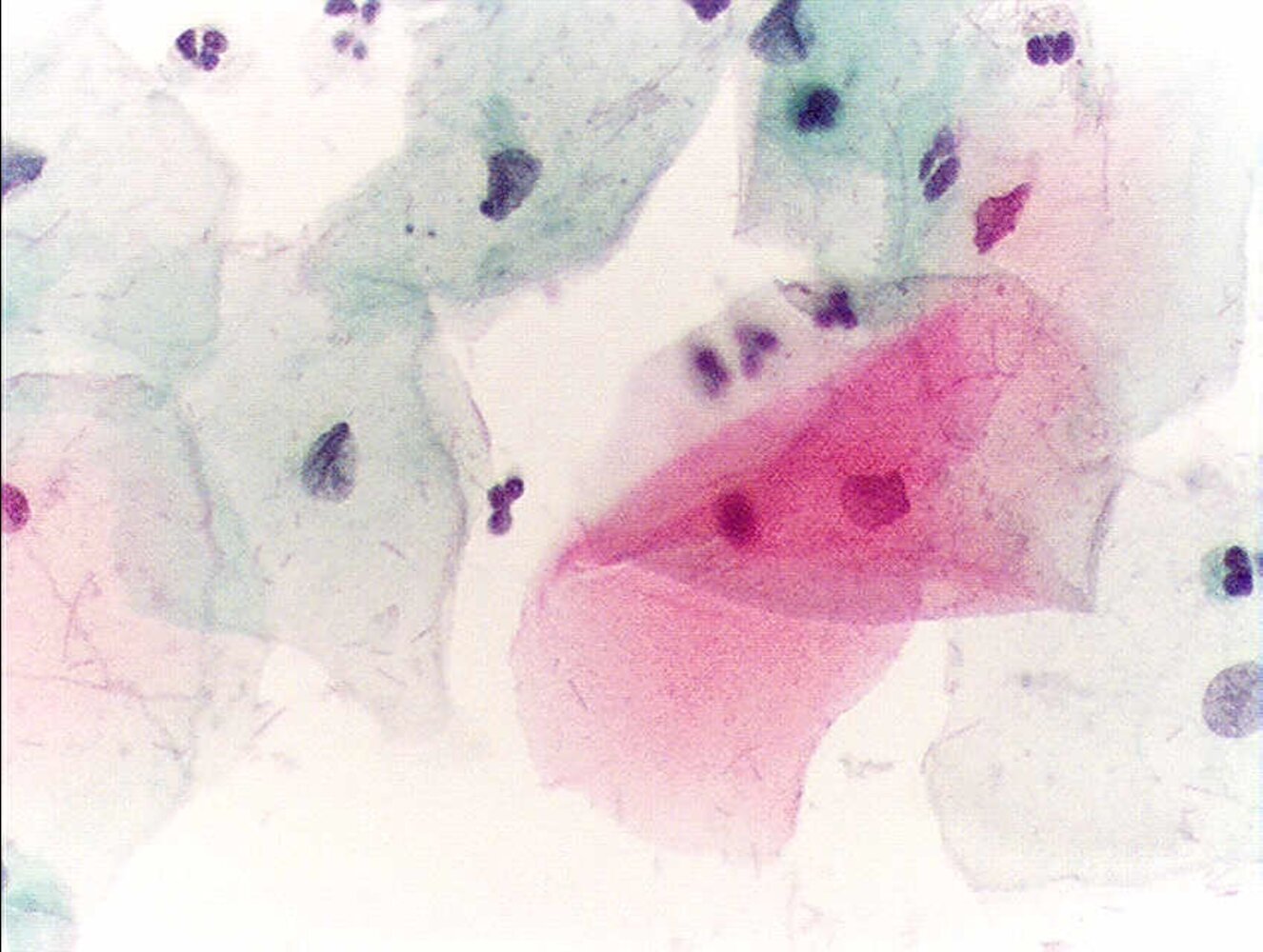
Photomicrograph of a cervical pap smear (Papanicolaou stain; high magnification)
Normal superficial squamous cells (pink cytoplasm, examples indicated by dashed outlines) and some intermediate squamous cells (example indicated by outline) are visible. An irregular clump of koilocytes (indicated by arrow) is visible with the characteristic perinuclear halos (indicated by arrowheads). The koilocytes also show slight nuclear enlargement with irregularly distributed chromatin; binucleation (yellow overlay) is also seen.
These are typical features of a low-grade squamous intraepithelial lesion (LSIL).
Source: “Low grade squamous intraepithelial lesion” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: added arrow. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
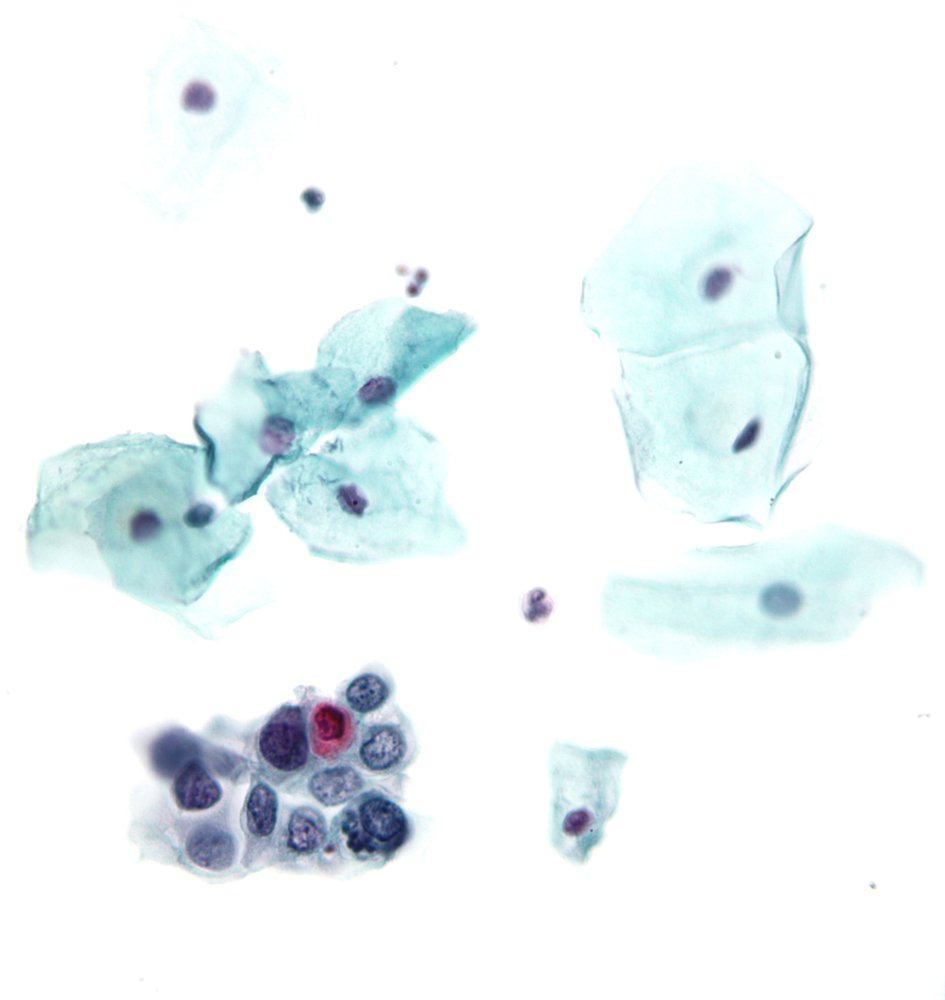
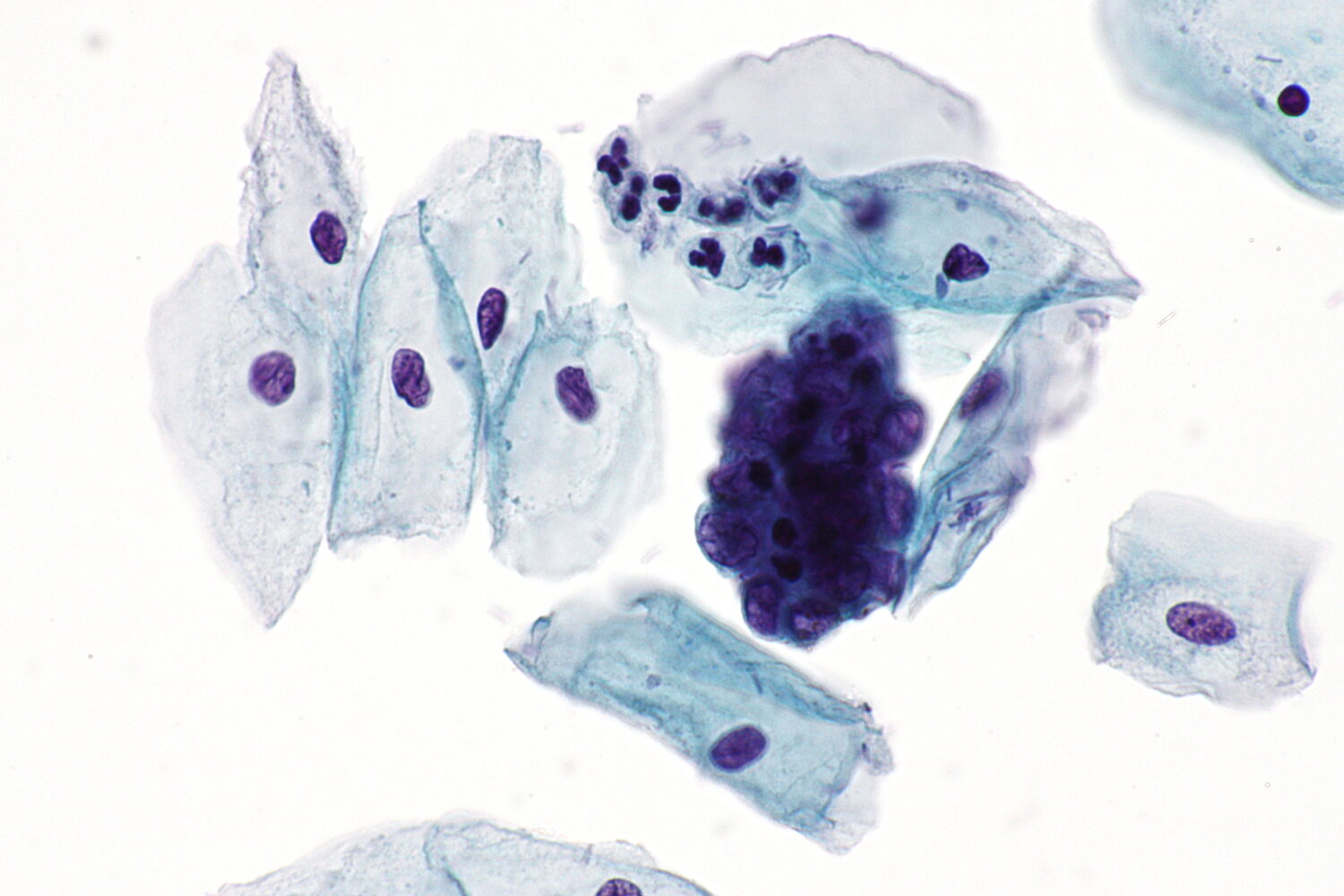
Photomicrograph of a Papanicolaou test sample of squamous cells of the cervix (Papanicolaou stain; very high magnification)
Multiple normal intermediate squamous cells (light blue cytoplasm, examples indicated by yellow overlay) and a neutrophil (arrowhead) can be seen. A sheet of smaller, abnormal, epithelial cells (dashed outline) is also present at the bottom of the image. These cells have irregular nuclear contours with a high nuclear-to-cytoplasmic ratio and irregular clumped chromatin. There is a dyskeratotic cell (red cytoplasm, arrow) within the clump of abnormal cells.
These findings are characteristic of severe dysplasia, i.e., a high-grade squamous intraepithelial lesion (HSIL).
Source: “High-grade squamous intraepithelial lesion” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
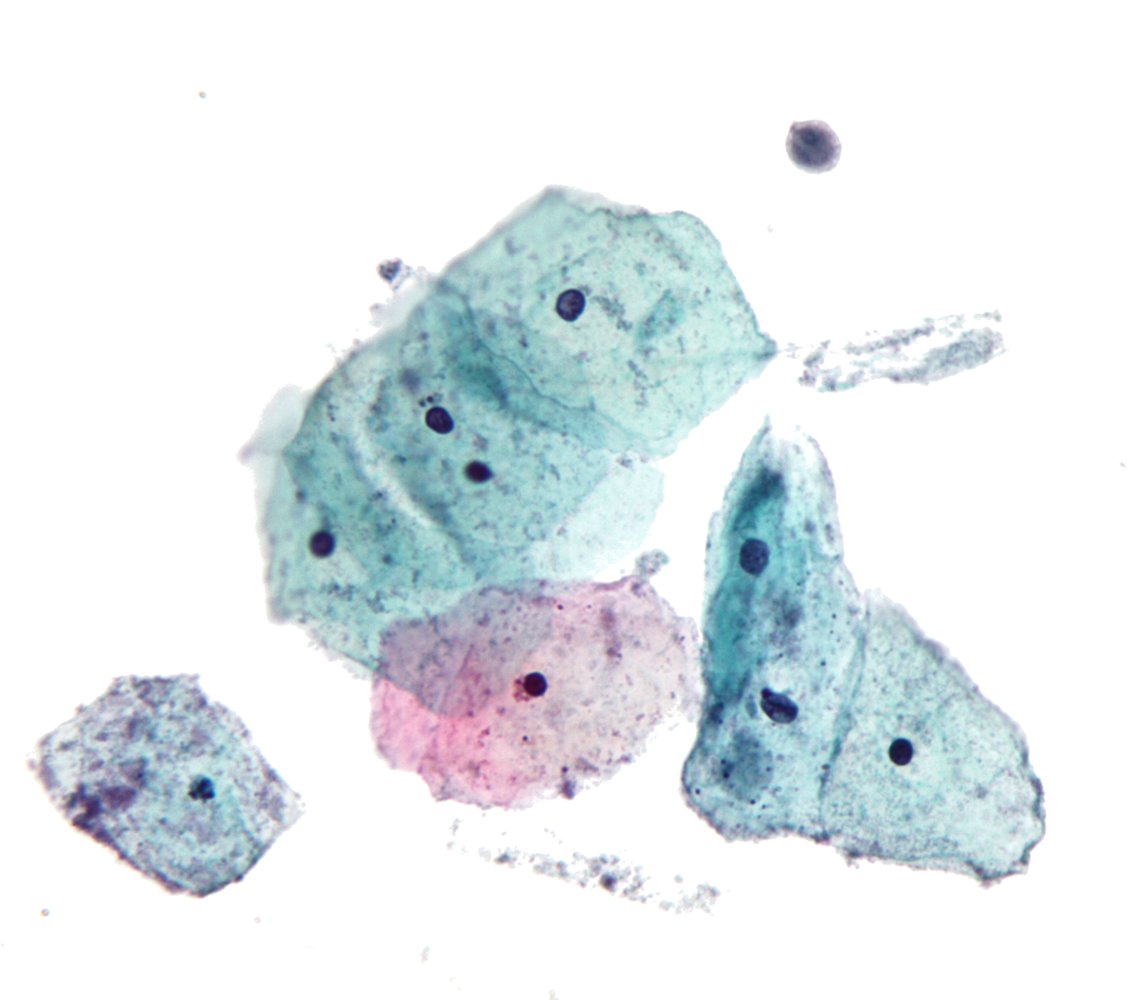
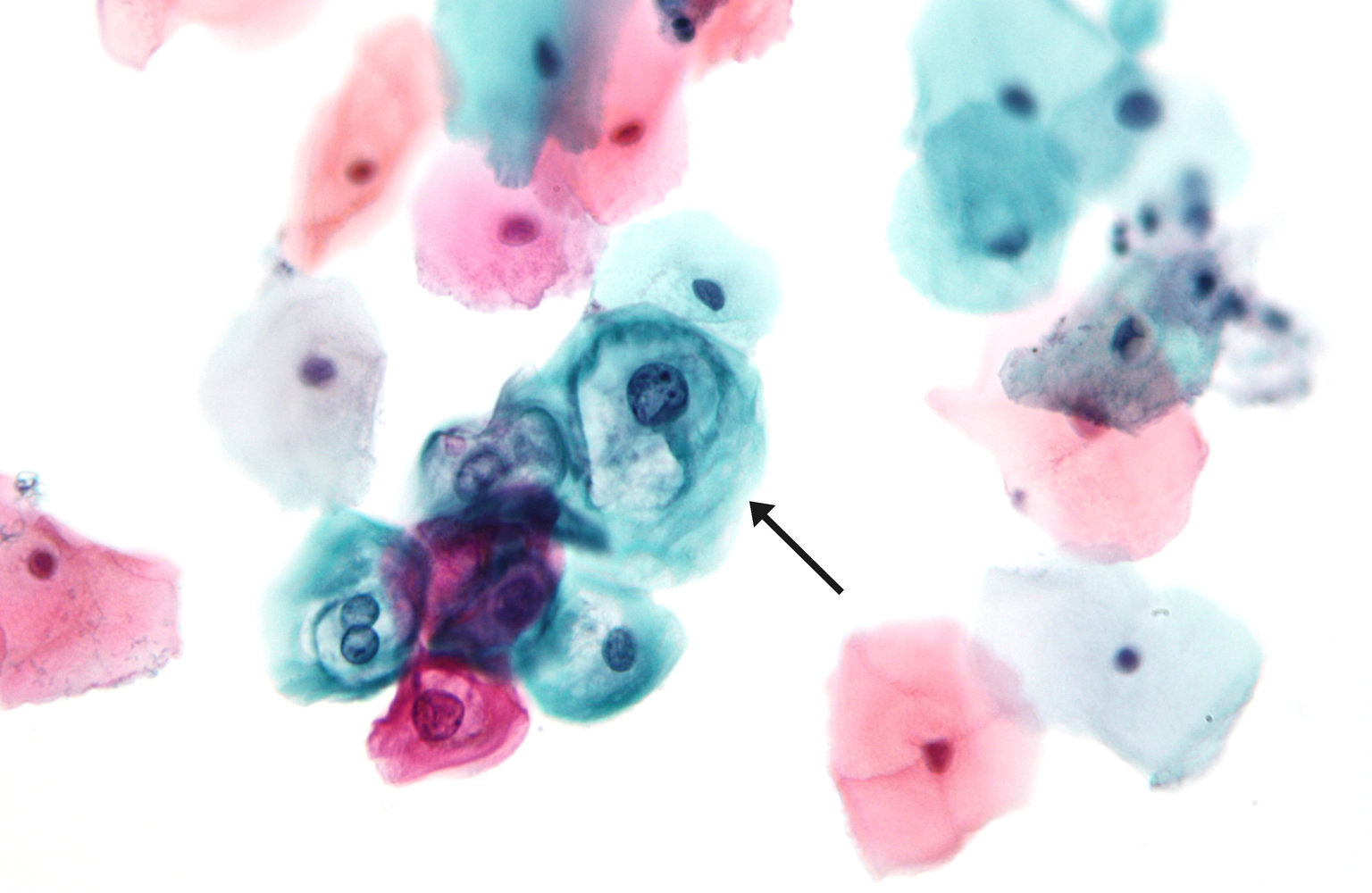
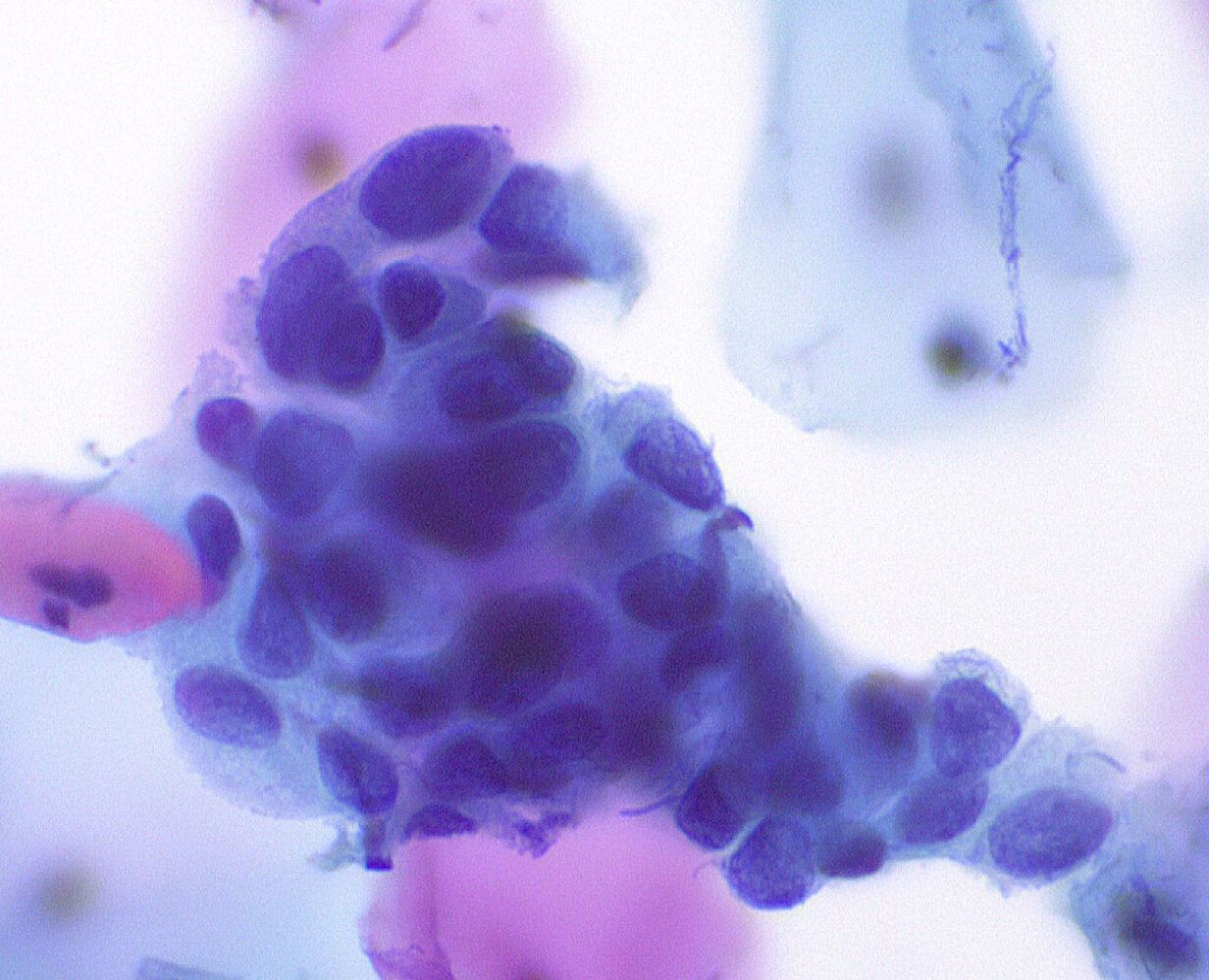
Photomicrograph of squamous cells of the cervix (Papanicolaou stain; very high magnification;)
There is a loosely connected group of abnormal squamous epithelial cells (blue-green cytoplasm). The nuclei are variable in size with a high nuclear-cytoplasmic ratio and there are course clumps of chromatin. The large cell with pink cytoplasm is a normal superficial squamous cell.
These findings are characteristic of severe dysplasia as seen in high-grade squamous intraepithelial lesion (HSIL).
Source: “High-Grade SIL, ThinPrep” by Ed Uthman, Flickr, licensed under CC BY 2.0.
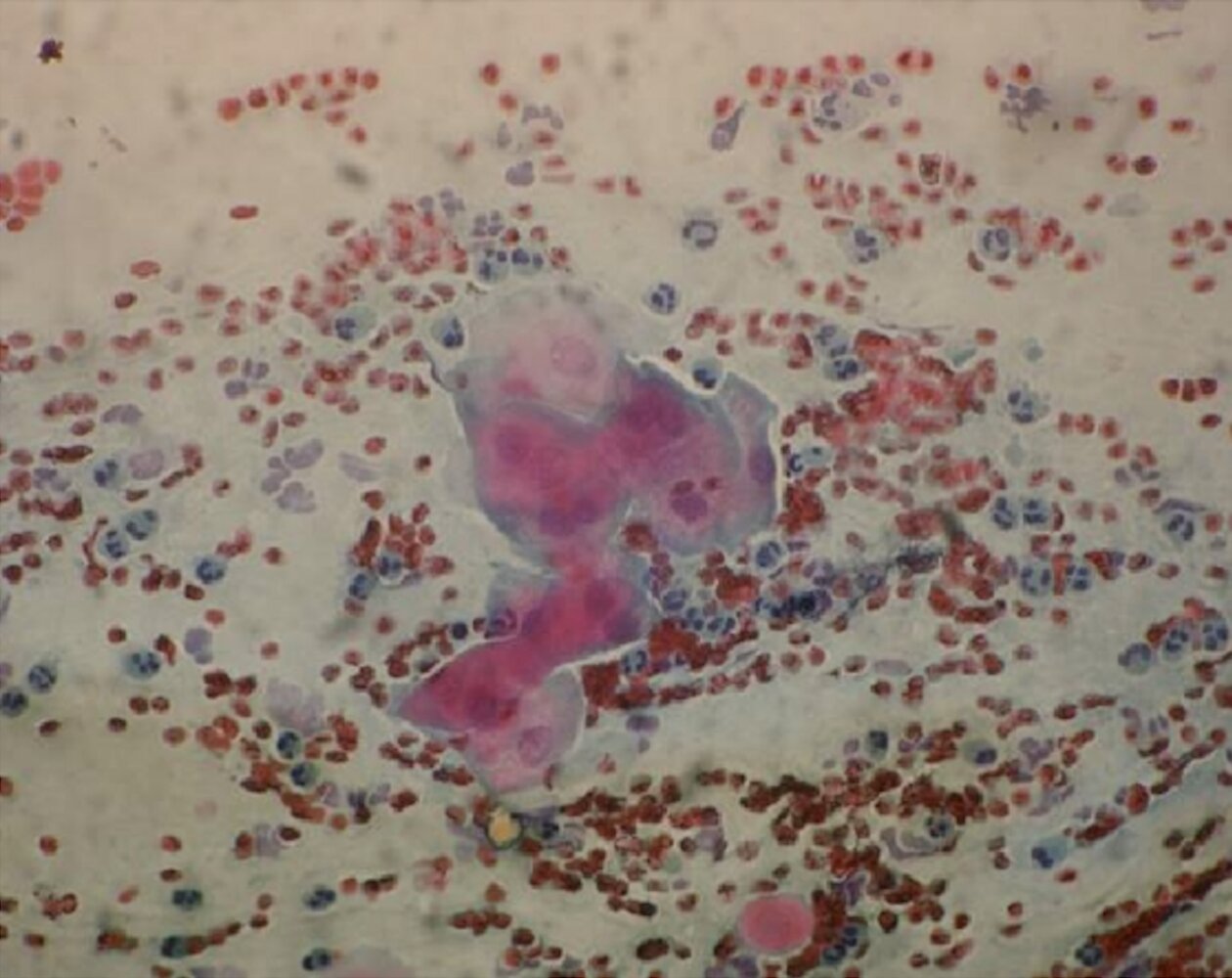
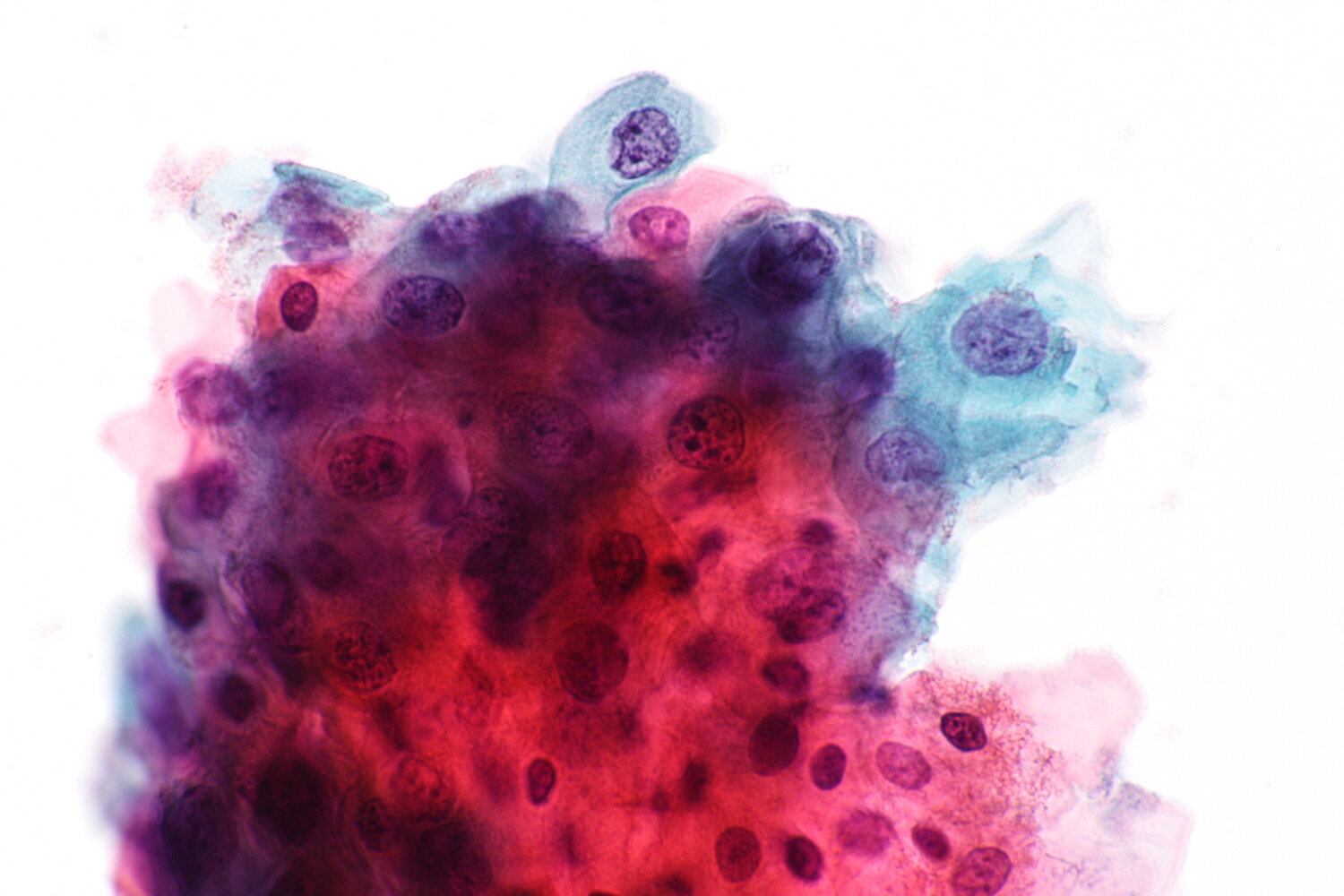
Photomicrograph of a cervicovaginal Pap smear (Papanicolaou stain; high magnification)
Multiple erythrocytes (examples indicated by yellow outlines) and neutrophils (indicating inflammation; examples indicated by arrowheads) can be seen. The center of the image shows a cluster of predominantly eosinophilic squamous cells (blue overlay) with disproportionally large nuclei (increased nuclear-cytoplasmic ratio; examples indicated by dashed outlines).
These findings are consistent with atypical squamous cells (ASC). High-grade squamous intraepithelial lesion (HSIL) cannot be excluded.
Source: “Fig 2D, In: Evaluation of Microbial Enzymes in Normal and Abnormal Cervicovaginal Fluids of Cervical Dysplasia: A Case Control Study” by Dasari S, Rajendra W, Valluru L, Hindawi, licensed under CC BY 3.0. Modifications: image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
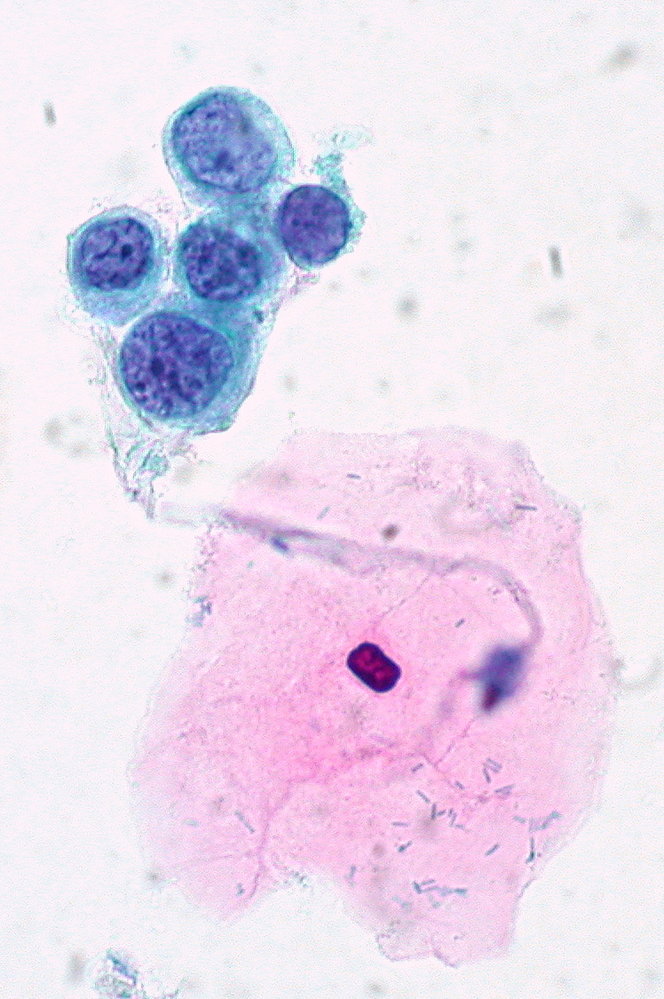
Photomicrograph of glandular cells of the cervix (liquid-based cytology (LBC); high magnification)
The endocervical cells are clumped and form a cluster. They also have atypically crowded hyperchromatic nuclei.
These findings are characteristic of atypical glandular cells (AGC) and are associated with malignant or premalignant disease.
Source: “Fig 3A, In: A Review of Computational Methods for Cervical Cells Segmentation and Abnormality Classification” by Conceição T, Braga C, Rosado L, Vasconcelos MJM, MDPI, licensed under CC BY 4.0. Modifications: image cropped.
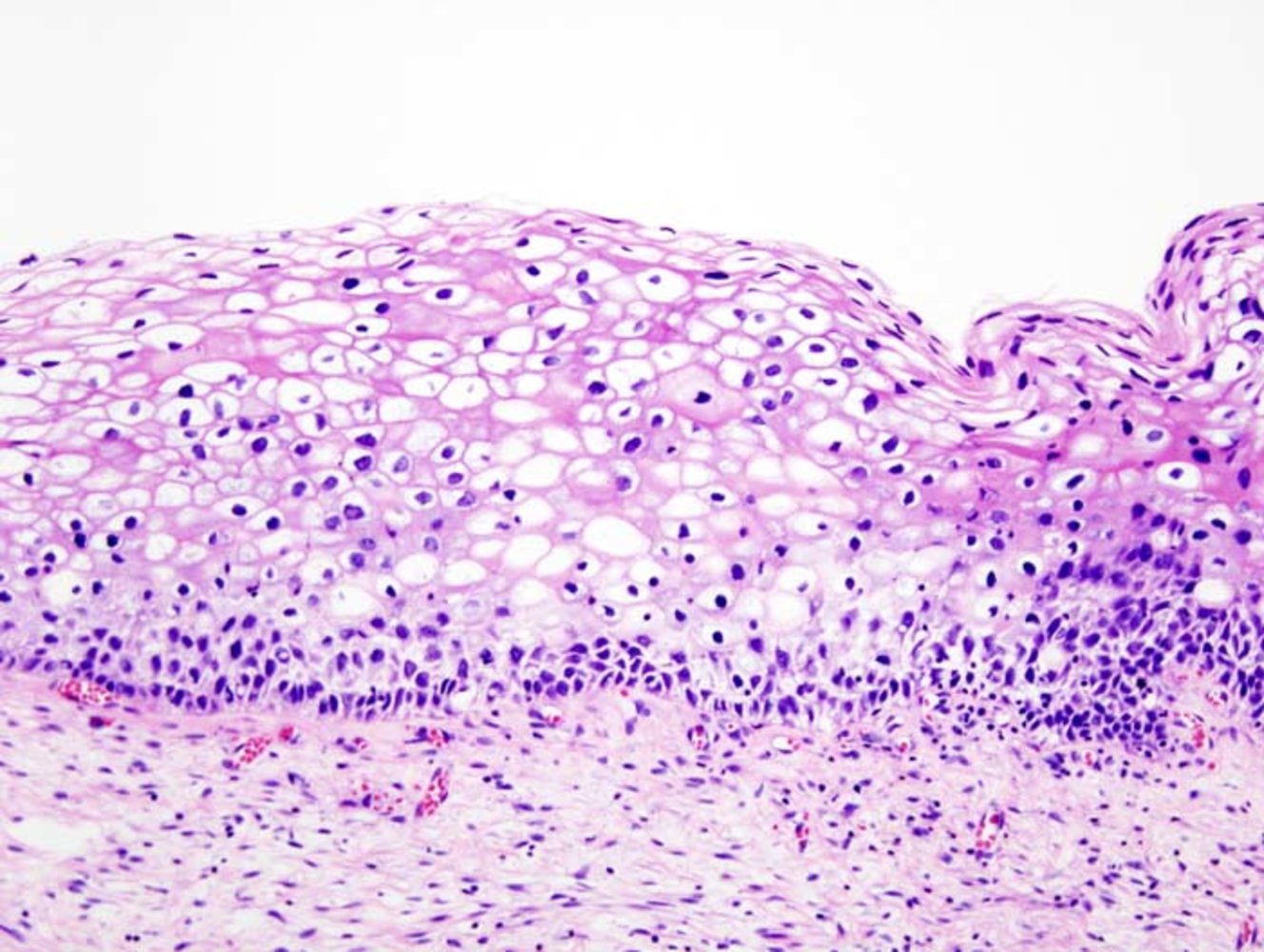
Photomicrograph of a cervical biopsy specimen (H&E stain; medium power magnification)
The cervical squamous epithelium shows loss of regular stratification of the basal and intermediate cell layers. Additionally, features of cellular atypia can be seen within these layers (irregular, enlarged, and hyperchromatic nuclei, indicated by arrowheads), and an abundance of koilocytes (epithelial cells with perinuclear halos and raisinoid nuclei, examples indicated by yellow overlay) are visible. A binucleated koilocyte can also be seen (arrow).
These features indicate a high-grade squamous intraepithelial lesion (HSIL/CIN2). This diagnosis was confirmed by immunohistochemistry (elevated MIB-1 and p16-positive).
Source: “Cervical intraepithelial neoplasia (2) koilocytosis” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
_koilocytosis.jpg){kind=link}
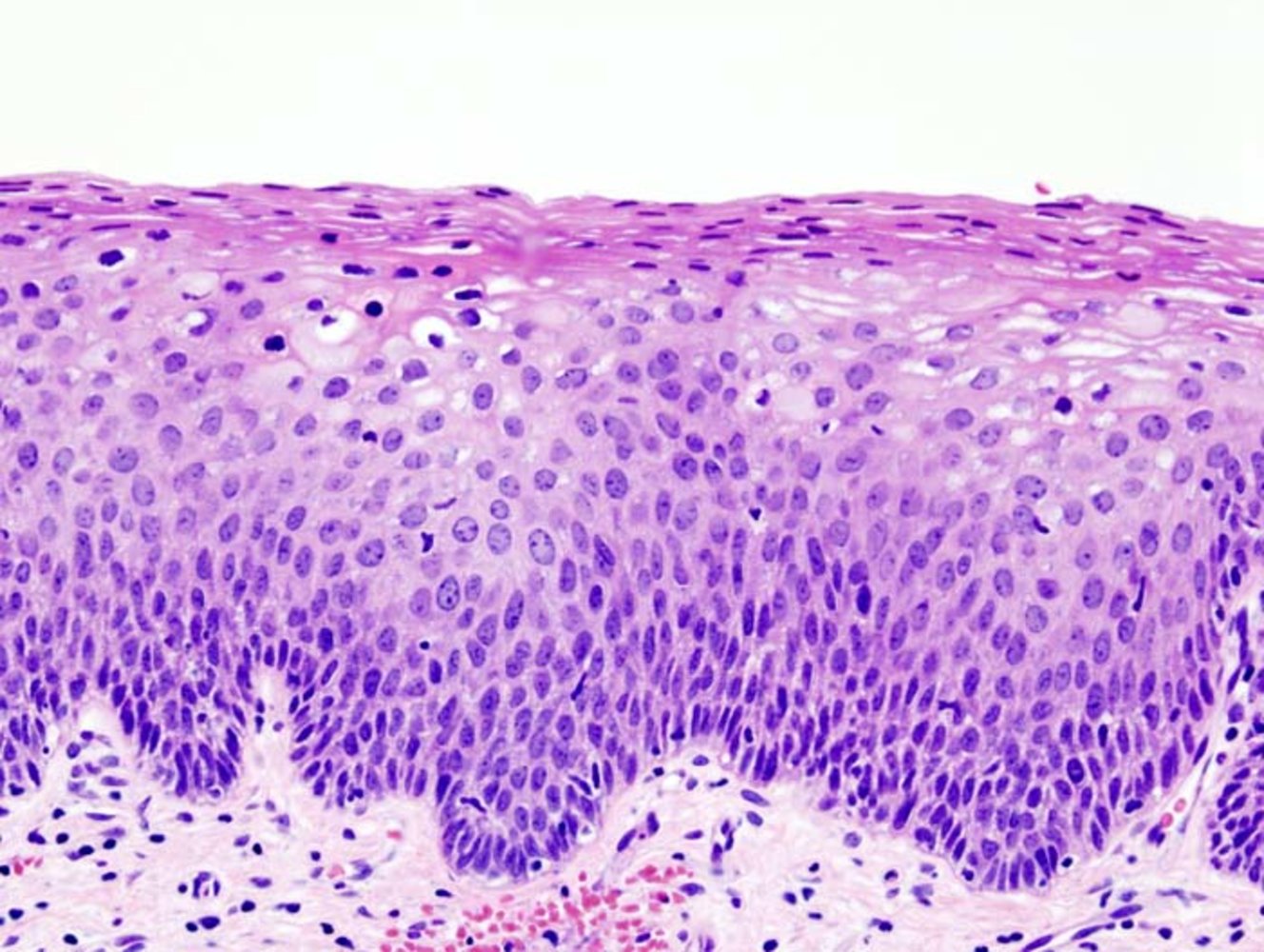
Photomicrograph of cervical tissue sample (high magnification; hematoxylin & eosin stain)
There is a loss of epithelial architecture extending into the middle third of the epithelium therefore the parabasal and intermediate layers cannot be differentiated. There is a high nuclear-cytoplasmic ratio, overlapping nuclei, and nuclear atypia. Epithelial cells with perinuclear halos are present, these cells are koilocytes and indicate HPV infection.
These findings are consistent with moderate dysplasia and (CIN II)
Source: “Cervical intraepithelial neoplasia (3) CIN2” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0.
_CIN2.jpg){kind=link}
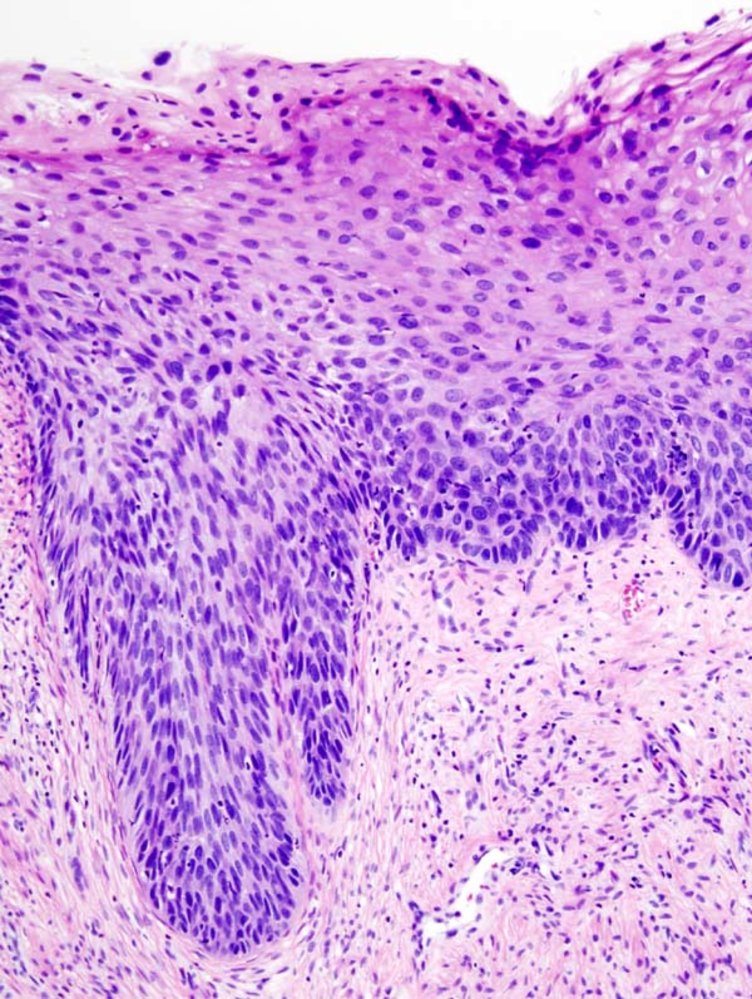
Photomicrograph of cervical tissue (H&E stain; very high magnification;)
There is a loss of epithelial architecture involving more than two-thirds of the epithelium, but the basement membrane is still intact. There is a high nuclear-to-cytoplasmic ratio, overlapping nuclei, and nuclear atypia. Mitotic figures can be seen. Epithelial cells with perinuclear halos are present in the superficial layers; these cells are koilocytes and indicate HPV infection.
These findings are consistent with severe dysplasia and (CIN III), and the changes are irreversible
Source: “Cervical intraepithelial neoplasia (4) CIN3” by KGH, Wikimedia Commons, licensed under CC BY-SA 3.0.
_CIN3.jpg){kind=link}
Overview of screening recommendations
Cervical cancer screening should be performed in all individuals with a cervix (regardless of their HPV vaccination status or sexual history). This includes individuals who are pregnant, have same-sex partners, have a history of a supracervical hysterectomy, or are transgender. [6][7][8][9]
- Goal: early detection and treatment of cervical cancer precursors [6][10]
- Initial screening modalities: primary HPV test, cytology-alone screening, and HPV/Pap cotesting [5][6][7][9]
- Screening modalities and intervals differ for individuals at average risk of cervical cancer and those with high-risk conditions for cervical cancer.
- See also “Cervical cancer screening during pregnancy” as needed.
Average-risk individuals [5][6][7][11]
An overview of recommendations is described here. See “Cervical cancer screening for individuals at average risk” for details.
Recommended screening period
- 21–65 years of age
- The American Cancer Society recommends initiating screening at 25 years of age. [6]
Management of abnormalities detected on screening
The “ASCCP Management Guidelines App & Web Application” can be used to estimate risk and determine the appropriate next steps; see “Tips & Links.”
-
Women ≥ 25 years of age: Management is based on the individual's risk of having or developing CIN3+ (risk-based approach).
- High risk: expedited treatment (i.e., treatment without a preceding colposcopic biopsy)
- Low risk: colposcopic biopsy or surveillance
-
Women < 25 years of age: A result-based approach is recommended.
- High-grade lesions: colposcopy and biopsy (expedited treatment is not recommended)
- Low-grade lesions: surveillance
Management of abnormalities detected on cervical histology
In women who undergo colposcopy and biopsy for abnormalities detected on screening, further management is determined by cervical histology results.
- HSIL (CIN3): Excisional treatment is recommended regardless of the patient's age.
-
HSIL (CIN2) or LSIL (CIN1)
- Women < 25 years of age: surveillance
- Women ≥ 25 years of age: excisional treatment, diagnostic excision, or surveillance (depending on the test results)
Long-term follow-up
- Following treatment of a high-grade cervical lesion, surveillance should be continued for at least 25 years.
High-risk individuals [5][7][9]
An overview of recommendations is described here. See “Cervical cancer screening for individuals at high risk” for details.
-
High-risk conditions for cervical cancer include:
-
Immunocompromised state
- Individuals living with HIV infection
- Individuals on immunosuppressive therapy
- Solid organ transplant recipient
- Allogeneic stem cell transplant recipient
- Exposure to diethylstilbestrol in utero
- Current or past abnormal cervical lesion
-
Immunocompromised state
- Initiate screening within a year of penetrative sexual activity; in women living with HIV, start screening at the time of HIV diagnosis.
- Life-long screening is recommended.
Screening modalities
hrHPV genotyping [5][6][12]
- Cervical cells are collected (similar to Pap smear collection) and screened for high-risk HPV genotypes via PCR-based assays.
- Samples may be collected by the patient themselves (self-sampling) or as an office procedure.
- Findings
- hrHPV positive: active (transient or persistent) infection with one or more high-risk HPV genotypes
- hrHPV negative: no active infection with high-risk HPV genotypes at the time of testing
Papanicolaou test (Pap smear/cervical cytology)
- A cytological test in which a cell sample from the cervix is stained with Papanicolaou dye and examined for cellular abnormalities, including precancerous changes
- Proper sample collection is essential.
- Findings are described under “Cervical cytology findings.”
Sample collection [6][9][13]
- Visualize the cervix (including the cervical transformation zone) using a sterile speculum.
- If needed, cleanse the cervix using a saline-soaked cotton swab.
- Insert the collection device in the external os. [14]
- An extended-tip spatula used in conjunction with an endocervical brush; or an endocervical broom can be used.
- A plastic device is preferred for liquid-based cytology.
- Rotate the device to scrape the endocervix, ectocervix, and the transition zone. [13]
- Extended-tip spatula and endocervical brush
- Insert the extended tip of the spatula into the endocervix, and gently rotate it 360° around the external os a few times (in one direction).
- Next, insert the endocervical brush into the endocervical canal and slowly rotate it 180° in one direction.
-
Endocervical broom
- Insert the central bristles into the endocervix; ensure that the shorter bristles are in contact with the ectocervix.
- Rotate the broom 5 times in the same direction.
- Extended-tip spatula and endocervical brush
- Prepare the sample for staining with Papanicolaou dye. [7]
- Conventional cytology: Smear and fixate the sample on a labeled glass slide.
- Liquid-based cytology (LBC): Rinse the sample in the preservative medium.
Conventional cytology should be performed 10–20 days after the first day of menses, while liquid-based cytology can be performed at any time. [9]
If using a spatula in conjunction with an endocervical brush, both samples can be placed on a single slide or within a single vial of the preservative medium. [13]
HPV/Pap cotesting [5][6]
- A cervical cancer screening strategy in which both cervical cytology (Pap smear) and HPV DNA testing are performed.
- Findings [5]
- Low-grade cotest result
- HPV-positive LSIL
- HPV-positive ASC-US
- HPV-positive NILM on two consecutive annual screens
- High-grade cotest result: any high-grade cervical cytology (regardless of HPV test result)
- Low-grade cotest result
Endocervical sampling [12][15]
Indications [15]
- To identify CIN2+ in the following high-risk situations:
- High-grade cytology results
- Cytological HSIL
- Atypical squamous cells that cannot exclude HSIL, atypical glandular cells, or carcinoma
- HPV test positive for HPV 16 or HPV 18
- Squamocolumnar junction (SCJ) not fully visualized at colposcopy
- Individuals who were previously treated for suspected precancer
- High-grade cytology results
- Consider endocervical sampling in:
- Women ≥ 40 years of age who are undergoing colposcopy
- All patients with CIN 2 who are opting for surveillance instead of treatment
Tools and procedure [15][16]
- Endocervical curette: Circumferentially scrape the endocervical canal with the curette (using a rotational motion or an in-and-out motion); preferably under colposcopic guidance.
- Endocervical brush (cytobrush) : Swipe the endocervix approx. 12 times with the brush. [12]
Endocervical sampling is contraindicated in pregnancy because of the increased risk of complications (e.g., cervical or membrane perforation, pregnancy loss). [5][15]
Endocervical samples and cervical biopsies should be sent in separate, clearly marked containers for histopathological or cytological examination. [12][15]
p16 immunohistochemistry (p16 IHC) [1][5]
-
Indications [1]
- Histological diagnosis of CIN2 (on cervical cancer screening)
- To rule out benign differential diagnoses of precancerous lesions
- Findings: Strong, diffuse p16 staining indicates that the lesion is more likely high-grade (precancerous).
The natural course of p16-positive CIN1 or p16-negative CIN3 is not currently known. Hence, p16 IHC is not routinely recommended for histologically unequivocal CIN1 or CIN3 as it does not change management. [1]
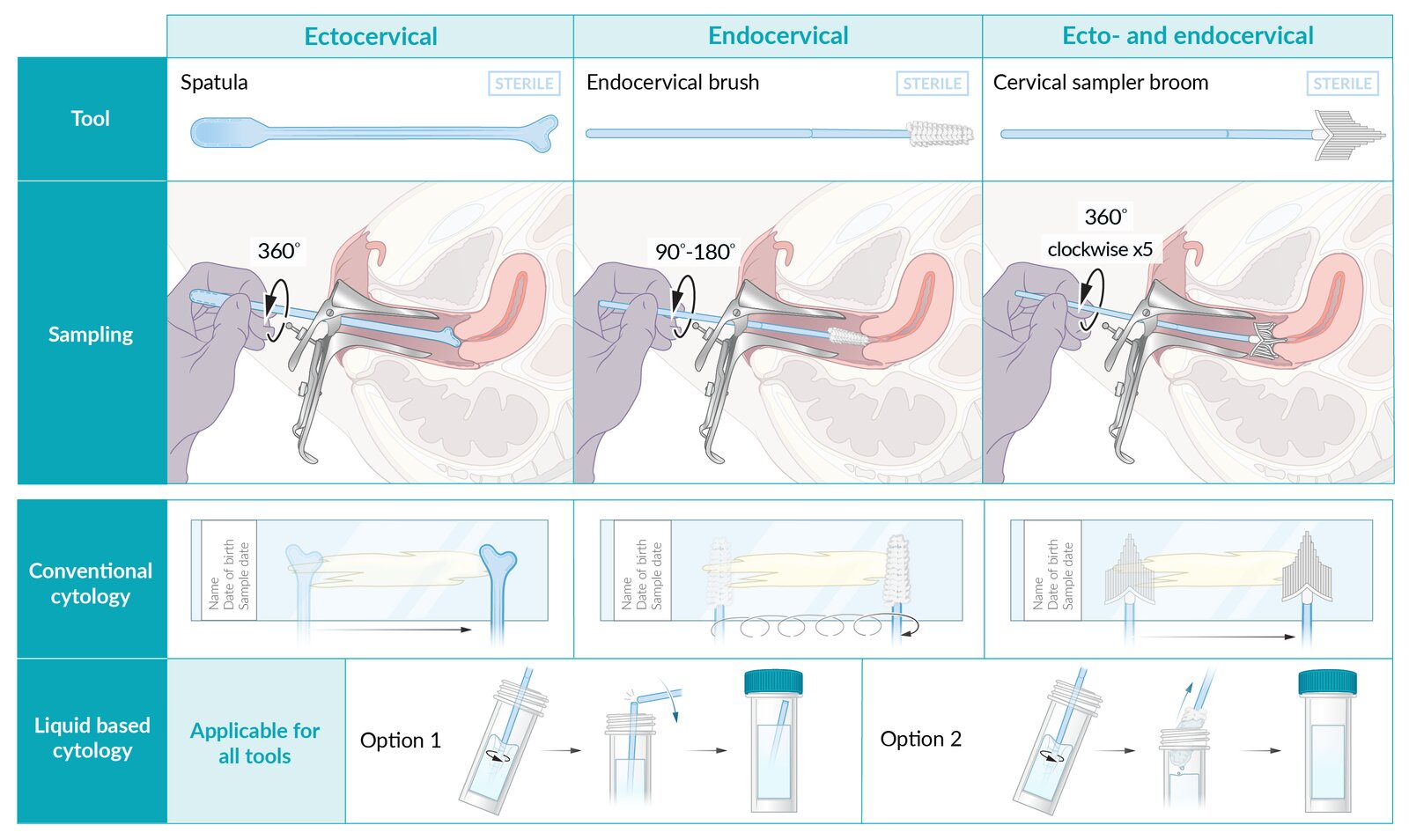
Sample collection tools:
– To obtain the necessary ecto- and endocervical sample, an extended-tip spatula can be used in conjunction with an endocervical brush, or a cervical broom can be used to sample the ecto- and endocervix simultaneously.
Sampling:
– If using the spatula and brush: The extended tip of the spatula is inserted into the endocervix, and gently rotated 360° around the external os a few times in one direction. Next, the endocervical brush is inserted into the endocervical canal and slowly rotated 90°–180° in one direction.
– If using the endocervical broom: The central bristles are inserted into the endocervix, ensuring that the shorter bristles are in contact with the ectocervix. The broom is rotated 5 times in the same direction.
Preparing the sample for staining with Papanicolaou dye:
– Conventional cytology: The sample is smeared on a labeled glass slide and fixated.
– Liquid-based cytology: The sample is rinsed in a vial of preservative medium. Depending on the device used, the head of the device may then be broken off and remain in the vial (option 1), or the device may be withdrawn (option 2).
© AMBOSS. See related article for detailed procedural guidance.
Source: “Fig 6, In: Introducing a novel model for simulating large loop excision of the transformation zone (LLETZ) using 3D printing technique” by Kiesel M, Beyers I, Kalisz A et al., SpringerLink, licensed under CC BY 4.0. Modifications: image cropped & removal of the letters E, F.
Screening protocols
Standard first-line screening protocols [5][6][7][12]
- Primary HPV testing (preferred): FDA-approved hrHPV genotyping (without Pap smear)
- Cytology-alone screening: Pap smear alone (without HPV genotyping)
- HPV/Pap cotesting: Pap smear with hr-HPV genotyping
According to the 2020 American Cancer Society (ACS) recommendations, primary HPV testing is the preferred modality for cervical cancer screening. Cytology-alone screening and HPV/Pap cotesting are acceptable alternatives if FDA-approved HPV tests are unavailable. [6][17]
Primary HPV testing and HPV/Pap cotesting are more accurate at cervical cancer risk estimation than cytology-alone screening. [5]
Reflex triage testing [5][11]
If the initial primary HPV test or cytology-alone test is positive, a reflex triage testing should be performed, ideally on the same laboratory specimen.
- Positive cytology-alone screening: Reflex hrHPV genotyping is performed to identify HPV 16 or HPV 18 infections.
- Positive primary HPV testing (regardless of genotype): Reflex cervical cytology is performed.
If reflex cervical cytology on the same laboratory specimen is not feasible in patients who are positive for HPV 16 or HPV 18, colposcopy should be performed; and a new sample for triage testing with cytology should be collected at colposcopy. [5]
Screening individuals at average risk for cervical cancer
The following recommendations are applicable to asymptomatic immunocompetent individuals who do not have a high-risk condition for cervical cancer.
Screening recommendations vary. The main differences are:
-
Age to start screening
- ACS: 25 years
- USPSTF: 21 years
-
Screening modality
- ACS: FDA-approved primary HPV testing is preferred for all age groups.
-
USPSTF
- Women ≥ 30 years: Any of the three standard initial screening protocols is acceptable.
- Women 21–29 years of age: Cytology-alone screening is recommended.
| Age-appropriate cervical cancer screening for individuals at average risk | ||
|---|---|---|
| USPSTF (2018) [5][7][8][12][17][18] | ACS (2020) [6][17] | |
| Recommended screening period |
|
|
| Screening modalities |
|
|
| Discontinuation of screening [6][7][17][18] |
|
|
Screening is not routinely recommended for average-risk individuals < 21 years because HPV infections and cervical intraepithelial neoplasias in this age group are likely to resolve without intervention. [7][9]
In the absence of any life-limiting conditions, individuals > 65 years without previously documented negative results should continue to be screened until criteria to discontinue are met. [6]
Initial management for abnormal results
- The following information applies to immunocompetent nonpregnant individuals ≥ 25 years of age with abnormalities detected on cervical cytology and/or HPV testing.
- See “Exceptions to the risk-based approach” for management of screening abnormalities in women < 25 years of age.
- See also “Cervical cancer screening during pregnancy”, and “Screening immunocompromised individuals for cervical cancer” as needed.
Risk assessment [5][11][12][17][19]
- CIN3 is a direct precursor to invasive cervical cancer.
- Management of abnormalities detected on cervical cancer screening depends on their risk of having or developing CIN3+.
- Risk estimation is based on several parameters, such as:
- Current results of HPV-based testing
- Past screening results
- Patient age, hysterectomy status, immune status, and presence of high-risk conditions for cervical cancer
- The “ASCCP Management Guidelines App & Web Application” can be used to estimate risk and determine the appropriate next steps; see “Tips & Links.”
Formerly, the management approach for abnormal cervical cancer screening was determined by test results alone, but recent recommendations have shifted to a risk-based approach. [5][11]
Personalized risk-based management [5][11][19]
Immediate risk of CIN3 ≥ 4%
High risk of CIN3
- Expedited treatment is preferred.
-
Options include:
- Excisional treatment (preferred): removal of the cervical transformation zone via loop electrosurgical excision procedure (LEEP), cold knife conization, and laser cone biopsy
- Ablation: includes cryotherapy, thermoablation, and laser ablation
Lower risk of CIN3
- Perform colposcopy and cervical biopsy.
- See “Management of abnormalities detected on cervical histology” for further management.
Immediate risk of CIN3 < 4%
- Surveillance with HPV-based testing every 1–5 years is recommended.
- Cytology-alone testing is acceptable only if HPV-based testing is not available.
Shared decision-making is recommended when considering expedited treatment. Patients should be informed of the risks and benefits of expedited treatment and its potential adverse effects on future pregnancy (e.g., PROM after LEEP). [5][6][20]
Exceptions to the risk-based approach [5]
- A result-based (rather than risk-based) approach to managing abnormalities detected on screening is indicated in the following select situations.
- An overview of the management of these situations is described below; refer to the “ASCCP Management Guidelines App & Web Application” in “Tips & Links” for further details.
Women < 25 years of age [5]
Management of cervical abnormalities detected on cytology-alone screening in this group of individuals includes:
-
Low-grade lesions (LSIL or ASC-US)
- Repeat cytology-alone screening annually for the next two years.
- If repeat cytology is normal for two consecutive years, resume age-appropriate screening.
- Colposcopy is recommended if a high-grade lesion is detected on repeat screening.
-
High-grade lesions (HSIL or ASC-H)
- Perform colposcopy and biopsy.
- See “Management of abnormalities detected on cervical histology” for further management.
Expedited treatment is not recommended in women < 25 years of age with high-grade cervical cytology as most cervical abnormalities in this population undergo spontaneous regression. [5]
Women ≥ 25 years of age with any of the following abnormalities detected on screening [5]
Colposcopy and cervical biopsy (followed by management of abnormalities detected on cervical histology) are recommended for all of the following scenarios.
- ASC-H on cytology (regardless of the HPV result)
- NILM on cytology in individuals positive for HPV 16 or HPV 18
- LSIL or higher on cytology-alone testing [21][22]
- Persistent HPV positive and/or persistent ASC-US or higher on cytology on repeat testing [12][21][22]
- If exact risk estimation is not feasible in an individual with two consecutive positive HPV tests [21][22]
Certain cervical cytology results [5]
-
Unsatisfactory cytology
- Patient of any age with unknown or negative HPV test result: Repeat age-appropriate cervical cancer screening in 2–4 months.
- Positive for HPV 16 or HPV 18: Colposcopy followed by management of abnormalities detected on cervical histology.
-
Patient ≥ 25 years of age with a positive HPV test (untyped)
- Repeat cytology-alone testing in 2–4 months
- OR colposcopy followed by management of abnormalities detected on cervical histology
-
Absent transformation zone
- Women 21–29 years of age: Continue routine age-appropriate screening; reflex HPV testing is not recommended.
- Women ≥ 30 years of age: Perform reflex HPV testing.
- HPV negative: Continue routine age-appropriate screening.
- HPV positive: Perform HPV-based test in 1 year; followed by risk-based management.
- Benign endometrial cells in postmenopausal women: Endometrial sampling is recommended.
-
Atypical glandular cells (AGC) or endocervical adenocarcinoma in situ (AIS)
- Colposcopy with endocervical sampling is appropriate for all nonpregnant individuals with AGCs to rule out cervical cancer, regardless of HPV test results.
-
Endometrial sampling to rule out endometrial cancer should be performed in nonpregnant individuals with AGC and any of the following:
- Age ≥ 35 years
-
Age < 35 years with:
- Abnormal uterine bleeding
- Risk factors for endometrial cancer (e.g., obesity, chronic anovulation)
- See “Management of abnormalities detected on cervical histology” for further management.
{kind=link}
Subsequent management after colposcopy and biopsy
Some individuals need to undergo colposcopy and biopsy for further evaluation of abnormalities detected on cervical cancer screening. Subsequent management is determined by the patient's age, abnormalities detected on cervical histology, and the preceding cervical cytology results.
General principles [5][11]
- Excisional treatment (e.g., LEEP, conization, laser cone biopsy) is preferred over ablation to manage histological HSIL.
- If surveillance is being considered:
- The following criteria should be met:
- The entire squamocolumnar junction and the upper limit of the lesion are fully visualized on colposcopy
- No CIN2+ or ungraded CIN detected on endocervical sampling
- In women < 25 years of age: Surveillance with colposcopy and cervical cytology is recommended.
- In women ≥ 25 years of age: Surveillance with colposcopy and/or HPV-based testing is recommended.
- The following criteria should be met:
- Consider p16 immunohistochemistry to: [1][5]
- Rule out a benign condition (e.g., benign epithelial change)
- Better identify high-grade CIN2 lesions
- An overview of the initial management of these situations is described below; refer to the “ASCCP Management Guidelines App & Web Application” in “Tips & Links” for further details, including surveillance intervals.
HPV infections are highly prevalent in women < 25 years of age, therefore, HPV-based testing is not recommended for surveillance in this group of individuals. [5]
If criteria for surveillance are not met, a diagnostic excisional procedure is recommended. [5]
Histological HSIL (CIN3) [5][11]
- All nonpregnant patients: Excisional treatment is recommended.
- Pregnant patients: See “Cervical cancer screening during pregnancy.”
CIN3 is an immediate precursor to invasive cervical cancer and should be treated regardless of age, unless the patient is pregnant. [5]
Hysterectomy is not recommended for the management of histological HSIL. [5]
Histological HSIL (CIN2) [5][11]
-
Women ≥ 25 years of age
- Consider excisional treatment for all nonpregnant patients.
- Surveillance may be considered if the patient's concerns about potential adverse effects on future pregnancies outweigh their concerns about cancer.
- Women < 25 years of age: Surveillance is recommended.
Histological HSIL unspecified [5][11]
- Women ≥ 25 years of age: Excisional treatment is recommended for all nonpregnant patients.
- Women < 25 years of age: Surveillance is acceptable.
Histological LSIL (CIN1) [5][11]
- Women ≥ 25 years of age: Consider surveillance, diagnostic excision, or treatment (excision or ablation) depending on the preceding cervical cytology results.
- Women < 25 years of age: Surveillance is recommended.
Endocervical adenocarcinoma in situ (AIS) [5][11]
- A diagnostic excisional procedure to rule out invasive cancer is recommended (even if hysterectomy is planned)
- Further management depends on the status of the excised margins.
- Positive margins
- Re-excision to achieve negative margins is recommended.
- Followed by simple or modified radical hysterectomy and follow-up for HSIL (cervix)
- Negative margins
- A simple hysterectomy is recommended.
- Close surveillance is acceptable in select cases if fertility preservation is desired.
- Positive margins
Follow-up after treatment of high-grade cervical lesions
- Individuals with high-grade cervical histology (HSIL CIN2, CIN3, or AIS) or high-grade cervical cytology (HSIL, persistent ASC-H) have a high risk of developing invasive cervical cancer even after treatment.
- Continued surveillance is recommended for at least 25 years after treatment even if the patient is > 65 years of age (unless there are life-expectancy-limiting conditions).
Women ≥ 25 years of age [5][11]
-
HPV-based testing is recommended at the following intervals.
- At 6 months after treatment
- Followed by annual HPV-based testing until three consecutive tests are negative
- Continued surveillance every 3 years for at least 25 years
Women < 25 years of age [5]
-
Cervical cytology is recommended at the following intervals.
- At 6 months after treatment
- Followed by 6-monthly cervical cytology until three consecutive tests are negative
- Continue annual cytology-alone surveillance until 25 years of age and then transition to HPV-based testing.
Screening individuals at high risk for cervical cancer
Immunocompromised state [5][23][24]
-
Age to start screening
- Individuals ≥ 21 years of age who are living with HIV: at the time of initial diagnosis with HIV [23][24]
- Other immunocompromised individuals: within 1 year of initial penetrative sexual activity [5]
-
Screening modalities and intervals
-
Age 21– 29 years
- Annual cytology-alone screening for 3 years
- If three consecutive screenings are negative, screening intervals can be increased to once every 3 years.
- Age ≥ 30 years: cytology-alone screening OR cotesting every 3 years
-
Age 21– 29 years
-
Management of abnormalities detected on screening
-
Colposcopy is recommended in the following cases:
- Cervical cytology of LSIL or higher (regardless of HPV test result, if performed)
- HPV positive ASC-US or higher
- Refer to the “ASCCP Management Guidelines App & Web Application” for management of other abnormalities; see “Tips & Links.”
-
Colposcopy is recommended in the following cases:
- Duration of screening: Lifelong screening is recommended. [5][9][23][24]
Although lifelong screening for cervical cancer is recommended for all immunocompromised individuals, other factors (e.g., life expectancy, risk of developing cervical cancer at a certain age) should also be taken into consideration. [23]
Immunocompromised individuals of any age with even low-grade cytologic abnormalities on screening are at high risk of invasive cervical cancer. [5][23]
In-utero exposure to diethylstilbestrol [6]
- These individuals are at a significantly increased risk of developing cervical cancer precursors and clear-cell carcinoma of the cervix.
- An individualized screening plan in consultation with a specialist is recommended.
Current or past abnormal cervical lesion
- See “Follow-up after treatment of high-grade cervical lesions.”
Screening during pregnancy
- All pregnant women should receive age-appropriate cervical cancer screening. [5][9][11]
- Screening modalities and intervals are the same as those for nonpregnant individuals. [9]
-
Management of pregnant individuals with high-grade lesions differs from that of nonpregnant patients.
- Suspected invasive cervical cancer
- A diagnostic excisional procedure is recommended to confirm the diagnosis.
- See “Management of invasive cervical cancer during pregnancy” for further details.
-
HSIL (CIN2 or CIN3)
- Colposcopic surveillance with HPV-based testing every 12–24 weeks is preferred.
- Deferring colposcopy until ≥ 4 weeks after delivery is acceptable.
- Endocervical AIS: Refer to a gynecologic oncologist for further management.
- Suspected invasive cervical cancer
Colposcopy and biopsy are safe during pregnancy and should ideally be performed by an experienced physician as physiological changes of the cervix during pregnancy make it difficult to detect abnormalities. [5]
Treatment of premalignant lesions (e.g., CIN2, CIN3) can be deferred until the postpartum period. [5]
Expedited treatment for HSIL, endocervical curettage, and endometrial biopsies are contraindicated during pregnancy. [5]
External Resources
- ASCCP Management Guidelines Web Application for Cervical Cancer Screening
- 2024 CDC Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV
- 2021 ACOG Practice Advisory: Updated Cervical Cancer Screening Guidelines
- 2020 ACS Guideline: Cervical Cancer Screening for Individuals at Average Risk
- 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors
- 2018 USPSTF Recommendation Statement: Screening for Cervical Cancer
- 2017 ASCCP Colposcopy Standards
References
- Curry SJ, Krist AH, et al. "Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement". JAMA. 320(7). :674-686. (2018)
- American Academy of Family Physicians. "Clinical Preventative Service Recommendation: Cervical Cancer". Am Fam Physician. (2019)
- "Updated Cervical Cancer Screening Guidelines". https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2021/04/updated-cervical-cancer-screening-guidelines. [2021-04-01]
- Perkins RB, Guido RS, Castle PE, et al. "2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors". J Low Genit Tract Dis. 24(2). :102-131. (2020)
- Marcus JZ, Cason P, Downs LS, Einstein MH, Flowers L. "The ASCCP Cervical Cancer Screening Task Force Endorsement and Opinion on the American Cancer Society Updated Cervical Cancer Screening Guidelines". J Low Genit Tract Dis. 25(3). :187-191. (2021)
- Burness JV, Schroeder JM, Warren JB. "Cervical Colposcopy: Indications and Risk Assessment". Am Fam Physician. 102(1). :39-48. (2020)
- Fontham ETH, Wolf AMD, Church TR, et al. "Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society". CA Cancer J Clin. 70(5). :321-346. (2020)
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- Saslow D, Runowicz CD, Solomon D, et al. "American Cancer Society Guideline for the Early Detection of Cervical Neoplasia and Cancer". CA Cancer J Clin. 52(6). :342-362. (2002)
- Schooff M, Lawlor A. "What is the best collection device for screening cervical smears?". Am Fam Physician. 69(7). :1661-2. (2004)
- Massad LS, Perkins RB, Naresh A, et al. "Colposcopy Standards: Guidelines for Endocervical Curettage at Colposcopy". J Low Genit Tract Dis. 27(1). :97-101. (2023)
- Damkjær M, Laursen JB, Petersen LK, et al. "Endocervical sampling in women with suspected cervical neoplasia: a systematic review and meta-analysis of diagnostic test accuracy studies". Am J Obstet Gynecol. (2022)
- Darragh TM, Colgan TJ, Cox JT, et al. "The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: Background and Consensus Recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology". Arch Pathol Lab Med. 136(10). :1266-1297. (2012)
- Egemen D, Cheung LC, Chen X, et al. "Risk Estimates Supporting the 2019 ASCCP Risk-Based Management Consensus Guidelines". J Low Genit Tract Dis. 24(2). :132-143. (2020)
- "Updated Guidelines for Management of Cervical Cancer Screening Abnormalities - 2020 (reaffirmed in 2022)". https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/10/updated-guidelines-for-management-of-cervical-cancer-screening-abnormalities. [2020-10-01]
- Sadler L. "Treatment for Cervical Intraepithelial Neoplasia and Risk of Preterm Delivery". JAMA. 291(17). :2100. (2004)
- Perkins RB, Guido RS, Castle PE, et al. "Erratum: 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors". J Low Genit Tract Dis. 25(4). :330-331. (2021)
- Massad LS, Einstein MH, Huh WK, et al. "2012 Updated Consensus Guidelines for the Management of Abnormal Cervical Cancer Screening Tests and Cancer Precursors". J Low Genit Tract Dis. 17(Supplement 1). :S1-S27. (2013)
- Wipperman J, Neil T, Williams T. "Cervical Cancer: Evaluation and Management". Am Fam Physician. 97(7). :449-454. (2018)
- "CDC - Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: Human Papillomavirus Disease 2021 (reviewed 2023)". https://web.archive.org/web/20241203115123/https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/human?view=full. [2023-01-11]
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV: Human Papillomavirus Disease". https://web.archive.org/web/20240802161116/https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf. [2024-07-09]
- Park KJ, Soslow RA. "Neoplastic Lesions of the Cervix". Elsevier. :227-293. (2020). ISBN: 9780323359092
- Nayar R, Wilbur DC. "The Pap Test and Bethesda 2014". Acta Cytol. 59(2). :121-132. (2015)
- Apgar BS, Zoschnick L, Wright TC Jr. "The 2001 Bethesda System terminology". Am Fam Physician. 68(10). :1992-8. (2003)