Summary
Cervical lymphadenopathy (LAD) is a > 1 cm enlargement of lymph nodes in the neck. In children, cervical LAD is common and most often represents an inflammatory response to an acute infection, such as a viral upper respiratory infection or strep throat. Less commonly, it can signal a more serious underlying condition (e.g., malignancy, mycobacterial infection, autoimmune disease). Benign nodes are typically small and mobile, while concerning nodes may be large, firm, fixed, and/or accompanied by constitutional symptoms. Diagnosis is primarily clinical, but diagnostic evaluation (e.g., laboratory studies, imaging, lymph node biopsy) may be required in the case of red flag features or diagnostic uncertainty. Management is directed at the underlying cause (e.g., observation for viral infections; antibiotics for suspected bacterial lymphadenitis). Prompt specialist referral is indicated for features suggesting malignancy or other systemic conditions.
Definitions
- Cervical lymphadenopathy is an enlargement of any cervical lymph node to > 1 cm in diameter or a palpable supraclavicular lymph node of any size. [1][2]
- The jugulodigastric lymph node is an exception; a diameter up to 1.5 cm is normal in children < 12 years of age. [1][2]
Etiology
Cervical LAD in children is most often caused by an infectious etiology. Approximately 45% of otherwise healthy children have isolated cervical LAD on physical examination. [1][3]
Acute cervical LAD [1][4][5]
Cervical LAD in children is considered acute if present < 2 weeks. [1][6]
Infectious causes
-
Viruses
- Common respiratory viruses (e.g., adenovirus, influenza virus, respiratory syncytial virus, rhinovirus, coronavirus)
- Enterovirus (i.e., coxsackievirus)
- Rubella
- Measles
- HSV
- Varicella zoster virus
- Bacteria
- Staphylococcus aureus
- Streptococcus pyogenes
- Oral anaerobes
- Less commonly, Haemophilus influenzae, Group B Streptococcus , and Corynebacterium diphtheriae
Noninfectious causes
- Kawasaki disease
- Serum sickness
- Immunizations (e.g., DTaP, polio, typhoid fever vaccines)
Most acute cervical LAD in children is due to viral respiratory infections or acute bacterial lymphadenitis caused by Staphylococcus aureus or Streptococcus pyogenes. [1][4]
Subacute and chronic cervical LAD [1][4][5]
Cervical LAD in children is considered subacute if present for 2–6 weeks and chronic if present for ≥ 6 weeks. [1][6]
Infectious
-
Viruses
- EBV and CMV: most common
- HIV
- Bacteria
- Bartonella henselae
- Mycobacterium tuberculosis
- Nontuberculous mycobacteria (e.g., Mycobacterium avium-intracellulare, Mycobacterium scrofulaceum)
- Pasteurella multocida
- Nocardia brasiliensis
- Treponema pallidum
- Protozoa: Toxoplasma gondii
- Fungi (e.g., Candida, Histoplasma, Coccidioides, and Aspergillus spp.)
Noninfectious
- Autoimmune conditions, e.g.:
- Juvenile idiopathic arthritis
- Systemic lupus erythematosus
-
Malignancy, e.g.:
- Leukemia
- Lymphoma
- Neuroblastoma
- Rhabdomyosarcoma
- Metastatic nasopharyngeal cancer [2]
-
Self-limited inflammatory conditions, e.g.:
- PFAPA syndrome [7]
- Necrotizing lymphadenitis
- Rosai-Dorfman-Destombes disease
Cervical LAD lasting > 6 months without change in size and character or associated systemic symptoms has a low likelihood of being neoplastic in origin. [1][3]
Clinical evaluation
Focused history [1][5]
- Onset, duration, and progression (e.g., change in size or character) of enlarged lymph nodes
- Associated symptoms
- Localized pain and/or tenderness
- Constitutional symptoms
- Symptoms suggesting a primary source of infection, e.g.:
- URI symptoms (e.g., sore throat, rhinorrhea, cough)
- Bacterial infection in the head and neck region (e.g., acute tonsillitis and pharyngitis, periodontal disease)
- Periodontal disease
- Red flags for cervical LAD in children
- Growth faltering [4]
- Exposures to: [5]
- Illness (e.g., tuberculosis)
- Travel
- Animals (e.g., cats or cat feces, rabbits, sheep)
- Recent vaccination (e.g., with DTaP, polio, typhoid fever vaccines)
- Relevant medical history (e.g., immunosuppressed state)
Focused examination [4][5]
- Vital signs, general appearance
-
Head and neck examination, including:
-
Palpation of head and neck lymph nodes
- Size
- Tenderness, warmth, erythema
- Consistency (e.g., soft, fluctuant, firm, rubbery)
- Mobile vs. fixed
- Unilateral vs. bilateral
- Signs of underlying etiology in the drainage region (including the oropharynx and dentition) [4]
-
Palpation of head and neck lymph nodes
- Assessment for red flags for cervical LAD in children
Examine all lymph node regions in children with cervical LAD, as systemic infections (e.g., due to EBV, CMV, HIV, or M. tuberculosis), autoimmune conditions, serum sickness, and malignancy may cause generalized LAD. [3][5]
Red flags for cervical LAD in children [1][5]
The following features prompt evaluation for serious underlying etiology (e.g., malignancy, granulomatous disease, autoimmune conditions).
-
Lymph node characteristics
- Size > 2 cm and/or rapidly enlarging lymph nodes
- Supraclavicular lymph node and/or lower cervical chain lymph nodes (any size)
- Lymph nodes that are hard, firm, rubbery, matted, or fixed
- Lymphadenopathy > 4 weeks
- Generalized lymphadenopathy
- Associated features, including:
- B symptoms
- Hepatosplenomegaly
- Bruising
- Rash
- Arthralgia and/or myalgia
- Children ≥ 8 years of age (red flag for malignancy)
Supraclavicular LAD and posterior cervical triangle LAD carry a much higher risk for malignancy or tuberculosis infection than anterior cervical LAD. [2][4]
Diagnosis
General principles [1][5]
- Diagnostic studies are not routinely recommended.
- Consider targeted diagnostics as needed based on the most likely underlying etiology.
- Refer to a pediatric specialist (e.g., infectious disease, ENT, hematology-oncology, rheumatology) for:
- Atypical infection (e.g., unresponsive to antibiotics)
- Red flags for cervical LAD in children
- Diagnostic uncertainty
- See "Common causes of cervical LAD in children" for characteristic diagnostic findings.
Reactive LAD caused by a viral URTI is the most common cause of acute cervical LAD in children and is diagnosed clinically.[1][5]
Laboratory studies [4][5]
Perform laboratory studies based on suspected underlying etiology of cervical LAD in children, e.g.:
-
Bacterial infection
- CBC
- Blood culture (in febrile or ill-appearing patients)
- Specific diagnostics for suspected causative organism, e.g.:
- Diagnostics of acute tonsillitis
- Diagnostics for tuberculosis
- Diagnostics for cat scratch disease
- Fine-needle aspiration and Gram stain, acid-fast stain, and cultures of lymph node material for anaerobic and aerobic bacteria and mycobacteria
-
Viral infection
- EBV serology
- Diagnostics for CMV
- HIV testing
- Malignancy: CBC, peripheral smear, LDH
- Inflammatory conditions: inflammatory markers (e.g., ESR, CRP)
Imaging [5][8][9]
Imaging is not routinely indicated in the evaluation of cervical LAD in children.
-
Diagnostic uncertainty: ultrasound neck with or without color Doppler ultrasound
- Preferred first-line modality in children
- Useful to differentiate between reactive lymphadenopathy and malignancy
- See "Lymph node ultrasound findings" for details.
-
Suspected malignancy or deep neck infection
- CT scan neck with IV contrast
- MRI neck with or without IV contrast
- Suspected lymphoma or granulomatous disease: chest x-ray
Biopsy [5][5][10]
-
Indications
- LAD of unclear etiology lasting > 4 weeks and unresponsive to antibiotic therapy
- Red flags for cervical LAD in children
- Diagnostic uncertainty
-
Modalities
- Excisional biopsy: preferred if lymphoma is suspected
- Core needle biopsy: Consider as an alternative to excisional biopsy in selected patients.
- Fine-needle aspiration (FNA) biopsy: Consider for persistent LAD of unclear etiology.
Management
Outpatient management is usually appropriate. Consider symptomatic and supportive care (e.g., antipyretics, nonopioid oral analgesia in children) as needed. [5]
Admit acutely ill children to hospital and consult a specialist (e.g., infectious diseases, critical care). Begin management of pediatric sepsis, if indicated.
Treatment of the underlying cause [5]
- Isolated cervical LAD with no red flag features in an otherwise healthy child: reassurance and observation
- Acute lymphadenitis likely due to a viral URTI: observation with follow-up in 2–4 weeks [4]
-
Acute lymphadenitis likely due to a bacterial infection
- Initiate antibiotic therapy (e.g., empiric antibiotic therapy for acute unilateral pyogenic cervical lymphadenitis, antibiotic therapy for GAS pharyngitis).
- Tailor antibiotics when culture and sensitivities are available.
- See "Common causes of cervical LAD in children" for details.
Avoid corticosteroids in patients with suspected acute lymphadenitis until a definitive diagnosis is made; corticosteroids can alter the histopathological appearance of lymphoma or malignancy. [5]
Referrals [5]
- Suspected malignancy: urgent referral to hematology-oncology
- Suspected periodontal disease: pediatric dentist
- Other specialists (e.g., infectious diseases, surgery, rheumatology) for additional studies and management of:
- Persistent LAD after observation for suspected viral etiology
- Inadequate response to antibiotic therapy within 72 hours
- Atypical infection (e.g., Mycobacterium tuberculosis, nontuberculous mycobacteria, fungal infection) [4]
- Suspected rheumatologic condition
Common causes
Common causes of acute cervical LAD in children
| Common causes of acute cervical LAD in children [1][4][5] | |||
|---|---|---|---|
| | Clinical features | Diagnostic findings | Management |
| Viral upper respiratory infection [1] |
|
|
|
| GAS pharyngitis [11][12] |
|
|
|
| Acute unilateral pyogenic cervical lymphadenitis [3][4][6][13] |
|
|
|
| Kawasaki disease (KD) [15][16] |
|
|
|
The most common causes of acute unilateral cervical lymphadenitis in children are Staphylococcus aureus and Streptococcus pyogenes. [1][4]
The most common causes of acute bilateral cervical lymphadenitis in children are viral infections and GAS infections. [1][4]
Common causes of subacute and chronic cervical LAD in children
| Common causes of subacute and chronic cervical LAD in children [1][5] | |||
|---|---|---|---|
| | Clinical features | Diagnostic findings | Management |
| Infectious mononucleosis [17][18] |
|
|
|
| Nontuberculous mycobacterial infection [1] |
|
|
|
| Mycobacteria tuberculosis [19] |
|
|
|
| Localized cat scratch disease [4][6] |
|
|
|
| Malignancy [1][5] |
|
|
|
| Toxoplasmosis [1][23] |
|
|
|
| PFAPA syndrome [7] |
|
|
|
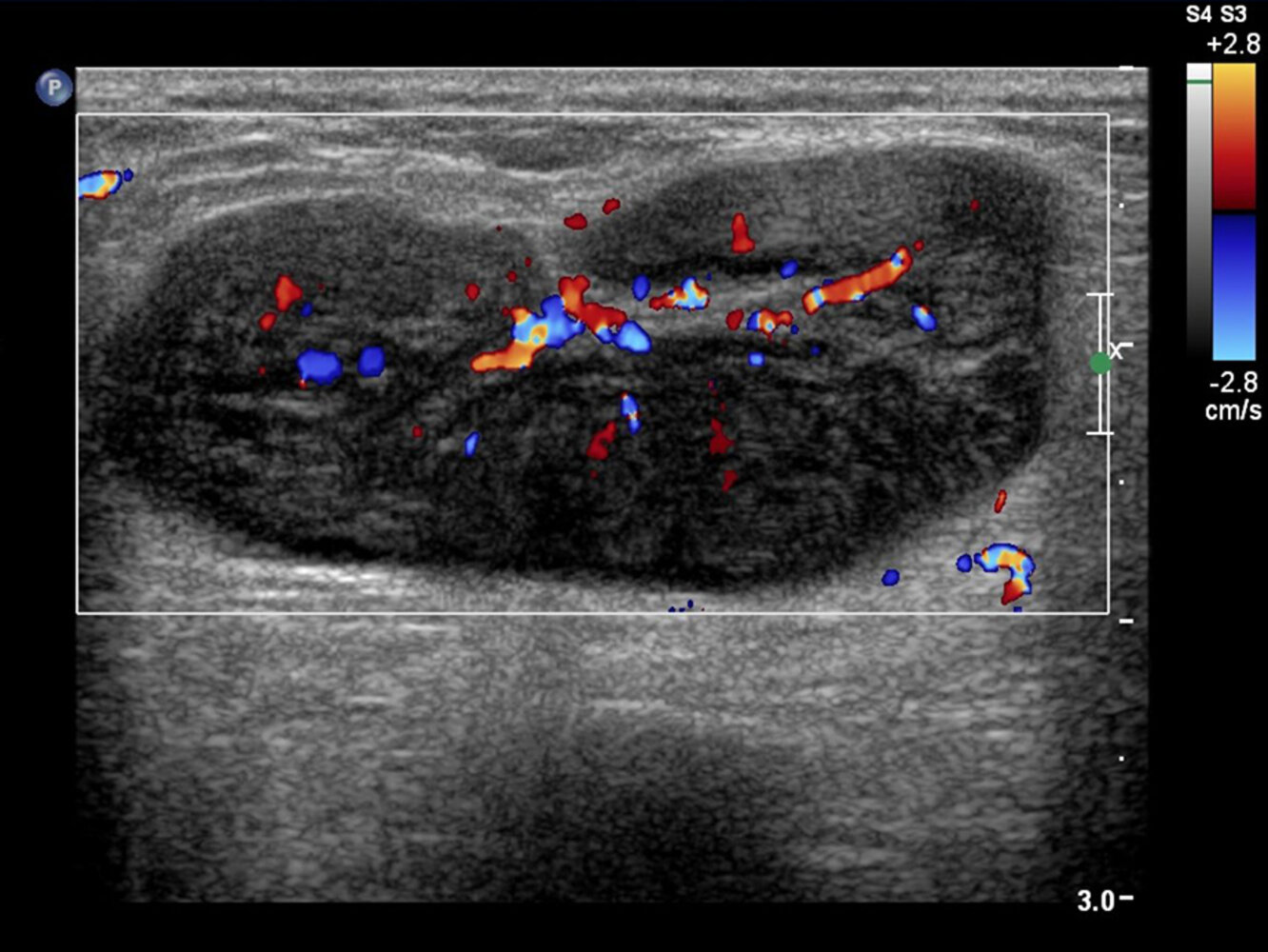
Ultrasound lymph node (with color Doppler; longitudinal plane) of a patient with lymphoma
An enlarged lymph node has maintained a reniform shape and well-demarcated margins. However, the region of the normally echogenic fatty hilum is atypically small (green overlay), and the node is more hypoechoic than normal, with increased posterior acoustic enhancement (yellow overlay). In addition, the parenchyma shows a pattern of reticulation (examples indicated by arrowheads), which has been described in lymphomatous nodes.
Ultrasound performed for lymph node evaluation assesses such characteristics as size, shape, parenchymal heterogeneity, cortical thickness, margin sharpness, and hilar visibility. There is an overlap in the ultrasound appearances of lymph nodes in primary and secondary malignancy and benign nodal disease.
Red and blue: hilar vessels
Image source of original image: sonographiebilder.de - Innere Medizin des Albertinen-Krankenhauses Hamburg. Original title: “Lymphom_Farbe_02”. Created by: Dr. J. Guntau. Modifications to original image: text removed, cropped image.
Mimics
Cervical lymphadenopathy is the most common neck mass in children. Other causes of neck masses in children include:
- Congenital and developmental neck masses [2][4][8]
- Thyroglossal duct cyst (second most common neck mass in children) [25]
- Branchial cleft cyst
- Dermoid cyst, epidermoid cyst
- Cystic hygroma
- Laryngocele
- Fibromatosis colli and congenital muscular torticollis
- Vascular malformations and tumors
-
Neoplastic masses [2]
- Thyroid cancer
- Tumors of the salivary glands
- Benign soft tissue tumor (e.g., pilomatrixomas, lipomas, fibromas, neurofibromas)
- Rhabdomyosarcoma
- Neuroblastoma [25]
- Metastatic nasopharyngeal carcinoma
- Other neck masses [4]
- Parotitis (e.g., due to mumps)
- Cervical rib
- See also "Mimics" in “Lymphadenopathy.”
External Resources
References
- Rosenberg T, Nolder A. "Pediatric Cervical Lymphadenopathy". Otolaryngol Clin North Am. 47(5). :721-731. (2014)
- Gaddey HL, Riegel AM. "Unexplained Lymphadenopathy: Evaluation and Differential Diagnosis". Am Fam Physician. 94(11). :896-903. (2016)
- Leung A, Davies H. "Cervical lymphadenitis: Etiology, diagnosis, and management". Curr Infect Dis Rep. 11(3). :183-189. (2009)
- Falk N, Joseph R, Dieujuste M. "Lymphadenopathy: Evaluation and Differential Diagnosis". Am Fam Physician. 112(3). :286-293. (2025)
- Gosche J, Vick L. "Acute, subacute, and chronic cervical lymphadenitis in children". Semin Pediatr Surg. 15(2). :99-106. (2006)
- Meier JD, Grimmer JF. "Evaluation and management of neck masses in children". Am Fam Physician. 89(5). :353-8. (2014)
- CARRA PFAPA Consensus Treatment Plan Workgroup, Amarilyo G, Rothman D, et al. "Consensus treatment plans for periodic fever, aphthous stomatitis, pharyngitis and adenitis syndrome (PFAPA): a framework to evaluate treatment responses from the childhood arthritis and rheumatology research alliance (CARRA) PFAPA work group". Pediatr Rheumatol. 18(1). (2020)
- Aulino J, Kirsch C, Burns J, et al. "ACR Appropriateness Criteria® Neck Mass-Adenopathy". J Am Coll Radiol. 16(5). :S150-S160. (2019)
- Ludwig B, Wang J, Nadgir R, et al. "Imaging of Cervical Lymphadenopathy in Children and Young Adults". American Journal of Roentgenology. 199(5). :1105-1113. (2012)
- Vaughn C, Fialkowski E, McDuffie L. "Pediatric Lymph Node Biopsy: Indications, Techniques, and Complications". Eur J Haematol. (2025)
- Dremmen M, Tekes A, Mueller S, et al. "Lumps and Bumps of the Neck in Children—Neuroimaging of Congenital and Acquired Lesions". J Neuroimaging. 26(6). :562-580. (2016)
- The Infectious Disease Society. "Errata: Shulman ST et al (Clin Infect Dis 2012; 55: e86-e102)". Clinical Infectious Diseases. 58(10). :1496-1496. (2014)
- Kalra MG, Higgins KE, Perez ED. "Common questions about streptococcal pharyngitis". Am Fam Physician. 94(1). :24-31. (2016)
- Fraser I. "Suppurative lymphadenitis". Curr Infect Dis Rep. 11(5). :383-388. (2009)
- Peters TR, Edwards KM. "Cervical lymphadenopathy and adenitis". Pediatr Rev. 21(12). :399-405. (2000)
- McCrindle BW, Rowley AH, Newburger JW, et al. "Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association". Circulation. 135(17). (2017)
- Gorelik M, Chung SA, Ardalan K, et al. "2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Kawasaki Disease". Arthritis Care Res. 74(4). :538-548. (2022)
- Sylvester JE, Buchanan BK, Silva TW. "Infectious Mononucleosis: Rapid Evidence Review". Am Fam Physician. 107(1). :71-78. (2023)
- Committee on Infectious Disease, American Academy of Pediatrics. "Red Book: 2024-2027 Report of the Committee on Infectious Diseases, 33rd Edition". American Academy of Pediatrics. (2024). ISBN: 9781610027373
- Fontanilla JM, Barnes A, et al. "Current Diagnosis and Management of Peripheral Tuberculous Lymphadenitis". Clinical Infectious Diseases. 53(6). :555-562. (2011)
- Mohapatra PR, Janmeja AK. "Tuberculous lymphadenitis". J Assoc Physicians India. 57. :585-90. (2009)
- Koutantou M, Kambas K, Makka S, et al. "Limitations of Serological Diagnosis of Typical Cat Scratch Disease and Recommendations for the Diagnostic Procedure". Can J Infect Dis Med Microbiol. 2023. :1-11. (2023)
- Ahuja AT, Ying M. "Sonographic Evaluation of Cervical Lymph Nodes". Am J Roentgenol. 184(5). :1691-1699. (2005)
- Furtado J, Smith J, Belfort R, Gattey D, Winthrop K. "Toxoplasmosis: A global threat". J Glob Infect Dis. 3(3). :281. (2011)
- Batu E. "Periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome: main features and an algorithm for clinical practice". Rheumatol Int. 39(6). :957-970. (2019)
- "Cervical Lymphadenitis"