Summary
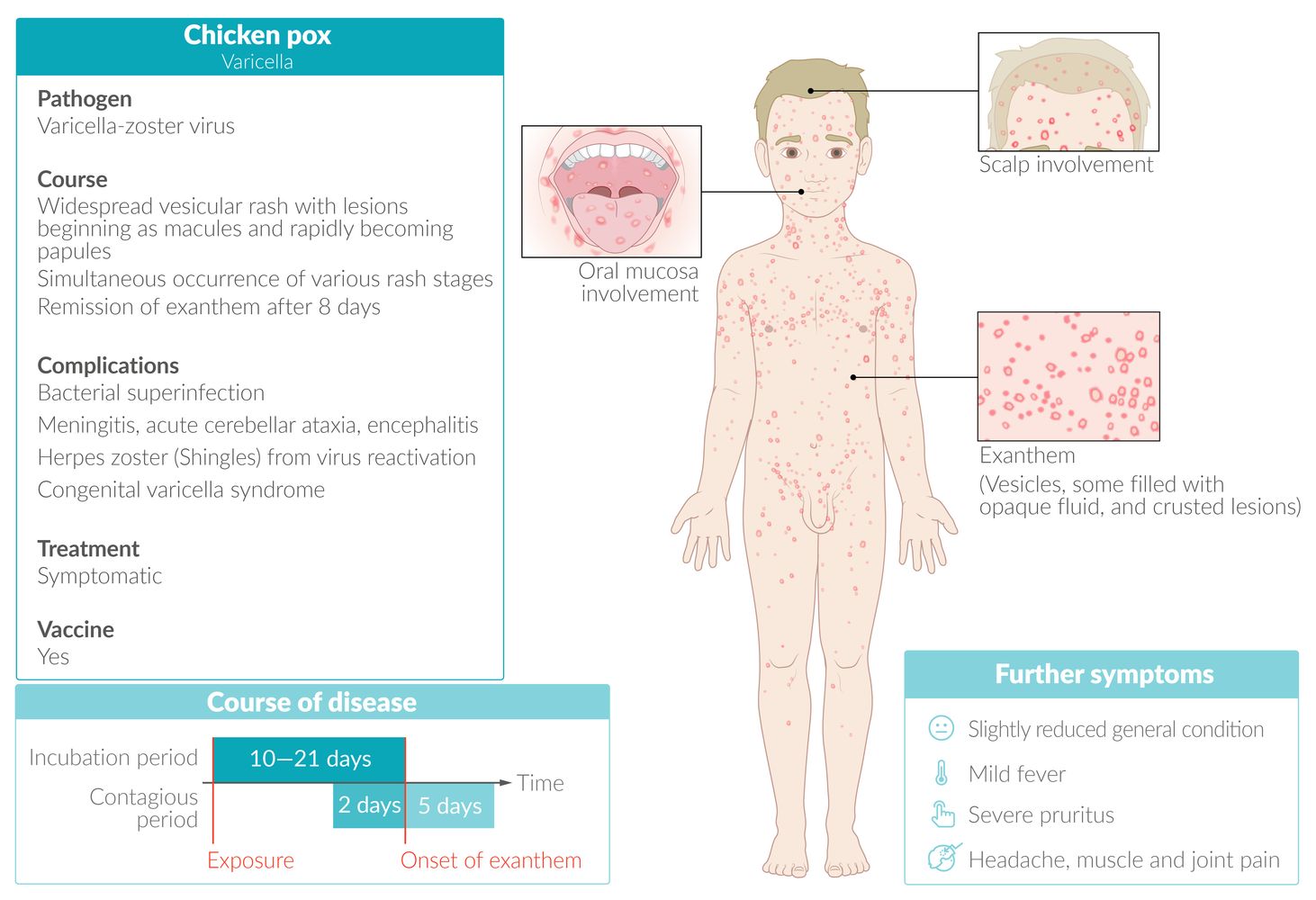
Chickenpox (i.e., varicella) is an infection caused by the varicella zoster virus (VZV). The condition predominantly affects children. Transmission occurs via inhalation of airborne droplets and direct contact with respiratory secretions or skin lesion fluids. Chickenpox manifests with an intensely pruritic rash characterized by sequential clusters of papules, vesicles, and pustules in various stages of development; the rash may be preceded by a prodrome of constitutional symptoms. A clinical diagnosis is made based on the appearance of the rash; confirmatory testing may be obtained for atypical rashes or severe infection. In immunocompetent individuals, chickenpox is self-limiting and managed symptomatically. Antiviral therapy is reserved for patients with severe infection or at high risk for complications (e.g., bacterial superinfection, invasive infections). Following resolution, the virus remains latent in the sensory nerve root ganglia; it can reactivate (see “Shingles”) during episodes of stress or immunosuppression. Prevention includes routine vaccination and, when indicated, postexposure prophylaxis.

© AMBOSS
Epidemiology
- Primarily occurs in children
- Before vaccines were widely introduced, ∼ 90% of all children had been infected by the age of 15.
References:[1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Pathogen: : varicella zoster virus (VZV), a human herpesvirus type 3 (HHV-3) [2]
-
Transmission [2]
- Airborne droplets
- Direct skin contact with VZV-infected vesicle fluid
- Transplacental
-
Infectivity
- Highly contagious
- Two days before and up to five days after the onset of exanthem (or until all the lesions have formed crusts) [3]
- Latency: can become latent after primary infection and reside inside the trigeminal and/or dorsal root ganglia [2]
Risk factors for severe VZV infection [3][4][5]
Individuals with any of the following factors are at risk of severe primary infection if they have no evidence of VZV immunity:
- Age > 12 years
- Immunosuppression
- Pregnancy
- Chronic skin or lung disease [3]
- Long-term salicylate therapy (e.g., aspirin)
-
Infancy
- < 28 days of age [6]
-
Premature infants during their initial hospitalization with any of the following:
- Born at < 28 weeks gestation
- Birth weight < 1 kg
- Born at ≥ 28 weeks to a nonimmune mother
- Household exposure [3]
Clinical features
- Incubation period: ∼ 2 weeks [3]
-
Prodrome phase (rare in children) [7]
- Constitutional symptoms (e.g., fever, malaise, headache, muscle or joint pain)
- 2–3 days prior to the onset of exanthem
-
Exanthem phase: characterized by approx. 250–500 severely pruritic lesions in varying stages of development ; [3][7]
- Lesion stages: papules→ superficial vesicles filled with clear fluid on an erythematous base (“dewdrop on rose petal” appearance) → umbilicated and crusted pustules → scabs fall off after 1–3 weeks, (often leaving a depressed base)
-
Skin involvement [3][7][8]
- Lesions first manifest centrally (i.e., face, scalp, and trunk) and spread to the extremities.
- The rash is ultimately distributed across the body, with the highest concentration of lesions in the central areas.
- Mucous membranes may be affected (typically oropharyngeal, and possibly urogenital).
- Ocular involvement may be present (see “VZV conjunctivitis”).
- Palms and soles are typically spared.
-
Features of severe varicella infection may develop, e.g.: [3]
- Prolonged high fever (> 1 week)
- Prolonged eruption of vesicles (> 5 days) [2]
- Signs of thrombocytopenia, including hemorrhagic skin lesions
- Symptoms of visceral dissemination (e.g., encephalitis, pneumonia)
- Latent phase: Following resolution of active skin infection, VZV remains latent in the sensory root ganglia; it can later reactivate (see "Shingles”). [7] [3]
Severe varicella infection is characterized by the prolonged eruption of vesicles, which are sometimes hemorrhagic, high fever > 1 week, and dissemination of VZV to the brain (encephalitis), liver (hepatitis), and/or lungs (pneumonia). [3]




")






A vesicle filled with clear fluid on an erythematous base is seen on the skin of this patients.
This appearance is referred to as a "dewdrop on a rose petal" and, in combination with other skin lesions, indicates infection with varicella-zoster virus (chickenpox).
Source: Courtesy of Dr. Gary M. White, MD

A diffuse rash is seen in various stages of lesion evolution (starry-sky appearance), with mainly ruptured vesicles and crusted erosions seen here.
These findings are typical for chickenpox.
This image is an adaptation. Source of original image: Wikimedia Commons. Original title: “Waterpokken”. Created by: Postertjack. Licensed under Public Domain. Modifications to original image: Pixelation of the orbital area.
{kind=link}

The face of the girl shows macules, vesicles, and papules on an erythematous base, as well as erupted vesicles and crusted papules. The simultaneous occurrence of various stages of rash is sometimes described as "starry sky" and is typical of chickenpox.
Source: "ID#: 10486", CDC/ Dr. John Noble, Jr., Centers for Disease Control and Prevention (CDC) licensed under Public Domain

A vesicle on an erythematous base, located on the right side of the hard palate.
Source: "ID#: 3176", CDC/ Heinz F. Eichenwald, MD, Centers for Disease Control and Prevention (CDC) licensed under Public Domain

Two small aphthae are visible at the tip of the tongue and one on the right side.
Aphthae are nonspecific; in this case, they were associated with varicella infection.
Source: Courtesy of Dr. Gary M. White, MD

Upper body of a young boy with exanthem showing the simultaneous occurrence of various stages of rash; mainly vesicles and pustules, no crusted erosions. This clinical finding is also referred to as "starry sky" and is typical of chickenpox.
Source: "Varicela Aranzales", Camiloaranzales, Wikimedia Commons licensed under Public Domain
{kind=link}

Two papules and a vesicle (center) are visible. The cloudy appearance of the vesicle fluid indicates that it is in the course of transitioning into a pustule.
The development of a rash manifesting with various stages simultaneously is typical of chickenpox.
Source: Courtesy of Dr. Gary M. White, MD

Chest of a child
Multiple vesicles filled with clear fluid on an erythematous base are visible.
This clinical finding is called "dewdrops on a rose petal," and it is classically seen in varicella (chickenpox).
Source: Courtesy of Dr. Gary M. White, MD

Multiple disseminated papules and vesicles on an erythematous base are visible on this patient's face. Numerous vesicles in the preauricular region appear umbilicated.
These lesions are caused by an infection with varicella zoster virus (VZV).
Source: “Varicelle importante chickenpox” by Grook da oger, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}

Photograph of skin lesions in various stages of evolution
Multiple cutaneous lesions are visible across the skin surface. Early lesions appear as erythematous macules, some of which have progressed to raised papules. Several papules have developed into superficial vesicles filled with clear fluid on an erythematous base. Older lesions show umbilicated pustules and crusting.
This polymorphic eruption is characteristic of varicella.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Subtypes and variants
Breakthrough varicella infection [3][9]
- Definition: a wild-type VZV infection that occurs in individuals who have received ≥ 1 dose of the chickenpox vaccine ≥ 42 days prior to symptom onset [3][9][10]
- Infectivity: infectious to close contacts [9]
-
Clinical features: generally mild compared to typical chickenpox infection [3]
- Manifests ≥ 42 days following any dose of chickenpox immunization [9][10]
- Shorter duration of illness and lower likelihood of fever
- Typically < 50 skin lesions with few or no vesicles (predominantly maculopapular lesions)
- Diagnosis: PCR test confirms a wild-type strain of VZV; see “Diagnostics of chickenpox.” [11][12]
- Treatment: Usually supportive; follow varicella infection prevention measures to reduce spread.
Vaccine-associated chickenpox rash [3][9][13]
- Definition: A vaccine-type VZV infection that occurs following chickenpox immunization. [11][14]
- Incidence: manifests in 5–10% of healthy individuals following chickenpox immunization [11]
- Infectivity: may rarely infect close contacts [9]
-
Clinical features
- A mild illness similar to breakthrough varicella infection [3][9][11]
- Typically manifests 5– 42 days (21 days median) after varicella immunization [9][14]
- Lesions are often present at the immunization injection site. [3]
- Diagnosis: PCR testing of lesions confirms vaccine-type strain (i.e., Oka strain); see “Diagnostics of chickenpox.” [11][12][13]
- Treatment: supportive
Diagnosis
General principles
- Typically diagnosed clinically based on characteristic clinical features
- Confirmatory diagnostic studies are usually only considered in the following cases: [2][15]
- Suspected VZV infection in patients with no rash or uncharacteristic rash
- Vaccinated patients with suspected varicella
- Patients with immunocompromised contacts
- Additional studies may be required for patients with severe infections.
Confirmatory studies [15][16]
- PCR (preferred test for active infection): detects VZV DNA [2][17][18]
- Direct fluorescent antibody testing on vesicular fluid
- Serology (IgM and IgG detection) can identify primary infection and serologic immunity. [3][15][17]
- Viral culture [7][17]
- Tzanck smear: not specific for VZV (may also be positive in HSV infections) [19]
Chickenpox is usually diagnosed clinically. Obtain laboratory testing in case of atypical rash or severe infections. [2]
Additional studies
Consider in severe varicella zoster infection, depending on clinical features.
- Bacterial superinfection of lesions: See “Diagnostics for sepsis" and "Diagnostics for pediatric sepsis."
-
Pneumonia [20]
- Chest imaging (CT or x-ray chest)
- Advanced studies: PCR of bronchoalveolar lavage, biopsy of lung tissue
-
Meningoencephalitis [21]
- PCR of CSF
- MRI brain [22]
- Thrombocytopenia: CBC
Visceral dissemination is more common in patients with HIV; consider HIV testing in patients with severe infection. [23]



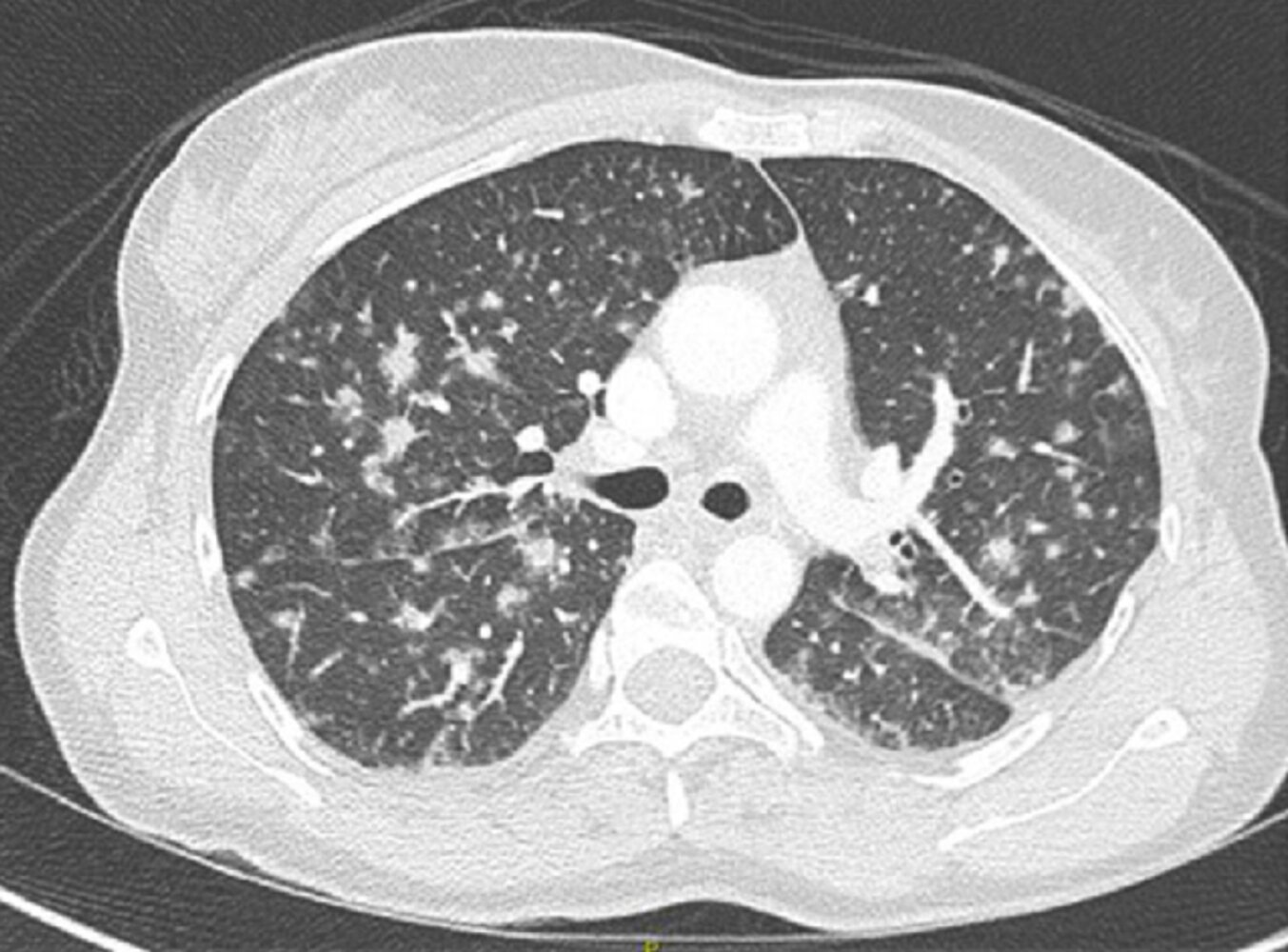
CT chest (lung window; axial plane) of a patient with acute respiratory failure, fever, and a skin rash typical of varicella
Numerous small noncalcified pulmonary nodules are present throughout both lungs (examples indicated by green overlay). Some nodules are circumscribed while others are ill-defined and accompanied by ground glass opacification (examples indicated by red overlay).
The radiographic appearance is compatible with acute varicella pneumonia in this patient with clinical signs and symptoms of varicella. In contrast, healed varicella pneumonia is characterized by the presence of numerous small calcified pulmonary nodules.
Yellow overlay: examples of thickened interlobular septa
Source: “Fig 1, In: Severe varicella-zoster virus pneumonia: a multicenter cohort study” by Mirouse A, Vignon P, Piron P et al., BMC, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
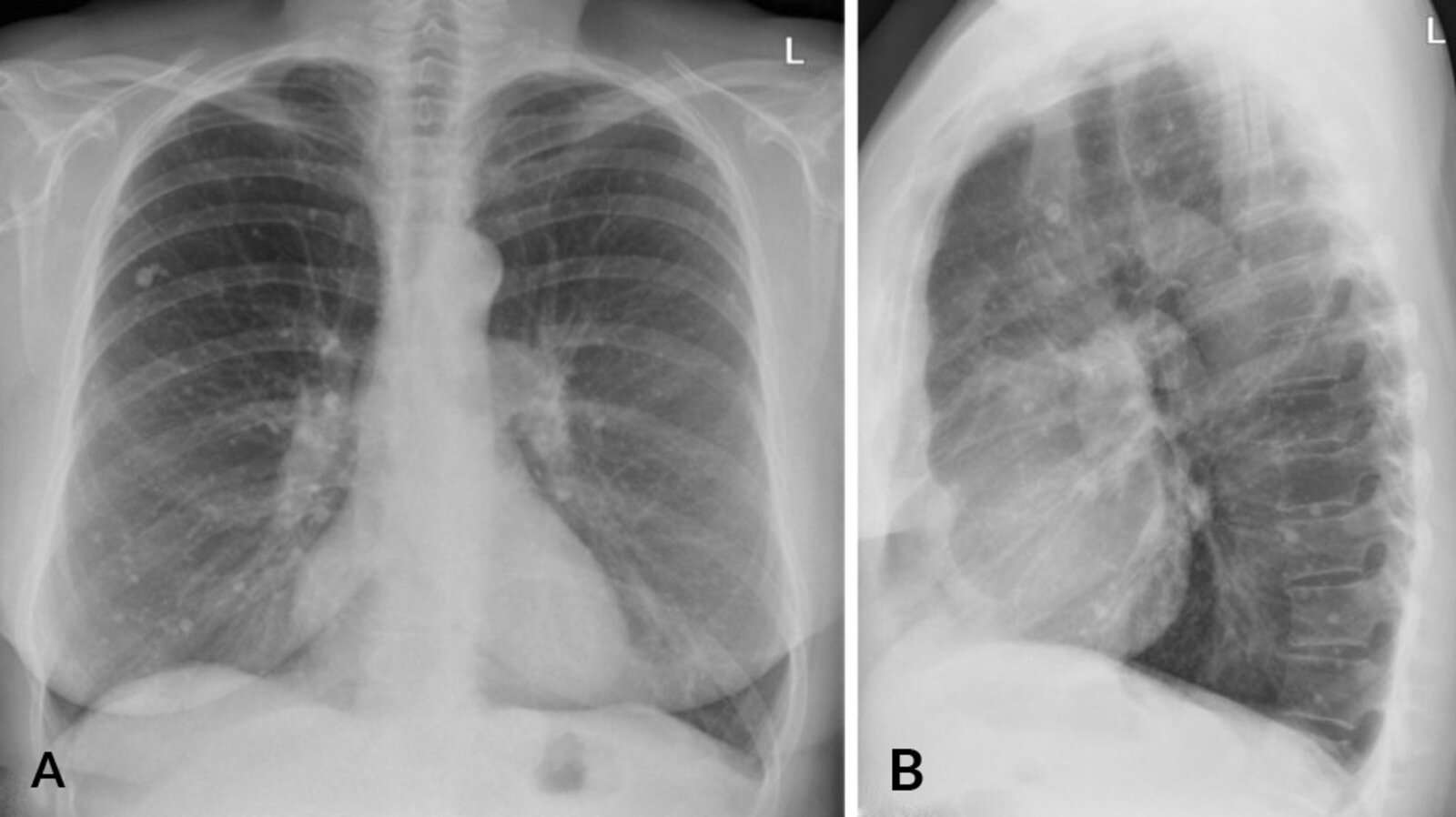
X-ray chest (A: PA view; B: lateral view) of a patient with a remote history of varicella
Numerous small calcified nodules in both lungs (examples indicated by arrowheads) are the sequela of healed varicella pneumonia.
The differential diagnosis of widely distributed small calcified pulmonary nodules includes various types of infection, pneumoconioses, metastases, and deposition diseases.
Source: “Fig 7A & B, In: Pulmonale Rundherde und Pneumonie Ein diagnostischer Leitfaden” by Frauenfelder T, Landsmann A, Springer Medizin, licensed under CC BY 4.0. Modifications: image cropped & replacement of lower case letters with upper case letters. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
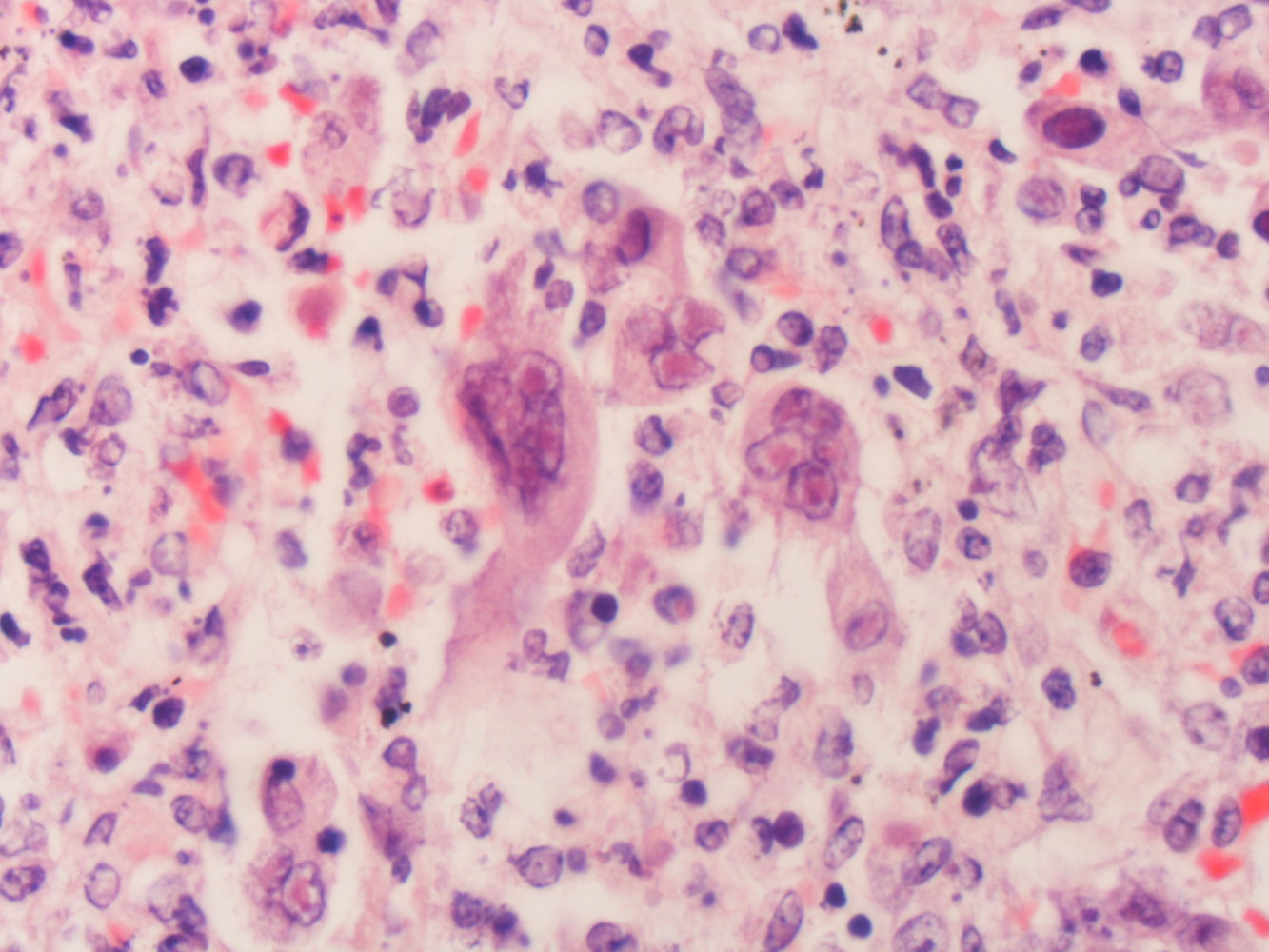
Microscopic image of lung tissue (H&E stain)
Several multinucleated giant cells (syncytial macrophages) can be seen in the center of the image (examples indicated by green overlay), surrounded by inflammatory infiltrate. The giant cells feature characteristic eosinophilic nuclear inclusions (Cowdry type A, blue overlay).
Giant cells with Cowdry type A inclusions are a characteristic histopathological finding in infections with varicella zoster virus, herpes simplex virus, and cytomegalovirus.
Source: “Herpes simplex infection Case 160” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
Differential diagnoses
Chickenpox may be confused with other conditions that involve widespread vesicles and/or crusting lesions, e.g.: [3][7]
- Disseminated herpes zoster (i.e., shingles)
- Herpes simplex virus: disseminated HSV, eczema herpeticum
- Enterovirus infection: atypical hand foot and mouth disease [24][25]
- Widespread bullous impetigo
- Monkeypox [7]
- Adverse reaction to smallpox vaccination: eczema vaccinatum, disseminated vaccinia [7][26][27]
- See also “Infectious rashes in childhood.”


The differential diagnoses listed here are not exhaustive.
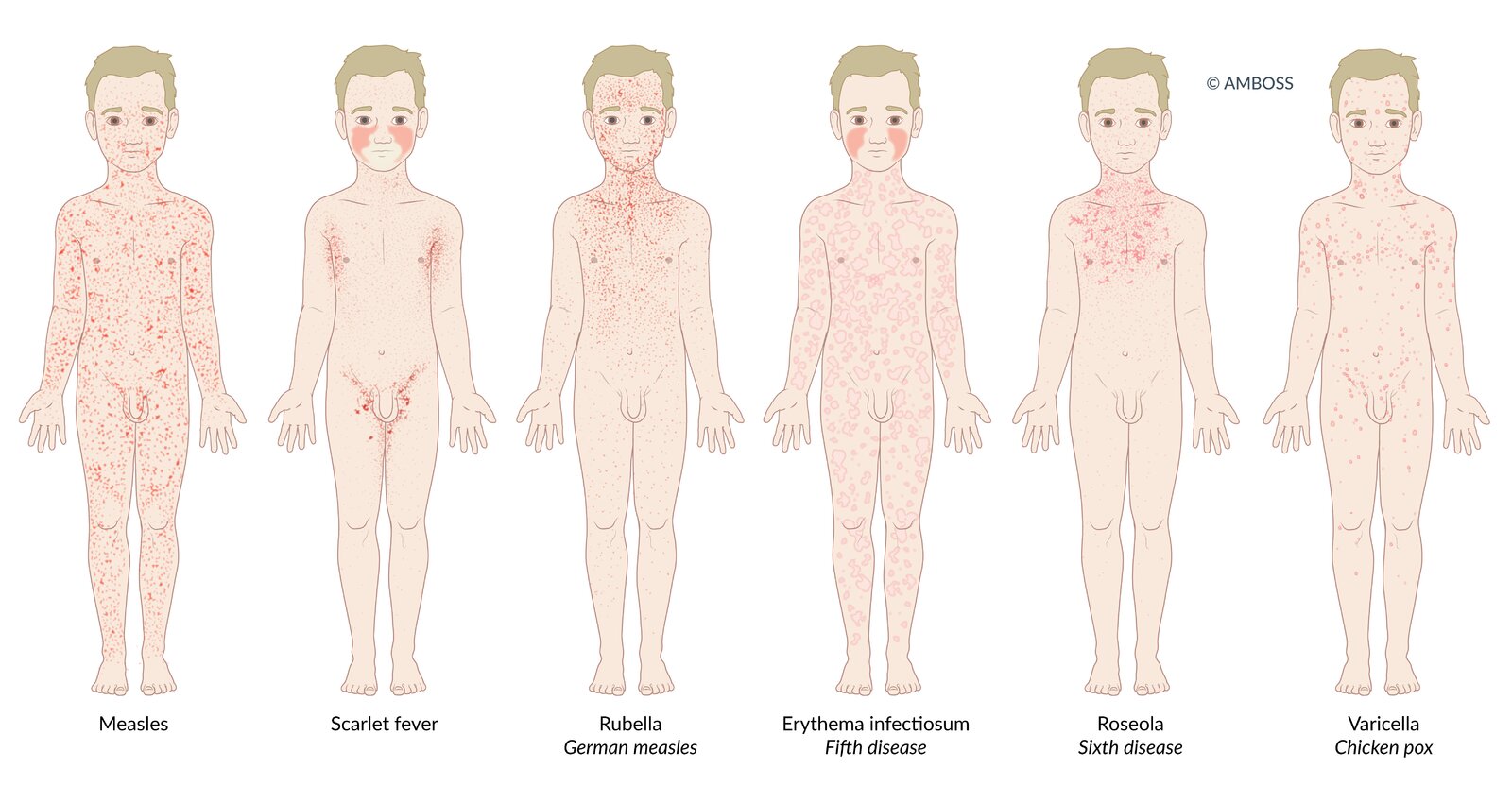
Many infectious diseases in children present with a rash (exanthem). The distribution and morphological characteristics of the exanthem allow the diseases to be differentiated from one another.
Measles: Patients present with a dark red, erythematous, maculopapular, partially confluent exanthem, which spreads from behind the ears to the rest of the body.
Scarlet fever: Patients present with a fine, light red rash with sandpaper-like texture. The exanthem begins on the neck or trunk and disseminates to the whole body. Cheeks may be flushed with perioral pallor. In flexural areas (e.g., axilla and groin), the rash may be more pronounced and linear petechiae (Pastia lines) may be present.
Rubella (German measles): Patients typically present with a nonconfluent, pink, maculopapular exanthem, which begins on the face and spreads to the trunk and extremities.
Erythema infectiosum (fifth disease): A confluent, maculopapular rash appears only in ¼ of patients. It may take on a lace-like, reticular appearance over time. Additionally, patients present with diffuse redness of the face with perioral sparing (slapped-cheek rash).
Roseola infantum (sixth disease): 3-7 days of high fever are followed by a sudden decrease in temperature and development of a patchy, blanching rose-pink maculopapular rash. The rash originates on the trunk, and may spread to the face and extremities.
Varicella (chickenpox): The exanthem affects the whole body, typically spreading to the scalp as well. Various stages of the rash occur simultaneously, which leads to the characteristic clinical finding known as “starry sky.”
© AMBOSS

© AMBOSS
Treatment
Approach [2]
- Start supportive treatment for all patients.
- Assess for indications for antiviral therapy for varicella; if present, determine duration of symptoms.
- Symptom duration ≤ 72 hours: Initiate immediate antiviral therapy. [3]
- Symptom duration > 72 hours: Consult with infectious diseases; antiviral therapy may be appropriate in immunocompromised patients because of prolonged viral replication. [3]
- Provide treatment for complications and superinfections (e.g., treatment of pneumonia, treatment of skin and soft tissue infections).
- Start measures to prevent transmission of VZV.
Most otherwise healthy children < 13 years of age with chickenpox can be treated with symptomatic treatment alone, but advise caregivers to return in the event of prolonged or worsening symptoms and/or signs of secondary bacterial skin infection. [2]
Supportive treatment [2]
- Treat fever and pain with acetaminophen (see “Nonopioid oral analgesia in children”). [2]
-
Pruritus ; [28]
- General advice for caregivers
- Apply cool compresses.
- Take lukewarm oatmeal baths.
- Trim fingernails or wear mitts to prevent scratching.
-
Medications
- Topical: calamine lotion, pramoxine gel [28]
- Oral antihistamines
- General advice for caregivers
Avoid use of aspirin and other salicylates (e.g., bismuth-subsalicylate) in children with chickenpox because of the risk of Reye syndrome. [3]
Avoid topical antihistamines and topical corticosteroids in patients with chickenpox because of the risk of systemic absorption when applied to large areas of skin. [29]
Antiviral therapy for VZV infection (high-risk patients only)
-
Indications for antiviral therapy
- Severe VZV infection
- Risk factors for severe VZV infection
-
Recommended treatment: Begin antiviral therapy as soon as possible (ideally within 24 hours of rash onset). ; [3]
- Immunocompromised individuals, neonates, and/or those with severe infection: IV acyclovir [2][3]
- Immunocompetent individuals, individuals with nonsevere infection: oral acyclovir or valacyclovir [3][8][30]
Patients with nonsevere infections and no risk factors for severe VZV infection do not require antiviral therapy and can be managed with supportive treatment only. [2]
Neonates, immunocompromised patients, and patients with severe infection should not receive oral acyclovir because of poor oral bioavailability. [3]
Complications
Adults have higher rates of complications from varicella compared to children. [2]
Skin [3]
- Bacterial superinfection; (including impetigo, phlegmon, necrotizing fasciitis), which often leads to scarring and is managed with systemic antibiotics
- Reactivation of latent VZV results in shingles (herpes zoster).
- Scarring
Central nervous system [3][31]
- Acute cerebellar ataxia: good prognosis, mainly self-limiting after several weeks
- Encephalitis (very rare): cramps, coma, poor prognosis
Lungs [3]
- Pneumonia (viral or bacterial)
Fetus (chickenpox during pregnancy) [3]
- Congenital varicella syndrome
We list the most important complications. The selection is not exhaustive.
Prognosis
- In healthy children, chickenpox infection generally has a benign course and heals without any consequences.
- Residual scarring may occur because of excessive scratching or bacterial superinfection.
- Immunosuppressed individuals are at a greater risk of the disease taking a generalized or even fatal course.
References:[2]
Prevention
Approach
- Provide primary prevention against varicella infection.
- Ensure children receive varicella vaccination as part of the routine immunization schedule.
- Offer catch-up vaccinations to individuals without evidence of VZV immunity.
- For infected patients: Initiate measures to limit transmission.
- Tell patients to avoid school/work until all lesions have scabbed over and no new lesions appear. [3]
- If hospitalized, start infection control measures to prevent nosocomial spread of varicella.
- If required by law, notify the health department for possible contact tracing.
- For close contacts:
- Assess for evidence of VZV immunity.
- Offer postexposure prophylaxis for chickenpox to individuals with no evidence of immunity.
Most US states mandate reporting cases of chickenpox to local and/or state health departments. [32]
Evidence of VZV immunity [3][8][9]
Any of the following constitutes evidence of immunity to chickenpox: [9][33]
- Documentation of age-appropriate varicella immunization
- Laboratory findings that confirm prior wild-type disease or serologic evidence of immunity (see “Diagnostics of chickenpox”)
- Attestation of past varicella or herpes zoster infection by a healthcare provider
Varicella vaccine [34][35][36]
-
General principles
- Consists of 2 doses of a live attenuated vaccine
- Available vaccines include: [3][5][37]
- A single-antigen varicella vaccine
- A combined measles, mumps, rubella, varicella (MMRV) vaccine [38]
- Recommended for all individuals without evidence of VZV immunity who have no contraindications to live vaccines
- Schedule: See “ACIP immunization schedule” for details on routine and catch-up schedules.
-
Adverse effects [3]
- Minor injection-site reaction and fever
- If MMRV is given at 12– 23 months of age: increased risk of febrile seizures
- Vaccine-associated chickenpox rash
- Future development of shingles [3]
Recommend the varicella vaccine to all nonimmune children and adults who do not have contraindications to live vaccination. [37][39]
Postexposure prophylaxis for chickenpox [4][9]
General principles
- Postexposure prophylaxis is recommended for nonimmune individuals exposed to chickenpox or shingles to prevent disease onset or mitigate disease course. [3][40]
- Eligibility is determined by assessing for evidence of VZV immunity and verifying exposure.
- High-risk interactions include:
- Indoor face-to-face contact with an infected individual for ≥ 5 minutes [3][9]
- Sharing a hospital room or living arrangements with an infected individual
- Active or passive immunization is given depending on risk factors.
- For patients who are ineligible for active immunization and cannot receive passive immunization: Consult infectious disease about possible chemoprophylaxis. [3]
- Passive immunization may prolong the incubation period of VZV; monitor patients for 28 days following exposure. [3][41]
- If symptoms develop following exposure, initiate treatment for varicella infection regardless of whether the patient received postexposure prophylaxis.
Determining postexposure prophylaxis
| Recommended management [3][9][41] | ||
|---|---|---|
| Evidence of VZV immunity | No evidence of VZV immunity | |
| Immunocompetent |
|
|
| Immunocompromised |
|
|
Active immunization
- Indications: immunocompetent patients ≥ 12 months of age with no evidence of VZV immunity [3]
-
Recommended prophylaxis
- Chickenpox immunization
- Give within 5 days following exposure (ideally within 3 days). [9]
- Follow-up vaccination: Complete the age-appropriate vaccination series per the immunization schedule.
Prophylaxis is not recommended for healthy individuals who are either too young for vaccination or who were exposed to VZV > 5 days prior to evaluation. [3]
Passive immunization
-
Indications
-
Individuals with no evidence of VZV immunity who are:
- Immunocompromised
- Pregnant
- Patients who have undergone bone marrow transplantation [9]
- Neonates, if the mother was symptomatic 5 days before or up to 2 days after birth [3][9]
-
Hospitalized premature babies if:
- Born < 28 weeks or with a birth weight ≤ 1 kg [41]
- Born ≥ 28 weeks to a mother without evidence of VZV immunity [41]
-
Individuals with no evidence of VZV immunity who are:
-
Recommended prophylaxis: Give as soon as possible within 10 days following exposure (ideally within 4 days). [41]
- Preferred: varicella-zoster immune globulin (VZIG) [3][41]
- If VZIG is unavailable within 10 days postexposure: intravenous immunoglobulin (IVIG) [3]
-
Follow-up vaccination
- Recommended for all patients without contraindications to live vaccination.
- Give 5–8 months after immunoglobulin therapy. [42]
Controlling varicella transmission in healthcare settings [43]
- Place patients with chickenpox on contact and airborne precautions (see “Infection prevention and control”). [3]
- All health care workers should have evidence of immunity to chickenpox.
- If a health care worker with no evidence of immunity is exposed, notify their supervisor and the occupational health department. [3]
Special patient groups
Varicella in pregnancy [6][9]
Overview
- Infection during pregnancy and the peripartum period is associated with significant complications.
- Pregnant woman: increased risk of varicella pneumonia [6]
- Fetus: congenital varicella syndrome [3][6]
- Neonate: neonatal varicella [3][6]
Diagnostics
- No modifications are required in pregnant patients.
- See “Diagnostics of chickenpox.”
Treatment
-
VZV diagnosed in pregnancy [18]
- Evaluate for evidence of fetal VZV infection with:
- Fetal imaging (i.e., ultrasound, MRI) [6][18]
- Amniocentesis for VZV PCR [18]
- Initiate antiviral therapy (see “Treatment of chickenpox”). [3][6][18]
- Evaluate for evidence of fetal VZV infection with:
-
VZV diagnosed in the peripartum period:
- Administer postexposure VZV prophylaxis to the neonate. [3]
- Separate the mother and child until the mother is no longer infectious. [3]
Prevention of varicella in pregnancy [6][9]
- Prior to pregnancy: Offer vaccination to patients with no evidence of VZV immunity who are willing to delay conception for 3 months. [6][9]
- During pregnancy:
- Screening for varicella immunity is a routine part of prenatal care.
- Offer nonimmune patients vaccination after pregnancy and postexposure VZV prophylaxis if an exposure occurs during pregnancy.
- See also “Prevention of chickenpox.”
Pregnant women should not receive the varicella vaccine. Nonimmune women should be vaccinated after delivery. [9]
Varicella in adults [1]
Overview
- Adults are more likely than children to have a prodrome of fever and malaise prior to rash. [7]
- Adult patients are more likely to experience complications of varicella. [2]
Management
- No modifications to diagnostics of chickenpox are required.
- For treatment of chickenpox in nonimmune adults, antiviral therapy is recommended.
Varicella in patients with HIV [23]
Overview
- Most adults with HIV have acquired varicella immunity prior to HIV infection.
- If infected, adults and adolescents with HIV are more likely to develop disseminated infection.
- See also “Cutaneous complications in HIV infection.”
Diagnostics
- No modifications are required in patients with HIV.
- See “Diagnostics of chickenpox.”
Treatment
- Antiviral treatment is recommended. [23]
- Discuss route of antiviral treatment with infectious diseases. [23]
- Uncomplicated infection is usually treated with oral antivirals
- Severe or complicated infection is usually treated with IV antivirals
- See also “Treatment of chickenpox.”
Prevention
- Discuss vaccination with infectious diseases; typically recommended for individuals with a well-preserved immune system. [23]
- Patients with no evidence of VZV immunity require passive immunization for postexposure prophylaxis. [23]
External Resources
References
- "Varicella". https://www.cdc.gov/vaccines/pubs/pinkbook/varicella.html
- Gershon AA, Breuer J, Cohen JI, et al. "Varicella zoster virus infection". Nat Rev Dis Primers. 1(1). (2015)
- AAP Committee on Infectious Diseases. "Red Book: 2021–2024 Report of the Committee on Infectious Diseases". American Academy of Pediatrics. (2021). ISBN: 9781610025218
- Lachiewicz AM, Srinivas ML. "Varicella-zoster virus post-exposure management and prophylaxis: A review". Prev Med Rep. 16. :101016. (2019)
- Blair RJ. "Varicella Zoster Virus". Pediatr Rev. 40(7). :375-377. (2019)
- Committee on Practice Bulletins. "Practice Bulletin No. 151: Cytomegalovirus, Parvovirus B19, Varicella Zoster, and Toxoplasmosis in Pregnancy". Obstetrics & Gynecology. 125(6). :1510-1525. (2015)
- Wolff K, Johnson RA, Suurmond D. "Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology". McGraw-Hill Medical. (2005). ISBN: 9780071440196
- Blaney SM, Giardino AP, Orange JS, et al. "Rudolph's Pediatrics, 23rd Edition". McGraw-Hill Education / Medical. (2018). ISBN: 9781259588594
- Marin M, Güris D, Chaves SS, et al. "Prevention of varicella: recommendations of the Advisory Committee on Immunization Practices (ACIP)". MMWR Recomm Rep. 56(RR-4). :1-40. (2007)
- Leung J, Broder KR, Marin M. "Severe varicella in persons vaccinated with varicella vaccine (breakthrough varicella): a systematic literature review". Expert Rev Vaccines. 16(4). :391-400. (2017)
- Quinlivan ML, Gershon AA, Steinberg SP, Breuer J. "Rashes Occurring after Immunization with a Mixture of Viruses in the Oka Vaccine Are Derived from Single Clones of Virus". J Infect Dis. 190(4). :793-796. (2004)
- Galea SA, Sweet A, Beninger P, et al. "The Safety Profile of Varicella Vaccine: A 10‐Year Review". J Infect Dis. 197(s2). :S165-S169. (2008)
- "Varicella Vaccine Safety and Monitoring Information for Healthcare Providers". https://web.archive.org/web/20220805193255/https://www.cdc.gov/vaccines/vpd-vac/varicella/hcp-vacc-safety-monitor.htm. [2012-04-05]
- Bernstein P, Furuya Y, Steinberg S, et al. "Vaccine-related varicella-zoster rash in a hospitalized immunocompetent patient". Am J Infect Control. 39(3). :247-9. (2011)
- "Chickenpox (Varicella) interpreting laboratory tests". https://web.archive.org/web/20220805194058/https://www.cdc.gov/chickenpox/lab-testing/lab-tests.html. [2021-04-28]
- "Collecting Specimens for Varicella Zoster Virus (VZV) Testing". https://web.archive.org/web/20220805195244/https://www.cdc.gov/chickenpox/lab-testing/collecting-specimens.html. [2021-04-28]
- Sauerbrei A. "Diagnosis, antiviral therapy, and prophylaxis of varicella-zoster virus infections". European Journal of Clinical Microbiology & Infectious Diseases. 35(5). :723-734. (2016)
- Mandelbrot L. "Fetal varicella - diagnosis, management, and outcome". Prenat Diagn. 32(6). :511-518. (2012)
- Kelly B, Shimoni T. "Reintroducing the Tzanck Smear". Am J Clin Dermatol. 10(3). :141-152. (2009)
- Mylarapu A, Yarabarla V, Padilla RM, Fasen M, Reddy P. "Healed Varicella Pneumonia: A Case of Diffuse Pulmonary Microcalcifications". Cureus. 13(6). :e15890. (2021)
- Alvarez JC, Alvarez J, Tinoco J, et al. "Varicella-Zoster Virus Meningitis and Encephalitis: An Understated Cause of Central Nervous System Infections". Cureus. 12(11). :e11583. (2020)
- Haaga JR, Boll D. "Computed Tomography & Magnetic Resonance Imaging Of The Whole Body E-Book". Elsevier Health Sciences. (2016). ISBN: 9780323278164
- "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: 2021 update". https://web.archive.org//web/20220807093439/https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf. [2021-06-22]
- Buttery VW, Kenyon C, Grunewald S, et al. "Atypical Presentations of Hand, Foot, and Mouth Disease Caused by Coxsackievirus A6 — Minnesota, 2014". MMWR Morb Mortal Wkly Rep. 64(30). :805. (2015)
- Centers for Disease Control and Prevention (CDC). "Notes from the field: severe hand, foot, and mouth disease associated with coxsackievirus A6 - Alabama, Connecticut, California, and Nevada, November 2011-February 2012". MMWR Morb Mortal Wkly Rep. 61(12). :213-4. (2012)
- Reed JL, Scott DE, Bray M. "Eczema Vaccinatum". Clin Infect Dis. 54(6). :832-840. (2012)
- "Monkeypox and Smallpox Vaccine Guidance". https://web.archive.org/web/20220901192437/https://www.cdc.gov/poxvirus/monkeypox/clinicians/smallpox-vaccine.html. [2019-12-02]
- Usatine R. "Color Atlas of Family Medicine 2/E". McGraw Hill Professional. (2013). ISBN: 9780071769648
- Mohundro BL, Horace A. "Itching like crazy: understanding chickenpox". US Pharm. 37(3). :58-60. (2012)
- Gilbert, DN; Chambers, HF. "Sanford Guide to Antimicrobial Therapy 2020". Antimicrobial Therapy, Inc. (2020). ISBN: 9781944272135
- Barkovich AJ. "Pediatric Neuroimaging". Lippincott Williams & Wilkins. (2005). ISBN: 9780781757669
- "Varicella Reporting and Surveillance". https://web.archive.org/web/20220808172258/https://www.cdc.gov/chickenpox/health-departments/conducting-surveillance.html. [2021-04-28]
- "Immunity Against (Protection From) Chickenpox". https://web.archive.org/web/20220809011254/https://www.cdc.gov/vaccines/vpd-vac/varicella/basic-immunity.htm. [2012-04-05]
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324163634/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2023-02-10]
- "Catch-up Immunization Schedule for Children and Adolescents Who Start Late or Who Are More than 1 Month Behind Recommendations for Ages 18 Years or Younger, United States, 2023". https://web.archive.org/web/20230324164753/https://www.cdc.gov/vaccines/schedules/hcp/imz/catchup.html. [2023-02-10]
- "Adult Immunization Schedule by Age Recommendations for Ages 19 Years or Older, United States, 2023". https://web.archive.org/web/20230324184103/https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html. [2023-02-10]
- "Child and Adolescent Immunization Schedule. Recommendations for Ages 18 Years or Younger, United States, 2022". https://web.archive.org/web/20220809054312/https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html. [2022-02-17]
- Klein NP, Fireman B, Yih WK, et al. "Measles-Mumps-Rubella-Varicella Combination Vaccine and the Risk of Febrile Seizures". Pediatrics. 126(1). :e1-e8. (2010)
- Murthy N, Wodi AP, Bernstein H, Ault KA. "Recommended Adult Immunization Schedule, United States, 2022". Ann Intern Med. (2022)
- Sampathkumar P, Drage LA, Martin DP. "Herpes Zoster (Shingles) and Postherpetic Neuralgia". Mayo Clinic Proceedings. 84(3). :274-280. (2009)
- Centers for Disease Control and Prevention (CDC). "Updated recommendations for use of VariZIG--United States, 2013". MMWR Morb Mortal Wkly Rep. 62(28). :574-6. (2013)
- "Timing and Spacing of Immunobiologics, General Best Practice Guidelines for Immunization: Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP)". https://web.archive.org/web/20220809053645/https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/timing.html#t-05. [2022-07-12]
- Advisory Committee on Immunization Practices., Centers for Disease Control and Prevention (CDC). "Immunization of health-care personnel: recommendations of the Advisory Committee on Immunization Practices (ACIP)". MMWR Recomm Rep. 60(RR-7). :1-45. (2011)