Summary
Early childhood, which typically spans from birth to 8 years of age, is characterized by rapid growth and development. Close monitoring during this period ensures children are meeting age-specific milestones and that deviations from expected developmental trajectories are quickly identified. Developmental delays affect ∼ 15% of children and can impact more than one domain (i.e., physical, language, cognitive, and social and emotional development); early identification and treatment can improve outcomes. Developmental milestones are an important component used to track a child's progress over time and provide a framework by establishing a set of skills or behaviors that most children are expected to achieve by a certain age. A child's development should be assessed at every well-child visit and whenever there is a concern for abnormal development. For children who are not meeting their milestones, an evaluation of abnormal pediatric development and relevant referrals are indicated.
See “Well-child visits” for more information on routine health assessments. For information on growth below the expected parameters for age, see “Growth faltering.”
Overview of normal development
Normal development in childhood involves the evolution and resolution of primitive reflexes, and the sequential development of motor, language, cognitive and social skills (tracked using developmental milestones). Throughout childhood, various behaviors (e.g., stranger anxiety, magical thinking, imaginary companions) may also be temporarily observed and are part of normal development; caregivers should be reassured that these behaviors will resolve as children age.
Primitive reflexes
General principles [1]
- Primitive reflexes are transient reflexes that manifest during infancy and disappear when subcortical motor inhibitory pathways develop (usually within the 1st year of life).
- Evaluation of primitive reflexes is an essential part of the newborn examination.
-
Abnormal primitive reflexes are those that are absent, asymmetric, and/or persist past the expected age range.
- Bilateral absence or prolonged reflexes: most commonly CNS dysfunction
-
Unilaterally absent or asymmetric reflexes are usually caused by one of the following: [2]
- Peripheral nerve dysfunction (e.g., brachial plexus injuries)
- Musculoskeletal involvement (e.g., neonatal clavicle fracture)
- Unilateral CNS injury (e.g., perinatal brain injury)
Multiple primitive reflexes in adults (i.e., frontal release signs) indicate frontal lobe dysfunction. [3][4]
Overview of primitive reflexes
| Overview of primitive reflexes [5][6] | |||
|---|---|---|---|
| Reflex | Description | Typical age range [5] | Clinical significance |
| Glabellar tap sign [4] |
|
|
|
| Snout reflex [4] |
|
|
|
| Rooting reflex |
|
|
|
| Sucking reflex |
|
|
|
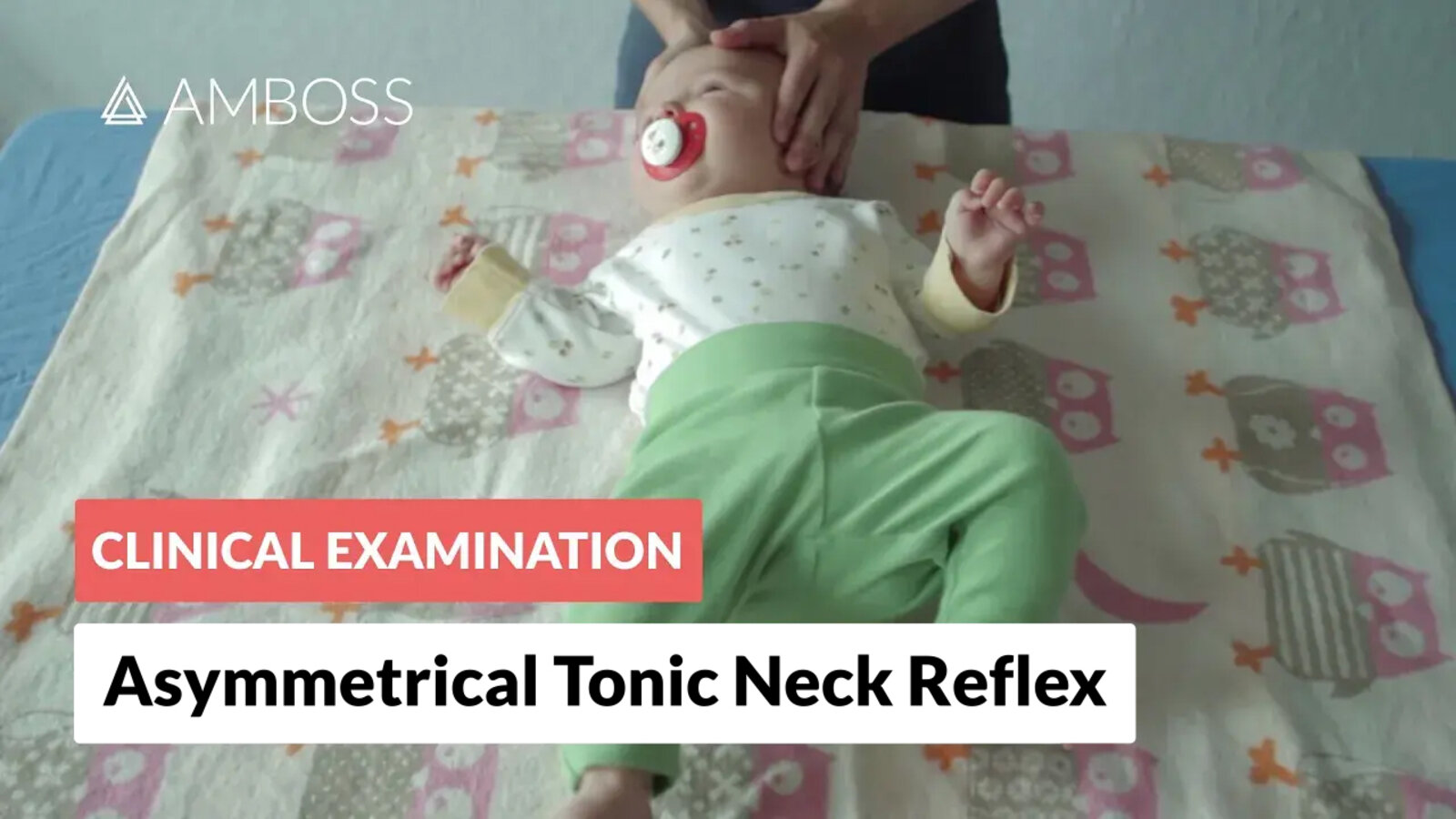
| Asymmetrical tonic neck reflex (ATNR) |
|
|
|
| Moro reflex (Startle reflex) |
|
|
|
| Palmar grasp reflex |
|
|
|
| Plantar grasp reflex |
|
|
|
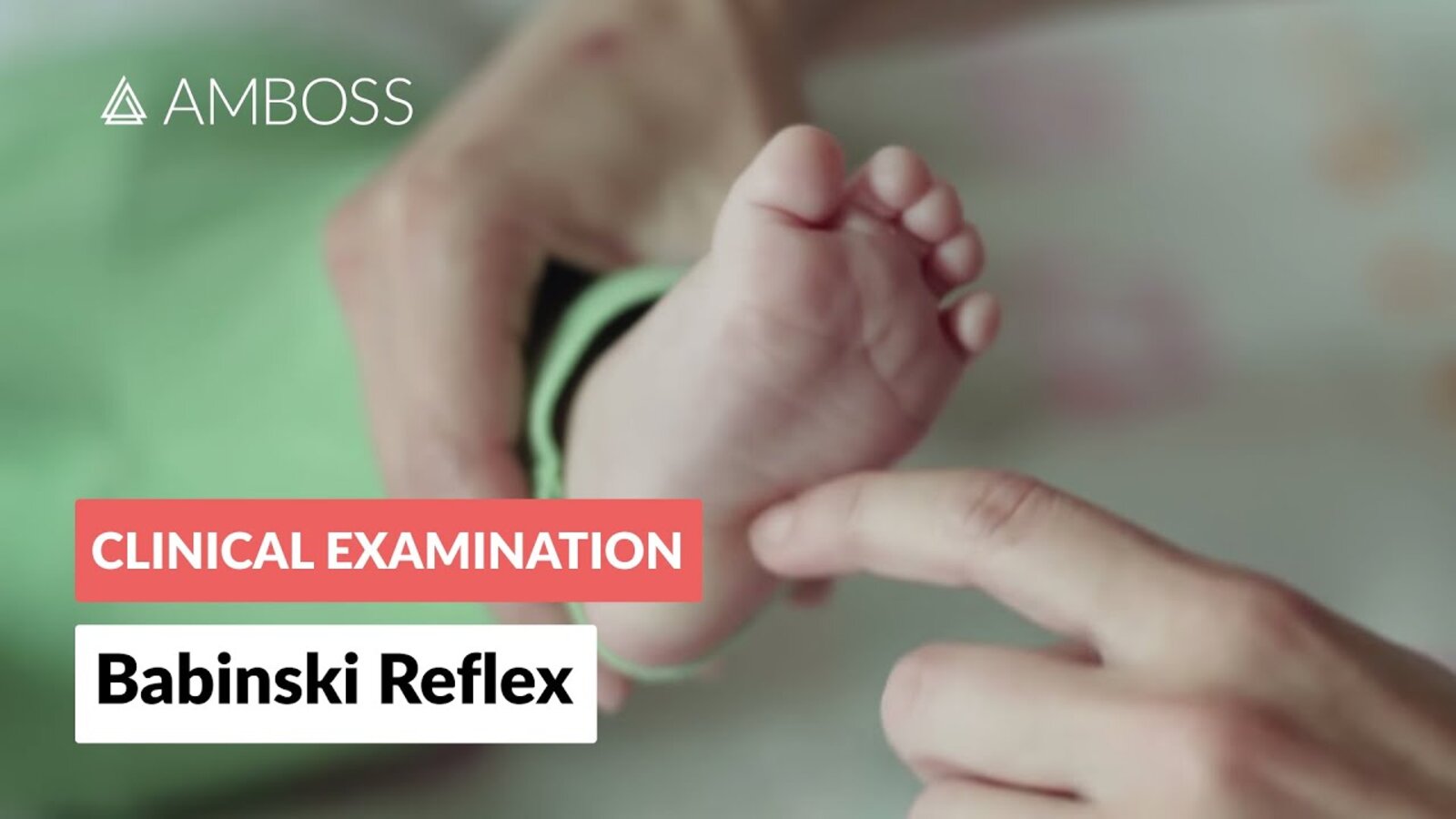
| Extensor plantar reflex (Babinski reflex) |
|
|
|
| Landau reflex |
|
|
|
| Parachute reflex |
|
|
|
| Truncal incurvation reflex (Galant reflex) [14] |
|
|
|
| Stepping reflex [16] |
|
|
|
")






With the infant in the supine position, turning the head to one side elicits extension of the ipsilateral extremities and flexion of the contralateral extremities. This reflex is often referred to as the fencing or bow and arrow posture.
Source: “Asymmetrical tonic neck reflex (ATNR) in a two-week-old female” by Samuel Finlayson, Wikimedia commons, licensed under CC BY-SA 4.0. Modifications: anonymized.
_in_a_two-week-old_female.jpg){kind=link}
© AMBOSS
© AMBOSS

© AMBOSS
© AMBOSS

© AMBOSS
Developmental milestones
General principles [17]
- Developmental milestones are the expected abilities that most children can do by a defined age and are:
- Divided into physical, cognitive, social, and emotional domains
- Continuously progressing as the child ages
- Adjusted to compensate for prematurity in infants < 2 years of age
- Assessed during routine well-child examinations and inpatient pediatric history and physical examinations
-
Abnormal development occurs when children fail to attain developmental milestone(s) by the expected age and/or in the expected order.
- ∼15% of children have developmental delay. [18]
- Common etiologies include:
- Neurodevelopmental disorders [19]
- Neurologic injury
- Child neglect
Developmental domains [5]
-
Motor development
- Gross motor development: the development of movements (e.g., sitting up, walking) that require the use of large muscle groups
- Fine motor development: the development of precise movements using hands and smaller muscles (e.g., picking up a small object)
-
Language development: the development of communication through either spoken or signed language
- Receptive language: the ability to understand and process language
- Expressive language: the ability to formulate language
- Cognitive development: the development of reasoning and problem-solving skills
- Social and emotional development: the development of self-regulation and attachment and interaction with others
Age-specific developmental milestones
- In 2022, the CDC recommended using the 75th percentile rather than the 50th percentile for developmental surveillance; the following tables reflect this change. [20][21]
- If a child is not meeting milestones, conduct an immediate evaluation of abnormal pediatric development. [20][22]
A wait-and-see approach is no longer recommended for potential developmental delay. [20][22]
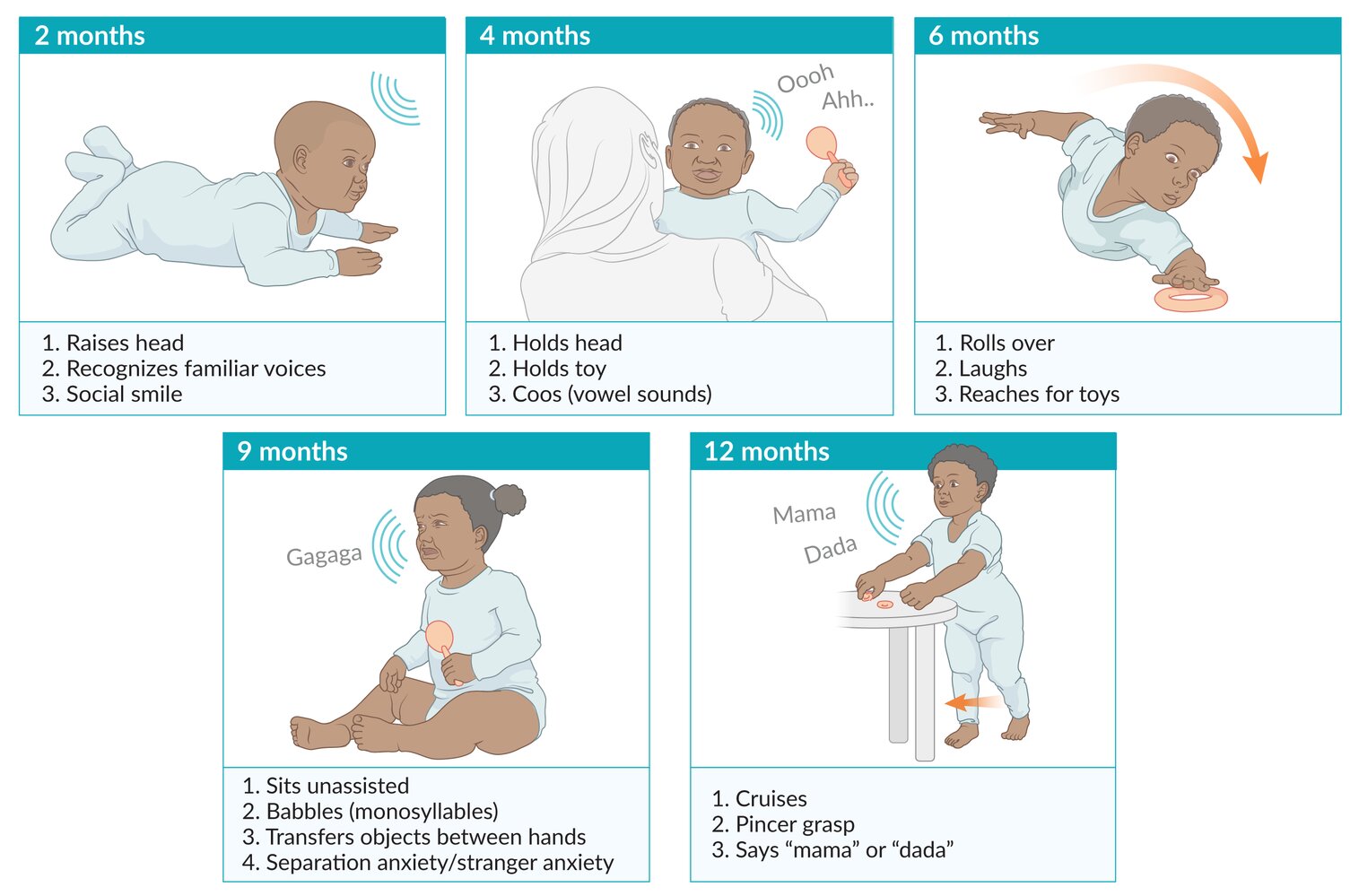
Developmental milestones in infants [20][21]
| Overview of developmental milestones in infants [20][21] | |||
|---|---|---|---|
| Motor development | Speech development | Cognitive and social development | |
| 2 months |
|
|
|
| 4 months |
|
|
|
| 6 months |
|
|
|
| 9 months |
|
|
|
| 12 months |
|
|
|
Children, including twin siblings, develop at different speeds and one child's milestones should not be used to evaluate another child's development.

Developmental milestones in childhood [20][21]
| Overview of developmental milestones in children 1–5 years [20][21] | |||
|---|---|---|---|
| Age | Motor development | Speech development | Cognitive and social development |
| 15 months |
|
|
|
| 18 months |
|
|
|
| 2 years |
|
|
|
| 2.5 years (30 months) |
|
|
|
| 3 years |
|
|
|
| 4 years |
|
|
|
| 5 years |
|
|
|
© AMBOSS
Language and speech development
Influencing factors of language and speech development
- Somatic and cognitive factors: e.g., hearing, musculature, brain development
- Environmental interaction: e.g., conversations, topic variety, being read to, family educational level, multilingualism
- Strong correlation with other developmental areas
- Cognitive skills: e.g., memory, perspective-taking
- Social development: e.g., communication, relationship building, social interaction
- Action control: aids in thought and action planning
- Emotion regulation: e.g., naming, understanding, and regulating emotions
Theories of language acquisition
-
Nativist theory or innateness hypothesis (by Noam Chomsky): posits an innate, biological capacity for language
-
Key concepts
- Language acquisition device (LAD): a theoretical pathway in the brain that allows infants to process and learn language with minimal input
- Universal grammar: an innate set of rules (e.g., syntax, nouns, verbs) hardwired in the brain, common to all human languages
-
Critical period: a sensitive time window (typically before puberty) during which language is most easily acquired
- Language acquisition becomes significantly more difficult after this period
-
Key concepts
-
Behavioral learning theory (by B.F. Skinner): views language as a learned behavior, not an innate capacity
- Acquisition occurs via operant conditioning and imitation
- Process: caregivers provide positive reinforcement (e.g., praise, affection) for vocalizations that approximate words (e.g., "ma-ma"), increasing the likelihood of their repetition
-
Social interactionist theory (by Lev Vygotsky): blends biological and social factors
- Language development is driven by a social desire to communicate and interact with others
- Emphasizes the role of the social and cultural environment in supporting language learning
Neurobiology of language
-
Key brain structures
-
Broca's area
- Location: left frontal lobe
- Function: speech production (motor control of articulation)
-
Wernicke's area
- Location: left temporal lobe
- Function: language comprehension (understanding spoken and written language)
-
Broca's area
-
Connecting pathway
- Arcuate fasciculus: a bundle of nerve fibers that connects Wernicke's area and Broca's area
-
Language-related pathologies
-
Broca's aphasia (expressive aphasia)
- Intact comprehension, but difficulty producing fluent speech
- Speech is often slow, halting, and telegraphic (e.g., "walk dog")
- Patients are typically aware of their deficit
-
Wernicke's aphasia (receptive aphasia)
- Impaired comprehension
- Speech is fluent and grammatical but nonsensical (a "word salad")
- Patients are often unaware of their deficit
-
Conduction aphasia
- Caused by damage to the arcuate fasciculus
- Intact comprehension (Wernicke's) and fluent speech (Broca's)
- Primary deficit: inability to repeat words or phrases
-
Broca's aphasia (expressive aphasia)

Language and cognition
-
Linguistic relativity (Sapir-Whorf hypothesis)
- Posits that the structure of a language influences a speaker's worldview and cognition
- Weak version (relativity): language influences thought and perception
- Strong version (determinism): language strictly limits what we are capable of thinking (less accepted)
-
Contrasting developmental models
-
Piaget: cognition precedes language
- Children must first develop cognitive concepts (schemas) before they can acquire the language to describe them
- Language is seen as a representation of existing thought
-
Vygotsky: language and thought develop interdependently
- Thought and language are separate functions in early infancy but merge later
- Language is not just an expression of thought, but also a critical tool for cognitive development, driven by social interaction
-
Piaget: cognition precedes language
Under the Sapir-Whorf hypothesis (linguistic relativity), speakers of a language lacking a specific term for "depression" may fail to cognitively categorize emotional distress as a distinct mental disorder. This frequently results in somatization, where psychological distress is perceived and reported exclusively as physical symptoms (e.g., fatigue or "heavy limbs") due to a lack of linguistic labels for abstract mood states.
Basic terms of language and speech development
- Receptive language: the ability to understand and process language
- Expressive language: the ability to formulate language
-
Speech development
-
Four levels
- Sound formation
- Speech rate
- Speech fluency
- Intonation and voice use
- Begins with the interplay of oral musculature and perception during sucking, swallowing, and chewing
- From 6 months of age
- Coordination of lips, tongue, jaw, and soft palate
- Coordination of breathing and voice
- Variation of speech rate
- Clinical relevance: speech sound disorder
-
Four levels
-
Language development
-
Four levels
- Sound acquisition
- Vocabulary
- Grammar
- Communicative competence
- Clinical relevance: language disorder
-
Four levels
Timeline of speech development
For the timeline of speech development, see the tables: "Developmental milestones in infants" and "Developmental milestones in children."
Timeline by level
1. Sound formation and acquisition
-
Levels
- Phonetics: subfield of linguistics concerned with the production, transmission, and perception of speech sounds
- Phonology: subfield of linguistics concerned with the function, arrangement, and meaning of speech sounds
-
Approximate timeline
- From birth: crying
- 3–4 months: cooing
- 6–7 months: rhythmic syllable chains (reduplicated babbling), e.g., "da-da-da"
-
10–12 months
- Variegated babbling (different consonants), e.g., "ma-ba"
- First words, e.g., "mama" or "no"
- By 3-4 years: early sounds
- Vowels: all
- Nasals: m, n (e.g., "mom", "no")
- Stops (plosives): p, b, t, d, k, g (e.g., "pop", "ball", "toy", "go")
- Glides: w, j ("we", "yes")
- By 5-6 years: middle sounds
- Sibilants ("hissing sounds"): s, z, sh ("sun", "zoo", "shoe")
- Fricatives: f, v ("fun, "van")
- Affricatives: ch, j ("chair", "jump")
- By 6- 7+ years: late sounds
- Liquids: l, r ("look", "run")
- Complex fricatives: th (as in "thumb"), TH (as in "that")
- Sibilant: zh ("treasure")
It is common for children to misarticulate the "Late 8" sounds (e.g., /r/, /l/, /s/, "th") in English. Saying "wabbit" (for "rabbit") is a normal developmental error, as mastery of these complex sounds is often not complete until ages 6-8.
2. Vocabulary acquisition
-
Vocabulary/lexicon: the total number of words a person knows at a given time
- Active vocabulary: words that an individual uses regularly in speech
- Passive vocabulary: words that an individual understands but does not actively use in speech
-
Approximate timeline
-
9–18 months: first words
- Stagnant vocabulary: few words remaining unchanged for several months
- Overextension: child applies a word too broadly (e.g., using "doggy" to refer to all four-legged animals with fur, not just dogs)
- Underextension: child applies a word too narrowly (e.g., using "doggy" exclusively for the family pet, while not recognizing that other dogs are also dogs)
-
18–24 months: vocabulary spurt
- Passive vocabulary: approx. 50–200 words
- Active vocabulary: approx. 50–200 words
- Children should have at least 50 active words by 24 months.
- 3 years: approx. 5–10 new words daily
- Continued vocabulary acquisition is influenced by environmental factors and the educational level of the family.
-
9–18 months: first words
During the vocabulary spurt at approx. 18–24 months, children learn about 9 new words every day!
3. Grammar acquisition
-
Levels
- Syntax: subfield of grammar concerned with the order of words (e.g., in English, "subject-verb-object")
- Morphology: subfield of grammar concerned with the word structure, including prefixes, suffixes, and tenses (e.g., "walk" vs. "walked," "cat" vs. "cats")
-
Approximate timeline
- 18–24 months: telegraphic speech (simple two- or three-word sentences, lacking grammatical morphemes; e.g., "mommy car," "more drink")
-
2–3 years: sentences get longer; usage of grammatical morphemes like the plural "-s" and the progressive "-ing
- Overgeneralization (or overregularization): child applies grammatical rule in all situations, even when it is incorrect ("I runned" instead of "I went" or "the mouses" instead of "the mice")
- 3–4 years: sentences become complex, incorporating subordinate clauses (e.g., "...because I'm hungry") and correct verb tenses
- 4–5 years: basic grammatical structures are largely mastered
Children move from telegraphic speech (∼ 18-24 months) to using complex sentences with grammatical morphemes and subordinate clauses by age 4-5.
4. Communicative competence
- Definition: verbal and non-verbal adaptation to individual communication situations, also referred to as pragmatics
-
Includes:
- Using non-verbal cues (e.g., tone, gestures, eye contact)
- Taking turns in conversation
- Perspective-taking (understanding the listener's knowledge)
- Understanding non-literal language (e.g., humor, irony, sarcasm)
-
Approximate timeline
- 0–12 months: pre-verbal interaction (e.g., eye contact)
- 12–24 months: single words for social functions (e.g., greeting, requesting)
- 2–3 years: simple back-and-forth conversations
- 3–4 years: developing perspective-taking; can adjust speech for the listener (e.g., simpler for a baby), role-playing
- 4–6 years: construction of logical sequences (telling of coherent stories)
- > 6 years: mastery of non-literal language (humor, sarcasm) and engaging in empathetic, complex conversation
Pragmatics refers to the social aspects of language use. It encompasses the ability to understand what to say, how to say it, and when to say it appropriately within a particular context. This includes recognizing the nuances of tone, body language, and the social norms that govern communication in different situations.
Disorders of language and speech development
- See: "Language disorder" and "Speech sound disorder"
An individual with autism spectrum disorder (ASD) might have an advanced vocabulary and grammar, but they will still struggle with the social use of language, such as understanding sarcasm, taking turns in conversation, or making appropriate eye contact.
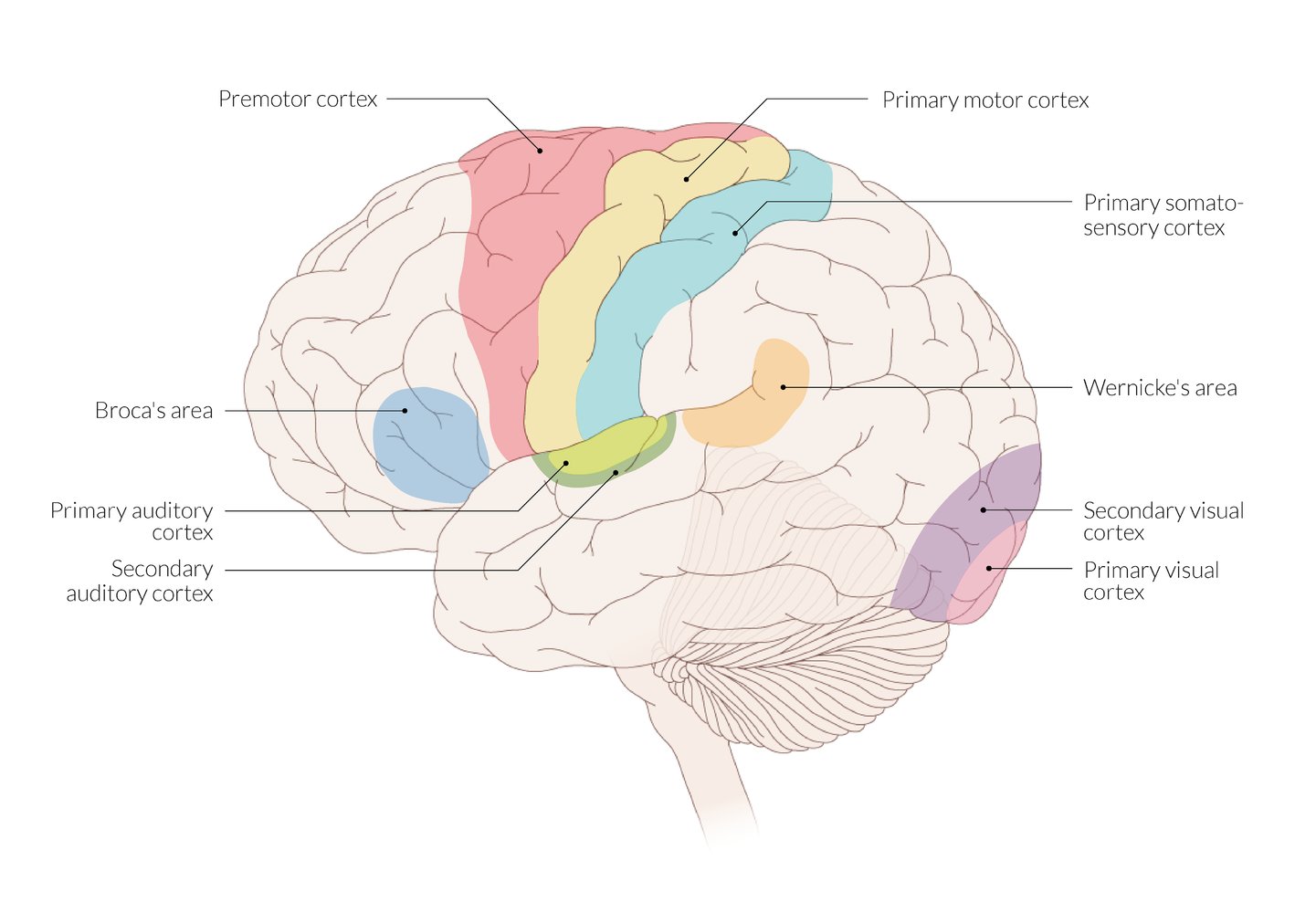
The primary motor cortex, in the frontal lobe, is the origin of the fibers of the pyramidal tract.
The primary and secondary auditory cortices, where auditory input is processed, are located in the temporal lobe. The primary visual cortex is located at the occipital pole and is surrounded by the secondary visual cortex.
Different functions converge at association areas. The most well-known examples are the motor (Broca) and sensory (Wernicke) areas of speech, which are commonly located in the dominant hemisphere.
© AMBOSS
Common developmental behaviors
Certain temporary pediatric behaviors are considered normal parts of cognitive, imaginative, and creative development, e.g.:
-
Stranger anxiety: when an infant is fearful of unknown individuals
- Expected ages: 6 months–3 years [24]
- Clinical features: crying and/or clinging to a known caregiver when around strangers
-
Separation anxiety: when an infant or young child is afraid of being separated from their caregiver
- Expected ages: peaks between 9 and 18 months and resolves by 3 years of age [25]
- Clinical features
- Crying and/or clinging to a caregiver if the caregiver tries to leave
- Continued crying after a caregiver has left
-
Pretend play: when a young child imitates adult activities and/or interactions [26]
- Expected ages: starts around 15–18 months
- Examples
- The use of real or toy items to imitate activities
- Symbolic play: the use of an item to represent other things
- Benefits: enhances creativity and provides practice for social skills, emotional regulation, and language development [5]
-
Temper tantrums
- Common from 2 to 5 years of age
-
Characterized by behaviors such as stomping and screaming
- No physical harm to others
- Usually only occurs in the presence of parents (not, e.g., in daycare)
- Child behaves normally in between tantrums
- Typically ceases by approx. 5 years of age
- Ignoring the child is the most effective approach to handle a temper tantrum (leads to behavioral extinction by eliminating positive reinforcement).
-
Magical thinking: when thoughts are believed to affect change and nonrelated events are causally linked [5][6]
-
Expected ages: ∼4–5 years
- Decreases with age
- Some persistence into adulthood may occur. [5][27]
- Examples
- Assuming their actions cause unrelated events
- Attributing emotions to an inanimate object
- Believing that wishing for something causes it to come true
-
Expected ages: ∼4–5 years
-
Imaginary companion: when a fictitious human, animal, or object is treated as if it were alive [28]
- Expected ages: Preschool and young school-aged children [28]
- Benefits are similar to those of pretend play. [28]
Common reactions to specific life events
Arrival of a sibling [29][30]
-
The arrival of a sibling can pose significant stress to a child, who may react with negative emotions (e.g., jealousy, anxiety, resentment, anger) and changes in behavior. Further typical reactions include:
-
Regression (psychiatry)
- Bedwetting in a toilet-trained child
- Finger or thumb sucking
- Demanding help with eating
- Wanting to drink from baby's bottle and/or wanting to breastfeed
- Speaking like a baby
- Changes in sleeping pattern
- Violent behavior towards the sibling and/or caregivers (e.g., hitting, biting)
-
Regression (psychiatry)
-
Counsel caregivers about the older child's possible reactions and advise them to:
- Avoid other major changes at the same time as the anticipated arrival (e.g., moving houses, starting new kindergarten).
- Organize caregiving support from other family and friends.
- Spend alone time with the older child after the baby's arrival.
- Encourage the older child to take part in the caretaking of their sibling and praise them for doing so.
- Acknowledge the older child's negative emotions and reinforce their importance and sense of security.
Understanding of death [31]
- A child's understanding of death depends strongly on their developmental age, personal experiences, and parental communication about death (including parents' spiritual and religious beliefs).
- An adult understanding of death involves the comprehension of the following concepts:
- Irreversibility: Death is permanent.
- Universality: All living things will die eventually, including oneself.
- Nonfunctionality: Upon death, all bodily processes end.
- Causation: Death is caused by a breakdown of bodily functions.
Concepts of death at different ages
- Infants and toddlers (0–2 years): no understanding of death
-
Preschoolers (3–5 years):
- Typically perceive death as something temporary and reversible
- May believe that they can influence death (“magical thinking”)
-
School-age children (6–12 years):
- Typically know that death is irreversible and universal, may understand the concept of nonfunctionality
- Often personify death (e.g., as a ghost)
- Have a strong interest in death, and may feel anxious and fearful about their own death or the death of caregivers
- Adolescents (13–18 years): typically have an adult understanding of death
Overview of abnormal development
General principles
- Early identification and treatment of developmental delay improve outcomes.
- In children < 2 years old who were born prematurely, the chronological age must be adjusted for gestational age. [6]
-
Developmental surveillance should be performed at every well-child visit and includes: [32]
- Inquiring if caregivers have any concerns
- Reviewing and updating developmental history
- Observing the child
- Identifying risk factors for developmental delay
-
Developmental screening uses validated tools and should be used at set well-child visits or if there are concerns. [18][32]
- Parent-completed tools can be used for initial screening.
- If abnormal, directly administered tools are used for further evaluation.
Types of abnormal development [6][17][33]
-
Developmental delay: Milestones occur in the expected order but not by the expected ages.
- 1 domain affected: isolated developmental delay
- ≥ 2 domains affected: global developmental delay [6]
-
Developmental dissociation
- Significant developmental delay in one domain when compared to the other domains
- Can occur in children with isolated developmental delay and in those with a global developmental delay
- Developmental deviation: Developmental milestones within a given domain are not achieved in the expected order.
- Developmental regression: the loss of previously acquired skills
Evaluation of abnormal pediatric development [6][18]
- Confirm developmental abnormalities are present using validated developmental screening (if not already performed).
- Obtain a full medical history (e.g., in utero, birth, past medical history, and family history).
- Evaluate for abnormal physical findings. [34]
- Perform a detailed neurological examination.
- Rule out hearing loss and vision loss.
- Screen and test for common underlying etiologies.
- For children with suspected global developmental delay, see also “Diagnostics of global developmental delay.”
Abnormal pediatric development can result from neglect and other forms of abuse; consider assessing for red flags for child maltreatment.
Management of abnormal pediatric development [18]
- Identify and treat underlying medical comorbidities (e.g., hearing loss).
- Refer to a specialist based on clinical features and local availability. [18]
- Speech and language or social delay: developmental pediatrician or psychologist for autism assessment
- Abnormal muscle tone or global developmental delay: neurology
- Dysmorphic features or clusters of physical abnormalities : genetics
- Involve relevant therapy services, as needed.
- Behavioral issues: behavioral therapy
- Emotional and/or cognitive issues: psychology
- Gross motor delay: physical therapy
- Fine motor delay: occupational therapy
- Speech delay: speech therapy
- Ensure regular follow-up.
- See also “Neurodevelopmental disorders.”
Anticipatory guidance for pediatric development
- Proactively discuss with caregivers ways of encouraging normal development, e.g.:
- Initiate supervised tummy time early. [35]
- Increase gradually based on the infant's interest level.
- The target is 30 minutes spread out over the day.
- Talk to and with the child. [36]
- Describe everyday activities to the child.
- Sing nursery rhymes.
- Promote early exposure to books.
- Point to and name everyday objects.
- Actively play with the child, e.g.: [37]
- Interact with reciprocal games like pat-a-cake, peek-a-boo, Simon says.
- Make different faces with the child.
- Demonstrate how to use age-appropriate toys or household items.
- Introduce different objects of different textures, sizes, and colors.
- Engage in role-playing.
- Initiate supervised tummy time early. [35]
- Advise on adequate sleep, nutrition, and physical exercise to support development (see “Anticipatory guidance for children”).
- Ensure caregivers know the expected developmental milestones for their child's age.
- Advise caregivers to consult a healthcare professional early if they have development concerns, rather than waiting to see if the child will catch up. [20]
Reading, talking, singing, and playing with infants promotes normal early pediatric development. [36]
External Resources
References
- Brooker RJ, Buss KA, Lemery-Chalfant K, et al. "The development of stranger fear in infancy and toddlerhood: normative development, individual differences, antecedents, and outcomes". Dev Sci. :n/a-n/a. (2013)
- Moini J, Koenitzer J, LoGalbo A. "Global Emergency of Mental Disorders". Academic Press. (2021). ISBN: 9780323858434
- "The Power of Play - How Fun and Games Help Children Thrive". https://web.archive.org/web/20230209175556/https://www.healthychildren.org/English/family-life/power-of-play/Pages/the-power-of-play-how-fun-and-games-help-children-thrive.aspx. [2022-06-13]
- Scharf RJ, Scharf GJ, Stroustrup A. "Developmental Milestones". Pediatr Rev. 37(1). :25-38. (2016)
- Kliegman RM, Geme JS. "Nelson Textbook of Pediatrics, 2-Volume Set". Elsevier. :3623-3633. (2019). ISBN: 9780323529501
- Brashier NM, Multhaup KS. "Magical thinking decreases across adulthood". Psychol Aging. 32(8). :681-688. (2017)
- Tracy R. Gleason. "The psychological significance of play with imaginary companions in early childhood". Learning & Behavior. 45(4). :432-440. (2017)
- Hewitt L, Kerr E, Stanley RM, Okely AD. "Tummy Time and Infant Health Outcomes: A Systematic Review". Pediatrics. 145(6). (2020)
- High PC, Klass P, et al. "Literacy Promotion: An Essential Component of Primary Care Pediatric Practice". Pediatrics. 134(2). :404-409. (2014)
- Yogman M, Garner A, Hutchinson J, et al. "The Power of Play: A Pediatric Role in Enhancing Development in Young Children". Pediatrics. 142(3). (2018)
- Zubler JM, Wiggins LD, Macias MM, et al. "Evidence-Informed Milestones for Developmental Surveillance Tools". Pediatrics. (2022)
- Gomella T, Cunningham M, Eyal F. "Neonatology: Management, Procedures, On-Call Problems, Diseases, and Drugs, Sixth Edition". McGraw Hill Professional. (2009). ISBN: 9780071544313
- Chapman MW, James MA. "Chapman's Comprehensive Orthopaedic Surgery". Jaypee Brothers Medical Publishers. (2019). ISBN: 9789351524977
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Schott JM. "The grasp and other primitive reflexes". J Neurol Neurosurg Psychiatry. 74(5). :558-560. (2003)
- Davis LE, King MK, Schultz JL. "Fundamentals of Neurologic Disease". Demos Medical Publishing. (2005). ISBN: 9781888799842
- Kamity R, Kapavarapu PK, Chandel A. "Feeding Problems and Long-Term Outcomes in Preterm Infants—A Systematic Approach to Evaluation and Management". Children. 8(12). :1158. (2021)
- Rousseau PV, Matton F, Lecuyer R, Lahaye W. "The Moro reaction: More than a reflex, a ritualized behavior of nonverbal communication". Infant Behav Dev. 46. :169-177. (2017)
- Schulkin J, Power M. "Integrating Evolutionary Biology Into Medical Education". Oxford University Press, USA. (2019). ISBN: 9780198814153
- Menkes JH, Sarnat HB, Maria BL. "Child Neurology". Lippincott Williams & Wilkins. (2006). ISBN: 9780781751049
- Patestas MA, Gartner LP. "A Textbook of Neuroanatomy". John Wiley & Sons. (2016). ISBN: 9781118677469
- McMillan JA, Feigin RD, DeAngelis C, Jones MD. "Oski's Pediatrics". Lippincott Williams & Wilkins. (2006). ISBN: 0781738946
- Bickley LS, Szilagyi PG, Bates B. "Bates' Guide to Physical Examination and History Taking". Lippincott Williams & Wilkins. (2009). ISBN: 9780781780582
- Jan M. "Manual of Child Neurology". Bentham Science Publishers. (2012). ISBN: 9781608050222
- Ali F, Harris N. "Orthopaedic Examination Techniques". Cambridge University Press. (2022). ISBN: 9781108796705
- Volling. "Family Transitions Following the Birth of a Sibling: An Empirical Review of Changes in the Firstborn’s Adjustment". Psychological Bulletin. 138. :497–528. (2012)
- "Sibling Rivalry - The Arrival of a Baby Brother or Sister". https://childpsychotherapy.org.uk/resources-families/understanding-childhood/sibling-rivalry-arrival-baby-brother-or-sister. [2020-01-01]
- Serwint et al. "The AAP Resilience in the Face of Grief and Loss Curriculum". Pediatrics. 138(5). (2016)
- Lipkin PH, Macias MM, Norwood KW, et al. "Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening". Pediatrics. 145(1). (2020)
- Vitrikas K, Savard D, Bucaj M. "Developmental Delay: When and How to Screen". Am Fam Physician. 96(1). :36-43. (2017)
- Blaney SM, Giardino AP, Orange JS, et al. "Rudolph's Pediatrics, 23rd Edition". McGraw-Hill Education / Medical. (2018). ISBN: 9781259588594
- Brown KA, Parikh S, Patel DR. "Understanding basic concepts of developmental diagnosis in children". Transl Pediatr. 9(S1). :S9-S22. (2020)
- Sigafoos J, et al. "Persistence of Primitive Reflexes in Developmental Disorders". J Autism Dev Disord. 8(2). :98-105. (2021)
- Savatt JM, Myers SM. "Genetic Testing in Neurodevelopmental Disorders". Front Pediatr. 9. (2021)
- "Learn the signs. Act Early. CDC’s Developmental Milestones". https://web.archive.org/web/20230408230612/https://www.cdc.gov/ncbddd/actearly/milestones/index.html#print. [2022-12-29]
- Zubler J, Whitaker T. "CDC's Revised Developmental Milestone Checklists". Am Fam Physician. 106(4). :370-371. (2022)
- Dosman CF, Andrews D, Goulden KJ. "Evidence-based milestone ages as a framework for developmental surveillance". Paediatr Child Health. 17(10). :561-568. (2012)