Summary
Child maltreatment is any act or failure to act that results in potential or actual harm to a child, usually involving a caregiver. Types of child maltreatment include neglect, physical abuse, sexual abuse, psychological maltreatment, and medical child abuse. Children under the age of 1 year are most commonly affected. Risk factors for child maltreatment include physical or developmental disabilities and caregiver factors (e.g., substance use disorders, intimate partner violence). When child maltreatment is suspected, use a trauma-informed approach to perform a detailed clinical evaluation, including evaluation of acute injuries, medical and developmental history, growth assessment, and a physical examination, ensuring detailed documentation. Management includes medical stabilization if necessary and immediately reporting any suspected child maltreatment to Child Protective Services (CPS). Additional diagnostic testing and management should be performed based on the type of abuse suspected (e.g., imaging for patients with suspected fractures, STI testing for suspected sexual abuse). Prevention includes the identification and management of risk factors for child maltreatment.
Overview
Definition [1][2]
- Any act or failure to act that results in potential or actual harm to a child, usually involving a caregiver
-
Types of child maltreatment include: [2]
- Child neglect
- Physical child abuse
- Child sexual abuse
- Psychological maltreatment of a child
- Medical child abuse
- Exact legal definitions of child maltreatment vary by state; check local laws.
Epidemiology [1]
- Approx. 7 per 1000 children in the US experience child maltreatment annually.
- The highest rate of child maltreatment and death is in children < 1 year of age. [1]
- The perpetrator is usually a caregiver (a parent is involved > 80% of the time).
- Affects children of all races and socioeconomic groups, but appears to be: [3][4]
- Overreported in Black, Latino, and multiracial families and households with low socioeconomic status
- Underreported in White and affluent families
Risk factors for child maltreatment [2][5]
Child factors
- Physical or developmental disabilities
- Behavioral issues
- Chronic medical conditions
- Preterm birth
- Unintentional or unwanted pregnancy
Caregiver and family factors
- Intimate partner violence
- Personal history of abuse during childhood
- Unemployment, financial hardship
- Low level of education
- Substance use disorders and/or mental health issues (e.g., depression)
- Limited understanding of parenting (e.g., of normal childhood behavior and development)
- Young and/or single parents
- Social isolation
- Other individuals residing in the home (e.g., partner of the parent or caregiver, foster siblings, extended family members) [1]
Approach to suspected child maltreatment
- Always use a trauma-informed approach in suspected cases of child maltreatment.
- Interview the child and parent/caregiver separately, if possible. [5]
- Elements of the assessment may be used as legal evidence. [2]
- Ensure detailed documentation.
- Swabs, clothing, and other items may contain biological evidence (e.g., blood, semen).
- Tailor assessment to the type of suspected abuse, but be aware that more than one type may have occurred.
Involve a multidisciplinary child abuse team and/or medical forensic specialists when available. [2][5]
Clinical evaluation [2][6]
-
History from the caregiver
- Medical and surgical history, including:
- Prenatal and birth history [5]
- Pediatric developmental history
- Developmental milestones
- Family history of genetic, metabolic, and bone diseases
- Social history for risk factors for child maltreatment
- Acute injuries: Ask about the nature, mechanism, and timing of injury.
- Medical and surgical history, including:
-
History from the child
- Conduct the interview without the caregiver present, if possible.
- Ask the child about their concerns and what occurred using age-appropriate, open-ended questions.
- Focus on information necessary for the diagnosis and treatment of medical conditions.
- Assess for potential mental health complications of abuse, including:
- Acute and posttraumatic stress disorders
- Signs of depression (see “Depression in children”)
-
Physical examination [2]
- Ensure a chaperone is present.
- Examine all systems, including complete skin examination for injuries (e.g., bruising).
- Assess growth (see also “Clinical features of growth faltering”).
- For acute injuries, see also:
- “Pediatric fractures”
- “Approach to burns”
- If child sexual abuse is suspected, see “Physical examination for child sexual abuse.”
Validated tools, e.g., modified versions of the HITS screen for children (PedHITSS) and teenagers (TeenHITSS), can help detect child maltreatment. [2][7]
Red flags for child maltreatment [5]
- History does not fit clinical findings or patterns of behavior for the child's age
- Changing history of an injury or illness
- Delay in seeking medical treatment
- Features of child neglect
- Injuries concerning for nonaccidental trauma
- Red flags for child sexual abuse
- Red flags for human trafficking
- Red flags for medical child abuse
Management [2][8]
- Notify Child Protective Services for all suspected cases of child maltreatment; , and if there is an immediate concern for safety, law enforcement.
- Admit to hospital if medical stabilization is required.
- Assess the safety of other individuals in the household.
- Determine if there are other children in the home; assess as needed. [3]
- Consider caregiver screening for intimate partner violence. [9]
- Tailor assessment to the suspected type of abuse (see the relevant sections for further information).
-
Physical child abuse
- Perform dedicated imaging of any suspected injury site and, if appropriate, a skeletal survey.
- Consider a coagulation panel and CBC to assess for coagulopathy. [10]
- Child sexual abuse: Offer STI screening and emergency contraception as needed.
- Suspected poisoning (accidental or intentional) : Consider toxicology screening. [3]
-
Physical child abuse
- Consult with specialists as needed, e.g.:
- Child abuse pediatricians
- Ophthalmology
- Radiology
- Orthopedics
- Mental health providers
Physicians are required by law to report concerns if there are red flags for child maltreatment. [8]
Child neglect
Child neglect is the failure to meet a child's basic physical, emotional, medical, or educational needs. [2]
Types of child neglect [2]
- Failure to provide appropriate food, clothing, or shelter
- Poor supervision and protection from potential harm
- Denying emotional support and social interaction
- Avoiding medical care when required
- Failure to meet educational needs
Child neglect is the most common form of child maltreatment. [2]
Clinical features of child neglect [2][11][12]
- Growth faltering
- Abnormal language, social, and/or emotional development
- Abnormal attachment (e.g., reactive attachment disorder)
- Frequent hunger
- Inadequate, inappropriate, or soiled clothing
- Poor personal hygiene
- Dental problems
- Social issues with peers or adults (e.g., disinhibited social engagement disorder)
- Behavioral concerns (e.g., impulse and conduct disorders)
- Clinical features of ADHD
- Substance use
Management [2]
- Inquire about contributing factors, e.g.:
- Poverty
- Insecure housing
- Food insecurity
- Barriers to accessing health care
- Provide education on safe care (see “Anticipatory guidance for children”) and refer to community resources.
- Refer to CPS for persistent neglect despite referrals for assistance.
- See also “Approach to suspected child maltreatment.”
Prognosis
Child neglect can have long-term intellectual, social, and mental health consequences and can result in death. [2]
Psychological maltreatment
Psychological maltreatment of a child is defined as recurrent actions and behaviors from parents or caregivers that have a negative impact on the cognitive, social, emotional, and physical development of a child. [13]
Types of psychological maltreatment [13]
- Spurning (e.g., name-calling, insulting)
- Terrorizing (e.g., intimidation, threats of violence)
- Isolating from peers and adults
- Exploiting and/or corrupting (e.g., allowing the child to witness abuse being inflicted on another)
- Emotional detachment
- Neglect for reasons other than inadequate resources
Clinical features [13]
- Attachment issues (e.g., reactive attachment disorder)
- Disruptive behaviors in childhood (e.g., aggression toward other children or animals, atypical tantrums)
- Developmental delay
- Issues with academic performance
- Impaired social skills
- Depressed or anxious mood
- Psychosocial short stature or growth faltering
Management
- See “Approach to suspected child maltreatment.”
- Additional management for psychological maltreatment includes:
- Close monitoring of behavioral and physical development over time
- Providing or referring to services based on the nature and consequences of abuse.
Prognosis
Psychological maltreatment is associated with mental health and substance use disorders in adulthood [14]
Physical child abuse
Overview [2][5][8]
- Physical abuse is any nonaccidental injury to a child.
- Most common in young children, particularly in the first year of life [3][15]
- Consider physical abuse with injuries involving any of the following:
- Patterns suspicious for nonaccidental injuries in children
- Multiple organ systems
- Sites that do not overlie bones
- Accompanying red flags for child maltreatment
| Features and mimics of physical child abuse [2][5] | ||
|---|---|---|
| Feature | Patterns suspicious for nonaccidental injuries in children | Mimics of physical child abuse |
| Bruises |
|
|
| Bite marks |
|
|
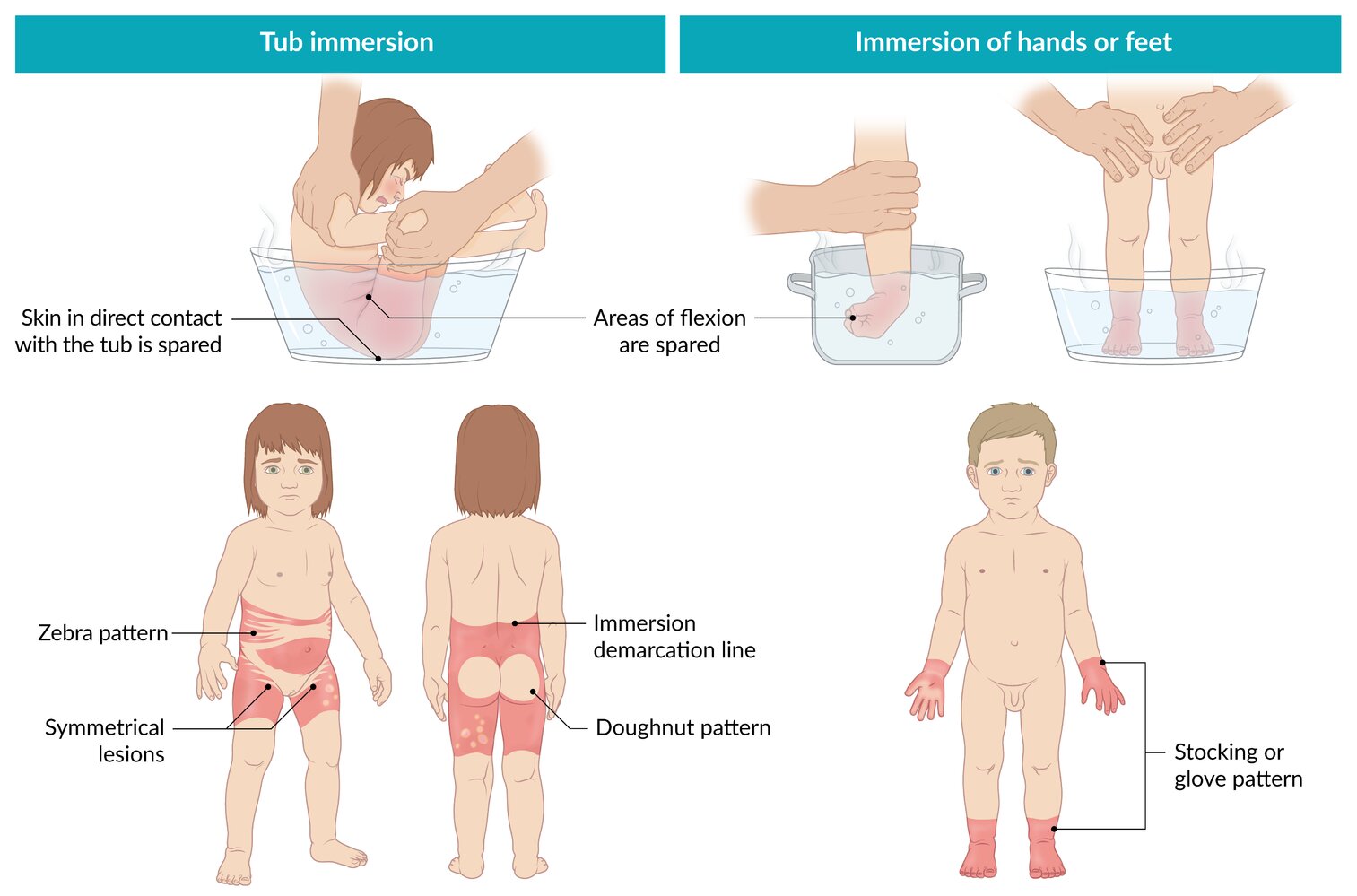
| Scalds and burns [16] |
|
|
| Fractures [8] |
|
|
| Abusive head trauma |
|
|
Maintain a high index of suspicion for physical child abuse in young children; up to 20% of nonaccidental fractures are misattributed to other causes in children < 3 years of age. [8]
Suspicious bruises (TEN4): Torso, Ear, Neck, any bruise in these locations in children ≤ 4 years of age and any bruise (regardless of location) in infants < 4 months of age
Management of physical child abuse [2][8]
- See “Approach to suspected child maltreatment.”
- Additional workup for suspected physical child abuse includes:
- Documenting injury characteristics in detail (e.g., location, size, shape, color, nature)
- Detailed imaging of any suspected injury sites
- Skeletal survey in younger and nonverbal children
- Consideration of coagulation panel and CBC for undiagnosed coagulopathy in children with isolated: [10]
- Bruising
- Intracranial hemorrhage
Other children in the household of victims of physical abuse should also be evaluated for evidence of abuse. [8]
Skeletal survey [8][15]
-
Indications [19]
- All children ≤ 24 months of age with suspected physical abuse
-
Assessment of children > 24 months of age with: [8][19]
- > 1 fractures with no history of injury or inconsistent with described injury
- Occult fractures
- Difficulties communicating (e.g., developmental delay)
-
Components: X-ray images of all of the following areas. [20]
- Skull
- Chest, including oblique views of the ribs
- Cervical, thoracic, and lumbosacral spine
- Pelvis
- Upper and lower extremities (including long bones, hands, and feet)
Repeat a focused skeletal survey in 2 weeks in patients ≤ 24 months of age with abnormal or equivocal findings on initial imaging and/or in whom clinical suspicion of physical abuse remains. [8][19]

There are multiple linear ecchymoses and abrasions with central sparing on the back of this child. The source of the injury is likely a cane or other cylindrical object. As the object strikes the skin, blood is forced out from the blood vessels, creating a central area of sparing between two linear ecchymoses.
Source: © IMPP

Back and head of a 4-year-old boy
The lateral back of the child (A) shows two elongated, scarred skin lesions (one with a central recess), which suggests physical abuse with an elongated cylindrical object (black arrows). Hematomas and swelling can be seen in the forehead area (B) and bilateral periorbital hematomas (red arrows) are visible. On the right shoulder, a hypopigmented area caused by a burn is visible (black arrow).
Source: “Figure 2, in: A Multispecialty Approach to the Identification and Diagnosis of Nonaccidental Trauma in Children” by Manan M, Rahman S, Komer L, et al., Cureus, licensed under CC BY 4.0.
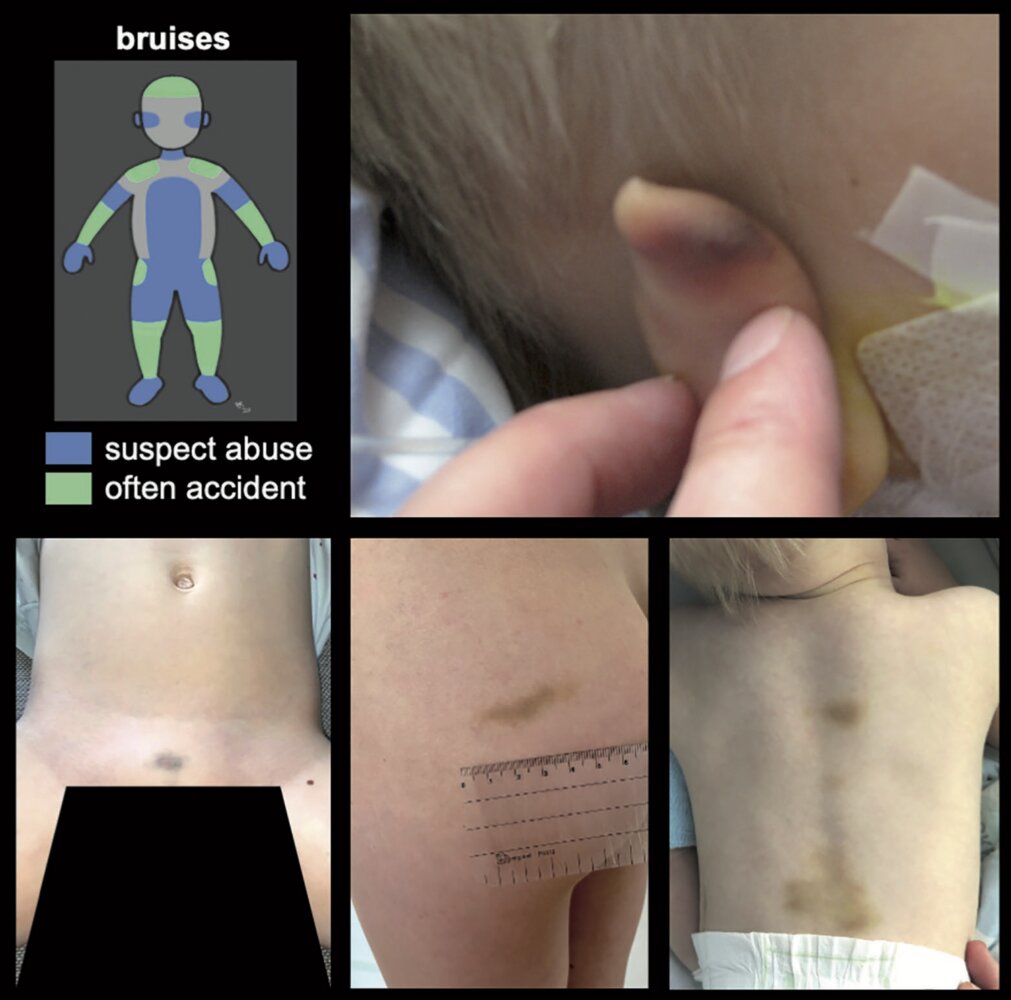
The diagram (top left) shows common locations of bruising in children typical for abuse (blue) and often caused by accidents (green).
The photographs show examples of bruises at locations suspicious for abuse, including the auricle (upper right), genital area (lower left), buttocks (lower middle), and back (lower right).
Source: “Figure 2, in: Physical child abuse demands increased awareness during health and socioeconomic crises like COVID-19 - A review and education material” by Martinkevich P, Larsen LL, Græsholt-Knudsen T, et al., Acta Orthopaedica, licensed under CC BY 4.0. Further notes: Image is part of the "supplementary data" of the paper

An approx. 5 cm, blue-gray macule with irregular borders is visible on the back. The macule has no evidence of hypertrichosis.
© AMBOSS

Maculopapular, reddish, non-blanching, palpable skin lesions (purpura) are seen on both the distal right arm and leg. On the lower leg, the lesions are partially confluent and present with scaling and erosion.
Source: "Purpura2", Okwikikim, Wikimedia Commons licensed under Public Domain
{kind=link}

Human bite mark on the left upper arm
There is a well-demarcated, ovoid contusion characterized by multiple punctate abrasions and ecchymosis, arranged in a pattern consistent with involvement of both the maxillary and mandibular dental arches. The central region of the lesion shows lighter bruising.
This appearance is characteristic of a human bite injury.
Source: “Fig. 1, in: Importância do odontolegista nas perícias criminais: análise de marca de mordida humana em um caso de homicídio” by Andrade Caneiro U, Marques Santiago B, da Silva Barbosa Freire CH, Morais Marques JA, Cardoso Bento MI, Research, Society and Development, licensed under CC BY 4.0.
© AMBOSS
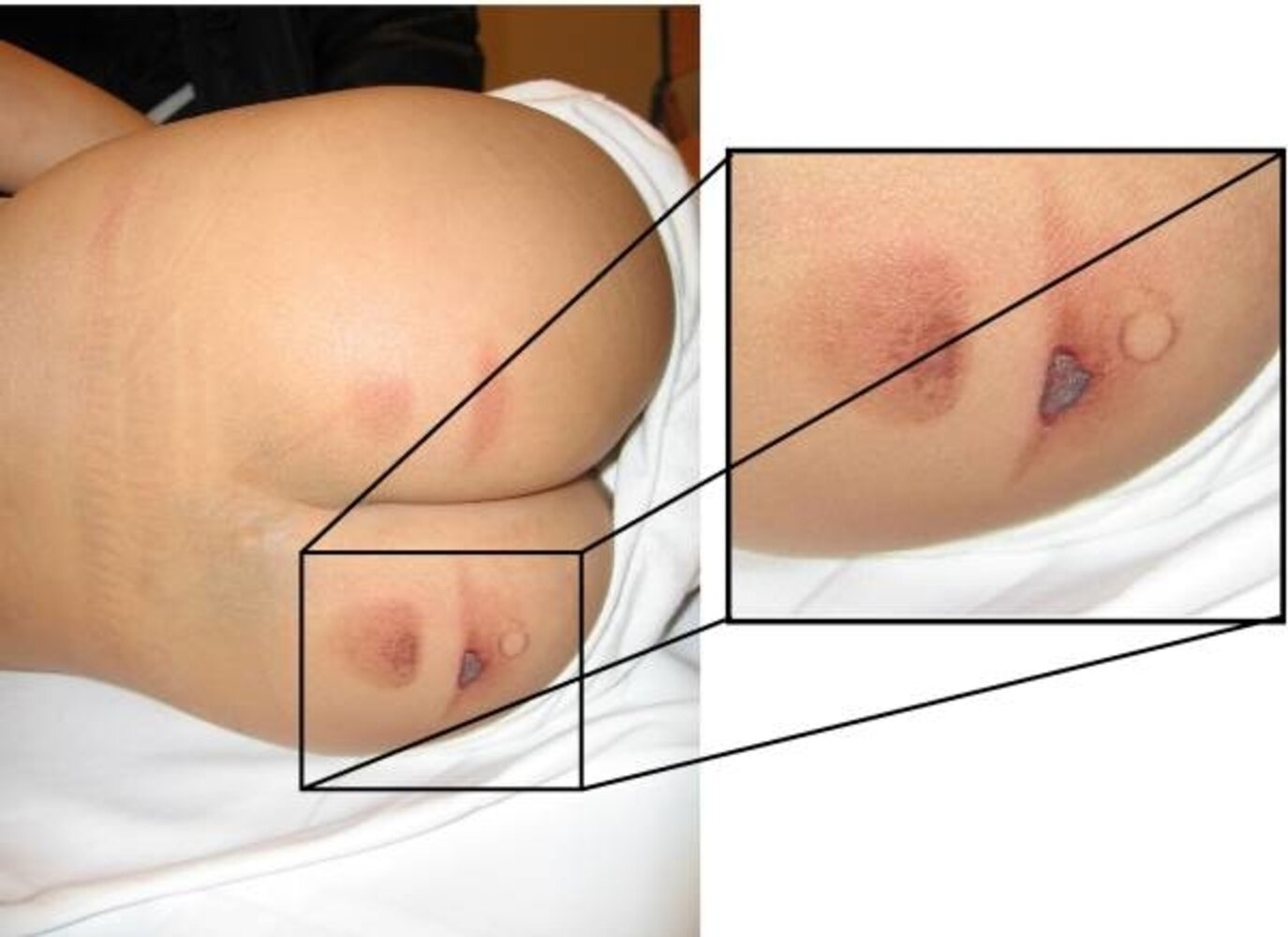
There are bilateral burns on the buttocks of this child.
Bilateral and well-demarcated burn lesions are suggestive of nonaccidental injury. Of note, the blue area at the top of the buttocks is a congenital dermal melanocytosis, which is a benign finding that is common in children and can be mistaken for bruising.
Source: “Figure 5, in: A Multispecialty Approach to the Identification and Diagnosis of Nonaccidental Trauma in Children” by Manan M, Rahman S, Komer L, et al., Cureus, licensed under CC BY 4.0.

Photograph of the torso, left shoulder, and neck
There are extensive, irregular areas of burn injury with varying wound depth and poorly defined margins. The mottled red/white coloration indicates a deep partial-thickness burn with damage extending down to the deeper layers of the dermis.
The irregular pattern of the burn suggests accidental injury.
Source: “Figure 3, in: Retrospective Evaluation of Progenitor Biological Bandage Use: A Complementary and Safe Therapeutic Management Option for Prevention of Hypertrophic Scarring in Pediatric Burn Care” by Al-Dourobi K, Laurent A, Deghayli L, et al., MDPI - Pharmaceuticals, licensed under CC BY 4.0. Modifications: Image cropped, number removed.

The shape of the bruises reflects the position and shape of cups applied to the skin.
Bruising resulting from cupping should be differentiated from other forms of injury (e.g., burns), especially in children.
Source: “Cupping results.jpg” by Bentevb, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

There is diffuse erythema of all visible skin. Large ruptured blisters are visible on the left lower leg, and a large flaccid unruptured blister can be seen on the left buttock.
Source: “Figure 1, in: Staphylococcal Scalded Skin Syndrome in Neonate” by K. Kouakou, M. E. Dainguy, K. Kassi, Case Reports in Dermatological Medicine, licensed under CC BY 3.0.

An erythematous rash with numerous small vesicles in a linear pattern can be seen on the left forearm.
This rash is typical of mild allergic contact dermatitis caused by urushiol-containing plants (e.g., poison oak). In more severe cases, bullae and pronounced edema may be present.
Source: "4484", CDC, Centers for Disease Control and Prevention, Atlanta, USA licensed under Public Domain


X-ray right elbow (A: AP view, B: lateral view) and CT right elbow (C: frontal plane; D: sagittal plane) of a 16-year-old baseball pitcher with progressive posterior elbow pain
No fracture is visible on the AP radiograph; however, a subtle irregular line (green arrows) projecting over trabecular bone on the lateral view raises the possibility of a fracture. CT images reveal a nondisplaced oblique fracture through the mid-third of the olecranon (white arrows).
Stress fractures may be very subtle or not visible at all on radiographs. Additional imaging is warranted when clinical findings suggest injury, but radiographs are equivocal or negative. CT, MRI, and bone scintigraphy have been used to further evaluate stress fractures.
Source: “Fig. 1, in: Treatment of stress fracture of the olecranon in throwing athletes with internal fixation through a small incision” by Fujioka H, Tsunemi K, Takagi Y, Tanaka J, BMC Sports Science, Medicine and Rehabilitation, licensed under CC BY 2.0. Modifications: letter markers removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

X-ray lower leg (AP view) of a child
A nondisplaced spiral fracture of the distal tibial diaphysis (arrows) is not accompanied by conspicuous periosteal reaction. The fibula is normal.
Toddler fractures are usually accidental injuries. They can be subtle and sometimes require additional views, follow-up radiographs, or bone scintigraphy for diagnosis. Ultrasound may also be useful.
Source: “Tibfracture.png” by Doc James, Wikimedia commons, licensed under CC BY-SA 3.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Source: “Figure 3, In: Locations of bruises suspicious of physical abuse in children” by Polina Martinkevich, Lise Langeland Larsen, Troels Græsholt-Knudsen, Gitte Hesthaven, Michel Bach Hellfritzsch, Karin Kastberg Petersen, Bjarne Møller-Madsen & Jan Duedal Rölfing, Acta Orthopaedica, licensed under CC BY 4.0.
Abusive head trauma (shaken baby syndrome)
General principles
- Abusive head trauma (shaken baby syndrome) is a characteristic pattern of intracranial trauma seen in severe physical child abuse. [21]
- Most common cause of death from head injury in children < 2 years of age [21]
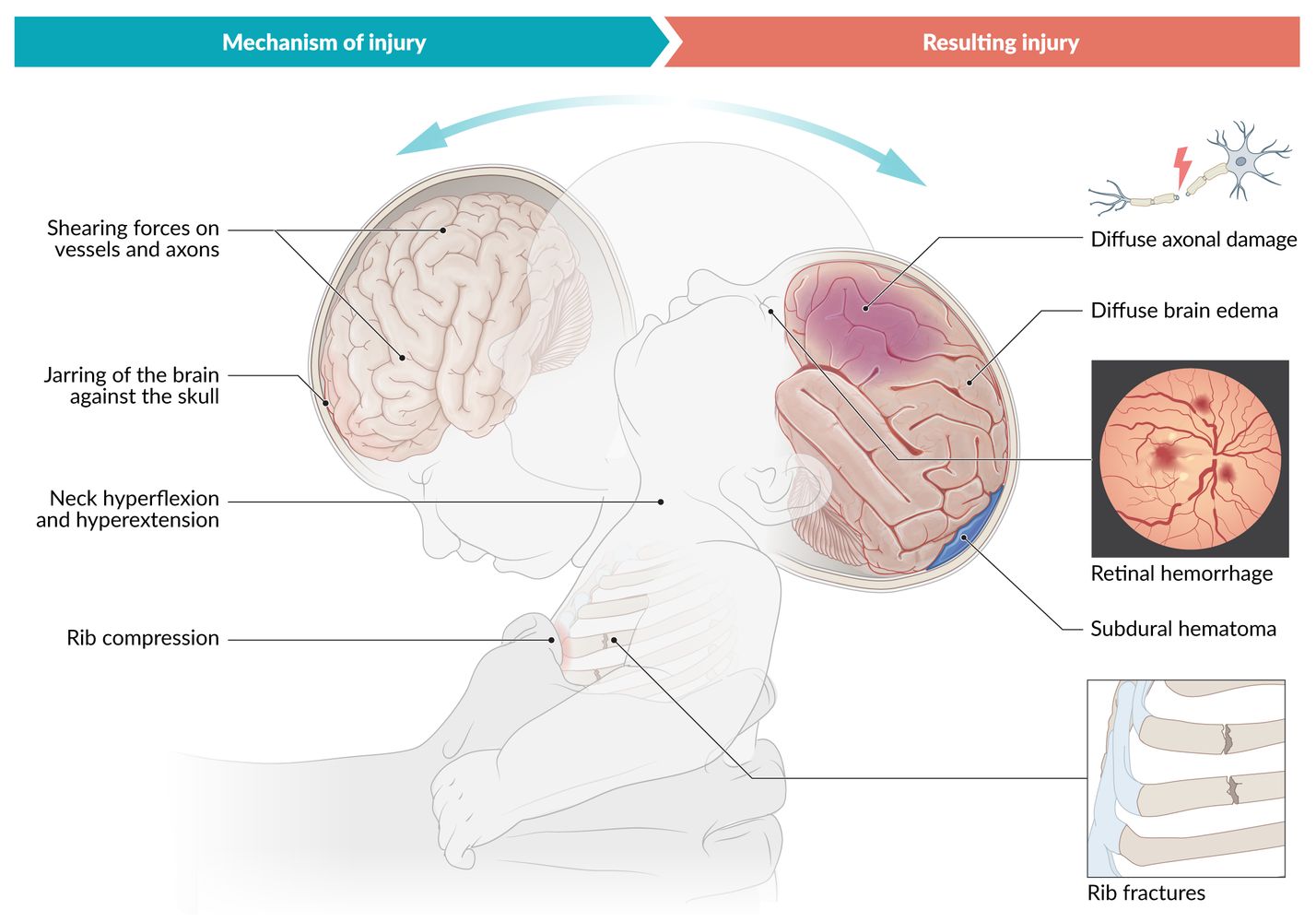
- Pathophysiology includes: [22]
- Rotational and shearing forces → shearing off of bridging veins → subdural hematoma
- Shaking of a child with weak neck support → respiratory problems and apnea → hypoxia → brain edema and ischemia → diffuse axonal damage
Clinical features [21][23][24]
- Irritability or lethargy
- Seizures
- Vomiting
- Inconsistent or implausible history from caregiver
-
On examination: external injuries may not be visible
- Retinal hemorrhages
- Tense fontanelle [25]
- Macrocephaly [24]
- Other injuries suggestive of physical child abuse
External injuries may be hardly evident or absent in abusive head trauma. [21]
Diagnostics [19][24]
-
Initial imaging: usually CT head without contrast
- Performed in the emergency setting for suspected acute bleeding and bony evaluation
- Findings include:
- Subdural hematomas and/or subarachnoid hemorrhage of varying ages
- Reversal sign: diffuse blurring of the gray-white matter interface coupled with increased density of the thalamus and cerebellum [25][26]
- Diffuse punctate hemorrhages [27]
- Skull fracture
-
Additional imaging
-
MRI brain is performed if CT head is abnormal or concern for trauma persists, to evaluate for: [19]
- Small volume extra-axial hemorrhage
- Developing parenchymal injuries
- MRI spine: for assessing spinal injuries [19]
- Skeletal survey: indicated for all children < 2 years of age with abusive head trauma [28]
-
MRI brain is performed if CT head is abnormal or concern for trauma persists, to evaluate for: [19]
-
Fundoscopy: performed by an ophthalmologist
- Assess within 24–36 hours of injury. [24]
- For signs, see “Findings in retinal hemorrhage.”
Differential diagnoses
See “Mimics of physical child abuse.”
Management
- Initial management of TBI to stabilize the patient
- See “Management of physical child abuse.”
Complications
- Death
- Neurological deficits (e.g., sight, hearing, and speech impairment)
- Posttraumatic epilepsy
- Developmental delay
Abusive head trauma is fatal in up to 20% of children. [24]




© AMBOSS
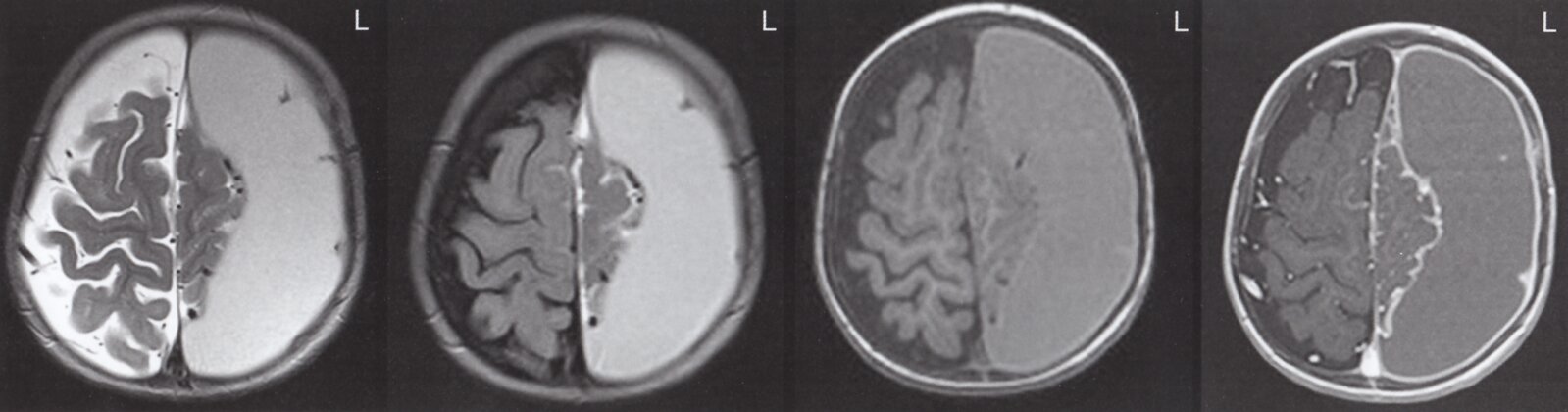
MRI head (axial plane; left to right: T2-weighted without contrast, T2 FLAIR without contrast, T1-weighted without contrast, T1-weighted with contrast) of infant one week after traumatic brain injury
An extracerebral crescent-shaped fluid collection (yellow overlay) is hyperintense on the T2-weighted sequence without contrast and produces mass effect on the left cerebral hemisphere with mild midline shift to the right side (indicated by dashed line and arrowheads). It is not restricted by cranial sutures and does not cross the midline, consistent with a subdural collection. The collection is hyperintense to CSF on the T2 FLAIR sequence and hyperintense to gray matter on the T1-weighted sequence without contrast, suggesting a subacute subdural hematoma. Meningeal enhancement is seen on the T1-weighted sequence with contrast (blue overlay).
Source: © IMPP
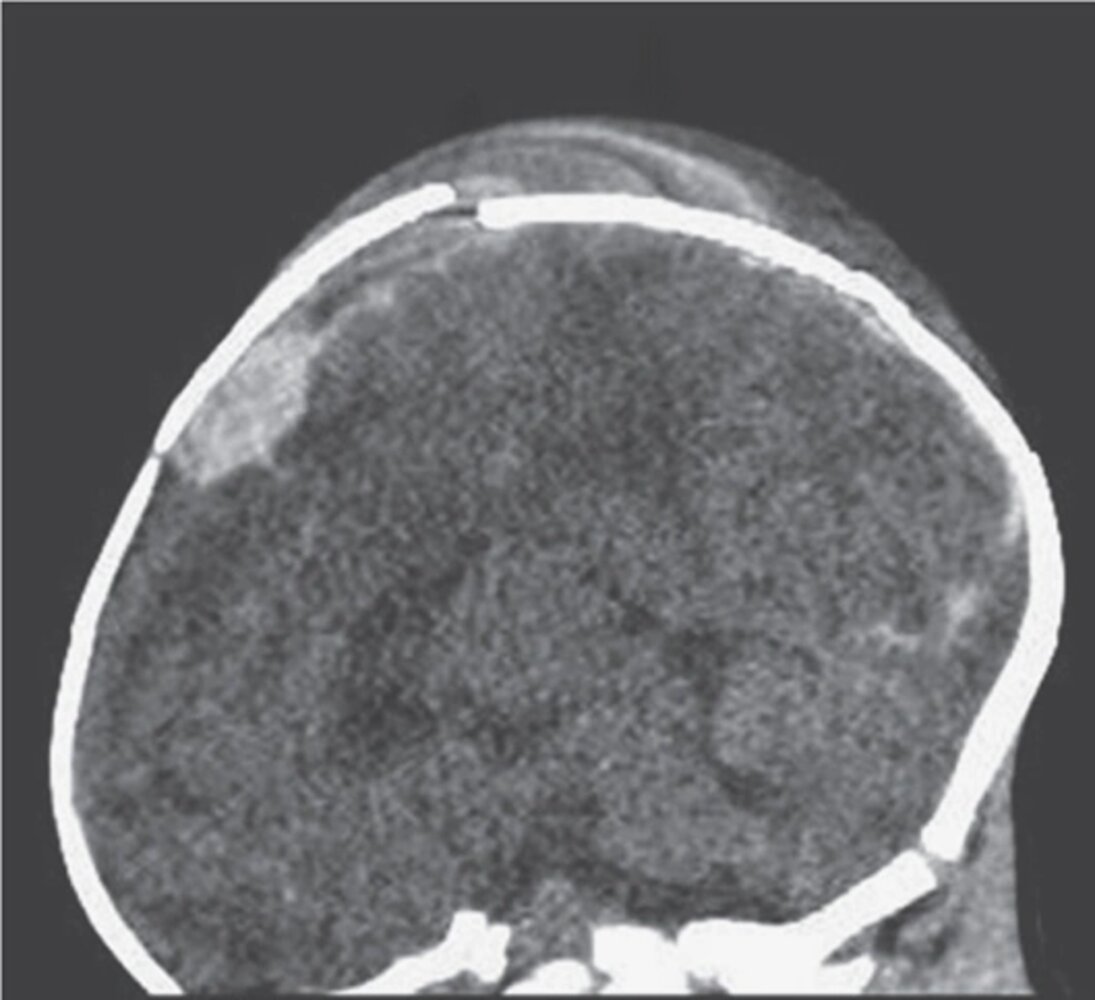
CT head (sagittal plane) of a 7-week-old boy with reduced consciousness
A displaced calvarial fracture (yellow overlay) is accompanied by an extra-axial hematoma (blue overlay) and a cephalohematoma (arrows).
This is an example of nonaccidental injury. A 7-week-old infant is incapable of self-mobilization. Although the diagnosis of nonaccidental injury cannot be made solely through imaging, the patient's age and the extent of this injury should prompt consideration of abusive head trauma.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
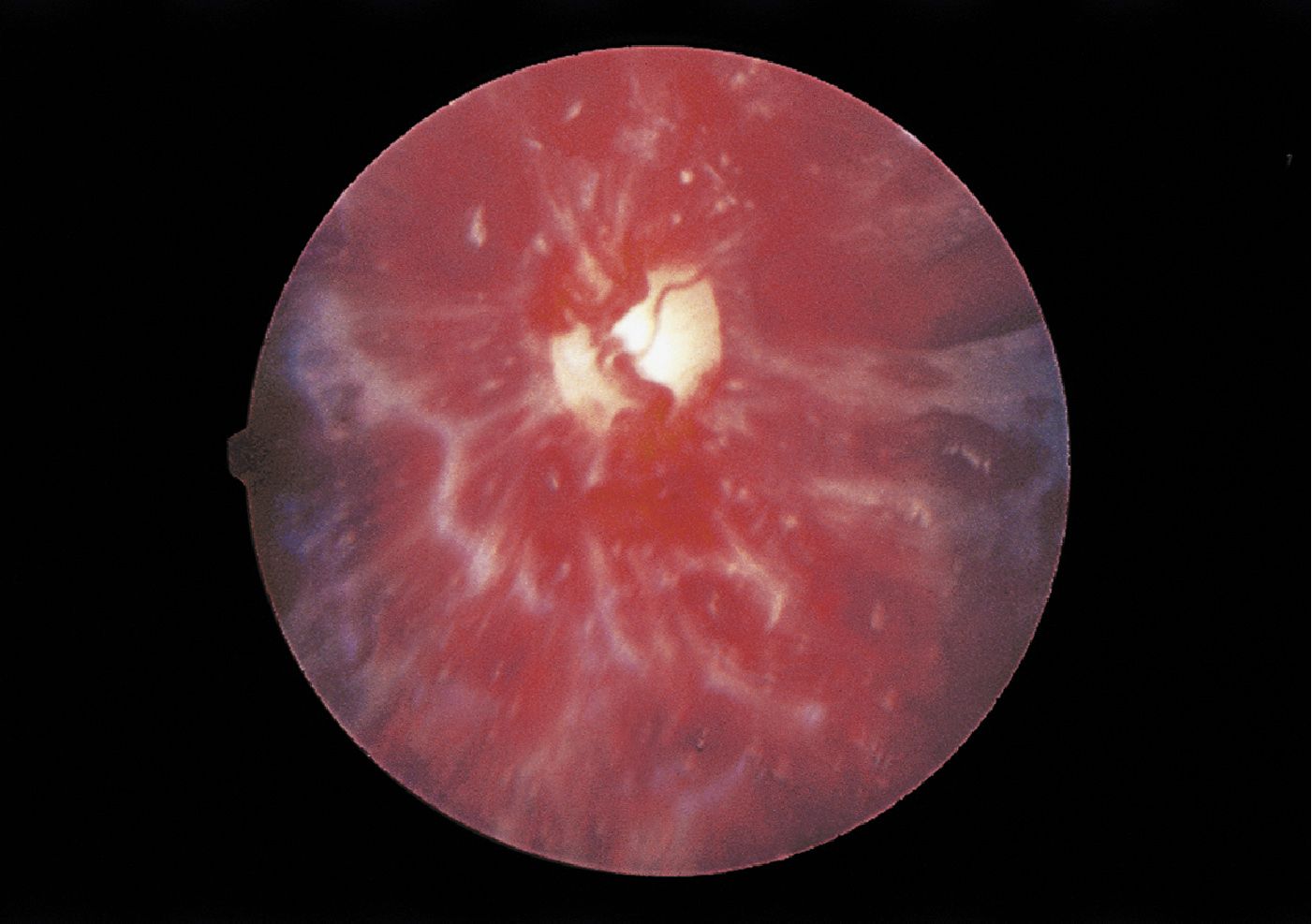
Fundus photography of the left eye of a 5-month-old infant presenting with seizures
There are multiple diffuse intraretinal and preretinal hemorrhages and a retinal fold (indicated by blue overlay).
These features should raise suspicion for abusive head trauma (shaken baby syndrome), a type of nonaccidental traumatic brain injury.
Blue circle: optic disc
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
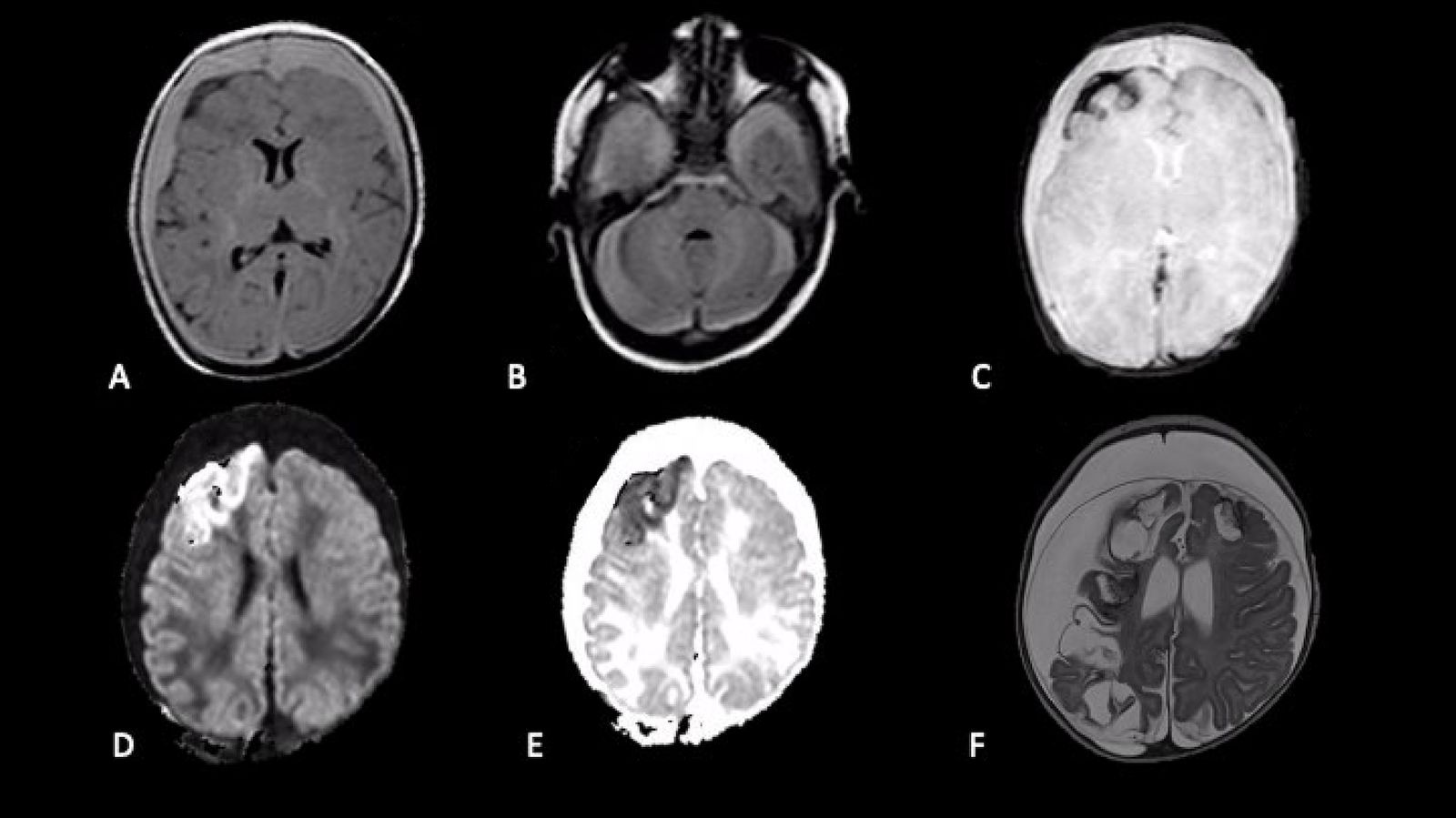
MRI head (axial plane) of a newborn who presented with with generalized seizures, fever, and vomiting
A and B: FLAIR
Crescentic supratentorial (A) and infratentorial (B) subdural hematomas (arrows) are slightly hyperintense to parenchyma.
C: Susceptibility-weighted imaging (SWI)
Hypointense subarachnoid hemorrhage (arrow) extends into right frontal lobe sulci.
D: Diffusion-weighted imaging (DWI) and E: apparent diffusion coefficient (ACD) map
Right frontal lobe cortical-subcortical hemorrhage appears hyperintense on DWI and hypointense on the ACD map (arrows).
F: T2-weighted (one-month follow-up) Bilateral cresentic subdural hygromas (arrows) and areas of encephalomalacia (examples indicated by arrowheads) are isointense to CSF. Mass effect from the hygromas causes compression of brain parenchyma and a thin membrane (blue overlay) is visible.
Source: “Figure 2, in: Shaken Baby Syndrome: Magnetic Resonance Imaging Features in Abusive Head Trauma” by Cartocci, Gaia, Vittorio Fineschi, Martina Padovano, Matteo Scopetti, Maria C. Rossi-Espagnet, and Costanza Giannì, Brain Sciences, licensed under CC BY 4.0. Modifications: - removed white rim - arrows and asterixes removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Child sexual abuse
Definitions
-
Child sexual abuse: involvement of a child in sexual activity with an adult or other child that involves any of the following [29]
- Lack of proper understanding and inability to provide informed consent
- Lack of developmental readiness and/or inability to provide consent
- Is illegal or socially unacceptable
- Child sex trafficking: a form of human trafficking involving any role in a child's participation in sexual activity for commercial purposes (e.g., recruitment, harboring, transporting) [1]
Epidemiology
- The perpetrator is usually an adult who is known to the child. [30]
- Estimated lifetime incidence: 5–25% [6]
Types of child sexual abuse
- Sexual intercourse (oral, anal, or vaginal penetration)
- Molestation (genital contact without penetration)
- Exposure to a perpetrator's genitalia
- Forced sexual interaction with another child or object
- Exposure to explicit material
Clinical features of child sexual abuse [6]
- Behavior or sexual insights that are age-inappropriate [31]
- Injuries in the genital, anal, and oral areas [32]
- Recurrent urinary tract infections
- Signs and symptoms of STIs
- Pregnancy
- Often no visible signs on physical examination
- See also “Red flags for human trafficking” and “Red flags for sexual assault.”
Differential diagnoses
See also “Vulvovaginitis in children.” [33]
Even in the absence of physical signs, sexual abuse should always be considered in young children presenting with behavioral changes or signs of sexually transmitted infections.
Management of suspected child sexual abuse [6][29]
Approach [6][32]
- See “Approach to suspected child maltreatment” for the basic principles of initiating an assessment.
- Refer directly to a specialized child sexual abuse service, if available. [6]
- If not available, as indicated:
- Perform STI testing.
- Initiate HIV postexposure prophylaxis.
- Give HPV and hepatitis B vaccinations.
- For postpubertal individuals, offer:
- Emergency contraception
- Pregnancy testing
- Prophylaxis for bacterial STIs (see “Postassault STI prophylaxis”). [32]
- Refer for a sexual assault forensic examination. [34]
- See gonorrhea in children and chlamydia in children
- Arrange appropriate follow-up.
- Consider repeat physical examination and STI testing in 2–6 weeks for patients with recent sexual contact.
- Repeat serological testing in 6–12 weeks if HIV, HBV, or syphilis is suspected and initial testing is negative.
- Refer to specialists (e.g., child abuse pediatrician, mental health providers) as indicated.
Collection of forensic evidence is recommended within 72 hours of abuse involving bodily fluids. [6]
Physical examination for child sexual abuse [6]
- Ensure a chaperone is present (e.g., caregiver or other medical professional).
- Outline the examination steps before starting.
- Examine the child fully for other signs of child maltreatment.
- Include an anogenital examination; instrumentation is not necessary in most cases.
Refer children with abnormalities on anogenital examination for specialist evaluation (e.g., child abuse pediatrician). [6]
Do not perform a speculum examination in a prepubertal child. Refer patients with suspected internal genital trauma for examination under anesthesia. [6]
STI testing [32]
-
Indications
- All adolescents evaluated for sexual abuse
- Younger children evaluated for abuse with certain factors, e.g.:
- Anogenital or oropharyngeal penetration
- Perpetrator is unknown
- Perpetrator is known to have an STI or is at high risk for STIs
- Household member with an STI
- High community STI rates
- Clinical features of STI or diagnosis of one STI
- Patient or family request
- Inability to communicate details of the abuse
-
Methods: Perform STI testing before initiating treatment to improve the accuracy of results. [32]
- All patients: testing for gonorrhea in children and chlamydia in children
- Vesicles or ulcers in the anogenital area: diagnostics for HSV
-
Serologic testing for the following, if suspected:
- Syphilis
- HIV
- Hepatitis B
- Girls only:
- Wet mount and culture for trichomoniasis
- Wet mount for bacterial vaginosis, if there is vaginal discharge
Presumptive treatment for bacterial STIs is not usually recommended for prepubertal children as the incidence of STIs after abuse is low, ascending infection is rare, and follow-up is more likely to take place than with adolescents or adults. [32]
Beyond the newborn period, diagnosis of an STI in children is highly suspicious for sexual abuse. [32]
Medical child abuse
Individuals who perpetrate medical child abuse usually have factitious disorder by proxy; this is covered separately in “Somatic symptom and related disorders.”
Definition
- Medical child abuse is a form of child maltreatment in which a caregiver fabricates and/or induces symptoms in a child, resulting in unwarranted and potentially harmful medical care. [35][36]
-
Symptoms may be:
- Induced by administering inappropriate drug therapy or other agents [35]
- Fabricated or exaggerated by contaminating samples (e.g., urine specimens) [35]
Clinical features [35]
- Signs and symptoms of induced illness, e.g.:
- Bleeding
- Neurological symptoms (e.g., seizures, CNS depression)
- Rashes
- Gastrointestinal symptoms (e.g., diarrhea, vomiting)
- Apnea
- Symptoms of urinary tract infection, hematuria
- Signs of infection (e.g., fever)
- Consequences of induced or fabricated illness, e.g.:
- Complications from procedures
- Mental health conditions
Red flags for medical child abuse [35]
- Medical history is inconsistent and/or history is incongruent with examination findings.
- Clinical findings that are unusual and occur in the presence of a single caregiver
- Reported history of unusual illnesses or deaths in other family members
- The caregiver is not relieved in response to reassurance that the child is healthy.
- Persistent requests for invasive diagnostics or treatments
- Conspicuously inadequate response to treatment for a particular condition
- Reported sensitivity to several substances or medications
Children with induced or fabricated illness often have a history of multisystem involvement and receive care from several specialists. [35]
Management [35]
- See “Approach to suspected child maltreatment.”
- Additional management in suspected medical abuse includes:
- Exclusion of medical causes of the symptoms [35]
- Referral of patients for a multidisciplinary evaluation, including CPS, mental health professionals, and child abuse specialists.
- See “Factitious disorder imposed on another” for details on DSM-5 diagnostic criteria and management of the perpetrator.
Victims of child medical abuse may be convinced by their perpetrator that they have a nonexistent illness. [35]
Prevention
- Educate all parents on the safe care of children (see “Anticipatory guidance for children”).
- Identify protective and risk factors for child maltreatment (e.g., through pediatric mental and social health screening).
- For patients with risk factors, offer interventions for the patient and/or family as indicated, e.g.: [30][37]
- Addressing social determinants of health
- Referring caregivers to psychosocial support services
- Referral for home visitation programs, where available
- Parenting programs focused on behavior and discipline
- Provide information on normal child development including age-appropriate behaviors to manage parent expectations.
- Discuss age-appropriate discipline as well as anger and conflict management techniques.
External Resources
- 2025 ACR Appropriateness Criteria: Suspected Physical Abuse-Child
- 2025 AAP Technical Report: Abusive Head Trauma in Infants and Children
- 2025 AAP Clincal Report: Evaluating Young Children with Fractures for Child Abuse
- 2024 AAP Clinical Report: The Pediatrician's Role in Preventing Child Maltreatment
- 2022 AAP Clinical Report: Evaluation for Bleeding Disorders in Suspected Child Abuse
References
- "Child Maltreatment 2023"
- Suniega EA, Krenek L, Stewart G. "Child Abuse: Approach and Management". Am Fam Physician. 105(5). :521-528. (2022)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Luken A, Nair R, Fix RL. "On Racial Disparities in Child Abuse Reports: Exploratory Mapping the 2018 NCANDS". Child Maltreat. 26(3). :267-281. (2021)
- Christian CW. "The Evaluation of Suspected Child Physical Abuse". Pediatrics. 135(5). (2015)
- Jenny C, Crawford-Jakubiak JE, et al. "The Evaluation of Children in the Primary Care Setting When Sexual Abuse Is Suspected". Pediatrics. 132(2). :e558-e567. (2013)
- Day PG, Woods SB, Gonzalez L, Fernandez-Criado R, Shakil A. "Validating the TeenHITSS to Assess Child Abuse in Adolescent Populations". Fam Med. 55(1). :12-19. (2023)
- Haney S, Scherl S, DiMeglio L, et al. "Evaluating Young Children With Fractures for Child Abuse: Clinical Report". Pediatrics. 155(2). (2025)
- Thackeray J, Livingston N, Ragavan MI, et al. "Intimate Partner Violence: Role of the Pediatrician". Pediatrics. 152(1). (2023)
- Anderst J, Carpenter SL, Abshire TC, et al. "Evaluation for Bleeding Disorders in Suspected Child Abuse". Pediatrics. 150(4). (2022)
- Choudhary AK, Servaes S, Slovis TL, et al. "Consensus statement on abusive head trauma in infants and young children". Pediatr Radiol. 48(8). :1048-1065. (2018)
- Blumenthal I. "Shaken baby syndrome". Postgrad Med J. 78(926). :732-735. (2002)
- Herman BE, Makoroff KL, Corneli HM. "Abusive Head Trauma". Pediatr Emerg Care. 27(1). :65-69. (2011)
- Narang SK, Haney S, Duhaime AC, et al. "Abusive Head Trauma in Infants and Children: Technical Report". Pediatrics. 155(3). (2025)
- Hsieh KLC, Zimmerman RA, Kao HW, Chen CY. "Revisiting Neuroimaging of Abusive Head Trauma in Infants and Young Children". AJR Am J Roentgenol. 204(5). :944-952. (2015)
- Mirsky D, Bardo D, Iyer R, et al. "ACR Appropriateness Criteria® Suspected Physical Abuse-Child: Update 2025". J Am Coll Radiol. (2026)
- Kavanagh EC. "The Reversal Sign". Radiology. 245(3). :914-915. (2007)
- Wright JN. "CNS Injuries in Abusive Head Trauma". AJR Am J Roentgenol. 208(5). :991-1001. (2017)
- Narang SK, Fingarson A, Lukefahr J, et al. "Abusive Head Trauma in Infants and Children". Pediatrics. 145(4). (2020)
- Stirling J, Gavril A, Brennan B, et al. "The Pediatrician’s Role in Preventing Child Maltreatment: Clinical Report". Pediatrics. 154(2). (2024)
- Barry MJ, Nicholson WK, et al. "Primary Care Interventions to Prevent Child Maltreatment". JAMA. 331(11). :951. (2024)
- Wootton-Gorges SL, Soares BP, Alazraki AL, et al. "ACR Appropriateness Criteria ® Suspected Physical Abuse—Child". J Am Coll Radiol. 14(5). :S338-S349. (2017)
- Collier ZJ, Roughton MC, Gottlieb LJ. "Negligent and Inflicted Burns in Children". Clin Plast Surg. 44(3). :467-477. (2017)
- Kos L, Shwayder T. "Cutaneous Manifestations of Child Abuse". Pediatr Dermatol. 23(4). :311-320. (2006)
- Vashi NA, Patzelt N, Wirya S, et al. "Dermatoses caused by cultural practices". J Am Acad Dermatol. 79(1). :1-16. (2018)
- "ACR–SPR Practice Parameter for the Performance and Interpretation of Skeletal Surveys in Children". https://web.archive.org/web/20260406175733/https://gravitas.acr.org/PPTS/DownloadPreviewDocument?ReleaseId=2&DocId=186. [2023-10-01]
- "Responding to children and adolescents who have been sexually abused: WHO clinical guidelines". https://web.archive.org/web/20250319003354/https://iris.who.int/bitstream/handle/10665/259270/9789241550147-eng.pdf?sequence=1. [2017-01-01]
- Kellogg ND. "Clinical Report—The Evaluation of Sexual Behaviors in Children". Pediatrics. 124(3). :992-998. (2009)
- Workowski KA, Bachmann LH, Chan PA, et al. "CDC Sexually Transmitted Infections Treatment Guidelines 2021". MMWR Recomm Rep. 70(4). :1-187. (2021)
- Romano ME. "Prepubertal Vulvovaginitis". Clin Obstet Gynecol. 63(3). :479-485. (2020)
- Crawford-Jakubiak JE, Alderman EM, Leventhal JM, et al. "Care of the Adolescent After an Acute Sexual Assault". Pediatrics. 139(3). (2017)
- Hibbard R, Barlow J, MacMillan H, et al. "Psychological Maltreatment". Pediatrics. 130(2). :372-378. (2012)
- Strathearn L, Giannotti M, Mills R, et al. "Long-term Cognitive, Psychological, and Health Outcomes Associated With Child Abuse and Neglect". Pediatrics. 146(4). (2020)
- Maguire SA, Williams B, Naughton AM, et al. "A systematic review of the emotional, behavioural and cognitive features exhibited by school‐aged children experiencing neglect or emotional abuse". Child Care Health Dev. 41(5). :641-653. (2015)
- Kairys S. "Child Abuse and Neglect". Pediatr Clin North Am. 67(2). :325-339. (2020)
- Flaherty EG, MacMillan HL, et al. "Caregiver-Fabricated Illness in a Child: A Manifestation of Child Maltreatment". Pediatrics. 132(3). :590-597. (2013)
- "Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR)"