Summary
Cholelithiasis refers to the presence of abnormal concretions (gallstones) in the gallbladder. About 10–20% of American adults have gallstones. Gallstones most commonly consist of cholesterol but may be pigmented (due to hemolysis or infection) or mixed. Cholelithiasis can manifest with biliary colic (postprandial RUQ pain) but is most commonly an incidental finding in asymptomatic individuals. The diagnosis is confirmed by ultrasound. Symptomatic cholelithiasis is managed with laparoscopic cholecystectomy.
See also “Choledocholithiasis,” “Acute cholecystitis,” and “Acute cholangitis.”
Overview


| Disorders caused by gallstones | ||||
|---|---|---|---|---|
| Cholelithiasis | Choledocholithiasis | Acute cholecystitis | Acute cholangitis | |
| Description |
|
|
|
|
| Mechanism |
|
|
|
|
| Clinical features |
|
|
|
|
| Laboratory findings |
|
|
|
|
| Diagnostic imaging |
|
|
|
|
| Treatment |
|
|
|
|
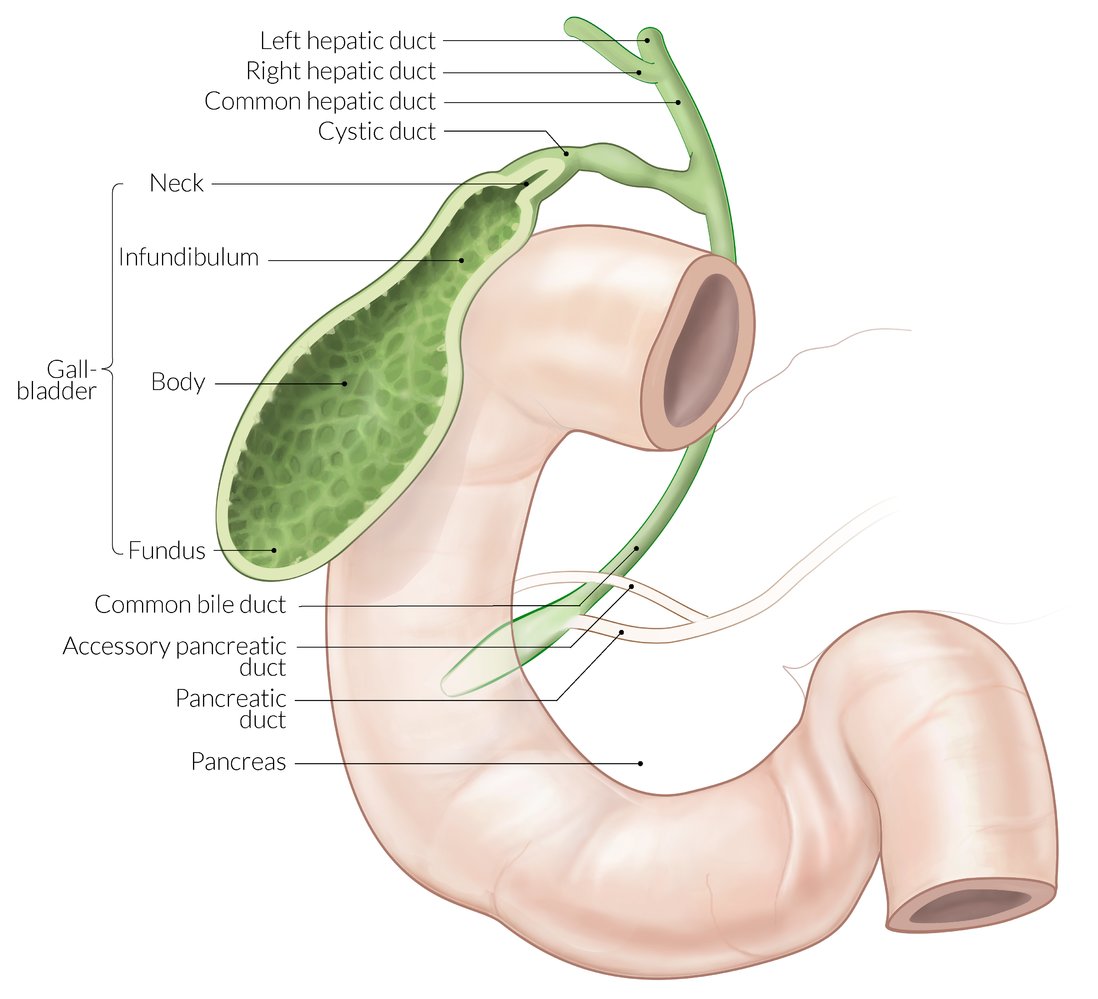
The right and left hepatic ducts join to form the common hepatic duct. The cystic duct joins the common hepatic duct to form the common bile duct. The main pancreatic duct drains into the common bile duct. The common bile duct opens into the descending part of the duodenum.
© AMBOSS
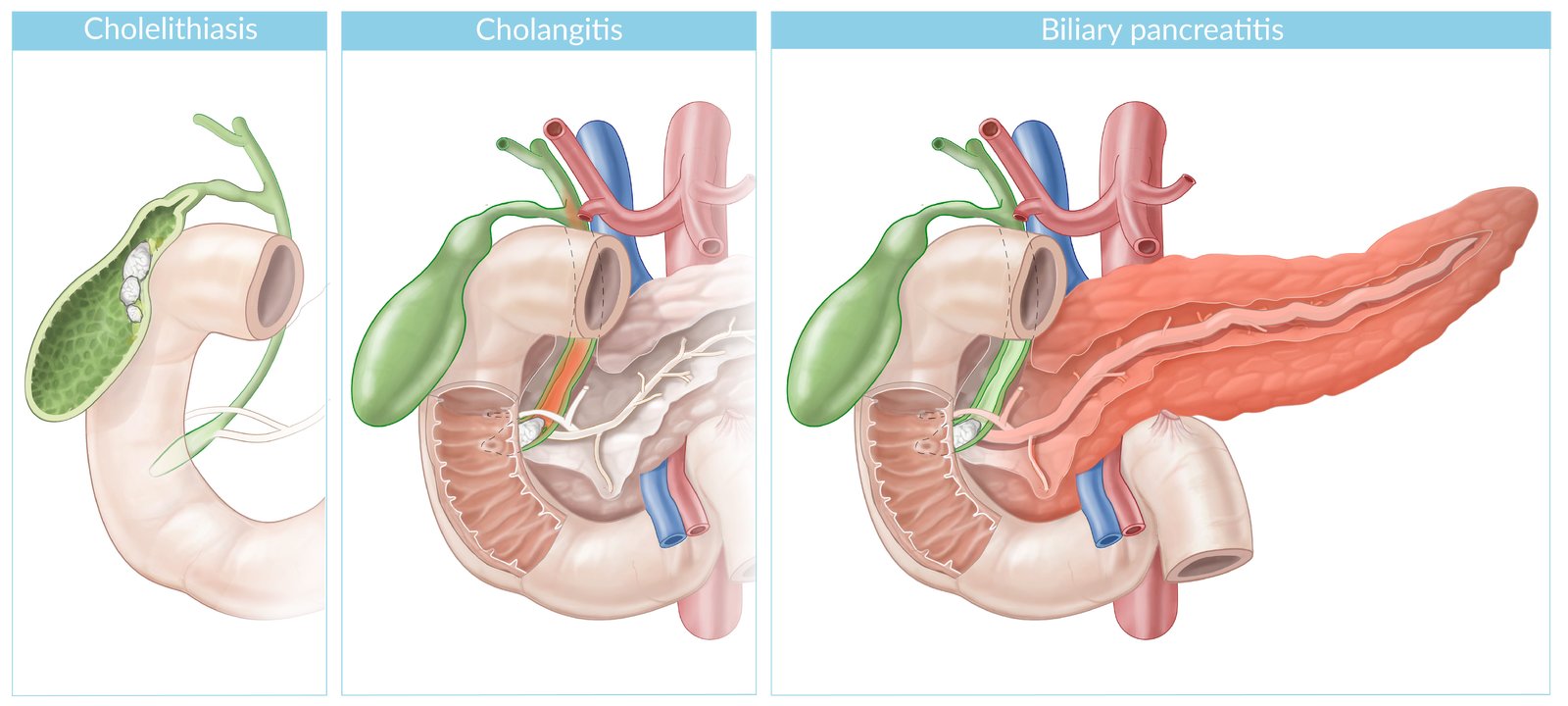
Cholelithiasis: the presence of gallstones within the gall bladder
Cholangitis: ascending biliary tract infection (orange shading) secondary to choledocholithiasis
Biliary pancreatitis: Pancreatic outflow obstruction secondary to choledocholithiasis allows for activation of pancreatic zymogens, resulting in pancreatic inflammation (orange shading).
© AMBOSS
Epidemiology
- Sex: ♀ > ♂ (2–3:1)
- Prevalence: approx. 10–20% of the adult population in developed countries
- Peak incidence: : > 40 years
References: [1][2]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
General
- Imbalance in bile salts, lecithin (stabilizer), cholesterol, calcium carbonate, and bilirubin
- Biliary stasis is a key component in gallstone formation.
- Impaired gallbladder emptying (e.g., due to bowel rest, prolonged total parenteral nutrition, pregnancy; ) → biliary sludge → bile stasis (cholestasis)
Cholesterol stones [1][2]
-
Risk factors
- Obesity, insulin resistance, dyslipidemia
-
Female sex
- Especially during reproductive years due to increased levels of estrogen and progesterone
- Increased estrogen levels cause increased secretion of bile rich in cholesterol, (lithogenic bile), which can result in the formation of cholesterol gallstones.
- Increased progesterone levels cause smooth muscle relaxation, decreased gallbladder contraction, and subsequent bile stasis with formation of gallstones.
- Multiparity or pregnancy
- Age (> 40 years of age)
- European, Native American, or Hispanic ancestry
- Family history
- Drugs: fibrates (inhibition of cholesterol 7-α hydroxylase), estrogen therapy, oral contraceptives
- Malabsorption (e.g., Crohn disease, ileal resection, cystic fibrosis)
- Rapid weight loss (e.g., after bariatric surgery)
- Pathophysiology: abnormal hepatic cholesterol metabolism → ↑ cholesterol concentration in bile and ↓ bile salts and lecithin → hypersaturated bile → precipitation of cholesterol and calcium carbonate → cholesterol stones or mixed stones
During pregnancy, increased estrogen levels cause increased secretion of lithogenic bile (rich in cholesterol), resulting in the formation of cholesterol gallstones. Increased progesterone levels cause smooth muscle relaxation, decreased and impaired gallbladder contraction, and subsequent bile stasis and formation of gallstones.
Rule of the 6 Fs: Fat, Female, Fertile, Forty, Fair-skinned, Family history.
Black pigment stones [2][3][4]
-
Risk factors
- Chronic hemolytic anemias (e.g., sickle cell disease, hereditary spherocytosis)
- (Alcoholic) cirrhosis
- Crohn disease
- Total parenteral nutrition
- Advanced age
- Pathophysiology: ↑ hemolysis → increase in circulating unconjugated bilirubin → increased uptake and conjugation of bilirubin → precipitation of bilirubin polymers and stone formation
Mixed/brown pigment stones [2][3][4][5]
- Risk factors: bacterial infections and parasites (e.g., Clonorchis sinensis, Opisthorchis species) in the biliary tract, sclerosing cholangitis [2]
- Pathophysiology: infection or infestation → release of β-glucuronidase (by injured hepatocytes and bacteria) → hydrolyzes conjugated bilirubin and lecithin in the bile → increased unconjugated bilirubin and fatty acids → precipitation of calcium carbonate, cholesterol, and calcium bilirubinate (dark color) in bile



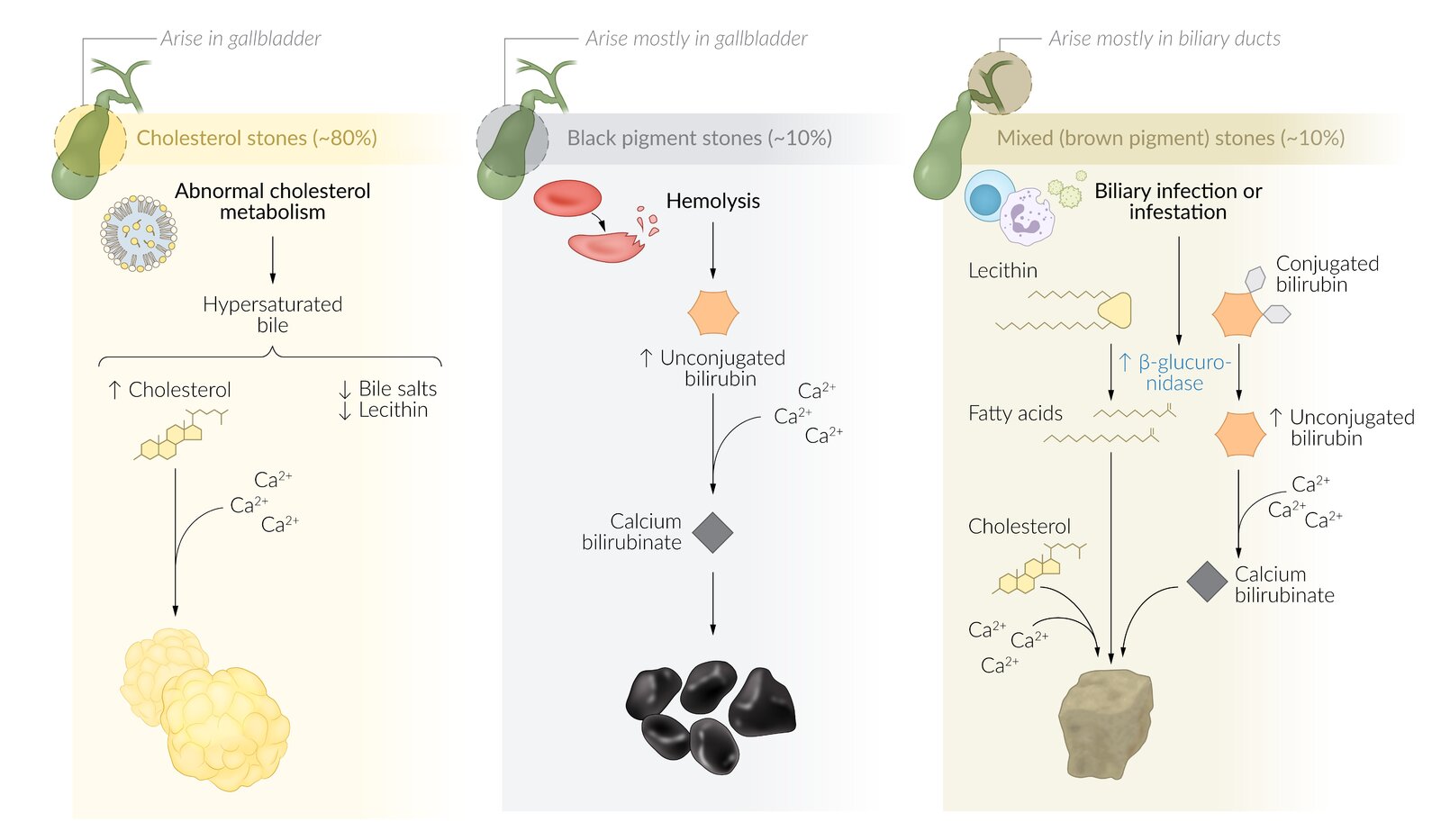
Cholesterol stones arise only in the gallbladder but can be transported into the cystic duct as well as the common bile duct and cause obstruction and stasis.
Pigmented gallstones contain varying amounts of calcium bilirubinate and can arise anywhere in the biliary tree. Black pigment stones arise mostly in the gallbladder (due to increased hemolysis; e.g., in sickle cell disease), whereas brown pigment stones typically arise in inflamed portions of the biliary duct (e.g., due to bacterial or parasitic infections).
© AMBOSS
© AMBOSS

The two larger gallstones in the neck of the gallbladder have an irregular consistency and yellowish-white to dark pigmentation, which indicates a high level of cholesterol. The stones located in the body and fundus are significantly smaller, darkly pigmented, and of different shapes, which is more suggestive of pigment stones due to bilirubin precipitation.
Source: “Gallstones” by Emmanuelm, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Clinical features
- Most gallstones are asymptomatic.
-
Biliary colic: constant, dull RUQ pain lasting < 6 hours
- Especially postprandial: vagal stimulation (e.g., cholecystokinin release following a fatty meal) → gallbladder contraction → attempts to force the stone into the cystic duct
- May radiate to the epigastrium, right shoulder, and back (referred pain)
- Nonspecific symptoms
- Nausea, vomiting, early satiety
- Bloating, dyspepsia
- Complications of cholelithiasis can be the first manifestation of gallstone disease.
Only a minority of patients with gallstones are symptomatic!
Diagnosis
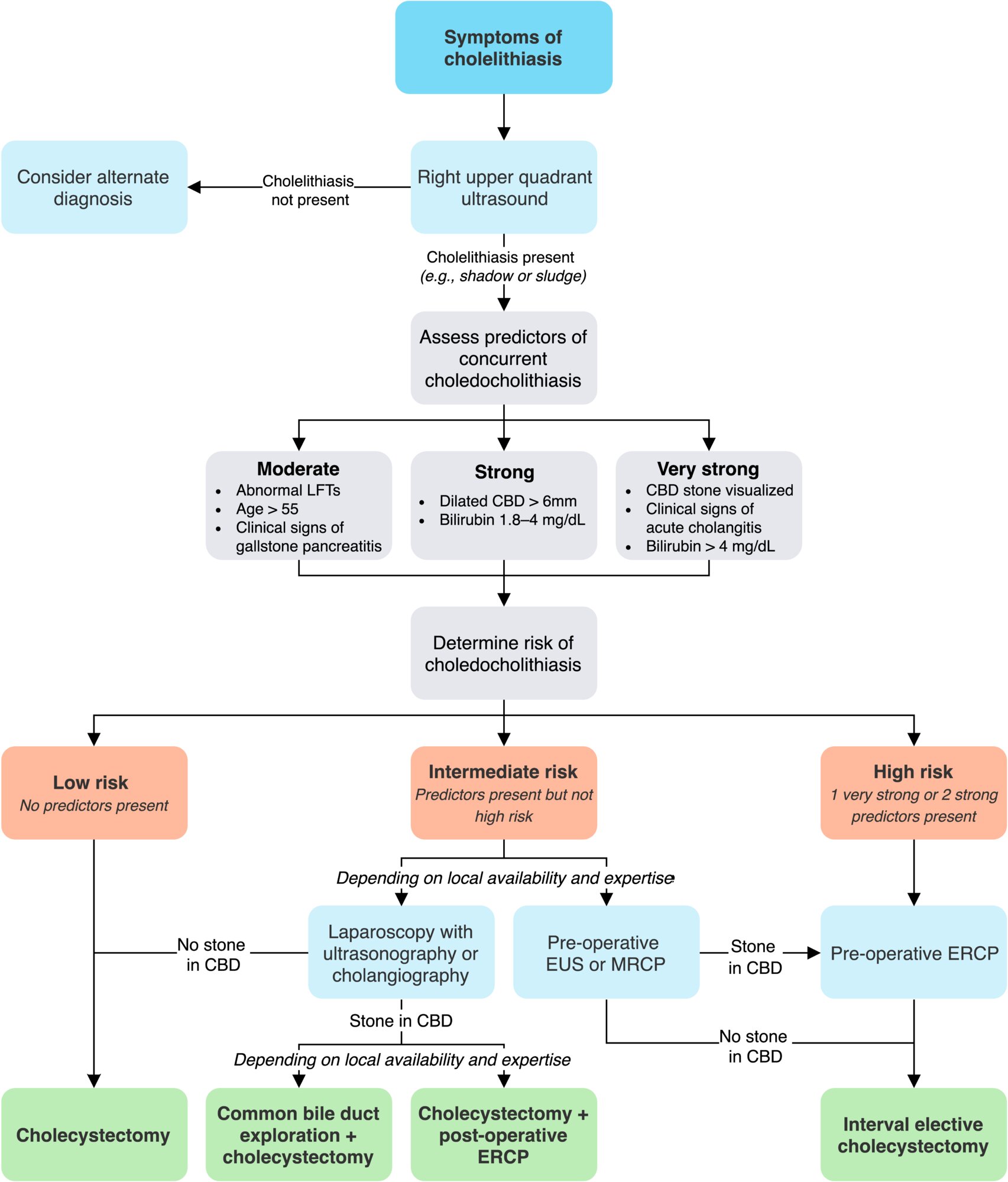
Approach [2]
See “Cholelithiasis in pregnancy” for considerations in pregnant individuals.
- Asymptomatic cholelithiasis : No diagnostic workup is required.
-
Suspected symptomatic cholelithiasis
- Obtain imaging for cholelithiasis: biliary point-of-care ultrasound (POCUS) or transabdominal RUQ ultrasound
- Rule out complications of cholelithiasis (e.g., acute cholecystitis or choledocholithiasis).
- If the diagnosis remains unclear: See “Diagnosis of acute abdominal pain.”

Laboratory studies for suspected cholelithiasis
Laboratory studies are typically normal in uncomplicated cholelithiasis but should be ordered to rule out other acute biliary conditions and/or other causes of acute abdominal pain.
- CBC: usually normal
- LFTs: usually normal
- Amylase, lipase: usually normal
Laboratory studies (e.g., WBC count, LFTs, lipase, amylase) are usually normal in uncomplicated cholelithiasis.
RUQ ultrasound for suspected cholelithiasis
If appropriately trained, consider performing a biliary POCUS.
- Indication: best initial test in suspected symptomatic cholelithiasis [6][7]
-
Characteristic findings [6]
- Cholelithiasis [8]
- Intraluminal highly echogenic foci
- Strong posterior acoustic shadowing
- Rolling stone sign: movement of the echogenic foci with the changing of patient posture
-
Biliary sludge [9][10][11]
- Low-level echogenic material in the dependent portion of the GB
- No posterior acoustic shadowing
- Slow movement with the changing of patient posture
- Cholelithiasis [8]
-
Accuracy: operator- and technique-dependent [12]
- RUQ ultrasound performed by a radiologist: ≥ 95% sensitivity and specificity for cholelithiasis
- Biliary POCUS performed by emergency providers: ∼ 90% sensitivity and specificity for cholelithiasis
If appropriately trained, consider performing a biliary POCUS to rule in cholelithiasis. If the study is negative, further investigations (e.g., laboratory studies, RUQ ultrasound performed by a radiologist, additional imaging) may be necessary. [12]





Additional imaging studies
Additional imaging may be required if complications of cholelithiasis (e.g., acute cholecystitis, acute cholangitis, choledocholithiasis, biliary pancreatitis) cannot be ruled out, or to evaluate for other causes of abdominal pain.
MRI abdomen without and with IV contrast with MRCP [6]
-
Indications
- Preferred second-line test if ultrasound findings are inconclusive
- Suspected choledocholithiasis (see ''Diagnostics'' in choledocholithiasis for further details)
- Supportive findings: well-defined hypointense (on T2) filling defect(s) within the gallbladder lumen [13]
CT abdomen with IV contrast [6]
-
Indications
- Inconclusive ultrasound findings; MRI is not available
- Suspected complications and/or differential diagnoses
- Preoperative planning after confirming the diagnosis
- Supportive findings (of radiopaque stones): well-defined hyperdense structure(s) within the gallbladder lumen
-
Disadvantages
- Only radiopaque stones are detectable (15–20% of stones are radiopaque). [14][15]
- Cannot detect the more common radiolucent pure cholesterol stones

Abdominal x-ray
- Indication: usually not indicated in the evaluation of cholelithiasis, but may be performed as part of the workup of acute abdominal pain
- Findings: gallstones with an outer radiopaque rim and radiolucent center [16]
- Disadvantages: similar to those of CT scan

X-ray and CT scan are rarely diagnostic in cholelithiasis because only 15–20% of stones are radiopaque. Pure cholesterol stones are radiolucent.
© AMBOSS
© AMBOSS
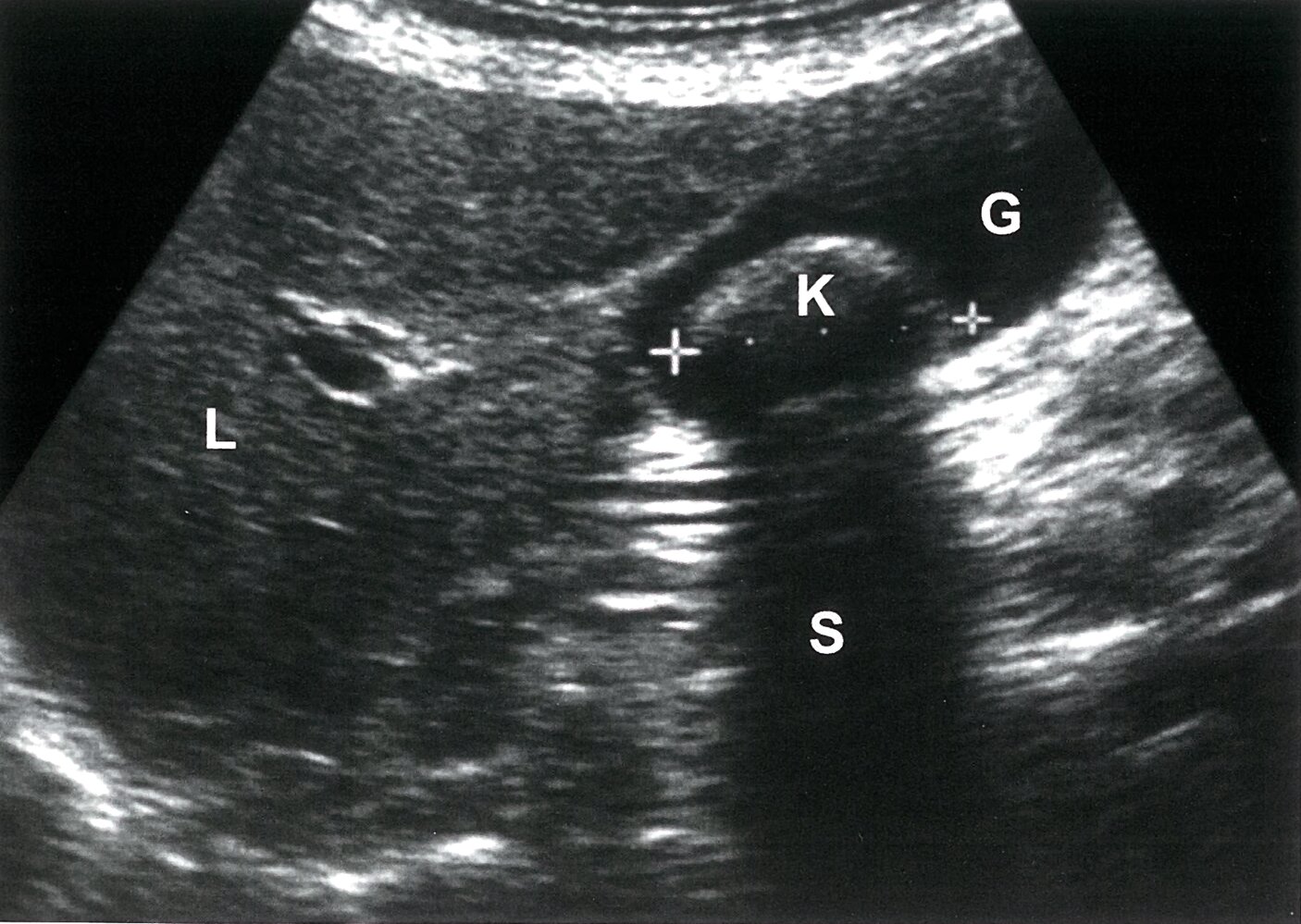
Ultrasound right upper quadrant (oblique plane)
A solitary calculus (K) in the dependent gallbladder (G) has a reflective anterior surface (green overlay) and casts a posterior acoustic shadow (S; green hatched overlay).
Characteristic ultrasound findings of cholelithiasis include a reflective anterior surface, marked posterior acoustic shadowing, and movement during repositioning of the patient.
L: liver
Source: © IMPP

Transabdominal ultrasound (right upper quadrant)
Several well-defined, hyperechoic structures varying in size and shape (green overlay) are visible in the infundibulum and proximal body of the gallbladder (G). These structures are obstructing the passage of the ultrasound waves, resulting in posterior acoustic shadowing (hypoechoic area; hatched green overlay).
Hyperechoic intraluminal structures casting a posterior acoustic shadow are characteristic features of cholelithiasis.
L: liver
© AMBOSS

Ultrasound gallbladder (longitudinal plane)
Acoustic enhancement (green overlay) is seen distal to the gallbladder except where multiple small dependent hyperechoic calculi (yellow overlay) reflect the ultrasound beam and cast an acoustic shadow (green hatched overlay). Biliary sludge (yellow hatched overlay) is slightly hyperechoic compared to anechoic bile. The gallbladder wall is thickened (normal size: 1–2 mm) and has a layered appearance (red overlay), with central hypoechoic edema.
These findings in a patient with typical clinical features of RUQ pain strongly indicate acute calculous cholecystitis. Additional findings that would support a diagnosis of cholecystitis include an obstructing calculus, positive Murphy sign, pericholecystic fluid, gallbladder dilatation, and hyperemia of the gallbladder wall on color Doppler.
G: gallbladder; L: liver
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
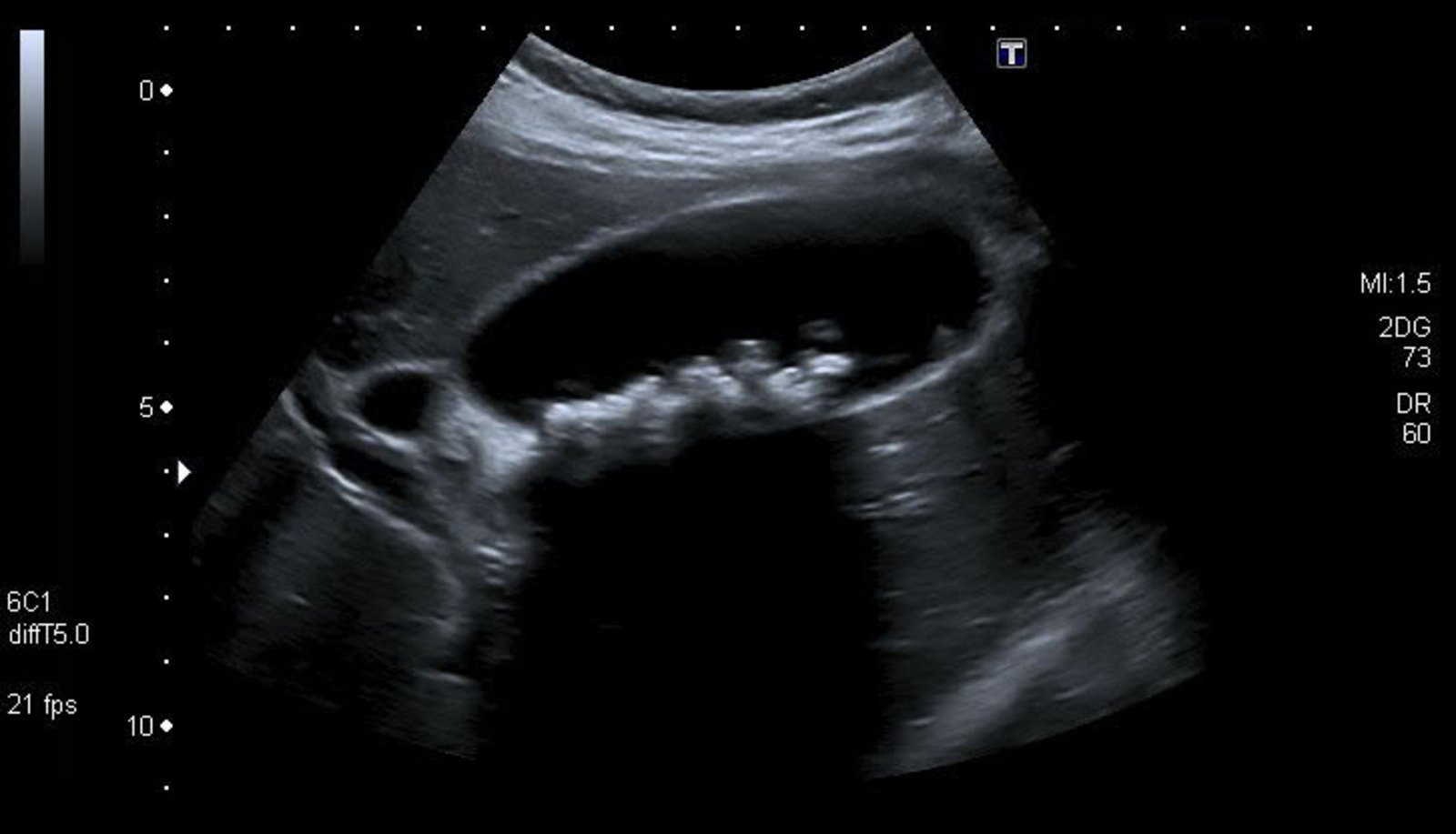
Ultrasound gallbladder (longitudinal plane)
Several dependent hyperechoic structures (green overlay) in the gallbladder lumen (G) absorb a portion of the ultrasound beam (dashed white line), resulting in posterior acoustic shadowing (hatched green overlay).
Gallbladder calculi are characteristically seen as mobile dependent hyperechoic intraluminal structures that produce acoustic shadowing. Shadowing is dependent on stone size, but independent of stone composition, calcium content, and shape.
L: liver; green outline: gallbladder wall
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Click on the overlay icon below the taskbar on the left to toggle the overlay on and off.
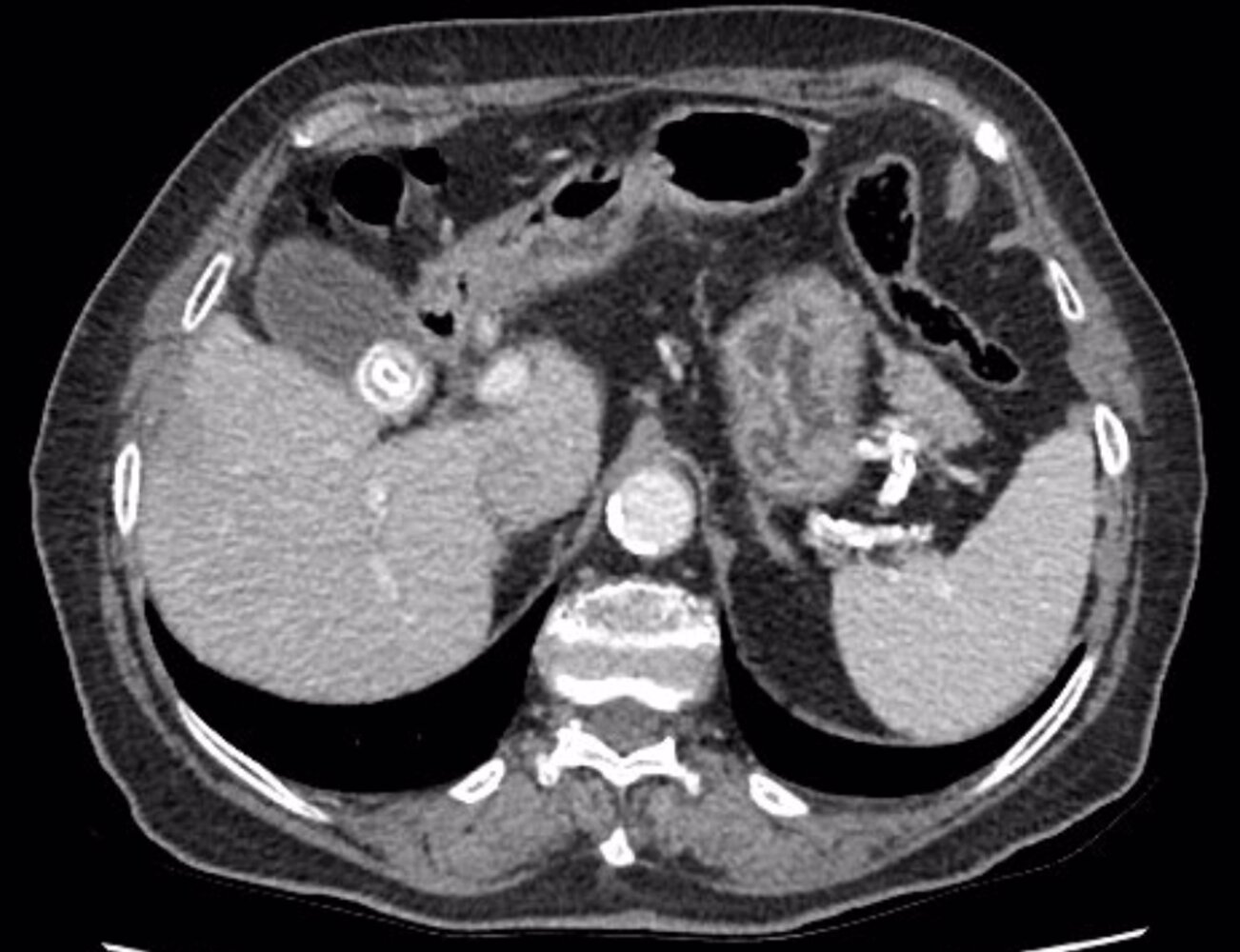
CT abdomen (with contrast; axial and coronal planes)
A laminated calcified calculus (red overlay) is present in the dilated gallbladder (green overlay), and a smaller calculus (yellow arrowhead) is seen in the distal common bile duct (blue overlay). A small gas-filled duodenal diverticulum (white arrowhead) is visible adjacent to the common bile duct calculus.
A cystic left ovarian lesion (yellow overlay) and numerous colonic diverticula (examples indicated by red arrowheads) are seen. There is extensive atherosclerotic calcification of the aorta (examples indicated by green arrowheads), coronary arteries, and several other arteries. A few subcentimeter hypodense lesions seen in the liver are likely cysts, and there is a small hiatal hernia.
Image source of original image: Radiologie Frechen-Erftstadt. Original title: “Cholecystolithiasis and choledocholithiasis”. Created by: Markus Le Blanc.
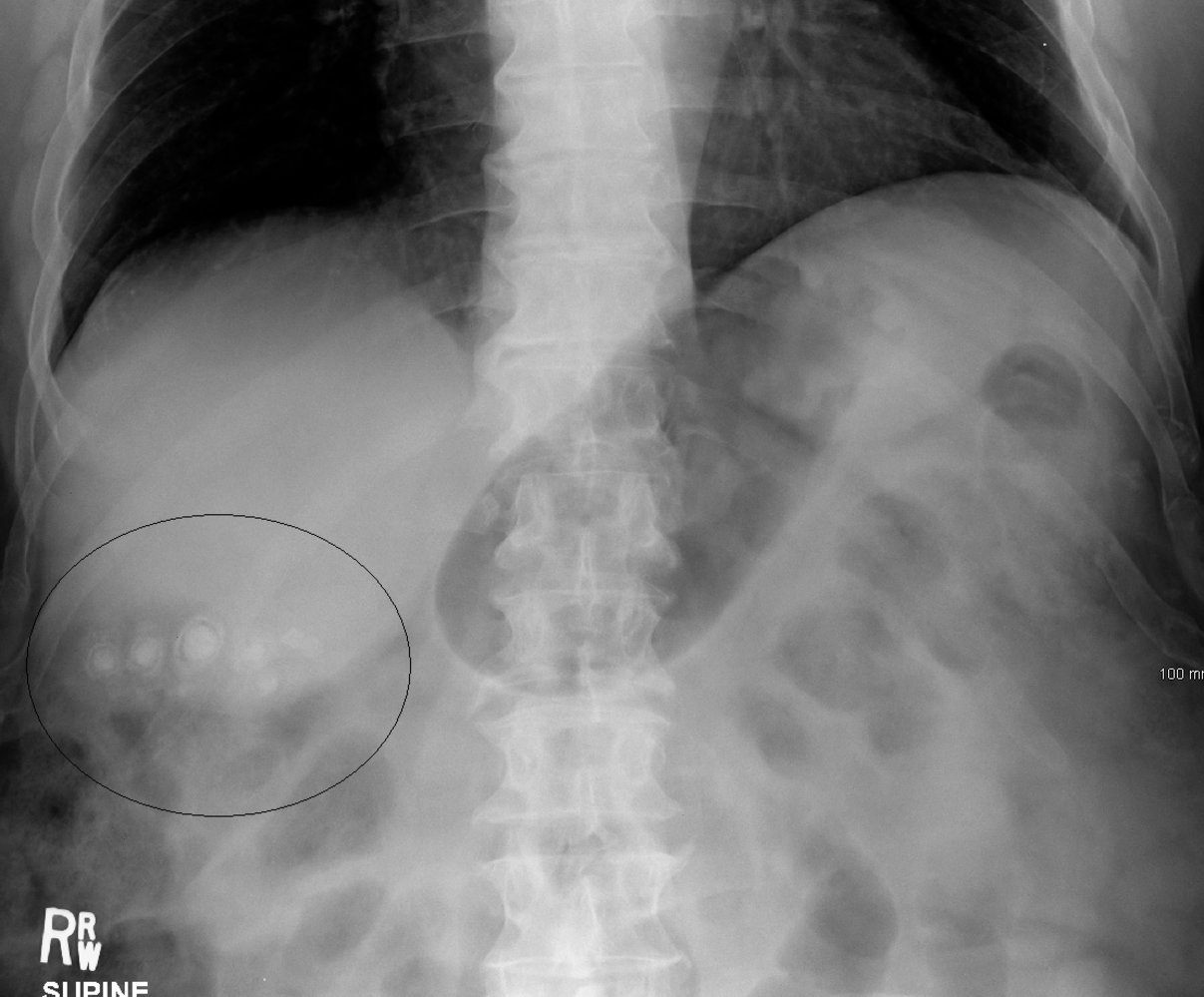
X-ray abdomen (AP view; supine position)
Multiple rounded calcified structures are visible in the right upper quadrant (black circle). Many have a laminated appearance, with a dense central calcification (green) surrounded by an inner lucent ring and outer calcified ring (white outline).
Pure cholesterol stones, the most common type of gallstone, are radiolucent on abdominal radiographs. Black pigment and mixed gallstones may contain sufficient calcium to be radiopaque.
Source: “StonesXray” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Differential diagnoses
Differential diagnosis of RUQ pain
- Abdominal (See also “Acute abdominal pain” and “Differential diagnosis of abdominal pain.”)
- Choledocholithiasis
- Acute cholecystitis
- Acute cholangitis
- Acute hepatic capsule swelling (e.g., acute hepatitis, perihepatitis, congestive hepatopathy)
- Gastroesophageal reflux, gastritis, gastrointestinal ulcers
- Early appendicitis
- Acute pancreatitis
- Right-sided diverticulitis
- Sphincter of Oddi dysfunction
-
Extra-abdominal
- Nephrolithiasis
- Acute coronary syndrome (See also “Chest pain.”)
- See also “Differential diagnosis of acute abdomen.”
Differential diagnoses of intraluminal gallbladder wall pathology
- Cholangiocarcinoma
- Gallbladder polyp
The differential diagnoses listed here are not exhaustive.
Treatment
Approach [2][17][18][19]
See “Cholelithiasis in pregnancy” for considerations in pregnant individuals.
-
Asymptomatic cholelithiasis
- Expectant management is typically sufficient.
- Consider the need for prophylactic cholecystectomy: See “Indications” in “Surgical Management.”
- Patients with gallstones found incidentally during an ED visit can be referred back to their primary care physician for shared decision-making regarding surgical consult.
-
Symptomatic uncomplicated cholelithiasis
-
Treatment of biliary colic
- Provide initial supportive therapy for acute biliary disease.
- Counsel on lifestyle modifications to prevent further attacks (see “Nonoperative management of cholelithiasis” for details.)
- Outpatient referral to general surgery for an elective cholecystectomy to prevent recurrence.
- Consider surgical consult and admission if the pain is intractable.
-
Treatment of biliary colic
-
Symptomatic complicated cholelithiasis
- Admit for further management and consult general surgery and/or gastroenterology.
- See “Acute cholecystitis,” “Acute cholangitis,” “Choledocholithiasis,” and “Biliary pancreatitis.”
Initial supportive therapy of acute biliary disease [17][19]
-
Bowel rest: NPO
- In biliary colic: until the pain subsides (typically within a few hours) [17]
- In other acute biliary conditions: The duration of NPO depends on the need for urgent interventional therapy
-
Analgesics [2]
-
NSAIDs: preferred first-line analgesics [2][20][21]
- Ketorolac
- Diclofenac
- Ibuprofen
-
Opioids: for severe pain that does not improve with NSAIDs or in patients with contraindications to NSAIDs [2][22]
- Morphine
- Buprenorphine [2][23]
- Meperidine [24][25]
- See also “Pain management.”
-
NSAIDs: preferred first-line analgesics [2][20][21]
- Spasmolytics (e.g., dicyclomine ): consider as adjuvant therapy with analgesics in patients with severe pain [2][17]
-
Treatment for protracted vomiting
- IV fluid therapy
- Antiemetics
- Consider NG tube insertion with suction.
Surgical management
- Procedure: elective laparoscopic cholecystectomy
-
Indications
- Symptomatic cholelithiasis
-
Asymptomatic cholelithiasis with any of the following:
- Increased risk of gallbladder cancer (e.g., gallbladder polyps, porcelain gallbladder, gallstones ≥ 3 cm) [2][17][26]
- Increased risk of developing complications (e.g., immunocompromised patients, multiple gallstones) [17][18]
- Increased risk of becoming symptomatic (e.g., hemolytic anemia, patients undergoing gastric bypass surgery) [17][27][28]
- Contraindication: suspected gallbladder cancer (see ''Treatment'' in “Biliary cancer”) [18][29]
- Preoperative precautions: Assess for predictors of choledocholithiasis in all symptomatic patients (see ''Diagnosis of choledocholithiasis”). [30]
- Timing: as early as possible in uncomplicated symptomatic cholelithiasis [2][31][32]
- Complications: See “Complications of cholecystectomy”.
Cholecystectomy is usually not indicated in asymptomatic cholelithiasis.
Nonoperative management of cholelithiasis [2]
Indications
- Patients at high risk of complications due to surgery or anesthesia (e.g., recent myocardial infarction)
- Patients unwilling to undergo surgery
Expectant management [17]
-
Lifestyle modifications :
- Low-fat diet (especially low in saturated fats) [33]
- Avoid lithogenic drugs, such as estrogen, fibrates. [34]
- Exercise regularly.
- Follow-up: if symptoms recur
Oral bile acid dissolution therapy
- May be useful in dissolving pure cholesterol stones (i.e., radiolucent stones) that are < 0.5 cm [17]
- Ursodeoxycholic acid (off-label)
- Duration of therapy: 6–24 months [17][33]
- Advantage: symptomatic improvement even if stones are not completely dissolved [33]
-
Disadvantages
- Ineffective in mixed stones
- High recurrence rates [2]
- Long duration of therapy
- Requires repeat imaging to track treatment response
Extracorporeal shock wave lithotripsy (ESWL)
ESWL is also used in the treatment of nephrolithiasis.
- Definition: : a noninvasive method of stone fragmentation using an acoustic pulse in the treatment of gallstones and pancreatic stones
- Indication: typically used for solitary stones that can be localized well on imaging (radiolucent)
-
Procedure
- Stones are localized using x-ray or ultrasound.
- A lithotriptor generates shock waves that are focused on the stone, fragmenting it in the process.
- Passage of stone fragments
- Biliary stones: through the biliary system into the duodenum.
- Pancreatic stones: through the pancreatic duct into the duodenum
- Advantage: is noninvasive: and can be performed on an outpatient basis [2]
-
Disadvantages
- Commonly causes biliary colic
- Lower success rate in the presence of multiple stones
- Risk of injury to adjacent solid organs (rare)
- Prognosis: high recurrence rate (between 40 and 60% within 5 years) [35][36]
ESWL is contraindicated in pregnancy. [37]
© AMBOSS
Acute management checklist
- Keep patient NPO.
- Provide initial supportive therapy for acute biliary disease (e.g., analgesia, IV fluids, antiemetics).
- Obtain RUQ ultrasound or perform biliary POCUS if available.
- Identify and manage complications of cholelithiasis (e.g., acute cholecystitis, acute cholangitis, choledocholithiasis, biliary pancreatitis).
- Refer to general surgery for an elective cholecystectomy to prevent recurrence.
Special patient groups
Cholelithiasis in pregnancy [38][39]
- Cholelithiasis affects 12% of pregnant individuals. [40][41]
- Incidentally detected cholelithiasis in asymptomatic individuals does not require further evaluation or management.
- Symptomatic cholelithiasis manifests similarly in pregnant and nonpregnant individuals.
- Additional differential diagnoses of cholelithiasis to consider in pregnant individuals include:
- HELLP syndrome (hemolysis, elevated liver enzymes, low platelets)
- Acute fatty liver of pregnancy
- Intrahepatic cholestasis of pregnancy
Diagnostics [38][39]
The diagnostic approach for cholelithiasis during pregnancy is similar to that for nonpregnant individuals, with the following additional considerations for imaging modalities.
- Preferred initial imaging modality: RUQ ultrasonography
- Diagnostic uncertainty: MRI without contrast [41][42][43]
- Suspected choledocholithiasis: MRCP or endoscopic ultrasound (in consultation with a specialist) [38]
ALP levels can be elevated in pregnant individuals who do not have biliary disease because of placental ALP production. [44]
Management of symptomatic cholelithiasis in pregnancy [39][44]
- Admit to the hospital for monitoring. [39]
- Provide initial supportive management of acute biliary disease as in nonpregnant patients, but avoid NSAIDs.
- Consult surgery for consideration of operative versus nonoperative management of cholelithiasis; use shared-decision making. [45]
- Laparoscopic cholecystectomy may be preferred over conservative management. [38][39][45]
- Consider corticosteroids to induce fetal lung maturity if indicated. [46]
- Assess for risk factors for venous thromboembolism and provide appropriate VTE prophylaxis. [46]
- For management of complications, see also “Acute pancreatitis during pregnancy” and “Acute cholecystitis in pregnancy.”
Do not delay emergency surgery (e.g., for complicated cholelithiasis) during pregnancy, regardless of the trimester. [45][46]
ERCP during pregnancy may be considered for the management of cholelithiasis complications (e.g., acute biliary pancreatitis, choledocholithiasis) if the benefits outweigh the risks of post-ERCP pancreatitis and fetal radiation exposure. [38]
Complications
General
-
Cholecystitis
- Acute cholecystitis (most common)
- Chronic cholecystitis
- Porcelain gallbladder
- Choledocholithiasis
- Acute cholangitis
- Acute biliary pancreatitis
- Biliary-enteric fistula: Cholecystoenteric/choledochoenteric fistula (rare) , which can cause gallstone ileus (rare) [47][48]



Complications due to gallstone impaction at the gallbladder neck or infundibulum
Mirizzi syndrome [49][50]
- Definition: extrinsic compression of the common bile duct (or any extrahepatic bile duct) by gallstone(s) impacted in the cystic duct or the infundibulum of the gallbladder [49][51]
- Clinical features: similar to choledocholithiasis
-
Diagnostics: preferably ERCP/MRCP
- Narrowing of the common hepatic duct
- Stone within the cystic duct
- Dilation of the intrahepatic biliary tree
-
Treatment
- ERCP-guided CBD stent placement may be considered preoperatively to allow for biliary drainage. [52]
- Open cholecystectomy may be preferred if diagnosed preoperatively. [50]
-
Complications [53][54]
- Cholecystocholedochal fistula: an abnormal communication between the gallbladder and the common bile duct
- Cholecystoenteric/choledochoenteric fistula (biliary-enteric fistula): an abnormal communication between the gallbladder or the CBD with the adjacent bowel
- Gallstone ileus: due to biliary-enteric fistula
Gallbladder mucocele (gallbladder hydrops) [47][55]
- Definition: marked distention of the gallbladder with sterile mucinous content due to chronic biliary outflow obstruction
-
Etiology [55]
- Impacted gallstone at the gallbladder neck (most common)
- Resolved acute cholecystitis [47]
- Tumors at the gallbladder neck or CBD (e.g., GB polyps, cholangiocarcinoma, carcinoma of pancreatic head)
- Acute inflammatory conditions (e.g., Kawasaki disease)
- Extrinsic compression of the biliary outflow tract (e.g., lymphadenopathy, adhesions, strictures)
- Pathophysiology: chronic biliary outflow obstruction → resorption of bile and secretion of mucin by biliary mucosa → collection of mucinous secretion within the gallbladder with no outflow → gross distention of the gallbladder
- Clinical features: asymptomatic mass in the RUQ; no signs of infection
- Diagnostics: (preferably ultrasound or CT); show grossly distended fluid-filled gall bladder without signs of inflammation [55]
-
Treatment
- In children with no evidence of cholecystitis: trial of conservative management [56]
- In adults: laparoscopic cholecystectomy [55]


We list the most important complications. The selection is not exhaustive.
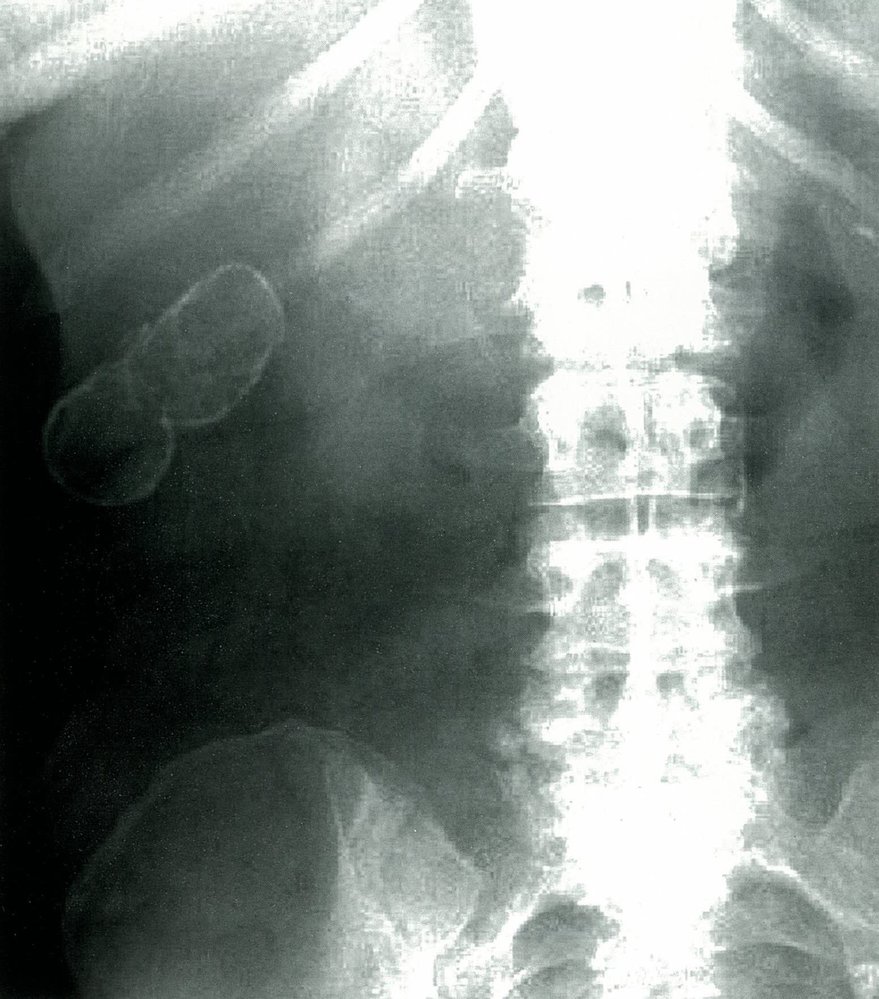
X-ray abdomen (AP view)
A well-defined oval lesion is visible in the right upper quadrant of the abdomen, encapsulated in a thin rim of radiodense material, indicating intramural calcification of the gallbladder.
This is the typical appearance of porcelain gallbladder, which is a consequence of chronic gallbladder inflammation that is usually secondary to cholelithiasis.
Source: © IMPP

Ultrasound right upper quadrant (left: portal vein and common bile duct; right: gallbladder) of a patient with elevated liver enzymes
The left image shows normal directional blood flow within the portal vein (red) and a dilated common bile duct (CBD) with a diameter of 0.94 cm. The right image shows marked posterior shadowing (indicated by dashed lines) and deep to hyperechoic areas of calcification (yellow overlay) along the anterior gallbladder wall. Additional small hyperechoic areas (indicated by arrowheads) at the posterior right aspect of the image in the region of the gallbladder also proved to be wall calcifications on CT (not shown).
A hyperechoic gallbladder wall with posterior acoustic shadowing is seen with porcelain gallbladder. The appearance should be distinguished from a gallbladder filled with calculi, which produces the wall-echo-shadow sign.
Source: “Fig. 2 and 3, in: A Case Report on Detecting Porcelain Gallbladder form Wall-Echo-Shadow Sign on Point-of-Care Ultrasound” by Fares Al-Khouja; Proma Mazumde; John Moeller, JETem, licensed under CC BY 4.0. Modifications: - image is a product of two separate images - arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

CT abdomen (with IV contrast; coronal plane)
Calculi are visible as hyperdense structures (green overlay) in the distal common bile duct (CBD). The CBD is dilated as a result of obstruction, and the distal duct shows inflammatory thickening (arrowheads).
GB: gallbladder; red overlay: gallbladder calculi
Source: “2 of 2, in: Choledocholithiasis” by Peña J, Journal of Education & Teaching in Emergency Medicine, licensed under CC BY 4.0. Modifications: arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS). Further notes: Images courtesy of JETem.org
Cholelithiasis: the presence of gallstones within the gall bladder
Cholangitis: ascending biliary tract infection (orange shading) secondary to choledocholithiasis
Biliary pancreatitis: Pancreatic outflow obstruction secondary to choledocholithiasis allows for activation of pancreatic zymogens, resulting in pancreatic inflammation (orange shading).
© AMBOSS
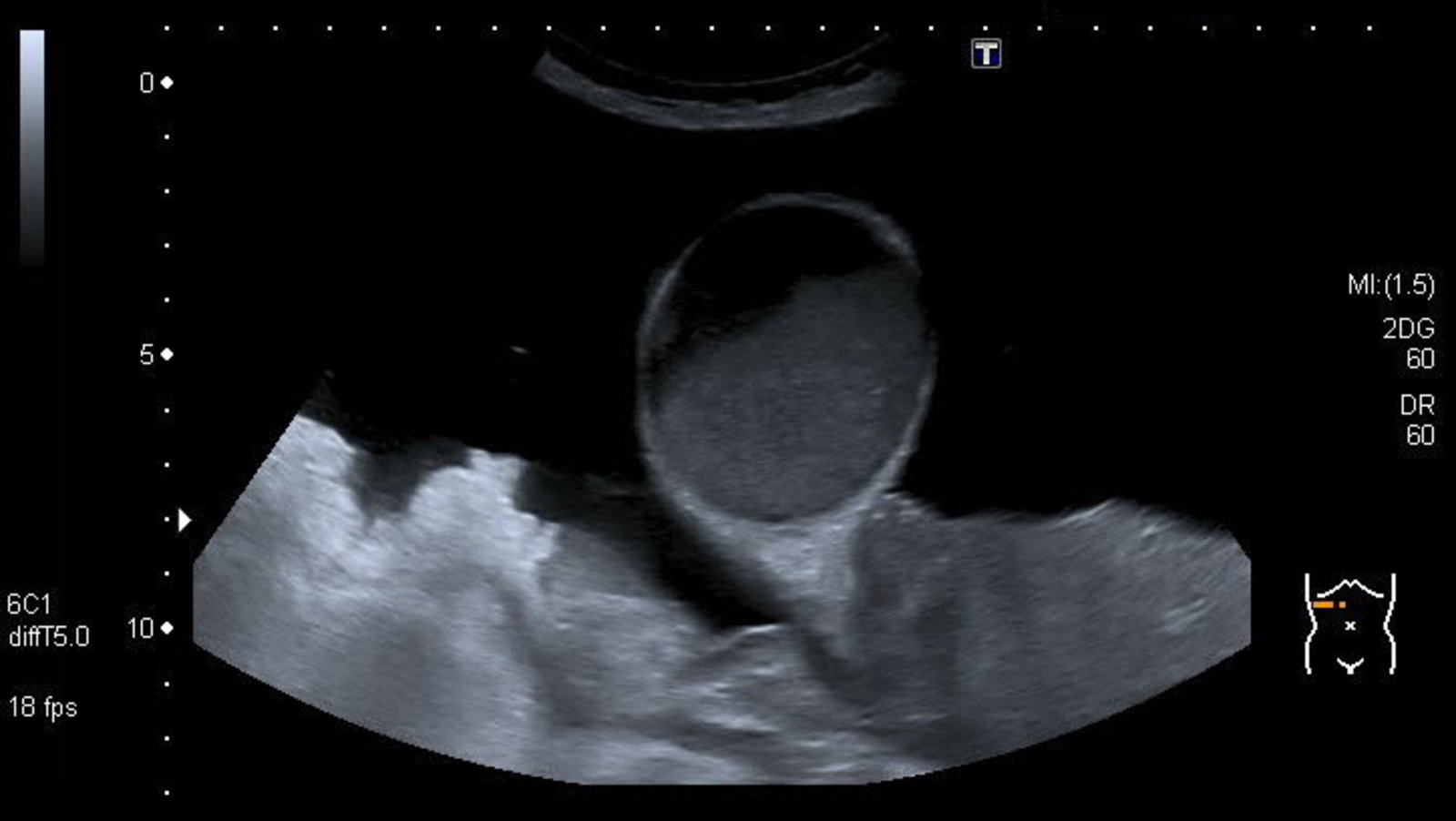
Ultrasound abdomen (right upper quadrant; transverse plane)
The gallbladder (G; green outline) is grossly distended and filled with a heteroechoic fluid (yellow overlay) as evidenced by the fluid meniscus.
These findings in a patient with an asymptomatic right upper quadrant mass are characteristic of a gallbladder mucocele.
L: liver (which appears cirrhotic); A: ascites
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.

Ultrasound abdomen (right upper quadrant; longitudinal plane)
The gallbladder (green outline) appears grossly distended and filled with a heteroechoic fluid (yellow overlay) as evidenced by the fluid meniscus. Multiple small concretions (arrowheads) are visible within the fluid.
These findings in a patient with an asymptomatic right upper quadrant mass are characteristic of a gallbladder mucocele.
In this patient, carcinoma of the pancreatic head had obstructed biliary outflow, resulting in the gallbladder mucocele (which manifested as Courvoisier sign) and ascites due to peritoneal carcinomatosis.
L: liver; K: kidney; In: intestine; A: ascites
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
External Resources
- 2024 AGA Clinical Practice Update on Pregnancy-Related Gastrointestinal and Liver Disease.
- 2021 ACOG Guide to Upper Gastrointestinal Tract, Biliary, and Pancreatic Disorders
- 2019 ASGE Guideline on the Role of Endoscopy in the Evaluation and Management of Choledocholithiasis
- 2018 AAST Emergency General Surgery Guideline Summaries: Acute Appendicitis, Acute Cholecystitis, Acute Diverticulitis, Acute Pancreatitis, and Small Bowel Obstruction
- 2017 American College of Gastroenterology Clinical Guideline on Liver Disease and Pregnancy
- 2016 EASL Clinical Practice Guidelines on the Prevention, Diagnosis and Treatment of Gallstones
- 2016 JSG Clinical Practice Guidelines for Cholelithiasis
- 2013 ACG Guideline for Management of Acute Pancreatitis
References
- Lack EE. "Pathology of the Pancreas, Gallbladder, Extrahepatic Biliary Tract, and Ampullary Region ". Oxford University Press. (2003). ISBN: 0195133927
- European Association for the Study of the Liver (EASL). "EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones.". J Hepatol. 65(1). :146-181. (2016)
- Bouchier IA. "The formation of gallstones.". Keio J Med. 41(1). :1-5. (1992)
- Goljan EF. "Rapid Review Pathology". Elsevier Saunders. (2018). ISBN: 9780323476683
- Stinton LM, Shaffer EA. "Epidemiology of gallbladder disease: cholelithiasis and cancer". Gut Liver. 6(2). :172-187. (2012)
- "American College of Radiology ACR Appropriateness Criteria® Right Upper Quadrant Pain". https://acsearch.acr.org/docs/69474/Narrative/. [2018-01-01]
- Bortoff GA, Chen MYM, Ott DJ, Wolfman NT, Routh WD. "Gallbladder Stones: Imaging and Intervention". RadioGraphics. 20(3). :751-766. (2000)
- Rossi P. "Biliary Tract Radiology". Springer Science & Business Media. (2012). ISBN: 9783642603433
- Kim M, Kang TW, Jang KM, et al. "Tumefactive Gallbladder Sludge at US:Prevalence and Clinical Importance". Radiology. 283(2). :570-579. (2017)
- Shaffer EA. "Gallbladder sludge: what is its clinical significance?". Curr Gastroenterol Rep. 3(2). :166-73. (2001)
- Bope ET, Kellerman RD. "Conn's Current Therapy 2016". Elsevier Health Sciences. (2015). ISBN: 9780323355353
- Ross M, Brown M, McLaughlin K, et al. "Emergency Physician-performed Ultrasound to Diagnose Cholelithiasis: A Systematic Review". Acad Emerg Med. 18(3). :227-235. (2011)
- Catalano OA, Sahani DV, Kalva SP, et al. "MR Imaging of the Gallbladder: A Pictorial Essay". RadioGraphics. 28(1). :135-155. (2008)
- Bortoff GA, Chen MY, Ott DJ, Wolfman NT, Routh WD.. "Gallbladder stones: imaging and intervention.". Radiographics. (2000)
- Klingensmith ME. "The Washington Manual of Surgery". LWW. (2019). ISBN: 9781975120061
- Murphy MC, Gibney B, Gillespie C, Hynes J, Bolster F. "Gallstones top to toe: what the radiologist needs to know". Insights Imaging. 11(1). (2020)
- Shirley A, Rivero H, et al. "Surgical and Nonsurgical Management of Gallstones". Am Fam Physician. (2014)
- Tazuma S, Unno M, Igarashi Y, et al. "Evidence-based clinical practice guidelines for cholelithiasis 2016". J Gastroenterol. 52(3). :276-300. (2016)
- Scarcella A. "What Is the Optimal Management for Biliary Colic and Who Requires Admission?". Springer International Publishing. :205-206. (2019). ISBN: 9783319983424
- Masudi T, Capitelli-McMahon H, Anwar S. "Acute pain management in symptomatic cholelithiasis". World Journal of Gastrointestinal Surgery. 8(10). :713. (2016)
- Henderson SO, Swadron S, Newton E. "Comparison of intravenous ketorolac and meperidine in the treatment of biliary colic". J Emerg Med. 23(3). :237-241. (2002)
- Fraquelli M, Casazza G, Conte D, Colli A. "Non-steroid anti-inflammatory drugs for biliary colic". Cochrane Database of Systematic Reviews. (2016)
- Khanna IK, Pillarisetti S. "Buprenorphine - an attractive opioid with underutilized potential in treatment of chronic pain.". Journal of pain research. 8. :859-70. (2015)
- Wu S-D. "Effects of narcotic analgesic drugs on human Oddi’s sphincter motility". World Journal of Gastroenterology. 10(19). :2901. (2004)
- Thune A, Baker RA, Saccone GTP, Owen H, Toouli J. "Differing effects of pethidine and morphine on human sphincter of Oddi motility". Br J Surg. 77(9). :992-995. (1990)
- Shaffer EA. "Gallbladder cancer: the basics.". Gastroenterology & hepatology. 4(10). :737-41. (2008)
- Swartz DE, Felix EL. "Elective cholecystectomy after Roux-en-Y gastric bypass: why should asymptomatic gallstones be treated differently in morbidly obese patients?". Surg Obes Relat Dis. 1(6). :555-60. (2005)
- Baron TH, Garg SK. "Routine cholecystectomy during Roux-en-Y gastric bypass with or without choledocholithiasis". Cochrane Database of Systematic Reviews. (2013)
- Han H-S, Yoon Y-S, Agarwal AK, et al. "Laparoscopic Surgery for Gallbladder Cancer: An Expert Consensus Statement". Dig Surg. 36(1). :1-6. (2018)
- Maple JT, Ben-Menachem T, Anderson MA, et al. "The role of endoscopy in the evaluation of suspected choledocholithiasis". Gastrointest Endosc. 71(1). :1-9. (2010)
- Gurusamy K, Samraj K, Davidson B. "Early versus delayed laparoscopic cholecystectomy for biliary colic". Cochrane Database of Systematic Reviews. (2008)
- Duncan CB, Riall TS. "Evidence-based current surgical practice: calculous gallbladder disease.". J Gastrointest Surg. 16(11). :2011-25. (2012)
- Goroll AH, Mulley AG. "Primary Care Medicine: Office Evaluation and Management of the Adult Patient". Lippincott Williams & Wilkins. (2000). ISBN: 9780781712484
- Michielsen PP, Fierens H, Van Maercke YM. "Drug-Induced Gallbladder Disease". Drug Safety. 7(1). :32-45. (1992)
- Rabenstein T, Radespiel-Troeger M, Hoepfner L, et al. "Ten years experience with piezoelectric extracorporeal shockwave lithotripsy of gallbladder stones". Eur J Gastroenterol Hepatol. 17(6). :629-639. (2005)
- Paumgartner G, Sauter GH. "Extracorporeal shock wave lithotripsy of gallstones: 20th anniversary of the first treatment". Eur J Gastroenterol Hepatol. 17(5). :525-527. (2005)
- ASGE Technology Committee, Watson RR, Parsi MA, et al. "Biliary and pancreatic lithotripsy devices.". VideoGIE : an official video journal of the American Society for Gastrointestinal Endoscopy. 3(11). :329-338. (2018)
- Ahmed A, Cheung RC, Keeffe EB. "Management of gallstones and their complications.". Am Fam Physician. 61(6). :1673-80, 1687-8. (2000)
- Reisner RM, Cohen JR. "Gallstone ileus: a review of 1001 reported cases.". Am Surg. 60(6). :441-6. (1994)
- Jarnagin WR. "Blumgart's Surgery of the Liver, Biliary Tract, and Pancreas". Elsevier. (2016). ISBN: 9780323340625
- Beltrán MA. "Mirizzi syndrome: history, current knowledge and proposal of a simplified classification.". World journal of gastroenterology. 18(34). :4639-50. (2012)
- van Eijck FC, van Veen RN, Kleinrensink GJ, Lange JF. "Hartmann's gallbladder pouch revisited 60 years later.". Surg Endosc. 21(7). :1122-5. (2007)
- Buxbaum JL, Abbas Fehmi SM, Sultan S, et al. "ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis". Gastrointest Endosc. 89(6). :1075-1105.e15. (2019)
- Abich E, Glotzer D, Murphy E. "Gallstone Ileus: An Unlikely Cause of Mechanical Small Bowel Obstruction". Case Reports in Gastroenterology. 11(2). :389-395. (2017)
- Abou-Saif A, Al-Kawas FH. "Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus.". Am J Gastroenterol. 97(2). :249-54. (2002)
- Khothsymuong RR, Kaminski J. "Gallbladder Hydrops". Journal of Diagnostic Medical Sonography. 20(4). :256-259. (2004)
- Sun Q, Zhang J, Yang Y. "Gallbladder Hydrops Associated With Kawasaki Disease: A Case Report and Literature Review". Clin Pediatr (Phila). 57(3). :341-343. (2017)
- Kothari S, Afshar Y, Friedman LS, Ahn J. "AGA Clinical Practice Update on Pregnancy-Related Gastrointestinal and Liver Disease: Expert Review". Gastroenterology. (2024)
- Schwulst SJ, Son M. "Management of Gallstone Disease During Pregnancy". JAMA Surg. 155(12). :1162. (2020)
- Patel H, Jepsen J. "Gallstone Disease: Common Questions and Answers.". Am Fam Physician. 109(6). :518-524. (2024)
- Tran TT, Ahn J, Reau NS. "ACG Clinical Guideline: Liver Disease and Pregnancy". Am J Gastroenterol. 111(2). :176-194. (2016)
- Bonomo RA, Chow AW, Edwards MS, et al. "2024 Clinical Practice Guideline Update by the Infectious Diseases Society of America on Complicated Intra-abdominal Infections: Risk Assessment, Diagnostic Imaging, and Microbiological Evaluation in Adults, Children, and Pregnant People". Clin Infect Dis. (2024)
- ACOG. "Committee Opinion No. 723: Guidelines for Diagnostic Imaging During Pregnancy and Lactation". Obstet Gynecol. 130(4). :e210-e216. (2017)
- Brown KE, Hirshberg JS, Conner SN. "Gallbladder and Biliary Disease in Pregnancy". Clin Obstet Gynecol. 63(1). :211-225. (2020)
- Kumar SS, Collings AT, Wunker C, et al. "SAGES guidelines for the use of laparoscopy during pregnancy". Surg Endosc. 38(6). :2947-2963. (2024)
- American College of Obstetricians and Gynecologists' Committee on Obstetric Practice. "ACOG Committee Opinion No. 775 Summary: Nonobstetric Surgery During Pregnancy". Obstet Gynecol. 133(4). :844-845. (2019)
- Pemberton JH. "Clinical manifestations and diagnosis of acute diverticulitis in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-acute-diverticulitis-in-adults. [2015-12-15]
- Zakko SF, Afdhal NH. "Acute cholecystitis: Pathogenesis, clinical features, and diagnosis". UpToDate. UpToDate. http://www.uptodate.com/contents/acute-cholecystitis-pathogenesis-clinical-features-and-diagnosis. [2016-12-15]
- Zakko SF. "Uncomplicated gallstone disease in adults". UpToDate. UpToDate. http://www.uptodate.com/contents/uncomplicated-gallstone-disease-in-adults. [2016-10-24]
- Steel PAD. "Acute Cholecystitis and Biliary Colic". WebMD. http://emedicine.medscape.com/article/1950020. [2017-01-18]
- Heuman DM. "Gallstones (Cholelithiasis)". WebMD. http://emedicine.medscape.com/article/175667-treatment. [2016-04-14]
- Lingenfelser T, Ell C. "Laser lithotripsy for the treatment of gallstones". UpToDate. UpToDate. http://www.uptodate.com/contents/laser-lithotripsy-for-the-treatment-of-gallstones. [2014-08-01]
- Solomkin JS, Mazuski JE, Bradley JS, et al. "Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America". Clin Infect Dis. 50(2). :133-164. (2010)
- "Choledocholithiasis". http://www.dovemed.com/diseases-conditions/choledocholithiasis/. [2016-08-04]
- Afdhal NH. "Epidemiology of and risk factors for gallstones". UpToDate. UpToDate. https://www.uptodate.com/contents/epidemiology-of-and-risk-factors-for-gallstones. [2016-11-28]
- Reshetnyak VI. "Concept of the pathogenesis and treatment of cholelithiasis". World J Hepatol. 4(2). :18-34. (2012)
- Jensen SW. "Postcholecystectomy Syndrome". WebMD. http://emedicine.medscape.com/article/192761. [2016-12-27]
- Soper NJ, Malladi P. "Laparoscopic cholecystectomy". UpToDate. UpToDate. https://www.uptodate.com/contents/laparoscopic-cholecystectomy. [2016-10-13]
- Denshaw-Burke M. "Gallbladder Cancer". WebMD. http://emedicine.medscape.com/article/278641-overview. [2015-09-14]
- Hassan AU. "USMLE Platinum Notes Step 2 Ck: The Complete Preparatory Guide". Jaypee Brothers Medical Publishers. (2016). ISBN: 9789352501724
- Afdhal NH. "Acute Cholangitis". UpToDate. UpToDate. http://www.uptodate.com/contents/acute-cholangitis. [2016-03-18]
- Ansaloni L, Pisano M, Coccolini F, et al. "2016 WSES guidelines on acute calculous cholecystitis". World J Emerg Surg. 11(1). (2016)
- Sahani DV, Samir AE. "Abdominal Imaging". Elsevier Health Sciences. (2016). ISBN: 9780323431613
- Nuño-Guzmán CM, Marín-Contreras ME, Figueroa-Sánchez M, Corona JL. "Gallstone ileus, clinical presentation, diagnostic and treatment approach". World J Gastrointest Surg. 8(1). :65. (2016)
- Ahmed M. "Acute cholangitis - an update". World J Gastrointest Pathophysiol. 9(1). :1-7. (2018)
- Zakko SF. "Overview of gallstone disease in adults". UpToDate. UpToDate. https://www.uptodate.com/contents/overview-of-gallstone-disease-in-adults?search=cholelithiasis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. [2018-09-05]
- Shea JA, Berlin JA, Escarce JJ, et al. "Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease.". Arch Intern Med. 154(22). :2573-81. (1994)
- Zakko S, Afdhal N. "Approach to the management of gallstones". UpToDate. UpToDate. https://www.uptodate.com/contents/approach-to-the-management-of-gallstones?search=cholelithiasis&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H3347959734. [2018-09-05]
- "Gallstones". http://www.dynamed.com/topics/dmp~AN~T114033/Gallstones#Management-1. [2017-11-20]
- Gurusamy KS, Giljaca V, Takwoingi Y, et al. "Ultrasound versus liver function tests for diagnosis of common bile duct stones.". The Cochrane database of systematic reviews. :CD011548. (2015)
- "Choledocholithiasis". http://www.dynamed.com/topics/dmp~AN~T116085/Choledocholithiasis#Overview-and-Recommendations. [2018-12-04]
- Zakko SF, Afdhal NH. "Acute calculous cholecystitis: Clinical features and diagnosis". UpToDate. UpToDate. https://www.uptodate.com/contents/acute-calculous-cholecystitis-clinical-features-and-diagnosis?search=cholecystitis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. [2018-11-08]
- Vollmer CM, Zakko SF, Afdhal NH. "Treatment of acute calculous cholecystitis". UpToDate. UpToDate. https://www.uptodate.com/contents/treatment-of-acute-calculous-cholecystitis?search=cholecystitis&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H3556800859. [2018-10-18]
- Afdhal NH. "Acalculous Cholecystitis: Clinical manifestations, diagnosis, and management". UpToDate. UpToDate. https://www.uptodate.com/contents/acalculous-cholecystitis-clinical-manifestations-diagnosis-and-management?search=acalculous%20cholecystitis&source=search_result&selectedTitle=1~28&usage_type=default&display_rank=1. [2018-07-18]
- Gomi H, Solomkin JS, Schlossberg D, et al. "Tokyo Guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :3-16. (2018)
- Kiriyama S, Kozaka K, Takada T, et al. "Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholangitis (with videos)". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :17-30. (2018)
- Miura F, Okamoto K, Takada T, et al. "Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis". Journal of Hepato-Biliary-Pancreatic Sciences. 25(1). :31-40. (2018)
- VanderVelde J, Goldberg RF. "Clinical Algorithms in General Surgery". Springer, Cham. (2019). ISBN: 9783319984971
- Mukai S, Itoi T, Baron TH, et al. "Indications and techniques of biliary drainage for acute cholangitis in updated Tokyo Guidelines 2018.". Journal of hepato-biliary-pancreatic sciences. 24(10). :537-549. (2017)
- Chandrasekhara V, Elmunzer BJ, Khashab M, Muthusamy M. "Clinical Gastrointestinal Endoscopy". Elsevier. (2018). ISBN: 9780323415095
- Anderson MA, Fisher L, Jain R, et al. "Complications of ERCP". Gastrointest Endosc. 75(3). :467-473. (2012)
- Manes G, Paspatis G, Aabakken L, et al. "Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline". Endoscopy. 51(05). :472-491. (2019)
- Rashid F, Rashid N, Waraich N, Ahmed J, Iftikhar SY. "Role of routine oesophago-gastroduodenoscopy before cholecystectomy.". Int J Surg. 8(3). :236-8. (2010)
- "American College of Radiology ACR Appropriateness Criteria® Jaundice". https://acsearch.acr.org/docs/69497/Narrative/. [2018-01-01]
- Kelly NM, Tham T. "Abnormal Liver Function Tests in Acute Cholecystitis With and Without Choledocholithiasis". Gastroenterology. 140(5). :S-450. (2011)
- Pereira-Limâ JC, Jakobs R, Busnello JV, et al. "The role of serum liver enzymes in the diagnosis of choledocholithiasis.". Hepatogastroenterology. 47(36). :1522-5. (2000)
- Peng WK, Sheikh Z, Paterson-Brown S, Nixon SJ. "Role of liver function tests in predicting common bile duct stones in acute calculous cholecystitis.". Br J Surg. 92(10). :1241-7. (2005)
- Senturk S, Miroglu TC, Bilici A, et al. "Diameters of the common bile duct in adults and postcholecystectomy patients: a study with 64-slice CT.". Eur J Radiol. 81(1). :39-42. (2012)
- Petrescu I, Bratu AM, Petrescu S, et al. "CT vs. MRCP in choledocholithiasis jaundice.". Journal of medicine and life. 8(2). :226-31. (2015)
- Miller FH, Hwang CM, Gabriel H, et al. "Contrast-Enhanced Helical CT of Choledocholithiasis". American Journal of Roentgenology. 181(1). :125-130. (2003)
- Harisinghani MM, Chen JW, Weissleder R. "Primer of Diagnostic Imaging". Elsevier. (2018). ISBN: 9780323357746
- Feldman M, Friedman LS, Brandt LJ. "Sleisenger and Fordtran's Gastrointestinal and Liver Disease- 2 Volume Set". Elsevier. (2020). ISBN: 9780323609623
- Molvar C, Glaenzer B. "Choledocholithiasis: Evaluation, Treatment, and Outcomes.". Seminars in interventional radiology. 33(4). :268-276. (2016)
- Memon MA, Hassaballa H, Memon MI. "Laparoscopic common bile duct exploration: the past, the present, and the future.". Am J Surg. 179(4). :309-15. (2000)
- Lee TY. "Optimal Evaluation of Suspected Choledocholithiasis: Does This Patient Really Have Choledocholithiasis?". Clinical endoscopy. 50(5). :415-416. (2017)
- Gurusamy KS, Giljaca V, Takwoingi Y, et al. "Endoscopic retrograde cholangiopancreatography versus intraoperative cholangiography for diagnosis of common bile duct stones". Cochrane Database of Systematic Reviews. (2015)
- Caldwell KM, Lee SJ, Leggett PL, et al. "Bouveret syndrome: current management strategies.". Clinical and experimental gastroenterology. 11. :69-75. (2018)
- Thaker AM, Mosko JD, Berzin TM. "Post-endoscopic retrograde cholangiopancreatography pancreatitis.". Gastroenterology report. 3(1). :32-40. (2015)
- Komarowska M, Snarska J, Troska P, Suszkiewicz R. "Recurrent residual choledocholithiasis after cholecystectomy – endoscopic exploration of bile ducts performed 6 times". Polish Annals of Medicine. 18(1). :118-124. (2011)
- Oak JH, Paik CN, Chung WC, Lee K-M, Yang JM. "Risk Factors for Recurrence of Symptomatic Common Bile Duct Stones after Cholecystectomy". Gastroenterology Research and Practice. 2012. :1-6. (2012)