Quick guide
Related quick guide: Acute kidney injury
Diagnostic approach
- Creatinine
- Cystatin C (if available)
- CBC
- Urine dipstick and microscopy
- Spot urine albumin and protein for UACR and UPCR
- Consider AKI or acute-on-chronic kidney injury.
- Comprehensive clinical evaluation to identify cause
- Renal ultrasound
- Classify based on CGA staging
Diagnostic criteria
- Persistence of eGFR < 60 mL/min/1.73 m2 (≥ G3a) and/or any of the following markers of kidney damage for > 3 months:
- Albuminuria (e.g., UACR > 30 mg/g, ≥ A2)
- Urine sediment abnormalities (e.g., hematuria, casts)
- Abnormalities due to tubulointerstitial dysfunction (e.g., electrolyte and/or acid-base imbalances, nitrogenous waste retention)
- Imaging showing structural abnormalities (e.g., in polycystic kidney disease)
- History of renal transplantation
- Histological abnormalities on biopsy
Management checklist
- Treat underlying cause.
- Adjust current medications based on eGFR; avoid nephrotoxins.
- Ensure appropriate fluid intake.
- Recommend dietary changes (e.g., low sodium, protein restriction if G3–G5).
- Pharmacotherapy to prevent disease progression (e.g., RAAS inhibitors, SGLT2 inhibitors, statins)
- Manage electrolyte imbalances.
- Manage metabolic acidosis.
- Manage anemia.
- Manage CKD-MBD.
- Consult nephrology for patients with red flag features.
Red flag features
- Indications for acute dialysis
- CKD progression
- High risk of CKD progression (i.e., eGFR G4–G5, albuminuria A3, high KFRE risk)
- Treatment-resistant hypertension or persistent hyperkalemia
- Hematuria, nephrolithiasis, or hereditary kidney disease
- Acute complications (e.g., pulmonary edema, infection, drug toxicity, uremic bleeding, calciphylaxis)
- AKI episode
Summary
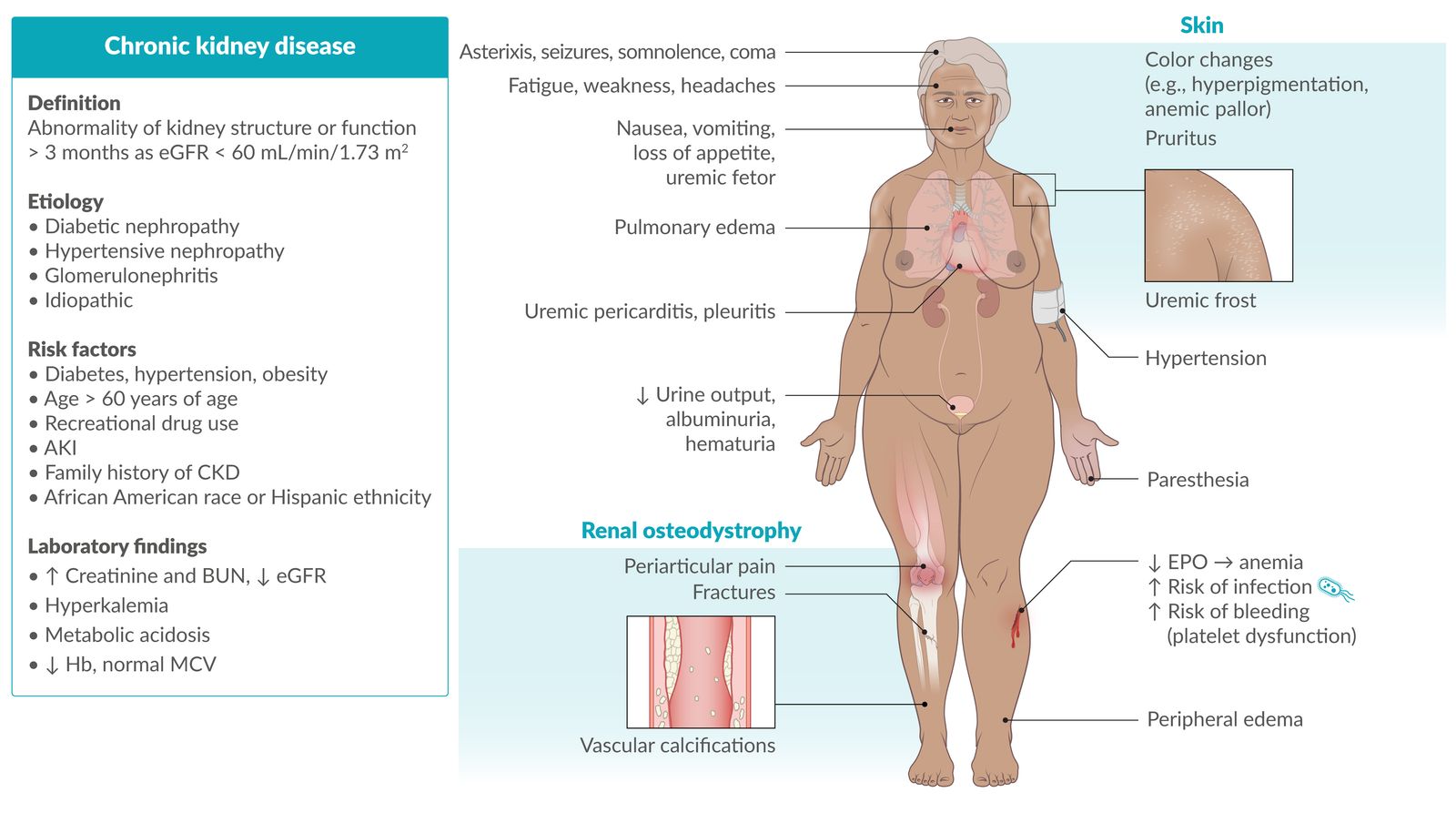
Chronic kidney disease (CKD) is defined as an abnormality of kidney structure or function that persists for > 3 months and affects health. The most common causes of CKD in the United States are diabetes mellitus, hypertension, and glomerulonephritis. Most patients remain asymptomatic until their kidney function is severely impaired due to the organ's efficient compensatory mechanisms and significant renal reserve. Patients are most commonly diagnosed via routine screening (e.g., screening of high-risk populations, routine blood tests that include serum creatinine to estimate glomerular filtration rate). At advanced disease stages, patients may present with symptoms of fluid overload (e.g., peripheral edema) and/or uremia (e.g., fatigue, pruritus). Patients with CKD have a significantly increased risk of developing atherosclerotic cardiovascular disease (ASCVD). Laboratory studies may show metabolic complications, such as hyperkalemia, hyperphosphatemia, hypocalcemia, and metabolic acidosis. Management is aimed at slowing CKD progression and preventing and/or managing complications. This includes treating the underlying disease, avoiding nephrotoxic substances, maintaining adequate hydration and nutrition, pharmacotherapy (e.g., RAAS inhibitors, SGLT2 inhibitors, and statins), and addressing complications such as anemia of CKD and CKD-mineral and bone disorder (CKD-MBD). Renal replacement therapy (i.e., dialysis or renal transplantation) is required if CKD progresses to end-stage renal disease (ESRD).
See also “Acute kidney injury” (AKI) and “Diabetic kidney disease” (DKD).
Epidemiology
-
Prevalence [1]
- An estimated 37 million individuals (15%) in the US have CKD.
- 726,000 individuals have ESRD.
- Incidence: > 350 cases of ESRD per million individuals annually [1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Diabetes mellitus (38%)
- Hypertension (26%)
- Glomerulonephritis (16%)
- Other causes (15%): e.g., polycystic kidney disease, analgesic misuse, amyloidosis
- Idiopathic (5%)
Pathophysiology
Pathophysiology depends on the underlying condition, any of which will eventually lead to progressive nephron loss, structural damage, and impaired kidney function.
Underlying conditions
Diabetic nephropathy [2]
- Hyperglycemia → nonenzymatic glycation of proteins → varying degrees of damage to all types of kidney cell.
- Pathological changes include:
- Hypertrophy and proliferation of mesangial cells, GBM thickening, and ECM protein accumulation → eosinophilic nodular glomerulosclerosis
- Thickening and diffuse hyalinization of afferent and efferent arterioles/interlobular arteries
- Interstitial fibrosis, TBM thickening, and tubular hypertrophy
Hypertensive nephropathy
- Caused by protective autoregulatory vasoconstriction of preglomerular vessels, increases in systemic blood pressure do not normally affect renal microvessels. [3]
- Increased systemic blood pressure (e.g., due to chronic hypertension) below the protective autoregulatory threshold → benign nephrosclerosis (sclerosis of afferent arterioles and small arteries) → ↓ perfusion → ischemic damage
- In case BP exceeds threshold → acute injury → malignant nephrosclerosis (petechial subcapsular hemorrhages, visible infarction with necrosis of mesangial and endothelial cells, thrombosis of glomeruli capillaries, luminal thrombosis of arterioles, and red blood cell extravasation and fragmentation) → failure of autoregulatory mechanisms → ↑ damage
Glomerulonephritis (GN)
- Noninflammatory GN (e.g., minimal change GN, membranous nephropathy, focal segmental glomerulosclerosis)
- Inflammatory GN (e.g., lupus nephritis, poststreptococcal GN, rapid progressive GN, hemolytic uremic syndrome)
Consequences
")
Reduced GFR
- ↓ Production of urine → ↑ extracellular fluid volume → total-body volume overload
- ↓ Excretion of waste products (e.g., urea, drugs)
-
↓ Excretion of phosphate → hyperphosphatemia
-
During the early stages of CKD, plasma phosphate levels will typically be normal due to the increased secretion of fibroblast growth factor 23 (FGF23). [4]
- FGF23 is produced by osteoblasts in response to initial hyperphosphatemia and increased calcitriol.
- Increased secretion of FGF23 leads to increased phosphate secretion and suppressed conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D.
- In advanced CKD, the effects of FGF 23 subside (most likely due to development of resistance in target tissues). [4]
-
During the early stages of CKD, plasma phosphate levels will typically be normal due to the increased secretion of fibroblast growth factor 23 (FGF23). [4]
- ↓ Maintenance of acid-base balance; → metabolic acidosis
- ↓ Maintenance of electrolyte concentrations → electrolyte imbalances (e.g., Na+ retention)
Reduced endocrine activity
- ↓ Hydroxylation of calcifediol → ↓ production of calcitriol → (in combination with ↓ excretion of phosphate) → ↓ serum Ca2+ → ↑ PTH
- ↓ Erythropoietin → ↓ stimulation of erythropoiesis
Reduced gluconeogenesis
- ↑ Risk of hypoglycemia
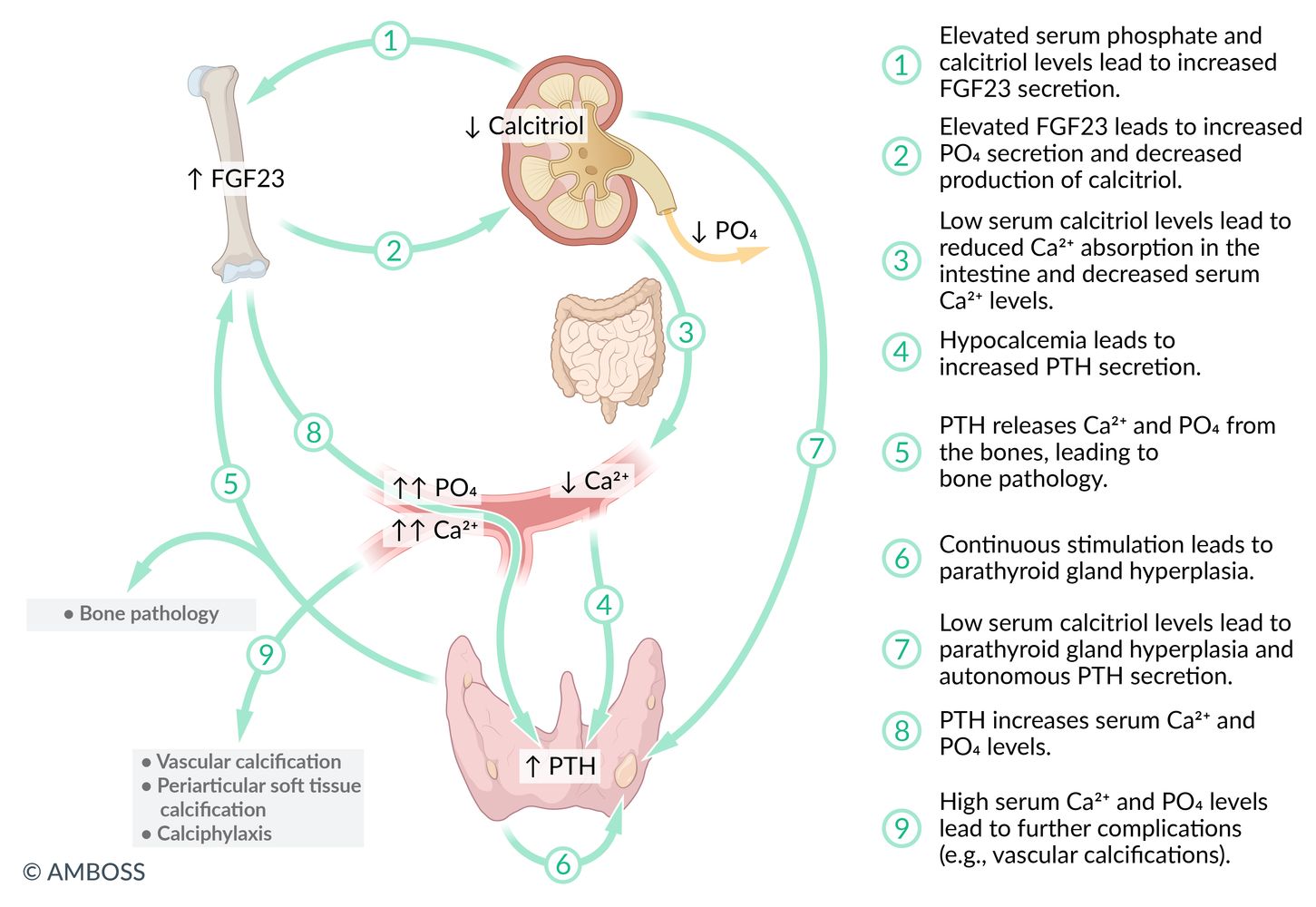
Diagram that illustrates the pathophysiological cascade of chronic kidney disease-mineral and bone disorder (CKD-MBD), focusing on the complex feedback loops involving fibroblast growth factor 23 (FGF23), calcitriol (vitamin D3), parathyroid hormone (PTH), calcium (Ca2+), and phosphate (PO4) in the context of chronic kidney dysfunction.
© AMBOSS
Clinical features
Patients are often asymptomatic until later stages due to the exceptional compensatory mechanisms of the kidneys.
Manifestations of Na+/H2O retention
- Hypertension and heart failure
- Pulmonary; and peripheral edema
Manifestations of uremia
- Definition: Uremia is defined as the accumulation of toxic substances due to decreased renal excretion. These toxic substances are mostly metabolites of proteins such as urea, creatinine, β2 microglobulin, and parathyroid hormone.
-
Constitutional symptoms
- Fatigue
- Weakness
- Headaches
-
Gastrointestinal symptoms
- Nausea and vomiting
- Loss of appetite
- Uremic fetor: characteristic ammonia- or urine-like breath odor
-
Dermatological manifestations
- CKD-associated pruritus
- Skin color changes (e.g., hyperpigmentation, pallor due to anemia)
- Uremic frost: uremia leads to high levels of urea secreted in the sweat, the evaporation of which may result in tiny crystallized yellow-white urea deposits on the skin.
-
Serositis
-
Uremic pericarditis: a complication of chronic kidney disease that causes fibrinous pericarditis
- Clinical features: chest pain worsened by inhalation
-
Physical examination findings
- Friction rub on auscultation
- ECG changes normally seen in nonuremic pericarditis (e.g., diffuse ST-segment elevation) are not usually seen.
- Pleuritis
-
Uremic pericarditis: a complication of chronic kidney disease that causes fibrinous pericarditis
-
Neurological symptoms
- Asterixis
-
Signs of uremic encephalopathy
- Seizures
- Somnolence
- Coma
- Peripheral neuropathy → paresthesias
-
Hematologic symptoms
- Anemia
- Leukocyte dysfunction → ↑ risk of infection
- ↑ Bleeding tendency caused by abnormal platelet adhesion and aggregation [5]
Kidney OUTAGES: hyperKalemia, renal Osteodystrophy, Uremia, Triglyceridemia, Acidosis (metabolic), Growth delay, Erythropoietin deficiency (anemia), Sodium/water retention (consequences of chronic kidney disease)




Scalp and forehead of a patient with a markedly elevated blood urea nitrogen level (approx. 100 mg/dL)
The widely disseminated tiny white spots are crystallized urea resulting from the evaporation of sweat that contains high amounts of urea.
This finding is a sign of severe azotemia, which is rare in settings where renal replacement therapy is available.
Source: “Uremic frost on forehead and scalp of young Afro-Caribbean male.jpg” by Fythrion, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}

Gross pathology specimen of cardiac tissue within the pericardium
The pericardium is covered with linear, fibrinous exudates consisting of fibrin strands (exemplary indicated by arrows) and leukocytes. The villus-like distribution of the exudates is the result of friction caused by the normal contractile movement of the heart.
Blue overlay: right lung
Green overlay: left lung
Source: © IMPP
© AMBOSS
Classification
General principles [6][7]
CKD is classified according to cause, eGFR category, and albuminuria category (CGA classification).
-
Clinical uses
- Standardized documentation of CKD stages (e.g., diabetic kidney disease G3A2)
- Identifying CKD progression
- Determining the frequency of patient monitoring
-
Interpretation: Higher stages are associated with a poorer prognosis. [8]
- Increased risk for CKD progression and mortality (e.g., all-cause mortality, cardiovascular mortality)
- Increased risk for complications (e.g., AKI, CKD-MBD)
Cause [6]
- Systemic vs. primary cause: Determine if the cause of CKD is systemic (e.g., diabetes) or primary (e.g., polycystic kidney disease).
-
Type: Determine the type (presumed or confirmed) of the damage within the kidney.
- Glomerular
- Tubulointerstitial
- Vascular
- Cystic and congenital
eGFR and albuminuria [6]
| Risk of progression and complications of CKD based on eGFR and albuminuria category [6] | ||||
|---|---|---|---|---|
| eGFR category(mL/min/1.73 m2) | Persistent albuminuria category(UACR) | |||
| A1: < 30 mg/g or < 3 mg/mmol (normal to mildly increased albuminuria) | A2: 30–300 mg/g or 3–30 mg/mmol (moderately increased albuminuria) | A3: > 300 mg/g or > 30 mg/mmol (severely increased albuminuria) | ||
| Stage G1 CKD: ≥ 90 (normal or high) | Low risk* | Moderate risk | High risk | |
| Stage G2 CKD: 60–89 (mildly low) | ||||
| Stage G3 CKD | G3a: 45–59 (mildly to moderately low) | Moderate risk | High risk | Very high risk |
| G3b: 30–44 (moderately to severely low) | High risk | Very high risk | ||
| Stage G4 CKD: 15–29 (severely low) | Very high risk | |||
| Stage G5 CKD: < 15 (kidney failure) | ||||
| *Stages G1A1 and G2A1 only indicate CKD if there are other markers of kidney damage. | ||||
End-stage renal disease (ESRD) [9]
- Irreversible kidney dysfunction with a GFR < 15 mL/min/1.73 m2
- AND manifestations of uremia requiring chronic renal replacement therapy with either dialysis (hemofiltration or hemodiafiltration) or renal transplantation
- Prognosis: Approx. 50% of individuals with ESRD die of cardiovascular disease.
Screening
Indications for screening [6]
Consider screening patients with risk factors for CKD, e.g.: [1][6]
-
Comorbidities
- ASCVD risk factors (e.g., hypertension, diabetes mellitus)
- Established cardiovascular diseases (e.g., coronary artery disease, heart failure)
- History of AKI
- Advanced age (> 60 years of age) [10]
- Genitourinary conditions (e.g., polycystic kidney disease, recurrent kidney stones)
- Autoimmune diseases (e.g., systemic lupus erythematosus, vasculitis)
- Gestational conditions (e.g., pre-eclampsia, eclampsia) and complications (e.g., preterm birth, small gestational size)
- Infectious diseases (e.g., HIV, schistosomiasis)
- Obesity
-
Exposures
- Substance use (e.g., smoking, alcohol, recreational drugs)
- Occupational exposure to toxic substances (e.g., cadmium, lead, mercury, pesticides, polycyclic hydrocarbons)
- Nephrotoxic medications (may cause chronic tubulointerstitial nephritis)
- Radiation therapy (may cause radiation nephritis)
- Family history: CKD or associated conditions
- Other: residence in areas with elevated CKD prevalence (e.g., areas with environmental toxins or high prevalence of APOL1 genetic variants)
Screening methods [6]
- Assess GFR (using eGFRcr-cys, if available, or eGFRcr) and urine albumin-to-creatinine ratio (UACR).
- If results are normal (i.e., eGFR ≥ 60 mL/min/1.73 m2, UACR < 30 mg/g, and no other markers of kidney damage):
- Retest frequency is based on individual risk.
- See also “Screening for diabetic kidney disease.” [11][12]
Diagnosis
Approach [6]
- Assess GFR to determine if the patient meets the criteria for CKD.
- Stage CKD according to the CGA classification using eGFRcr-cys (if available) and UACR.
- Determine the underlying cause with a thorough clinical evaluation and noninvasive testing.
- Kidney biopsy is typically reserved for rapid and unexplained decline in GFR and/or to confirm the underlying cause.
- Estimate risk of CKD progression to kidney failure for timely referral for renal transplantation and/or dialysis access planning.
- Refer to nephrology for urgent renal replacement therapy if any indications for acute dialysis are identified.
A single abnormal GFR or UACR level is not diagnostic for CKD.
Confirm CKD with repeat testing if albuminuria, hematuria, or low GFR are detected incidentally.
Assessment of GFR [6]
Use a validated equation tested within the relevant geographical region. Avoid incorporating race into assessment of GFR.
Estimated GFR (eGFR)
- Serum creatinine-based eGFR formulas (eGFRcr): preferred initial test for most patients
-
Creatinine and cystatin C-based eGFR (eGFRcr-cys) is preferred when:
- There is diagnostic uncertainty
- eGFRcr may be inaccurate
- CKD staging is required
- Cystatin C-based eGFR (eGFRcys): less accurate than eGFRcr-cys
- Measured urine creatinine clearance: Consider when eGFRcr-cys may be inaccurate and mGFR is unavailable.
When eGFRcr and eGFRcys align, all three estimates (i.e., eGFRcr, eGFRcys, and eGFRcr-cys) have a similar degree of accuracy. When eGFRcr and eGFRcys differ, eGFRcr-cys is more accurate than eGFRcr or eGFRcys. [6]

Measured GFR (mGFR)
- Gold-standard test but not routinely indicated
- May be considered in selected cases when a more accurate assessment would alter management.
Diagnostic criteria [6]
Criteria for CKD
- Persistence of eGFR < 60 mL/min/1.73 m2 (≥ G3a)
-
AND/OR persistence of any of the following markers of kidney damage:
- History of renal transplantation
- Imaging showing structural abnormalities (e.g., in polycystic kidney disease)
- Histological abnormalities on biopsy
- Abnormalities due to tubulointerstitial dysfunction, e.g.:
- Electrolyte and acid-base imbalances
- Retention of nitrogenous wastes
- Reduced production of erythropoietin, 1,25-dihydroxyvitamin D, and/or renin
- Urine sediment abnormalities (e.g., hematuria, casts)
- Albuminuria: e.g., urine albumin-to-creatinine ratio (UACR) > 30 mg/g (≥ A2)
- PLUS proof of chronicity (i.e., duration of > 3 months) established by any of the following:
- Comparison of current and previous GFR, albuminuria, proteinuria, and/or urine microscopies (if available)
- Suggestive imaging findings (e.g., small hyperechoic kidneys on ultrasound)
- Suggestive histopathological findings (e.g., atrophy and/or fibrosis)
- Suggestive medical history (e.g., history of conditions known to contribute to or cause CKD)
- Repeat measurements after > 3 months
Suspect AKI (with or without underlying CKD) in patients with a rapid rise in creatinine level (i.e., over days rather than weeks to months).
A diagnosis of CKD requires a persistent eGFR < 60 mL/min/1.73 m2 and/or markers of kidney damage lasting more than 3 months.
CKD progression
-
CKD progression is defined as either of the following:
- A decline in renal function leading to a change in eGFR category
- A sustained decline in eGFR of > 5 mL/min/1.73 m2 per year (known as “rapid progression”)
- Risk of progression to ESRD [6]
- Calculate for patients stage G3 CKD to stage G5 CKD.
- Use a validated calculator, e.g., kidney failure risk equation (KFRE).
- Interpretation
- Five-year kidney failure risk 3–5%: Consider nephrology referral.
- Two-year kidney failure risk > 10%: Consider multidisciplinary care.
- Two-year kidney failure risk > 40%: Consider planning and preparation for renal replacement therapy and referral for transplantation.
Validated risk-stratification tools can be used to identify patients at increased risk for kidney failure to help guide appropriate referrals to specialist nephrology care.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Initial studies
Laboratory studies [6]
Blood tests
- Serum markers to assess eGFR
- Creatinine (preferred initial test): ↑ levels
-
Cystatin C: ↑ levels
- Consider as the initial test if creatinine may be inaccurate; see “Assessment of GFR.”
- Obtain (if available) for all patients with confirmed CKD for CKD staging.
- ↑ BUN
- Hemostasis: ↑ bleeding time, normal PT, PTT and platelet count (see “Diagnostic workup of bleeding disorders”)
Urine studies
- Spot UACR
- Used to determine the albuminuria category for CKD staging [6]
- Elevated levels indicate albuminuria.
- ↑ Spot urine protein-to-creatinine ratio (UPCR): may show nephrotic-range proteinuria
-
Urine dipstick
- Proteinuria on urine dipstick requires confirmation with quantitative UACR or UPCR.
- May show hematuria
- Urine microscopy: may show abnormal urine sediment (e.g., waxy casts)
Suspect plasma cell dyscrasia if the UPCR is significantly higher than the UACR. Send a urine sample for protein electrophoresis to identify urine proteins other than albumin (e.g., Bence Jones protein).
Ultrasound of the kidneys and urinary tract [6]
- First-line imaging technique for the assessment of kidney structure
- Consider obtaining for all patients to further support the diagnosis and help determine the etiology.
- Findings that suggest chronic kidney damage include: [13]
- ↓ Kidney length (< 10 cm)
- ↓ Parenchymal and/or cortical thickness
- ↑ Cortical echogenicity
- Cysts
- Calcifications
- Findings that suggest specific etiologies
- Ureteral or renal pelvic dilation suggests obstructive nephropathy.
- Bilaterally enlarged kidneys with multiple cysts suggest polycystic kidney disease.
- Cortical nephrocalcinosis suggests chronic glomerulonephritis or chronic pyelonephritis. [14]

Consider obtaining an ultrasound of the kidneys and urinary tract as part of the routine evaluation of all patients with CKD.
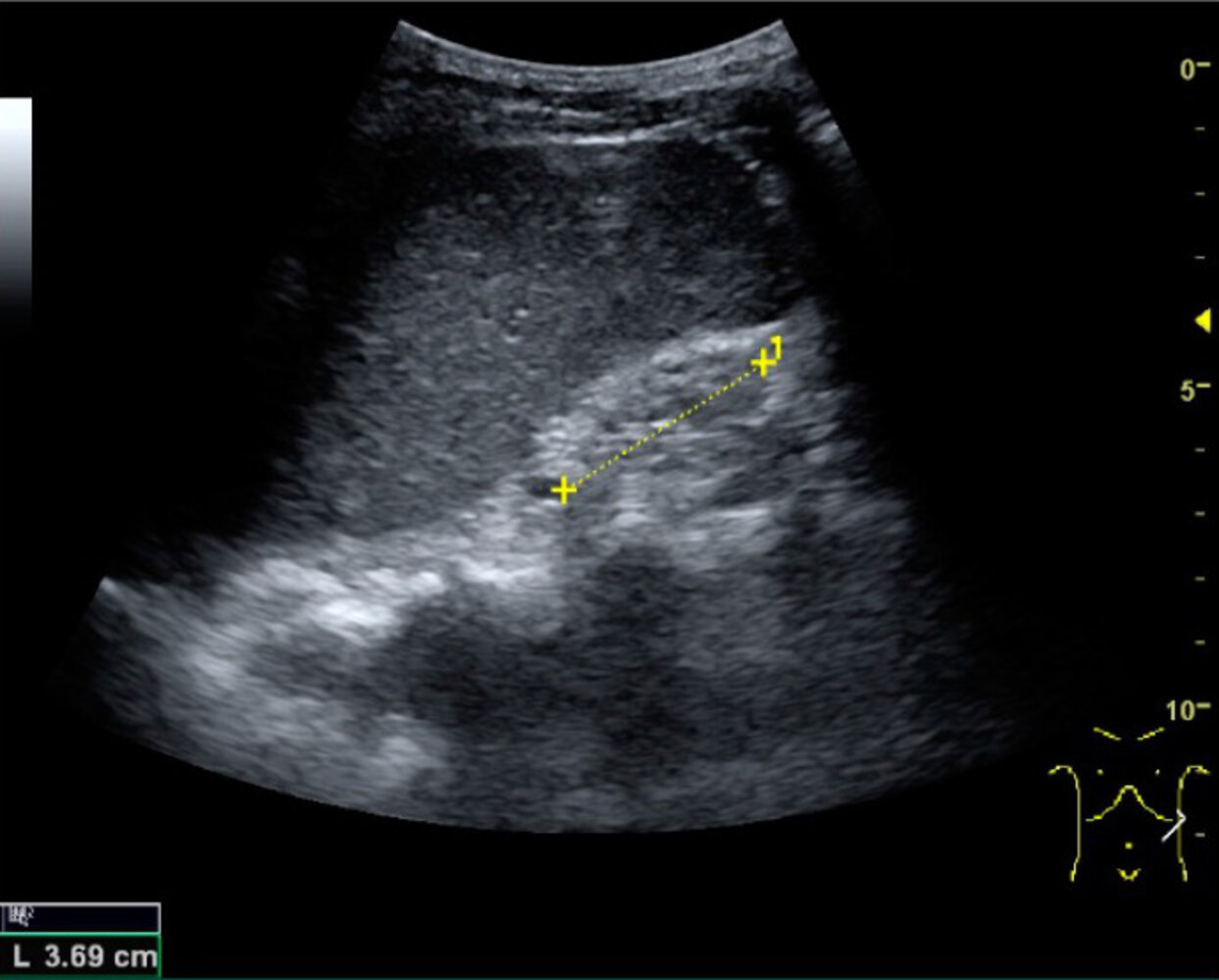
Ultrasound abdomen (left kidney)
A small hyperechoic left kidney (green overlay) was identified adjacent to the spleen (S) on an oblique image of the left upper quadrant.
Examples of ultrasound findings that may be seen in the setting of chronic renal disease include reduced kidney size and cortical thickness, increased cortical echogenicity, marginal irregularities, calcifications, and cysts.
Source: “Fig 25, In: Ultrasonography of the Kidney: A Pictorial Review” by Lindskov Hansen K, Bachmann Nielsen M, Ewertsen C, MDPI, licensed under CC BY 4.0. Modifications: Image cropped. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Additional studies
Additional studies should be considered based on clinical suspicion or if an underlying cause of CKD is not apparent following an initial assessment. [6]
Integration of information from the patient's clinical presentation, laboratory tests, imaging, and in some cases, renal biopsy is needed to determine the underlying cause.
Noninvasive testing [6]
| Investigations for specific underlying causes of CKD | ||
|---|---|---|
| Examples | Suggestive features | Common additional studies |
| Diabetes |
|
|
| Glomerulonephritis |
|
|
| Multiple myeloma |
|
|
| Renal artery stenosis |
|
|
| Amyloidosis |
|
|
Renal biopsy [6]
- Often not required to establish the cause
- Consider in either of the following situations:
- Rapid and unexplained decline in eGFR
- Need for diagnostic confirmation of the underlying cause (e.g., glomerulonephritis) prior to starting disease-specific therapy
Discuss the risks and benefits of biopsy with the patient and use shared decision-making.
Management
The following guidance applies to patients with CKD stage G1–G5 who are not on dialysis and have not had renal transplantation.
Approach [6]
The goals of management are to delay the progression of CKD and prevent and/or manage complications.
- Treat the underlying causes of CKD (if identified).
- Start comprehensive management.
- Provide recommendations on nutrition and vaccinations, and adjust current medications as required.
- Consider indications for pharmacotherapy for CKD (e.g., RAAS inhibitors, SGLT2 inhibitors, statins).
- Primary prevention of ASCVD
- Assess for evidence of metabolic complications and start management under specialist guidance.
- Monitor for CKD progression.
- Continuously evaluate the need for advanced care.
If CKD progression or complications are detected during follow-up, review the current management and assess for reversible causes of progression (e.g., nephrotoxin exposure, medications affecting glomerular perfusion, urinary tract obstruction).
Prevention of AKI in patients with CKD is vital to prevent disease progression.
If there are indications for acute dialysis, urgently start renal replacement therapy.
ASCVD risk assessment [6]
- Untreated CKD is an ASCVD risk-enhancing factor.
- Perform the following in all patients:
- Diabetes mellitus screening
- Screening for hypertension
- Screening for lipid disorders
- ASCVD risk calculation using an equation that has been validated in CKD patients or that includes eGFR and albuminuria (e.g., PREVENT equations)
Management of ASCVD reduces cardiovascular morbidity and mortality and helps prevent CKD progression.
Cardiovascular disease (e.g., coronary artery disease, stroke) is the leading cause of death in patients with CKD. The risk of cardiovascular events is higher in patients with more advanced stages of CKD. [15]
Lifestyle changes
- Encourage a healthy lifestyle, including:
- Smoking cessation and cessation of any tobacco products
- Weight loss in patients with overweight or obesity
- Moderate-intensity physical activity for 150 minutes per week
- For any recommendations, consider the patient's age, ethnicity, comorbidities, and access to resources.
- Reassess lifestyle factors every 3–6 months.
Nutrition [6]
- Fluid intake: Ensure appropriate fluid intake and avoid dehydration.
-
Protein and energy consumption in CKD
- Mediterranean diet or DASH diet
- Protein intake of 0.8 g/kg/day in adult patients with CKD stage G3–G5
- Avoid a high protein intake of > 1.3 g/kg/day in patients at risk for CKD progression.
- Recommend avoiding highly-processed foods.
-
Electrolytes
- Sodium restriction (< 2 g/day): for individuals with CKD stage G3–G5
- Potassium intake adjustment: avoidance of high-potassium foods in patients with CKD stage G4–G5 to reduce the risk for hyperkalemia
- Phosphorus intake adjustment: as needed to maintain serum phosphate levels in the normal range
- Micronutrients: Consider multivitamin supplementation; for patients with inadequate dietary vitamin (e.g., vitamin D) intake. [16]
Dietary protein restriction must only be prescribed under close clinical supervision and in consultation with a nutritionist.
Obtain a nutritionist consult for all patients with CKD.
Medication management [6][17]
- Renally cleared medications: Adjust dosing based on the patient's eGFR.
-
Potentially nephrotoxic substances
- Avoid use (unless the benefits outweigh the risks).
- Frequently monitor renal function and electrolytes and, if indicated, measure drug levels. [15]
- Contrast imaging
- The risk of contrast-induced nephropathy is highest in patients with an eGFR < 30 mL/min/1.73 m2.
- For information on prevention, see “Contrast-induced nephropathy.”
Weigh the risks and benefits of potentially nephrotoxic substances on an individual basis.
In acutely ill patients with CKD, consider temporarily holding renally cleared medications and medications that can detrimentally affect glomerular perfusion (e.g., NSAIDs, ACE inhibitors, ARBs) to reduce the risk for AKI.
Vaccinations
Patients with CKD are at an increased risk for infection.
- Live attenuated vaccines: Consider offering the MMR vaccine and varicella vaccine to patients who have not been vaccinated since infancy or do not have immunity.
-
Inactivated vaccines
- Ensure influenza, pneumococcal, and hepatitis B vaccinations are up-to-date. [18]
- See “Immunization schedule” for recommendations on indications, timing, and frequency.
Patients with CKD may be immunocompromised. Consider the patient's current immune status and consult a specialist before administering live vaccines. [15]
Nephrology consultation [6]
Indications for nephrology consultation include any of the following:
- CKD progression
- High risk for CKD progression
- KFRE with 5-year risk of progression to ESRD of 3–5%
- eGFR category G4–G5 and/or albuminuria category A3 (i.e., UACR > 300 mg/g)
- Treatment-resistant hypertension or persistent hyperkalemia
- Hematuria, nephrolithiasis, or hereditary kidney disease
- AKI episode
Renal replacement therapy [6]
Plan for pre-emptive renal transplantation and/or dialysis access in adults if the eGFR falls to < 15–20 ml/min per 1.73 m2 or if the KFRE 2-year risk is > 40%. [6]
-
Nonoperative (hemodialysis or peritoneal dialysis)
- Indications include:
- Hemodynamic or metabolic complications that are refractory to medical therapy, e.g.:
- Volume overload or hypertension
- Metabolic acidosis
- Hyperkalemia
- Serositis (e.g., uremic pericarditis)
- Other manifestations of uremia (e.g., signs of encephalopathy, intractable pruritus)
- Refractory deterioration in nutritional status
- Hemodynamic or metabolic complications that are refractory to medical therapy, e.g.:
- Indications include:
- Operative: renal transplantation
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Pharmacotherapy
Antihypertensives [6][19]
- Systolic blood pressure (SBP) target
- SBP < 120 mm Hg is recommended (if tolerated). [6]
- Consider higher targets (e.g., < 130–140 mm Hg) for selected patients.
- First-line therapy: RAAS inhibitors (i.e., ACE inhibitors or ARBs)
- Start in patients with CKD stage G1–G4) and moderately to severely increased albuminuria (A2–A3) with or without diabetes.
- Consider for patients with normal to mildly increased albuminuria (A1).
- Consider an additional nonsteroidal mineralocorticoid receptor antagonist (e.g., finerenone) in selected adults with T2DM.
- Benefits: renal protection and reduced proteinuria
-
Risks: may cause hyperkalemia and/or an initial decline in eGFR
- Check serum creatinine and potassium levels within 2–4 weeks of starting therapy.
- Consider a potassium binder (e.g., sodium zirconium cyclosilicate, patiromer) if serum potassium is mildly elevated (i.e., 5.5-5.9 mEq/L).
- Hold or reduce the RAAS inhibitor dose if symptomatic hypotension or uncontrollable hyperkalemia develop or if there is a decline in eGFR by > 30% within 4 weeks of starting therapy or increasing a dose.
- Consider additional antihypertensive therapy:
- For patients with an initial SBP ≥ 20 mm Hg above target
- For patients who do not reach the target while on monotherapy at the optimal dose
- Second-line agents include:
- Loop diuretics or thiazide diuretics
- Calcium channel blockers (CCBs)
- Beta-blockers: usually reserved for patients with cardiovascular comorbidities
- Steroidal aldosterone receptor antagonists: usually reserved for treatment resistant hypertension
- See “Antihypertensive therapy” for information on medication dosages and contraindications.
Avoid any combination of ACE inhibitors, ARBs, and/or direct renin inhibitors due to the increased risk for hyperkalemia and AKI.
Blood pressure control is essential to prevent ASCVD complications, reduce mortality, and help delay disease progression in patients with CKD.
Lipid lowering therapy [6][20][21]
- Goal: reduction of ASCVD risk
-
Fasting lipid panel
- Order at diagnosis and repeat only if the results may alter management.
- May show dyslipidemia (↑ triglycerides are common)
-
Statin therapy: indicated for prevention of ASCVD and management of ASCVD in patients with CKD
- Start for all patients ≥ 50 years of age.
- Consider initial combination therapy with ezetimibe for patients ≥ 50 years of age with an eGFR < 60 mL/min/1.73 m2 (i.e., eGFR category G3a–G5).
- Consider for patients 18–49 years of age with concomitant coronary artery disease, history of ischemic stroke, diabetes mellitus and/or 10-year ASCVD risk > 10%.
For patients with an eGFR < 60 mL/min/1.73 m2 (eGFR category G3–G5), adjust the statin dose to reduce the risk for toxicity.
Individuals with CKD often have dyslipidemia (e.g., ↑ triglycerides, ↑ LDL, ↓ HDL) due to alterations in lipoprotein metabolism.
Diabetes medications [6][22]
-
SGLT2 inhibitors [6]
- Recommended for patients with or without diabetes who have:
- eGFR ≥ 20 mL/min/1.73 m2 and UACR ≥ 200 mg/g
- Concomitant heart failure regardless of albuminuria level
- Once started, continue even if eGFR declines to < 20 mL/min/1.73 m2.
- Stop therapy if it cannot be tolerated or if starting RRT.
- Withhold therapy during surgery, prolonged fasting, or critical medical illness.
- Recommended for patients with or without diabetes who have:
- GLP-1 receptor agonists: indicated in patients with T2DM and CKD who have not met glycemic targets despite metformin and SGLT2 inhibitor use or who cannot use those medications
-
General considerations
- HbA1c may not accurately reflect glycemic control in patients with CKD and an eGFR < 30 mL/min/1.73 m2; confirm with results from ambulatory glucose monitoring.
- Medications may need to be reduced or stopped as eGFR declines.
- See “Diabetic kidney disease” for further information on managing diabetes in patients with CKD.
SGLT-2 inhibitors and GLP-1 receptor agonists can slow CKD progression and reduce urinary albumin excretion and ASCVD events. [22][23]
Discontinue metformin in patients who develop CKD stage G4–G5; continue SGLT-2 inhibitors if tolerated.
Uric acid-lowering therapy [6]
- Recommended for symptomatic hyperuricemia after a first episode of gout (particularly if uric acid level is > 9 mg/dL)
- Not recommended to delay CKD progression in patients with asymptomatic hyperuricemia
- Xanthine oxidase inhibitors are preferred over uricosuric agents.
Low-dose colchicine or glucocorticoids (intra-articular or oral) are preferred over NSAIDs to treat acute gout in patients with CKD.
Antiplatelet therapy [6]
- Indicated for the management of ASCVD
- May be considered for primary prevention of ASCVD in high-risk individuals (e.g., patients with CKD and diabetes) [15][23]
Monitoring for complications
- Screening tests for complications are indicated in all patients with CKD at diagnosis to establish a baseline.
- Patients with CKD categories G3–G5 require repeat testing at regular intervals.
In CKD, close surveillance of serum potassium, calcium, and phosphate levels is essential.
| Overview of screening for CKD complications [6] | ||||
|---|---|---|---|---|
| Screening test | Screening frequency (CKD category G3–G5) | Potential findings | Management | |
| CBC |
|
|
|
|
| Potassium [17] |
|
|
|
|
| Mineral and bone disorder panel [24] | PTH |
|
|
|
| Phosphate and total calcium |
|
|
||
| Vitamin D |
|
|
||
| Coagulation screen |
|
|
|
|
| Blood gases |
|
|
|
|
Screening and periodic monitoring for complications are indicated in all patients with CKD and eGFR < 60 mL/min/1.73 m2.
Dot phrase
Chronic kidney disease (outpatient management)
Assessment: This is a @AGE@-year-old @SEX@ with CKD, stage [***] (eGFR *** mL/min/1.73 m2), likely secondary to [***hypertension/diabetes]. [***Unstable/Stable] renal function over the past year. [***No] current signs of uremia or acute decompensation. Recent labs show [K+ *** mmol/L] and ACR [***]. Blood pressure [***is/is not] at target of [***/*** mm Hg]. [***No] evidence of mineral and bone disorder or anemia.
Plan:
–BMP in 3 months to monitor renal function and electrolytes; last value: [***]
–Urine ACR annually; last value: [***]
–CBC annually; last hemoglobin [***]; consider ESAs for Hb ≤ 9–10 g/dL in anemia of CKD
–PTH annually; last value [***]
–Continue/Increase/Decrease [ACE/ARB *** mg ***frequency] for blood pressure and renal protection.
–Start/Continue [***statin *** mg once daily] for ASCVD risk reduction.
–Avoid NSAIDs and nephrotoxic agents.
–Low-sodium and low-potassium diet
–Educate on CKD progression and signs of worsening (e.g., fatigue, swelling, reduced urine output).
–Discuss importance of medication adherence, adequate fluid intake, and dietary modifications.
–Follow up in 3 months to review labs and reassess kidney function.
–Refer to nephrology if CKD progresses.
Complications
For recommendations on screening tests and frequencies, see “Monitoring for complications.” Specialist consultation (e.g., with a nephrologist) is advised for the management of complications.
Common acute complications [26]
- Pulmonary edema
- Hyperkalemia
- Infection [27]
- Bacteremia secondary to UTI or pneumonia
- IV catheter-related infection
- Hemodialysis catheter-related infection
- Peritoneal dialysis-associated peritonitis
- Drug toxicity [28]
- See also “Complications of hemodialysis” and “Complications of peritoneal dialysis.”
Maintain a low threshold for suspecting infections and initiating empiric antibiotics, as signs of sepsis may be vague or absent in patients with CKD. [26][29]
Uremic bleeding [30][31][32]
- Definition: prolonged or spontaneous bleeding caused by uremic platelet dysfunction
- Clinical features: ecchymoses, purpura, epistaxis, bleeding at venipuncture sites, GI bleeding, intracranial hemorrhage
- Diagnosis: clinical diagnosis; bleeding time is typically prolonged when checked.
-
Treatment
- Red blood cell transfusion and/or erythropoietin-stimulating agents for a goal Hb ≥ 10 g/dL [32]
- Desmopressin (off-label) for rapid-onset short-term control [32]
- Renal replacement therapy [30][32]
- Cryoprecipitate transfusion: Consider for life-threatening hemorrhage or before emergency surgery. [30][32]
- Conjugated estrogen: Consider in consultation with nephrology for slow-onset long-term control. [30][32]
Calciphylaxis [33][34]
- Definition: a rare but potentially life-threatening condition characterized by dermal and subcutaneous arteriolar calcifications that cause painful skin necrosis
-
Risk factors
- Most commonly seen in patients with ESRD who are receiving dialysis
- Comorbidities: diabetes mellitus, obesity, CKD-mineral and bone disorder, warfarin therapy
-
Clinical features
- Intensely painful skin lesions (e.g., livedo reticularis, purpura, plaques, nodules)
- Necrotic skin ulcerations, typically covered with black eschar
- Areas of firm, painful, subcutaneous tissue
- Secondary bacteremia and sepsis
-
Diagnosis
- A skin biopsy is required for definitive diagnosis but may provoke new lesions.
- Clinical diagnosis may be made in patients with ESRD with a typical presentation. [34]
-
Differential diagnosis
- Warfarin skin necrosis
- Nephrogenic systemic fibrosis
- Vasculitis
- Purpura fulminans
- Cholesterol emboli
-
Treatment [33][34]
- Multidisciplinary care
- Supportive measures
- Provide wound care and aggressive pain management.
- Consider holding potentially offending medications: warfarin, calcium and iron supplements, vitamin D preparations.
- Treat CKD-mineral and bone disorder.
- Optimize renal replacement therapy.
- Monitor for infection and initiate appropriate sepsis management if indicated.
- Pharmacotherapy: Consider a trial of sodium thiosulfate in consultation with a specialist. [33][34]


Calciphylaxis is a rare condition with very high mortality. Early recognition and aggressive management are essential, although response to therapy is often poor.
Anemia in chronic kidney disease [35]
Definitions
- Anemia in CKD: anemia in a patient with CKD, regardless of the cause
- Anemia of CKD: normocytic, normochromic anemia caused by CKD, primarily due to reduced erythropoietin production; exacerbated by uremia, inflammation, and shortened red blood cell survival
-
Anemia in patients aged ≥ 15 years with CKD is defined by the following Hb thresholds:
- Male individuals: Hb < 13.0 g/dL
- Female individuals: Hb < 12.0 g/dL
-
Hb thresholds for anemia in pediatric patients with CKD are age-specific.
- Age 6 months–4 years: Hb < 11.0 g/dL
- Age 5–11 years: Hb < 11.5 g/dL
- Age 12–14 years: Hb < 12.0 g/dL
Etiology
- Anemia of CKD: ↓ synthesis of erythropoietin → ↓ stimulation of RBC production → normocytic, normochromic anemia
-
Anemia in CKD
- Iron deficiency
- Gastrointestinal bleeding
- Malignancy
- Bone marrow dysfunction (e.g., myelodysplastic disorders)
- Malnutrition
- Vitamin B12 deficiency
- Folate deficiency
- Hemolysis
- Hyperparathyroidism
- Hypothyroidism
- Systemic infection and/or inflammation
Diagnosis
-
Initial laboratory studies
-
CBC
- ↓ Hb
- MCV is usually normal but may be low in patients with concurrent iron deficiency.
-
Iron studies, e.g.:
- Reticulocyte production index
- Serum ferritin
- Transferrin saturation (TSAT)
-
CBC
-
Interpretation of iron studies
- Systemic iron deficiency
- ↓ TSAT (i.e., < 20%)
- AND ↓ ferritin (< 100 ng/mL in patients not receiving dialysis or < 200 ng/mL in patients receiving dialysis)
-
Iron-restricted erythropoiesis
- ↓ TSAT (< 20%)
- AND normal or ↑ ferritin (more than 100–200 ng/mL)
- Systemic iron deficiency
-
Testing frequency
- Stage G3 CKD: annually
- Stage G4 CKD: twice per year
- Stage G5 CKD: every 3 months
- Further studies: Perform an evaluation of anemia (e.g., vitamin B12 and folate levels) if iron deficiency is ruled out and/or suspicion of additional etiology remains high.
Evaluate patients with MCV < 80 μm3 and/or ferritin < 45 ng/mL for blood loss anemia.
Management
Rule out differential diagnoses and address correctable causes of anemia (e.g., iron deficiency).
-
Iron therapy (oral or IV)
- Patients receiving hemodialysis
- Initiate if ferritin is ≤ 500 ng/mL and TSAT is ≤ 30%.
- IV iron is preferred (e.g., low molecular weight iron dextran, iron sucrose, ferric gluconate).
- Patients not receiving hemodialysis: Initiate if ferritin is < 100 ng/mL and TSAT is < 40% OR ferritin is 100–300 ng/mL and TSAT is < 25%.
- Hold iron therapy if ferritin is > 700 ng/mL or TSAT is ≥ 40% to prevent iron overload.
- Patients receiving hemodialysis
-
Erythropoiesis-stimulating agents (ESAs): preferred over hypoxia-inducible factor prolyl hydroxylase inhibitors
- Agents include epoetin alfa and beta, darbepoetin, and methyl polyethylene glycol-epoetin beta.
- Patients receiving hemodialysis: Consider when Hb is ≤ 9.0–10.0 g/dL.
- Patients not receiving hemodialysis: Consider on a case-by-case basis for symptomatic anemia in consultation with a nephrologist.
- Check Hb levels 2–4 weeks after initiating or adjusting therapy.
- Target Hb: < 11.5 g/dL in adults
- Monitor Hb levels every 3 months in patients on stable maintenance therapy.
- Adverse effects include an increased risk of thrombosis, increased blood pressure, and headache.
- Hypoxia-inducible factor prolyl hydroxylase inhibitors (e.g., daprodustat): for patients with ESA hyporesponsiveness or contraindications to ESAs
-
RBC transfusions: Avoid if possible to reduce the risk of allosensitization.
- Harms and benefits should be carefully weighed.
- The decision to transfuse is based on the presence and severity of clinical features of anemia rather than Hb level.
ESAs have been associated with increased mortality, stroke, and venous thromboembolism and are not recommended for patients with Hb levels ≥ 10 g/dL.
Anemia in CKD is associated with an increased risk of mortality, major adverse cardiovascular events, heart failure, and CKD progression.
Chronic kidney disease-mineral and bone disorder (CKD-MBD) [36][37]
-
Definitions
- CKD-MBD refers to abnormalities in mineral and/or bone metabolism in CKD.
- Renal osteodystrophy refers specifically to issues with bone metabolism due to CKD.
-
Pathophysiology
-
CKD results in hypocalcemia via different mechanisms.
- ↓ Renal excretion of phosphate → hyperphosphatemia → calcium phosphate precipitation in tissues → ↓ Ca2+
- ↓ Renal hydroxylation of vitamin D → ↓ 1,25-dihydroxyvitamin D → ↓ intestinal Ca2+ absorption → ↓ Ca2+
- Chronically decreased calcium levels can cause secondary hyperparathyroidism, which can progress to tertiary hyperparathyroidism.
-
CKD results in hypocalcemia via different mechanisms.
-
Histological classification
- Secondary hyperparathyroidism: high turnover bone disease or osteitis fibrosa cystica (metabolic bone disease)
- Osteomalacia: defective bone mineralization
- Mixed uremic bone disease: secondary hyperparathyroidism with osteomalacia
- Adynamic bone disease: decreased bone formation without osteomalacia
-
Clinical features (may be asymptomatic initially)
- Musculoskeletal
- Fractures
- Bone and periarticular pain
- Muscular weakness and pain
- Extraskeletal
- Focal vascular calcification (atherosclerotic plaques)
- Diffuse vascular calcification (medial calcific sclerosis and calcific uremic arteriolopathy)
- Musculoskeletal
-
Diagnostics [37]
- Laboratory studies: frequent monitoring with a mineral and bone disorder panel
- Imaging (not routinely indicated)
- X-ray may show sclerotic changes (rugger jersey spine), brown tumors, and/or subperiosteal bone thinning.
- Consider bone mineral density testing for patients with CKD category G3–G5.
-
Treatment (under specialist guidance): The goal is to normalize phosphate, calcium, and PTH levels. [36][37]
-
Treatment of hyperphosphatemia, e.g.:
- Dietary phosphate restriction
- Phosphate binders (e.g., sevelamer)
-
Treatment of hyperparathyroidism, e.g.:
- Cholecalciferol or ergocalciferol supplementation for vitamin D deficiency or insufficiency
- Calcitriol (not routinely recommended)
- Calcimimetics (e.g., cinacalcet)
- Parathyroidectomy (last-line therapy)
-
Treatment of hyperphosphatemia, e.g.:
Hyperphosphatemia, hypocalcemia, and insufficient production of vitamin D in patients with CKD may lead to secondary hyperparathyroidism and consequent renal osteodystrophy.
Growth delay and developmental delay in children
- Contributing factors include:
- Malnutrition (protein and calorie deficit)
- Metabolic acidosis
- Growth hormone resistance
- Anemia
- Renal osteodystrophy
Chronic kidney disease-associated pruritus [38]
- Definition: chronic, generalized pruritus that is frequently associated with advanced kidney disease
-
Prevalence
- Patients undergoing hemodialysis: ∼ 70%
- Patients not undergoing hemodialysis: ∼ 25%
-
Clinical features
- Generalized and symmetrical pruritus
- Exacerbated by dry conditions, temperature extremes, stress, and bathing
- Absence of primary skin lesions; secondary skin lesions from repetitive scratching
- Xerosis
-
Diagnosis
- Diagnosis of exclusion
- Primary dermatological conditions, drug-induced pruritus (e.g., from ACE inhibitors, beta blockers), and other systemic causes must be ruled out.
- See "Diagnosis of pruritus."
-
Management
- Emollients
- Optimizing dialysis efficacy
- Gabapentinoids
- Narrowband UVB phototherapy
- Difelikefalin
- Kidney transplantation
CKD-associated pruritus is associated with severe sleep disturbances and reduced quality of life.
We list the most important complications. The selection is not exhaustive.
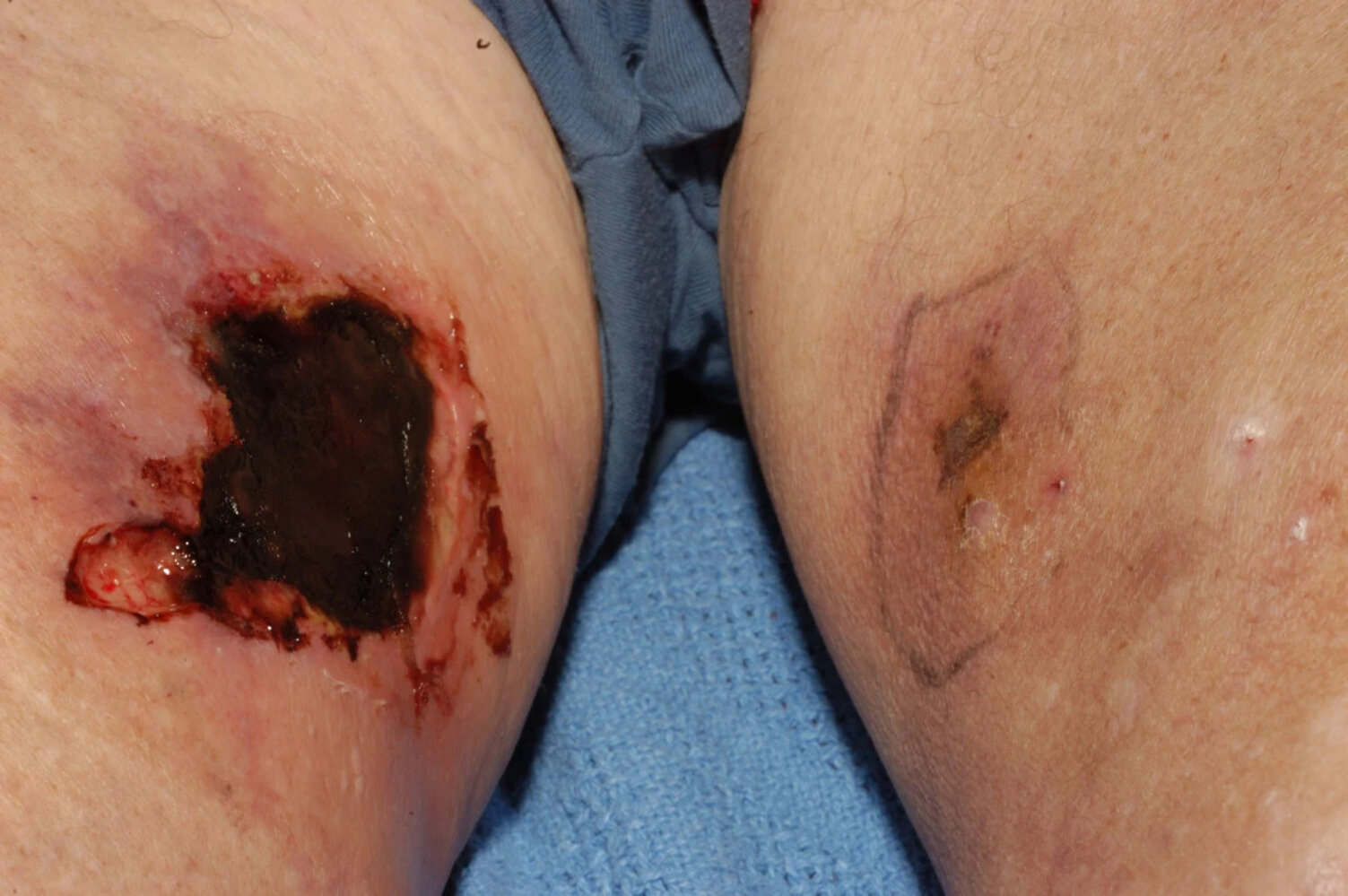
Photograph of the medial aspect of the upper legs of a male patient
The left leg shows a small, well circumscribed, darkened macule surrounded by light purple discoloration, resembling early stage gangrene. The right leg shows a larger, well-demarcated, gangrenous lesion surrounded by purple discoloration.
These findings are typical of early (left leg) and advanced (right leg) calciphylaxis.
Source: “Fig 1, In: Calciphylaxis following kidney transplantation: a case report” by Hanvesakul R, Silva MA, Hejmadi R et al., BMC, licensed under CC BY 2.0.

Severely calcified arteries and the loss of soft tissue at the tips of the index and middle fingers
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Diagram that illustrates the pathophysiological cascade of chronic kidney disease-mineral and bone disorder (CKD-MBD), focusing on the complex feedback loops involving fibroblast growth factor 23 (FGF23), calcitriol (vitamin D3), parathyroid hormone (PTH), calcium (Ca2+), and phosphate (PO4) in the context of chronic kidney dysfunction.
© AMBOSS
Special patient groups
Chronic kidney disease in pregnancy [39]
-
Overview
- Prevalence of CKD in women of childbearing age is estimated to be 0.1–4%.
- Research suggests that pregnancy negatively affects kidney function in women with CKD (as evidenced by, e.g., doubling of creatinine, progression to next stage).
- CKD negatively influences pregnancy outcomes by increasing the risk of maternal and fetal complications (see below).
- Physiological anatomic (e.g., dilation of the renal collecting system, changes in kidney length and volume) and hemodynamic changes (e.g., decreased mean arterial pressure) can pose a challenge to monitoring kidney function and diagnosing complications.
-
Maternal complications
- Preeclampsia
- Concomitant hypertension and proteinuria
- Preterm delivery
- Cesarean delivery
-
Fetal complications
- Intrauterine growth restriction
- Low birth weight
- Fetal/neonatal death
-
Management
- Patients should be cared for by a multidisciplinary team, including nephrologists, neonatologists, and health care personnel specialized in high-risk obstetrics.
- Optimization of blood pressure (i.e., < 140/90 mm Hg) to reduce the risk of preeclampsia and other complications (see “Overview of antihypertensives to avoid during pregnancy” for details)
- Minimization of proteinuria: Treatment depends on the underlying etiology (e.g., pregnancy-safe immunosuppression with prednisone or calcineurin inhibitors in lupus nephritis).
- Consideration of anticoagulation in individuals with severe proteinuria
- Prevention of preeclampsia with aspirin before 16 weeks of gestation and calcium and vitamin D supplementation throughout the pregnancy
Related One-Minute Telegram
- One-Minute Telegram 106-2024-2/2: Real-world implications of dialysis vs. medical management in older adults with CKD
- One-Minute Telegram 67-2023-2/3: Empagliflozin improves outcomes in chronic kidney disease
- One-Minute Telegram 63-2022-2/3: The interval between hemodialysis and surgery matters
- One-Minute Telegram 63-2022-3/3: No revelations on the best anticoagulant for patients with end-stage kidney disease
- One-Minute Telegram 51-2022-3/3: Are glucocorticoids a safe and effective treatment for IgA nephropathy?
- One-Minute Telegram 14-2020-3/3: GFR formulas are just estimates, but can we estimate better?
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- CKD Assessment Tool and eGFR Calculator from the National Kidney Foundation
- KDIGO Guideline Hub
- 2026 KDIGO Clinical Practice Guideline for the Management of Anemia in Chronic Kidney Disease
- 2024 KDIGO Clinical Practice Guideline for the Evaluation and Management of CKD
- 2021 KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease
- 2020 KDIGO Diabetes Management in CKD Guideline
- 2020 Update to the KDOQI Clinical Practice Guideline for Nutrition in CKD
- 2014 KDIGO Clinical Practice Guideline for Lipid Management in CKD
- One-Minute Telegram
References
- "Chronic Kidney Disease in the United States, 2019". https://web.archive.org/web/20200907155315/https://www.cdc.gov/kidneydisease/publications-resources/2019-national-facts.html#calculation
- Kim JH, Baek CH, Min JY, et al. "Desmopressin improves platelet function in uremic patients taking antiplatelet agents who require emergent invasive procedures". Ann Hematol. 94(9). :1457-1461. (2015)
- Stevens PE, Ahmed SB, Carrero JJ, et al. "KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease". Kidney Int. 105(4). :S117-S314. (2024)
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Dalrymple LS, Go AS. "Epidemiology of Acute Infections among Patients with Chronic Kidney Disease". Clin J Am Soc Nephrol. 3(5). :1487-1493. (2008)
- Roberts DM, Sevastos J, Carland JE, et al. "Clinical Pharmacokinetics in Kidney Disease". Clin J Am Soc Nephrol. 13(8). :1254-1263. (2018)
- Campanelli F, Soudry-Faure A, Avondo A, et al. "Septic patients without obvious signs of infection at baseline are more likely to die in the ICU". BMC Infect Dis. 22(1). (2022)
- Hedges SJ, Dehoney SB, Hooper JS, Amanzadeh J, Busti AJ. "Evidence-based treatment recommendations for uremic bleeding". Nat Clin Pract Nephrol. 3(3). :138-153. (2007)
- Baaten CCFMJ, Sternkopf M, Henning T, et al. "Platelet Function in CKD: A Systematic Review and Meta-Analysis". J Am Soc Nephrol. 32(7). :1583-1598. (2021)
- Kaw D, Malhotra D. "Platelet Dysfunction and End-Stage Renal Disease". Semin Dial. 19(4). :317-322. (2006)
- Nigwekar SU, Kroshinsky D, Nazarian RM, et al. "Calciphylaxis: Risk Factors, Diagnosis, and Treatment". Am J Kidney Dis. 66(1). :133-146. (2015)
- Nigwekar SU, Thadhani R, Brandenburg VM. "Calciphylaxis". N Engl J Med. 378(18). :1704-1714. (2018)
- Tonelli M, Berns J, Bozkurt B, et al. "KDIGO 2026 Clinical Practice Guideline for the Management of Anemia in Chronic Kidney Disease (CKD)". Kidney International. 109(1). :S1-S99. (2026)
- Gilbert, SJ; Weiner, DE. "National Kidney Foundation's Primer on Kidney Disease". Elsevier Health Sciences. (2017). ISBN: 9780323477949
- Ketteler M, Block GA, Evenepoel P, et al. "Executive summary of the 2017 KDIGO Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD) Guideline Update: what’s changed and why it matters". Kidney Int. 92(1). :26-36. (2017)
- Cheng AY, Wong LS. "Uremic Pruritus: From Diagnosis to Treatment". Diagnostics (Basel). 12(5). (2022)
- Kanwar YS, Sun L, Xie P, Liu F, Chen S. "A Glimpse of Various Pathogenetic Mechanisms of Diabetic Nephropathy". Annual Review of Pathology: Mechanisms of Disease. 6(1). :395-423. (2011)
- Bidani AK, Griffin KA. "Pathophysiology of Hypertensive Renal Damage". Hypertension. 44(5). :595-601. (2004)
- Courbebaisse M, Lanske B. "Biology of Fibroblast Growth Factor 23: From Physiology to Pathology". Cold Spring Harbor Perspectives in Medicine. 8(5). :a031260. (2017)
- "How to Classify CKD". https://www.kidney.org/professionals/explore-your-knowledge/how-to-classify-ckd
- Levey AS, de Jong PE, Coresh J, et al. "The definition, classification, and prognosis of chronic kidney disease: a KDIGO Controversies Conference report". Kidney Int. 80(1). :17-28. (2011)
- Agarwal R. "Defining end-stage renal disease in clinical trials: a framework for adjudication". Nephrology Dialysis Transplantation. 31(6). :864-867. (2015)
- "KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease". https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf. [2013-01-01]
- Ikizler TA, Burrowes JD, Byham-Gray LD, et al. "KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update". American Journal of Kidney Diseases. 76(3). :S1-S107. (2020)
- Chen TK, Knicely DH, Grams ME. "Chronic Kidney Disease Diagnosis and Management". JAMA. 322(13). :1294. (2019)
- "Renal Disease and Adult Vaccination". https://web.archive.org/web/20201016160814/https://www.cdc.gov/vaccines/adults/rec-vac/health-conditions/renal-disease.html
- Cheung AK, Chang TI, Cushman WC, et al. "KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease". Kidney Int. 99(3). :S1-S87. (2021)
- Mikolasevic I, Žutelija M, Mavrinac V, Orlic L. "Dyslipidemia in patients with chronic kidney disease: etiology and management". International Journal of Nephrology and Renovascular Disease. Volume 10. :35-45. (2017)
- Wanner C, Tonelli M. "KDIGO Clinical Practice Guideline for Lipid Management in CKD: summary of recommendation statements and clinical approach to the patient". Kidney Int. 85(6). :1303-1309. (2014)
- De Boer IH, Caramori ML, Chan JCN, et al. "Executive summary of the 2020 KDIGO Diabetes Management in CKD Guideline: evidence-based advances in monitoring and treatment". Kidney Int. 98(4). :839-848. (2020)
- Ali S, Dave N, Virani SS, Navaneethan SD. "Primary and Secondary Prevention of Cardiovascular Disease in Patients with Chronic Kidney Disease". Curr Atheroscler Rep. 21(9). (2019)
- Levin A, Bakris GL, Molitch M, et al. "Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease". Kidney Int. 71(1). :31-38. (2007)
- Viswanathan G, Sarnak MJ, Tighiouart H, Muntner P, Inker LA. "The association of chronic kidney disease complications by albuminuria and glomerular filtration rate: a cross-sectional analysis". Clin Nephrol. 80(07). :29-39. (2013)
- "Aging and Kidney Disease". https://www.kidney.org/news/monthly/wkd_aging
- ElSayed NA, McCoy RG, et al. "11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes—2025". Diabetes Care. 48(Supplement_1). :S239-S251. (2024)
- de Boer IH, Khunti K, Sadusky T, et al. "Diabetes Management in Chronic Kidney Disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO)". Diabetes Care. (2022)
- Hui D, Hladunewich MA. "Chronic Kidney Disease and Pregnancy". Obstetrics & Gynecology. 133(6). :1182-1194. (2019)
- Moghazi S, Jones E, Schroepple J, et al. "Correlation of renal histopathology with sonographic findings.". Kidney Int. 67(4). :1515-20. (2005)
- Schepens D, Verswijvel G, Kuypers D, Vanrenterghem Y. "Renal cortical nephrocalcinosis". Nephrology Dialysis Transplantation. 15(7). :1080-1082. (2000)