Summary
Chronic lymphocytic leukemia (CLL) is a type of B-cell malignancy that manifests with lymphocytic leukocytosis. CLL is the most common type of leukemia in adults and is typically diagnosed in older individuals (≥ 65 years of age). Clinical features include painless lymphadenopathy, fatigue, chronic pruritus, and increased susceptibility to infections. However, most cases are asymptomatic and diagnosed based on incidental laboratory findings. Diagnosis requires persistent monoclonal B-cell lymphocytosis (≥ 5000/mm3 for ≥ 3 months) with immunophenotypic markers consistent with CLL on flow cytometry. Peripheral blood smear typically shows a high percentage of small mature lymphocytes and smudge cells (Gumprecht shadows). Several molecular markers are used to predict prognosis and guide treatment, the most important being the negative prognostic markers del(17p) and TP53 mutation. Advances in targeted therapy have improved patient outcomes in CLL and small molecule inhibitors (e.g., ibrutinib, venetoclax) are now first-line treatment for most patients. Chemoimmunotherapy may be an effective alternative for some patients. Patients with low-risk disease (Rai stage 0) should be managed expectantly. Allogeneic stem cell transplantation is a curative treatment option but is often not possible because of the older age and multiple comorbidities of most patients with CLL.
Definitions
- Chronic lymphocytic leukemia: a type of proliferative B-cell malignancy that manifests with lymphocytic leukocytosis [1]
- Small lymphocytic lymphoma (SLL): a type of B-cell lymphoma with the same genetic and molecular markers as CLL that manifests primarily in the lymph nodes, bone marrow, and other lymphatic tissue rather than with leukocytosis [1][2]
Some sources classify CLL as a low-grade non-Hodgkin lymphoma because the origin cell is likely a mature B lymphocyte. However, as the malignant cells are present in the blood, it is considered to be a leukemia. SLL is the manifestation of this condition in lymphatic tissue, and is therefore considered to be a lymphoma. [1]

© AMBOSS
Epidemiology
- Sex: ♂ > ♀ (∼ 2:1)
- Age: The median age at the time of diagnosis is 70–72 years (incidence of CLL increases with age).
- Most common type of leukemia in adults
References:[3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Risk factors
- Older age
- Environmental factors: organic solvents
- Family history
Pathophysiology
Acquired mutations in hematopoietic stem cells → increased proliferation of leukemic B cells with impaired maturation and differentiation in the bone marrow, resulting in:
- Suppression of the proliferation of normal blood cells
-
Immunosuppression
- Hypogammaglobulinemia
- Granulocytopenia
- Thrombocytopenia
- Anemia
-
Immunosuppression
- Infiltration of the lymph nodes, liver, and spleen


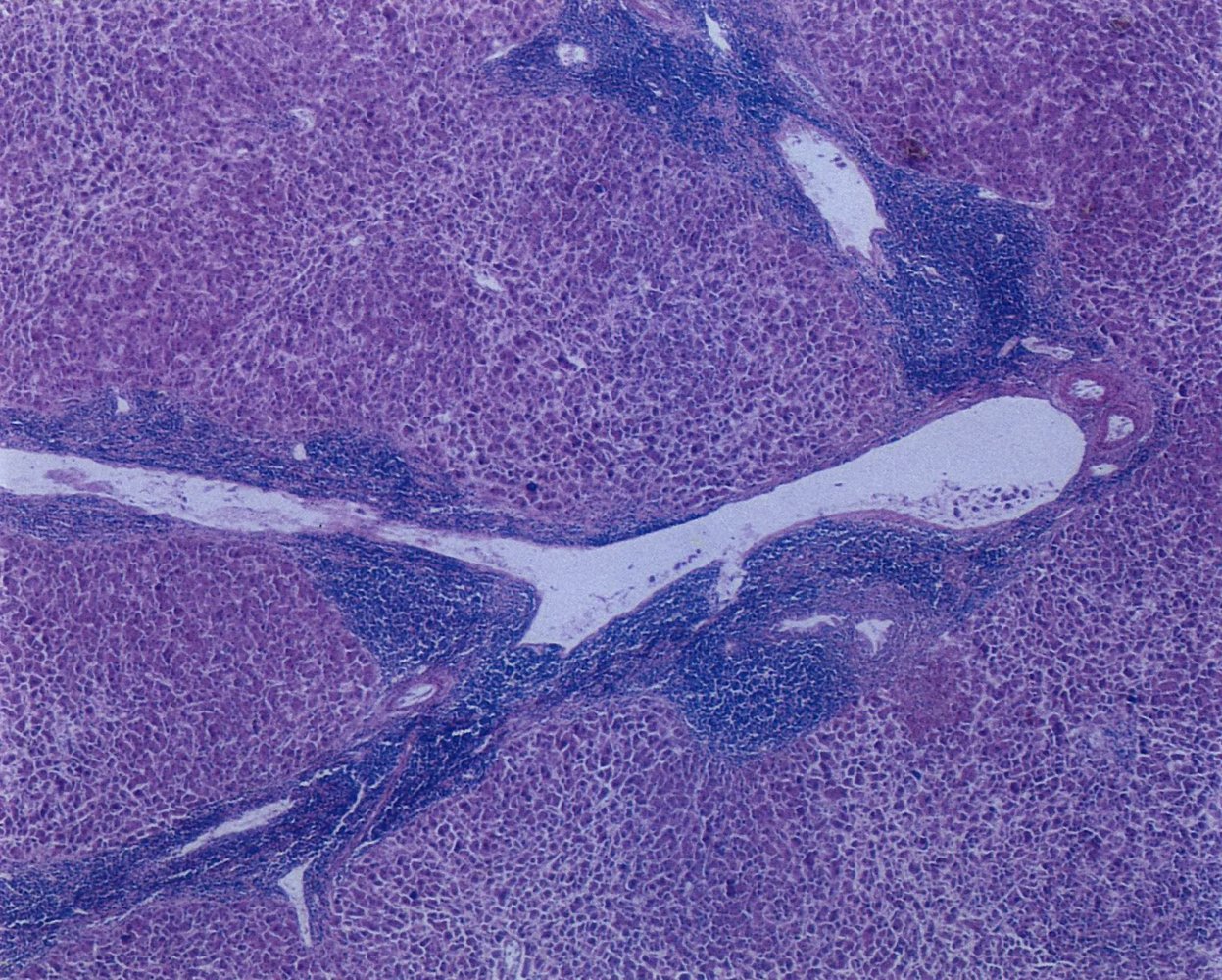
Photomicrograph of a liver tissue specimen (H&E stain; intermediate power magnification)
The branch of the portal vein (P) runs horizontally through the image and forms the portal triad (circle) with the artery and bile duct. A central vein (example indicated by “C”) can be seen in the middle of each hepatic lobule. There are numerous lymphocytic periportal infiltrates (example indicated by “L” and red overlay) due to chronic lymphocytic leukemia (CLL).
Source: © IMPP
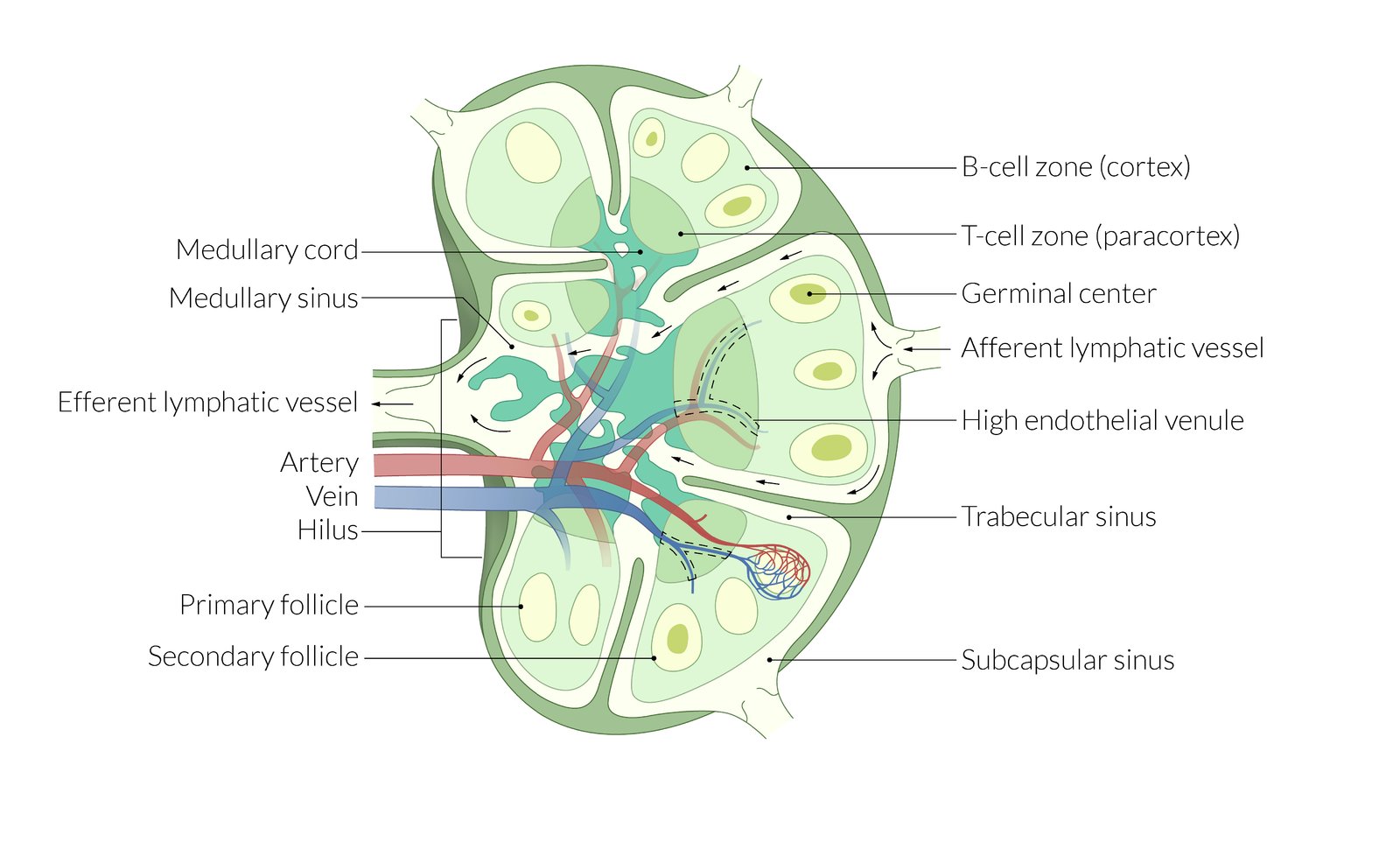
The parenchyma of the lymph node is divided into a B-cell zone (cortex), a T-cell zone (paracortex), and the marrow. The cortex contains primary and secondary lymph follicles with germinal centers, which allow affinity maturation of B cells. At the hilum (concave side), blood vessels enter and efferent lymphatic vessels leave the node. The entering artery and vein branch into a large capillary network. Special high endothelial venules in the paracortex allow for lymphocyte extravasation.
Afferent lymphatic vessels enter through the capsule at many points in the periphery and open into the subcapsular sinus. The cortical sinus runs from the cortex via the paracortex to the medullary sinus, which then drains into the efferent lymphatic vessel.
© AMBOSS
Clinical features
About half of cases of CLL remain asymptomatic for a long period, resulting in late or incidental diagnosis.
- Weight loss, fever, night sweats, fatigue (B symptoms)
- Painless lymphadenopathy
- Hepatomegaly and/or splenomegaly may occur.
-
Repeated infections
- Severe bacterial infections (e.g., necrotic erysipelas)
- Mycosis (candidiasis)
- Viral infections (herpes zoster)
- Symptoms of anemia and thrombocytopenia
-
Dermatologic symptoms
- Leukemia cutis
- Chronic pruritus
- Chronic urticaria
Lymphadenopathy is a typical finding in lymphoid malignancies such as CLL and helps to differentiate CLL from CML, a myeloid malignancy.
References:[3][4]
Diagnosis
General principles [1][2][5]
- Diagnosis requires persistent monoclonal lymphocytosis plus CLL immunophenotype confirmed by flow cytometry.
- Most patients are asymptomatic and evaluated based on incidental laboratory findings.
- Biopsy may be indicated in certain patients, e.g., if the diagnosis is uncertain.
- Refer to hematology or oncology for further evaluation and management.
In patients with confirmed CLL, staging (e.g., using the Rai staging system) and the presence of prognostic markers are used to guide management.
Laboratory studies [1][2][5][6]
Obtain a CBC, peripheral blood smear, and flow cytometry for all patients.
-
Diagnostic criteria
- Persistent (≥ 3 months) lymphocytosis (≥ 5000/mm3) [1][6]
-
CLL immunophenotype confirmed by flow cytometry, including :
- Expression of CD5, CD19, CD20 , CD23 [2]
- Light chain restriction (kappa or lambda)
-
Additional findings: may further support the diagnosis
-
Cytopenias
- Anemia (usually normochromic, normocytic): may be caused by AIHA [5][7]
- Thrombocytopenia
- Granulocytopenia
-
Peripheral blood smear may show:
- High percentage of small mature lymphocytes
- Smudge cells (Gumprecht shadows): mature lymphocytes that rupture easily; appear as artifacts on a blood smear [8]
-
Cytopenias
The occurrence of both AIHA and ITP is known as Evans syndrome. [5][6]
In CLL, the smudge cells on a peripheral blood smear look like Crushed Little Lymphocytes.
")
")

")
")
Prognostic markers in CLL [5]
-
Indications for testing
- Confirmed CLL diagnosis
- Repeat testing prior to initiating or changing treatment
-
Methods [2][5][6]
- Cytogenetic testing
- FISH to assess for common structural chromosomal aberrations in CLL, e.g., del(17p)
- Immunoglobulin heavy chain variable region (IGHV) mutational status
- TP53 mutational status
- Serum studies: β2-microglobulin and LDH
- Cytogenetic testing
-
Interpretation
- Adverse prognosis: e.g., del(17p) , del(11q), TP53 mutation, elevated β2-microglobulin, elevated LDH
- Intermediate prognosis: trisomy 12 [1]
- Favorable prognosis: IGHV mutation , isolated del(13q)
Biopsies [1]
-
Bone marrow aspiration and biopsy [2]
- Not routinely required for diagnosis
- Consider in patients with cytopenias to determine the cause.
- Typical findings in aspirate include a high percentage of small mature lymphocytes.
- Lymph node biopsy: Consider if the diagnosis is uncertain or for the diagnosis of SLL or Richter transformation.
")
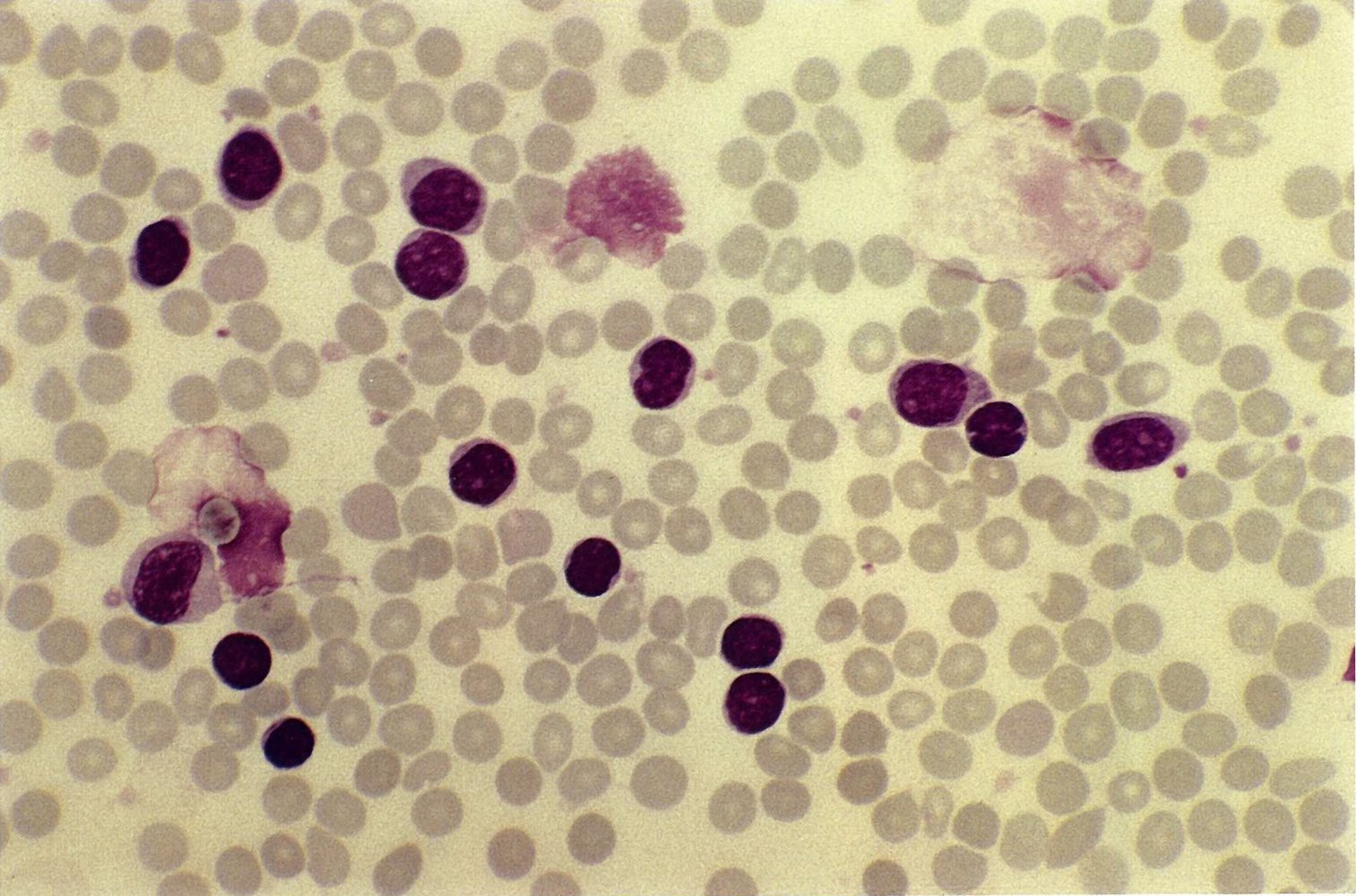
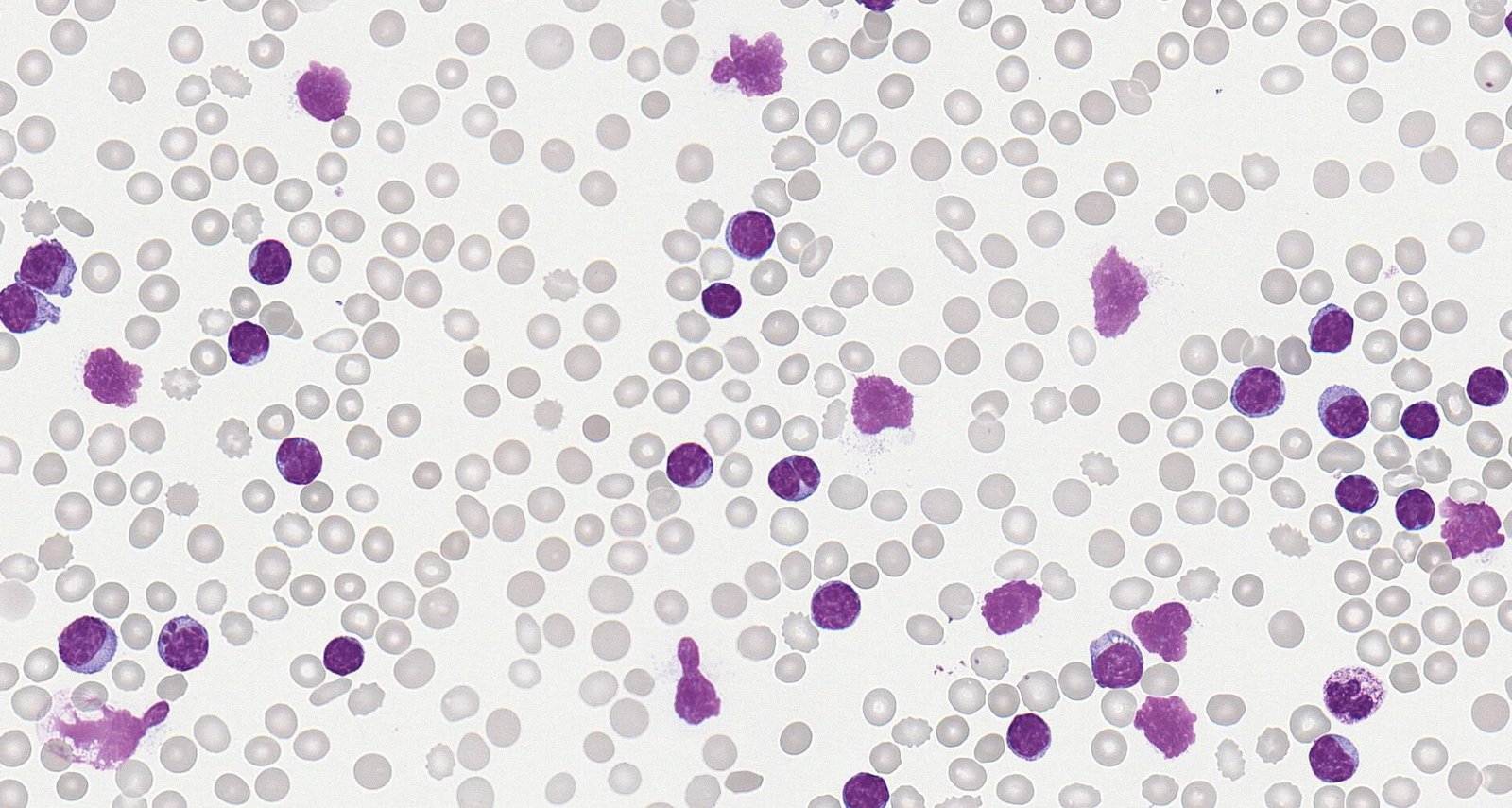
Photomicrograph of a peripheral blood smear (Giemsa stain; high magnification)
An increased number of small lymphocytic (examples indicated by yellow overlay) cells and Gumprecht shadows (also known as “smudge cells;” blue overlay) can be seen among erythrocytes (examples indicated by hatched blue overlay). Gumprecht shadows are ruptured small neoplastic lymphocytes characteristic of but not specific for CLL.
Source: © IMPP
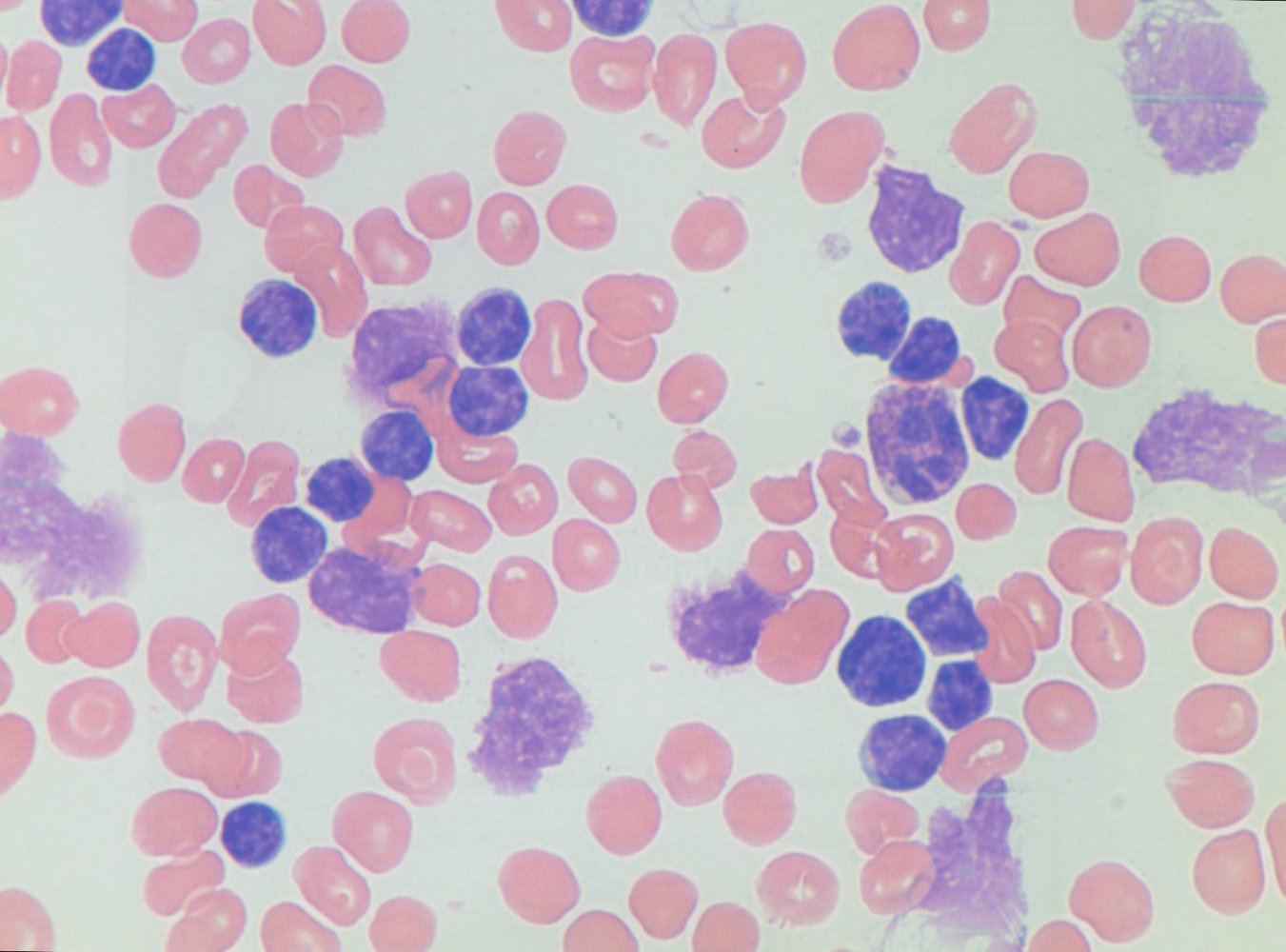
Photomicrograph of a peripheral blood smear (Giemsa stain; high magnification)
Erythrocytes (examples indicated by white arrowheads), a neutrophil (black arrowhead), several small lymphocytes (examples indicated by yellow hatched overlay), and smudge cells (blue overlay) can be seen.
Smudge cells, also known as Gumprecht shadows, are ruptured small neoplastic lymphocytes and are a characteristic but nonspecific feature of CLL.
Source: © IMPP
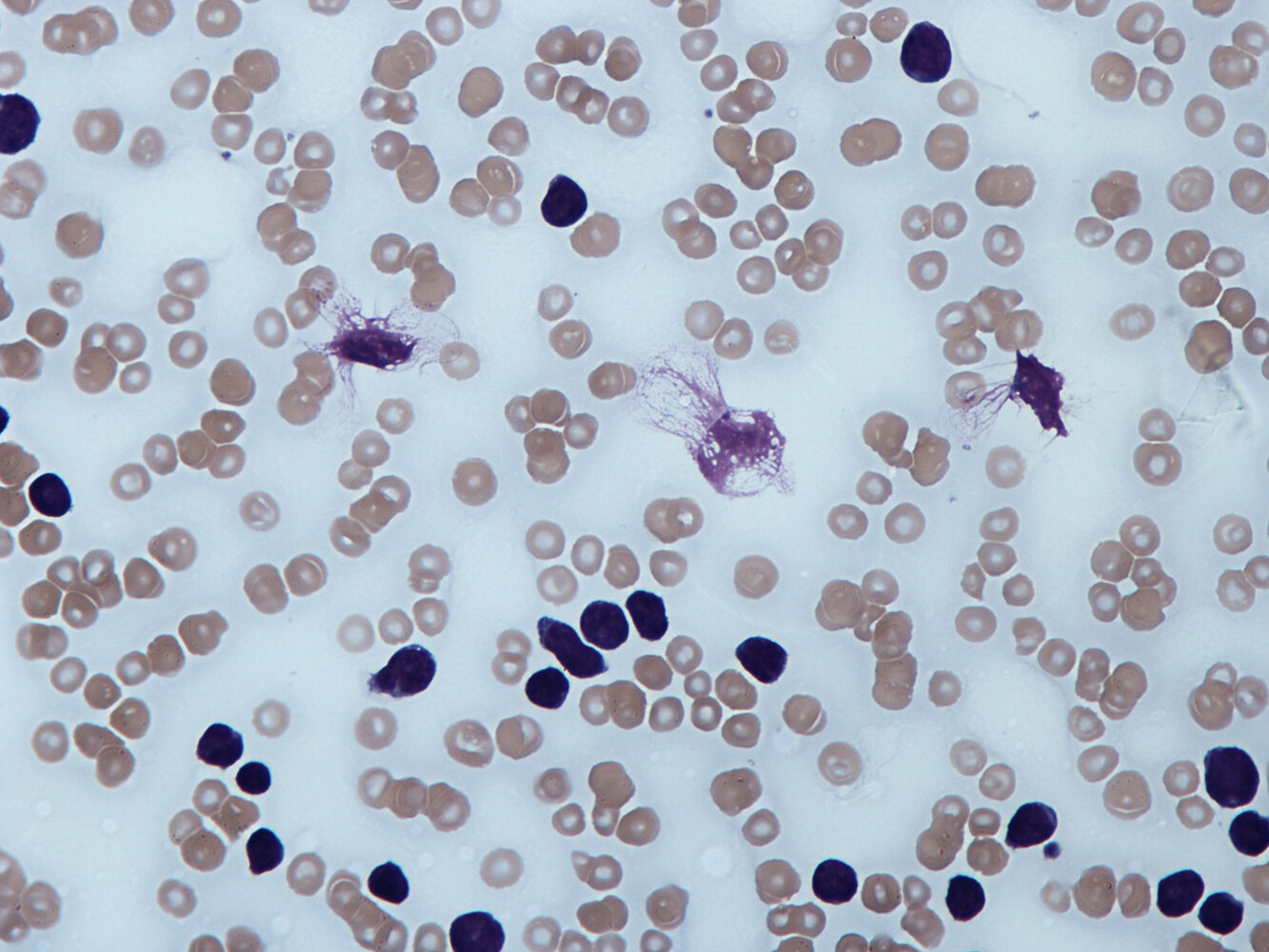
Photomicrograph of a blood smear (H&E stain; high magnification) of a patient after splenectomy
Smudge cells (Gumprecht shadows) are present (red overlay). These artifacts are caused by ruptured mature lymphocytes. There is also a lack of Howell-Jolly bodies in the erythrocytes, which may indicate the presence of an accessory spleen.
The presence of smudge cells is characteristic of chronic lymphocytic leukemia, however, it is a nonspecific finding.
Source: © IMPP
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Prof. Dr. Karl-Anton Kreuzer, Facharzt für Innere Medizin, Hämatologie und Onkologie
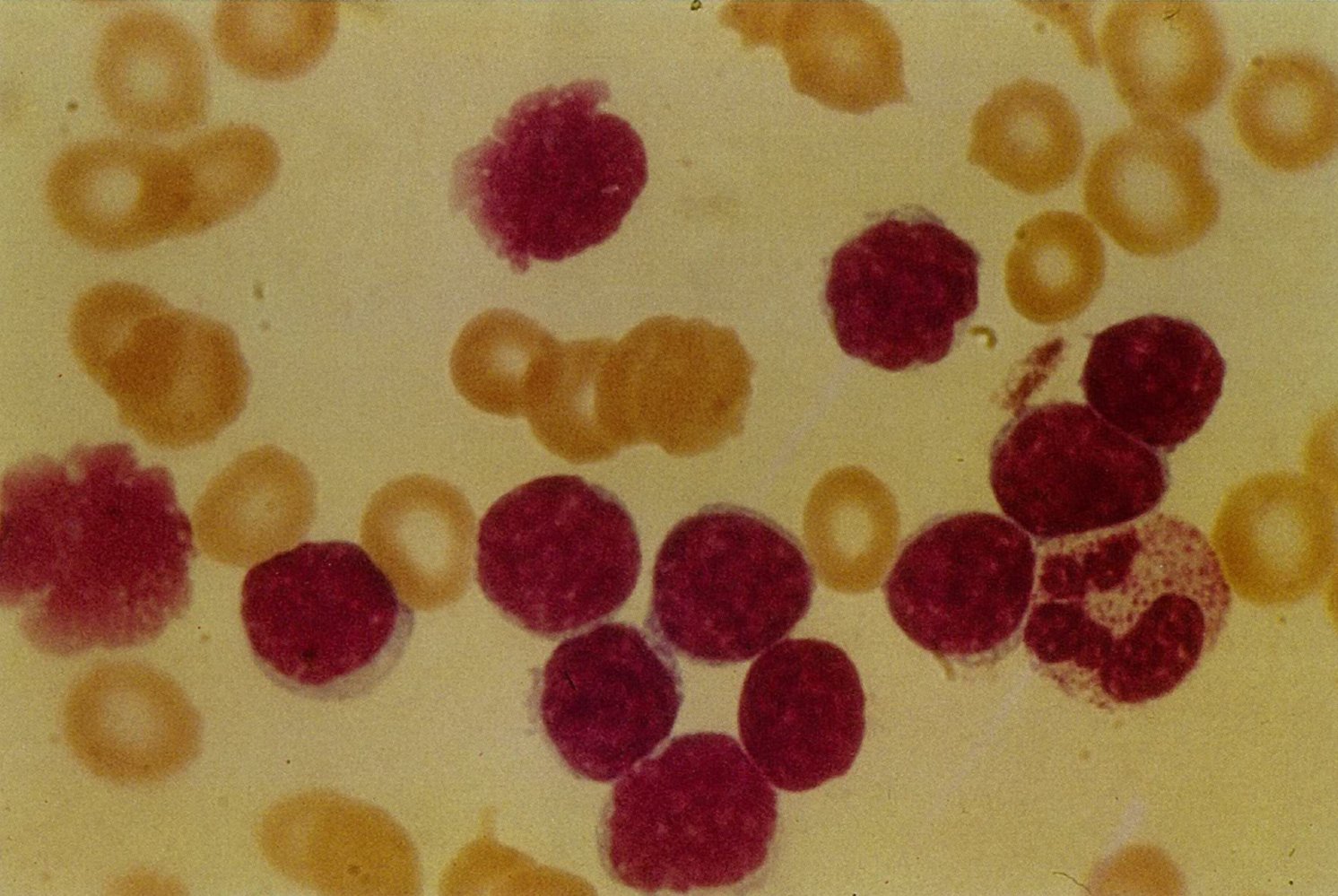
Photomicrograph of a peripheral blood smear (Giemsa stain; high magnification)
The smear shows an increase in lymphocytic cells with minimal cytoplasm and dark round nuclei (examples indicated by yellow overlay). Some of those cells are fragmented (smudge cells; also referred to as “Gumprecht shadows;” blue arrowheads).
Smudge cells are artificially ruptured neoplastic lymphocytes and are a characteristic, but nonspecific, feature of CLL.
Source: “Smear_cells.jpg” by Dr Graham Beards, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
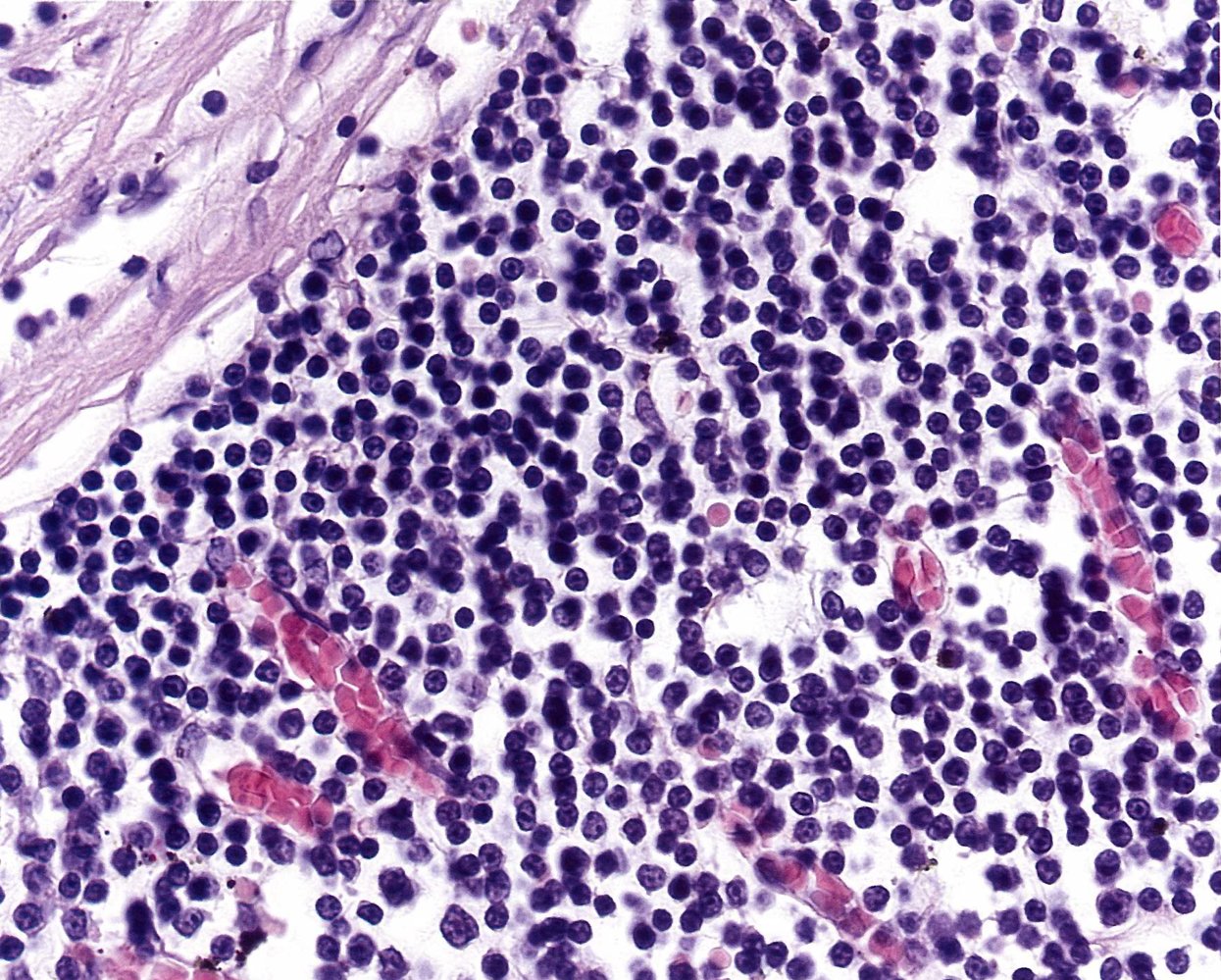
Photomicrograph of a bone marrow specimen (H&E stain; intermediate magnification)
Diffuse bone marrow infiltration with small lymphocytic cells (L) is seen. The cells in CLL typically show scant cytoplasm and are small in diameter, comparable to the size of erythrocytes (R), which can be seen in the sinusoids.
Source: © IMPP
Classification
Rai staging system
| Rai staging system [2][6][9] | |||
|---|---|---|---|
| Rai stage | Modified Rai stage | Findings | |
| 0 | Low risk | Isolated lymphocytosis | |
| I | Intermediate risk | Lymphocytosis | PLUS lymphadenopathy |
| II | PLUS hepatomegaly and/or splenomegaly | ||
| III | High risk | PLUS anemia (Hb < 11 g/dL) | |
| IV | PLUS thrombocytopenia (platelets < 100,000/mm3) | ||
Other staging systems [2]
- Binet staging system: commonly used for staging and informing treatment decisions in European countries
- CLL international prognostic index (CLL-IPI): risk stratification score based on age, clinical stage (Rai or Binet), and the presence of prognostic molecular markers
| Binet staging system [2] | ||
|---|---|---|
| Definition | Additional findings | |
| Stage A |
|
|
| Stage B |
|
|
| Stage C |
|
|
Differential diagnoses
- Acute lymphoblastic leukemia (ALL)
- Autoimmune hemolytic anemia (AIHA)
- Mantle cell lymphoma
- Hairy cell lymphoma
The differential diagnoses listed here are not exhaustive.
Treatment
General principles [2][10]
Management should be specialist guided. Consider enrollment in a clinical trial.
-
Indications for anticancer therapy : based on disease risk (Rai staging) and disease activity [2]
-
Low-risk disease (Rai stage 0)
- Expectant management
- Regular follow-ups to assess for disease progression and indications for treatment [10]
- Intermediate risk disease (Rai stage I or II)
- Consider expectant management if stable and asymptomatic.
- Medical therapy: indicated for progressive or symptomatic disease (i.e., active disease )
- High-risk disease (Rai stage III or IV): medical therapy
-
Low-risk disease (Rai stage 0)
-
Anticancer therapy may include:
- Targeted therapy, e.g., ibrutinib, rituximab, alemtuzumab
- Chemoimmunotherapy, e.g., FCR: fludarabine, cyclophosphamide, rituximab
- Allogeneic HSCT: currently the only curative treatment option (not routinely performed)
CLL is a malignancy with a slow rate of cell division and disease progression. Treatment of low-risk disease is usually not recommended and is unlikely to extend survival.
Pretreatment evaluation [2]
- Clinical assessment: physical examination, and functional status assessment (e.g., ECOG score)
-
Laboratory studies
- CMP: to document baseline organ function [2][5]
- Repeat cytogenetic testing; see “Prognostic markers in CLL.”
- Immunoglobulin levels: to evaluate for hypogammaglobulinemia [5][6]
- Infectious disease serology: for HBV, HCV, HIV, and CMV [2][11]
- Direct Coombs test: to assess for AIHA
-
Imaging
- Chest x-ray: to evaluate for mediastinal lymphadenopathy
- Further imaging is not routinely required for diagnosis unless clinically indicated.
- Further testing (e.g., CT scan, bone marrow biopsy): may be necessary for patients enrolling in clinical trials.
 score")
Pharmacotherapy
- The pretreatment evaluation is used to determine which regimen is used.
- In most patients with CLL, a BTK inhibitor or BCL-2 inhibitor is the first-line treatment. [11][12][13]
| Overview of pharmacotherapy for CLL [11][14] | |||
|---|---|---|---|
| Therapy | Examples | Indications | |
| Targeted therapies | Small molecule inhibitors |
|
|
| Monoclonal antibodies |
|
|
|
| Chemoimmunotherapy |
|
|
|
Allogeneic stem cell transplantation [15][16]
- Curative treatment for CLL
- High-risk procedure with a 20% mortality rate [1][15][16]
- Consider for young patients with few or no comorbidities and:
- Del(17p) and/or TP53 mutation
- Disease that is refractory to targeted therapy
Supportive care [2][16]
Evaluate for and manage any complications, including:
-
Infectious diseases
- Ensure routine vaccinations (e.g., influenza, pneumococcus) are up-to-date.
- Consider infection prophylaxis (e.g., HHV, VZV, and PCP prophylaxis ). [16]
- Consider IVIG therapy for patients with hypogammaglobulinemia who have recurrent infections.
- Autoimmune cytopenias: Manage AIHA and ITP (e.g., with glucocorticoids) as needed.
- Complications of anticancer therapy: Consider the need for G-CSF for anticancer therapy-induced myelosuppression.
Live vaccines are contraindicated in patients with CLL because of the risk of severe complications. [2]
Infectious diseases are common in patients with CLL. Evaluating for and managing infectious diseases can reduce the risk of severe illness and complications. [16]
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Complications
- Immunosuppression with subsequent infections (most common cause of death)
- Secondary malignancies
- Hyperviscosity syndrome
- Autoimmune hemolytic anemia (of both the warm and cold agglutinin type)
-
Richter transformation or Richter syndrome: transformation into a high-grade NHL (usually diffuse large B cell lymphoma)
- Occurrence: ∼ 5% of cases
- Diagnostic indicators:
- Rapidly progressive lymphadenopathy → lymph node biopsy required
- New onset of B symptoms
- ↑ LDH
- Treatment: similar to symptomatic CLL and advanced stages
References:[17][18]
We list the most important complications. The selection is not exhaustive.
Prognosis
Prognostic factors [6]
- Older age is associated with a poor overall survival rate.
- Rai staging
- Adverse prognostic markers in CLL, e.g.:
- Del(17p13)
- Elevated β2-microglobulin level
- Blood lymphocyte doubling time: Rapid doubling is associated with a high risk of disease progression.
External Resources
- 2018 International Workshop on Chronic Lymphocytic Leukemia (iwCLL) Guidelines for Diagnosis, Indications for Treatment, Response Assessment, and Supportive Management of CLL
- 2021 European Society for Medical Oncology (ESMO), Chronic Lymphocytic Leukemia: ESMO Clinical Practice Guidelines for Diagnosis, Treatment, and Follow-Up
References
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Hallek M, Cheson BD, Catovsky D, et al. "iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL.". Blood. 131(25). :2745-2760. (2018)
- Mir MA. "Chronic Lymphocytic Leukemia (CLL)". WebMD. http://emedicine.medscape.com/article/199313. [2017-02-03]
- Rai KR, Sawitsky A, Cronkite EP, et al. "Clinical staging of chronic lymphocytic leukemia.". Blood. 46(2). :219-34. (1975)
- Nabhan C, Rosen ST. "Chronic lymphocytic leukemia: a clinical review". JAMA. 312(21). :2265-2276. (2014)
- Rai KR, Stilgenbauer S. "Clinical Presentation, Pathologic Features, Diagnosis, and Differential Diagnosis of Chronic Lymphocytic Leukemia". UpToDate. UpToDate. https://www.uptodate.com/contents/clinical-presentation-pathologic-features-diagnosis-and-differential-diagnosis-of-chronic-lymphocytic-leukemia. [2018-02-01]
- Caligiuri M, Levi MM, Kaushansky K, et al. "Williams Hematology, 9E". McGraw-Hill Education / Medical. (2015). ISBN: 9780071833004
- Tsang M, Parikh SA. "A Concise Review of Autoimmune Cytopenias in Chronic Lymphocytic Leukemia". Curr Hematol Malig Rep. 12(1). :29-38. (2017)
- Mitra A, Dwyre DM, Schivo M, et al. "Leukoerythroblastic reaction in a patient with COVID‐19 infection". Am J Hematol. 95(8). :999-1000. (2020)
- Davis AS, Viera AJ, Mead MD. "Leukemia: an overview for primary care". Am Fam Physician. 89(9). :731-738. (2014)
- Eichhorst B, Robak T, Montserrat E, et al. "Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up". Ann Oncol. 32(1). :23-33. (2021)
- Woyach JA, Ruppert AS, Heerema NA, et al. "Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL". N Engl J Med. 379(26). :2517-2528. (2018)
- Burger JA, Tedeschi A, Barr PM, et al. "Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia". N Engl J Med. 373(25). :2425-2437. (2015)
- Brem EA, O’Brien S. "Frontline Management of CLL in 2021". JCO Oncol Pract. 18(2). :109-113. (2022)
- Kharfan-Dabaja MA, Kumar A, Hamadani M, et al. "Clinical Practice Recommendations for Use of Allogeneic Hematopoietic Cell Transplantation in Chronic Lymphocytic Leukemia on Behalf of the Guidelines Committee of the American Society for Blood and Marrow Transplantation". Biol Blood Marrow Transplant. 22(12). :2117-2125. (2016)
- Stilgenbauer S, Furman RR, Zent CS. "Management of Chronic Lymphocytic Leukemia". Am Soc Clin Oncol Educ Book. :164-175. (2015)
- Dearden C. "Disease-specific complications of chronic lymphocytic leukemia". Hematology. 2008(1). :450-456. (2008)
- Tadmor T, Shvidel L, Bairey O, et al. "Richter's transformation to diffuse large B-cell lymphoma: A retrospective study reporting clinical data, outcome, and the benefit of adding rituximab to chemotherapy, from the Israeli CLLStudy Group". Am J Hematol. 89(11). :E218-E222. (2014)
- "CLL Staging". http://www.lls.org/leukemia/chronic-lymphocytic-leukemia/diagnosis/cll-staging. [2017-04-14]
- Wierda WG, Byrd JC, Abramson JS, et al. "Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma, Version 4.2020". Journal of the National Comprehensive Cancer Network. 18(2). :185-217. (2020)
- Hallek M, Cheson BD, Catovsky D, et al. "Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines.". Blood. 111(12). :5446-56. (2008)
- Rosenthal A. "Small Molecule Inhibitors in Chronic Lymphocytic Lymphoma and B Cell Non-Hodgkin Lymphoma". Current Hematologic Malignancy Reports. 12(3). :207-216. (2017)