Summary
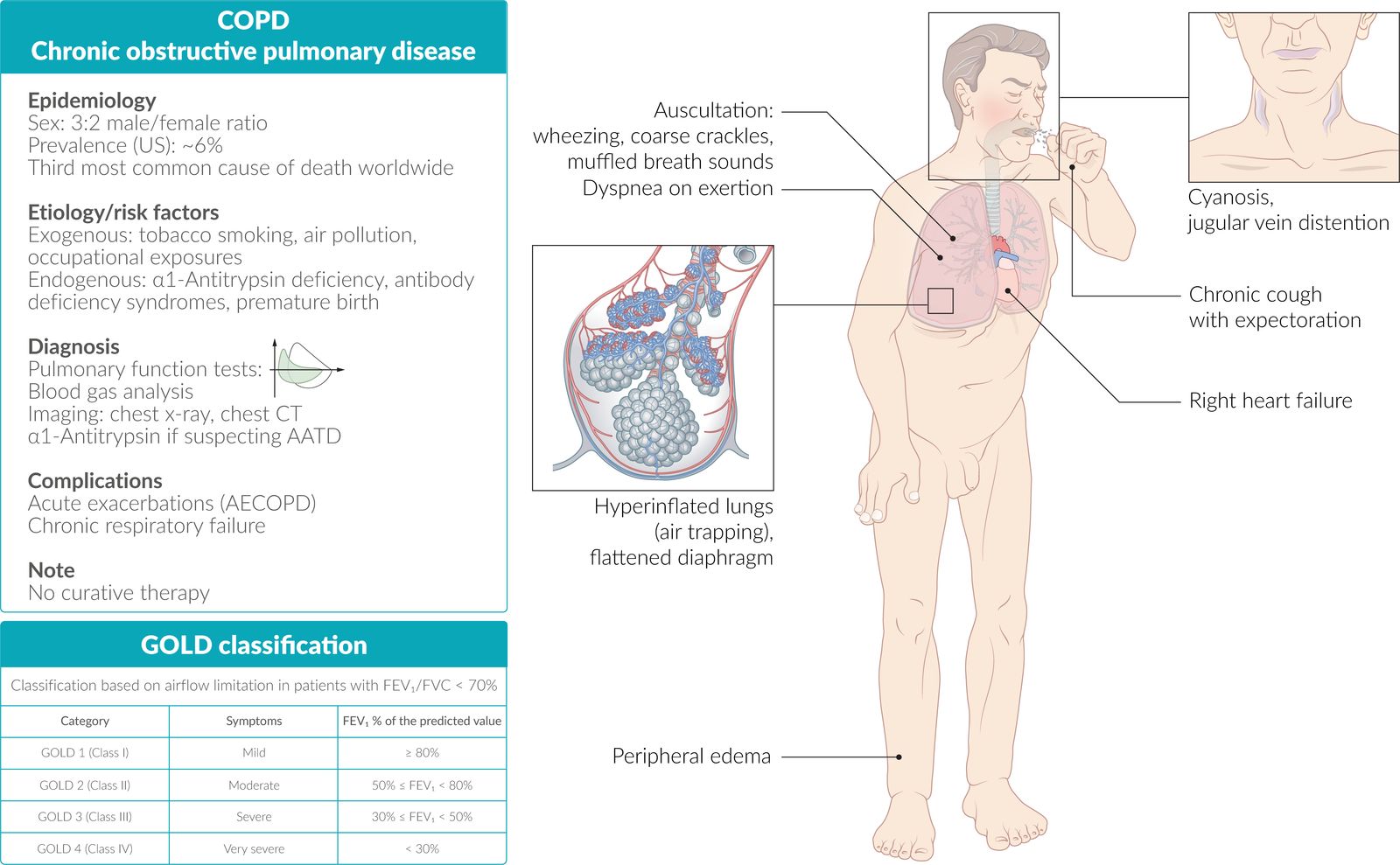
Chronic obstructive pulmonary disease (COPD) is characterized by chronic respiratory symptoms resulting from airflow obstruction and alveolar gas exchange abnormalities. It is predominantly caused by inhaled toxins (e.g., tobacco smoke or air pollution). Some individuals are genetically predisposed to COPD, particularly those with α1-antitrypsin deficiency (AATD). COPD begins with chronic airway inflammation, which usually progresses to emphysema, a condition that is characterized by permanent dilatation of pulmonary air spaces distal to the terminal bronchioles. These changes cause a loss of diffusion area, which can lead to inadequate oxygen absorption (hypoxemia) and CO2 release (hypercapnia). Clinical features include dyspnea and productive cough and, in later stages, tachypnea, tachycardia, and cyanosis. Diagnosis is primarily based on clinical presentation and pulmonary function tests (PFTs), which typically show a decreased ratio of forced expiratory volume (FEV) to forced vital capacity (FVC). Imaging studies are helpful in assessing disease severity and the extent of possible complications. Treatment options mainly consist of short-acting and long-acting bronchodilators and inhaled corticosteroids. Individuals with advanced disease may benefit from oxygen supplementation and/or noninvasive ventilation. COPD can cause complications such as pulmonary hypertension or respiratory failure. The most significant complication is acute exacerbation of COPD.

© AMBOSS
Definitions
- Chronic obstructive pulmonary disease: a lung condition characterized by persistent respiratory symptoms (cough, dyspnea) and airflow limitation (postbronchodilator FEV1:FVC ratio < 0.70), which is caused by a combination of small airway obstruction and parenchymal destruction
- Chronic bronchitis: productive cough for at least 3 months per year for 2 consecutive years that cannot be explained by an alternative diagnosis
- Emphysema: permanent dilatation of pulmonary air spaces distal to the terminal bronchioles that is caused by the destruction of the alveolar walls and pulmonary capillaries required for gas exchange
- Preserved ratio impaired spirometry (PRISm): A term describing individuals with postbronchodilator FEV1:FVC ratio ≥ 0.70 but an FEV1 < 80% of the predicted value.
Chronic bronchitis (a clinically defined condition) and emphysema (an anatomically defined condition) often occur simultaneously in patients with COPD. [2]
Epidemiology
- Sex: 3:2 male/female ratio [3][4]
- Prevalence: 6% [5]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
Exogenous factors
-
Tobacco use ; [6]
- Smoking is the major risk factor for COPD, but those who have quit ≥ 10 years ago are not at increased risk. [7]
- Passive smoking
-
Exposure to air pollution or fine dusts [8]
- Nonorganic dust: such as industrial bronchitis in coal miners [9]
- Organic dust: ↑ incidence of COPD in areas where biomass fuel (e.g., wood, animal dung) is regularly burned indoors
Endogenous factors
-
Lung growth and development abnormalities [1]
- Recurrent pulmonary infections and tuberculosis
- Premature birth [10]
- α1-antitrypsin deficiency
- Airway hyperresponsiveness
- Antibody deficiency syndrome (e.g., IgA deficiency)
- Primary ciliary dyskinesia (e.g., Kartagener syndrome)
Classification
GOLD classification [1]
GOLD spirometric grades inform the prognosis of a patient; GOLD groups guide pharmacological management.
GOLD grades
| GOLD spirometric grades [1] | |
|---|---|
| Grade | Postbronchodilator FEV1% of the predicted value |
| GOLD 1: mild | ≥ 80% |
| GOLD 2: moderate | 50–79% |
| GOLD 3: severe | 30–49% |
| GOLD 4: very severe | < 30% |
Cutoff points between GOLD spirometric grades according to the FEV1%: 30 + 50 = 80
GOLD groups [1]
| GOLD group assessment [1] | |||
|---|---|---|---|
| Group | Exacerbations in the past year | Severity of symptoms | |
| mMRC dyspnea scale | CAT score | ||
| GOLD group A |
|
|
|
| GOLD group B |
|
|
|
| GOLD group E |
|
|
|
Pathophysiology
COPD is characterized by chronic airway inflammation and tissue destruction. [6][11]
Chronic inflammation
It results from significant exposure to noxious stimuli, increased oxidative stress (most commonly due to cigarette smoke) as well as by increased release of reactive oxygen species by inflammatory cells.
-
Increased number of neutrophils, macrophages, and CD8+ T lymphocytes → release of cytokines → amplification of inflammation and induction of structural changes of lung parenchyma (e.g., via stimulation of growth factor release)
- CD8+ T lymphocytes mediate inflammation in individuals with COPD.
- CD4+ T lymphocytes and eosinophils mediate inflammation in individuals with bronchial asthma.
- Overproduction of growth factor → peribronchiolar fibrosis → narrowing of airway → obliteration → emphysema (airflow limitation)
-
Promotion of goblet cell proliferation and hypertrophy, mucus hypersecretion, and impaired ciliary function → chronic productive cough
- Reid index is the ratio of the thickness of the submucosal mucus-secreting glands to the thickness between the epithelium and cartilage in the bronchial tree.
- Reid index > 0.5 is characteristic of chronic bronchitis. [12]
- Smooth muscle hyperplasia of the small airways and pulmonary vasculature (mainly due to hypoxic vasoconstriction) → pulmonary hypertension → cor pulmonale
Tissue destruction [13]
- Bronchopulmonary inflammation → ↑ proteases
-
Nicotine use (or other noxious stimuli) inactivates protease inhibitors (especially α1-antitrypsin) → imbalance of protease and antiprotease → ↑ elastase activity → loss of elastic tissue and lung parenchyma (via destruction of the alveolar walls), which causes:
- Enlargement of airspaces → ↓ elastic recoil and ↑ compliance of the lung → ↓ tethering of small airways → expiratory airway collapse and obstruction → air trapping and hyperinflation → ↓ ventilation (due to air-trapping) and ↑ dead space → ↓ DLCOand ↑ ventilation-perfusion mismatch (V/Q) → hypoxemia and hypercapnia
- Pulmonary shunt and ↓ blood volume in pulmonary capillaries → ↑ number of alveoli that are ventilated but not perfused (↑ dead space) → ↓ DLCO and ↑ V/Q → hypoxemia and hypercapnia
- Imbalance of oxidants and anti-oxidants and an overabundance of free radicals → chronic inflammation and inactivation of anti-elastase → breakdown of elastic tissue.

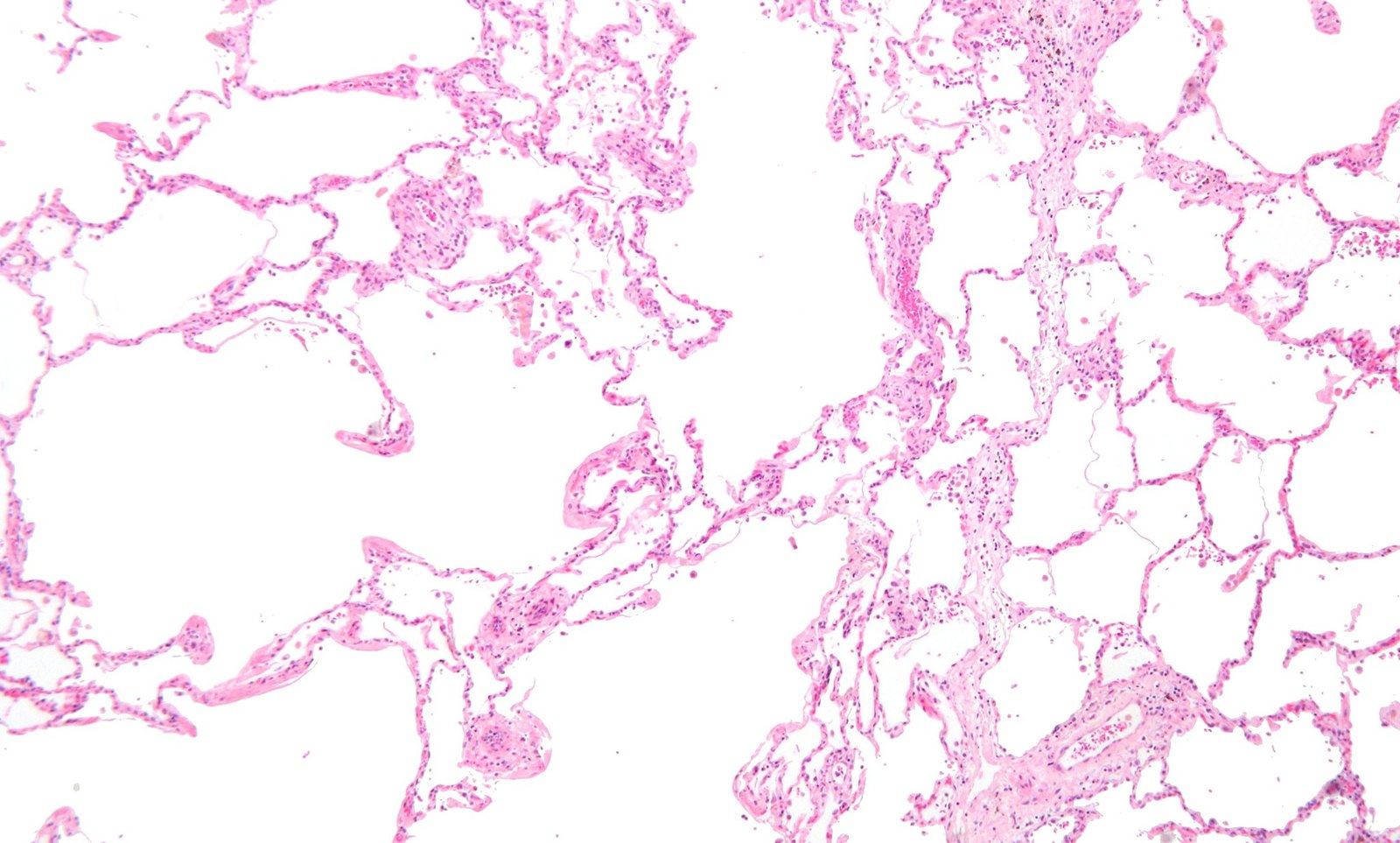
Microscopic image of lung tissue (H&E stain)
On the right side of this image, there are relatively preserved alveoli with normal airspace (NAS, dark blue overlay).
On the left side, alveoli architecture is destroyed and the airspace is enlarged (ENS, turquois overlay).
In the lower part of the images, capillaries with thick walls can be seen (arrows)
These findings indicate pulmonary emphysema.
Source: “Emphysema low mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Clinical features
Symptoms are minimal or nonspecific until the disease reaches an advanced stage.
Presenting findings [6]
- Chronic cough with expectoration (expectoration typically occurs in the morning)
-
Dyspnea and tachypnea
- Initial stages: only on exertion
- Advanced stages: continuously
-
Pursed lip breathing
- The patient breathes in through the nose and breathes out slowly through pursed lips.
- This style of breathing increases airway pressure and prevents bronchial collapse during the last phase of expiration.
- More commonly seen in patients with emphysema
- Prolonged expiratory phase, end-expiratory wheezing, crackles, muffled breath sounds, and/or coarse rhonchi on auscultation
- Cyanosis due to hypoxemia
- Tachycardia
Features of advanced COPD [14]
- Congested neck veins
- Barrel chest: This deformity is most commonly seen in individuals with emphysema.
- Asynchronous movement of the chest and abdomen during respiration
- Use of accessory respiratory muscles due to diaphragmatic dysfunction
- Hyperresonant lungs, reduced diaphragmatic excursion, and relative cardiac dullness on percussion
- Decreased breath sounds on auscultation: “silent lung”
- Peripheral edema (most often ankle edema)
- Right ventricular hypertrophy with signs of right heart failure and cor pulmonale
- Hepatomegaly
- Often weight loss and cachexia
- Secondary polycythemia
- Confusion: due to hypoxemia and hypercapnia
- Nail clubbing in the case of certain comorbidities (e.g., bronchiectasis, pulmonary fibrosis, lung cancer) [15]
Nail clubbing is not a finding specific to COPD; its presence usually suggests comorbidities such as bronchiectasis, pulmonary fibrosis, or lung cancer.
Pink puffer and blue bloater [14]
According to their clinical appearance, patients with COPD are often categorized as either “Pink Puffer” or “Blue Bloater”.
| Pink puffer vs. blue bloater | ||
|---|---|---|
| Pink Puffer | Blue Bloater | |
| Main pathomechanism |
|
|
| Clinical features |
|
|
| PaO2 |
|
|
| PaCO2 |
|
|

Features of COPD due to AATD
- Age of onset is generally younger (< 60 years)
- Also, often have hepatic signs and symptoms (jaundice) related to hepatitis or cirrhosis

Prominent facial features commonly seen in patients with chronic bronchitis are obesity and signs of right heart failure (e.g., cyanosis, edema).
Source: © IMPP
Subtypes and variants
Emphysema subtypes
Emphysema is characterized by the destruction of lung parenchyma and is often seen in patients with advanced pulmonary disease. The presence of emphysema does not necessarily correlate with spirometric findings. Emphysema can be divided into the following subtypes: [1][16]
-
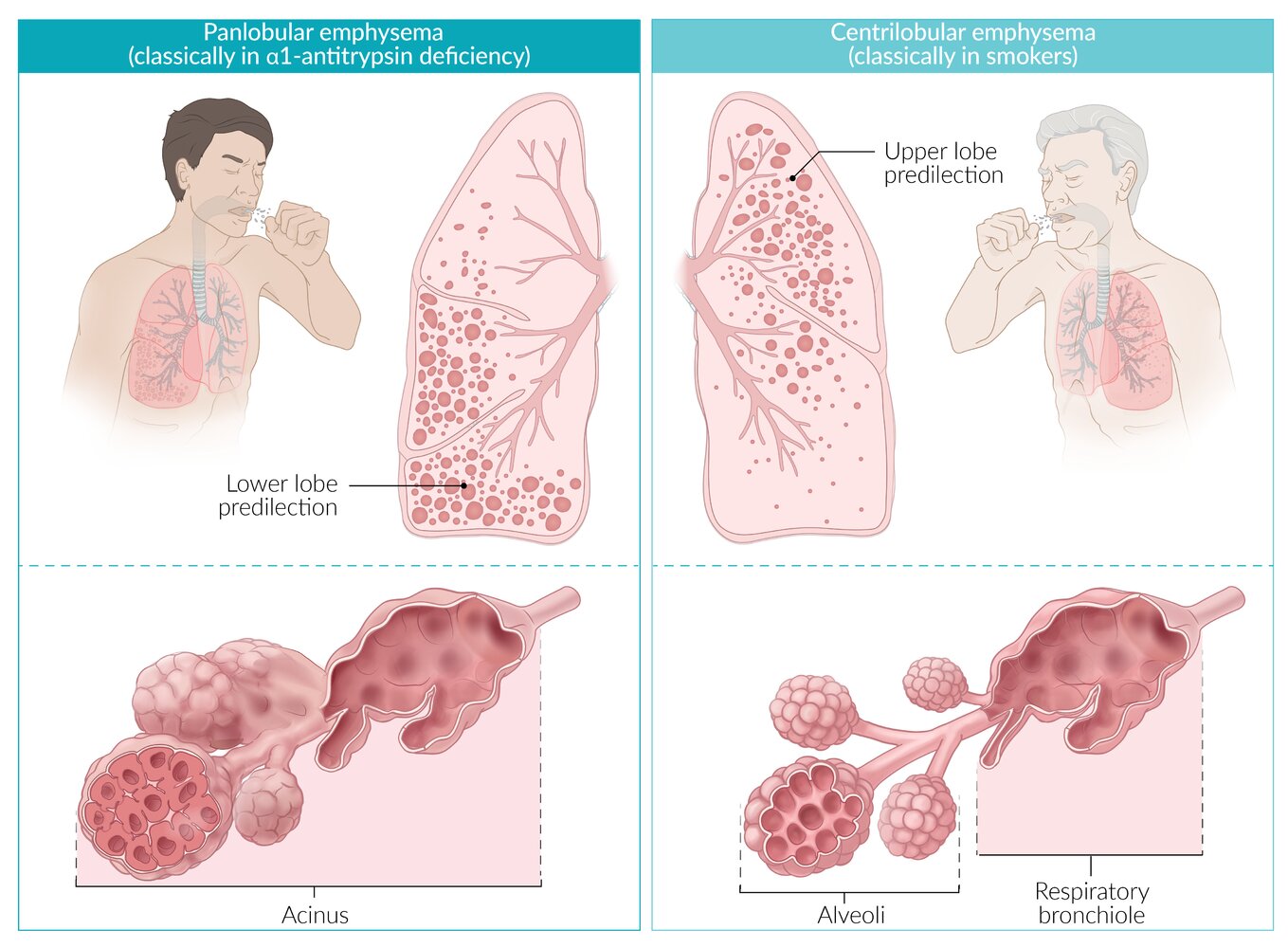
Centrilobular emphysema (centriacinar emphysema)
- Most common type of emphysema
- Classically seen in smokers
- Characterized by the destruction of the respiratory bronchiole (central portion of the acinus); spares distal alveoli
- Usually affects the upper lobes
-
Panlobular emphysema (panacinar emphysema)
- Rare type of emphysema
- Associated with AATD
- Characterized by the destruction of the entire acinus (respiratory bronchiole and alveoli)
- Usually affects the lower lobes
-
Other subtypes
-
Cicatricial emphysema
- Mainly caused by exposure to quartz dust
- Results in chronic inflammation and nodular scar formation
-
Giant bullous emphysema
- Characterized by large bullae (congenital or acquired) that extrude into the surrounding tissue
- Bullae may rupture, leading to pneumothorax.
- Depending on the shape of the bullae, resection should be considered.
-
Age-related emphysema
- Loss of pulmonary elasticity with age may lead to an emphysematous lung.
- Considered a normal consequence of aging
-
Cicatricial emphysema
“Smoke rises up:” Centriacinar emphysema is associated with smoking and primarily involves the upper lobes of the lungs.


© AMBOSS
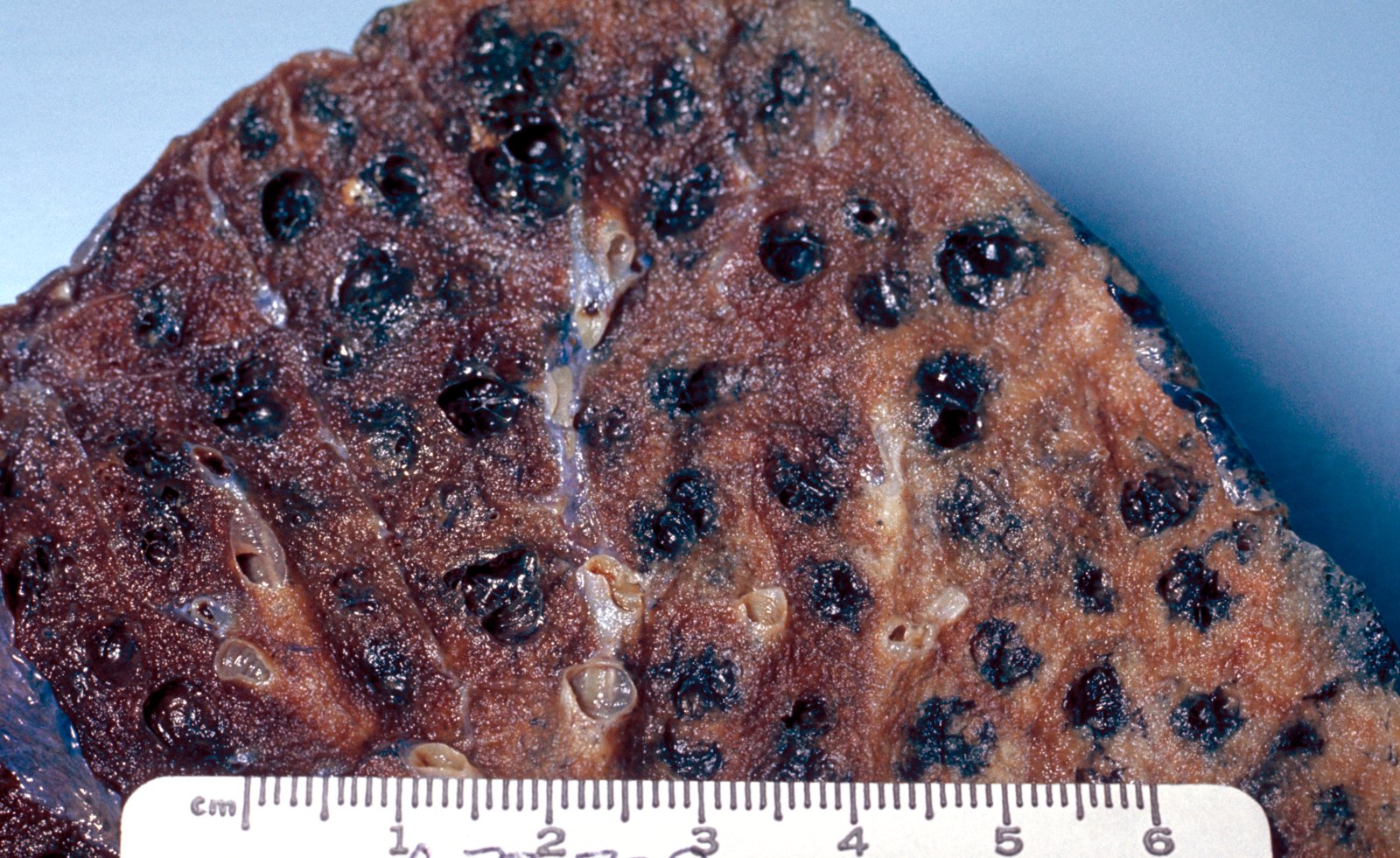
Gross specimen of peripheral lung tissue
There are emphysematous acini (green overlay) distributed throughout normal pulmonary parenchyma.
Source: "ID#: 865", CDC/ Dr. Edwin P. Ewing, Jr., Centers for Disease Control and Prevention licensed under Public Domain
Diagnosis
Approach [1]
- Suspect COPD in patients with either:
- Typical symptoms of COPD
- COPD risk factors
- Obtain spirometry to confirm significant airflow limitation (FEV1:FVC < 70%).
- Screen for AATD.
- Consider additional diagnostic testing as indicated, e.g.:
- Advanced PFTs
- Chest imaging
The USPSTF recommends against screening asymptomatic adults for COPD. The GOLD guideline recommends screening with spirometry in patients undergoing annual lung cancer screening with low-dose CT scans and patients with incidental imaging findings consistent with COPD. [1][17]
Initial tests [1][2]
-
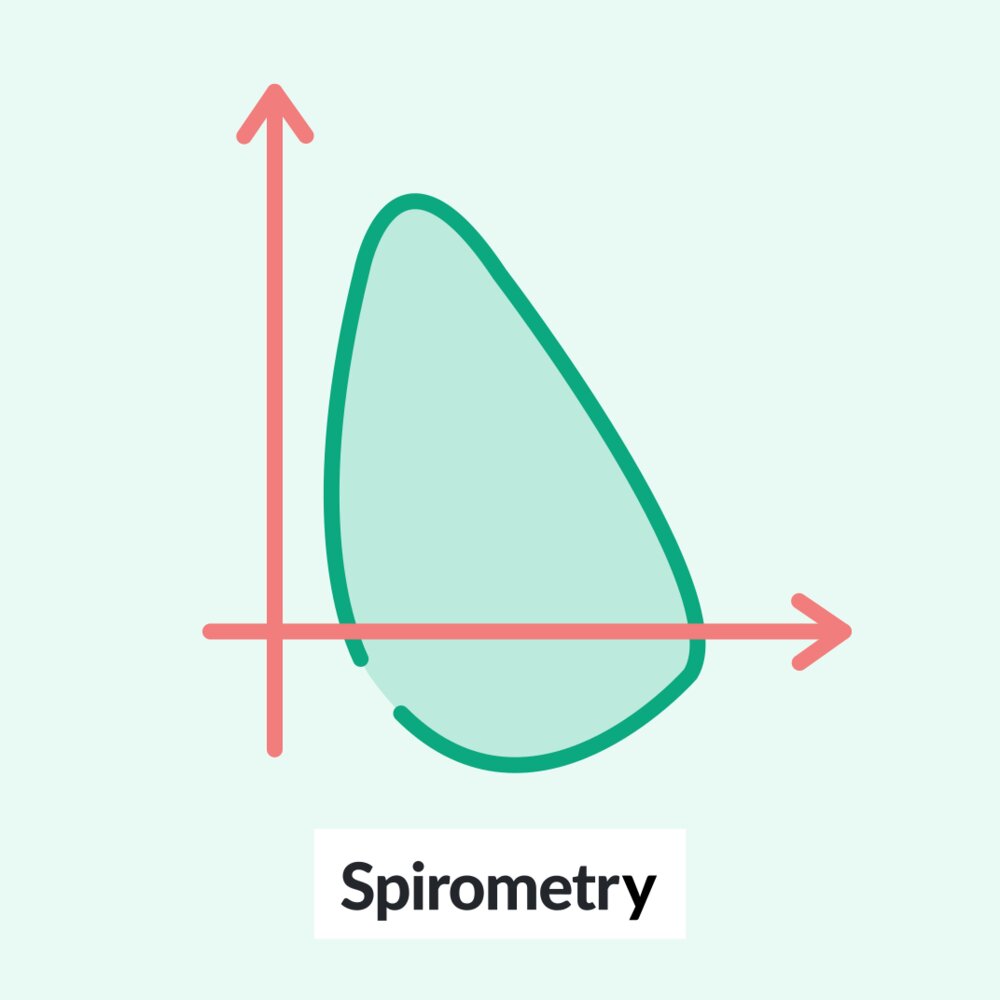
Spirometry
- FEV1:FVC < 70% after bronchodilator inhalation confirms the diagnosis.
- ↓ FEV1 (FEV1 % of the predicted value determines the GOLD spirometric grade.)
- Normal or ↓ FVC
- Serum AAT level: Screen all patients with confirmed COPD for AATD upon initial diagnosis.
“A COP with low FEVer”: FEV1 for COPD patients.
Additional testing
Advanced pulmonary function testing
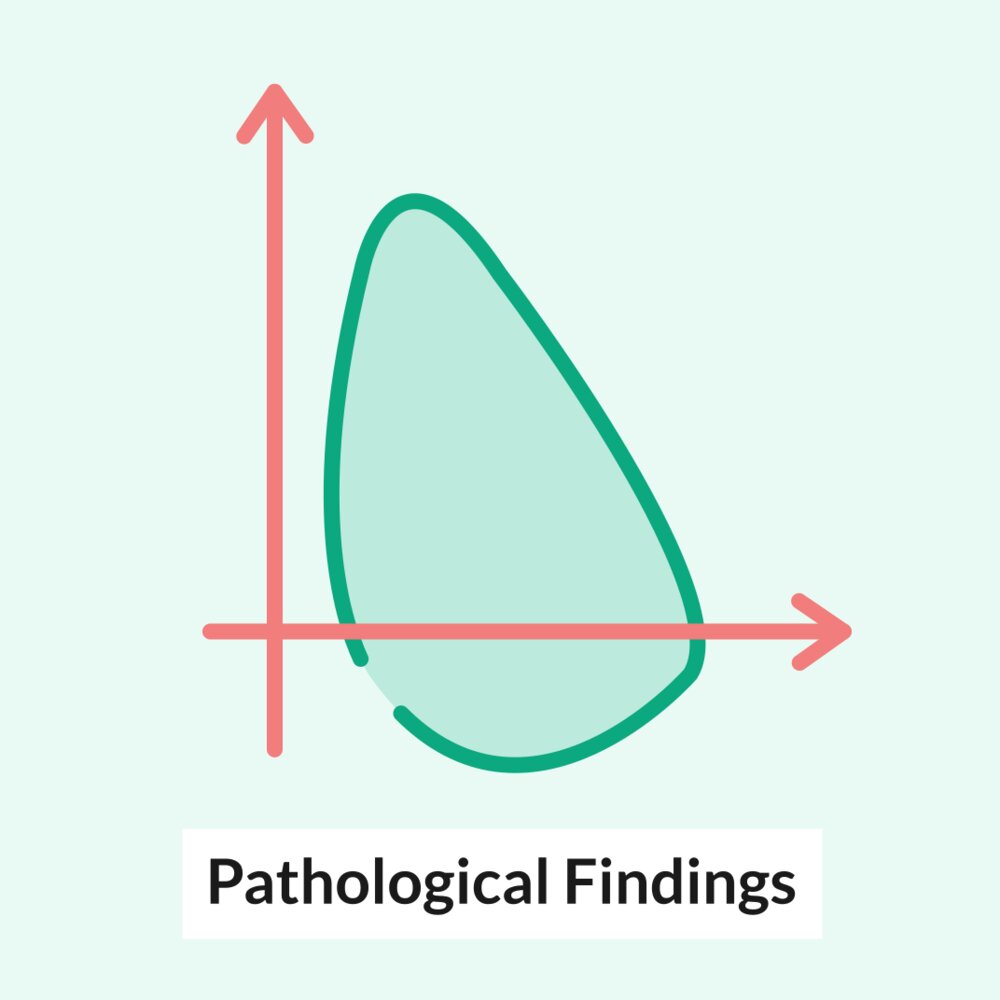
Characteristic changes are observed in patients with significant emphysema and small airway abnormalities.
-
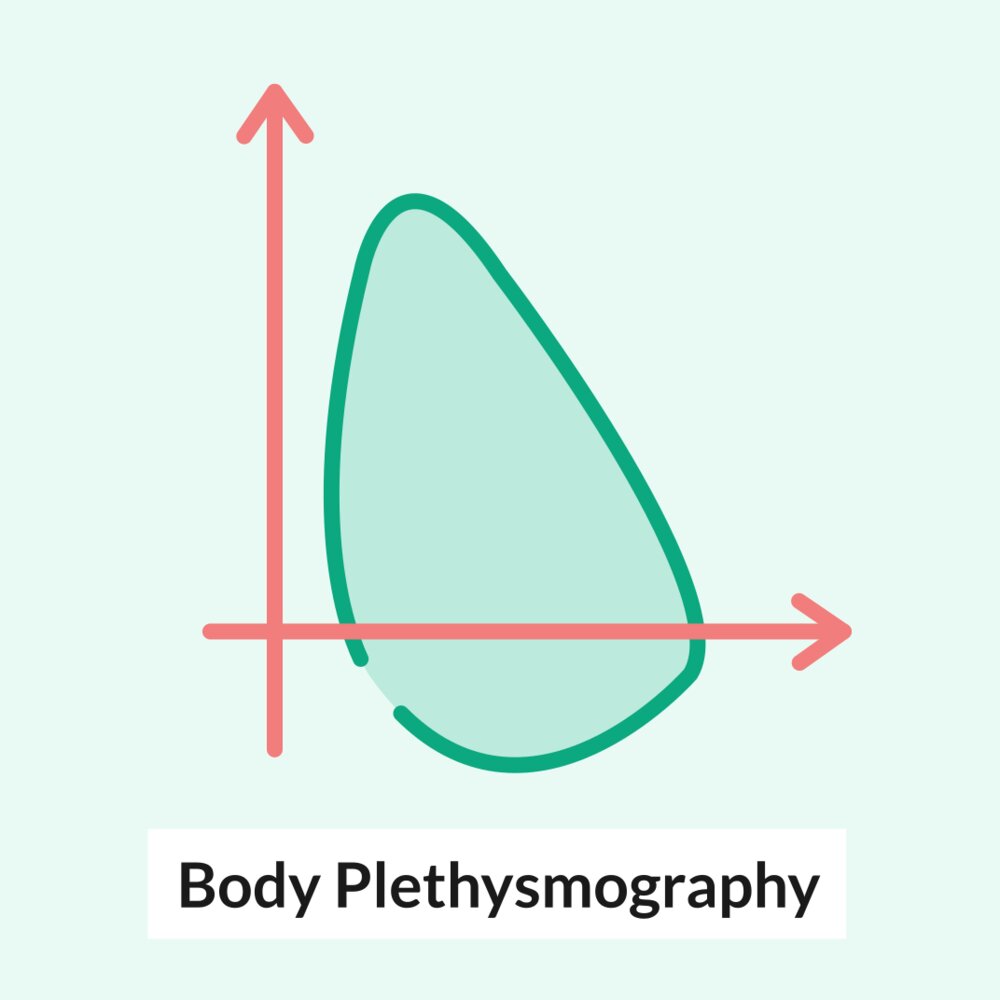
Body plethysmography
- ↑ Total lung capacity (TLC)
- ↑ Functional residual capacity (FRC)
- ↑ Residual volume (RV)
- Single-breath diffusing capacity: ↓ DLCO
- Postbronchodilator test: A negative response (change in FEV1 < 12%) is more common in patients with COPD than asthma (see “COPD vs. asthma”). [18][19]
Reversibility of bronchoconstriction is not a reliable factor for differentiating between COPD and asthma. [1]




Assessment for respiratory failure
-
Pulse oximetry
- Obtain in patients with signs of respiratory distress or signs of right heart failure.
- Measure at rest and on ambient air or usual oxygen prescription.
-
ABG
- Obtain in patients with SO2 < 92% and/or acute illness (e.g., altered mental status, AECOPD).
- Findings
- May show hypoxemic respiratory failure (↓ PO2) with or without hypercapnic respiratory failure (↑ PCO2)
- Chronic hypercapnia due to CO2 trapping is common in patients with severe COPD.
Chest imaging [1][2]
Chest imaging is not needed for diagnosis; consider based on clinical context to assess for alternative diagnoses, comorbidities, or complications.
-
Chest x-ray findings in COPD
- Signs of pulmonary hyperinflation
- Increased anteroposterior diameter; (barrel chest)
- Pushed down and flattened diaphragm
- Horizontal ribs and widened intercostal spaces
- Hyperlucency of lung tissue (decreased lung markings)
- Long and narrow heart shadow
- Signs of bullous emphysema: parenchymal bullae or pulmonary blebs
- Signs of pulmonary hyperinflation
-
CT chest findings
- Similar to CXR findings; may additionally reveal characteristic patterns of emphysema
- Panacinar emphysema: common in patients with AATD
- Centriacinar emphysema: common in patients with COPD and a history of tobacco use
- May show signs of bronchiectasis, e.g., thickened bronchial walls
- Similar to CXR findings; may additionally reveal characteristic patterns of emphysema










Other
-
CBC [2]
- Secondary polycythemia, ↑ hematocrit
- Eosinophil counts may be used to guide decisions on management of inhaled corticosteroids. [1]
- ECG/TTE: Right ventricular hypertrophy may be seen in patients with advanced COPD. [20]
© AMBOSS
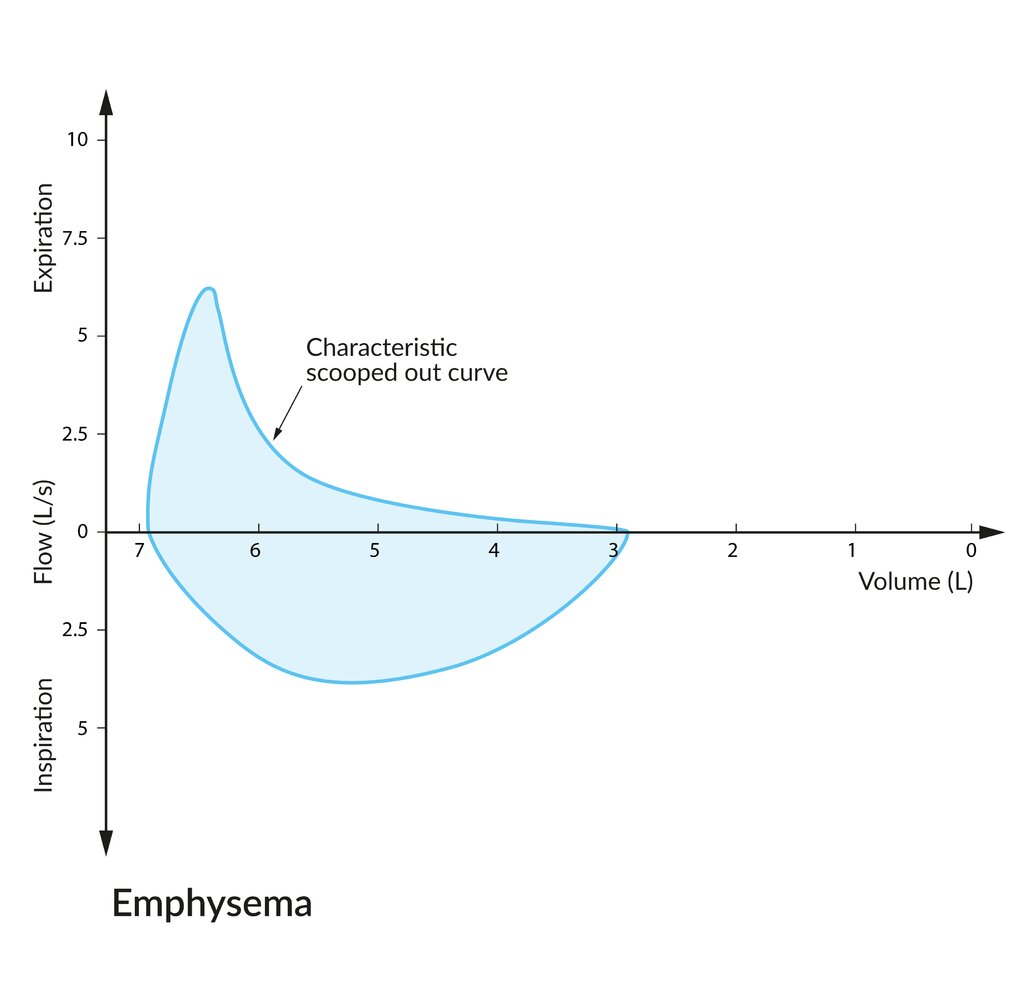
Since expiratory flow is obstructed by the collapse of small airways, the peak expiratory flow rate is lower than normal with a concave (scooped) curve towards the residual volume. The residual volume (∼ 3 L) and total lung capacity (∼ 7 L) are abnormally high due to the lung's increased compliance, decreased recoil, and air trapping.
© AMBOSS
© AMBOSS
© AMBOSS
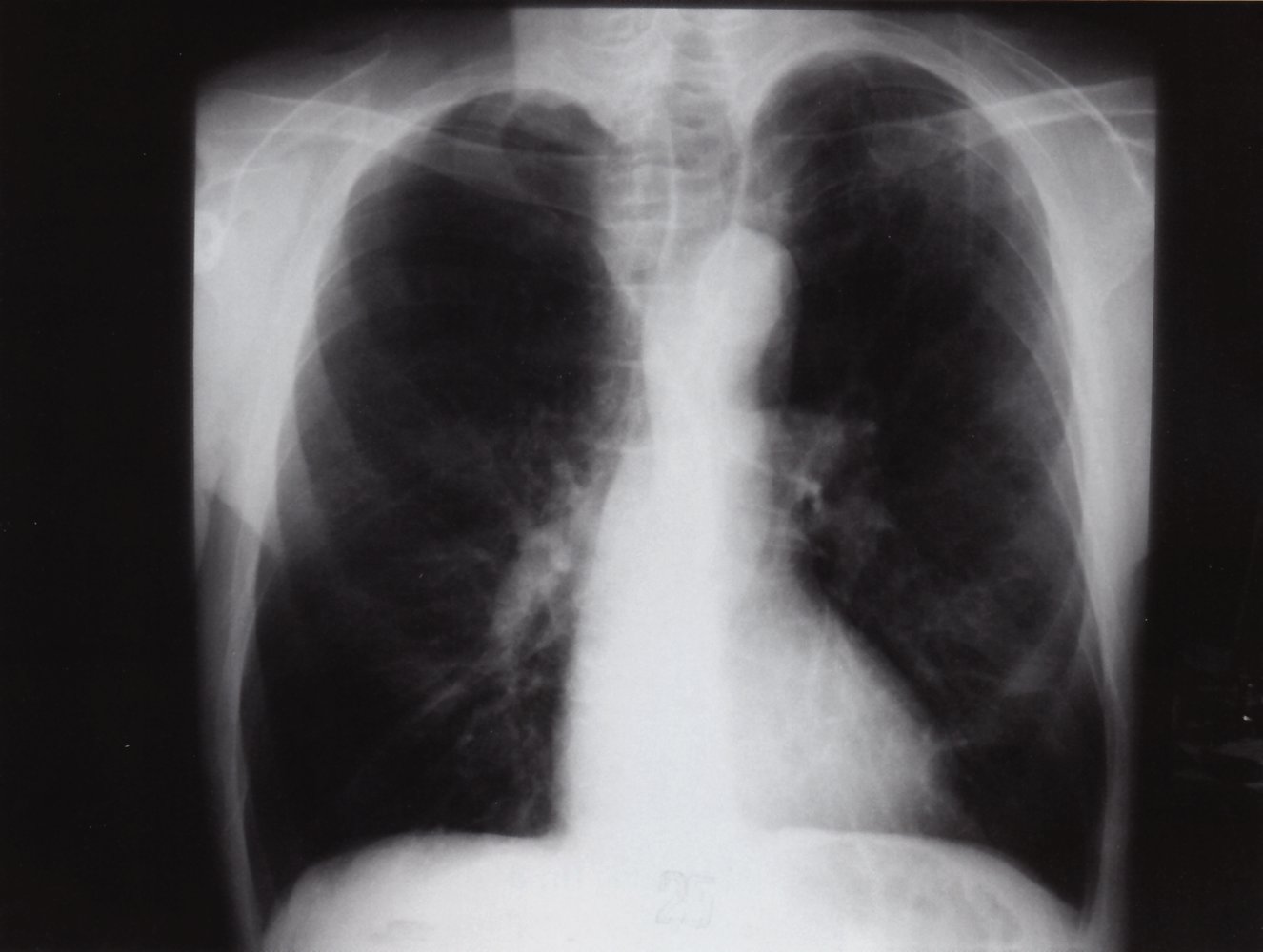
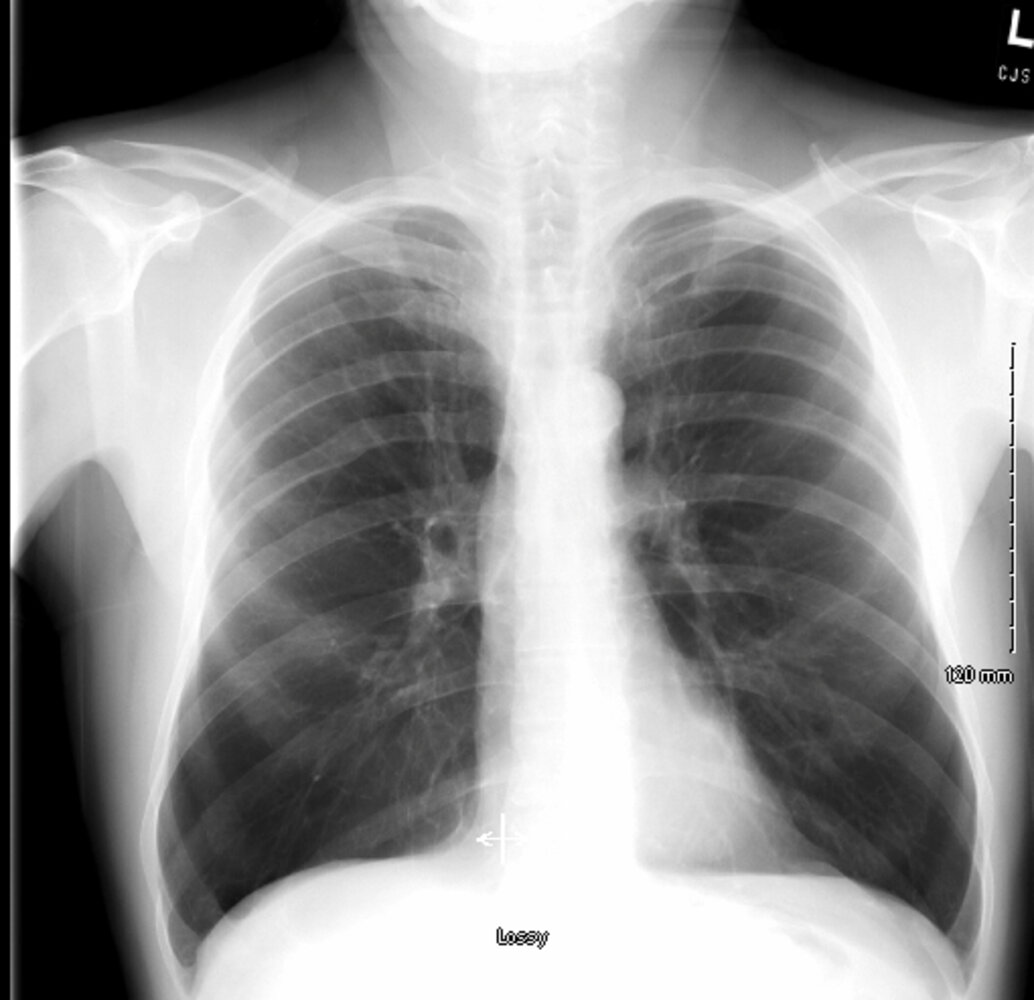
X-ray chest (PA view) of a patient with a history of emphysema
The lungs are hyperlucent, with diaphragmatic flattening (indicated by dashed lines and arrows) and widening of the costophrenic sulci (indicated by white lines). The findings are consistent with air trapping.
An additional finding is asymmetry of the lung apices with slightly increased opacification in the left apex (red overlay) compared to the right. The chronicity cannot be determined from this single study, and the differential for chronic causes includes both scar and malignancy. A second small indeterminate opacity projects in the lower left lung (green overlay).
Source: © IMPP
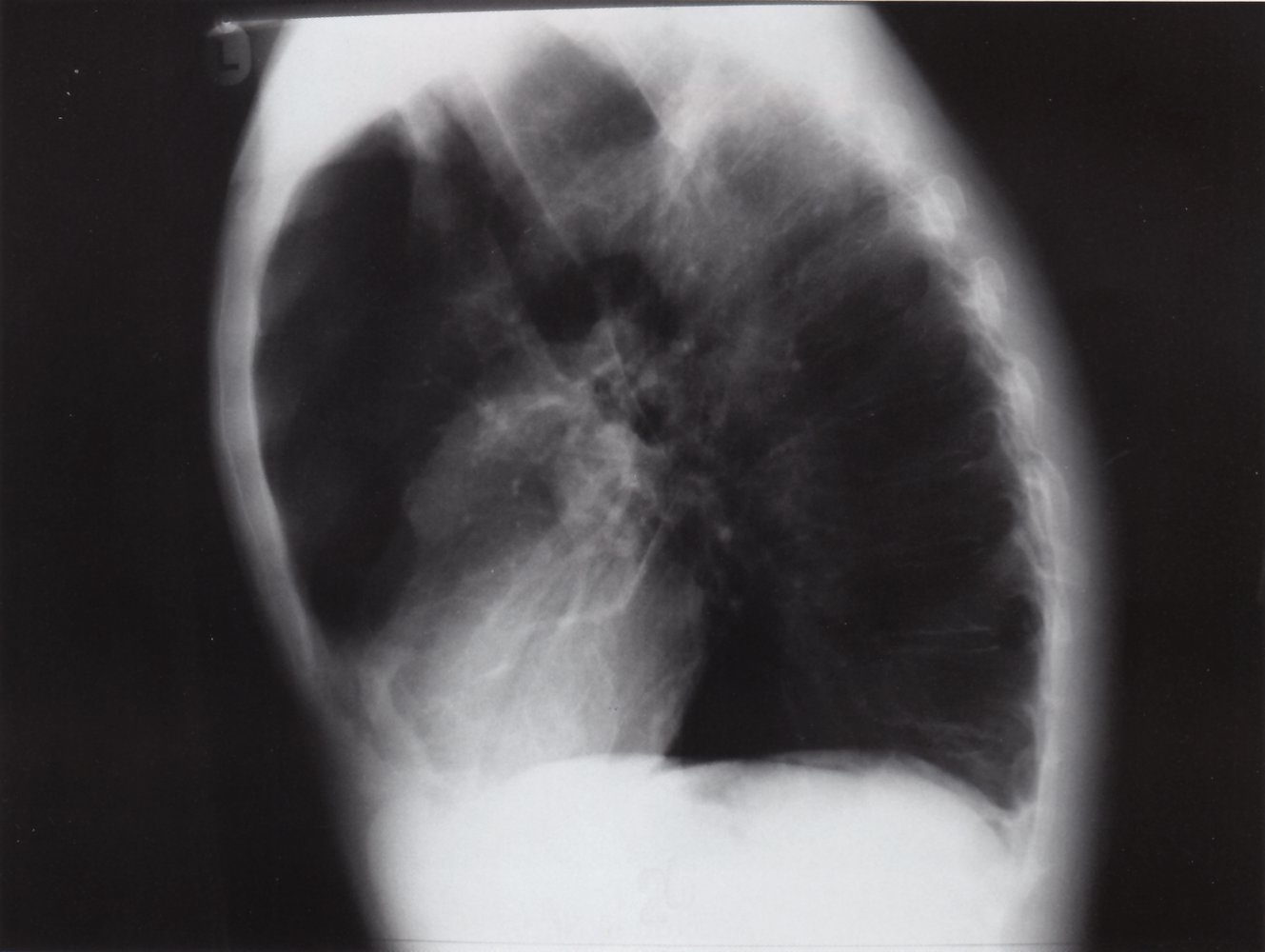
X-ray chest (lateral view) of a patient with a history of emphysema
The lungs are hyperinflated with flattening of the hemidiaphragms, widening of the retrosternal space (green overlay), and increased anteroposterior diameter of the thorax (barrel chest; white bracket).
An area of opacification (red overlay) projecting over the spine above the aortic arch corresponds to an abnormality in the left apex on the PA view.
Source: © IMPP
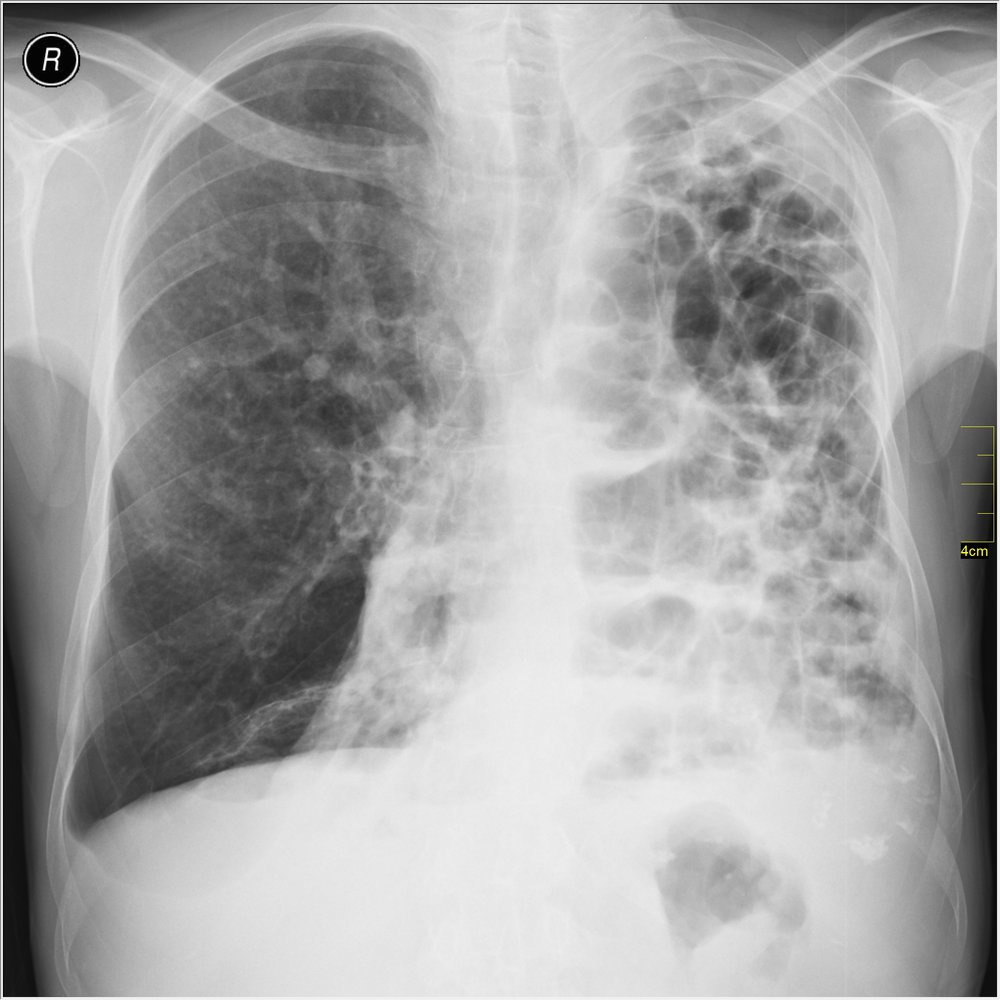
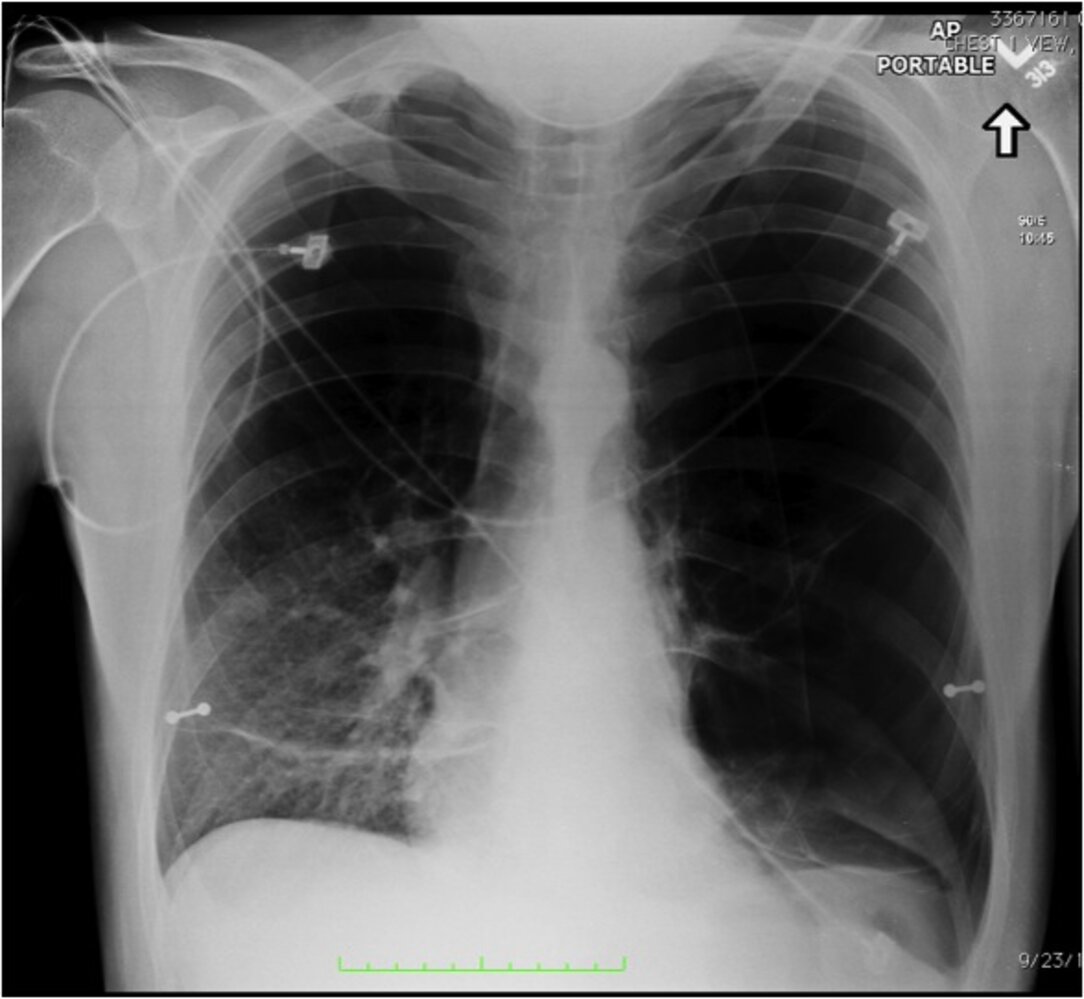
X-ray chest (PA view)
Bilateral ring-shaped opacities (examples indicated by green outlines) mainly affecting the left lung are visible, with corresponding tracheal deviation (white arrows) and loss of the left heart border. The wide intercostal spaces, horizontal ribs, and flattened diaphragm indicate lung hyperinflation. Blunting of the right costophrenic angle (green arrow and green overlay) indicates a small right-sided pleural effusion. The transparency in the right lower lung field appears increased, while distinct pulmonary vascular markings (indicated by white outline) are visible in the right middle and upper lung field.
These findings are consistent with end-stage bullous emphysema.
Source: “Medical X-Ray imaging WFH07 nevit” by Nevit Dilmen, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
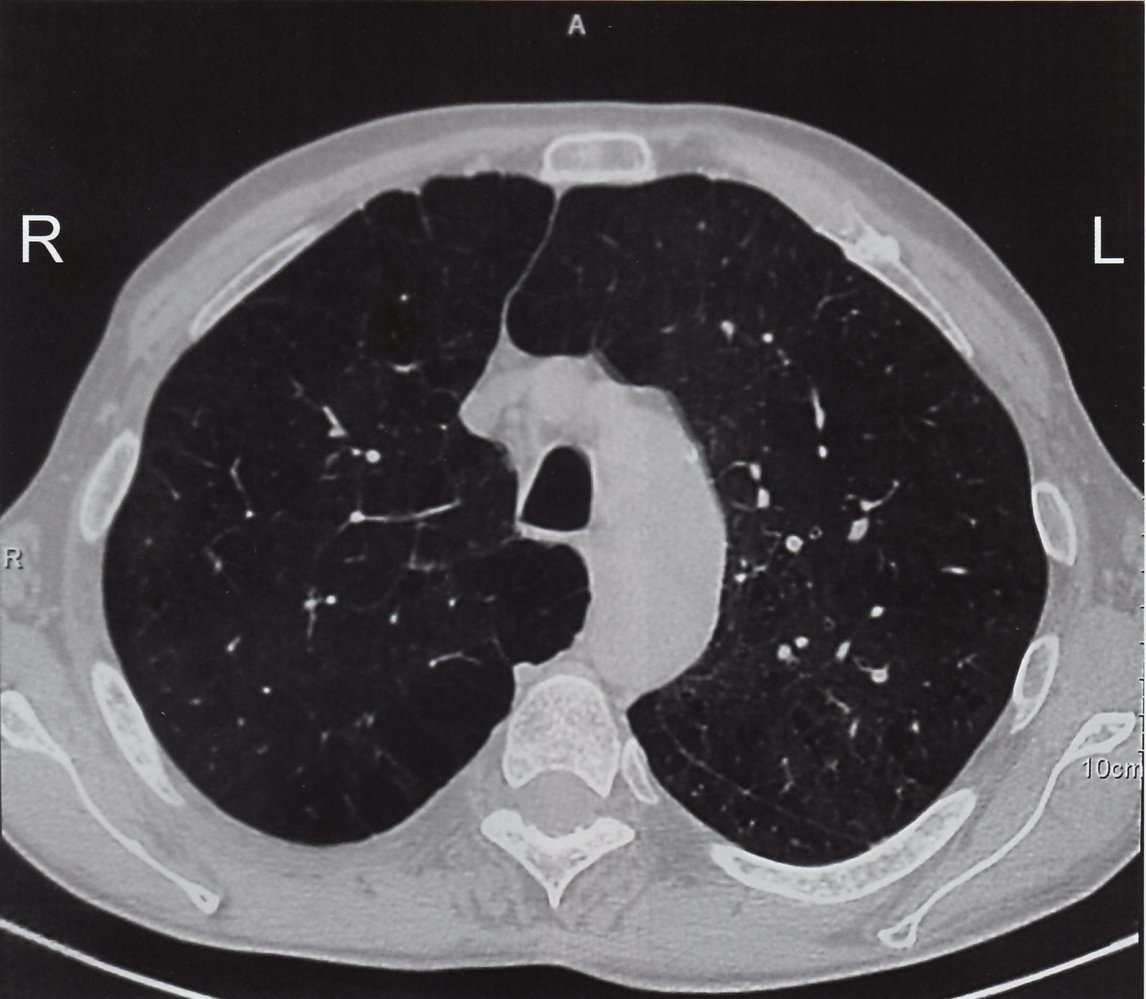
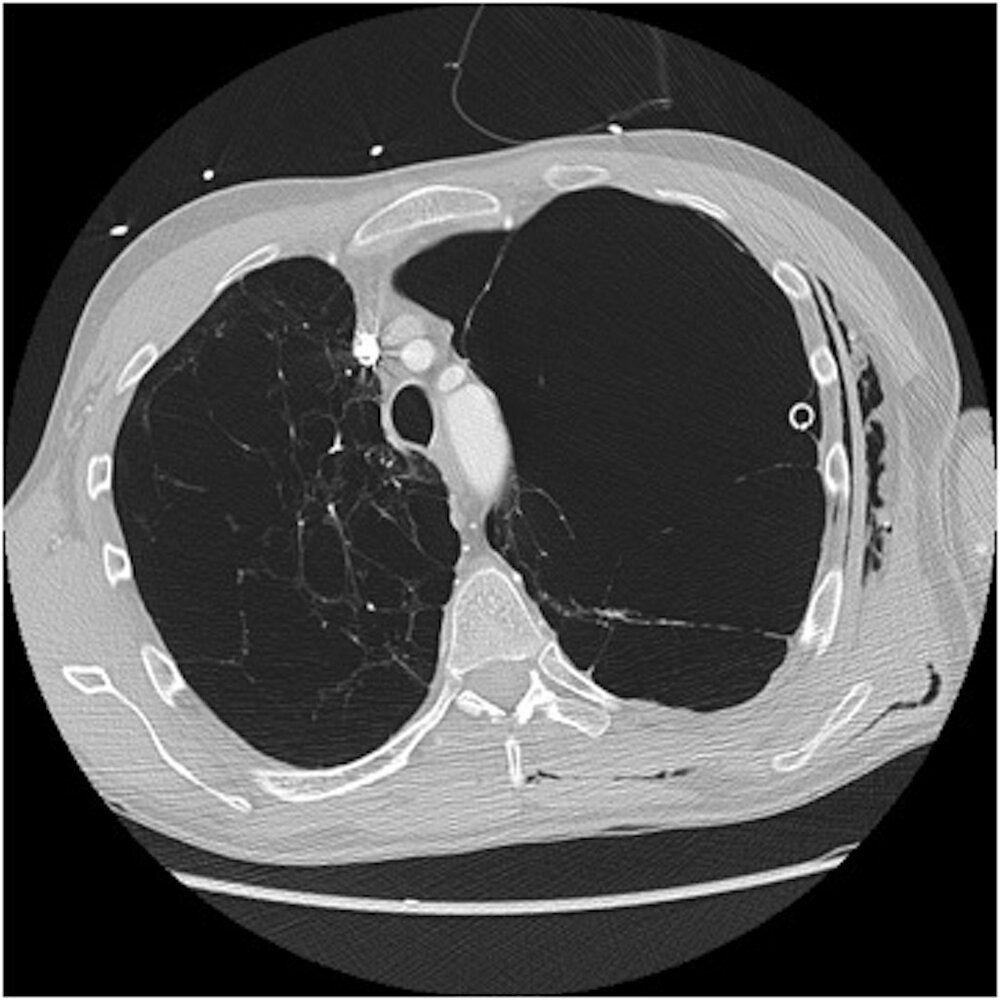
CT chest (high-resolution; axial plane) of a patient with panlobular emphysema
Reduced attenuation of the lung parenchyma is the result of abnormal enlargement of distal air spaces accompanied by destruction of secondary pulmonary lobules. Some narrowed thick-walled bronchi are also seen (examples indicated by white arrows).
The pattern of destruction in panlobular (panacinar) emphysema (green overlay) is diffuse within the secondary pulmonary lobule and the structures of the lobule are generally poorly seen on CT. In contrast, centrilobular (centriacinar) emphysema preserves visualization of much of the anatomy of the secondary lobule.
Source: © IMPP


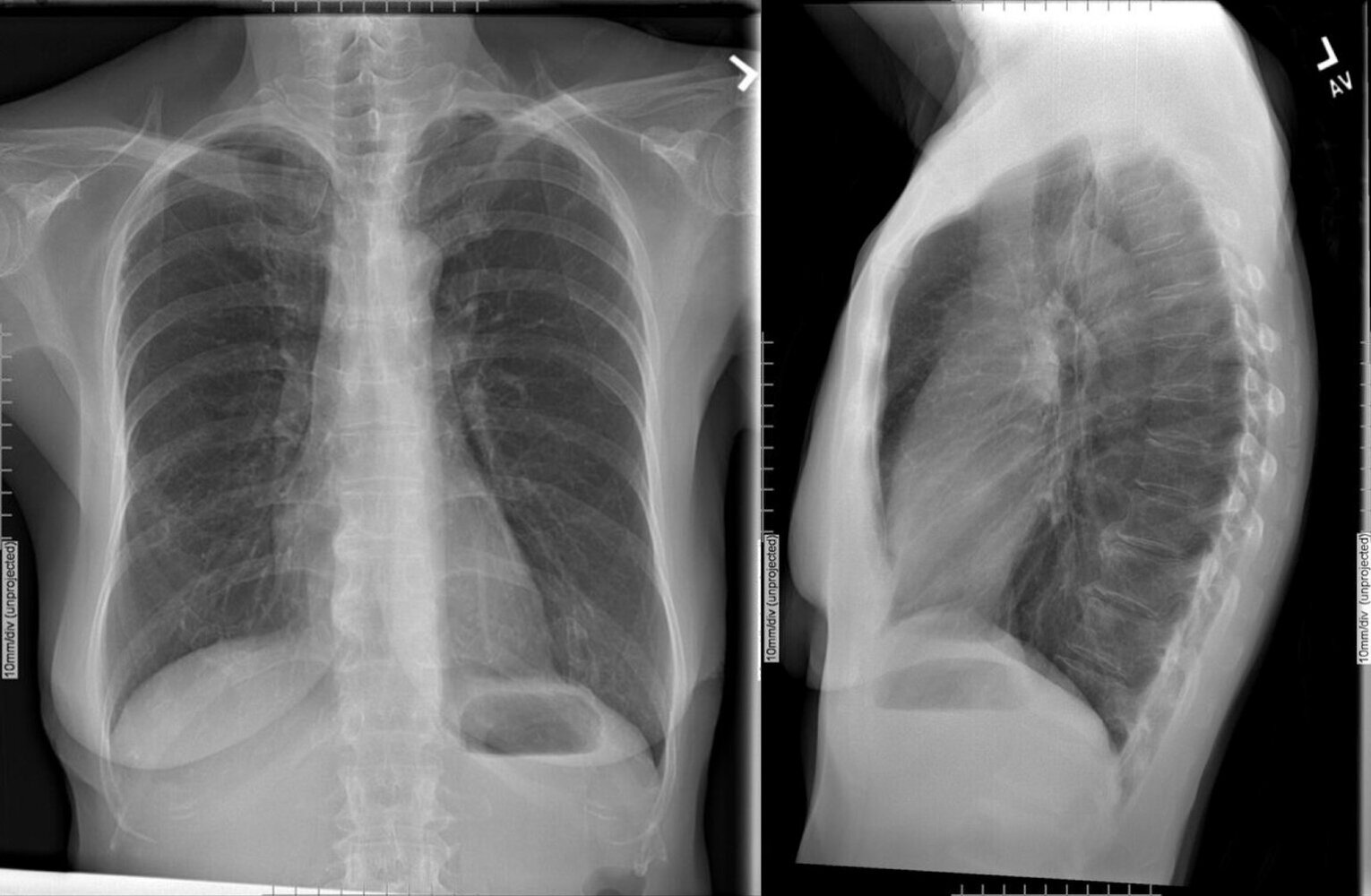
Xray chest (PA and lateral) of patient with a history of COPD
The lung volumes are large, with depression of the hemidiaphragms and greater than ten posterior ribs seen on the PA view. Additionally, the retrosternal space is enlarged on the lateral view. These findings indicate lung hyperinflation.
The cardiac silhouette size is normal and no abnormal opacities are present in the lungs. Hypertrophic degenerative changes are present in the thoracic and lumbar spine.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Differential diagnoses
- Asthma (see “Comparison of asthma and COPD”)
- Heart failure
- Bronchiectasis
- Tuberculosis
- Bronchiolitis
- See also “Differential diagnosis of chronic cough.”
The differential diagnoses listed here are not exhaustive.
Management
Management of acute COPD exacerbation is discussed in AECOPD.
Approach [1]
- Assess for both:
- Symptom severity and history of exacerbations to determine the GOLD group
- Comorbidities that may influence treatment, e.g., asthma
- Provide nonpharmacological management of COPD for all patients.
- Initiate pharmacological treatment of COPD based on GOLD group.
- At follow-up:
- Review inhaler technique.
- Adjust medication based on the adequacy of symptom control.
- Repeat spirometry annually to track any decline in FEV1.
- In patients with advanced disease, consider:
- Long-term oxygen therapy
- Interventional treatment, e.g., lung volume reduction surgery
Nonpharmacological management of COPD [1]
Lifestyle modifications
- Counsel on smoking cessation and options for pharmacotherapy, e.g., varenicline.
- Encourage physical activity to reduce the risk of acute exacerbations.
- Recommend maintenance of a healthy nutritional status.
- Educate patients on:
- Indoor air pollution mitigation, e.g., nonpolluting cooking stoves
- Personal protective equipment to prevent work-related lung diseases
Tobacco smoking cessation is the single most effective step to slow the decline in lung function in patients with COPD.
Supportive care
-
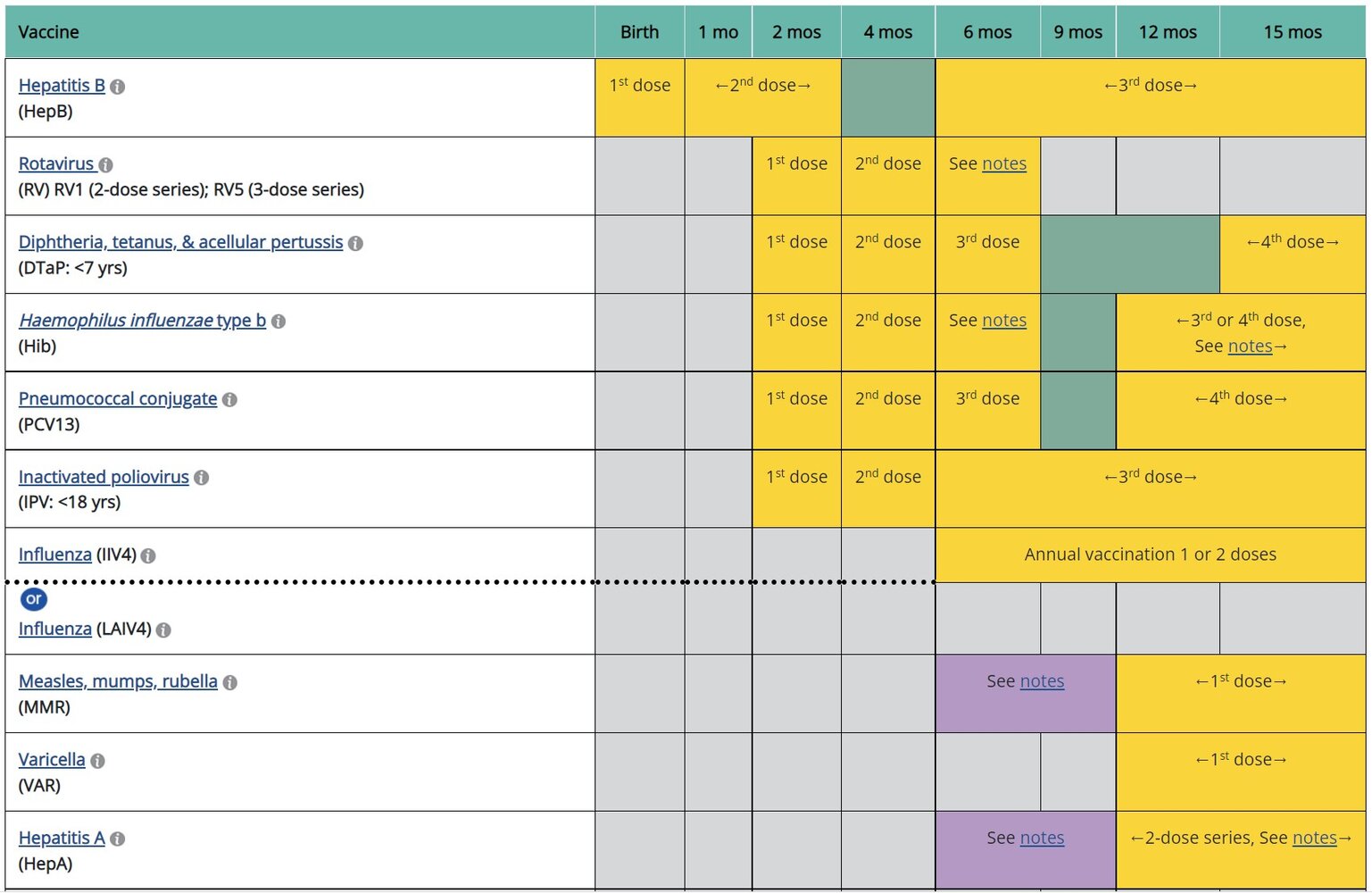
Recommended immunizations in COPD
- Influenza vaccination (annual)
- Pneumococcal vaccination: for patients ≥ 19 years of age [1]
- COVID-19 vaccination
- Tdap vaccination: if not administered in adolescence
- Zoster vaccination: for patients > 50 years of age [1]
- RSV vaccination: for patients ≥ 60 years of age and/or with chronic lung or heart disease [1]
- See also “ACIP immunization schedule.”
- Pulmonary rehabilitation: especially helpful for patients with moderate to severe disease
Vaccinations against pneumococcus and influenza reduce the risk of respiratory infections and complications in patients with COPD. [1]
Management of comorbidities
Screen for common comorbidities at the first visit and at regular intervals, then treat as indicated.
- Screening for depression and anxiety
- Screening for osteoporosis
- ASCVD risk assessment
- Assessment for malnourishment
- Lung cancer screening for patients with COPD resulting from tobacco use
Further notes: Materials developed and hosted by the CDC and available free of charge on the CDC website. Reference to specific commercial products, manufacturers, companies, or trademarks does not constitute its endorsement or recommendation by the U.S. Government, Department of Health and Human Services, or Centers for Disease Control and Prevention.
Pharmacological treatment
See “Pharmacotherapy for AECOPD” for treatment of acute exacerbations.
General principles [1]
- Bronchodilators are the mainstay of pharmacological treatment.
- Inhaled corticosteroids (ICS), e.g., budesonide, fluticasone, or beclomethasone, should only be used in combination with long-acting bronchodilators.
- A single inhaler may be more effective than multiple inhalers when available and affordable.
- Patient education on proper inhaler technique is essential for adequate symptom control.
- Describe and demonstrate when prescribing a new inhaler.
- Observe the patient's technique for each inhaler at follow-up visits.
- Identify common errors, e.g., inadequate exhalation prior to inhalation.
- For patients with both COPD and asthma, choose medications based on stepwise treatment of chronic asthma.
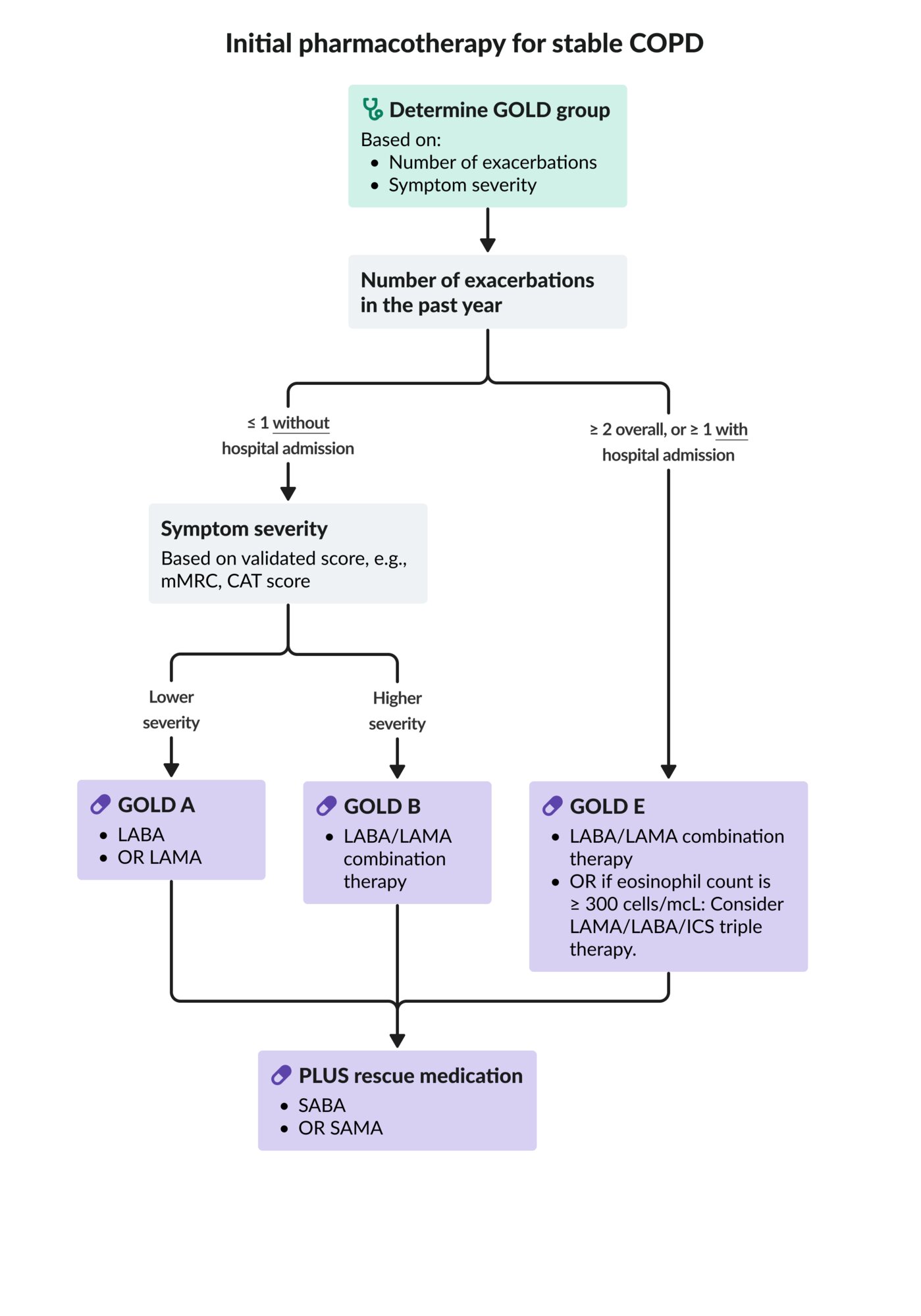
Initial treatment
| Initial pharmacological treatment of stable COPD [1] | ||||
|---|---|---|---|---|
| GOLD group | Daily regimen | Rescue medication | ||
| GOLD group A |
|
|
||
| GOLD group B |
|
|||
| GOLD group E |
|
|||
| ||||
If treatment response is inadequate, consider poor inhaler technique and/or poor adherence as causes.

Follow-up treatment [1]
- Maintain inhaler therapy if dyspnea and exacerbations are well controlled with the current regimen.
- If not, assess for:
- Adherence
- Inhaler technique
- Comorbid conditions that could explain symptoms
- Reinforce nonpharmacological management of COPD.
- Adjust treatment based on the predominant trait (i.e., dyspnea or exacerbations), not on the GOLD group at diagnosis.
| Follow-up treatment in COPD [1] | ||
|---|---|---|
| Predominant trait | Current treatment | Follow-up treatment |
| Persistent dyspnea |
|
|
|
|
|
| Persistent exacerbations |
|
|
|
|
|
|
|
|
Follow-up treatment adjustments are based on treatable traits (dyspnea and frequency of exacerbations) and are made irrespective of the patient's GOLD group (A, B, or, E) at diagnosis. [1]
Other drugs [1]
-
Methylxanthines (e.g., theophylline)
- Nonselectively antagonize adenosine receptors and inhibit phosphodiesterase
- May be trialed if other bronchodilators are not available
- Unproven benefit
-
Mucolytics (e.g., N-acetylcysteine, erdosteine)
- Liquefy mucus by reducing the disulfide bonds of mucoproteins
- Can be useful in reducing exacerbations in certain patients
There is insufficient evidence to support treating stable COPD with antitussives, vasodilators, or leukotriene antagonists. [1]
CAT: COPD Assessment Test
COPD: chronic obstructive pulmonary disease
GOLD: Global Initiative for Chronic Obstructive Lung Disease
ICS: inhaled corticosteroid
LABA: long-acting beta agonist (e.g., salmeterol or formoterol)
LABA/LAMA: combination of a LABA and a LAMA (e.g., umeclidinium/vilanterol)
LAMA/LABA/ICS: combination of a LAMA, LABA, and an ICS (e.g., fluticasone furoate/umeclidinium/vilanterol)
LAMA: long-acting muscarinic antagonist (e.g., tiotropium bromide)
mMRC: modified Medical Research Council
SABA: short-acting beta agonist (e.g., albuterol)
SAMA: short-acting muscarinic antagonist (e.g., ipratropium bromide)
© AMBOSS
Management of advanced disease
Respiratory support [1]
-
Long-term oxygen therapy (LTOT)
- Indications
- PaO2 ≤ 55 mm Hg or SaO2 ≤ 88% at rest despite optimal medication
- OR PaO2 55–60 mm Hg in patients with pulmonary hypertension, CHF, or polycythemia
- Target oxygen saturation: > 90%
- Recommended duration: continuous oxygen therapy for ≥ 15 hours/day
- Reevaluate after 60–90 days (with ABG or pulse oximetry).
- Indications
-
Ventilatory support
- Continuous positive airway pressure is useful in patients with COPD and obstructive sleep apnea.
- Long-term noninvasive positive-pressure ventilation may be considered in select patients with severe chronic hypercapnia.
For patients started on LTOT, check blood gasses frequently (with ABG or VBG) to ensure adequate oxygenation without unintended acidosis and CO2 retention. [1]
LTOT increases survival in patients with severe resting hypoxemia.
Invasive treatment
- Surgical bullectomy: indicated in severe emphysema with hyperinflation and large bullae
-
Lung volume reduction
- Indicated for severe emphysema and hyperinflation without large bullae
- Severely affected emphysematous areas of the lung are removed either surgically (lung volume reduction surgery) or endoscopically
- Lung transplantation: may be indicated for very severe COPD, patients not eligible for bullectomy or lung volume reduction, and those with surgical contraindications
Palliative care [1]
- Optimize nonpharmacological management of COPD
- Offer palliative symptom control for all patients with inadequate relief from optimal medical therapy, e.g.:
- Palliative pharmacotherapy for breathlessness
- Mind-body interventions (e.g., mindfulness practice)
- Initiate early discussion regarding end-of-life care and hospice wishes.
Palliative measures (e.g., low-dose opiates, fans blowing onto the patient's face, or acupuncture) can be used if distressing breathlessness persists despite optimal medical therapy. [21][22]
Complications
-
Chronic respiratory failure [6]
- Long-standing partial respiratory failure (PO2 at rest < 60 mm Hg)
- Hypoxemic and hypercapnic respiratory failure (PO2 at rest < 60 mm Hg and PCO2 > 45 mm Hg)
- Occurs in advanced COPD due to progressive emphysematous changes and loss of diffusion surface area
- Acute exacerbation of COPD
- Cor pulmonale (right heart failure)
- Secondary spontaneous pneumothorax due to rupture of bullae (especially in bullous emphysema)
We list the most important complications. The selection is not exhaustive.
Prognosis
-
40–70% of all COPD patients survive the first 5 years after diagnosis. [23]
- Survival rates vary significantly depending on the severity of the disease. [23]
- The BODE index (Body mass, Obstruction, Dyspnea, Exercise) estimates prognosis in patients with COPD. [24]
-
Measures that improve survival
- Cessation of tobacco use
- Long-term oxygen therapy in patients with severe resting hypoxemia
- COPD is the third most common cause of death worldwide. [25]
Related One-Minute Telegram
- One-Minute Telegram 134-2025-2/3: Are MDIs a breath of fresh air? Not for the climate
- One-Minute Telegram 127-2025-1/3: Morphine misses the mark for breathlessness in COPD
- One-Minute Telegram 99-2024-1/3: Specialized care of newly diagnosed asthma and COPD leads to better outcomes
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Venkatesan P. "GOLD COPD report: 2025 update". Lancet Respir Med. 13(1). :e7-e8. (2025)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Peter J. Barnes. "Sex Differences in Chronic Obstructive Pulmonary Disease Mechanisms". American Journal of Respiratory and Critical Care Medicine. (2016)
- Georgios Ntritsos, Jacob Franek, Evangelos Evangelou, et al. "Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis". International Journal of Chronic Obstructive Pulmonary Disease. (2018)
- Wheaton AG, Cunningham TJ, Ford ES, Croft JB, Centers for Disease Control and Prevention (CDC).. "Employment and activity limitations among adults with chronic obstructive pulmonary disease--United States, 2013.". MMWR Morb Mortal Wkly Rep. 64(11). :289-95. (2015)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Liu Y, Pleasants R, Croft J, et al. "Smoking duration, respiratory symptoms, and COPD in adults aged ≥45 years with a smoking history". International Journal of Chronic Obstructive Pulmonary Disease. :1409. (2015)
- "Household air pollution and health". http://www.who.int/mediacentre/factsheets/fs292/en/. [2016-02-01]
- "Occupational and work-related diseases". http://www.who.int/occupational_health/activities/occupational_work_diseases/en/. [2017-02-27]
- Stocks J, Sonnappa S. "Early life influences on the development of chronic obstructive pulmonary disease". Therapeutic Advances in Respiratory Disease. 7(3). :161-173. (2013)
- Kumar V, Abbas AK, Aster JC. "Robbins & Cotran Pathologic Basis of Disease". Elsevier Saunders. (2014). ISBN: 9781455726134
- Oberholzer M, Dalquen P, Wyss M, Rohr HP. "The applicability of the gland/wall ratio (Reid-Index) to clinicopathological correlation studies.". Thorax. 33(6). :779-784. (1978)
- Kim V, Rogers TJ, Criner GJ. "New concepts in the pathobiology of chronic obstructive pulmonary disease". Proc Am Thorac Soc. 5(4). :478-85. (2008)
- Barnes PJ, Drazen JM, Rennard SI. "Asthma and COPD". Academic Press. (2009). ISBN: 9780123740014
- Sarkar M, Mahesh D, Madabhavi I. "Digital clubbing". Lung India. 29(4). :354. (2012)
- Mangione CM, Barry MJ, et al. "Screening for Chronic Obstructive Pulmonary Disease". JAMA. 327(18). :1806. (2022)
- Stanojevic S, Kaminsky DA, Miller MR, et al. "ERS/ATS technical standard on interpretive strategies for routine lung function tests". Eur Respir J. 60(1). :2101499. (2021)
- "Global Strategy for Asthma Management and Prevention (2022 update)". https://web.archive.org/web/20230115002305/https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf. [2022-01-01]
- Harrigan RA. "ABC of clinical electrocardiography: Conditions affecting the right side of the heart". BMJ. 324(7347). :1201-1204. (2002)
- Nishimura K, Tsukino M. "Clinical course and prognosis of patients with chronic obstructive pulmonary disease". Curr Opin Pulm Med. 6(2). :127-132. (2000)
- Celli BR, Cote CG, Marin JM, et al. "The Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise Capacity Index in Chronic Obstructive Pulmonary Disease". N Engl J Med. 350(10). :1005-1012. (2004)
- "The top 10 causes of death". http://www.who.int/mediacentre/factsheets/fs310/en/. [2017-01-01]
- Anderson AE, Foraker AG. "Centrilobular emphysema and panlobular emphysema: two different diseases". Thorax. 28(5). :547-550. (1973)
- Nici L, Mammen MJ, Charbek E, et al. "Pharmacologic Management of Chronic Obstructive Pulmonary Disease. An Official American Thoracic Society Clinical Practice Guideline". Am J Respir Crit Care Med. 201(9). :e56-e69. (2020)
- Bausewein C, Booth S, Gysels M, Higginson I. "Non-pharmacological interventions for breathlessness in advanced stages of malignant and non-malignant diseases.". Cochrane Database Syst Rev.. :CD005623. (2008)