Summary
Chronic pancreatitis (CP) is characterized by progressive inflammation that results in irreversible damage to the structure and function of the pancreas. Chronic heavy alcohol use is the most common cause of CP, followed by pancreatic ductal obstruction. Approximately 30% of CP cases are idiopathic. Affected individuals may be asymptomatic or present with abdominal pain and features of exocrine pancreatic insufficiency (e.g., steatorrhea, weight loss) or endocrine pancreatic insufficiency (e.g., prediabetes, diabetes). Diagnosis is confirmed with imaging, which typically shows pancreatic calcifications, ductal strictures, and ductal dilations. Pancreatic function tests (e.g., fecal elastase-1 measurement, 72-hour fecal fat estimation) assess the degree of enzyme deficiency. Medical therapy should include patient counseling and education, pain management, and monitoring and management of complications (e.g., via oral pancreatic enzyme replacement therapy). Interventional therapy may be required for patients with intractable pain or other complications (e.g., celiac ganglion block, partial or complete pancreatic resection).
Etiology
- Chronic heavy alcohol use (most common, esp. men) [1]
- Pancreatic ductal obstruction: strictures (e.g., due to trauma, stones)
- Tobacco use
- Idiopathic pancreatitis
-
Hereditary pancreatitis [2]
- PRSS1 gene mutation (autosomal dominant inheritance), SPINK1 gene mutation
- Age of onset < 20 years
- Characterized by a positive family history and the absence of other risk factors
- Autoimmune pancreatitis
-
Systemic disease
- Cystic fibrosis: ∼ 2% of cystic fibrosis patients develop chronic pancreatitis. [3]
- Severe hypertriglyceridemia (levels > 1,000 mg/dL)
- Primary hyperparathyroidism (hypercalcemia)
-
Tropical pancreatitis
- Most common cause in the tropics (esp. southern India)
- Young age at onset
The TIGAR-O system categorizes etiologies of chronic pancreatitis: Toxic-Metabolic, Idiopathic, Genetic, Autoimmune, Recurrent acute/severe pancreatitis, and Obstructive. [4][5]
Pathophysiology
- Autodigestion and inflammation: damage to pancreatic acinar cells; (e.g., alcohol), outflow obstruction of pancreatic enzymes or premature activation of trypsinogen to trypsin; → intrapancreatic activation of digestive enzymes (e.g., amylase and lipase) → autodigestion of pancreatic tissue → inflammatory reaction
- Fibrosis: exposure to toxins and/or inflammatory mediators (e.g., alcohol, cytokines) → activation of pancreatic stellate cells

References:[6]
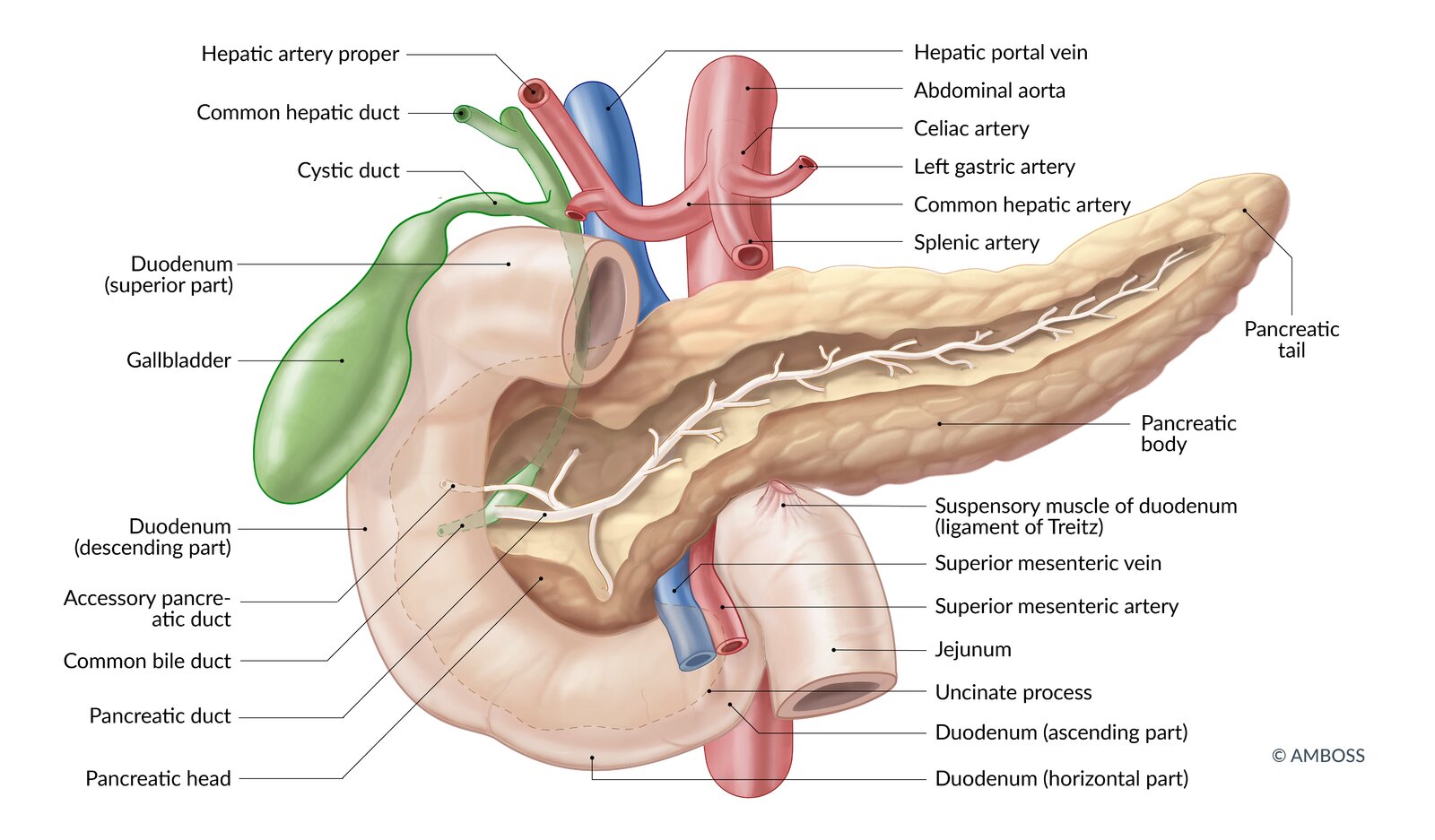
The main pancreatic duct and the common bile duct merge and enter the descending part of the duodenum at the major duodenal papilla. The accessory duct enters at the minor duodenal papilla.
Note: individual ductal anatomy may vary
© AMBOSS
Clinical features
-
Epigastric abdominal pain (main symptom)
- Pain radiates to the back, is relieved on bending forward, and is exacerbated after eating.
- Pain is initially episodic and becomes persistent as the disease progresses.
- Often associated with nausea and vomiting
-
Features of pancreatic insufficiency: late manifestation (after 90% of the pancreatic parenchyma is destroyed)
-
Steatorrhea (exocrine enzyme deficiency)
- Cramping abdominal pain, bloating, diarrhea
- Can lead to a deficiency of fat-soluble vitamins (A, D, E, and K)
- Malabsorption and weight loss
- Pancreatic diabetes (endocrine hormone deficiency)
-
Steatorrhea (exocrine enzyme deficiency)
In the later stages of chronic pancreatitis, patients may not experience any pain.
References:[1][7]
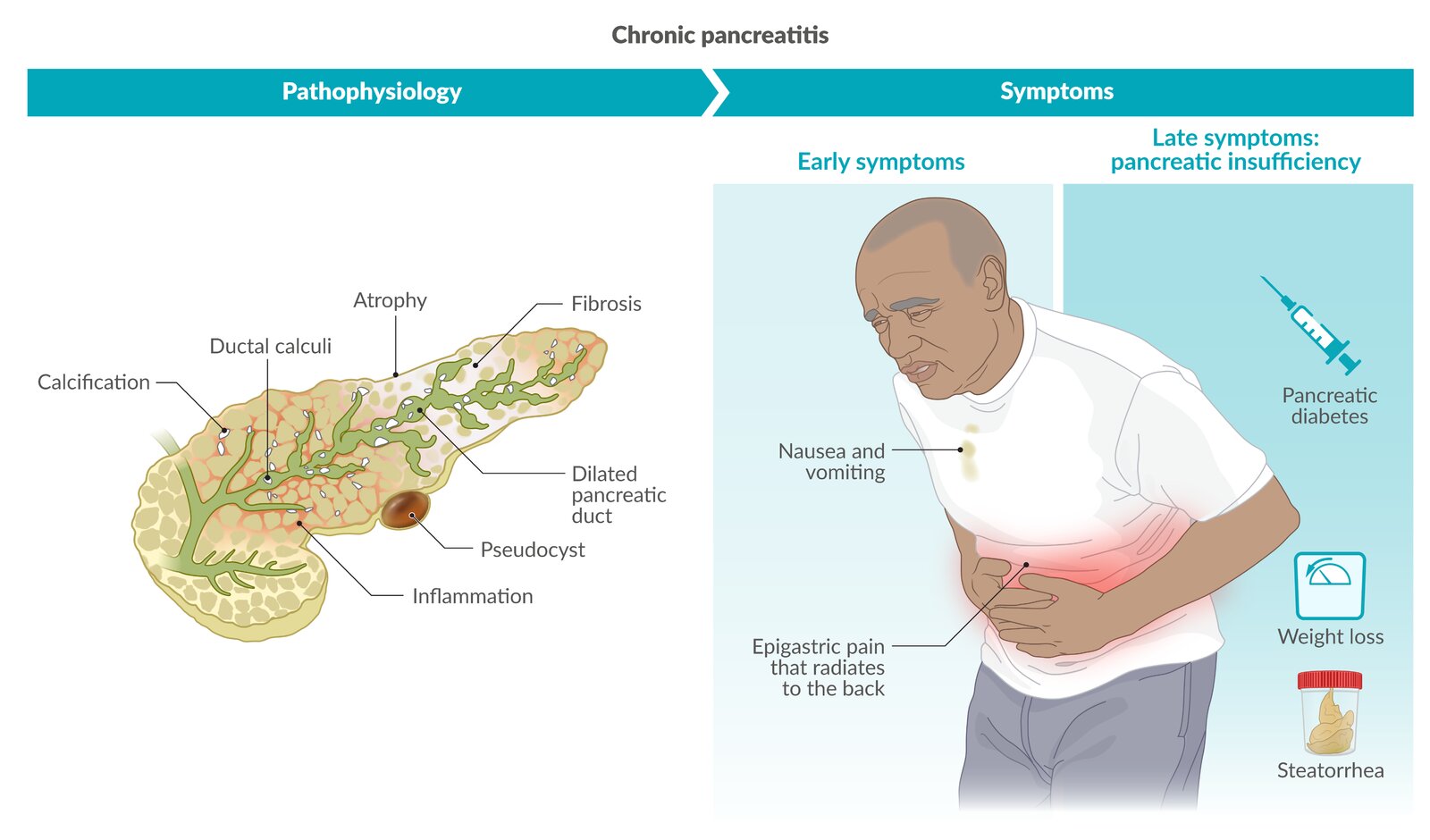
In chronic pancreatitis, inflammation and fibrosis of pancreatic tissue can manifest with abdominal pain (main symptom), which is often accompanied by nausea and vomiting. Symptoms of exocrine pancreatic insufficiency (e.g., steatorrhea, weight loss) and endocrine pancreatic insufficiency (pancreatic diabetes) typically occur late when more than 90% of pancreatic tissue is destroyed.
© AMBOSS
Diagnosis
Approach [4][8][9][10][11]
There is no single test for the diagnosis of chronic pancreatitis; risk factors, clinical features, imaging studies, and pancreatic function tests may all be considered in the determination of a diagnosis.
-
Initial survey: Identify findings raising suspicion for chronic pancreatitis.
- Characteristic abdominal pain
- Signs indicative of:
- Exocrine pancreatic insufficiency (e.g., steatorrhea, weight loss)
- Endocrine pancreatic insufficiency (e.g., diabetes)
- Risk factors for chronic pancreatitis
-
Initial studies
- Imaging studies (most important) to confirm structural changes
- Laboratory testing to assess for complications and identify the underlying cause
-
Additional studies: if initial studies were nondiagnostic
- Pancreatic function tests
- Histology
- Genetic testing
A STEP-wise approach to diagnosing chronic pancreatitis may include: Survey, Tomography/imaging, Endoscopic imaging, and Pancreatic function testing.
Imaging [4][8][12]
First-line imaging
-
Abdominal CT (with and without contrast) or MRI/MRCP
- Best initial imaging modalities to establish a diagnosis
- Can exclude gastrointestinal malignancies (e.g., pancreatic carcinoma)
- Supportive findings
- Pancreatic ductal dilations and calcifications on plain CT (more sensitive than x-ray)
- “Chain of lakes” appearance of the main pancreatic duct
- Pancreatic atrophy


 sign in chronic pancreatitis")


")
Additional imaging [4][13]
-
Abdominal ultrasound [13]
- Low sensitivity for detecting pancreatic pathologies
- Findings
- Indistinct margins and enlargement
- Pancreatic calcifications
- Ductal strictures, dilation, or stones
- Abdominal x-ray: visible pancreatic calcifications (highly specific, but only seen in ∼ 30% of cases) [14]
-
Endoscopic ultrasound (EUS)
- Can detect early changes that indicate chronic pancreatitis
- Indication: reserved for cases in which a CT scan and/or MRI are nondiagnostic [4]
- Findings include: [15]
- Parenchymal lobularity and hyperechoic foci
- Ductal dilation and calcification
-
Secretin-enhanced MRCP
- Improves visualization of pancreatic ducts [16] [4]
- Indication: high clinical suspicion but inconclusive cross-sectional imaging and EUS
- Findings: ductal strictures and dilations or ectasia
-
ERCP: Not routinely recommended because of availability of noninvasive imaging, high risk, and cost [11]
- Can simultaneously identify and treat early pathologies (e.g., duct dilation, stent insertion)
- Findings
- Ductal stones, which are visible as filling defects
- “Chain of lakes” or “string of pearls” appearance (characteristic feature)
- Irregularity and/or dilation of the main pancreatic duct [17]
Laboratory studies [8]
- Serum pancreatic enzyme levels: Lipase (specific) and amylase (nonspecific) are often normal.
- CBC: WBCs may be elevated in infection or abscess.
- Calcium: Hypercalcemia may suggest hyperparathyroidism, a rare cause of chronic pancreatitis.
- Triglycerides: Severe hypertriglyceridemia can cause pancreatitis.
- Liver enzymes and liver function tests: elevated in biliary or ductal obstruction
- Fasting plasma glucose and/or HbA1c: elevated levels could suggest type 3c diabetes (pancreatogenic diabetes mellitus)
- Fat-soluble vitamins and zinc: to identify deficiency and establish baseline
Pancreatic enzyme levels are often normal in chronic pancreatitis and cannot be used to confirm or rule out the diagnosis. In contrast, acute pancreatitis typically causes significant enzyme elevation.
Pancreatic function tests [4][8]
Consider for patients with features of exocrine pancreatic insufficiency or for those in whom diagnosis of chronic pancreatitis has not been confirmed by imaging.
-
Fecal elastase-1 (FE-1): most common test
- Can support a diagnosis of steatorrhea due to exocrine pancreatic insufficiency [18]
- Interpretation (exact cutoffs are controversial) [4]
- FE-1 < 200 mcg/g: abnormal, potential pancreatic exocrine insufficiency
- FE-1 < 100 mcg/g: Suspect pancreatic exocrine insufficiency.
-
72-hour quantitative fecal fat estimation: confirmatory test for steatorrhea
- Patients consume 100 g of fat per day for 72 hours.
- Interpretation: Fecal fat > 7 g per day is diagnostic of steatorrhea.
-
Serum trypsinogen: not routinely recommended [4]
- May be elevated in acute pancreatitis, pain, cystic fibrosis
- < 20 ng/mL is suggestive of severe pancreatic insufficiency.
-
Direct tests of pancreatic function
- Cholecystokinin analog (cerulein), secretin, or a combination, are administered parenterally.
- Pancreatic enzyme and bicarbonate levels of duodenal fluid are measured.
- Low amylase, lipase, trypsin, and bicarbonate levels are suggestive of exocrine pancreatic insufficiency.
The presence of exocrine pancreatic insufficiency (as confirmed by pancreatic function tests) is not required to establish a diagnosis of chronic pancreatitis but can further support the diagnosis.
Histology [4]
- Indications: reserved for high-risk patients if the diagnosis has not been established after thorough evaluation
-
Characteristic findings [10]
- Bands of interlobular fibrosis
- Acinar atrophy
- Intraductal concretions
Histology is rarely used to diagnose chronic pancreatitis because of procedural risks and the possibility of sampling errors that lead to false-negative results.
Genetic testing [19]
-
Indications include:
- Family history of chronic pancreatitis
- Young patients with idiopathic pancreatitis
-
Tests include:
- PRSS1 gene mutations: diagnostic of hereditary pancreatitis
- CFTR gene mutations: seen in ∼ 30% of patients with idiopathic chronic pancreatitis
- SPINK1 gene mutations: seen in ∼ 20% of patients with hereditary or idiopathic chronic pancreatitis
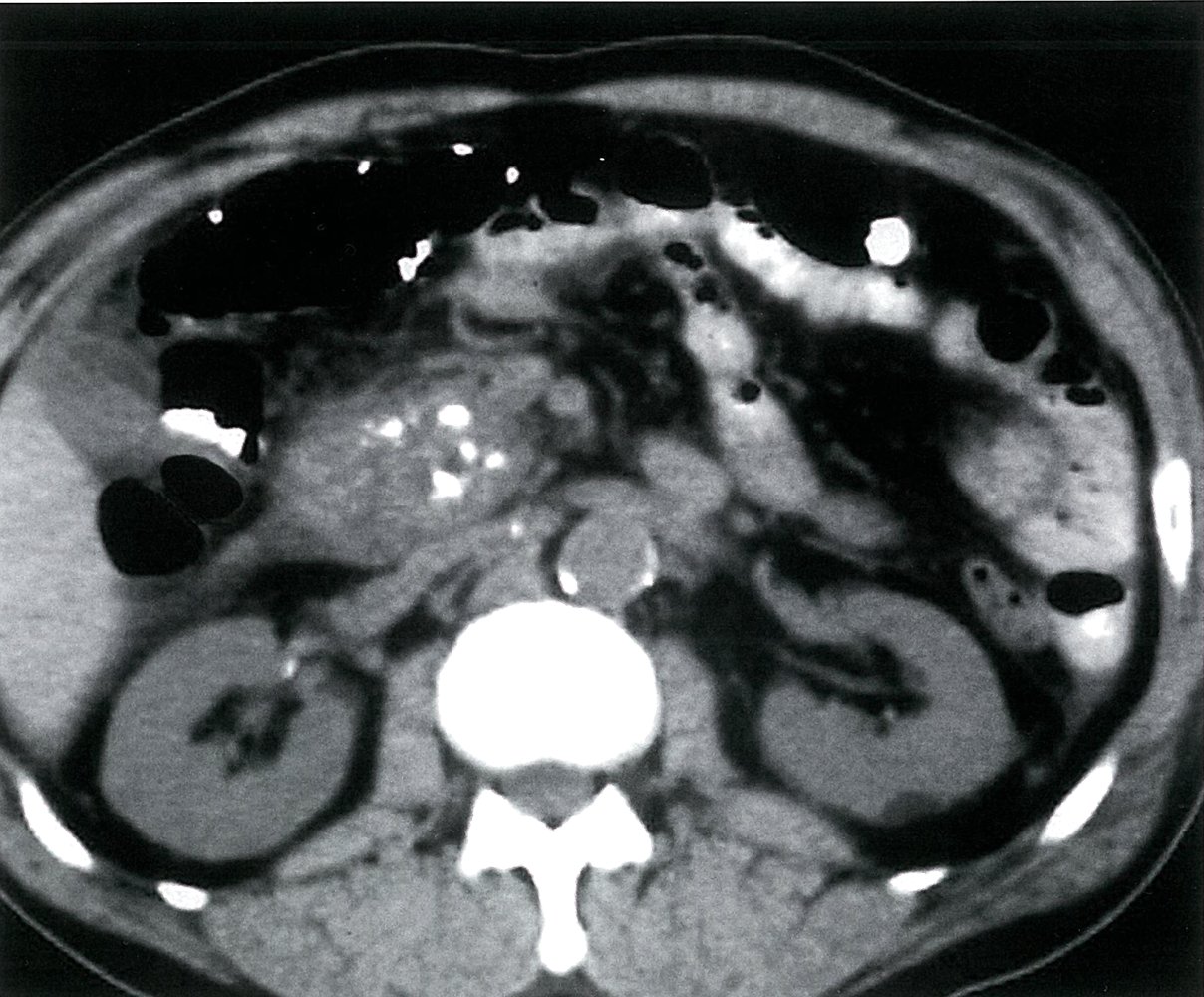
CT abdomen (with contrast; axial plane)
An enlarged heterogeneous pancreatic head (green overlay) contains multiple calcifications, which is characteristic of chronic pancreatitis. Peripancreatic inflammatory fatty stranding (red overlay) is also seen.
Incidental findings include a small hypodense cyst (yellow overlay) in the dorsal parenchyma of the left kidney and atherosclerotic vascular calcifications (blue overlay). Intravenous contrast is seen in the liver (L), and oral contrast is seen in the bowel loops (indicated by arrows).
Source: © IMPP

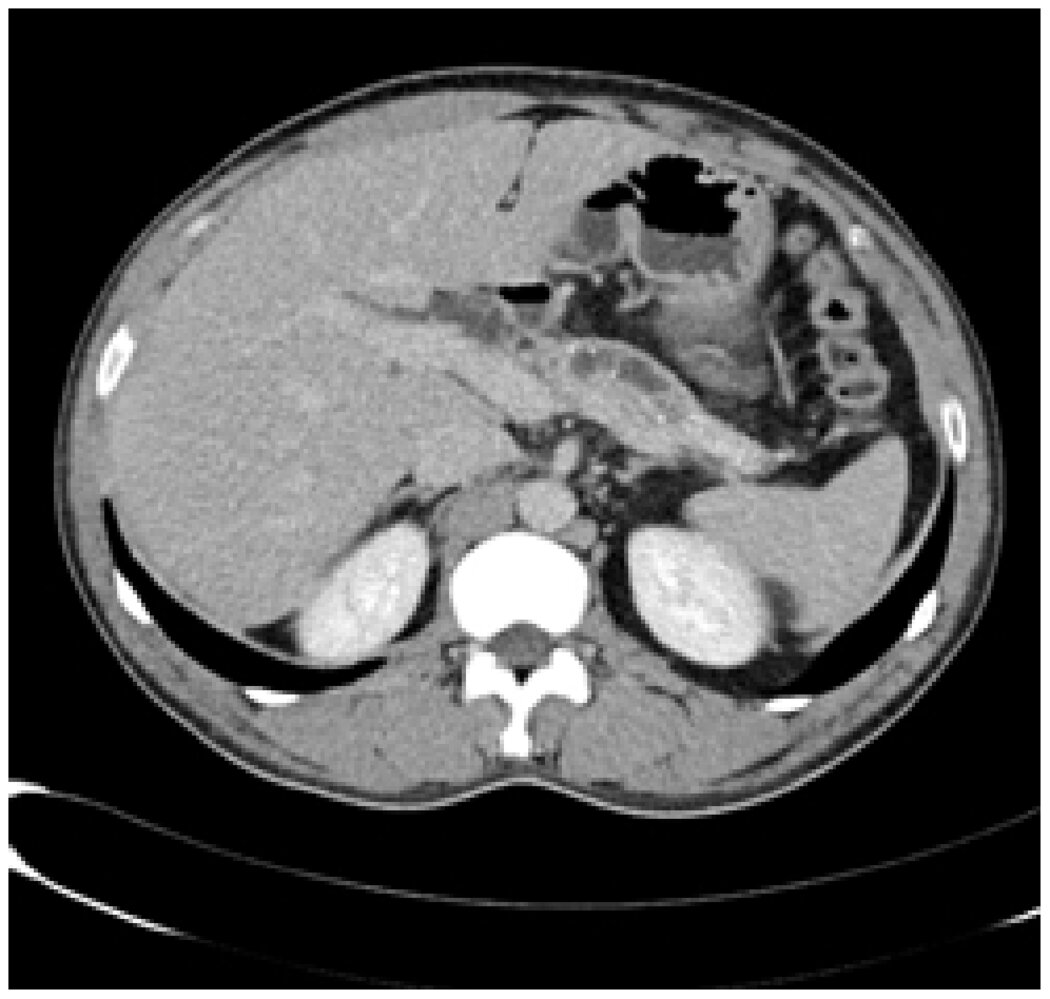
CT abdomen (with contrast; axial plane)
Multiple coarse calcifications (examples indicated by black arrowheads) in the pancreatic parenchyma are diagnostic of chronic pancreatitis. The pancreatic head also contains a hypodense structure (green overlay) that could represent a duct or small mass. A cholecystectomy clip is seen (red overlay).
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
CT abdomen (with contrast; axial plane) of a patient with autoimmune pancreatitis
The pancreas is partially visualized; the head is not included. Within the body, the main pancreatic duct shows alternating segments of dilatation and stenosis, giving it its string-of-beads or chain-of-lakes appearance (red arrowheads; cf. illustration). There is atrophy of the pancreatic parenchyma, and a few punctate calcifications are seen (white arrowheads).
The CT features are compatible with a diagnosis of chronic pancreatitis. Pseudocysts and pseudoaneurysms may also be seen with chronic pancreatitis.
BD: bile duct; K: kidneys; L: liver; Sp: spleen: St: stomach; PV: portal vein
Source: “Fig. 14, in: Clinical Analysis of 36 Cases of Autoimmune Pancreatitis in China” by Xingang Zhang, Xinpeng Zhang, Wei Li et al., Plos One, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).


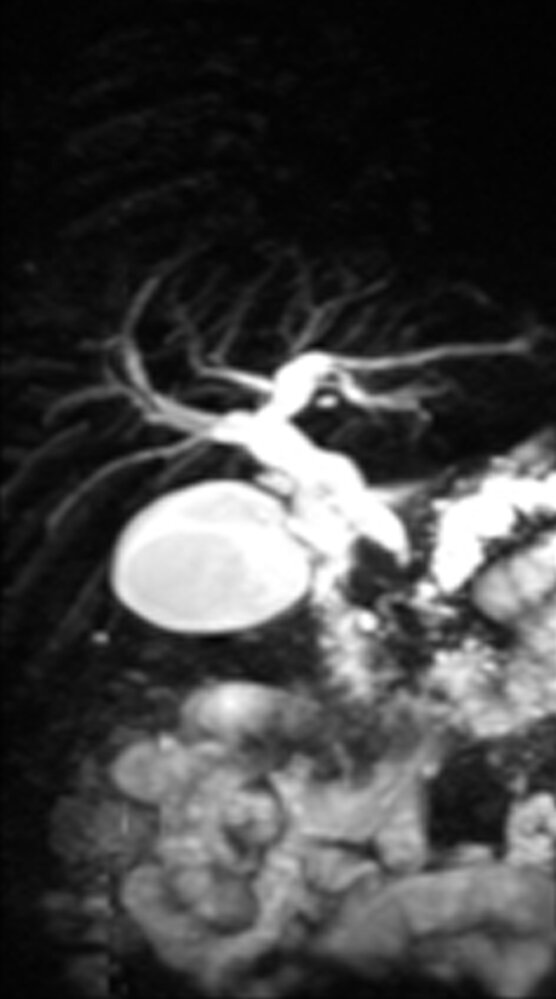
Magnetic resonance cholangiopancreatography (MRCP)
The main pancreatic duct is irregular, with alternating areas of stenosis and dilatation producing a beaded appearance (indicated by red outline). Small dilated side branches (indicated by arrowheads) are also seen, and there is beak-shaped tapering of a distal common bile duct stricture (yellow overlay).
Beading of the main pancreatic duct (chain of lakes sign) is a characteristic finding of chronic pancreatitis.
CBD: common bile duct; GB: gallbladder; PD: pancreatic duct
Source: “Fig. 20, in: Clinical Analysis of 36 Cases of Autoimmune Pancreatitis in China” by Xingang Zhang; Xinpeng Zhang; Wei Li et al., Plos One, licensed under CC BY 4.0. Modifications: cropped image. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Treatment
Approach [4][8][9][11]
- Provide patient education: Chronic pancreatitis is a relapsing and remitting disease.
- Start treatment of pain
- Recommend abstinence from nicotine and alcohol for all patients. [10]
- Monitor for and manage complications of chronic pancreatitis (e.g., pancreatic enzyme replacement therapy for exocrine pancreatic insufficiency).
- Initiate directed treatment of the underlying etiology of chronic pancreatitis, e.g.:
- Management of alcohol use disorder and nicotine addiction
- Management of hypertriglyceridemia in adults
- Management of hyperparathyroidism
Patients with CP may benefit from a multidisciplinary team providing individualized pain management and addressing psychosocial factors. [11]
Pharmacological pain management [4]
Provide pain management in a stepwise approach (see “Treatment of pain” for dosages).
- Start with nonopioid oral analgesics (e.g., NSAIDs and acetaminophen if not contraindicated).
- Consider adjuvant analgesics. [9]
- Tricyclic antidepressants (e.g., amitriptyline)
- SSRIs (e.g., fluoxetine)
- SNRIs (e.g., duloxetine)
- Gabapentinoids (e.g., pregabalin)
- Consider antioxidant therapy (e.g., combinations of selenium, ascorbic acid, beta carotene, and methionine).
- Limit opioid analgesics.
Pain management in chronic pancreatitis requires careful assessment and frequent reevaluation.
Interventional therapy
Endoscopic
- Indication: pain not adequately managed with pharmacotherapy
-
Procedures
- Celiac ganglion block repeated as needed (provides 3–6 months of relief)
- Endoscopic papillotomy with ductal dilation, stent placement, and removal of stones if present
- Extracorporeal shock wave lithotripsy (ESWL) to dissolve stones
Surgical [8]
-
Indications
- Intractable pain not adequately managed with pharmacotherapy or endoscopic procedures
- Other: suspected malignancy, complications
-
Procedures
- Thoracoscopic bilateral splanchnicectomy [20]
- Surgical decompression
- Lateral pancreaticojejunostomy: if the main pancreatic duct is dilated (> 5 mm)
- Sphincterotomy or sphincteroplasty
- Surgical resection
- Pancreaticoduodenectomy (Whipple procedure)
- Distal pancreatectomy
- Pylorus-preserving pancreaticoduodenectomy
- Total pancreatectomy with islet autotransplant (TPIAT) (last-line curative therapy)
Total pancreatectomy is the only known cure for chronic pancreatitis; it should be reserved for select patients with chronic pain after all other measures have failed. [4]
Complications
Recurrent acute pancreatitis [8]
See “Acute pancreatitis.”
Exocrine pancreatic insufficiency
- Pathophysiology in chronic pancreatitis: tissue atrophy and fibrosis → deficiency of lipase, amylase, and protease → maldigestion, steatorrhea, and malabsorption
- This condition is described in detail in the article “Malabsorption.”
Endocrine pancreatic insufficiency
- Pathophysiology: Destruction of beta cells leads to endocrine insufficiency with pancreatogenic diabetes (type 3c diabetes mellitus). [21]
- Clinical features: Brittle, insulin-dependent diabetes
-
Diagnostics
- Screen all patients annually with HbA1c or fasting plasma glucose measurement.
- See “Diagnostics” in “Diabetes mellitus.”
-
Treatment
- Specialist consultation (endocrinology) is advised.
- See “Antihyperglycemic treatment” in “Diabetes mellitus.”
Pancreatic pseudocysts [8][22]
Definition
Encapsulated collection of pancreatic fluid that develops 4 weeks after an acute attack of pancreatitis (can occur in both acute and chronic pancreatitis) [8]
Pathophysiology
Pancreatic secretions leak from damaged ducts → inflammatory reaction of surrounding tissue → encapsulation of secretions by granulation tissue
Clinical features [23]
- Often asymptomatic
- Painless abdominal mass
-
Pressure effects
- Gastric outlet obstruction (early satiety, nonbilious vomiting, abdominal pain)
- Obstruction of the distal duodenum (bilious vomiting) may result in steatorrhea.
- Bile duct obstruction with jaundice
Diagnostics [24]
- First line: CT abdomen with contrast
- Findings: Extrapancreatic fluid collection within well-defined wall or capsule with contrast enhancement
-
Other imaging modalities
-
Transabdominal ultrasound
- Fast and readily available
- High sensitivity, but low negative predictive value
- ERCP (gold-standard test): more invasive, but allows treatment to be performed
- MRI/MRCP: highly sensitive and specific test, but associated with high cost
-
Transabdominal ultrasound



Treatment [25]
-
Conservative management: : asymptomatic patients with small pancreatic pseudocysts and no complications
- Symptom management (e.g., nonopioid analgesics for pain, antiemetics for nausea)
- Alcohol cessation
- Low-fat diet with small, frequent meals
- Imaging surveillance
-
Endoscopic drainage
- First-line treatment
- Indications
- Asymptomatic patients with chronic large pancreatic pseudocysts
-
Symptomatic cysts
- Nausea and vomiting
- Anorexia and weight loss
- Persistent abdominal pain
- Suspected malignancy
- Complications
- Gastric outlet, duodenal, or biliary obstruction (e.g., common bile duct stenosis)
- Hemorrhage
- Infection
- Pancreatic pseudoaneurysm
- Compression of large vessels
- Pancreaticopleural fistula
- Percutaneous drainage: reserved for patients in whom endoscopic drainage is not technically feasible or was previously unsuccessful
-
Surgical drainage
- The cyst is drained into the stomach, duodenum, or jejunum (i.e., cystogastrostomy, cystoduodenostomy, cystojejunostomy).
- Reserved for patients in whom endoscopic and/or percutaneous interventions were previously unsuccessful or where surgical access is useful to treat suspected complications (e.g., necrosis, infection) in addition to drainage
- ERCP transpapillary drainage: reserved for pseudocysts that connect with the pancreatic duct
Complications
- Infection: fever, abdominal pain, sepsis
- Pseudocyst rupture: pancreatic ascites/pancreaticopleural fistula
- Erosion into an abdominal vessel: hemorrhage into the cyst
Pancreatic ascites
Pathophysiology
Ductal disruption (due to an acute attack of pancreatitis, pancreatic surgery and/or trauma) or a pseudocyst leak/rupture → pancreatic ascites
Clinical features
- Abdominal distention; variable abdominal pain
- Dyspnea
- Peripheral edema
- Free fluid in the peritoneal cavity
Diagnostics
- Ascitic fluid analysis: exudate (high protein: > 3 g/dL; low SAAG: < 1.1 g/dL) with high amylase levels (> 1,000 IU/L)
-
Imaging: ERCP, CECT, MRCP
- Identify ascites and the site(s) of the leak
- ERCP is preferred, as it allows treatment to be performed in the same sitting.
Management
-
Conservative management
- Indicated for all patients [26]
- Nothing by mouth, IV fluids, parenteral nutrition
- Somatostatin analogs (octreotide)
-
Interventions
- Repeated paracenteses
- Stenting of the pancreatic duct: if ERCP shows ductal disruption [27]
-
Surgery: indicated in patients showing no improvement after 4 weeks of conservative management (see “Pancreatic and hepatic surgery”)
- Pancreatic resection
- Surgery for pancreatic pseudocyst
- Lateral pancreaticojejunostomy
Further complications
- Pancreatic abscess
- Portal vein thrombosis
- Splenic vein thrombosis
- Pancreatic cancer (especially in patients with hereditary pancreatitis)
General screening for pancreatic cancer is not currently recommended. Screen patients (with a triphasic pancreas protocol CT) who develop weight loss, protracted abdominal pain, or functional decline. [4][8]
We list the most important complications. The selection is not exhaustive.
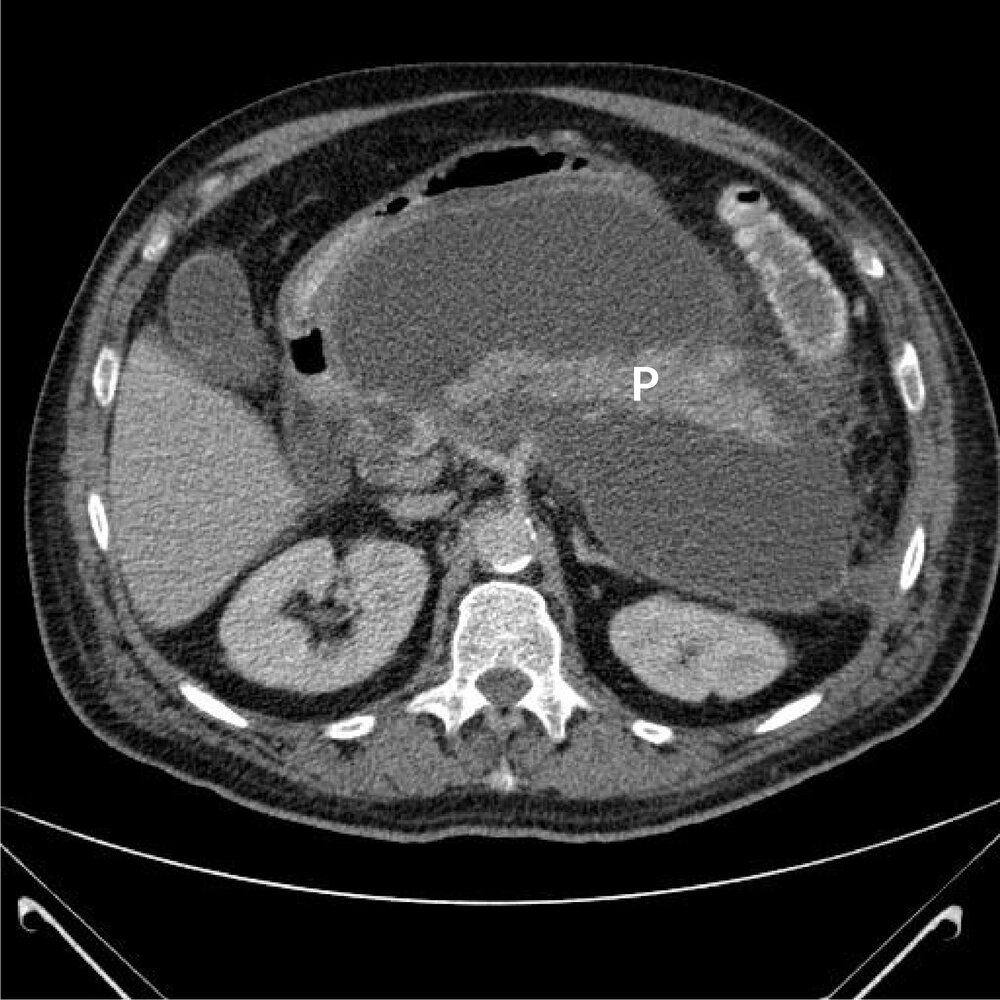
CT abdomen (with contrast; axial view)
A large circumscribed fluid collection (green overlay) with an enhancing wall (red overlay) surrounds the pancreas (P).
Source: “Pankreaspseudocyste 01 THWZ” by Thomas Zimmermann, Wikimedia Commons, licensed under CC BY-SA 3.0. Modifications: added P for pancreas, arrows removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Ultrasound abdomen of a patient with a history of pancreatitis
Targeted image shows a rounded, predominantly anechoic lesion (green overlay) with a few internal echoes and posterior acoustic enhancement (yellow overlay). Adjacent pancreas (P) tissue is visible.
P: pancreas
Source: © IMPP
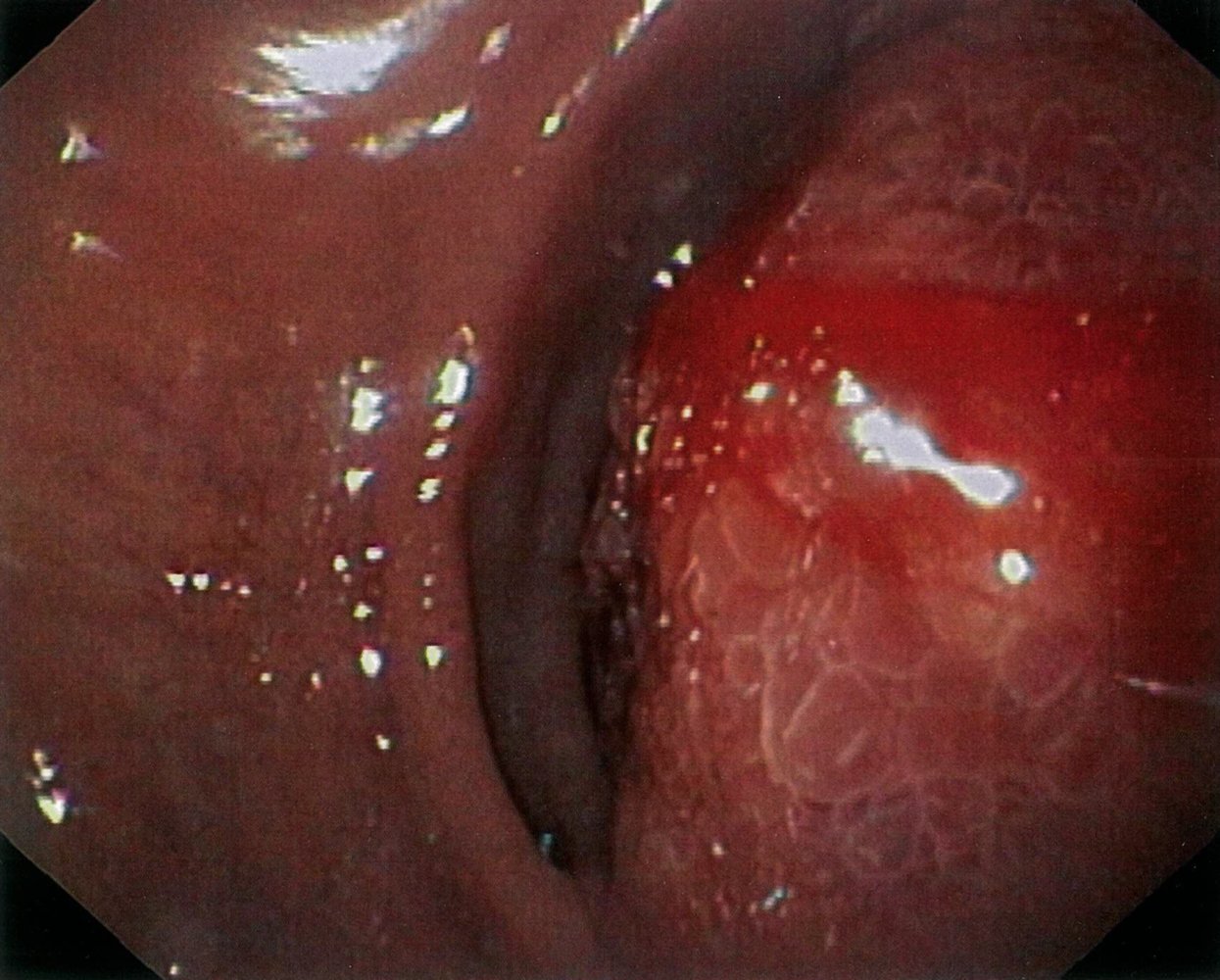
Endoscopic view of the duodenum
On the right, the lumen is partially obstructed due to extraluminal compression. The covering mucosa is edematous and an oozing hemorrhage can be seen. On the left, the typical plicae circulares of the duodenum are visible.
These findings are consistent with a pancreatic pseudocyst. Cross-sectional imaging should be performed to confirm the diagnosis.
Source: © IMPP
External Resources
References
- Apte MV, Pirola RC, Wilson JS. "Mechanisms of alcoholic pancreatitis". J Gastroenterol Hepatol. 25(12). :1816-1826. (2010)
- Howes N, Greenhalf W, Stocken DD, Neoptolemos JP. "Cationic Trypsinogen Mutations and Pancreatitis". Clin Lab Med. 25(1). :39-59. (2005)
- De Boeck K, Weren M, Proesmans M, Kerem E. "Pancreatitis among patients with cystic fibrosis: correlation with pancreatic status and genotype". Pediatrics. 115(4). :e463-469. (2005)
- Gardner TB, Adler DG, Forsmark CE, et al. "ACG Clinical Guideline: Chronic Pancreatitis". Am J Gastroenterol. 115(3). :322-339. (2020)
- Whitcomb DC. "Pancreatitis: TIGAR-O Version 2 Risk/Etiology Checklist With Topic Reviews, Updates, and Use Primers". Clin Transl Gastroenterol. 10(6). :e00027. (2019)
- "Chronic Pancreatitis"
- Barry K. "Chronic Pancreatitis: Diagnosis and Treatment". Am Fam Physician. 97(6). :385-393. (2018)
- Gupte A, Goede D, Tuite R, Forsmark CE. "Chronic pancreatitis". BMJ. :k2126. (2018)
- Majumder S, Chari ST. "Chronic pancreatitis". Lancet. 387(10031). :1957-1966. (2016)
- Vege SS, Chari ST. "Chronic Pancreatitis". N Engl J Med. 386(9). :869-878. (2022)
- Conwell DL et al. "American Pancreatic Association Practice Guidelines in Chronic Pancreatitis: evidence-based report on diagnostic guidelines.". Pancreas. 43(8). :1143-62. (2014)
- Issa Y, Kempeneers MA, van Santvoort HC, et al. "Diagnostic performance of imaging modalities in chronic pancreatitis: a systematic review and meta-analysis". Eur Radiol. 27(9). :3820-3844. (2017)
- Steer ML, Waxman I, Freedman S. "Chronic Pancreatitis". N Engl J Med. 332(22). :1482-1490. (1995)
- Duggan SN, Chonchubhair HMN, Lawal O, O'Connor DB, Conlon KC. "Chronic pancreatitis: A diagnostic dilemma". World J Gastroenterol. 22(7). :2304-2313. (2016)
- Manfredi R, Pozzi Mucelli R. "Secretin-enhanced MR Imaging of the Pancreas". Radiology. 279(1). :29-43. (2016)
- Hadidi A. "Pancreatic duct diameter: Sonographic measurement in normal subjects". J Clin Ultrasound. 11(1). :17-22. (1983)
- Nandhakumar N, Green MR. "Interpretations: How to use faecal elastase testing". Archives of Disease in Childhood - Education and Practice. 95(4). :119-123. (2010)
- Witt H. "The SPINK in chronic pancreatitis: similar finds, different minds". Gut. 50(5). :590-591. (2002)
- Maher JW, Johlin FC, Pearson D. "Thoracoscopic splanchnicectomy for chronic pancreatitis pain". Surgery. 120(4). :603-609. (1996)
- Hart PA, et al. "Type 3c (pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer". The Lancet Gastroenterology & Hepatology. 1(3). :226-237. (2016)
- "Pancreatic pseudocyst". https://medlineplus.gov/ency/article/000272.htm. [2019-10-16]
- Go VLW, Maule WF, Reber HA. "The Pancreas: biology, pathobiology, and disease". Raven Press. (1993). ISBN: 9780881679861
- Aghdassi AA, Mayerle J, Kraft M, et al. "Pancreatic pseudocysts – when and how to treat?". HPB (Oxford). 8(6). :432-441. (2006)
- Aghdassi A, Mayerle J, Kraft M, et al. "Diagnosis and Treatment of Pancreatic Pseudocysts in Chronic Pancreatitis". Pancreas. 36(2). :105-112. (2008)
- Kozarek RA. "Management of pancreatic ascites". Gastroenterol Hepatol. 3(5). :362-264. (2007)
- Kanneganti K, Srikakarlapudi S, Acharya B, Sindhaghatta V, Chilimuri S. "Successful Management of Pancreatic Ascites with both Conservative Management and Pancreatic Duct Stenting". Gastroenterology Res. 2(4). :245-247. (2009)
- Masamune A, Watanabe T, Kikuta K, Shimosegawa T. "Roles of pancreatic stellate cells in pancreatic inflammation and fibrosis". Clin Gastroenterol Hepatol. 7(11 Suppl). :S48-54. (2009)