Summary
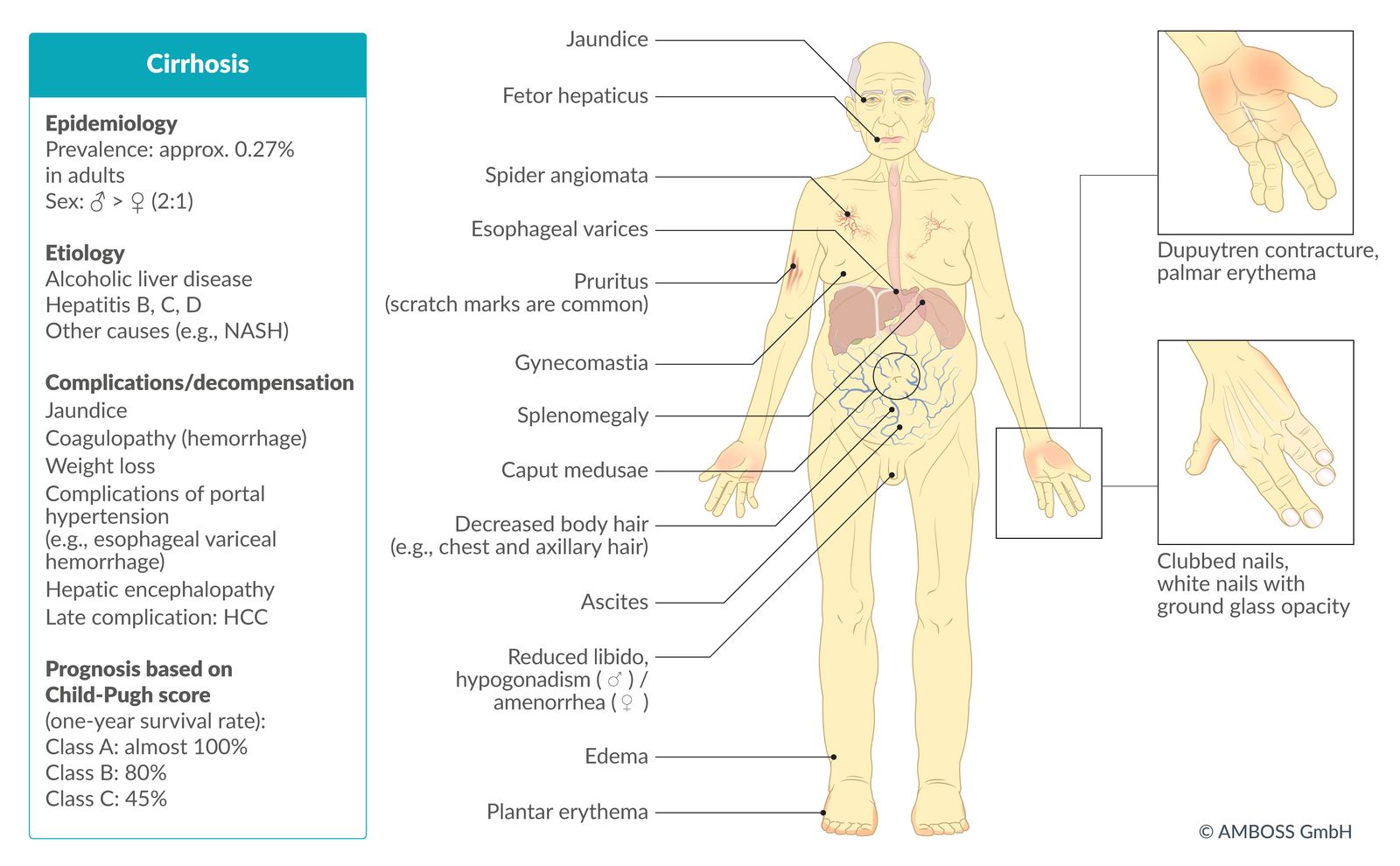
Cirrhosis is the final stage of chronic liver disease (CLD) and it is characterized by regenerative nodules and fibrous septae in liver parenchyma in response to chronic hepatic injury. Cirrhosis is most commonly due to excessive alcohol consumption, metabolic dysfunction-associated steatotic liver disease, or hepatitis C. Other causes include inflammatory or metabolic diseases, such as primary biliary cirrhosis and hemochromatosis. Subsequent hepatic repair mechanisms lead to fibrosis progressing to cirrhosis with abnormal tissue architecture and impaired liver function. Patients can present with a range of symptoms, including ascites; hepatosplenomegaly; and skin manifestations of cirrhosis, such as jaundice, spider angiomata, and/or palmar erythema. Men may also present with signs of feminization (e.g., gynecomastia, hypogonadism). In severe cases, the accumulation of toxic metabolites or involvement of additional organs can lead to complications such as hepatic encephalopathy and hepatorenal syndrome (HRS). Laboratory study findings indicate hepatocyte damage (e.g., elevated liver enzymes, hyperbilirubinemia) and/or impaired hepatic synthetic function (e.g., prolonged prothrombin time, low albumin). Abdominal ultrasound typically shows atrophic, heterogeneous liver parenchyma with a nodular surface. A biopsy is the method of choice for confirming the diagnosis; however, it is usually only performed if the results from other diagnostic modalities are inconclusive. Management consists of treatment of the underlying disease (e.g., avoidance of toxic substances, antiviral drugs), adequate calorie intake, and treating complications, e.g., esophageal varices, hepatocellular carcinoma (HCC). In cases of decompensated cirrhosis, interventional procedures may be used to alleviate symptoms (e.g., paracentesis to drain ascites) or as a bridge until liver transplantation is possible.
For details about pulmonary complications that occur in individuals with cirrhosis (e.g., hepatopulmonary syndrome, portopulmonary hypertension, and hepatic hydrothorax), see "Pulmonary complications of cirrhosis."

© AMBOSS
Definitions
- Liver fibrosis: the reversible proliferation of fibroblasts and accumulation of excessive extracellular matrix components (e.g., crosslinked type 1 collagen) in liver parenchyma in response to hepatic injury [1]
- Advanced chronic liver disease (ACLD): suspected cirrhosis in the absence of biopsy, based on liver elastography and platelet count [2]
- Cirrhosis: the final stage of CLD; characterized by regenerative nodules and fibrous septae (usually irreversible) in liver parenchyma in response to hepatic injury [2][3]
- Compensated cirrhosis: the asymptomatic stage of cirrhosis in which complications of portal hypertension (e.g., overt ascites, variceal bleeding, hepatic encephalopathy) are absent; evidence of portal hypertension (e.g., gastroesophageal varices) may be present.
- Decompensated cirrhosis: the development of complications of portal hypertension (e.g., overt ascites, variceal bleeding, hepatic encephalopathy) in a patient with cirrhosis; often triggered by an acute event (e.g., infection, alcohol intake, certain medications) but can also develop gradually (e.g., accumulation of fluid in ascites)
Epidemiology
- Prevalence: approx. 0.27% in US adults [4]
- Sex: ♂ > ♀ (2:1) [5]
-
Mortality [5]
- Responsible for approx. 1–2% of all deaths in the US (12th leading cause of death)
- Most deaths occur in the fifth to sixth decade of life.
Epidemiological data refers to the US, unless otherwise specified.
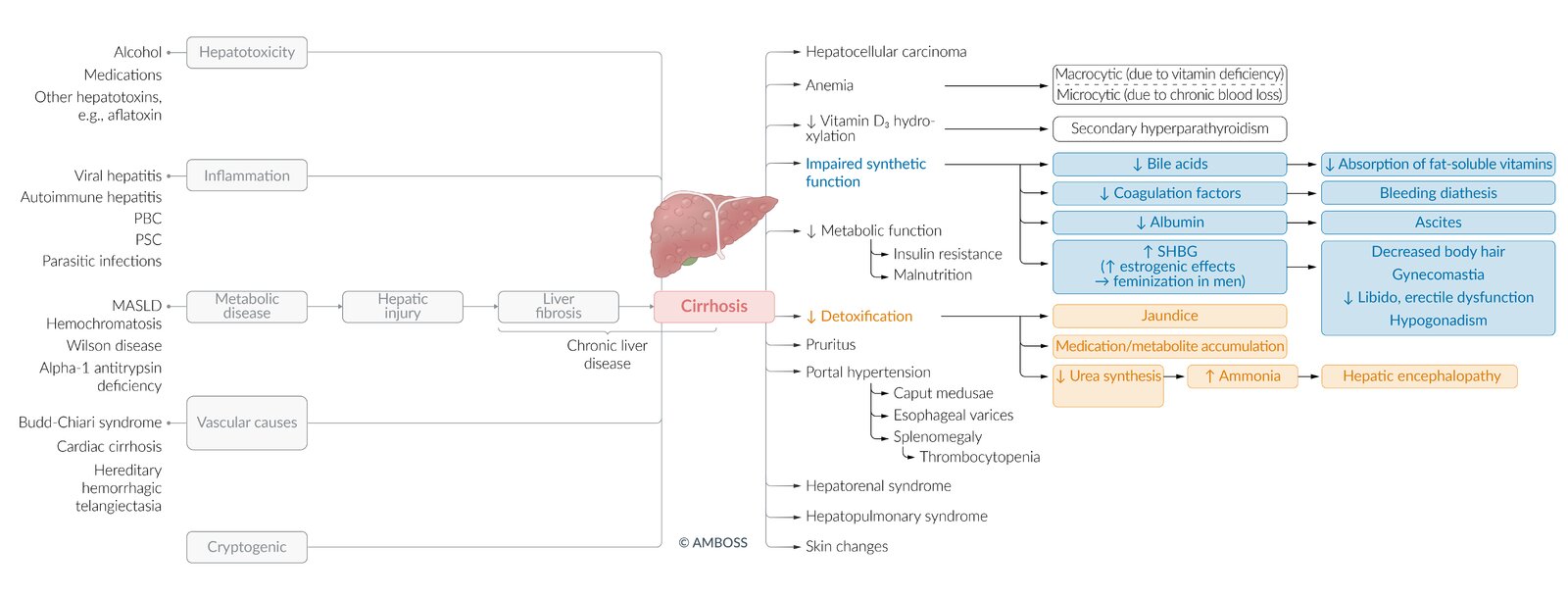
Etiology
See also “Etiology of chronic liver disease.”
- Chronic hepatitis C (most common cause of cirrhosis in the US)
- Chronic alcohol use disorder (AUD)
- Metabolic dysfunction-associated steatotic liver disease (MASLD)
- Autoimmune conditions: e.g., type 1 AIH, PBC, PSC
- Genetic conditions: e.g., hereditary hemochromatosis, Wilson disease, α1-antitrypsin deficiency
- Hepatic vein congestion or vascular anomalies: e.g., Budd-Chiari syndrome, cardiac cirrhosis
- Cryptogenic cirrhosis: cirrhosis of unknown etiology despite adequate diagnostics

Cryptogenic cirrhosis is a diagnosis of exclusion and should only be considered after a complete patient evaluation has ruled out all other possible causes of cirrhosis.
Hepatitis C, alcohol-associated liver disease, and MASLD are the most common causes of cirrhosis worldwide. [6]
© AMBOSS
Pathophysiology
- Cirrhosis is characterized by irreversible diffuse fibrosis of the liver (the final common pathway for chronic liver diseases).
- Pathogenesis is multifactorial.
- Different liver cells and cytokines are involved in the activation and progression of liver fibrosis.
- Cytokine‑mediated activation of hepatic stellate cells has been identified as a central element for developing fibrosis.
-
The following three mechanisms have been described for all types of liver cirrhosis: [7]
-
Degeneration and necrosis of hepatocytes
- Activated Kupffer cells destroy hepatocytes, activate hepatic stellate cells, and promote inflammation.
- Inflammatory cytokines (e.g., TGF-β, PDGF) → hepatocyte apoptosis and hepatic stellate cell activation → excess collagen production
-
Fibrotic tissue and regenerative nodules replace the liver parenchyma
- Hepatocyte destruction triggers repair mechanisms → excess formation of connective tissue (fibrosis)
- Excessive connective tissue in periportal zone and centrilobular zone → regenerative nodules and fibrous septa → compression of hepatic sinusoids and venules → ↑ portal vein hydrostatic pressure → intrasinusoidal hypertension → ↓ functional sinusoids
- Loss of liver function: sinusoidal capillarization → loss of fenestration and scar tissue formation→ impaired substrate exchange → loss of normal liver function (exocrine and metabolic)
-
Degeneration and necrosis of hepatocytes
Clinical features
Cirrhosis can be asymptomatic or manifest with nonspecific features. Symptoms are triggered by an acute event (e.g., infection, certain medications) or due to gradual progression of liver damage.
Nonspecific features
- Patients are often initially asymptomatic.
- Fatigue, malaise, anorexia, and weight loss
Specific features
Dermal features
- Pruritus
- Jaundice
- Telangiectasia: most commonly spider angioma (a central red arteriole with numerous, thin arterial extensions, commonly manifesting on light, sun-exposed skin and the trunk)
- Caput medusae
- Palmar erythema (plantar erythema also possible) [8]
- Nail clubbing
- Petechiae and purpura
- Generally dry and atrophic skin
- White nails with ground-glass opacity (also known as “Terry nails”)
- Lacquered lips, smooth red tongue
")





Abdominal features
- Nausea, vomiting
- Hepatomegaly (possibly causing dull RUQ pain)
- Splenomegaly
- Ascites
Hormonal disorders
-
Hyperestrogenism [9]
- Changes in the hepatic metabolization of sex hormones cause an imbalance in the estrogen-androgen ratio, resulting in a marked increase in systemic estrogen levels.
-
In men, increased estrogen levels cause feminization.
- Gynecomastia
- Hypogonadism; (e.g., testicular atrophy, reduced libido, erectile dysfunction, infertility)
- Decreased body hair (e.g., loss of chest hair, a female pattern of pubic hair distribution)
- In women, a massive increase in estrogen can cause amenorrhea.
Other
- Asterixis
- Fetor hepaticus: bad breath with a characteristic sweet, pungent smell caused by an accumulation of dimethyl sulfide
- Dupuytren contracture (in patients with cirrhosis due to AUD) [10][11]
- Peripheral edema [12]
- See also “Clinical features” in “Portal hypertension.”
Specific clinical features due to rare causes
- Hemochromatosis: dark, bronze skin color, and diabetes (bronze diabetes)
-
Wilson disease
- Neurological/psychiatric symptoms (parkinsonism and personality changes)
- Indirect hyperbilirubinemia due to hemolysis.
- Alpha‑1 antitrypsin deficiency: lung emphysema (typically before 50 years of age) [13]

Image source of original image: www.medizinwelten.de. Created by: Dr. R. Feik, Klinikum Achern.

Small dilated blood vessels with a threadlike appearance are visible.
This is the typical appearance of telangiectasia.
Source: “Teleangiektasie” by Klaus D. Peter, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}

A telangiectasia characterized by a vascular arcade branching out from a central arteriolar point. Spider angiomas can arise during childhood or pregnancy as well as in patients with liver disease or thyrotoxicosis.
Source: Courtesy of Dr. Gary M. White, MD

© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
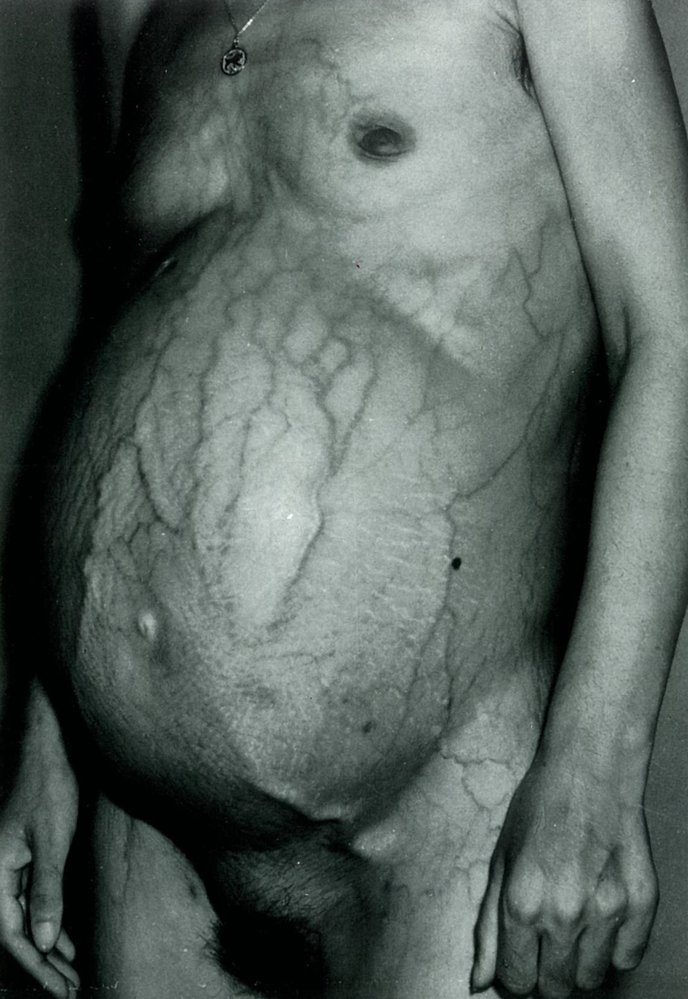
There is distention of the abdomen (ascites) and periumbilical dilatation of subcutaneous veins (caput medusae).
These findings are characteristics of decompensated liver disease.
Source: © IMPP

There is bulbous enlargement of the distal phalanges and the nail curvatures are markedly increased.
Source: “CongenitalHeartCase-133” by Herbert L. Fred, MD and Hendrik A. van Dijk, openstax cnx, licensed under CC BY-SA 3.0.
Diagnosis
General principles [14][15]
- Diagnosis is typically based on a combination of typical clinical features, laboratory findings, and features on imaging.
- Initial evaluation
- Routine laboratory studies and screening for the underlying etiology (e.g., viral hepatitis panel)
- Abdominal ultrasound to evaluate the liver parenchyma and detect complications
- Additional evaluation (e.g., noninvasive liver fibrosis assessment, liver biopsy) may be needed to stage fibrosis or if the etiology remains unclear.
Patients with cirrhosis are usually either asymptomatic with incidental abnormal findings on laboratory studies or imaging, or present late with features of decompensated cirrhosis.
Laboratory studies
Routine laboratory studies [14][16][17]
Laboratory findings are nonspecific and the presence and degree of abnormality may vary.
-
Liver chemistries
-
Transaminases: ↑ ALT and AST
- ALT > AST: present in most liver diseases (e.g., MASLD, viral hepatitis)
- AST > ALT: indicative of alcohol-associated liver disease and/or cirrhosis of any etiology
- Massive AST and/or ALT elevation (> 15 times ULN): Consider differential diagnoses (e.g., acetaminophen toxicity, acute viral hepatitis, autoimmune hepatitis).
- ↑ Bilirubin (may be normal initially)
- ↑ ALP
- ↑ Gamma‑glutamyl transferase (GGT)
-
Transaminases: ↑ ALT and AST
- Coagulation studies: ↑ prothrombin time (↑ INR) because of decreased production of coagulation factors
-
CBC
- Thrombocytopenia: due to decreased thrombopoietin production by the liver and/or splenomegaly [16]
- Anemia: multiple potential causes, e.g., vitamin B12 or folate deficiency , chronic blood loss, splenic sequestration
- Leukopenia
-
CMP
- ↓ Albumin
- ↓ Total protein
- Hyponatremia
Liver chemistries may be normal in early compensated cirrhosis. [14]
Some CBC abnormalities are due to the combination of increased hepatic and splenic sequestration of thrombocytes (portal hypertension leads to splenomegaly with hypersplenism) and decreased production of hematopoietic factors by the liver.
Hepatocyte injury: ↑ AST, ALT, ALP, GGT. Synthetic dysfunction: ↑ bilirubin and PT/INR; ↓ albumin and platelets
Additional laboratory studies [14][17][18][19]
These studies may help to identify the underlying etiology and further evaluate liver function. Modification may be required based on clinical features and the presence of risk factors.
-
Viral hepatitis: especially in patients with risk factors
- Hepatitis B and hepatitis C: HBsAg, IgM anti-HBc, anti-HCV
- Hepatitis A and hepatitis E: IgM HAV, IgM HEV
- MASLD: fasting lipid levels and HbA1c
- Hemochromatosis: serum iron, ferritin, transferrin saturation
- Alcohol-associated liver disease: assess for alcohol use disorder; consider measuring alcohol biomarkers.
- Autoimmune hepatitis: total IgG or serum electrophoresis (showing hypergammaglobulinemia), ANA, ASMA, anti-LKM-1 antibody, anti-soluble liver antigen antibody
- Alpha-1 antitrypsin deficiency: alpha-1 antitrypsin level and phenotype
- Wilson disease: serum ceruloplasmin, serum total and free copper, urinary copper
- Primary biliary cholangitis: antimitochondrial antibodies (AMA or AMA-M2), ALP, bilirubin
- Primary sclerosing cholangitis: cholestasis parameters (GGT, ALP, and bilirubin), pANCA, IgG
- Other tests [20][21]
- Ammonia (not routinely indicated) [21]
- Plasma cholinesterase
- Serum protein electrophoresis: ↓ albumin band, ↑ gamma band, and unchanged alpha‑1, alpha‑2, and beta globulin fractions [20]

Imaging
Abdominal ultrasound with Doppler [14][22]
-
Indications
- Suspected cirrhosis: best initial test
- Established cirrhosis: for HCC screening and detecting complications
-
Findings
-
Liver form and structure
- Nodular liver surface
- Atrophy of the right lobe
- Loss of structural homogeneity (hyperechoic or variable increase in echogenicity) with fibrous septa
-
Liver size
- Initially enlarged [23]
- Atrophy with disease progression [23]
- Hypertrophy of the caudate lobe and left lobe [22][24]
- Atrophy of segment IV
-
Other possible findings
- Changes in liver vasculature
- Complications of portal hypertension: ascites, splenomegaly, portal vein thrombosis (PVT), increased portosystemic collateral flow [25]
-
Liver form and structure


CT abdomen [22][26]
- Indication: patients in whom adequate assessment with ultrasound is not possible (e.g., because of obesity)
-
Findings: similar to those on ultrasound
- Relative hypertrophy of the left lobe and caudate lobe
- Regenerative nodules
- Irregular liver surface
- Indirect findings: ascites, splenomegaly, portosystemic collaterals

Noninvasive liver fibrosis assessment
Blood biomarker-based scores [14][27]
These biomarker-based tools can be used as an adjunct to confirm and stage cirrhosis of certain etiologies.
-
AST-to-platelet ratio index (APRI)
- Indications: chronic hepatitis B and C, MASLD, AIH, and PBC
- Parameters: AST and platelet count
- Interpretation: APRI > 1 is suggestive of cirrhosis.
-
Fibrosis-4 score
- Indications: chronic hepatitis B and C and MASLD
- Parameters: age, platelet count, AST and ALT levels
- Interpretation: Thresholds for identifying advanced fibrosis depend on the underlying cause.
-
NAFLD fibrosis score
- Indication: MASLD
- Parameters: age, BMI, AST, ALT, platelet count, albumin, and diabetes (or impaired fasting glucose)
- Interpretation: A score > 0.676 is predictive of advanced fibrosis in MASLD.

Liver elastography [14][28][29]
- Definition: an imaging technique that measures liver stiffness to help determine the degree of fibrosis
-
Indications
- Diagnosis and staging of liver fibrosis and cirrhosis in adults with chronic HCV, chronic HBV, MASLD, ALD, or chronic cholestatic liver disease [30]
- Diagnostic confirmation of suspected portal hypertension
-
Modalities
- Transient elastography (most common): uses a device (FibroScan®) that only performs elastography; no direct visualization of the liver [29]
- Acoustic radiation force impulse: integrated into a conventional ultrasound system, enabling simultaneous elastography and visualization of the liver [31]
- Magnetic resonance elastography: uses MRI to generate a map of tissue stiffness (i.e., elastogram) according to the propagation of induced shear waves [32]
Liver biopsy [14][17]
-
Indications
- In cases of diagnostic uncertainty (gold standard)
- Grading and staging of inflammation and fibrosis (e.g., using the IASL score or METAVIR score)
- Monitoring treatment response (e.g., in autoimmune hepatitis)
- Evaluation of focal lesions
- Findings: See “Pathology.”
Noninvasive studies can identify mild fibrosis and advanced fibrosis but cannot accurately identify intermediate stages; therefore, invasive studies may be needed.
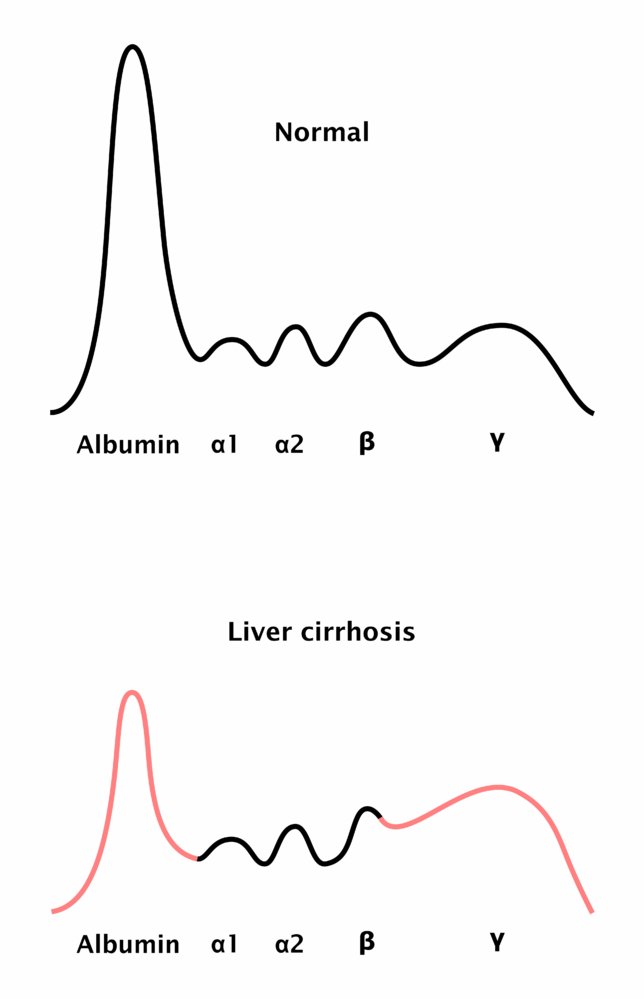
Serum protein electrophoresis in cirrhosis shows a reduced albumin band, an increased gamma band, and a beta-gamma bridge.
© AMBOSS

Ultrasound liver (longitudinal oblique plane)
The liver (L) has decreased in size and has an irregular surface (examples indicated by arrowheads), consistent with cirrhosis. The presence of ascites (green overlay) indicates decompensated cirrhosis.
Other ultrasound findings that may be seen in cirrhosis include coarse and heterogeneous echotexture, segmental hypertrophy and atrophy, Doppler flow alterations, and splenomegaly. Elastography can be performed to measure liver stiffness.
G: gallbladder; PV: portal vein
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
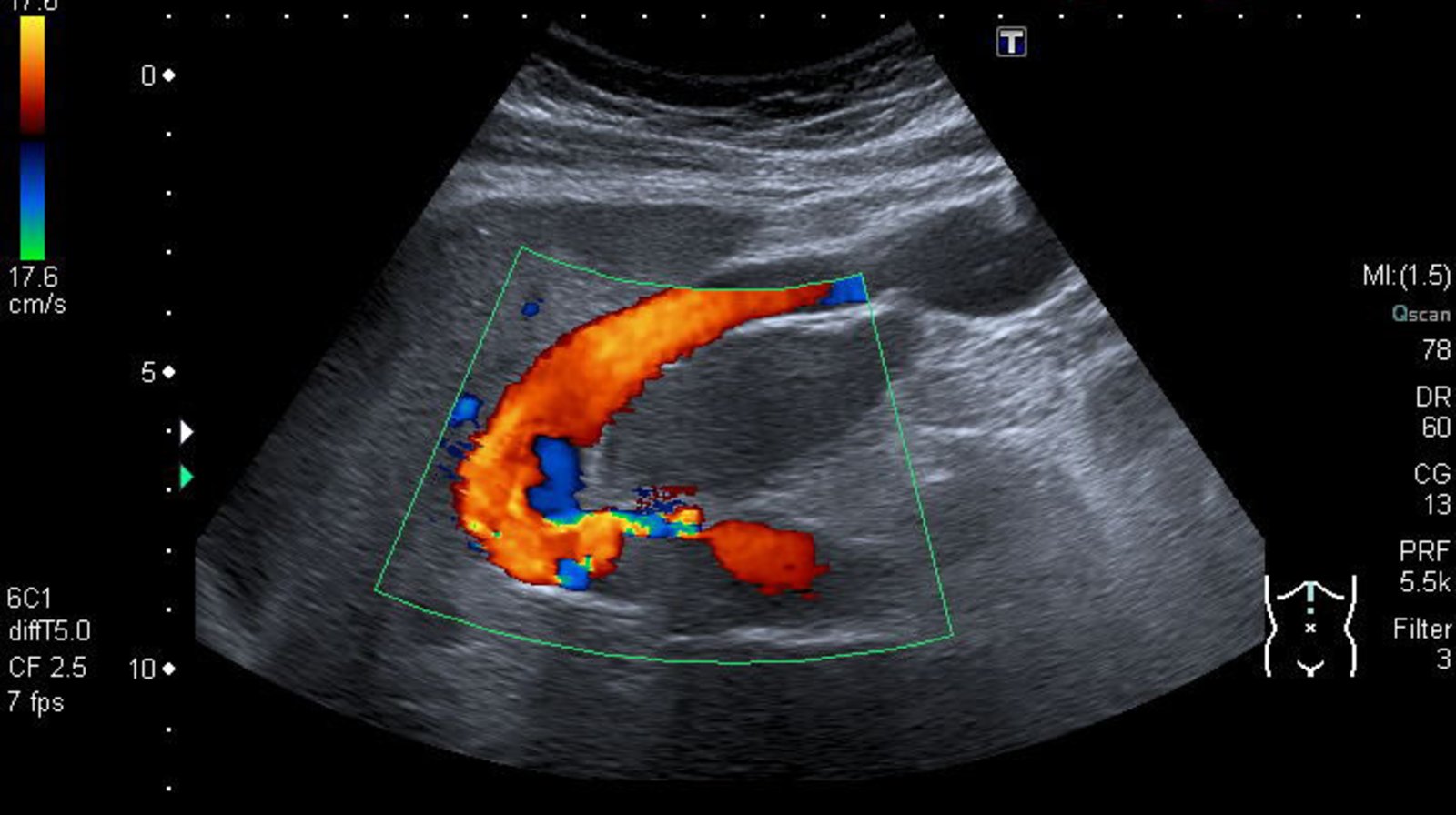
Ultrasound liver (color Doppler; longitudinal plane) of a patient with hepatic cirrhosis
The umbilical vein is dilated. The direction of blood flow (arrow) is primarily toward the transducer (red), from the liver (L) to the umbilicus.
The findings are consistent with recanalization of a paraumbilical vein, which occurs secondary to portal hypertension.
Arrow: flow direction
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
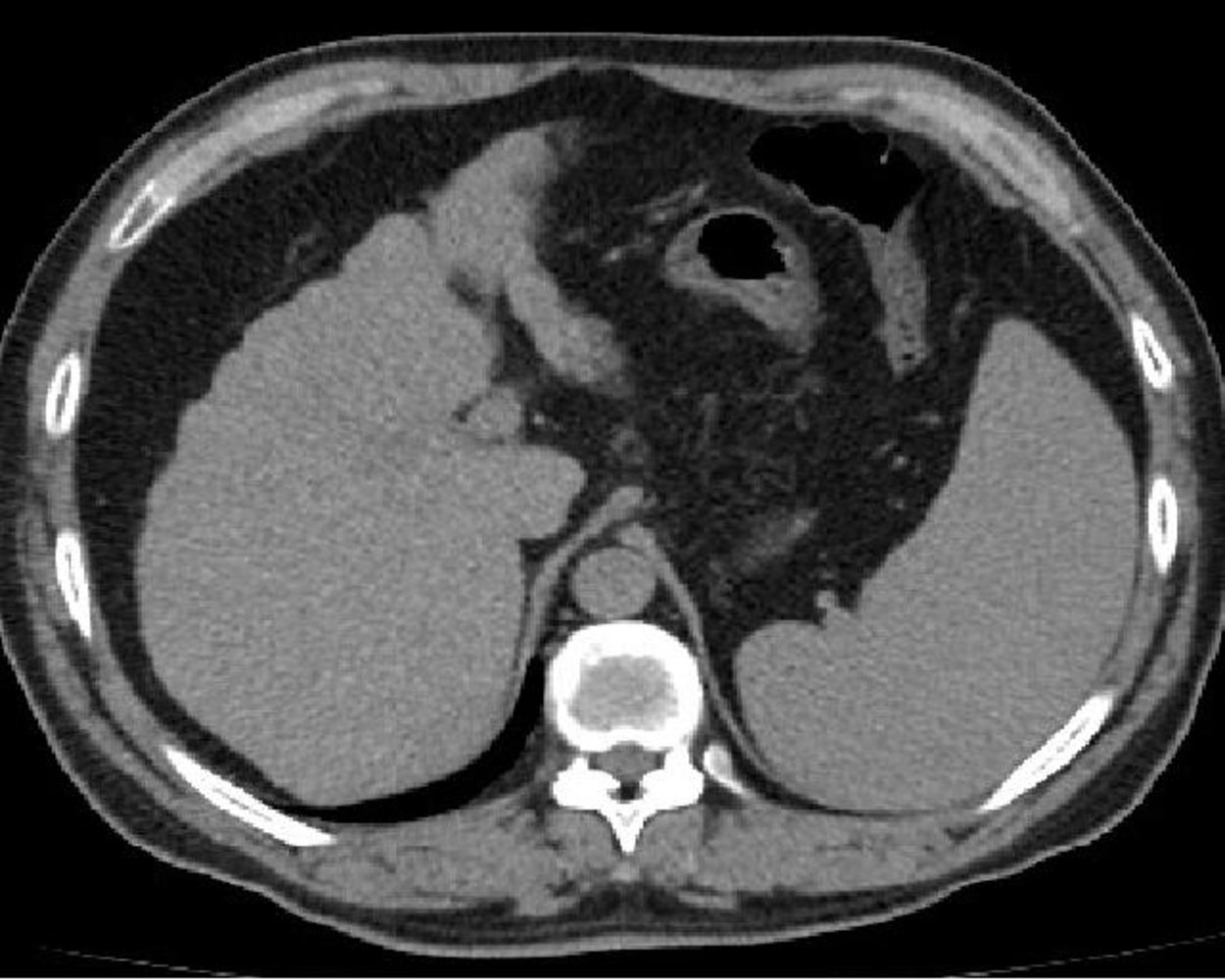
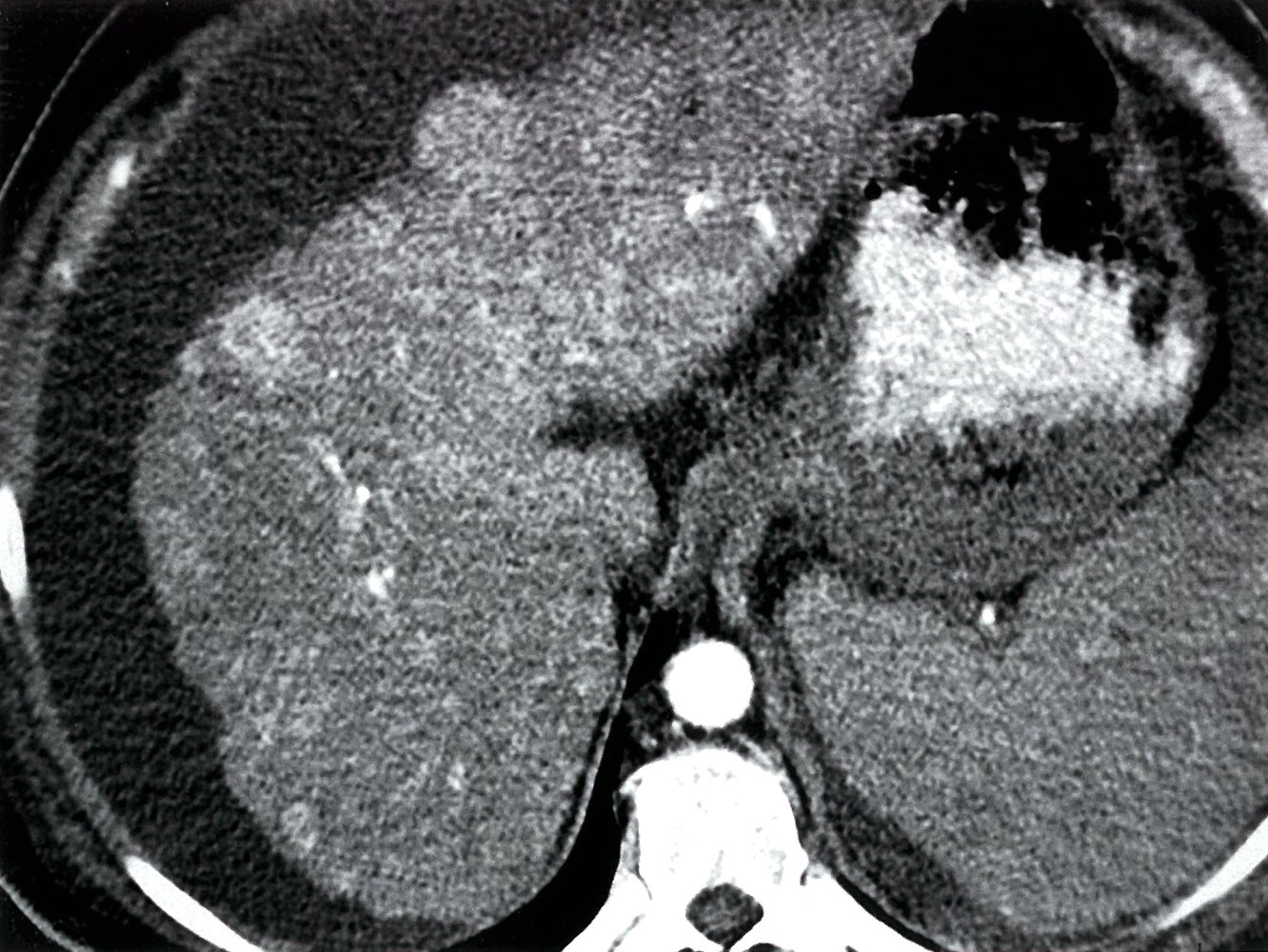
CT abdomen (without contrast; axial plane)
Atrophy and nodularity (indicated by white arrows) are seen along the anterolateral margin of the liver. The spleen is enlarged (green overlay).
The findings are consistent with hepatic cirrhosis with portal hypertension and splenomegaly.
An additional finding is a small hypoattenuating lesion in the lateral segment of the left lobe.
Source: “Liver cirrhosis” by Inversitus, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Prognosis
MELD and Child-Pugh scores are essential for assessing liver disease severity and guiding treatment decisions.
Model for end-stage liver disease score (MELD score) [33]
- Used to predict the three-month mortality rate of patients with cirrhosis
- Primarily used to prioritize patients for liver transplantation [33]
- Patients are given a score from 6 to 40 based on serum bilirubin, INR, and creatinine levels.
- Patients with high scores have the worst prognosis without intervention and should therefore be prioritized for transplantation (if appropriate)
Child-Pugh score [34]
- A prognostic grading scale that assesses survival rate and predicts the likelihood of developing complications based on bilirubin and albumin levels, prothrombin time, and the presence of ascites and encephalopathy
- Can be used as a prognostic scoring system [35]
- Child‑Pugh class A: one-year survival rate of ∼ 100%
- Child‑Pugh class B: one-year survival rate of ∼ 80%
- Child‑Pugh class C: one-year survival rate of ∼ 45%
| Child-Pugh score | |||
|---|---|---|---|
| Findings | Points | ||
| 1 | 2 | 3 | |
| Serum albumin (g/dL) | > 3.5 | 2.8–3.5 | < 2.8 |
| Serum bilirubin (mg/dL) | < 2.0 | 2.0–3.0 | > 3.0 |
| INR | < 1.7 | 1.7–2.3 | > 2.3 |
| Ascites | None | Mild | Moderate |
| Hepatic encephalopathy | None | Minimal | Advanced |
| |||
CHILD's ABCDEs: Albumin, Bilirubin, Coagulation (i.e., ↑ INR), Distended abdomen (i.e., ascites), and Encephalopathy
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Management
Treat the underlying condition (e.g., treatment of AUD, antivirals for HCV) and refer to a specialist (e.g., hepatologist) to optimize management.
Supportive care for cirrhosis [3][14][36][37]
-
Encourage alcohol abstinence
- Complete abstinence is recommended.
- Initiate treatment for alcohol use disorder if present.
-
Reconcile medication list
- Stop hepatotoxic medications.
- Avoid prescribing medications associated with complications, e.g.: [36]
- NSAIDs
- Opioids
- Benzodiazepines in patients with hepatic encephalopathy
- Medications that reduce effective arterial volume (e.g., ACE inhibitors, ARBs) in patients with ascites [38]
-
Reduce the risk of infection-associated complications, e.g.:
- Recommended immunizations: pneumococcal (PPSV23), hepatitis A, hepatitis B, influenza, SARS-CoV-2, and tetanus vaccination [39]
- Avoidance of raw seafood and unpasteurized dairy [14]
-
Address nutritional status [37]
- Routinely assess for malnutrition, including:
- Micronutrient deficiencies (e.g., zinc deficiency, vitamin D deficiency)
- Frailty assessment and/or sarcopenia assessment (e.g., hand grip strength, calf circumference)
- See “Clinical evaluation” and “Diagnosis” in “Unintentional weight loss and malnutrition in adults.”
- Dietary recommendations
- Aim for 1.0–1.5 g of protein per kilogram of dry body weight daily; protein restriction is not recommended. [37]
- Recommend eating frequent small meals.
- Consider early specialized nutritional support to hospitalized patients with cirrhosis.
- Routinely assess for malnutrition, including:
Screening for complications
HCC and portal vein thrombosis [2]
- Abdominal ultrasound every 6 months in patients with compensated cirrhosis [2]
- See “Screening for hepatocellular carcinoma” and “Portal vein thrombosis” for details.
Esophageal varices [2][40]
For patients with known varices, see “Monitoring of low-risk varices” in “Esophageal varices.”
- Decompensated cirrhosis: EGD upon diagnosis to assess for varices and high-risk features for esophageal variceal hemorrhage
-
Compensated cirrhosis with evidence of CSPH
-
EGD in patients not already treated with a nonselective beta blocker (NSBB) who have both:
- Liver stiffness > 20 kPa on transient elastography [2]
- Platelet count ≤ 150,000/mm3 [2]
- Frequency
- Every 2 years if ongoing liver injury [2]
- Every 3 years if no ongoing liver injury [2]
-
EGD in patients not already treated with a nonselective beta blocker (NSBB) who have both:
- Compensated cirrhosis without CSPH: annual platelet count and liver stiffness assessment (with transient elastography), or EGD if noninvasive liver fibrosis assessment is unavailable
Do not screen for esophageal varices with EGD if results will not change management (e.g., patients without CSPH who have liver stiffness < 20 kPa AND platelet count > 150,000/mm3, patients already treated with NSBBs). [2]
Management of common complications
-
See “Treatment of ascites” for details on:
- Fluid restriction if hyponatremic [38]
- Serum sodium level < 125 mmol/L: < 1L/day and cessation of diuretics
- Serum sodium level < 120 mmol/L: Consider IV albumin and additional fluid restriction.
- Dietary sodium restriction, e.g., ≤ 2 g/day [38]
- Pharmacotherapy, e.g., spironolactone (off-label) [38]
- Paracentesis indications and considerations
- Management of refractory ascites
- Fluid restriction if hyponatremic [38]
-
See “Spontaneous bacterial peritonitis” for details on:
- Prophylaxis for SBP
- Indications for diagnostic paracentesis in SBP
- Peritoneal fluid analysis in SBP
- Empiric antibiotic therapy for SBP
- Adjunctive therapy, e.g., IV albumin (off-label) [38]
- Monitoring, e.g., repeat paracentesis after 48 hours to assess response to antibiotics [38]
- Acute management checklist for SBP
-
See “Esophageal varices” for details on:
- Prophylaxis against variceal bleeding with NSBBs, e.g., carvedilol [2]
-
Management of esophageal variceal hemorrhage
- Vasoactive medication, e.g., octreotide (off-label) [41]
- Antibiotic prophylaxis, e.g., ceftriaxone (off-label) [38]
-
See “Treatment of hepatic encephalopathy” for details on:
- Treatment with lactulose
- Disposition
- Prevention with lactulose and rifaximin
-
See “Hepatorenal syndrome” for details on:
- Diagnostic criteria for HRS-AKI
- Treatment for HRS-AKI (e.g., terlipressin, renal replacement therapy)




Liver transplant [42]
- Liver transplant is the only curative treatment option.
- Indications for liver transplant evaluation include:
- Occurrence of an index complication (i.e., ascites, hepatic encephalopathy, variceal hemorrhage)
- Hepatocellular dysfunction resulting in a MELD score of ≥ 15
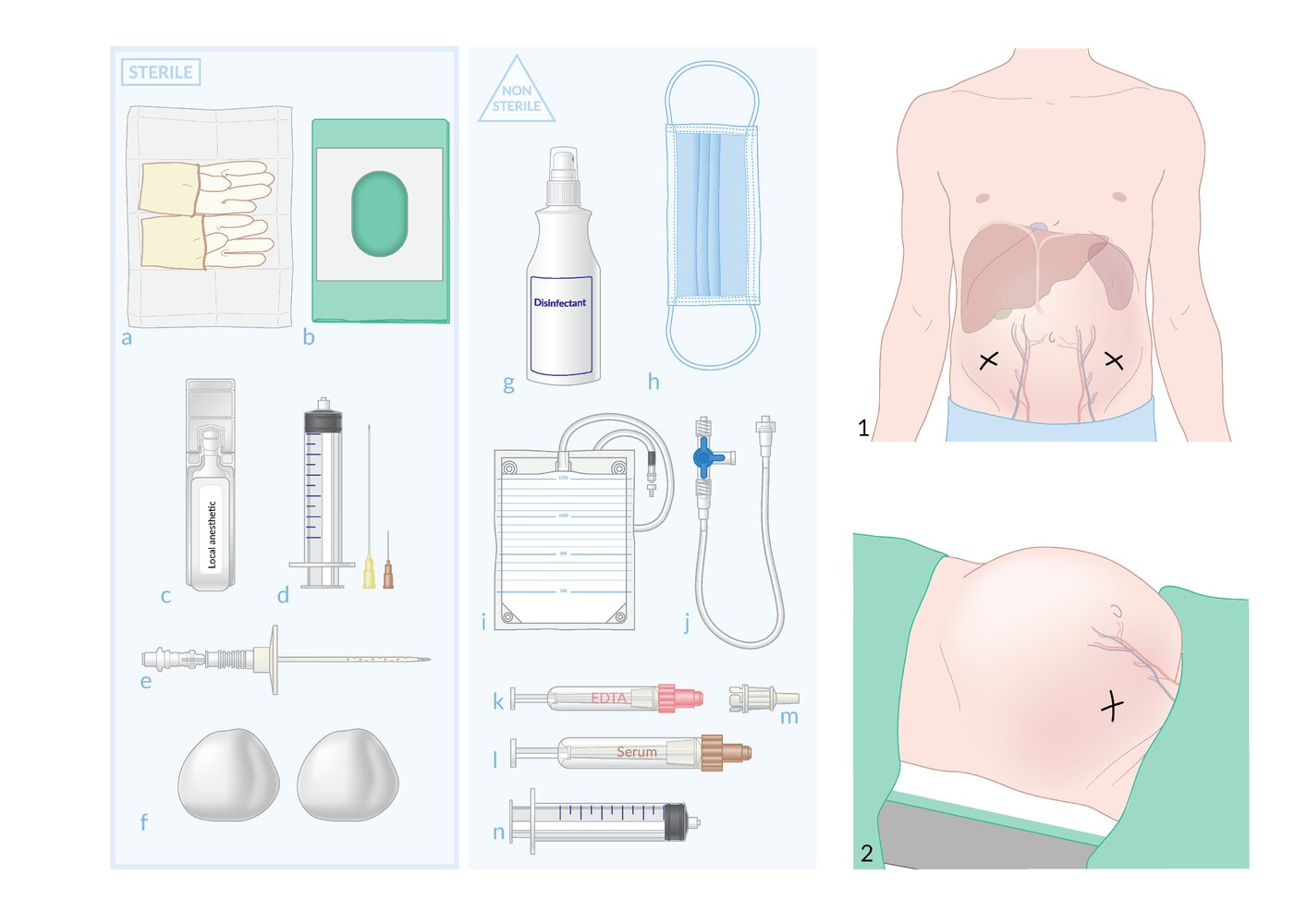
Sterile materials (left)
(a) Gloves
(b) Fenestrated surgical drape
(c) Local anesthetic
(d) Syringe and needles for superficial and deep infiltration of local anesthetic
(e) Paracentesis needle and catheter
(f) Gauze
Nonsterile materials (middle)
(g) Antiseptic
(h) Face mask
(i) Drainage system
(j) Three-way stopcock and fluid collection tubing
(k–l) Specimen collection vials
(m) Adapter for sample collection
(n) Syringe for sample collection
Insertion and positioning (right)
(1) Insertion site: typically in the lower quadrants, ~ 4–5 cm cephalad and ~ 4–5 cm medial to the anterior superior iliac spine
(2) Positioning: The patient is usually supine, either completely flat or with the upper body slightly elevated.
© AMBOSS
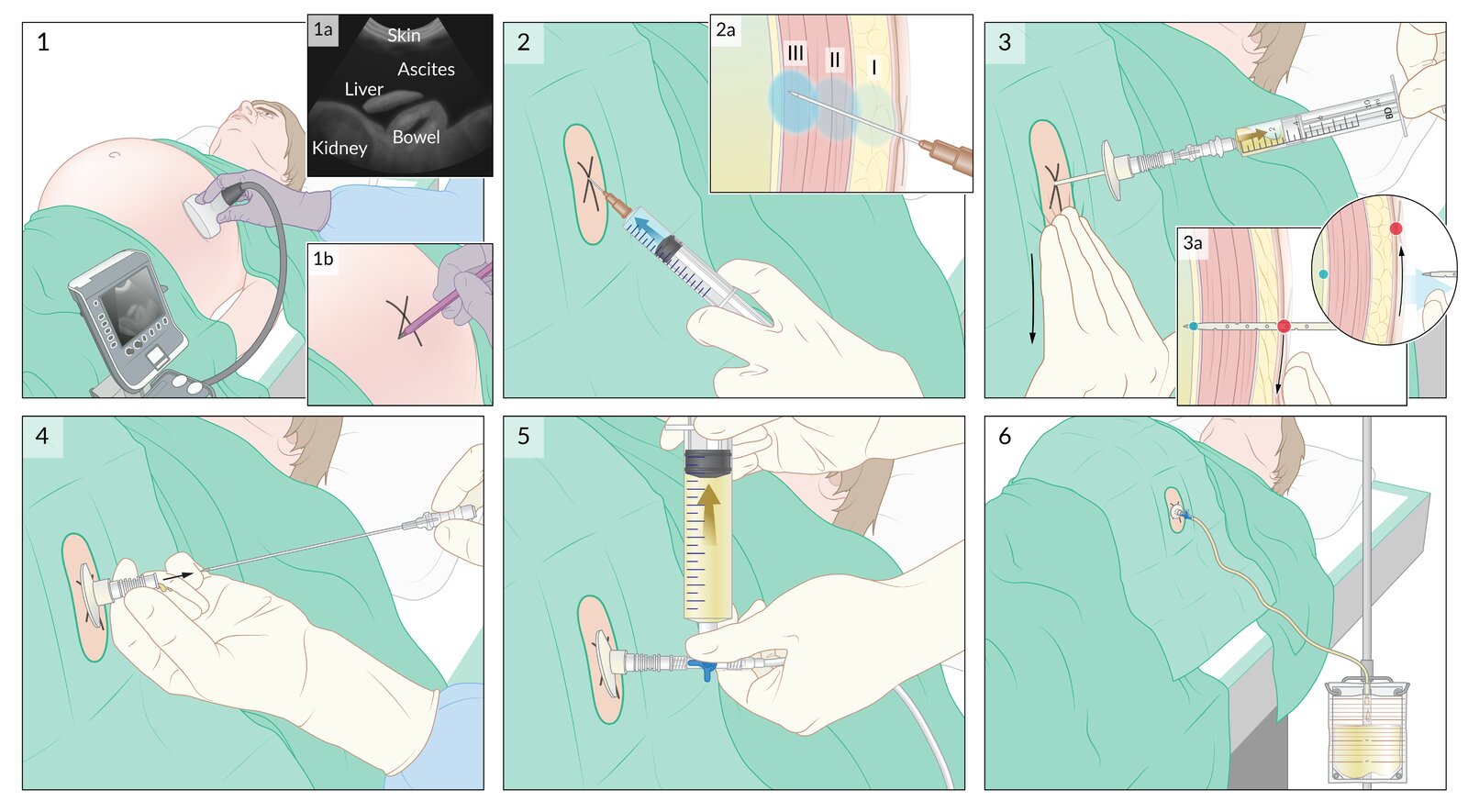
(1) Organs at procedural risk and fluid collections are identified with ultrasound (1a). The optimal needle insertion site is determined and a mark is placed on the skin (1b).
(2) Local anesthetic is injected into the skin and subcutaneous tissue around the insertion site (I), musculature (II), and peritoneum (III).
(3) The skin is pulled downward approx. 2 cm and the paracentesis needle is inserted into the skin and advanced while applying negative pressure to the plunger. The presence of fluid in the syringe indicates that the needle has entered the peritoneal cavity.
(3a) Z-track technique: The skin is pulled down before inserting the paracentesis needle so that the skin insertion site (red dot) no longer aligns with the peritoneal entry site (blue dot) after the needle and catheter are removed, thus preventing leakage of fluid.
(4) The needle and catheter unit are advanced a few millimeters further, the catheter is slid off the needle into the peritoneal cavity, and the needle is removed.
(5) A three-way stopcock is attached to the catheter and 60 mL of fluid is aspirated for diagnostic studies.
(6) If therapeutic paracentesis is planned, the catheter is connected to a drainage system with high-pressure tubing.
© AMBOSS
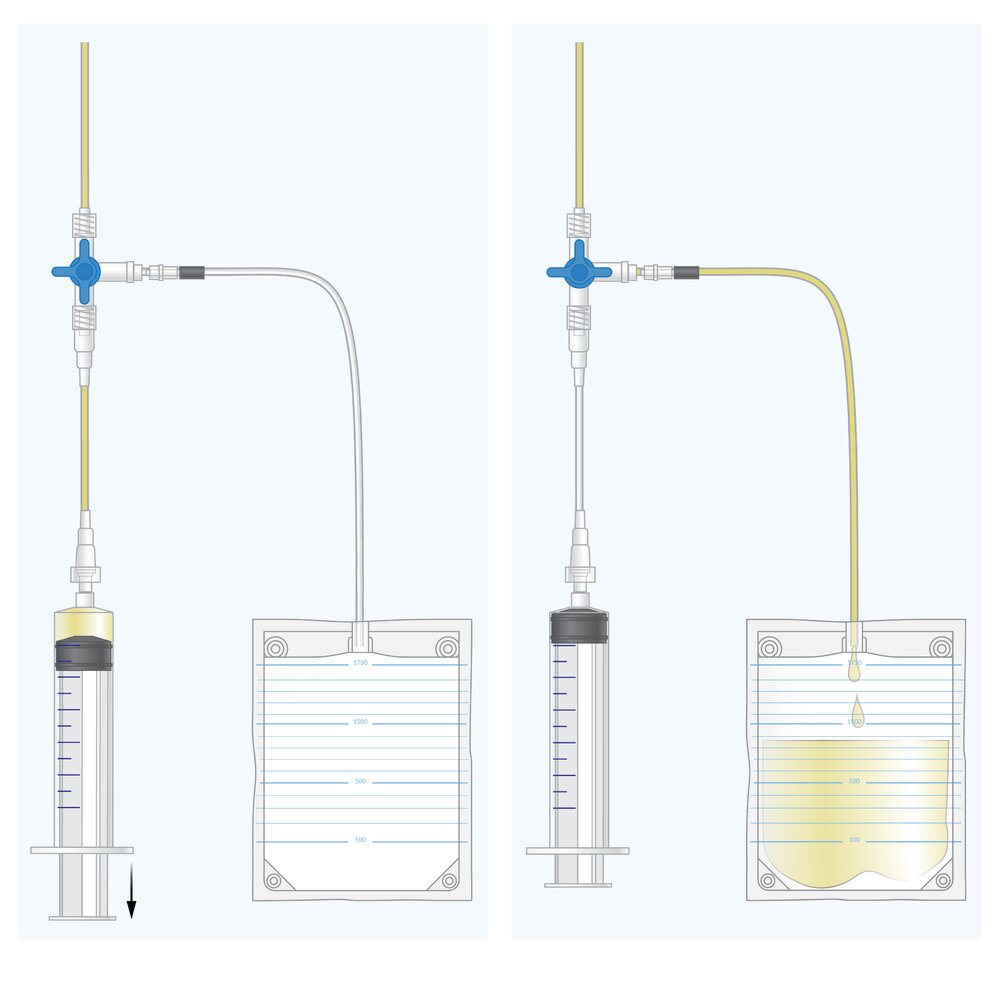
A three-way stopcock (three-way tap) is a device that allows the flow of fluid or air to be adjusted between three different ports (in three possible configurations). It is often used in procedures such as thoracocentesis or paracentesis, in which fluid or air is removed from body cavities.
In this illustration, each of the three small levers on the blue handle of the three-way stopcock indicates the position of a port.
Left: The blue handle is turned to close off the drainage bag. The syringe can be used to aspirate fluid or air from the inlet port.
Right: The blue handle is turned to close off the syringe. Fluid or air from the inlet port can freely enter the drainage bag.
The handle can also be turned to a third position to allow two-way flow between the syringe and drainage bag. The position allowing flow between all three ports simultaneously is not possible on a three-way stopcock (in contrast to a four-way stopcock).
© AMBOSS
© AMBOSS
Dot phrase
Cirrhosis (decompensated, inpatient management)
Assessment: This is a @AGE@-year-old @SEX@ with a history of cirrhosis secondary to [**alcohol, hepatitis C, MASH] presenting with evidence of decompensation. Current issues include [ascites [**new-onset, refractory, associated with abdominal discomfort]; hepatic encephalopathy [**confusion, asterixis, somnolence]; variceal bleeding [**hematemesis, melena]; infection [**SBP, sepsis]]. Precipitating factors include [**infection, gastrointestinal bleeding, alcohol use, medication nonadherence].
Plan
Disposition
–[ICU admission] (if hemodynamically unstable)
–OR [Inpatient admission] (if hemodynamically stable)
Diagnostics [if not already done]
–Initial labs: CBC, CMP, coagulation studies, blood cultures, ammonia level
–Imaging: abdominal ultrasound with Doppler to evaluate for portal vein thrombosis
–Ascitic fluid analysis (if ascites present)
–Cell count, differential, protein, albumin, and culture
–Serum-ascitic albumin gradient to differentiate causes
Monitoring
–BP: goal MAP ≥ 65 mm Hg
–Daily assessment for hepatic encephalopathy
–Daily BMP, urine output
Ascites
–Sodium restriction: < 2 g/day
–Diuretics: spironolactone 100 mg and furosemide 40 mg (adjust in a 10:4 ratio based on response)
–Goal weight loss: 0.5–1 kg/day
–Tense ascites: large-volume paracentesis with albumin infusion (6–8 g per L of fluid removed)
Hepatic encephalopathy
–Lactulose: 30–45 mL PO every 1–2 hours to induce rapid laxation
–Rifaximin 400 mg PO every 8 hours (add if recurrent or persistent encephalopathy)
Variceal bleeding (if present or suspected)
–GI consult for urgent upper endoscopy within 12–24 hours for suspected bleeding
–Octreotide 50 mcg bolus, then 50 mcg/hour continuous infusion
–Prophylactic antibiotics: ceftriaxone 1 g IV once daily for 7 days
Infection [**SBP or other infections]
–Cefotaxime 2 g IV every 8 hours for suspected SBP
–Treat sepsis with IV fluids and broad-spectrum antibiotics as per source.
Chronic liver disease
–Avoid alcohol, NSAIDs, sedatives, and unnecessary medications.
–Carvedilol for variceal bleed prevention
–Immunizations: pneumococcal, hepatitis A and B, influenza, SARS-CoV-2, and tetanus
Referral for liver transplant evaluation
–Indicated for decompensated cirrhosis or MELD score ≥ 15
–Consult hepatology for evaluation of transplant candidacy.
F/E/N
–Protein intake: 1.0–1.5 g/kg/day; avoid restriction unless encephalopathy is refractory.
–Caloric intake: 25–35 kcal/kg/day
–Fluid restriction (if serum sodium < 120 mmol/L)
Pathology
- Fibrosis (fibrous septa)
- Replacement of normal liver tissue with collagenous regenerative nodules (histological staging is based on the size of the regenerative nodules) [43]
- Abnormal cell activation with infiltration of inflammatory cells
- Loss of physiological vessel architecture (central vein disappearance)
| Size of the regenerative nodules | Occurrence | |
|---|---|---|
| Micronodular |
|
|
| Macronodular |
|
|
| Both |
|
|
- See “Alcohol-associated liver disease,” “Hepatitis B,” and “Hepatitis C” for specific pathological findings related to these conditions.



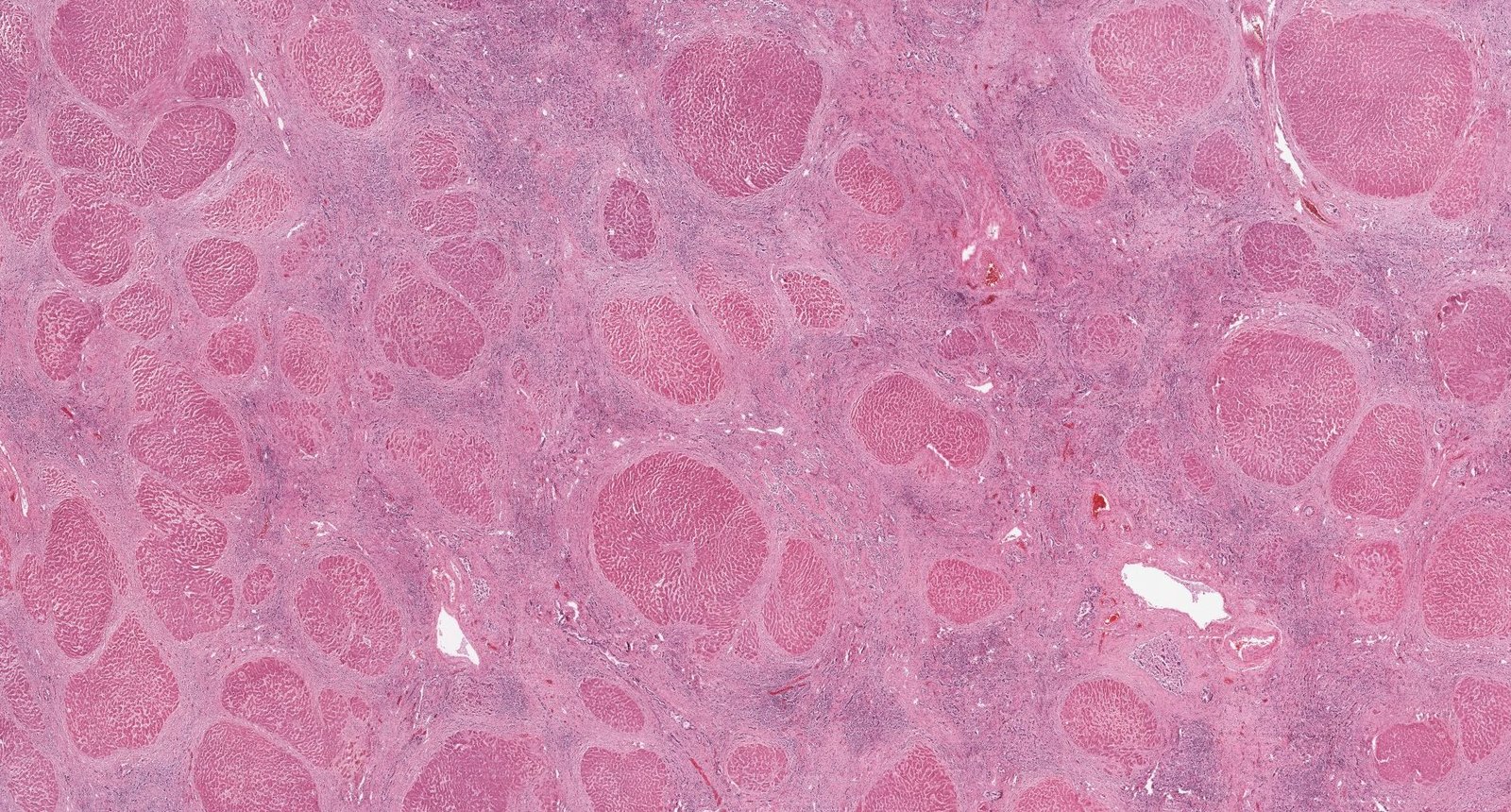
Photomicrograph of a liver biopsy specimen (H&E stain; low magnification)
Nodules of regenerating hepatocytes surrounded by regions of collagenous fibers can be seen. The proliferation of bile ducts is also visible within the connective tissue.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
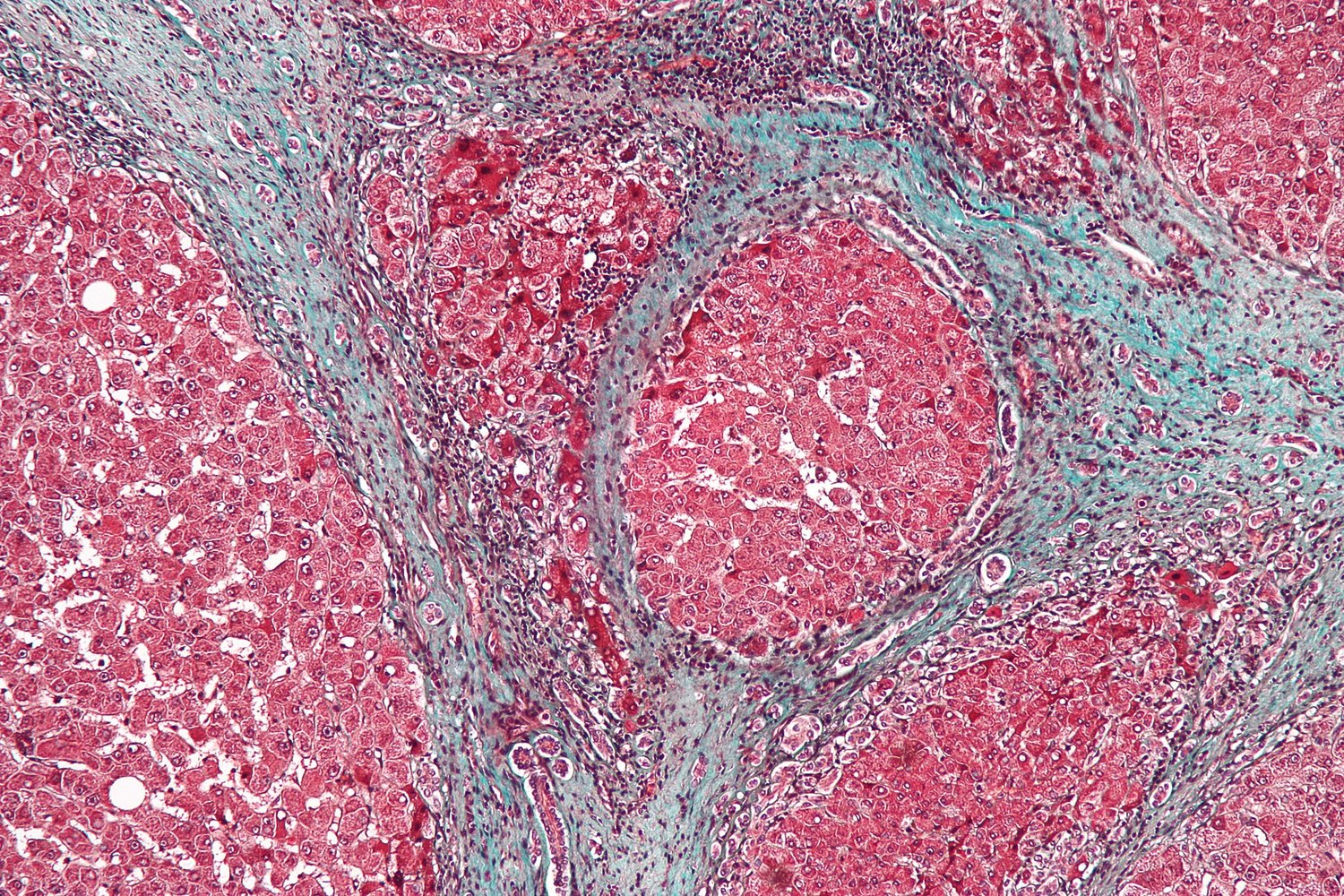
Photomicrograph of a liver biopsy specimen (trichrome stain; high magnification)
A regenerative nodule composed of a cluster of hepatocytes (purple overlay), extensive fibrosis (stained blue), and the portal triad (yellow overlay) can be seen.
Regenerative nodules and fibrous septa are characteristic features of liver cirrhosis.
Source: “Cirrhosis high mag” by Michael Bonert ("Nephron"), Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
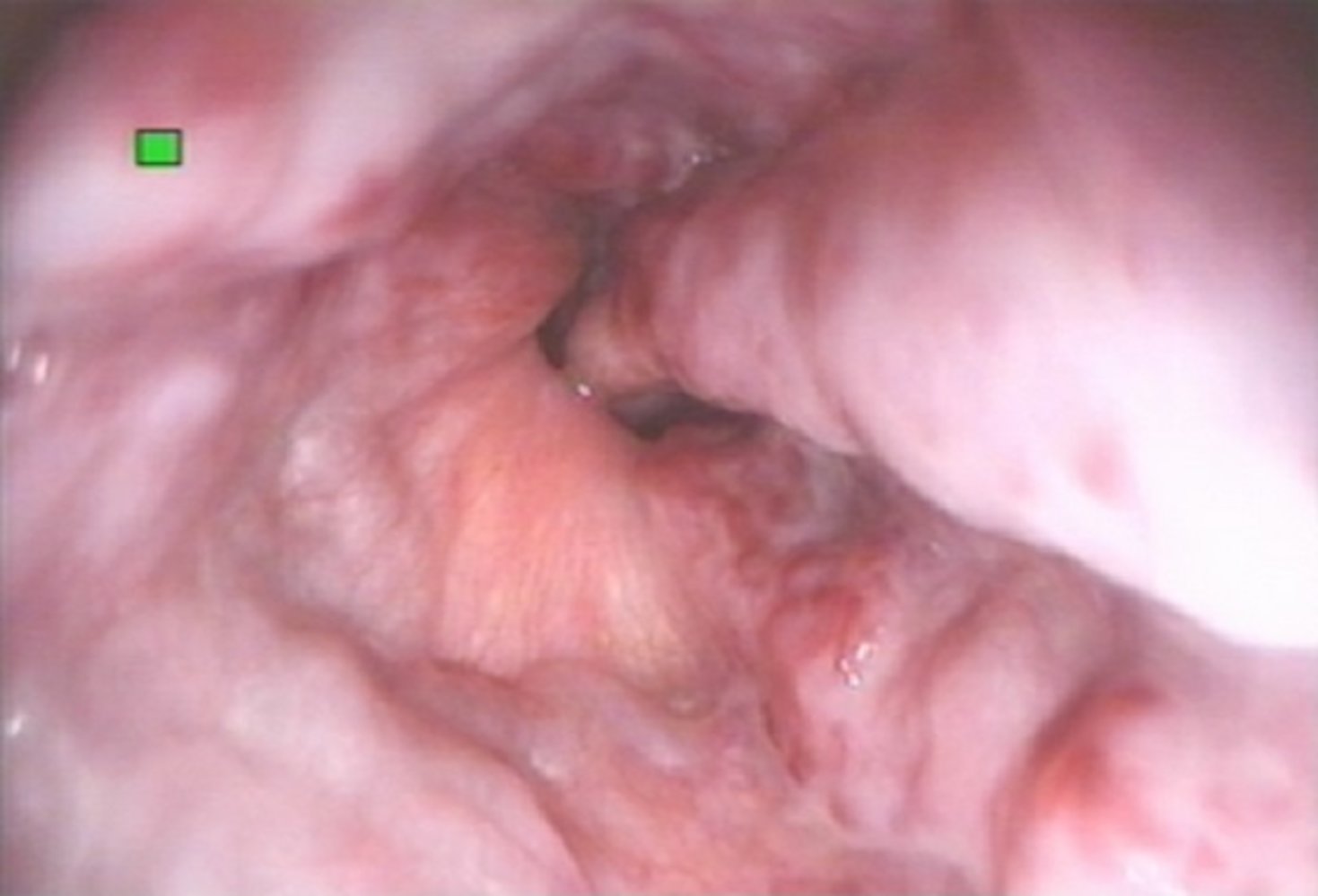
Laparoscopic view of the liver
The liver surface is covered in small nodules (< 3 mm in size).
Source: © IMPP
Complications
Overview [38]
| Overview of common complications of cirrhosis [3][14][44][45] | |
|---|---|
| Portal hypertension complications |
|
| Cardiopulmonary complications |
|
| Hemostatic abnormalities (coagulopathy) |
|
| Metabolic complications |
|
| Malignancy |
|
Cirrhosis-associated ascites and edema and elevated bleeding risk increase the risk for hypovolemic shock.
Vitamin K infusion may improve clotting function in select patients with vitamin K deficiency; it is unlikely to be effective in patients with advanced liver disease and coagulopathy.




We list the most important complications. The selection is not exhaustive.
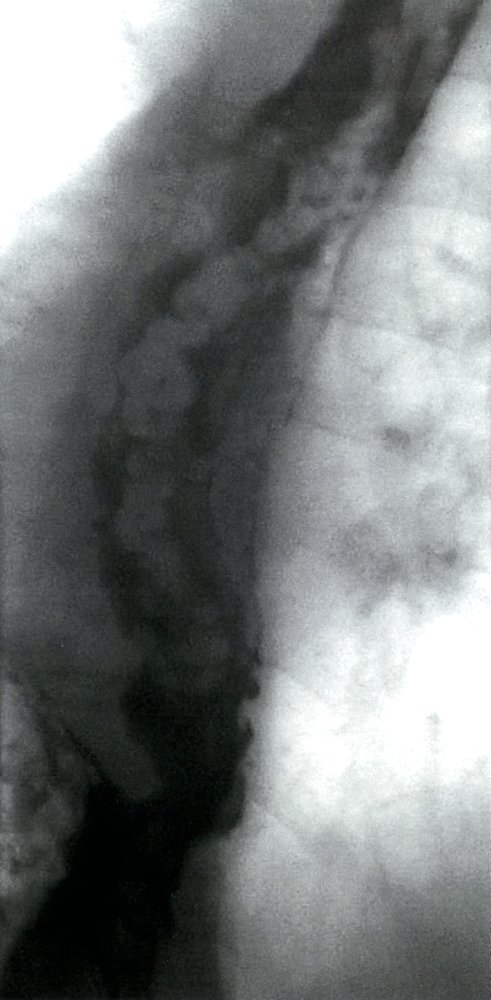
Fluoroscopy (barium swallow; oblique view)
Numerous serpiginous defects project into the contrast-filled (green overlay) esophageal lumen.
This appearance is consistent with esophageal varices.
S: stomach
Source: © IMPP
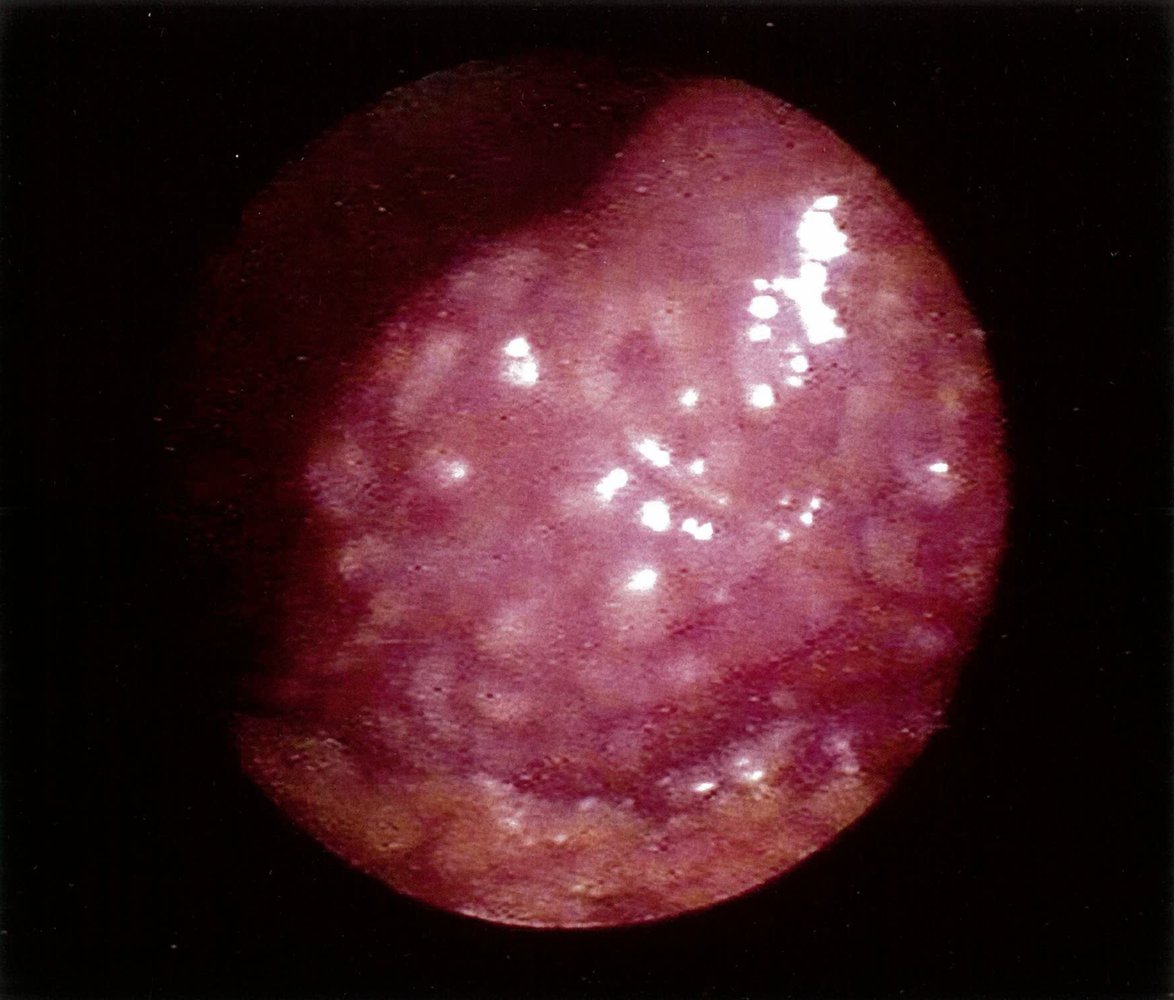
Endoscopic view of the distal esophagus
Dilated, submucosal veins are visible, most prominently at the 2, 4, 7, and 11 o'clock positions. Several cherry-red spots are visible on the varices, suggesting a recent or impending variceal bleed.
Source: “Figure 2 (b) in: Etiology and Management of Hemorrhagic Complications of Portal Hypertension in Children” by Alejandro Costaguta, Fernando Alvarez, International Journal of Hepathology, licensed under CC BY 3.0.

Autopsy sample of liver tissue
Macroscopic signs of cirrhosis are a nodular appearance of the normally homogeneous liver tissue (examples outlined by white overlay) with prominent septation (examples outlined by red overlay). Dispersed are greenish nodules, consistent with multifocal hepatocellular carcinoma (example of tumor nodule indicated by arrow, other examples outlined by black overlay).
The green hue seen here is due to tumor-associated bile retention.
Source: “Figure 4, in: Acute Right Ventricular Failure in a Patient with Hepatic Cirrhosis” by Jose Soto Soto, Xochiquetzal Geiger, Margaret M. Johnson, Case Reports in Pulmonology, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
CT abdomen (with IV and oral contrast; axial plane) of a patient with multifocal hepatocellular carcinoma
Contrast-enhanced masses (examples indicated by arrowheads) are visible within the liver, which is small in size and has a nodular contour and heterogeneous enhancement. The spleen is enlarged. Ascites (green overlay) can be seen in the left upper quadrant.
Hepatocellular carcinoma is the main diagnostic consideration if either a single mass or multiple masses are seen in a liver with imaging features of cirrhosis.
A: aorta; L: liver; Sp: spleen; St: stomach
Source: © IMPP
Decompensated cirrhosis
- Definition: the development of overt ascites, overt hepatic encephalopathy, or variceal bleeding in patients with cirrhosis [2]
- Onset: can be triggered by an acute event (e.g., bleeding, sepsis) or develop gradually (e.g., ascites, encephalopathy) [46][47]
-
Common precipitating factors[47]
- Infection (e.g., spontaneous bacterial peritonitis) or sepsis
- Alcohol consumption
- Medications (e.g., NSAIDs)
- GI bleeding
- Dehydration
- Constipation
- Acute PVT
- HCC
-
Diagnostics: to establish the cause of decompensation
- CBC, BMP, liver chemistries
- Magnesium and phosphate levels
- Coagulation panel
- Consider type and screen.
- Paracentesis in patients with ascites
- CRP, blood cultures, urinalysis and culture, chest x-ray
- Abdominal ultrasound to assess for PVT
-
Acute management: See “Management of acute liver failure.” [3][41][47]
- Gastroenterology consult
- Treat the underlying cause and complications (if applicable).
- Prognosis: In patients with decompensated cirrhosis, survival rates are usually poor unless liver transplantation is performed.
Special patient groups
Liver cirrhosis in pregnancy [48][49]
-
Maternal complications
-
Worsening of liver cirrhosis; pregnancy in individuals with advanced disease is associated with increased risk of:
- New-onset ascites or worsening of ascites
- Liver failure
- Hepatorenal syndrome
- Variceal bleeding (during pregnancy and/or labor)
-
Increased risk of pregnancy-related complications, including:
- Gestational diabetes
- Placental abruption
- Preeclampsia
- Postpartum hemorrhage
- Spontaneous abortion, need of cesarean delivery, preterm delivery
-
Worsening of liver cirrhosis; pregnancy in individuals with advanced disease is associated with increased risk of:
- Fetal complications: associated with increased rates of newborn asphyxia and small size for gestational age
Related One-Minute Telegram
- One-Minute Telegram 131-2025-2/3: Prophylactic antibiotics for GI bleeds: less may be more
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
References
- Scaglione S, Kliethermes S, Cao G, et al. "The Epidemiology of Cirrhosis in the United States: A Population-based Study.". Journal of Clinical Gastroenterology. 49(8). :690-696. (2015)
- Yoon, Chen. "LIVER CIRRHOSIS MORTALITY IN THE UNITED STATES:NATIONAL, STATE, AND REGIONAL TRENDS, 2000–2015". U.S. Department of Health and Human Services Public Health Service National Institutes of Health. (2018)
- Devarbhavi H, Asrani SK, Arab JP, et al. "Global burden of liver disease: 2023 update". J Hepatol. 79(2). :516-537. (2023)
- Goljan EF. "Rapid Review Pathology". Elsevier Saunders. (2018). ISBN: 9780323476683
- Nevzati E, Shafighi M, Bakhtian KD, et al. "Estrogen Induces Nitric Oxide Production Via Nitric Oxide Synthase Activation in Endothelial Cells". Springer International Publishing. :141-145. (2014). ISBN: 9783319049809
- Cavanaugh J, Niewoehner CB, Nuttall FQ. "Gynecomastia and cirrhosis of the liver". Arch Intern Med. 150(3). :563-565. (1990)
- Alser O, Kuo R, Furniss D. "Nongenetic Factors Associated with Dupuytren’s Disease: A Systematic Review". Plastic & Reconstructive Surgery. 146(4). :799-807. (2020)
- Broekstra D, Groen H, Molenkamp S, Werker P, van den Heuvel E. "A Systematic Review and Meta-Analysis on the Strength and Consistency of the Associations between Dupuytren Disease and Diabetes Mellitus, Liver Disease, and Epilepsy". Plastic & Reconstructive Surgery. 141(3). :367e-379e. (2018)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Meseeha M, Attia M. "Alpha 1 Antitrypsin Deficiency". StatPearls. (2020)
- Smith A, Baumgartner K, Bositis C. "Cirrhosis: Diagnosis and Management". Am Fam Physician. 100(12). :759-770. (2019)
- Wiegand J, Berg T. "The Etiology, Diagnosis and Prevention of Liver Cirrhosis". Dtsch Arztebl Int. (2013)
- Qamar AA, Grace ND. "Abnormal hematological indices in cirrhosis". Can J Gastroenterol. 23(6). :441-445. (2009)
- Kwo PY, Cohen SM, Lim JK. "ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries". Am J Gastroenterol. 112(1). :18-35. (2017)
- Newsome PN, Cramb R, Davison SM, et al. "Guidelines on the management of abnormal liver blood tests". Gut. 67(1). :6-19. (2017)
- Crabb DW, Im GY, Szabo G, Mellinger JL, Lucey MR. "Diagnosis and Treatment of Alcohol‐Associated Liver Diseases: 2019 Practice Guidance From the American Association for the Study of Liver Diseases". Hepatology. 71(1). :306-333. (2020)
- Vavricka SR, Burri E, Beglinger C, Degen L, Manz M. "Serum Protein Electrophoresis: An Underused but Very Useful Test". Digestion. 79(4). :203-210. (2009)
- Ge PS, Runyon BA. "Serum Ammonia Level for the Evaluation of Hepatic Encephalopathy". JAMA. 312(6). :643. (2014)
- Procopet B, Berzigotti A. "Diagnosis of cirrhosis and portal hypertension: imaging, non-invasive markers of fibrosis and liver biopsy". Gastroenterol Rep (Oxf). 5(2). :79-89. (2017)
- Sangster GP, Previgliano CH, Nader M, Chwoschtschinsky E, Heldmann MG. "MDCT Imaging Findings of Liver Cirrhosis: Spectrum of Hepatic and Extrahepatic Abdominal Complications". HPB Surg. 2013. :1-12. (2013)
- Sagoo MG, Aland RC, Gosden E. "Morphology and morphometry of the caudate lobe of the liver in two populations.". Anat Sci Int. 93(1). :48-57. (2018)
- Shi Q, Xiong K, Ding B, Ye X. "Clinical characteristics of cirrhosis patients with umbilical vein recanalization: A retrospective analysis". Medicine. 100(35). :e26774. (2021)
- Horowitz JM, Kamel IR, et al. "ACR Appropriateness Criteria ® Chronic Liver Disease". J Am Coll Radiol. 14(11). :S391-S405. (2017)
- Lin Z-H, Xin Y-N, Dong Q-J, et al. "Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis". Hepatology. 53(3). :726-736. (2011)
- Ferraioli G, Filice C, Castera L, et al. "WFUMB Guidelines and Recommendations for Clinical Use of Ultrasound Elastography: Part 3: Liver". Ultrasound Med Biol. 41(5). :1161-1179. (2015)
- Ferraioli G. "Review of Liver Elastography Guidelines". J Ultrasound Med. 38(1). :9-14. (2018)
- Sterling RK, Duarte-Rojo A, Patel K, et al. "AASLD Practice Guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis". Hepatology. (2024)
- Frulio N, Trillaud H, et al. "Acoustic Radiation Force Impulse (ARFI) and Transient Elastography (TE) for evaluation of liver fibrosis in HIV-HCV co-infected patients". BMC Infect Dis. 14(1). (2014)
- Sack I. "Magnetic resonance elastography from fundamental soft-tissue mechanics to diagnostic imaging". Nat Rev Physics. 5(1). :25-42. (2022)
- Kasper DL, Fauci AS, Hauser SL, et al. "Harrison's Principles of Internal Medicine". McGraw-Hill Education. (2015). ISBN: 9780071802161
- Angeli P, Bernardi M, Villanueva C, et al. "EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis". J Hepatol. 69(2). :406-460. (2018)
- Ge PS, Runyon BA. "Treatment of Patients with Cirrhosis". N Engl J Med. 375(8). :767-777. (2016)
- Singal AK, Wong RJ, Dasarathy S, et al. "ACG Clinical Guideline: Malnutrition and Nutritional Recommendations in Liver Disease". Am J Gastroenterol. 120(5). :950-972. (2025)
- Biggins SW, Angeli P, Garcia-Tsao G, et al. "Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases". Hepatology. 74(2). :1014-1048. (2021)
- Karvellas CJ, Bajaj JS, Kamath PS, et al. "AASLD Practice Guidance on Acute-on-chronic liver failure and the management of critically ill patients with cirrhosis". Hepatology. (2023)
- Kaplan DE, Bosch J, Ripoll C, et al. "AASLD practice guidance on risk stratification and management of portal hypertension and varices in cirrhosis". Hepatology. (2023)
- de Franchis R, Bosch J, Garcia-Tsao G, et al. "Baveno VII – Renewing consensus in portal hypertension". J Hepatol. 76(4). :959-974. (2022)
- Garcia‐Tsao G, Abraldes JG, Berzigotti A, et al. "Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases". Hepatology. 65(1). :310-335. (2016)
- "Evaluation for liver transplantation in adults: 2013 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation". https://aasldpubs.onlinelibrary.wiley.com/doi/10.1002/hep.26972. [2014-03-01]
- Tolman KG, Fonseca V, Dalpiaz A, Tan MH. "Spectrum of Liver Disease in Type 2 Diabetes and Management of Patients With Diabetes and Liver Disease". Diabetes Care. 30(3). :734-743. (2007)
- Fisher L, Fisher A. "Vitamin D and Parathyroid Hormone in Outpatients With Noncholestatic Chronic Liver Disease". Clin Gastroenterol Hepatol. 5(4). :513-520. (2007)
- Kisseleva T, Brenner D. "Molecular and cellular mechanisms of liver fibrosis and its regression". Nat Rev Gastroenterol Hepatol. 18(3). :151-166. (2020)
- Goldberg DS, Olthoff KM. "Standardizing MELD Exceptions: Current Challenges and Future Directions". Curr Transplant Rep. 1(4). :232-237. (2014)
- Schuppan D, Afdhal NH. "Liver cirrhosis". Lancet. 371(9615). :838-851. (2008)
- Tsoris A, Marlar CA. "Use Of The Child Pugh Score In Liver Disease". StatPearls. (2020)
- D’Amico G, Bernardi M, Angeli P. "Towards a new definition of decompensated cirrhosis". J Hepatol. 76(1). :202-207. (2022)
- McPherson S, Dyson J, Austin A, Hudson M. "Response to the NCEPOD report: development of a care bundle for patients admitted with decompensated cirrhosis—the first 24 h". Frontline Gastroenterol. 7(1). :16-23. (2014)
- Gao X, Zhu Y, Liu H, Yu H, Wang M. "Maternal and fetal outcomes of patients with liver cirrhosis: a case-control study". BMC Pregnancy Childbirth. 21(1). (2021)
- Tiribelli C, Rigato I. "Liver cirrhosis and pregnancy". Annals of Hepatology. 5(3). :201. (2006)
- "Underlying cause of death 1999-2018 on CDC WONDER online database."
- Nusrat S. "Cirrhosis and its complications: Evidence based treatment". World Journal of Gastroenterology. 20(18). :5442. (2014)
- Mansour D, McPherson S. "Management of decompensated cirrhosis.". Clin Med. 18(Suppl 2). :s60-s65. (2018)
- Ng CK, Chan MH, Tai MH, Lam CW. "Hepatorenal syndrome". Clin Biochem Rev. 28(1). :11-7. (2007)
- Francoz C, Durand F, Kahn JA, Genyk YS, Nadim MK. "Hepatorenal Syndrome". Clinical Journal of the American Society of Nephrology. 14(5). :774-781. (2019)
- Ponziani FR. "Portal vein thrombosis: Insight into physiopathology, diagnosis, and treatment". World Journal of Gastroenterology. 16(2). :143. (2010)
- Wu M, Schuster M, Tadros M. "Update on Management of Portal Vein Thrombosis and the Role of Novel Anticoagulants". Journal of Clinical and Translational Hepatology. 7(X). :1-11. (2019)
- Primignani M. "Portal vein thrombosis, revisited". Digestive and Liver Disease. 42(3). :163-170. (2010)
- Grilo Bensusan I, Pascasio JM, Tirado JL, et al. "The utility of the macro-aggregated albumin lung perfusion scan in the diagnosis and prognosis of hepatopulmonary syndrome in cirrhotic patients candidates for liver transplantation". Revista Española de Enfermedades Digestivas. (2017)
- Porres-Aguilar M, Altamirano JT, Torre-Delgadillo A, Charlton MR, Duarte-Rojo A. "Portopulmonary hypertension and hepatopulmonary syndrome: a clinician-oriented overview". European Respiratory Review. 21(125). :223-233. (2012)