Summary
Clavicle fractures are common, especially in children and adolescents, and often result from a direct fall onto the shoulder. They are classified by location using the Allman classification system, with two-thirds of fractures located in the midshaft. Patients typically present with signs of fracture such as swelling, focal tenderness, and reduced arm mobility, or more specific signs such as shoulder drooping or skin tenting around the clavicle. Diagnosis is confirmed with x-ray, although additional imaging studies such as CTA may be needed for suspected vascular injury. Treatment is based on fracture location and may include conservative fracture management and/or surgical fracture care.
Epidemiology
- Common (accounts for ∼ 2.6% of all fractures) [1]
- Most commonly occurs in children and adolescents [2]
- Most common birth trauma in newborns [3]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Direct trauma (∼ 95% of cases) [4]
- Fall onto the shoulder (most common cause), e.g., from bicycle accident
- Direct blow to the clavicle, e.g., from a football tackle
- Indirect trauma (∼ 5% of cases): mainly falls onto an outstretched hand [4]
- Birth trauma (see “Birth-related clavicle fracture”)
Pathophysiology
A midshaft fracture is the most common clavicle fracture because it is the thinnest segment of bone and lacks ligamentous and muscular support. [5]
Classification
Allman classification system [6]
The Allman classification system categorizes fractures of the clavicle according to fracture location.
| Group | Location of fracture |
|---|---|
| I | Midshaft fracture/middle third (∼ 69% of cases) |
| II | Lateral/distal third (∼ 28% of cases) |
| III | Medial/proximal third (∼ 3% of cases) |

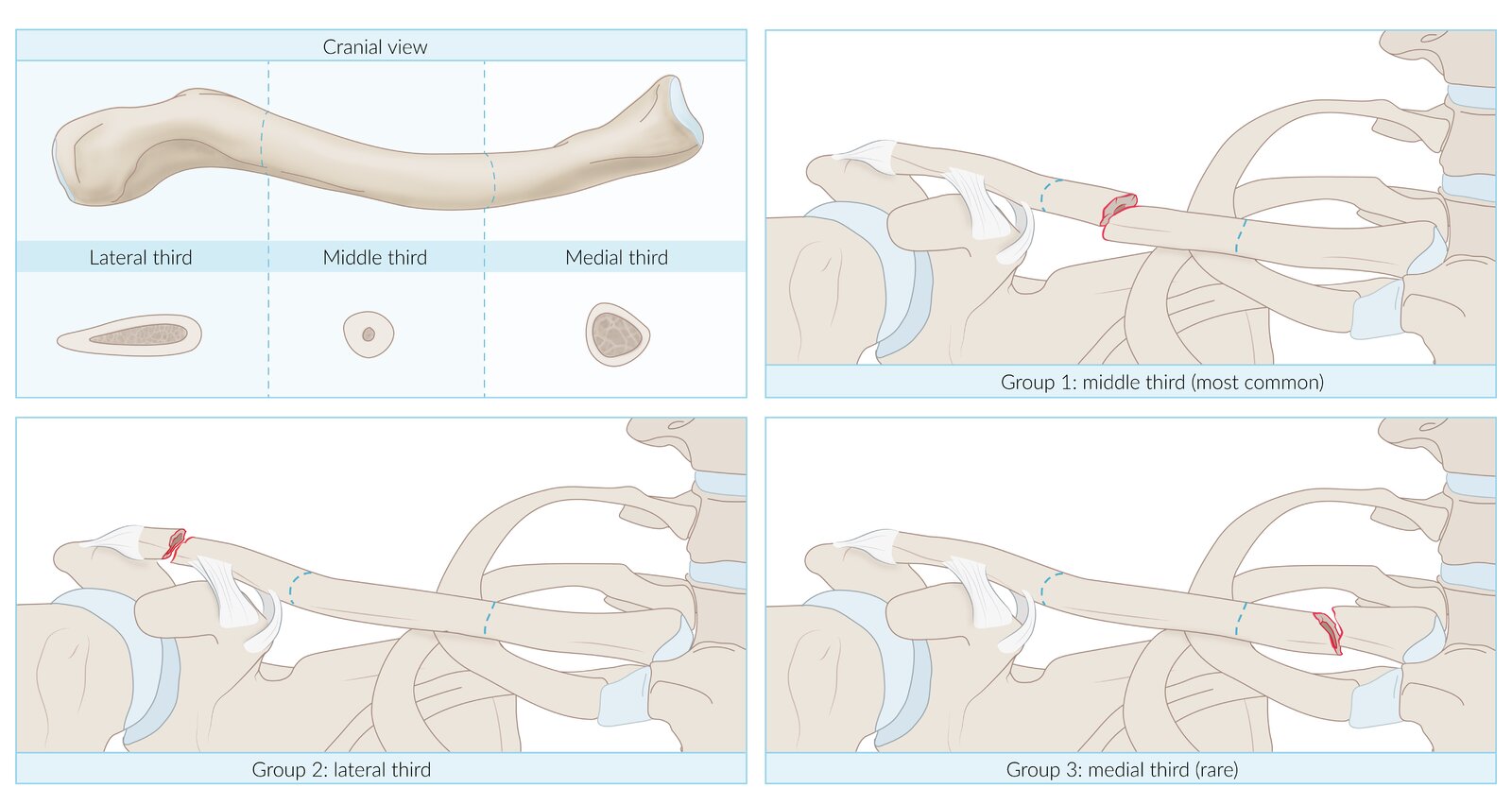
The Allman classification divides the clavicle into three equal segments, according to which fractures are classified.
© AMBOSS
Clinical features
- Signs of fracture, e.g., pain, ecchymosis, swelling
- Sagging of the shoulder due to downward distracting force of the weight of the upper limb on the lateral fracture fragment
- Skin tenting over the clavicle due to the upward distracting force of the sternocleidomastoid on the medial fracture fragment
- Shortening of the clavicle due to the medial distracting force (adduction) of the pectoralis major on the lateral fracture fragment



Left shoulder of a patient with a displaced clavicle fracture
A bony, nodular prominence (orange arrow) is visible in the area of the supraspinatus muscle. The skin and soft tissue above the prominence are under pressure and resemble a tent. The surrounding skin shows a hematoma that extends to the upper arm.
The described findings are characteristic of skin tenting and typically occur in cases of displaced clavicle fractures.
Source: “Fig 1, In: A variant of a type V lateral clavicle fracture involving a posteriorly displaced medial segment. A case report” by Goss TP, Li X, BMC Sports Science, Medicine and Rehabilitation, licensed under CC BY 2.0.
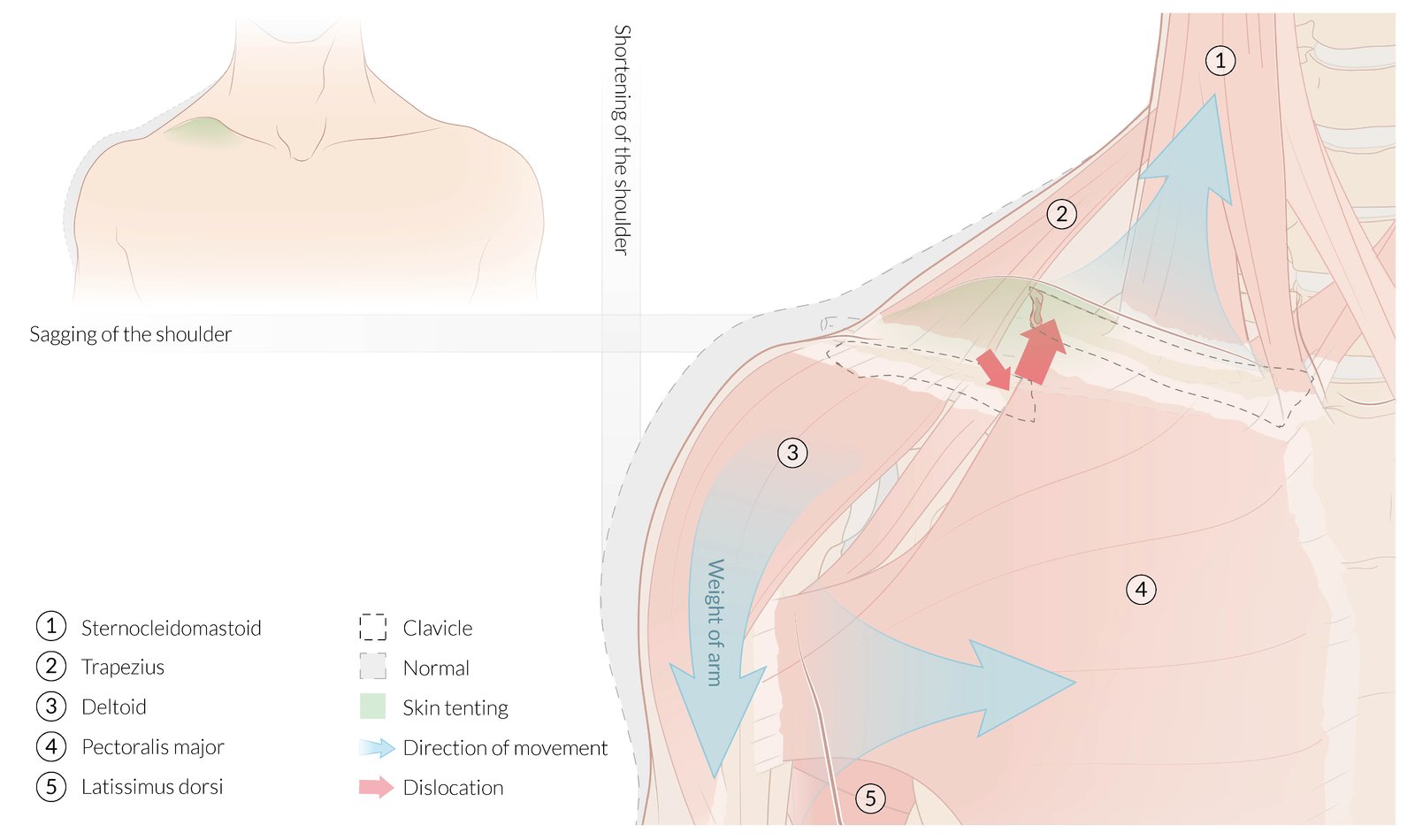
The junction of the medial second third and the lateral first third is the most common site of clavicle fractures, as depicted here. Distracting forces cause a downward dislocation of the lateral fracture fragment and an upward dislocation of the medial fracture fragment, resulting in the following clinical features:
- Sagging of the ipsilateral shoulder due to downward distracting force of the weight of the upper limb on the lateral fracture fragment
- Shortening of the ipsilateral shoulder due to the medial distracting force of the pectoralis major on the lateral fracture fragment
- Tenting of the skin over the fracture site due to the upward distracting force of the sternocleidomastoid on the medial fracture fragment
© AMBOSS
Diagnosis
Clinical evaluation [5][7]
Any findings that suggest neurovascular injury or an open fracture should prompt urgent orthopedic consultation.
-
Neurovascular examination
- Evaluate for brachial plexus injury, e.g., upper extremity paresthesias or weakness. [8][9]
- Assess for subclavian artery injury, e.g., weak or absent upper extremity pulses. [9][10]
- Skin examination: Evaluate for laceration, tearing, and skin tenting.
- Lung examination: Assess for signs of pneumothorax.
Posteriorly displaced fracture fragments may result in injuries to the brachial plexus, subclavian vessels, and lung apex. [5]
Imaging [5][7]
X-ray
- Indication: best initial test for suspected clavicle fracture
- Views: anterior-posterior and 45° cephalic tilt
- Findings: radiographic fracture signs, fracture fragments, displacement, angulation, and/or shortening





Additional imaging [5][7]
- CT upper extremity or chest: for assessing associated injuries, intraarticular fractures, preoperative planning for complicated fractures, and inconclusive x-ray findings
- CT angiography upper extremity or chest: for suspected vascular injury [10]
- MRI upper extremity: to assess intraarticular or ligamentous injury and soft tissue structures in high-grade acromioclavicular separations to guide management decisions [11]
- Ultrasound: may be used for suspected pediatric clavicle fractures [12]
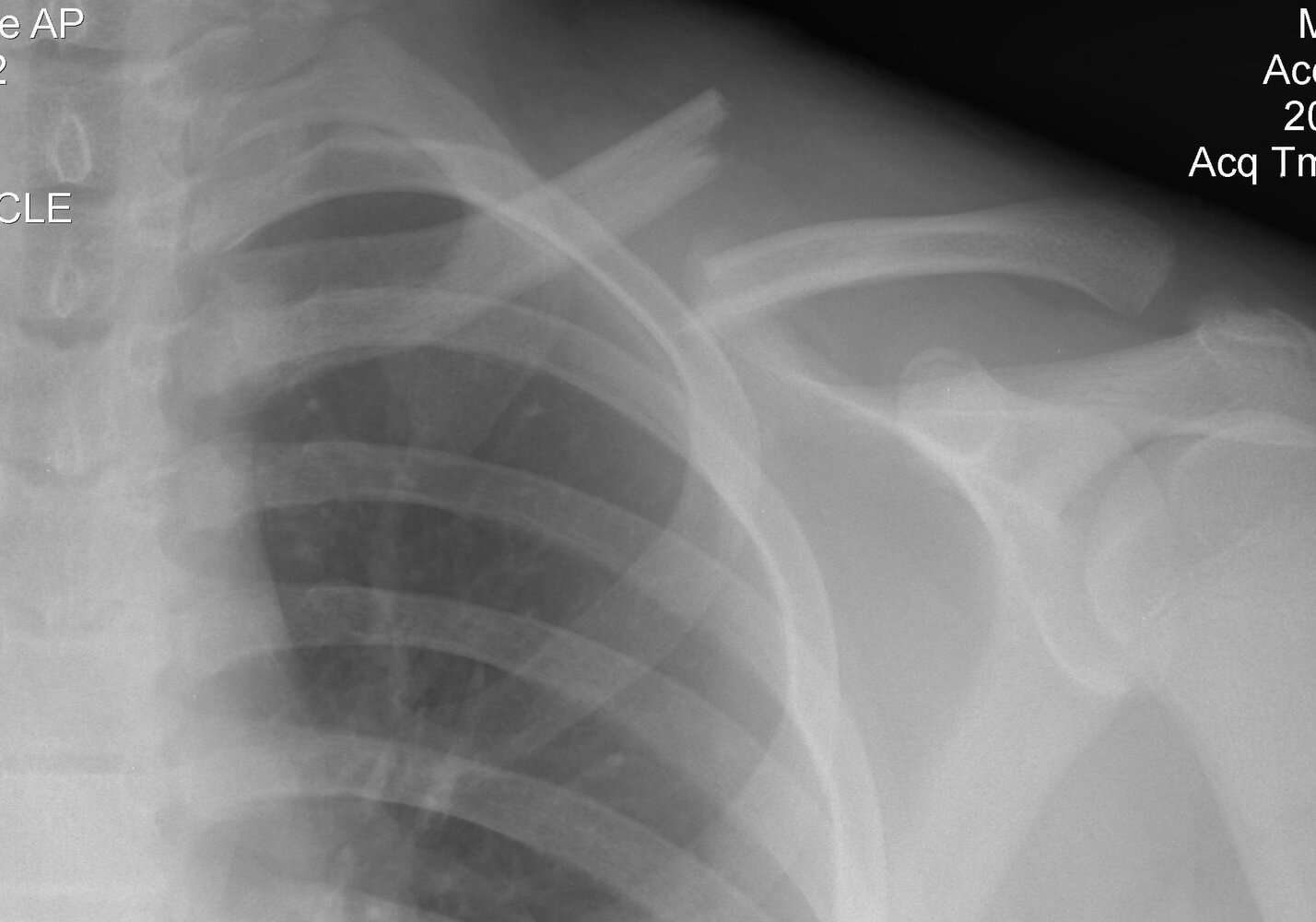
X-ray left shoulder (AP view)
There is a complete fracture of the middle third of the left clavicle (green overlay). The medial fragment is displaced cranially and the lateral fragment is displaced caudally, with some overlap between the two fragments.
This is the typical radiological appearance of a clavicular fracture, which most commonly occurs at the junction of the middle third and lateral third of the clavicular shaft.
Source: “X-ray of a left clavicle fracture” by Majorkev, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

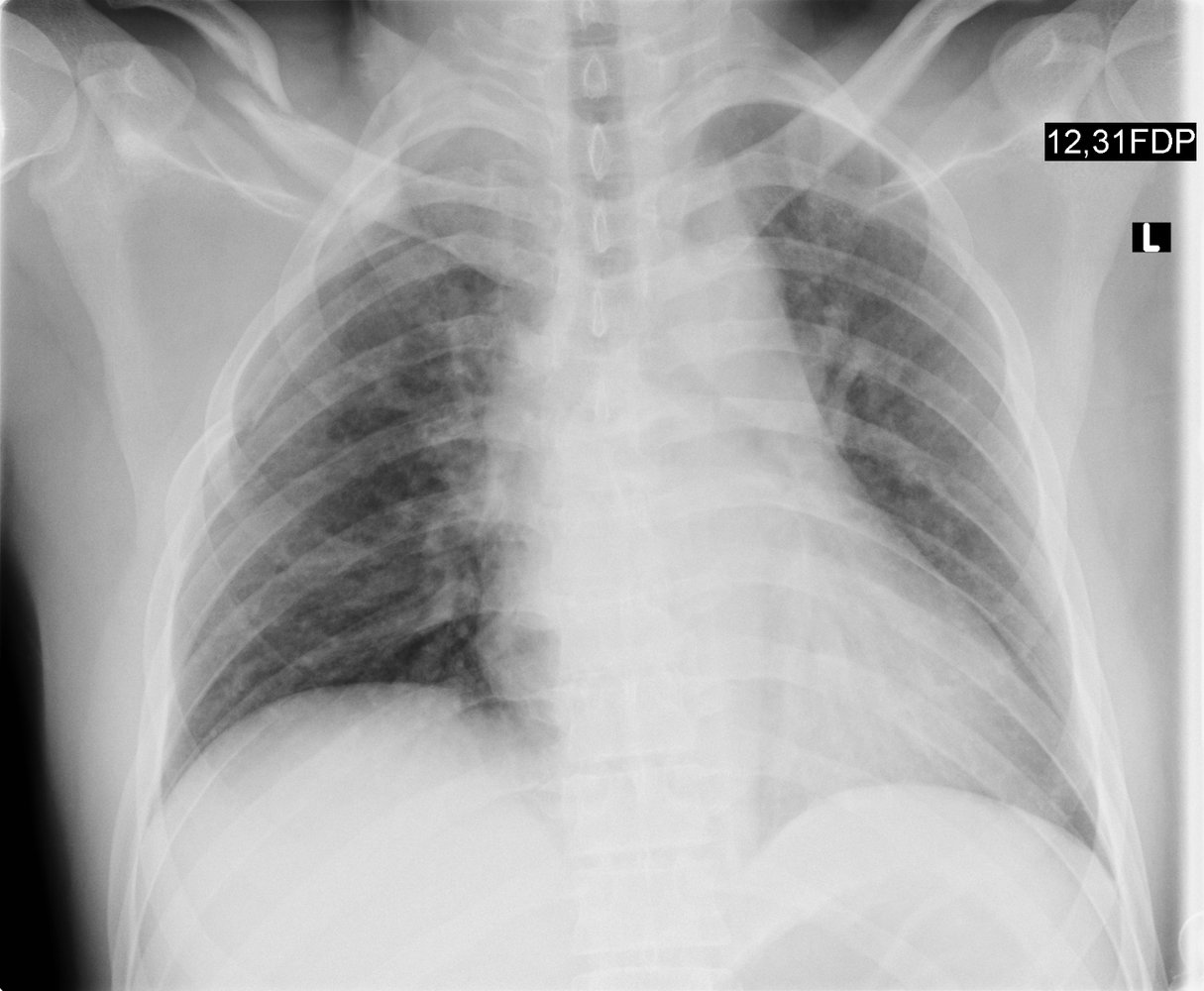
AP radiograph of the shoulder joint: lateral clavicle fracture.
Source: © IMPP
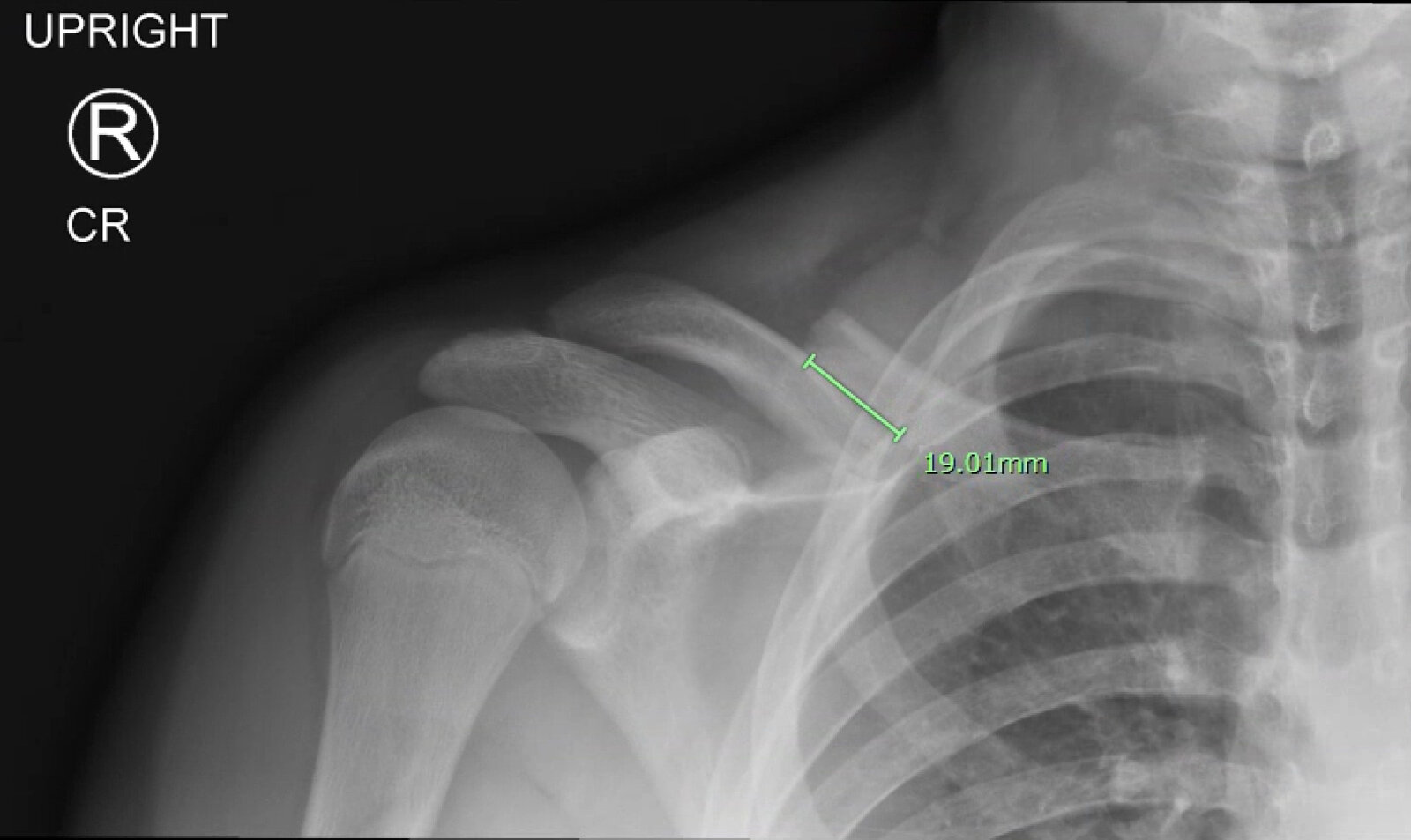
X-ray right clavicle (AP view)
A mid-shaft fracture is visible, with full shaft-width inferior displacement of the distal fragment and overriding of the fragments by 19 mm. No callus formation is visible.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
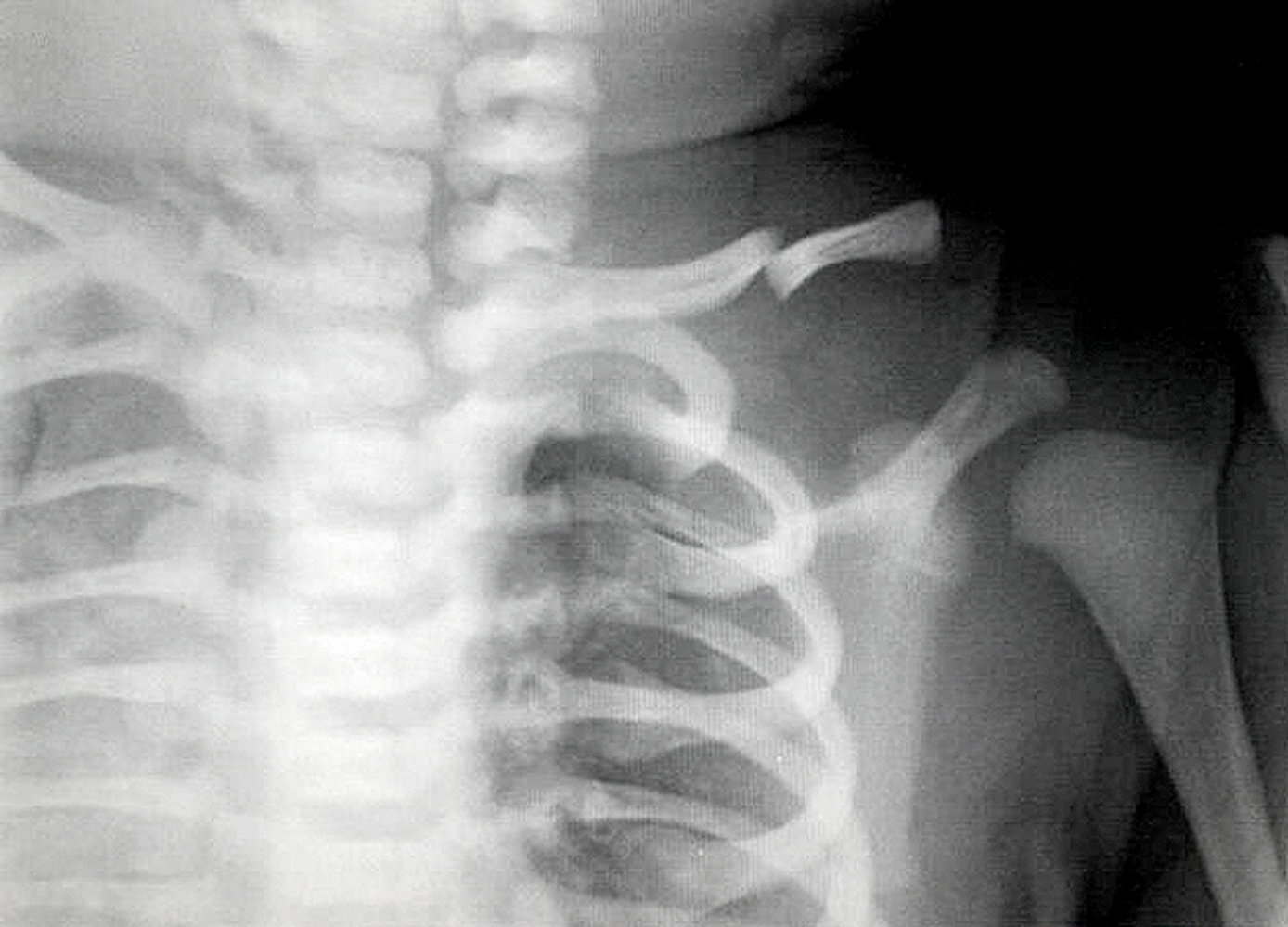
X-ray upper chest (AP view) of a newborn
A complete fracture of the mid-third of the left clavicle shows overriding of the fragments (green overlay).
Fractures of the clavicle are the most common birth trauma and may be complete or incomplete. Major causes include extended arms in breech presentation deliveries and shoulder dystocia in vertex presentation deliveries.
1: left first rib; white outlines: clavicle
Source: “Neonatal clavicle fracture” by ADMIN, http://www.anatomybox.com, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
X-ray chest (PA view) of a patient with polytrauma from a motor vehicle collision
A displaced fracture (green overlay) of the mid-shaft of the right clavicle is accompanied by fractures of the third and fourth ribs (red overlay). Subtle buckling of the cortex of the first rib also suggests a fracture (arrowheads). A first rib fracture is a marker of severity in polytrauma, frequently associated with severe organ injury.
Our great thanks to PD Dr. M. Jergas (Center for Diagnostic and Interventional Radiology, St. Elizabeth Hospital, Cologne) for kindly providing this image.
Differential diagnoses
- Acromioclavicular joint injury
- Sternoclavicular joint injury
- Rib fracture
- Scapular fracture
- Shoulder dislocation
- Rotator cuff injury
The differential diagnoses listed here are not exhaustive.
Treatment
General principles [13][14][15]
- Most clavicle fractures are managed conservatively, regardless of their Allman classification. [13]
-
Surgical fracture management is increasing, e.g., in patients with:
- Young age
- Few comorbidities
- High-energy injury mechanisms
- Midshaft (group I) fractures [13]
- Medial (group III) fractures [13]
- Concerns about professional impact (e.g., in athletes) or cosmesis
Initial management [7]
- Provide general fracture care, including analgesia for fractures.
- Immobilize with an arm sling for comfort as soon as a clavicle fracture is suspected.
- Identify indications to consult orthopedics for fractures.
- Consult surgery if there is suspicion of an intrathoracic injury (e.g., pneumothorax, subclavian artery injury)
- Arrange prompt follow-up with orthopedics for all patients.
Rule out concomitant intrathoracic injuries in patients with medial (group III) clavicle fractures.
Conservative management [7][15]
Recommended for nondisplaced, closed fractures
- Immobilize in an arm sling for 4–8 weeks.
- Perform early passive range of motion exercises.
- Avoid noncontact sports for 6 weeks and contact sports for 2–4 months. [5]
- See also “Conservative fracture management.”
Surgical fracture management [13][14][15]
Indications
-
High risk for malunion or nonunion
- Significant displacement
- Shortening > 2 cm
- Severely comminuted
- Open fractures
- Neurovascular injury
- Skin tenting
Operative techniques
Depend on fracture location and type and include:
- Intramedullary nailing
- Plate fixation
- Ligament repair: typically for lateral (group II) fractures


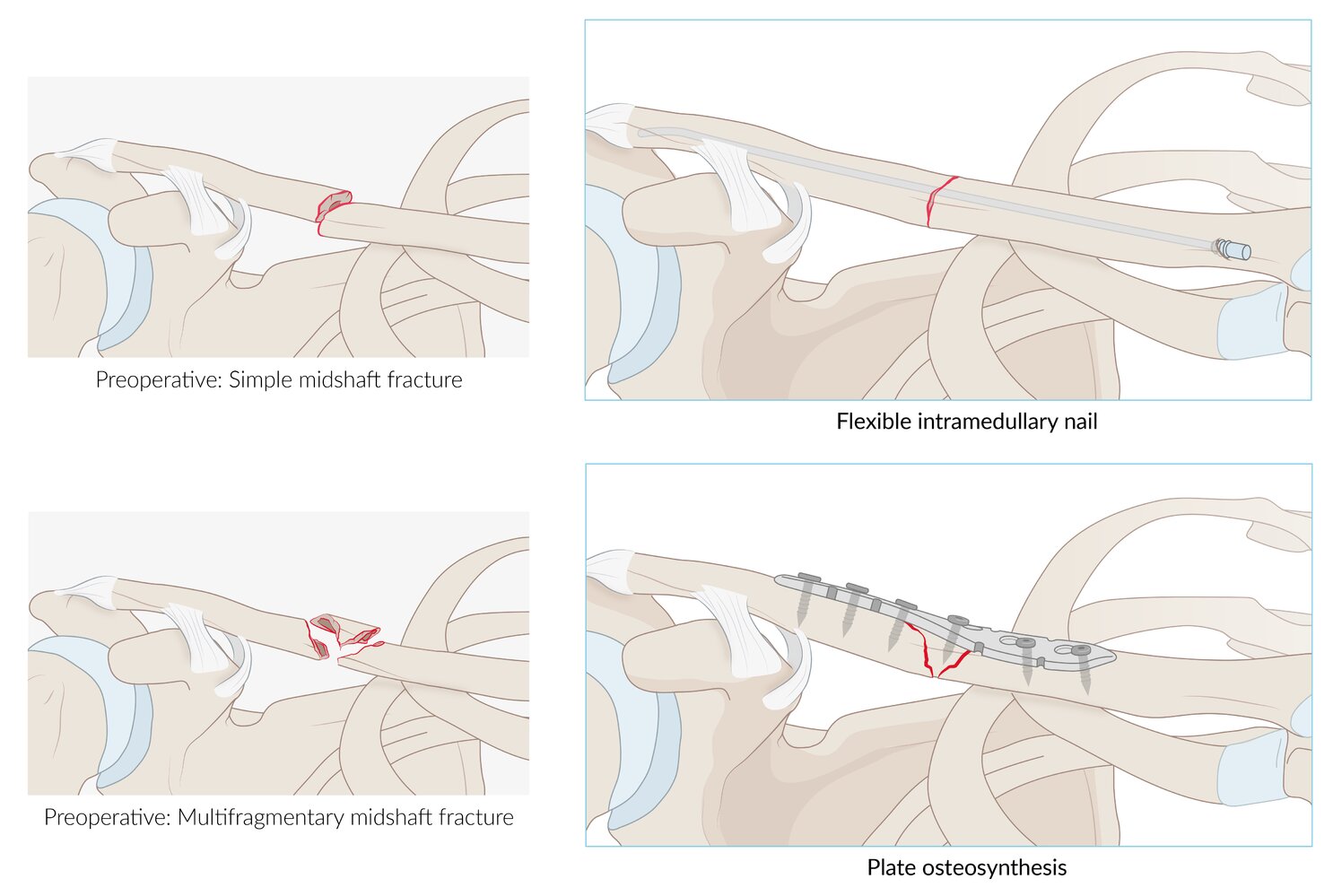
Midshaft clavicle fractures are most commonly treated conservatively, but fixation may be indicated, e.g., in excessively displaced fractures, vascular injury, or nonunion/malunion. Surgical treatment options include, e.g., a flexible intramedullary nail or plate osteosynthesis.
© AMBOSS
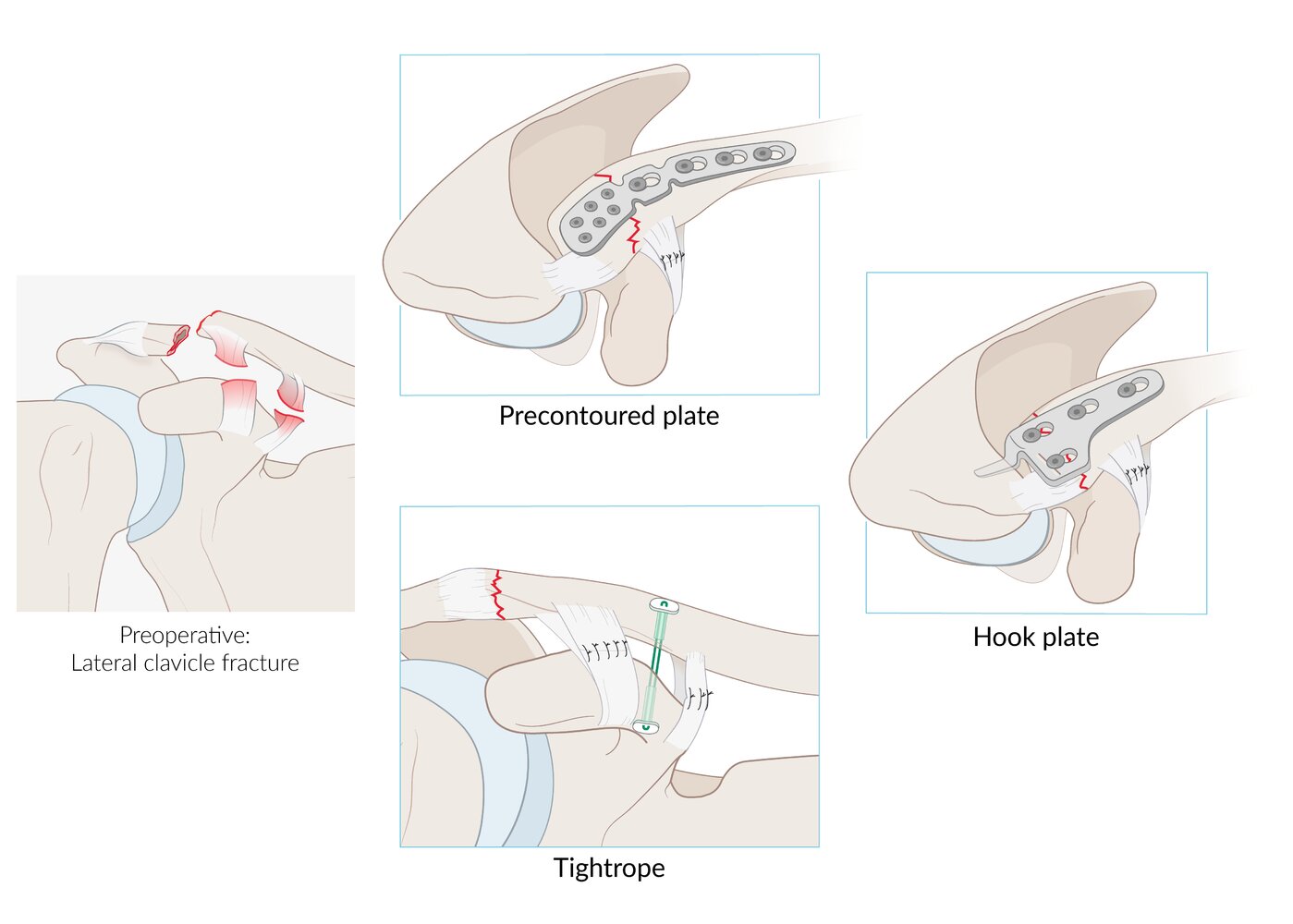
This illustration shows different surgical techniques for the reconstruction of lateral clavicle fractures (fracture is shown on the left). If necessary, the respective method is combined with suturing of ruptured ligaments.
© AMBOSS
Complications
- Fracture complications: e.g., nonunion, malunion [7]
- Neurovascular injuries: e.g., brachial plexus injury, subclavian artery injury
- Lung injuries: e.g., pneumothorax, hemothorax [7]
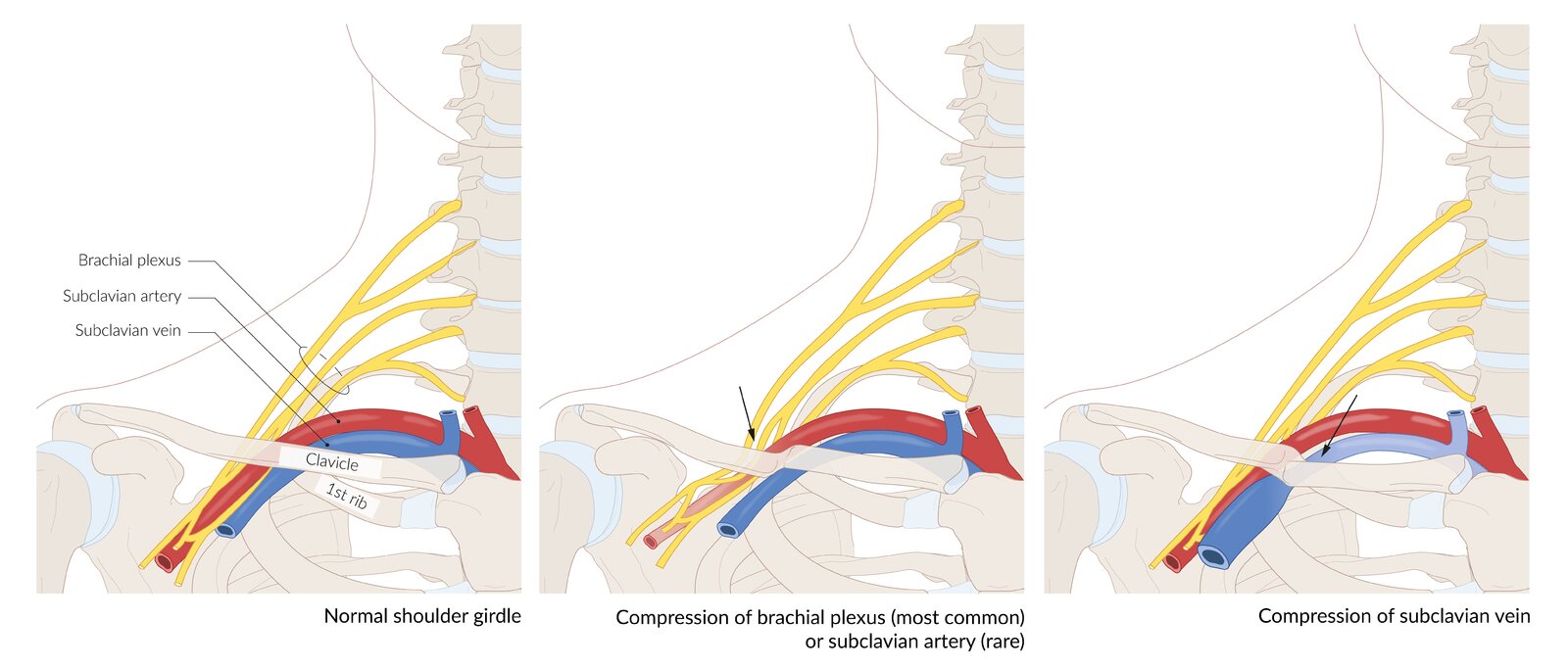
- Thoracic outlet syndrome

We list the most important complications. The selection is not exhaustive.
© AMBOSS
References
- Stanley D, Trowbridge EA, Norris SH. "The mechanism of clavicular fracture. A clinical and biomechanical analysis.". The Journal of bone and joint surgery. British volume. 70(3). :461-4. (1988)
- Robinson CM. "Fractures of the clavicle in the adult. Epidemiology and classification.". J Bone Joint Surg Br. 80(3). :476-84. (1998)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Pecci M, Kreher JB. "Clavicle fractures.". Am Fam Physician. 77(1). :65-70. (2008)
- Kim MS. "Conservative treatment for brachial plexus injury after a displaced clavicle fracture: a case report and literature review". BMC Musculoskelet Disord. 23(1). (2022)
- Tay E, Grigorian A, Schubl SD, et al. "Brachial Plexus Injury Significantly Increases Risk of Axillosubclavian Vessel Injury in Blunt Trauma Patients With Clavicle Fractures". Am Surg. 87(5). :747-752. (2020)
- Arnold S, Gilroy D, Laws P et al. "Subclavian artery laceration following clavicle fracture, successfully treated with a combined endovascular and open surgical approach". BMJ Case Rep. 14(7). :e241382. (2021)
- Flores DV, Goes PK, Gómez CM, et al. "Imaging of the Acromioclavicular Joint: Anatomy, Function, Pathologic Features, and Treatment". Radiographics. 40(5). :1355-1382. (2020)
- Hassankhani A, Amoukhteh M, Jannatdoust P et al. "A systematic review and meta-analysis on the diagnostic utility of ultrasound for clavicle fractures". Skeletal Radiol. 53(2). :307-318. (2023)
- Dhodapkar MM, Modrak M, Halperin SJ, et al. "Trends in and Factors Associated With Surgical Management for Closed Clavicle Fractures". J Am Acad Orthop Surg Glob Res Rev. 7(12). (2023)
- Wiesel B, Nagda S, Mehta S, Churchill R. "Management of Midshaft Clavicle Fractures in Adults". J Am Acad Orthop Surg. 26(22). :e468-e476. (2018)
- Lian J, Chan FJ, Levy BJ. "Classification of Distal Clavicle Fractures and Indications for Conservative Treatment". Clin Sports Med. 42(4). :685-693. (2023)
- Postacchini F, Gumina S, De Santis P, Albo F. "Epidemiology of clavicle fractures". Journal of Shoulder and Elbow Surgery. 11(5). :452-456. (2002)
- Robinson CM. "Fractures of the clavicle in the adult". J Bone Joint Surg Br. 80-B(3). :476-484. (1998)
- ROBERTS S, HERNANDEZ C, MABERRY M, et al. "Obstetric clavicular fracture: The enigma of normal birth". Obstetrics & Gynecology. 86(6). :978-981. (1995)