Summary
Colorectal cancer (CRC) is the fourth most commonly diagnosed cancer in the United States. Risk factors include a positive family history, hereditary syndromes, diet, and a number of conditions, such as inflammatory bowel disease. Most colorectal cancers (95%) are adenocarcinomas. Clinical signs are often nonspecific and may include a change in bowel habits, lower GI bleeding, and weight loss. These features as well as iron deficiency anemia in men older than 50 years of age and postmenopausal women are red flags for CRC. Since the introduction of screening with direct visualization or stool-based testing, early-stage carcinomas have become easier to diagnose in asymptomatic patients. Complete colonoscopy with histopathologic analysis confirms the diagnosis. Staging of the cancer is necessary to evaluate the extent of disease and determine the appropriate management. Curative surgical resection of colorectal cancers and metastases is preferred when feasible. The type and extent of resection depend on the stage of the cancer. In addition, for cancer stages ≥ II, chemotherapy is required for colon cancer and chemotherapy and/or radiation therapy for rectal cancer. Surveillance following CRC treatment is essential to identify and manage recurrence and/or metastases. As the incidence of CRC is high, screening for CRC is recommended for all individuals, starting at 45–50 years of age (earlier in high-risk individuals).
Epidemiology
-
Incidence [1][2]
- Excluding skin cancers, colorectal cancer is the fourth most common cancer in the US overall
- Accounts for ∼ 8% of all new cancer cases in the US
- Peak incidence: between 65 and 74 years of age
- Prevalence: ∼ 0.4%
- Mortality: third leading cause of cancer-related deaths in the US overall
")
")
Epidemiological data refers to the US, unless otherwise specified.
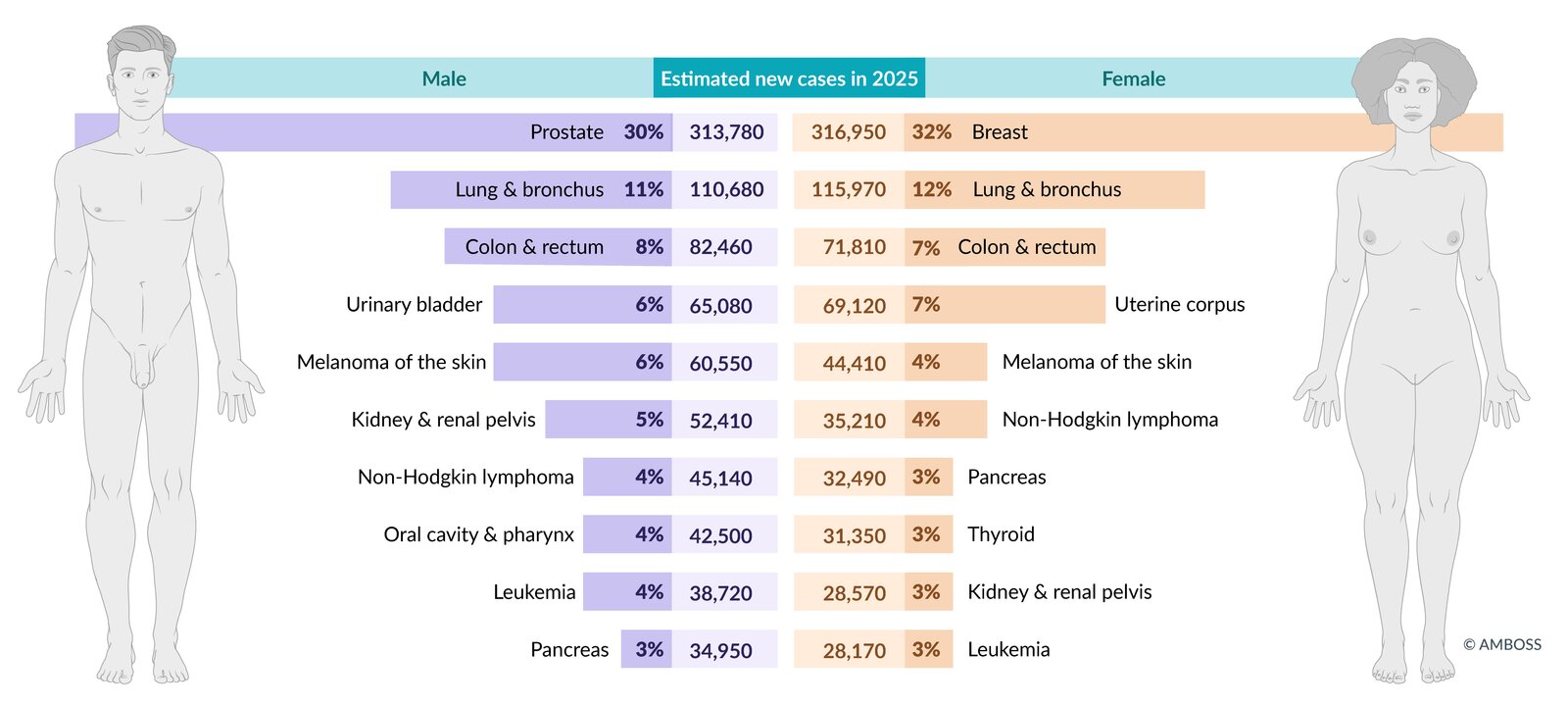
Estimated incidence of the most common cancers in the US in total figures and as a percentage of total cancer incidence (excluding non-melanoma skin cancers and in-situ carcinoma, except urinary bladder). Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
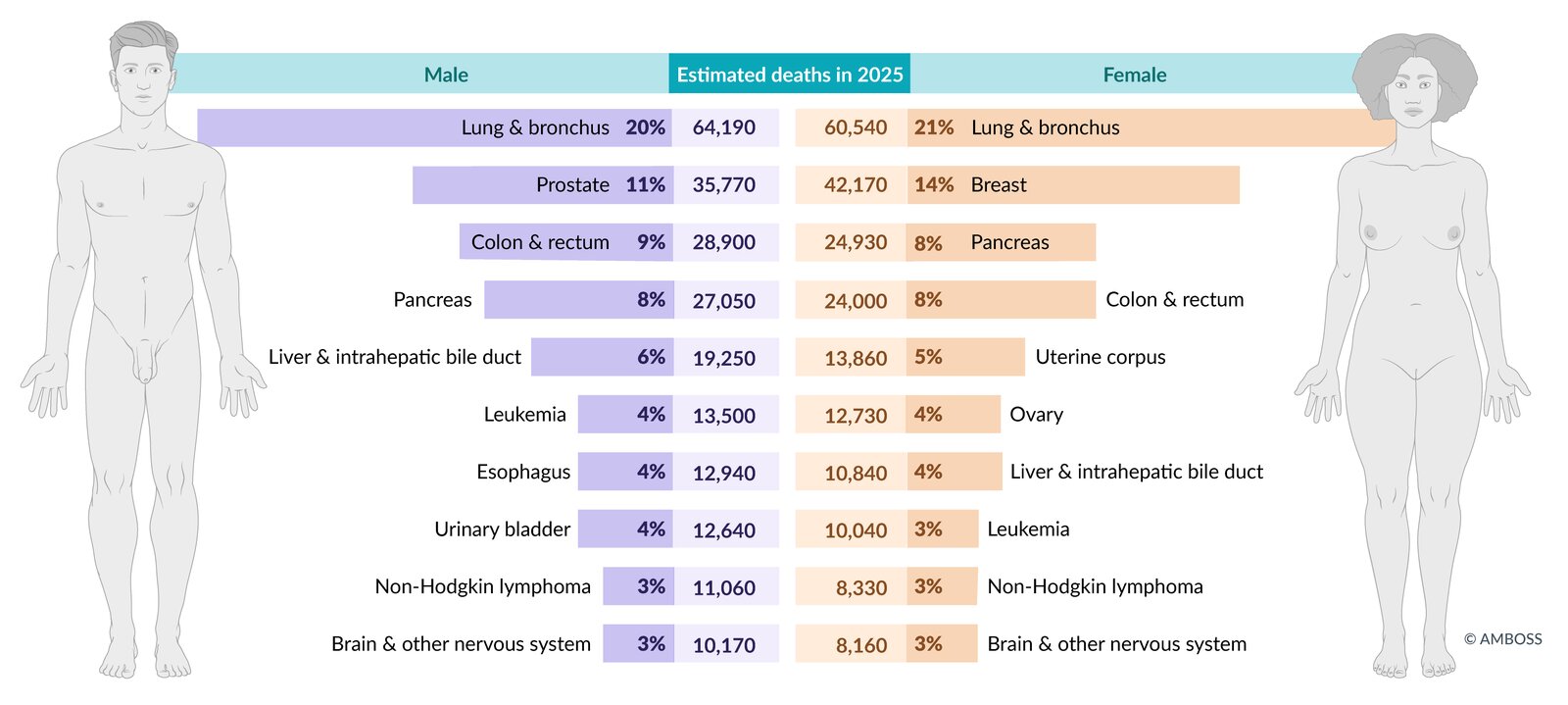
Estimated mortality from the most common cancers in the US in total figures and as a percentage of total cancer mortality. Figures are prospective estimates of the American Cancer Society for 2025.
© AMBOSS. Data source: Cancer Facts & Figures 2024, American Cancer Society, access date 06/28/24 (https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf)
Etiology
Colorectal carcinogenesis pathways (molecular pathology)
-
Chromosomal instability pathway in colon cancer: The adenoma-carcinoma sequence is the progressive accumulation of mutations in oncogenes (e.g., KRAS) and tumor suppressor genes (e.g., APC, TP53) that results in the slow transformation of adenomas into carcinomas.
- APC gene mutation (loss of cellular adhesion and increased cellular proliferation) → KRAS gene mutation (unregulated cellular signaling and cellular proliferation) → TP53 and DCC gene mutation
- Most cases of sporadic CRC develop via this pathway.
- Microsatellite instability pathway in colon cancer: due to methylation or mutations in mismatch repair genes (MMR genes, e.g., MLH1 or MSH2)
-
Hypermethylation phenotype pathway in colon cancer
- CpG island methylator phenotype (CIMP): global hypermethylation of CpG islands → silencing of MMR gene expression
- Associated with BRAF mutations
- Up to 20% of sporadic CRCs develop from serrated polyps that underwent malignant transformation via this pathway.
-
COX-2 overexpression
- Associated with colorectal cancer
- Possible protective effect of long-term use of aspirin and other NSAIDs

Risk factors for colorectal cancer [3]
- Age: older age (> 40 years) [4]
-
Hereditary syndromes
- Family history: Approx. 25% of individuals with colorectal cancer (CRC) have a positive family history.
- Familial adenomatous polyposis: 100% of individuals will have developed CRC by the age of 40 years, Gardner syndrome, Turcot syndrome, Peutz-Jeghers syndrome, Juvenile polyposis syndrome)
- Hereditary nonpolyposis colorectal cancer (HNPCC): progression to CRC in 80% of cases
-
Associated conditions
- Colorectal adenomas and serrated polyps (see “Colonic polyps”)
-
Inflammatory bowel disease: chronic inflammation → hyperplasia → non-polypoid dysplasia → neoplasia [5]
- Ulcerative colitis
- Crohn disease
- Endocarditis and bacteremia due to S. gallolyticus [6]
- Diabetes mellitus type 2
-
Lifestyle
- Smoking
- Alcohol consumption
-
Diet
- Obesity
- Processed meat
- High-fat and low-fiber
- Pathogens: Streptococcus bovis, Clostridium septicum
- Other: History of abdominal radiation during childhood
Protective factors [3]
- Long-term use of aspirin and other NSAIDs
- Physical activity
- Diet rich in fiber and vegetables and lower in meat
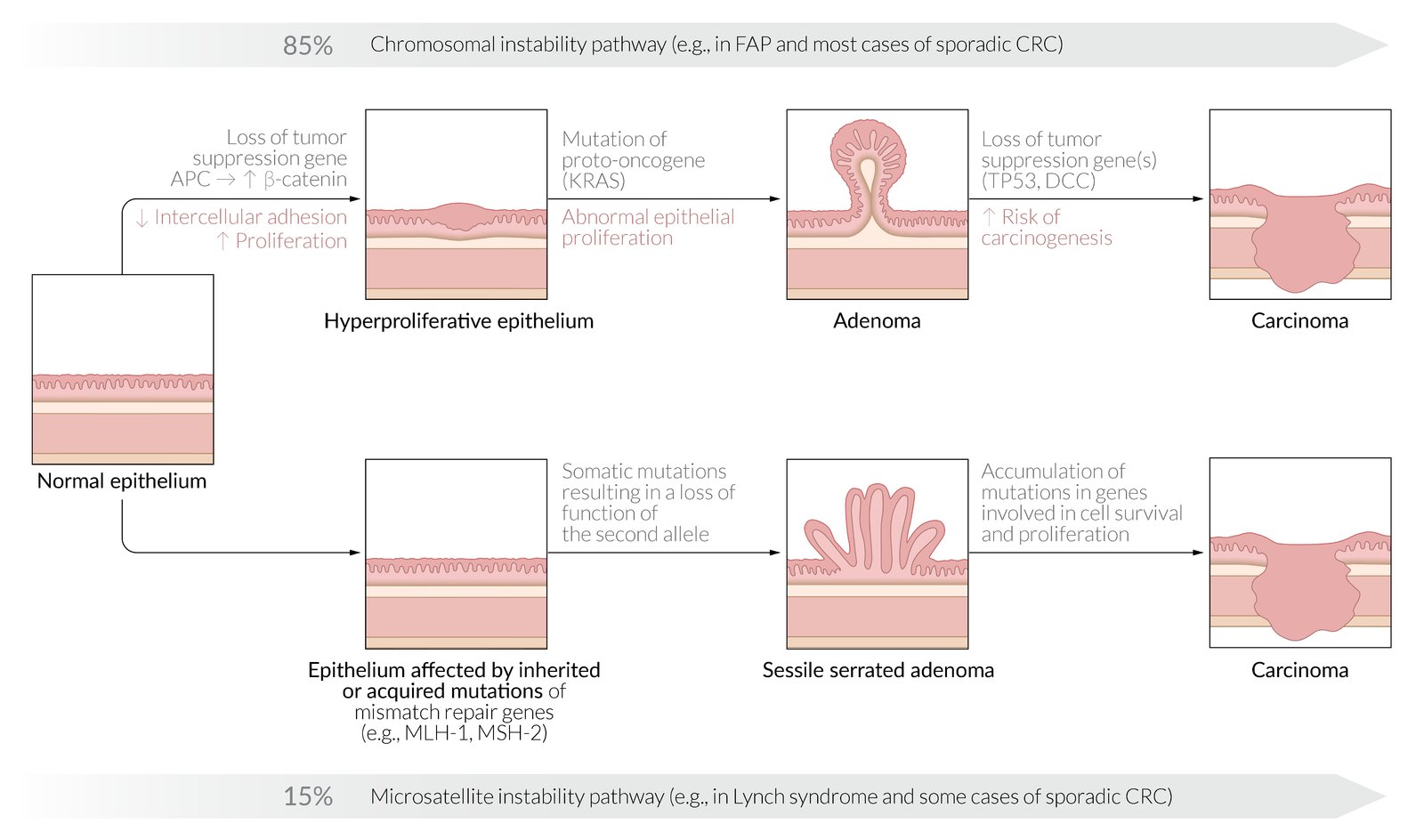
Top: Chromosomal instability pathway (adenoma-carcinoma sequence)
- Loss of the tumor suppressor gene, APC, results in hyperproliferative epithelium due to a loss of cellular adhesion and increased cellular proliferation. A mutation in KRAS results in unregulated cellular signaling and cellular proliferation, leading to the formation of an adenoma. Loss of the tumor suppressor genes TP53 and DCC results in the malignant transformation of an adenoma to carcinoma. The chromosomal instability pathway is responsible for carcinomas in FAP (loss of APC) as well as in most cases of sporadic colorectal carcinoma.
Bottom: Microsatellite instability pathway
- Acquired or inherited mutations in the mismatch repair genes (esp. MLH1 and MSH2) result in abnormal proliferation and the formation of adenoma and carcinoma. The microsatellite instability pathway is responsible for carcinomas in Lynch syndrome (HNPCC) and a few cases of sporadic colorectal carcinoma.
© AMBOSS
Clinical features
Colorectal cancer can be asymptomatic, particularly during the early stages.
Constitutional symptoms [7]
- Weight loss
- Fever
- Night sweats
- Fatigue
- Abdominal discomfort (symptoms similar to diverticulitis, especially in carcinoma of the rectosigmoid or descending colon)
Right-sided colon carcinomas [7][8]
- Definition: large bowel malignancies arising from the cecum, ascending colon, or transverse colon
-
Clinical features
- Occult bleeding or melena
- Manifestations of iron deficiency anemia (due to chronic bleeding)
- Diarrhea
Iron deficiency anemia in men > 50 years of age and postmenopausal women should raise suspicion for colorectal cancer.
Left-sided colon carcinomas [7][8]
- Definition: large bowel malignancies arising from the splenic flexure, descending colon, sigmoid colon, or the rectosigmoid junction
-
Clinical features
- Changes in bowel habits (size, consistency, frequency)
- Blood-streaked stools
- Colicky abdominal pain (due to obstruction)
Bowel obstruction occurs earlier in left-sided colon carcinomas because the distal colon has a smaller lumen than the proximal colon and contains solid fecal matter.
Rectal carcinomas [7][8]
- Definition: large bowel malignancies located ≤ 15 cm from the anal verge [9]
-
Clinical features
- Hematochezia
- ↓ Stool caliber (pencil-shaped stool)
- Rectal pain
- Tenesmus
- Flatulence
- Fecal incontinence
Cancers located ≤ 15 cm proximal to the anal verge are considered rectal carcinomas; cancers above this point are considered colon cancers.
Consider colorectal cancer in every patient with rectal bleeding, even if there is a history of hemorrhoids or diverticular disease.
Metastatic disease [10]
CRC can metastasize through hematogenous, lymphatic, transperitoneal, and contiguous routes. Symptomatic metastases may be the first manifestation of CRC.
-
Liver metastases (most common site of metastasis: ; 40–50%)
- Ascites, abdominal distention
- Hepatomegaly, RUQ pain
- Jaundice [11]
- Anorexia, early satiety
-
Lung metastases
- Dyspnea
- Cough
- Hemoptysis
- Pleural effusion
-
Peritoneal metastases
- Ascites, abdominal distension, diffuse abdominal pain
- Bowel obstruction
- Evidence of distant lymphatic spread: Virchow node (rare) [12]
Typically, cancers of the colon and upper rectum initially metastasize to the liver via the portal vein, and cancers of the lower rectum initially metastasize to the lung via the inferior vena cava.

Red flags for colorectal cancer [13][14][15]
The sensitivity and specificity of symptoms of colorectal cancer are limited. The following features have the strongest association with CRC, especially in patients with risk factors for colorectal cancer, and should always prompt further investigation.
- Melena, hematochezia
- Altered bowel habits
- Unexplained weight loss
- Unexplained iron deficiency anemia, especially in men older than 50 years of age and postmenopausal women
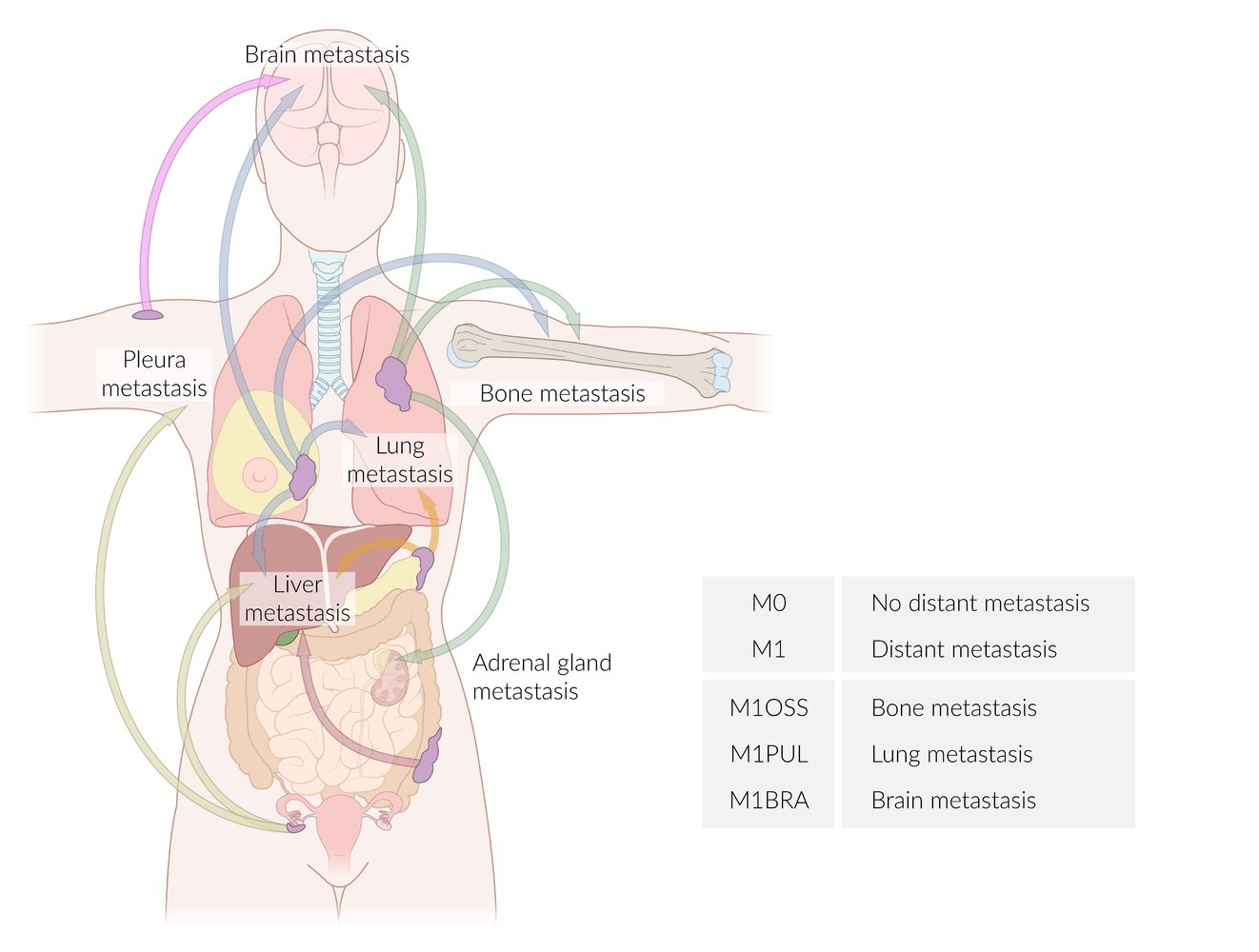
Arrows have been color-coded according to the site of the primary tumor:
Pink: skin cancer
Blue: breast cancer
Green: lung cancer
Orange: pancreatic cancer
Red: colon cancer
Lime: ovarian cancer
The table provides examples of suffixes used to specify the affected organs according to the TNM classification.
© AMBOSS
Diagnosis
All patients with suspected CRC should undergo a complete colonoscopy with biopsy of suspicious lesions. Once the diagnosis is confirmed, additional tests to stage the cancer are required to guide management.
Initial workup [9][16]
Digital rectal examination
- Indication: all patients with lower gastrointestinal bleeding (LGIB) or other red flags for CRC
-
Findings
- Distal rectal cancers may be palpable.
- Evidence of blood on DRE may indicate CRC.
-
Important considerations
- DRE is a part of the routine clinical evaluation in patients with lower gastrointestinal symptoms.
- Endoscopic evaluation is essential if there is any suspicion for CRC, such as:
- Inconclusive DRE in a patient with LGIB
- Any risk factor for CRC
- Any red flag for CRC
- Assess sphincter tone during DRE to plan optimal surgical resection for rectal cancer.
Flexible sigmoidoscopy with or without anoscopy [13]
-
Indication: Consider in patients with scanty intermittent hematochezia and all of the following features.
- Age < 40 years
- No other red flags for CRC
- No risk factor for CRC
- Important consideration: Patients who do not fulfill any of these criteria require a complete colonoscopy.
-
Findings and next steps
- Inconclusive sigmoidoscopy or lesion that raises concern for malignancy : Perform a complete colonoscopy.
- Benign pathology confirmed: Manage accordingly (see, e.g., “Hemorrhoids” and “Anal fissures”).

Complete colonoscopy
Colonoscopy is the gold standard test for CRC as it allows for direct visualization and biopsy of polyps and suspicious lesions. [17]
- Indication: : all patients with suspected CRC
-
Typical findings [18]
- Ulceroproliferative friable mass
- A biopsy is required to confirm the diagnosis (see “Pathology” section for details).
-
Important considerations: Consider the following to identify synchronous tumors if colonoscopy cannot be completed (e.g., patients with occlusive CRC). [9][16]
- Pretreatment CT colonography or capsule endoscopy [16][19]
- Intra- or postoperative colonoscopy
- In patients with rectal cancer, reattempt complete colonoscopy after neoadjuvant chemotherapy if there is evidence of tumor regression. [9]
A complete colonoscopy is imperative in all patients with suspected/confirmed CRC as multiple adenocarcinomas (synchronous tumors) are present in up to 5% of cases. [20]



Double-contrast barium enema (uncommonly performed)
- Indication: an alternative to CT colonography in patients who decline/cannot undergo a complete colonoscopy at presentation
-
Findings
- Endoluminal filling defect typically with irregular margins
- Apple core lesion (napkin ring sign): sharply defined circumferential narrowing of the bowel caused by a stenosing CRC [16][21][22]
-
Important considerations
- Double-contrast barium enema is not routinely recommended because of its low diagnostic yield and the widespread availability of CT colonography. . [16][23]
- Findings that raise suspicion for CRC on barium enema require biopsy and histopathological confirmation.

Preoperative staging
-
All colorectal cancers: Assess for local and distant spread (T stage, N stage, and M stage). [16][24]
- CT abdomen, pelvis, and chest (with IV and oral contrast)
- Consider CTA or MRI of the liver if hepatic metastases are suspected. [25] [24]
- Evaluate for specific sites of metastasis based on clinical suspicion (e.g., diagnostic laparoscopy and peritoneal cytology for suspected peritoneal metastasis). [26][27]
- Typical findings of distant metastasis
- Hepatic metastases: multiple hypodense lesions during the portal venous phase of CTA ; may show peripheral washout [25]
- Pulmonary metastases: multiple, peripheral nodules of varying sizes [28][29]
- See also “Differential diagnosis of pulmonary nodules” and “Metastatic liver disease.”
-
Additional staging workup in rectal cancer [9]
- Pelvic MRI with and without IV contrast: to determine T stage and N stage
- Rectal endoscopic ultrasound: Consider in early tumor stages or if MRI is contraindicated.
- Rigid proctosigmoidoscopy: to assess the distance of the tumor from the anus


Laboratory studies [16]
-
Carcinoembryonic antigen (CEA): Obtain baseline levels in all patients before initiating treatment. ; [16]
- Monitor CEA levels during treatment and follow-up to assess response to treatment and evaluate recurrence.
- Should not be used for screening [30]
- CBC: may show microcytic anemia (iron deficiency anemia)
- Liver chemistries and coagulation: may be abnormal in patients with multiple hepatic metastases
- Counseling and genetic testing: for patients < 50 years of age with CRC or those with a family history of CRC at a young age (see “Revised Bethesda guidelines” for details)
CEA is a prognostic marker and should not be used to screen for colorectal cancer.
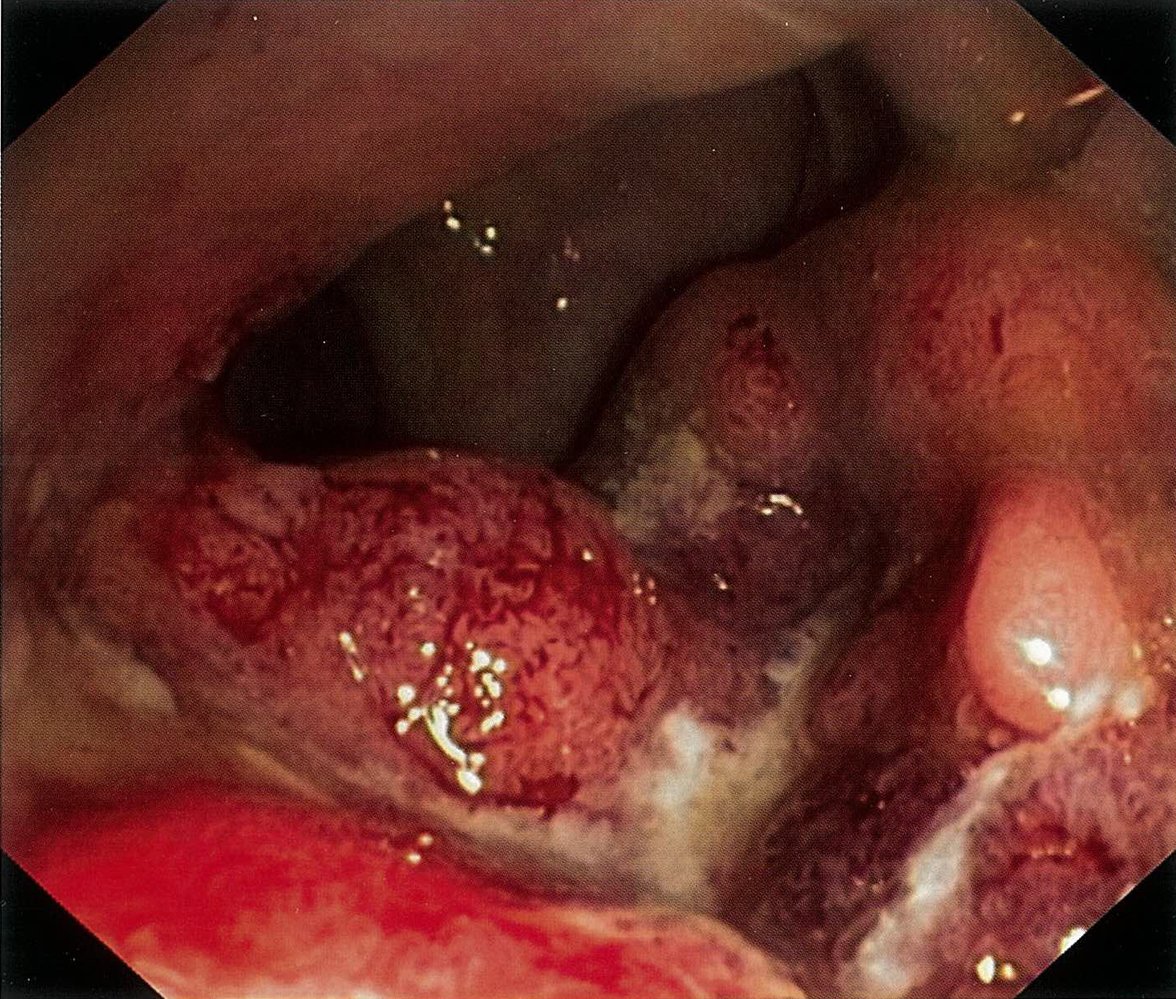
Endoscopic view of the rectum
An exophytic, ulcerated mass with raised edges covers more than half of the circumference and partially obstructs the lumen. The tumor's surface is amorphous and shows minor spontaneous bleeding.
These findings are strongly suggestive of rectal cancer.
Source: © IMPP
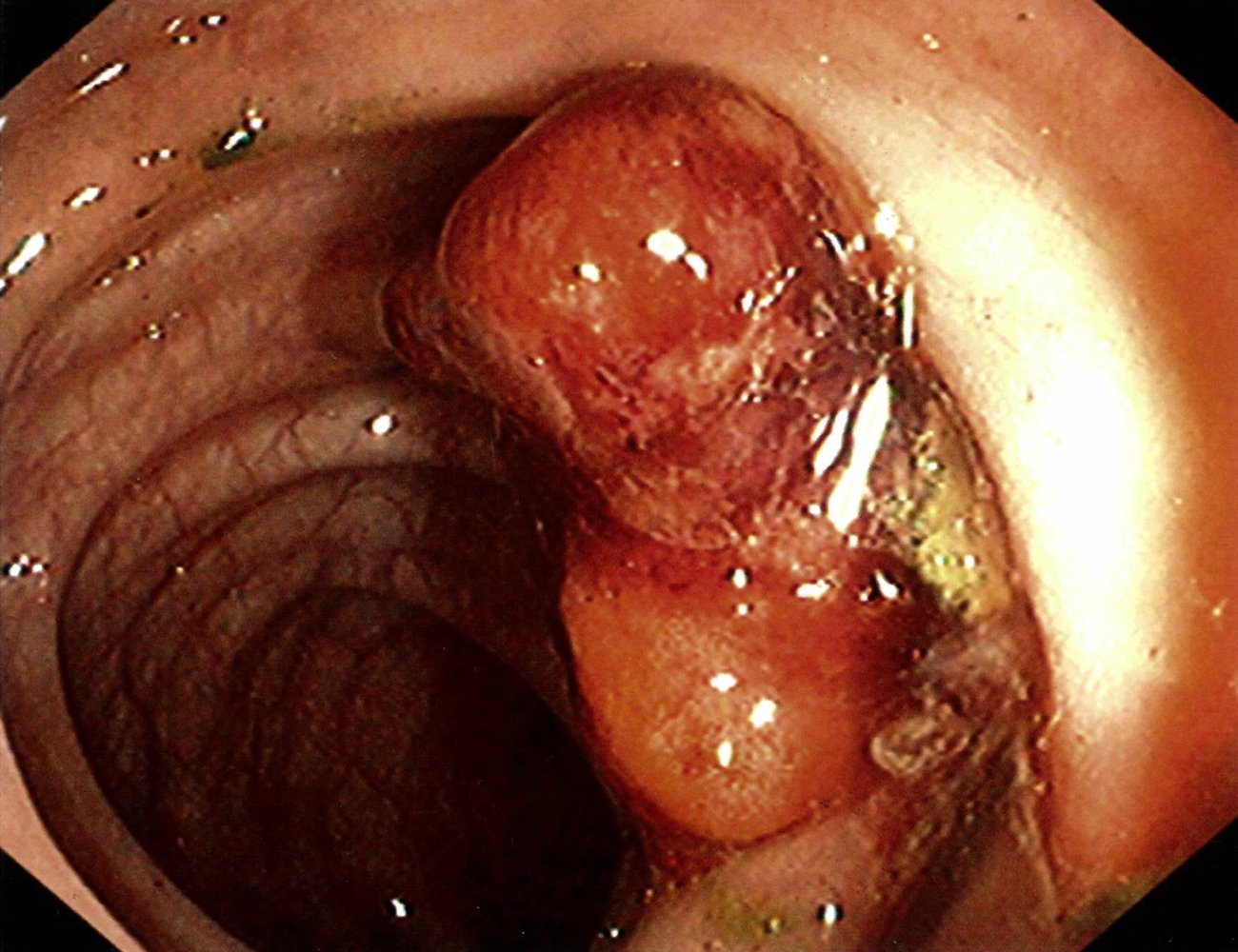
Endoscopic view of the ascending colon
An irregular exophytic mass with raised edges is visible. The surface is amorphous and shows minor bleeding.
These features are highly suggestive of colon cancer. However, histopathology is necessary to confirm the diagnosis.
Source: © IMPP
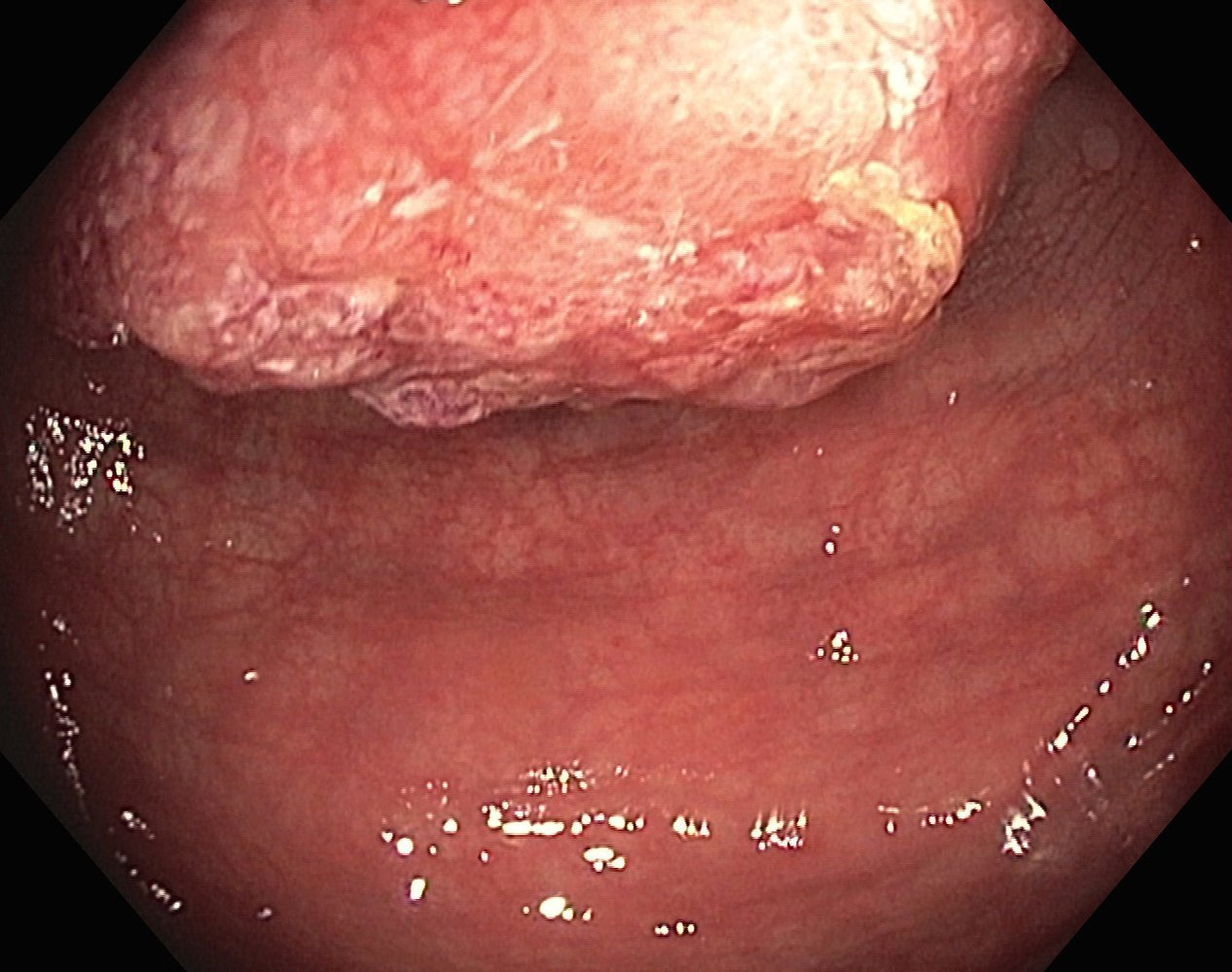
Endoscopic view of the colon
An exophytic tumor with an irregular and partially amorphous surface is visible (green overlay). The tumor almost entirely obstructs the lumen of the colon. The surrounding mucosa has a normal surface and vascular pattern.
These features are consistent with adenocarcinoma. Histopathology is necessary to confirm the diagnosis.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
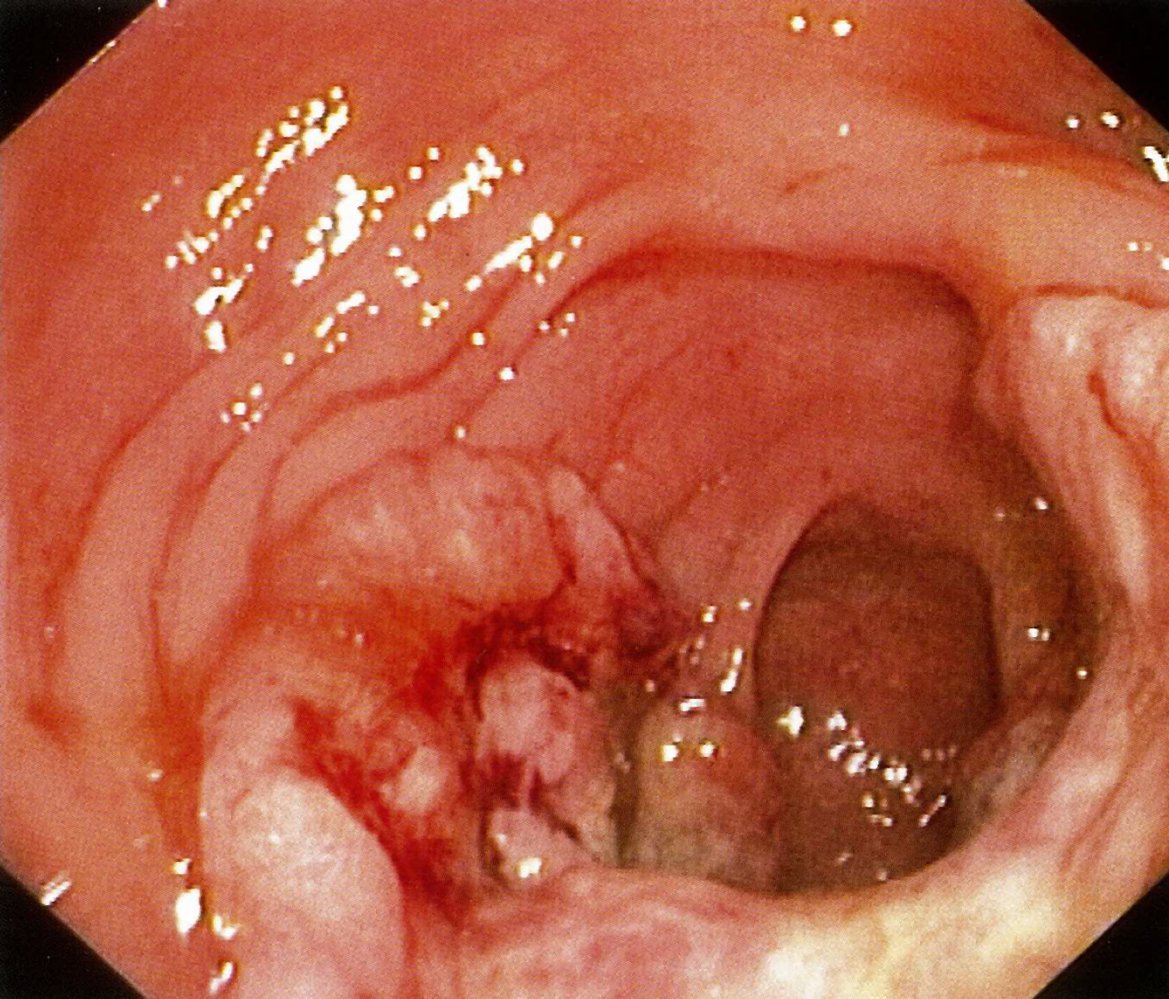
Endoscopic view of the colon
An exophytic, ulcerated mass with raised edges covers more than half of the colon's circumference (green overlay). The surface is amorphous and shows minor spontaneous hemorrhage.
These features are highly suggestive of adenocarcinoma. However, histopathology is necessary to confirm the diagnosis.
Source: © IMPP

Fluoroscopy (barium enema; lateral view)
An apple core sign (also called napkin ring sign; green overlay) is seen in the distal descending colon. It is the result of annular constriction by a colorectal carcinoma.
Source: “Radiology apple core sign” by agarger, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
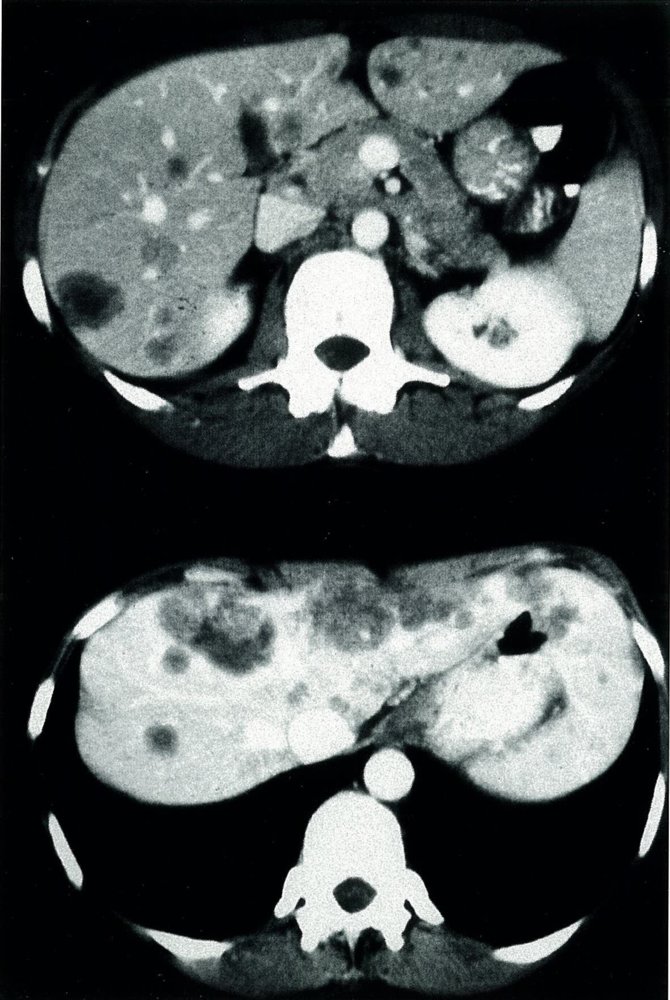
CT abdomen (with contrast; axial plane; top: late arterial phase; bottom: late portal phase) of a patient with colon cancer
Multiple hypodense lesions (green overlay) are visible throughout the liver. Some lesions contain necrotic areas (hatched overlay).
A: aorta; HV: hepatic vein; S: stomach; Sp: spleen; K: kidney; Pa: pancreas; IVC: inferior vena cava; SMV: superior mesenteric vein; VB: vertebral body
Source: © IMPP
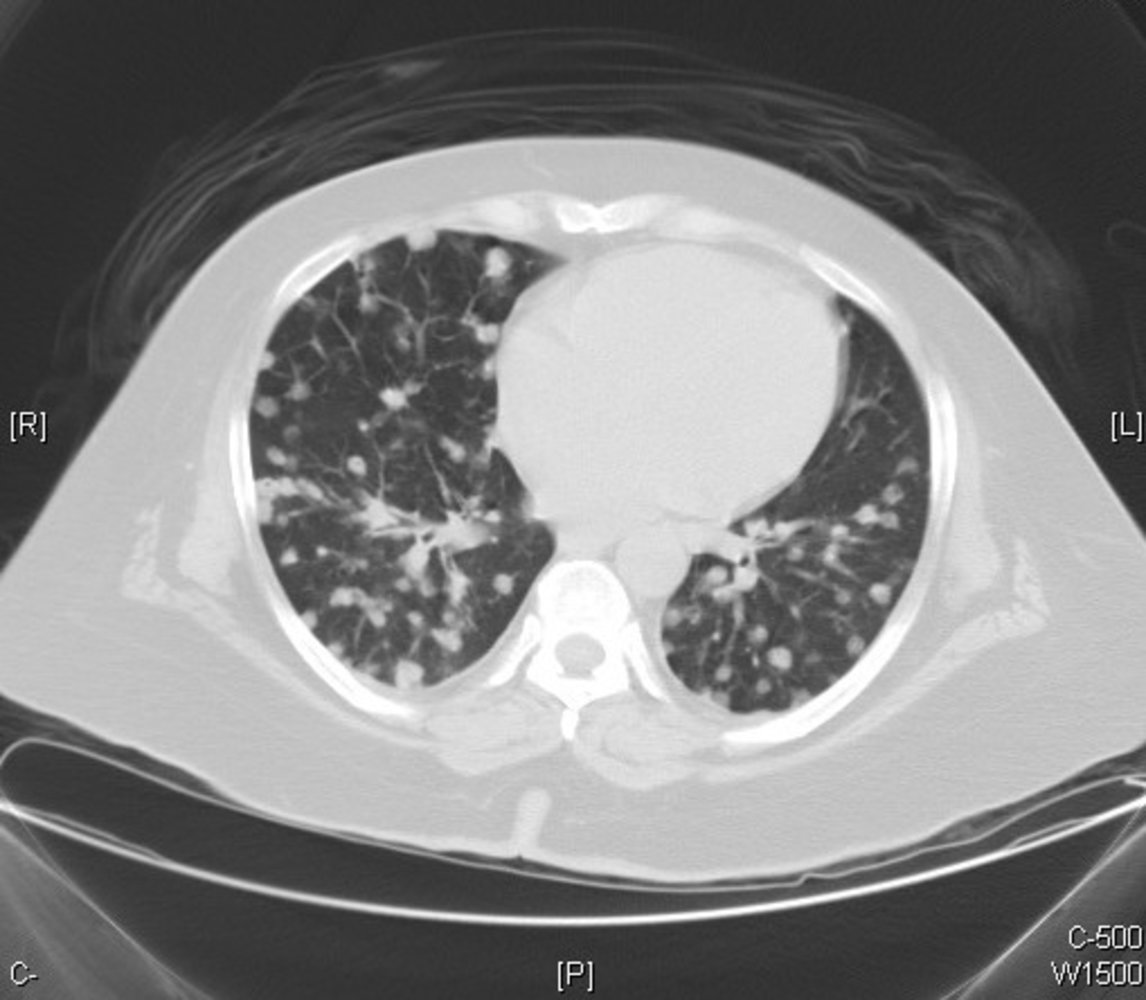
CT chest (axial plane; lung window) of a patient with lung metastases from colon carcinoma
Multiple small, circumscribed nodules of varying sizes (examples indicated by green overlays) can be seen in both lungs. A few nodules (examples indicated by red overlays) contain small foci of air, which may represent small bronchioles or sites of early cavitation.
Source: “Metastatic colonic adenocarcinoma - CT scan - Case 263” by Yale Rosen, Flickr, licensed under CC BY-SA 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 2.0.
Staging
Once the diagnosis is confirmed, CRC should be staged to determine management. The American Joint Committee for Cancer (AJCC) TNM classification is currently the standard staging system used in clinical practice. The Dukes classification is a simplified approach to staging that is of academic interest but is not used to guide management.
| Colorectal cancer staging | |||
|---|---|---|---|
| AJCC staging 8th edition (simplified) [31] | TNM stage | Corresponding Dukes classification stage | Description |
| 0 |
|
|
|
| I |
|
|
|
| II |
|
|
|
| III |
|
|
|
| IV |
|
|
|
Differential diagnoses
Differential diagnoses based on clinical presentation
- Differential diagnoses of lower GI bleeding
- Differential diagnoses of diarrhea
- Differential diagnoses of constipation
- Differential diagnoses of large bowel obstruction
- Differential diagnoses of metastatic liver disease
Small bowel neoplasms
-
Epidemiology
- Less than 5% of all gastrointestinal cancers
- Mainly benign lesions (> 95%)
- Malignant small bowel cancers (1–3%)
- 40% small bowel adenocarcinoma
- 30% neuroendocrine tumors
- 20% lymphoma
- 10% gastrointestinal stromal tumors (GIST), leiomyosarcoma, liposarcoma, metastatic disease
-
Diagnostics
- Endoscopy
- Ultrasound
- Hydro-MRI
- Capsule endoscopy
-
Treatment
- Resection of the small bowel
- R1 resection requires adjuvant chemotherapy
-
Complications
- Bleeding
- Ileus
- Metastatic spread
- Carcinoid syndrome in the case of neuroendocrine cancers of the small bowel
- Prognosis (if malignant): 5-year survival rate is ∼ 68% [33]


The differential diagnoses listed here are not exhaustive.
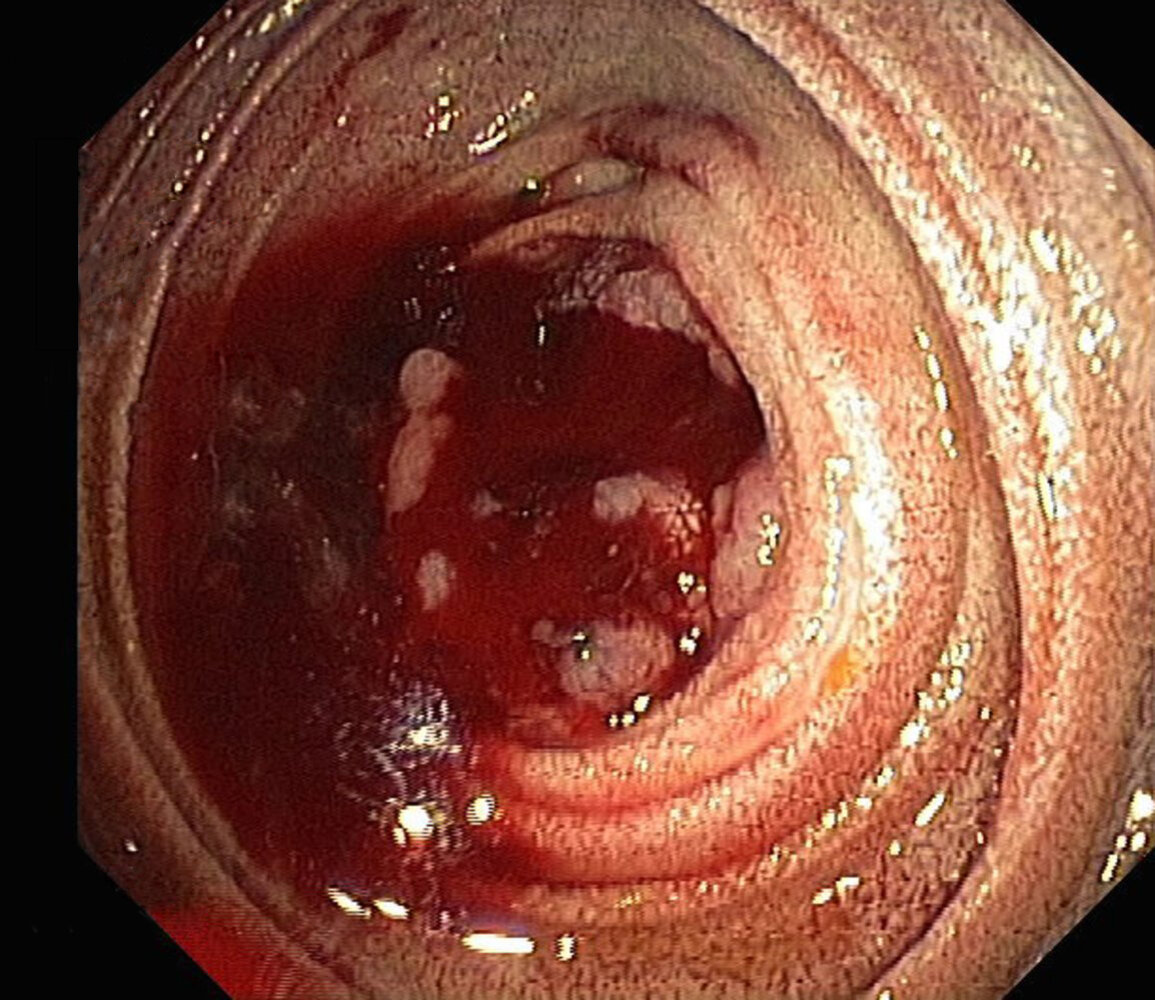
Endoscopic view of the distal duodenum
An actively bleeding polyploid tumor is partially obstructing the duodenum, making macroscopic assessment difficult.
Actively bleeding polyploid tumors in the small intestine should raise suspicion for malignancy. Histopathological examination of the tumor biopsy revealed a poorly differentiated mucinous adenocarcinoma.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
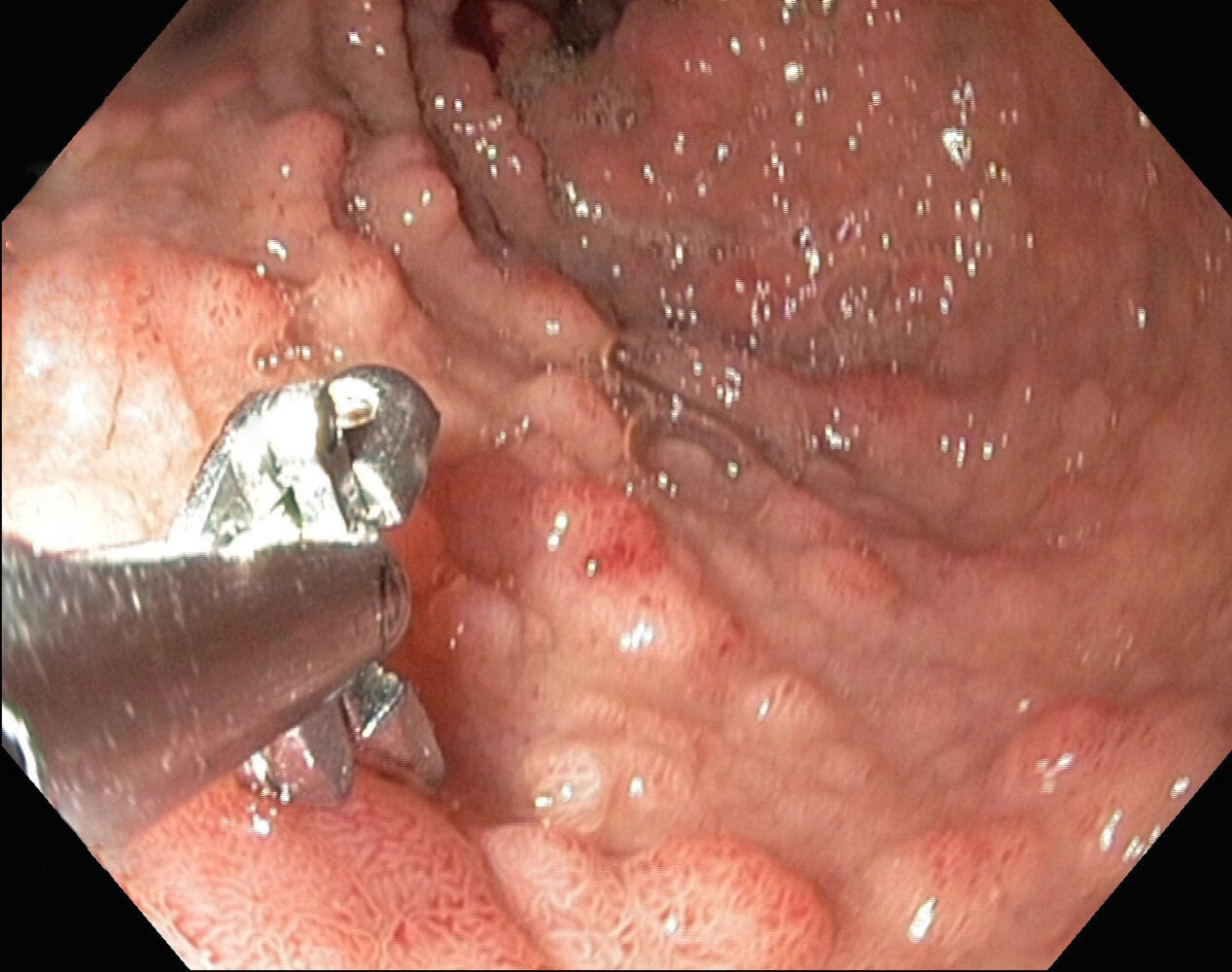
Endoscopic view of the duodenum
Flat polypoid lesions are visible over the entire mucosa. No normal duodenal mucosa can be seen. Biopsy forceps are visible on the lower left side.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Treatment
General principles [9][16]
- A multidisciplinary approach is recommended.
- Treatment depends primarily on the location of the tumor and the TNM stage.
- Curative treatment is primarily surgical and may involve neoadjuvant or adjuvant chemotherapy and/or radiation therapy.
- Palliative treatment may involve chemotherapy, radiation therapy, and, in some cases, surgery.
- See “Treatment of colon cancer” and “Treatment of rectal cancer” for details.
Surgery for colorectal cancer [9][16]
Curative surgery
-
Surgery of primary tumor
- Indicated in any resectable primary tumor with no metastasis or resectable distant metastases
- Conventional or laparoscopic approach is possible [16]
- Complete resection with clear margins (R0 resection) is associated with the best prognosis.
- See “Surgery for colon cancer” and “Surgery for rectal cancer” for details.
-
Regional lymph node dissection: performed routinely alongside resection of the primary tumor
- Resection of mesenteric lymph nodes along the path of lymphatic drainage
- Histological analysis of 12 removed lymph nodes to accurately define the lymph node status is required for accurate staging. [32]
-
Resection of metastases
- Indicated in patients with resectable metastases (e.g., liver and/or lung metastasis)
- May significantly improve the survival of patients with limited metastatic disease.
Palliative surgery
Consider in patients with nonresectable distant metastases to prevent or treat complications of colorectal cancer.
- Intestinal bypass (e.g., ileocolonic anastomosis, colostomy) or enteral stenting for obstructing/occlusive CRC
- Tumor resection to manage immediately life-threatening complications, such as complete bowel obstruction, persistent GI bleeding, or perforation. [16]
Systemic therapy [9][16][34]
Systemic therapy is indicated in most patients with colon or rectal cancer. See “Treatment of colon cancer by stage” and “Treatment of rectal cancer by stage” for details. [34][35]
-
Chemotherapy regimens
- FOLFOX: folinic acid (leucovorin) PLUS 5-fluorouracil (5-FU) PLUS oxaliplatin
- FOLFIRI: folinic acid (leucovorin) PLUS 5-fluorouracil (5-FU) PLUS irinotecan
- CAPOX: capecitabine PLUS oxaliplatin
-
Biologics
- Anti-VEGF antibodies (e.g., bevacizumab)
- EGFR antibodies (e.g., cetuximab)
Radiation therapy
- Rectal cancer: standard treatment modality in most stages of rectal cancer [9]
-
Colon cancer
- Not a standard modality because of adverse effects on the small intestine leading to enteritis and strictures
- May be used in palliative care to treat bone and brain metastases [36][37]
Treatment of colon cancer
Principles of colon cancer treatment [16]
| Treatment of colon cancer by stage | ||
|---|---|---|
| AJCC stage | Treatment approach | |
| Stage I |
|
|
| Stage II |
|
|
| Stage III |
|
|
| Stage IV |
|
|
The treatment of colon cancer is mainly surgical, supplemented with chemotherapy. Radiation therapy is not a standard therapeutic modality for colon cancers.
Surgery for colon cancer [16][38][39]
- Colectomy with lymph node dissection is indicated in all resectable tumors.
- The extent of the resection depends on the location of the tumor as well as the blood supply and lymphatic drainage of the affected region.
- En bloc resection of infiltrated adjacent tissue is recommended to obtain an R0 resection.
- In patients with peritoneal metastases, consider cytoreductive surgery in combination with intraperitoneal chemotherapy (HIPEC or hyperthermic intraperitoneal chemotherapy). [16]
- Bowel continuity should be restored via anastomosis when feasible; a stoma (temporary/permanent) may be needed. [40]
| Typical surgeries for colon cancer [38][39][41] | |||
|---|---|---|---|
| Type of resection | Description | Indication | |
| Hemicolectomy | Right hemicolectomy |
|
|
| Extended right hemicolectomy |
|
|
|
| Left hemicolectomy |
|
|
|
| Sigmoid colectomy |
|
|
|
| Subtotal or total abdominal colectomy |
|
|
|
| Less commonly used techniques |
|
||









© AMBOSS
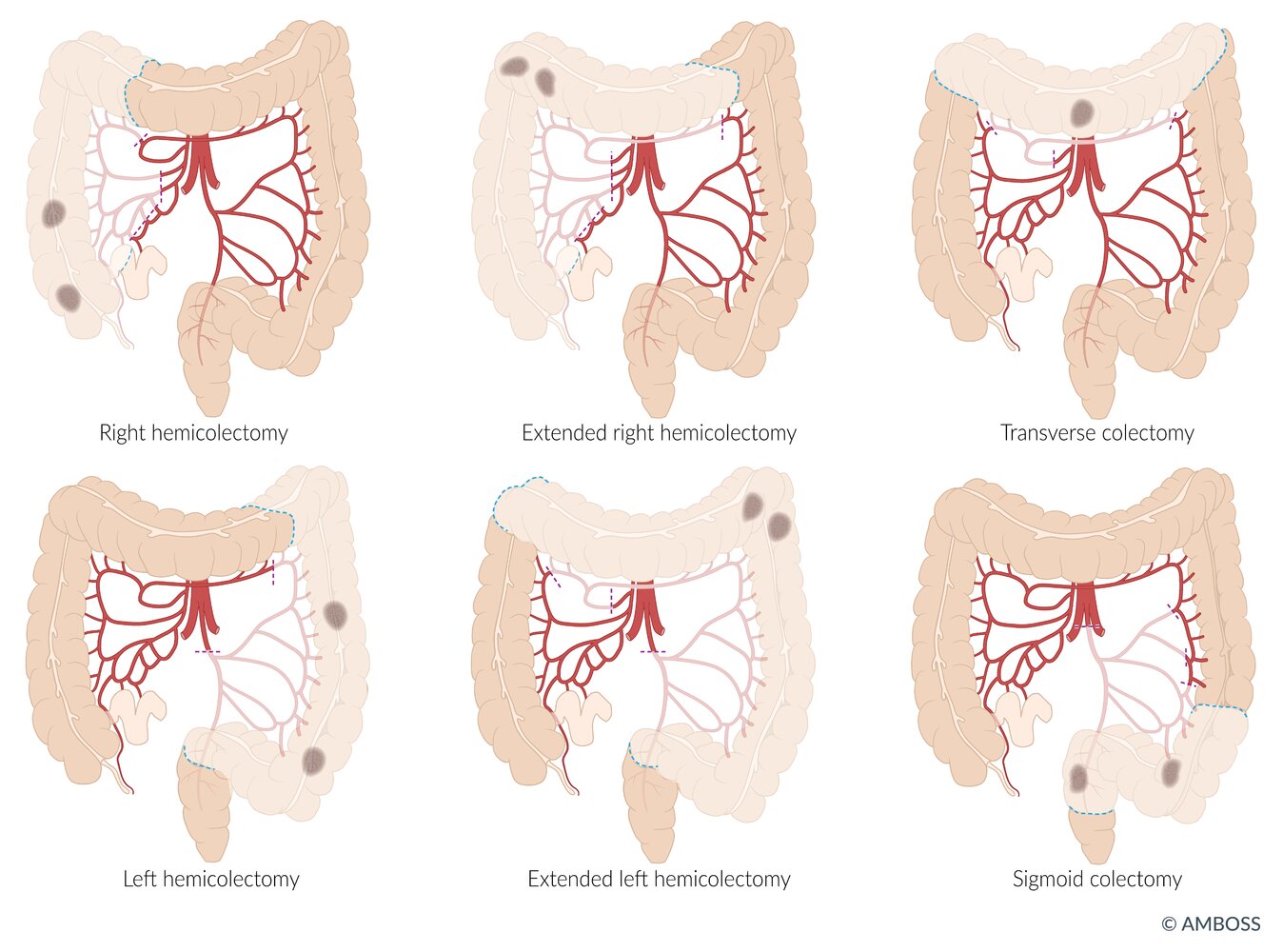
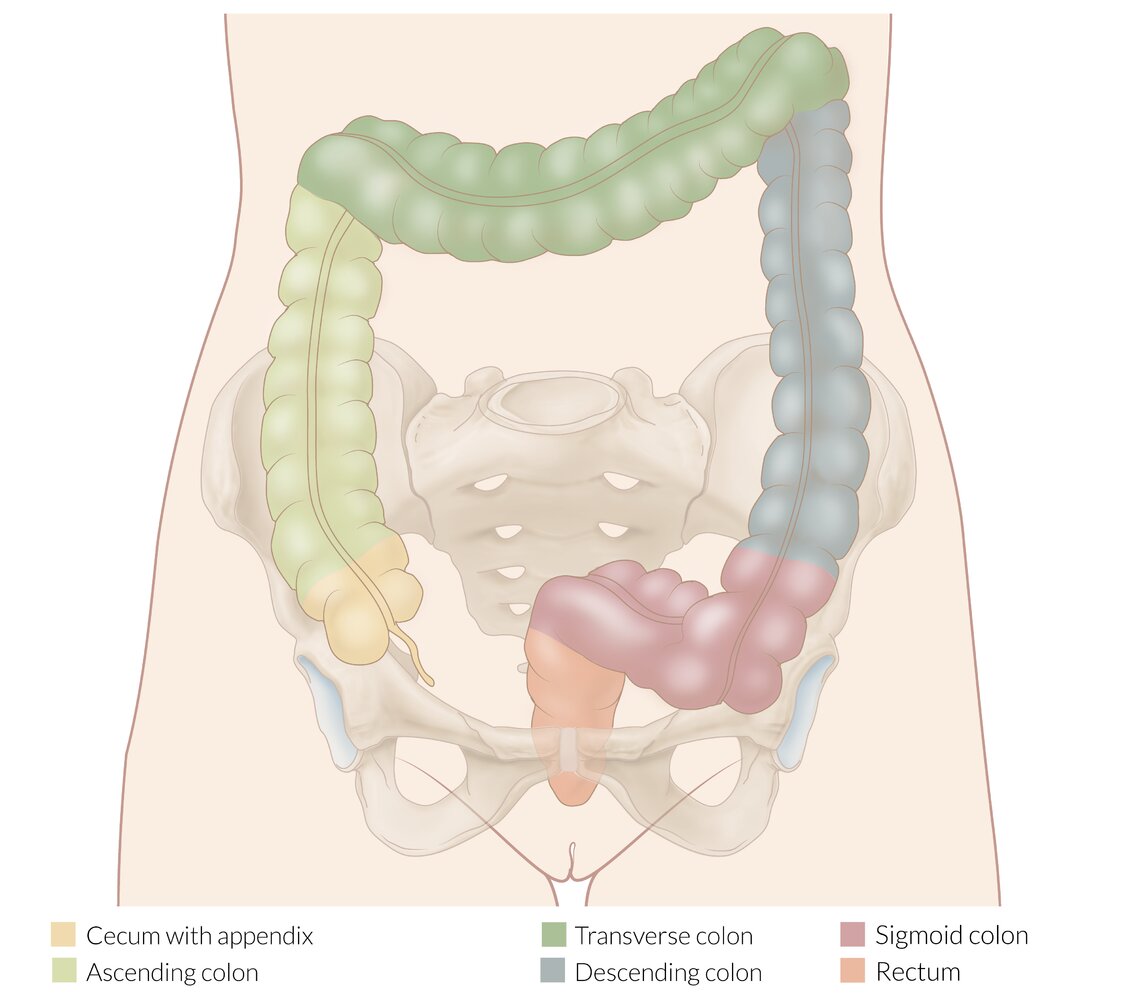
The site and extent of resection are determined by the location of tumors (indicated as gray lesions) as well as the blood supply and lymphatic drainage of the affected section of the bowel.
© AMBOSS
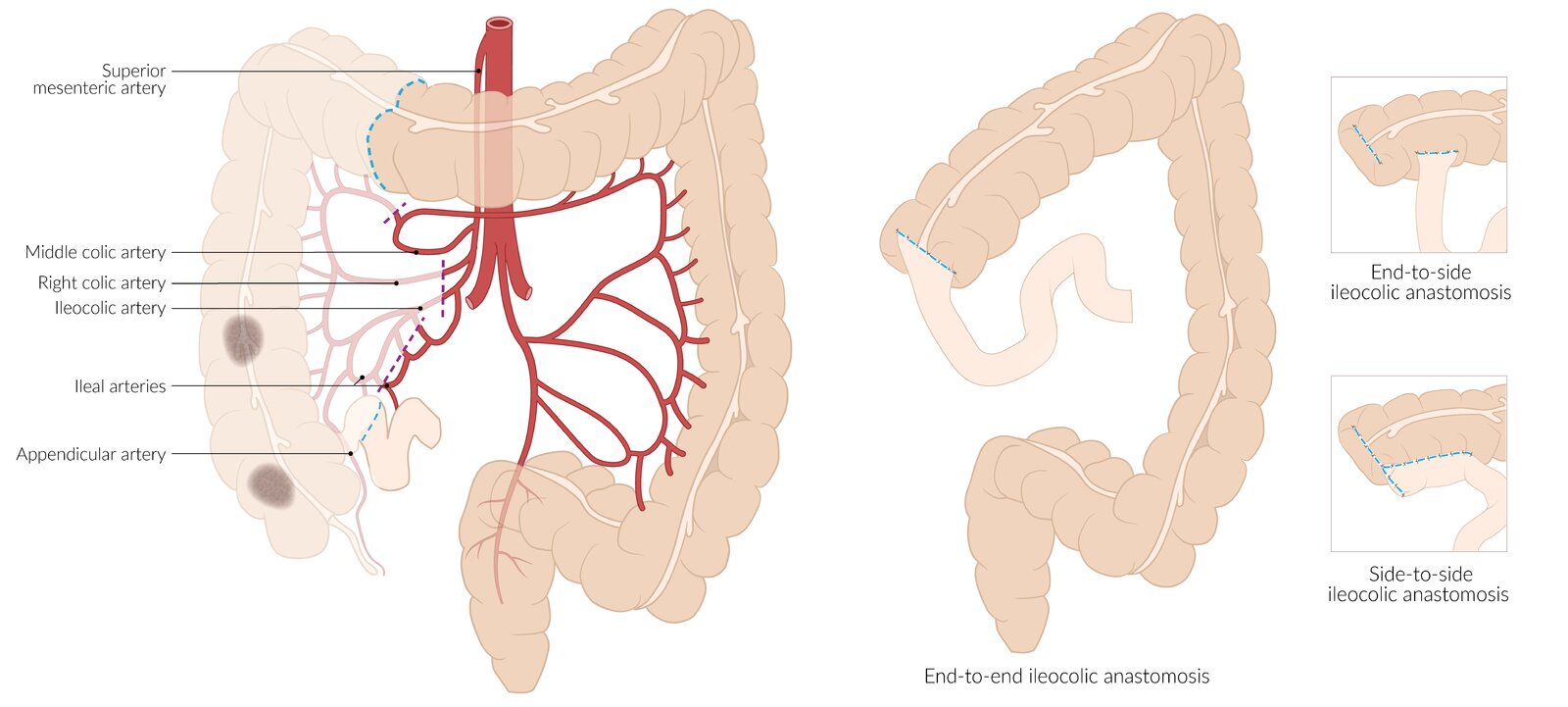
Extent of resection (left): between the distal ileum and proximal third of the transverse colon (blue dashed lines). The arterial blood supply to this section, including the ileocolic artery, right colic artery, and right branch of the middle colic artery, is ligated (purple dashed lines). Malignancy (lesions shown in gray) is a common indication for this procedure.
Reconstruction (right): typically achieved via end-to-end, end-to-side, or side-to-side ileocolic anastomosis
© AMBOSS
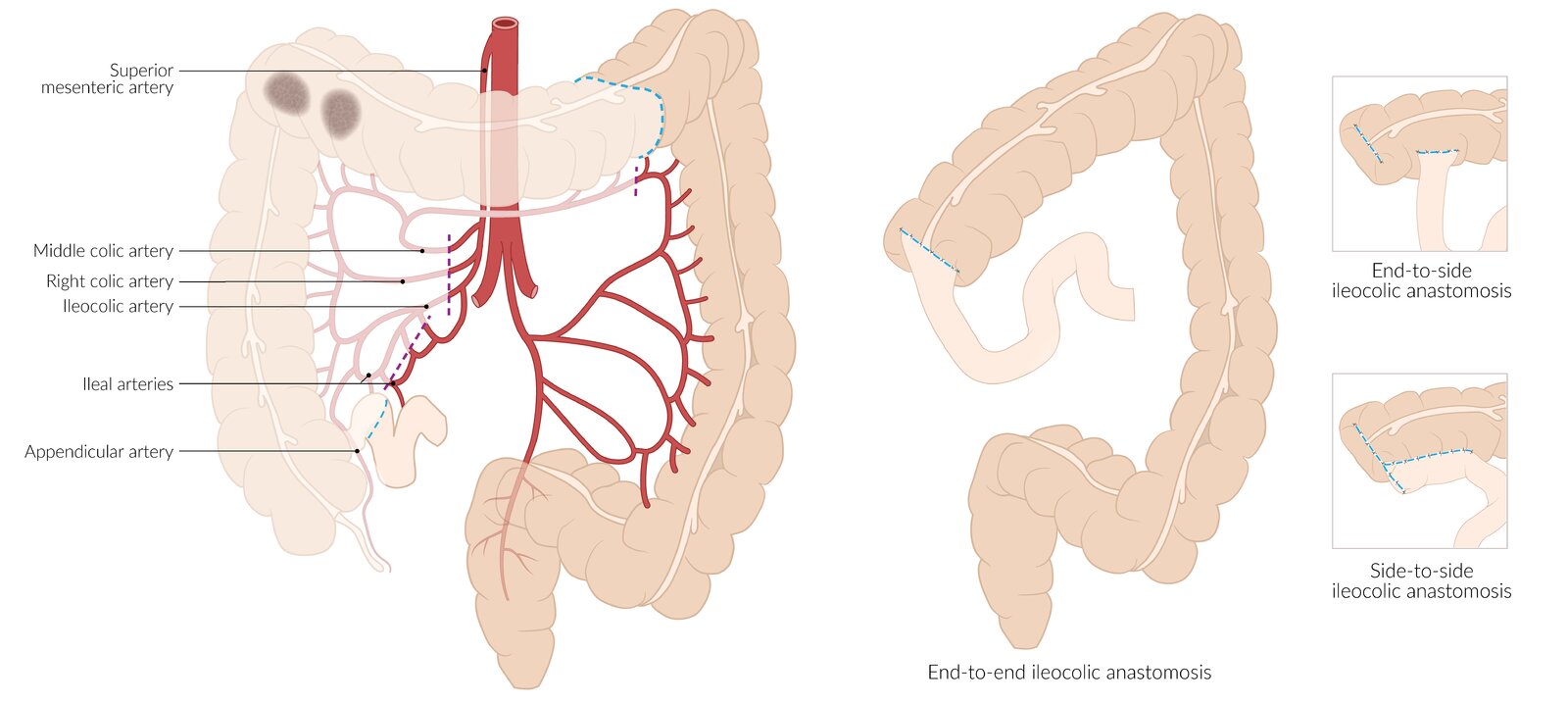
Extent of resection (left): between the distal ileum and distal third of the transverse colon (blue dashed lines). The arterial blood supply to this section, including the ileocolic artery, ileal arteries, and right and middle colic arteries, is ligated (purple dashed lines). Malignancy (lesions shown in gray) is a common indication for this procedure.
Reconstruction (right): typically achieved via end-to-end, end-to-side, or side-to-side ileocolic anastomosis
© AMBOSS
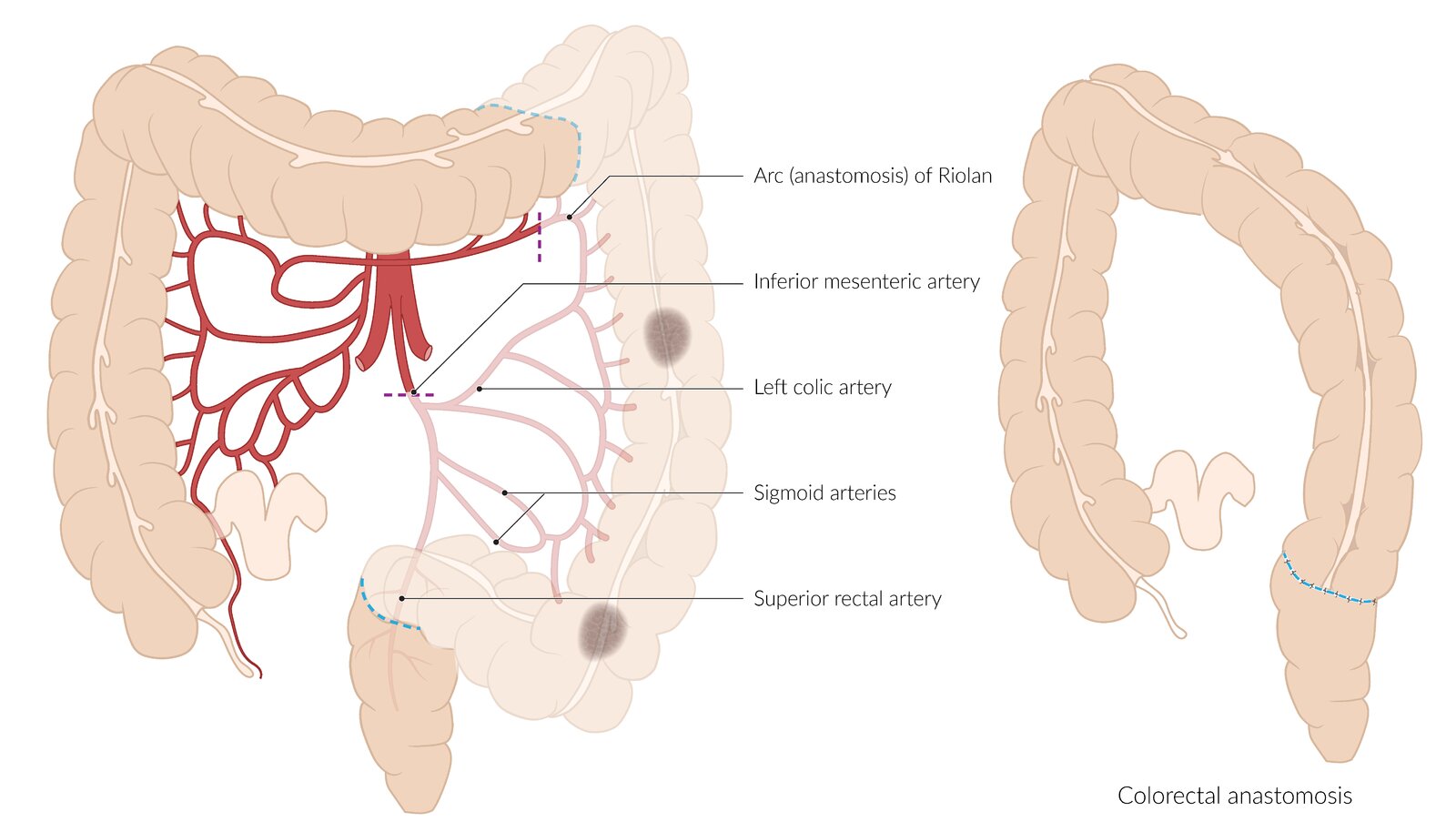
Extent of resection (left): between the distal third of the transverse colon and sigmoid colon (blue dashed lines). The arterial blood supply to this section, including the inferior mesenteric artery and the left branch of the middle colic artery, is ligated (purple dashed lines). Malignancy (lesions shown in gray) is a common indication for this procedure.
Reconstruction (right): typically achieved via end-to-end colorectal anastomosis
© AMBOSS
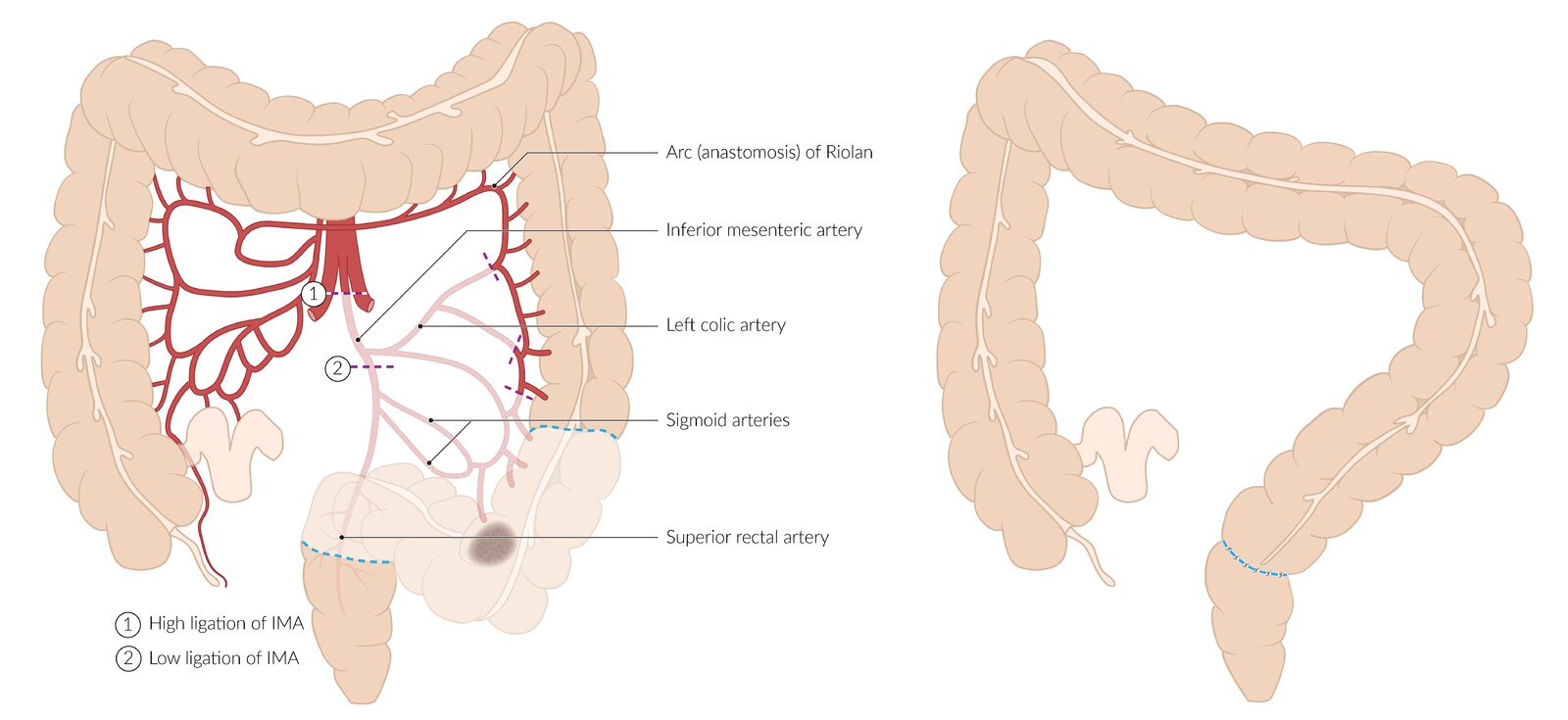
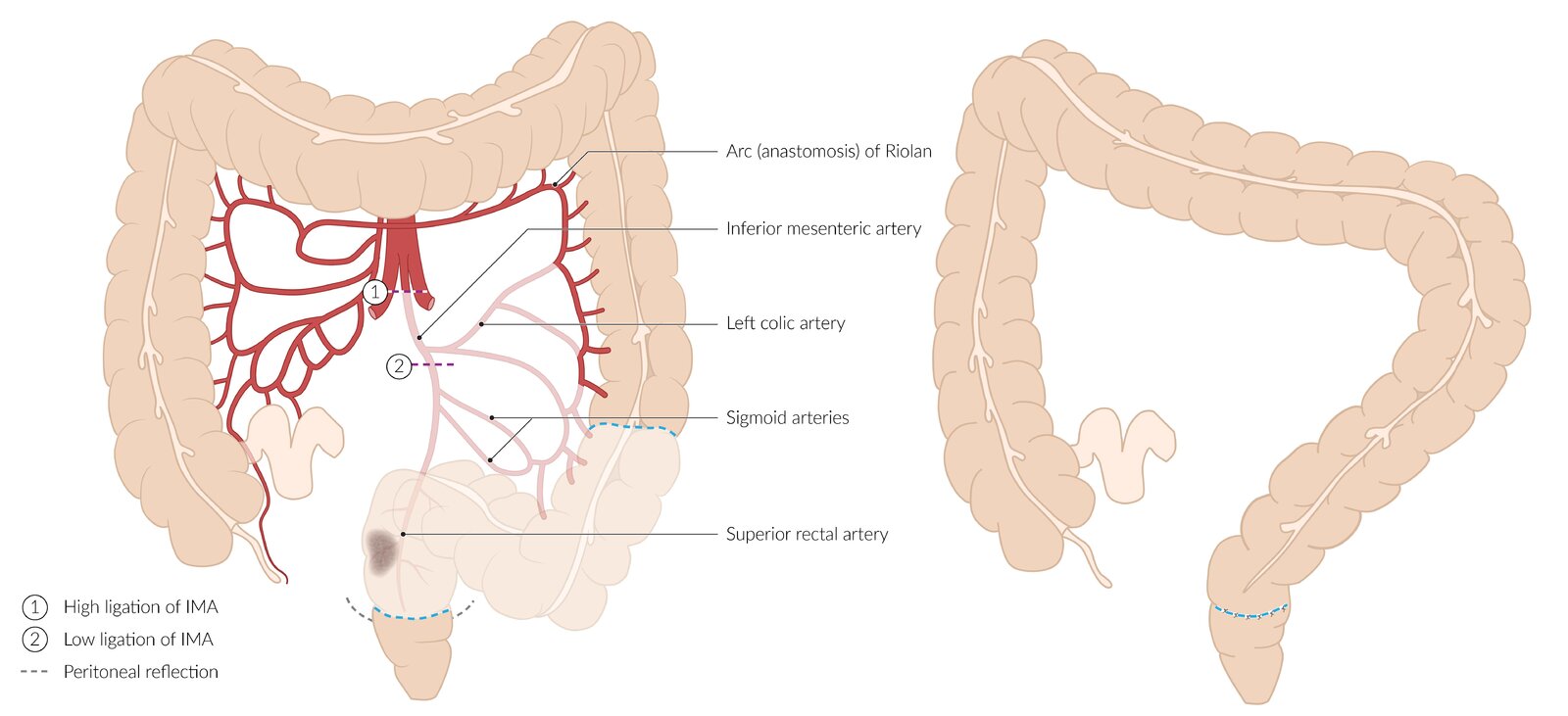
Extent of resection (left): sigmoid colon (blue dashed lines). The arterial blood supply to this section, the inferior mesenteric artery, is ligated either near its origin from the aorta (1) or distal to the origin of the left colic artery (2). Malignancy (lesion shown in gray) is a common indication for this procedure.
Reconstruction (right): typically achieved via end-to-end colorectal anastomosis
© AMBOSS
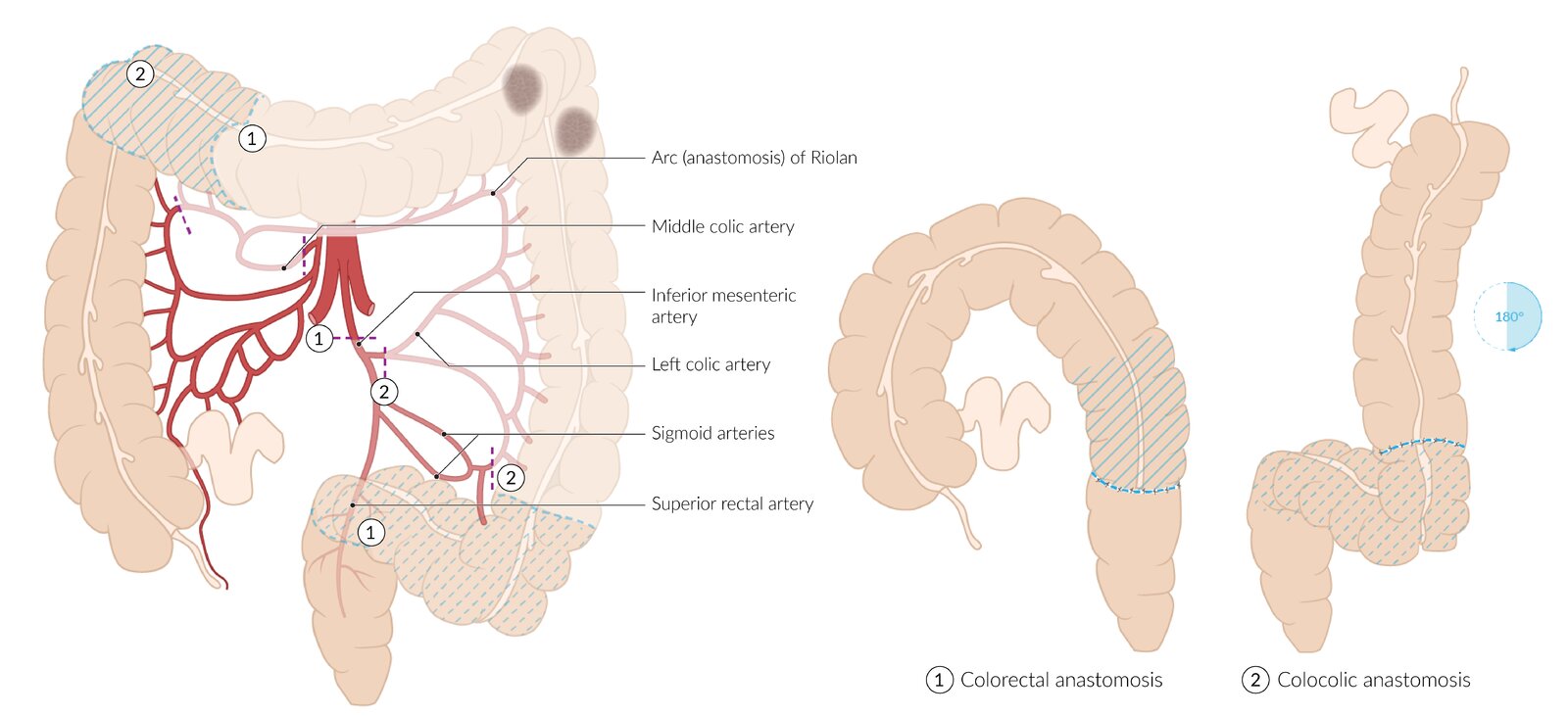
Extent of resection (left): highly variable, depending on the underlying disease (lesions, shown in gray, indicate malignancy) and blood supply. Options include:
(1) Resection from the middle third of the transverse colon to the sigmoid colon (including area indicated by blue dashed hatching), with ligation of the middle colic artery and the inferior mesenteric artery (purple dashed lines)
(2) Resection from the proximal third of the transverse colon (including area indicated by blue hatching) to the descending colon, with ligation of the middle colic artery and the left colic artery (purple dashed lines)
Reconstruction (right): typically achieved via end-to-end colorectal anastomosis (for resection 1) or colocolic anastomosis (for resection 2). Colocolic anastomosis requires 180° rotation of the ascending colon.
© AMBOSS
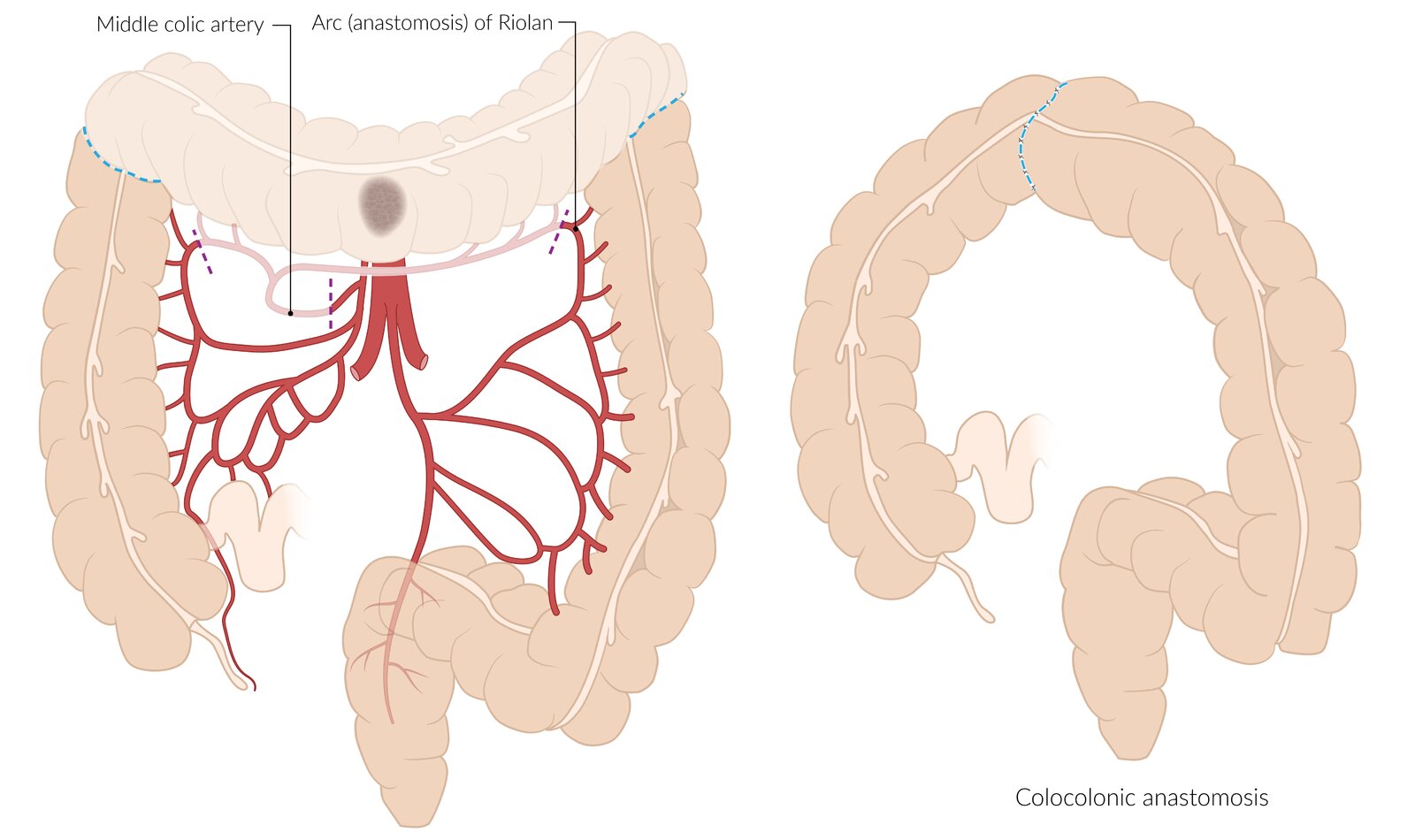
Extent of resection (left): between hepatic and splenic flexures (blue dashed lines). The arterial blood supply to this section, including the middle colic artery and its anastomotic connections with the right and left colic arteries, is ligated (purple dashed lines). Malignancy (lesion shown in gray) is a common indication for this procedure.
Reconstruction (right): typically achieved via end-to-end colocolonic anastomosis
© AMBOSS
Extent of resection (left): sigmoid colon and upper rectum (the area between blue dashed lines); the distal resection margin is above the peritoneal reflection. The arterial blood supply to this section, the inferior mesenteric artery, is ligated either near its origin from the aorta (1) or distal to the origin of the left colic artery (2). Malignancy (lesion shown in gray) is a common indication for this procedure.
Reconstruction (right): typically achieved via end-to-end colorectal anastomosis
© AMBOSS
Treatment of rectal cancer
Principles of rectal cancer treatment [9][34]
| Treatment of rectal cancer by stage | |
|---|---|
| AJCC Stage | Treatment approach |
| Stage I |
|
| Stage II |
|
| Stage III |
|
| Stage IV |
|
Surgery for rectal cancer [9]
- The extent of the resection depends on the location of the tumor and the TNM stage.
- The sphincter tone and the distance of the tumor from the anal verge (e.g., via rigid proctosigmoidoscopy) should be assessed preoperatively to plan appropriate surgical resection.
- Consider gynecology and/or urology consult if imaging shows a regional spread past the rectum.
| Typical surgeries for rectal cancer | |||
|---|---|---|---|
| Description | Indication | Tumor stage | |
| Transanal excision |
|
|
|
| Low anterior resection (LAR) |
|
|
|
| Abdominoperineal resection (APR) |
|
|
|
A complete TME is necessary to adequately assess the nodal status and prevent recurrence.


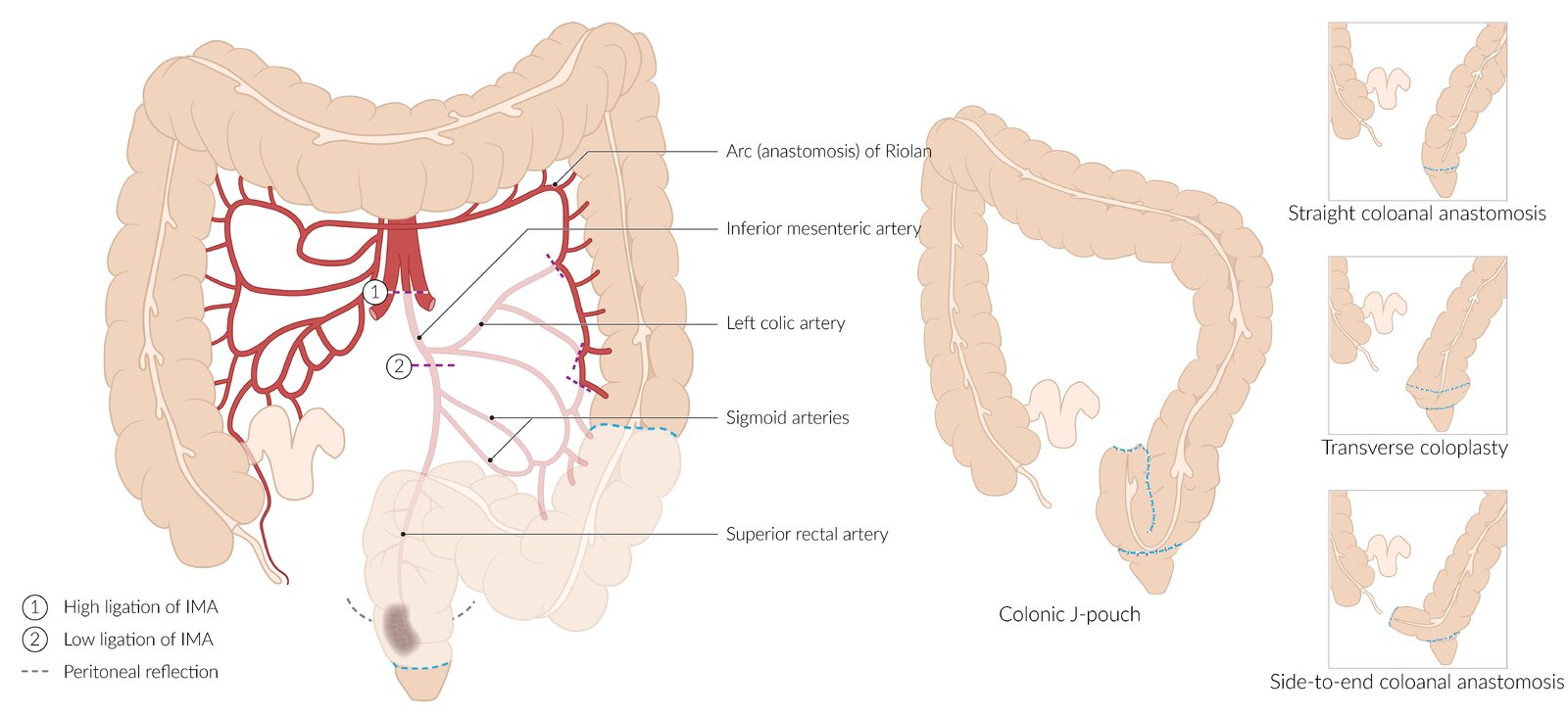
Extent of resection (left): sigmoid colon and rectum (the area between blue dashed lines); the distal resection margin is below the peritoneal reflection, but the anal sphincter is preserved. The arterial blood supply to the resected tissues, the inferior mesenteric artery, is ligated either near its origin from the aorta (1) or distal to the origin of the left colic artery (2). Malignancy (lesion shown in gray) is a common indication for this procedure.
Reconstruction (right): may be achieved via end-to-end (straight) or side-to-end coloanal anastomosis, or using a colonic J-pouch or transverse coloplasty technique
© AMBOSS
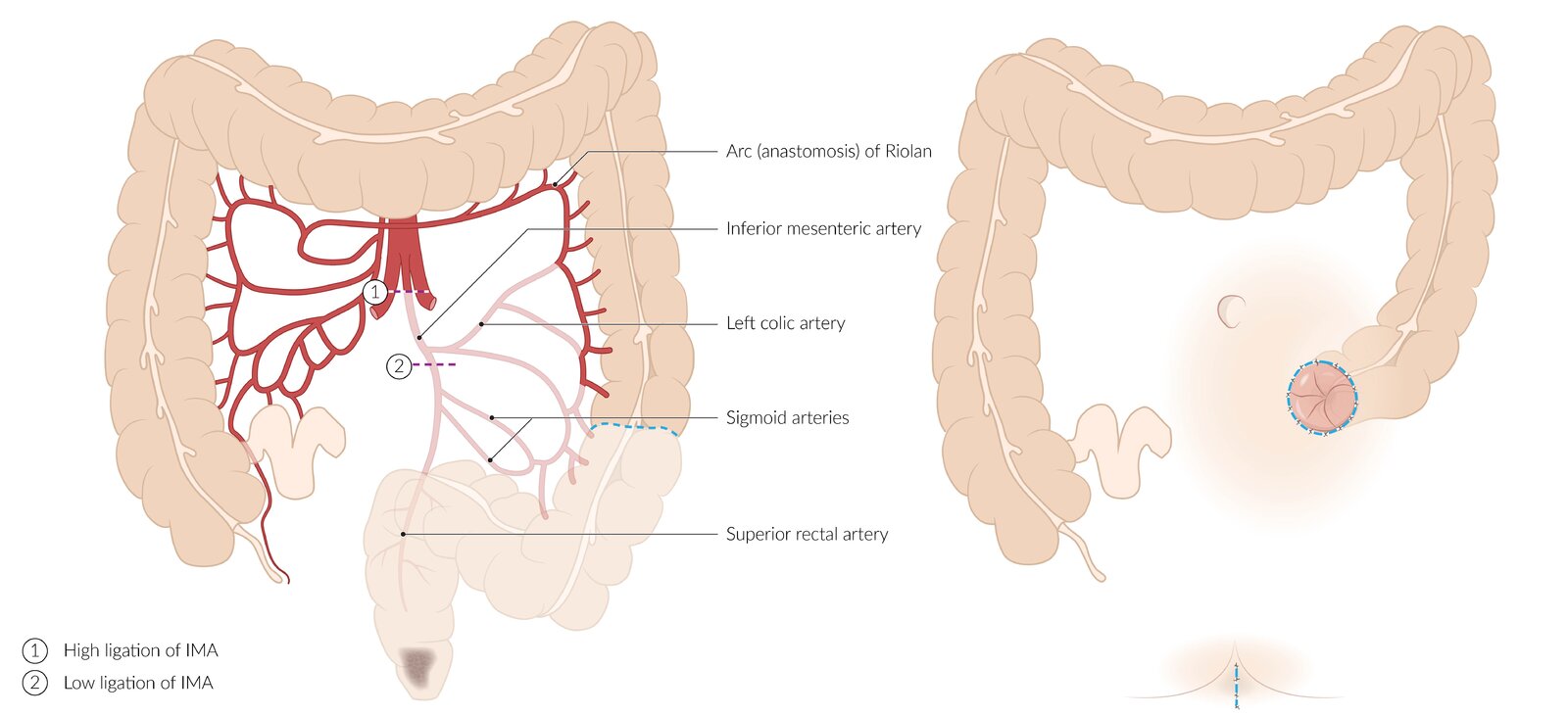
Extent of resection (left): sigmoid colon, rectum, and anus (area below the blue dashed line). The arterial blood supply to this section, the inferior mesenteric artery, is ligated either near its origin from the aorta (1) or distal to the origin of the left colic artery (2). A common indication for this procedure is malignancy close to the anal sphincter (gray lesion).
Closure (right): The perineal defect is closed (sutures indicated by blue dashed line) and an end stoma is created from the descending colon (sutures indicated by blue dashed circle).
© AMBOSS
© AMBOSS
Pathology
Gross pathology
- Right-sided colon carcinomas: mostly exophytic mass
- Left-sided colon carcinomas: mostly infiltrating mass



Histopathology
- Most common: adenocarcinoma (95%)
-
Less common
- Mucinous adenocarcinoma
- Signet ring cell carcinoma
- Small cell carcinoma
- Adenosquamous carcinoma (rare)
- Squamous cell carcinoma of the colon (rare)
95% of all colorectal cancers are adenocarcinomas.
")
")

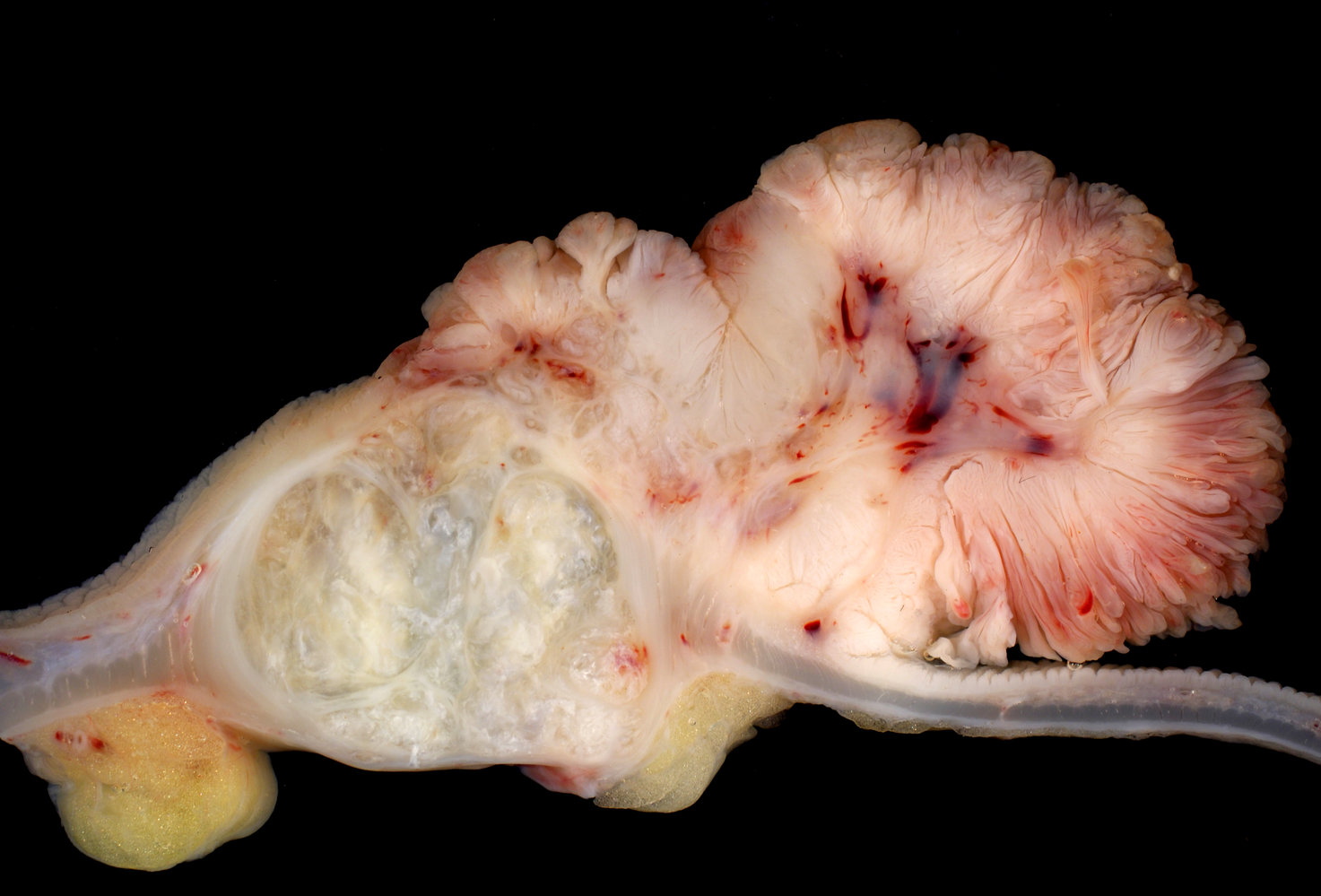
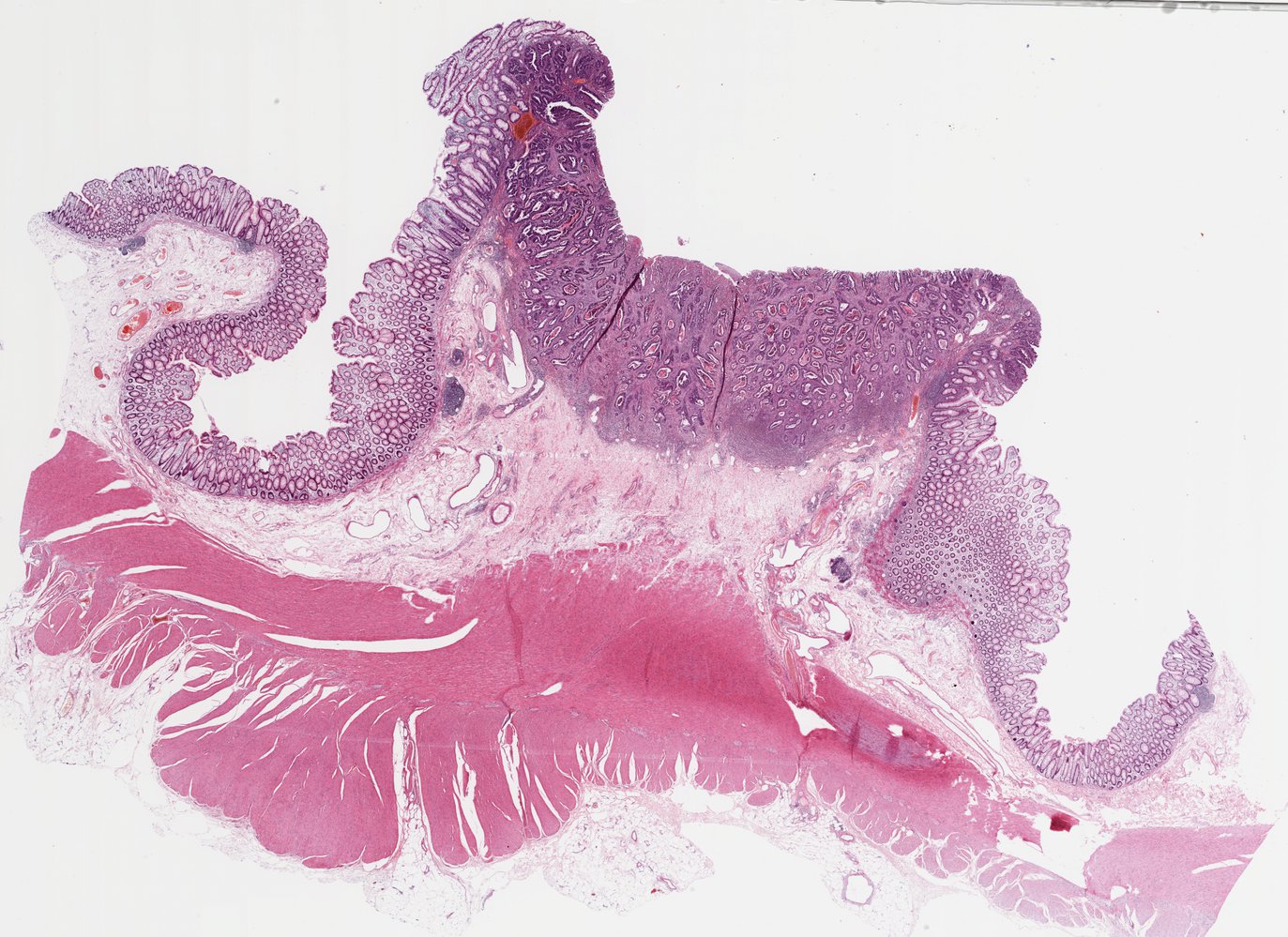
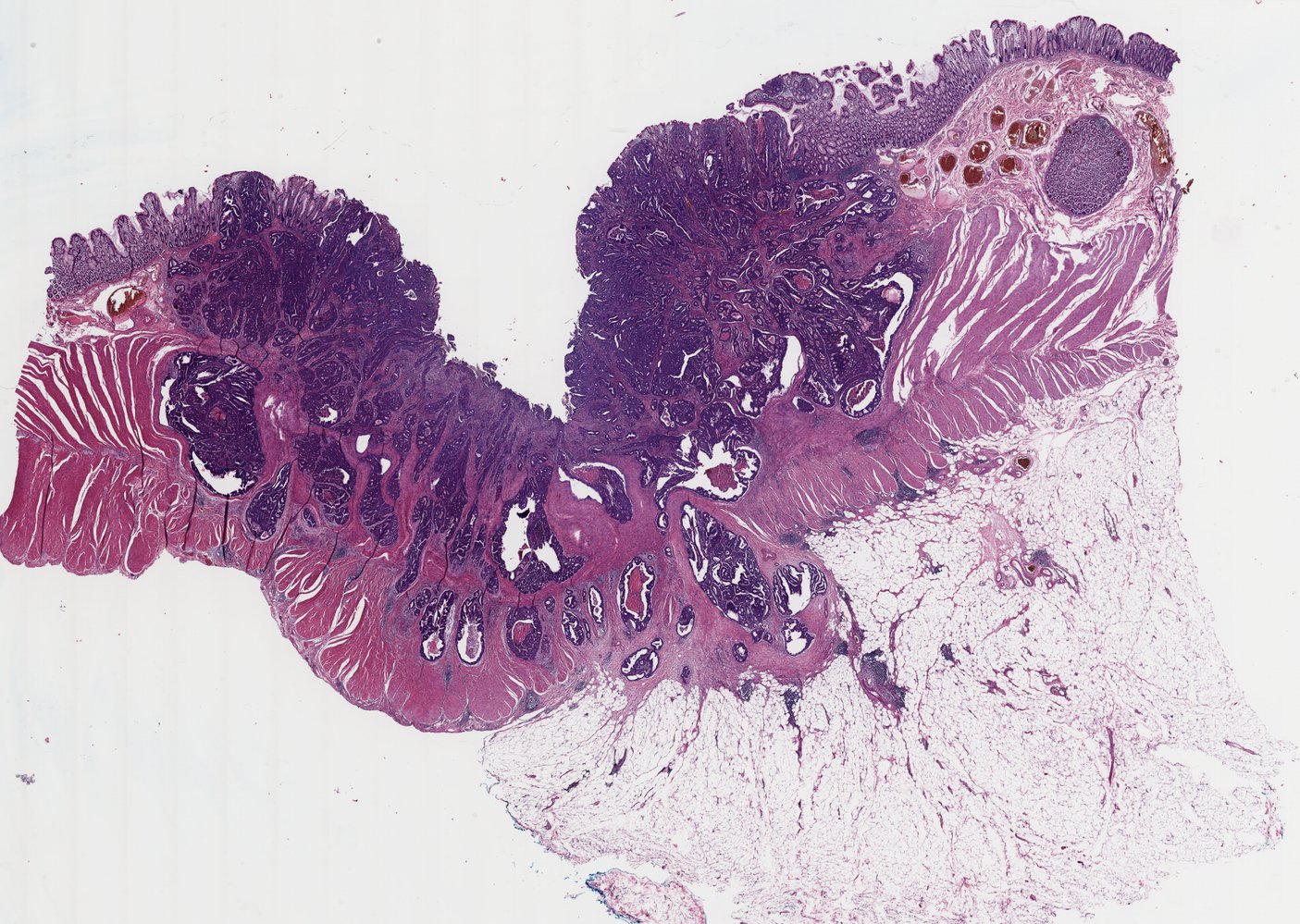
Longitudinal section of a specimen of the ascending colon
Large villous adenoma (1) transitioning into an invasive adenocarcinoma (2). The tumor has broken through the muscular layer (red overlay) of the colon and invaded the subserous layer.
Source: “Adenocarcinoma of Ascending Colon Arising in Villous Adenoma” by Ed Uthman, MD, Flickr, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).

Surgical resection specimen of a colon
A large, nodular, dark grey, tumorous mass is visible at the center of the specimen.
Source: “Large Colon Cancer Arising in Adenoma” by Ed Uthman, M.D., Flickr, licensed under CC BY 2.0.
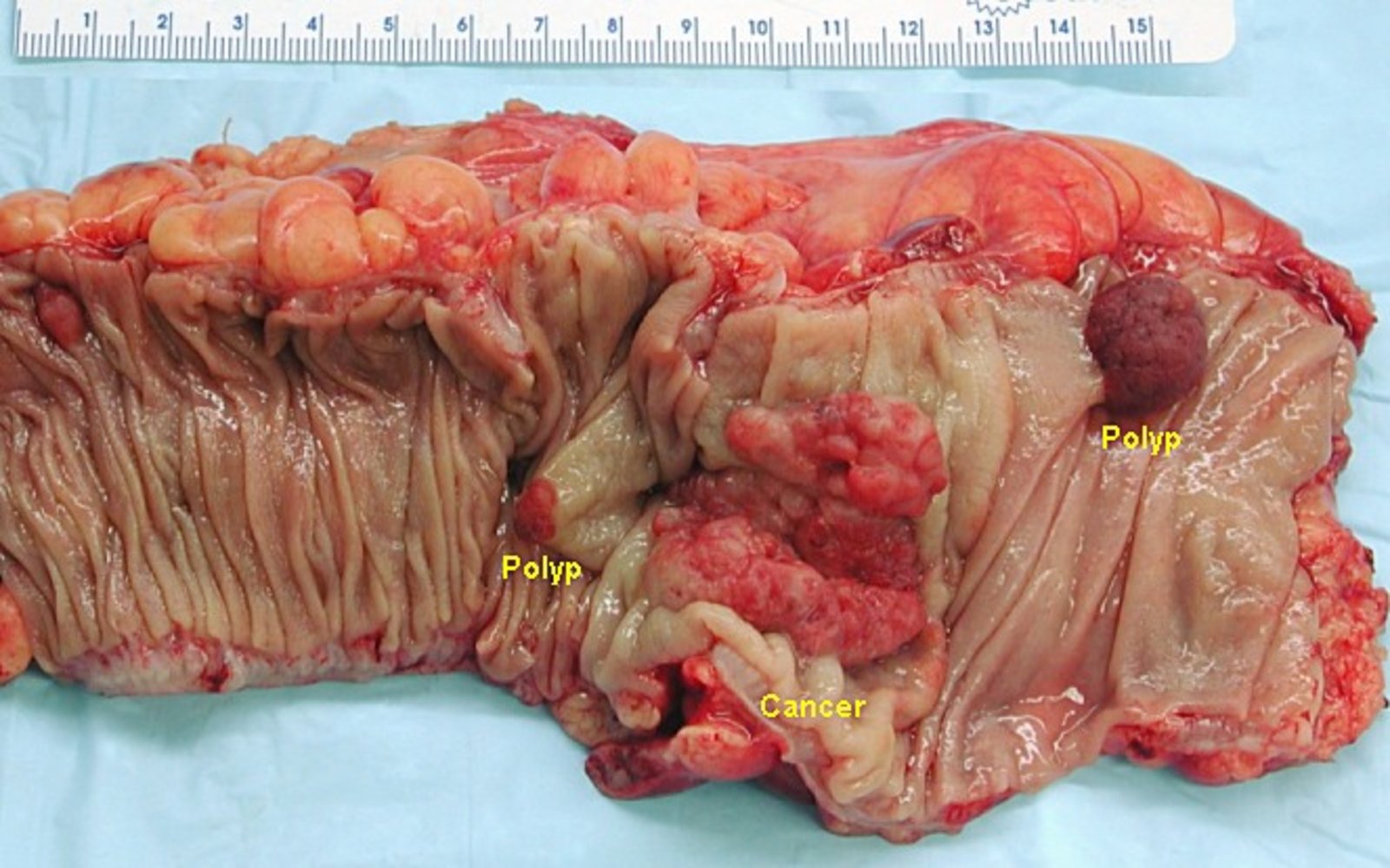
Photograph of a longitudinally opened proctocolectomy specimen
Two different pathologic alterations of the mucosa are visible: a colorectal carcinoma (purple overlay) and two adenomatous polyps (green overlays; possible preliminary stages of colon carcinomas). The mucosa on the left part of the specimen appears to be intact.
Source: “Gross appearance of an opened colectomy specimen containing an invasive colorectal carcinoma and two adenomatous polyps” by Emmanuelm, Wikimedia Commons, licensed under CC BY 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
{kind=link}

Photomicrograph of colonic tissue (H&E stain)
The hyperchromatic area on the right two-thirds of this image shows a moderately differentiated colonic adenocarcinoma. The cells lining the colonic glands appear hyperchromatic, with basally oriented nuclei with atypical features. The lumen of these glands contains necrotic debris. The colonic glands, which are typically only present in the mucosal layer, are visible in the submucosa, but not beyond (pT1). Goblet cells are absent. (They would appear as unstained cells between the lining epithelial cells.) Desmoplasia is identifiable as fibrous tissue surrounding the tumor cells.
Normal colonic mucosa is identifiable on the left third of the image as paler staining tissue. Note the abundance of goblet cells.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Photomicrograph of colonic tissue (H&E stain)
Colonic glands, which should only be present in the mucosal layer, are visible in all the layers of the colonic wall, including the outermost serosal layer (pT3). The glands are lined by tall columnar epithelial cells with basally oriented nuclei. The lumen of these glands contains necrotic debris. Goblet cells (which would appear as unstained cells between the lining of epithelial cells) are absent. The fibrous tissue surrounding the tumor cells indicates desmoplasia.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
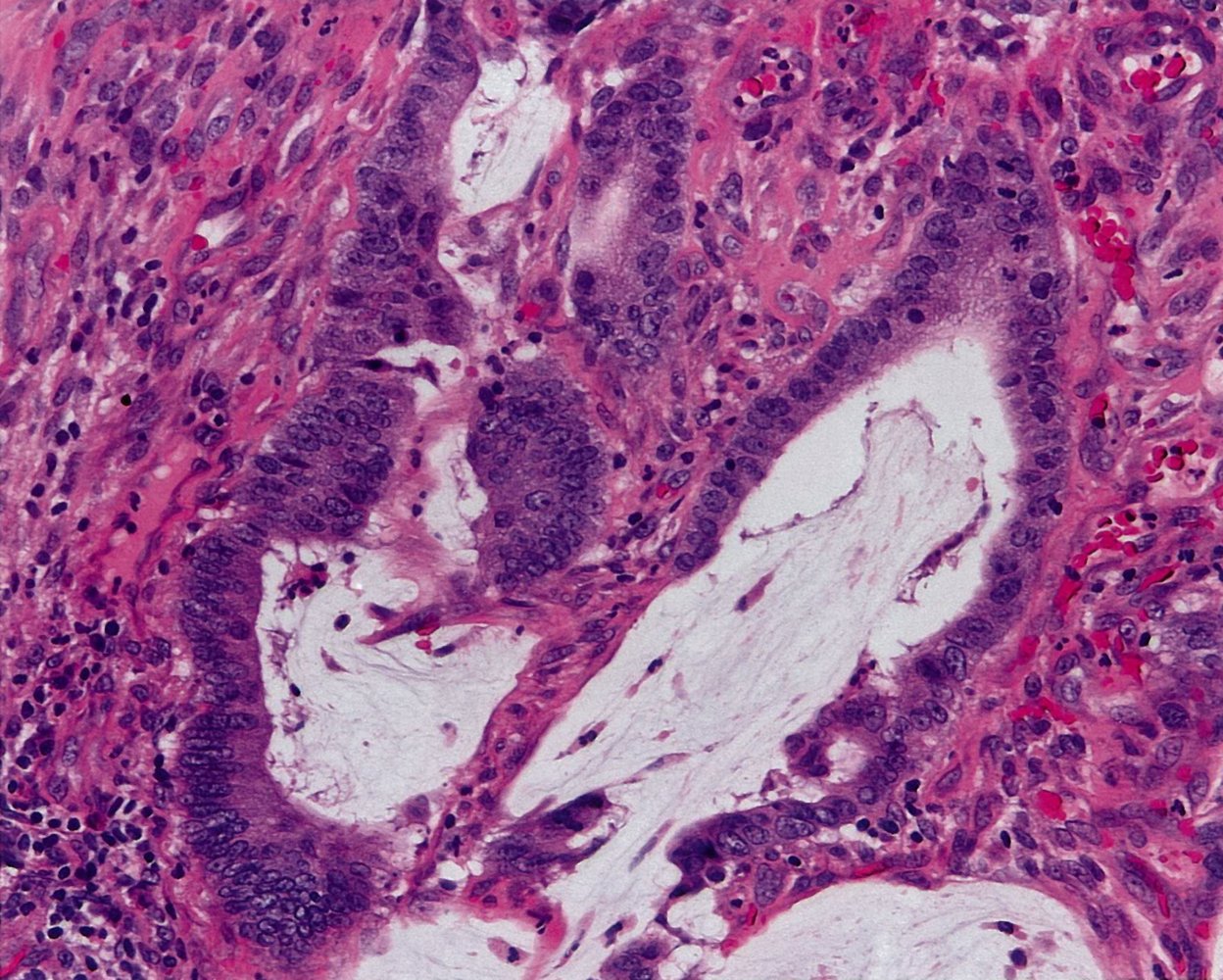
Photomicrograph of tissue biopsied from a colonic polyp (H&E stain; 400x magnification)
The hyperchromatic purple (highly basophilic) cells in the center of this image are colonic epithelial cells. They have hyperchromatic cytoplasm and large, mitotic nuclei (red overlay), which are signs of malignancy. The cells surround pools of extracellular mucin (green overlay). Inflammatory cells are visible in the stroma surrounding the glands.
Mucinous pools that make up at least 50% of the tumor mass are characteristic of mucinous adenocarcinoma.
Source: © IMPP
Complications
Peritoneal carcinomatosis [43][44]
- Definition: a terminal feature of abdominal cancers (most commonly of the ovary, appendix, or colon) characterized by seeding of the tumor to the peritoneum
- Epidemiology: : depends on underlying malignancy; peritoneal carcinomatosis develops in ∼ 10% of individuals with colorectal cancer [45]
- Etiology: primary tumor metastasizes to the peritoneal surface
-
Clinical features
- Ascites
- Fistulas
- Fatigue
- Abdominal pain, nausea, cachexia
- Diagnostics: CT is preferred; typically shows metastatic studding (tumor nodules studding the surface of the peritoneum) and omental caking
-
Treatment
- Operable disease: involves cytoreductive surgery followed by hyperthermic intraperitoneal chemotherapy (HIPEC), systemic chemotherapy, targeted therapy, and/or immune checkpoint inhibitors
- Inoperable disease: experimental pressurized intraperitoneal aerosolized chemotherapy or repeated intraperitoneal chemotherapy infusion
- Complications: bowel, biliary, and/or ureteral obstruction
- Prognosis: : poor; 5-year survival rates after cytoreductive surgery and HIPEC are approx. 40%
We list the most important complications. The selection is not exhaustive.
Follow-up
All patients with CRC should be followed up closely after curative treatment to ensure early identification and management of recurrence. These recommendations are consistent with the American Society of Colon and Rectal Surgeons' 2015 guidelines. [46][47][48]
-
Patient history, physical examination, CEA level
- Every 3–6 months for 2 years
- Every 6 months for an additional 3 years
- CT chest/abdomen/pelvis: annually for 5 years
-
Colonoscopy
- 1 year after preoperative colonoscopy
- Every 3–5 years in the further follow-up, depending on findings
-
Proctoscopy/sigmoidoscopy
- Recommended additional follow-up modality after the treatment of rectal cancer
- Every 6–12 months for 3–5 years
- May be supplemented with endorectal ultrasound
- Recommended duration of close follow-up: 5 years following the completion of curative treatment
90% of recurrences occur within the first five years following treatment. [48]
Prognosis
-
Five-year survival rate [2]
- Localized disease: 90%
- Regional spread: 72%
- Distant metastases: 14%
- All stages combined: 65%
Screening
Screening modalities and screening intervals depend on individual risk factors and differ for individuals at average risk and those at high risk of CRC.
Individuals at average risk (general population) [49][50][51]
-
Criteria for average risk of CRC include:
- No history of CRC, IBD, or adenomatous polyps
- No family history of hereditary colon cancer syndromes (e.g., HNPCC, familial adenomatous polyposis)
-
Recommended screening age
- All individuals ≥ 45 years of age [49][51]
- The decision to continue screening in patients aged 75–85 years should be made on a case-by-case basis. [49]
-
Screening modalities: Consider individual risk factors and patient preference when choosing a screening method.
- Direct visualization
- Gold standard: Complete colonoscopy every 10 years if no polyps or carcinomas are detected
- Alternatives
- CT colonography or capsule endoscopy every 5 years [50]
- Flexible sigmoidoscopy every 5–10 years
- Stool-based testing
-
Annual fecal immunochemical testing (FIT)
- Uses antibodies to detect occult GI bleeding
- Has a higher sensitivity for CRC than FOBT
- All positive stool-based test results need to be confirmed using colonoscopy.
-
Annual fecal occult blood test (FOBT)
- Used to detect the presence of blood in feces that is not visibly apparent.
- Used as a screening tool for colorectal carcinoma, but upper gastrointestinal bleeding (e.g., from a peptic ulcer) can also yield positive results
- A positive result merits additional follow-up (e.g., upper endoscopy, colonoscopy)
- Has poor sensitivity for detecting polyps
-
Multitargeted stool DNA test every 3 years
- A stool-based assay that detects certain mutations typical for early colorectal carcinoma, such as mutations of the KRAS gene.
- Used as a screening tool for colorectal carcinoma
- Positive tests are followed up with colonoscopy
-
Annual fecal immunochemical testing (FIT)
- Direct visualization
Individuals at high risk [21][50]
| Colorectal cancer screening for high-risk individuals | ||
|---|---|---|
| High-risk characteristics | Screening recommendations | |
| History of adenomatous polyps |
|
|
| History of CRC |
|
|
| Positive family history (Also consider genetic testing in patients with multiple affected family members or relatives affected at a young age) | ≥ 2 first-degree relatives with CRC diagnosed at any age |
|
| ≥ 1 first-degree relative with CRC or advanced adenoma diagnosed at < 60 years of age | ||
| ≥ 1 first-degree relative with CRC or advanced adenoma diagnosed at ≥ 60 years of age |
|
|
| One second-degree relative with CRC or advanced adenoma |
|
|
| Other high-risk conditions | Hereditary syndromes associated with increased risk of CRC (e.g., FAP, HNPCC) |
|
| Inflammatory bowel disease | ||
Primary prevention
- Control modifiable risk factors for CRC. [52][53][54]
- Increase physical activity.
- Optimize nutrition.
- Decrease or stop alcohol consumption and smoking.
- Optimize treatment of conditions that increase the risk of CRC (e.g., IBD, HTN, diabetes, hyperlipidemia). [52]
- Long-term aspirin therapy may reduce the incidence of CRC. [50][55]
-
Low-dose aspirin may be considered based on shared decision making if all of the following parameters are met:
- Age 50–69 years with life expectancy > 10 years
- No comorbidity or use of other pharmacotherapy that increases the risk for bleeding
- Risk of cardiovascular disease ≥ 10% for the next 10 years (see “ASCVD risk assessment” and “10-year ASCVD risk categories” for details)
- High likelihood of adherence to aspirin therapy for at least 10 years
- Important considerations
- Aspirin therapy does not replace screening for CRC or alter screening intervals.
- It is unclear if aspirin therapy provides additional benefits over CRC screening or if its benefits outweigh the risks.
-
Low-dose aspirin may be considered based on shared decision making if all of the following parameters are met:
Related One-Minute Telegram
- One-Minute Telegram 144-2026-1/3: Is meat-free risk-free? A pooled cohort view of diet and cancer
- One-Minute Telegram 130-2025-2/3: A FIT-ting option for colorectal cancer screening?
- One-Minute Telegram 125-2025-1/3: Exercise your right to better colon cancer outcomes
- One-Minute Telegram 68-2023-3/3: They tested their poo, but didn’t follow through
- One-Minute Telegram 65-2022-1/3: 2022 U.S. Preventive Services Task Force: summary of recommendations
- One-Minute Telegram 62-2022-3/3: Colonoscopy for colorectal cancer screening saves lives, but only if you get one
- One-Minute Telegram 50-2022-1/3: The aspirin debate rages on: 2022 USPSTF updated recommendations
- One-Minute Telegram 41-2021-2/2: 2021 U.S. Preventive Services Task Force: Summary of recommendations
Interested in the newest medical research, distilled down to just one minute? Sign up for the One-Minute Telegram in “Tips and links” below.
External Resources
- Sign up for the One-Minute Telegram
- US Preventive Services Task Force Recommendations (Colorectal Cancer)
- 2022 US Multi-Society Task Force on Colorectal Cancer: Updates on Age to Start and Stop Colorectal Cancer Screening
- 2021 ACG Clinical Guidelines: Colorectal Cancer Screening
- 2020 ASCRS Clinical Practice Guidelines for the Management of Rectal Cancer
- 2017 US Multi-Society Task Force on Colorectal Cancer: Colorectal Cancer Screening Recommendations
- 2017 ASCRS Clinical Practice Guidelines for the Treatment of Colon Cancer
- 2015 ASCRS Practice Guideline for the Surveillance of Patients After Curative Treatment of Colon and Rectal Cancer
References
- "Key Statistics for Colorectal Cancer". https://www.cancer.org/cancer/colon-rectal-cancer/about/key-statistics.html. [2017-01-05]
- "Cancer Stat Facts: Colorectal Cancer". https://seer.cancer.gov/statfacts/html/colorect.html
- "Colorectal Cancer Risk Factors". https://www.cancer.org/cancer/colon-rectal-cancer/causes-risks-prevention/risk-factors.html
- Haggar FA, Boushey RP. "Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors.". Clinics in colon and rectal surgery. 22(4). :191-7. (2009)
- Xie J, Itzkowitz SH. "Cancer in inflammatory bowel disease". World journal of gastroenterology. 14(3). :378-89. (2008)
- Abdulamir AS, Hafidh RR, Abu bakar F. "The association of Streptococcus bovis/gallolyticus with colorectal tumors: the nature and the underlying mechanisms of its etiological role". J Exp Clin Cancer Res. 30(1). :11. (2011)
- "Colorectal Cancer Signs and Symptoms". https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-staging/signs-and-symptoms.html. [2020-06-29]
- Phipps AI, Lindor NM, Jenkins MA, et al. "Colon and Rectal Cancer Survival by Tumor Location and Microsatellite Instability". Diseases of the Colon & Rectum. 56(8). :937-944. (2013)
- You YN, Hardiman KM, Bafford A, et al. "The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Rectal Cancer". Dis Colon Rectum. 63(9). :1191-1222. (2020)
- Moghadamyeghaneh Z, Alizadeh RF, Phelan M, et al. "Trends in colorectal cancer admissions and stage at presentation: impact of screening". Surg Endosc. 30(8). :3604-3610. (2015)
- Nichols SD, Albert S, Shirley L, et al. "Outcomes in patients with obstructive jaundice from metastatic colorectal cancer and implications for management.". J Gastrointest Surg. 18(12). :2186-91. (2014)
- Suliman MS, Singh M, Ajmeri AN, Stuart DL, Teka ST. "Virchow's node: a case report of an extremely rare presentation of metastasis of adenocarcinoma with mucinous features from the colon.". International journal of general medicine. 12. :137-140. (2019)
- Pasha SF, Shergill A, Acosta RD, et al. "Guideline: The role of endoscopy in the patient with lower GI bleeding". Gastrointest Endosc. 79(6). :875-885. (2014)
- Adelstein B-A, Macaskill P, Chan SF, Katelaris PH, Irwig L. "Most bowel cancer symptoms do not indicate colorectal cancer and polyps: a systematic review". BMC Gastroenterol. 11(1). (2011)
- Astin M, Griffin T, Neal RD, Rose P, Hamilton W. "The diagnostic value of symptoms for colorectal cancer in primary care: a systematic review". B J Gen Pract. 61(586). :e231-e243. (2011)
- Weiser MR. "AJCC 8th Edition: Colorectal Cancer". Ann Surg Oncol. 25(6). :1454-1455. (2018)
- Tong G-J, Zhang G-Y, Liu J, et al. "Comparison of the eighth version of the American Joint Committee on Cancer manual to the seventh version for colorectal cancer: A retrospective review of our data". World J Clin Oncol. 9(7). :148-161. (2018)
- Vogel JD, Eskicioglu C, Weiser MR, Feingold DL, Steele SR. "The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Colon Cancer". Dis Colon Rectum. 60(10). :999-1017. (2017)
- Lin JS, Piper MA, Perdue LA, et al. "Screening for Colorectal Cancer". JAMA. 315(23). :2576. (2016)
- Saito S, Tajiri H, Ikegami M. "Endoscopic features of submucosal deeply invasive colorectal cancer with NBI characteristics". Clin J Gastroenterol. 8(6). :353-359. (2015)
- Horvat N, Raj A, Ward JM, et al. "Clinical Value of CT Colonography Versus Preoperative Colonoscopy in the Surgical Management of Occlusive Colorectal Cancer". American Journal of Roentgenology. 210(2). :333-340. (2018)
- Thiels CA, Naik ND, Bergquist JR, et al. "Survival following synchronous colon cancer resection". J Surg Oncol. 114(1). :80-85. (2016)
- Rex DK, Boland CR, Dominitz JA, et al. "Colorectal cancer screening: Recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer". Gastrointest Endosc. 86(1). :18-33. (2017)
- Alzaraa A, Krzysztof K, Uwechue R, Tee M, Selvasekar C. "Apple-core lesion of the colon: a case report". Cases J. 2(1). :7275. (2009)
- Neri E, Faggioni L, Cerri F, et al. "CT colonography versus double-contrast barium enema for screening of colorectal cancer: comparison of radiation burden". Abdom Imaging. 35(5). :596-601. (2010)
- Fowler KJ, Kaur H, Cash BD, et al. "ACR Appropriateness Criteria ® Pretreatment Staging of Colorectal Cancer". J Am Coll Radiol. 14(5). :S234-S244. (2017)
- Sahani DV, Kalva SP. "Imaging the Liver". Oncologist. 9(4). :385-397. (2004)
- Jacobson R, Sherman SK, Dadaleh F, Turaga KK. "Peritoneal Metastases in Colorectal Cancer". Ann Surg Oncol. 25(8). :2145-2151. (2018)
- McMullen JRW, Selleck M, Wall NR, Senthil M. "Peritoneal carcinomatosis: limits of diagnosis and the case for liquid biopsy". Oncotarget. 8(26). :43481-43490. (2017)
- Seo JB, Im J-G, Goo JM, Chung MJ, Kim M-Y. "Atypical Pulmonary Metastases: Spectrum of Radiologic Findings". Radiographics. 21(2). :403-417. (2001)
- O'Leary MP, Parrish AB, Tom CM, MacLaughlin BW, Petrie BA. "Staging Rectal Cancer: The Utility of Chest Radiograph and Chest Computed Tomography". Am Surg. 82(10). :1005-1008. (2016)
- Duffy MJ. "Carcinoembryonic Antigen as a Marker for Colorectal Cancer: Is It Clinically Useful?". Clin Chem. 47(4). :624-630. (2001)
- "Cancer Stat Facts: Small Intestine Cancer". https://seer.cancer.gov/statfacts/html/smint.html
- Benson AB, Venook AP, Al-Hawary MM, et al. "NCCN Guidelines Insights: Rectal Cancer, Version 6 2020". J Natl Compr Canc Netw. 18(7). :806-815. (2020)
- Benson AB, Venook AP, Al-Hawary MM, et al. "NCCN Guidelines Insights: Colon Cancer, Version 2.2018". J Natl Compr Canc Netw. 16(4). :359-369. (2018)
- Lutz S, Balboni T, Jones J, et al. "Palliative radiation therapy for bone metastases: Update of an ASTRO Evidence-Based Guideline". Practical Radiation Oncology. 7(1). :4-12. (2016)
- Pease NJ, Edwards A, Moss LJ. "Effectiveness of whole brain radiotherapy in the treatment of brain metastases: a systematic review". Palliative Medicine. 19(4). :288-299. (2005)
- Bokey EL, Chapuis PH, Dent OF, et al. "Surgical Technique and Survival in Patients Having a Curative Resection for Colon Cancer". Dis Colon Rectum. 46(7). :860-866. (2003)
- Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL. "Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice". Elsevier. (2016). ISBN: 9780323299879
- Goulder F. "Bowel anastomoses: The theory, the practice and the evidence base". World Journal of Gastrointestinal Surgery. 4(9). :208. (2012)
- Feig BW, Ching DC. "The M.D. Anderson Surgical Oncology Handbook". Lippincott Williams & Wilkins. (2012). ISBN: 9781451154092
- Leijssen LGJ, Dinaux AM, Amri R, et al. "A Transverse Colectomy is as Safe as an Extended Right or Left Colectomy for Mid-Transverse Colon Cancer". World J Surg. 42(10). :3381-3389. (2018)
- Kranenburg O, Speeten K van der, Hingh I de. "Peritoneal Metastases From Colorectal Cancer: Defining and Addressing the Challenges". Frontiers in Oncology. 11. (2021)
- Levy AD, Shaw JC, Sobin LH. "Secondary Tumors and Tumorlike Lesions of the Peritoneal Cavity: Imaging Features with Pathologic Correlation". RadioGraphics. 29(2). :347-373. (2009)
- Segelman J, Granath F, Holm T, et al. "Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer". Br J Surg. 99(5). :699-705. (2012)
- Steele SR, Chang GJ, Hendren S, et al. "Practice Guideline for the Surveillance of Patients After Curative Treatment of Colon and Rectal Cancer". Dis Colon Rectum. 58(8). :713-725. (2015)
- Costas-Chavarri A, Nandakumar G, Temin S, et al. "Treatment of Patients With Early-Stage Colorectal Cancer: ASCO Resource-Stratified Guideline". J Glob Oncol. :1-19. (2019)
- Kahi CJ, Boland CR, Dominitz JA, et al. "Colonoscopy Surveillance After Colorectal Cancer Resection: Recommendations of the US Multi-Society Task Force on Colorectal Cancer". Gastroenterology. 150(3). :758-768.e11. (2016)
- Patel SG, May FP, Anderson JC, et al. "Updates on Age to Start and Stop Colorectal Cancer Screening: Recommendations From the U.S. Multi-Society Task Force on Colorectal Cancer". Am J Gastroenterol. 117(1). :57-69. (2021)
- Shaukat A, Kahi CJ, Burke CA, et al. "ACG Clinical Guidelines: Colorectal Cancer Screening 2021". Am J Gastroenterol. 116(3). :458-479. (2021)
- Davidson KW, Barry MJ, et al. "Screening for Colorectal Cancer". JAMA. 325(19). :1965. (2021)
- Bibbins-Domingo K. "Aspirin Use for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: U.S. Preventive Services Task Force Recommendation Statement". Ann Intern Med. 164(12). :836. (2016)
- Thanikachalam K, Khan G. "Colorectal Cancer and Nutrition". Nutrients. 11(1). :164. (2019)
- Chan AT, Giovannucci EL. "Primary Prevention of Colorectal Cancer". Gastroenterology. 138(6). :2029-2043.e10. (2010)
- Guirguis-Blake JM, Evans CV, Perdue LA, Bean SI, Senger CA. "Aspirin Use to Prevent Cardiovascular Disease and Colorectal Cancer". JAMA. 327(16). :1585. (2022)