Summary
Congenital infections are caused by pathogens transmitted from mother to child during pregnancy (transplacentally) or delivery (peripartum). They can have a substantial negative impact on fetal and neonatal health. The acronym TORCH stands for the causative pathogens of congenital infections: Toxoplasma gondii, others (including Treponema pallidum, Listeria, varicella zoster virus, and parvovirus B19), rubella virus, cytomegalovirus (CMV), and herpes simplex virus (HSV). TORCH infections can cause spontaneous abortion, premature birth, and intrauterine growth restriction (IUGR). These infections can also cause abnormalities in the CNS, the skeletal and endocrine systems, and the complex organs (e.g., cardiac defects, vision and hearing loss). Prophylaxis is of great importance during pregnancy. Primary prevention includes vaccination for varicella and rubella (prior to pregnancy), hygiene measures (washing hands and avoiding certain foods), and screening for syphilis during pregnancy. Affected infants require regular follow-ups to monitor for hearing loss, ophthalmological abnormalities, and developmental delays.
Several other pathogens can also be vertically transmitted during pregnancy and have detrimental effects on the fetus and/or newborn. These include HIV in pregnancy, perinatal hepatitis B, group B streptococci, E. coli, gonococcal infections and chlamydial infections, West Nile virus, Zika virus, measles virus, enterovirus, and adenovirus. The pathogens are discussed in more detail in their respective articles.
Overview
Description
Congenital TORCH infections are vertically transmitted infections (acquired directly from the mother and transmitted to the embryo, fetus, or newborn through the placenta or birth canal) that are capable of significantly influencing fetal and neonatal morbidity and mortality
- Toxoplasmosis
- Others (e.g., syphilis, varicella, parvovirus B19 infection, listeriosis)
- Rubella
- Cytomegaly (CMV)
- Herpes simplex virus (HSV) infection
Common findings in TORCH infections
- During pregnancy: may cause intrauterine fetal demise and miscarriage
- In neonates
- Hepatosplenomegaly
- Jaundice
- Lethargy
- Growth retardation
- Thrombocytopenia
| Overview of congenital TORCH infections | ||||
|---|---|---|---|---|
| Infection | Clinical features | Diagnosis | Treatment | Prevention |
| Toxoplasmosis |
|
|
|
|
| Syphilis |
|
|
|
|
| Listeriosis |
|
|
|
|
| Varicella zoster virus (VZV) |
|
|
|
|
| Parvovirus B19 |
|
|
|
|
| Rubella |
|
|
|
|
| Cytomegalovirus (CMV) |
|
|
|
|
| Herpes simplex virus (HSV) |
|
|
|
|
Transplacental transmission occurs following primary infection of a seronegative mother during pregnancy. Maternal IgM antibodies, which are unable to cross the placenta, form first. Protective IgG antibodies, which are able to cross the placenta, have not yet been formed, so the infant is not protected from infection via the placenta.
In general, the earlier in pregnancy a TORCH infection occurs, the more severe the complications.
Attenuated live vaccines (measles, mumps, rubella, and varicella) are contraindicated in pregnancy. Conception should be avoided for 1 month after immunization with live vaccines.
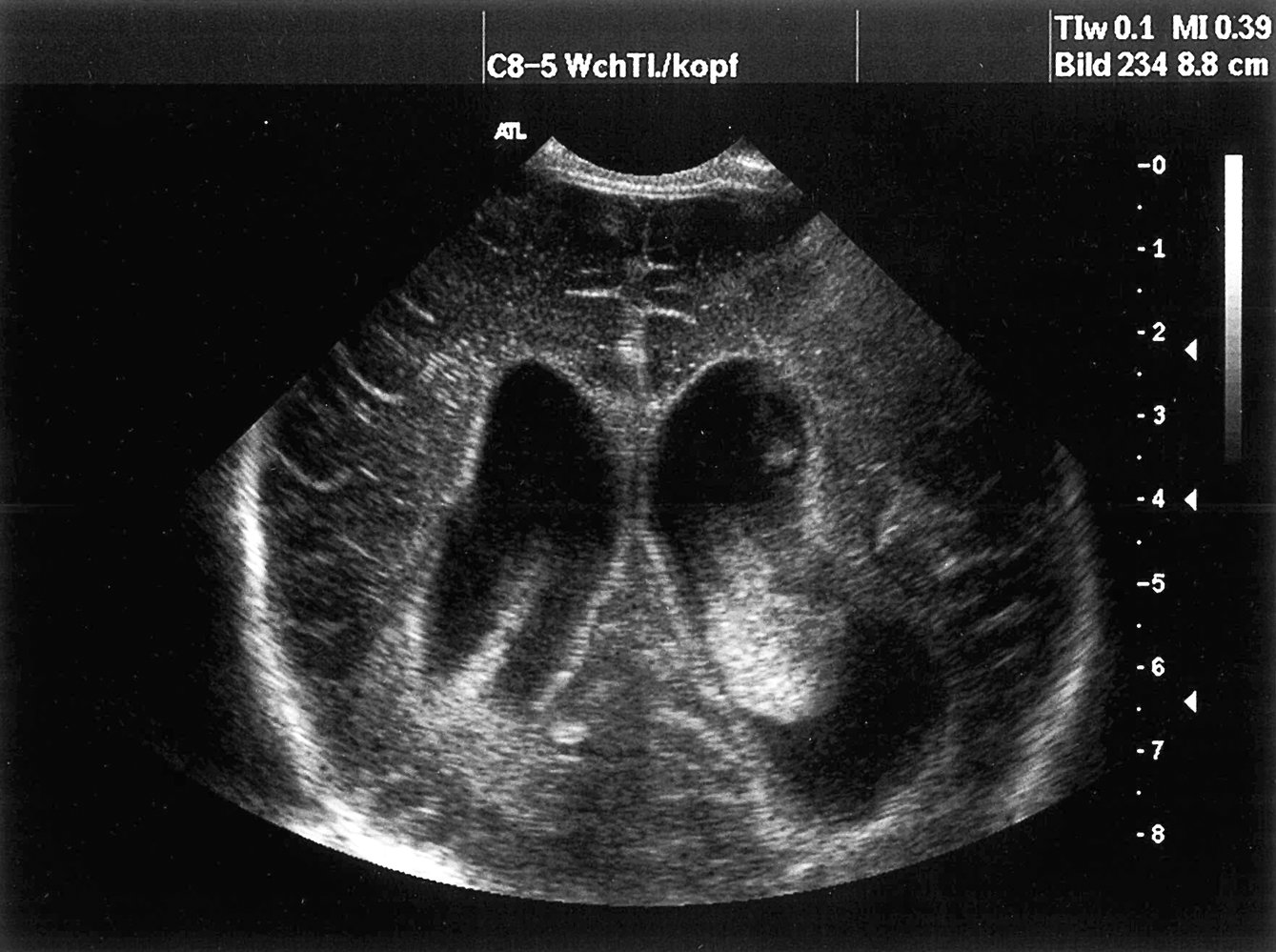
Ultrasound of the CNS, coronal section: dilated lateral ventricles with hyperechoic deposits that are compatible with intraventricular hemorrhage (green areas). (Arrow = periventricular calcification)
Source: © IMPP
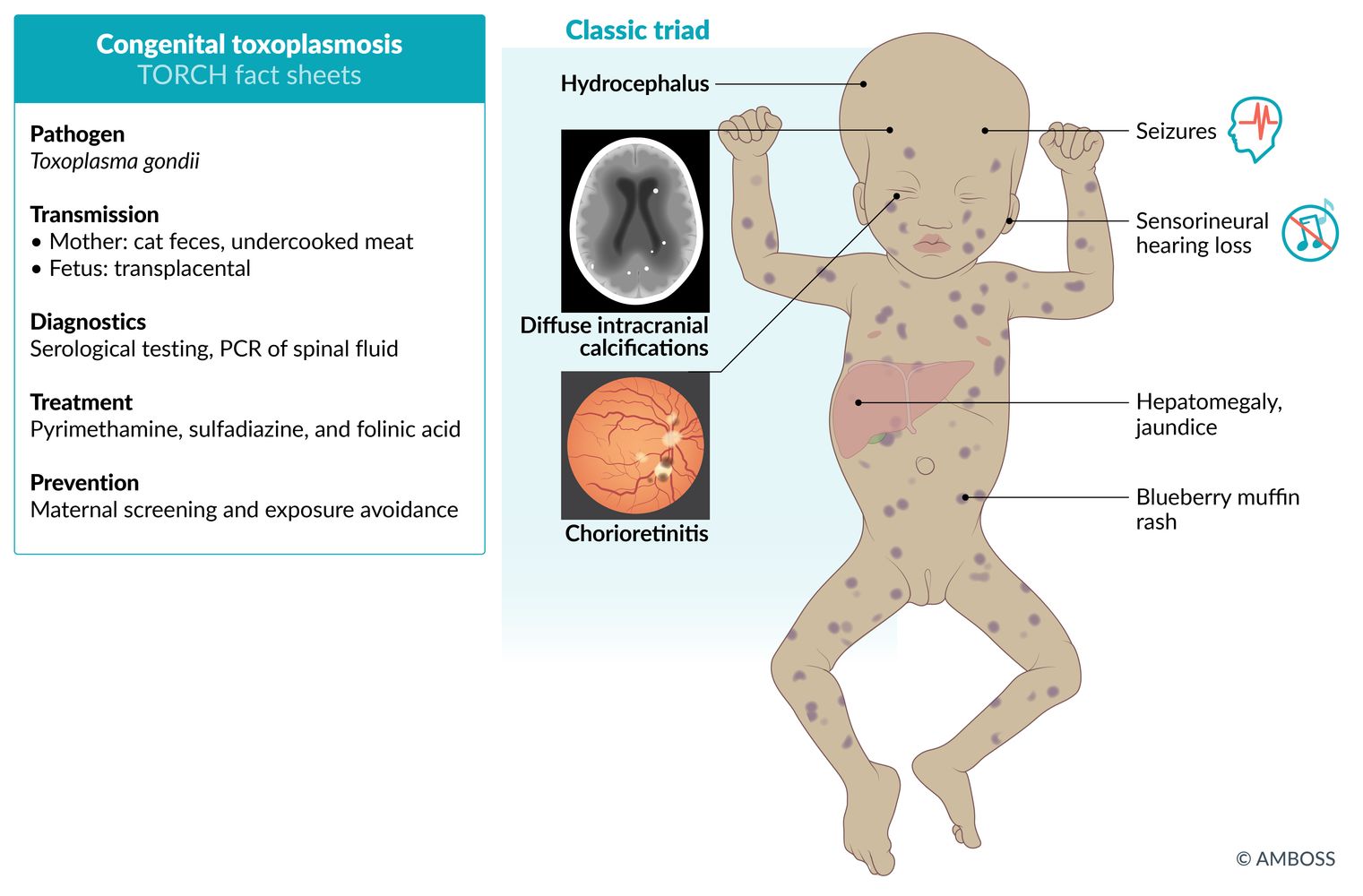
Congenital toxoplasmosis
Epidemiology
∼ 0.5–1:10,000 live births per year in the US [2]
Pathogen
Toxoplasma gondii

Transmission
-
Mother
- Cat feces
- Raw or insufficiently cooked meat
- Unpasteurized milk (especially goat milk)
- See “Etiology” in “Toxoplasmosis.”
-
Fetus
-
Transplacental transmission
- First trimester: ∼ 15%
- Third trimester: ∼ 70%
-
Transplacental transmission
Clinical features [3]
-
First trimester
- Increased risk of premature birth and spontaneous abortion
-
Classic triad of toxoplasmosis
- Chorioretinitis (a form of posterior uveitis)
- Diffuse intracranial calcifications
- Hydrocephalus
- Possible other nonspecific clinical features
- Petechiae and purpura (blueberry muffin rash)
- Fever
- Jaundice
- Hepatosplenomegaly
- Lymphadenopathy
- Pneumonitis
- Seizures
- Macrocephaly or microcephaly [4]
- Thrombocytopenia
- Second or third trimester: subclinical or mild toxoplasmosis
-
Sequelae of congenital toxoplasmosis
- Epilepsy
- Intellectual disability
- Visual disabilities; (chorioretinitis → increased risk of chorioretinal scars , cataracts, and glaucoma)
- Sensorineural hearing loss

Diagnostics [5]
- Mother: See “Diagnostics” in “Toxoplasmosis.”
- Fetus: PCR for T. gondii DNA in amniotic fluid
-
Newborn
- CT/MRI: intracranial calcifications, hydrocephalus, ring-enhancing lesions
- T. gondii-specific IgM antibodies (CSF, serum)
- PCR forT. gondii DNA (CSF, serum)
- Ophthalmological evaluation: chorioretinitis



Treatment [6][7]
-
Maternal infection
- < 18 weeks' gestation: immediate administration of spiramycin to prevent fetal toxoplasmosis [8]
- ≥ 18 weeks' gestation: pyrimethamine, sulfadiazine, and folinic acid
- Neonates or fetal infection confirmed by amniocentesis: pyrimethamine, sulfadiazine, and folinic acid
Prevention [3]
- Avoid raw, undercooked, and cured meats.
- Wash hands frequently, especially after touching soil (e.g., during gardening).
- Avoid contact with cat litter.
The 4 Cs of congenital toxoplasmosis: Cerebral calcifications, Chorioretinitis, hydroCephalus, and Convulsions.
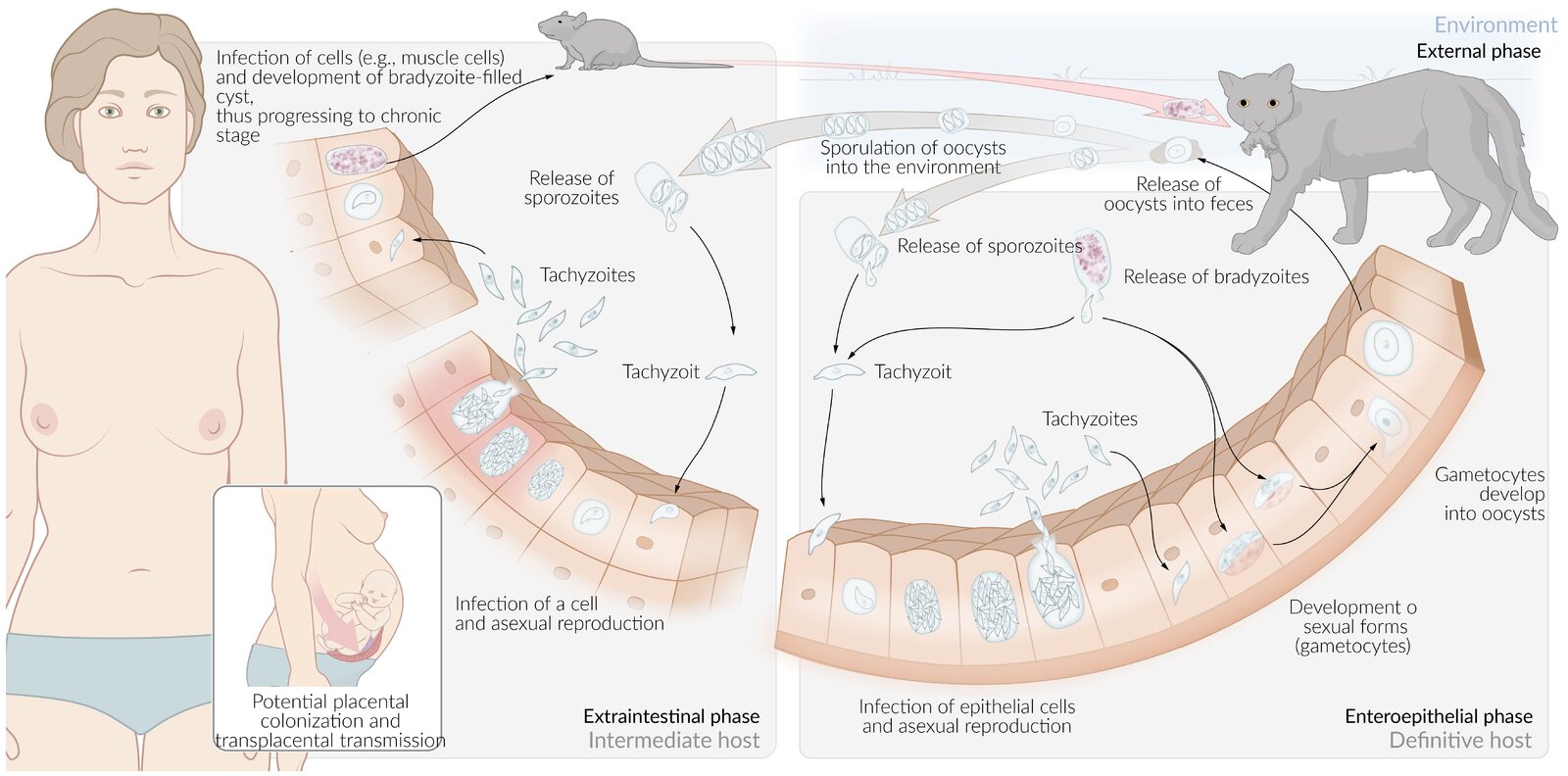
The life cycle of toxoplasmosis involves transmission to a human host through the ingestion of cat feces particulate that contains oocysts or ingestion of meat (i.e., pork) containing Toxoplasma cysts. Cross-placental transmission is possible after the initial infection of pregnant women.
© AMBOSS
© AMBOSS
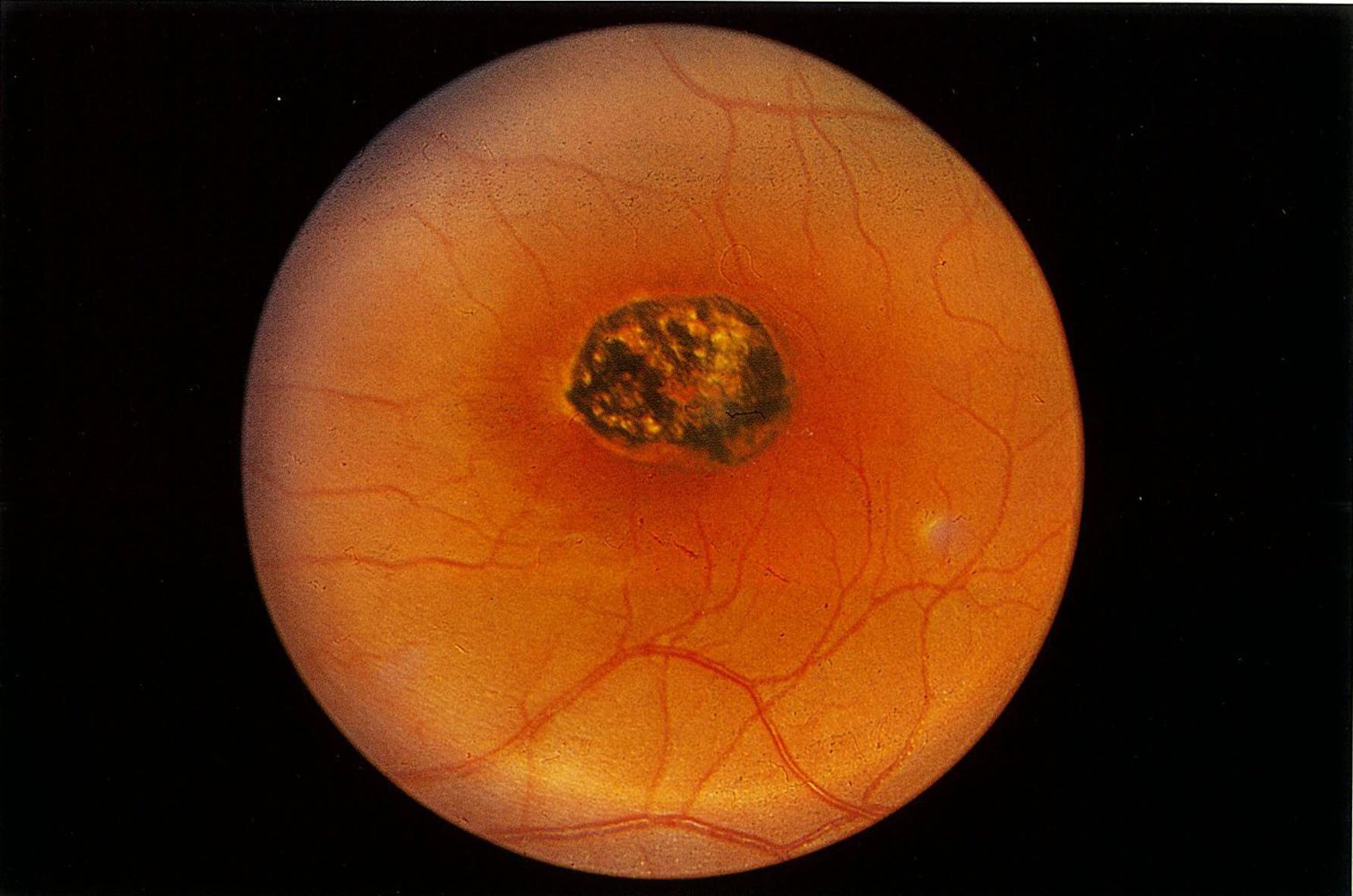
Fundus photography of the left eye of an infant (optic disc not shown)
The macular area shows a sharply demarcated scar with depigmentation and hyperpigmentation, affecting both the retina and choroid. This clinical finding is a typical sign of congenital toxoplasmosis.
Source: © IMPP
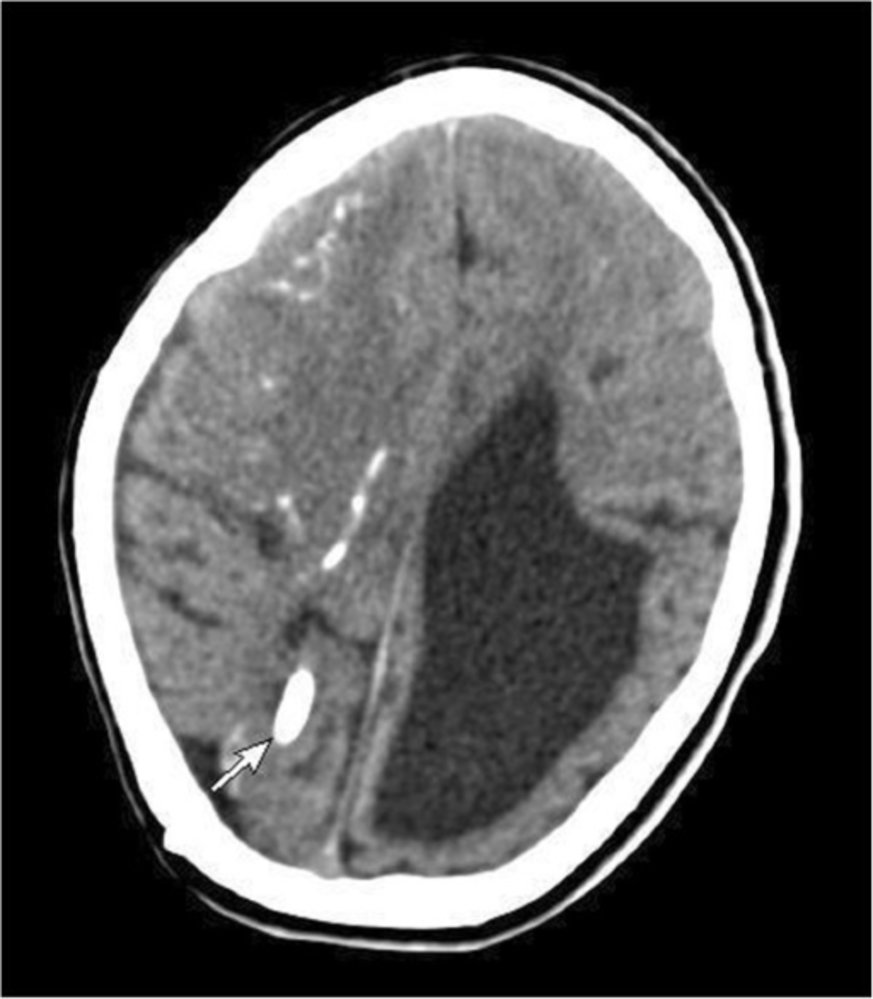
Cranial CT scan of an infant (IV contrast; axial view)
The left lateral ventricle is highly dilated (hatched red overlay). Hyperdensities are visible in the parenchyma of the right frontal lobe (green overlay) and in the occipital lobe (green overlay; white arrow), indicating parenchymal calcifications.
Hydrocephalus (ventriculomegaly) and parenchymal calcifications are typical radiological features of congenital toxoplasmosis.
Source: “Figure 1. in: Congenital toxoplasmosis presenting as central diabetes insipidus in an infant: a case report.” by Mohamed S, Osman A, Al Jurayyan NA, Al Nemri A, Salih MA, BMC Research Notes, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
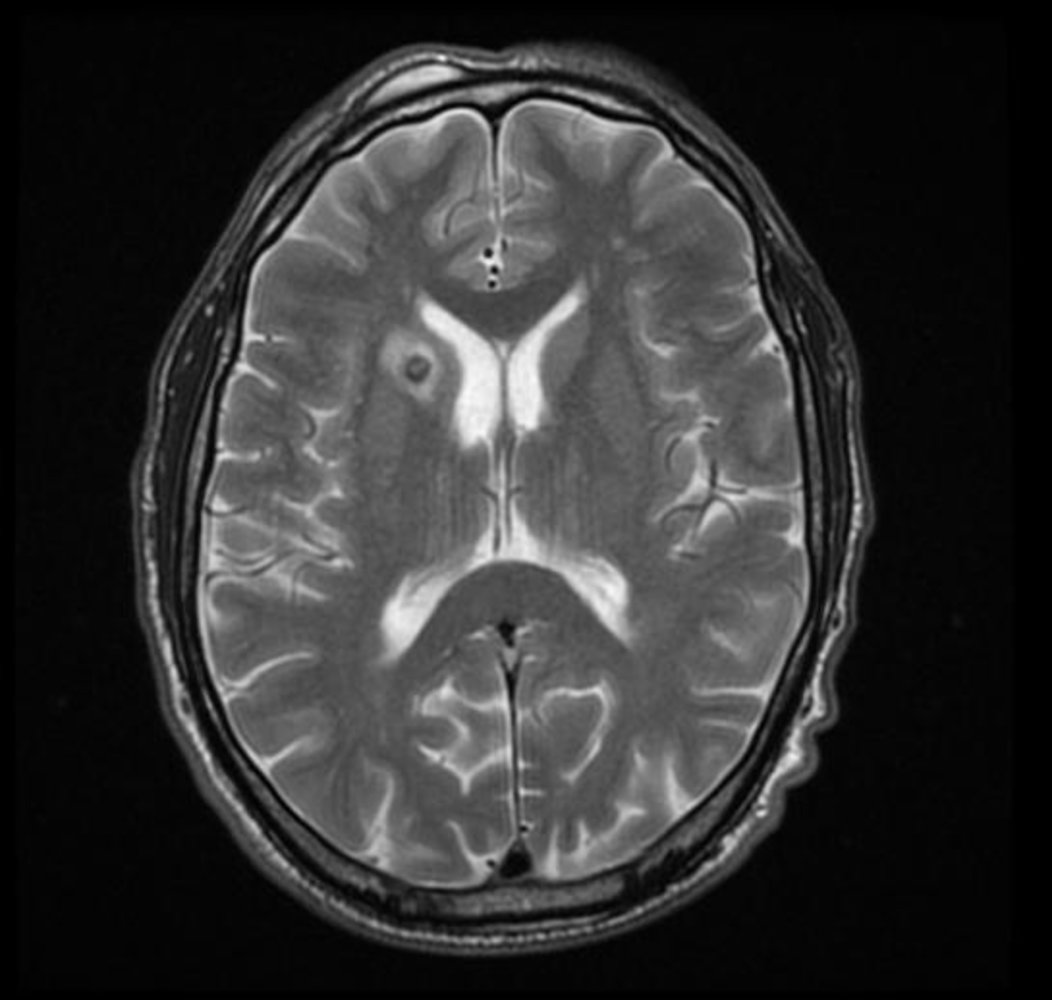
MRI head (T2-weighted; with contrast; axial plane) of a patient with cerebral toxoplasmosis
A small nodule (hatched overlay) in the right internal capsule is accompanied by hyperintense perilesional edema (solid overlay).
Neurotoxoplasmosis more commonly manifests with multiple lesions and it has a propensity for the corticomedullary junction, thalami, and basal ganglia. It is a leading cerebral opportunistic infection in patients with AIDS.
Source: “Intracranial toxoplasmosis 001.jpg” by Prashanth Saddala., Wikidoc, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
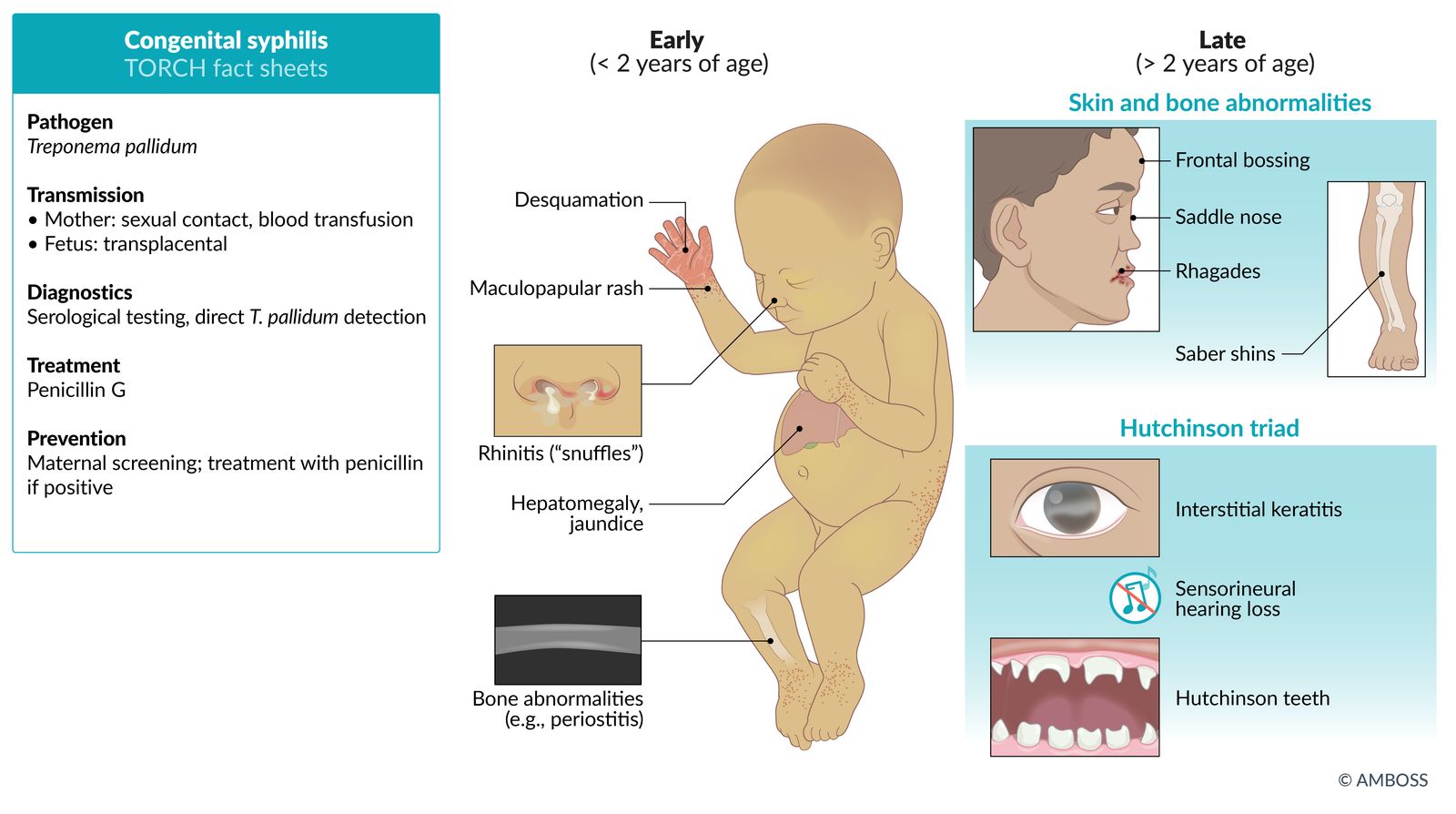
Congenital syphilis
Epidemiology
∼ 23:100,000 live births per year in the US [9]
Pathogen
Treponema pallidum
Transmission [9]
-
Mother
- Sexual contact (contact with infectious lesion)
- See “Etiology” in “Syphilis.”
-
Fetus: transplacental transmission from infected mother
- Increased risk of transmission with recent syphilis infection
- Risk of transmission increases with gestational age
- Neonate: perinatal transmission during birth
Clinical features of congenital syphilis [10]
-
In utero syphilis
- Miscarriage
- Stillbirth
- Hydrops fetalis
-
Early congenital syphilis (onset < 2 years of age)
- Hepatomegaly and jaundice
- Rhinorrhea; with white or bloody nasal discharge (also called “snuffles”)
- Maculopapular rash on palms and soles; a bullous form of the rash called pemphigus syphiliticus may be present at birth.
- Skeletal abnormalities (e.g., metaphyseal dystrophy, periostitis)
- Generalized lymphadenopathy (nontender)
-
Late congenital syphilis (onset > 2 years of age)
- Typical facial features: saddle nose, frontal bossing, short maxilla
- Dental findings: Hutchinson's teeth (notched, widely spaced teeth); mulberry molars (poorly developed first molars)
- Eyes and ears [11]
-
Syphilitic keratitis: nonulcerative, interstitial keratitis that develops as a late complication of syphilis
- More common in patients with congenital syphilis than acquired syphilis
- Causes stromal inflammation
- Sensorineural hearing loss
-
Syphilitic keratitis: nonulcerative, interstitial keratitis that develops as a late complication of syphilis
- Skin: rhagades (perioral fissures, cracks, and/or scars, particularly near the corners of the mouth and nose)
- Skeletal
-
Saber shins
- An anterior bowing of the tibia, causing it to resemble a saber
- Other causes include rickets and Paget disease of bone.
- Painless arthritis in knees and other joints
-
Saber shins
- Neurological: cranial nerve palsies (e.g., CN VIII defect causing deafness), intellectual disability, hydrocephalus




Diagnosis [12]
- Mother: See “Diagnostics of syphilis in pregnancy.”
- Fetus: repeated ultrasound examinations (placentomegaly, hepatomegaly, ascites, and/or hydrops fetalis)
-
Neonate
- RPR or VDRL (serum)
- Dark-field microscopy or PCR of CSF
- CBC and differential
- Radiographs of the long bones
- Further studies depend on clinical features of congenital syphilis

Treatment
- Neonates: 10 days of IV penicillin G [12]
-
Mothers
- Treatment depends on whether diagnosed prenatally or postnatally
- See “Treatment of syphilis in pregnancy” and Treatment of syphilis.”
Prevention [9]
- Prenatal screening for syphilis and, if positive, antibiotic treatment: should take place in early pregnancy because placental transmission is most likely to occur after the first trimester.
- Nationally notifiable condition: Congenital syphilis and syphilitic childbirth must be reported to the local or state health department.
Hutchinson triad: interstitial keratitis, sensorineural hearing loss, Hutchinson teeth
© AMBOSS

A face of a newborn infant with perioral fissures (rhagades; indicated by black arrow) and nasal discharge (indicated by white arrow) can be seen.
These clinical features are characteristic of congenital syphilis.
Source: "ID#: 2246", CDC/ Dr. Norman Cole, Centers for Disease Control and Prevention licensed under Public Domain

Plantar surfaces of the feet in a newborn with congenital syphilis
The right foot shows a fluid-filled blister. The left foot shows a blister that has already peeled.
These features suggest pemphigus syphiliticus, which is pathognomonic for congenital syphilis.
Source: © IMPP

The central incisor teeth are narrow and notched (Hutchinson teeth), while the molars are not fully developed (mulberry molars). These findings occur after continued inflammation and scar formation through congenital syphilis.
Source: "ID#: 2385", Susan Lindsley, Centers for Disease Control and Prevention licensed under Public Domain Further notes: Public Health Image Library (PHIL); ID: 2385

Photomicrograph of testicular tissue (dark-field microscopy and immunofluorescence; very high magnification) from a rabbit
Spiral bacteria are visible.
This is the characteristic appearance of spirochetes.
Source: "2335", CDC/ C.W. Hubbard, Centers for Disease Control and Prevention's Public Health Image Library licensed under Public Domain
Congenital listeriosis
Epidemiology
∼ 3:100,000 live births per year in the US [13]
Pathogen
Listeria monocytogenes
Transmission [14]
-
Mother
- Contaminated food: especially raw milk products
- Other possible sources: fish, meat, and industrially processed vegetables (e.g., ready-made salads)
- See “Etiology” in “Listeriosis.”
-
Fetus
- Transplacental transmission from an infected mother
- Direct contact with infected vaginal secretions and/or blood during delivery
Clinical features [15]
-
Listeriosis of pregnancy
- Increased risk of premature birth and spontaneous abortion
-
Early-onset syndrome: granulomatosis infantiseptica
- Severe systemic infection characterized by disseminated abscesses (may develop in any organ system)
- Most common findings: respiratory distress and skin lesions
- Signs of meningitis may already develop.
-
Neonatal listeriosis
- Late-onset syndrome (5 days to 3 weeks after birth): Listeria meningitis/encephalitis
- See “Neonatal infection.”
Diagnosis
Culture from blood or CSF samples (pleocytosis) [16]
Treatment
IV ampicillin and gentamicin (for both mother and newborn) [16]
Prevention [14]
- Avoidance of soft cheeses
- Avoidance of potentially contaminated water and food
- Nationally notifiable condition: Listeriosis must be reported to the local or state health department.
- See “Food and water safety.”
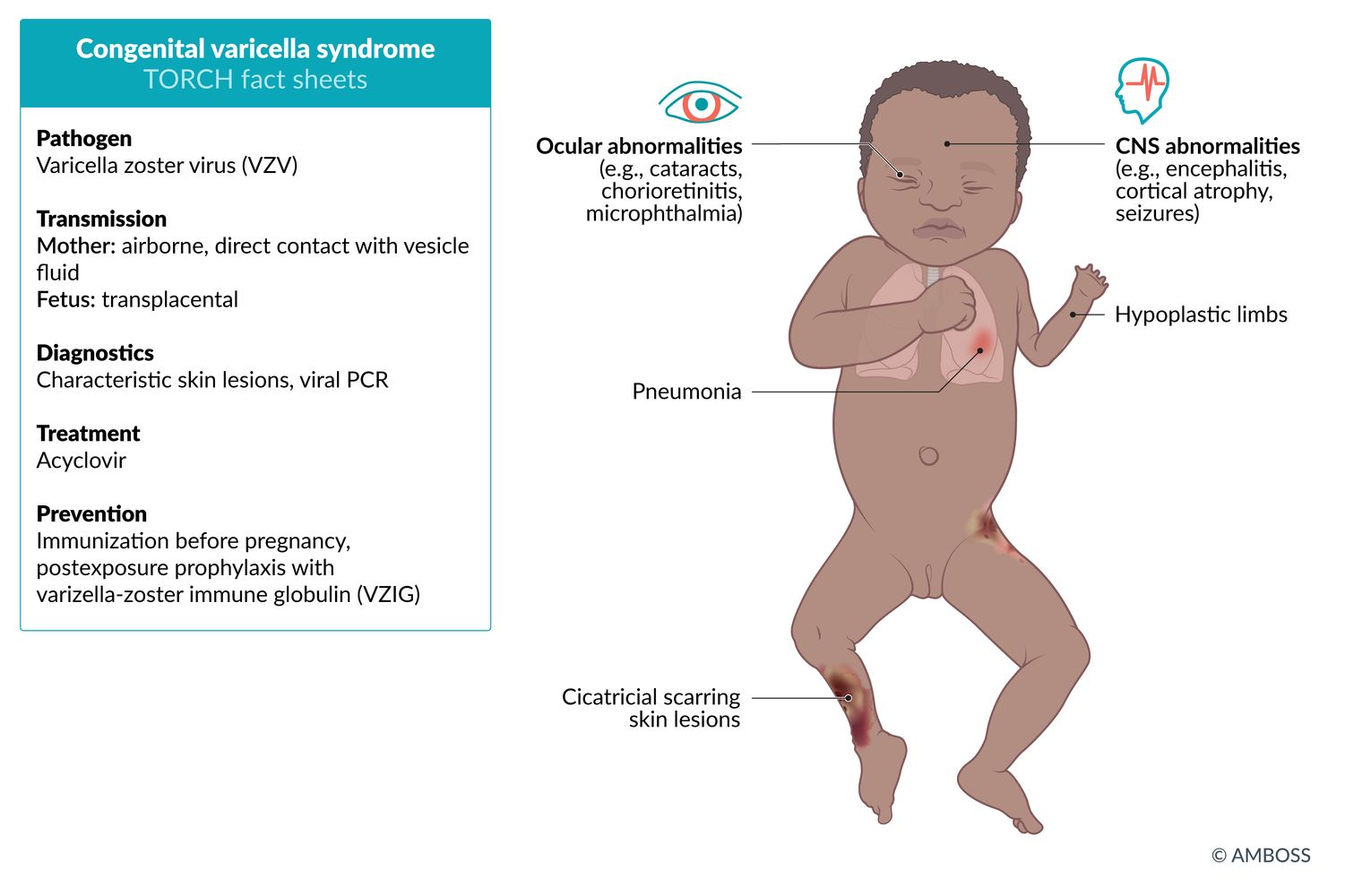
Congenital varicella infection
Epidemiology
- Seroprevalence in the general population is ∼ 95%. [17]
- Most mothers have been vaccinated, so congenital infection is rare (< 2%). [17]
Pathogen
Varicella-zoster virus (VZV)
Transmission [18]
-
Mother
- Primary infection
- Airborne droplets
- Direct skin contact with vesicle fluid
- Reactivation: usually in immunocompromised individuals
- See “Chickenpox” and “Shingles.”
- Primary infection
- Fetus: transplacental transmission from an infected mother
Clinical features [18]
-
Congenital varicella syndrome (infection during first and second trimester) ; [19]
- Hypertrophic scars (cicatricial skin lesions)
- Limb defects (e.g., hypoplasia)
- Ocular defects (e.g., chorioretinitis, cataracts, microphthalmia)
- CNS defects (e.g., cortical atrophy, seizures, intellectual disability), hydrocephalus
-
Neonatal varicella
- Mild infection (maternal exanthem > 5 days before birth)
- Severe infection (maternal exanthem < 5 days before birth): hemorrhagic exanthem; , encephalitis, pneumonia, or congenital varicella syndrome (mortality rate of up to 30%)

Diagnosis [18]
-
Newborn and mother
- Usually clinical diagnosis is confirmed by appearance of skin lesions
- DFA or PCR of fluid collected from blisters or cerebrospinal fluid (CSF)
- Serology
- Fetus: PCR for VZV DNA (in fetal blood, amniotic fluid) and ultrasound to detect fetal abnormalities
Treatment [18]
- For pregnant women or newborns with (severe) infection: acyclovir
- Administer postexposure prophylaxis in newborns if mother displays symptoms of varicella < 5 days before delivery: IgG antibodies (varicella-zoster immune globulin, VZIG) [20]
- For other indications for varicella postexposure prophylaxis, see “Prevention” in “Varicella.”
- Cesarean delivery if lesions are present at the delivery
- Breastfeeding is encouraged because of the possible protective effect of antibodies in breast milk.
Prevention
- Immunization of seronegative women before pregnancy
- VZIG in pregnant women without immunity within 10 days of exposure
- Nationally notifiable condition: Varicella must be reported to the local or state health department.
© AMBOSS
Congenital parvovirus B19 infection
Epidemiology [21]
- ∼ 5% incidence in pregnant women per year in the US
- Higher prevalence in daycare workers and elementary school teachers
Pathogen
- Parvovirus B19
- Mechanism of action: infection of erythrocyte progenitor cells in bone marrow and endothelial cells by attaching to their P antigen → cell destruction → hydrops fetalis in neonates and pure RBC aplasia in adults
Transmission
-
Mother
- Mainly via aerosols
- Rarely hematogenous transmission
- See “Fifth disease.”
- Fetus: transplacental transmission from infected mother
Clinical features [21]
- Severe anemia and possibly fetal hydrops
- Fetal demise and miscarriage/stillbirth in approximately 10% of cases (Risk is highest in the first and second trimesters.)
- Most intrauterine infections do not result in fetal developmental defects.
Diagnosis
- Mother: serologic assays for IgG and IgM against parvovirus B19
| Serologic assay analysis for parvovirus B19 | ||
|---|---|---|
| Results | Positive IgM | Negative IgM |
| Positive IgG |
|
|
| Negative IgG |
|
|
-
Fetus [21]
- PCR for parvovirus B19 DNA (amniotic fluid or blood)
- Periodic ultrasound of fetal vessels for anemia and hydrops fetalis (every 1–2 weeks)
- In cases of suspected anemia according to Doppler ultrasound, fetal hemoglobin levels are determined via the umbilical vein.
Treatment
- Intrauterine fetal blood transfusion in cases of severe fetal anemia
- Additional platelet transfusion if thrombocytopenia is also present
Prevention
- Hand hygiene (frequent hand washing)
- Pregnant women with risk factors for TORCH infection should avoid potentially contaminated workplaces (e.g., schools, pediatric clinics).
Congenital rubella infection
Epidemiology
Most mothers have been vaccinated, so congenital infection is very rare. [22]
Pathogen
Rubella virus
Transmission
-
Mother
- Mainly via airborne droplets
- See “Rubella.”
-
Fetus
- Transplacental from infected mother
- Risk of fetal infection is high in the first trimester, decreased in the second trimester and then increased again in the third trimester. [23]
-
Risk of congenital rubella syndrome [24]
- 1–12 weeks gestation (period of organogenesis): highest risk
- 12–20 weeks gestation: very low
- > 20 weeks gestation: no documented cases
Clinical features [24]
- Intrauterine rubella infection: miscarriage, preterm birth, fetal growth restriction (especially likely if infection occurs during the first trimester)
-
Congenital rubella syndrome
-
Triad of congenital rubella syndrome
- Cardiac defect; : most common defect (e.g., patent ductus arteriosus, pulmonary artery stenosis)
- Cataracts: Other eye manifestations may also occur later in life, including glaucoma and salt and pepper retinopathy (abnormal retinal pigmentation)
- Cochlear defect: bilateral sensorineural hearing loss
- Early features
- Hepatosplenomegaly, jaundice
- Hemolytic anemia, thrombocytopenia
- Petechiae and purpura, i.e., blueberry muffin rash (due to extramedullary hematopoiesis in the skin)
- Transient meningitis and/or encephalitis
- Pneumonia
- Late features
- CNS defects: microcephaly, intellectual disability, panencephalitis
- Skeletal abnormalities
- Endocrine disorders (e.g., diabetes, thyroid dysfunction)
- Vascular disease
- Immune defects
-
Triad of congenital rubella syndrome
 cataract")
Diagnosis [25]
-
Newborn and mother
- PCR for rubella RNA (throat swab, CSF)
- Serology (abnormally high or persistent concentrations of IgM and/or IgG antibodies)
- Viral culture (nasopharynx, blood)
-
Fetus
- IgM antibody serology (chorionic villi, amniotic fluid)
- PCR for rubella RNA (chorionic villi, amniotic fluid)
Treatment
-
Intrauterine rubella infection [25]
- < 16 weeks: Counsel about potential maternal-fetal transmission and the possibility of terminating the pregnancy.
- > 16 weeks: reassurance and symptomatic therapy (e.g., acetaminophen)
- Congenital rubella syndrome: supportive care (based on individual disease manifestations) and surveillance (including monitoring for late-term complications)
Prevention [26]
- Immunization of seronegative women before pregnancy
- Nationally notifiable condition: Suspected congenital rubella syndrome must be reported to the local or state health department.
CCC-Triad of congenital rubella syndrome: Cataracts, Cochlear defects, Cardiac abnormality
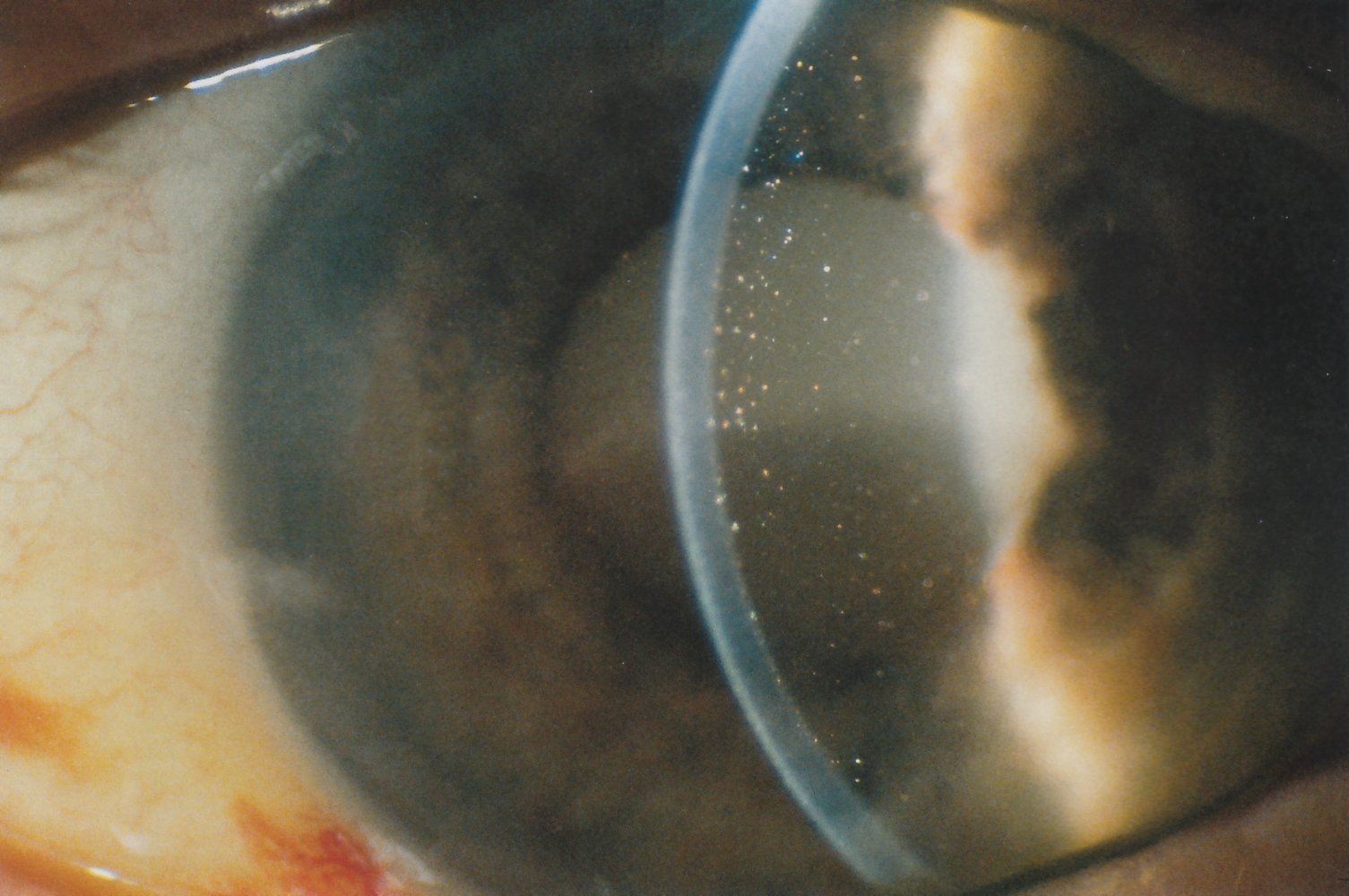
Slit-lamp photography
The completely opacified lens is visible in the pupil. Its darker, inferior part represents the sunken nucleus (blue overlay) within the liquified cortex (white upper part; yellow overlay). This is the typical appearance of Morgagnian hypermature cataract. The anterior chamber shows deposits, probably macrophages filled with lens protein (examples indicated by arrowheads). This suggests a phacocytic process, which, if left untreated, can lead to phacolytic glaucoma.
Hatched overlay: optical cross-section of the cornea; produced by slit-lamp
Source: © IMPP
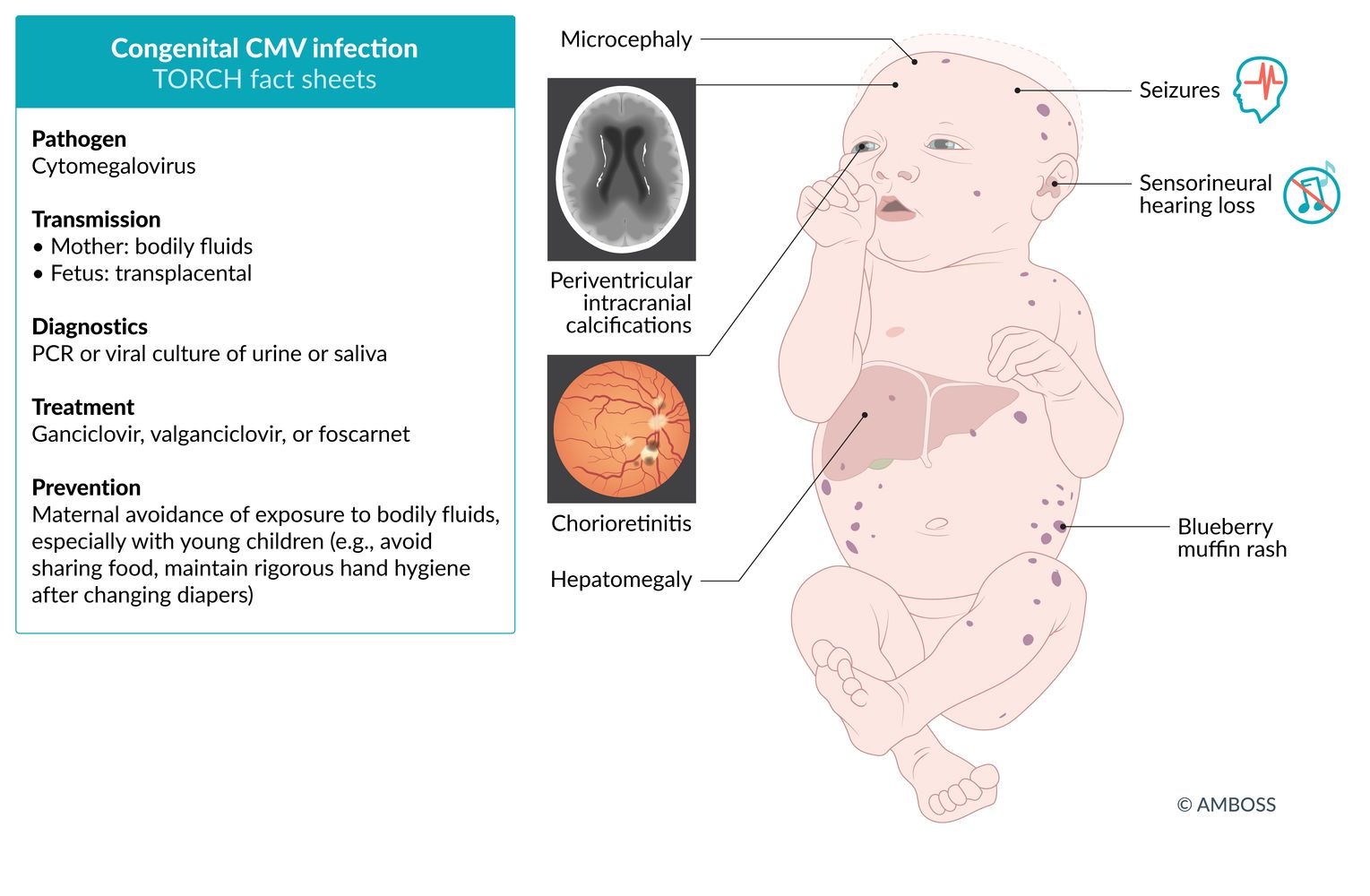
Congenital CMV infection
Epidemiology
∼ 0.5–1% of live births per year in the US [27]
Pathogen
Cytomegalovirus
Transmission
-
Mother: via CMV-contaminated blood, urine, saliva, and genital secretions
- Blood transfusions
- Sexual transmission
- Droplet transmission
- Transplant-transmitted infection (e.g., bone marrow, lungs, kidneys)
- See “Cytomegalovirus infection.”
- Fetus: : transplacental transmission from an infected mother
- Newborn: : during birth or postnatal via breastmilk from infected mother
Clinical features [28]
-
Fetal infection
- Increased risk of fetal demise
- IUGR
- Oligohydramnios or polyhydramnios, placental abnormalities
-
Newborn infection
- Severity
- Subclinical infection (∼ 90%): ∼ 10% go on to develop a late complication (most commonly hearing loss) [28]
- Symptomatic infection at birth (∼ 10%): ∼ 70–80% go on to develop a late complication.
-
CNS findings
- Hydrocephalus
- Microcephaly .
- Sensorineural hearing loss (∼ 30%) [29]
- Chorioretinitis (∼ 10%)
- Nonspecific findings (similar to other TORCH infections)
- Petechiae, purpura (blueberry muffin rash)
- Hepatosplenomegaly, jaundice
- Small for gestational age (SGA)
- Seizures, lethargy, poor suck
- Hemolytic anemia, thrombocytopenia
- Pneumonia
- Late complications
- Hearing loss, vision impairment
- Psychomotor retardation, intellectual disability
- Dental abnormalities
- Severity

Diagnosis [30][31]
-
Fetus and newborn
- CNS imaging: hydrocephalus, periventricular calcifications, or intraventricular hemorrhage
- Ultrasound: periventricular calcifications, hyperechogenic foci (bowel and liver, ascites), and hydrops fetalis
-
Newborn and mother
- CMV IgM antibodies (blood)
- Viral culture or PCR for CMV DNA (urine, saliva)
-
Fetus
- Viral culture or PCR for CMV DNA (amniotic fluid)
- CMV IgM antibodies (fetal blood)


Differential diagnosis [30]
-
Congenital toxoplasmosis
- Causes chorioretinitis, hydrocephalus, and intracranial calcifications
- Intracranial calcifications in congenital toxoplasmosis typically show ring-enhancement.
Treatment
-
Fetus
- Severe anemia: intrauterine blood transfusions
- Thrombocytopenia: platelet transfusions
-
Newborn
- Supportive therapy of symptoms (e.g., fluid and electrolyte imbalances, anemia, thrombocytopenia, seizures, secondary infections)
- Ganciclovir, valganciclovir, or foscarnet
- Mother: valacyclovir is the only therapy approved during pregnancy [32]
Prevention
- Frequent hand washing, especially after contact with bodily secretions of small children (e.g., diaper changing)
- Avoidance of food sharing with children
- Avoidance of kissing small children on the mouth
Congenital toxoplasmosis may manifest with symptoms resembling congenital CMV infection.
© AMBOSS
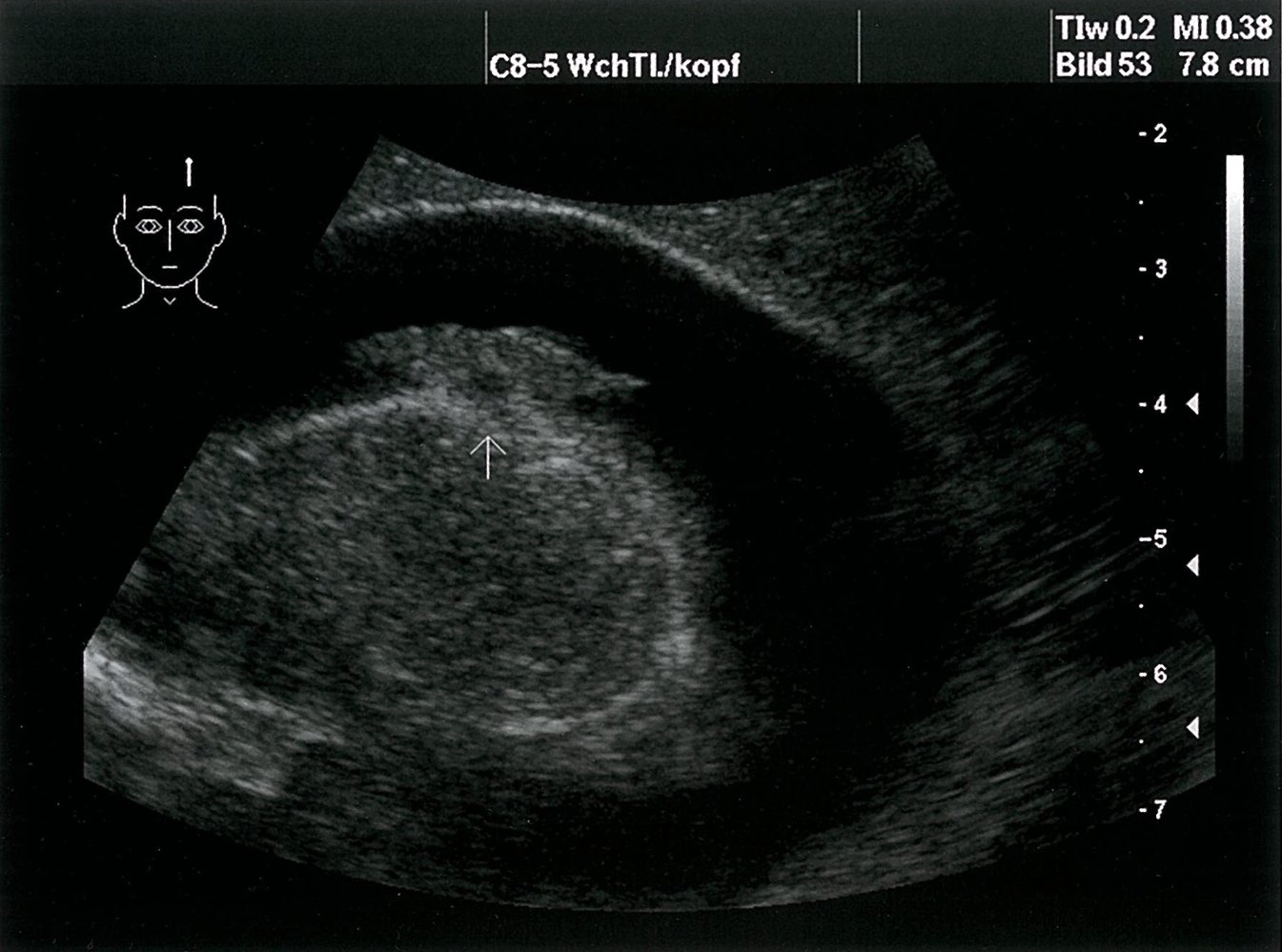
Ultrasound of the CNS, parasagittal section: dilated lateral ventricles with hyperechoic deposits that are compatible with intraventricular hemorrhage
Source: © IMPP
Ultrasound of the CNS, coronal section: dilated lateral ventricles with hyperechoic deposits that are compatible with intraventricular hemorrhage (green areas). (Arrow = periventricular calcification)
Source: © IMPP
Congenital herpes simplex virus infection
- Congenital herpes simplex virus infection a rare intrauterine infection that typically manifests at birth.
- For details, see "Neonatal herpes simplex virus infection."
References
- Peyron F, Mc Leod R, Ajzenberg D, et al. "Congenital Toxoplasmosis in France and the United States: One Parasite, Two Diverging Approaches". PLoS Negl Trop Dis. 11(2). :e0005222. (2017)
- McAuley JB. "Congenital Toxoplasmosis". Journal of the Pediatric Infectious Diseases Society. 3(suppl_1). :S30-S35. (2014)
- Patel P. "Congenital Infections of the Nervous System". CONTINUUM: Lifelong Learning in Neurology. 27(4). :1105-1126. (2021)
- McLeod R, Boyer K, Karrison T, et al. "Outcome of Treatment for Congenital Toxoplasmosis, 1981-2004: The National Collaborative Chicago-Based, Congenital Toxoplasmosis Study". Clinical Infectious Diseases. 42(10). :1383-1394. (2006)
- "Clinical Care of Toxoplasmosis". https://web.archive.org/web/20250819094742/https://www.cdc.gov/toxoplasmosis/hcp/clinical-care/index.html. [2024-01-22]
- Cantey PT, Montgomery SP, Straily A. "Neglected Parasitic Infections: What Family Physicians Need to Know-A CDC Update". Am Fam Physician. 104(3). :277-287. (2021)
- "Toxoplasmosis in Pregnancy". https://www.glowm.com/section_view/heading/Toxoplasmosis%20in%20Pregnancy/item/187
- Centers for Disease Control and Prevention. "Three Cases of Congenital Rubella Syndrome in the Postelimination Era: Maryland, Alabama, and Illinois, 2012". MMWR Morb Mortal Wkly Rep. 62(12). :226-229. (2013)
- Katow S. "Rubella Virus Genome Diagnosis during Pregnancy and Mechanism of Congenital Rubella". Intervirology. 41(4-5). :163-169. (1998)
- "Chapter 15: Congenital Rubella Syndrome". https://web.archive.org/web/20201101034443/https://www.cdc.gov/vaccines/pubs/surv-manual/chpt15-crs.html. [2020-04-28]
- Dontigny L, Arsenault MY, Martel MJ, et al. "SOGC Clinical Practice Guidelines: Rubella in Pregnancy". J Obstet Gynaecol Can. 30(2). :152–158. (2008)
- "Prevention of Measles, Rubella, Congenital Rubella Syndrome, and Mumps, 2013: Summary Recommendations of the Advisory Committee on Immunization Practices (ACIP)". https://web.archive.org/web/20241226075912/https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6204a1.htm. [2013-06-14]
- "Sexually Transmitted Disease Surveillance 2017". https://web.archive.org/web/20201112042443/https://www.cdc.gov/std/stats17/Syphilis.htm. [2018-07-24]
- Lago EG, Vaccari A, Fiori RM. "Clinical Features and Follow-up of Congenital Syphilis". Sex Transm Dis. 40(2). :85-94. (2013)
- L. Pessoa, V. Galvao. "Clinical aspects of congenital syphilis with Hutchinson's triad". Case Reports. 2011(dec21 1). :bcr1120115130-bcr1120115130. (2011)
- Wendel Jr. GD, Sheffield JS, Hollier LM, et al. "Treatment of Syphilis in Pregnancy and Prevention of Congenital Syphilis". Clinical Infectious Diseases. 35(s2). :S200-S209. (2002)
- "2017 Nationally Notifiable Conditions". https://web.archive.org/web/20170428041334/https://wwwn.cdc.gov/nndss/conditions/notifiable/2017/. [2017-01-01]
- Janakiraman V. "Listeriosis in pregnancy: diagnosis, treatment, and prevention". Rev Obstet Gynecol. 1(4). :179-85. (2008)
- Mardis BA, Conley CS, Kyle JA. "Listeriosis: An Overview". US Pharm. 37(8). :38-41. (2012)
- Madjunkov M, Chaudhry S, Ito S. "Listeriosis during pregnancy". Arch Gynecol Obstet. 296(2). :143-152. (2017)
- "Congenital CMV Infection". https://web.archive.org/web/20201028195748/https://www.cdc.gov/cmv/clinical/congenital-cmv.html. [2020-04-28]
- Boppana SB, Ross SA, Fowler KB. "Congenital Cytomegalovirus Infection: Clinical Outcome". Clinical Infectious Diseases. 57(suppl 4). :S178-S181. (2013)
- Fowler KB, Boppana SB. "Congenital cytomegalovirus (CMV) infection and hearing deficit". Journal of Clinical Virology. 35(2). :226-231. (2006)
- Kathleen R. Fink, MD, Mahesh M. Thapa, et al. "Neuroimaging of Pediatric Central Nervous System Cytomegalovirus Infection". Radiological Society of North America. (2010)
- Lipitz S, Yinon Y, Malinger G, et al. "Risk of cytomegalovirus-associated sequelae in relation to time of infection and findings on prenatal imaging". Ultrasound Obstet Gynecol. 41(5). :508-514. (2013)
- Khalil, A, Heath P, et al. "Congenital Cytomegalovirus Infection: Update on Treatment". BJOG: An International Journal of Obstetrics & Gynaecology. 125(1). :e1-e11. (2017)
- Andreas Sauerbrei, MD. "Preventing congenital varicella syndrome with immunization". Canadian Medical Association Journal. (2011)
- "Varicella". https://web.archive.org/web/20201107142824/https://www.cdc.gov/vaccines/pubs/pinkbook/varicella.html. [2019-04-15]
- Smith CK, Arvin AM. "Varicella in the fetus and newborn". Seminars in Fetal and Neonatal Medicine. 14(4). :209-217. (2009)
- Auriti C, Piersigilli F, De Gasperis MR, Seganti G. "Congenital Varicella Syndrome: Still a Problem?". Fetal Diagn Ther. 25(2). :224-229. (2009)
- Shrim A, Koren G, Yudin MH, et al. "Management of Varicella Infection (Chickenpox) in Pregnancy". Journal of Obstetrics and Gynaecology Canada. 34(3). :287-292. (2012)
- Lamont RF, Sobel JD, Vaisbuch E, et al. "Parvovirus B19 infection in human pregnancy". BJOG. 118(2). :175-186. (2010)