Summary
Contraception is the prevention of pregnancy through the use of medications, medical devices, or behaviors. Many different contraceptive options (both hormonal and nonhormonal) exist, allowing individuals to choose a method suited to their medical needs and pregnancy prevention priorities; some methods offer additional noncontraceptive benefits. Hormonal contraceptives contain estrogen and/or progestins to prevent ovulation, fertilization, and/or implantation of an embryo. Nonhormonal contraceptives include sterilization, the copper IUD, barrier methods of contraception, and behavioral methods of contraception. The duration of contraception provided ranges from the length of intercourse (e.g., condoms) to years (long-acting reversible contraception such as IUDs and the progestin implant). The choice of contraception involves shared decision-making that balances the individual patient's preferences with the risks of contraceptive use. The US Medical Eligibility Criteria (USMEC) for contraceptive use are used to provide risk-based guidance for individuals with coexisting medical conditions. Although often neglected, easy access to contraception, including emergency contraception, is an important part of medical care for all individuals who require it. Some contraception is available without a prescription; most require a prescription or a health care professional to fit them.
Overview
Hormonal and nonhormonal contraception
-
Hormonal contraception
-
Uses progestin with or without estrogen to prevent conception through one or a combination of the following:
- Prevention of ovulation
- Thickening of cervical mucus
- Creation of an inhospitable intrauterine environment
- Examples include the hormonal IUD, combined hormonal contraception, and progestin-only pill, implant, or injection.
-
Uses progestin with or without estrogen to prevent conception through one or a combination of the following:
-
Nonhormonal contraception
- Prevents conception without altering natural hormones
-
The mechanism of action depends on the method.
- Copper IUD: creation of an inhospitable intrauterine environment
- Barrier methods: prevention of sperm reaching the uterus
- Behavioral methods: avoidance of sex during the fertile window
- Sterilization: blockage of the passage of gametes
Overview of methods [1][2][3]
- All methods of contraception are reversible except sterilization.
- Choice of method is tailored to patient preference and comorbid medical conditions.
- For further information, see specific sections.
| Overview of contraceptive methods [1][2][3] | |||
|---|---|---|---|
| Options | Duration and efficacy | Additional information | |
| Sterilization [3][4] |
|
|
|
| Long-acting reversible contraceptives (LARC) [5][6][7] |
|
|
|
| Progestin-only contraceptive injection [1][9] |
|
|
|
| Short-acting hormonal contraception [1][2][6] |
|
|
|
| Barrier contraceptives [3][4][10] |
|
|
|
| Behavioral contraception methods [4] |
|
|
|
Contraceptive efficacy
The efficacy of contraceptive methods is reported as the contraceptive failure rate, i.e., the percentage of individuals who become pregnant within 12 months of initiating a contraceptive method. [11]
- Failure rate with typical use: includes all individuals using that method regardless of whether it is used correctly and/or consistently [11]
- Failure rate with perfect use, also called the Pearl index: includes only individuals who use the method correctly and consistently; mainly used in clinical studies [11]
85% of female individuals currently using a contraceptive method would become pregnant within 1 year if contraception were stopped. [4]
Approach to initiating contraceptives
Selecting a method [12][13]
- Assess the individual's:
- Future reproductive goals
- Previous experience with contraception
-
Past medical history to determine USMEC for contraceptive use (may require a limited physical exam)
- Some contraceptive methods are contraindicated for patients with select medical conditions.
- Encourage patients with conditions that increase the risk of complications in pregnancy to use LARCs.
- Individual contraceptive preferences
- Outline which methods an individual can safely use.
- Explain a combination of methods may be necessary to meet all of an individual's needs, e.g.:
- Condoms for STI protection
- AND LARC for highly effective contraception
Patient preference, comorbid medical conditions, and availability will affect the choice of contraception.
Prescribing contraception [12]
- Avoid barriers to contraceptive use.
- Use a quick start approach rather than waiting until the next menstrual cycle.
- Use patient history to reasonably exclude pregnancy rather than requiring a pregnancy test.
- Offer STI testing, but do not require individuals to wait for results to initiate contraception. [8]
- Do not require a routine pelvic examination and Pap smear.
- Offer telehealth appointments for initiation of contraception and repeat prescriptions, when possible. [14]
- Prescribe a one-year supply of contraceptives. [6]
- Provide basic patient education (e.g., management of unscheduled bleeding, missed or delayed contraception).
- Advise patients to return at any point to discuss concerns or change contraceptive method.
All methods of contraception can be initiated at any time during the menstrual cycle. [6]
Reasonable exclusion of pregnancy
Patients do not require a pregnancy test prior to initiating contraception (including emergency contraception) if the following conditions are met. [8]
- No clinical features of pregnancy
- AND meets any of the following criteria
- ≤ 7 days since menses began or the patient had a spontaneous or induced abortion
- < 4 weeks postpartum
-
< 6 months postpartum and both:
- Exclusively or almost exclusively (> 85% of feeds) breastfeeding
- Amenorrheic
- Since the beginning of prior menses has either:
- Had no sexual intercourse
- Been consistently using a dependable contraceptive method
U.S. Medical Eligibility Criteria (USMEC) for contraceptive use
The following information is used by health care providers for individuals with specific medical conditions or medically relevant factors (e.g., age) to estimate individualized levels of risk versus benefit when choosing a method of contraception.
Category definitions [6][15]
- USMEC category 1: no limitations on use
- USMEC category 2: benefits generally outweigh risks
- USMEC category 3: risks often outweigh benefits (relative contraindication)
- USMEC category 4: risks outweigh benefits (absolute contraindication)
Category definitions only apply to contraception indications and do not apply when contraceptives are used to treat other medical conditions (e.g., ovarian cysts). [15]
Contraindications for contraceptive methods [15]
- Recommend alternative forms of contraception to individuals with absolute contraindications.
-
For patients with relative contraindications, these methods may be used following shared decision-making if the patient:
- Cannot use alternative forms of contraception
- Does not wish to use alternative forms of contraception
- Consult USMEC guidelines for more detailed information.
| Relative and absolute contraindications for contraceptive methods [8][15] | ||
|---|---|---|
| Absolute (USMEC category 4) | Relative (USMEC category 3) | |
| Contraindications to copper IUD |
|
|
| Contraindications to hormonal IUD |
|
|
| Contraindications to progestins |
|
|
| Contraindications to CHCs |
|
|
The CDC has developed a free app (see “Tips and links”) to help select a contraceptive method based on guidelines from the US Medical Eligibility Criteria for Contraceptive Use (USMEC) and the US Selected Practice Recommendations for Contraceptive Use (USSPR). [16][17]
Conditions for which highly effective contraception is recommended
Some medical conditions and/or therapies are associated with adverse outcomes in the setting of pregnancy; long-acting, highly-effective contraception is recommended for patients with any of the following: [15]
- Cardiac conditions, e.g.,: [18][19]
- Severe valvular heart disease
- Pulmonary hypertension
- Ischemic heart disease
- Stage 2 hypertension (SBP ≥ 160 mm/Hg, DBP ≥ 100 mm/Hg)
- Peripartum cardiomyopathy
- Stroke
- Cystic fibrosis
- Epilepsy; see “Epilepsy and contraception.”
- Sickle cell disease
- Bariatric surgery within the previous 2 years
- Breast cancer
- Certain gynecological neoplasms
- Insulin-dependent diabetes ≥ 20 years' duration and/or with vascular complications
- Infections: tuberculosis, schistosomiasis with liver fibrosis, untreated or uncontrolled HIV
- VTE or conditions with an increased risk of VTE
- Solid organ transplant within the previous 2 years
- Certain liver cancers
- Use of teratogenic medications
- Certain types of chronic kidney disease
Surgical sterilization
General principles [6][20]
- Sterilization is only indicated in patients who desire or, for medical reasons, require a permanent end to fertility.
- Individual autonomy is of utmost importance.
- Highly effective at preventing pregnancy [6]
- Does not protect against STIs (but may decrease risk of PID in females) [21]
If indicated for medical reasons, other procedures also result in sterilization, e.g., hysterectomy and/or bilateral oophorectomy in females and bilateral orchiectomy in males.
Bilateral tubal ligation [6]
-
Description
- A surgical procedure in which both fallopian tubes are permanently blocked or severed
- Prevents fertilization by removing the connection between the uterus and ovaries
- Generally performed under local anesthesia with or without sedation
- Failure rates: 0.5% (perfect and typical use) [4]
-
Available methods [21]
- Laparoscopy or minilaparotomy
- Tubal ligation with or without salpingectomy
- Electrocoagulation of the oviduct
- Clipping or banding of the fallopian tubes
- Postprocedure counseling: No backup contraception is required.
-
Complications [6]
- Hemorrhage
- Infection
- If pregnancy occurs, there is an elevated risk of it being ectopic, but the absolute risk of an ectopic pregnancy is extremely low. [6]
Notify patients that age and waiting period restrictions may apply depending on local protocols. [22]
Vasectomy [6][8]
-
Description
- A minimally invasive procedure, performed under local anesthesia resulting in permanent occlusion of the vas deferens; can be performed by: [6][8]
- Division of the vas deferens [6][8]
- Intraluminal cautery to induce fibrosis
- Sperm cannot enter the ejaculate, which prevents fertilization.
- A minimally invasive procedure, performed under local anesthesia resulting in permanent occlusion of the vas deferens; can be performed by: [6][8]
- Failure rates: perfect use 0.10%, typical use 0.15% [4][6]
- Postprocedure counseling: Backup contraception is required until azoospermia is confirmed with a sperm sample 8–16 weeks after surgery. [6][8]
-
Complications [6]
- Hematoma
- Surgical site infection
- Sperm granuloma: a collection of sperm due to leakage from the vas deferens into the surrounding interstitium; occurs in ∼ 40% of men following vasectomy [23]
- Postvasectomy pain syndrome: the accumulation of testicular fluid in the epididymis after a vasectomy resulting in a chronic, dull, aching pain in the testes
Intrauterine devices
This information pertains to using IUDs as routine contraception. Additional information on IUD use is available in “Emergency contraception.”
General principles
- IUDs are small T-shaped devices that are inserted into the uterus.
- Can be nonhormonal (copper IUD) or contain progestin (hormonal IUD)
- Used for both regular and emergency contraception [24]
- Mainly thought to work by preventing fertilization, but may also decrease the likelihood of implantation
- Reversible and highly effective as are user-independent
- Can be used by nulliparous or parous individuals [8]
- Last between 3–12 years
- May provide additional noncontraceptive benefits of IUDs, e.g.: [6][25]
- Reduced risk of cervical and endometrial cancers [6]
- Decreased menstrual pain and bleeding (progestin IUDs); see also “Noncontraceptive benefits of progestins.” [6][25]

Types of IUDs
Copper intrauterine device [4][6]
-
Description
- Hormone-free, copper-containing intrauterine device
-
Longest-lasting reversible method of contraception:
- FDA-approved up to 10 years after insertion
- Studies show effectiveness for up to 12 years [6]
-
Mechanism of action [5][25]
- Cu+ ions create localized inflammation that decreases sperm viability and function (prevents fertilization). [26]
- May decrease the likelihood of implantation
- Failure rates: ∼ 0.6% [4]
The copper IUD may cause heavy and prolonged menstrual bleeding, especially during the first 3–6 months after placement. [6][8]
Hormonal IUD [6]
-
Description
- Long-term, reversible levonorgestrel-releasing intrauterine device (contains no estrogen)
- FDA approved for 3–8 years after insertion (depending on the IUD) [6]
-
Mechanism of action: local effects of progestin [5][25]
-
Prevents fertilization via:
- Cervical mucous changes block the sperm from reaching an oocyte
- Decreased sperm function and viability
- Decreases the likelihood of implantation via changes to the endometrial lining [5]
- Unlike systemic progestins, progestin IUDs do not reliably suppress ovulation.
-
Prevents fertilization via:
- Failure rates: 0.1–0.4% [2][4][5]
40–50% of individuals with progestin-containing IUD will become amenorrheic after 2 years. [8]
Initiation of IUDs [8][27]
Preplacement evaluation
- Ensure the patient does not have contraindications to copper IUDs/contraindications to hormonal IUDs.
- Perform a bimanual exam and speculum-assisted visualization of the cervix.
- Obtain pregnancy test; only if unable to reasonably exclude pregnancy. [8]
- Offer routine STI screening; STI testing is not required prior to placement.
Procedure
- Performed at an outpatient visit
- Can be performed during any part of the menstrual cycle [8]
- Offer analgesia to all patients. [28][29]
- Procedural pain
- Topical lidocaine spray [28]
- OR lidocaine-prilocaine cream [28]
- OR paracervical block
- Postprocedural pain: NSAIDs (for dosages, see “Oral analgesia”) [28]
- Procedural pain
- If IUD insertion is unsuccessful, consider misoprostol. [8]
NSAIDs may decrease postprocedural pain but do not provide sufficient analgesia for IUD insertion when used alone. [28]
Postprocedure counseling
- Educate patients on the adverse effects and complications of IUDs. [8]
- Advise continued condom use for STI protection. [8]
- Discuss the consideration of backup contraception for the first 7 days. [5][8][30]
- Checking for IUD strings to confirm correct placement.
- Advise patients that return to fertility may be immediate if the device is removed or expelled.
Follow up
At subsequent routine visits: [8]
- Ensure strings are present (first routine visit) [31]
- Ask about side effects and patient concerns.
Adverse effects and complications of IUDs [6]
-
Adverse effects: pain and menstrual changes (typically resolve within 3–6 months) ; [6][8]
- All IUDs: temporary cramping and discomfort
- Hormonal IUD: abnormal uterine bleeding (e.g., spotting, irregular menses), amenorrhea
- Copper IUD: heavy menstrual bleeding, dysmenorrhea
- Complications [5][32]
- Expulsion [5]
- Uterine perforation [5]
- If pregnancy occurs, there is an elevated risk of it being ectopic, but the absolute risk of an ectopic pregnancy is extremely low. [5][6]
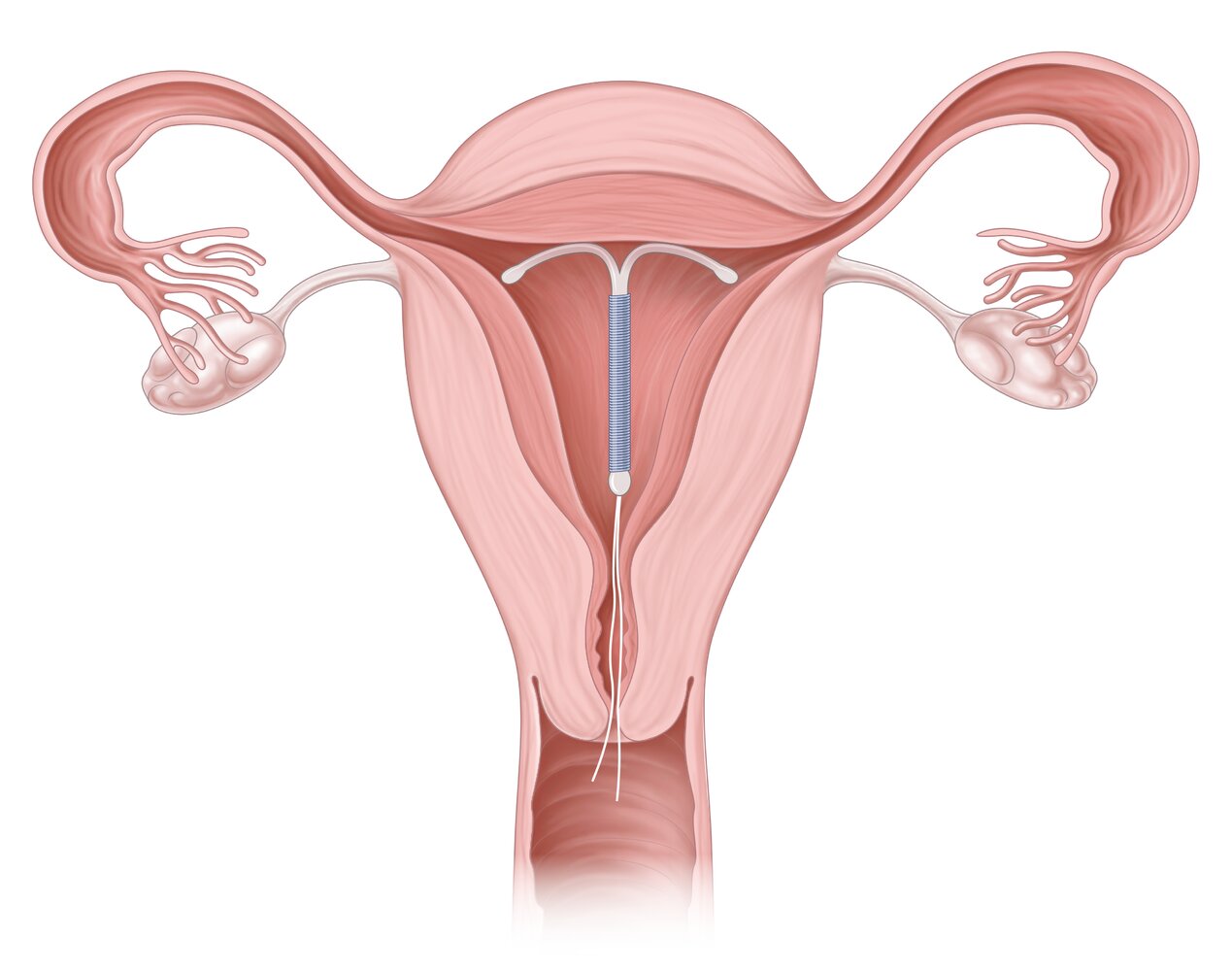
An intrauterine device (IUD) is a small, T-shaped birth control device inserted into the uterus to prevent pregnancy. There are two main types: nonhormonal copper and progestin-releasing. This illustration depicts the correct positioning of an IUD inside the uterus.
© AMBOSS
Hormonal contraception
General principles
- Hormonal contraception offers some of the most reliable protection against pregnancy.
- Noncontraceptive benefits of hormonal contraception can also be used to treat a variety of medical conditions.
- Multiple options of varying durations exist:
- Long-acting contraception: progestin IUD, progestin implant
- Intermediate-acting contraception: depot medroxyprogesterone acetate
- Short-acting contraception: CHCs or POPs
- For individuals with contraindications to CHCs, progestin-only contraception can often be used.
- Patients with contraindications to progestins should be offered nonhormonal contraception.
Mechanism of action for hormonal contraceptives
-
Estrogen: suppresses release of GnRH from the hypothalamus → ↓ release of pituitary gonadotropins (FSH, LH) [1]
- Decreased FSH → prevents ovarian folliculogenesis [1]
- Decreased LH → inhibition of ovulation [1]
-
Progestin: synthetic progesterone → [1]
- Inhibits GnRH and LH secretion → suppressed ovulation (main contraceptive mechanism) [1]
- Inhibits endometrial proliferation → decreases chance of embryo implantation [1]
- Changes cervical mucus (↓ volume and ↑ viscosity) and impairs fallopian tube peristalsis → inhibits sperm migration and embryo implantation [1]
- Inhibits follicular maturation
Noncontraceptive benefits of hormonal contraception [1][6][33]
-
Noncontraceptive benefits of CHCs
- Regulation of menstrual cycles
- Decreased menstrual bleeding, including induced amenorrhea [1]
- Less painful menstruation
- Decrease in hormone level fluctuations
- Decreased risk of endometrial and ovarian cancers [6]
- Ovarian cyst prevention
- Reduction of free testosterone
- May increase bone mineral density
-
Noncontraceptive benefits of progestins: The main benefits are a result of endometrial atrophy.
- Decreased menstrual pain
- Reduced menstrual bleeding, inducing induced amenorrhea (varies by formulation)
- Decreased risk of endometrial cancer
If patients desire amenorrhea, consider using CHCs (continuous use), DMPA, a high-dose norethindrone acetate POP, or a progestin IUD. [33][34]
Combined hormonal contraception
General principles
- CHCs provide highly effective, short-acting, reversible contraception if taken perfectly.
- Contains a combination of estrogen and progestins
- Ovulation is suppressed via systemic estrogen with all forms of CHCs. [6]
- More contraindications to CHCs exist than to other forms of contraception.
- CHCs are taken daily, weekly, or monthly, and efficacy is often affected by adherence.
Noncontraceptive benefits for CHCs
Noncontraceptive benefits of CHCs mean they can be used to treat multiple gynecological and nongynecological conditions, e.g.: [33][35]
- Polycystic ovary syndrome (PCOS)
- Endometriosis
- Abnormal uterine bleeding, heavy menstrual bleeding [1]
- Primary dysmenorrhea
- Mittelschmerz
- Benign ovarian cysts [1]
- Heavy menstrual bleeding associated with uterine leiomyomas [36]
- Hyperandrogenism, including hirsutism and acne (see “Hormonal therapy for acne”) [1]
- Other conditions temporally associated with menstruation
- Menstrual-related migraine (without aura) [37]
- Premenstrual dysphoric disorder (PMDD)
- Menstrual acne
Types of CHCs [1][4][6]
| Overview of combined hormonal contraceptives | ||
|---|---|---|
| Description | Additional information | |
| Combined oral contraceptives (COCs) [1][6] |
|
|
| Contraceptive patch [4][6] |
|
|
| Vaginal ring [4][6] |
|
|
CHCs can be used continuously, avoiding a scheduled withdrawal bleed, but extended or continuous use is associated with an increased incidence of breakthrough bleeding. [43]
Initiation of CHCs
- Provide adequate counseling to ensure this is the most appropriate option for the patient (see “Approach to initiating contraceptives”).
- Ensure the patient has no contraindications to CHCs.
- Determine if the patient requires backup contraception. [6]
- ≤ 5 days from day 0 of LMP: Backup contraception is not required.
- > 5 days from day 0 of LMP or > 7 days after miscarriage or abortion: Recommend backup contraception for 7 days.
- Inform patients about the common adverse effects of CHCs.
- Ensure patients know what to do if contraception is late or missed.
Educate all patients on contraindications to CHCs and advise patients to stop CHCs immediately and consult a healthcare professional if any contraindications develop.
Adverse effects of CHCs [6]
Mainly related to the adverse effects of estrogen, e.g.:
- Common
- Headaches
- Breast tenderness
- GI symptoms: nausea, GERD [44]
- Mood swings
- Irregular bleeding [6]
- Worsening acne [6]
- Serious (rare)
- Venous thromboembolism (VTE) [45]
- Cardiovascular conditions: hypertension, stroke, myocardial infarction
- Hepatocellular adenoma development [46]
Many patients believe weight gain is a side effect of CHCs, however, studies have not shown an association. [47]
Progestin-only contraception
General overview [1][33]
- Progestin-only contraceptives are highly effective.
- May be an option for individuals with contraindications to CHCs
- Reversible duration ranges from short-acting (daily tablets) to long-acting (implants and hormonal IUDs)
- Can be used to manage:
- Abnormal uterine bleeding
- Primary dysmenorrhea
- Endometriosis
Types of progestin-only contraception [6][8]
| Overview of progestin-only contraception [8] | ||
|---|---|---|
| Description | Additional information | |
| Progestin-only contraceptive pills (POPs) [6][8] |
|
|
| Depot medroxyprogesterone acetate (DMPA) [1][6][9] |
|
|
| Progestin IUD [6] |
|
|
| Progestin implant [8] |
|
|
Initiating progestin-only contraception
For patients wishing to use the hormonal IUD, see “Initiating an IUD.”
- Provide adequate counseling to ensure this is the most appropriate option for the patient (see “Approach to initiating contraceptives”).
- Ensure the patient has no contraindications to progestins.
- Determine if the patient requires backup contraception. [6]
- ≤ 5 days from day 0 of LMP: Backup contraception is not required.
- > 5 days from day 0 of LMP: Recommend backup contraception for patients starting POPs.
- > 7 days from day 0 of LMP: Recommend backup contraception for 7 days for patients starting DMPA or implant.
- > 7 days after miscarriage or abortion: Recommend backup contraception for all methods.
- Inform patients about common adverse effects of progestins.
- Ensure patients know what to do if contraception is late or missed.
Adverse effects of progestins [6]
- Irregular menstrual cycles, amenorrhea, breakthrough bleeding
- GI symptoms: abdominal pain, nausea
- Dizziness
- Headaches
- Mood changes
- Breast tenderness
- Follicular cysts (in nonbreastfeeding female individuals)
- Delayed return to fertility (with DMPA use)
Progestin-only contraceptive methods are commonly believed to cause weight gain; however, studies have not shown an association. [52]
Barrier methods of contraception
General principles [53]
- Barrier methods of contraception prevent fertilization by blocking the sperm from reaching an oocyte.
- Condoms provide additional protection against STIs.
- Some forms are available without prescription
- May be used as a primary or adjunctive method of contraception
-
Efficacy can be low.
- Even with perfect use, barrier methods are less effective than hormonal contraception or IUDs.
- Improper application and poor adherence are common and can reduce efficacy further.
Because barrier methods of contraception must be utilized with each sexual encounter, there is a high risk of poor adherence.
Types of barrier methods of contraception [3][4]
Condoms [3][4][6]
- Two types exist:
- External condom: a thin sheath of material (e.g., latex, polyisoprene) that covers the penis [53]
- Internal condom: a thin sheath of material inserted into the vagina (or rectum)
- Prevent most sexually transmitted infections, including HIV (excluding lambskin condoms)
- To avoid breakage or misplacement: [53]
- Use with lubricants (water or silicone-based); oil-based lubricants should never be used with latex condoms
- Avoid simultaneous use of internal and external condoms
- Failure rates
- External condom: perfect use 2%, typical use 18% [4]
- Internal condom: perfect 5%, typical 25% [4]
Ineffective placement is more likely with internal condoms compared to the external condom as insertion may be uncomfortable and difficult for some individuals. [53]
")
Contraceptive diaphragms, sponges, and cervical caps [6]
- Devices placed inside the vagina to prevent semen from reaching the cervix
- Used with spermicide (or contraceptive gel for patients using the contraceptive diaphragm)
- Must remain in place for at least 6 hours after intercourse; can be inserted 6 hours or more prior to intercourse. [6][10]
- Contraindicated in patients with the following characteristics: [6]
- History of toxic shock syndrome
- HIV or at high risk for HIV infection
- Contraceptive diaphragm and caps:< 6 weeks postpartum or post-second trimester abortion
- Adverse effects
- Urinary retention leading to UTI [6]
- Toxic shock syndrome [6]
| Overview of contraceptive diaphragms, sponges, and caps | ||
|---|---|---|
| Description | Failure rate | |
| Contraceptive diaphragm [4][6][10] |
|
|
| Cervical cap [6][10][15] |
|
|
| Contraceptive sponge [4][6] |
|
|
Do not use oil-based lubricants with latex contraceptive diaphragms or caps. [6]


Topical barrier methods [6][54]
- Spermicide and contraceptive gels are placed in the vagina to prevent sperm from reaching the uterus.
- Inserted prior to sexual intercourse, either with other forms of barrier contraception (e.g., contraceptive diaphragm) or alone.
- Advise patients not to douche afterward as this decreases efficacy and increases the risk of STIs.
- Adverse effects include vaginal irritation.
Spermicide [4][6]
- A chemical (usually nonoxynol-9) inserted in the vagina prior to sexual intercourse to damage sperm cells [6]
- Available over the counter as gels, creams, foams, films, and suppositories
- Insertion time prior to intercourse and duration of action vary by formulation. [55]
- Failure rate: perfect use 18%, typical use ∼ 28% [4]
- Use is contraindicated in individuals with HIV or at risk for HIV infection.
Contraceptive gel [54]
- A prescription-only gel inserted into the vagina to create an inhospitable environment for sperm
- Insert up to 1 hour prior to sexual intercourse
- Failure rate: perfect use ∼ 4%, typical use 11–14% [54]
- May be used with condoms and contraceptive diaphragms
- Avoid in individuals with:
- Recurrent urinary tract infections
- Urinary tract abnormalities
- A vaginal ring for contraception
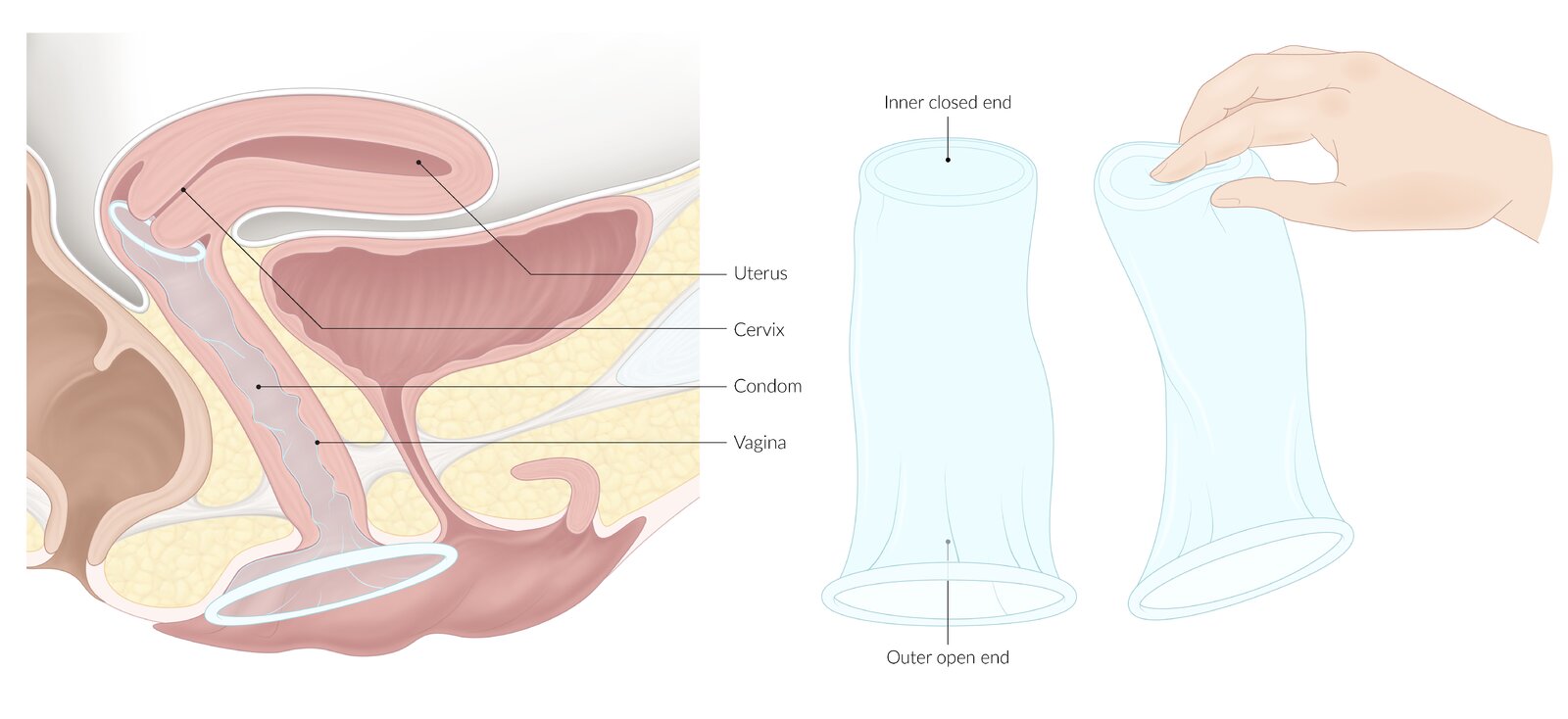
The smaller closed inner ring is placed within the vagina, the larger open-ended outer ring rests outside the vagina on the perineum.
© AMBOSS
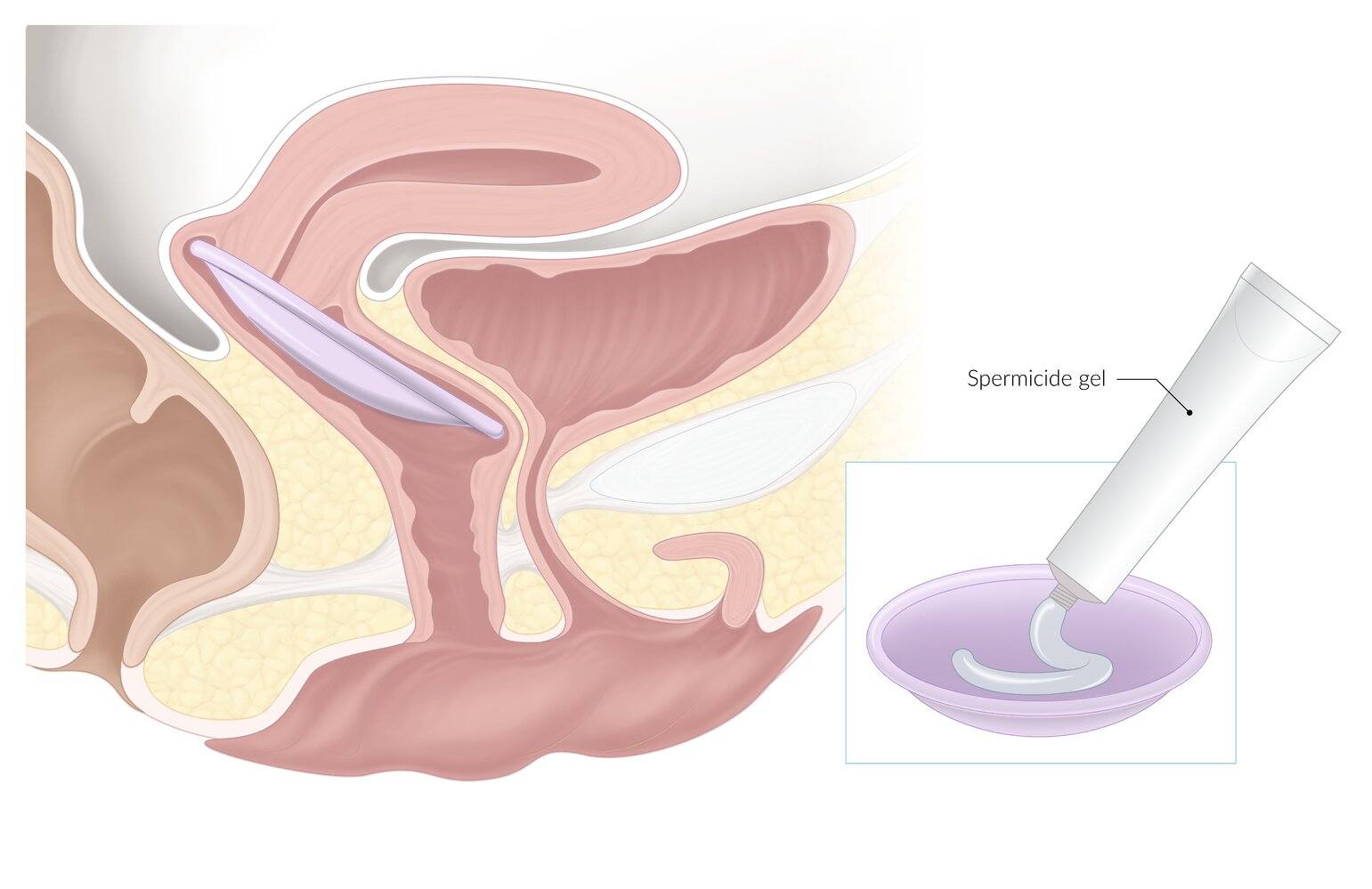
A dome-shaped barrier device that is used in combination with spermicide to prevent pregnancy. The device is placed into the anterior and posterior fornix of the vagina to prevent sperm from entering the cervix.
© AMBOSS
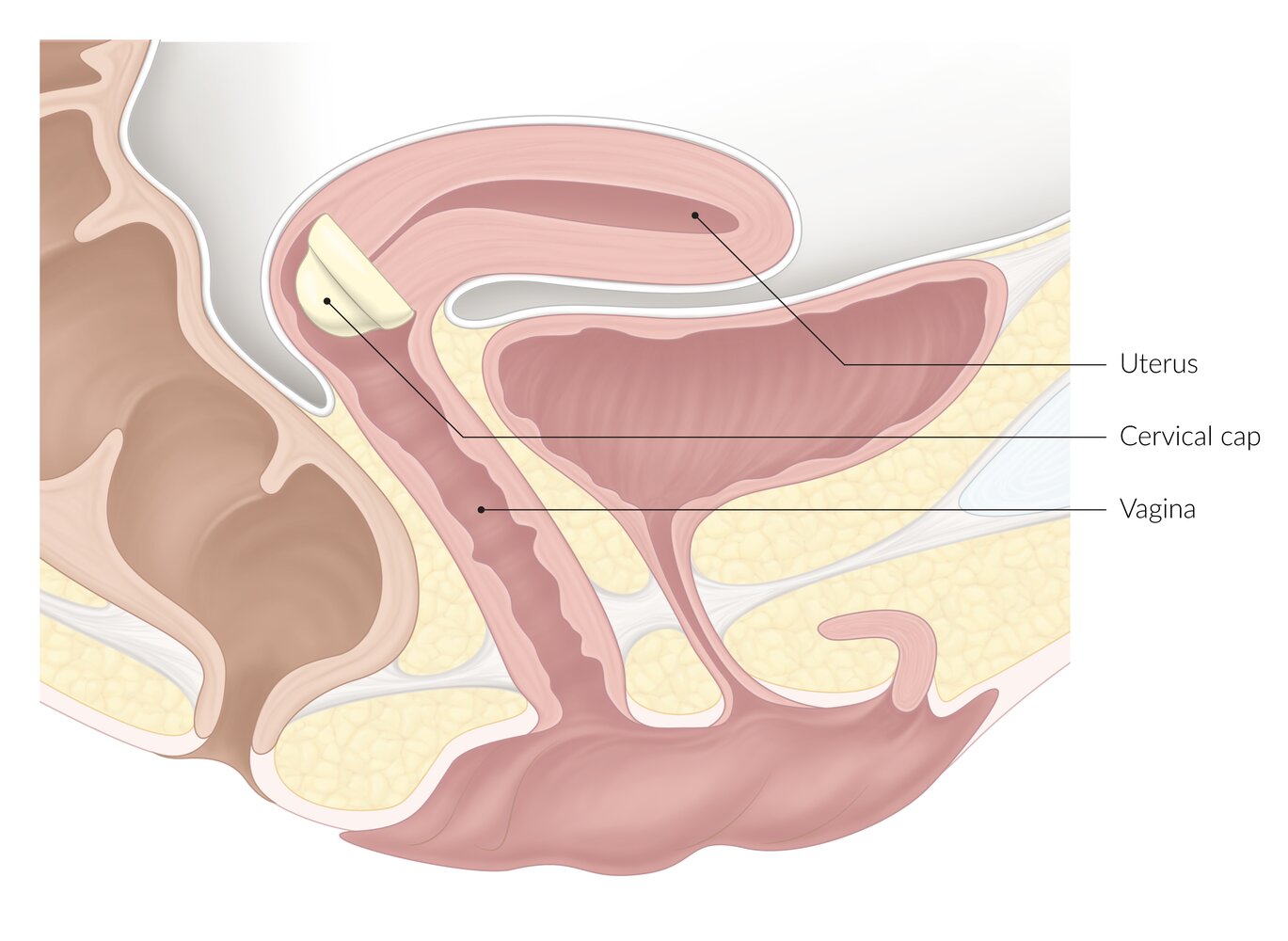
A dome-shaped latex or plastic barrier device that is placed over the cervical os to prevent pregnancy (should be used with spermicide).
© AMBOSS
Behavioral methods of contraception
General principles [6]
- Behavioral methods of contraception are usually less effective than most other methods of contraception.
- Individuals may choose to use behavioral methods of contraception because of:
- A preference for a natural method of contraception
- The desire or need to avoid hormonal contraception
- Cost as behavioral methods are a free form of contraception.
Types of behavioral methods of contraception [4][6]
| Overview of behavioral methods of contraception [4][6] | |||
|---|---|---|---|
|
Description |
Additional information | ||
| Fertility awareness-based methods [4][6] |
|
|
|
| Lactational amenorrhea [4][56] |
|
|
|
| Coitus interruptus [4][6][58] |
|
|
|
Vaginal douching is not recommended as a form of contraception because of limited efficacy and adverse effects including increased risk of STIs, PID, vaginal infections, and ectopic pregnancy. [6][59]

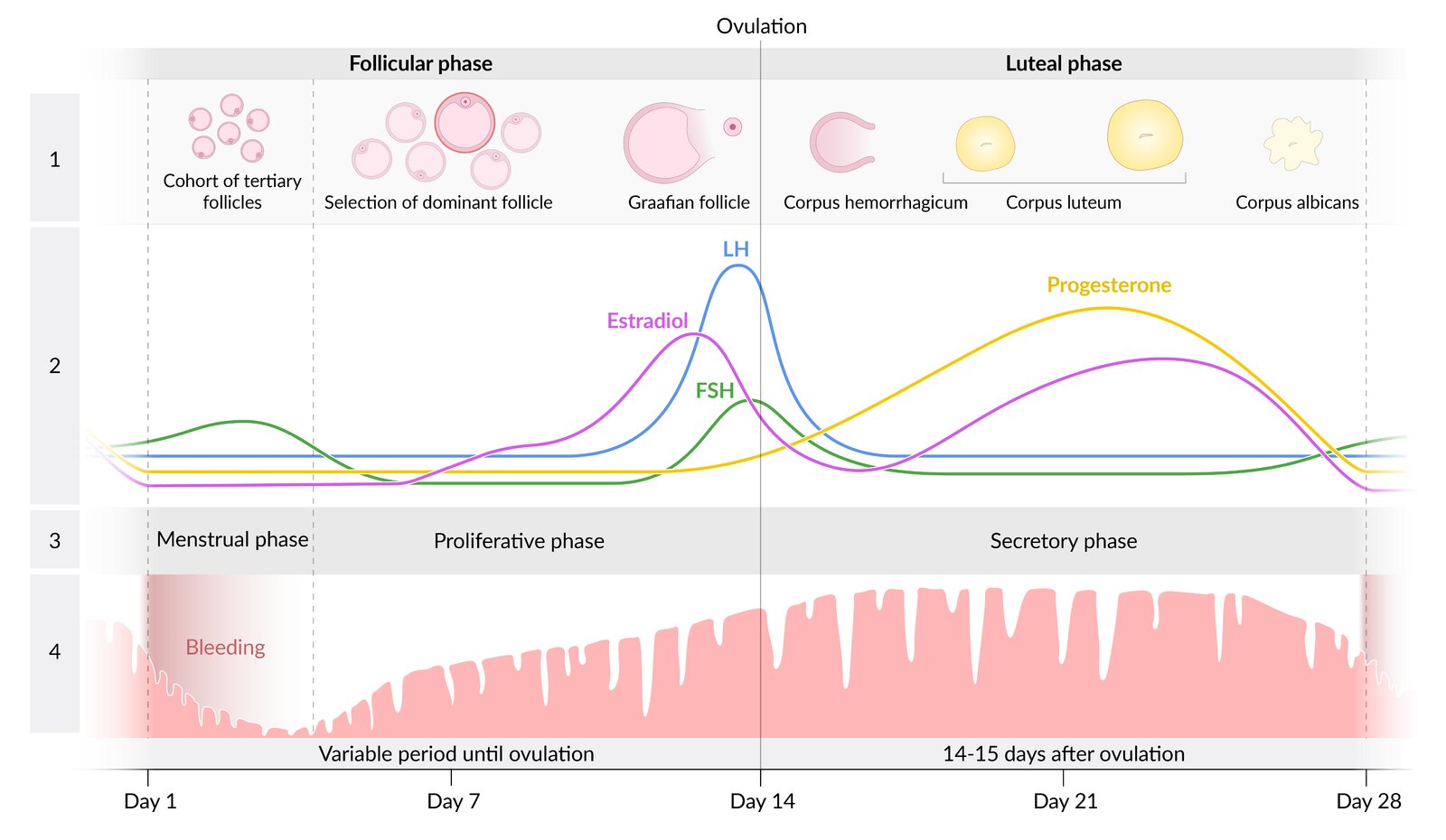
The menstrual cycle consists of two phases: the follicular and the luteal phase. The onset of menses marks the beginning of the follicular phase, which usually lasts 12–14 days but may be variable. The luteal phase begins on the day of ovulation and lasts 14 days.
During the follicular phase, FSH and LH stimulate the development of several follicles, one of which develops as the dominant follicle into the Graafian follicle. An LH surge initiates ovulation. As the oocyte reaches the fallopian tube, the ruptured follicle transforms into the corpus luteum, which produces progesterone. If no pregnancy occurs, the corpus luteum regresses and the progesterone level drops. This drop induces vasospasms in the uterine spiral arteries, ischemia, and sloughing off of the functional endometrial layer, which leads to menstrual bleeding (menstrual phase). During the proliferative phase, the endometrium is built up again in preparation for oocyte implantation during the secretory phase.
1: stages of follicle development; 2: hormone levels; 3: phases of the endometrial cycle; 4: development of the endometrium during the cycle
© AMBOSS
Fertility awareness-based methods
General principles
- Fertility awareness-based methods estimate when a female individual is likely to be ovulating and fertile.
- When used for contraception, individuals avoid unprotected sex during the fertile window to decrease the chance of conception.
- May be based on calendar dates or symptoms suggestive of ovulation
- User dependent; typical use failure rate can be high.
Some patients use mobile apps to track fertility; efficacy for contraception is unclear. [60]
Calendar methods [6][61]
- Description: Count the days since the last menstrual period to estimate when ovulation is likely. [6]
- Basis for method: Ovulation occurs ∼14 days before the next menstrual period. [6]
-
Fertile window: Several methods exist for calculating the fertile window.
- Standard days method: If menstrual cycles are consistently between 26 and 32 days, avoid unprotected intercourse between days 8 and 19. [6]
- Calendar rhythm method: depends on the length of the individual's menstrual cycles [6]
- Start of fertile window: length of shortest menstrual cycle minus 18 days
- End of fertile window: length of longest menstrual cycle minus 11 days
- Failure rate: perfect use 5%, typical use 12% [6]
- Caveat: Use carefully or delay starting calendar methods in individuals without regular menstrual cycles. [6]
Symptom-based methods [6][61]
- Description: : Symptoms (e.g., cervical mucus, body temperature, breast tenderness) related to menstrual cycle hormone fluctuations are used to estimate when ovulation is likely.
-
Caveat: Use carefully or delay starting symptom-based methods in individuals with: [6]
- Recent pregnancy (due to hormonal changes)
- Irregular menstrual cycles
- An acute or chronic condition that alters body temperature
- Medications that alter cervical secretions or body temperature
Cervical mucus methods [6][61]
- Description: Check for cervical mucus at least once a day and monitor changes to estimate when ovulation is likely.
-
Basis for method [61]
- Prior to ovulation, cervical mucus increases and becomes thin, stretchy, and slippery.
- Following ovulation, cervical mucus decreases and becomes thicker and sticky.
-
Fertile window
- TwoDay method: from the onset of cervical mucus until 2 consecutive “dry” days [6]
- Ovulation method: from the onset of cervical mucus until 4 days after the peak of cervical mucus secretions [6]
- Failure rate: perfect use 3–4%, typical use 14–23% [6]
While unprotected intercourse is considered safe between the end of menstruation and before cervical mucus appears, avoid 2 consecutive days of intercourse so that residual semen can disappear and not be confused with cervical mucus. [6]
Basal body temperature method [6][61]
- Description: Measure the body temperature daily upon first awakening to estimate when ovulation is likely.
- Basis for method: After ovulation, the corpus luteum produces progesterone, which increases body temperature by 0.2–0.5°C. [6][62]
- Fertile window: day 1 until 3 days following the temperature increase [6][61]
- Failure rate: no reliable information
- Caveat: affected by conditions that alter body temperature (e.g., fever)
Symptothermal method [6][59][61]
- Description: A combination of the basal body temperature method, cervical mucus method, and other symptoms of ovulation (e.g., breast sensitivity, mittelschmerz) [4]
-
Fertile window: from day 1 of menstruation until both of the following have occurred
- 3 days have passed since the basal body temperature increase
- 4 days after peak cervical mucus [6]
- Failure rate: perfect use < 1%, typical use 2% [6]
Troubleshooting
Discussion of common issues with contraception should be part of contraceptive counseling for all patients. Consider provision of emergency contraception in advance to patients using less reliable methods of contraception. [63]
Management of unscheduled bleeding with contraceptive use
Unscheduled vaginal bleeding may occur with the use of hormonal contraceptives and IUDs. [8][64]
- Reassure patients that irregular bleeding typically improves after 3–6 months. [6][8]
- Ensure contraception is taken as scheduled. [65]
- Work up for underlying pathologies if bleeding is heavy or accompanied by other symptoms. [65]
- If bleeding persists and is bothersome to the patient, provide management based on the method of contraception. [8]
- Copper IUDs: NSAIDS for 5–7 days
-
Progestin implant and DMPA
- NSAIDS for 5–7 days
- Consider oral CHCs or estrogen for 10–20 days. [8]
- POPs: Options are limited; consider drospirenone if not already using. [64][66]
- Cyclic use of CHCs: Adjust the dosages of the estrogen and/or progestin components. [64]
- Extended use or continuous use of CHCs: Hold hormone-containing pills for 3–4 days. [8]
- Consider alternative contraception if irregular or heavy bleeding persists despite appropriate management and is bothersome to the patient.
In individuals with a progestin IUD or progestin implant, heavy or prolonged vaginal bleeding is very uncommon; consider evaluation for an alternative cause. [8]
Missed or delayed contraception
- Determine duration of the missed or delayed contraception.
- For significantly delayed or missed contraception; the following additional contraceptive precautions are generally recommended; follow package insert for specific guidance.
- Restart method immediately.
- Abstain or use barrier contraception for 7 days.
- Consider emergency contraception if the patient has had unprotected sex in the previous 5 days.
| Management recommendations for missed or delayed contraception [8][67] | |
|---|---|
| Method | Missed or delayed contraception |
| Oral contraceptives |
|
| Contraceptive patch |
|
| Combined vaginal ring |
|
| DMPA |
|
Emergency contraception
General principles [6][63][68]
- Emergency contraception is used to prevent pregnancy following unprotected or inadequately protected intercourse.
- Effective for up to 5 days after intercourse
- Works by disrupting ovulation or fertilization
- Not a form of abortion as does not disrupt established pregnancies
- Options include the IUD and emergency contraceptive pills.
- Choice is based on patient weight and preference for ongoing contraception.
Initiation of emergency contraception [8][68][69]
- Obtain a pregnancy test if unable to reasonably exclude pregnancy.
- Discuss available methods with the individual and evaluate for contraindications.
- Preferred (due to efficacy): IUD or ulipristal acetate
- Alternative: levonorgestrel pill (preferably within 72 hours) or Yuzpe regimen [68]
- Preferentially consider placing an IUD for individuals who:
- Desire an IUD for long-term contraception
- Have a BMI ≥ 25 or have a body weight of > 85 kg ≥ 70 kg (≥ 154 lb) [27][63][69]
- If using emergency contraceptive pills, especially the Yuzpe regimen, consider prophylactic antiemetics. [70]
- Provide ongoing management after emergency contraception.
Emergency contraception should be initiated as soon as possible to maximize efficacy. [68]
Types of emergency contraception
IUD for emergency contraception [27]
-
General principles
- The IUD is the most effective method of emergency contraception (≥ 99% efficacy). [2][24][68]
- Efficacy is unaffected by obesity and/or body weight. [63]
- Can provide long-lasting (up to 12 years) contraception
- Timing: within 5 days of unprotected intercourse
- Mechanism of action: prevents fertilization and may affect the oocyte and endometrial lining [68]
- Types of IUDs: copper IUD and progestin IUD (levonorgestrel 52 mg) [24][63]
- Contraindications: See “Contraindications to copper IUD” and “Contraindications to hormonal IUD.” [71]
- Adverse effects: See “Adverse effects and complications of IUDs.”
Emergency contraceptive pills (ECPs) [27][68][69]
-
General principles
- Do not disrupt embryo implantation or established pregnancies
- Significantly less effective in individuals with a BMI ≥ 25 or above a specified weight cut-off [27][63][69]
-
Timing after unprotected intercourse [8]
- Levonorgestrel: most effective when taken within 3 days
- Ulipristal acetate and the Yuzpe regimen can be used within 5 days [27]
-
Types of ECPs
-
Ulipristal acetate (prescription only)
- An antiprogestin that inhibits the progesterone receptor → inhibition or delay of ovulation and decreased endometrial proliferation → impaired fertilization [1][27][72]
- Efficacy: approx. 99% if taken within 5 days of unprotected intercourse [68]
- Repeat dosing in one cycle can be considered using shared decision-making. [63]
-
Levonorgestrel (emergency contraceptive)
- A high dose of progestin delays ovulation and impairs luteal function [27][69][73]
- Efficacy: approx. 98% if given within 3 days of unprotected intercourse [68]
- Available over the counter, without a prescription
- Can be used multiple times in one menstrual cycle [63]
- Use with caution in individuals with a BMI ≥ 25 OR weighing ≥ 70 kg [63]
-
Yuzpe regimen (prescription only) [27][70]
- A combination of ethinyl estradiol and levonorgestrel → inhibits LH and FSH → prevents the estrogen surge → inhibits LH surge → prevents ovulation
- Efficacy: approx. 86% if taken within 5 days
-
Ulipristal acetate (prescription only)
-
Contraindications
- Established pregnancy is the only contraindication.
- Contraindications for hormonal contraceptives do not apply to emergency contraceptives [6][68]
-
Adverse effects of ECPs
- Headache, fatigue, dizziness
- Nausea, vomiting [8]
- Breast tenderness
- Dysmenorrhea, menstrual changes
Ulipristal acetate is the most effective emergency contraceptive pill. [68][69]
All individuals, including those with USMEC contraindications for contraceptive methods, can use ECPs safely and effectively. [6]
Ongoing management after emergency contraception [69]
All patients
- Educate the patient on expected adverse effects.
- Screen for intimate partner violence and sex trafficking. [63][74]
- Recommend a pregnancy test if the next menstrual period is ≥ 1 week after its expected date.
- Offer STI screening.
- For victims of sexual assault: Provide management of recent sexual assault. [68]
Patients with IUDs
- Advise patients to return immediately if the IUD is expelled.
- If patients do not wish to keep the IUD long-term, offer to start immediate hormonal contraception.
Patients who took ECPs
- Offer to initiate or place a referral for a reliable method of contraception.
- If the patient desires hormonal contraception, educate the patient on when they may initiate or resume it.
-
Ulipristal
- Wait 5 days after taking ulipristal
- Use a barrier method of contraception until the next menstrual period. [68]
-
Levonorgestrel or Yuzpe regimen
- Initiate immediately.
- Use a barrier method of contraception for 7 days.
-
Ulipristal
An intrauterine device (IUD) is a small, T-shaped birth control device inserted into the uterus to prevent pregnancy. There are two main types: nonhormonal copper and progestin-releasing. This illustration depicts the correct positioning of an IUD inside the uterus.
© AMBOSS
Special patient groups
Contraception in epilepsy
- See “Epilepsy and contraception.”
Contraception in adolescent individuals [14][75][76]
- Contraception is an important component of adolescent health care.
- Approx. 30% of high school students are sexually active. [75]
- Most pregnancies during adolescence are unintended. [77]
- Allow minors to consent to contraception without parental notification if permitted by state laws.
- Educate adolescents on all forms of contraception and use shared decision-making when initiating contraceptives. [14]
- Avoid barriers to contraceptive use; offer same-day procedures (e.g., implant insertion, IUD placement) if possible. [14]
- Regardless of contraceptive method chosen, emphasize the role of condom use for prevention of STIs. [14]
- When short-acting methods of hormonal contraception are used, encourage the use of automated reminders to improve adherence.
- Regularly scheduled visits to discuss contraception and reproductive and sexual health in adolescents may increase adherence.
- Consider providing adolescents with advance prescription and counseling for emergency contraceptive pills. [70]
Use the initiation of contraception as a prompt to discuss healthy relationships, intimate partner violence, and STI prevention (including HPV vaccination). [14]
Be aware of all local and state laws regarding contraception for adolescents.
Adolescents can purchase progestin-only pills and emergency contraceptive pills over the counter without parents being informed. [14]
Contraception in postpartum individuals [8]
- Progestin-only contraception and IUDs can generally be used throughout the postpartum period.
-
Combined hormonal contraceptives (CHCs) may be contraindicated during the postpartum period depending on:
- Number of days postpartum
- Presence of postpartum risk factors for VTE
- Whether the patient is breastfeeding
- Before prescribing contraception, consider any other contraindications for contraceptive methods.
| Postpartum contraceptive options [8] | |
|---|---|
| Recommendation | |
| < 21 days postpartum |
|
| 21–29 days postpartum |
|
| 30–42 days postpartum |
|
| > 42 days postpartum |
|
If < 21 days postpartum, avoid estrogen-containing OCPs (i.e., CHCs) due to the increased risk of venous thromboembolism. [8]
CHCs can decrease breast milk supply in some individuals; women having difficulties with breastfeeding may wish to consider alternative contraceptive options. [8]
Contraception after spontaneous or induced abortion [6][78]
- All methods of contraception are safe to use immediately in the absence of other contraindications for contraceptive methods. [8]
- IUD expulsion rates may be elevated. [78]
- If contraception is initiated > 7 days after miscarriage or abortion, backup contraception is recommended (unless a copper IUD has been placed). [6]
Contraception and menopause
See “Contraception during perimenopause.”
Contraception in transgender and nonbinary individuals [2][79]
See “Reproductive health care for transgender individuals.”
Contraception for underserved individuals
Patients can consider contraceptive methods available without prescription:
- Condoms
- Spermicide
- Contraceptive sponge
- Levonorgestrel emergency contraceptive pill
- Behavioral contraceptive methods
- Norgestrel progesterone-only pill
Related One-Minute Telegram
- One-Minute Telegram 82-2023-3/3: COX blocking to prevent unwanted pregnancy
External Resources
- 2025 AAP Policy Statement: Contraception for Adolescents
- 2025 ACOG Clinical Consensus No. 9: Pain Management for In-Office Uterine and Cervical Procedures
- 2024 U.S. Medical Eligibility Criteria for Contraceptive Use
- 2024 ACOG Practice Bulletin 8: Permanent Contraception: Ethical Issues and Considerations
- 2023 Society of Family Planning: Emergency Contraception
- 2022 WHO Family Planning Global Handbook for Providers
- 2022 Society of Family Planning: Extended use of long-acting reversible contraception
- 2022 ACOG Practice Bulletin 1: Patient-Centered Contraceptive Counseling
- 2017 ACOG Practice Bulletin 186: Long-Acting Reversible Contraception: Implants and Intrauterine Devices
- U.S. Selected Practice Recommendations for Contraceptive Use, 2016
- USMEC contraception app
- CDC Contraception app
References
- Nguyen AT, Curtis KM, Tepper NK, et al. "U.S. Medical Eligibility Criteria for Contraceptive Use, 2024". MMWR Recomm Rep. 73(4). :1-126. (2024)
- "Family Planning: A Global Handbook for Providers"
- Curtis KM, Jatlaoui TC, Tepper NK, et al. "U.S. Selected Practice Recommendations for Contraceptive Use, 2016". MMWR Morb Mortal Wkly Rep. 65(4). :1-66. (2016)
- "CDC USMEC USSPR Contraception App". https://web.archive.org/web/20230128132619/https://www.cdc.gov/reproductivehealth/contraception/contraception-app.html. [2022-05-19]
- Clark EA, Curtis KM. "Contraception Recommendations: Updates for the Busy Clinician". Am Fam Physician. 106(3). :227-228. (2022)
- Teal S, Edelman A. "Contraception Selection, Effectiveness, and Adverse Effects". JAMA. 326(24). :2507. (2021)
- ACOG. "Practice Bulletin No. 110: Noncontraceptive Uses of Hormonal Contraceptives". Obstet Gynecol. 115(1). :206-218. (2010)
- ACOG. "General Approaches to Medical Management of Menstrual Suppression". Obstetrics & Gynecology. 140(3). :528-541. (2022)
- Paradise SL, Landis CA, Klein DA. "Evidence-Based Contraception: Common Questions and Answers". Am Fam Physician. 106(3). :251-259. (2022)
- "Reproductive Health - Contraception - How Effective Are Birth Control Methods?". https://web.archive.org/web/20170701080150/https://www.cdc.gov/reproductivehealth/contraception/index.htm. [2017-02-09]
- Trussell J. "Contraceptive failure in the United States". Contraception. 83(5). :397-404. (2011)
- ACOG. "Practice Bulletin No. 186: Long-Acting Reversible Contraception: Implants and Intrauterine Devices". Obstet Gynecol. 130(5). :e251-e269. (2017)
- Dethier D, Qasba N, Kaneshiro B. "Society of Family Planning clinical recommendation: Extended use of long-acting reversible contraception". Contraception. 113. :13-18. (2022)
- ACOG. "Committee Opinion No. 602: Depot medroxyprogesterone acetate and bone effects". Obstet Gynecol. 123(6). :1398-1402. (2014)
- Gallo MF, Et. Al. "Cervical cap versus diaphragm for contraception". Cochrane Database of Systematic Reviews. 2012(5). (2002)
- Sundaram A, Vaughan B, Kost K, et al. "Contraceptive Failure in the United States: Estimates from the 2006-2010 National Survey of Family Growth". Perspect Sex Reprod Health. 49(1). :7-16. (2017)
- Ott MA, Sucato GS, Leroy-Melamed M, et al. "Contraceptive Counseling and Methods for Adolescents: Clinical Report". Pediatrics. 156(1). (2025)
- ACOG. "Committee Opinion No. 710: Counseling Adolescents About Contraception.". Obstet Gynecol. 130(2). :e74-e80. (2017)
- Ott MA, Hoopes AJ, Sucato GS, et al. "Contraception for Adolescents: AAP Policy Statement". Pediatrics. (2025)
- AAP. "Options Counseling for the Pregnant Adolescent Patient". Pediatrics. 150(3). (2022)
- Upadhya KK, Breuner CC, Alderman EM, et al. "Emergency Contraception". Pediatrics. 144(6). (2019)
- ACOG. "Access to Postabortion Contraception". Obstet Gynecol. 138(2). :e91-e95. (2021)
- ACOG. "Health Care for Transgender and Gender Diverse Individuals". Obstet Gynecol. 137(3). :e75-e88. (2021)
- Lesnewski R. "Initiating Hormonal Contraception". Am Fam Physician. 103(5). :291-300. (2021)
- ACOG. "Patient-Centered Contraceptive Counseling". Obstet Gynecol. 139(2). :350-353. (2022)
- Turok DK, Gero A, Simmons RG, et al. "Levonorgestrel vs. Copper Intrauterine Devices for Emergency Contraception". N Engl J Med. 384(4). :335-344. (2021)
- Averbach S, Hofler L. "Long-Acting Reversible Contraception With Contraceptive Implants and Intrauterine Devices". JAMA. 327(20). :2013. (2022)
- Minalt N, Caldwell A, Yedlicka GM, et al. "Association between intrauterine device use and endometrial, cervical, and ovarian cancer: an expert review". Am J Obstet Gynecol. 229(2). :93-100. (2023)
- Bosworth MC, Olusola PL, Low SB. "An update on emergency contraception.". Am Fam Physician. 89(7). :545-50. (2014)
- ACOG. "Pain Management for In-Office Uterine and Cervical Procedures". Obstet Gynecol. (2025)
- Curtis KM, Nguyen AT, Tepper NK, et al. "U.S. Selected Practice Recommendations for Contraceptive Use, 2024". MMWR. Recomm Rep. 73(3). :1-77. (2024)
- Fay KE, Clement AC, Gero A, et al. "Rates of pregnancy among levonorgestrel and copper intrauterine emergency contraception initiators: Implications for backup contraception recommendations". Contraception. 104(5). :561-566. (2021)
- Juliana Melo, Mary Tschann, Reni Soon, Melissa Kuwahara, Bliss Kaneshiro. "Women's willingness and ability to feel the strings of their intrauterine device". Int J Gynaecol Obstet. 137(3). :309-313. (2017)
- Reed SD, Zhou X, Ichikawa L, et al. "Intrauterine device-related uterine perforation incidence and risk (APEX-IUD): a large multisite cohort study". Lancet. 399(10341). :2103-2112. (2022)
- McNeilly AS, Tay CC, Glasier A. "Physiological mechanisms underlying lactational amenorrhea.". Ann N Y Acad Sci. 709. :145-55. (1994)
- McNeilly AS. "Neuroendocrine changes and fertility in breast-feeding women". Prog Brain Res. :207-214. (2001)
- Woods JL, et al. "Contraceptive Withdrawal in Adolescents: A Complex Picture of Usage". J Pediatr Adolesc Gynecol. 22(4). :233-237. (2009)
- J. L. Martino. "Vaginal Douching: Evidence for Risks or Benefits to Women's Health". Epidemiol Rev. 24(2). :109-124. (2002)
- Colquitt CW, Martin TS. "Contraceptive Methods". Int J Pharm Pract. 30(1). :130-135. (2016)
- Steinberg J, Lynch SE. "Lactic Acid, Citric Acid, and Potassium Bitartrate (Phexxi) Vaginal Gel for Contraception.". Am Fam Physician. 103(10). :628-629. (2021)
- Chappell BT, Griffin BL, Howard B. "Mechanisms of action of currently available woman-controlled, vaginally administered, non-hormonal contraceptive products". Ther Adv Reprod Health. 16. :263349412211071. (2022)
- ACOG. "Permanent Contraception: Ethical Issues and Considerations". Obstet Gynecol. 143(2). :e31-e39. (2024)
- ACOG committee on practice bulletins. "ACOG Practice Bulletin No. 208: Benefits and Risks of Sterilization". Obstet Gynecol. 133(3). :e194-e207. (2019)
- ACOG. "Committee Opinion No. 695: Sterilization of Women: Ethical Issues and Considerations.". Obstet Gynecol. 129(4). :e109-e116. (2017)
- Cheng L, MacLennan GT, Bostwick DG. "Urologic Surgical Pathology". Saunders. (2019). ISBN: 9780323549417
- Salcedo J, Cleland K, Bartz D, Thompson I. "Society of Family Planning Clinical Recommendation: Emergency contraception". Contraception. 121. :109958. (2023)
- American College of Obstetricians and Gynecologists. "Emergency Contraception". Obstetrics & Gynecology. 126(3). :e1-e11. (2015)
- American College of Obstetricians and Gynecologists. "Access to Emergency Contraception". Obstetrics & Gynecology. 130(1). :251-252. (2017)
- Koyama A, Hagopian L, Linden J. "Emerging Options for Emergency Contraception". Clin Med Insights Reprod Health. 7. :CMRH.S8145. (2013)
- Snow SE, Melillo SN, Jarvis CI. "Ulipristal Acetate for Emergency Contraception". Ann Pharmacother. 45(6). :780-786. (2011)
- Matyanga CMJ, Dzingirai B. "Clinical Pharmacology of Hormonal Emergency Contraceptive Pills". Int J Reprod Med. 2018. :1-5. (2018)
- Lewis NV, Moore THM, Feder GS, Macleod J, Whiting P. "Use of emergency contraception among women with experience of domestic violence and abuse: a systematic review". BMC Womens Health. 18(1). (2018)
- Bonnema RA, McNamara MC, Spencer AL. "Contraception choices in women with underlying medical conditions.". Am Fam Physician. 82(6). :621-8. (2010)
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Gynecology. "ACOG Practice Bulletin No. 228: Management of Symptomatic Uterine Leiomyomas (reaffirmed 2025)". Obstet Gynecol. 137(6). :e100-e115. (2021)
- Lyall M, de Oliveira BR, Mody SK. "Considerations for Contraceptive Use Among Patients with Migraines". Curr Obstet Gynecol Rep. 12(2). :57-63. (2023)
- Johnson J. "Evaluation of extended and continuous use oral contraceptives". Ther Clin Risk Manag. Volume 4. :905-911. (2008)
- ACOG. "ACOG Practice Bulletin No. 206: Use of Hormonal Contraception in Women With Coexisting Medical Conditions". Obstet Gynecol. 133(2). :e128-e150. (2019)
- Gialeraki A, Valsami S, Pittaras T, Panayiotakopoulos G, Politou M. "Oral Contraceptives and HRT Risk of Thrombosis". Clin Appl Thromb Hemost. 24(2). :217-225. (2017)
- Faculty of Sexual and Reproductive Health. "FSRH Guideline (January 2019, amended October 2023) Combined Hormonal Contraception". BMJ Sex Reprod Health. 45(Suppl 1). :1-93. (2019)
- Al-Haddad S, Branham KKR, Clare CA. "Advances in contraception: vaginal contraceptive rings". Ther Adv Reprod Health. 17. (2023)
- Damm T, Lamvu G, Carrillo J, Ouyang C, Feranec J. "Continuous vs. cyclic combined hormonal contraceptives for treatment of dysmenorrhea: a systematic review". Contracept X. 1. :100002. (2019)
- Kang A, Khokale R, Awolumate OJ, Fayyaz H, Cancarevic I. "Is Estrogen a Curse or a Blessing in Disguise? Role of Estrogen in Gastroesophageal Reflux Disease". Cureus. (2020)
- Trenor CC, Chung RJ, Michelson AD et al. "Hormonal contraception and thrombotic risk: a multidisciplinary approach". Pediatrics. 127(2). :347-357. (2011)
- Haring MPD, Gouw ASH, de Haas RJ, et al. "The effect of oral contraceptive pill cessation on hepatocellular adenoma diameter: A retrospective cohort study". Liver Int. 39(5). :905-913. (2019)
- Gallo MF, Lopez LM, Grimes DA, et al. "Combination contraceptives: effects on weight". Cochrane Database Syst Rev. 2014(1). (2014)
- Palacios S, Colli E, Regidor PA. "Bleeding profile of women using a drospirenone-only pill 4 mg over nine cycles in comparison with desogestrel 0.075 mg". PLoS ONE. 15(6). :e0231856. (2020)
- Fleurant E, Mokashi M, Simon MA. "Over-the-Counter Progestin-Only Oral Contraceptives". JAMA. (2023)
- Fraser I, Weisberg E. "Contraception and endometriosis: challenges, efficacy, and therapeutic importance". Open Access J Contracept. :105. (2015)
- "Calcium Fact Sheet for Health Professionals". https://web.archive.org/web/20231011185652/https://ods.od.nih.gov/factsheets/calcium-HealthProfessional/. [2022-10-06]
- Lopez LM, Ramesh S, Chen M, et al. "Progestin-only contraceptives: effects on weight". Cochrane Database Syst Rev. 2016(8). (2016)
- Earle S, Marston HR, Hadley R, Banks D. "Use of menstruation and fertility app trackers: a scoping review of the evidence". BMJ Sex Reprod Health. 47(2). :90-101. (2020)
- "ACOG fertility awareness based methods". https://web.archive.org/web/20231002102423/https://www.acog.org/womens-health/faqs/fertility-awareness-based-methods-of-family-planning
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Allen R, Villavicencio J. "Unscheduled bleeding and contraceptive choice: increasing satisfaction and continuation rates". Open Access J Contracept. :43. (2016)
- Schrager S. "Abnormal uterine bleeding associated with hormonal contraception". Am Fam Physician. 65(10). :2073-80. (2002)
- Archer DF, Mansour D, Foidart JM. "Bleeding Patterns of Oral Contraceptives with a Cyclic Dosing Regimen: An Overview". J Clin Med. 11(15). :4634. (2022)
- World Health Organization Department of Reproductive Health and Research (WHO/RHR) and Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs (CCP), Knowledge for Health Project.. "Family Planning - A global handbook for providers". WHO. (2018). ISBN: 9780999203705
- The American College of Obstetricians and Gynecologists. "ACOG Practice Bulletin No. 212: Pregnancy and Heart Disease". Obstetrics & Gynecology. 133(5). :e320-e356. (2019)
- American College of Obstetricians and Gynecologists’ Committee on Adolescent Health Care. "Gynecologic Considerations for Adolescents and Young Women With Cardiac Conditions". Obstet Gynecol. 136(5). :e90-e99. (2020)