Summary
The cornea is the external, transparent layer of the eye covering the iris and pupil. The cornea is highly sensitive, and corneal disorders (e.g., abrasions, infection, erosion, ulcers, foreign bodies) are often painful and associated with reduced visual acuity. Diagnosis is most commonly clinical, based on slit lamp examination with fluorescein staining. Treatment includes supportive care (including analgesics) and foreign body removal, if present. Topical antibiotics may be used, e.g., in corneal abrasions and corneal ulcers. Therapeutic contact lenses are used in keratoconus. Keratoplasty (corneal transplantation) is generally a last resort for patients with significant visual impairment or failed treatment for infection.
For inflammatory disorders of the cornea, see “Conjunctivitis” and “Keratitis.”
Anatomy of the cornea

Also see “Cornea” in “Eye and orbit.”
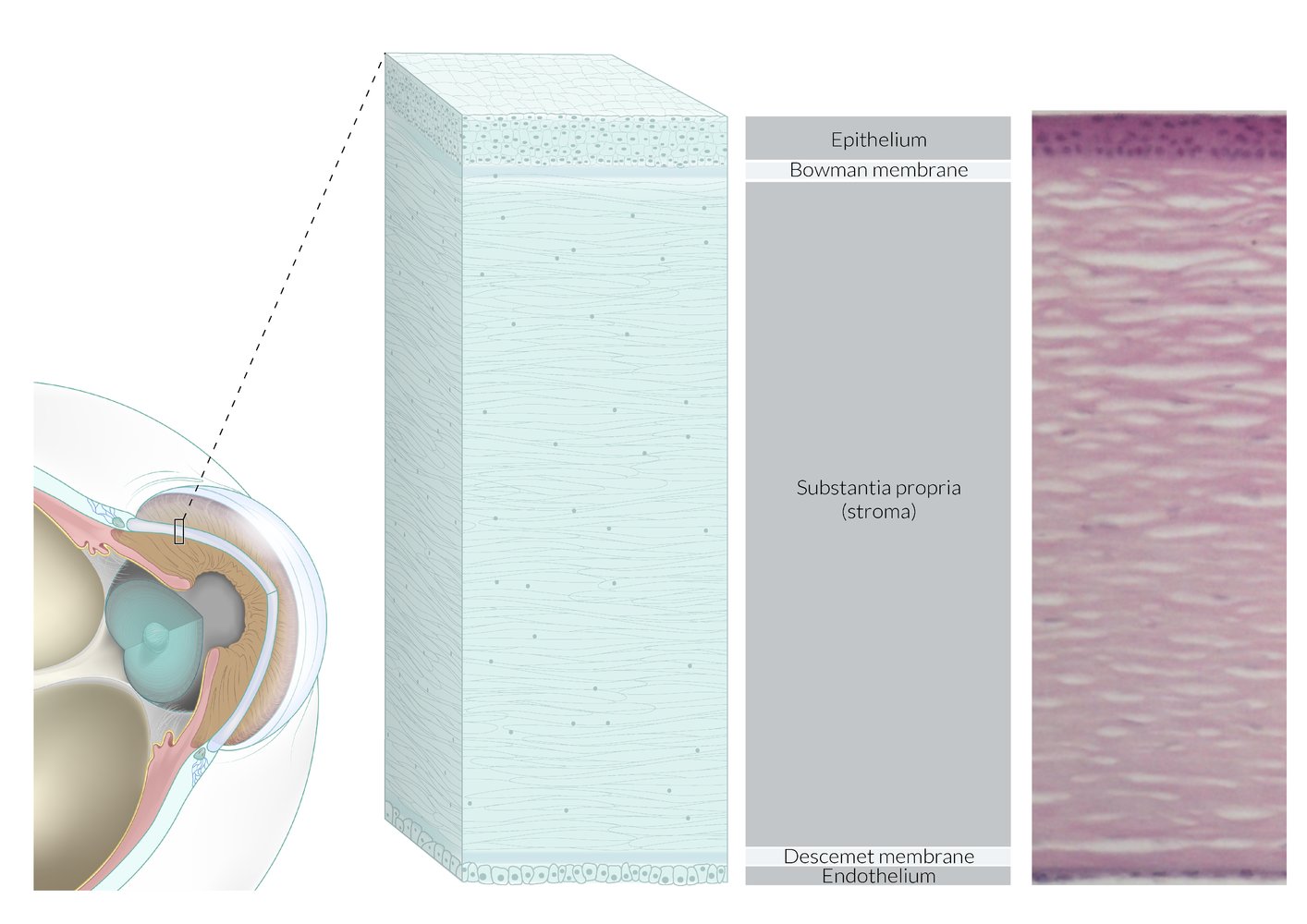
The sclera and cornea form the fibrous tunic of the eyeball. The cornea is composed of five layers (anterior to posterior): corneal epithelium (stratified squamous, nonkeratizing epithelium), Bowman membrane (collagen fibrils, no cells), substantia propria (collagen fibers, fibroblasts, proteoglycans, and water), Descemet membrane (basement membrane), and endothelium (single layer of squamous cells).
© AMBOSS
Corneal abrasion
Definition [1]
A defect in the epithelial surface of the cornea caused by trauma
Etiology [2]
- Direct injury (e.g., scratch from fingernail or makeup brush)
- Foreign body under the eyelid
- Prolonged contact lens wear or improperly fitted lenses
- Entropion
- Trachoma
Clinical features [1][2]
- Foreign body sensation in the eye
- Eye pain
- Epiphora
- Photophobia
- Blurred vision
- Conjunctival injection
Diagnostics [1][2]
- Corneal abrasion is a clinical diagnosis.
- Perform a thorough eye examination, including slit lamp examination with fluorescein staining.
- Characteristic findings on slit lamp examination include:
- Traumatic injury: linear or geographic shapes
- Contact lens-related: round, central defect composed of punctate lesions
- Foreign body under eyelid: multiple vertical lines
Resolution of pain with local anesthetic in the setting of superficial eye injury suggests corneal abrasion. [2]
Exclude open globe injury and corneal foreign bodies in all patients with corneal abrasion.



Management [1][2]
- Remove foreign body from the cornea and/or eyelid if present.
-
Provide analgesia for corneal pain. [3][4]
- Oral NSAIDs: mild to moderate pain
- Topical NSAIDs, e.g., ketorolac (off-label) [1]
- Systemic opioid analgesics: severe pain [1][2]
- Consider prophylactic topical antibiotics for:
- Deep or potentially contaminated abrasions (e.g., erythromycin ) [1][2]
- Contact lens wearers or immunocompromise: antibiotics with antipseudomonal activity, e.g., ciprofloxacin (off-label) [1][2]
- Consider short-term (i.e., < 24 hours) topical anesthetics (e.g., tetracaine) with caution. [5][6][7]
- Avoid eye patches. [3][8]
Limit use of topical NSAIDs to 2–3 days due to risk of corneal toxicity. [1]
Disposition [1][2]
- Consult ophthalmology urgently for:
- Signs of active infection (e.g., corneal infiltrate)
- Corneal ulcer
- Evidence of open globe injury
- Hypopyon or hyphema
- Retained foreign body
- Chemical burns
- Arrange follow-up in 24 hours if corneal abrasion is > 4 mm, contact lens-related, or accompanied by a decrease in visual acuity.
- Refer to ophthalmology if symptoms have not improved at follow-up.
Complications [1][2]
- Infection (e.g., bacterial keratitis)
- Corneal ulcer
- Traumatic iritis
- Recurrent corneal erosion
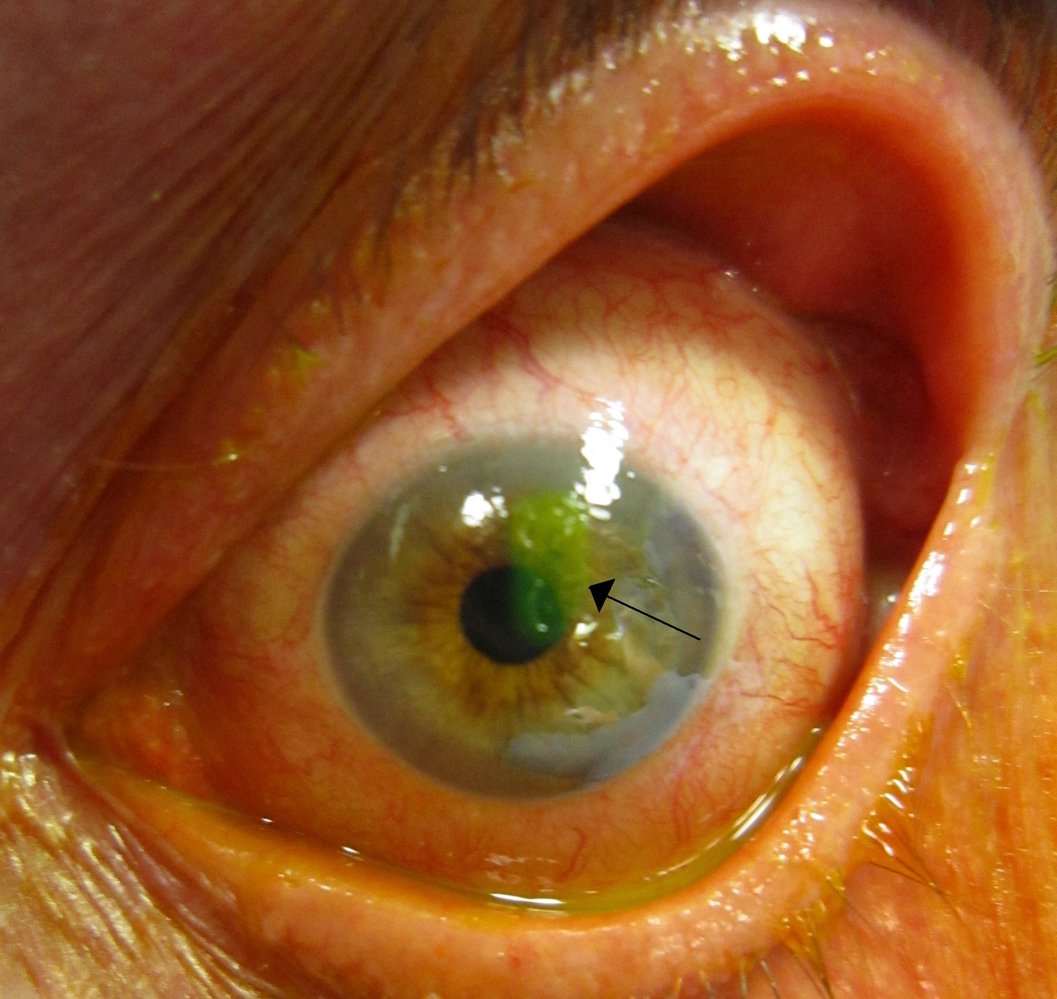
Slit-lamp photography of the left eye with fluorescein staining
A small area of green staining (black arrow) confirms a corneal abrasion. Significant conjunctival injection is also visible.
Source: “Human cornea with abrasion highlighted by fluorescein staining” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 3.0.
{kind=link}
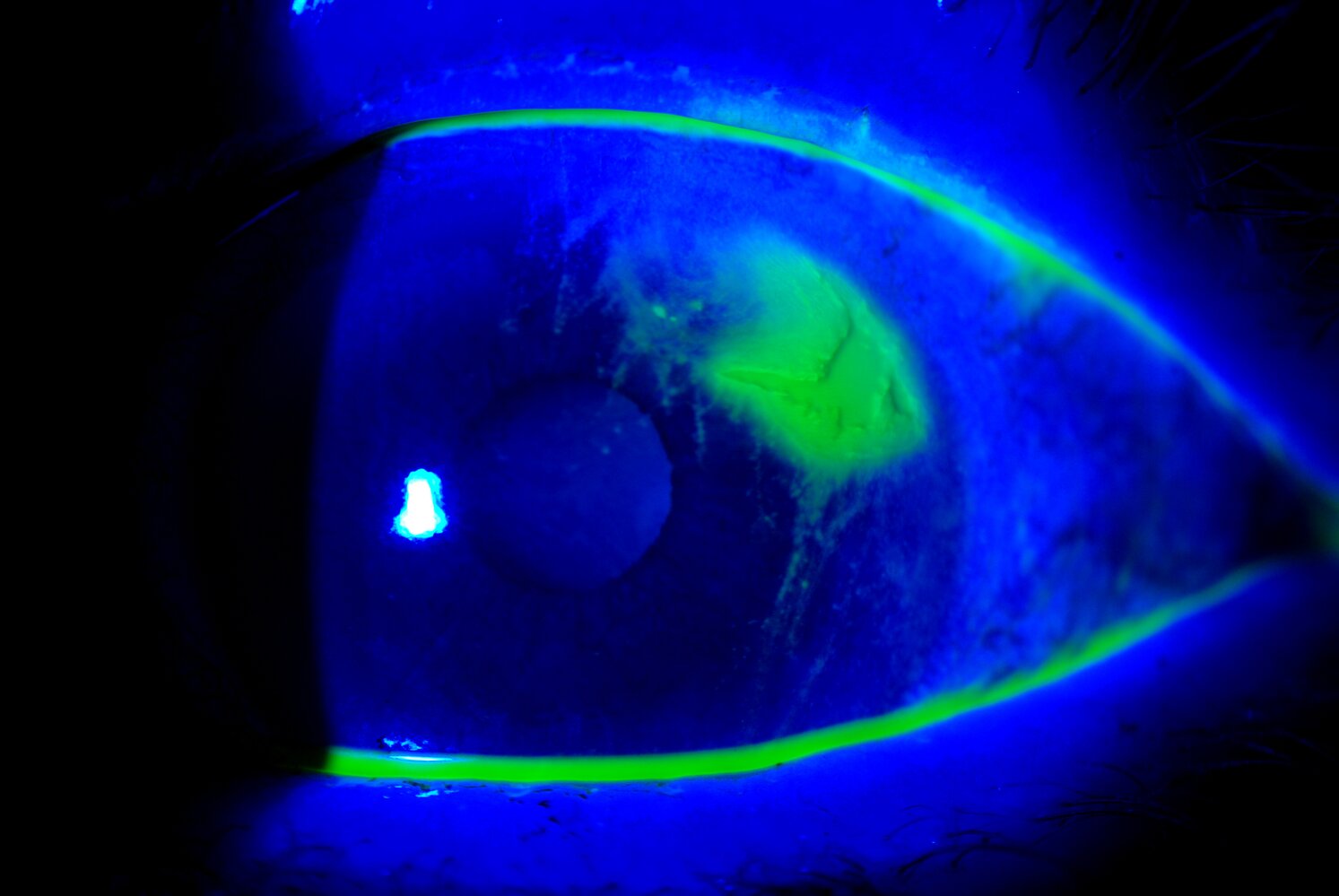
Slit-lamp photography of the left eye with fluorescein staining and blue light
An irregularly shaped corneal abrasion, clearly highlighted by the yellow-green fluorescein stain, is visible. Faintly stained scratch marks (indicated by white overlay and line) can be seen around the abrasion (marked by dotted line).
The irregular shape of the defect and the scratch marks indicate an upper subtarsal foreign body as the underlying cause. Upper eyelid ectropionization is required to confirm the diagnosis and for immediate treatment.
This image is an adaptation. Source of original image: Retina Gallery. Original title: “49487_009”. Created by: Mayo Clinic Jacksonville, Florida. Licensed under Public Domain. Modifications to original image: removal of the date in the lower left corner.

Corneal abrasion on fluorescein staining
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
Corneal laceration
For full-thickness lacerations, see “Open globe injury.” [2][9]
- Definition: traumatic corneal defect caused by a sharp object
- Diagnostics: slit lamp examination to exclude full-thickness defects and foreign bodies [2]
-
Management
- Consult ophthalmology urgently.
- Conservative management of small, superficial lesions is similar to that of corneal abrasions.
- Deeper or more extensive lesions may require surgical repair.
Corneal foreign body
Etiology [1][2]
-
Most commonly results from dust or debris blown into the eye during:
- High-risk activities without adequate protective eyewear, e.g., grinding, drilling, sawing, welding, mowing
- Exposure to high winds
Clinical features [1][2]
- History of sudden onset and persistent discomfort following trauma
- Signs of ocular inflammation: copious tearing, redness, foreign body sensation, difficulty keeping the eye open, photophobia, and blurred vision
Diagnostics [1][2]
- Perform a thorough eye examination, including slit lamp examination, evaluation for open globe injury, and eversion of the upper eyelid.
- Characteristic findings on examination include:
- Visible foreign body
- Rust rings
- Corneal defect without visible foreign body
- If no foreign body is seen but suspicion of penetrating injury is high, obtain imaging (e.g., orbital CT scan or ultrasound). [10]
Corneal foreign bodies that penetrate the full thickness of the cornea should be considered as open globe injuries that require urgent ophthalmology consultation. [2]
MRI is contraindicated for the evaluation of suspected metallic foreign bodies.


Management [2][10]
Corneal foreign body removal
Utilize a stepwise approach from the least to most invasive technique.
- Administer a topical anesthetic (e.g. tetracaine )
- Irrigate the affected eye copiously with saline.
- Sweep a moist cotton swab over the object and cornea.
- Attempt removal with a 25–27 gauge needle, corneal spud, or burr drill.
- Ask the patient to look at a distant object to stabilize the eye.
- Visualize the foreign body using magnification (e.g., loupes, slit lamp).
- Hold the instrument tangential to the cornea.
- If using a needle or corneal spud: Scoop or pick up the foreign body with the instrument.
- If using a burr drill: Hold the burr against the foreign body until removed.
- Residual rust rings may be removed during initial presentation or after 24–48 hours.
Do not attempt to remove the foreign body if an open globe injury is suspected.
Supportive treatment [1][2][10]
-
Tetanus prophylaxis
- Indicated for penetrating eye injury
- Consider for potentially contaminated foreign bodies, concomitant chemical burns, or tissue necrosis
- Analgesia and antibiotic prophylaxis: See “Corneal abrasion” for indications and recommendations.
Disposition [1][2]
- Consult ophthalmology urgently for:
- Suspected open globe injury
- Inability to remove a foreign body
- Large or deep foreign bodies
- Foreign bodies affecting the central field of vision
- See also “Corneal abrasion.”
Complications [1][2][10]
Complications from a corneal foreign body are rare but may include:
- Corneal abrasion
- Open globe injury
- Secondary iritis [11]
- Rust rings may delay corneal healing and/or impair visual acuity (if centrally located).

Right eye
A small brown foreign body (arrowhead) and a slight rust ring can be seen on the temporal corneal margin. Significant conjunctival injections are also visible.
Source: “Foreign body in eye” by E van Herk, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Slit-lamp photography of the right eye (fluorescein stain) of an individual with tearing and redness after working with a grinding wheel
The paracentral cornea shows a brown rust ring (green overlay). The small brownish flecks are iris nevi (example indicated by arrowhead).
Rust rings develop from metallic foreign bodies of the cornea that are not removed promptly.
Source: "51434_001.JPG", Mayo Clinic Jacksonville, Florida, Retina Gallery licensed under Public Domain
Corneal erosion
-
Definition [12]
- Detachment of the corneal epithelium from the tissue layers below, including the basement membrane and Bowman membrane
- Recurrent corneal erosion: chronic relapsing corneal erosion
-
Etiology [13]
- Spontaneous due to lack of regenerative capacity of the cornea, associated with the following risk factors:
- Corneal dystrophy
- Corneal ulcers (e.g., from herpes simplex keratitis )
- Contact lens use, especially if poorly fitted
- Diabetes mellitus
- Dry eye disease
- Secondary to injury of the cornea (e.g., corneal abrasion, entropion)
- Spontaneous due to lack of regenerative capacity of the cornea, associated with the following risk factors:
- Clinical findings: sudden-onset symptoms similar to those of corneal abrasion, typically upon waking or without obvious signs of ocular trauma.
- Diagnostics: See “Corneal abrasion.”
-
Treatment [1]
- Acute (within 24 hours of symptom onset)
- As with corneal abrasion
- Artificial tears and nightly lubricant eye drops
- Recurrent corneal erosion or symptoms > 24 hours
- Specialized ophthalmological treatment may include the following [14]
- Therapeutic contact lenses
- Stromal micropuncture
- Corneal epithelial debridement and/or phototherapeutic keratectomy
- Specialized ophthalmological treatment may include the following [14]
- Acute (within 24 hours of symptom onset)
-
Prognosis
- Excellent, provided diagnosis and treatment are initiated promptly
- Complete healing of recurrent corneal erosion may take years.

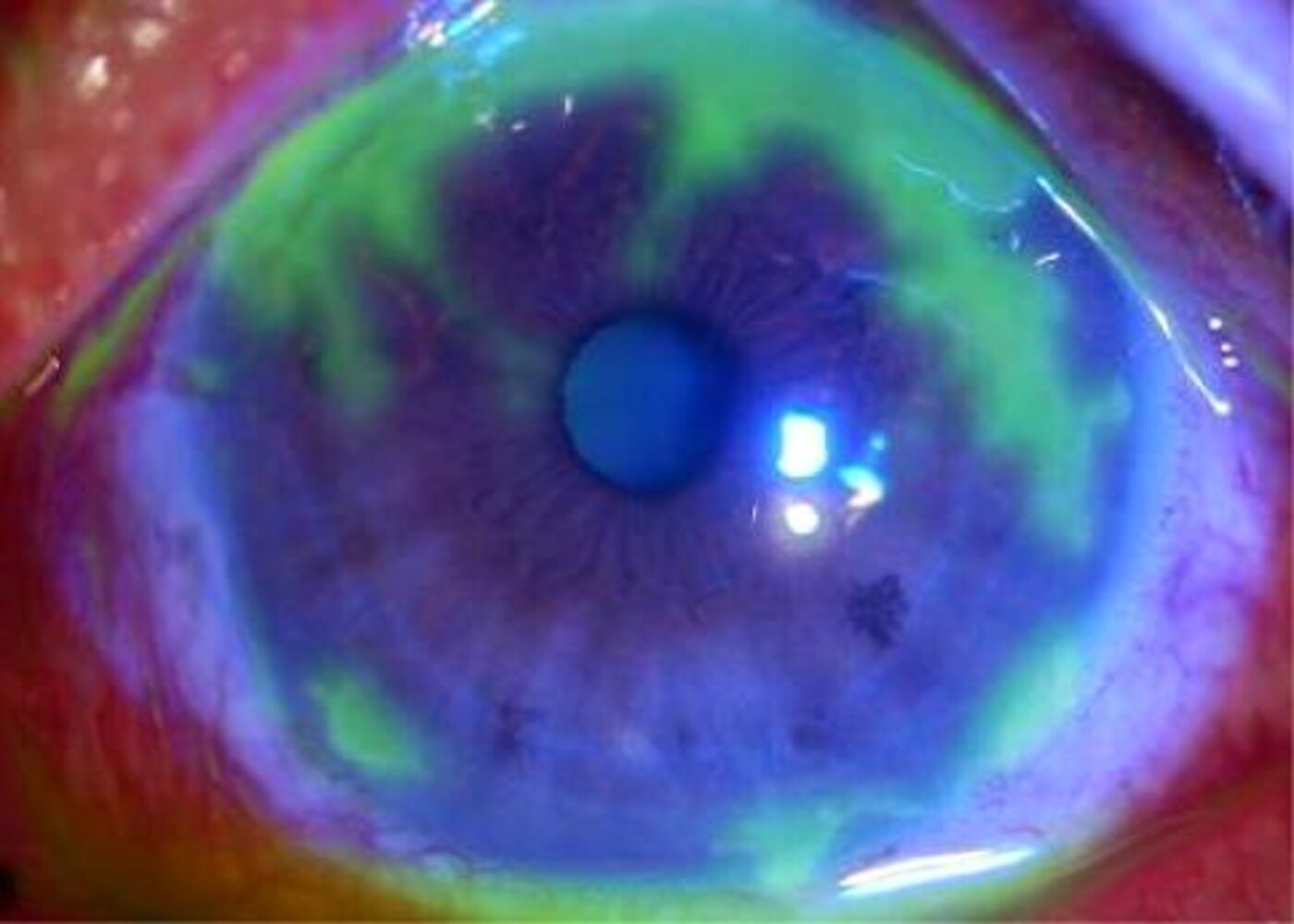
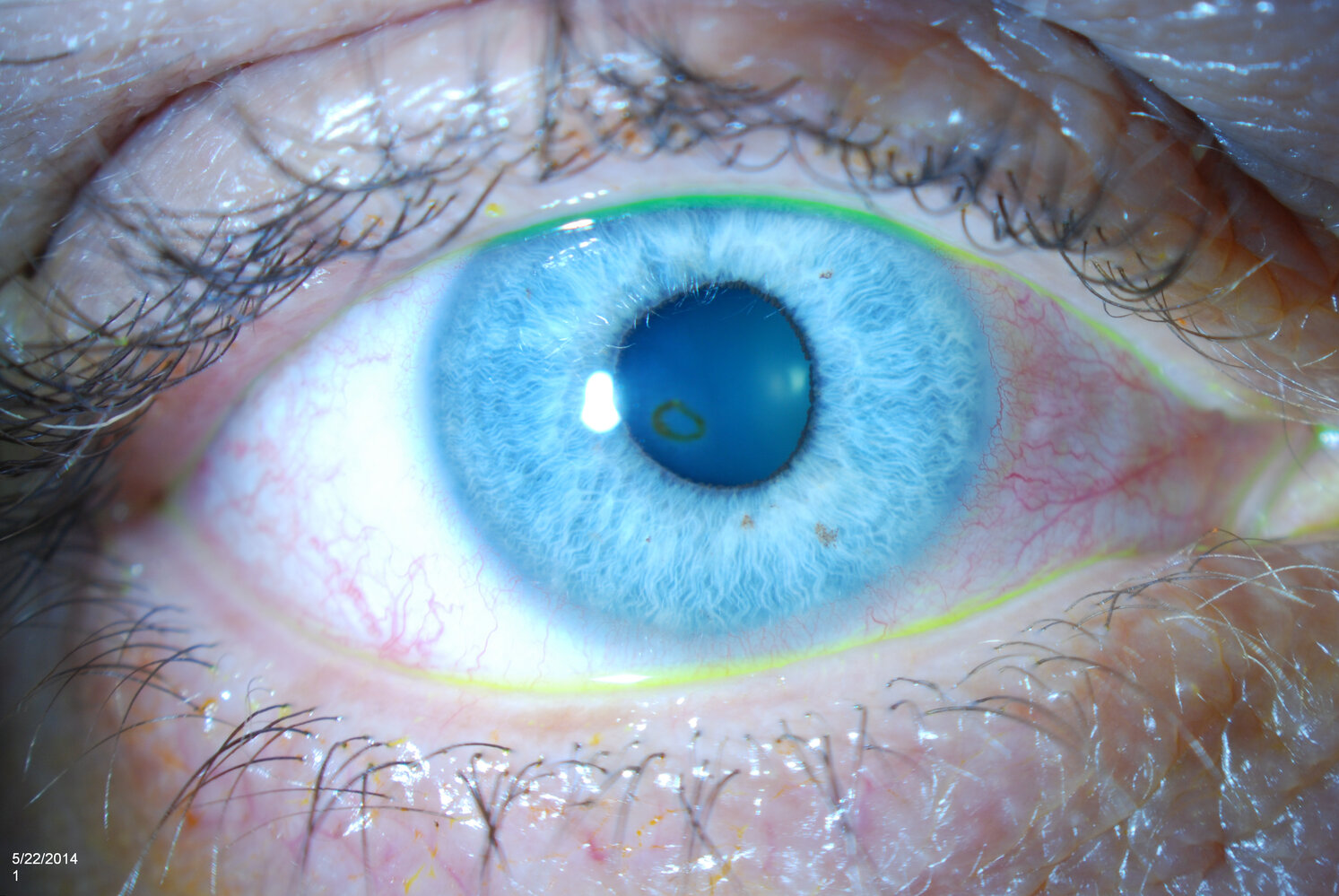
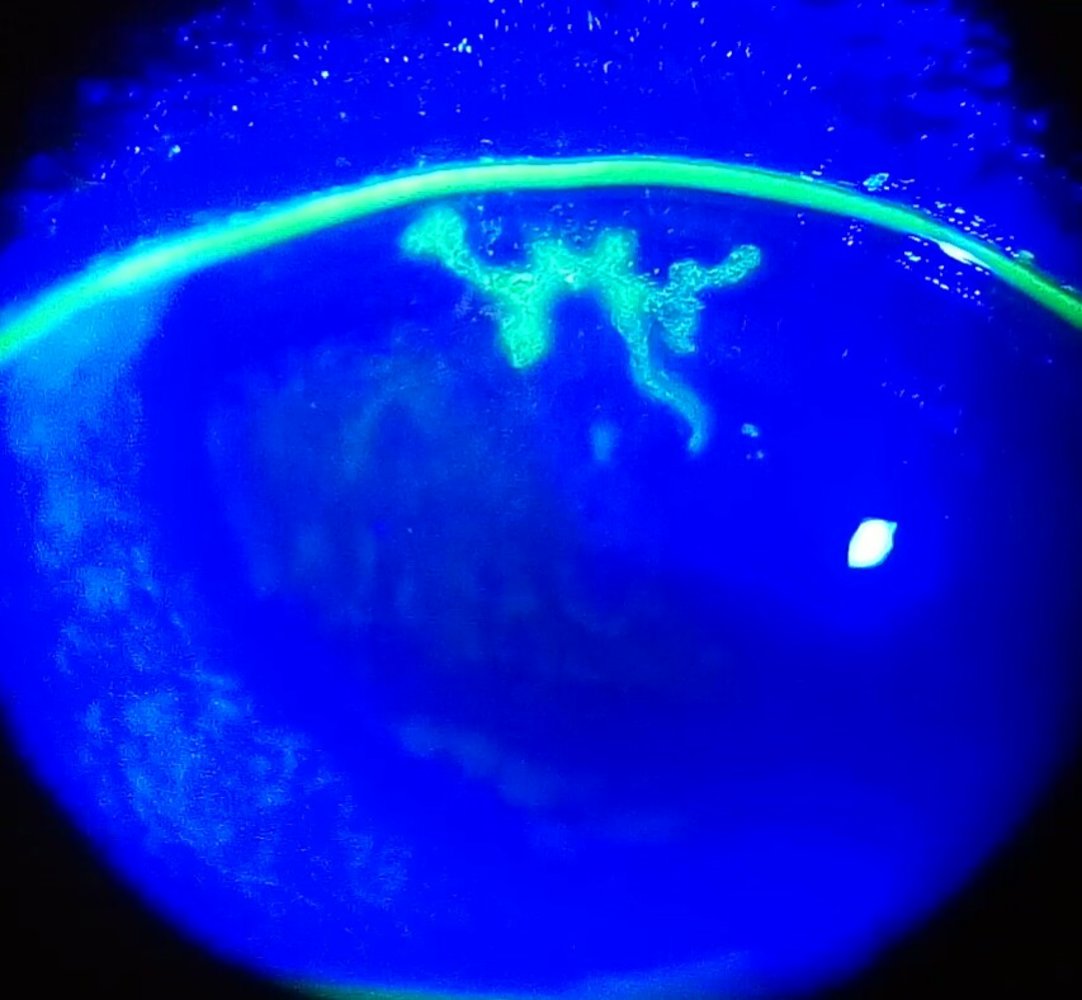
Slit lamp photography with fluorescein application under cobalt blue light filter
Fluorescein staining of the cornea under blue light shows green fluorescence of geographic epithelial defects. These defects are characteristic of herpes simplex keratitis, though less common than dendritic epithelial defects, which represent the hallmark of herpes simplex keratitis.
Source: “Figure 1B, in: Bilateral herpetic keratitis presenting with unilateral neurotrophic keratitis in pemphigus foliaceus: a case report” by H. K. Yang, Y. K. Han, W. R. Wee et al., BMC - Journal of Medical Case Reports, licensed under CC BY 2.0. Modifications: Image cropped. B removed.
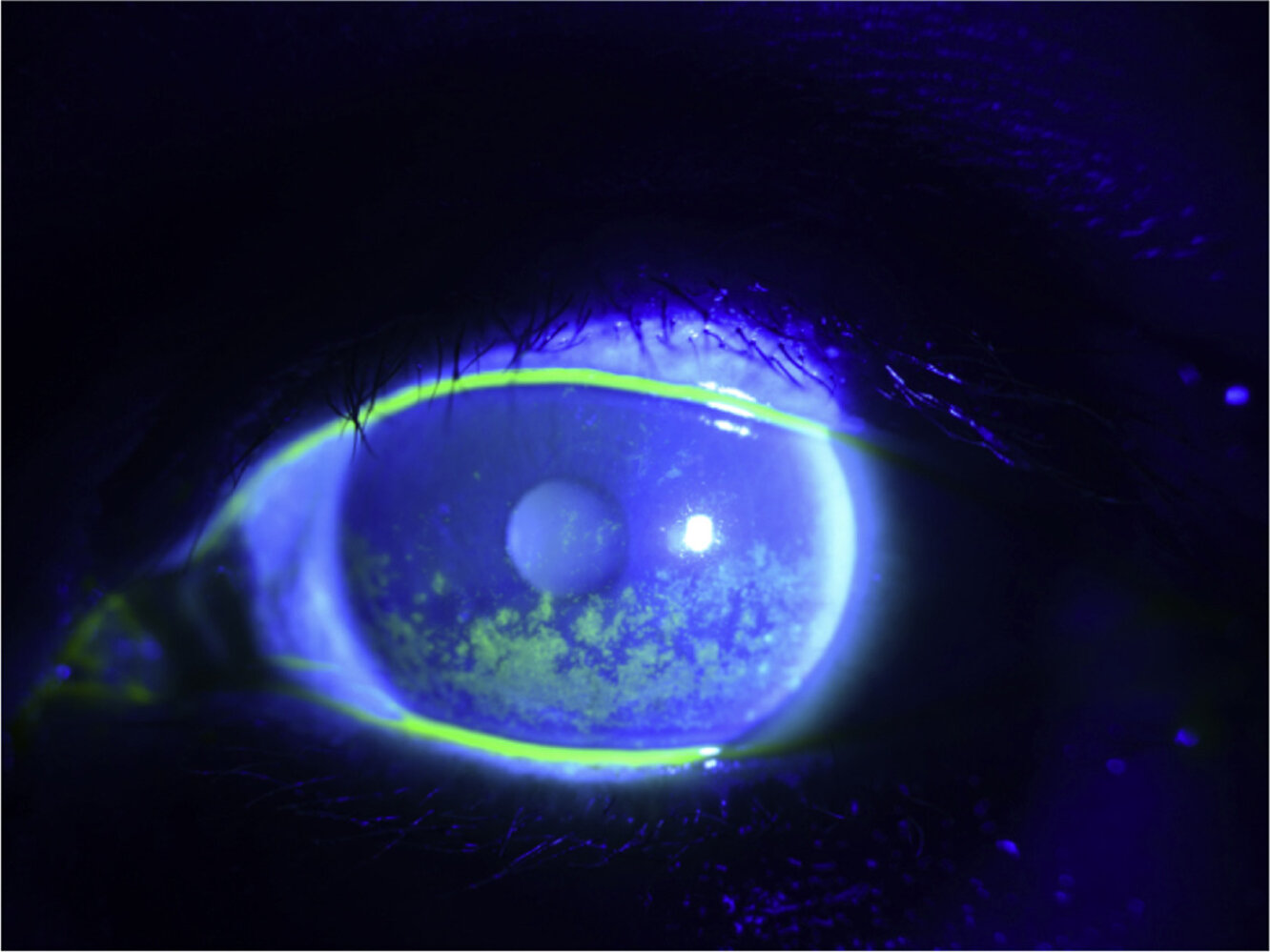
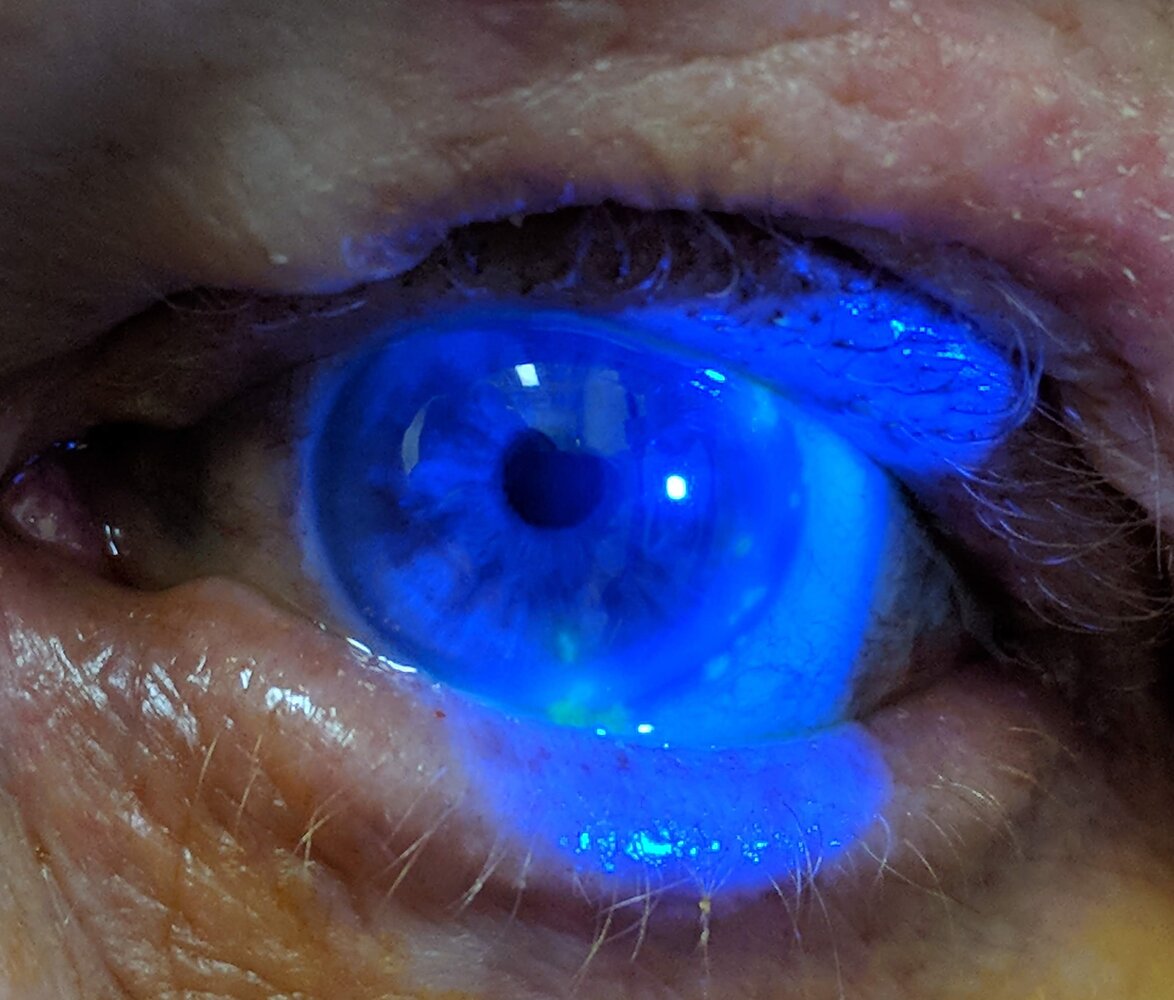
Slit-lamp photography of the left eye under cobalt blue light filter and fluorescein staining
Multiple diffuse pinpoint erosions (green staining) are seen on the surface of the cornea.
This appearance is characteristic of punctate epithelial erosions that often occur secondary to keratoconjunctivitis sicca (dry eye), as in the severe course seen here.
Source: “Figure 1b, in: Scleral lens for severe dry eye status post lacrimal gland resection for adenoid cystic carcinoma” by D. J. Oh, R. Michael, P. Setabutr et al., Elsevier - American Journal of Ophthalmology Case Reports, licensed under CC BY 4.0.
Corneal ulcer
Definition [2]
- Corneal ulcer: (ulcerative keratitis): a defect of the corneal epithelium and underlying stroma that occurs secondary to infection or inflammation
- Infectious keratitis: an infection of the cornea (also called “infectious corneal ulcer”) [15]
- Peripheral ulcerative keratitis: inflammation at the margin of the corneal stroma caused by autoimmune disease (also called “peripheral corneal ulceration”) [16]
Etiology
Corneal ulcers most frequently occur as a complication of keratitis. [2][17]
-
Bacterial keratitis
- Common organisms: Staphylococcus, Streptococcus, Mycobacterium, and Pseudomonas
-
Risk factors:
- Contact lens wearing
- Corticosteroid use
- Eye trauma
- Prior ocular surgery
-
Viral keratitis
- Herpes simplex keratitis
- Herpes zoster keratitis
- Fungal keratitis: most common in agricultural workers and patients using corticosteroids
-
Noninfectious keratitis [16][18]
- Autoimmune disease, e.g., rheumatoid arthritis, systemic lupus erythematosus
- Keratoconjunctivitis sicca


Clinical features [2][17]
- Eye pain and/or foreign body sensation
- Epiphora
- Conjunctival injection
- Photophobia
- Blurry/decreased vision
- Discharge from eye
Diagnostics [2][17]
Corneal ulcer is a clinical diagnosis based on slit lamp examination with fluorescein staining. Bacterial and viral cultures can help direct definitive treatment.
-
Characteristic findings on slit lamp examination
- Corneal epithelial defect
- Stromal edema or infiltration
- Anterior chamber cells and flare (∼ 25% of patients) [19]
-
Findings indicating viral corneal ulcer
-
Herpes simplex keratitis
- Herpetic lesions on conjunctiva or lids
- Slit lamp examination: dendritic lesions or amoeba-shaped ulcer
-
Herpes zoster keratitis
- Dermatomal vesicular rash
- Possible signs of uveitis, iritis, or choroiditis
- Slit lamp examination: similar to HSV keratitis
- See also: “Viral keratitis”
-
Herpes simplex keratitis



Management [2][17]
-
All patients
- Consult ophthalmology urgently.
- Provide analgesia for corneal pain.
-
Corneal ulcer secondary to bacterial keratitis [20]
- Initiate broad-spectrum topical antibiotics (e.g., ciprofloxacin ).
- Consider topical corticosteroids and/or systemic antibiotics in consultation with ophthalmology.
-
Corneal ulcer secondary to herpes simplex keratitis [20][21]
- Initiate topical or systemic antiviral therapy.
- Topical: e.g., trifluridine [21]
- Systemic: e.g., famciclovir (off-label) [21]
- Topical corticosteroids may be administered in consultation with ophthalmology for keratitis affecting the stroma or endothelium.
- Initiate topical or systemic antiviral therapy.
-
Corneal ulcer secondary to herpes zoster keratitis
- Initiate antiviral therapy for herpes zoster.
- See also “Herpes zoster ophthalmicus.”
Disposition [2][17]
- All patients should be seen by ophthalmology within 24 hours.
- Admit patients with:
- Herpes zoster ophthalmicus and immunocompromise or retinal involvement
- Severe symptoms
- No access to urgent ophthalmologic follow-up care
Complications [1][2]
- Vision loss
- Corneal scarring and/or perforation
-
Endophthalmitis
Corneal ulcers are an ophthalmological emergency and can result in permanent corneal scarring and vision loss.
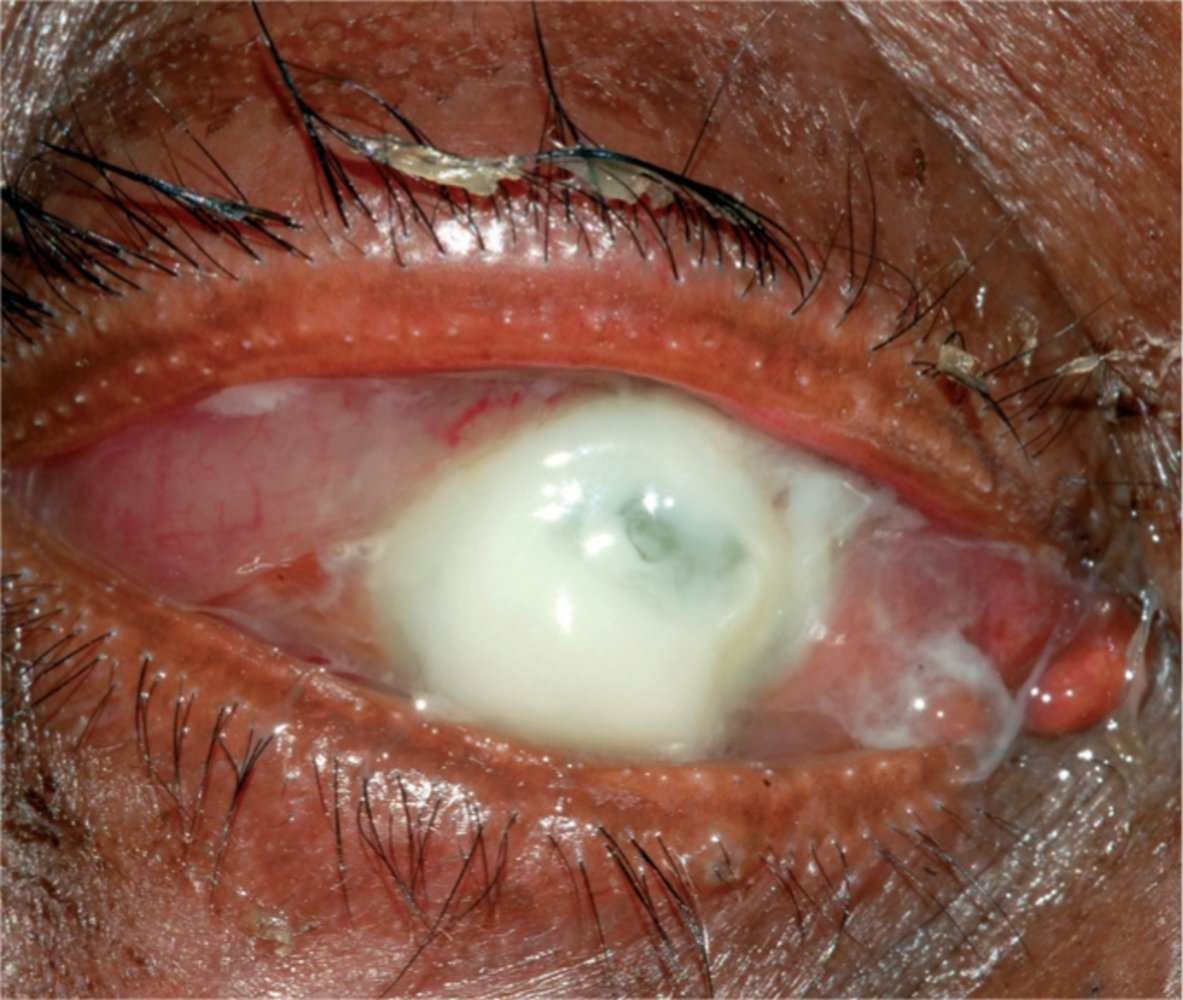
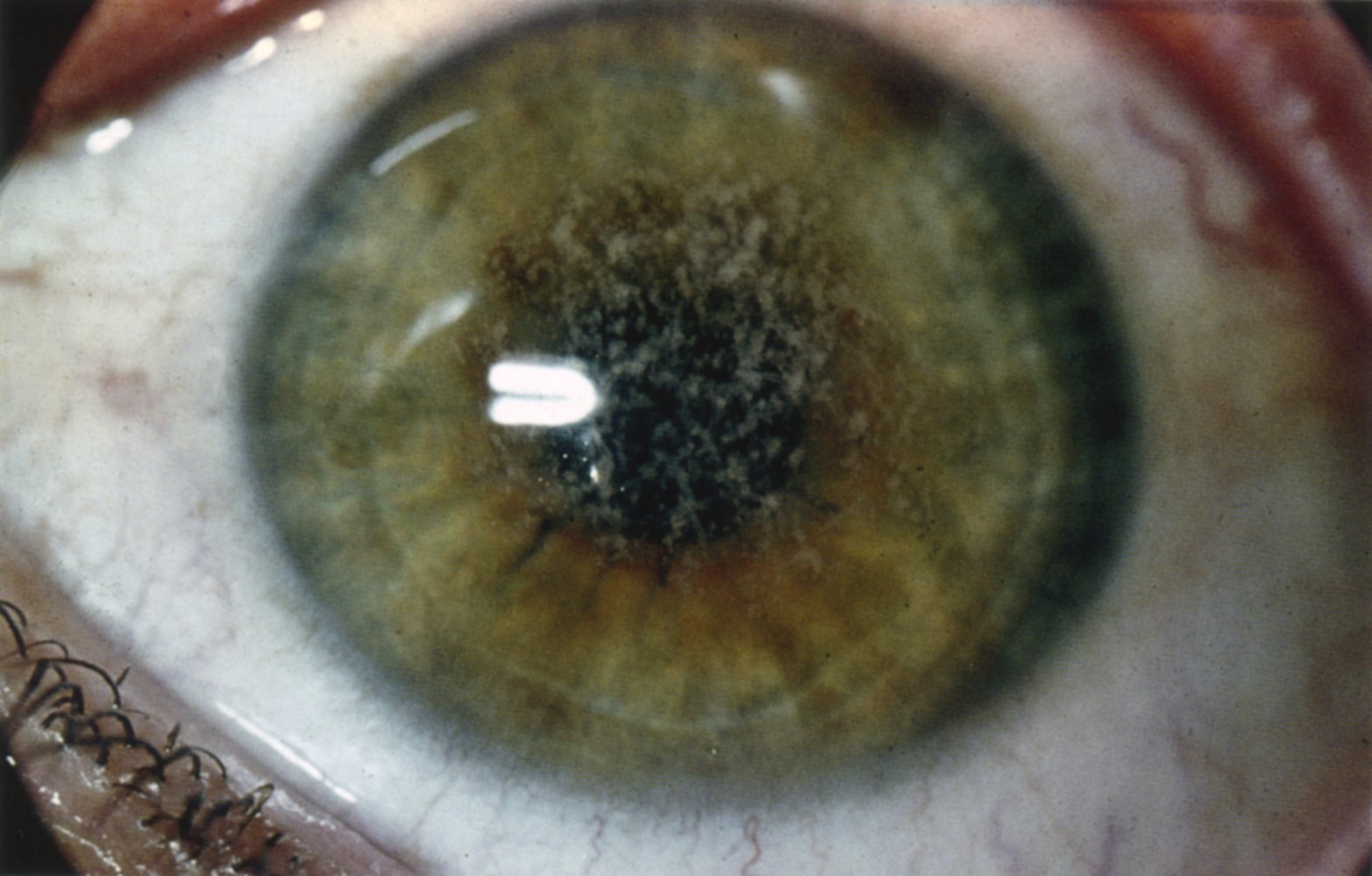
Slit lamp photograph of the right eye
Severe necrosis and ulceration of the cornea can be seen (white area). Purulent secretion and massive chemosis of the conjunctiva are also present.
This is the appearance of very severe bacterial keratitis, in this case caused by pseudomonas aeruginosa, where the cornea can become necrotic and perforate in the course of a few days.
Source: “Figure 1 in: Managing corneal disease: focus on suppurative keratitis” by Madan P Upadhyay, Muthiah Srinivasan, John P Whitcher, Community Eye Health, licensed under CC BY 3.0.
Slit-lamp photography of the left eye
A greyish infiltrate on the medial inferior part of the cornea can be seen (green overlay). The lesion does not have well-defined borders and shows ring infiltration (red overlay).
This is a typical finding of infectious keratitis, caused here by Cladosporium sp., as shown by microbiological testing.
Source: “Figure 1: Fungal keratitis caused by Cladosporium sp” by Steve Chih-Hsuan Cheng, Ying-Yu Lin, Chien-Neng Kuo, Li-Ju Lai, BMC Ophthalmology Journal, licensed under CC BY 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Slit-lamp photography with fluorescein stain and cobalt blue light filter
Dendritic lesions of the cornea appear green under cobalt blue illumination after fluorescein stain.
These lesions are characteristic of keratitis caused by herpes simplex virus (HSV).
Source: “Dendritic corneal ulcer” by Imrankabirhossain, Wikimedia Commons, licensed under CC BY-SA 4.0.
{kind=link}
Slit lamp photography with fluorescein application under cobalt blue light filter
Fluorescein staining of the cornea under blue light shows green fluorescence of geographic epithelial defects. These defects are characteristic of herpes simplex keratitis, though less common than dendritic epithelial defects, which represent the hallmark of herpes simplex keratitis.
Source: “Figure 1B, in: Bilateral herpetic keratitis presenting with unilateral neurotrophic keratitis in pemphigus foliaceus: a case report” by H. K. Yang, Y. K. Han, W. R. Wee et al., BMC - Journal of Medical Case Reports, licensed under CC BY 2.0. Modifications: Image cropped. B removed.
Slit-lamp photography, blue-light filter with fluorescein staining of a left eye
Superficial patchy erosions, marked by the fluorescein staining, are visible in a geographic pattern on the surface of the cornea (examples indicated by red overlay).
In combination with the cutaneous red lesions in the supraorbital region, the findings are typical for keratitis caused by herpes zoster ophthalmicus.
Source: “HerpesZosterOpth” by James Heilman, MD, Wikimedia Commons, licensed under CC BY-SA 4.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 4.0.
{kind=link}
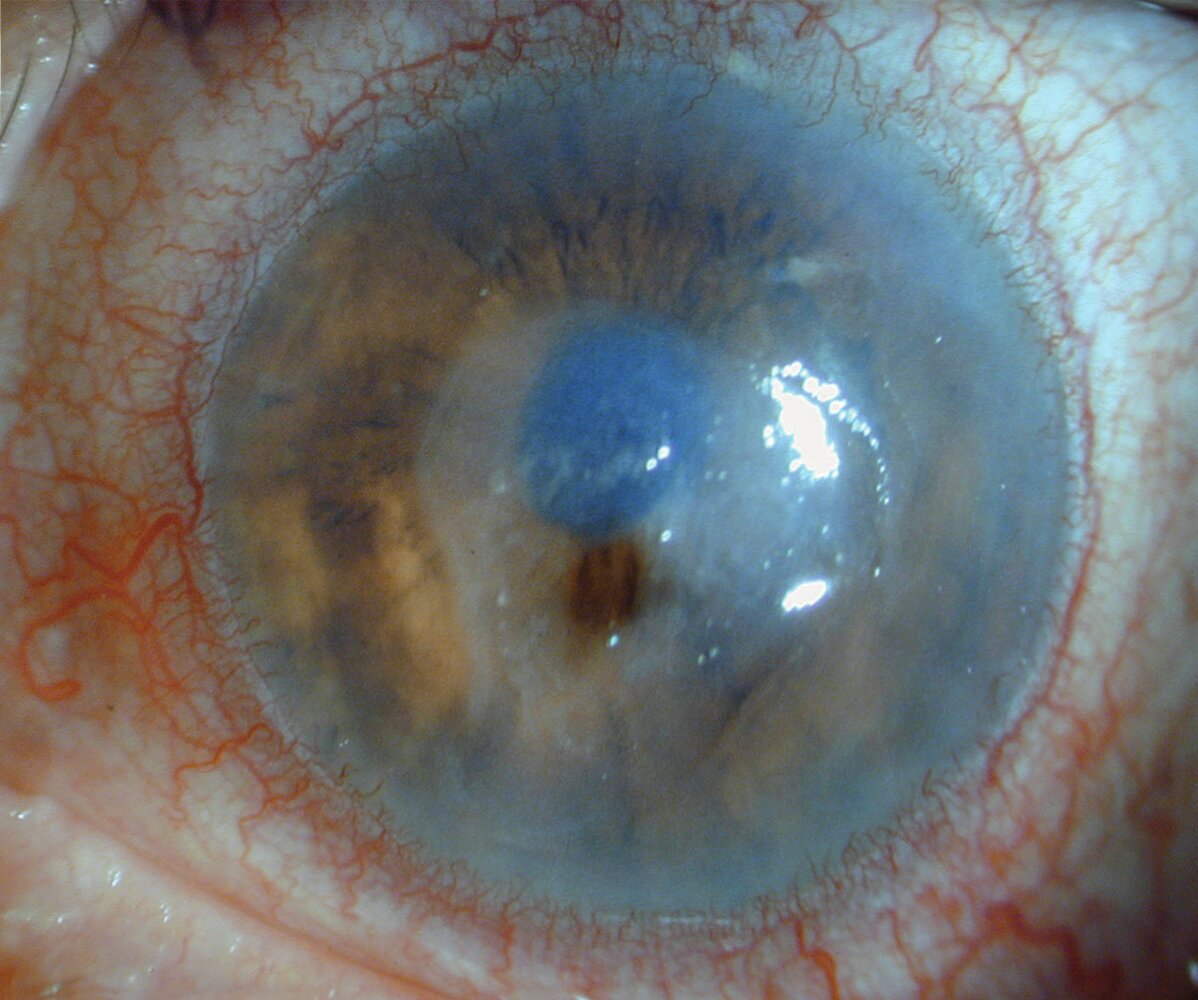
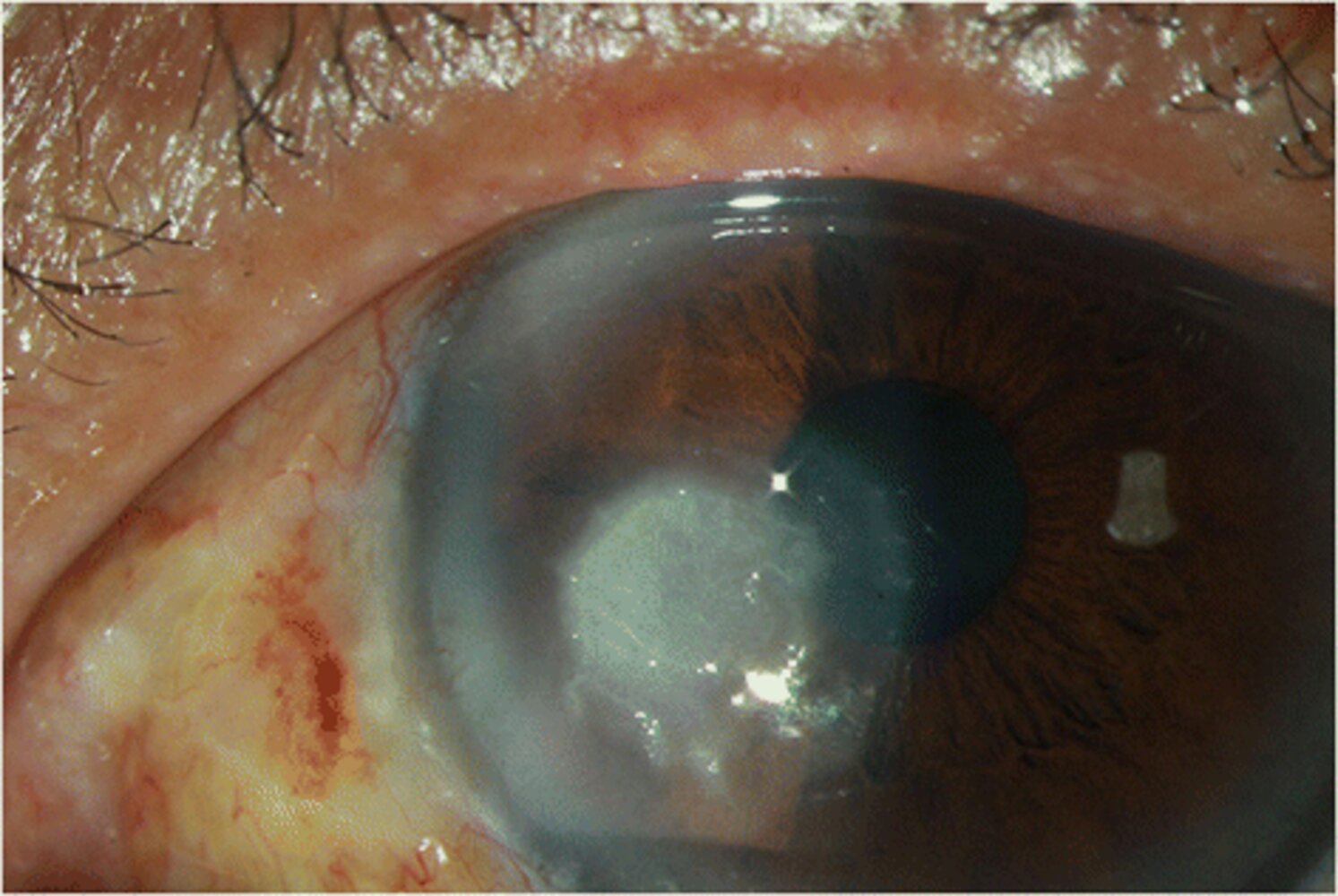
Left eye of a patient with vision loss, mild discomfort, and secretion in addition to a 5-year history of joint pain and ulnar deviation of the MCP joints
There is mixed injection. The cornea shows an ulcer with loss of stroma and clouding (yellow overlay). The ulcer is perforated with iris incarceration (black overlay). Hence, the pupil is ovoid rather than round (blue hatched overlay).
Corneal ulcers and corneal perforation are associated with rheumatic arthritis. The majority of these ulcers appear in the periphery of the cornea.
Source: © IMPP
Corneal degeneration, dystrophy, and deposits
Corneal degeneration
- Definition: changes of the cornea that cause corneal deterioration and, potentially, dysfunction
-
Etiology
- Normal aging
- Secondary to various pathological processes (e.g., calcium salt deposits in band keratopathy associated with hypercalcemia in the setting of sarcoidosis)
Band keratopathy
- Definition: a type of corneal degeneration that involves the appearance of a band-shaped area of calcification across the central cornea [12]
-
Etiology
- Idiopathic
-
Risk factors
- Hypercalcemia (e.g., hyperparathyroidism, sarcoidosis), hyperphosphatemia (e.g., chronic renal failure)
- Chronic, inflammatory eye disease (e.g., uveitis, keratitis)
- Exposure to harmful chemicals (e.g., mercury vapors)
- Family history of band keratopathy
- Pathophysiology: increased serum calcium, serum phosphate, and/or corneal surface pH (caused by chronically inflamed eyes) → change in solubility of calcium and phosphate → calcium phosphate precipitation out of tears, aqueous humor, and corneal tissue → calcium phosphate deposition as salts in the Bowman layer and superficial stroma of the cornea
-
Clinical findings
- Decreased visual acuity
- Foreign body sensation
- Photophobia
-
Diagnostics
- Slit lamp examination showing band-like, horizontal, opaque white areas on the cornea
- Follow-up includes investigation of underlying causes and may include:
- Serum calcium and phosphate measurement
- Parathyroid hormone level measurement
- Renal function tests
- Sarcoidosis workup (e.g., serum ACE, chest x-ray)
-
Treatment
- Treatment of the underlying cause (e.g., uveitis, hypercalcemia)
- Superficial debridement and lamellar keratectomy
- Prognosis: Visual deficits caused by band keratopathy can typically be treated successfully but will recur if the underlying condition is not addressed.

Corneal dystrophy [22]
- Definition: A group of inherited noninflammatory disorders that cause the buildup of various substances in the cornea and result in morphological changes.
-
Classification: There are many different types of corneal dystrophy. The most common are:
- Fuchs corneal dystrophy (see below for details)
- Lattice corneal dystrophy
- Map-dot-fingerprint corneal dystrophy
- Etiology: inherited condition
-
Clinical findings: Because corneal dystrophies are a heterogeneous group of diseases, they can affect the eye in different ways. Symptoms may include:
- Progressive visual impairment
- Corneal erosion (see “Symptoms” in corneal erosion, above)
- Diagnostics: visible structural changes and/or deposits on slit lamp examination
-
Treatment
- See “Treatment” in corneal erosion, above.
- Keratoplasty in severe cases or when other treatment modalities have not been successful


Fuchs dystrophy
- Definition: inherited disease that predisposes to progressive loss of corneal endothelial cells
- Pathophysiology: corneal endothelial cells are responsible for maintaining the transparency of the cornea by balancing water and electrolyte flow into and out of the corneal layers; deterioration of corneal endothelial cells → decreased outflow of water from the corneal stroma → corneal edema, opacification, and bullous epithelial detachment [23]
-
Clinical findings
- Reduced visual acuity
- Blurred vision, glare, and halos, often improving over the course of the day [24]
- Eye pain or foreign body sensation in the eye
-
Diagnostics
- Early Fuchs dystrophy is asymptomatic, but cornea guttata (droplet-shaped structures in the Descemet membrane consisting of collagen and thought to have been secreted by stressed corneal endothelial cells) can be seen on slit lamp examination.
- Advanced disease: Slit lamp examination shows corneal thickening, edema, bullae, and fibrotic scarring.
-
Treatment [25]
- Asymptomatic patients do not require treatment.
- Symptomatic treatment
- Medical treatment to dehydrate the cornea: hyperosmolar eye drops, warm dry air (e.g., hair dryer held at arm's length)
- For pain or foreign body sensation in the eye: NSAIDs, bandage contact lenses
- Keratoplasty: indicated in advanced disease with marked loss of vision that does not improve over the course of the day and if pain cannot be alleviated by symptomatic treatment

Corneal deposits
A variety of substances can accumulate in the cornea to create deposits. Two of the more well-known causes of corneal deposits are presented below.
Arcus senilis (corneal arcus)
- Definition: a condition associated with normal aging, in which annular deposits of lipids appear around the corneal margin
-
Epidemiology: Incidence increases with age. [26]
- 60% in those 50–60 years
- Almost 100% in those > 80 years
- Clinical findings: asymptomatic
- Diagnostics: slit lamp examination
-
Treatment
- In older patients: no treatment necessary
- Occurrence before 50 years of age: rule out lipid disorders

Kayser-Fleischer ring
- Definition: green-brown, copper deposits are a diagnostic sign of Wilson disease (See “Clinical features” in Wilson disease.)

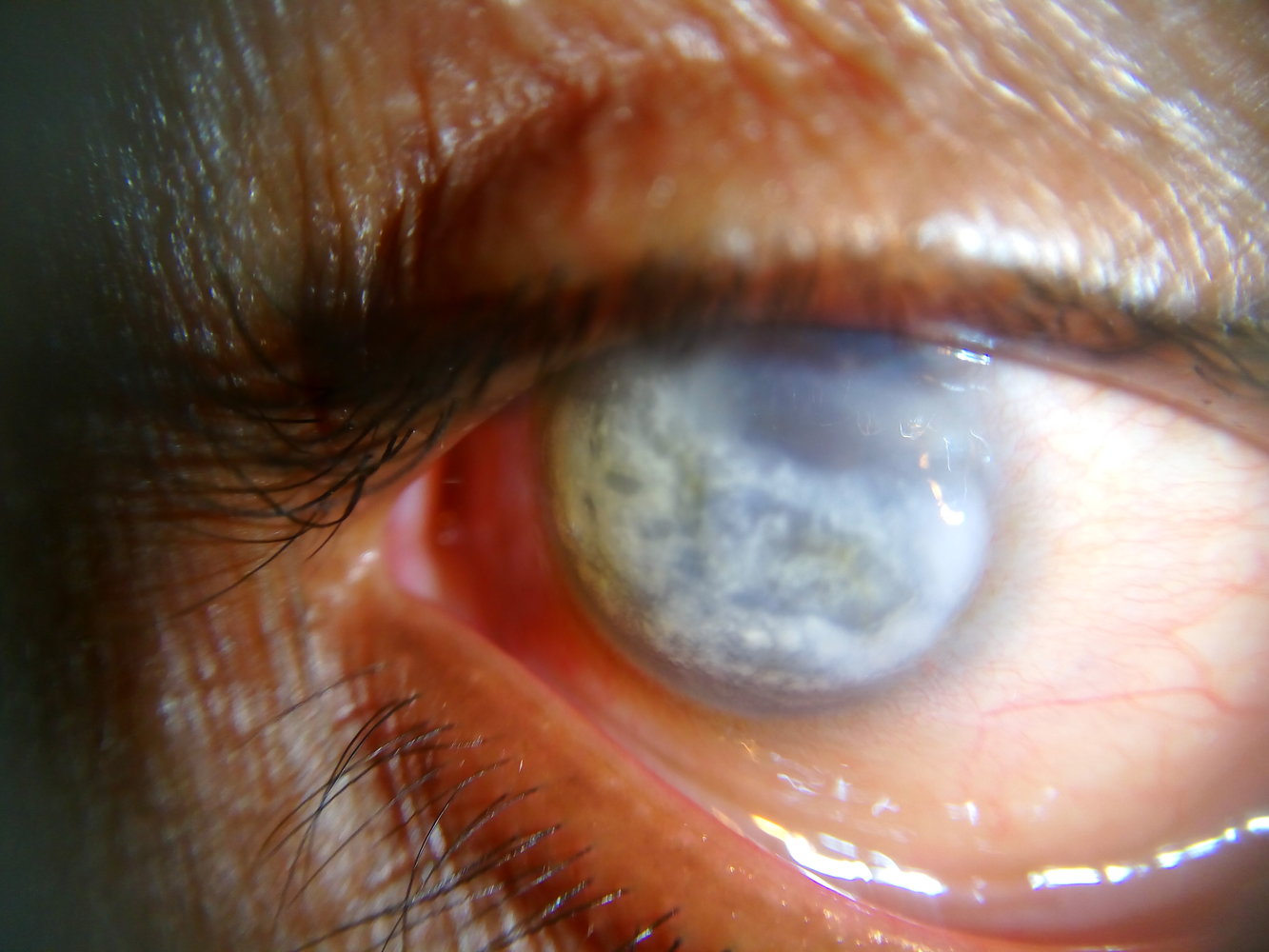
Slit-lamp examination of the right eye
Several white, horizontal, band-like deposits are visible across the inferior two-thirds of the cornea.
This is the characteristic appearance of severe band keratopathy.
Source: “Band keratopathy of a 60-year-old male. in: Band keratopathy” by Imrankabirhossain, Wikimedia Commons, licensed under CC BY-SA 4.0.
Slit-lamp photography
Several localized opacities are spread mainly in or on the central cornea. The depth of the opacities can only be specified by further slit-lamp examination.
This is a common finding in granular corneal dystrophy.
Source: © IMPP
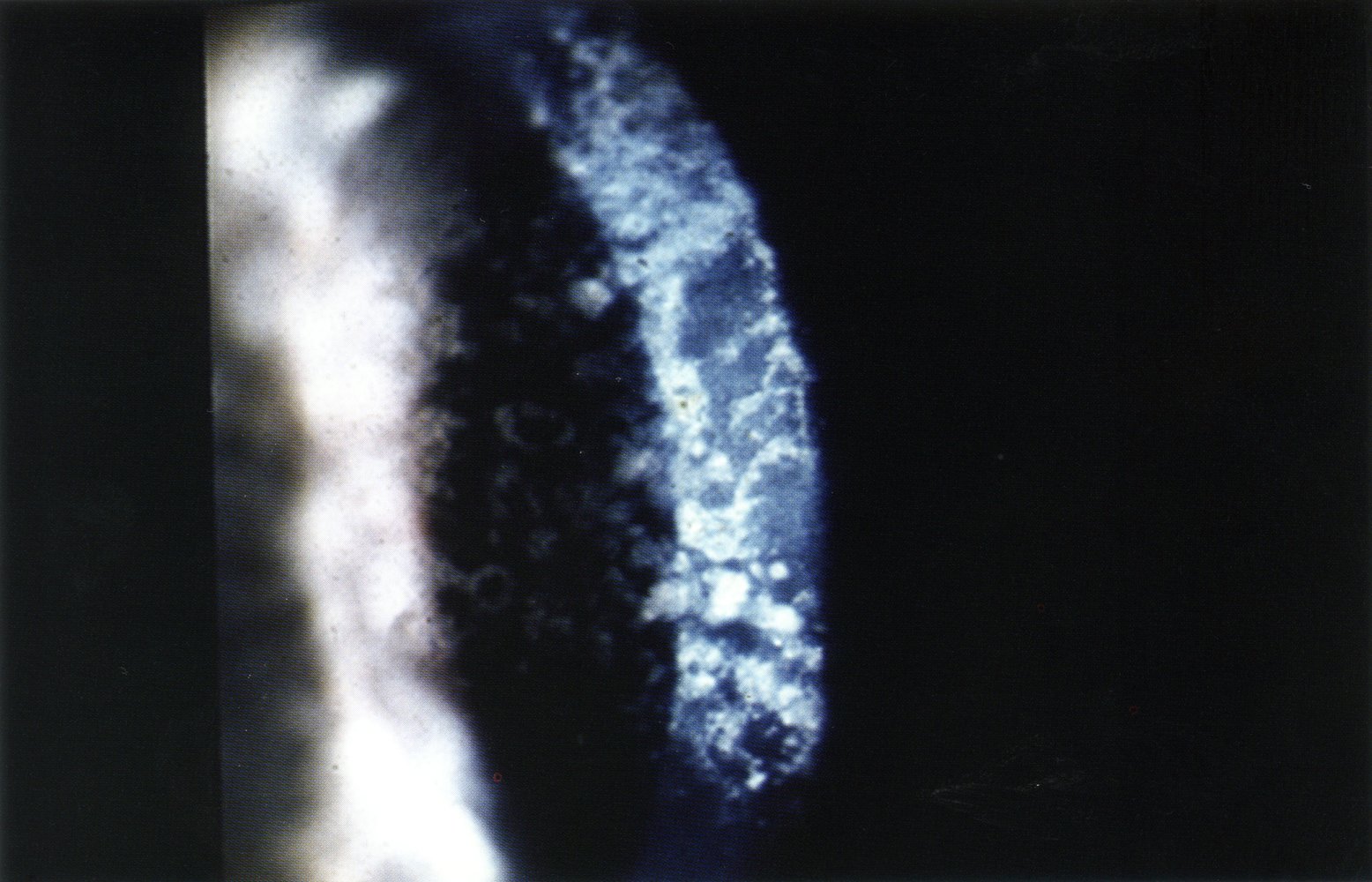
Slit-lamp examination of the cornea (optical cross section)
Several white opacities are visible throughout the stroma.
This is a typical finding in an advanced stage of granular corneal dystrophy.
Source: © IMPP
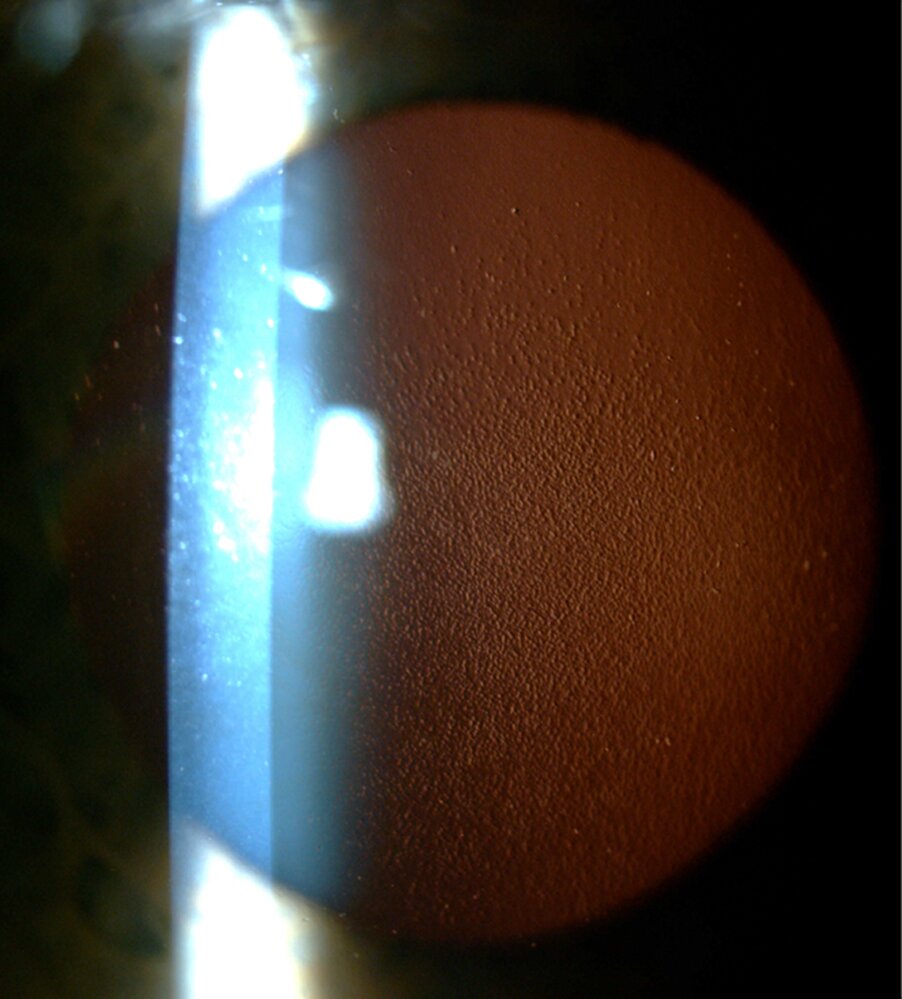
Slit-lamp photography of a patient with Fuchs dystrophy in retroillumination
Multiple guttae (focal excrescences of Descemet membrane) are visible as small dots. This typical appearace is also referred to as “beaten metal” appearance.
Source: “Fig. 1a in: Fuchs Endothelial Corneal Dystrophy: Strong Association with rs613872 Not Paralleled by Changes in Corneal Endothelial TCF4 mRNA Level” by Monika Ołdak, Ewelina Ruszkowska, Monika Udziela, Dominika Oziębło, Ewelina Bińczyk, Aneta Ścieżyńska et al., Hindawi, licensed under CC BY 3.0.
Slit-lamp photography of the left eye
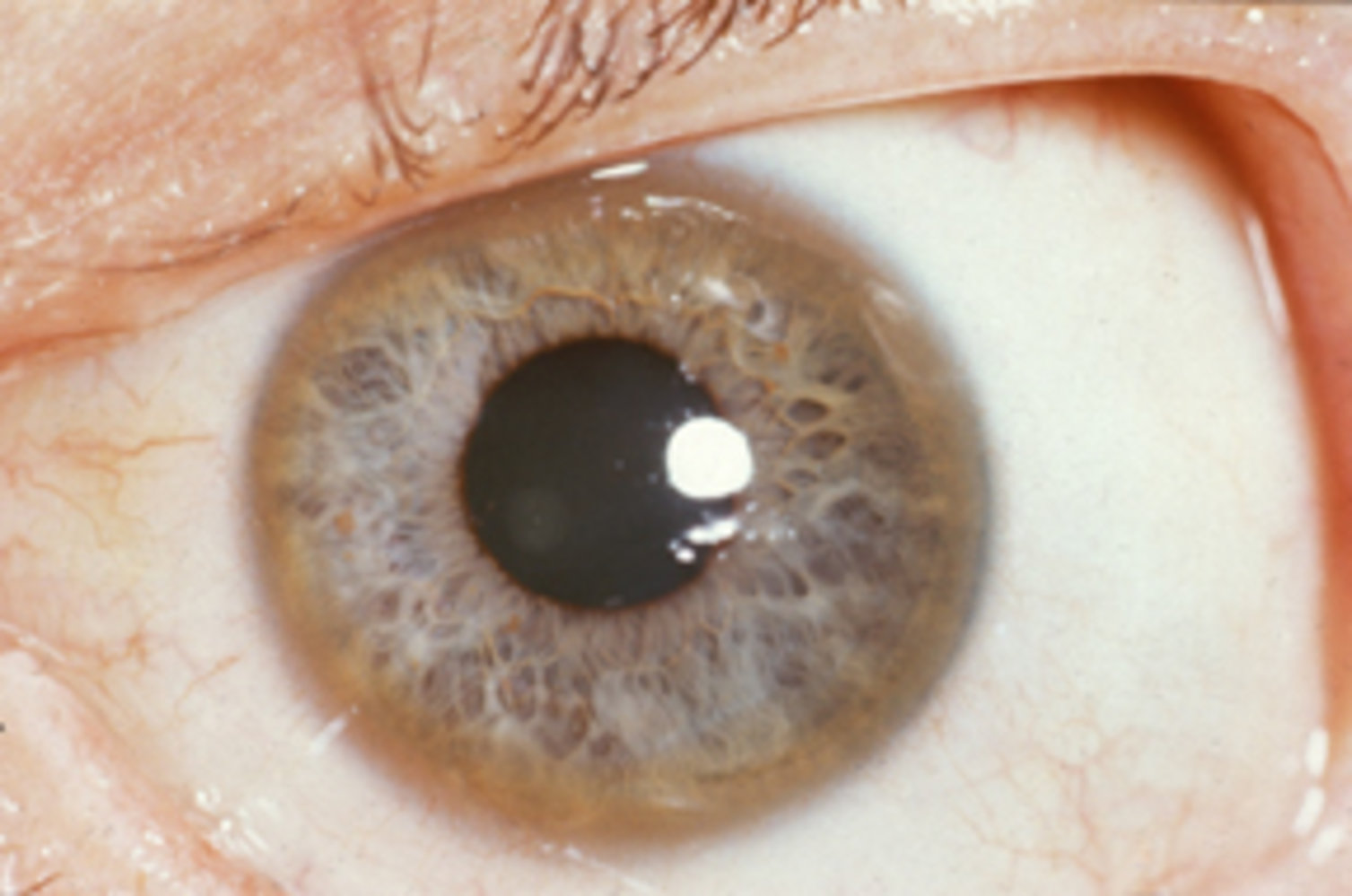
A white opacity, caused by lipid deposition, lines the lower and slightly also the upper periphery of the cornea while being clearly separated from the limbus by clear cornea.
This is the typical appearance of an arcus senilis. In the early stages, it is usually seen in the inferior cornea. It may extend to a full circle in more advanced stages. If present in young individuals blood lipid levels should be examined.
Source: “Figure 1, in: Correlating corneal arcus with atherosclerosis in familial hypercholesterolemia” by Loren A Zech, Jeffery M Hoeg, Lipids in Health and Disease, licensed under CC BY 2.0. Modifications: Cropping.
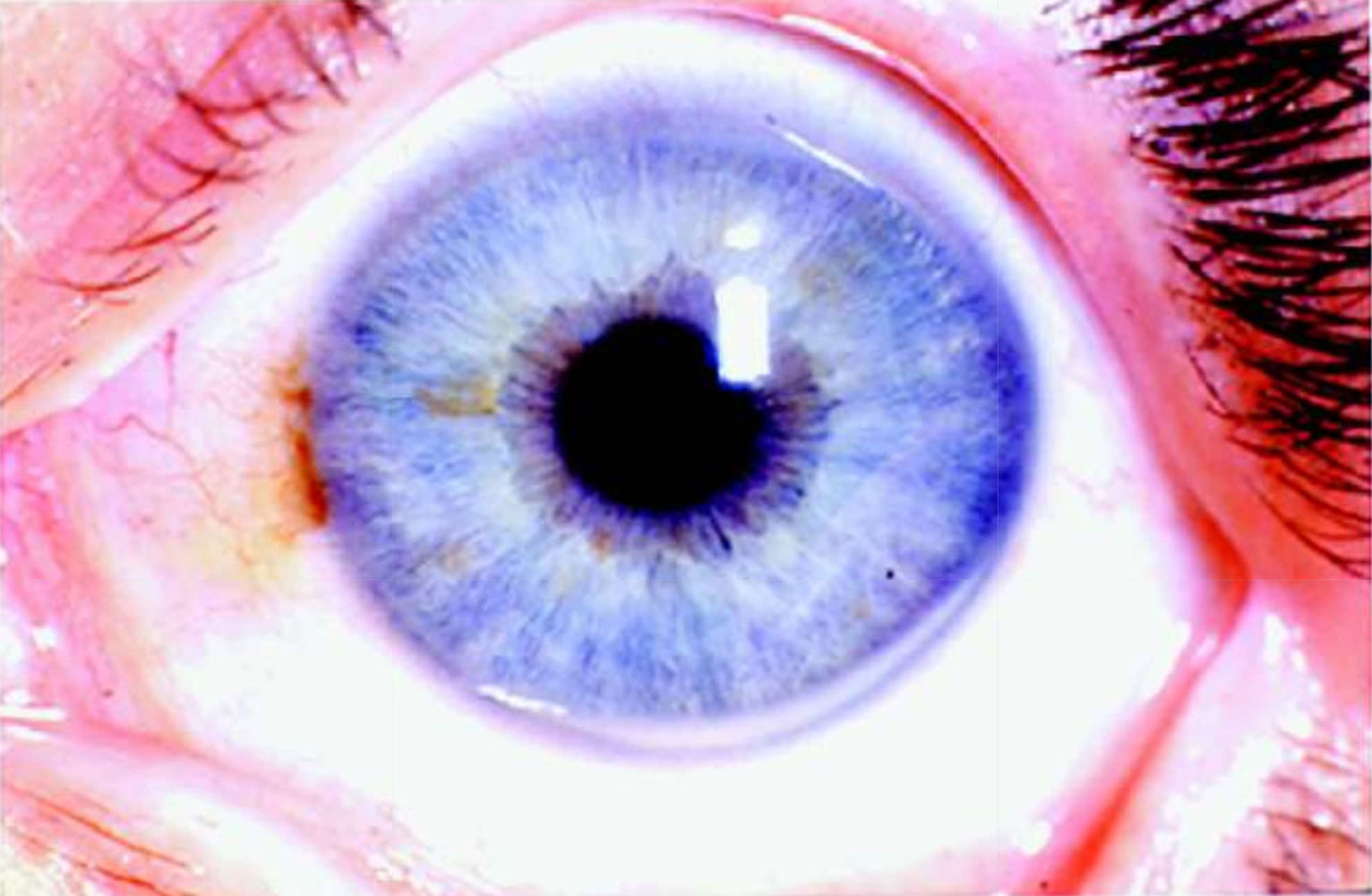
Slit-lamp photography of a left eye
A brown ring is visible in the periphery of the cornea (Kayser-Fleischer ring; green overlay).
Kayser-Fleischer rings are typically seen in Wilson disease.
Source: “Images of Memorable Cases: Case 9: Kayser-Fleischer_ring” by Herbert L. Fred, MD, Hendrik A. van Dijk, Wikimedia Foundation, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
Curvature anomalies of the cornea
Keratoconus
- Definition: a noninflammatory corneal condition in which the cornea becomes thinner than normal and develops a conic shape, bulging outward at the center [27]
-
Etiology: unknown; frequently associated with other conditions
- Neurodermatitis
- Allergic asthma
- Hay fever
- Marfan syndrome
- Ehlers-Danlos syndrome
- Down syndrome
- A positive family history of keratoconus has been found in a minority of cases (10%)
-
Clinical findings: symptoms are often initially unilateral; however, they always become bilateral in the further course of disease [22]
- Progressive decrease in visual acuity
- Myopia
- Astigmatism
- Photophobia
-
Diagnostics
- Slit lamp examination showing protrusion and thinning of the cornea
- Ultrasound pachymetry (measurement of corneal thickness via ultrasound)
- Computerized corneal topography
-
Treatment [28]
- Correcting astigmatism and myopia: glasses or rigid gas permeable contact lenses [28]
- In progressive keratoconus: crosslinking with UV-A light (corneal crosslinking)
- If conservative treatment options fail: keratoplasty
-
Complications
- Corneal hydrops (corneal rupture): tearing of the Descemet membrane and endothelium → penetration of intraocular fluid into the stromal tissue of the cornea → acute pain and deterioration in vision caused by corneal opacification

Keratoglobus [28]
- Definition: noninflammatory corneal condition, in which the cornea becomes thinner than normal and develops a more globular shape, bulging outward at the center
- Etiology: unknown; associated with disorders of collagen synthesis (Marfan syndrome, Ehlers-Danlos syndrome)
- Clinical findings, diagnostics, and treatment: similar to those of keratoconus
Astigmatism
- See astigmatism

Anterior segment of a right eye
The cornea is cone-shaped, producing a V-shaped indentation on the lower eyelid, known as Munson sign, when the patient gazes downward.
This is the characteristic appearance of advanced keratoconus.
Source: “Figure 3, in: Molecular and Histopathological Changes Associated with Keratoconus” by M. Lotfy Khaled, I. Helwa, M. Drewry et al., Hindawi - BioMed Research International, licensed under CC BY 4.0.
Inflammatory conditions of the cornea
- See “Keratitis” and “Conjunctivitis.”
Keratoplasty (corneal transplantation)
Keratoplasty (corneal transplantation) [29]
-
Indications
- Significant visual impairment as a result of pathological changes in the cornea, e.g., opacification, irregular curvature
- Keratitis that cannot be controlled by conservative treatment
-
Procedure: replacement of diseased cornea with cornea harvested from a recently deceased donor
- Perforating keratoplasty (replacement of the complete cornea): indicated when both anterior and posterior corneal layers are damaged
- Lamellar keratoplasty (replacement of only the anterior or posterior corneal layers): indicated when only anterior or posterior corneal layers are damaged
-
Follow-up care
- Graft rejection prevention: corticosteroid eye drops
- Monitoring and treatment for graft rejection

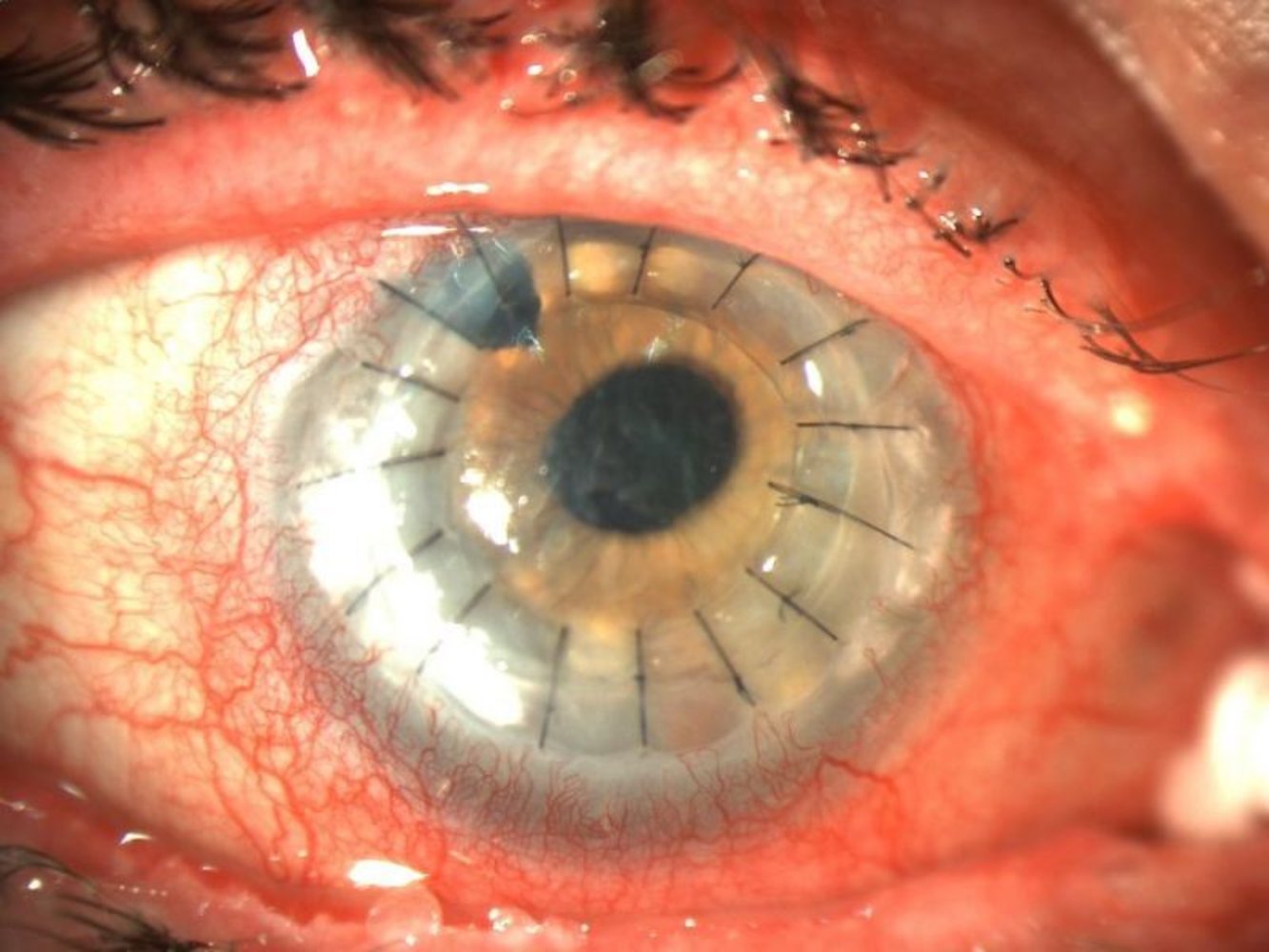
Postoperative slit-lamp photograph of a keratoplasty of the right eye
A series of interrupted stitches (example traced by white solid line) are visible around the entire course of the cornea (corneal graft marked by blue overlay). The peripheral host corneal tissue shows neovascularization (examples indicated by black arrows; corneal limbus marked by white dashed line). There is an iridectomy at the 11-o'clock position (marked by yellow dashed line). Significant conjunctival injections are also visible.
Source: “Fresh keratoplasty” by Philipp Franko Zeitz, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
References
- "Recurrent Corneal Erosion". http://eyewiki.org/Recurrent_Corneal_Erosion. [2016-05-22]
- "Facts About the Cornea and Corneal Disease". https://www.nei.nih.gov/health/cornealdisease. [2016-05-01]
- Jurkunas UV. "Fuchs Endothelial Corneal Dystrophy Through the Prism of Oxidative Stress". Cornea. 37. :S50-S54. (2018)
- "What Is Fuchs' Dystrophy?". https://www.aao.org/eye-health/diseases/what-is-fuchs-dystrophy. [2017-09-01]
- "Fuchs’ Endothelial Dystrophy". http://eyewiki.aao.org/Fuchs%E2%80%99_Endothelial_Dystrophy
- "Corneal arcus". https://www.aao.org/bcscsnippetdetail.aspx?id=75f705e5-3ebe-4593-837d-5ae7bc3d44f3. [2019-01-01]
- "Corneal Erosion". https://www.aao.org/eye-health/diseases/what-is-corneal-erosion. [2014-07-19]
- Wipperman JL, Dorsch JN. "Evaluation and management of corneal abrasions". Am Fam Physician. 87(2). :114-20. (2013)
- "Treatment of Recurrent Corneal Erosions". https://www.aao.org/eyenet/article/treatment-of-recurrent-corneal-erosions. [2013-03-01]
- Abudou M, Wu T, Evans JR, Chen X. "Immunosuppressants for the prophylaxis of corneal graft rejection after penetrating keratoplasty". Cochrane Database Syst Rev. (2015)
- Wayman LL. "Keratoconus". UpToDate. UpToDate. https://www.uptodate.com/contents/keratoconus. [2019-01-01]
- Wallang BS, Das S. "Keratoglobus". Eye. 27(9). :1004-1012. (2013)
- Walls R, Hockberger R, Gausche-Hill M, Erickson TB, Wilcox SR. "Rosen's Emergency Medicine 10th edition- Concepts and Clinical Practice E-Book". Elsevier Health Sciences. (2022). ISBN: 9780323757904
- Yu CW, Kirubarajan A, Yau M, Armstrong D, Johnson DE. "Topical pain control for corneal abrasions: A systematic review and meta‐analysis". Acad Emerg Med. 28(8). :890-908. (2021)
- Wakai A, Lawrenson JG, Lawrenson AL, et al. "Topical non-steroidal anti-inflammatory drugs for analgesia in traumatic corneal abrasions". Cochrane Database Syst Rev. 2017(5). (2017)
- Sulewski M, Leslie L, Liu SH, et al. "Topical ophthalmic anesthetics for corneal abrasions". Cochrane Database Syst Rev. 2023(10). (2023)
- Green SM, Tomaszewski C, Valente JH, Lo B, Milne K. "Use of Topical Anesthetics in the Management of Patients With Simple Corneal Abrasions: Consensus Guidelines From the American College of Emergency Physicians". Ann Emerg Med. 83(5). :477-489. (2024)
- Chuck RS, Jeng BH, Lum F. "Consensus Guidelines versus Evidence-Based Medicine in the Treatment of Corneal Abrasions". Ophthalmology. 131(5). :524-525. (2024)
- Lee MD, Driver TH, Seitzman GD. "Cornea Specialists Do Not Recommend Routine Usage of Topical Anesthetics for Corneal Abrasions". Ann Emerg Med. 74(3). :463-466. (2019)
- Cabrera‐Aguas M, Khoo P, Watson SL. "Infectious keratitis: A review". Clin Exp Ophthal. 50(5). :543-562. (2022)
- Cao Y, Zhang W, Wu J, Zhang H, Zhou H. "Peripheral Ulcerative Keratitis Associated with Autoimmune Disease: Pathogenesis and Treatment". J Ophthalmol. 2017. :1-12. (2017)
- Gilani CJ, Yang A, Yonkers M, Boysen-Osborn M. "Differentiating Urgent and Emergent Causes of Acute Red Eye for the Emergency Physician". Western Journal of Emergency Medicine. 18(3). :509-517. (2017)
- Sheppard J, Shen Lee B, Periman LM. "Dry eye disease: identification and therapeutic strategies for primary care clinicians and clinical specialists". Ann Med. 55(1). :241-252. (2022)
- Konstantopoulou K, Del’Omo R, Morley AM, et al. "A comparative study between clinical grading of anterior chamber flare and flare reading using the Kowa laser flare meter". Int Ophthalmol. 35(5). :629-633. (2012)
- Austin A, Lietman T, Rose-Nussbaumer J. "Update on the Management of Infectious Keratitis". Ophthalmology. 124(11). :1678-1689. (2017)
- "Herpes Simplex Virus Keratitis: A Treatment Guideline". https://www.aao.org/clinical-statement/herpes-simplex-virus-keratitis-treatment-guideline#top. [2014-06-01]
- Roberts JR. "Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care". Elsevier. (2018). ISBN: 9780323354783
- Safari S, McLaughlin CJ, Shah A, Kane BG. "Prolonged Ocular Foreign Body Found on Repeat Visit to a Second Emergency Department". Cureus. (2023)
- Vora GK, Haddadin R, Chodosh J. "Management of Corneal Lacerations and Perforations". Int Ophthalmol Clin. 53(4). :1-10. (2013)
- Grehn F. "Augenheilkunde". Springer Verlag (2005). (2006). ISBN: 3540256997
- Lang GK, et al. "Augenheilkunde". Thieme Verlag (2008). (2008). ISBN: 9783131028341
- Weiss J, Møller H, Lisch W, et al. "IC3D-Klassifikation von Hornhautdystrophien". Klin Monatsbl Augenheilkd. 228(Suppl 01). :1-S39. (2011)