Summary
Cranial nerve palsy is characterized by a decreased or complete loss of function of one or more cranial nerves. Cranial nerve palsies can be congenital or acquired. Multiple cranial neuropathies are commonly caused by tumors, trauma, ischemia, or infections. While diagnosis can usually be made based on clinical features, further investigation is often warranted to determine the specific cause. Contrast-enhanced MRI is usually the preferred imaging modality to evaluate the affected nerve and any soft tissue abnormalities. A CT scan may be indicated to evaluate for bony lesions and fractures that may be compressing the nerve. Management is mainly aimed at treating the underlying cause. Surgery may be indicated for individuals with severe disability (e.g., acute traumatic cranial nerve palsies, persistent symptoms despite conservative measures). Spontaneous resolution over months may occur, especially in cranial nerve palsies secondary to microangiopathy.
Facial nerve palsy is covered in detail separately.
Cranial nerve types and functions
| Overview of cranial nerves and their function [1] | |||
|---|---|---|---|
| Cranial nerve | Nerve type | Function | |
| I | Olfactory nerve |
|
|
| II | Optic nerve |
|
|
| III | Oculomotor nerve |
|
|
|
|
||
| IV | Trochlear nerve |
|
|
| V | Trigeminal nerve |
|
|
|
|
||
| VI | Abducens nerve |
|
|
| VII | Facial nerve |
|
|
|
|
||
|
|
||
| VIII | Vestibulocochlear nerve |
|
|
| IX | Glossopharyngeal nerve |
|
|
|
|
||
|
|
||
| X | Vagus nerve |
|
|
|
|
||
|
|
||
|
|
||
| XI | Accessory spinal nerve |
|
|
| XII | Hypoglossal nerve |
|
|
“Some Say Marry Money, But My Brother Says Big Brain Matters More:” CN I is sensory, CN II is sensory, CN III is motor, CN IV is motor, CN V is both (mixed), CN VI is motor, CN VII is both (mixed), CN VIII is sensory, CN IX is both (mixed), CN X is both (mixed), CN XI is motor, and CN XII is motor.
CN VII (Seven) controls Salivation by innervating Submandibular and Sublingual glands.

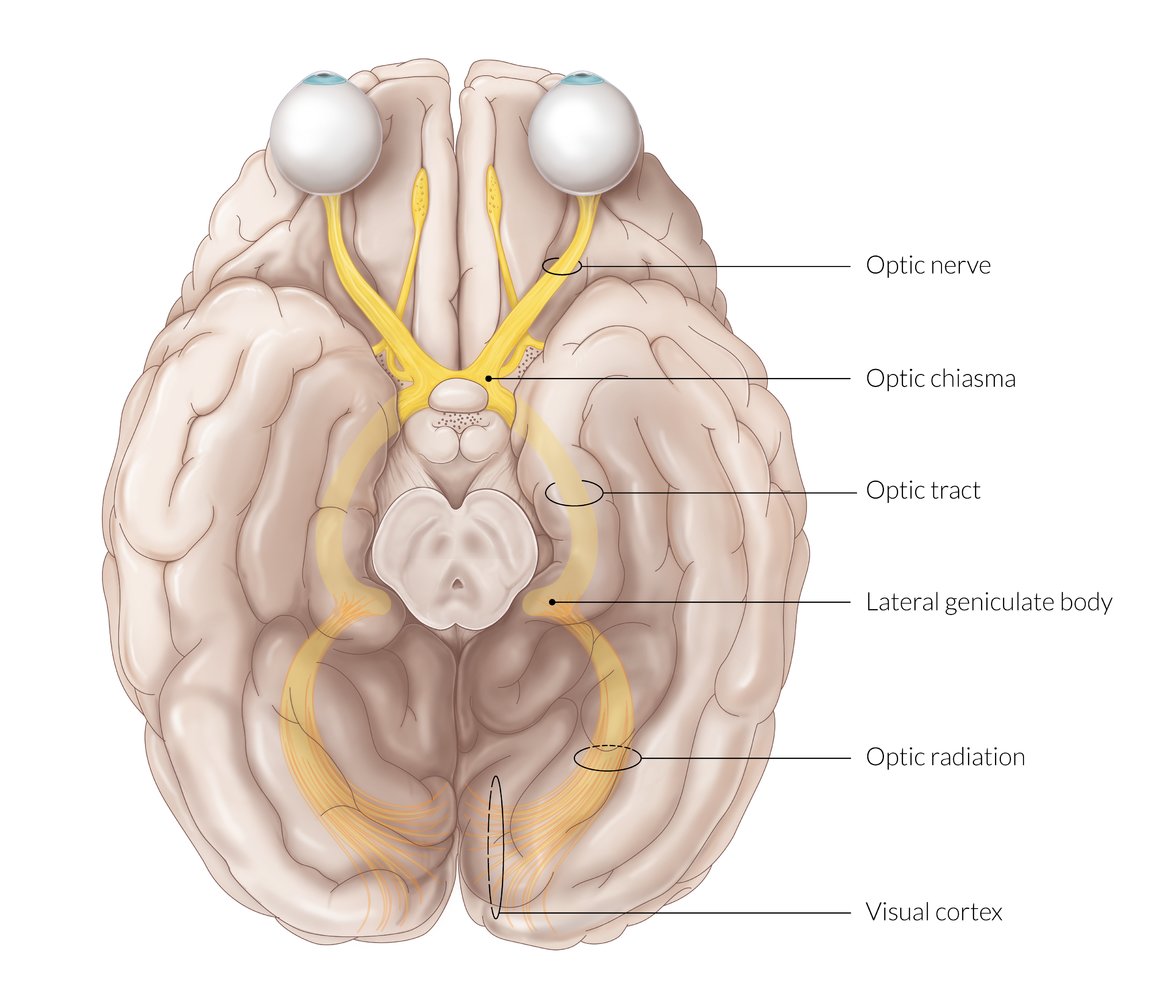
Optic nerve
- Intraorbital part: Each optic nerve arises from the axons of the retinal ganglion cells and leaves the eyeball through the lamina cribrosa of the sclera (at the posterior aspect of the eyeball).
- Intracranial part: Each optic nerve enters the middle cranial fossa through the optic canal and ends inferior to the pituitary gland at the optic chiasm, where the nasal fibers (carrying information from the temporal visual fields) cross to the opposite side.
Optic tracts: arise from the optic chiasm, wind around the midbrain, and end at the lateral geniculate body of the thalamus
Optic radiations: arise from the lateral geniculate body and terminate in the visual cortex of the occipital lobe
© AMBOSS
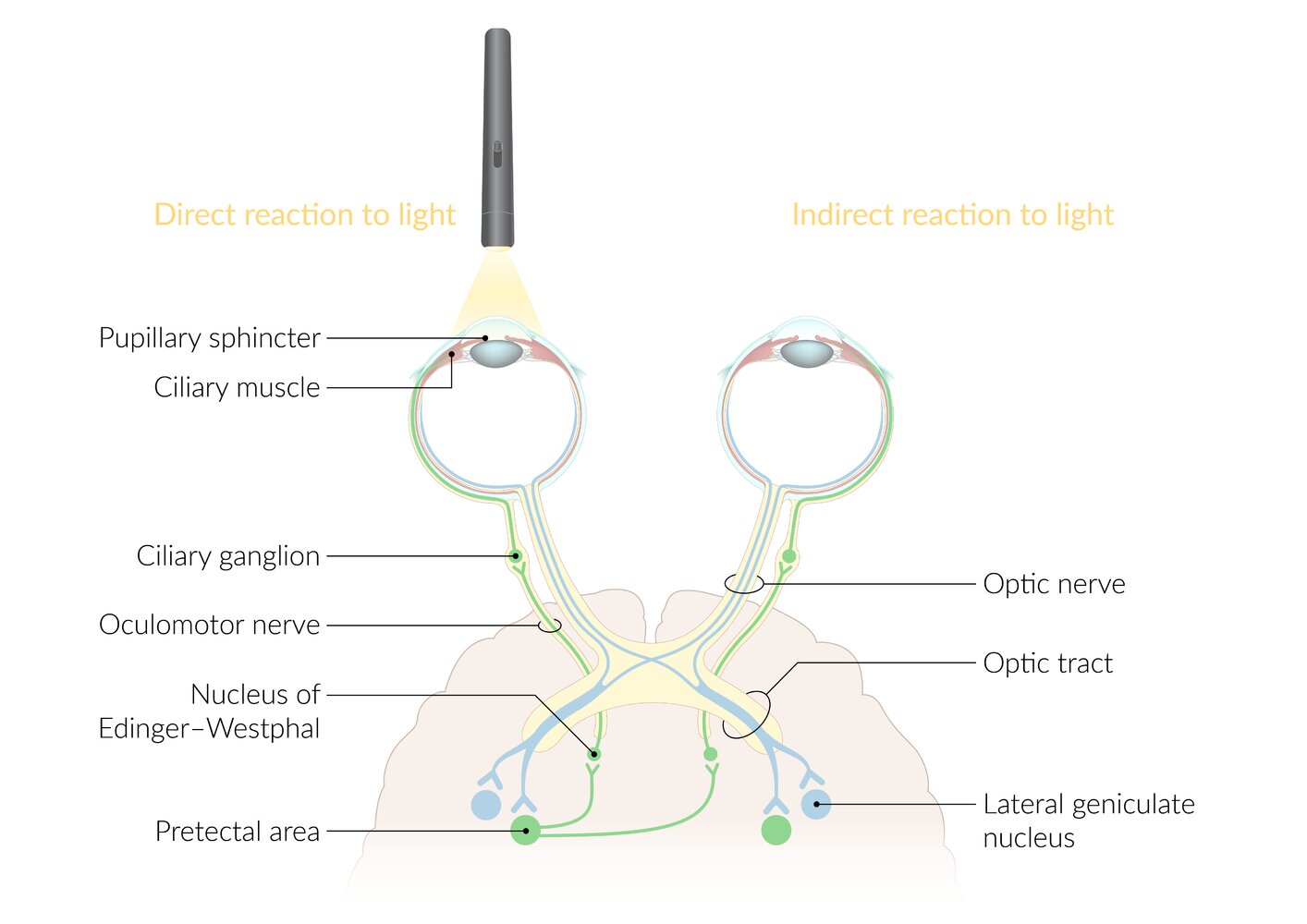
The afferent pathway (blue tract) is initiated when light hits the retina:
- Retinal photoreceptors → ipsilateral optic nerve → nuclei of bilateral pretectal areas (nasal fibers of the optic nerve cross to the contralateral side at the optic chiasma)
The efferent pathway (green tract) transmits neural impulses to the iris sphincter muscle:
- Nuclei of pretectal area → bilateral Edinger Westphal nuclei (parasympathetic preganglionic nucleus of the oculomotor nerve) → bilateral oculomotor nerves (synapse at the ciliary ganglion) → bilateral iris sphincter muscle (and ciliary muscle) → bilateral pupillary constriction (and accomodation).
Shining a light into one eye causes constriction of the ipsilateral pupil (direct pupillary reflex) as well as that of the contralateral pupil (indirect or consensual pupillary reflex).
© AMBOSS
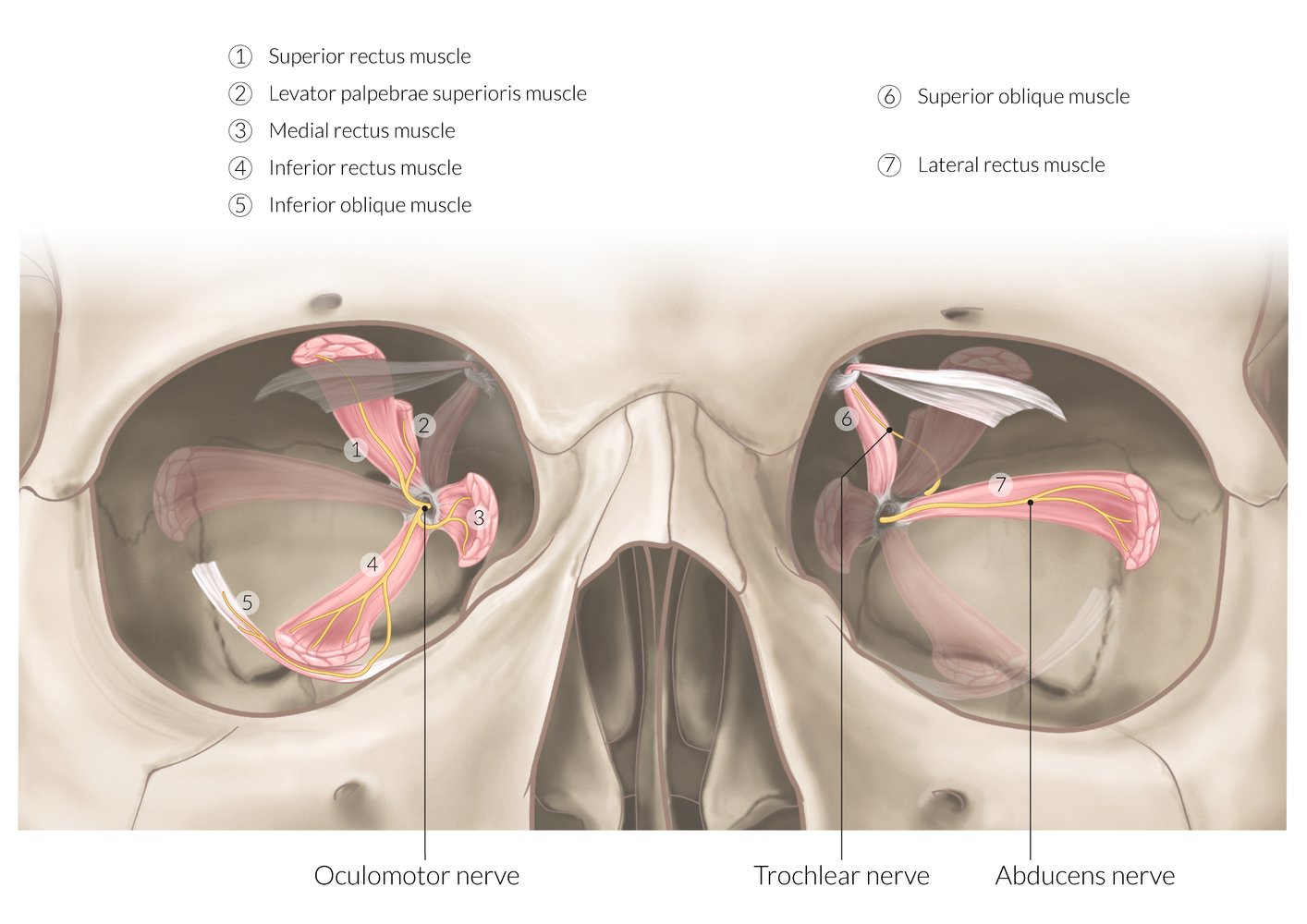
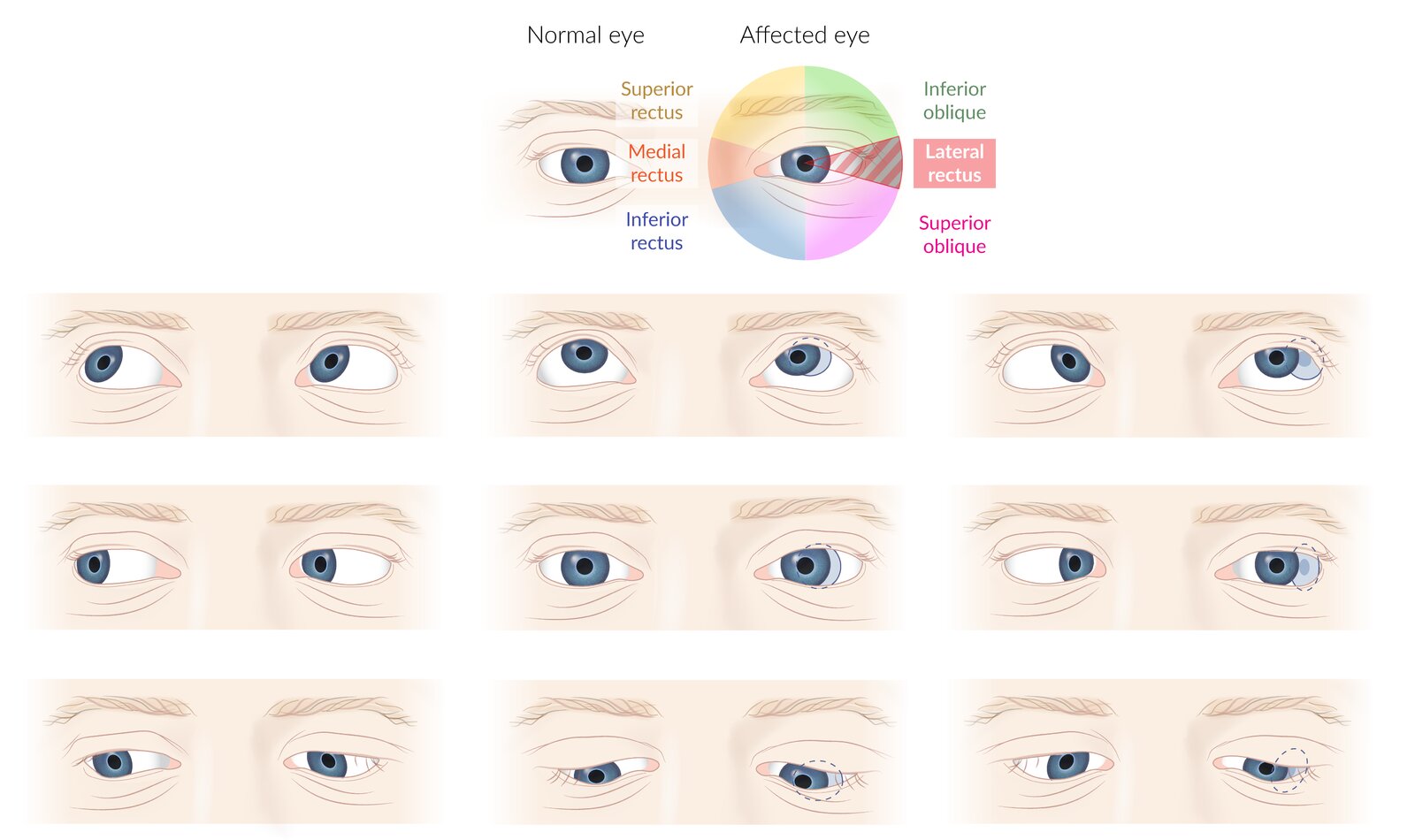
The oculomotor nerve innervates all extraocular muscles (1–5) apart from the superior oblique muscle (6; innervated by the trochlear nerve) and the lateral rectus muscle (7; innervated by the abducens nerve).
© AMBOSS
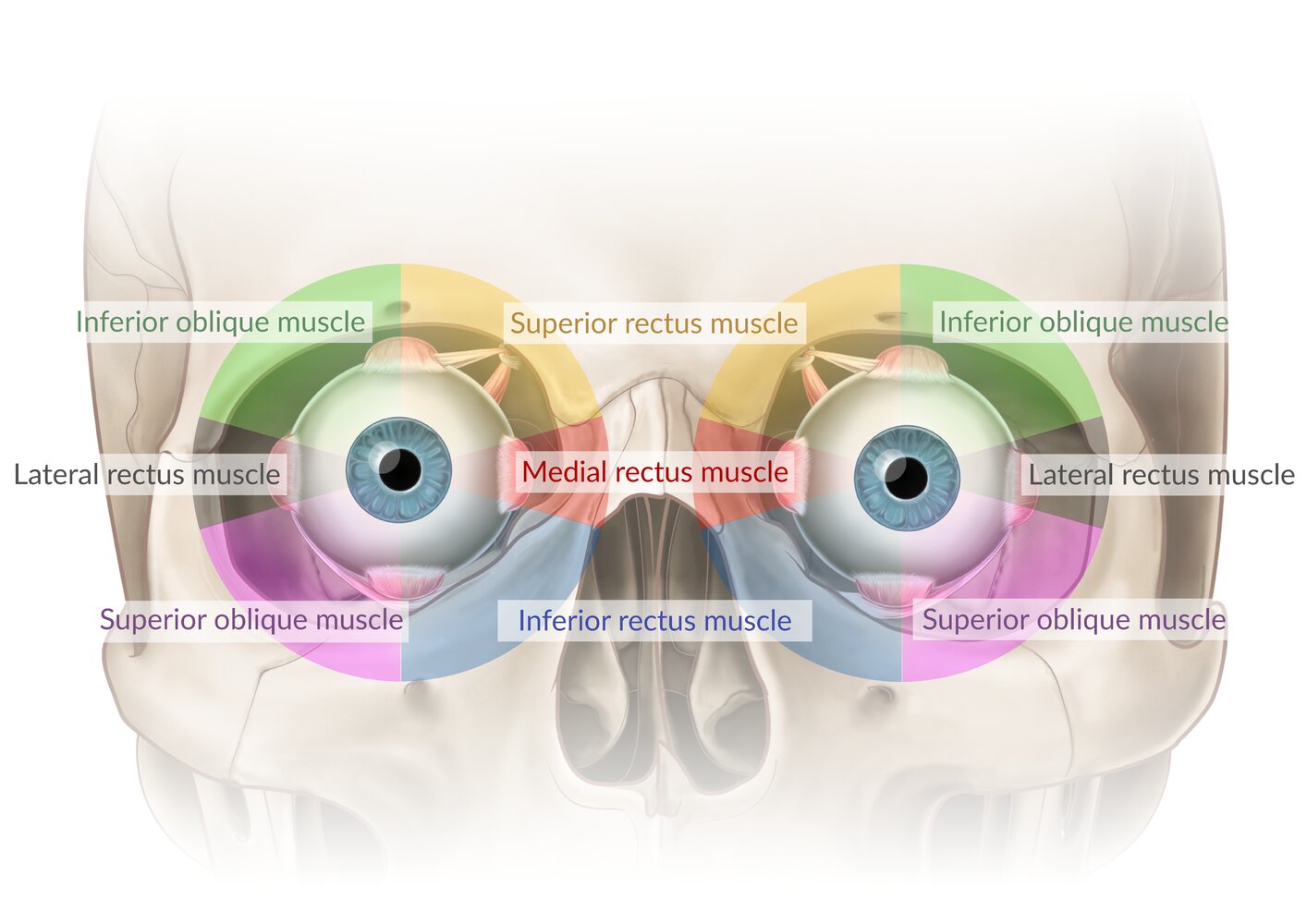
This illustration depicts the directions the individual extraocular muscles would move the gaze if acting in isolation.
Note that for all muscles, except the lateral and medial recti, these are not the directions in which these muscles are tested clinically. The difference arises because eye movements are the result of complex interactions between several extraocular muscles. Therefore, the movement used to test a particular muscle clinically is the movement that most effectively excludes the participation of other muscles. For example, while the superior oblique (SO) depresses and abducts the eye when acting in isolation (as shown here), depression is also produced by the inferior rectus (IR), and abduction is also produced by the lateral rectus (LR). However, due to their different points of insertion, the IR is the more efficient depressor of the eye in abduction, while the SO is the more efficient depressor in adduction. Looking down and inwards, therefore, allows the isolated clinical examination of the SO. Similar principles apply to the movements used for clinical testing of the IR, SR, and IO.
© AMBOSS
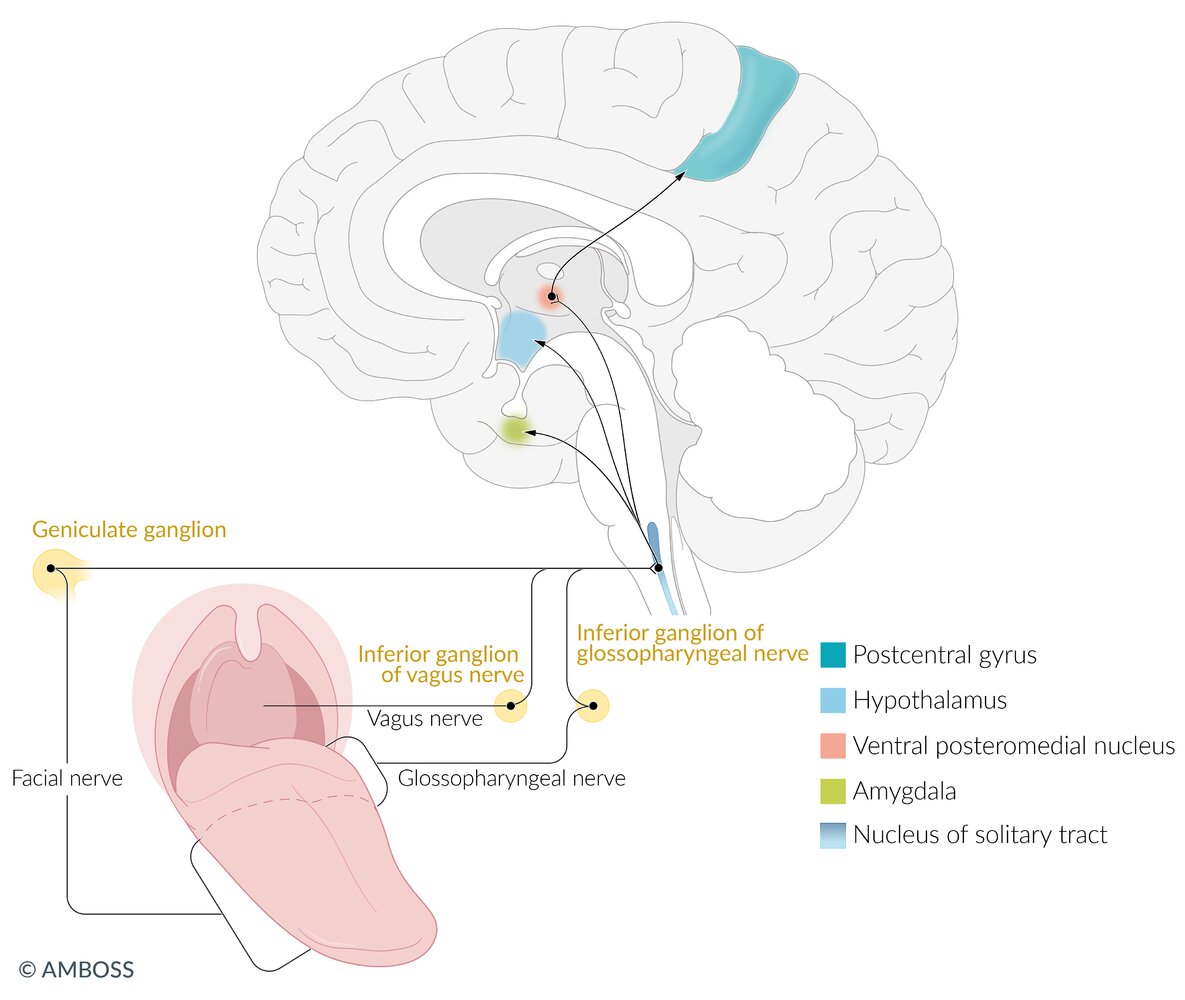
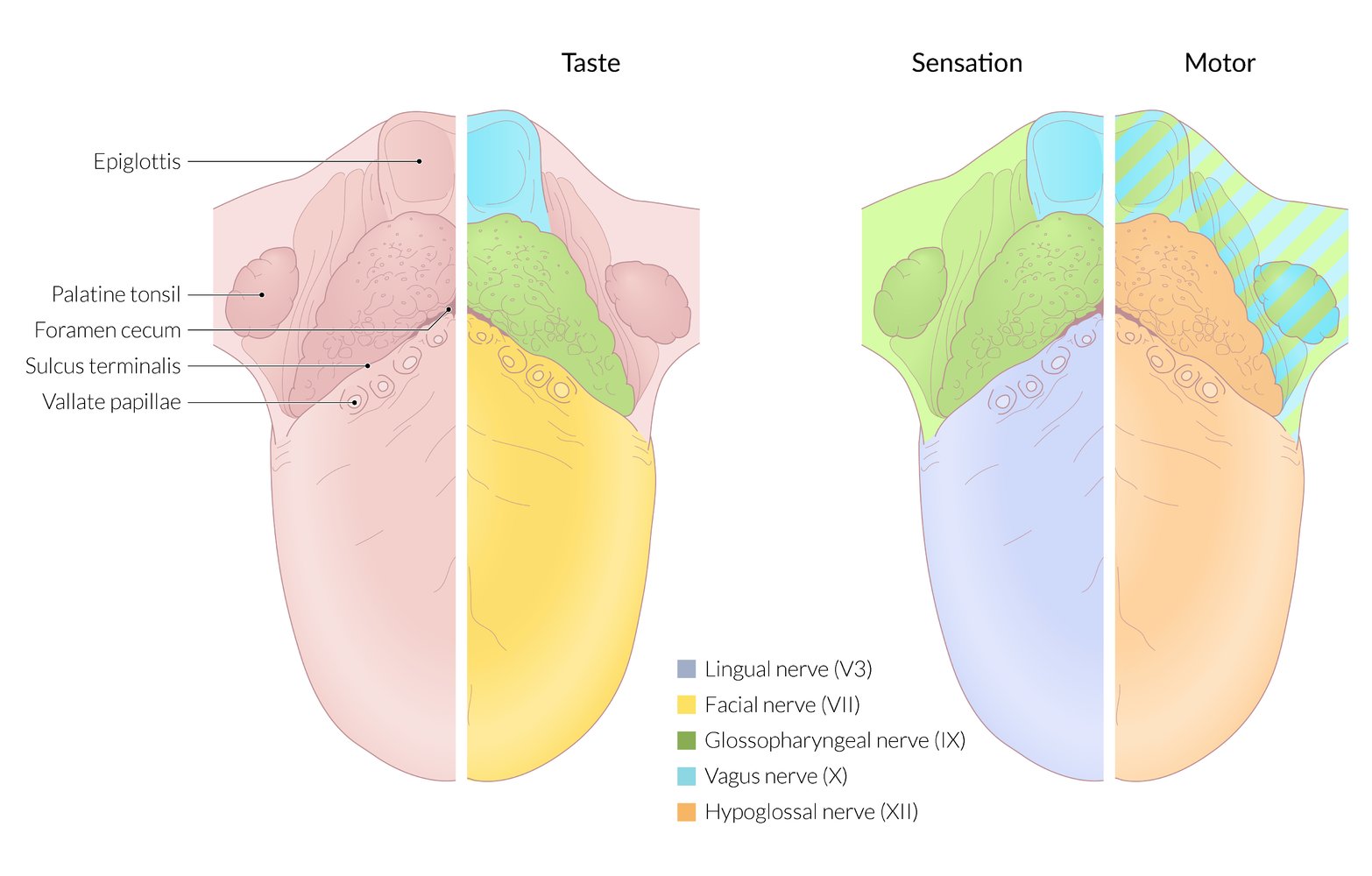
The first neuron of the taste pathway is located in the ganglia of the facial, vagus, and glossopharyngeal nerves. The afferent gustatory nerve fibers join to form the nerve tract that projects to the nucleus of the solitary tract.
Second-order neurons project from the medulla oblongata in three distinct branches. Projections to the hypothalamus and amygdala transmit the emotional component of taste perception. Projections to the ventral posterior nucleus (VPM) of the thalamus transmit to the gustatory cortex at the foot of the postcentral gyrus for conscious taste perception.
© AMBOSS
© AMBOSS
Origin and pathways of the cranial nerves
Gross anatomy
| Origin and pathways of the cranial nerves | |||||
|---|---|---|---|---|---|
| Cranial nerve | Nerve origin | Foramina/Structures | Cranial nerve nuclei | Destination | Pathway |
| CN I |
|
|
|
|
|
| CN II |
|
|
|
|
|
| CN III |
|
|
|
|
|
| CN IV |
|
|
|
|
|
| CN V |
|
|
|
|
|
| CN VI |
|
|
|
|
|
| CN VII |
|
|
|
|
|
| CN VIII |
|
|
|
|
|
| CN IX |
|
|
|
|
|
| CN X |
|
|
|
|
|
| CN XI |
|
|
|
|
|
| CN XII |
|
|
|
|
|
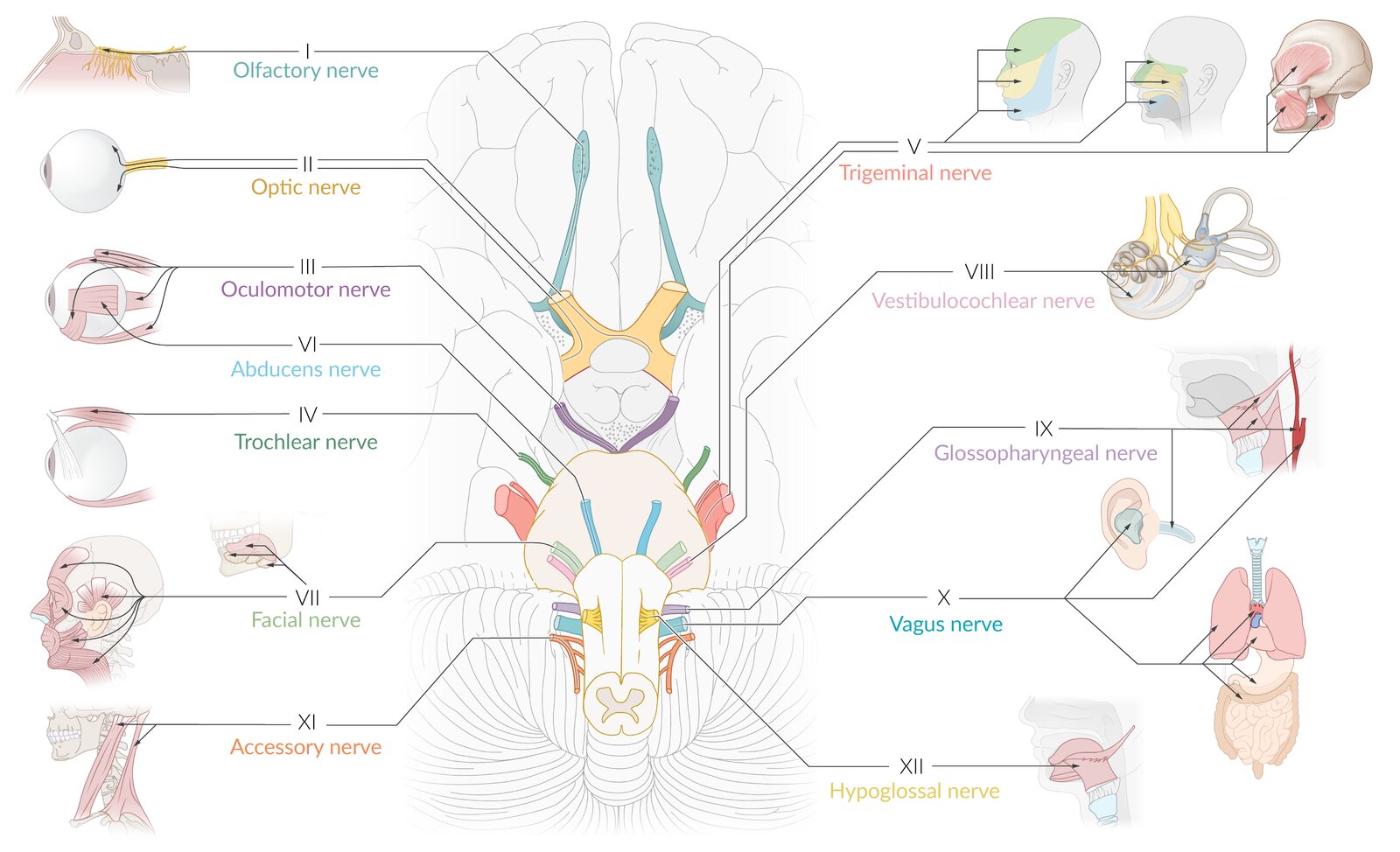
CN I–IV are located in the midbrain, V–VIII in the pons,and IX–XII in the medulla.
The nuclei located in the medial brainstem are factors of 12, except 1 and 2 (i.e., CN III, CN IV, CN VI, and CN XII).
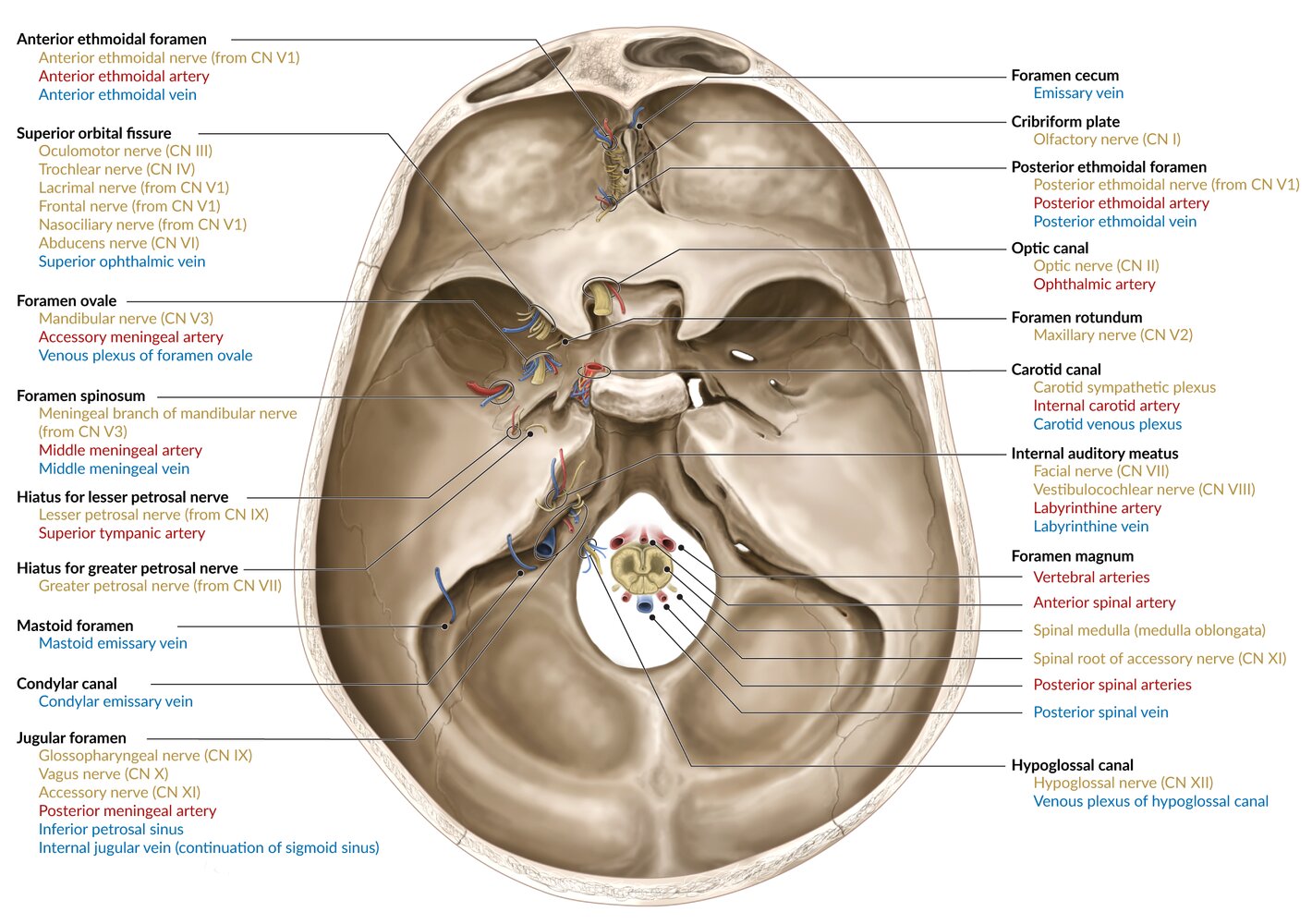
“Standing Room Only”: CN V1 exits through Superior orbital fissure, CN V2 exits through foramen Rotundum, and CN V3 exits through foramen Ovale.
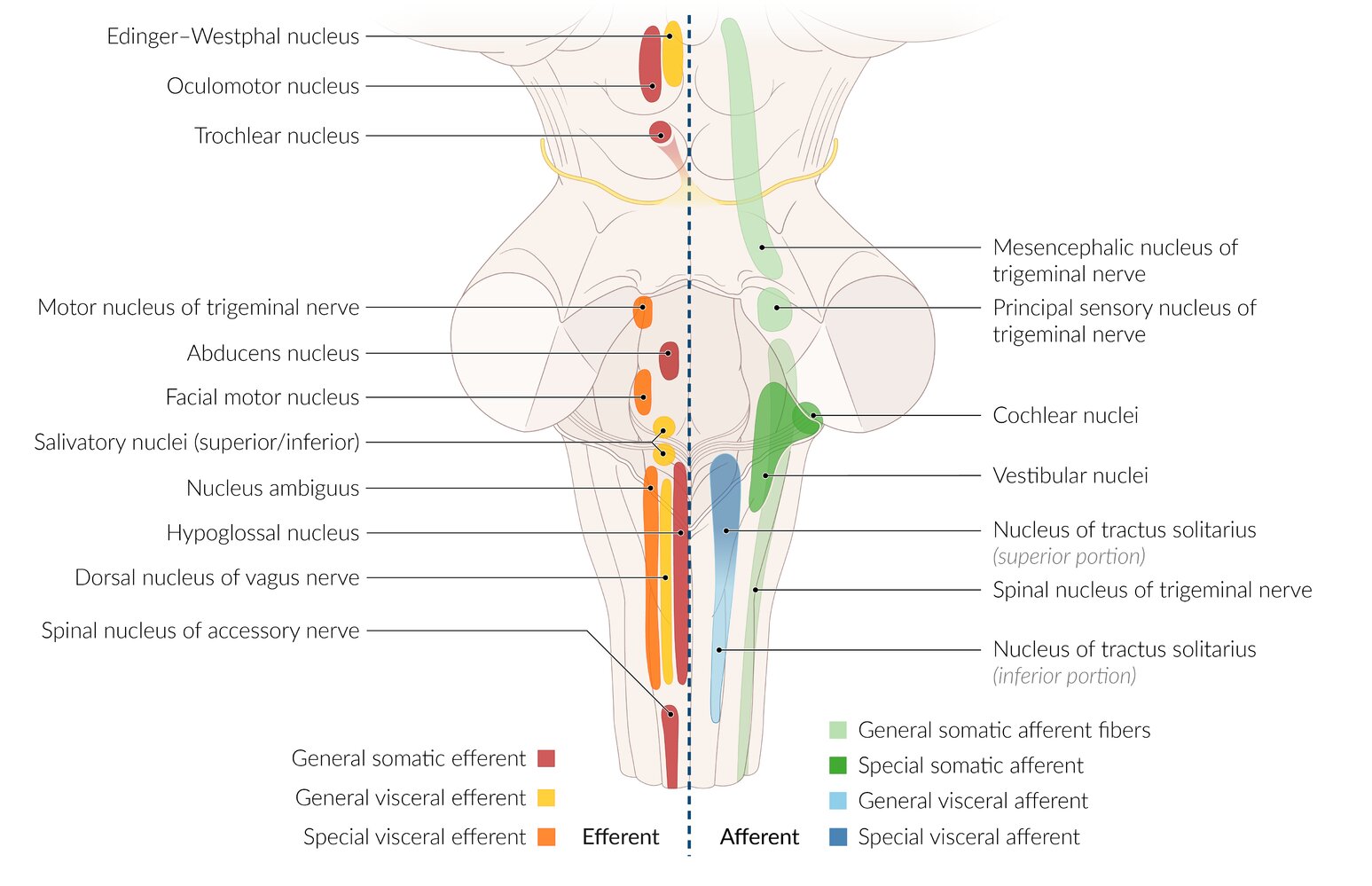
The sulcus limitans in the 4th ventricle separates the CN Motor nuclei in the Medial part of the brain stem (basal plate) from the sensory nuclei in the Lateral part (aLar plate).








")


")


3D Anatomy

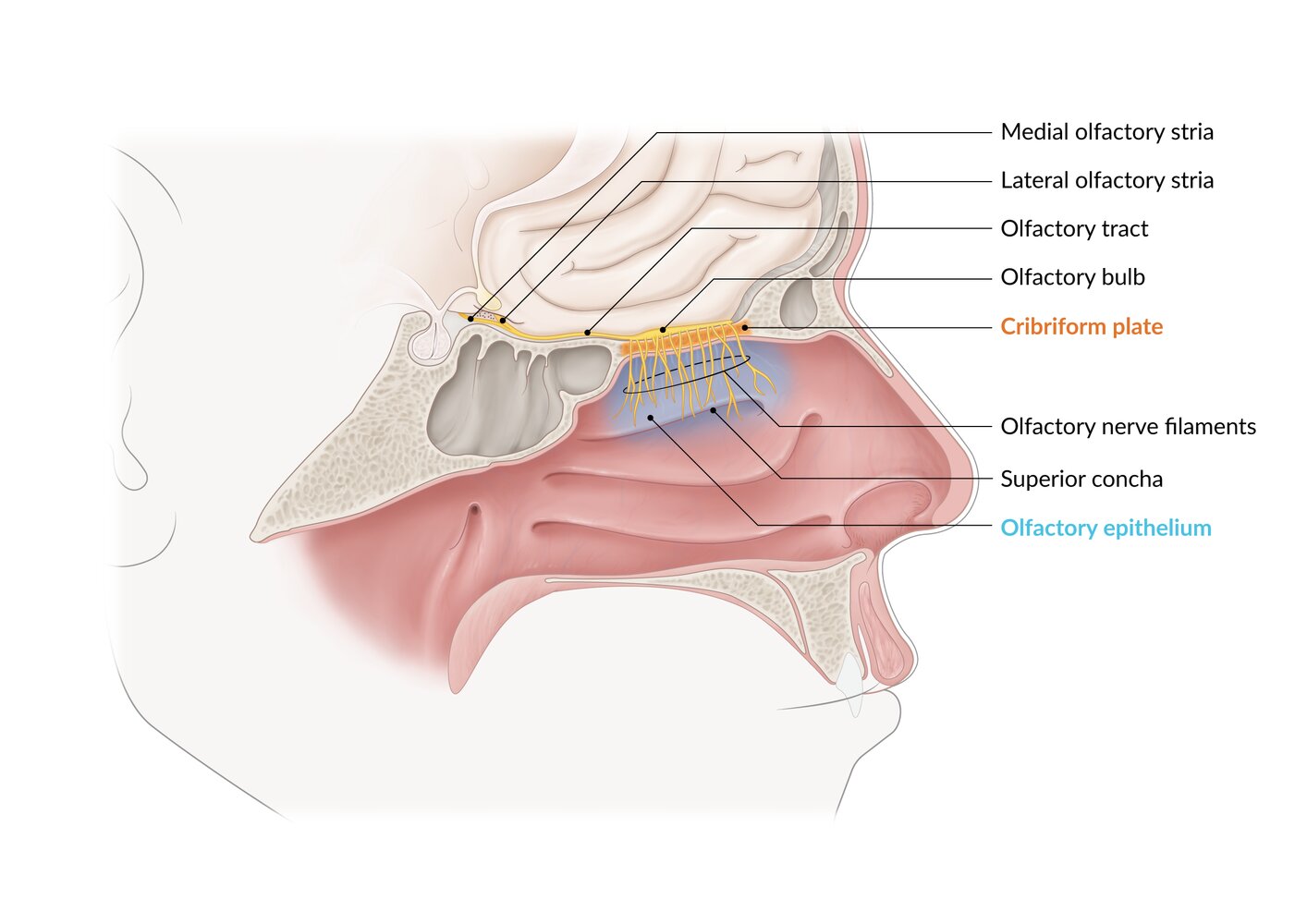
The olfactory epithelium covers the superior concha, the roof of the nose, and the upper parts of the nasal septum. This epithelium contains the olfactory receptor neurons, whose axons unite into small bundles (olfactory nerve filaments), pass through the cribriform plate, and enter the olfactory bulb, where they synapse on second-order neurons. The axons of these second-order neurons form the olfactory tract, which divides into the medial and lateral olfactory striae.
© AMBOSS
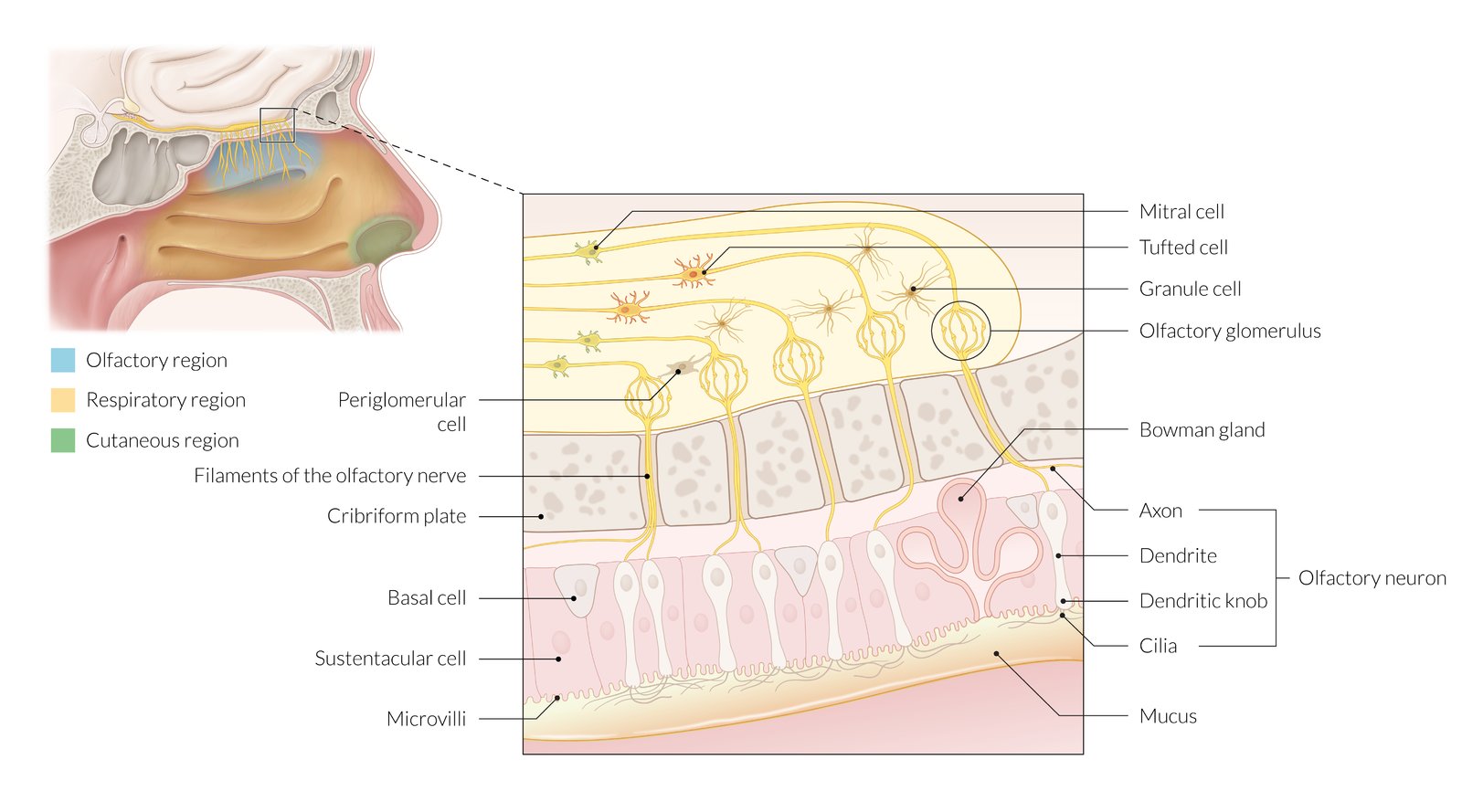
The olfactory mucosa consists of olfactory receptor neurons, sustentacular cells, basal cells, and olfactory glands. The olfactory receptor neurons have a single apical dendrite with multiple sensory cilia. The axons of the olfactory receptor neurons pass through the cribriform plate and enter the olfactory bulb, where they synapse with mitral cells and tufted cells. Periglomerular cells connect the glomeruli. Granule cells are predominantly inhibitory interneurons of the olfactory bulb and their dendrodentritic synapses contribute to lateral inhibition.
© AMBOSS
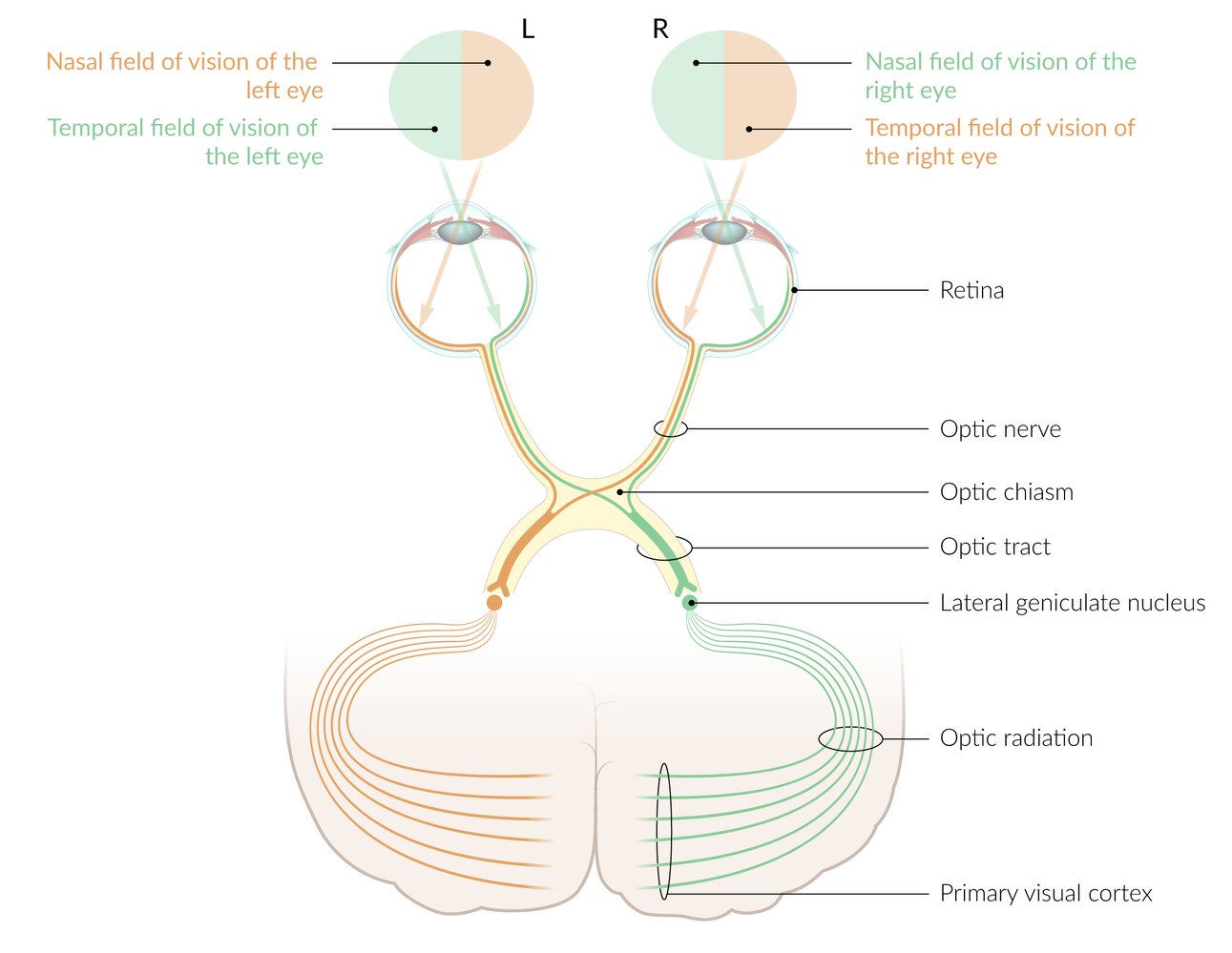
1. Retina: The visual pathway begins at the retina. The temporal field of vision is projected onto the nasal portion of the retina and the nasal field of vision is projected onto the temporal portion of the retina.
2. Optic nerves: The axons of the retinal ganglion cells merge to form the optic nerve, which carries the nasal and temporal fibers of the ipsilateral retina.
3. Optic chiasm: The two optic nerves meet at the optic chiasm, where the nasal fibers of each retina cross over to the contralateral side. The temporal fibers remain uncrossed.
4. Optic tracts: Each optic tract carries contralateral nasal fibers and ipsilateral temporal fibers (i.e., the right optic tract carries the nasal fibers of the left eye and the temporal fibers of the right eye). I.e., each optic tract carries the contralateral visual field of each eye.
5. Lateral geniculate nucleus (LGN): The optic tracts synapse onto the ipsilateral LGN.
6. Optic radiation: consists of neurons that carry visual information from the ipsilateral LGN to the ipsilateral primary visual cortex
7. Primary visual cortex: The visual pathway terminates at the primary visual cortex, which is located at the posterior aspect of the occipital lobe. It is responsible for the perception of sight. The right visual cortex receives visual information from the right nasal field and the left temporal field of vision, i.e. the left visual field of each eye.
© AMBOSS
Optic nerve
- Intraorbital part: Each optic nerve arises from the axons of the retinal ganglion cells and leaves the eyeball through the lamina cribrosa of the sclera (at the posterior aspect of the eyeball).
- Intracranial part: Each optic nerve enters the middle cranial fossa through the optic canal and ends inferior to the pituitary gland at the optic chiasm, where the nasal fibers (carrying information from the temporal visual fields) cross to the opposite side.
Optic tracts: arise from the optic chiasm, wind around the midbrain, and end at the lateral geniculate body of the thalamus
Optic radiations: arise from the lateral geniculate body and terminate in the visual cortex of the occipital lobe
© AMBOSS
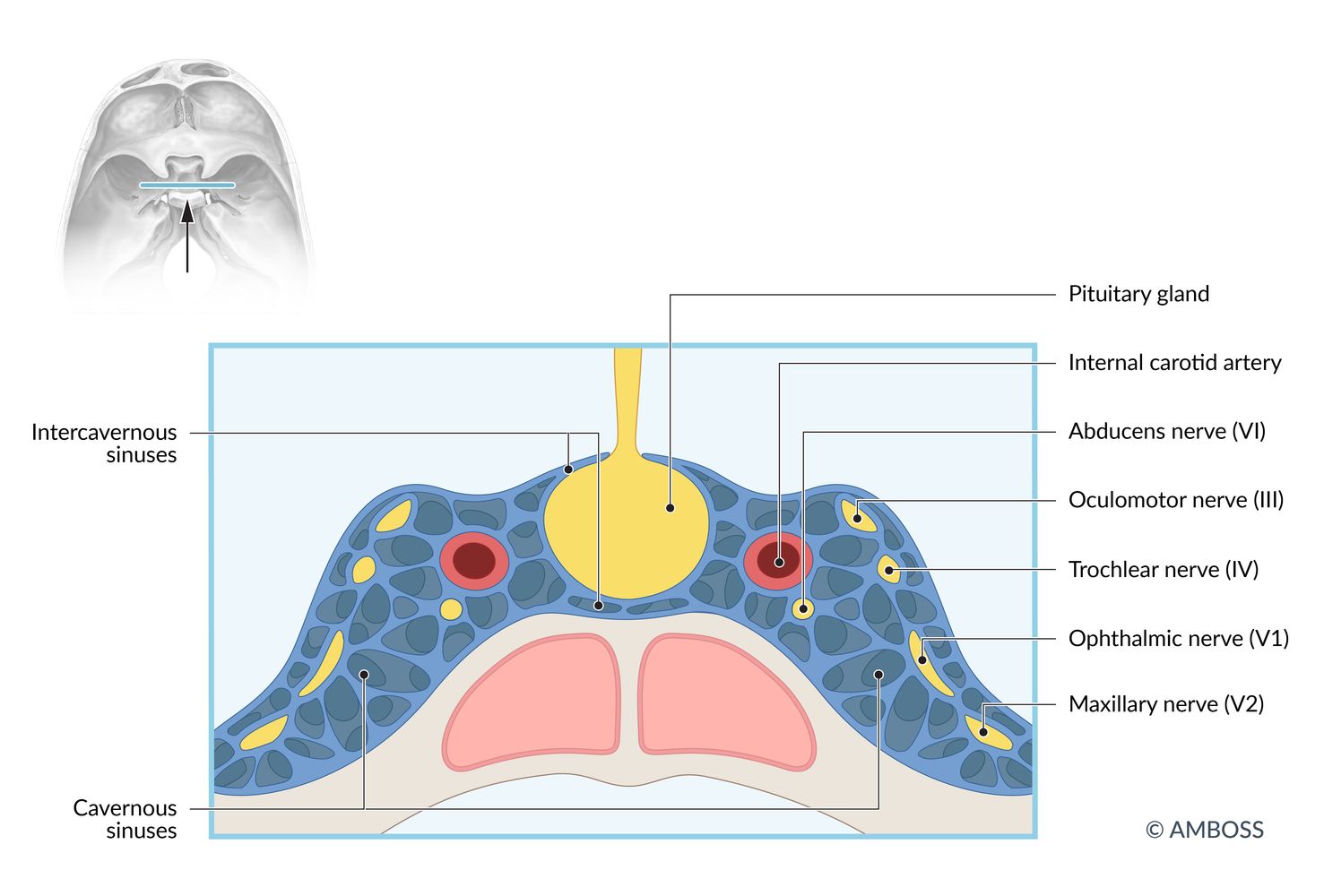
The pituitary gland lies within the pituitary fossa and is surrounded by the left and right cavernous sinuses and the intercavernous sinuses connecting them. The internal carotid artery and the abducens nerve pass through the middle of each cavernous sinus, while the oculomotor, trochlear, ophthalmic, and maxillary nerves are located towards the lateral wall of the sinuses.
© AMBOSS

Anatomical preparation of the left orbit and cavernous sinus (dorsolateral view)
Click on the microscope icon to zoom in and out of the specimen.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: Fr. Dr. Schliwa, Universität Bonn, Anatomisches Institut
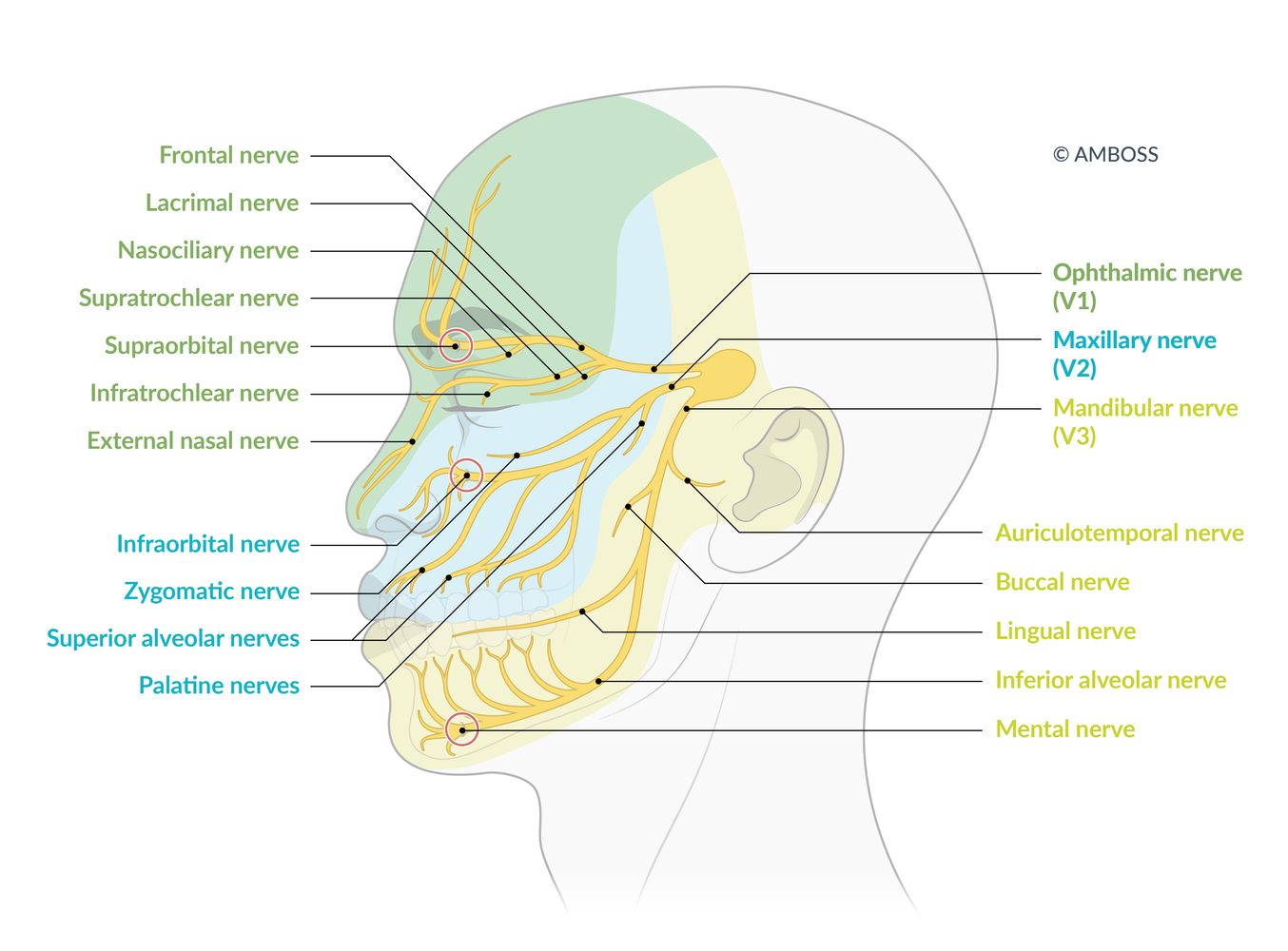
Illustrated are the 3 main branches of the trigeminal nerve (V1–V3), the areas in which they supply sensory innervation, and their subsidiary branches. The terminal superficial branches of V1–V3 are, respectively, the supraorbital, infraorbital, and mental nerves, which exit the skull at their eponymous foramina (marked with red circles). These exit points are clinically relevant as injection points for a superficial trigeminal nerve block.
© AMBOSS
© AMBOSS
The first neuron of the taste pathway is located in the ganglia of the facial, vagus, and glossopharyngeal nerves. The afferent gustatory nerve fibers join to form the nerve tract that projects to the nucleus of the solitary tract.
Second-order neurons project from the medulla oblongata in three distinct branches. Projections to the hypothalamus and amygdala transmit the emotional component of taste perception. Projections to the ventral posterior nucleus (VPM) of the thalamus transmit to the gustatory cortex at the foot of the postcentral gyrus for conscious taste perception.
© AMBOSS
Oblique cut of the right petrous temporal bone, exposing the course of the facial nerve (VII).
© AMBOSS
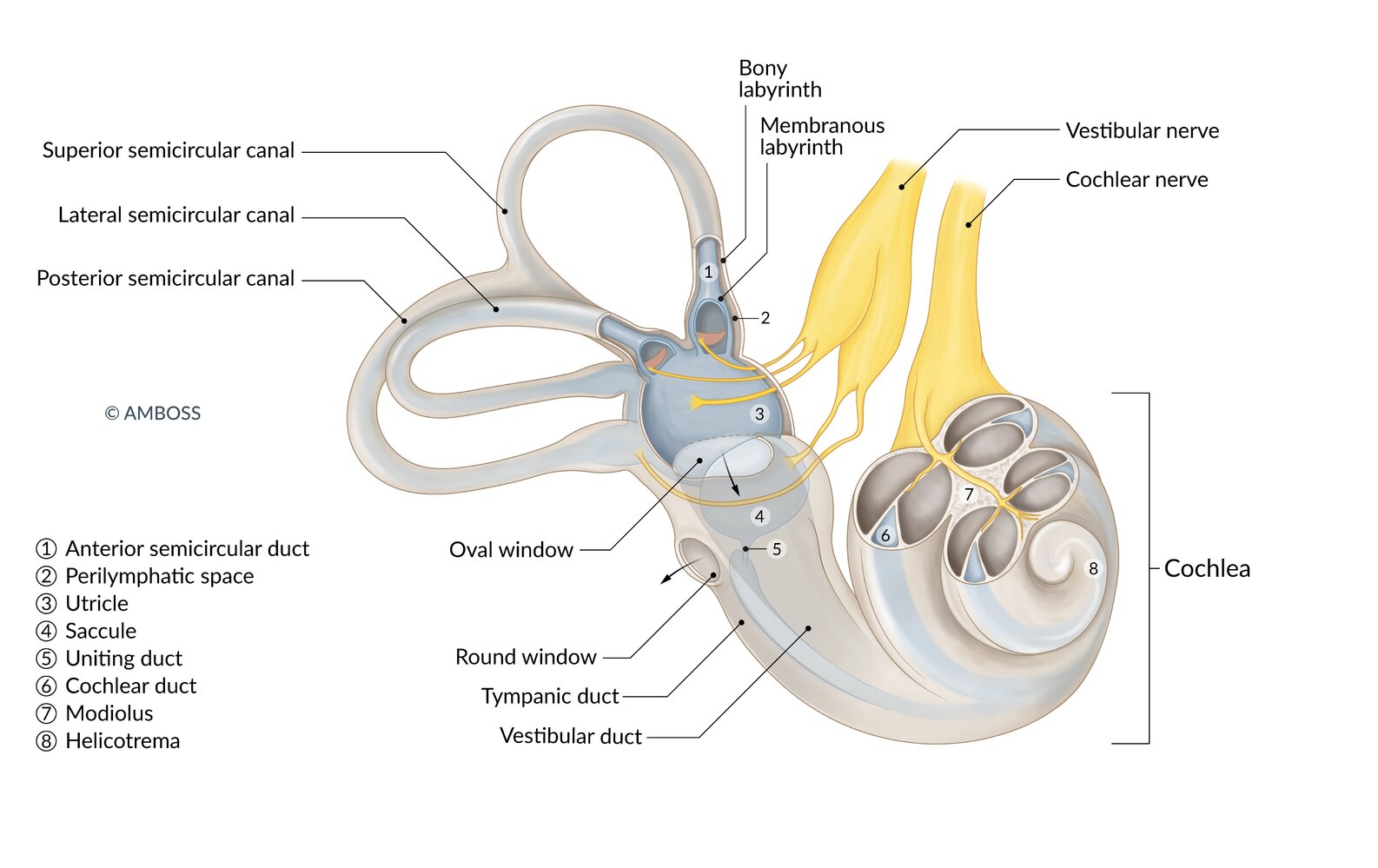
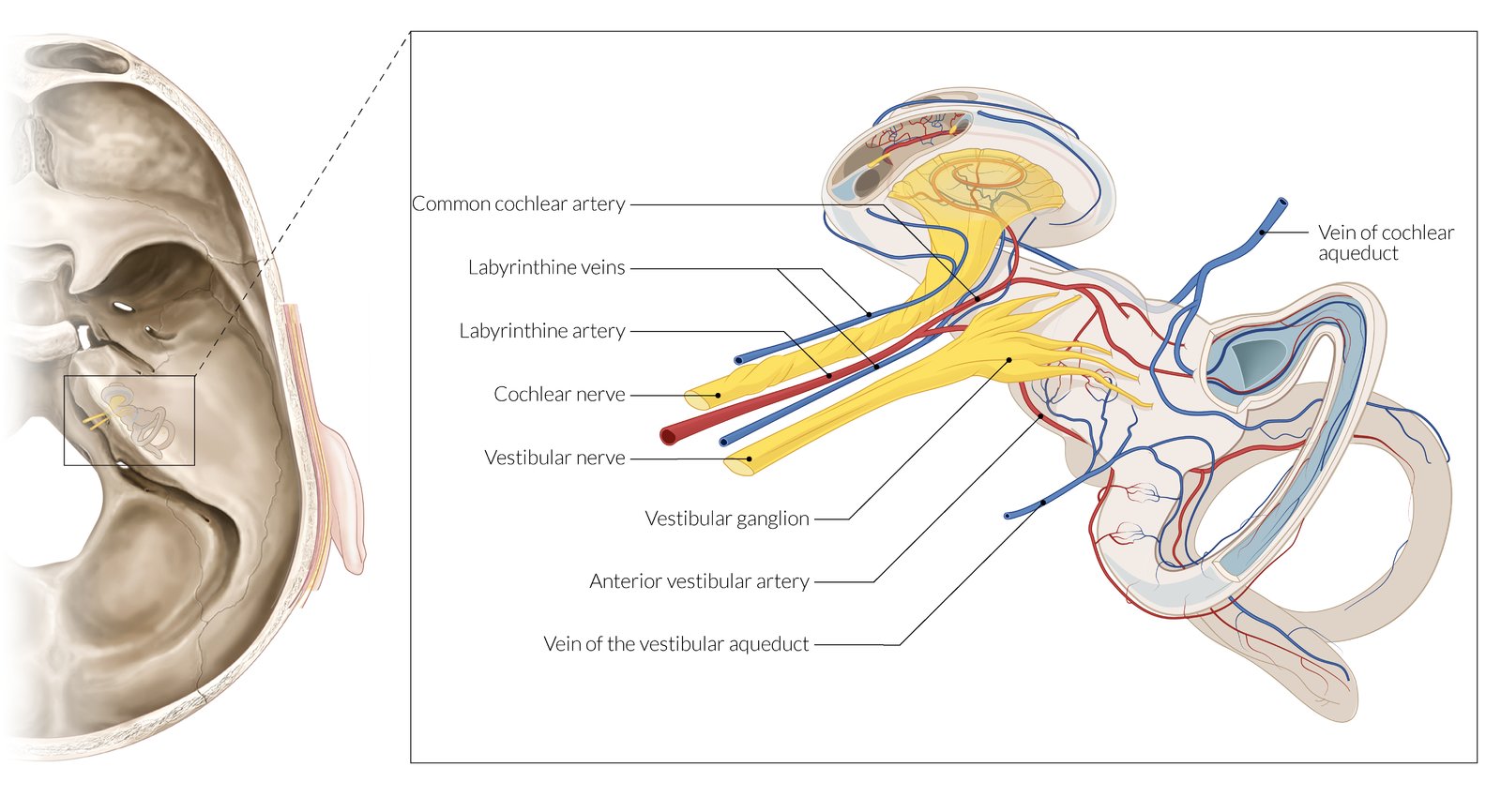
The inner ear consists of a bony labyrinth with a membranous labyrinth inside it, separated by a space containing perilymph fluid. It contains the cochlea and vestibular system. The cochlea (on the right) is responsible for the conversion of sound waves into neuronal signals, which are transmitted via the cochlear nerve (depicted by a cartoon DJ). The vestibular system (on the left) consists of three semicircular canals, the saccule, and the utricle. Semicircular canals detect angular acceleration in three planes: the superior or anterior semicircular canal in the sagittal plane, the posterior semicircular canal in the coronal plane, and the lateral or horizontal semicircular canal in the transverse plane. The saccule and utricle contain cells that detect linear motion in the vertical and horizontal planes, respectively. The neuronal signals from the semicircular canals are transmitted via the vestibular nerve (depicted by a dancing cartoon).
© AMBOSS
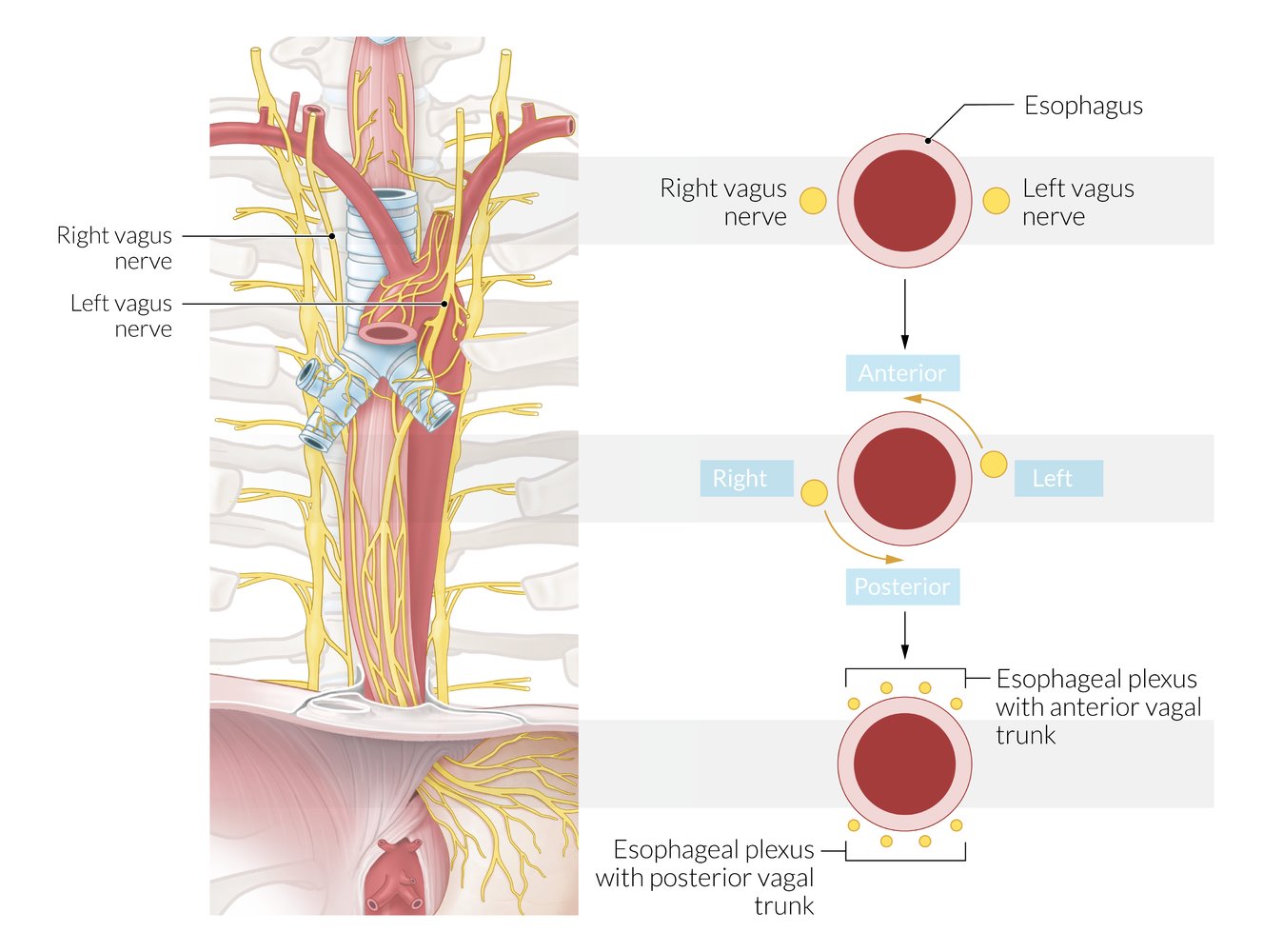
During embryonic development, the stomach rotates 90 degrees clockwise on the longitudinal axis. As a result, the left vagus nerve runs along the front of the esophagus (anterior), whereas the right vagus nerve descends along the back of the esophagus (posterior).
Below the level of the tracheal bifurcation, both vagus nerves exchange fibers that form the anterior and posterior esophageal plexus. The esophageal plexus then extends downward into the anterior (containing mainly fibers from the left vagus) and posterior vagal trunk (containing mainly fibers from the right vagus). The vagal trunks carry parasympathetic fibers to the lower esophagus.
The anterior vagal trunk ends on the anterior side of the stomach. The posterior vagal trunk provides parasympathetic innervation of the gastrointestinal tract up to the splenic flexure.
© AMBOSS
Ventral view
© AMBOSS
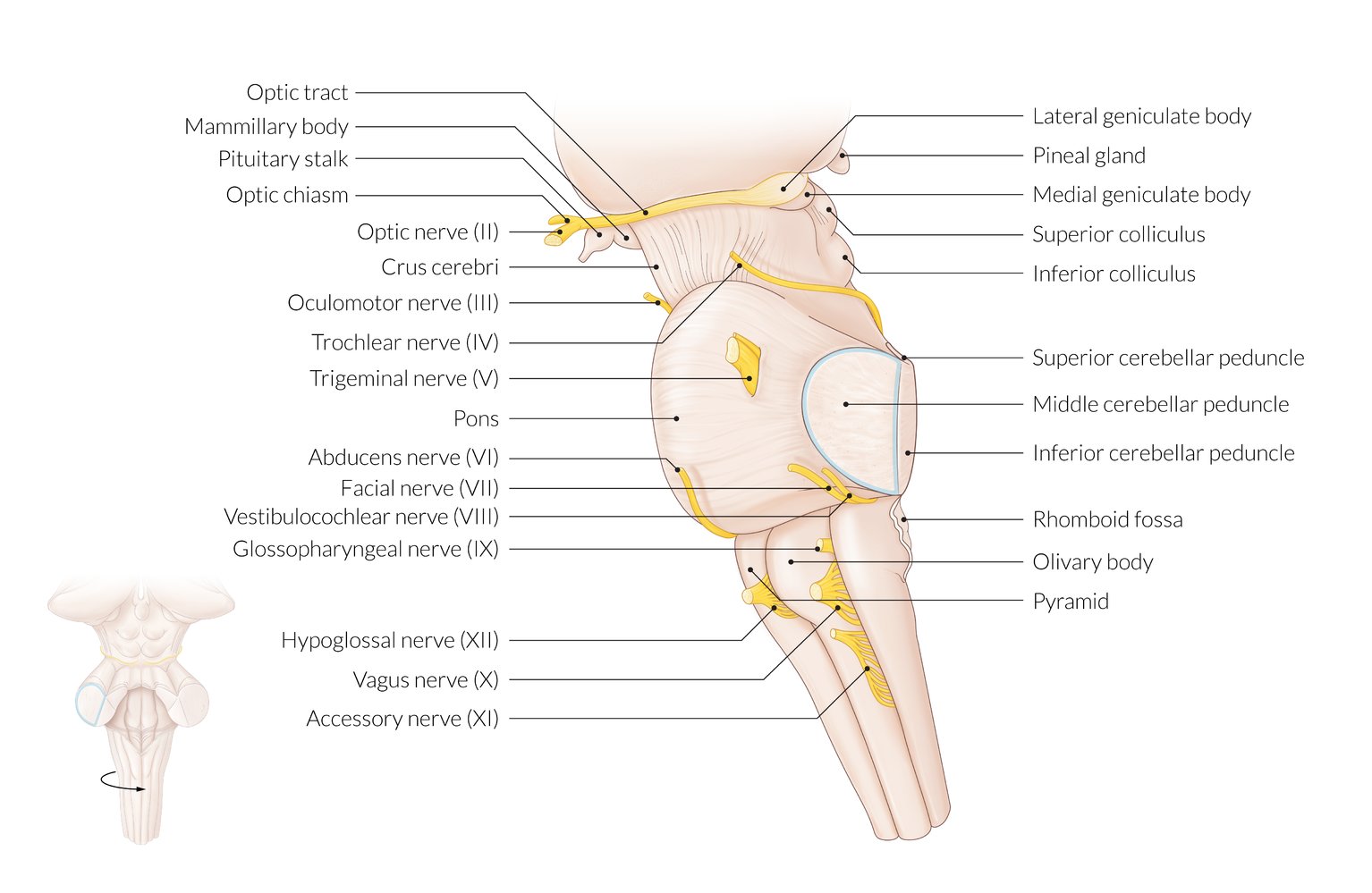
Lateral view
© AMBOSS
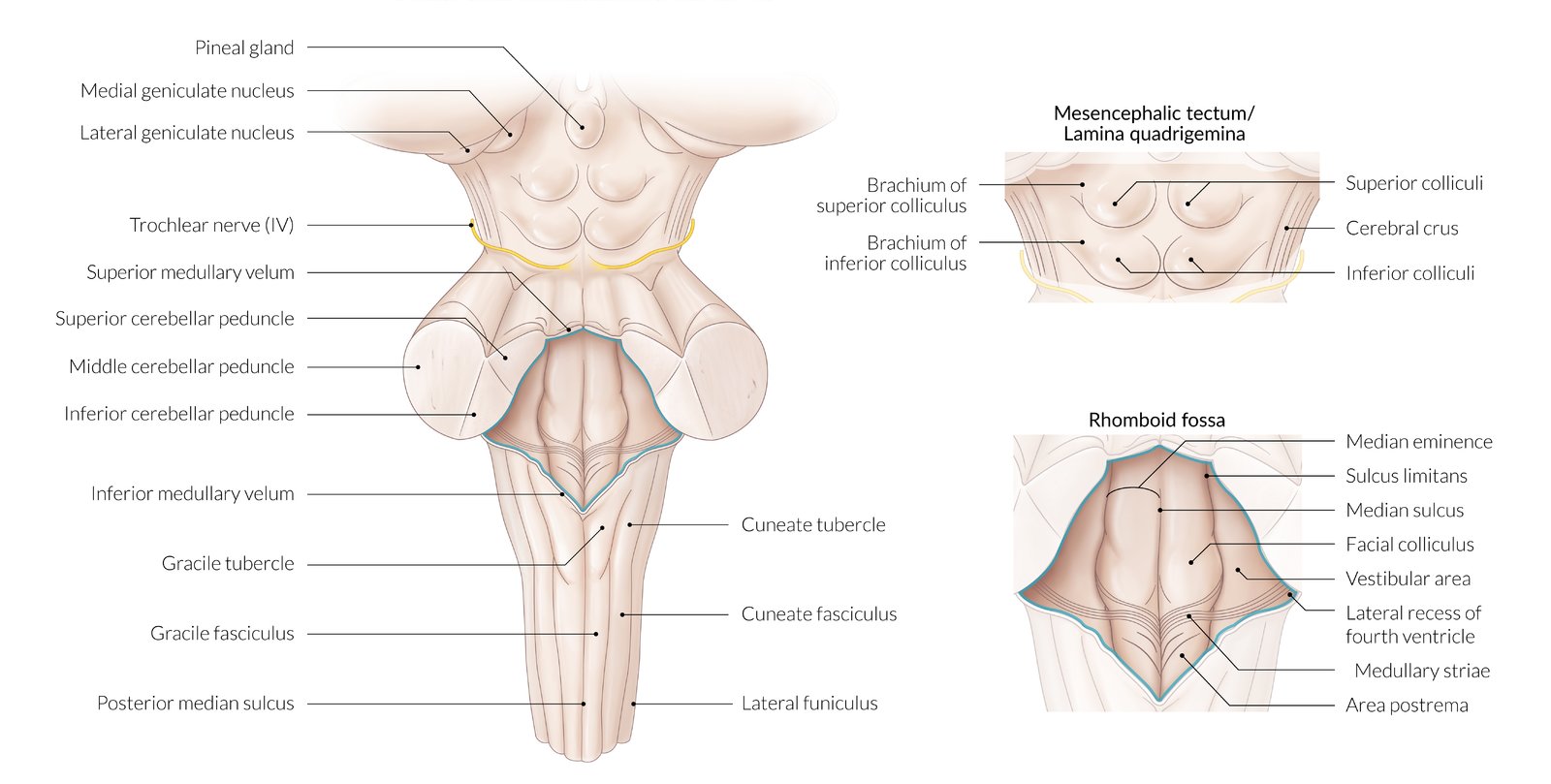
Dorsal view
The mesencephalic tectum and rhomboid fossa have distinct structures and functions. The rhomboid fossa is flanked by three pairs of cerebellar peduncles (superior, middle, and inferior) that connect the brainstem to the ipsilateral cerebellar cortex.
© AMBOSS
Sagittal section of the brainstem
© AMBOSS
Dorsal view of the brainstem
© AMBOSS
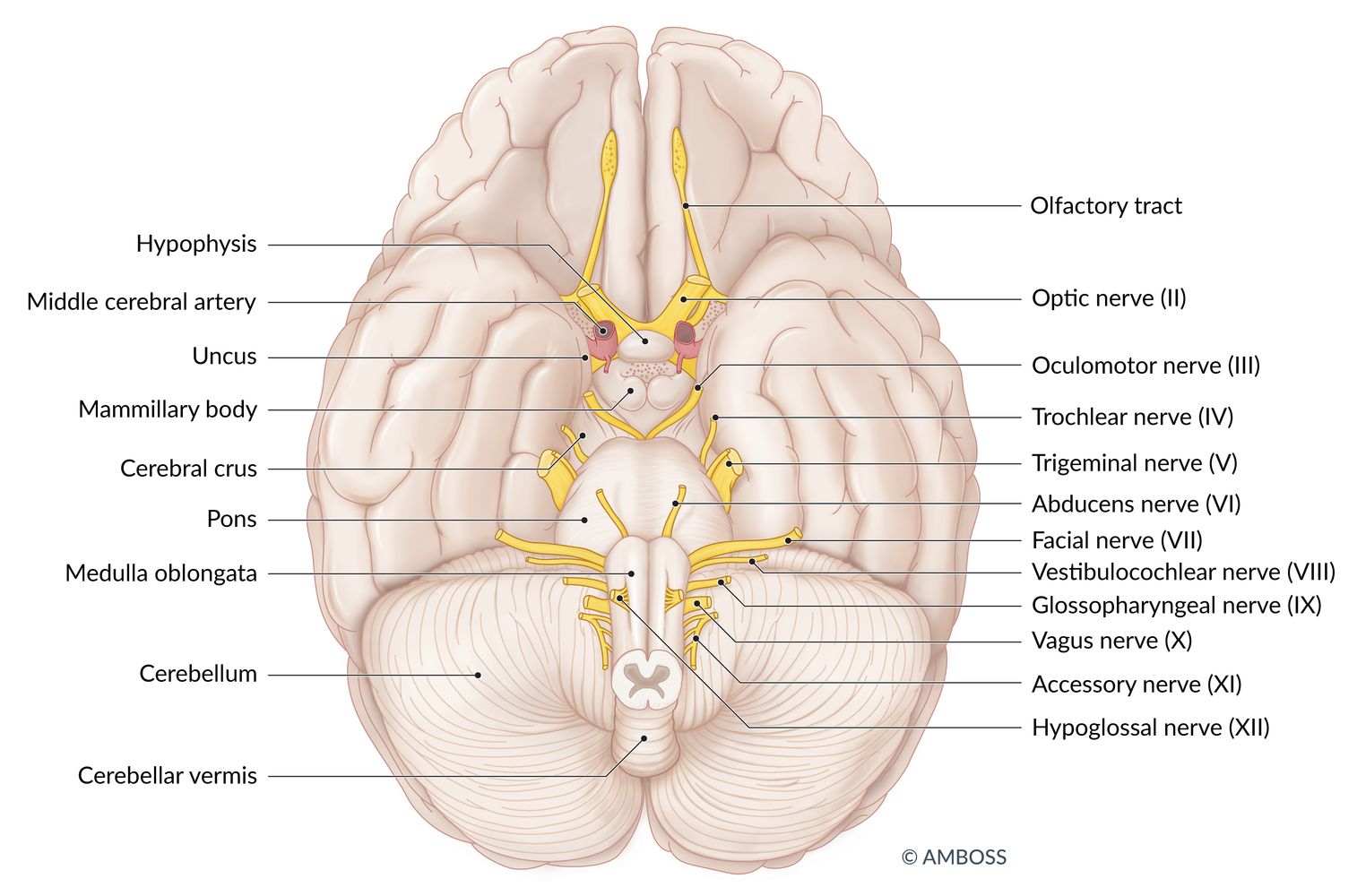
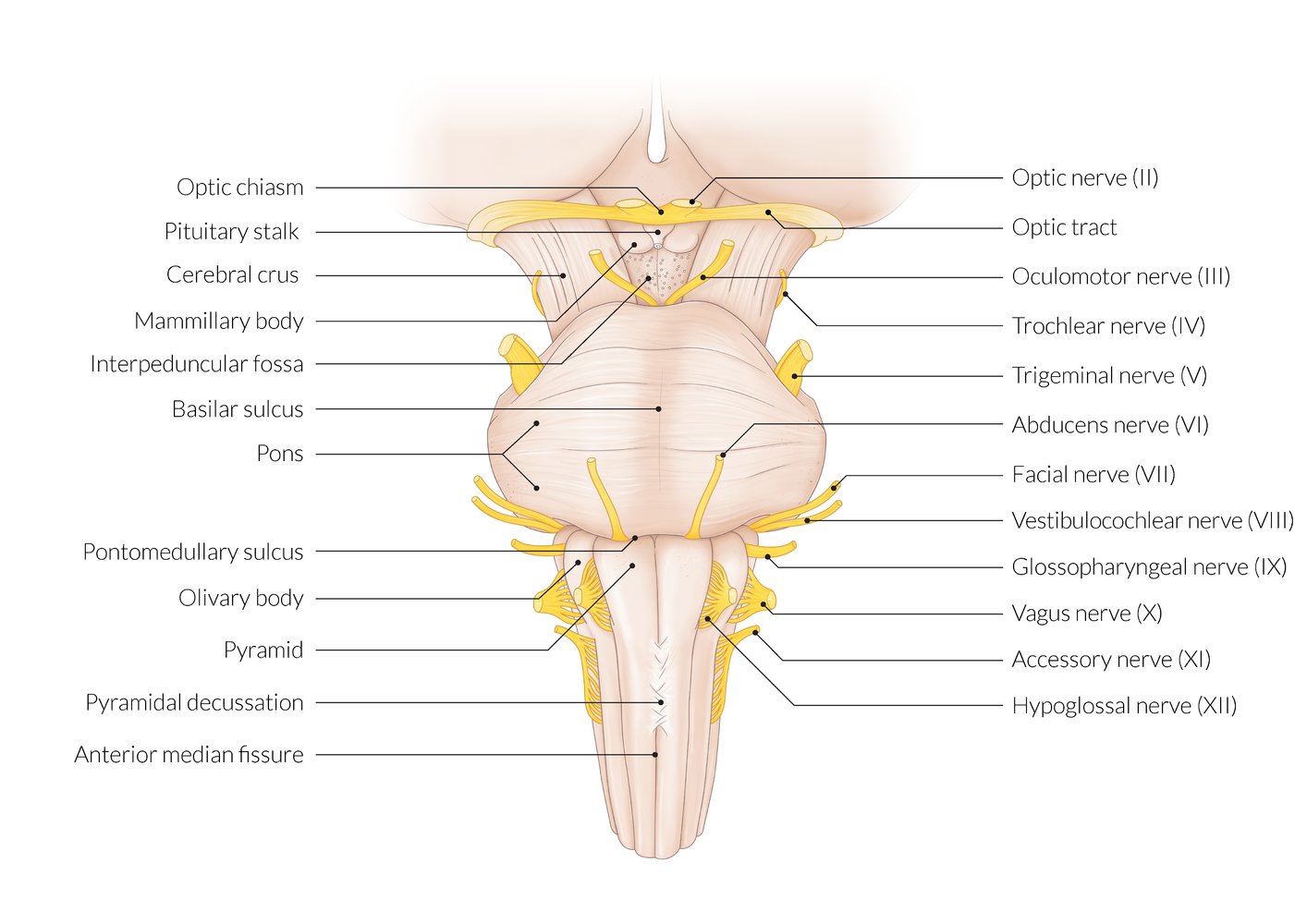
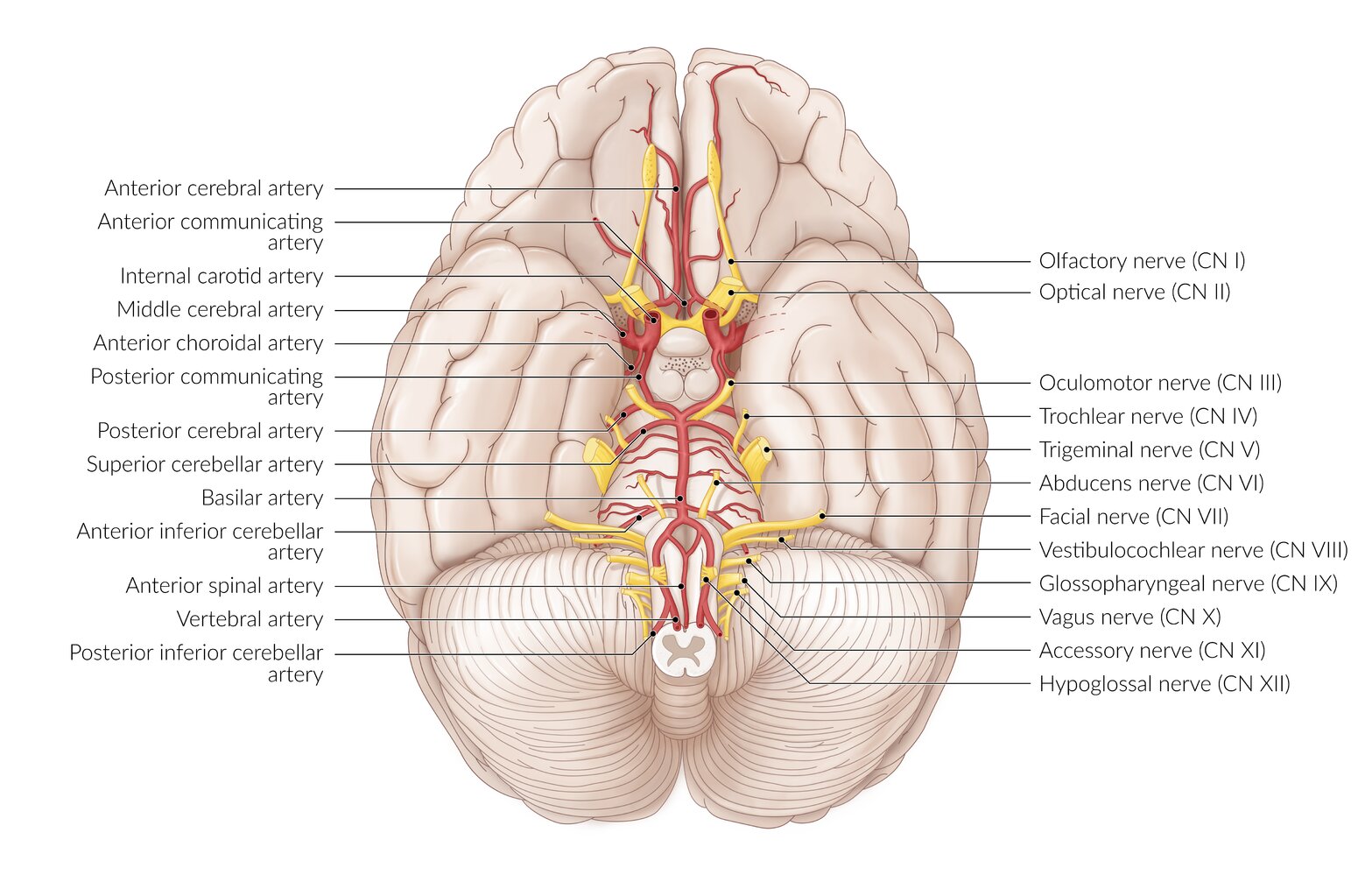
Ventral view of the brain
Anterior cerebrum: CN I and II. CN I, the olfactory nerve, is not visible in this view. The labeled olfactory tract forms the continuation of the olfactory pathway from the olfactory bulb, where CN I synapses.
Midbrain: CN III and IV
Pons: CN V, VI, VII, and VIII
Medulla: CN IX, X, XI, and XII
© AMBOSS
© AMBOSS

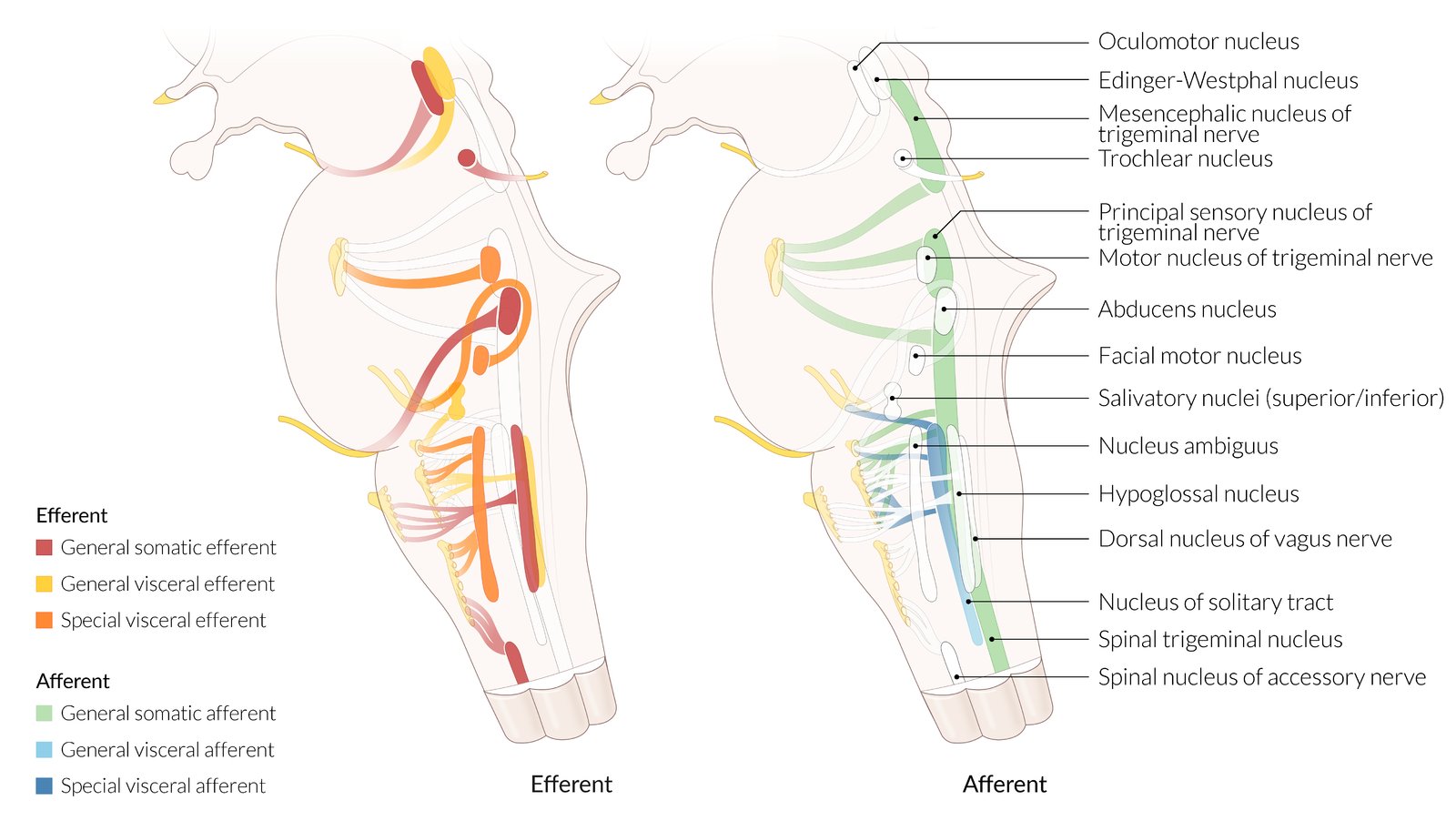
Transverse section
Typically, the efferent cranial nuclei are located medially while the afferent nuclei are located more laterally.
© AMBOSS
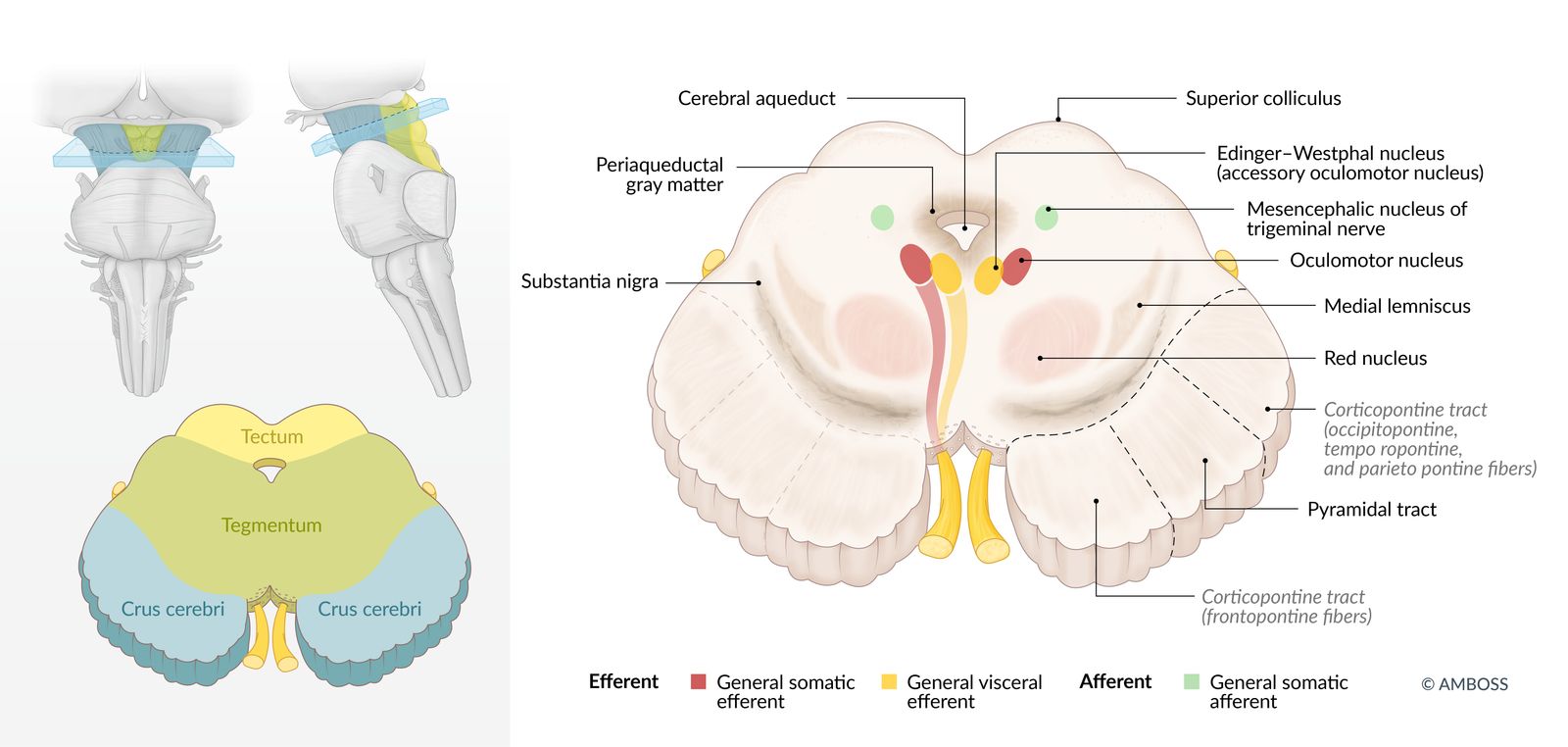
Left: Transverse section at the level of the superior colliculi
The mesencephalon contains the tectum (yellow), the tegmentum (green), and the crus cerebri (blue).
Right: Transverse section
Important functional structures are depicted.
© AMBOSS
Superior view of internal surface
© AMBOSS
© AMBOSS
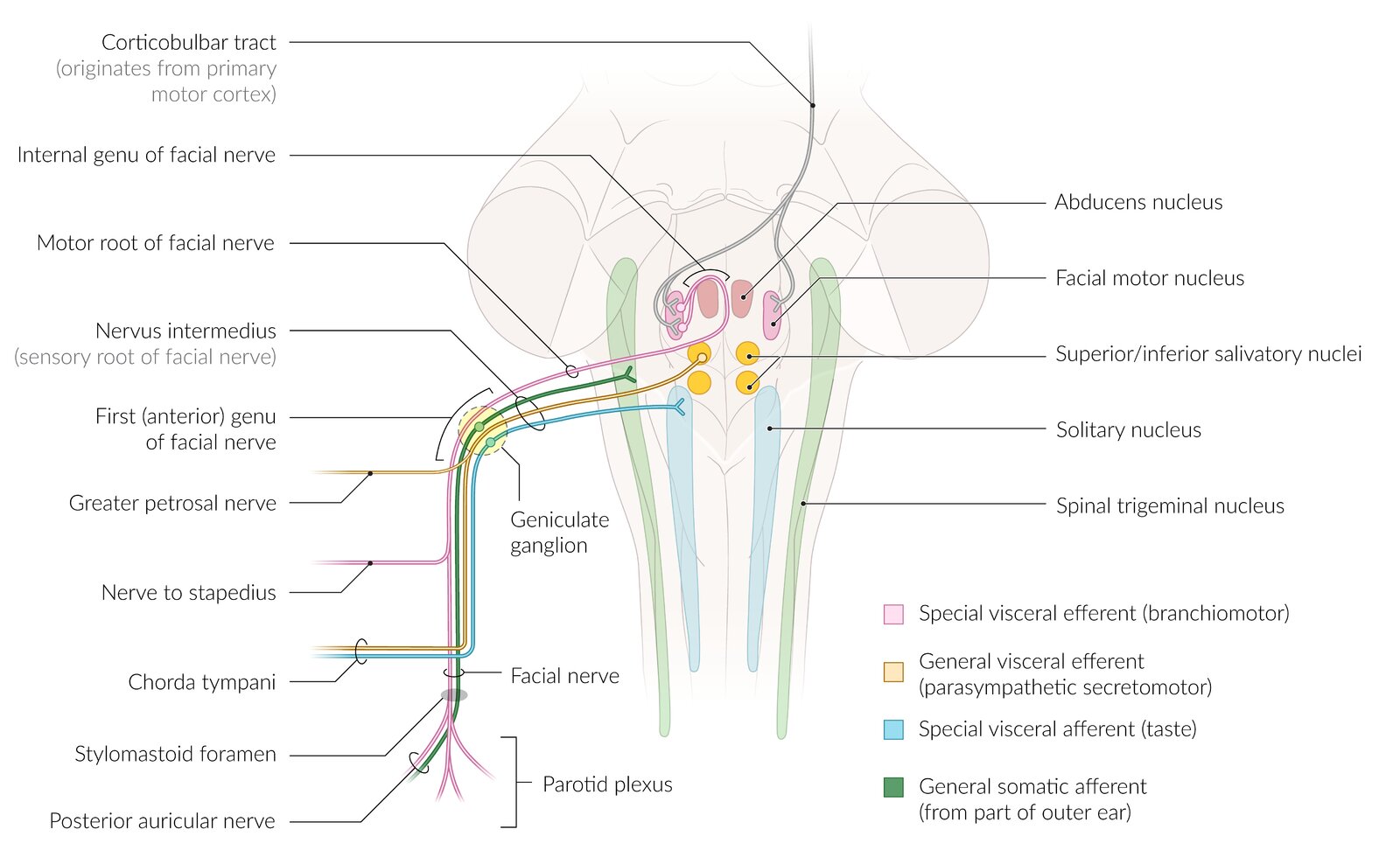
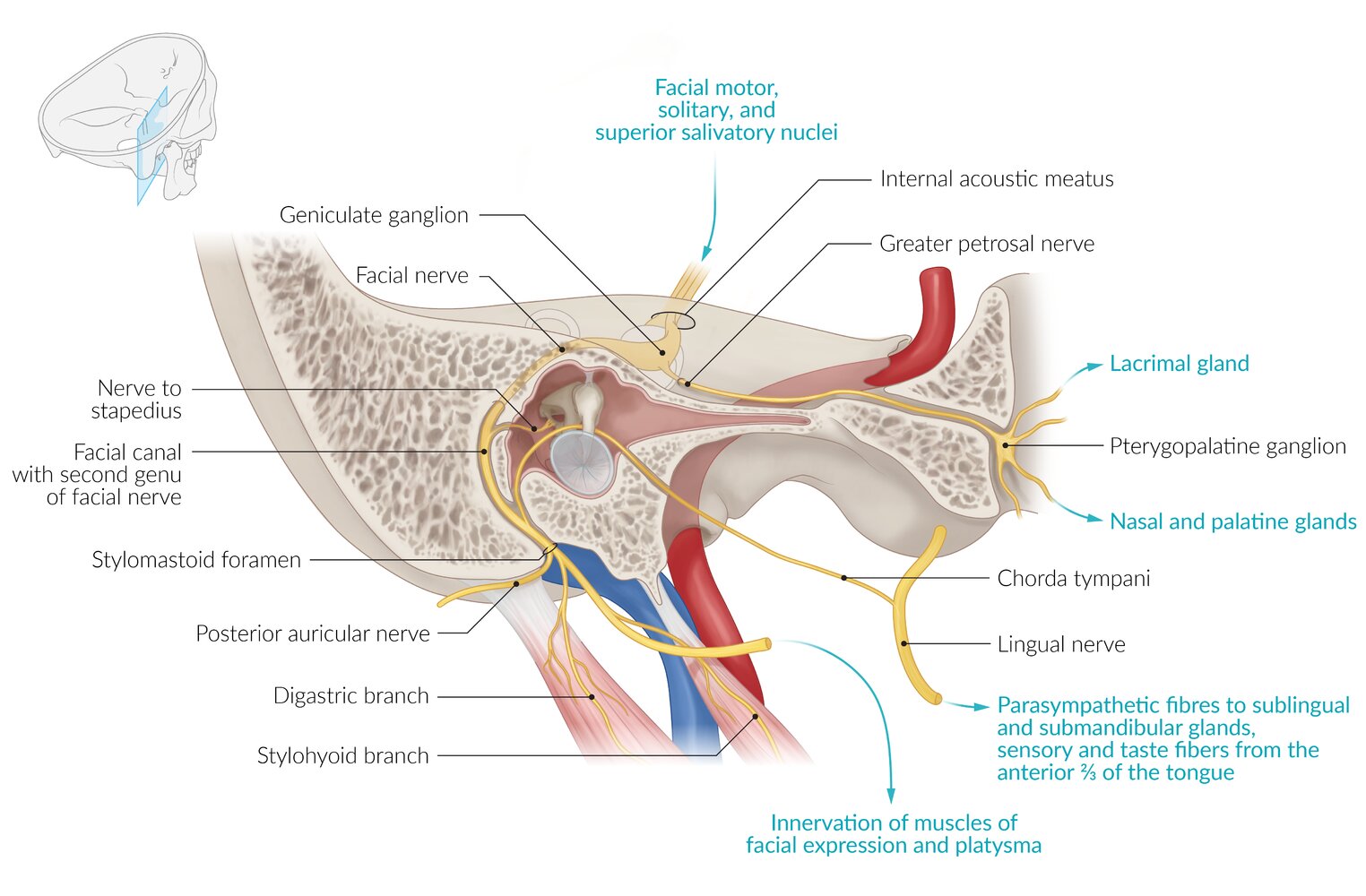
This illustration shows the central connections of the facial motor nucleus. The (motoric) facial nerve is accompanied by the Nervus intermedius which originates from the superior/inferior salivatory nuclei, the solitary nucleus, and the spinal trigeminal nucleus. The nerve fibers build the first (anterior) genu of the facial nerve, are then split up, and eventually build the greater petrosal nerve, the nerve to the stapedius, the chorda tympani, and the facial nerve (including the posterior auricular nerve).
© AMBOSS
Click the menu icon on the top left to explore all the features.
- The home icon enables you to explore the 3-D model yourself.
- The list icon opens a panel with all the labeled structures; click on any of the eye icons to make the structures visible, transparent, or invisible (e.g., visualize deeper structures by making the more superficial structures invisible).
- Use the label icon to toggle the labels on and off.
- Use the scissor icon to change the cross-sectional plane of the 3-D model.
- Click play to start the guided tour.
Additional tools
- Use the arrows at the bottom of the screen to explore different aspects and views.
- Use your mouse/keypad to change the orientation of the 3-D model.
- Hover over the structures to make the label appear.
Did you find this 3-D model useful? We look forward to your feedback!
Clinical approach to cranial nerve palsy
- Confirm the diagnosis clinically with a cranial nerve examination.
- Consider further evaluation for underlying cause based on clinical suspicion.
- General principles of imaging [16][17][18]
-
MRI (without and with IV contrast)
- Usually the preferred first-line imaging modality for direct imaging of the nerve(s)
- Can also identify soft tissue etiologies (e.g., cavernous sinus thrombosis in CN III–VI palsy)
- CT with IV contrast
- Preferred for the evaluation of bony lesions or skeletal trauma (e.g., orbital fractures, skull base fractures)
- Preferred first line imaging modality to evaluate sinonasal pathology (e.g., in CN I palsy)
- MR angiography: Consider for patients with suspected vascular pathology (e.g., aneurysm for CN III palsy).
-
MRI (without and with IV contrast)
- Laboratory studies (e.g., CBC, inflammatory markers, and antigen-specific ANAs) as needed to evaluate for neoplastic, infectious, inflammatory, or autoimmune etiologies
-
Electromyography (EMG): can be used to assess the severity of nerve injury
- Fibrillation potentials: indicate nerve degeneration
- Polyphasic potentials: indicate nerve regeneration
- Absence of motor action potentials (on EMG in combination with electroeurography): surgical intervention likely needed
- General principles of imaging [16][17][18]
- Consult neurology and other relevant specialties.
- Management includes addressing the underlying cause and supportive care; spontaneous recovery may occur.
Olfactory nerve palsy (I)
Etiology
- Acquired
- Most commonly due to trauma to the lateral and occipital regions (e.g., ethmoid bone fracture)
- Intracranial space-occupying lesion (e.g., meningioma)
- Infection (e.g., meningitis)
-
Congenital
- Primary: congenital anosmia
- Secondary in diseases such as Kallmann syndrome and primary ciliary dyskinesia
Clinical features [16][19]
-
Anosmia (hyposmia or dysosmia may be present instead)
- Sudden anosmia typically occurs secondary to trauma.
- Progressively worsening anosmia is suggestive of an obstructive lesion or a neurodegenerative disease.
- Altered perception of taste
Diagnostics [16][17][20][21]
Cranial nerve examination
Diagnosis is clinical and based on:
- Comprehensive history
- Cranial nerve examination: inability to identify certain smells (e.g., peppermint, coffee) [20]
- Assess for common differential diagnoses of olfactory dysfunction, such as sinonasal pathology. [21]
- Perform a head and neck exam.
- Consult otolaryngology for nasal endoscopy.
Further evaluation [20]
Evaluate for the underlying cause.
-
Imaging [16][17][18]
- CT maxillofacial region (with IV contrast): preferred for trauma or suspected sinonasal pathology not confirmed on nasal endoscopy
- MRI head (without and with IV contrast): preferred for a suspected primary neurological cause [18]
- Laboratory studies (e.g., CBC, eosinophil count, thyroid function tests): to evaluate for other etiologies as guided by clinical probability
Treatment
- Consult neurology.
- Address any treatable causes identified.
- Consider a trial of olfactory training. [20][22][23]
- A self-administered therapy in which the patient exposes themselves to 4 different odors for ∼10 seconds twice daily for about 12–24 weeks.
- Associated with improved olfactory sensitivity, especially in olfactory dysfunction secondary to trauma and infections
- Spontaneous recovery (typically over months to years) can occur in up to half the patients with anosmia. [20][21]
Counsel patients on coping strategies such as monitoring for signs of spoiled food and installing smoke and gas detectors. [24]

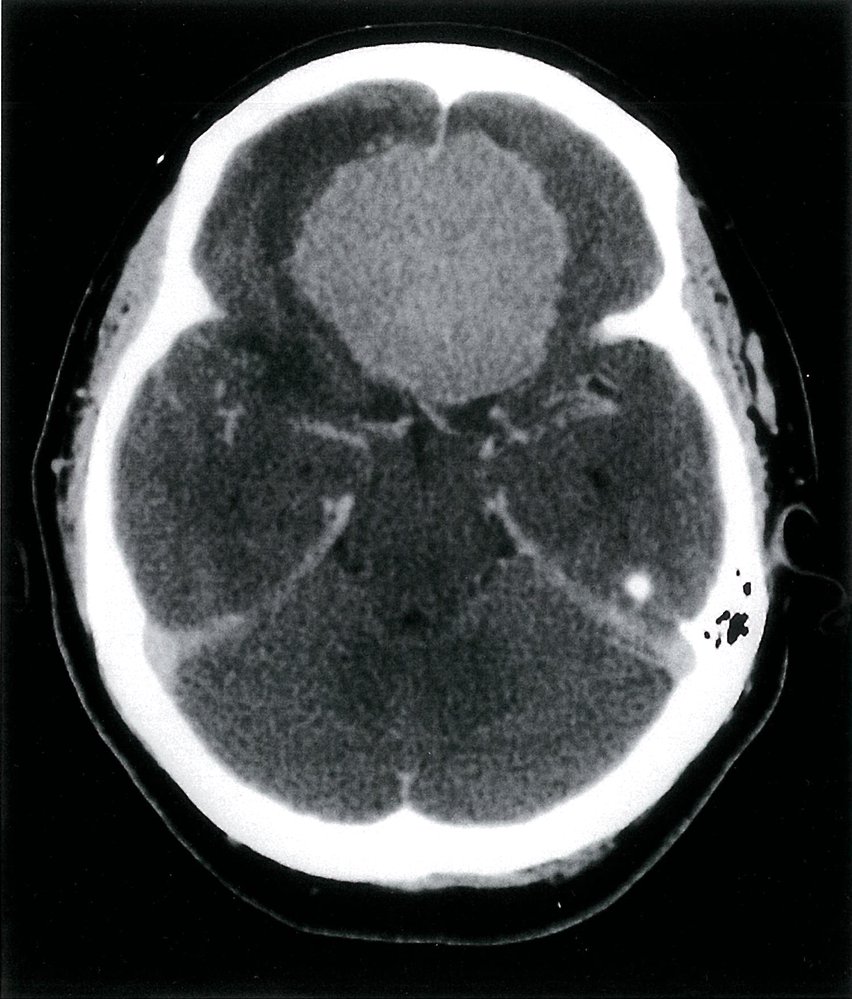
CT head (with contrast; axial plane)
A rounded circumscribed extraaxial mass (blue overlay) located in the midline low anterior cranial fossa shows homogenous contrast enhancement.
Source: © IMPP
Optic nerve palsy (II)
Etiology
- Acquired
- Ischemic optic neuropathy (i.e., caused by microvascular disease, giant cell arteritis)
- Inflammation (optic neuritis): multiple sclerosis, sarcoidosis, viral infections (e.g., measles, mumps)
- Trauma
- Tumors: e.g., optic nerve glioma, pituitary adenoma
- Elevated intracranial pressure: e.g., hydrocephalus
- Malnutrition: vitamin B12 deficiency
- Drugs: sildenafil, amiodarone, ethambutol
- Toxins: e.g., ethyl alcohol, mercury, lead
- Congenital
- Primary: optic nerve hypoplasia
- Secondary: infantile nystagmus, sensory strabismus
Clinical features [16]
- Impaired vision, including blindness (may start as night blindness), depending on the site of the lesion
- Features of the underlying disease, such as: [25]
- Uhthoff phenomenon in multiple sclerosis
- Jaw claudication and headache in giant cell arteritis
Diagnostics [16][25]
Cranial nerve examination
Diagnosis is clinical and based on a comprehensive ocular examination as part of the cranial nerve examination, which includes:
- Assessment of pupillary response, visual field exam, and visual acuity tests
- Complete transection: ipsilateral blindness and loss of direct and indirect pupillary reflex [17]
- Pituitary adenoma (compression to the optic chiasm): bitemporal hemianopia [4]
- Unilateral optic nerve dysfunction: relative afferent pupillary defect [25][26]
-
Fundoscopy: findings depend on the underlying cause and include
- Papillitis
- Papilledema in ↑ ICP
- Optic atrophy in compression (e.g., tumor)
Further evaluation[27]
Consider further evaluation for underlying cause based on clinical findings.
-
Imaging [17]
- CT head (without IV contrast): initial evaluation of trauma or orbital complications of sinusitis
- MRI head and orbits (with IV contrast): initial evaluation of suspected tumor, optic neuritis, or neurodegenerative diseases
-
Laboratory studies to evaluate for the underlying cause (as guided by clinical probability); examples include: [28][29]
- ESR and CRP
- ANA and antigen-specific ANAs
- Toxic exposure tests





Treatment [16][25]
- Address any underlying etiologies identified.
- Consult neurosurgery and/or ophthalmology.
- Traumatic CN II palsy: Options include surgery, high-dose corticosteroids, and observation.
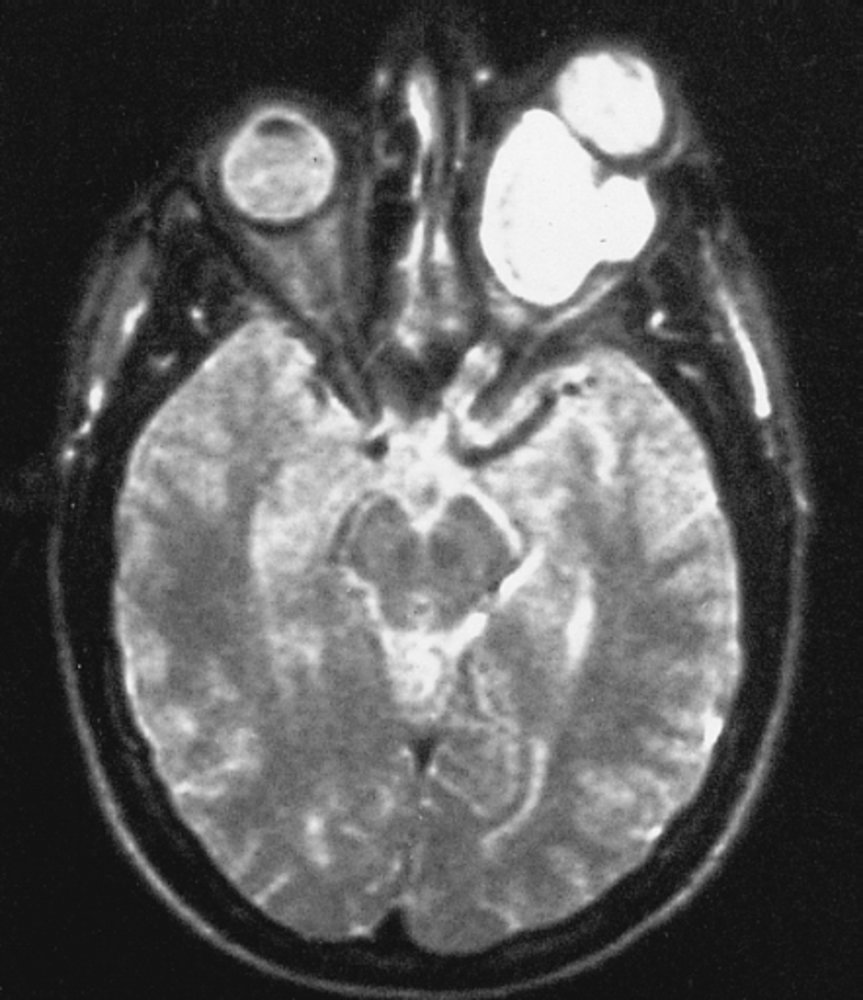
MRI head (T2-weighted; axial plane)
There is a large hyperintense mass (green overlay) in the left intraconal space displacing the ocular globe out of the orbital cavity (exophthalmos). The intraconal space is located posterior to the globe and contained within the cone formed by the recti muscles. The mass is well-defined and displaces rather than invades surrounding structures. The left optic nerve is not visualized on this image, and the mass either arises from it or displaces it. The normal-appearing right optic nerve (red overlay) is well visualized.
The differential diagnosis for intraconal masses depends on whether or not the lesion is continuous with the optic nerve. Differential diagnoses for masses involving the optic nerve include, but are not limited to, meningioma, glioma, and lymphoma. Differential diagnoses for masses not involving the nerve include, but are not limited to, hemangioma, schwannoma, and rhabdomyosarcoma.
Source: "Optic glioma", The Armed Forces Institute of Pathology, Wikimedia Commons, The Armed Forces Institute of Pathology licensed under Public Domain
{kind=link}
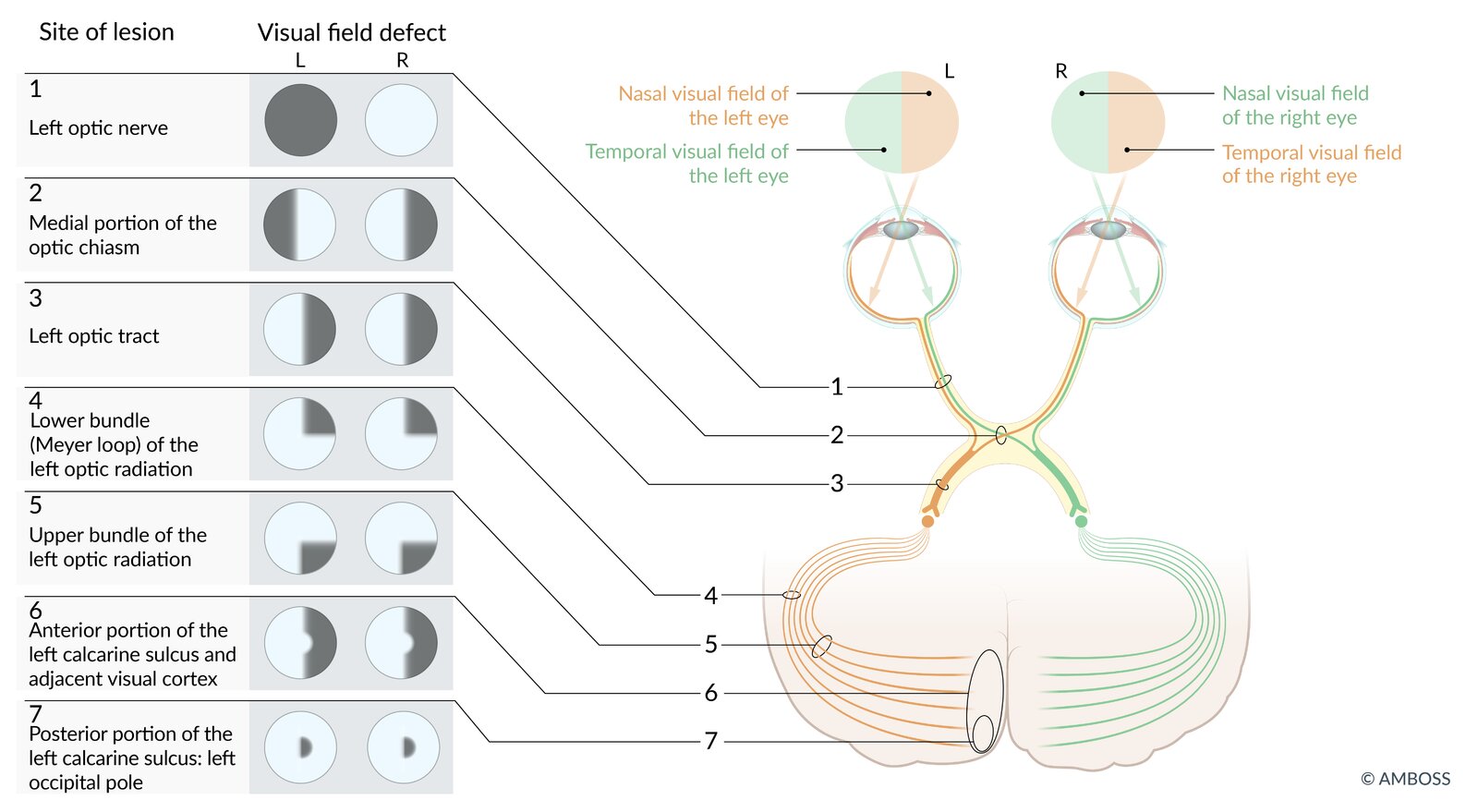
(1) Ipsilateral anopsia
(2) Bitemporal heteronymous hemianopsia
(3) Contralateral homonymous hemianopsia
(4) Contralateral upper homonymous quadrantanopsia
(5) Contralateral lower homonymous quadrantanopsia
(6) Contralateral homonymous hemianopsia with macular sparing
(7) Contralateral homonymous central scotoma
© AMBOSS
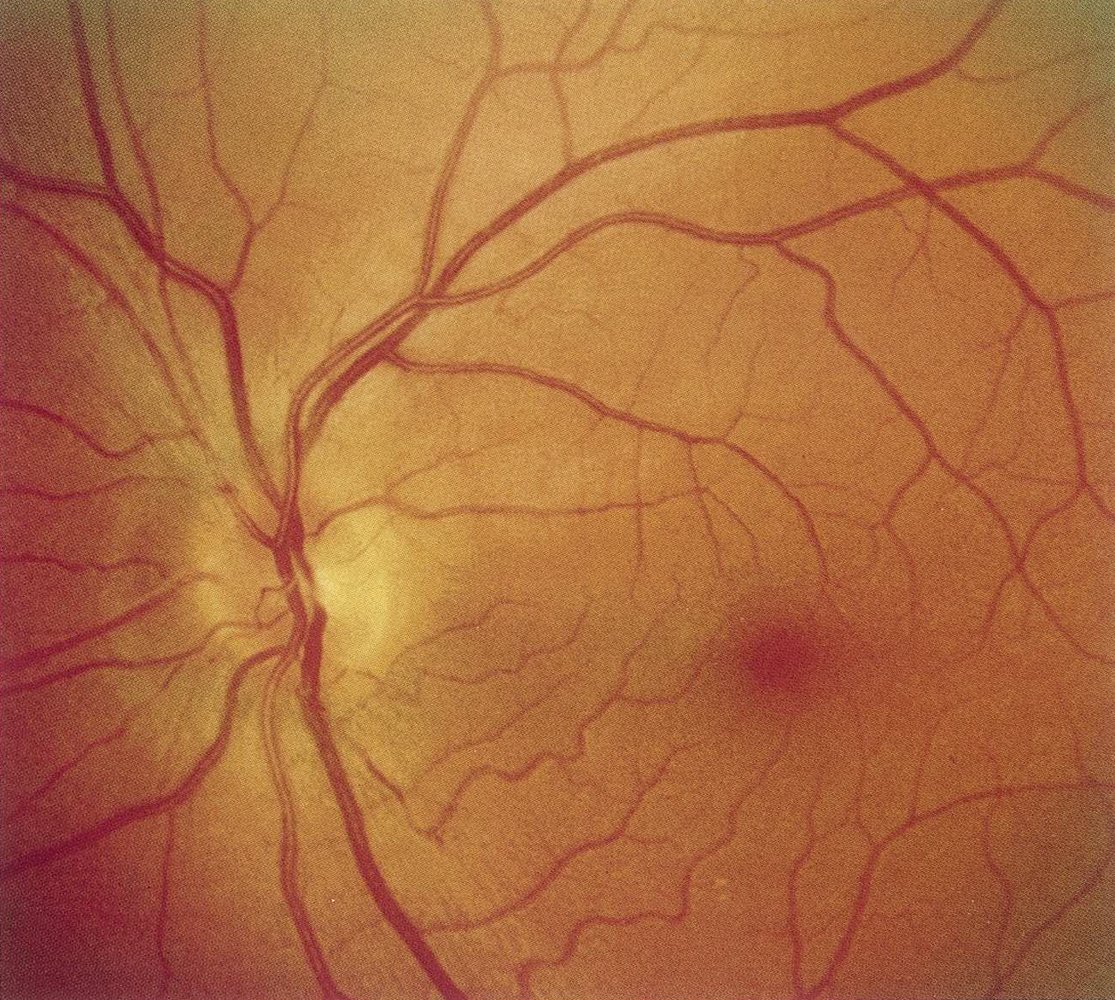
Fundus photography of the left eye of a patient with acute vision loss and painful eye movements
Discrete optic disc edema is visible: Discrete blurring of the nasal superior, superior, and temporal superior disc margin can be seen (green overlay). Otherwise, the fundus is normal.
This finding, in addition to the patient's symptoms, suggests papillitis in optic neuritis.
M: macula; circle: optic disc
Source: © IMPP
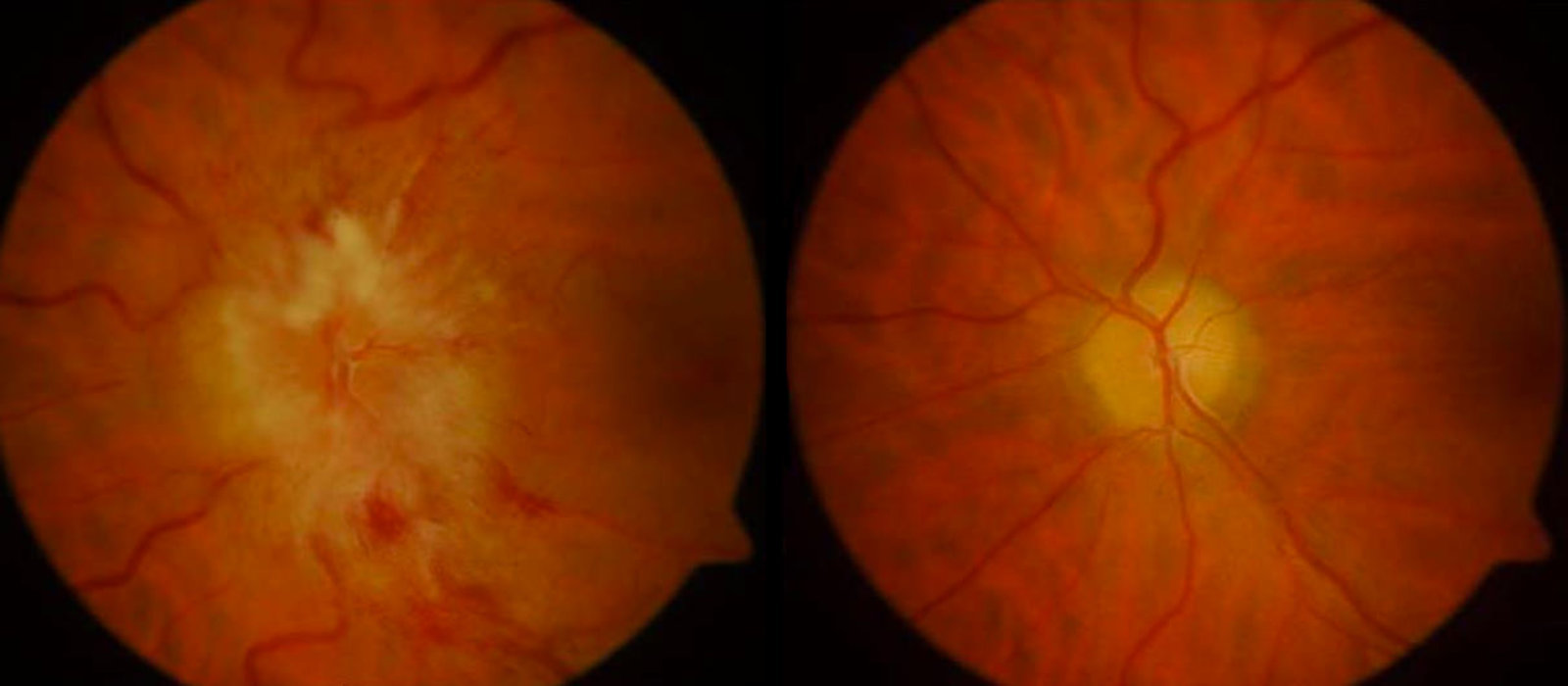
Fundus photography of the left eye
Left image: Blurred disc margins (green overlay) with venous dilatation and tortuosity (blue overlay) and small hemorrhages (examples indicated by arrowheads) are visible.
Blurred disc margins suggest optic disc edema. In intracranial hypertension, as seen in this image, optic disc edema is called papilledema.
Right image: Resolution of optic disc edema after treatment. Sharp disc margins and normal retinal vessels are visible. There are no hemorrhages.
© AMBOSS. This image was adapted from the image “Figure 1, in: A 43-year-old woman on triptorelin presenting with pseudotumor cerebri: a case report” by Uday Kumar Bhatt, Imran Haq, Venkata S. Avadhanam, Kim Bibby, Journal of Medical Case Reports, licensed under CC BY 2.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above (© AMBOSS).
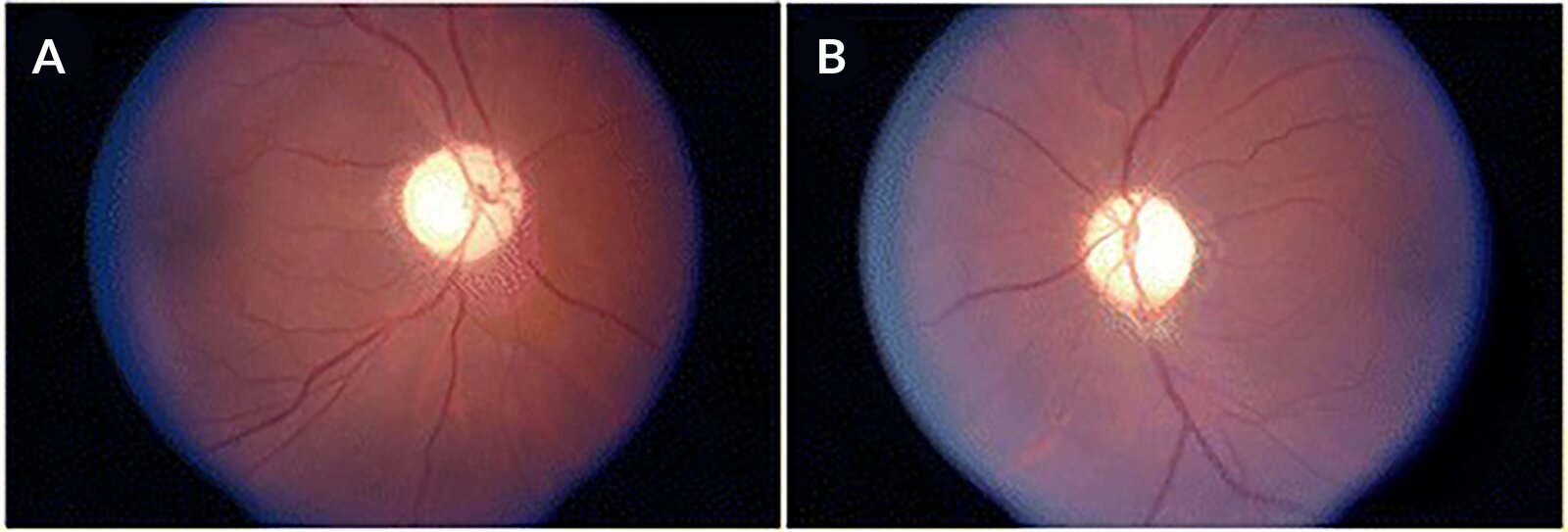
Fundus photographs (a: left eye; b: right eye)
Optic nerve pallor, a characteristic manifestation of optic atrophy, is visible.
Source: “Figure 1, in: Case report of optic atrophy in Dentatorubropallidoluysian Atrophy (DRPLA)” by M. R. Silver, K. D. Sethi, S. H. Mehta et al., BMC - Neurology, licensed under CC BY 4.0. Modifications: Image order changed, letters replaced.
Oculomotor nerve palsy (III)
Etiology
| Etiology of CN III palsy | ||
|---|---|---|
| Structure | Cause | Clinical features |
| Oculomotor nuclei |
|
|
| Basilar segment |
|
|
|
|
|
| Intracavernous segment |
|
|
| Intraorbital segment |
|
|
| Isolated oculomotor nerve palsy |
|
|
Parasympathetic fibers of CN III are located superficially and motor fibers are located centrally. Parasympathetic fibers are more susceptible to compressive lesions (e.g., uncal herniation, aneurysm of the posterior communicating artery). Motor fibers are more susceptible to ischemia (e.g., vasculitis, diabetes, atherosclerosis).
Clinical features [31]
- Horizontal diplopia that worsens when the head is turned away from the side of the lesion
- Ptosis
- Light sensitivity
- Additional features may be present, depending on the cause and the level of the oculomotor nerve lesion.
Diagnostics [16][31]
Cranial nerve examination
Diagnosis is clinical and based on a comprehensive ocular examination as part of the cranial nerve examination.
-
Assessment of extraocular muscle function : Lesions of the motor portion typically produce paralytic squint.
- Down-and-out gaze: affected eye looks outwards (exotropia) and downwards (hypotropia)
- Adduction weakness
-
Assessment of pupillary response (afferent: CN II; efferent: CN III)
- Lesions of the autonomic (parasympathetic) portion result in loss of the pupillary reflex.
- See also “Physiology and abnormalities of the pupil” for details on oculomotor nerve lesions and drugs that affect pupillary size.
Oculomotor nerve palsy leaves you down and out.
Impaired pupillary reaction with relative sparing of motor function is typically seen in compressive lesions. Prominent motor dysfunction with sparing of the pupil is typically seen in ischemic lesions. However, pupillary findings cannot reliably distinguish between the etiologies of oculomotor palsy. [28][32][33]





Further evaluation
Evaluate for underlying cause based on clinical findings.
| Workup for suspected CN III palsy [17][27] | ||
|---|---|---|
| Clinical findings | Likely underlying cause | Further evaluation |
| Complete palsy with dilated pupil OR Incomplete palsy regardless of pupillary findings |
|
|
| Complete palsy with a normal pupillary reflex (pupillary sparing) |
|
|
MRI orbits (without and with IV contrast) should be obtained in patients with ophthalmoplegia and a history of trauma, or those with evidence of orbital injury or inflammation (i.e., enopthalmos, proptosis, chemosis). [27]
MRI head should also be obtained in patients ≤ 50 years old with a history of cancer and additional neurologic findings, including nonisolated cranial nerve palsy. [34]
Treatment [16][31]
-
Compressive lesions
- Immediate neurosurgery referral for management
- Posterior communicating artery aneurysm requires urgent neurosurgical clipping or endovascular coiling [36][37]
- Consider strabismus surgery if symptoms do not improve after treatment of the underlying cause.
-
Ischemic microangiopathy or demyelinating lesions
- Medical management with control of the underlying disease
- Ischemic CN III palsy typically resolves spontaneously within 6–8 weeks. [17][31]
- Prism glasses or an eye patch can be used to improve diplopia while awaiting resolution.
Motor fibers are in the Middle of CN III, while Parasympathetic fibers are on the Periphery of the nerve.

Patient with new-onset right-sided ptosis, diplopia, and a history of migraine
The left image shows ptosis of the right eyelid. Upon manual opening of the right eyelid, a dilated pupil and exotropia due to impaired medial gaze can be seen (right image).
Combination of ptosis, mydriasis, and exotropia (and hypotropia) are the classic signs of complete cranial nerve III palsy.
In patients with headaches and new-onset neurological symptoms, secondary causes should be investigated.
© AMBOSS. This image was adapted from the image “Fig. 1 and 2, in: A Case Report of Posterior Communicating Artery Aneurysm Presenting as Cranial Nerve 3 Palsy in a Young Female Patient with Migra” by Colin Danko; Dustin Williams, JETem, licensed under CC BY 4.0.
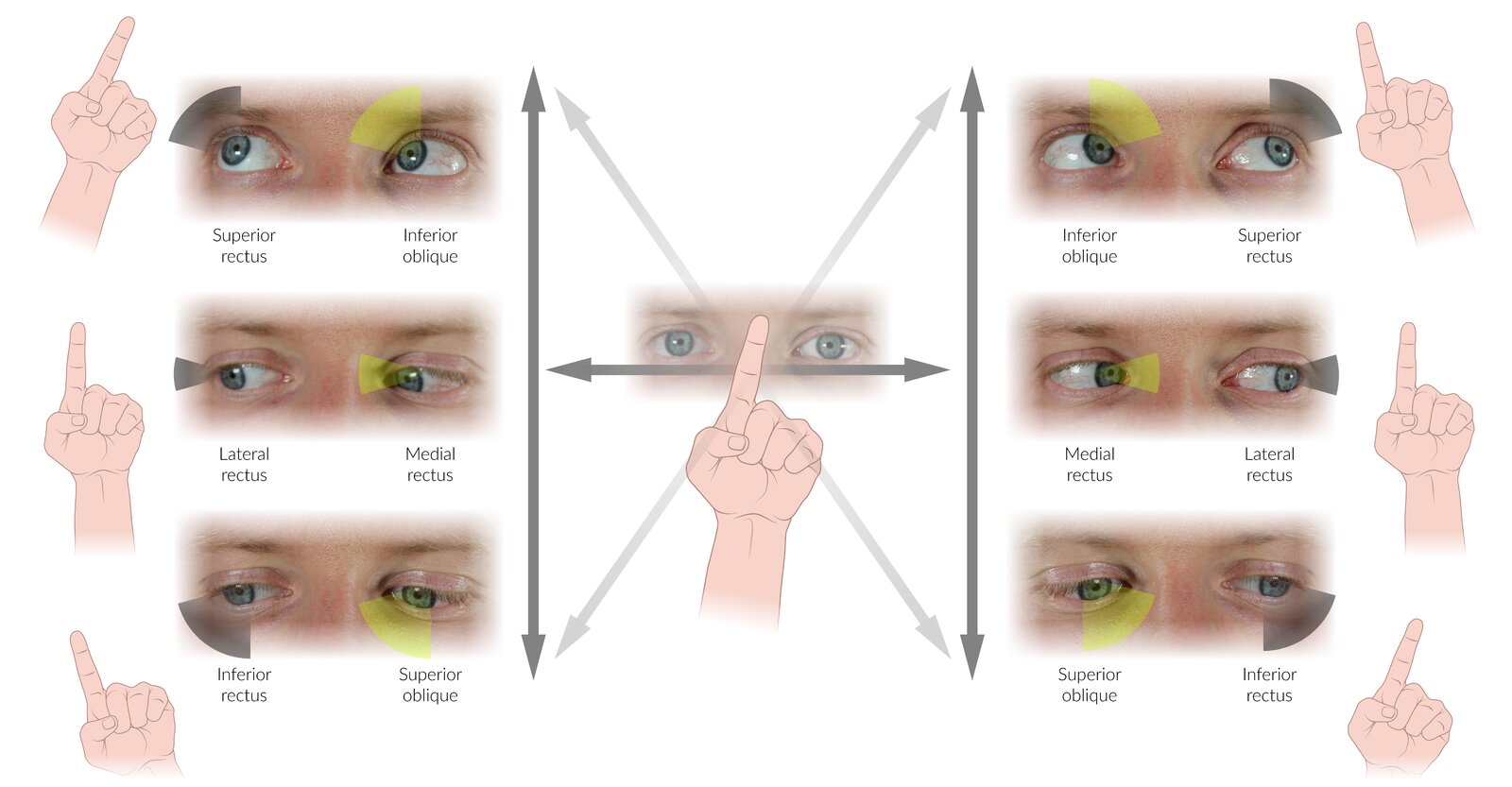
A quick clinical examination of extraocular muscle function can be performed by asking the patient to follow the examiner's finger with the eyes while keeping the head immobile. Tracing the letter “H” in the air (dark grey arrows) will prompt the patient to move through the 6 cardinal positions of gaze. In these positions, a single muscle is the primary mover for each eye.
Some examiners find it beneficial to return to the center between each cardinal position, drawing a star shape (dark grey horizontal arrow plus light grey arrows), while others combine the complete “H” and diagonal movements.
Note that for all muscles except the lateral- and medial recti, the directions in which these muscles are tested clinically (shown here) differ from the direction they would move the eyeball if acting in isolation. The difference arises because eye movements are the result of complex interactions between several extraocular muscles. Therefore, the movement used to test a particular muscle clinically is the movement that most effectively excludes the participation of other muscles. For example, while the superior oblique (SO) depresses and abducts the eye when acting in isolation, depression is also produced by the inferior rectus (IR), and abduction is also produced by the lateral rectus (LR). However, due to their different points of insertion, the IR is the more efficient depressor of the eye in abduction, while the SO is the more efficient depressor in adduction. Looking down and inwards, therefore, allows the isolated clinical examination of the SO (as shown here). Similar principles apply to the movements used for clinical testing of the IR, SR, and IO.
© AMBOSS
Oculomotor nerve palsy (here, of the left eye) causes ipsilateral impairment of both motor and autonomic (parasympathetic) nerve functions. Paralysis of the inferior rectus, medial rectus, superior rectus, and inferior oblique muscles results in downward deviation (hypotropia) and outward deviation (exotropia) of the affected eye (down-and-out gaze) due to the unopposed actions of the lateral rectus and superior oblique muscles. Weakness of the levator palpebrae superioris muscle results in ptosis and impairment of parasympathetic function in mydriasis (as well as loss of accommodation and pupillary light reflex, which are not shown). Patients present with horizontal or horizontal and vertical double vision (diplopia) that worsens when turning the gaze away from the affected side. The ptosis, however, may prevent patients from experiencing diplopia.
© AMBOSS

Eyes and forehead of a 20-year-old female patient with tubercular meningitis
Image A shows bilateral ptosis, due here to paralysis of the levator palpebrae superioris. To open her eyes, the patient must contract the frontalis muscle, resulting in the forehead wrinkles seen in image B. Both eyes deviate outwards (exotropia) and downwards (hypotropia) from the primary gaze position. This occurs due to the unopposed actions of the lateral rectus and superior oblique muscles, which are the only unaffected extraocular muscles. Mydriasis indicates involvement of the parasympathetic portion of the oculomotor nerve.
Ptosis, mydriasis, exotropia, and hypotropia are the classic signs of complete oculomotor palsy. Complete oculomotor palsy is more commonly unilateral than bilateral.
Source: “Fig 1, In: Bilateral Complete Oculomotor Palsy in Tubercular Meningitis” by Gaba S, Gupta M, Lamba AS, Bhardwaj A, Gupta H, Cureus, licensed under CC BY 4.0.
The afferent pathway (blue tract) is initiated when light hits the retina:
- Retinal photoreceptors → ipsilateral optic nerve → nuclei of bilateral pretectal areas (nasal fibers of the optic nerve cross to the contralateral side at the optic chiasma)
The efferent pathway (green tract) transmits neural impulses to the iris sphincter muscle:
- Nuclei of pretectal area → bilateral Edinger Westphal nuclei (parasympathetic preganglionic nucleus of the oculomotor nerve) → bilateral oculomotor nerves (synapse at the ciliary ganglion) → bilateral iris sphincter muscle (and ciliary muscle) → bilateral pupillary constriction (and accomodation).
Shining a light into one eye causes constriction of the ipsilateral pupil (direct pupillary reflex) as well as that of the contralateral pupil (indirect or consensual pupillary reflex).
© AMBOSS
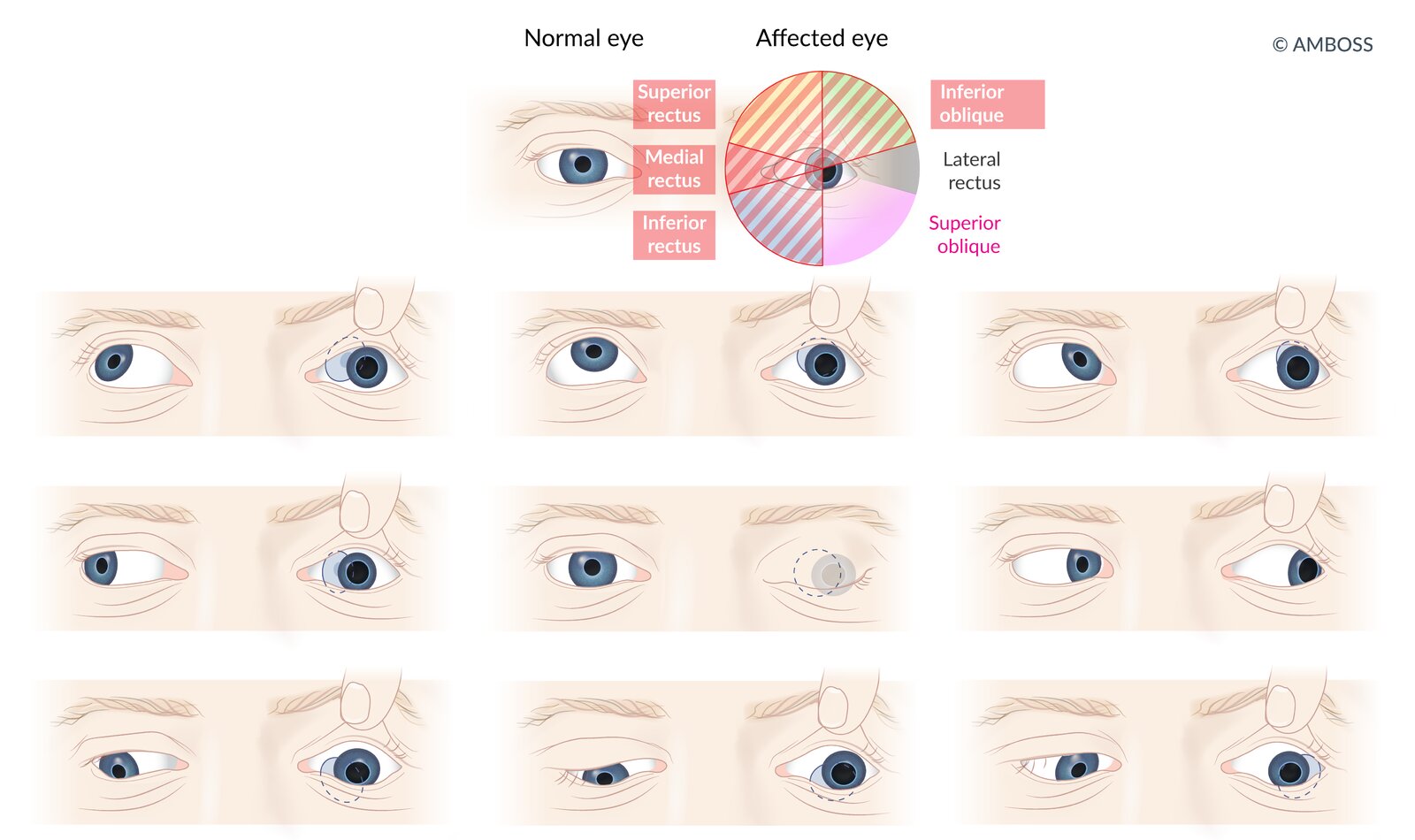
Oculomotor nerve palsy (here of the right eye) causes ipsilateral impairment of both motor and autonomic (parasympathetic) nerve functions. Paralysis of the superior rectus, inferior rectus, medial rectus, and inferior oblique muscles results in downward deviation (hypotropia) and outward deviation (exotropia) of the affected eye (down-and-out gaze) due to the unopposed actions of the lateral rectus and superior oblique muscles. Weakness of the levator palpebrae superioris muscle results in ptosis and impairment of parasympathetic function in mydriasis.
© AMBOSS
Trochlear nerve palsy (IV)
Etiology
- Acquired
- Microvascular damage (diabetes, hypertension, arteriosclerosis)
- Cavernous sinus thrombosis
- Trauma
- Congenital: fourth nerve palsy
Clinical features
- Vertical or oblique diplopia
- Exacerbated on downgaze (e.g., reading, walking downstairs) away from side of affected muscle [38]
- Worsens when patient turns the head towards the paralyzed muscle → compensatory head tilt to the opposite side of the lesion
With damage to the CN IV, you cannot look at the floor.

Diagnostics
Cranial nerve examination
Diagnosis is clinical, based on cranial nerve examination, which includes: [38][39]
-
Assessment of extraocular muscle function
- Extorsion of the eye
- Inability to depress and adduct the eyeball simultaneously
- Park-Bielchowsky test: ipsilateral hypertropia that worsens on contralateral gaze and ipsilateral head tilt



Imaging [17][27][34]
- Not routinely required
- Consider MRI head and orbits (without and with IV contrast) in consultation with a neurologist in the following situations
- History of trauma
- Patients ≤ 50 years old with a history of cancer and additional neurologic findings, including nonisolated cranial nerve palsy
- Persistent palsy after 3 months (in all age groups)
- Progression of symptoms
Treatment [16][40]
- Consult neurology and ophthalmology.
- Symptoms often resolve spontaneously within six months of onset.
- Prism glasses or an eye patch can be used to improve diplopia while awaiting resolution.
- Surgical realignment may be needed for persistent CN IV palsy.

While the right eye fixates straight, the left eye deviates upwards (hypertropia). This may be due to congenital superior oblique palsy or trochlear nerve palsy.
Source: “Figure 3. in: Understanding, detecting, and managing strabismus.” by Eugene M Helveston, Community eye health journal, licensed under CC BY 2.0.
A quick clinical examination of extraocular muscle function can be performed by asking the patient to follow the examiner's finger with the eyes while keeping the head immobile. Tracing the letter “H” in the air (dark grey arrows) will prompt the patient to move through the 6 cardinal positions of gaze. In these positions, a single muscle is the primary mover for each eye.
Some examiners find it beneficial to return to the center between each cardinal position, drawing a star shape (dark grey horizontal arrow plus light grey arrows), while others combine the complete “H” and diagonal movements.
Note that for all muscles except the lateral- and medial recti, the directions in which these muscles are tested clinically (shown here) differ from the direction they would move the eyeball if acting in isolation. The difference arises because eye movements are the result of complex interactions between several extraocular muscles. Therefore, the movement used to test a particular muscle clinically is the movement that most effectively excludes the participation of other muscles. For example, while the superior oblique (SO) depresses and abducts the eye when acting in isolation, depression is also produced by the inferior rectus (IR), and abduction is also produced by the lateral rectus (LR). However, due to their different points of insertion, the IR is the more efficient depressor of the eye in abduction, while the SO is the more efficient depressor in adduction. Looking down and inwards, therefore, allows the isolated clinical examination of the SO (as shown here). Similar principles apply to the movements used for clinical testing of the IR, SR, and IO.
© AMBOSS
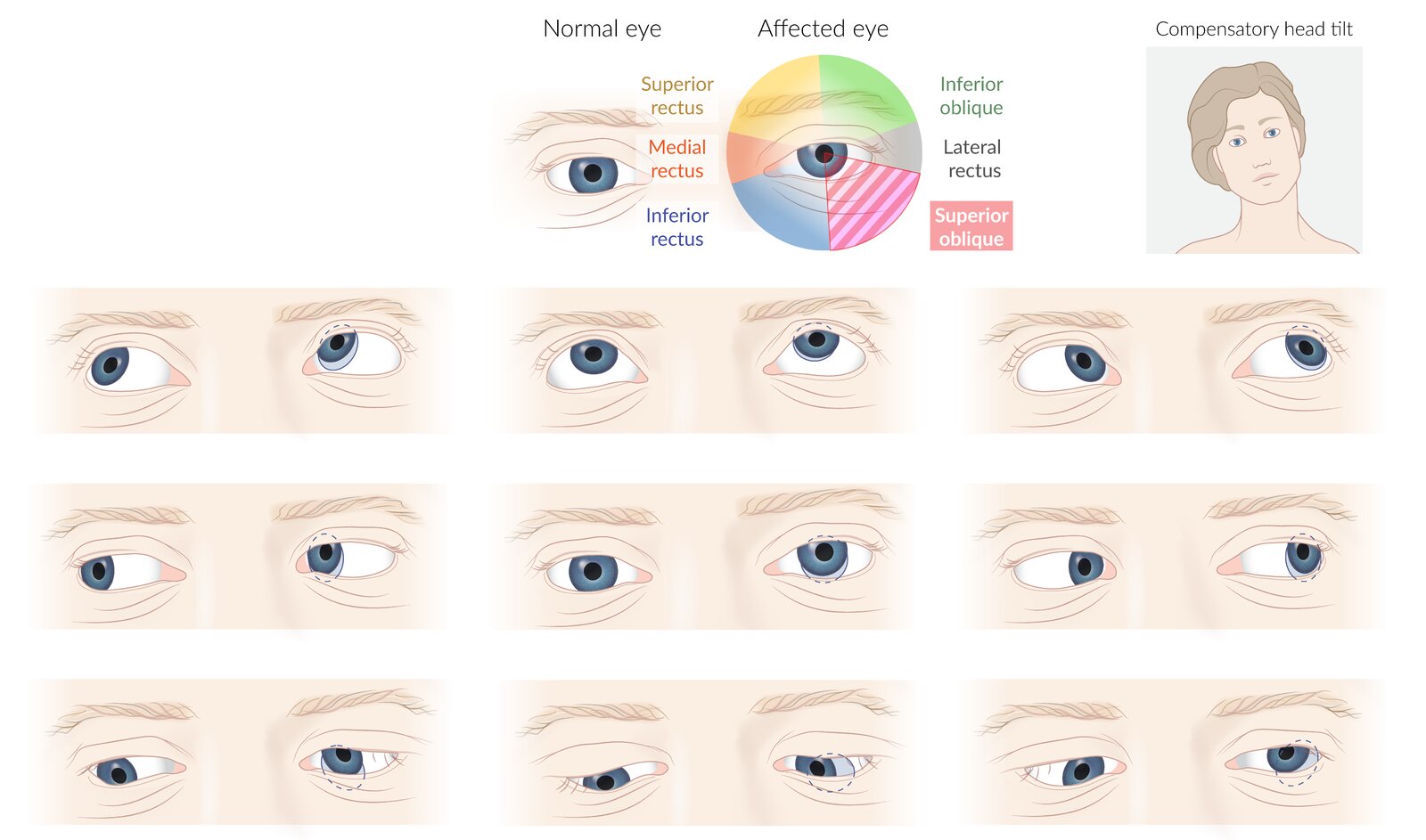
Trochlear nerve palsy (here of the left eye) causes paralysis of the ipsilateral superior oblique muscle. This leads to hypertropia (upwards deviation) that increases in adduction, excyclotorsion (outward rotation) of the affected eye and slight limitation of abduction. The findings may be discrete.
Patients typically present with vertical or oblique diplopia. Hypertropia and diplopia usually increases with ipsilateral head-tilt and decreases with contralateral head-tilt. Patients may adopt the latter as a compensatory posture (upper right of image).
© AMBOSS
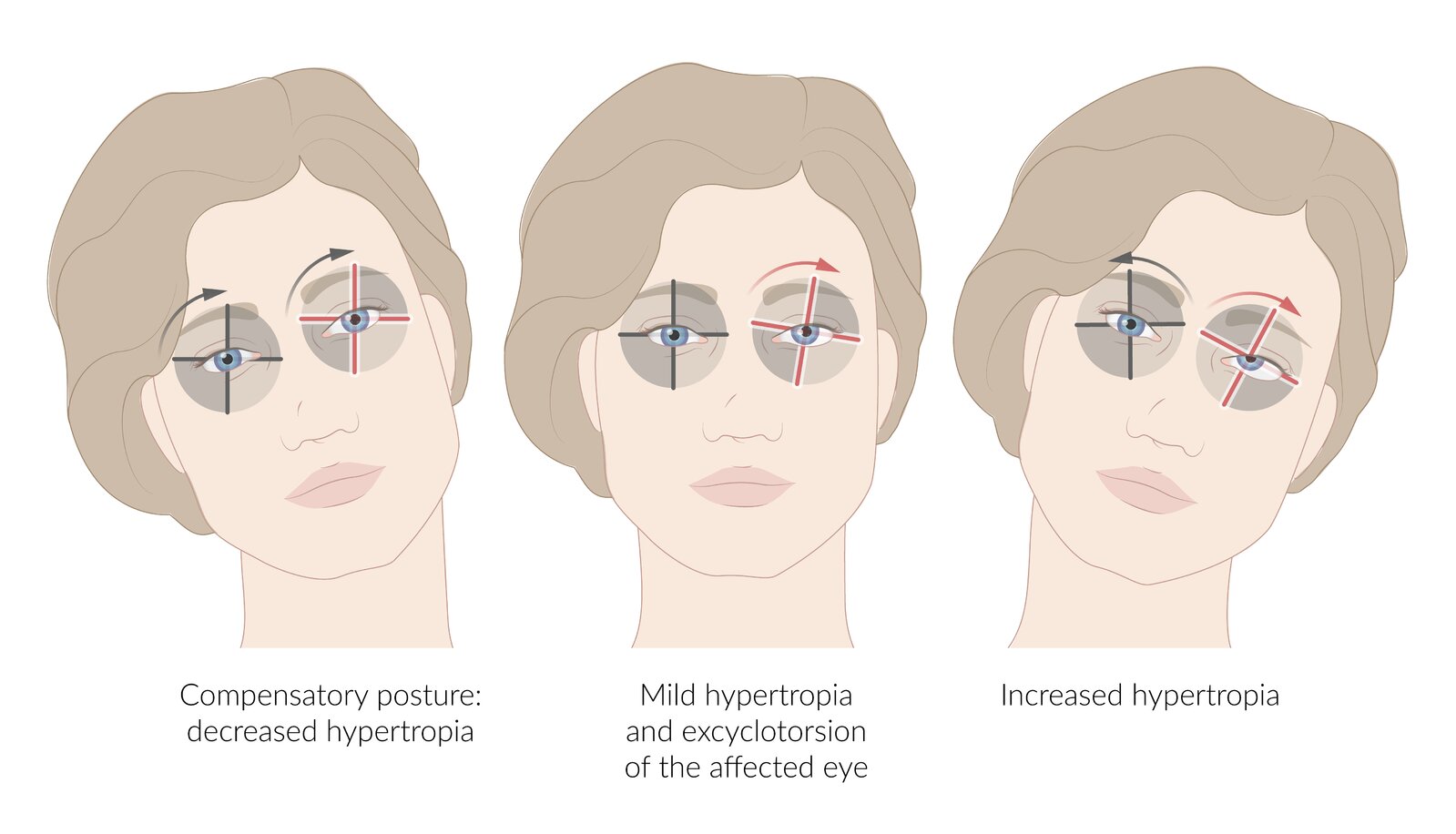
Trochlear nerve palsy (here of the left eye) causes paralysis of the ipsilateral superior oblique muscle. This leads to hypertropia (upwards deviation) and excyclotorsion (outward rotation) of the affected eye (middle image). Patients typically present with vertical or oblique diplopia. Hypertropia and diplopia may increase with ipsilateral head-tilt (right image) and decrease with contralateral head-tilt (left image; patients may adopt this posture as a compensatory posture).
© AMBOSS
Trochlear nerve palsy (here of the right eye) causes paralysis of the ipsilateral superior oblique muscle. This leads to hypertropia (upwards deviation) that increases in adduction and with ipsilateral head-tilt, slight limitation of abduction, and excyclotorsion (outward rotation). Patients typically present with diplopia, which may increase with ipsilateral head-tilt and improve with contralateral head-tilt (patients may present in this position, having adopted it to compensate the deficit).
© AMBOSS
Trigeminal nerve palsy (V)
Etiology
- Tumor
- Vascular compression
- Trauma, including maxillofacial or oral surgery, and mandibular molar extractions
- Inflammation of the nerve
- Cavernous sinus thrombosis
Clinical features
Clinical features depend on the site of the lesion and can include (see “Localizing features of CN V palsy” for details):
- Altered sensation over the face and tongue
- Weakness in muscles of mastication
- Hearing impairment
Diagnostics [16][41]
Cranial nerve examination
Diagnosis is clinical, based on ear examination, nose and throat examination, and cranial nerve examination.
- Assess for decreased facial sensation to light touch, pain (can also be increased), and/or temperature (CN V1, V2).
- Assess for diminished/absent corneal reflex or lacrimation reflex (CN V1).
-
Assess muscles of mastication (CN V3) for:
- Signs of atrophy
- Decreased strength (e.g., open mouth against resistance)
- Jaw jerk reflex
| Localizing features of CN V palsy | ||
|---|---|---|
| Peripheral trigeminal nerve lesions | Ophthalmic nerve (CN V1) |
|
| Maxillary nerve (CN V2) |
|
|
| Mandibular nerve (CN V3) |
|
|
| Lesion of the tensor tympani branch |
|
|
| Lesions of the trigeminal nerve nuclei (depending on the nuclei affected) |
|
|
The primary features of trigeminal neuropathy are numbness and/or weakness in the areas of trigeminal nerve innervation, whereas the primary feature of trigeminal neuralgia is intermittent sharp pain in the same area without sensory or motor deficits. [41]


Further evaluation
Consider further evaluation for underlying cause based on clinical findings.
-
Imaging [16][17][41]
- Not routinely required if the underlying cause is clear (e.g., peripheral paresthesia following mandibular molar extraction)
- History of head trauma: Consider CT head and skull base.
- Suspected intracranial hemorrhage, tumor, cavernous sinus thrombosis : MRI head (without and with IV contrast)
- Laboratory studies (as needed): e.g., CBC, ESR, RPR, ANA and antigen-specific ANAs
Treatment [16][41]
- Consult neurology and maxillofacial surgery.
- Traumatic CN V palsy (e.g., following dental surgery) often resolves spontaneously within six months of symptom onset.
- Consider adjuvant analgesics as needed for pain.
- Treat the underlying cause (e.g., see “Treatment of cavernous sinus thrombosis”).
- Screen for and treat complications.
- Monitor for tongue and mouth injuries due to decreased sensation.
- Screen for inadequate nutrition due to weak mastication.
- Consider biofeedback training for chronic pain and weakness.
- Screen for corneal edema due to absent corneal reflex; consider protective contact lenses.
- Screen for symptoms of depression.
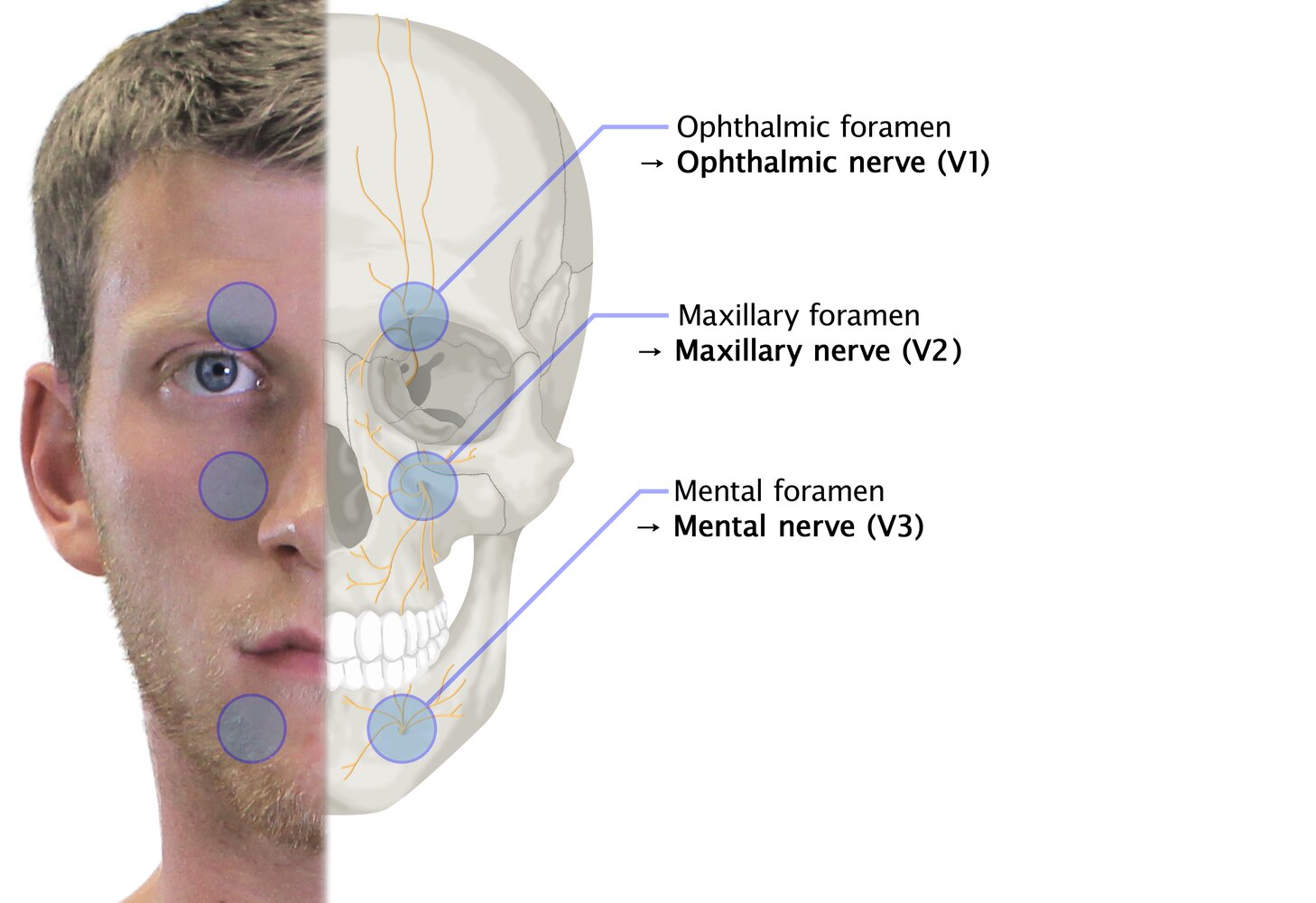
Branches of the trigeminal nerve (CN V) and the foramina through which they exit the skull.
© AMBOSS
© AMBOSS
Abducens nerve palsy (VI)
Etiology [10][42]
- Acquired
- Trauma (e.g., at the superior orbital fissure)
- Pseudotumor cerebri
- Cavernous sinus thrombosis
- Space-occupying lesion causing downward pressure (e.g., tumor)
- Diabetic neuropathy
- Giant cell arteritis (GCA)
- Congenital: Duane syndrome (a rare type of strabismus characterized by an impaired abduction and ptosis on adduction) [43]
Abducens nerve palsy is the most common ocular cranial nerve palsy.
Clinical features
- Horizontal diplopia that worsens when looking at distant objects
- Inability to look laterally in the affected eye
- Features of the underlying cause
Diagnostics [42][44]
Cranial nerve examination
Diagnosis is clinical, based on the examination of the extraocular muscles as part of the cranial nerve examination.
- Esotropia: medial deviation of the affected eye at primary gaze
- Inability to abduct the affected eye



Further evaluation [42]
Evaluate for underlying cause based on clinical findings.
-
MRI head and orbits (with IV contrast) if any of the following are present: [17][34][42][44]
- Patients < 50 years of age
- History of cancer
- No ischemic risk factors
- Additional neurologic findings, including nonisolated cranial nerve palsy
- No evidence of resolution after 3 months
- Evaluation of all other patients (or patients with normal neuroimaging): [42][44]
- Consult neurology and/or ophthalmology.
- Assess for ischemic risk factors : e.g., Check blood pressure, blood glucose, lipid profile, ESR.
- Assess for underlying infection, autoimmune etiologies, or mimics (e.g., thyroid eye disease, myasthenia gravis) as needed.
- CBC, ANA
- Syphilis diagnostics,
- Thyroid function tests, AChR antibody levels
- Consider lumbar puncture.
Treatment
- Consult neurology and ophthalmology.
- Treat the underlying cause.
- Complete resolution of isolated CN VI palsy is seen in 75–88% of patients within 6 months of symptom onset. [42]
- Prism glasses or eye patching may be considered to manage disabling diplopia.
- Consider strabismus surgery for chronic CN VI palsy.[45]
Abducens nerve palsy (here of the left eye) impairs the function of the lateral rectus muscle. This causes esotropia (medial deviation) of the affected eye and limits its abduction. Patients present with horizontal diplopia that worsens when turning the gaze to the affected side or looking at distant objects.
© AMBOSS
Abducens nerve palsy (here of the right eye) impairs the function of the lateral rectus muscle and, thus, abduction of the affected eye. This causes horizontal diplopia that increases when turning the gaze to the affected side or in far vision.
© AMBOSS

Child gazing to the right
The patient is unable to abduct the right eye while the adduction of the left eye is intact.
Source: “Figure 1. in: Cerebral venous thrombosis in a child with nephrotic syndrome: case report” by Shalinee Bhoobun, Alhaji Alusaine Jalloh, Kathryn H Jacobsen, Pan African Medical Journal, licensed under CC BY 4.0.
Facial nerve palsy (VII)
- See “Facial nerve palsy.”
Vestibulocochlear nerve palsy (VIII)
Etiology
- Bacterial meningitis (most common cranial nerve palsy)
- Lyme disease
- Tumor (e.g., acoustic neuroma, neurofibromatosis type 2)
- Trauma: basilar skull fracture (damage to the CN VIII within the internal acoustic meatus → symptoms of vestibular and cochlear nerve damage)
Clinical features
- Hearing loss
- Vertigo
- Motion sickness [46]
- Tinnitus
Diagnostics [47][48]
Cranial nerve examination
Diagnosis is clinical, based on a comprehensive examination of the ears, hearing, and vestibular system, as part of the cranial nerve examination.
- Evaluation of cochlear nerve function (Rinne test, Weber test, audiometry) : sensorineural hearing loss
- Evaluation of vestibular nerve function (HINTS exam, vestibular function tests): features of peripheral vertigo (see “Peripheral vs. central vertigo”)
- Abnormal head impulse test
- Horizontal nystagmus; gaze fixation suppresses nystagmus
- Skew deviation is absent
If a tuning fork is unavailable, a hum test may be used as an alternative to the Weber test [48]
In patients with sudden hearing loss, audiometry should be performed within 14 days from the onset of symptoms. [48]
Further evaluation
Consider further evaluation for underlying cause based on clinical findings.
- Laboratory studies as needed: e.g., CBC, ANA, or testing for Lyme disease, syphilis, TB, or HIV
- Imaging: MRI head and brainstem with IV contrast (to assess for, e.g., vestibular schwannoma, multiple sclerosis, TIA) [17][48]
Treatment [48]
- Consult neurology and/or otolaryngology.
- Treatment is aimed at resolving underlying causes (e.g., surgical excision and/or radiation for a tumor).
- Consider expectant management with scheduled repeat audiometry to assess for spontaneous recovery.
- For severe sensorineural hearing loss, consider initial treatment with prednisone within two weeks of symptom onset. [48]
Glossopharyngeal nerve palsy (IX)
Etiology
- Idiopathic
- Compression (e.g., aneurysm, tumor, retropharyngeal abscess)
- Trauma (skull base fractures)
Clinical features
Isolated CN IX palsy is rare and may be asymptomatic due to shared sensory and motor nuclei with adjacent nerves. [49]
- Throat and ear pain (glossopharyngeal neuralgia)
- Mild dysphagia
- Altered taste over the posterior aspect of the tongue
- Difficulty swallowing
Lesions that affect the glossopharyngeal nerve typically also affect the vagus nerve because the two nerves exit the jugular foramen in close proximity. [16][49]
Diagnostics [49]
Cranial nerve examination
Diagnosis is clinical, based on the cranial nerve examination.
- Ipsilateral diminished or absent gag response (afferent limb).
- Loss of taste in the posterior third of the tongue.
- Sensory loss over the soft palate, upper pharynx, and posterior third of the tongue (including loss of taste sensation)
The carotid sinus baroreceptors are innervated by the carotid sinus nerve, a branch of the glossopharyngeal nerve. Injury to the glossopharyngeal nerve may result in impairment of the baroreceptor reflex. [50]
Further evaluation
- Consider high-resolution MRI orbit, face, and neck, in conjunction with MRI head (without and with IV contrast) to assess for underlying cause. [17][18][51]
Treatment
- Consults [49]
- Neurology for all patients
- Otolaryngology for patients with laryngeal or pharyngeal symptoms (for laryngoscopy)
- Speech therapy as needed
- Address suspected underlying cause if identified.
- Consider acute pain management with adjuvant analgesics for glossopharyngeal neuralgia. [51]
© AMBOSS
Vagus nerve palsy (X)
Etiology
- Trauma (skull base fractures)
- Diabetes
- Inflammation
- Aortic aneurysms
- Neurodegenerative conditions
- Tumors
- Surgery (e.g, recurrent nerve injury during thyroidectomy)

Clinical features
- Nasal speech
- Dysphagia, aspiration
-
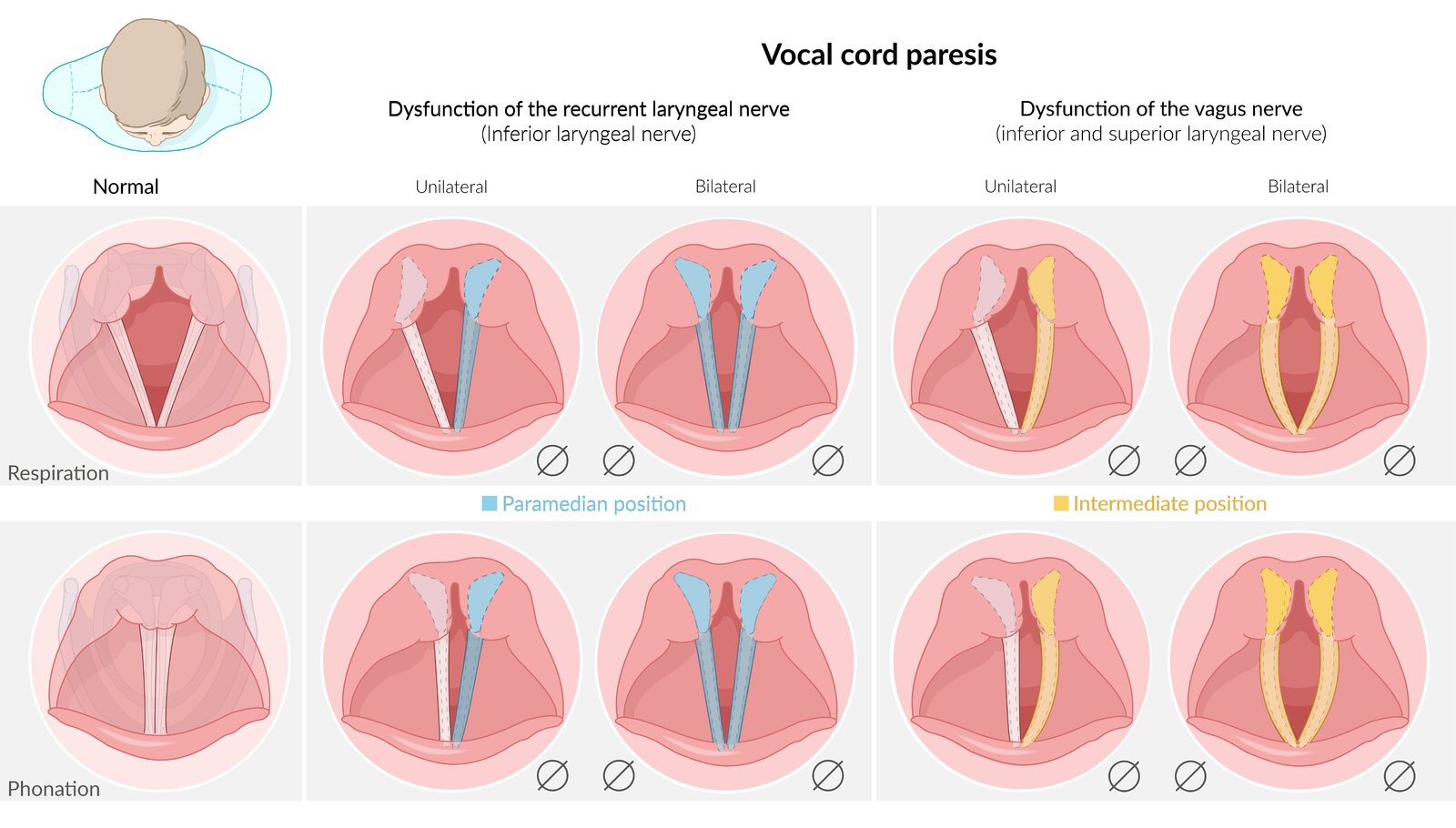
Vocal cord paralysis, manifesting as:
- Dysphonia (hoarseness) in unilateral recurrent laryngeal nerve palsy
- Aphonia and inspiratory stridor in bilateral recurrent laryngeal nerve palsy
- Features of gastroparesis, e.g., postprandial bloating
Unilateral vocal cord paralysis may be asymptomatic due to compensation from the contralateral vocal cord.
Lesions that affect the vagus nerve typically also affect the glossopharyngeal nerve because the two nerves exit the jugular foramen in close proximity. [16][49]
Diagnostics [16][49][52]
Cranial nerve examination
- Perform a focused HEENT examination and cranial nerve examination, assessing for:
- Diminished or absent gag reflex (efferent limb) and/or cough reflex (afferent limb; impulses travel via the internal laryngeal nerve)
- Uvular deviation: Articulating "ahh" will cause the uvula to deviate away from the affected side.
- Flaccid paralysis and ipsilateral lowering of soft palate
- Pharyngeal dysfunction: Ask the patient to swallow some water; choking or difficulty swallowing indicated dysfunction.
- Tachycardia (resting heart rate > 100 beats per minute)
- Observe the patient's breathing and voice, assessing for: [52]
- Stridor: May indicate bilateral vocal cord palsy; perform immediate airway management and consult otolaryngology.
- Dysphonia: Hoarseness is suggestive of unilateral vocal cord palsy; aphonia is suggestive of bilateral vocal cord palsy.
- Dysarthria: Dysphonia with dysarthria and dysphagia may indicate neurological pathology (e.g., amyotrophic lateral sclerosis).
-
Consult otolaryngology for evaluation of larynx and pharynx, including: [49][52]
- Laryngoscopy (direct and indirect): to identify vocal cord palsy (unilateral or bilateral)
- Fiberoptic nasolaryngoscopy: to evaluate the upper respiratory tract for structural abnormalities or foreign bodies
Isolated palsy of the recurrent laryngeal nerve(s) indicates that the site of the lesion is most likely distal to the hyoid bone. More proximal lesions manifest with dysphagia, nasal speech, palatal paralysis, and uvular deviation. [17][49]
Dysphonia in a patient with a neck mass, dyspnea, stridor, progressive neurological symptoms, history of tobacco use, or history of surgery on the head, neck, or chest requires urgent evaluation by an otolaryngology specialist to evaluate for a potentially serious underlying cause. [52]

Further evaluation [16][17][18]
Based on clinical and laryngoscopic findings, consult neurology and consider further evaluation, including:
- MRI head and brainstem (without and with IV contrast): to evaluate for proximal or intracranial etiologies, such as stroke or neoplasms
- CT neck and proximal chest (with IV contrast): to evaluate for distal causes, such as thyroid, neck mass, or thoracic aortic aneurysm
Treatment [49][52]
Treatment varies depending on the cause and severity of symptoms; options include the following:
- Expectant management: Patients with dysphonia of unclear cause may be observed for up to 4 weeks if no indications for expedited laryngoscopy are present.
- Voice therapy: may be performed alone or in conjunction with surgery [53]
-
Surgery [54]
- Unilateral vocal cord palsy: interventions to reduce the glottic opening (e.g., injection laryngoplasty) or thyroplasty
- Bilateral vocal cord palsy: tracheostomy or interventions to enlarge the glottic opening (e.g., lateral fixation of the vocal fold, arytenoidectomy, and/or cordotomy)
Bilateral vocal cord palsy with stridor and dyspnea is a potentially airway-threatening condition. Consult otolaryngology urgently to secure the airway (e.g., via tracheostomy). [54]
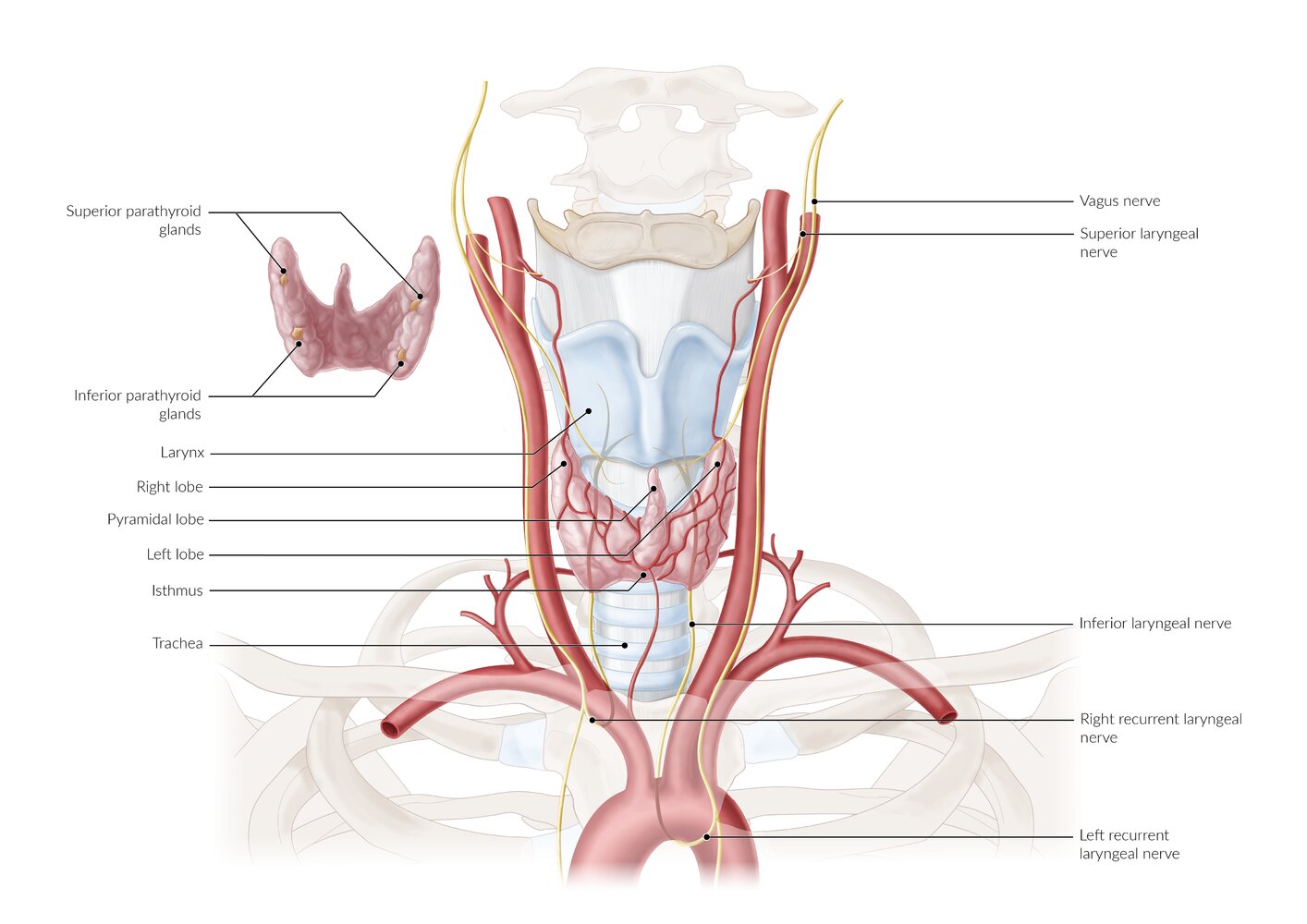
The thyroid gland is located in front of the trachea in the lower neck and consists of two lobes connected by an isthmus. A third pyramidal lobe extending from the isthmus is present in 50% of patients. This third lobe is a remnant of the thyroglossal duct.
The parathyroid glands are located posterior to the thyroid gland; they may vary in number and location. The recurrent laryngeal nerves (RLN) branch off from the vagus nerve; the left RLN loops under the aortic arch, and the right RLN passes beneath the subclavian artery. Both RLNs are vulnerable to injury during thyroid surgery as they ascend to the larynx behind the thyroid gland. Unilateral RLN injury may result in hoarseness, and bilateral RLN injury may cause dyspnea and stridor.
© AMBOSS
© AMBOSS
Accessory nerve palsy (XI)
Etiology
- Iatrogenic: most commonly from surgery of lateral cervical region; , especially posterior border of sternocleidomastoid muscle (e.g., resection of posterior cervical lymph nodes, radical neck dissection)
- Trauma (e.g., sternoclavicular joint dislocation, acromioclavicular joint dislocation)
- Tumor
Clinical features [55]
- Shoulder pain and heaviness
- Difficulty or inability to raise hand overhead
- Neckline asymmetry
Diagnostics [16][17]
Cranial nerve examination
Diagnosis is clinical, based on the cranial nerve examination.
- Inspect upper back, shoulder, and neck
-
Paresis, atrophy, and/or asymmetry of the trapezius muscle
- Ipsilateral shoulder drooping
- Lateral winging of the scapula
- Paresis, atrophy, and/or asymmetry of the sternocleidomastoid
-
Paresis, atrophy, and/or asymmetry of the trapezius muscle
- Assess the trapezius muscle.
- Ask the patient to shrug their shoulders.
- CN XI palsy results in weakness during elevation of the ipsilateral shoulder.
- Assess the sternocleidomastoid muscle.
- Ask the patient turn their head from side to side.
- CN XI palsy results in weakness in turning the head towards the contralateral side
Muscular atrophy is a late sequelae of CN XI palsy. [55]
Further evaluation
Consider further evaluation for underlying cause based on clinical findings. Studies may include:
- Imaging (i.e., MRI orbit, face, neck without and with IV contrast or CT neck with IV contrast): to evaluate for possible underlying compressive cause (e.g., malignancy) [17][18]
- Electromyography (EMG): to assess severity of impairment
Accessory nerve palsy should be part of the differential diagnosis of neck and shoulder pain. [55]
Treatment [16]
- Consult neurology and/or head and neck or plastic surgery.
-
Conservative measures can be considered for patients with mild dysfunction and/or evidence of improvement on follow-up. [55]
- Pain control with arm sling
- Physical therapy to strengthen shoulder girdle musculature
- Surgical measures (e.g., nerve grafting, neurolysis) [55][56]
- May be preferred for acute traumatic causes with severe dysfunction
- Consider within 6 months of onset if there is poor response to conservative management
Hypoglossal nerve palsy (XII)
Etiology
- Tumors (e.g., glomus jugulare)
-
Trauma
- Occipital condyle fractures, skull base fractures
- Iatrogenic trauma (e.g., neck dissection, endotracheal intubation, laryngeal mask airway) [57]
- Dissection of the internal carotid artery
- Stroke
- Demyelination
Clinical features
- Dysarthria
- Difficulty swallowing
- Atrophy and fasciculation of the tongue on the side of the lesion
Diagnostics [17]
Cranial nerve examination
Diagnosis is clinical, based on the cranial nerve examination. Ask the patient to:
- Press tongue against each cheek: Pressure to the cheek of the affected side might be increased.
- Stick out their tongue
- Deviation of the tongue to the ipsilateral side when protruded due to weakness of the ipsilateral tongue muscles.
- Signs of unilateral lower motor neuron damage: tongue atrophy, fasciculations, or asymmetry

Further evaluation
Consider further evaluation to identify lesion location and underlying cause based on clinical findings. Studies may include:
- Imaging [17][18]
- MRI head and neck (without and with IV contrast) : to locate nerve lesion and possible etiologies
- CT skull base and neck with IV contrast: may be performed in conjunction with MRI to evaluate the foramina and skull base (e.g., for fractures, skull base tumors)
- Electromyography (EMG): to assess severity of of nerve damage
Treatment [16]
- Consult neurology and speech language pathology.
- Consider early surgery in acute nerve injury. [16]
- Unilateral nerve injury
- May spontaneously resolve within 6 months.
- Advise patients to chew on the unaffected side.
- Bilateral nerve injury: Consider enteral feeding strategies for swallowing difficulty.
© AMBOSS
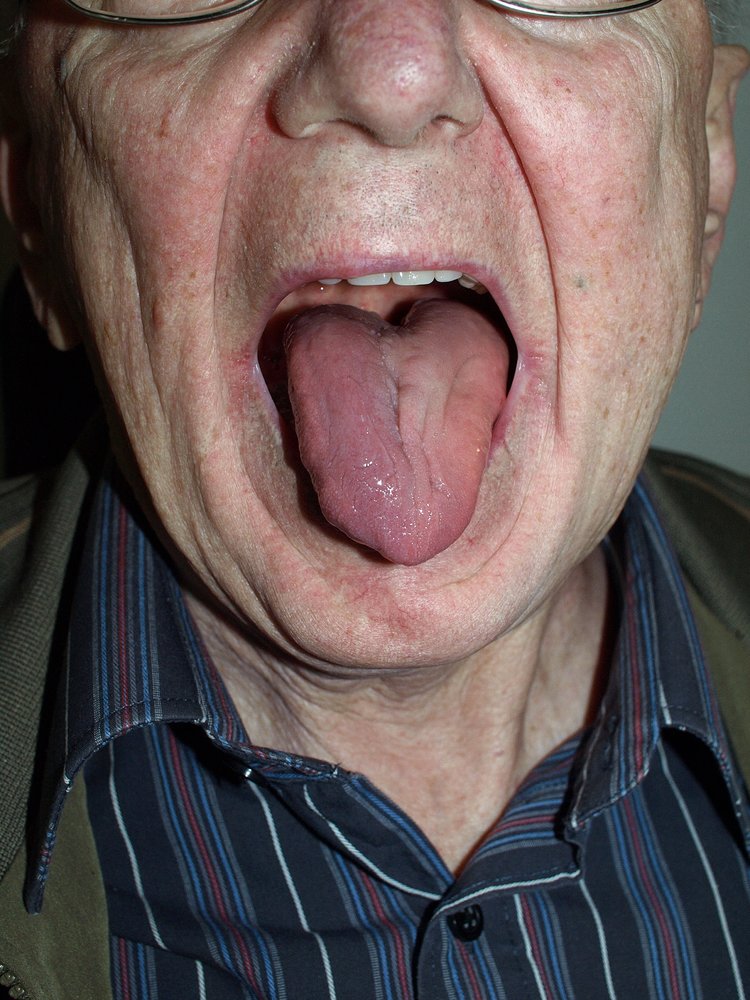
The muscles of the left side of the tongue have atrophied, which can be seen in the slight deviation of the tip of the tongue to the left and the smoother surface of the left side.
This finding is typically seen in lesions affecting the left hypoglossal nerve (XII). When the tongue protrudes, it deviates to the side of the lesion. Hypoglossal nerve lesions can be the result of peripheral (i.e., trauma, postoperative) or central (i.e., ischemia, poliomyelitis) damage.
Source: “Hypoglossal paralysis” by Klaus D. Peter, Wikimedia Commons, licensed under CC BY 3.0.
{kind=link}
Multiple cranial neuropathies
| Overview of multiple cranial neuropathies [58][59][60] | |||
|---|---|---|---|
| Condition | Affected cranial nerve | Cause | Clinical features |
| Chronic meningitis |
|
|
|
| Jugular foramen syndrome |
|
|
|
| Cavernous sinus syndrome |
|
|
|
| Cerebellopontine angle syndrome |
|
|
|
| Guillain-Barré syndrome |
|
|
|
| Multiple sclerosis |
|
|
|
External Resources
References
- Erman AB, Kejner AE, Hogikyan ND, Feldman EL. "Disorders of cranial nerves IX and X". Semin Neurol. 29(1). :85–92. (2009)
- Tubbs RS. "Nerves and Nerve Injuries". Academic Press. (2015). ISBN: 9780128026533
- Biaggioni I, Shibao CA, Diedrich A, et al. "Blood Pressure Management in Afferent Baroreflex Failure". J Am Coll Cardiol. 74(23). :2939-2947. (2019)
- Khaku A, Patel V, Zacharia T, Goldenberg D, McGinn J. "Guidelines for Radiographic Imaging of Cranial Neuropathies". Ear Nose Throat J. 96(10-11). :E23-E39. (2017)
- Blumenfeld A, Nikolskaya G. "Glossopharyngeal Neuralgia". Curr Pain Headache Rep. 17(7). (2013)
- Policeni B et al. "ACR Appropriateness Criteria ® Cranial Neuropathy". J Am Coll Radiol. 14(11). :S406-S420. (2017)
- Morillon P, Bremner F. "Trochlear nerve palsy.". Br J Hosp Med (Lond). 78(3). :C38-C40. (2017)
- Sharma AK, Kim DD, Fraser JA. "Pearls & Oy-sters: Paradoxical Head Tilt in a Congenital Fourth Nerve Palsy". Neurology. 97(3). :e320-e323. (2021)
- Murchison AP. "Neuroimaging and Acute Ocular Motor Mononeuropathies". Arch Ophthal. 129(3). :301. (2011)
- Kennedy TA, Corey AS, Policeni B, et al. "ACR Appropriateness Criteria® Orbits Vision and Visual Loss". J Am Coll Radiol. 15(5). :S116-S131. (2018)
- Lueck CJ. "Infranuclear ocular motor disorders". Elsevier. :281-318. (2011). ISBN: 9780444529039
- "The abducens nerve (CN VI)". https://teachmeanatomy.info/head/cranial-nerves/abducens-nerve/. [2019-03-13]
- Elder C, Hainline C, Galetta SL, Balcer LJ, Rucker JC. "Isolated Abducens Nerve Palsy: Update on Evaluation and Diagnosis". Curr Neurol Neurosci Rep. 16(8). (2016)
- "Duane syndrome". https://rarediseases.org/rare-diseases/duane-syndrome/
- Chan J, Albretson J. "Causes of isolated recurrent ipsilateral sixth nerve palsies in older adults: a case series and review of the literature". Clinical Ophthalmology. :373. (2015)
- Peragallo JH, Bruce BB, Hutchinson AK, et al. "Functional and Motor Outcomes of Strabismus Surgery for Chronic Isolated Adult Sixth Nerve Palsy". Neuro-Ophthalmology. 38(6). :320-325. (2014)
- Stachler RJ, Francis DO, Schwartz SR, et al. "Clinical Practice Guideline: Hoarseness (Dysphonia) (Update)". Otolaryngol Head Neck Surg. 158(1_suppl). :S1-S42. (2018)
- Taito M, Taito S, Banno M, et al. "Voice rehabilitation for laryngeal cancer after radiotherapy: a systematic review and meta-analysis". Eur Arch Otorhinolaryngol. 276(6). :1573-1583. (2019)
- Li Y, Garrett G, Zealear D. "Current Treatment Options for Bilateral Vocal Fold Paralysis: A State-of-the-Art Review". Clinical and experimental otorhinolaryngology. 10(3). :203-212. (2017)
- Chandawarkar RY, Cervino LA, Pennington GA. "Management of Iatrogenic Injury to the Spinal Accessory Nerve". Plast Reconstr Surg. 111(2). :611-617. (2003)
- Setter K, Voloshin I, Bigliani L. "Operative Treatment of Spinal Accessory Nerve Palsy". Techniques in Shoulder and Elbow Surgery. Volume 5(Issue 1). :25-36. (2004)
- Smith JH, Cutrer FM. "Numbness matters: A clinical review of trigeminal neuropathy". Cephalalgia. 31(10). :1131-1144. (2011)
- Shah AC, Barnes C, Spiekerman CF, Bollag LA. "Hypoglossal nerve palsy after airway management for general anesthesia: an analysis of 69 patients". Anesth Analg. 120(1). :105-120. (2015)
- Blumenfeld H. "Neuroanatomy Through Clinical Cases". Wiley-Blackwell. (2010). ISBN: 9780878936137
- Yanovitch T, Buckley E. "Diagnosis and management of third nerve palsy". Curr Opin Ophthalmol. 18(5). :373-378. (2007)
- Moore KL, Dalley AF, Agur AMR. "Clinically Oriented Anatomy". Lippincott Williams & Wilkins. (2013). ISBN: 9781451119459
- Tamhankar MA, Biousse V, Ying G-S, et al. "Isolated Third, Fourth, and Sixth Cranial Nerve Palsies from Presumed Microvascular versus Other Causes". Ophthalmology. 120(11). :2264-2269. (2013)
- Fang C, Leavitt JA, Hodge DO, et al. "Incidence and Etiologies of Acquired Third Nerve Palsy Using a Population-Based Method". JAMA Ophthalmology. 135(1). :23. (2017)
- Sadagopan KA, Wasserman BN. "Managing the patient with oculomotor nerve palsy". Curr Opin Ophthalmol. 24(5). :438-447. (2013)
- Steiner T, Juvela S, Unterberg A, et al. "European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage". Cerebrovasc Dis. 35(2). :93-112. (2013)
- Thompson BG, Brown RD, Amin-Hanjani S, et al. "Guidelines for the Management of Patients With Unruptured Intracranial Aneurysms". Stroke. 46(8). :2368-2400. (2015)
- Carroll CG, Campbell WW. "Multiple Cranial Neuropathies". Seminars in Neurology. 29(1). :53-65. (2009)
- Willison HJ, Jacobs BC, van Doorn PA. "Guillain-Barré syndrome". Lancet. 388. :717-727. (2016)
- "Multiple Sclerosis (MS)". https://www.merckmanuals.com/professional/neurologic-disorders/demyelinating-disorders/multiple-sclerosis-ms. [2016-08-01]
- "Peripheral Vestibular Nystagmus". https://www.aao.org/bcscsnippetdetail.aspx?id=d20f8ad8-845e-46fc-b7ed-7d00216c2726
- Thomas Brandt, Marianne Dieterich. "The dizzy patient: don't forget disorders of the central vestibular system". Nature Reviews Neurology. 13(6). :352-362. (2017)
- Chandrasekhar SS, Tsai Do BS, Schwartz SR, et al. "Clinical Practice Guideline: Sudden Hearing Loss (Update)". Otolaryngology–Head and Neck Surgery. 161(1_suppl). :S1-S45. (2019)
- "The olfactory nerve (CN I) and olfactory pathway". https://teachmeanatomy.info/head/cranial-nerves/olfactory-cni/. [2018-12-24]
- "The optic nerve (CN II) and visual pathway". https://teachmeanatomy.info/head/cranial-nerves/optic-cnii/. [2018-10-19]
- "The oculomotor nerve (CN III)". https://teachmeanatomy.info/head/cranial-nerves/oculomotor/. [2019-03-13]
- "The trochlear nerve (CN IV)". https://teachmeanatomy.info/head/cranial-nerves/trochlear-nerve/. [2019-03-13]
- "The opthalmic division of the trigeminal nerve (CNV1)". https://teachmeanatomy.info/head/nerves/ophthalmic-nerve/. [2017-12-22]
- "The opthalmic division of the trigeminal nerve (CNV2)". https://teachmeanatomy.info/head/nerves/maxillary-nerve/. [2018-12-24]
- "The opthalmic division of the trigeminal nerve (CNV3)". https://teachmeanatomy.info/head/nerves/mandibular-nerve/. [2018-04-02]
- "The facial nerve (CN VII)". https://teachmeanatomy.info/head/cranial-nerves/facial-nerve/. [2017-12-31]
- "The vestibulocochlear nerve (CN VIII)". https://teachmeanatomy.info/head/cranial-nerves/vestibulocochlear/. [2018-08-07]
- "The glossopharyngeal nerve (CN IX)". https://teachmeanatomy.info/head/cranial-nerves/glossopharyngeal-nerve/. [2018-01-02]
- "The accessory nerve (CN XI)". https://teachmeanatomy.info/head/cranial-nerves/accessory/. [2018-01-02]
- "The hypoglossal nerve (CN XII)". https://teachmeanatomy.info/head/cranial-nerves/hypoglossal/. [2019-01-20]
- Bähr M, Frotscher M. "Duus' Topical Diagnosis in Neurology". Thieme Medical Pub. (2012). ISBN: 9783136128053
- Ahmed HU. "A case of mistaken muscles". BMJ. 324(7343). :962-962. (2002)
- Wrobel BB, Leopold DA. "Smell and taste disorders.". Facial Plast Surg Clin North Am. 12(4). :459-68, vii. (2004)
- Bromley SM. "Smell and taste disorders: a primary care approach.". Am Fam Physician. 61(2). :427-36, 438. (2000)
- Malaty J, Malaty IA. "Smell and taste disorders in primary care". Am Fam Physician. 88(12). :852-9. (2013)
- Pellegrino R, Han P, Reither N, Hummel T. "Effectiveness of olfactory training on different severities of posttraumatic loss of smell". Laryngoscope. 129(8). :1737-1743. (2019)
- Pekala K, Chandra RK, Turner JH. "Efficacy of olfactory training in patients with olfactory loss: a systematic review and meta-analysis". International Forum of Allergy & Rhinology. 6(3). :299-307. (2015)
- Pinto JM. "Olfaction". Proc Am Thorac Soc. 8(1). :46-52. (2011)
- Riordan-Eva P. "Clinical assessment of optic nerve disorders". Eye (Lond). 18(11). :1161-1168. (2004)
- Vodopivec I, Rizzo JF. "Ophthalmic manifestations of giant cell arteritis". Rheumatology. 57(suppl_2). :ii63-ii72. (2018)
- Behbehani R. "Clinical approach to optic neuropathies.". Clin Ophthalmol. 1(3). :233-46. (2007)
- "DIAGNOSIS: How are vestibular disorders diagnosed?". https://vestibular.org/understanding-vestibular-disorder/diagnosis
- "The vagus nerve (CN X)". https://teachmeanatomy.info/head/cranial-nerves/vagus-nerve-cn-x/. [2019-01-28]
- "Gastroparesis Diagnosis". https://www.ucsfhealth.org/conditions/gastroparesis/diagnosis.html
- "Bedside Water-Swallow Testing for Dysphagia". https://www.jwatch.org/na41936/2016/07/28/bedside-water-swallow-testing-dysphagia. [2016-07-28]