Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- CBC
- CMP
- CRP
- Stool fecal calprotectin
- Stool studies to evaluate for infectious diarrhea (e.g., C. difficile toxin)
- Cross-sectional enterography (MRE or CTE)
- Consult gastroenterology for endoscopy.
Red flag features
- Hemodynamic instability
- Peritoneal signs
- High fever
- Signs of bowel obstruction
- Severe hematochezia
- Toxic megacolon
Management checklist
- IV access and fluid resuscitation
- NPO
- Pain management
- Oral glucocorticoids for most patients (e.g., budesonide for limited disease, prednisone for moderate to severe colonic disease)
- IV glucocorticoids (e.g., methylprednisolone ) for severe to fulminant CD
- Broad-spectrum empiric antibiotic therapy for intraabdominal infections, only if infection is suspected
- Consult gastroenterology for medication management.
- Consult general surgery if complications are suspected.
Summary
Crohn disease (CD) is an inflammatory bowel disease (IBD) of unclear etiology. Unlike ulcerative colitis, CD is not limited to the colon but can manifest anywhere in the gastrointestinal tract. Clinical features commonly include diarrhea, weight loss, and abdominal pain. Extraintestinal manifestations may occur in the eyes, joints, and skin. Diagnosis is based on laboratory studies (e.g., elevated CRP, fecal calprotectin), characteristic endoscopic features (e.g., ulcerations, skip lesions, cobblestone appearance), and evidence of intestinal inflammation on imaging. Medical management aims to induce and maintain remission; it is tailored to the patient and influenced by the location and severity of CD. Acute flares are typically managed with glucocorticoids and biologics (e.g., anti-TNF-α antibodies). Maintenance therapy (using, e.g., biologics, immunomodulators) focuses on limiting the frequency and duration of inflammatory episodes. Surgery is ultimately required in up to half of patients with CD; clinical manifestations commonly recur after surgery. Complications of CD include malabsorption, iron and vitamin deficiency, strictures, bowel obstruction, intraabdominal abscesses, and increased risk of bowel cancer.

© AMBOSS
Epidemiology
- Prevalence: 1 case per 500 population
- Incidence: ∼ 6 cases per 100,000 population per year [1]
- Sex: ♂ = ♀
- Typical age of onset: bimodal distribution with one peak at 15–35 years and another one at 55–70 years [2][3]
-
Populations with higher prevalence [4]
- Individuals of Northern European descent
- Individuals of Ashkenazi Jewish descent
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Cause: Immune dysregulation and dysbiosis, which promotes chronic inflammation, the ultimate cause of which is not fully understood.
-
Risk factors [4]
- Familial aggregation
- Genetic predisposition (e.g., mutation of the NOD2 gene, HLA-B27 association)
- Tobacco smoke
Smoking tobacco is the primary modifiable risk factor for CD. Therefore, smoking cessation is especially important in patients with CD.
Pathophysiology
Inflammation
Inflammation is most likely caused by immune dysregulation.
- Dysregulation of IL-23-Th17 signaling → unrestrained Th17 cell function → inflammation → local tissue damage (edema, erosions/ulcers, necrosis) → obstruction, fibrotic scarring, stricture, and strangulation of the bowel [5]
- Mutations in the nucleotide oligomerization binding domain 2 (NOD2) protein are likely involved in the development of CD.
Abscess and fistula formation
- Intestinal aphthous ulcers → transmural fissures and inflammation of the intestinal walls → adherence of other organs or the skin → penetration of tissue → microperforation and abscess formation → macroperforation into these structures → fistula formation
Clinical features
CD typically has a chronic intermittent course with episodic acute flares and periods of remission. Clinical features differ according to the severity of CD. Patients with mild CD may be asymptomatic while patients with fulminant CD have severe symptoms.
Constitutional symptoms [6]
- Low-grade fever
- Weight loss
- Fatigue
Gastrointestinal symptoms [6]
CD most commonly affects the terminal ileum and colon, but involvement of any part of the GI tract (from mouth to anus) is possible. In contrast to ulcerative colitis, rectal involvement is uncommon.
- Chronic diarrhea
- Lower gastrointestinal bleeding (uncommon)
- Abdominal pain, typically in the RLQ
- Palpable abdominal mass in the RLQ
- Features of upper gastrointestinal CD [7]
- Often asymptomatic
- Epigastric pain
- Nausea and vomiting
- Dysphagia, odynophagia, dyspepsia
- Signs of gastric outlet obstruction (e.g., early satiety, postprandial fullness) [8]
- Features of CD complications
- Malabsorption (e.g., weight loss, anemia, failure to thrive ; )
- Enterocutaneous or perianal fistulas, often associated with abscess formation [9]
Perianal lesions are occasionally the first manifestation of Crohn disease.[10]


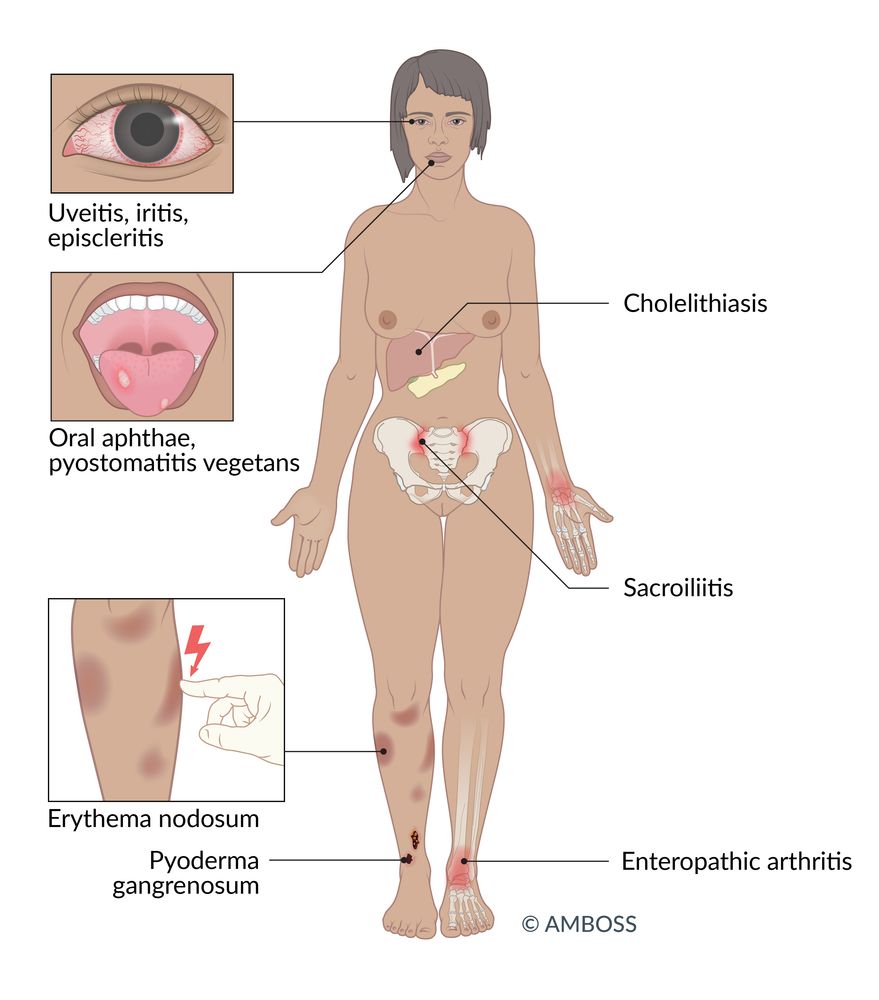
Extraintestinal symptoms [11]
Extraintestinal manifestations of CD are present in 20–30% of patients with CD. [12]
-
Joints
-
Enteropathic arthritis
- A seronegative spondyloarthropathy that develops in association with inflammatory bowel disease
- Typically affects joints of the lower extremities but can also involve the spine (e.g., sacroiliitis, spondylitis, inflammation of peripheral joints).
- Nail clubbing [13]
-
Enteropathic arthritis
-
Eyes
- Uveitis
- Iritis
- Episcleritis
- Liver/bile ducts: cholelithiasis
- Urogenital system: urolithiasis (mostly calcium oxalate stones)
-
Oral mucosa
- Oral aphthae
- Pyostomatitis vegetans
-
Skin
- Erythema nodosum
- Acrodermatitis enteropathica
- Pyoderma gangrenosum


A large mass, with erythema of the overlying skin, can be seen in the right lower quadrant of the abdomen.
The chronic inflammation of Crohn disease can cause adhesions, fistulas, abscesses, or strictures, most commonly in the terminal ileum, which may result in a palpable or even visible mass.
Source: © IMPP
© AMBOSS
Classification
Crohn disease severity
The severity of CD is based on clinical features, laboratory studies, and anatomical findings. [10]
| Crohn disease severity [10] | |||
|---|---|---|---|
| Clinical features | Laboratory studies | Anatomical findings (on endoscopy or imaging) | |
| Mild CD |
|
|
|
| Moderate to severe CD |
|
|
|
| Severe to fulminant CD |
|
|
|
Diagnosis
Approach [10][14]
- Evaluate patients with chronic diarrhea and/or abdominal pain for CD.
-
Obtain laboratory studies (blood and stool) to:
- Rule out differential diagnoses of CD (e.g., infectious gastroenteritis).
- Assess and monitor disease activity.
-
Consult gastroenterology for endoscopy with histological examination to:
- Definitively diagnose CD.
- Determine the extent and severity of disease.
- Assess distribution and monitor disease activity.
- Perform cross-sectional imaging to establish the location and severity of disease and identify complications.
Endoscopy, cross-sectional imaging, and laboratory studies are required for the initial evaluation of suspected CD, evaluation of an acute flare, and monitoring the response to therapy.
Laboratory studies [6][10]
Blood tests
- CBC: may show anemia, ↑ platelets (reactive thrombocytosis)
-
Inflammatory markers: CRP, ESR
- CRP has a greater correlation with disease activity than ESR.
- Both may be normal in patients with mild CD.
-
CMP
- ↑ Creatinine
- ↓ Albumin (marker of inflammation)
- Iron studies, vitamin B12, folate: to evaluate for micronutrient deficiency [15]
-
Serology: not routinely recommended due to low sensitivity
- ↑ Anti-saccharomyces cerevisiae antibodies: more commonly elevated in CD than in ulcerative colitis
- pANCA: more commonly elevated in ulcerative colitis than in CD [10][16]
- Specialized studies
- Thiopurine methyltransferase (TPMT) activity
- Genetic testing: considered in selected patients
Stool studies
- Stool analysis ; of diarrhea: to identify bacterial infection (including C. difficile infection), ova, and/or cysts (see also "Diagnostics for infectious gastroenteritis")
-
Fecal calprotectin and/or fecal lactoferrin: noninvasive markers of intestinal inflammation
- Fecal calprotectin: elevated (> 50–100 μg/g)
- Used to monitor disease activity and response to therapy
- Helps differentiate IBD from irritable bowel syndrome
Anemia in CD may result from chronic disease, iron deficiency, and/or vitamin B12 deficiency.
Endoscopy
Ileocolonoscopy [10]
-
Indication: all patients with suspected CD
- Assesses the distribution and severity of the disease
- Aids differentiation of CD from other diseases (e.g., ulcerative colitis)
- Monitors disease activity (e.g., active disease, remission)
- Can be used therapeutically (e.g., stricture dilatation)
-
Supportive findings [10][14][17]
- Skip lesions: segmental and/or discontinuous pattern of involvement (interspersed with normal tissue)
- Linear and/or serpiginous ulcerations
- Small aphthous ulcerations
- Cobblestone sign: inflamed edematous sections interspersed with deep ulcerations that resemble cobblestones
- Erythema, fissures, strictures, and fistulas
-
Biopsy
- Histopathology: Confirm CD (e.g., chronic inflammation).
- Exclude CMV colitis in unresponsive CD (e.g., immunohistochemistry for CMV antigens): See "Diagnosis of CMV infection." [18]
Discontinuous areas of inflammation, cobblestone appearance of the affected mucosa, and mucosal ulcerations are hallmark endoscopic findings of CD. [19]
Other endoscopic techniques [10]
- Upper endoscopy: if upper GI involvement is suspected [10][20]
- Video capsule endoscopy: Consider in patients with suspected small bowel CD (as an alternative to cross-sectional imaging).
Small bowel evaluation is an essential part of the initial diagnostic workup of CD. Almost one-third of patients with CD have only small bowel disease, which may not be visible on ileocolonoscopy. [10]



Imaging [6][10][21][22]
Cross-sectional imaging is used to evaluate the entire GI tract, and it can identify inflammation and complications (e.g., bowel obstruction, abscess, fistula) that are not visible on endoscopy.
Indications
- Suspected CD (part of initial evaluation)
- Localization of inflammation and assessment of severity [10][21]
- Evaluation of suspected acute flare or complications (e.g., abscess)
- Before starting biologics: to ensure there are no pyogenic complications (e.g., abscess)
- Serial imaging to assess response to therapy
Modalities and supportive findings
-
Cross-sectional enterography (MR enterography, CT enterography): preferred imaging modality for CD ; [10]
- Edematous thickening of the intestinal wall
- Mucosal enhancement, mesenteric fat stranding
- Creeping fat: excessive mesenteric fat around the affected segments of bowel [23]
- Can also identify:
- Complications (e.g., strictures, fistulas, abscesses)
- Extraluminal disease (e.g., cholelithiasis, urolithiasis)
- Response to therapy (e.g., healing of ulcers)
- CT abdomen and pelvis (with IV contrast): preferred in acutely ill patients who cannot tolerate PO contrast
-
Additional modalities [10][21]
-
Ultrasound abdomen
- Consider for initial evaluation of suspected CD and for disease monitoring. [21]
- Supportive finding (of active disease): bowel wall thickening (> 4 mm)
- Plain x-ray abdomen: Consider for expedited assessment of complications.
-
MRI abdomen and pelvis (with IV contrast) or endscopic ultrasound [10][21]
- Preferred modality to evaluate for perianal fistulas and/or abscess
- Endoscopic ultrasound can be used to monitor treatment response.
-
Ultrasound abdomen




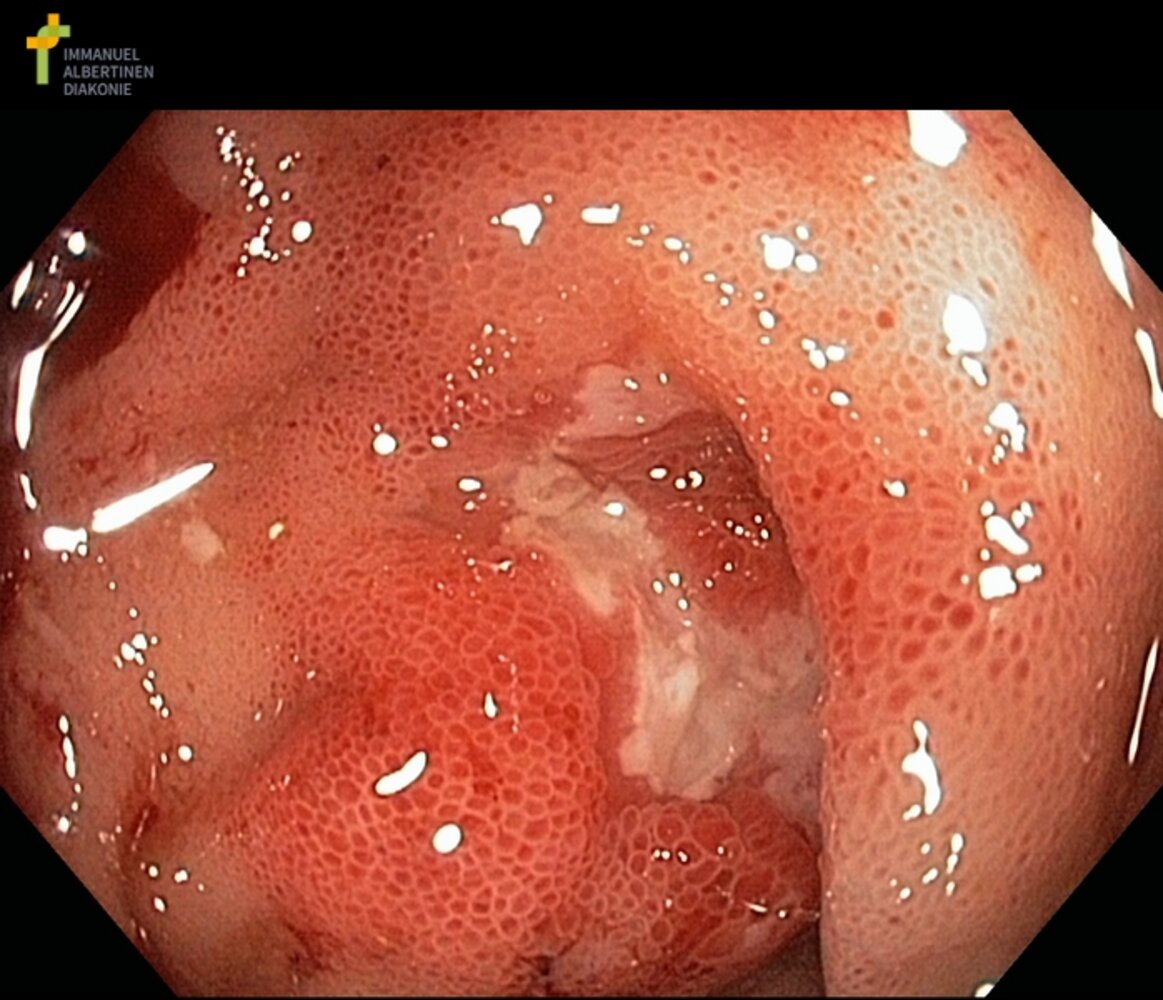
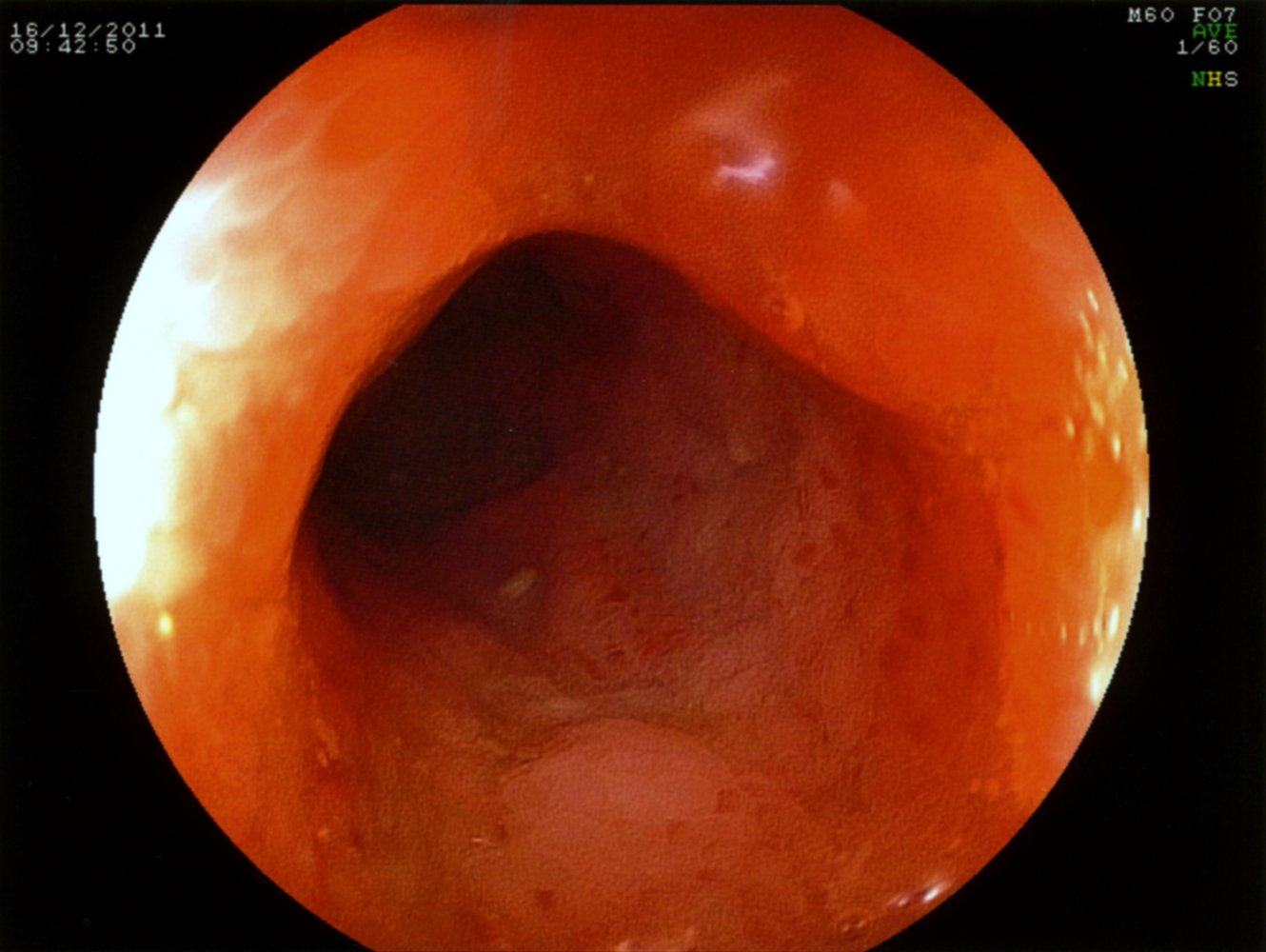
Endoscopic view of the terminal ileum
A fibrin-covered serpiginous ulceration is visible. The surrounding mucosa is erythematous and edematous.
These findings are characteristic of Crohn disease.
Our great thanks to Albertinen Krankenhaus, Hamburg, Germany, for kindly providing this case.
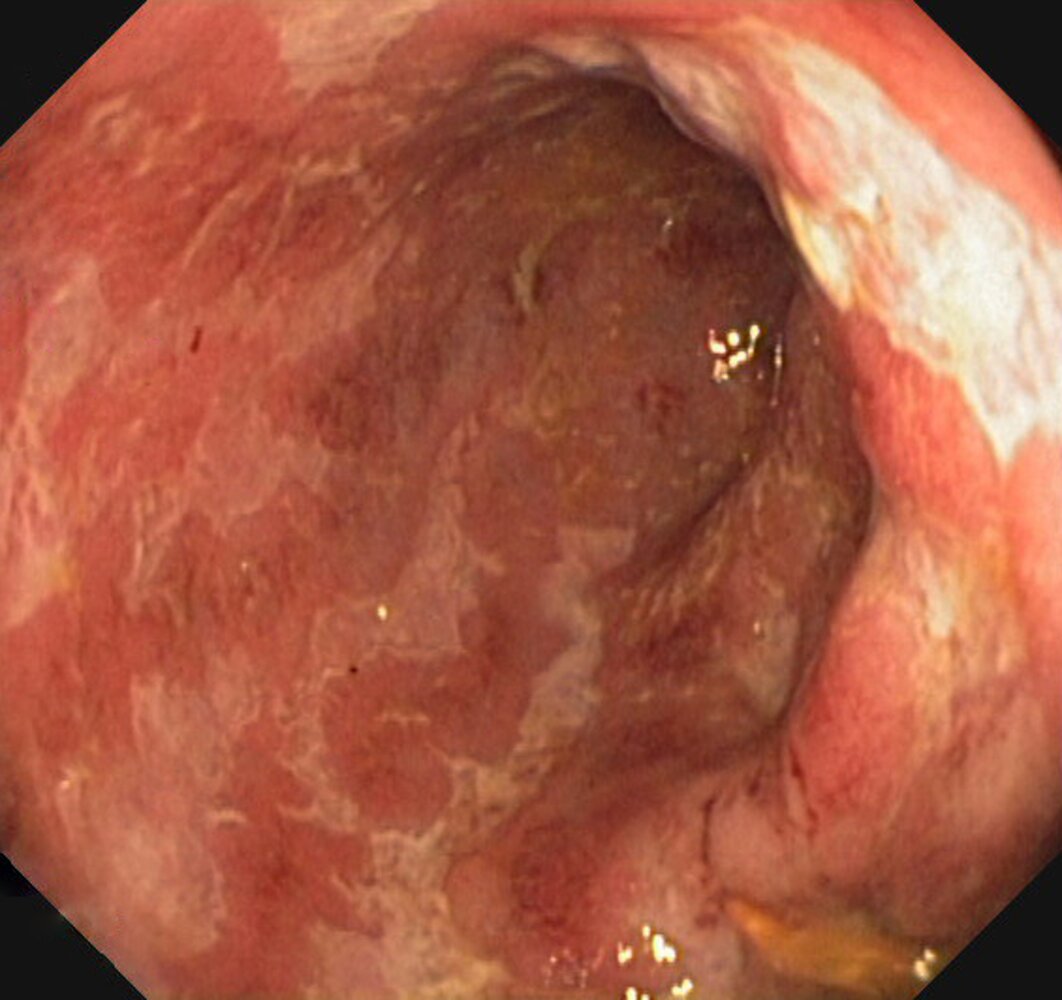
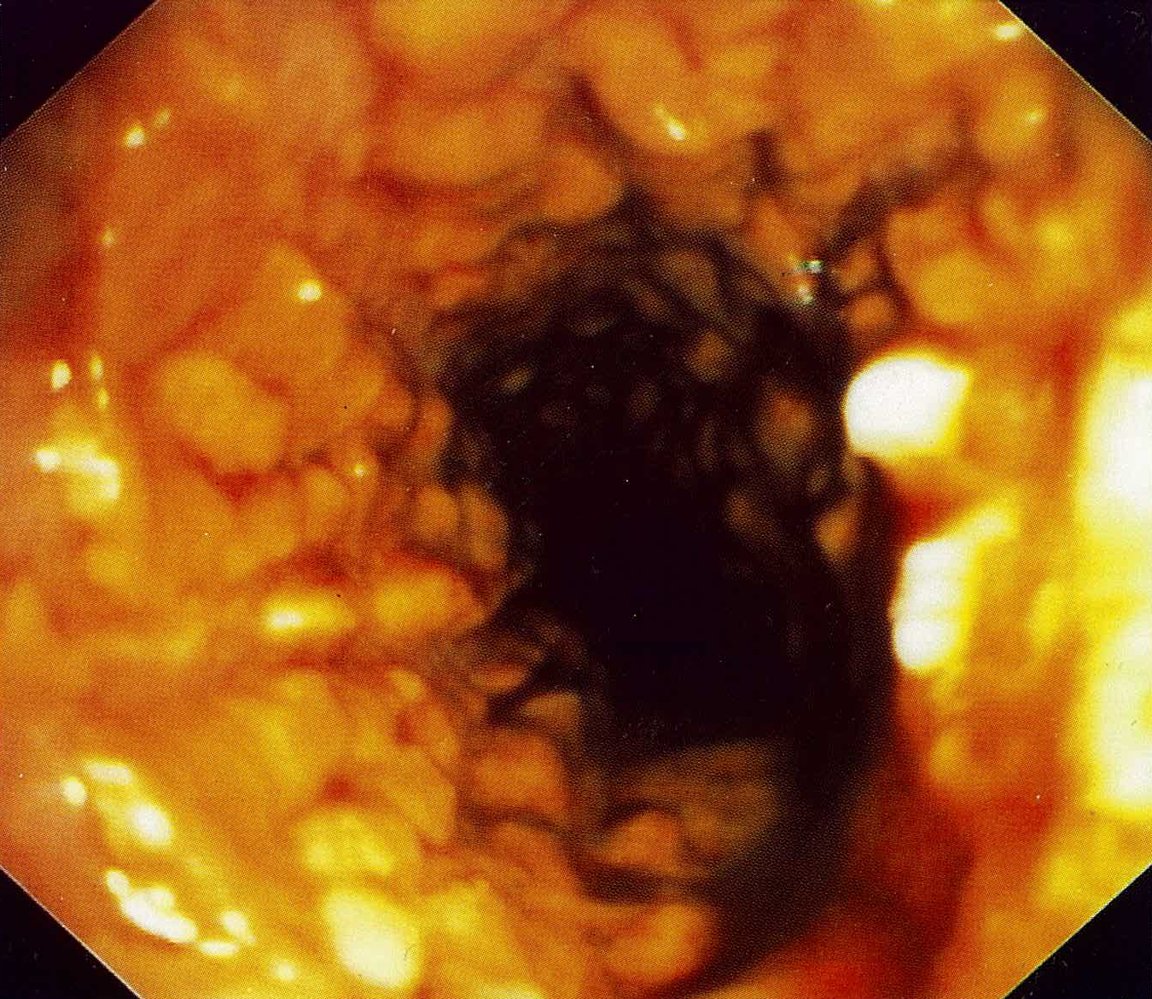
Endoscopic view of the colon
Multiple linear and serpiginous ulcerations covered with fibrinous exudate can be seen. The mucosa between the ulcerations is erythematous and has lost its normal vascular pattern.
These findings are characteristic of Crohn disease.
Our great thanks to sono.gallery, a medical ultrasound library by Dr. Daniel Merkel, for providing the images and videos.
Endoscopic view of the terminal ileum
Erythema and small aphthous ulcerations are visible on the mucosa. The edematous surface resembles a cobblestone appearance.
These findings are characteristic of Crohn disease.
Source: © IMPP
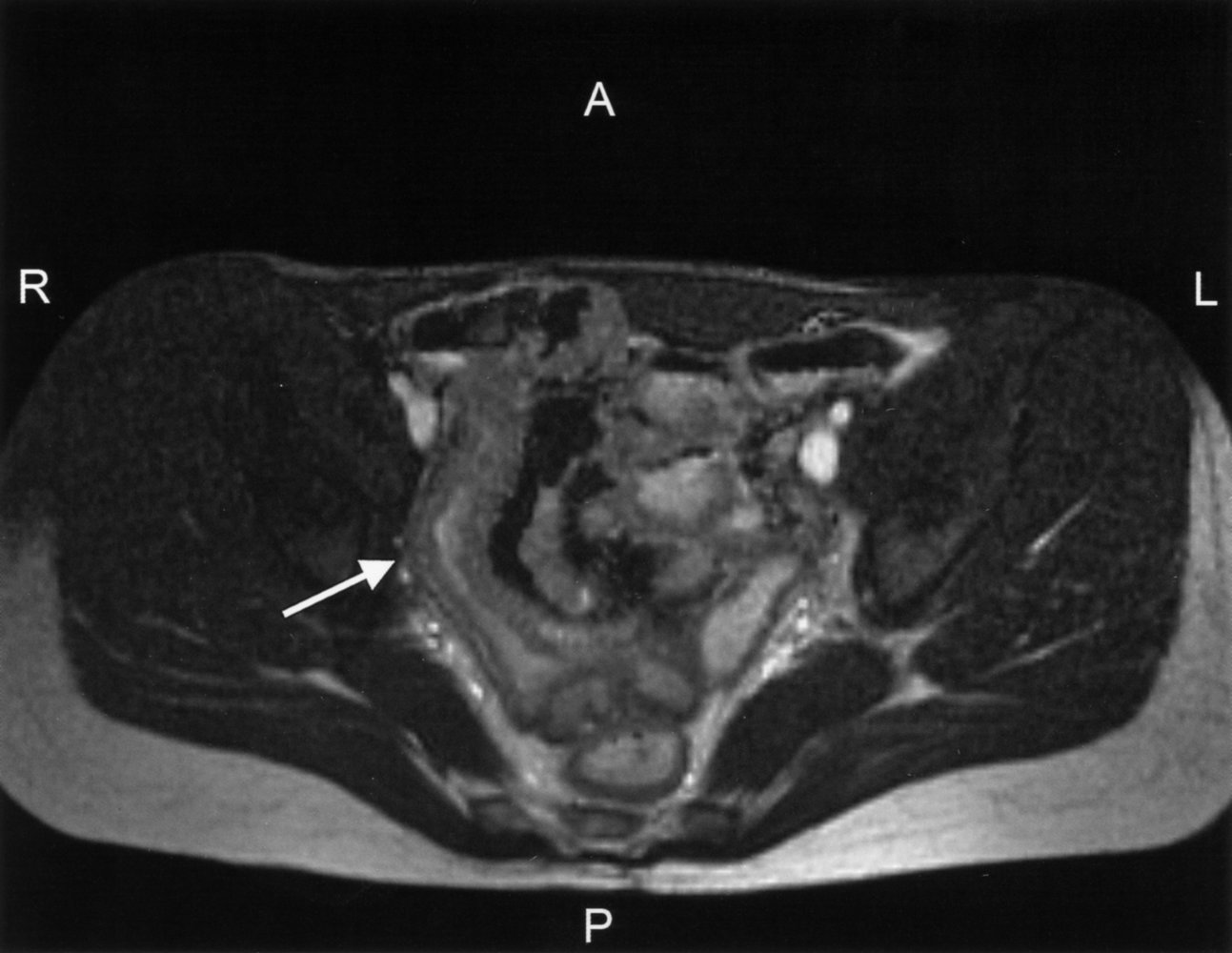
MR enterography of a patient with Crohn disease
The wall of the terminal ileum is thickened (green overlay, white arrow) and its lumen is narrowed (green arrows, 1).
ICJ = ileocecal junction; C = colon
Source: © IMPP
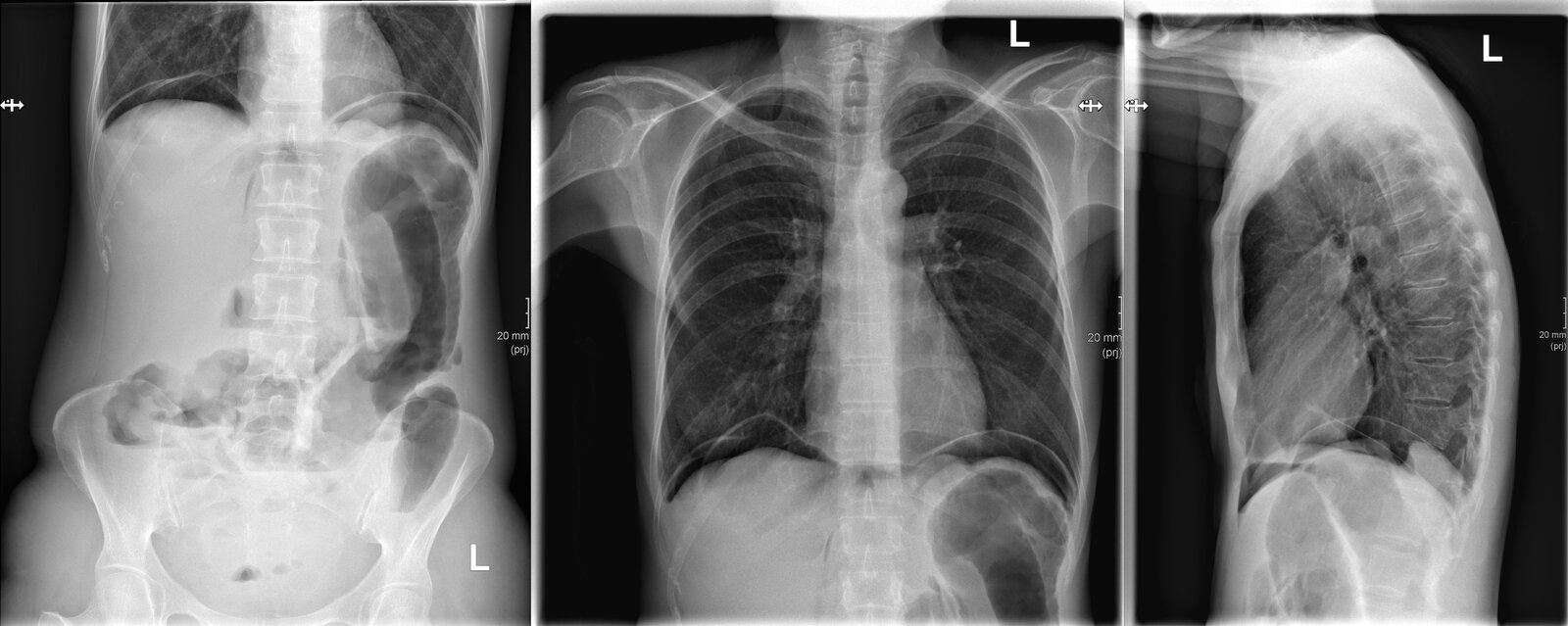
X-ray abdomen (AP erect view) and chest (PA and lateral views)
Multiple air-fluid levels are seen in the colon and small bowel (examples indicated by black lines). Some dilated segments of left colon are seen and gas is present in the peritoneal space as a result of bowel perforation. Gas is primarily located beneath the diaphragms (green overlay) because of the erect positioning of the patient. Additional gas has dissected into the retroperitoneum (examples indicated by red overlay) and is visible as linear collections parallel to the spine.
Our great thanks to Kerstin Bohse, MD (Klinikum Pfeiffersche Stiftungen), for kindly providing this case.
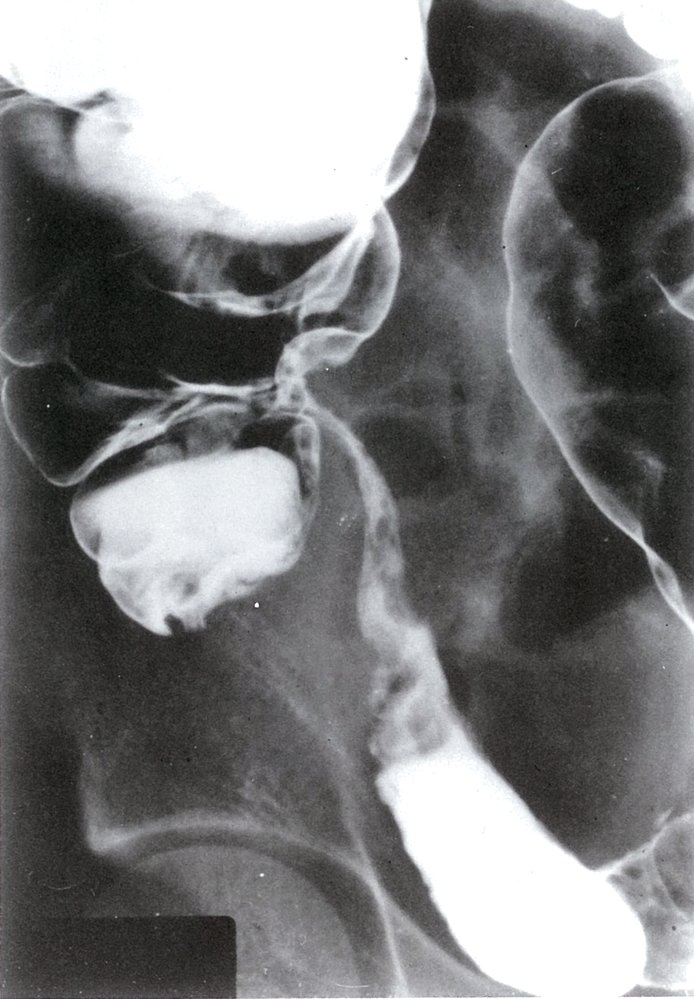
Fluoroscopy (enteroclysis; right lower quadrant; AP view) of a patient with Crohn disease
The terminal ileum (I) is incompletely distended as a result of stricture (S) formation. It has a string-like appearance and is separated from other bowel loops.
The most common location of the string sign in Crohn disease is the terminal ileum. Separation from adjacent bowel loops is due to an increase in adjacent mesenteric fat.
C = cecum; A = ascending colon
Source: © IMPP

Fluoroscopy small bowel (enteroclysis; view of pelvis) of a patient with Crohn disease
Contrast is present throughout the small bowel. A narrowed segment consistent with a stricture (green overlay) did not distend during the procedure.
Sacroiliac (SI) joints: arrows
Source: “Duenndarmstenose Morbus Crohn KM-Passage 010” by Hellerhoff, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
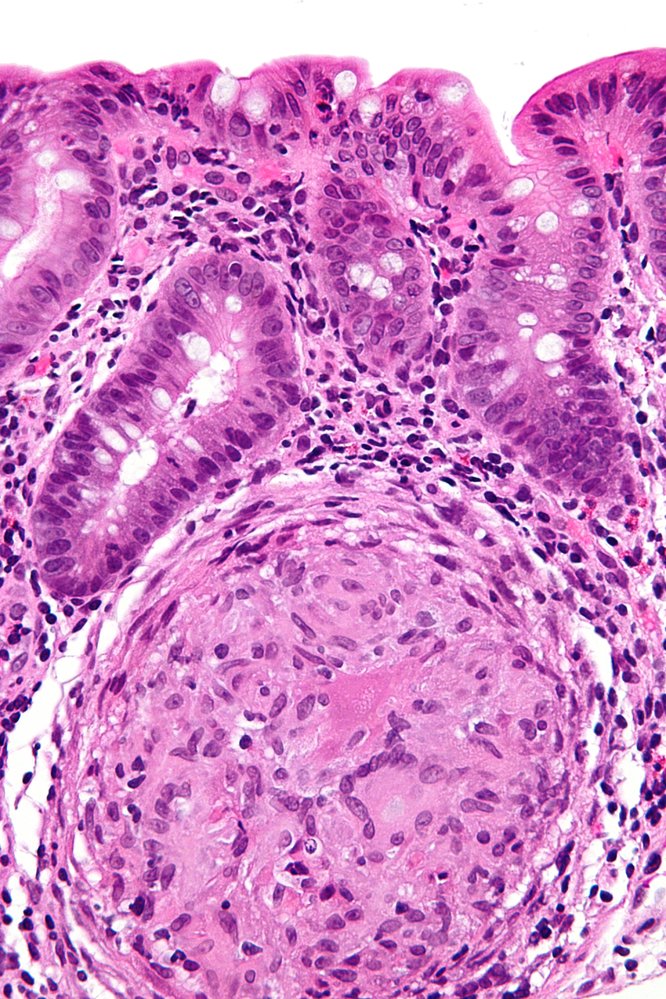
Pathology
-
Transmural inflammation: all mucosal layers of the intestinal wall are involved
- Noncaseating granulomas [24]
- Giant cells
- Distinct lymphoid aggregates of the lamina propria
- Creeping fat
- Hypertrophic lymph nodes





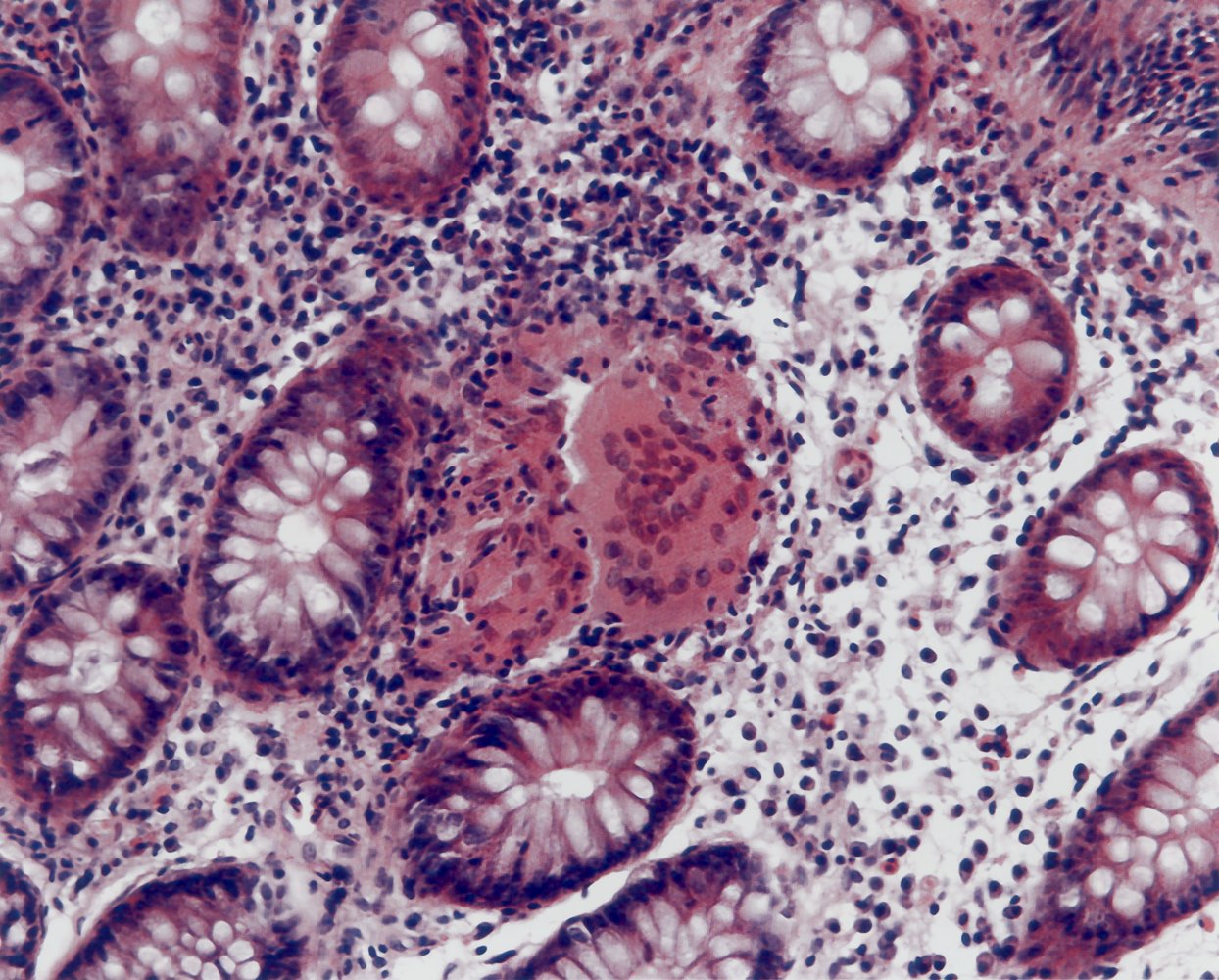
Photomicrograph of colonic mucosal tissue (H&E stain; 450x magnification)
Colonic crypts (example indicated by green dashed outline) with goblet cells (examples indicated by yellow overlays) and an epithelioid cell granuloma without necrosis (red overlay) are visible. In the area immediately surrounding the granuloma and its multinucleated giant cell (purple overlay), a lymphocytic infiltrate (white arrowhead) and numerous neutrophil granulocytes can be found.
These findings are characteristic of Crohn disease.
Source: © IMPP
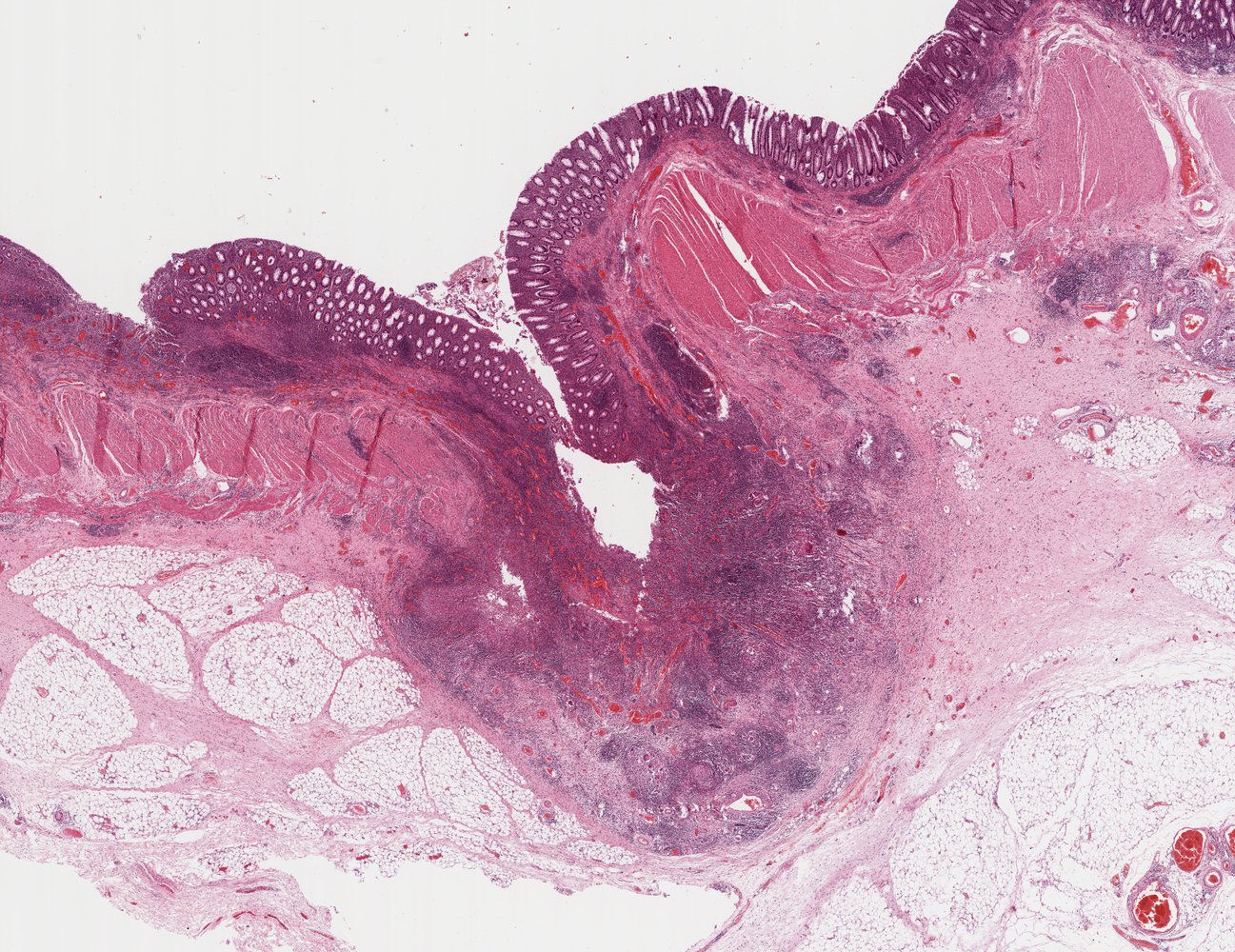
Photomicrograph of a biopsy specimen of the cecum (H&E stain; low magnification)
Large numbers of lymphocytes, giant cells, and epithelioid cells are seen clustered around a large granuloma.
This is a typical histological finding in Crohn disease.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
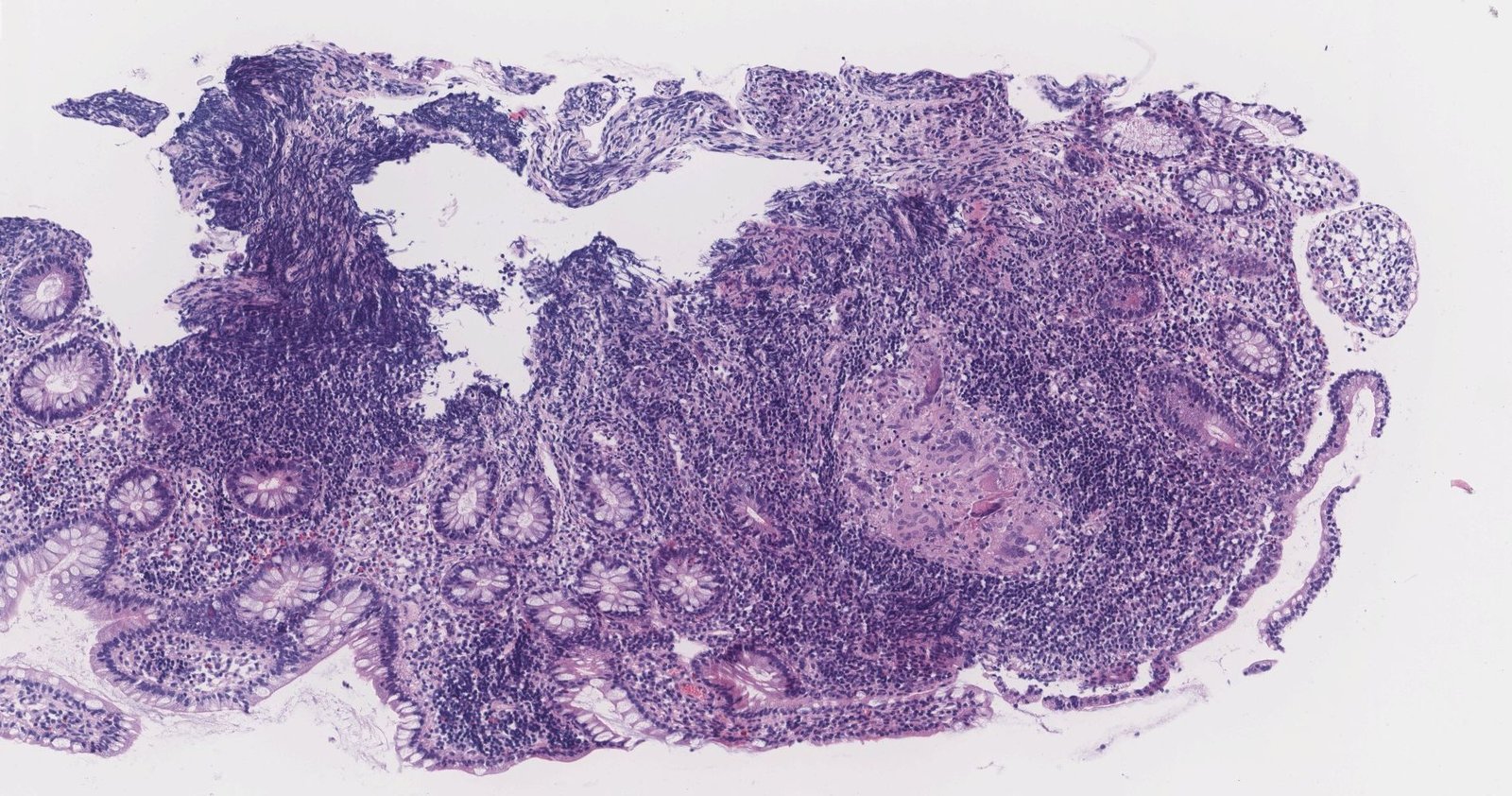
Photomicrograph of biopsy specimen of the colon (H&E stain; low magnification)
There are epithelioid cell granulomas and inflammation penetrating from the colonic mucosa to the subserosal adipose tissue, with a strong contrast between the areas of active inflammation and those free of inflammation.
This is a typical histological finding of Crohn disease.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. Alberto Perez Bouza
Photomicrograph of a colon biopsy specimen (H&E stain; high magnification)
Infiltrating neutrophils (examples indicated by arrowheads) can be seen in the crypts in the upper part of the image. A noncaseating granuloma (green overlay) is visible in the lower part of the image.
These features indicate transmural inflammation, which is a characteristic finding of Crohn disease.
Source: “Crohn's disease - colon - very high mag” by Nephron, Wikimedia Commons, licensed under CC BY-SA 3.0. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}

Photograph of surgical resection specimen
There are marked inflammatory changes of the colonic mucosa. A cobblestone pattern of the mucosa is visible in the lower right edge of the specimen.
Source: © IMPP
Treatment
General principles [10]
- Refer all patients to gastroenterology.
- Tailor therapy to the severity of CD, phase of the disease (acute flare or remission), and risk of progression of CD.
- Early use of biologics (e.g., anti-TNF-α antibodies) is the standard of care in new active CD.
- Surgery may be required to manage complications and is an option for isolated short-segment disease.
- Lifestyle modifications (e.g., smoking cessation) may decrease the incidence of complications.
- Regular monitoring of disease activity and screening for complications are essential aspects of long-term management.
Management of acute flare of CD
- Hemodynamic support as needed (e.g., for severe to fulminant CD): IV fluids, electrolyte repletion
- Consult gastroenterology early to determine choice of induction therapy.
- Screen for and administer prophylaxis against common infectious diseases.
- Patients with severe or fulminant CD typically require hospitalization.
- Initiate thromboprophylaxis as needed (e.g., presence of risk factors for VTE, hospitalization). [22][25]
- Identify and treat malnutrition and micronutrient deficiency.
Infectious disease screening and prophylaxis [22]
Perform prior to initiating therapy if feasible as most medications for CD can cause immunosuppression.
- Update immunization status at diagnosis: See “ACIP immunization schedule” for details.
- Screen for viral infections (hepatitis B, hepatitis C, HIV, Epstein-Barr virus) and tuberculosis. [15][22]
- Consult infectious disease before initiating therapy if screening tests are positive. [22]
Pharmacological treatment [10][26]
-
Induction phase
- Used to manage acute flares.
- Agents that have a rapid onset of action (e.g., glucocorticoids, biologics) are used.
- Should be continued until there is objective evidence of remission (typically < 3 months). [10]
- Endoscopic evidence of remission (e.g., healing ulcers) is currently the best indicator of remission of colonic CD. [10][27]
- Noninvasive markers of intestinal inflammation (fecal calprotectin, cross-sectional imaging) are suitable alternatives to evaluate for remission.
-
Maintenance phase
- Used to maintain remission (e.g., in new active CD regardless of severity, in patients with moderate or severe CD, and/or those at high risk of progression of CD) [10][28]
- Biologics and immunomodulators are the principal agents of maintenance therapy.
- Typically continued for a prolonged period of time. [29]
Symptoms alone do not accurately correlate with disease activity. Use objective markers of disease severity (e.g., biomarkers, imaging, endoscopy) to assess the severity of CD, guide treatment, and verify remission. [10]
Overview of commonly used medications [10][26]
-
Glucocorticoids
- Primarily used to induce remission
-
Agents used (depending on severity of CD):
-
Controlled ileal release budesonide
- A formulation of the synthetic steroid budesonide that is released in environments with a pH ≥ 5.5, which facilitates drug delivery distal to the proximal small bowel
- Used to treat Crohn disease that involves sites of inflammation in the ileum and/or ascending colon
- Oral prednisone
- IV methylprednisolone
-
Controlled ileal release budesonide
-
Biologics
-
Anti-TNF-α antibodies (e.g., adalimumab, infliximab, certolizumab)
- Increasingly used as a primary agent to induce remission.
- Also used to maintain remission and manage CD refractory to immunomodulators
- Anti-leukocyte trafficking antibody (e.g., vedolizumab) and anti-p40 antibody; (e.g., ustekinumab): used mainly to induce and maintain remission in moderate to severe CD
-
Anti-TNF-α antibodies (e.g., adalimumab, infliximab, certolizumab)
-
Immunomodulators: e.g., thiopurine analogs (azathioprine, 6-mercaptopurine), methotrexate
- Used to maintain remission
- Can be used as a steroid-sparing agent
-
5-aminosalicylic acid derivative: sulfasalazine
- May be considered to induce remission of mild colonic or ileocolonic CD
- Not effective in isolated small bowel disease
-
Antibiotics: not recommended for the primary treatment of CD
- Metronidazole may be beneficial in the prevention of postoperative recurrence of CD.
- Broad-spectrum antibiotics are used for the treatment of abscesses and systemic infections.
Glucocorticoids can be used to induce remission, but they should be discontinued once the acute flare has been managed. [10][22]
Early use of biologics (e.g., anti-TNF-α antibodies) is the standard of care in new, active CD, in moderate to severe disease, and/or if patients have risk factors for progression of CD. [10][26]
Treatment regimens based on disease severity
| Medical management of Crohn disease[10][26][30] | ||
|---|---|---|
| Severity | Common regimens | |
| Induction of remission[10] | Maintenance of remission[10] | |
| Mild CD to moderate CD |
|
|
| Moderate to severe CD[26][32] |
|
|
| Severe to fulminant CD |
|
|
Almost 20% of patients with CD are steroid refractory. [33]
Supportive therapy
-
Pain management [34]
- Use multimodal therapy (e.g., acetaminophen and/or antidepressants).
- Consult pain specialists early.
- Avoid opioids if possible, and use sparingly and with caution if necessary: See also "Risk mitigation for opioid prescribing."
- Antidiarrheal therapy: Consider loperamide . [35]
-
Lifestyle modifications [10]
- Smoking cessation
- NSAID avoidance [10]
- Stress, depression, and anxiety management
-
Dietary optimization
- Enteral nutrition is preferred over parenteral nutrition. [36]
- Identify and treat micronutrient deficiency: Iron deficiency, vitamin D deficiency, and vitamin B12 deficiency are common. [22]
- Identify and treat malabsorption syndrome: E.g., supplement calories, protein, and micronutrients (vitamins, zinc, calcium, iron).
Poor pain control and/or increased opioid use may indicate inadequate disease management. [37]
Antidiarrheals should not be used in patients with bowel obstruction, abdominal tenderness, or signs of systemic infection (e.g., fever). [35]
Surgery [10]
Half of patients with CD require major abdominal surgery within 10 years of diagnosis. [10][36]
-
Indications
- Severe complications (e.g., bowel obstruction; , intraabdominal abscess, perianal abscess) [10]
- Unsuccessful medical therapy
- Symptom control in disease localized to a short segment of the bowel [10][38]
-
Procedures [38]
- Surgical drainage of abscess [10][38]
- Laparoscopic or open resection of the diseased bowel segment (small bowel resection, segmental colectomy) [38]
- Strictureplasty (bowel-sparing technique) [10][38]
Surgery can lead to remission but is not curative, and short bowel syndrome may occur following multiple procedures.
Long-term management
Monitoring of disease activity [10]
-
Endoscopic monitoring
- Schedule an endoscopic exam 6–9 months after treatment is initiated. [39]
- Routine monitoring endoscopy is not recommended in the remission phase.
- Periodic cross-sectional imaging (MR enterography, CTE) : especially in patients with small bowel disease. [10]
- Serial CRP and fecal calprotectin: to assess inflammatory status and treatment efficacy (treating-to-target) [10][27]
Screening for intestinal cancer [10]
- Chronic inflammation increases the risk of intestinal cancer. [22]
- Schedule surveillance colonoscopy with biopsies. [10]
- After 8 years after CD onset in patients with ≥ 30% colonic involvement
- At diagnosis in patients with primary sclerosing cholangitis
Additional preventive care in IBD [40]
- Measures to prevent complications of glucocorticoid therapy
-
Vaccinations [6][40]
- Administer age-appropriate vaccinations preferably before starting immunosuppressant therapy.
- Ensure immunizations are up to date at each follow-up.
- Recommend pneumococcal vaccine, SARS-CoV-2 vaccine, hepatitis B vaccine (if not immune), and yearly influenza vaccine (inactivated).
- Consider herpes zoster vaccine, RSV vaccine, and varicella vaccine.
- See “ACIP immunization schedule” for details.
- Annual screening for skin cancer[40]
- Annual cervical cancer screening: See “Cervical cancer screening for individuals at high risk.” [40]
- Screening for anemia and malnutrition (e.g., CBC, iron-binding studies, folate, vitamin B12, LDH, vitamin D, albumin) [6]
-
Screening for osteoporosis with DXA
- Recommended in all patients with > 3 months cumulative lifetime exposure to glucocorticoids [40]
- Consider screening the following patients at diagnosis and periodically thereafter:
- Children at high risk of osteopenia [41]
- Adults with risk factors for osteoporosis [42]
- Annual screening for depression and anxiety.[40]
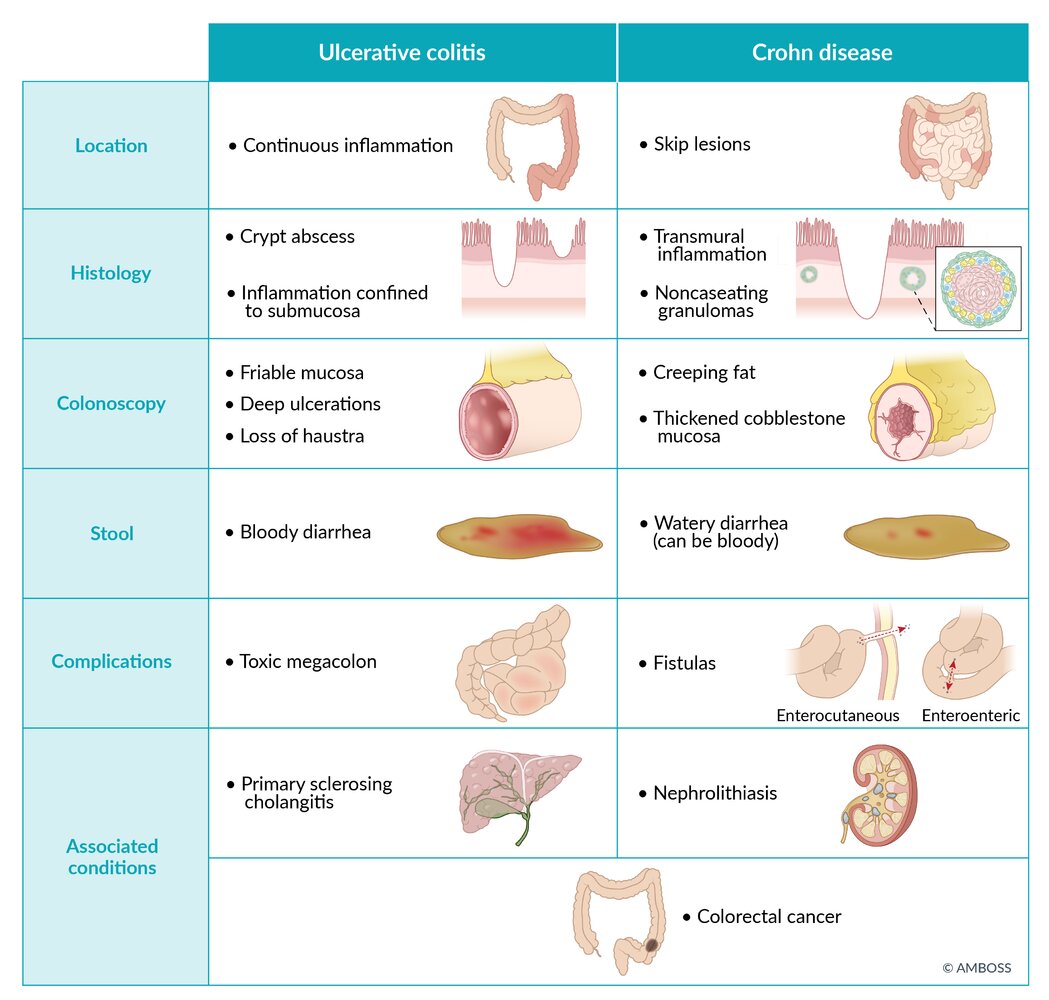
Differential diagnoses
Crohn disease vs. ulcerative colitis
| Ulcerative colitis and Crohn disease | ||
|---|---|---|
| Ulcerative colitis | Crohn disease | |
| Pathophysiology |
|
|
| Frequency/type of defecation |
|
|
| Nutritional status |
|
|
| Physical examination |
|
|
| Extraintestinal manifestations |
|
|
| ||
| Fistulas |
|
|
| Other complications |
|
|
| Cancer risk |
|
|
|
|
|
| Antibodies |
|
|
| Endoscopy and imaging | ||
| Location |
|
|
| Pattern of inflammation |
|
|
| Typical diagnostic findings |
|
|
| Histology |
|
|
| ||
| Treatment | ||
| Medication |
|
|
| ||
| Surgery |
|
|
The crone and the fat granny skipped over the wrecked cobblestones: the most important features of Crohn disease are creeping fat, granuloma, skip lesions, rectal sparing, and cobblestone sign.
Other differential diagnoses
- Acute appendicitis
- Infectious gastroenteritis/colitis [41]
- Noninfectious colitis (ischemic colitis, radiation colitis, adverse drug reaction, etc.) [41]
- Diverticulitis
- Irritable bowel syndrome
- Gastrointestinal tuberculosis
- Malignant intestinal transformations
- Celiac disease [41]
- Indeterminate colitis
The differential diagnoses listed here are not exhaustive.
© AMBOSS
© AMBOSS
Endoscopic view of the colon
Diffuse nodularity and inflammation of the colonic mucosa are visible.
These features are consistent with gastrointestinal tuberculosis. A clinical examination and biopsy are required to confirm the diagnosis.
Source: © IMPP
Complications
Fistulizing CD [10][45]
-
Overview
- Occurs in one-third of patients with CD
- Typically involves the perianal region
- Internal fistulas may involve the bladder, vagina, and/or another portion of the intestine.
- Recurrences are common
- Clinical features: depend on location of the fistula (see “Fistulas”)
- Diagnosis: MRI of the pelvis and/or endoscopic ultrasound
-
Management: Interdisciplinary management including gastroenterology and surgery is required. [10]
-
Anal fistula
- Fistulotomy or seton placement
- Biologic PLUS antibiotic in addition to surgery
-
Internal fistula
- Medical therapy (typically a biologic)[10]
- Consider surgery when the patient is medically optimized.
-
Anal fistula
Other intestinal complications
- Colorectal cancer (especially in the case of pancolitis)
- Short bowel syndrome and associated issues after surgery
- Stenosis/strictures → bowel obstruction/(sub)ileus
- Intestinal perforation → peritonitis
- Primary sclerosing cholangitis
-
Impaired bile acid reabsorption
- Bile acid diarrhea
- Bile acid malabsorption → steatorrhea and deficiencies in fat-soluble vitamins
- Abscess formation/phlegmons
Systemic complications
-
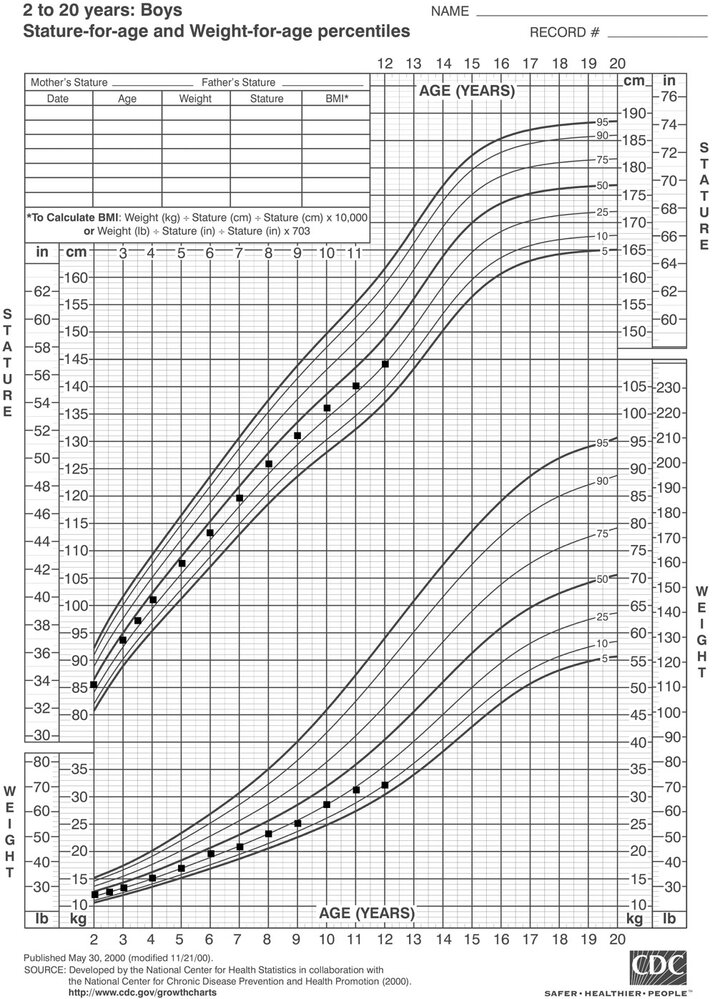
Signs of malabsorption syndrome
- Weight loss
- Failure to thrive and growth failure in children
-
Anemia
- Iron deficiency anemia
- Anemia of chronic disease
- Megaloblastic anemia (vitamin B12 deficiency due to impaired absorption in the chronically inflamed ileum)
- Osteoporosis
- Amyloidosis
We list the most important complications. The selection is not exhaustive.
Special patient groups
Crohn disease in children
See “Inflammatory bowel disease in children.”
Crohn disease in pregnancy
See “Inflammatory bowel disease in pregnancy.”
Prognosis
CD is a chronic disease that is not curable. Patients with any of the following features are at high risk of progression to severe disease; early advanced treatment is recommended to prevent complications of CD. [10]
- Ileocolonic involvement at diagnosis
- Upper GI involvement
- Severe disease (e.g., extensive anatomical involvement, deep ulcers)
- Early need for glucocorticoids
- Young age at diagnosis (< 30 years)
- Perianal or rectal disease
- Previous stenosis, fistula, and/or abscess
- Extraintestinal clinical features at diagnosis
Failure to achieve and maintain remission on therapy is associated with worse clinical outcomes, including stricture and fistula formation and the need for surgery. [27]
External Resources
References
- Loftus EV Jr. "Update on the Incidence and Prevalence of Inflammatory Bowel Disease in the United States.". Gastroenterology & hepatology. 12(11). :704-707. (2016)
- Feuerstein JD, Cheifetz AS. "Crohn Disease: Epidemiology, Diagnosis, and Management". Mayo Clinic Proceedings. 92(7). :1088-1103. (2017)
- "Overview of Crohn's Disease". https://www.crohnscolitisfoundation.org/what-is-crohns-disease/overview
- Daniel C Baumgart, William J Sandborn. "Crohn's disease". The Lancet. 380(9853). :1590-1605. (2012)
- Lichtenstein GR, Loftus EV, Afzali A, et al. "ACG Clinical Guideline: Management of Crohn's Disease in Adults". Am J Gastroenterol. 120(6). :1225-1264. (2025)
- Ray Boyapati, Jack Satsangi, Gwo Tzer Ho. "Pathogenesis of Crohn's disease". F1000Prime Reports. 7. (2015)
- Veauthier B, Hornecker JR. "Crohn's Disease: Diagnosis and Management". Am Fam Physician. 98(11). :661-669. (2018)
- Cohen N, Sror N, Naseer M, et al. "Diagnosis and Management of Upper Gastrointestinal Involvement in Adult Patients With Crohn’s Disease: A Systematic Review". J Clin Gastroenterol Hepatol. (2025)
- Sahyoun L, Gaidos J. "Advances in diagnosis and therapy for upper gastrointestinal Crohn's disease". Curr Opin Gastroenterol. 41(6). :426-431. (2025)
- Makowiec F, Jehle EC, Becker HD, Starlinger M. "Perianal abscess in Crohn's disease". Dis Colon Rectum. 40(4). :443-450. (1997)
- Levine JS, Burakoff R. "Extraintestinal manifestations of inflammatory bowel disease.". Gastroenterology & hepatology. 7(4). :235-41. (2011)
- Vadstrup K, Alulis S, Borsi A, et al. "Extraintestinal Manifestations and Other Comorbidities in Ulcerative Colitis and Crohn Disease: A Danish Nationwide Registry Study 2003–2016". Crohn's & Colitis 360. 2(3). (2020)
- Kapsoritakis AN, Psychos AK, Sfiridaki A, Zintzaras E, Potamianos SP. "Finger clubbing and erythropoietin serum levels in active IBD". Inflamm Bowel Dis. 12(6). :535-536. (2006)
- Spiceland CM, Lodhia N. "Endoscopy in inflammatory bowel disease: Role in diagnosis, management, and treatment". World J Gastroenterol. 24(35). :4014-4020. (2018)
- Cappello M, Morreale GC. "The Role of Laboratory Tests in Crohn's Disease.". Clin Med Insights Gastroenterol.. 9. :51-62. (2016)
- Rubin DT, Ananthakrishnan AN, Siegel CA, et al. "ACG Clinical Guideline Update: Ulcerative Colitis in Adults". Am J Gastroenterol. 120(6). :1187-1224. (2025)
- Rameshshanker R. "Endoscopy in inflammatory bowel disease when and why". World J Gastrointest Endosc. 4(6). :201. (2012)
- A. Ross S, Novak Z, Pati S, B. Boppana S. "Overview of the Diagnosis of Cytomegalovirus Infection". Infect Disord Drug Targets.. 11(5). :466-474. (2011)
- Lee JM, Lee KM. "Endoscopic Diagnosis and Differentiation of Inflammatory Bowel Disease". Clin Endoscop. 49(4). :370-5. (2016)
- Pimentel AM, Rocha R, Santana GO. "Crohn's disease of esophagus, stomach and duodenum". World journal of gastrointestinal pharmacology and therapeutics. 10(2). :35-49. (2019)
- Kim DH, Chang KJ, Fowler KJ, et al. "ACR Appropriateness Criteria® Crohn Disease". Journal of the American College of Radiology. 17(5). :S81-S99. (2020)
- Cushing K, Higgins PDR. "Management of Crohn Disease". JAMA. 325(1). :69. (2021)
- Kredel LI, Siegmund B. "Adipose-Tissue and Intestinal Inflammation - Visceral Obesity and Creeping Fat". Frontiers in Immunology. 5. (2014)
- Timmermans WMC, van Laar JAM, van Hagen PM, van Zelm MC. "Immunopathogenesis of granulomas in chronic autoinflammatory diseases". Clinical & Translational Immunology. 5(12). :e118. (2016)
- Casanova MJ, Chaparro M, Molina B, et al. "Prevalence of Malnutrition and Nutritional Characteristics of Patients With Inflammatory Bowel Disease". Journal of Crohn's and Colitis. 11(12). :1430-1439. (2017)
- Axelrad JE, Lichtiger S, Yajnik V. "Inflammatory bowel disease and cancer: The role of inflammation, immunosuppression, and cancer treatment". World Journal of Gastroenterology. 22(20). :4794. (2016)
- Turner D, Ruemmele FM, Orlanski‐Meyer E, et al. "Management of Paediatric Ulcerative Colitis, Part 1". J Pediatr Gastroenterol Nutr. 67(2). :257-291. (2018)
- Egberg MD, Gulati AS, Gellad ZF, Melmed GY, Kappelman MD. "Improving Quality in the Care of Patients with Inflammatory Bowel Diseases". Inflamm Bowel Dis. 24(8). :1660-1669. (2018)
- Scott F, Ananthakrishnan A, Click B, et al. "AGA Living Clinical Practice Guideline on the Pharmacologic Management of Moderate-to-Severe Crohn’s Disease". Gastroenterology. 169(7). :1397-1448. (2025)
- Colombel JF, Panaccione R, et. al.. "Effect of tight control management on Crohn's disease (CALM): a multicentre, randomised, controlled phase 3 trial". The Lancet. 390(10114). :2779-2789. (2017)
- Lin MV, Blonski W, Lichtenstein GR. "What is the optimal therapy for Crohn’s disease: step-up or top-down?". Expert Rev Gastroenterol Hepatol. 4(2). :167-180. (2010)
- Ray K Boyapati, Joana Torres, Carolina Palmela, et al. "Withdrawal of immunosuppressant or biologic therapy for patients with quiescent Crohn's disease". Cochrane Database of Systematic Reviews. (2018)
- Sulz MC, Burri E, Michetti P, et al. "Treatment Algorithms for Crohn’s Disease". Digestion. 101(Suppl. 1). :43-57. (2020)
- Gomollón F, Dignass A, Annese V, et al. "3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management". Journal of Crohn's and Colitis. 11(1). :3-25. (2016)
- Feuerstein JD, Ho EY, Shmidt E, et al. "AGA Clinical Practice Guidelines on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn’s Disease". Gastroenterology. 160(7). :2496-2508. (2021)
- Lichtenstein GR, Loftus EV, Isaacs KL, et al. "ACG Clinical Guideline: Management of Crohnʼs Disease in Adults". Am J Gastroenterol. 113(4). :481-517. (2018)
- Coates M, Clarke K, Williams E, et al. "Abdominal Pain in Inflammatory Bowel Disease: An Evidence-Based, Multidisciplinary Review". Crohns Colitis 360. 4(5). :137-43. (2023)
- Shah SB, Hanauer SB. "Treatment of diarrhea in patients with inflammatory bowel disease: concepts and cautions.". Rev Gastroenterol Disord. 7 Suppl 3. :S3-10. (2007)
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. "Crohn's disease". The Lancet. 389(10080). :1741-1755. (2017)
- Xue CE, Shen QH, Wang Y, Zhang JY, Lin FR. "[Clinical Significance of the Serum EPO Level in Patients with Iron Deficiency Anemia].". Zhongguo shi yan xue ye xue za zhi. 23(5). :1410-4. (2015)
- Adamina M, Bonovas S, Raine T, et al. "ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment". Journal of Crohn's and Colitis. 14(2). :155-168. (2019)
- Feuerstein JD, Isaacs KL, Schneider Y, et al. "AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis". Gastroenterology. 158(5). :1450-1461. (2020)
- Peyrin-Biroulet L, Sandborn W, Sands BE, et al. "Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target.". Am J Gastroenterol. 110(9). :1324-38. (2015)
- Farraye FA, Melmed GY, Lichtenstein GR, et al. "ACG Clinical Guideline Update: Preventive Care in Inflammatory Bowel Disease". Am J Gastroenterol. 120(7). :1447-1473. (2025)
- Farraye FA, Melmed GY, Lichtenstein GR, Kane SV. "ACG Clinical Guideline: Preventive Care in Inflammatory Bowel Disease". Am J Gastroenterol. 112(2). :241-258. (2017)