Quick guide
Diagnostic approach
- ABCDE survey
- Targeted clinical evaluation
- Assess severity (e.g., using the Westley croup score).
- Consider chest and neck x-ray.


Do not examine the throat of a child with significant stridor because the resulting agitation may precipitate complete airway obstruction.
Do not delay treatment for diagnostic studies.
Red flag features
- Altered mental state
- Dyspnea at rest
- Stridor at rest
- Severe retractions
- Cyanosis
- Pulsus paradoxus
Management checklist
- Consult anesthesia and/or ENT early for severe cases.
- Keep the child calm and comfortable.
- Continuous cardiac and pulse oximetry monitoring
- Supplemental O2 for patients with hypoxemia and/or respiratory distress
- All patients: dexamethasone
- Moderate or severe croup: Add nebulized racemic epinephrine .
- Prepare for difficult airway management.
- Supportive care as needed (e.g., antipyretics, IV fluids)
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.

X-ray neck of a young child (AP view)
The upper tracheal air column, which normally appears with a square-shouldered configuration, has assumed a conical shape (green overlay) reminiscent of a church steeple (steeple sign; cf. illustration).
The steeple sign indicates subglottic airway narrowing and is most commonly seen in croup. However, it may also appear in other conditions (e.g., bacterial tracheitis, tumors). An accompanying lateral radiograph might additionally show inspiratory overdistention of the hypopharynx.
Source: “Croup steeple sign” by Dr Frank Gaillard, Wikimedia Foundation, licensed under CC BY-SA 3.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
{kind=link}
Summary
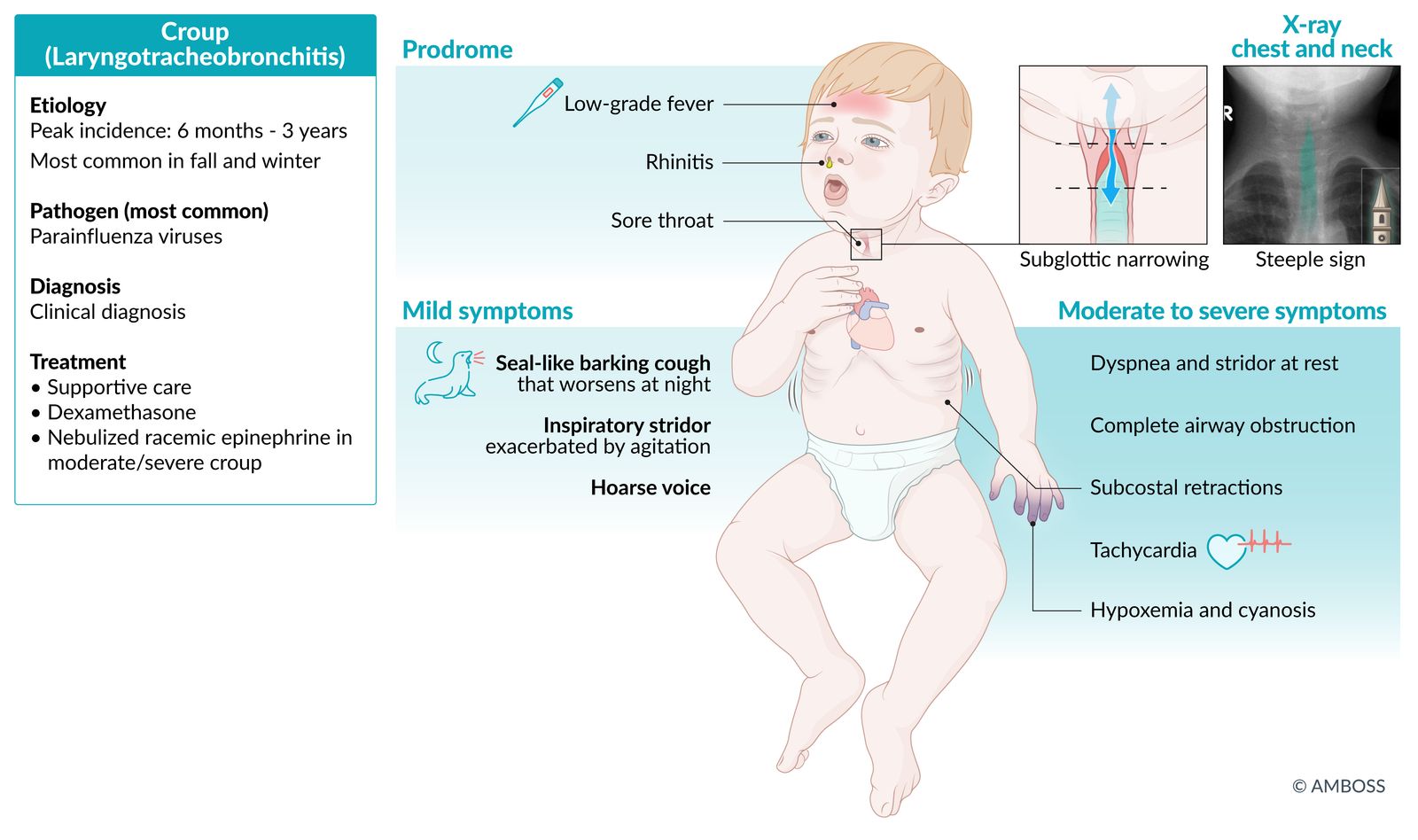
Viral croup (i.e., acute laryngotracheobronchitis) is an inflammation of the upper airway that occurs in young children. It is most often caused by the parainfluenza virus. This condition is characterized by a barking cough, hoarse voice, and inspiratory stridor, all of which often worsen at night. More severe symptoms are associated with higher degrees of airway obstruction and include signs of respiratory distress, which can rarely progress to respiratory failure. Croup is primarily a clinical diagnosis, and diagnostic studies are only performed for severe disease, diagnostic uncertainty, or recurrent episodes of croup. All patients with viral croup should receive glucocorticoids (preferably dexamethasone) and supportive treatment. Patients with moderate or severe croup should also be evaluated for admission and receive nebulized racemic epinephrine and supplemental oxygen. The prognosis of uncomplicated croup is good, and complete recovery typically occurs within seven days of onset.

© AMBOSS
Epidemiology
- Peak incidence: 6 months to 3 years
- Most common in fall and winter
References:[1]
Epidemiological data refers to the US, unless otherwise specified.
Etiology
- Most common pathogen: parainfluenza viruses (75% of cases) [2]
- Other pathogens: respiratory syncytial virus (RSV), adenovirus, influenza virus, SARS-CoV-2 (COVID-19) [3][4]
Pathophysiology
-
Important membrane-bound virulence factors of parainfluenza virus include:
- Hemagglutinin: binds sialic acid → viral entry
- Neuraminidase: release and spread of virions
- Viral infection → inflammation of the upper airway with edema formation and infiltration of inflammatory cells → narrowing of subglottic airway (inspiratory stridor) and increased work of breathing
Clinical features
- Prodromal phase: 1–2 days of upper respiratory tract infection symptoms (rhinitis, low-grade fever, sore throat) [3][5]
- Symptoms of croup ; last 2–7 days and typically manifest in the late evening/night. [3]
-
Characteristic features include seal-like barking cough, hoarseness, and inspiratory stridor due to subglottic narrowing. [3][5]
- Mild croup: Stridor may be absent or only manifest in agitated individuals.
-
Moderate croup
- Stridor and dyspnea may be present at rest.
- Thoracic retractions are typically visible.
- Affected individuals may be tachycardic or tachypneic.
-
Severe croup
- Severe stridor and dyspnea are present at rest.
- Air entry is decreased.
- Hypoxemia, an altered mental state, and/or other signs of impending respiratory failure may be present.
- Upper airway obstruction can cause pulsus paradoxus. [6]
- Agitation can worsen symptoms and precipitate complete airway obstruction.
Do not examine the throat of a child with significant stridor because the resulting agitation may precipitate complete airway obstruction. [7]

Original title: “baby with Croup Stridor Barking Cough visual & audio sound - When to Hospitalize.”. Created by: Juliette Anderson.
© AMBOSS
Subtypes and variants
Spasmodic croup [8][9]
- Etiology: may be triggered by allergies, airway hyperreactivity, or GERD
-
Clinical features
- Barking cough
- Hoarse voice
- Nightly symptoms that resolve during the day
- Diagnostics: See “Diagnostics of croup.”
-
Treatment
- Manage underlying cause (e.g., GERD).
- See “Treatment of croup.”
Diagnosis
General principles [3][10][11]
- Croup is most commonly diagnosed based on the presence of characteristic clinical features of croup.
- Diagnostic studies are not routinely required; do not delay treatment in unstable patients to obtain studies.
- Indications for diagnostic studies include:
- Atypical presentation or diagnostic uncertainty, to rule out differential diagnoses of stridor
- Severe disease
- Recurrent episodes of croup
Do not delay treatment of stridor to perform diagnostic studies.
Imaging
-
X-ray chest and neck (anteroposterior and lateral) [11]
- May identify subglottic narrowing ; on anteroposterior view (steeple sign)
- May show concurrent lower airway involvement [12]
- CT chest and neck: usually performed for differential diagnoses or suspected underlying congenital abnormalities [3][13]
- Laryngoscopy/bronchoscopy: may be performed for suspected foreign bodies or atypical croup [8]
The steeple sign is not specific to croup; it may also be present with bacterial tracheitis, epiglottitis, and noninfectious etiologies such as thermal injuries and neoplasms. [3]
Laboratory studies
-
Respiratory viral panel
- Usually reserved for patients who do not respond to initial treatment [3]
- Most commonly shows parainfluenza; coinfections are common. [5]
- CBC: may help distinguish between bacterial and viral infections [3]
-
Blood gas [14]
- Indicated for severe respiratory symptoms, e.g., signs of impending respiratory failure
- May show hypoxemia and/or CO2 retention
X-ray neck of a young child (AP view)
The upper tracheal air column, which normally appears with a square-shouldered configuration, has assumed a conical shape (green overlay) reminiscent of a church steeple (steeple sign; cf. illustration).
The steeple sign indicates subglottic airway narrowing and is most commonly seen in croup. However, it may also appear in other conditions (e.g., bacterial tracheitis, tumors). An accompanying lateral radiograph might additionally show inspiratory overdistention of the hypopharynx.
Source: “Croup steeple sign” by Dr Frank Gaillard, Wikimedia Foundation, licensed under CC BY-SA 3.0. Modifications: - arrow removed. The supplementary image with overlays of relevant areas was adapted from the image mentioned above and licensed under CC BY-SA 3.0.
Management
Approach [3][10][11]
-
Keep the patient calm and minimize distress.
- Allow the patient to maintain a comfortable position (usually semi-upright). [7]
- Examine the child in the parent's lap. [15]
- Avoid examining the throat as this may precipitate airway obstruction. [7]
- Hypoxemia/signs of impending respiratory failure: Initiate immediate stabilization (e.g., supplemental oxygenation, intubation).
-
Perform a croup severity assessment to guide treatment; consider using a scoring system (e.g., Westley croup score).
- All patients: dexamethasone and supportive care as needed (e.g., antipyretics, IV fluids)
- Patients with moderate/severe croup: Add nebulized racemic epinephrine.
- Regularly reassess patients. [10]
- Admit patients with admission criteria for croup, e.g., severe croup, age < 6 months.
Agitation can worsen symptoms and precipitate complete airway obstruction; keep children calm and defer distressing procedures (e.g., IV placement) until facilities are in place for immediate intubation if required. [16]
Nebulized racemic epinephrine rapidly relieves symptoms of respiratory distress. Dexamethasone provides longer symptom relief but takes up to 6 hours to reduce airway swelling. [3]
Humidified air, both in the hospital and as a home remedy (e.g., steam inhalation), has been used to treat croup, but there is no evidence that it is effective. [3][5][17]
Immediate stabilization [3]
- Contact anesthesia or ENT early because children with croup have difficult airways.
- Initiate respiratory support.
-
Hypoxemia (e.g., pulse oximetry < 92%) and/or signs of respiratory distress
- Start supplemental oxygen (typically humidified).
- Consider modifications to oxygen delivery to prevent worsening agitation. [7][18]
-
Respiratory failure or signs of impending respiratory failure [12]
- Endotracheal intubation is required.
- Bring the difficult airway cart to the bedside.
- The most experienced physician should perform the intubation.
-
Hypoxemia (e.g., pulse oximetry < 92%) and/or signs of respiratory distress
Individuals with croup have difficult airways due to glottic and subglottic stenosis; if intubation is needed, notify anesthesia or ENT as early as possible. [3]
Evidence on the efficacy of helium-oxygen (heliox) mixtures in croup is mixed; routine use is not recommended. [19]
Croup severity assessment
- Follow local or institutional protocols where available.
- Croup scoring systems are susceptible to interobserver variability. [20]
- The most commonly used score is the Westley croup score. [20]
| Westley croup score [3][21] | ||
|---|---|---|
| Clinical features | Score | |
| Level of consciousness | Normal | 0 |
| Disoriented | 5 | |
| Cyanosis | None | 0 |
| With agitation | 4 | |
| At rest | 5 | |
| Stridor | None | 0 |
| With agitation | 1 | |
| At rest | 2 | |
| Air entry | Normal | 0 |
| Decreased | 1 | |
| Markedly decreased | 2 | |
| Retractions | None | 0 |
| Mild | 1 | |
| Moderate | 2 | |
| Severe | 3 | |
Interpretation
| ||
Over 80% of croup cases are mild. [22]
Treatment
- Give dexamethasone (off-label). [3][23]
- Reduces airway swelling within 6 hours
- Effects last up to 72 hours.
- Start supportive care. [3][22]
- Ensure recommended daily fluid intake (oral or IV).
- Offer antipyretics if febrile.
- Educate the family on concerning features, e.g., signs of respiratory distress, signs of significant dehydration.
-
Moderate croup/severe croup: Add nebulized epinephrine. [3][12]
- Preferred: racemic epinephrine [3][12]
- Reduces airway swelling within 30 minutes
- Monitor for 2–4 hours for return of symptoms. [3][11]
- Dose may be repeated as needed.
- Alternative: L-epinephrine [3]
- Preferred: racemic epinephrine [3][12]
Suspect other causes of stridor if there are no symptoms of an upper respiratory infection and if symptoms do not respond to treatments for croup.
Disposition
- Discharge home with return precautions can be considered in the following cases:
- Mild croup
- Moderate croup that has responded to a single nebulized epinephrine treatment
- Patients with severe croup or other risk factors should be admitted; consider pediatric ICU.
Admission criteria for croup [10][12]
- Severe croup
- Need for oxygen or IV fluids
- > 1 treatment with nebulized epinephrine
- Age < 6 months
- Persistent tachypnea or tachycardia
- Complex medical history (congenital cardiac or pulmonary disease, premature birth)
This calculator is provided by the third-party QXMD, who is solely responsible for its content and functionality.
Created by: QxMD.
Differential diagnoses
- See “Causes of stridor,” e.g.:
- Spasmodic croup
- Epiglottitis
- Diptheria
- Foreign body aspiration
- Other causes [3]
- Asthma/virus-induced wheeze
- Pneumonia
The differential diagnoses listed here are not exhaustive.
Complications
- Respiratory failure (rare)
- Pulmonary edema
- Pneumothorax
- Pneumomediastinum
- Secondary bacterial infection (e.g., bacterial tracheitis)
- Cardiac arrest and death
We list the most important complications. The selection is not exhaustive.
Prognosis
- The prognosis in uncomplicated cases is good, with full recovery.
- Parents should be aware that croup tends to recur.
- Most often within a week after recovery
- If croup recurs within the peak incidence age (six months to three years), airway abnormalities should be suspected.
- If croup recurs outside the peak incidence age, atopic conditions, airway lesions or gastroesophageal reflux should be suspected.
External Resources
References
- Lowen AC, Mubareka S, Steel J, Palese P. "Influenza virus transmission is dependent on relative humidity and temperature". PLos Pathog. 3(10). :1470-6. (2007)
- Branche AR, Falsey AR. "Parainfluenza Virus Infection". Semin Respir Crit Care Med. 37(4). :538-54. (2016)
- Smith DK, McDermott AJ, Sullivan JF. "Croup: Diagnosis and Management". Am Fam Physician. 97(9). :575-580. (2018)
- Brewster RC, Parsons C, Laird-Gion J, et al. "COVID-19–Associated Croup in Children". Pediatrics. 149(6). (2022)
- Bower J, McBride JT. "Croup in Children (Acute Laryngotracheobronchitis)". Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. :762-766.e1. (2015)
- Bergelson J, Zaoutis T, Shah SS. "Pediatric Infectious Diseases E-Book". Elsevier Health Sciences. (2008). ISBN: 9780323076333
- American Academy of Pediatrics. "Pediatric Education for Prehospital Professionals". Jones & Bartlett Publishers. (2013). ISBN: 9781449607647
- Hospital JH. "The Harriet Lane Handbook". Elsevier. (2020). ISBN: 9780323674072
- Blaney SM, Giardino AP, Orange JS, et al. "Rudolph's Pediatrics, 23rd Edition". McGraw-Hill Education / Medical. (2018). ISBN: 9781259588594
- Walls R, Hockberger R, Gausche-Hill M. "Rosen's Emergency Medicine". Elsevier Health Sciences. (2018). ISBN: 9780323354790
- Vezzetti R, Carlson J, Pennington D. "Pediatric Imaging for the Emergency Provider E-Book". Elsevier Health Sciences. (2021). ISBN: 9780323708500
- Cooper T, Kuruvilla G, Persad R, El-Hakim H. "Atypical Croup". Otolaryngol Head Neck Surg. 147(2). :209-214. (2012)
- Greydanus DE, Patel DR, Reddy VN. "Handbook of Clinical Pediatrics". World Scientific. (2010). ISBN: 9789814280495
- Durand ML, Deschler DG. "Infections of the Ears, Nose, Throat, and Sinuses". Springer. (2018). ISBN: 9783319748351
- Rudolf M, Luder A, Jeavons K. "Essential Paediatrics and Child Health". John Wiley & Sons. (2020). ISBN: 9781119420248
- Moore M, Little P. "Humidified air inhalation for treating croup". Cochrane Database Syst Rev. (2006)
- Ortiz-Alvarez O. "Acute management of croup in the emergency department". Paediatr Child Health. 22(3). :166-169. (2017)
- Moraa I, Sturman N, McGuire TM, van Driel ML. "Heliox for croup in children". Cochrane Database Syst Rev. 2021(8). (2021)
- Chan A, Langley J, LeBlanc J. "Interobserver variability of croup scoring in clinical practice". Paediatr Child Health. 6(6). :347-351. (2001)
- Westley CR. "Nebulized Racemic Epinephrine by IPPB for the Treatment of Croup". American Journal of Diseases of Children. 132(5). :484. (1978)
- Cherry JD. "Croup". N Engl J Med. 358(4). :384-391. (2008)
- Parker CM, Cooper MN. "Prednisolone Versus Dexamethasone for Croup: a Randomized Controlled Trial". Pediatrics. 144(3). (2019)
- Quraishi H, Lee DJ. "Recurrent Croup". Pediatr Clin North Am. 69(2). :319-328. (2022)