Summary
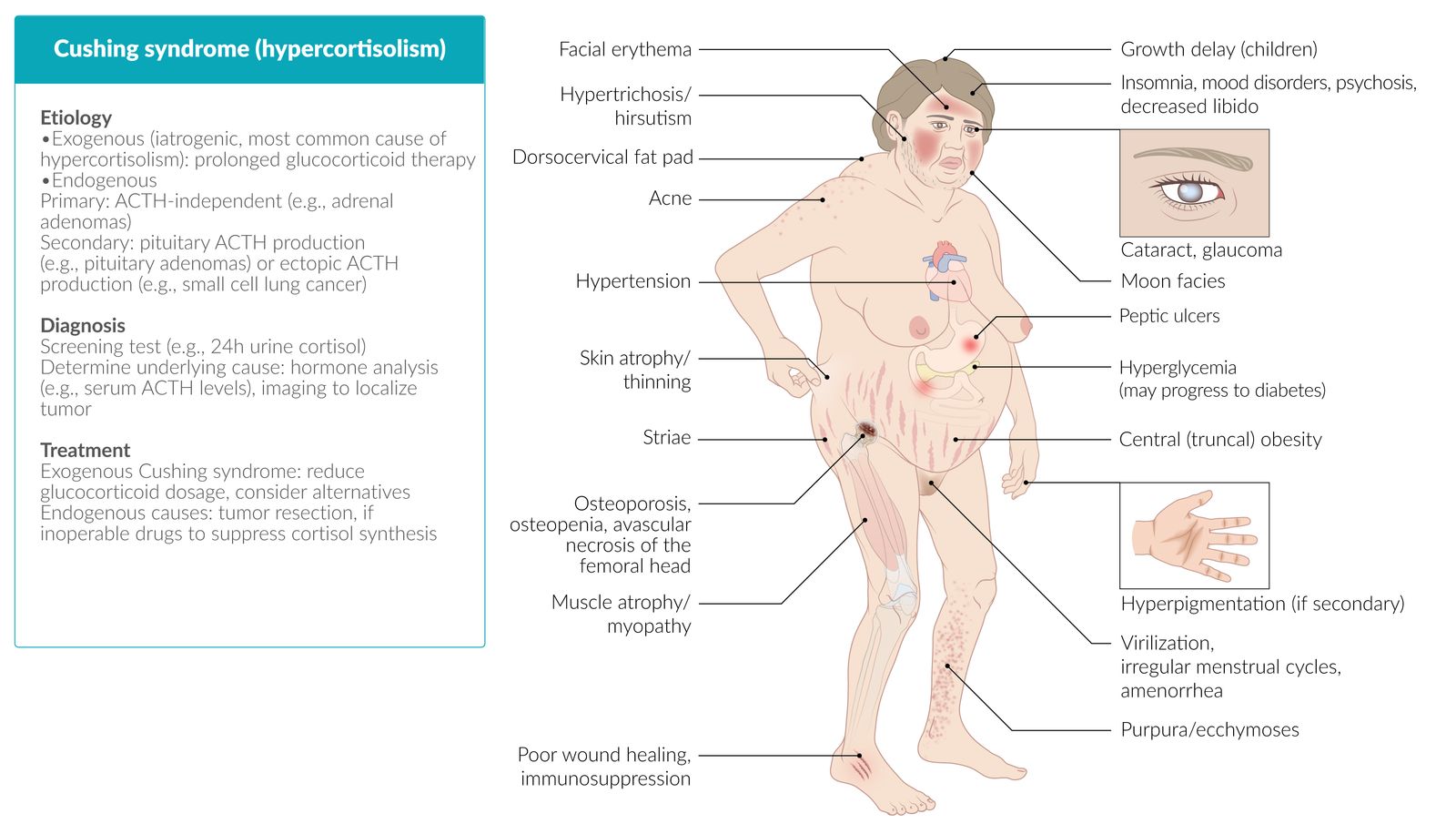
Cushing syndrome is an endocrine disorder caused by hypercortisolism, most commonly due to exogenous glucocorticoid administration (iatrogenic Cushing syndrome). Cushing syndrome can also be caused by endogenous overproduction of cortisol. Primary hypercortisolism is caused by autonomous overproduction of cortisol by the adrenal gland (e.g., due to an adrenal adenoma or carcinoma). Secondary hypercortisolism is the result of elevated adrenocorticotropic hormone (ACTH) due to overproduction by either a pituitary adenoma (Cushing disease) or ectopic, paraneoplastic foci (e.g., in patients with small cell lung cancer). Typical clinical features include central obesity, thin and easily bruisable skin, abdominal striae, secondary hypertension, hyperglycemia, and proximal muscle weakness. Prepubertal children with Cushing syndrome also commonly present with lack of height gain and excessive weight gain. Measurement of cortisol (urine free and/or late-night salivary cortisol) and/or the dexamethasone suppression test are used to diagnose hypercortisolism. Serum ACTH levels are used to differentiate between primary and secondary hypercortisolism. Depending on the suspected type of Cushing syndrome, additional studies may include imaging, further hormone testing, and bilateral sampling of the inferior petrosal sinus. The treatment of endogenous hypercortisolism primarily involves surgical removal of the source of excessive cortisol (e.g., adrenalectomy) or ACTH (e.g., transsphenoidal hypophysectomy) production. Pharmacological treatment aimed at normalizing cortisol levels (e.g., metyrapone) may be used in addition to surgical treatment or as second-line treatment if surgery is unsuccessful.
 fact sheet")
© AMBOSS
Etiology
Exogenous (iatrogenic) Cushing syndrome
- Prolonged glucocorticoid therapy → hypercortisolism → decreased ACTH → bilateral adrenal atrophy
- Most common cause of hypercortisolism
Endogenous Cushing syndrome
| Overview of endogenous Cushing syndrome [1][2] | |||
|---|---|---|---|
| Types | Primary hypercortisolism (ACTH-independent Cushing syndrome) | Secondary hypercortisolism | |
| Pituitary ACTH production (Cushing disease) | Ectopic ACTH production | ||
| Relative frequency [3] |
|
|
|
| Sex |
|
|
|
| Causes |
|
|
|
While the term “Cushing syndrome” can be applied to any cause of hypercortisolism, “Cushing disease” refers specifically to secondary hypercortisolism that results from excessive production of ACTH by pituitary adenomas.
Secondary hypercortisolism is also called ACTH-dependent Cushing syndrome because hypercortisolism is the result of increased ACTH levels.

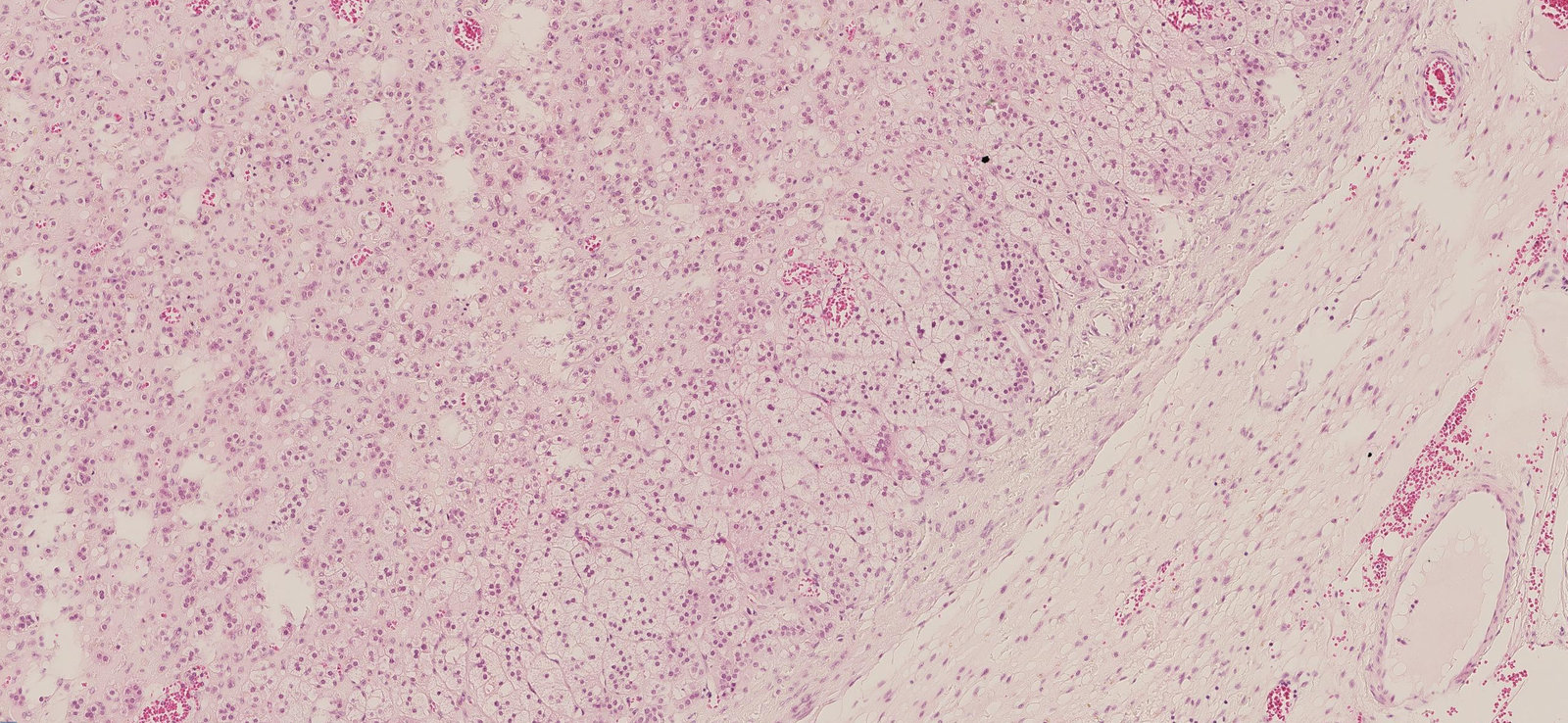
Photomicrograph of adrenal gland tissue (H&E stain; 350x magnification)
Adrenal adenomas are characterized histologically by large cells with a foamy cytoplasm (examples indicated in green), and are therefore similar to the cells in the zona fasciculata. The shape of the cells and their nuclei may be pleomorphic. A fibrous capsule (black) separates the adenoma cells from the other cells of the adrenal gland.
Click on the Smartzoom button to view the entire specimen through a virtual microscope.
Source: © Smart Zoom, Smart In Media. Image and annotations in digital microscopy: PD Dr. med. Alberto Perez Bouza, Facharzt für Pathologie
Clinical features
For additional features in children, see “Cushing syndrome in children.”
Skin [2]
- Thin, easily bruisable skin with ecchymoses
- Stretch marks (classically purple abdominal striae)
- Hirsutism
- Acne
-
If secondary hypercortisolism: often hyperpigmentation (darkening of the skin due to an overproduction of melanin), especially in areas that are not normally exposed to the sun (e.g., palm creases, oral cavity)
- Caused by excessive ACTH production because melanocyte-stimulating hormone (MSH) is cleaved from the same precursor as ACTH called proopiomelanocortin (POMC)
- Not a feature of primary hypercortisolism
- Delayed wound healing
- Flushing of the face
")
Neuropsychological
- Anxiety, irritability
- Lethargy, fatigue
- Sleep disturbance
- Memory deficits
- Depression
- Psychosis
Musculoskeletal [2]
- Osteopenia, osteoporosis, pathological fractures, avascular necrosis of the femoral head
- Muscle atrophy/weakness
Endocrine and metabolic [3]
- Insulin resistance; → hyperglycemia (see “Diabetes mellitus”) → mild polyuria in the case of severe hyperglycemia
- Dyslipidemia
-
Weight gain characterized by
- Central obesity
- Round face (sometimes called “moon facies”)
- Dorsocervical fat pad
- Supraclavicular fat pads
- ♂: Decreased libido, gynecomastia
- ♀: Decreased libido, virilization, and/or irregular menstrual cycles (e.g., amenorrhea)

Other features [1]
- Secondary hypertension (∼ 90% of cases)
- Increased susceptibility to infections (due to immunosuppression)
- Peptic ulcer disease
- Cataracts
“CUSHINGOID” is the acronym for side effects of corticosteroids: Cataracts, Ulcers, Striae/Skin thinning, Hypertension/Hirsutism/Hyperglycemia, Infections, Necrosis (of the femoral head), Glucose elevation, Osteoporosis/Obesity, Immunosuppression, Depression/Diabetes.
Patients with secondary hypercortisolism due to ectopic ACTH production may present with rapid onset of hypertension and hypokalemia without other typical features of Cushing syndrome.
Consider a diagnosis of hypercortisolism in patients who present with proximal muscle weakness, central obesity, thinning skin, weight gain, sleep disturbance, and/or depression.

Multiple vertical, approx. 2-cm wide, violaceous striae are visible along the lateral and ventral thorax of this 32-year-old, overweight man.
This constellation of features suggests Cushing syndrome.
Source: © IMPP

The patient's face appears noticeably round with increased bilateral fat deposition. The cheeks appear plethoric, which is caused by vasodilation of small arteries and arterioles (flushing).
Source: “Figure 1a, in: A Challenging Case of an Ectopic Cushing Syndrome” by J. M. Nunes, E. Pinho, I. Camões et al., Hindawi - Case Reports in Medicine, licensed under CC BY 3.0. Modifications: Original image was made up of 4 images. Image cropped and enlarged.
Diagnosis
Approach [1][4][5]
- Evaluate for clinical features of Cushing syndrome.
- Rule out exogenous Cushing syndrome caused by glucocorticoid administration.
- Obtain initial testing to confirm hypercortisolism; consult endocrinology if the diagnosis remains unclear.
- Refer to endocrinology for further diagnostics and treatment if hypercortisolism is confirmed.
- Identify the cause of hypercortisolism.
- Consider nonneoplastic causes of endogenous hypercortisolism (pseudo-Cushing).
- Determine if Cushing syndrome is ACTH-dependent.
- Order further testing depending on the suspected type of Cushing syndrome.
Prolonged glucocorticoid therapy is the most common cause of hypercortisolism (exogenous Cushing syndrome); further testing is not required in these patients.
Routine laboratory studies [6]
Not required to establish the diagnosis, but if performed, may show the following typical findings:
- Hypernatremia, hypokalemia, metabolic alkalosis
- Hyperglycemia: due to stimulation of gluconeogenic enzymes (e.g., glucose-6-phosphatase) and inhibition of glucose uptake in peripheral tissue
- Hyperlipidemia (hypercholesterolemia and hypertriglyceridemia)
- CBC: leukocytosis without left shift (predominantly neutrophilic), eosinopenia
Testing for hypercortisolism [2][3][4][5][7]
Any of the following tests can be used. The diagnosis is confirmed if at least two of the tests have abnormal results.
-
Urine free cortisol ; [2]
- Free cortisol is measured in a complete 24-hour urine collection.
- Supportive finding: ↑ urine free cortisol [2][3]
-
Low-dose dexamethasone suppression test
- 1 mg of dexamethasone is administered between 11 pm and midnight and serum cortisol is measured the following morning between 8 and 9 am.
- Supportive finding: ↑ early morning serum cortisol level (> 50 nmol/L) [5]
-
Late-night salivary cortisol
- A saliva sample is collected at the patient's usual bedtime.
- Supportive finding: ↑ salivary cortisol (> 4 nmol/L) [5][8]
-
Late-night serum cortisol: not routinely recommended as the initial test but can be used in patients with inconsistent results from previous tests
- A serum sample is taken from the patient (awake or asleep).
- Supportive finding: ↑ serum cortisol (> 210 nmol/L) [4]
Consult an endocrinologist for further evaluation if any of the findings above are present or if the results are negative despite a high pretest probability.
Identifying the cause [5]
Initial evaluation
- Consider nonneoplastic and physiological causes of hypercortisolism based on clinical features and patient history (e.g., depression, heavy alcohol use, obesity) and in pregnant patients. [9]
-
Measure serum ACTH levels.
- Low (< 5 pg/mL): Suspect primary hypercortisolism (ACTH-independent). [2][10]
- Inappropriately normal OR elevated (> 20 pg/mL): Suspect secondary hypercortisolism (ACTH-dependent). [2][3][10]
-
Proceed based on the results.
-
If ACTH-independent hypercortisolism is suspected: Obtain adrenal MRI and/or CT.
- Assess for an adrenal tumor (e.g., adrenal adenoma, carcinoma, hyperplasia).
- The adrenal cortex contralateral to the tumor shows atrophy due to reduced ACTH stimulation.
- If ACTH-dependent hypercortisolism is suspected: Obtain further testing.
-
If ACTH-independent hypercortisolism is suspected: Obtain adrenal MRI and/or CT.
Differentiating between Cushing syndrome and nonneoplastic-physiologic hypercortisolism can be very challenging. If there is any doubt, refer the patient to a specialized center.

Further testing in patients with ACTH-dependent hypercortisolism [2][5]
The goal is to differentiate between Cushing disease and ectopic ACTH production. A combination of tests is often necessary.
-
Obtain a pituitary MRI to evaluate for Cushing disease (see also “Diagnostics” in “Pituitary adenoma”).
- Pituitary adenoma > 10 mm confirms Cushing disease.
- If there is no evidence of a pituitary adenoma or findings are unclear, obtain either: [5]
- Bilateral sampling of the inferior petrosal sinus
- Hormone testing in ACTH-dependent hypercortisolism
-
If ectopic ACTH production is suspected: imaging to locate the ACTH-producing primary malignancy (e.g., SCLC, RCC, neuroendocrine tumor).
- Multiple studies are often necessary. [10]
- May include a thin-slice whole-body CT scan and functional imaging (e.g., PET scan)
Abdominal CT or MRI in a patient with Cushing disease will show bilateral hyperplasia of both the zona fasciculata and zona reticularis.
| Hormone testing in ACTH-dependent hypercortisolism [2][5] | ||
|---|---|---|
| Important considerations | Findings | |
| CRH stimulation test [10] |
|
|
| Desmopressin stimulation test | ||
| High-dose dexamethasone suppression test [2] |
|
|
The results of these tests must always be considered in the clinical context, and a combination of tests is usually necessary. Hormone-secreting pituitary microadenomas cannot always be detected on imaging and, conversely, small endocrine-inactive tumors may be detected in healthy individuals, potentially leading to overdiagnosis.
| Differential diagnosis of Cushing syndrome [2][5] | ||||
|---|---|---|---|---|
| Normal | Primary hypercortisolism | Ectopic ACTH secretion | Cushing disease | |
| ACTH levels | ↔︎ | ↓ | ↑ | |
| Low-dose dexamethasone suppression test | ↓ Cortisol | ↔︎ Cortisol | ||
| High-dose dexamethasone suppression test | ↓ Cortisol | ↔︎ Cortisol | ↓ Cortisol | |
| CRH and desmopressin stimulation tests | ↑ ACTH, ↑ cortisol | ↔︎ ACTH, ↔︎ cortisol | ↑ ACTH, ↑ cortisol | |
In Cushing syndrome, only patients with Cushing disease remain (partially) susceptible to cortisol suppression (high-dose dexamethasone suppression test) and stimulation (CRH stimulation test).
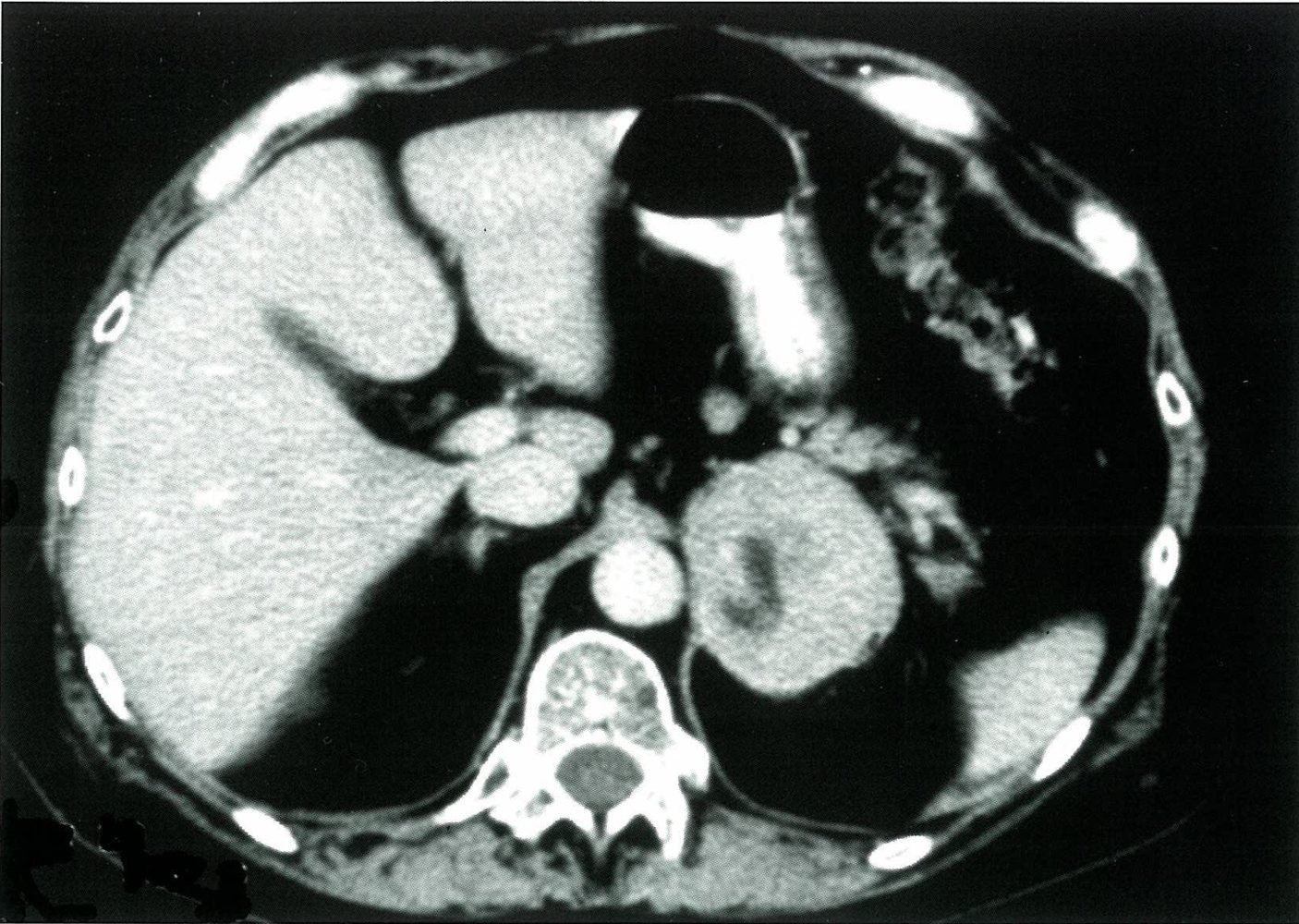
CT abdomen (with oral and intravenous contrast; axial plane)
A large heterogeneously enhancing left adrenal mass (M) shows central necrosis (green overlay). No plane is seen between the mass and the adjacent diaphragmatic crus (arrow). The right adrenal gland is small (red overlay).
A: aorta; L: liver; I: intestine; M: adrenal mass; Sp: spleen; St: stomach; Vb: vertebral body
Source: © IMPP
Treatment
The following section applies to endogenous Cushing syndrome. For patients with exogenous Cushing syndrome, consider lowering the dose of glucocorticoids or replacing them.
Approach [2][3][5][11]
- Manage with a multidisciplinary team including an endocrinologist.
- First-line treatment: tumor resection
- Second-line or adjunctive therapy: pharmacological treatment
Patients who develop adrenal insufficiency after surgery require lifelong glucocorticoid replacement therapy.
Enzyme inhibitors (e.g., metyrapone, ketoconazole) suppress cortisol synthesis, while glucocorticoid antagonists block the action of cortisol in peripheral tissues.
Supportive management [11]
- Educate patients about the disease, including the risk of recurrence and the increased risk for venous thromboembolism.
- Ensure vaccinations are up-to-date in accordance with the ACIP immunization schedule.
- Screen for and treat any common comorbidities (e.g., diabetes, hypertension, osteoporosis, psychiatric disorders).
First line: curative surgery [12]
Radiotherapy and/or chemotherapy may be indicated as part of the management of the causative tumor.
Surgical procedures
- Primary hypercortisolism: : unilateral or bilateral laparoscopic or open adrenalectomy for adrenocortical tumors
- Cushing disease: transsphenoidal hypophysectomy
- Ectopic ACTH production: tumor resection with node dissection, as appropriate
Follow-up
- Patients should receive lifelong monitoring for recurrence by a specialist.
-
Glucocorticoid replacement therapy is often necessary after surgery.
- Reevaluate 6–18 months after unilateral adrenalectomy or resection of ACTH-secreting tumors.
- Lifelong glucocorticoid replacement therapy is required after bilateral adrenalectomy (see “Treatment” in “Adrenal insufficiency”).
Pharmacological treatment
Decisions about pharmacotherapy should be guided by an endocrinologist.
| Pharmacological treatment of Cushing syndrome [5][11] | |||
|---|---|---|---|
| Examples | Indications | ||
| Enzyme inhibitors |
|
|
|
| Glucocorticoid antagonists |
|
||
| Pituitary targeted drugs | Dopamine agonists |
|
|
| Somatostatin analogues |
|
||
Bilateral adrenalectomy [11]
-
Indications
- Primary hypercortisolism caused by bilateral adrenal disease (recommended curative treatment)
- Emergency treatment in severe ACTH-dependent hypercortisolism that cannot be controlled pharmacologically
- Symptomatic treatment for metastatic or occult ectopic tumors
-
Complication: Nelson syndrome (post adrenalectomy syndrome) [13]
- Etiology: bilateral adrenalectomy in patients with a previously undetected pituitary adenoma
- Pathophysiology: bilateral adrenalectomy → no endogenous cortisol production → no negative feedback from cortisol on the hypothalamus → ↑ CRH production → uncontrolled enlargement of preexisting but undetected ACTH-secreting pituitary adenoma → ↑ secretion of ACTH and MSH → manifestation of symptoms due to pituitary adenoma and ↑ MSH
- Clinical features: headache, bitemporal hemianopia (mass effect), cutaneous hyperpigmentation
- Diagnostics
- High levels of β-MSH and ACTH
- Pituitary adenoma on MRI confirms the diagnosis.
- Treatment: surgery (e.g., transsphenoidal resection) and/or pituitary radiation therapy (e.g., if the tumor cannot be fully resected)
Cushing syndrome in children
Etiology [5][14]
- Most common: exogenous glucocorticoid exposure [14]
- Less common: endogenous Cushing syndrome [5][14]
- Children < 6 years: usually due to adrenal causes
- Children ≥ 6 years: usually due to ACTH-secreting pituitary tumors
Clinical features [5][14][15]
- Clinical features of Cushing syndrome are similar in adults and children.
- Key findings specific to children include:
- Lack of height gain combined with excessive weight gain
- Atypical pubertal development (e.g., delayed gonadarche, advanced adrenarche)

Diagnosis [5][14]
Diagnostics for Cushing syndrome are similar in children and adults, with the following exceptions:
- Refer to a pediatric endocrinologist to differentiate ACTH-dependent causes from ACTH-independent causes.
- The following tests require adaptations for children: [15]
- Dexamethasone suppression test: Lower doses may be required depending on weight.
- Urinary free cortisol: Correct for body surface area.
- Consider genetic screening in children with any of the following: [5]
- A family history of endocrine tumors
- Clinical features suggesting a genetic syndrome
Management [5][14]
Refer all children to a multidisciplinary center with specialist expertise (e.g., pediatric endocrinology, neurosurgery). Management of Cushing syndrome is similar in children and adults, with the following exceptions:
- Ketoconazole (off-label) or metyrapone (off-label) is the preferred pharmacotherapy when indicated. [5]
-
Growth hormone replacement is often necessary to optimize height.
- Evaluate for growth hormone deficiency 3–6 months postoperatively. [5]
- Replace growth hormone if deficiency is confirmed.

Photograph of a child's face.
A round, flushed face (moon facies) and increased facial hair growth (hirsutism) are seen.
These features are characteristic of Cushing syndrome.
© Massachusetts Medical Society. All rights reserved. AMBOSS SE, exclusive licensee.
References
- Castinetti F, Morange I, Conte-Devolx B, Brue T. "Cushing’s disease". Orphanet J Rare Dis. 7(1). :41. (2012)
- Feelders R, Sharma S, Nieman L. "Cushing's syndrome: epidemiology and developments in disease management". Clin Epidemiol. :281. (2015)
- Nieman LK, Ilias I. "Evaluation and treatment of Cushing’s syndrome". Am J Med. 118(12). :1340-1346. (2005)
- Lynnette K. Nieman, Beverly M. K. Biller, James W. Findling, et al. "The Diagnosis of Cushing's Syndrome: An Endocrine Society Clinical Practice Guideline". The Journal of Clinical Endocrinology & Metabolism. 93(5). :1526-1540. (2008)
- Fleseriu M, Auchus R, Bancos I, et al. "Consensus on diagnosis and management of Cushing's disease: a guideline update". The Lancet Diabetes & Endocrinology. 9(12). :847-875. (2021)
- Jameson JL, Fauci AS, Kasper DL, et al. "Harrison's Principles of Internal Medicine, Twentieth Edition (Vol.1 & Vol.2)". McGraw-Hill Education / Medical. (2018). ISBN: 9781259644030
- Carroll TB, Findling JW. "The diagnosis of Cushing's syndrome.". Rev Endocr Metab Disord. 11(2). :147-53. (2010)
- Papanicolaou DA, Yanovski JA, Cutler GB, Chrousos GP, Nieman LK. "A Single Midnight Serum Cortisol Measurement Distinguishes Cushing’s Syndrome from Pseudo-Cushing States1". The Journal of Clinical Endocrinology & Metabolism. 83(4). :1163-1167. (1998)
- Findling JW, Raff H. "DIAGNOSIS OF ENDOCRINE DISEASE: Differentiation of pathologic/neoplastic hypercortisolism (Cushing’s syndrome) from physiologic/non-neoplastic hypercortisolism (formerly known as pseudo-Cushing’s syndrome)". European Journal of Endocrinology. 176(5). :R205-R216. (2017)
- Arnaldi G, Angeli A, Atkinson AB, et al. "Diagnosis and Complications of Cushing’s Syndrome: A Consensus Statement". J Clin Endocrinol Metab. 88(12). :5593-5602. (2003)
- Lynnette K. Nieman, Beverly M. K. Biller, James W. Findling, et al. "Treatment of Cushing's Syndrome: An Endocrine Society Clinical Practice Guideline". The Journal of Clinical Endocrinology & Metabolism. 100(8). :2807-2831. (2015)
- R. van der Pas, F.W.G. Leebeek, L.J. Hofland, W.W. de Herder, R.A. Feelders. "Hypercoagulability in Cushing's syndrome: prevalence, pathogenesis and treatment". Clin Endocrinol (Oxf). 78(4). :481-488. (2013)
- Banasiak MJ, Malek AR. "Nelson syndrome: comprehensive review of pathophysiology, diagnosis, and management". Neurosurg Focus. 23(3). :1-10. (2007)
- Lodish MB, Keil MF, Stratakis CA. "Cushing’s Syndrome in Pediatrics". Endocrinol Metab Clin North Am. 47(2). :451-462. (2018)
- Ferrigno R, Hasenmajer V, Caiulo S, et al. "Paediatric Cushing’s disease: Epidemiology, pathogenesis, clinical management and outcome". Rev Endocr Metab Disord. 22(4). :817-835. (2021)